Dr Nagham Al-Mozany. Colorectal Surgeon Auckland City Hospital Clinical Senior Lecturer University of Auckland
|
|
|
- Rosalind Holt
- 5 years ago
- Views:
Transcription

1 Dr Nagham Al-Mozany Colorectal Surgeon Auckland City Hospital Clinical Senior Lecturer University of Auckland 12:05-13:00 WS #33: Management of Benign Rectal Bleeding




2 Management of Benign Rectal Bleeding and Red flags DR. NAGHAM AL-MOZANY
3 Declaration of conflict of interest I CONFIRM THAT I DO NOT HAVE ANY CONFLICT OF INTEREST TO DECLARE
4 I never ate sweet things before I met you, I didn t know someone could be so passionate working with poo



5 Who am I? Colorectal & General Surgeon Auckland City Hospital MacMurray Centre (private) Mercy Hospital University of Auckland RACS
6 Presentation Objectives Classification of rectal bleeding Identifying red flags Overview of common rectal bleeding presentations Cases Take home messages QUIZ with Prize for the winner! Mercy Stand

7

8 Classification of rectal bleeding Age of patient



9 Classification of rectal bleeding: Age of patient Site of bleeding Upper GI source Anything in the middle Lower GI source


10 Site of bleeding-anything in the middle Small bowel GIST tumour

11 Classification of rectal bleeding Age of patient Site of bleeding Painful or Painless


12 Nature of Perianal pain Think Anal Fissure Tearing sensation Burning Glass shards/sharp Razor blades coming out of my bottom Hot poker

13 Nature of Perianal pain THINK HAEMORRHOIDS... Dull ache Throbbing Discomfort Worse on sitting

14 Classification of rectal bleeding Age of patient Site of bleeding Painful or Painless Colour of blood

15 Colour: Does it really matter? Colour/Nature of bleeding Fresh Malaena Clots Mixed in or separate to stool Volume Frequency Stool type

16
17 Patient History Key Points Painful/Painless Duration Frequency Colour of blood Blood mixed or separate from stools +/- mucus Change in bowel habit Unintentional weight loss
18 Patient History Key Points Blood dripping/on wiping Prolapsing masses Type of Stool (Bristol stool chart) Straining on defecation Anti-coagulants/NSAIDS/Laxatives Topical ointments Previous colonoscopy/gastroscopy

19 Patient Examination Abdominal examination Rectal examination
20 What do you look for during a rectal examination Inspect: Signs of Pruritis Ani / anal irritation Hygiene External haemorrhoids/skin tags Fissures Fistulas/Sinus opening
21 If you don t put your finger in, you might put your foot in it Bailey & Love s Textbook of Surgery
22 Rectal examination Anal tone (hyper-/hypo-/normal) Mass? Prostate/Cervix Tender or not? Blood on glove? Bed Side Adjuncts.


23 Proctoscopy

24 Rigid Sigmoidoscopy
25 Investigations FBC, Iron studies Faecal specimen Faecal calprotectin >200mcg/g normal range 0-50mcg/g Sensitivity 70%, specificity 92% for intestinal inflammation Don t check FOBT using Faecal Immunochemical Test (FIT) It is only suitable for, and validated as a screening test for colorectal cancer when applied to an average risk, asymptomatic population
26 Referral Criteria for Direct Access Outpatient Colonoscopy or CT Colonography 2/52 category: Known or suspected CRC (on imaging, or palpable, or visible on PR exam) Unexplained rectal bleeding (benign anal causes treated or excluded) with iron deficiency anaemia Altered bowel habit > six weeks duration + unexplained rectal bleeding (benign anal causes treated or excluded) aged 50 years
27 6/52 category Altered bowel habit > six weeks duration + unexplained rectal bleeding (benign anal causes treated or excluded), aged years Unexplained rectal bleeding (benign anal causes treated or excluded) aged 50 years Unexplained iron deficiency anaemia NZGG Category 2: family history plus one or more of altered bowel habit > six weeks duration + unexplained rectal bleeding (benign and anal causes treated or excluded), aged 40 years NZGG Category 3: family history plus one or more of altered bowel habit > six weeks duration + unexplained rectal bleeding (benign and anal causes treated or excluded), aged 25 years Suspected/assessment inflammatory bowel disease Imaging reveals polyp > 5mm
28 Urgent referral triage Rectal bleeding? Tenesmus? Change in bowel habit >6/52? Unexplained weight loss? Abdominal pain or mass? Mass on rectal examination? Iron deficiency anaemia?
29 Common presentations of rectal bleeding Anal fissure Haemorrhoids Diverticular disease Colorectal cancer
30 Anal Fissure Tear in anoderm of the anal canal Any age group 15-50y Main symptoms: Severe pain during defecation Burning/Sharp/Glass shards Pruritis ani +/- discharge Bright red bleeding on wiping



31 Aetiology? Trauma Sphincter spasm Ischaemia
32 Classification of fissures- Think 6/52! ACUTE FISSURE Painful to examine Bleeding Hypertonic sphincter (anal spasms) CHRONIC FISSURE Sentinel pile posteriorly at edge of anus Hypertrophic anal papilla anteriorly Muscle fibres of internal sphincter seen


33 Acute fissure Posterior


34 Chronic fissure
35 Anal Fissures Fissures occurring off to the midline think of Crohn s disease, anal cancer, STI s, TB, HIV 4% of Crohn s disease patients will have an anal fissure as the first manifestation of Crohn s disease
36 Treatment Relieve Sphincter Spasm Alleviate Ischaemia Promote healing
37 How to relieve sphincter spasm? Chemical: GTN, Calcium channel blockers Neurotoxic: Botox Mechanical: Sphincterotomy
38 Treatment of fissures- Think 6/52 NON-OPERATIVE Dietary Modification Laxatives e.g. Metamucil, Lactulose OPERATIVE Botox Surgery (Lateral sphincterotomy) Topical therapy Avoid steroid creams

39 Nitroglycerin (GTN topical therapy) Relaxes the internal anal sphincter Reduces anal sphincter spasm Promotes blood flow to fissure site and promotes healing 0.2% concentration Efficacy 46-86%

40 TDS for 6/52 Headaches (dose related) If elderly on GTN for angina, then use BD for 6/52 Contraindicated in pregnancy and lactation Not indicated in chronic fissures

41 Topical Calcium channel blockers (2% Diltiazem ointment) Vasodilator Promotes blood flow to the anal sphincter muscle Relaxes sphincter muscle tone Reduced frequency of headaches Itchiness/perianal skin irritation

42

43 When to refer patients with fissures? Chronic fissure Failure to improve post 6/52 treatment Atypical fissures ( OFF to the midline), suspected Crohn s patients Painless fissures

44 What would I do Botulinum Toxin A Lasts 3-6 months Costs $ Prevents release of acetylcholine by presynaptic nerve terminals Minor temporary flatus incontinence and leakage

45 What would I do Sphincterotomy Requires anaesthesia Day case admission Efficacy 90-95% 1-2% risk of permanent incontinence

46
47 Common presentations of rectal bleeding Anal fissure Haemorrhoids Diverticular disease Colorectal cancer
48








49 Aetiology of Haemorrhoids/ Piles 40% of people are asymptomatic

50 I have roid rage. It s not from taking steroids but actually from an extremely painful haemorrhoid
51 Symptoms Haematochezia- drips in toilet bowl, splashes Pruritis ani Mucus discharge Prolapse Pain Anaemia from haemorrhoidal bleeding is rare



52 Investigation

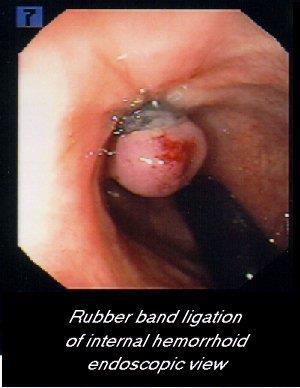
53 Classification of haemorrhoids Internal: Above dentate/pectinate line Usually not painful Painful if thrombosed or necrotic May prolapse 4 grades

54


55 Refer acutely: Gangrenous/Necrotic internal haemorrhoids

56 External thrombosed haemorrhoid Very painful Pain resolves in 3-4 days Swelling takes few weeks to disappear Skin tag
 Stool softners Lignocaine gel Ultraproct Ice")
57 Management of thrombosed external haemorrhoids: (Nagham s cocktail) Analgesia (Paracetamol, NSAID, Tramadol) Stool softners Lignocaine gel Ultraproct Ice Gloved
58 Perianal haematoma? external thrombosed haemorrhoid Collection of blood around the anus Caused by ruptured vein Severe pain and sudden onset of perianal skin swelling Cannot be pushed in Pain settles after 5 days Five day wonder Blue tinge to skin Marble

59 When to refer a perianal haematoma? Refer acutely if Not settled
60 Complications of haemorrhoids Bleed Prolapse Ulcerate Thrombosis Strangulate Gangrene Fibrosis Skin tag
61 If in doubt, send a photo with the referral REMEMBER TO ASK PERMISSION FROM YOUR PATIENT FIRST!

