TEST-RETEST RELIABILITY OF PELVIC FLOOR MUSCLE CONTRACTION. Ingeborg Hoff BRÆKKEN, PhD student, Msci, PT, Manual therapist 1
|
|
|
- Avis Collins
- 5 years ago
- Views:
Transcription
1 TEST-RETEST RELIABILITY OF PELVIC FLOOR MUSCLE CONTRACTION MEASURED BY 4D ULTRASOUND Ingeborg Hoff BRÆKKEN, PhD student, Msci, PT, Manual therapist 1 Memona MAJIDA, Consultant gynaecologist 2 Marie Ellström ENGH, Ph.D. Associate professor 2,3 Kari BØ, professor, Ph.D, PT, Exercise scientist 1 1. Norwegian School of Sport Sciences, Department of Sports Medicine, Oslo, Norway 2. Akershus university hospital. Department of obstetrics and gynaecology, Lørenskog, Norway 3. University of Oslo, Norway. The work was preformed at the Norwegian School of Sport Sciences Correspondent author: Ingeborg Hoff Brækken Norwegian School of Sport Sciences Department of Sports Medicine Short title: Pelvic floor muscle contraction Word count: 2930 words
2 TEST-RETEST RELIABILITY OF PELVIC FLOOR MUSCLE CONTRACTION MEASURED BY 4D ULTRASOUND INTRODUCTION A correct pelvic floor muscle (PFM) contraction was described by Kegel (1) as an inward lift and squeeze around urethra, vagina and rectum. In addition, DeLancey (2;3) suggested that a PFM contraction may press the urethra against the pubic symphysis (PS), further mechanically increasing urethral pressure. Traditionally PFM function and strength have been assessed by visual observation, digital palpation and use of different manometers and dynamometers (4). None of these measurement methods are capable of simultaneously measuring both the lifting and squeezing function in a responsive, reliable and valid way. Neither can any of these methods measure muscle morphology. Today imaging techniques such as ultrasound and magnetic resonance imaging have the potential of yielding more detailed information about muscle morphology and action during PFM contraction. 3D and 4D ultrasound allow multi planar imaging, assessment in an upright body position and utilizing a rapid sampling time. In addition, there are few contraindications and it may, due to relatively low cost, therefore be adopted into future clinical practice (5). To date, mainly the lift of the bladder neck (BN) has been investigated (6;7). To our knowledge only one study has quantified pubovisceral muscle length reduction (8), and no studies have quantified narrowing of levator hiatus (LH) area and transverse distance during contraction. Position of cervix uteri, rectal ampulla or back sling of the puborectal muscle has not been assessed, neither has the magnitude nor the direction of the displacement of these organs during PFM contraction. The aims of the present study were to evaluate test-retest measurements of functional aspects
3 of PFM contraction using 4D real time ultrasound by: 1. Measuring pubovisceral muscle length, LH area, antero-posterior and transverse dimensions at rest and maximal contraction (axial plane) 2. Measuring lift (displacement) of the BN, cervix uteri, rectal ampulla and back sling of the puborectal muscle (sagittal plane)
4 MATERIALS AND METHODS The study was designed as a test-retest intra-tester study. Two test series were performed with an interval of 7 to 35 days. The participants received a random identification number. The assessor was blinded to the results of test 1 during test 2. Subjects Seventeen female volunteers were recruited for the study. Inclusion criterion was ability to contract the PFMs. Correct contraction was defined as inward lift of the PFM as assessed by ultrasound. Exclusion criterion was inability to understand instructions given in the Norwegian language. No volunteers had to be excluded. The study was approved by the Regional Medical Ethics Committee, and the Data Inspectorate of Norway. All subjects gave written informed consent to participate. Apparatus A GE Voluson 730 expert ultrasound system (GE Healthcare, Oslo, Norway) with 4-8 MHz curved array 3D/4D ultrasound transducer (RAB 4-8 l/obstetric) was used. The field of view angle was set to its maximum of 70 º in the sagittal plane and volume acquisition angle to 85 º in the coronal plane (frame rate was 3 Hz). Procedure Prior to the ultrasound examination all participants answered a short questionnaire regarding age, weight, height, birth history, symptoms of pelvic organ prolapse and education. Pelvic organ prolapse quantification (POPQ was not performed in this study. One gynaecologist (MM) performed the ultrasound examinations. A physical therapist (IHB) gave instructions to the participants and supervised the test procedure on both days. Participants were instructed to void before the examination. The PFM contraction was performed in the standing position
5 and recorded at least three times. It took approximately 10 seconds to perform and was recorded using 4D real time ultrasound. The ultrasound transducer was placed on the perineum in the sagittal plane directed cranially. Only a minor part of the PS was scanned in order to include the back sling of the puborectal muscle. Ultrasound analyses Analyses of 4D real time volumes were conducted offline on a laptop by one investigator (IHB), using the software 4D View v 5.0 (GE Healthcare, Oslo, Norway), blinded to clinical data. The PFM contraction with the most cranial displacement was analysed. All volumes were previewed and excluded from analysis unless a significant portion of the pubovisceral muscle was visible. Analyses in the axial plane Measurements were performed in the axial plane of minimal hiatal dimensions (Fig 1), going from the inferio-posterior margin of the PS to the anorectal junction, as described by Dietz el al.(5). Measurements were done at rest and at maximal contraction. At contraction the inclination of the axial plane increases because the anorectal junction elevates. The back sling of the puborectal muscle forms a bump posterior to the rectum in the mid-sagittal plane (9), which forms the anorectal junction. In order to ensure that the minimal hiatal dimensions were found, the marker dot was placed at the inferio-posterior margin of the PS and the sagittal plane was rotated, whereas the axial plane was carefully observed until the whole pubovisceral muscle was visualised and the LH had its minimum antero-posterior distance. The area of LH is bordered by the pubovisceral muscle, PS and inferior pubic ramus (Fig 1). The transverse distance was measured at the widest part of LH. The length of the pubovisceral
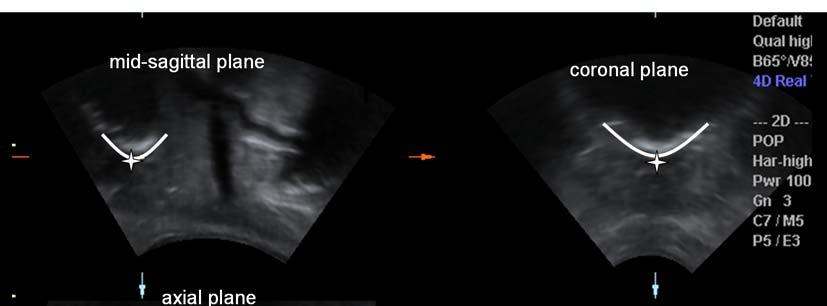
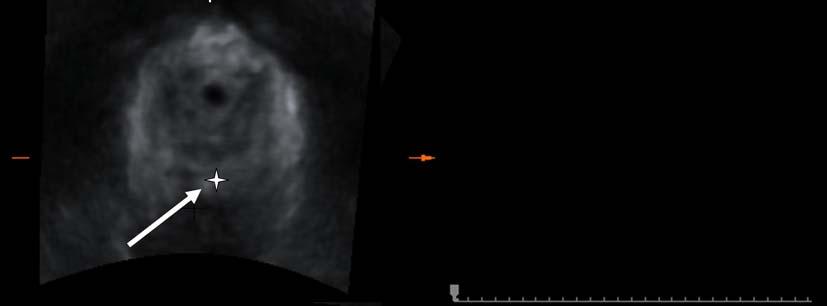
6 muscle was measured as the inner border of the muscle sling, from the right to the left inferior pubic ramus around the rectum (contractile elements only). Analyses in the sagittal plane At rest and on maximum contraction the position of the BN (internal urethral meatus) was identified in all three planes. The rectal ampulla has a valley shape, and was mainly identified in the mid-sagittal plane. It was necessary to view the sagittal planes lateral to the mid-sagittal to ensure that the lowest part of the rectal ampulla was identified. In addition, the axial plane was carefully observed to ensure that the rectal ampulla was located in the rectum (Fig II), as it can be misinterpreted as the cervix uteri located in the vagina. Cervix uteri has a wide W shape that can be visualised on high quality ultrasound images (Fig III). It was identified simultaneously in at least the sagittal and coronal planes. In order to detect cervixes that are not centred, sagittal planes lateral to the mid-sagittal plane were viewed. The back sling of the puborectal muscle was identified viewing the sagittal and axial planes simultaneously. The movement of the urethra against the PS was quantified by a horizontal distance drawn from the infero-posterior margin of the PS to the mid urethra. Positions of all the structures in the sagittal plane were analysed using two different systems. The position of the structures were analysed in a horizontal (x-axis) and vertical position (yaxis) relative to a horizontal reference line, at the level of the inferio-posterior margin of the PS, as described by Dietz et al. (10) (Fig III). The levator plate angle was defined as the angle between the horizontal reference line and the line from the inferio-posterior margin of the PS to the anorectal angle. In addition, displacement of the structures was assessed with an onscreen vector-based method described by Reddy et al. (11). This system provides information about the magnitude of the displacement, not about direction of the lift.
7 Statistical analysis Statistical analysis was performed using SPSS version 15. Test-retest intra-tester reliability was analysed using intra-class correlation coefficient (ICC, repeated measures) with 95% confidence interval (CI). ICC values under 0.20 were considered poor, fair, moderate, good, and very good. Results are given as mean values with 95% CI for test 1 values. Wilcoxon nonparametric test was used to test the hypothesis that the two variables have the same distribution, analysed from test 1. P values <0.05 were considered significant. We were not able to find any studies measuring constriction of levator hiatus during voluntary muscle contraction. In line with other published reliability studies in this area we included between participants. An a-posteriori power calculation using observed standard deviations from a former study (12) was preformed. With 80 % power and 5 % significance level, a least detectable change of 1.49 cm 2 for the levator area constriction and 0,92 cm 2 for muscle shortening was found.
8 RESULTS The mean age of the participants was 47.9 yrs (range 29-71), mean number of births 1.8 (range 0-4) and body mass index 22.8 kg/m 2 (95%CI = ). One participant had undergone a forceps delivery, and another a caesarean delivery. Two (11.7 %) of the women reported that they sometimes experienced minor bulging of the rectum. Eight women were pre-menopausal. Eleven had college/university education and nine experienced strenuous physical work. The interval between the tests was 15.9 days (range 7-35). Measurements in the axial plane ICC values and measurements of the hiatal dimensions in the axial plane are given in Table 1. Very good reliability vas found for measurements of narrowing of LH area during contraction, LH area and transverse distance at rest and antero-posterior distance at maximum contraction. Shortening of the antero-posterior, transverse distance and pubovisceral muscle length demonstrated good reliability, as did the measurement of the antero-posterior distance and muscle length at rest and area of LH at maximum contraction. Reduction in LH transverse distance and muscle length shortening from rest to contraction showed poor and fair reliability, respectively. The LH area at rest measured 19.7 cm 2 (95% CI= ). During maximum contraction the whole area was reduced by 25% (95% CI=18-32) to cm 2 (95% CI= ). The LH antero-posterior distance shortened 22%, from 5.9 cm (95% CI= ) to 4.6 cm (95% CI= ). The transverse distance of LH shortened 6 % (95% CI=3-10). The length of the pubovisceral muscle (contractile elements only) was 12.5 cm (95% CI= ) at rest, and shortened 21% (95% CI=15-26) to 9.70 cm (95% CI= ) during contraction.