62 What can you do?
63 You don t defecate in a library so you shouldn t read in the bathroom
64 The effectiveness of Sitz bath in managing adult patients with anorectal disorders: A systematic review Siew Ping DL(1), Chi TP, Li GJBI Libr Syst Rev. 2010;8(11): M, Nk EA. 4 RCTs No significant impact in reducing overall intensity of pain and post operative pain No impact in accelerating wound healing Patients satisfied using Sitz bath CONCLUSION: No strong evidence to support the use of sitz bath for pain relief, and accelerate wound healing. No complications were reported

65

66

67



68
69 What Laxative do I prescribe? Fiber supplements: Soften the stool and stimulate a bowel movement e.g. Metamucil Osmotic laxatives: Increase the amount of fluid secreted within the intestines, resulting in softer and easier-to-pass stools e.g. Lactulose Herbal stimulant laxatives: contain anthranoids that stimulate the intestines, improving motility in the gut e.g. Senna Stimulant laxatives: Speed up colonic motility thus inducing a bowel movement e.g. Ducolax


70 The Natural Stuff.

71 Used in haemorrhoids and pruritis ani symptoms Contains cinchocaine HCL: provides analgesia, anaesthesia and spasmolytic Hydrocortisone: anti-pruritic and anti-inflammatory Topical ointments Suppository Topical therapy for haemorrhoids $

72 Topical therapy for haemorrhoids Contains zinc sulphate and pramoxine HCL Reduces irritation Acts as an astringent Anti-pruritic Topical ointment and suppositories $15.99 online pharmacy
73 Topical therapy for haemorrhoids Long acting Fluocortolone: antiinflammatory, anti-pruritic and anti-allergenic Cinchocaine: Local anaesthetic Topical BD-QID Suppository: OD-TDS No more than 1/12 use
74 Who to refer to colorectal surgeon? Symptomatic grade 1-2 internal haemorrhoids that have failed medical treatment Grade 3-4 bleeding internal haemorrhoids Acute thrombosed external haemorrhoids that are not improving Necrotic/gangrenous internal haemorrhoids Large skin tags causing pruritis and discharge symptoms


75 Sclerotherapy with 5% oily phenol

76


77 Excisional haemorrhoidectomy (open/closed)
78 Common presentations of rectal bleeding Anal fissure Haemorrhoids Diverticular disease Colorectal cancer

79 Diverticular Disease Common Left-sided Painless Rectal bleeding Alternating diarrhoea/constipation Risk Factors: NSAID

80 Diverticular bleeding Massive volumes Frequent bleeding, unstable REFER acutely for CT Angiogram Low volume, frequent, stable refer for scope

81

82 Colorectal cancer

83 Select a cancer group: Registrations Number of registrations, 2015 Rate (registrations per 100,000) Cancer (ICD Code) Male Female Total Male Female Total Digestive organs - C15-C Oesophagus - C Stomach - C Small intestine - C Colon, rectum and rectosigmoid junction - C18-C Anus - C Liver - C Gallbladder - C Other biliary tract - C Pancreas - C Other digestive organs - C Source: New Zealand Cancer Registry Note: rates are expressed per 100,000 population and age standardised to the WHO World Standard Population.
84 Figure 1: Female cancer registration rates, by site,25+, Maori and Non-Maori Māori females had a significantly lower colorectal cancer registration rate than non-māori females (RR 0.80, CI )
85 NBSP rolled out across DHBs in 2017 Entire NZ to offer bowel screening by end of 2021 Eligible age 60-74

86 Tenesmus Incomplete evacuation Blood Usually painless Change in bowel habit >6/52 Iron deficiency anaemia PR Mass Refer urgently!

87 CEA (Carcinogenic Embryonic Antigen) Useful for surveillance (detecting recurrence) Not for screening Not all bowel cancers secrete the glycoprotein Increasing trend is VIP Sensitivity 30-80% Specificity 40%
88 CEA (Carcinogenic Embryonic Antigen) Auckland normal range 0-3 ug/l Confounding factors: Smoking Infection IBD Liver cirrhosis Chemo and Radiotherapy

89
90 Case 40 yr Female, 3/12 history of prolapsing, bleeding haemorrhoids that require digitation. She has trialled ultraproct and stool softners without effect. Q: What type of haemorrhoid does she have and what do you do? A. External haemorrhoid. Continue with current management B. Grade 2 Internal haemorrhoid. Continue with current management C. Grade 2 Internal haemorrhoid. Refer to colorectal surgeon for banding D. Grade 3 Internal haemorrhoid. Refer to colorectal surgeon for banding E. External haemorrhoid. Refer to colorectal surgeon for surgery
91 Case 40 yr Female, 3/12 history of prolapsing, bleeding haemorrhoids that require digitation. She has trialled ultraproct and laxatives without effect. Q: What type of haemorrhoid does she have and what do you do? A. External haemorrhoid. Continue with current management B. Grade 2 Internal haemorrhoid. Continue with current management C. Grade 2 Internal haemorrhoid. Refer to colorectal surgeon for banding D. Grade 3 Internal haemorrhoid. Refer to colorectal surgeon for banding E. External haemorrhoid. Refer to colorectal surgeon


92 Case : 27 yr female, with change in bowel habit, mucus discharge and mild perianal pain

93 Case : 69 yr female, 1/7 history of with rectal bleeding, frequency of 30 minutes, on Warfarin. No previous scopes. What is the likely diagnosis? What would you do?
94 Case : 71 yr male with 1/12 intermittent rectal bleeding, mixed with stool, on Clopidogrel, change in bowel habit, difficult emptying and LIF pain What are the differential diagnoses? What would you do?


95 Stricture of sigmoid colon


96 Diverticular stricture vs. Colon cancer

97
98 TAKE HOME MESSAGES Pain or Painless If you don t put your finger in it, you put your foot in it! Be aware of atypical/chronic fissures Red flags for CRC


99 If in doubt, please call us

100 Thank you for your time
Dr Stephanie Ulmer General Surgeon Middlemore Hospital Auckland
 Dr Stephanie Ulmer General Surgeon Middlemore Hospital Auckland 16:30-17:25 WS #168: Modern Treatment of Haemorrhoids 17:35-18:30 WS #180: Modern Treatment of Haemorrhoids (Repeated) BOTTOMS Science and
Dr Stephanie Ulmer General Surgeon Middlemore Hospital Auckland 16:30-17:25 WS #168: Modern Treatment of Haemorrhoids 17:35-18:30 WS #180: Modern Treatment of Haemorrhoids (Repeated) BOTTOMS Science and
Management Of Rectal Bleeding In The Community: How A Shared Care Approach Can Benefit Dr. Daniel Lee
 Management Of Rectal Bleeding In The Community: How A Shared Care Approach Can Benefit Dr. Daniel Lee MD, MMed (S'pore), FRCS (Edin) Associate Consultant Department of Surgery 9 January 2016 Incidence
Management Of Rectal Bleeding In The Community: How A Shared Care Approach Can Benefit Dr. Daniel Lee MD, MMed (S'pore), FRCS (Edin) Associate Consultant Department of Surgery 9 January 2016 Incidence
Anal Fissure: Finding the Root Cause
 Anal Fissure: Finding the Root Cause Michael A. Jobst, MD, FACS, FASCRS Surgical Associates, PC -- Lincoln, NE 27 th Annual Management of Colon and Rectal Diseases February 23, 2019 Objectives Differentiate
Anal Fissure: Finding the Root Cause Michael A. Jobst, MD, FACS, FASCRS Surgical Associates, PC -- Lincoln, NE 27 th Annual Management of Colon and Rectal Diseases February 23, 2019 Objectives Differentiate
Treatment of haemorrhoids. Mr Rowan Collinson FRACS Colorectal and General Surgeon Auckland
 Treatment of haemorrhoids Mr Rowan Collinson FRACS Colorectal and General Surgeon Auckland Much overlap of haemorrhoidal symptoms with other conditions Is it just the haemorrhoids? what type of haemorrhoidal
Treatment of haemorrhoids Mr Rowan Collinson FRACS Colorectal and General Surgeon Auckland Much overlap of haemorrhoidal symptoms with other conditions Is it just the haemorrhoids? what type of haemorrhoidal
Anterior anal fissure is much more common in women and may arise following vaginal delivery.
 ANAL FISSURE Definition An anal fissure (synonym: fissure-in-ano) is a longitudinal split in the anoderm of the distal anal canal which extends from the anal verge proximally towards, but not beyond, the
ANAL FISSURE Definition An anal fissure (synonym: fissure-in-ano) is a longitudinal split in the anoderm of the distal anal canal which extends from the anal verge proximally towards, but not beyond, the
Bright-red bleeding: If you have piles, you might see bright-red bleeding on the toilet paper, in the toilet bowl or on the surface of the faeces.
 What are haemorrhoids/piles? In the inner lining of the anus there are three haemorrhoidal cushions of tissue, which help to seal the anus and contribute to the control of the bowels (continence). Often,
What are haemorrhoids/piles? In the inner lining of the anus there are three haemorrhoidal cushions of tissue, which help to seal the anus and contribute to the control of the bowels (continence). Often,
Hemorrhoids. What are hemorrhoids? What is the cause? What are the symptoms?
 What are hemorrhoids? Hemorrhoids Hemorrhoids are swollen veins in the lower end of your intestine (rectum) or the anus. The anus is the opening where bowel movements pass out of your body. Hemorrhoids
What are hemorrhoids? Hemorrhoids Hemorrhoids are swollen veins in the lower end of your intestine (rectum) or the anus. The anus is the opening where bowel movements pass out of your body. Hemorrhoids
Hemorrhoids. Carlos R. Alvarez-Allende PGY-III Colorectal Surgery
 Hemorrhoids Carlos R. Alvarez-Allende PGY-III Colorectal Surgery Overview Anatomy Classification Etiology Incidence Symptoms Differential Diagnosis Medical Management Surgical Management Anatomy Anal canal
Hemorrhoids Carlos R. Alvarez-Allende PGY-III Colorectal Surgery Overview Anatomy Classification Etiology Incidence Symptoms Differential Diagnosis Medical Management Surgical Management Anatomy Anal canal
A painful problem. Symptoms of haemorrhoids. Causes of haemorrhoids. Your evaluation
 A painful problem Haemorrhoids, cushions of swollen veins in the anal canal, are often a source of embarrassment. They shouldn t be they re a very common problem that affects all kinds of people, including
A painful problem Haemorrhoids, cushions of swollen veins in the anal canal, are often a source of embarrassment. They shouldn t be they re a very common problem that affects all kinds of people, including
Colorectal Problems In Primary Care
 Colorectal Problems In Primary Care Lincoln Israel General and Colorectal Surgeon Middlemore Hospital Middlemore Hospital Mercy Hospital Auckland Colorectal Centre (Gilgit Rd Specialist Centre) Manukau
Colorectal Problems In Primary Care Lincoln Israel General and Colorectal Surgeon Middlemore Hospital Middlemore Hospital Mercy Hospital Auckland Colorectal Centre (Gilgit Rd Specialist Centre) Manukau
General Surgery. Haemorrhoids
 General Surgery Haemorrhoids Hemorrhoids_PRINT.indd 1 5/9/2016 5:50:45 PM A painful problem Haemorrhoids, cushions of swollen veins in the anal canal, are often a source of embarrassment. They shouldn
General Surgery Haemorrhoids Hemorrhoids_PRINT.indd 1 5/9/2016 5:50:45 PM A painful problem Haemorrhoids, cushions of swollen veins in the anal canal, are often a source of embarrassment. They shouldn
Perianal diseases. What causes pain in the bottom? What causes lumps around the bottom? What examination is likely?
 In association with: Primary Care Society for Gastroenterology INFORMATION ABOUT Perianal diseases www.corecharity.org.uk What are perianal diseases? What causes an itchy bottom? What causes pain in the
In association with: Primary Care Society for Gastroenterology INFORMATION ABOUT Perianal diseases www.corecharity.org.uk What are perianal diseases? What causes an itchy bottom? What causes pain in the
Constipation Information Leaflet THE DIGESTIVE SYSTEM. gutscharity.org.uk
 THE DIGESTIVE SYSTEM http://healthfavo.com/digestive-system-for-kids.html This factsheet is about Constipation Constipation is a symptom that can mean different things to different people but the usual
THE DIGESTIVE SYSTEM http://healthfavo.com/digestive-system-for-kids.html This factsheet is about Constipation Constipation is a symptom that can mean different things to different people but the usual
Haemorrhoidectomy. Colorectal Surgery. Patient Information
 Haemorrhoidectomy Colorectal Surgery Patient Information What are haemorrhoids? Haemorrhoids, also know as piles, are soft fleshy lumps just inside the back passage (anus). They have a rich blood supply
Haemorrhoidectomy Colorectal Surgery Patient Information What are haemorrhoids? Haemorrhoids, also know as piles, are soft fleshy lumps just inside the back passage (anus). They have a rich blood supply
Referral Criteria for Direct Access Outpatient Colonoscopy or Computed Tomography Colonography
 Referral Criteria for Direct Access Outpatient Colonoscopy or Computed Tomography Colonography 2019 Released 2019 health.govt.nz Citation: Ministry of Health. 2019. Referral Criteria for Direct Access
Referral Criteria for Direct Access Outpatient Colonoscopy or Computed Tomography Colonography 2019 Released 2019 health.govt.nz Citation: Ministry of Health. 2019. Referral Criteria for Direct Access
Piles / Sclerosing. Endoscopy Department. Patient information leaflet
 Piles / Sclerosing Endoscopy Department Patient information leaflet You will only be given this leaflet if you have been diagnosed with piles / sclerosing. The information below outlines the condition,
Piles / Sclerosing Endoscopy Department Patient information leaflet You will only be given this leaflet if you have been diagnosed with piles / sclerosing. The information below outlines the condition,
The Use of Glyceryl Tri-Nitrate Ointment in Treatment of Chronic Fissure in Ano