9 Measurements in the sagittal plane Test-retest values from measurements in the sagittal plane (Table 2) showed good and very good reliability, using the method of Reddy et al. (11), and showed more variable results using the method of Dietz al. (10). The position of the cervix uteri was only detected in three pairs of 17 volumes, and therefore was not analyzed. The distance from the mid urethra to the PS was 1.1 cm (95% CI= 1,0-1.2) at rest, and the distance shortened significantly by 1.1mm (95% CI= ) during contraction (p=0.03). Quantifying of the lift and direction of the displacement for BN, rectal ampulla and back sling of the puborectal muscle are presented in Table 2. During PFM contraction the BN demonstrated a displacement of 1.1 cm (95% CI= ), whereas the back sling of the muscle moved 2.0 cm (95% CI= ), rectal ampulla moved 2.0 cm (95% CI= ) and cervix uteri moved 1.5 cm (95% CI= ). All the pelvic organs moved in a cranioanterior direction. The rectal ampulla and back sling of the muscle moved significantly more than the BN (p=0.004, 0.002, respectively). During PFM contraction the BN moved 2.8 (95% CI = ) times more in the cranial direction than the anterior direction (p= 0.002). Rectal ampulla moved 2.0 (95% CI = ) times, and the back sling of the muscle moved 2.7 (95% CI = ) times as much in the cranial compared to the anterior direction (p= and 0.001, respectively). The antero-posterior distance of LH can be measured both in the axial and sagittal plane (Fig II and III). In the sagittal plane, this distance was 5.7 cm (95% CI= ) at rest, and during contraction it shortened 19% (95% CI=14-24). The total muscle length shortening was 1.5 (95% CI= ) times greater than the shortening of antero-posterior distance of LH. The increase in levator plate angle during contraction was 13 degrees (95% CI= 7-18).
10 DISCUSSION In the axial plane of minimal hiatal dimensions the reliability was good to very good for LH area, LH antero-posterior dimension, LH transverse dimension, pubovisceral muscle length and LH narrowing. Reduction of LH transverse distance and shortening of muscle length showed poor and fair reliability, respectively. During a PFM contraction the LH area was reduced by 25%. This reduction occurred mainly as a result of shortening of the anteroposterior distance. The pubovisceral muscle length shortened 21 %. In the mid sagittal plane the displacement of BN, rectal ampulla and back sling of the poborectal muscle measured with on-screen vector assessment demonstrated good reliability. The pelvic organs moved twice as much, or more, in the cranial direction compared to the anterior direction. During PFM contraction the back sling of the muscle rotated 13 degrees upwards around the PS, like a windscreen wiper. This means that the organs positioned at the furthest distance from the PS (back sling of the muscle and rectal ampulla) moved more than the BN, which is positioned closer to the PS. Additionally the circle reduces its diameter during contraction by approximately 20% (LH antero-posteror distance). Our results regarding reliability of BN displacement correspond with the reliability values of Reddy et al. (11),using the same measurement system. Since the present study is a test-retest reliability study it does not seek to demonstrate correlation with clinical symptoms or specific patient populations. The reliability coefficient for the resting area of LH demonstrated higher values (ICC: 0.86) compared to those found by Dietz et al. (5) (ICC: 0.74) and Yang et al. (13) (ICC: 0.63). The values for BN displacement during contraction found by Bo et al.(14), Dietz (15), and our values are higher than those found by other research groups (6;10;11). The differences may be due to different populations.
11 Searches on PubMed database did not reveal any studies regarding pubovisceral muscle length, muscle length reduction, narrowing of LH area and transverse distances, nor elevation of cervix uteri, rectal ampulla or back sling of the muscle during PFM contraction. The current lack of evidence for lift of the posterior compartments of the pelvic floor may be due to image techniques. When using ultrasound to measure the position and movement of the back sling of the muscle - the rectal ampulla and the cervix uteri - the method developed by Schaer et al. (16) cannot be used, since the whole PS is not totally scanned. To date, there are two possible ultrasound techniques than can be used for this purpose, both relatively independent of the position of the PS (11;17). We suggest that a possible way to evaluate the function of the puborectal muscle is to analyse muscle length shortening in the axial plane. An indirect reduction of muscle length shortening can be analysed in the sagittal plane (LH antero-posterior distance), using standard 2D ultrasound. The LH antero-posterior shortening will increase the tension in the anococcygeal ligament, and this can result in an anterior rotation of the coccygeal bone, as demonstrated with MRI by Bo et al. (18). The puborectal muscle thereby can lift, in addition to the main squeeze function. The lift of the pelvic organs mainly occurs due to shortening of the cranial orientation of the pubovaginal, puboperineal and puboanal muscles (19;20). The iliococcygeal muscle elevates the central region of the posterior pelvic floor, hence it will not provide much lift to the cervix uteri or BN (21). The relationship between the strength of the PFM and the degree of LH narrowing and lift of the pelvic organs remains to be further elucidated. A limitation of the present study can be the selection and number of participants. This study was not designed to define values for the normal population, but rather to evaluate test-retest reliability for measurements of the action of the levator ani muscles and pelvic organ motions
12 during PFM contraction. The present study demonstrates that not only the BN, but also the posterior compartment of the pelvic floor can be investigated and located using 4D ultrasound. While the measurable data most often showed acceptable reliability, one can question the reliability due to the high technical failure rate for measurements of the rectal ampulla and back sling of the puborectal muscle. The cervix uteri was identified in only three out of 17 records, and was therefore the most difficult organ to identify. When analysing the volumes we realised that if the transducer had been placed further posteriorly, less of the PS and more of the posterior compartments would have been scanned. Another explanation for the relatively high technical failure rate for some measurements can be difference in morphology among women. The larger size of the LH the harder it is to capture both the anterior and posterior compartments with a perineal transducer. Data should not be extrapolated to women with pelvic floor dysfunction, since it is likely that these women may have greater variability in anatomy and biomechanics. Several randomized controlled trials (RCTs) and systematic reviews have shown that pelvic floor muscle training (PFMT) is effective in treatment of stress and mixed urinary incontinence in women (22;23). However, to date there is scant knowledge whether the exercises affect muscle morphology (24). Possible long term effects of PFMT may be narrowing of the LH, increased cross sectional area, elevated position of the pelvic organs at rest and increased stiffness of the muscles and connective tissue. To test these hypotheses reliable measurements are needed. Randomized controlled trials using these measurements are under way.
13 CONCLUSIONS 4D ultrasound is capable of reliably measuring muscle length, narrowing of LH area, reduction of LH antero-posterior dimension and lift of BN, rectal ampulla and back sling of the puborectal muscle. Hence it is possible to use ultrasound to increase the knowledge about long term mechanisms of cure and improvement of the outcomes of PFMT. During contraction the LH area narrowed 25% and the muscle length shortened 21%. In addition the back sling of the muscle and the rectal ampulla moved more than the BN and the displacement of the pelvic organs were two times, or more, greater in the cranial versus anterior direction.
14 ACKNOWLEDGEMENTS We gratefully acknowledge support for this research through the EXTRA funds from the Norwegian Foundation for Health and Rehabilitation and the Norwegian Women s Public Health Association. We also thank Helena Frawley for important English revision of the manuscript and Hans Peter Dietz and Wolfgang Umek for valuable help setting up the ultrasound technique and analyses.
15 Legends to figures Figure I: Measurements in the axial plane of minimal hiatal dimensions. Levator hiatus area (LH area) is marked with lines. LH ap= levator hiatus; antero-posterior diameter. LH rl= Levator hiatus; transverse diameter right-left. PS= pubic symphysis. Figure II: Identifying rectal ampulla simultaneously in the sagittal, coronal and axial plane. The marker dot is marked as a star. The axial plane can be viewed to ensure that the rectal ampulla is located in the rectum (arrow). Figure III: Identifying and measuring the back sling of the puborectal muscle (PRB), levator hiatus antero-posterior distances (LH ap), levator plate angel (LPA), rectal ampulla (RA), cervix uteri (CU), bladder neck (BN, internal urethral meatus) in the mid-sagittal plane.
16 Reference List (1) Kegel A. Stress incontinence and genital relaxation. Ciba Clin Sympos 1952;2: (2) DeLancey JO. Structural aspects of the extrinsic continence mechanism. Obstet Gynecol 1988 Sep;72(3 Pt 1): (3) DeLancey JO. The anatomy of the pelvic floor. Curr Opin Obstet Gynecol 1994 Aug;6(4): (4) Bo K, Sherburn M. Evaluation of female pelvic-floor muscle function and strength. Phys Ther 2005 Mar;85(3): (5) Dietz HP, Shek C, Clarke B. Biometry of the pubovisceral muscle and levator hiatus by three-dimensional pelvic floor ultrasound. Ultrasound Obstet Gynecol 2005 Jun;25(6): (6) Thompson JA, O'sullivan PB, Briffa K, Neumann P, Court S. Assessment of pelvic floor movement using transabdominal and transperineal ultrasound. Int Urogynecol J Pelvic Floor Dysfunct 2005 Jul;16(4): (7) Peschers UM, Vodusek DB, Fanger G, Schaer GN, DeLancey JO, Schuessler B. Pelvic muscle activity in nulliparous volunteers. Neurourol Urodyn 2001;20(3): (8) Thyer I, Shek C, Dietz HP. New imaging method for assessing pelvic floor biomechanics. Ultrasound Obstet Gynecol 2008 Feb 6;31(2): (9) Margulies RU, Hsu Y, Kearney R, Stein T, Umek WH, DeLancey JO. Appearance of the levator ani muscle subdivisions in magnetic resonance images. Obstet Gynecol 2006 May;107(5): (10) Dietz HP, Wilson PD, Clarke B. The use of perineal ultrasound to quantify levator activity and teach pelvic floor muscle exercises. Int Urogynecol J Pelvic Floor Dysfunct 2001;12(3): (11) Reddy AP, DeLancey JO, Zwica LM, Ashton-Miller JA. On-screen vector-based ultrasound assessment of vesical neck movement. Am J Obstet Gynecol 2001 Jul;185(1): (12) Braekken IH, Majida M, Ellstrom-Engh M, Dietz HP, Umek W, Bo K. Test-retest and intra-observer repeatability of two-, three- and four-dimensional perineal ultrasound of pelvic floor muscle anatomy and function. Int Urogynecol J Pelvic Floor Dysfunct 2007 Jun 29. (13) Yang JM, Yang SH, Huang WC. Biometry of the pubovisceral muscle and levator hiatus in nulliparous Chinese women. Ultrasound Obstet Gynecol 2006 Oct;28(5): (14) Bo K, Sherburn M, Allen T. Transabdominal ultrasound measurement of pelvic floor muscle activity when activated directly or via a transversus abdominis muscle contraction. Neurourol Urodyn 2003;22(6):582-8.