 Bahrain Medical Bulletin, Vol. 28, No. 4, December 2006 The Use of Glyceryl Tri-Nitrate Ointment in Treatment of Chronic Fissure in Ano Suhair Al-Saad, MBChB,FRCS I,CABS,* Hamdi Al- Shenawi, MBBS, FRCS
Bahrain Medical Bulletin, Vol. 28, No. 4, December 2006 The Use of Glyceryl Tri-Nitrate Ointment in Treatment of Chronic Fissure in Ano Suhair Al-Saad, MBChB,FRCS I,CABS,* Hamdi Al- Shenawi, MBBS, FRCS
Benign anorectal diseases
 Benign anorectal diseases Symptoms Bleeding Pruritus Discharge Fecal incontinence Diarrhea Constipation False need to defecate Examinations Clinical exam Anuscopy Rectosigmoidoscopy Endosonography MRI
Benign anorectal diseases Symptoms Bleeding Pruritus Discharge Fecal incontinence Diarrhea Constipation False need to defecate Examinations Clinical exam Anuscopy Rectosigmoidoscopy Endosonography MRI
Office Management of Anorectal Disease. Waqar Qureshi, MD, FRCP, FACG, FASGE Professor Baylor College of Medicine Houston Texas
 Office Management of Anorectal Disease Waqar Qureshi, MD, FRCP, FACG, FASGE Professor Baylor College of Medicine Houston Texas Commonly seen Anorectal Disease Hemorrhoids Anal fissures Pruritus Abscesses
Office Management of Anorectal Disease Waqar Qureshi, MD, FRCP, FACG, FASGE Professor Baylor College of Medicine Houston Texas Commonly seen Anorectal Disease Hemorrhoids Anal fissures Pruritus Abscesses
Abstract. Successful use of 0.2% Glyceryl Trinitrate ointment for anal fissures in Erbil city, Iraq. Abdulqadir M. Zangana (1) Kawa F.
 Kawa F.") Successful use of 0.2% Glyceryl Trinitrate ointment for anal fissures in Erbil city, Iraq Abdulqadir M. Zangana (1) Kawa F. Dizaye (2) (1) Professor of Surgery, CABS-FICS-MD, Head of Department of surgery,
Successful use of 0.2% Glyceryl Trinitrate ointment for anal fissures in Erbil city, Iraq Abdulqadir M. Zangana (1) Kawa F. Dizaye (2) (1) Professor of Surgery, CABS-FICS-MD, Head of Department of surgery,
Saratoga Schenectady Endoscopy Center, LLC Burnt Hills, N.Y Hemorrhoids. National Digestive Diseases Information Clearinghouse
 Hemorrhoids National Digestive Diseases Information Clearinghouse U.S. Department of Health and Human Services NATIONAL INSTITUTES OF HEALTH What are hemorrhoids? Hemorrhoids are swollen and inflamed veins
Hemorrhoids National Digestive Diseases Information Clearinghouse U.S. Department of Health and Human Services NATIONAL INSTITUTES OF HEALTH What are hemorrhoids? Hemorrhoids are swollen and inflamed veins
What Is Constipation?
 CONSTIPATION What Is Constipation? Constipation is when you have infrequent or hard-to-pass bowel movements (meaning they are painful or you have to strain), have hard stools or feel like your bowel movements
CONSTIPATION What Is Constipation? Constipation is when you have infrequent or hard-to-pass bowel movements (meaning they are painful or you have to strain), have hard stools or feel like your bowel movements
Dr David Rowbotham. The Leeds Teaching Hospitals NHS Trust NHS
 Dr David Rowbotham The Leeds Teaching Hospitals NHS Trust NHS Useful Titbits from the World of Gastroenterology David Rowbotham Clinical Director & Consultant Gastroenterologist Dept of Gastroenterology
Dr David Rowbotham The Leeds Teaching Hospitals NHS Trust NHS Useful Titbits from the World of Gastroenterology David Rowbotham Clinical Director & Consultant Gastroenterologist Dept of Gastroenterology
Further information You can get more information and share your experience at
 CR08 Lateral Internal Sphincterotomy Further information You can get more information and share your experience at www.aboutmyhealth.org Local information You can get information locally from: Taunton
CR08 Lateral Internal Sphincterotomy Further information You can get more information and share your experience at www.aboutmyhealth.org Local information You can get information locally from: Taunton
To help you understand your operation, it is helpful to have a basic knowledge of how the body works (see Figure 1).
.") Page 1 of 11 Anterior resection Introduction This leaflet tells you about the procedure known as an anterior resection. It explains what the procedure involves and also some of the common complications
Page 1 of 11 Anterior resection Introduction This leaflet tells you about the procedure known as an anterior resection. It explains what the procedure involves and also some of the common complications
Original Research Article
 MEDICAL AND SURGICAL MANAGEMENT OF ANAL FISSURE - A PROSPECTIVE STUDY Chitra Subramanian 1, Ashoka Chakravarthi Damodharan 2, Prabhu Kumarappan Chibandaram 3, Manoharan Appavu 4, Gourab Kundu 5 1Associate
MEDICAL AND SURGICAL MANAGEMENT OF ANAL FISSURE - A PROSPECTIVE STUDY Chitra Subramanian 1, Ashoka Chakravarthi Damodharan 2, Prabhu Kumarappan Chibandaram 3, Manoharan Appavu 4, Gourab Kundu 5 1Associate
Rectal Bleeding. Exceptional healthcare, personally delivered
 Rectal Bleeding Exceptional healthcare, personally delivered Content n The surgical team has assessed you because you have had bleeding from the back passage (rectal bleeding). n But your condition needs
Rectal Bleeding Exceptional healthcare, personally delivered Content n The surgical team has assessed you because you have had bleeding from the back passage (rectal bleeding). n But your condition needs
Anorectal physiology test
 Anorectal physiology test We hope this factsheet will help to answer some of your questions about having an anorectal physiology test. If you have any further questions or concerns, please don t hesitate
Anorectal physiology test We hope this factsheet will help to answer some of your questions about having an anorectal physiology test. If you have any further questions or concerns, please don t hesitate
, may spread caudally to present as a perianal abscess, laterally across the external sphincter to form an ischiorectal abscess or, rarely,
 ANORECTAL ABSCESSES , may spread caudally to present as a perianal abscess, laterally across the external sphincter to form an ischiorectal abscess or, rarely, superiorly above the anorectal junction
ANORECTAL ABSCESSES , may spread caudally to present as a perianal abscess, laterally across the external sphincter to form an ischiorectal abscess or, rarely, superiorly above the anorectal junction
Principles of Surgery - Ano rectal region: Haemorrhoids
 Principles of Surgery - Ano rectal region: Haemorrhoids Maurice Brygel Director, Melbourne Hernia Clinic (www.hernia.net.au) Fellow, Royal Australian College of Surgeons (RACS) Correspondence Maurice Brygel
Principles of Surgery - Ano rectal region: Haemorrhoids Maurice Brygel Director, Melbourne Hernia Clinic (www.hernia.net.au) Fellow, Royal Australian College of Surgeons (RACS) Correspondence Maurice Brygel
Tel Aviv Sourasky Medical Center
 Yehuda Kariv, MD Colorectal Unit Division of Surgery Tel Aviv Sourasky Medical Center Basic concepts Current evidence What s new Proposed treatment algorithm Mechanism of Disease Internal sphincter hypertonicity
Yehuda Kariv, MD Colorectal Unit Division of Surgery Tel Aviv Sourasky Medical Center Basic concepts Current evidence What s new Proposed treatment algorithm Mechanism of Disease Internal sphincter hypertonicity
Bowel cancer risk in the under 50s. Greg Rubin Professor of General Practice and Primary Care
 Bowel cancer risk in the under 50s Greg Rubin Professor of General Practice and Primary Care Prevalence of GI problems in the consulting population Thompson et al, Gut 2000 Number of patients % of patients
Bowel cancer risk in the under 50s Greg Rubin Professor of General Practice and Primary Care Prevalence of GI problems in the consulting population Thompson et al, Gut 2000 Number of patients % of patients
Anal Fissure. The basis of conservative treatment for an anal fissure is simple. If you have
 Anal Fissure An anal fissure is a cut in the anal canal resulting from trauma. Most people suffering from an anal fissure experience pain during or after defecation (the act of moving one s bowels, a number
Anal Fissure An anal fissure is a cut in the anal canal resulting from trauma. Most people suffering from an anal fissure experience pain during or after defecation (the act of moving one s bowels, a number
Colorectal Surgery Benign Anal Conditions...
 Colorectal Surgery Benign Anal Conditions... Lee Dvorkin Consultant General, Colorectal & Laparoscopic Surgeon, NMUH Clinical Lead for General Surgery, NMH Senior Clinical Lecturer, UCLH Associate Professor
Colorectal Surgery Benign Anal Conditions... Lee Dvorkin Consultant General, Colorectal & Laparoscopic Surgeon, NMUH Clinical Lead for General Surgery, NMH Senior Clinical Lecturer, UCLH Associate Professor
Dr Alasdair Patrick. Dr Nagham Al-Mozany. 9:45-10:10 Where Are We Up To With Bowel Cancer Screening?
 Dr Alasdair Patrick Gastroenterologist and General Physician Middlemore Hospital Auckland Dr Nagham Al-Mozany Colorectal Surgeon Auckland City Hospital Clinical Senior Lecturer University of Auckland 9:45-10:10
Dr Alasdair Patrick Gastroenterologist and General Physician Middlemore Hospital Auckland Dr Nagham Al-Mozany Colorectal Surgeon Auckland City Hospital Clinical Senior Lecturer University of Auckland 9:45-10:10
Patient Information Leaflet
 Patient Information Leaflet Your Haemorrhoid Operation What are haemorrhoids? Everyone has swellings in the anal canal (back passage) called anal cushions. These bulges in the lining of the anal canal
Patient Information Leaflet Your Haemorrhoid Operation What are haemorrhoids? Everyone has swellings in the anal canal (back passage) called anal cushions. These bulges in the lining of the anal canal
Robotic Ventral Rectopexy
 Robotic Ventral Rectopexy What is a robotic ventral rectopexy? The term rectopexy refers to an operation in which the rectum (the part of the bowel nearest the anus) is put back into its normal position
Robotic Ventral Rectopexy What is a robotic ventral rectopexy? The term rectopexy refers to an operation in which the rectum (the part of the bowel nearest the anus) is put back into its normal position
Guideline scope Diverticular disease: diagnosis and management
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline scope Diverticular disease: diagnosis and management The Department of Health in England has asked NICE to develop a clinical guideline on diverticular
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline scope Diverticular disease: diagnosis and management The Department of Health in England has asked NICE to develop a clinical guideline on diverticular
ACG Clinical Guideline: Management of Benign Anorectal Disorders
 ACG Clinical Guideline: Management of Benign Anorectal Disorders Arnold Wald, MD, MACG 1, Adil E. Bharucha, MBBS, MD 2, Bard C. Cosman, MD, MPH, FASCRS 3 and William E. Whitehead, PhD, MACG 4 1 Division
ACG Clinical Guideline: Management of Benign Anorectal Disorders Arnold Wald, MD, MACG 1, Adil E. Bharucha, MBBS, MD 2, Bard C. Cosman, MD, MPH, FASCRS 3 and William E. Whitehead, PhD, MACG 4 1 Division
Suggestions for Perianal Care in patients with itching or irritation:
 Suggestions for Perianal Care in patients with itching or irritation: Itching (and sometimes pain, even intense pain) in the anal area is termed pruritis ani (proo-rii-tus a-ni) and is in essence adult
Suggestions for Perianal Care in patients with itching or irritation: Itching (and sometimes pain, even intense pain) in the anal area is termed pruritis ani (proo-rii-tus a-ni) and is in essence adult
DISEASES OF THE COLON, RECTUM, & ANUS
 DISEASES OF THE COLON, RECTUM, & ANUS Rocco Ricciardi, MD, MPH Chief, Section of Colon & Rectal Surgery Massachusetts General Hospital Associate Professor of Surgery Harvard Medical School CASE 1 Hemorrhoid
DISEASES OF THE COLON, RECTUM, & ANUS Rocco Ricciardi, MD, MPH Chief, Section of Colon & Rectal Surgery Massachusetts General Hospital Associate Professor of Surgery Harvard Medical School CASE 1 Hemorrhoid
Prevention of Bowel Cancer: which patients do I send for colonoscopy?
 Prevention of Bowel Cancer: which patients do I send for colonoscopy? Dr Chris Groves Consultant Gastroenterologist and Honorary Senior Lecturer St George s Hospital and Medical School Director, SW London
Prevention of Bowel Cancer: which patients do I send for colonoscopy? Dr Chris Groves Consultant Gastroenterologist and Honorary Senior Lecturer St George s Hospital and Medical School Director, SW London
01/07/2018 MANAGEMENT OF RECTAL TENESMUS PRESENTATION OUTLINE
 MANAGEMENT OF RECTAL TENESMUS Dr. Áine Ní Laoire The Oxford Advanced Pain & Symptom Management Course Nottingham 27 th June 2018 PRESENTATION OUTLINE Definition A Clinical Case Epidemiology Pathophysiology
MANAGEMENT OF RECTAL TENESMUS Dr. Áine Ní Laoire The Oxford Advanced Pain & Symptom Management Course Nottingham 27 th June 2018 PRESENTATION OUTLINE Definition A Clinical Case Epidemiology Pathophysiology
Patient Information Leaflet
 Patient Information Leaflet Haemorrhoid Operation What are haemorrhoids? Everyone has swellings in the anal canal (back passage) called anal cushions. These bulges in the lining of the anal canal act like
Patient Information Leaflet Haemorrhoid Operation What are haemorrhoids? Everyone has swellings in the anal canal (back passage) called anal cushions. These bulges in the lining of the anal canal act like
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION. 9 May 2007
 The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 9 May 2007 RECTOGESIC 4 mg/g, rectal ointment B/1 (CIP 376 537-0) Applicant : PROSTRAKAN PHARMA SAS Glyceryl trinitrate
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 9 May 2007 RECTOGESIC 4 mg/g, rectal ointment B/1 (CIP 376 537-0) Applicant : PROSTRAKAN PHARMA SAS Glyceryl trinitrate
This is the portion of the intestine which lies between the small intestine and the outlet (Anus).
.") THE COLON This is the portion of the intestine which lies between the small intestine and the outlet (Anus). 3 4 5 This part is responsible for formation of stool. The large intestine (colon- coloured
THE COLON This is the portion of the intestine which lies between the small intestine and the outlet (Anus). 3 4 5 This part is responsible for formation of stool. The large intestine (colon- coloured
COLORECTAL CARCINOMA
 QUICK REFERENCE FOR HEALTHCARE PROVIDERS MANAGEMENT OF COLORECTAL CARCINOMA Ministry of Health Malaysia Malaysian Society of Colorectal Surgeons Malaysian Society of Gastroenterology & Hepatology Malaysian
QUICK REFERENCE FOR HEALTHCARE PROVIDERS MANAGEMENT OF COLORECTAL CARCINOMA Ministry of Health Malaysia Malaysian Society of Colorectal Surgeons Malaysian Society of Gastroenterology & Hepatology Malaysian
Haemorrhoidectomy. Mr. Sanjay Singh MBBS, MS, FRACS, FRCS (UK) Consultant Surgeon 2-4 Charles Street MOGO NSW 2536 Tel: Fax:
 Consultant Surgeon 2-4 Charles Street MOGO NSW 2536 Tel: Fax:") www.mogodaysurgery.com.au Mr. Sanjay Singh MBBS, MS, FRACS, FRCS (UK) Consultant Surgeon 2-4 Charles Street MOGO NSW 2536 Tel: 02 4474 3774 Fax: 02 4474 3775 Write questions or notes here: Haemorrhoidectomy
www.mogodaysurgery.com.au Mr. Sanjay Singh MBBS, MS, FRACS, FRCS (UK) Consultant Surgeon 2-4 Charles Street MOGO NSW 2536 Tel: 02 4474 3774 Fax: 02 4474 3775 Write questions or notes here: Haemorrhoidectomy
Assessing rectal bleeding: A common symptom of haemorrhoids
 Assessing rectal bleeding: A common symptom of haemorrhoids Rectal bleeding is a red flag sign and one of the referral criteria for a 2-week wait to see a specialist. However, in most cases, it is commonly
Assessing rectal bleeding: A common symptom of haemorrhoids Rectal bleeding is a red flag sign and one of the referral criteria for a 2-week wait to see a specialist. However, in most cases, it is commonly
Listed below are some of the words that you might come across concerning diseases and conditions of the bowels.
 Listed below are some of the words that you might come across concerning diseases and conditions of the bowels. Abscess A localised collection of pus in a cavity that is formed by the decay of diseased