17 (15) Dietz HP. Levator function before and after childbirth. Aust N Z J Obstet Gynaecol 2004 Feb;44(1): (16) Schaer GN, Koechli OR, Schuessler B, Haller U. Perineal ultrasound for evaluating the bladder neck in urinary stress incontinence. Obstet Gynecol 1995 Feb;85(2): (17) Dietz HP, Haylen BT, Broome J. Ultrasound in the quantification of female pelvic organ prolapse. Ultrasound Obstet Gynecol 2001 Nov;18(5): (18) Bo K, Lilleas F, Talseth T, Hedland H. Dynamic MRI of the pelvic floor muscles in an upright sitting position. Neurourol Urodyn 2001;20(2): (19) DeLancey JO, Ashton-Miller JA. MRI of intact and inured female pelvic floor muscles. In: Bo K, Berghmans B, Morkved S, Kampen MV, editors. Evidence-Based Physical Therapy for the pelvic floor. Elsevier; p (20) Kearney R, Sawhney R, DeLancey JO. Levator ani muscle anatomy evaluated by origin-insertion pairs. Obstet Gynecol 2004 Jul;104(1): (21) Ashton-Miller JA, DeLancey JO. Functional anatomy of the female pelvic floor. In: Bo K, Berghmans B, Morkved S, Kampen MV, editors. Evidence-Based Physical Therapy for the pelvic floor. Elsevier; p (22) Wilson PD, Berghmans B, Hay-Smith J, Moore K, Nygaard I, Sinclair L, et al. Adult conservative Management. In: Abrams P, Cardozo L, Khoury S, Wein A, editors. Incontinence ed. Health Publication Ltd; p (23) Hay-Smith E, Bo K, Berghmans L, Hendriks H, de BR, van Waalwijk van DE. Pelvic floor muscle training for urinary incontinence in women. Cochrane Database Syst Rev 2007;(3):CD (24) Bo K. Pelvic floor muscle training is effective in treatment of female stress urinary incontinence, but how does it work? Int Urogynecol J Pelvic Floor Dysfunct 2004 Mar;15(2):76-84.
18 Table 1. Test-retest analyses for measurement in the axial plane during pelvic floor contraction. Mean values with 95% confidence interval (CI) and ICC with 95% CI are shown. Test 1 Test 2 ICC Technical failure rate LH area rest ( ( ( % (10/34) (cm 2 ) 22.67) (n=11) 23.42) (n=13) 0.97) (n=8) LH area contraction ( ( (0.50-6% (2/34) (cm 2 ) 16.58) 17.69) (n=15) 0.92) (n=15) LH area narrowing (%) ( ) (n=11) ( ) (n=13) 0.92 ( ) (n=8) LH ap rest (cm) 5.87 ( ) 6.10 ( ) 0.70 ( % (6/34) (n=15) (n=13) 0.91) (n=11) LH ap contraction (cm) 4.58 ( ) (n=16) 4.64 ( ) (n=16) 0.92 ( ) (n=15) 6% (2/34) LH ap reduction (%) ( ) (n=15) ( ) (n=13) 0.63 ( ) (n=11) LH rl rest (cm) 4.25 ( ) 4.36 ( ) 0.82 (0.57-3% (1/34) (n=16) 0.93) (n=16) LH rl contraction 3.97 ( ) 4.19 ( ) 0.73 (0.39-3% (1/34) (cm) (n=16) 0.90) (n=16) LH rl reduction (%) 6.34 ( ) (n=16) 4.05 ( ) 0 (0-0.34) (n=16) Muscle length rest ( ( ( % (5/34) (cm) 13.79) (n=15) 14.18) (n=14) 0.92) (n=12) Muscle length 9.70 ( ) 9.57 ( ) 0.79 (0.50-6% (2/34) contraction (cm) (n=16) (n=16) 0.93) (n=15) Muscle length shortening (%) ( ) (n=15) ( ) (n=14) 0.40 (0-0.78) (n=12) LH= Levator hiatus, ap= antero-posterior distance, rl= right-left transverse distance.
19 Table 2. Test-retest analyses for displacement of the pelvic organs in the sagittal plane during pelvic floor contraction. The on screen vector method developed by Reddy et al (11) are being compared the method with a horizontal reference line developed by Dietz et al. (10). Mean with 95% confidence interval (CI) are chosen. Test 1 (cm) BN 1.13 ( ) (n=16) BN Anterior direction BN Cranial direction Rectal ampulla Rectal ampulla Anterior direction Rectal ampulla Cranial direction Puborectalis back sling Puborectalis back sling Anterior direction Puborectalis back sling Cranial direction 2.04 ( ) (n=13) 1.98 ( ) (n=13) On screen vector Test 2 ICC Technical (cm) failure 1.17 ( ) 2.09 ( ) (n=12) 1.94 ( ) (n=11) 0.81 ( ) (n=16) 0.80 ( ) (n=11) 0.75 ( ) (n=9) rate 3% (1/34) 26% (9/34) 29% (10/34) Test 1 (cm) 1.01 ( ) 0.90 ( ) 0.34 ( ) 1.96 ( ) (n=12) 1.64 ( ) (n=12) 0.94 ( ) (n=12) 1.82 ( ) (n=13) 1.64 ( ) (n=13) 0.75 ( ) (n=13) Horizontal reference line Test 2 ICC (cm) 1.01 ( ) 0.78 ( ) 0.49 ( ) 2.29 ( ) (n=11) 1.52 ( ) (n=12) 0.97 ( ) (n=11) 2.13 ( ) (n=11) 1.94 ( ) (n=11) 0.78 ( ) (n=11) 0.56 ( ) 0.61 ( ) 0.49 ( ) 0.68 ( ) (n=10) 0.25 (0-0.72) (n=11) 0.31 (0-0.77) (n=10) 0.75 ( ) (n=9) 0.69 ( ) (n= 9) 0.84 ( ) (n=9) Technical failure rate 0% 0% 29% (10/34) 32% (11/34) 29% (10/34) 29% (10/34) BN= Bladder Neck
20 Figure I
21 Figure II
22 Figure III
Learning process for performing and analyzing 3D/4D transperineal ultrasound imaging and interobserver reliability study
 Ultrasound Obstet Gynecol 2013; 41: 312 317 Published online in Wiley Online Library (wileyonlinelibrary.com). DOI: 10.1002/uog.11192 Learning process for performing and analyzing 3D/4D transperineal ultrasound
Ultrasound Obstet Gynecol 2013; 41: 312 317 Published online in Wiley Online Library (wileyonlinelibrary.com). DOI: 10.1002/uog.11192 Learning process for performing and analyzing 3D/4D transperineal ultrasound
Constriction of the levator hiatus during instruction of pelvic floor or transversus abdominis contraction: a 4D ultrasound study
 DOI 10.1007/s00192-008-0719-3 ORIGINAL ARTICLE Constriction of the levator hiatus during instruction of pelvic floor or transversus abdominis contraction: a 4D ultrasound study Kari Bø & Ingeborg H. Brækken
DOI 10.1007/s00192-008-0719-3 ORIGINAL ARTICLE Constriction of the levator hiatus during instruction of pelvic floor or transversus abdominis contraction: a 4D ultrasound study Kari Bø & Ingeborg H. Brækken
Original Article Efficacy of 3D ultrasound on diagnosis of women pelvic flour dysfunction
 Int J Clin Exp Med 2016;9(8):16523-16528 www.ijcem.com /ISSN:1940-5901/IJCEM0028796 Original Article Efficacy of 3D ultrasound on diagnosis of women pelvic flour dysfunction Aifang Chen 1*, Yingzi Zhang
Int J Clin Exp Med 2016;9(8):16523-16528 www.ijcem.com /ISSN:1940-5901/IJCEM0028796 Original Article Efficacy of 3D ultrasound on diagnosis of women pelvic flour dysfunction Aifang Chen 1*, Yingzi Zhang
This file was dowloaded from the institutional repository Brage NIH - brage.bibsys.no/nih
 This file was dowloaded from the institutional repository Brage NIH - brage.bibsys.no/nih Bø, K., Hilde, G., Stær-Jensen, J., Brækken, I. H. (2011). Can the Paula method facilitate co-contraction of the
This file was dowloaded from the institutional repository Brage NIH - brage.bibsys.no/nih Bø, K., Hilde, G., Stær-Jensen, J., Brækken, I. H. (2011). Can the Paula method facilitate co-contraction of the
Ballooning of the levator hiatus
 Ultrasound Obstet Gynecol 2008; 31: 676 680 Published online 12 May 2008 in Wiley InterScience (www.interscience.wiley.com). DOI: 10.1002/uog.5355 Ballooning of the levator hiatus H. P. DIETZ*, C. SHEK*,
Ultrasound Obstet Gynecol 2008; 31: 676 680 Published online 12 May 2008 in Wiley InterScience (www.interscience.wiley.com). DOI: 10.1002/uog.5355 Ballooning of the levator hiatus H. P. DIETZ*, C. SHEK*,
Pelvic floor function in elite nulliparous athletes
 Ultrasound Obstet Gynecol 2007; 30: 81 85 Published online 14 May 2007 in Wiley InterScience (www.interscience.wiley.com). DOI: 10.1002/uog.4027 Pelvic floor function in elite nulliparous athletes J. A.
Ultrasound Obstet Gynecol 2007; 30: 81 85 Published online 14 May 2007 in Wiley InterScience (www.interscience.wiley.com). DOI: 10.1002/uog.4027 Pelvic floor function in elite nulliparous athletes J. A.