Listed below are some of the words that you might come across concerning diseases and conditions of the bowels. Abscess A localised collection of pus in a cavity that is formed by the decay of diseased
The Digestive System or tract extends from the mouth to the anus.
 The Digestive System or tract extends from the mouth to the anus. FUNCTION The Digestive System breaks down and absorbs food materials e.g. amino acids, glucose DEFINITIONS: Ingestion: Ingestion is the
The Digestive System or tract extends from the mouth to the anus. FUNCTION The Digestive System breaks down and absorbs food materials e.g. amino acids, glucose DEFINITIONS: Ingestion: Ingestion is the
JMSCR Vol 06 Issue 08 Page August 2018
 www.jmscr.igmpublication.org Impact Factor (SJIF): 6.379 Index Copernicus Value: 79.54 ISSN (e)-2347-176x ISSN (p) 2455-0450 DOI: https://dx.doi.org/10.18535/jmscr/v6i8.85 Comparative Study of Pharmacotherapy,
www.jmscr.igmpublication.org Impact Factor (SJIF): 6.379 Index Copernicus Value: 79.54 ISSN (e)-2347-176x ISSN (p) 2455-0450 DOI: https://dx.doi.org/10.18535/jmscr/v6i8.85 Comparative Study of Pharmacotherapy,
Gastrointestinal Hemorrhage, Lower
 Gastrointestinal Hemorrhage, Lower What is a lower gastrointestinal hemorrhage? A lower gastrointestinal (GI) hemorrhage, also called lower GI bleeding or rectal bleeding, is abnormal blood loss from the
Gastrointestinal Hemorrhage, Lower What is a lower gastrointestinal hemorrhage? A lower gastrointestinal (GI) hemorrhage, also called lower GI bleeding or rectal bleeding, is abnormal blood loss from the
J of Evolution of Med and Dent Sci/ eissn , pissn / Vol. 3/ Issue 22/June 02, 2014 Page 6243
 CHEMICAL SPHINCTEROTOMY VERSUS SURGICAL SPHINCTEROTOMY (LATERAL INTERNAL SPHINCTEROTOMY) FOR CHRONIC FISSURE-IN-ANO OUTCOME Madhusudhan M. Gopivallabh 1, Ganapathy Puranik 2, K. S. Hanumanthaiah 3, Prashantha
CHEMICAL SPHINCTEROTOMY VERSUS SURGICAL SPHINCTEROTOMY (LATERAL INTERNAL SPHINCTEROTOMY) FOR CHRONIC FISSURE-IN-ANO OUTCOME Madhusudhan M. Gopivallabh 1, Ganapathy Puranik 2, K. S. Hanumanthaiah 3, Prashantha
Case Presentation and Discussion on GI Bleeding Nolan Ortega Aludino, M.D.
 Case Presentation and Discussion on GI Bleeding Nolan Ortega Aludino, M.D. General Data R.L. R.L. 4343 years old MaleMale PacoPaco Manila Chief Complaint Anal Anal bleeding History of Present Illness 3
Case Presentation and Discussion on GI Bleeding Nolan Ortega Aludino, M.D. General Data R.L. R.L. 4343 years old MaleMale PacoPaco Manila Chief Complaint Anal Anal bleeding History of Present Illness 3
Neurogenic Bowel: What You Should Know. A Guide for People with Spinal Cord Injury
 Neurogenic Bowel: What You Should Know A Guide for People with Spinal Cord Injury Why Is This Information Important? Before SCI, you didn t have to think about bowel movements After SCI, you may need more
Neurogenic Bowel: What You Should Know A Guide for People with Spinal Cord Injury Why Is This Information Important? Before SCI, you didn t have to think about bowel movements After SCI, you may need more
A Guide to Your Burning Questions
 The #1 Doctor Recommended Brand A Guide to Your Burning Questions Use products as directed. 2017 Pfizer Consumer Healthcare Put an End to Your Uncomfortable Questions We understand that talking about hemorrhoids
The #1 Doctor Recommended Brand A Guide to Your Burning Questions Use products as directed. 2017 Pfizer Consumer Healthcare Put an End to Your Uncomfortable Questions We understand that talking about hemorrhoids
Patient information leaflet. Royal Surrey County Hospital. NHS Foundation Trust. Haemorrhoids. Day Surgery Unit
 Patient information leaflet Royal Surrey County Hospital NHS Foundation Trust Haemorrhoids Day Surgery Unit What are haemorrhoids? The anal canal (back passage) contains cushions of tissue at the top of
Patient information leaflet Royal Surrey County Hospital NHS Foundation Trust Haemorrhoids Day Surgery Unit What are haemorrhoids? The anal canal (back passage) contains cushions of tissue at the top of
Constipation. What is constipation? What is the criteria for having constipation? What are the different types of constipation?
 What is constipation? is defined as having a bowel movement less than 3 times per week. It is usually associated with hard stools or difficulty passing stools. You may have pain while passing stools or
What is constipation? is defined as having a bowel movement less than 3 times per week. It is usually associated with hard stools or difficulty passing stools. You may have pain while passing stools or
Guidelines for the Manual Evacuation of Faeces
 Rationale Guidelines for the Manual Evacuation of Faeces These guidelines are to provide the required information for designated registered nurses, health care assistants and bank support workers to perform
Rationale Guidelines for the Manual Evacuation of Faeces These guidelines are to provide the required information for designated registered nurses, health care assistants and bank support workers to perform
Treatment Of Chronic Anal fissure (TOCA): a Randomized Clinical trial on Levorag Emulgel versus Diltiazem gel 2%
: a Randomized Clinical trial on Levorag Emulgel versus Diltiazem gel 2%") Protocol Treatment Of Chronic Anal fissure (TOCA): a Randomized Clinical trial on Levorag Emulgel versus Diltiazem gel 2% Dr. Andreas Nordholm-Carstensen, Dr. Kikke Hagen and Dr. Peter-Martin Krarup Digestive
Protocol Treatment Of Chronic Anal fissure (TOCA): a Randomized Clinical trial on Levorag Emulgel versus Diltiazem gel 2% Dr. Andreas Nordholm-Carstensen, Dr. Kikke Hagen and Dr. Peter-Martin Krarup Digestive
A guide to Anoplasty (anal surgery)
") Saint Mary s Hospital Newborn Intensive Care Unit Information for Parents A guide to Anoplasty (anal surgery) Introduction This information leaflet is designed to help parents and families to care for
Saint Mary s Hospital Newborn Intensive Care Unit Information for Parents A guide to Anoplasty (anal surgery) Introduction This information leaflet is designed to help parents and families to care for
What is Colorectal Cancer?
 COLORECTAL CANCER (CRC) What is Colorectal Cancer? Colorectal cancer (also known as colon cancer) is cancer of the colon and/or rectum and occurs when a growth in the lining of the colon or rectum becomes
COLORECTAL CANCER (CRC) What is Colorectal Cancer? Colorectal cancer (also known as colon cancer) is cancer of the colon and/or rectum and occurs when a growth in the lining of the colon or rectum becomes
Bleeding in the Digestive Tract
 Bleeding in the Digestive Tract National Digestive Diseases Information Clearinghouse National Institute of Diabetes and Digestive and Kidney Diseases NATIONAL INSTITUTES OF HEALTH U.S. Department of Health
Bleeding in the Digestive Tract National Digestive Diseases Information Clearinghouse National Institute of Diabetes and Digestive and Kidney Diseases NATIONAL INSTITUTES OF HEALTH U.S. Department of Health
CONSTIPATION FUNDING RESEARCH INTO DISEASES OF THE GUT, LIVER & PANCREAS
 ALL YOU NEED TO KNOW ABOUT CONSTIPATION FUNDING RESEARCH INTO DISEASES OF THE GUT, LIVER & PANCREAS THIS FACTSHEET IS ABOUT CONSTIPATION Constipation is a symptom that can mean different things to different
ALL YOU NEED TO KNOW ABOUT CONSTIPATION FUNDING RESEARCH INTO DISEASES OF THE GUT, LIVER & PANCREAS THIS FACTSHEET IS ABOUT CONSTIPATION Constipation is a symptom that can mean different things to different
1/3/2008. Karen Burke Priscilla LeMone Elaine Mohn-Brown. Medical-Surgical Nursing Care, 2e Karen Burke, Priscilla LeMone, and Elaine Mohn-Brown
 Medical-Surgical Nursing Care Second Edition Karen Burke Priscilla LeMone Elaine Mohn-Brown Chapter 20 Caring for Clients with Bowel Disorders Diarrhea Pathophysiology Result from impaired water absorption
Medical-Surgical Nursing Care Second Edition Karen Burke Priscilla LeMone Elaine Mohn-Brown Chapter 20 Caring for Clients with Bowel Disorders Diarrhea Pathophysiology Result from impaired water absorption