Guide to Pelvic Floor Multicompartment Scanning
 Guide to Pelvic Floor Multicompartment Scanning These guidelines have been prepared by Giulio A. Santoro, MD, PhD, Head Pelvic Floor Unit, Section of Anal Physiology and Ultrasound, Coloproctology Service,
Guide to Pelvic Floor Multicompartment Scanning These guidelines have been prepared by Giulio A. Santoro, MD, PhD, Head Pelvic Floor Unit, Section of Anal Physiology and Ultrasound, Coloproctology Service,
Urogynaecology. Introduction. G Hilde, a,b J Stær-Jensen, b F Siafarikas, b,c K Gjestland, b M Ellstr om Engh, b,c KBø a,b
 DOI: 10.1111/1471-0528.12321 www.bjog.org Urogynaecology How well can pelvic floor muscles with major defects contract? A cross-sectional comparative study 6 weeks after delivery using transperineal 3D/4D
DOI: 10.1111/1471-0528.12321 www.bjog.org Urogynaecology How well can pelvic floor muscles with major defects contract? A cross-sectional comparative study 6 weeks after delivery using transperineal 3D/4D
Biometry of the pubovisceral muscle and levator hiatus by three-dimensional pelvic floor ultrasound
 Ultrasound Obstet Gynecol 2005; 25: 580 585 Published online 10 May 2005 in Wiley InterScience (www.interscience.wiley.com). DOI: 10.1002/uog.1899 Biometry of the pubovisceral muscle and levator hiatus
Ultrasound Obstet Gynecol 2005; 25: 580 585 Published online 10 May 2005 in Wiley InterScience (www.interscience.wiley.com). DOI: 10.1002/uog.1899 Biometry of the pubovisceral muscle and levator hiatus
The pelvic floor muscles (PFM) form
 form") Correlation of Digital Palpation and Transabdominal Ultrasound for Assessment of Pelvic Floor Muscle Contraction Amir Massoud Arab, PT, PhD 1 ; Roxana Bazaz Behbahani, PT, BSc 2 ; Leila Lorestani, PT,
Correlation of Digital Palpation and Transabdominal Ultrasound for Assessment of Pelvic Floor Muscle Contraction Amir Massoud Arab, PT, PhD 1 ; Roxana Bazaz Behbahani, PT, BSc 2 ; Leila Lorestani, PT,
Dynamic rehabilitative ultrasound for pelvic floor disorders Introduction in techniques and hands-on-workshop
 Dynamic rehabilitative ultrasound for pelvic floor disorders Introduction in techniques and hands-on-workshop Bärbel Junginger, B.Sc. /physiotherapist, manualtherapist (IFOMPT) Kaven Baessler, MD, PhD
Dynamic rehabilitative ultrasound for pelvic floor disorders Introduction in techniques and hands-on-workshop Bärbel Junginger, B.Sc. /physiotherapist, manualtherapist (IFOMPT) Kaven Baessler, MD, PhD
New imaging method for assessing pelvic floor biomechanics
 Ultrasound Obstet Gynecol 2008; 31: 201 205 Published online in Wiley InterScience (www.interscience.wiley.com). DOI: 10.1002/uog.5219 New imaging method for assessing pelvic floor biomechanics I. THYER*,
Ultrasound Obstet Gynecol 2008; 31: 201 205 Published online in Wiley InterScience (www.interscience.wiley.com). DOI: 10.1002/uog.5219 New imaging method for assessing pelvic floor biomechanics I. THYER*,
NIH Public Access Author Manuscript Int Urogynecol J. Author manuscript; available in PMC 2012 December 06.
 NIH Public Access Author Manuscript Published in final edited form as: Int Urogynecol J. 2011 December ; 22(12): 1491 1495. doi:10.1007/s00192-011-1458-4. URETHRAL CLOSURE PRESSURES AMONG PRIMIPAROUS WOMEN
NIH Public Access Author Manuscript Published in final edited form as: Int Urogynecol J. 2011 December ; 22(12): 1491 1495. doi:10.1007/s00192-011-1458-4. URETHRAL CLOSURE PRESSURES AMONG PRIMIPAROUS WOMEN
This file was dowloaded from the institutional repository Brage NIH - brage.bibsys.no/nih
 This file was dowloaded from the institutional repository Brage NIH - brage.bibsys.no/nih Bø, K., Majida, M., Engh, M. E. (2012). Does a ring pessary in situ influence the pelvic floor muscle function
This file was dowloaded from the institutional repository Brage NIH - brage.bibsys.no/nih Bø, K., Majida, M., Engh, M. E. (2012). Does a ring pessary in situ influence the pelvic floor muscle function
Why are some women with pelvic floor dysfunction unable to contract their pelvic floor muscles?
 Australian and New Zealand Journal of Obstetrics and Gynaecology 2013; 53: 574 579 DOI: 10.1111/ajo.12133 Original Article Why are some women with pelvic floor dysfunction unable to contract their pelvic
Australian and New Zealand Journal of Obstetrics and Gynaecology 2013; 53: 574 579 DOI: 10.1111/ajo.12133 Original Article Why are some women with pelvic floor dysfunction unable to contract their pelvic
Pelvic Floor Ultrasound Imaging. Prof HP Dietz (Sydney) A/Prof KL Shek (Sydney) Dr R Guzman Rojas (Santiago de Chile) Dr Kamil Svabik (Prague)
 A/Prof KL Shek (Sydney) Dr R Guzman Rojas (Santiago de Chile) Dr Kamil Svabik (Prague)") Pelvic Floor Ultrasound Imaging Workshop IUGA 2015 Nice Faculty: Prof HP Dietz (Sydney) A/Prof KL Shek (Sydney) Dr R Guzman Rojas (Santiago de Chile) Dr Kamil Svabik (Prague) The use of translabial ultrasound
Pelvic Floor Ultrasound Imaging Workshop IUGA 2015 Nice Faculty: Prof HP Dietz (Sydney) A/Prof KL Shek (Sydney) Dr R Guzman Rojas (Santiago de Chile) Dr Kamil Svabik (Prague) The use of translabial ultrasound
Levator trauma is associated with pelvic organ prolapse
 DOI: 10.1111/j.1471-0528.2008.01751.x www.blackwellpublishing.com/bjog Urogynaecology Levator trauma is associated with pelvic organ prolapse HP Dietz, a JM Simpson b a Department of Obstetrics and Gynaecology,
DOI: 10.1111/j.1471-0528.2008.01751.x www.blackwellpublishing.com/bjog Urogynaecology Levator trauma is associated with pelvic organ prolapse HP Dietz, a JM Simpson b a Department of Obstetrics and Gynaecology,
Association between Magnetic Resonance Imaging Findings of the Pelvic Floor and de novo Stress Urinary Incontinence after Vaginal Delivery
 Original Article Genitourinary Imaging https://doi.org/10.3348/kjr.2018.19.4.715 pissn 1229-6929 eissn 2005-8330 Korean J Radiol 2018;19(4):715-723 Association between Magnetic Resonance Imaging Findings
Original Article Genitourinary Imaging https://doi.org/10.3348/kjr.2018.19.4.715 pissn 1229-6929 eissn 2005-8330 Korean J Radiol 2018;19(4):715-723 Association between Magnetic Resonance Imaging Findings
Aetiology 1998 Bump & Norton Theoretical model
 Kate Lough MSc MCSP Handout IUGA Nice 2015 Physiotherapy and the Provision of Pelvic Floor Muscle Training and Lifestyle Intervention in the Conservative Management of Pelvic Organ Prolapse an evidence
Kate Lough MSc MCSP Handout IUGA Nice 2015 Physiotherapy and the Provision of Pelvic Floor Muscle Training and Lifestyle Intervention in the Conservative Management of Pelvic Organ Prolapse an evidence
ORIGINAL ARTICLE. Judith A. Thompson & Peter B. O Sullivan & N. Kathryn Briffa & Patricia Neumann
 Int Urogynecol J (2007) 18:779 786 DOI 10.1007/s00192-006-0225-4 ORIGINAL ARTICLE Comparison of transperineal and transabdominal ultrasound in the assessment of voluntary pelvic floor muscle contractions
Int Urogynecol J (2007) 18:779 786 DOI 10.1007/s00192-006-0225-4 ORIGINAL ARTICLE Comparison of transperineal and transabdominal ultrasound in the assessment of voluntary pelvic floor muscle contractions
Levator Plate Upward Lift on Dynamic Sonography and Levator Muscle Strength
 ORIGINAL RESEARCH Levator Plate Upward Lift on Dynamic Sonography and Levator Muscle Strength Ghazaleh Rostaminia, MD, Jennifer Peck, PhD, Lieschen Quiroz, MD, S. Abbas Shobeiri, MD Received December 4,
ORIGINAL RESEARCH Levator Plate Upward Lift on Dynamic Sonography and Levator Muscle Strength Ghazaleh Rostaminia, MD, Jennifer Peck, PhD, Lieschen Quiroz, MD, S. Abbas Shobeiri, MD Received December 4,
High-field (3T) magnetic resonance defecography with functional assessment of the evacuation phase: A pictorial essay
 magnetic resonance defecography with functional assessment of the evacuation phase: A pictorial essay") High-field (3T) magnetic resonance defecography with functional assessment of the evacuation phase: A pictorial essay Poster No.: C-430 Congress: ECR 2009 Type: Educational Exhibit Topic: Abdominal and
High-field (3T) magnetic resonance defecography with functional assessment of the evacuation phase: A pictorial essay Poster No.: C-430 Congress: ECR 2009 Type: Educational Exhibit Topic: Abdominal and
Original paper Med Ultrason 2016, Vol. 18, no. 3,
 Original paper Med Ultrason 2016, Vol. 18, no. 3, 345-350 DOI: 10.11152/mu.2013.2066.183.zsu Reproducibility in pelvic floor biometric parameters of nulliparous women assessed by translabial three-dimensional
Original paper Med Ultrason 2016, Vol. 18, no. 3, 345-350 DOI: 10.11152/mu.2013.2066.183.zsu Reproducibility in pelvic floor biometric parameters of nulliparous women assessed by translabial three-dimensional
Abstract. Introduction
 Original article doi:10.1111/codi.12740 Assessment of pubovisceral muscle defects and levator hiatal dimensions in women with faecal incontinence after vaginal delivery: is there a correlation with severity
Original article doi:10.1111/codi.12740 Assessment of pubovisceral muscle defects and levator hiatal dimensions in women with faecal incontinence after vaginal delivery: is there a correlation with severity
Minimal criteria for the diagnosis of avulsion of the puborectalis muscle by tomographic ultrasound
 Int Urogynecol J (2011) 22:699 704 DOI 10.1007/s00192-010-1329-4 ORIGINAL ARTICLE Minimal criteria for the diagnosis of avulsion of the puborectalis muscle by tomographic ultrasound Hans Peter Dietz &
Int Urogynecol J (2011) 22:699 704 DOI 10.1007/s00192-010-1329-4 ORIGINAL ARTICLE Minimal criteria for the diagnosis of avulsion of the puborectalis muscle by tomographic ultrasound Hans Peter Dietz &
Is pelvic organ support different between young nulliparous African and Caucasian women?
 Ultrasound Obstet Gynecol 2016; 47: 774 778 Published online 2 May 2016 in Wiley Online Library (wileyonlinelibrary.com). DOI: 10.1002/uog.15811 Is pelvic organ support different between young nulliparous
Ultrasound Obstet Gynecol 2016; 47: 774 778 Published online 2 May 2016 in Wiley Online Library (wileyonlinelibrary.com). DOI: 10.1002/uog.15811 Is pelvic organ support different between young nulliparous
Inter- and intraobserver reliability for diagnosing levator ani changes on magnetic resonance imaging
 Ultrasound Obstet Gynecol 2013; 42: 347 352 Published online in Wiley Online Library (wileyonlinelibrary.com). DOI: 10.1002/uog.12462 Inter- and intraobserver reliability for diagnosing levator ani changes
Ultrasound Obstet Gynecol 2013; 42: 347 352 Published online in Wiley Online Library (wileyonlinelibrary.com). DOI: 10.1002/uog.12462 Inter- and intraobserver reliability for diagnosing levator ani changes
A. FALKERT, A. WILLMANN, E. ENDRESS, P. MEINT and B. SEELBACH-GÖBEL ABSTRACT
 Ultrasound Obstet Gynecol 2013; 41: 204 209 Published online in Wiley Online Library (wileyonlinelibrary.com). DOI: 10.1002/uog.11214 Three-dimensional ultrasound of pelvic floor: is there a correlation
Ultrasound Obstet Gynecol 2013; 41: 204 209 Published online in Wiley Online Library (wileyonlinelibrary.com). DOI: 10.1002/uog.11214 Three-dimensional ultrasound of pelvic floor: is there a correlation
The prevalence of major abnormalities of the levator ani in urogynaecological patients
 DOI: 10.1111/j.1471-0528.2006.00819.x www.blackwellpublishing.com/bjog Urogynaecology The prevalence of major abnormalities of the levator ani in urogynaecological patients HP Dietz, a AB Steensma b a
DOI: 10.1111/j.1471-0528.2006.00819.x www.blackwellpublishing.com/bjog Urogynaecology The prevalence of major abnormalities of the levator ani in urogynaecological patients HP Dietz, a AB Steensma b a
International Journal of Health Sciences and Research ISSN:
 International Journal of Health Sciences and Research www.ijhsr.org ISSN: 2249-9571 Original Research Article Correlation of Digital Examination Vs Perineometry in Measuring the Pelvic Floor Muscles Strength
International Journal of Health Sciences and Research www.ijhsr.org ISSN: 2249-9571 Original Research Article Correlation of Digital Examination Vs Perineometry in Measuring the Pelvic Floor Muscles Strength
Biometry of the pubovisceral muscle and levator hiatus in nulliparous Chinese women
 Ultrasound Obstet Gynecol 2006; 28: 710 716 Published online in Wiley InterScience (www.interscience.wiley.com). DOI: 10.1002/uog.3825 Biometry of the pubovisceral muscle and levator hiatus in nulliparous
Ultrasound Obstet Gynecol 2006; 28: 710 716 Published online in Wiley InterScience (www.interscience.wiley.com). DOI: 10.1002/uog.3825 Biometry of the pubovisceral muscle and levator hiatus in nulliparous
Comprehensive 3D Pelvic Floor Ultrasonography with emphasis on endovaginal (EVUS) and endoanal imaging (EAUS) W44, 30 August :00-18:00
 and endoanal imaging (EAUS) W44, 30 August :00-18:00") Comprehensive 3D Pelvic Floor Ultrasonography with emphasis on endovaginal (EVUS) and endoanal imaging (EAUS) W44, 30 August 2011 14:00-18:00 Start End Topic Speakers 14:00 14:10 Introduction: Pre-test,
Comprehensive 3D Pelvic Floor Ultrasonography with emphasis on endovaginal (EVUS) and endoanal imaging (EAUS) W44, 30 August 2011 14:00-18:00 Start End Topic Speakers 14:00 14:10 Introduction: Pre-test,
PELVIC FLOOR ULTRASOUND
 PELVIC FLOOR ULTRASOUND How, When, Why Part 1: Phyllis Glanc MD Sunnybrook Health Science Center University of Toronto Phyllis.Glanc@sunnybrook.ca www.phyllisglanc.com (current exact handout) Disclosures
PELVIC FLOOR ULTRASOUND How, When, Why Part 1: Phyllis Glanc MD Sunnybrook Health Science Center University of Toronto Phyllis.Glanc@sunnybrook.ca www.phyllisglanc.com (current exact handout) Disclosures
Association between ICS POP-Q coordinates and translabial ultrasound findings: implications for definition of normal pelvic organ support
 Ultrasound Obstet Gynecol 216; 47: 36368 Published online 29 January 216 in Wiley Online Library (wileyonlinelibrary.com). DOI: 1.12/uog.14872 Association between ICS POP-Q coordinates and translabial
Ultrasound Obstet Gynecol 216; 47: 36368 Published online 29 January 216 in Wiley Online Library (wileyonlinelibrary.com). DOI: 1.12/uog.14872 Association between ICS POP-Q coordinates and translabial
This file was dowloaded from the institutional repository Brage NIH - brage.bibsys.no/nih
 This file was dowloaded from the institutional repository Brage NIH - brage.bibsys.no/nih Bø, Kari (2012). Pelvic floor muscle training in treatment of female stress urinary incontinence, pelvic organ
This file was dowloaded from the institutional repository Brage NIH - brage.bibsys.no/nih Bø, Kari (2012). Pelvic floor muscle training in treatment of female stress urinary incontinence, pelvic organ
Does childbirth alter the reflex pelvic floor response to coughing?
 Ultrasound Obstet Gynecol (2012) Published online in Wiley Online Library (wileyonlinelibrary.com). DOI: 10.1002/uog.10083 Does childbirth alter the reflex pelvic floor response to coughing? H. P. DIETZ,
Ultrasound Obstet Gynecol (2012) Published online in Wiley Online Library (wileyonlinelibrary.com). DOI: 10.1002/uog.10083 Does childbirth alter the reflex pelvic floor response to coughing? H. P. DIETZ,
Does delayed child-bearing increase the risk of levator injury in labour?
 Australian and New Zealand Journal of Obstetrics and Gynaecology 2007; 47: 491 495 Blackwell Publishing Asia Original Article Delayed child-bearing and levator injury Does delayed child-bearing increase
Australian and New Zealand Journal of Obstetrics and Gynaecology 2007; 47: 491 495 Blackwell Publishing Asia Original Article Delayed child-bearing and levator injury Does delayed child-bearing increase
Ultrasound Characteristics of Patients with Urinary Stress Incontinence with or without Genital Prolapse
 www.kjurology.org http://dx.doi.org/10.4111/kju.2012.53.10.691 Voiding Dysfunction Ultrasound Characteristics of Patients with Urinary Stress Incontinence with or without Genital Prolapse Vesna S. Antovska
www.kjurology.org http://dx.doi.org/10.4111/kju.2012.53.10.691 Voiding Dysfunction Ultrasound Characteristics of Patients with Urinary Stress Incontinence with or without Genital Prolapse Vesna S. Antovska
Diagnosis of cystocele type by clinical examination and pelvic floor ultrasound
 Ultrasound Obstet Gynecol 2012; 39: 710 714 Published online in Wiley Online Library (wileyonlinelibrary.com). DOI: 10.1002/uog.10156 Diagnosis of cystocele type by clinical examination and pelvic floor
Ultrasound Obstet Gynecol 2012; 39: 710 714 Published online in Wiley Online Library (wileyonlinelibrary.com). DOI: 10.1002/uog.10156 Diagnosis of cystocele type by clinical examination and pelvic floor
Measuring echogenicity and area of the puborectalis muscle: method and reliability
 Ultrasound Obstet Gynecol 2014; 44: 481 485 Published online in Wiley Online Library (wileyonlinelibrary.com). DOI: 10.1002/uog.13409 Measuring echogenicity and area of the puborectalis muscle: method
Ultrasound Obstet Gynecol 2014; 44: 481 485 Published online in Wiley Online Library (wileyonlinelibrary.com). DOI: 10.1002/uog.13409 Measuring echogenicity and area of the puborectalis muscle: method
The relationship between postpartum levator ani muscle avulsion and signs and symptoms of pelvic floor dysfunction
 DOI: 10.1111/1471-0528.12666 www.bjog.org Urogynaecology The relationship between postpartum levator ani muscle avulsion and signs and symptoms of pelvic floor dysfunction K van Delft, a AH Sultan, a R
DOI: 10.1111/1471-0528.12666 www.bjog.org Urogynaecology The relationship between postpartum levator ani muscle avulsion and signs and symptoms of pelvic floor dysfunction K van Delft, a AH Sultan, a R
Does levator ani injury affect cystocele type?
 Ultrasound Obstet Gynecol 2010; 36: 618 623 Published online in Wiley Online Library (wileyonlinelibrary.com). DOI: 10.1002/uog.7712 Does levator ani injury affect cystocele type? V. H. EISENBERG*, V.
Ultrasound Obstet Gynecol 2010; 36: 618 623 Published online in Wiley Online Library (wileyonlinelibrary.com). DOI: 10.1002/uog.7712 Does levator ani injury affect cystocele type? V. H. EISENBERG*, V.
Healthy adults can more easily elevate the pelvic floor in standing than in crook-lying: an experimental study
 Healthy adults can more easily elevate the pelvic floor in standing than in crook-lying: an experimental study Malina Kelly, B-K Tan, Judith Thompson, Sara Carroll, Melissa Follington, Alicia Arndt and
Healthy adults can more easily elevate the pelvic floor in standing than in crook-lying: an experimental study Malina Kelly, B-K Tan, Judith Thompson, Sara Carroll, Melissa Follington, Alicia Arndt and
Special Thank You NO DISCLOSURES. Objectives. Pelvic Floor Dysfunction Role of Ultrasound Text
 Special Thank You Pelvic Floor Dysfunction Role of Ultrasound Phyllis Glanc Sunnybrook Health Sciences Center Department Medical Imaging Associate Professor, University of Toronto phyllis.glanc@sunnybrook.ca
Special Thank You Pelvic Floor Dysfunction Role of Ultrasound Phyllis Glanc Sunnybrook Health Sciences Center Department Medical Imaging Associate Professor, University of Toronto phyllis.glanc@sunnybrook.ca
Bladder neck mobility in continent nulliparous women
 British Journal of Obstetrics and Gynaecology March 2001, Vol. 108, pp. 320±324 Bladder neck mobility in continent nulliparous women Ursula M. Peschers a, *, Gabi Fanger b, Gabriel N. Schaer c, David B.
British Journal of Obstetrics and Gynaecology March 2001, Vol. 108, pp. 320±324 Bladder neck mobility in continent nulliparous women Ursula M. Peschers a, *, Gabi Fanger b, Gabriel N. Schaer c, David B.