What is a Colonoscopy?
 What is a Colonoscopy? A colonoscopy is a test to look inside your colon. A colonoscopy is done by a gastroenterologist, a doctor trained in looking at the gastrointestinal (GI) tract. The main tool used
What is a Colonoscopy? A colonoscopy is a test to look inside your colon. A colonoscopy is done by a gastroenterologist, a doctor trained in looking at the gastrointestinal (GI) tract. The main tool used
Faecal Incontinence: Assessment and Management
 Mrs PK; 56 yrs; Married; 2 children Faecal Incontinence: Assessment and Management Professor Marc A Gladman MBBS DFFP PhD MRCOG FRCS (UK) FRACS Professor of Colorectal Surgery >10 years of incontinence
Mrs PK; 56 yrs; Married; 2 children Faecal Incontinence: Assessment and Management Professor Marc A Gladman MBBS DFFP PhD MRCOG FRCS (UK) FRACS Professor of Colorectal Surgery >10 years of incontinence
What you can expect at your doctors
 What you can expect at your doctors Investigations and Procedures Tests are not always necessary Current guidelines encourage gastroenterologists to make a positive diagnosis of Irritable Bowel Syndrome
What you can expect at your doctors Investigations and Procedures Tests are not always necessary Current guidelines encourage gastroenterologists to make a positive diagnosis of Irritable Bowel Syndrome
ANALYSIS GENERAL SURGERY Medical Science, Volume 10, Number 39, July 23, 2014
 ANALYSIS GENERAL SURGERY Medical Science, Volume 10, Number 39, July 23, 2014 ISSN 2321 7359 EISSN 2321 7367 Acute anal fissure - an urban scenario Medical Science The International Weekly Journal for
ANALYSIS GENERAL SURGERY Medical Science, Volume 10, Number 39, July 23, 2014 ISSN 2321 7359 EISSN 2321 7367 Acute anal fissure - an urban scenario Medical Science The International Weekly Journal for
Colonoscopy. patient information from your surgeon & SAGES. Colonoscopy 1
 Colonoscopy patient information from your surgeon & SAGES Colonoscopy 1 Colonscopy About colonoscopy What is a colonoscopy? Colonoscopy is a procedure that enables your surgeon to examine the lining of
Colonoscopy patient information from your surgeon & SAGES Colonoscopy 1 Colonscopy About colonoscopy What is a colonoscopy? Colonoscopy is a procedure that enables your surgeon to examine the lining of
2012 update. Bowel Cancer. Information for people at increased risk of bowel cancer. Published by the New Zealand Guidelines Group
 2012 update Bowel Cancer Information for people at increased risk of bowel cancer Published by the New Zealand Guidelines Group i Contents Introduction 1 The bowel 1 Bowel cancer 3 What are the symptoms
2012 update Bowel Cancer Information for people at increased risk of bowel cancer Published by the New Zealand Guidelines Group i Contents Introduction 1 The bowel 1 Bowel cancer 3 What are the symptoms
Ulcerative Colitis. ulcerative colitis usually only affects the colon.
 Ulcerative Colitis Introduction Ulcerative colitis is an inflammatory bowel disease. It is one of the 2 most common inflammatory bowel diseases. The other one is Crohn s disease. Ulcerative colitis and
Ulcerative Colitis Introduction Ulcerative colitis is an inflammatory bowel disease. It is one of the 2 most common inflammatory bowel diseases. The other one is Crohn s disease. Ulcerative colitis and
Elderly Man With Chronic Constipation
 Elderly Man With Chronic Constipation Linda Nguyen, MD Director, Neurogastroenterology and Motility Clinical Assistant Professor Stanford University Overview Normal bowel function Defining Constipation:
Elderly Man With Chronic Constipation Linda Nguyen, MD Director, Neurogastroenterology and Motility Clinical Assistant Professor Stanford University Overview Normal bowel function Defining Constipation:
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE SCOPE
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Constipation: management of idiopathic constipation in children in primary and secondary care 1.1 Short title Constipation
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Constipation: management of idiopathic constipation in children in primary and secondary care 1.1 Short title Constipation
Colorectal Cancer. Mark Chapman. MA MS FRCS EBSQ(coloproct) 21 st March 2018 Consultant Coloproctologist
 21 st March 2018 Consultant Coloproctologist") Colorectal Cancer Mark Chapman MA MS FRCS EBSQ(coloproct) 21 st March 2018 Consultant Coloproctologist Overview Epidemiology of colorectal cancer Adenoma carcinoma sequence Tumour diagnosis & staging Treatment
Colorectal Cancer Mark Chapman MA MS FRCS EBSQ(coloproct) 21 st March 2018 Consultant Coloproctologist Overview Epidemiology of colorectal cancer Adenoma carcinoma sequence Tumour diagnosis & staging Treatment
Local Glyceryl Trinitrate Versus Lateral Internal Sphincterotomy In Management Of Anal Fissure
 ISPUB.COM The Internet Journal of Surgery Volume 22 Number 2 Local Glyceryl Trinitrate Versus Lateral Internal Sphincterotomy In Management Of Anal Fissure G El-Labban, G El-Gazzaz, E Hokamam Citation
ISPUB.COM The Internet Journal of Surgery Volume 22 Number 2 Local Glyceryl Trinitrate Versus Lateral Internal Sphincterotomy In Management Of Anal Fissure G El-Labban, G El-Gazzaz, E Hokamam Citation
PAUL E. SAVOCA, MD, FACS, FASCRS Consent Form for Hemorrhoidectomy
 PAUL E. SAVOCA, MD, FACS, FASCRS Consent Form for Hemorrhoidectomy The doctor has explained that I have the following condition: Hemorrhoids- abnormally enlarged anal veins. The following procedure will
PAUL E. SAVOCA, MD, FACS, FASCRS Consent Form for Hemorrhoidectomy The doctor has explained that I have the following condition: Hemorrhoids- abnormally enlarged anal veins. The following procedure will
GUIDANCE ON THE INDICATIONS FOR DIAGNOSTIC UPPER GI ENDOSCOPY, FLEXIBLE SIGMOIDOSCOPY AND COLONOSCOPY
 Position Statement produced by BSG, AUGIS and ACPGBI GUIDANCE ON THE INDICATIONS FOR DIAGNOSTIC UPPER GI ENDOSCOPY, FLEXIBLE SIGMOIDOSCOPY AND COLONOSCOPY Introduction In 2011 the Independent Practice
Position Statement produced by BSG, AUGIS and ACPGBI GUIDANCE ON THE INDICATIONS FOR DIAGNOSTIC UPPER GI ENDOSCOPY, FLEXIBLE SIGMOIDOSCOPY AND COLONOSCOPY Introduction In 2011 the Independent Practice
DIVERTICULOSIS MEDICAL AND SURGICAL MANAGEMENT. Simon Radley Consultant Surgeon March 2013
 DIVERTICULOSIS MEDICAL AND SURGICAL MANAGEMENT Simon Radley Consultant Surgeon March 2013 Definitions Diverticulosis: presence of diverticulae Diverticular disease: diverticulae associated with symptoms
DIVERTICULOSIS MEDICAL AND SURGICAL MANAGEMENT Simon Radley Consultant Surgeon March 2013 Definitions Diverticulosis: presence of diverticulae Diverticular disease: diverticulae associated with symptoms
Chronic constipation in the elderly
 Chronic constipation in the elderly 1 Dec,2011 R 2 Natta Asanaleykha Epidemiology Definition Scope The impact of chronic constipation in the elderly Pathophysiology Evaluation the elderly patient with
Chronic constipation in the elderly 1 Dec,2011 R 2 Natta Asanaleykha Epidemiology Definition Scope The impact of chronic constipation in the elderly Pathophysiology Evaluation the elderly patient with
Colon Investigation. Flexible Sigmoidoscopy
 Colon Investigation Flexible Sigmoidoscopy What is a flexible sigmoidoscopy? Flexible sigmoidoscopy is a frequently performed test to investigate the lower part of the bowel. This is an endoscopic test
Colon Investigation Flexible Sigmoidoscopy What is a flexible sigmoidoscopy? Flexible sigmoidoscopy is a frequently performed test to investigate the lower part of the bowel. This is an endoscopic test
PELVIC PAIN : Gastroenterological Conditions
 PELVIC PAIN : Gastroenterological Conditions Departman Tarih Prof. A. Melih OZEL, MD Department of Gastroenterology Anadolu Medical Center Hospital Gebze Kocaeli - TURKEY Presentation plan 15 min. Introduction