PELVIC FLOOR ASSESSMENT
 Fetal and Maternal Medicine Review 2009; 20:1 49 66 C 2009 Cambridge University Press doi:10.1017/s096553950900237x First published online 17 March 2009 PELVIC FLOOR ASSESSMENT HANS PETER DIETZ Nepean
Fetal and Maternal Medicine Review 2009; 20:1 49 66 C 2009 Cambridge University Press doi:10.1017/s096553950900237x First published online 17 March 2009 PELVIC FLOOR ASSESSMENT HANS PETER DIETZ Nepean
17 th European congress of Physical Rehabilitation Medicine. 38th SIMFER congress
 17 th European congress of Physical Rehabilitation Medicine 38th SIMFER congress European Rehabilitation: Quality, Evidence, Efficacy and Effectiveness Venice, May 23 27 2010 THE PHYSIATRIST AND URO-GYNECOLOGICAL
17 th European congress of Physical Rehabilitation Medicine 38th SIMFER congress European Rehabilitation: Quality, Evidence, Efficacy and Effectiveness Venice, May 23 27 2010 THE PHYSIATRIST AND URO-GYNECOLOGICAL
Use of a visual analog scale for evaluation of bother from pelvic organ prolapse
 Ultrasound Obstet Gynecol 2014; 43: 693 697 Published online in Wiley Online Library (wileyonlinelibrary.com). DOI: 10.1002/uog.13222 Use of a visual analog scale for evaluation of bother from pelvic organ
Ultrasound Obstet Gynecol 2014; 43: 693 697 Published online in Wiley Online Library (wileyonlinelibrary.com). DOI: 10.1002/uog.13222 Use of a visual analog scale for evaluation of bother from pelvic organ
M. OTCENASEK*, L. KROFTA*, V. BACA, R. GRILL, E. KUCERA*, H. HERMAN*, I. VASICKA*, J. DRAHONOVSKY* and J. FEYEREISL*
 Ultrasound Obstet Gynecol 2007; 29: 692 696 Published online in Wiley InterScience (www.interscience.wiley.com). DOI: 10.1002/uog.4030 Bilateral avulsion of the puborectal muscle: magnetic resonance imaging-based
Ultrasound Obstet Gynecol 2007; 29: 692 696 Published online in Wiley InterScience (www.interscience.wiley.com). DOI: 10.1002/uog.4030 Bilateral avulsion of the puborectal muscle: magnetic resonance imaging-based
Test-Retest Reliability of an Instrumented Speculum for Measuring Vaginal Closure Force
 Neurourology and Urodynamics 26:858 863 (2007) Test-Retest Reliability of an Instrumented Speculum for Measuring Vaginal Closure Force J.M. Miller, 1,4 * y J.A. Ashton-Miller, 2{ D. Perruchini, 3 and J.O.L.
Neurourology and Urodynamics 26:858 863 (2007) Test-Retest Reliability of an Instrumented Speculum for Measuring Vaginal Closure Force J.M. Miller, 1,4 * y J.A. Ashton-Miller, 2{ D. Perruchini, 3 and J.O.L.
Bill Landry BScPT, BScH, MCPA, CAFCI Family Physiotherapy Centre of London
 Bill Landry BScPT, BScH, MCPA, CAFCI blandry@fpclondon.com Family Physiotherapy Centre of London Objectives To describe the scope of post-prostatectomy incontinence To describe what s been done To provide
Bill Landry BScPT, BScH, MCPA, CAFCI blandry@fpclondon.com Family Physiotherapy Centre of London Objectives To describe the scope of post-prostatectomy incontinence To describe what s been done To provide
Pelvic Floor Muscle Training Concept
 Intervention published in Trials 2015 Nov 17;16(1):524 as additional file 1 Pelvic Floor Muscle Training Concept for Women Suffering from Stress Urinary Incontinence Helena Luginbuehl 1,2, Corinne Lehmann
Intervention published in Trials 2015 Nov 17;16(1):524 as additional file 1 Pelvic Floor Muscle Training Concept for Women Suffering from Stress Urinary Incontinence Helena Luginbuehl 1,2, Corinne Lehmann
What are we talking about? Symptoms. Prolapse Risk Factors. Vaginal bulge 1 Splinting. ?? Pelvic pressure Back pain 1 Urinary complaints 2
 Options for Vaginal Prolapse What are we talking about? Michelle Y. Morrill, M.D. Director of Urogynecology The Permanente Medical Group Kaiser, San Francisco Assistant Professor, Volunteer Faculty Department
Options for Vaginal Prolapse What are we talking about? Michelle Y. Morrill, M.D. Director of Urogynecology The Permanente Medical Group Kaiser, San Francisco Assistant Professor, Volunteer Faculty Department
Effect of postpartum pelvic floor muscle training in prevention and treatment of urinary incontinence: a one-year follow up
 British Journal of Obstetrics and Gynaecology August 2000, V01107, pp. 1022-1028 Effect of postpartum pelvic floor muscle training in prevention and treatment of urinary incontinence: a one-year follow
British Journal of Obstetrics and Gynaecology August 2000, V01107, pp. 1022-1028 Effect of postpartum pelvic floor muscle training in prevention and treatment of urinary incontinence: a one-year follow
Axial Plane Imaging. Hans Peter Dietz. Levator Ani Complex
 6 Axial Plane Imaging Hans Peter Dietz Levator Ani Complex It is only very recently that imaging of the levator ani has become feasible using translabial ultrasound. The inferior aspects of the levator
6 Axial Plane Imaging Hans Peter Dietz Levator Ani Complex It is only very recently that imaging of the levator ani has become feasible using translabial ultrasound. The inferior aspects of the levator
Effect of PFMT: Kegel, LA, USA Pelvic floor rehabilitation. Problems with systematic reviews / meta-analysis 15/10/2013
 Exercise programs for the pelvic floor evidence for an optimal program? ICS Barcelona PT-Roundtable 2013 Kari Bø Professor, PhD PT, Exercise Scientist Affiliations to disclose: Enter Organisation/relationship
Exercise programs for the pelvic floor evidence for an optimal program? ICS Barcelona PT-Roundtable 2013 Kari Bø Professor, PhD PT, Exercise Scientist Affiliations to disclose: Enter Organisation/relationship
Efficacy of Adding Active Technique as Biofeedback to Pelvic Floor Muscles Training on Cure of Female Stress Urinary Incontinence- A Systematic Review
 Med. J. Cairo Univ., Vol. 85, No. 1, March: 289-294, 2017 www.medicaljournalofcairouniversity.net Efficacy of Adding Active Technique as Biofeedback to Pelvic Floor Muscles Training on Cure of Female Stress
Med. J. Cairo Univ., Vol. 85, No. 1, March: 289-294, 2017 www.medicaljournalofcairouniversity.net Efficacy of Adding Active Technique as Biofeedback to Pelvic Floor Muscles Training on Cure of Female Stress
Clinical Study Perineal Ultrasound as a Complement to POP-Q in the Assessment of Cystoceles
 BioMed Research International, Article ID 740925, 7 pages http://dx.doi.org/10.1155/2014/740925 Clinical Study Perineal Ultrasound as a Complement to POP-Q in the Assessment of Cystoceles Laila Najjari,
BioMed Research International, Article ID 740925, 7 pages http://dx.doi.org/10.1155/2014/740925 Clinical Study Perineal Ultrasound as a Complement to POP-Q in the Assessment of Cystoceles Laila Najjari,
How common is pelvic floor muscle atrophy after vaginal childbirth?
 Ultrasound Obstet Gynecol 2014; 43: 3 Published online 2 December 2013 in Wiley Online Library wileyonlinelibrary.com. DOI: 10.1002/uog.12543 How common is pelvic floor muscle atrophy after vaginal childbirth?
Ultrasound Obstet Gynecol 2014; 43: 3 Published online 2 December 2013 in Wiley Online Library wileyonlinelibrary.com. DOI: 10.1002/uog.12543 How common is pelvic floor muscle atrophy after vaginal childbirth?
MATERIALS AND METHODS We recruited 8 older women with weekly FI aged years (older incontinent
 Fecal incontinence in older women: are levator ani defects a factor? Christina LewickyGaupp, MD; Cynthia Brincat, MD; Aisha Yousuf, MD; Divya A. Patel, PhD; John O. L. Delancey, MD; Dee E. Fenner, MD OBJECTIVE:
Fecal incontinence in older women: are levator ani defects a factor? Christina LewickyGaupp, MD; Cynthia Brincat, MD; Aisha Yousuf, MD; Divya A. Patel, PhD; John O. L. Delancey, MD; Dee E. Fenner, MD OBJECTIVE:
[ clinical commentary ]
![[ clinical commentary ]](/thumbs/77/74903938.jpg "[ clinical commentary ]") Jackie L. Whittaker, PT, FCAMT 1 Judith A. Thompson, Dip PT, Post-grad Dip PT, PhD 2 Deydre S. Teyhen, PT, PhD, OCS 3 Paul Hodges, PhD, MedDr, BPhty (Hons) 4 Rehabilitative Ultrasound Imaging of Pelvic
Jackie L. Whittaker, PT, FCAMT 1 Judith A. Thompson, Dip PT, Post-grad Dip PT, PhD 2 Deydre S. Teyhen, PT, PhD, OCS 3 Paul Hodges, PhD, MedDr, BPhty (Hons) 4 Rehabilitative Ultrasound Imaging of Pelvic
A Bearinger, SPT; B Cobb, SPT; L Shank, SPT; M Gevontmakher, SPT
 What goes up must come down? An analysis of the Periform Plus intravaginal sensor with indicator using simultaneous Ultrasound imaging and Surface Electromyography in healthy continent women. A Bearinger,
What goes up must come down? An analysis of the Periform Plus intravaginal sensor with indicator using simultaneous Ultrasound imaging and Surface Electromyography in healthy continent women. A Bearinger,
Workshop 2 IUGA, DUBLIN MAY 2013: PREVENTION AND TREATMENT OF URINARY INCONTINENCE DURING PREGNANCY AND AFTER CHILDBIRTH Chair: Kari Bø
 Workshop 2 IUGA, DUBLIN MAY 2013: PREVENTION AND TREATMENT OF URINARY INCONTINENCE DURING PREGNANCY AND AFTER CHILDBIRTH Chair: Kari Bø Childbirth Injuries and the Pelvic Floor Wael Agur MD MRCOG Consultant
Workshop 2 IUGA, DUBLIN MAY 2013: PREVENTION AND TREATMENT OF URINARY INCONTINENCE DURING PREGNANCY AND AFTER CHILDBIRTH Chair: Kari Bø Childbirth Injuries and the Pelvic Floor Wael Agur MD MRCOG Consultant
Modern methods of imaging in urogynecology when do we really need them?
 Archives of Perinatal Medicine 23(2), 77 81, 2017 ORIGINAL PAPER Modern methods of imaging in urogynecology when do we really need them? GRZEGORZ SURKONT, EDYTA WLAŹLAK Abstract Imaging is more often used
Archives of Perinatal Medicine 23(2), 77 81, 2017 ORIGINAL PAPER Modern methods of imaging in urogynecology when do we really need them? GRZEGORZ SURKONT, EDYTA WLAŹLAK Abstract Imaging is more often used
USING AN INVERSE METHOD TO OBTAIN THE MATERIAL PARAMETERS OF THE MOONEY-RIVLIN CONSTITUTIVE MODEL FOR PELVIC FLOOR MUSCLES
 Congresso de Métodos Numéricos em Engenharia 2015 Lisboa, 29 de Junho a 2 de Julho, 2015 APMTAC, Portugal, 2015 USING AN INVERSE METHOD TO OBTAIN THE MATERIAL PARAMETERS OF THE MOONEY-RIVLIN CONSTITUTIVE
Congresso de Métodos Numéricos em Engenharia 2015 Lisboa, 29 de Junho a 2 de Julho, 2015 APMTAC, Portugal, 2015 USING AN INVERSE METHOD TO OBTAIN THE MATERIAL PARAMETERS OF THE MOONEY-RIVLIN CONSTITUTIVE
3D Dynamic Ultrasound In Obstructed Defecation
 3D Dynamic Ultrasound In Obstructed Defecation By Ramy Salahudin Abdelkader Assist. Lecturer of General Surgery Cairo University Introduction Pelvic floor is complex system, with passive and active components
3D Dynamic Ultrasound In Obstructed Defecation By Ramy Salahudin Abdelkader Assist. Lecturer of General Surgery Cairo University Introduction Pelvic floor is complex system, with passive and active components
IUGA : Introduction: Pre-test, Course objectives, clinical (Max 1000 words) and rationale for pelvic floor imaging S.
 and rationale for pelvic floor imaging S.") IUGA WS 7 Workshop Outline Chairman: S. Abbas Shobeiri, MD (USA) IUGA Title of workshop Comprehensive 3D Pelvic Floor Ultrasonography with emphasis on endovaginal (EVUS) and endoanal imaging IU(EA (EAUS)
IUGA WS 7 Workshop Outline Chairman: S. Abbas Shobeiri, MD (USA) IUGA Title of workshop Comprehensive 3D Pelvic Floor Ultrasonography with emphasis on endovaginal (EVUS) and endoanal imaging IU(EA (EAUS)
Functional anatomy of the female pelvic floor and lower urinary tract Stefano Floris, MD, PhD Department of Obstetrics and Gynaecology
 Functional anatomy of the female pelvic floor and lower urinary tract Stefano Floris, MD, PhD Department of Obstetrics and Gynaecology Ospedale San Giovanni di Dio, Gorizia, Italy ANATOMY URINARY CONTINENCE
Functional anatomy of the female pelvic floor and lower urinary tract Stefano Floris, MD, PhD Department of Obstetrics and Gynaecology Ospedale San Giovanni di Dio, Gorizia, Italy ANATOMY URINARY CONTINENCE
Laparoscopic sacrocolpopexy: how low does the mesh go?
 Ultrasound Obstet Gynecol 2017; 49: 404 408 Published online 7 February 2017 in Wiley Online Library (wileyonlinelibrary.com). DOI: 10.1002/uog.15882 Laparoscopic sacrocolpopexy: how low does the mesh
Ultrasound Obstet Gynecol 2017; 49: 404 408 Published online 7 February 2017 in Wiley Online Library (wileyonlinelibrary.com). DOI: 10.1002/uog.15882 Laparoscopic sacrocolpopexy: how low does the mesh
NIH Public Access Author Manuscript Eur J Obstet Gynecol Reprod Biol. Author manuscript; available in PMC 2010 May 1.
 NIH Public Access Author Manuscript Published in final edited form as: Eur J Obstet Gynecol Reprod Biol. 2009 May ; 144(Suppl 1): S159 S165. doi:10.1016/j.ejogrb.2009.02.021. Dynamics of Female Pelvic
NIH Public Access Author Manuscript Published in final edited form as: Eur J Obstet Gynecol Reprod Biol. 2009 May ; 144(Suppl 1): S159 S165. doi:10.1016/j.ejogrb.2009.02.021. Dynamics of Female Pelvic
NIH Public Access Author Manuscript Int Urogynecol J Pelvic Floor Dysfunct. Author manuscript; available in PMC 2010 January 1.
 NIH Public Access Author Manuscript Published in final edited form as: Int Urogynecol J Pelvic Floor Dysfunct. 2009 February ; 20(2): 171 175. doi:10.1007/ s00192-008-0738-0. The Cough Game : Are there
NIH Public Access Author Manuscript Published in final edited form as: Int Urogynecol J Pelvic Floor Dysfunct. 2009 February ; 20(2): 171 175. doi:10.1007/ s00192-008-0738-0. The Cough Game : Are there
Pelvic Floor Muscle Function, Pelvic Floor Dysfunction, and Diastasis Recti Abdominis: Prospective Cohort Study
 Neurourology and Urodynamics Pelvic Floor Muscle Function, Pelvic Floor Dysfunction, and Diastasis Recti Abdominis: Prospective Cohort Study Kari Bø, 1,2 * Gunvor Hilde, 2 Merete Kolberg Tennfjord, 1 Jorun
Neurourology and Urodynamics Pelvic Floor Muscle Function, Pelvic Floor Dysfunction, and Diastasis Recti Abdominis: Prospective Cohort Study Kari Bø, 1,2 * Gunvor Hilde, 2 Merete Kolberg Tennfjord, 1 Jorun
Effect of postpartum pelvic floor muscle training on vaginal symptoms and sexual dysfunction secondary analysis of a randomised trial
 DOI: 10.1111/1471-0528.13823 www.bjog.org Urogynaecology Effect of postpartum pelvic floor muscle training on vaginal symptoms and sexual dysfunction secondary analysis of a randomised trial M Kolberg
DOI: 10.1111/1471-0528.13823 www.bjog.org Urogynaecology Effect of postpartum pelvic floor muscle training on vaginal symptoms and sexual dysfunction secondary analysis of a randomised trial M Kolberg
Jennifer Kruger practice with POP? 17:20 17:40 How should PFM evaluation tool influence our
 W38: Digital palpation to imaging: how should pelvic-floor-muscle evaluation tools influence physiotherapy practice? Workshop Chair: Chantale Dumoulin, Canada 21 October 2014 14:00-18:00 Start End Topic
W38: Digital palpation to imaging: how should pelvic-floor-muscle evaluation tools influence physiotherapy practice? Workshop Chair: Chantale Dumoulin, Canada 21 October 2014 14:00-18:00 Start End Topic
Pregnancy related pelvic floor dysfunction- suggested teaching presentation for Midwives
 Pregnancy related pelvic floor dysfunction- suggested teaching presentation for Midwives 1 Aims of this self assessment competency To equip Midwives with the knowledge and skills to teach pelvic floor
Pregnancy related pelvic floor dysfunction- suggested teaching presentation for Midwives 1 Aims of this self assessment competency To equip Midwives with the knowledge and skills to teach pelvic floor
Transperineal ultrasound to assess the effect of tension-free vaginal tape position on flow rates
 Ultrasound Obstet Gynecol 2010; 36: 379 383 Published online 3 August 2010 in Wiley Online Library (wileyonlinelibrary.com). DOI: 10.1002/uog.7640 Transperineal ultrasound to assess the effect of tension-free
Ultrasound Obstet Gynecol 2010; 36: 379 383 Published online 3 August 2010 in Wiley Online Library (wileyonlinelibrary.com). DOI: 10.1002/uog.7640 Transperineal ultrasound to assess the effect of tension-free
Perineometer as a strength assessment & training tool for pelvic floor muscles in stress urinary incontinent elderly women
 Original article: Perineometer as a strength assessment & training tool for pelvic floor muscles in stress urinary incontinent elderly women Dr. Shwetanjali Gandhe, Dr. Shyam Ganvir 1MPT student, Dept.
Original article: Perineometer as a strength assessment & training tool for pelvic floor muscles in stress urinary incontinent elderly women Dr. Shwetanjali Gandhe, Dr. Shyam Ganvir 1MPT student, Dept.
Pelvic Floor and More.. Urinary Continence. Urinary Incontinence. Normal Bladder Function
 Pelvic Floor and More.. Jo Pitts Women s and Men s Health Physiotherapist Milton Keynes University Hospital Women s and Men s Health Physiotherapy at MKUH Pregnancy-related back and pelvic girdle pain
Pelvic Floor and More.. Jo Pitts Women s and Men s Health Physiotherapist Milton Keynes University Hospital Women s and Men s Health Physiotherapy at MKUH Pregnancy-related back and pelvic girdle pain
ijer.skums.ac.ir Risk factors of pelvic organ prolapse in Iranian women: a cross-sectional study
 International Journal of Epidemiologic Research, 2014; 1 (1): 29-34. ijer.skums.ac.ir Risk factors of pelvic organ prolapse in Iranian women: a cross-sectional study Ashraf Direkvand-Moghadam 1 ; Zeinab
International Journal of Epidemiologic Research, 2014; 1 (1): 29-34. ijer.skums.ac.ir Risk factors of pelvic organ prolapse in Iranian women: a cross-sectional study Ashraf Direkvand-Moghadam 1 ; Zeinab
Imaging of Pelvic Floor Weakness. Dr Susan Kouloyan-Ilic Radiologist Epworth Medical Imaging The Women s, Melbourne
 Imaging of Pelvic Floor Weakness Dr Susan Kouloyan-Ilic Radiologist Epworth Medical Imaging The Women s, Melbourne Outline Overview and Epidemiology Risk Factors, Causes and Results Review of Relevant
Imaging of Pelvic Floor Weakness Dr Susan Kouloyan-Ilic Radiologist Epworth Medical Imaging The Women s, Melbourne Outline Overview and Epidemiology Risk Factors, Causes and Results Review of Relevant
Pelvic floor muscle strength evaluation in different. body positions in nulliparous healthy women and its correlation with sexual activity.