PELVIC PAIN : Gastroenterological Conditions Departman Tarih Prof. A. Melih OZEL, MD Department of Gastroenterology Anadolu Medical Center Hospital Gebze Kocaeli - TURKEY Presentation plan 15 min. Introduction
Stool softeners are medicines like (ducolox - pericolace - senokot). You want the stool to remain soft so it is easier to empty the bowel.
. You want the stool to remain soft so it is easier to empty the bowel.") "Bowel Management" How the Body Works The food you eat and drink provides your body with many nutrients. These nutrients give you energy and help you stay healthy. As food moves through your body it breaks
"Bowel Management" How the Body Works The food you eat and drink provides your body with many nutrients. These nutrients give you energy and help you stay healthy. As food moves through your body it breaks
IBS. Patient INFO. A Guide to Irritable Bowel Syndrome
 Patient INFO IBS A Guide to Irritable Bowel Syndrome The information provided by the AGA Institute is not medical advice and should not be considered a replacement for seeing a medical professional. About
Patient INFO IBS A Guide to Irritable Bowel Syndrome The information provided by the AGA Institute is not medical advice and should not be considered a replacement for seeing a medical professional. About
Inflammatory Bowel Disease. Your Illness and Its Treatment
 Inflammatory Bowel Disease Your Illness and Its Treatment What Is Inflammatory Bowel Disease? Inflammatory bowel disease (IBD) is inflammation (irritation and swelling) of the digestive tract. Your digestive
Inflammatory Bowel Disease Your Illness and Its Treatment What Is Inflammatory Bowel Disease? Inflammatory bowel disease (IBD) is inflammation (irritation and swelling) of the digestive tract. Your digestive
North West London Pathology. Faecal Occult Blood testing. Mrs Sophie Barnes FRCPath Consultant Clinical Scientist
 Faecal Occult Blood testing Mrs Sophie Barnes FRCPath Consultant Clinical Scientist Learning objectives Background Guidelines for colorectal cancer detection Tests available to detect occult blood in faeces
Faecal Occult Blood testing Mrs Sophie Barnes FRCPath Consultant Clinical Scientist Learning objectives Background Guidelines for colorectal cancer detection Tests available to detect occult blood in faeces
Constipation. Information for adults. GI Motility Clinic (UMCCC University Medical Clinics of Campbelltown and Camden) Page 1
 Page 1") Constipation Information for adults GI Motility Clinic (UMCCC University Medical Clinics of Campbelltown and Camden) Page 1 Contents Role of the large intestine..3 Mass movements in the large intestine..4
Constipation Information for adults GI Motility Clinic (UMCCC University Medical Clinics of Campbelltown and Camden) Page 1 Contents Role of the large intestine..3 Mass movements in the large intestine..4
Laparoscopic Ventral. Mesh Rectopexy (LVMR)
") Laparoscopic Ventral Mesh Rectopexy (LVMR) Questions & Answers GLASGOW COLORECTAL CENTRE Ross Hall Hospital 221 Crookston Road Glasgow G52 3NQ e-mail: info@colorectalcentre.co.uk Ph: Main hospital switchboard
Laparoscopic Ventral Mesh Rectopexy (LVMR) Questions & Answers GLASGOW COLORECTAL CENTRE Ross Hall Hospital 221 Crookston Road Glasgow G52 3NQ e-mail: info@colorectalcentre.co.uk Ph: Main hospital switchboard
Bowel Cancer Information Leaflet THE DIGESTIVE SYSTEM
 THE DIGESTIVE SYSTEM This factsheet is about bowel cancer Throughout our lives, the lining of the bowel constantly renews itself. This lining contains many millions of tiny cells, which grow, serve their
THE DIGESTIVE SYSTEM This factsheet is about bowel cancer Throughout our lives, the lining of the bowel constantly renews itself. This lining contains many millions of tiny cells, which grow, serve their
Doctor s Instructions. Patient: Heather Crawford Age: 65 years old. PMH 2012: Hypertension 2014: Diverticular Disease
 Doctor s Instructions Patient: Heather Crawford Age: 65 years old PMH 2012: Hypertension 2014: Diverticular Disease Drug History NKDA Amlodipine 5mg OD Actor s Script *The most important things to remember
Doctor s Instructions Patient: Heather Crawford Age: 65 years old PMH 2012: Hypertension 2014: Diverticular Disease Drug History NKDA Amlodipine 5mg OD Actor s Script *The most important things to remember
HOW TO CITE THIS ARTICLE:
 STUDY ON USE OF TOPICAL DILTIAZEM VERSUS TOPICAL GLYCERYL TRINITRATE (GTN) IN THE TREATMENT OF CHRONIC ANAL FISSURE: A RETROSPECTIVE STUDY Madhu Lata Rana 1, Narayan Jeet Singh 2, Avtar Singh Bansal 3,
STUDY ON USE OF TOPICAL DILTIAZEM VERSUS TOPICAL GLYCERYL TRINITRATE (GTN) IN THE TREATMENT OF CHRONIC ANAL FISSURE: A RETROSPECTIVE STUDY Madhu Lata Rana 1, Narayan Jeet Singh 2, Avtar Singh Bansal 3,
Functional anorectal disorders
 Functional anorectal disorders Anton Emmanuel Swiss Coloproctology Study Group, January 2019 National Hospital for Neurology & Neurosurgery Approach Pelvic floor neurophysiology Faecal incontinence (Dr
Functional anorectal disorders Anton Emmanuel Swiss Coloproctology Study Group, January 2019 National Hospital for Neurology & Neurosurgery Approach Pelvic floor neurophysiology Faecal incontinence (Dr
The Role of Surgery in Inflammatory Bowel Disease. Cory D Barrat, MD Colon and Rectal Surgeon Mercy Health
 The Role of Surgery in Inflammatory Bowel Disease Cory D Barrat, MD Colon and Rectal Surgeon Mercy Health THANKS FOR INVITING ME! I have no financial disclosures Outline - Who am I and what do I do? -
The Role of Surgery in Inflammatory Bowel Disease Cory D Barrat, MD Colon and Rectal Surgeon Mercy Health THANKS FOR INVITING ME! I have no financial disclosures Outline - Who am I and what do I do? -
8/29/2016 DIVERTICULAR DISEASE: WHAT EVERY NURSE PRACTITIONER SHOULD KNOW. LENORE LAMANNA Ed.D, ANP-C LEARNING OBJECTIVES
 DIVERTICULAR DISEASE: WHAT EVERY NURSE PRACTITIONER SHOULD KNOW LENORE LAMANNA Ed.D, ANP-C LEARNING OBJECTIVES Define Diverticular Disease Discuss Epidemiology and Pathophysiology of Diverticular disease
DIVERTICULAR DISEASE: WHAT EVERY NURSE PRACTITIONER SHOULD KNOW LENORE LAMANNA Ed.D, ANP-C LEARNING OBJECTIVES Define Diverticular Disease Discuss Epidemiology and Pathophysiology of Diverticular disease
"The Complete Guide to Hemorrhoids"
 Another ebookwholesaler Publication "The Complete Guide to Hemorrhoids" By Seymour Wells Understanding, Managing and Treating Hemorrhoids Proudly brought to you by WOW Enterprises Inc. Email Recommended
Another ebookwholesaler Publication "The Complete Guide to Hemorrhoids" By Seymour Wells Understanding, Managing and Treating Hemorrhoids Proudly brought to you by WOW Enterprises Inc. Email Recommended
Anal sphincter exercises. Information for patients Sheffield Teaching Hospitals
 Anal sphincter exercises Information for patients Sheffield Teaching Hospitals Anal sphincter exercises to help lessen leakage from the bowel Sphincter exercises, when practiced correctly, can build up
Anal sphincter exercises Information for patients Sheffield Teaching Hospitals Anal sphincter exercises to help lessen leakage from the bowel Sphincter exercises, when practiced correctly, can build up
Rectal Cancer. About the Colon and Rectum. Symptoms. Colorectal Cancer Screening
 Patient information regarding care and surgery associated with RECTAL CANCER by Robert K. Cleary, M.D., John C. Eggenberger, M.D., Amalia J. Stefanou., M.D. location: Michigan Heart and Vascular Institute,
Patient information regarding care and surgery associated with RECTAL CANCER by Robert K. Cleary, M.D., John C. Eggenberger, M.D., Amalia J. Stefanou., M.D. location: Michigan Heart and Vascular Institute,
Anal fissure The surgical approach
 Fissure- Workshop 36. Schweizerische Koloproktologie Tagung, 17. Januar 2015 Anal fissure The surgical approach PD Dr. med. Antonio Nocito Head of the Departement of Surgery Kantonsspital Baden Switzerland
Fissure- Workshop 36. Schweizerische Koloproktologie Tagung, 17. Januar 2015 Anal fissure The surgical approach PD Dr. med. Antonio Nocito Head of the Departement of Surgery Kantonsspital Baden Switzerland