 ORIGINAL Article Vol. 39 (6): 847-852, November - December, 2013 doi: 10.1590/S1677-5538.IBJU.2013.06.11 Pelvic floor muscle strength evaluation in different body positions in nulliparous healthy women
ORIGINAL Article Vol. 39 (6): 847-852, November - December, 2013 doi: 10.1590/S1677-5538.IBJU.2013.06.11 Pelvic floor muscle strength evaluation in different body positions in nulliparous healthy women
Vincent Letouzey, MD, PhD
 How to protect the perineum and prevent obstetric perineal trauma Standards of OASIS diagnosis: Primary (clinical) and Secondary (ultrasound) Vincent Letouzey, MD, PhD Obst/Gyne Dept Nîmes University Hospital
How to protect the perineum and prevent obstetric perineal trauma Standards of OASIS diagnosis: Primary (clinical) and Secondary (ultrasound) Vincent Letouzey, MD, PhD Obst/Gyne Dept Nîmes University Hospital
John Laughlin 4 th year Cardiff University Medical Student
 John Laughlin 4 th year Cardiff University Medical Student Prolapse/incontinence You need to know: Pelvic floor anatomy in relation to uterovaginal support and continence The classification of uterovaginal
John Laughlin 4 th year Cardiff University Medical Student Prolapse/incontinence You need to know: Pelvic floor anatomy in relation to uterovaginal support and continence The classification of uterovaginal
Applied Anatomy and Physiology of the Pelvic Floor. Dr David Tarver Consultant Radiologist, Poole
 Applied Anatomy and Physiology of the Pelvic Floor Dr David Tarver Consultant Radiologist, Poole Pelvic Floor 1. Sacrospinous Ligament 2. Levator Ani A Puborectalis B. Pubococcygeus C. Iliococcygeus 3.
Applied Anatomy and Physiology of the Pelvic Floor Dr David Tarver Consultant Radiologist, Poole Pelvic Floor 1. Sacrospinous Ligament 2. Levator Ani A Puborectalis B. Pubococcygeus C. Iliococcygeus 3.
Operative Vaginal Delivery and Pelvic Floor Trauma. Anna Padoa, MD Urogynecology Service Dept of Ob & Gyn Assaf Harofe Medical Center
 + Operative Vaginal Delivery and Pelvic Floor Trauma Anna Padoa, MD Urogynecology Service Dept of Ob & Gyn Assaf Harofe Medical Center + Vaginal birth and the pelvic floor Mechanisms of injury Damage to
+ Operative Vaginal Delivery and Pelvic Floor Trauma Anna Padoa, MD Urogynecology Service Dept of Ob & Gyn Assaf Harofe Medical Center + Vaginal birth and the pelvic floor Mechanisms of injury Damage to
Gynecology Dr. Sallama Lecture 3 Genital Prolapse
 Gynecology Dr. Sallama Lecture 3 Genital Prolapse Genital(utero-vaginal )prolapse is extremely common, with an estimated 11% of women undergoing at least one operation for this condition. Definition: A
Gynecology Dr. Sallama Lecture 3 Genital Prolapse Genital(utero-vaginal )prolapse is extremely common, with an estimated 11% of women undergoing at least one operation for this condition. Definition: A
The Urethral Motion Profile Before and After Suburethral Sling Placement
 The Urethral Motion Profile Before and After Suburethral Sling Placement Ka Lai Shek,* Varisara Chantarasorn and Hans Peter Dietz From the Nepean Clinical School, University of Sydney, Sydney, Australia
The Urethral Motion Profile Before and After Suburethral Sling Placement Ka Lai Shek,* Varisara Chantarasorn and Hans Peter Dietz From the Nepean Clinical School, University of Sydney, Sydney, Australia
Pelvic Floor Exercise. Brigi0e Fung Physiotherapist
 Pelvic Floor Exercise Brigi0e Fung Physiotherapist Treatment for urinary incontinence Pelvic floor muscle exercise (Kegel, 1948) Bladder retraining Behaviour modification Treatment for urinary incontinence
Pelvic Floor Exercise Brigi0e Fung Physiotherapist Treatment for urinary incontinence Pelvic floor muscle exercise (Kegel, 1948) Bladder retraining Behaviour modification Treatment for urinary incontinence
Long-term follow-up of sacrocolpopexy mesh implants at two time intervals at least 1 year apart using 4D transperineal ultrasound
 Ultrasound Obstet Gynecol 2017; 49: 398 403 Published online in Wiley Online Library (wileyonlinelibrary.com). DOI: 10.1002/uog.15891 Long-term follow-up of sacrocolpopexy mesh implants at two time intervals
Ultrasound Obstet Gynecol 2017; 49: 398 403 Published online in Wiley Online Library (wileyonlinelibrary.com). DOI: 10.1002/uog.15891 Long-term follow-up of sacrocolpopexy mesh implants at two time intervals
NEWER DIMENSIONS IN THE EVALUATION OF PELVIC PATHOLOGY BY TRANSPERINEAL ULTRASONOGRAPHY S. C. Sanjay 1, N. Krishnappa 2, Anil Kumar Shukla 3
 NEWER DIMENSIONS IN THE EVALUATION OF PELVIC PATHOLOGY BY TRANSPERINEAL ULTRASONOGRAPHY S. C. Sanjay 1, N. Krishnappa 2, Anil Kumar Shukla 3 HOW TO CITE THIS ARTICLE: S. C. Sanjay, N. Krishnappa, Anil
NEWER DIMENSIONS IN THE EVALUATION OF PELVIC PATHOLOGY BY TRANSPERINEAL ULTRASONOGRAPHY S. C. Sanjay 1, N. Krishnappa 2, Anil Kumar Shukla 3 HOW TO CITE THIS ARTICLE: S. C. Sanjay, N. Krishnappa, Anil
NOTES FROM GUTMAN LECTURE 10/26 Use this outline to study from. As you go through Gutman s lecture, fill in the topics.
 NOTES FROM GUTMAN LECTURE 10/26 Use this outline to study from. As you go through Gutman s lecture, fill in the topics. Anatomy above the arcuate line Skin Camper s fascia Scarpa s fascia External oblique
NOTES FROM GUTMAN LECTURE 10/26 Use this outline to study from. As you go through Gutman s lecture, fill in the topics. Anatomy above the arcuate line Skin Camper s fascia Scarpa s fascia External oblique
Is levator avulsion a predictor of cystocele recurrence following anterior vaginal mesh placement?
 Ultrasound Obstet Gynecol 2013; 42: 230 234 Published online in Wiley Online Library (wileyonlinelibrary.com). DOI: 10.1002/uog.12433 Is levator avulsion a predictor of cystocele recurrence following anterior
Ultrasound Obstet Gynecol 2013; 42: 230 234 Published online in Wiley Online Library (wileyonlinelibrary.com). DOI: 10.1002/uog.12433 Is levator avulsion a predictor of cystocele recurrence following anterior
Options for Vaginal Prolapse. What is prolapse? What is prolapse? Disclosures 10/23/2013. Michelle Y. Morrill, M.D. None
 Options for Vaginal Prolapse Disclosures None Michelle Y. Morrill, M.D. Director of Urogynecology Kaiser, San Francisco Assistant Professor, Volunteer Faculty Department of Ob/Gyn, UCSF What is prolapse?
Options for Vaginal Prolapse Disclosures None Michelle Y. Morrill, M.D. Director of Urogynecology Kaiser, San Francisco Assistant Professor, Volunteer Faculty Department of Ob/Gyn, UCSF What is prolapse?
The Egyptian Journal of Hospital Medicine (April 2018) Vol. 71 (3), Page
 Vol. 71 (3), Page") The Egyptian Journal of Hospital Medicine (April 2018) Vol. 71 (3), Page 2742-2750 Role of dynamic MRI in assessment of Pelvic Floor Dysfunction in Females Nada Ahmed Hussein, Naglaa Hussein Shebrya, Nermeen
The Egyptian Journal of Hospital Medicine (April 2018) Vol. 71 (3), Page 2742-2750 Role of dynamic MRI in assessment of Pelvic Floor Dysfunction in Females Nada Ahmed Hussein, Naglaa Hussein Shebrya, Nermeen
How can we measure bladder volumes in women with advanced pelvic organ prolapse?
 Ultrasound Obstet Gynecol 215; 46: 233 238 Published online in Wiley Online Library (wileyonlinelibrary.com). DOI: 1.12/uog.14678 How can we measure bladder volumes in women with advanced pelvic organ
Ultrasound Obstet Gynecol 215; 46: 233 238 Published online in Wiley Online Library (wileyonlinelibrary.com). DOI: 1.12/uog.14678 How can we measure bladder volumes in women with advanced pelvic organ
Over Active Pelvic Floor
 Over Active Pelvic Floor Maeve Whelan SMISCP Specialist Chartered Physiotherapist, Women s Health Background The concept of an overactive pelvic floor (OAPF) is relatively new in pelvic floor rehabilitation.
Over Active Pelvic Floor Maeve Whelan SMISCP Specialist Chartered Physiotherapist, Women s Health Background The concept of an overactive pelvic floor (OAPF) is relatively new in pelvic floor rehabilitation.
The diagnostic strength of the 24-h pad test for self-reported symptoms of urinary incontinence in pregnancy and after childbirth
 Int Urogynecol J (8) 19:525 53 DOI.7/s192-7-472-z ORIGINAL ARTICLE The diagnostic strength of the 24-h pad test for self-reported symptoms of urinary incontinence in pregnancy and after childbirth Jacobus
Int Urogynecol J (8) 19:525 53 DOI.7/s192-7-472-z ORIGINAL ARTICLE The diagnostic strength of the 24-h pad test for self-reported symptoms of urinary incontinence in pregnancy and after childbirth Jacobus
Iraqi JMS. Perineal Ultrasound for Evaluating Bladder Neck and Urethra in Stress Urinary Incontinence
 Iraqi JMS Published by Al-Nahrain College of Medicine ISSN 1681-6579 Email: iraqi_jms_alnahrain @yahoo.com http://www.colmed-nahrain.edu.iq/ Perineal Ultrasound for Evaluating Bladder Neck and Urethra
Iraqi JMS Published by Al-Nahrain College of Medicine ISSN 1681-6579 Email: iraqi_jms_alnahrain @yahoo.com http://www.colmed-nahrain.edu.iq/ Perineal Ultrasound for Evaluating Bladder Neck and Urethra
Original article J Bas Res Med Sci 2015; 2(2): The incidence of recurrent pelvic organ prolapse: A cross sectional study
: The incidence of recurrent pelvic organ prolapse: A cross sectional study") The incidence of recurrent pelvic organ prolapse: A cross sectional study Ashraf Direkvand-Moghadam 1, Ali Delpisheh 2, Azadeh Direkvand-Moghadam 3* 1. Psychosocial Injuries Research Center, Faculty of
The incidence of recurrent pelvic organ prolapse: A cross sectional study Ashraf Direkvand-Moghadam 1, Ali Delpisheh 2, Azadeh Direkvand-Moghadam 3* 1. Psychosocial Injuries Research Center, Faculty of
Moneli Golara Consultant Obstetrician and Gynaecologist Royal Free NHS Trust Barnet Hospital
 Moneli Golara Consultant Obstetrician and Gynaecologist Royal Free NHS Trust Barnet Hospital Pelvic Organ Prolapse (POP)- herniation of pelvic organs into vaginal walls Common Huge impact on daily activities
Moneli Golara Consultant Obstetrician and Gynaecologist Royal Free NHS Trust Barnet Hospital Pelvic Organ Prolapse (POP)- herniation of pelvic organs into vaginal walls Common Huge impact on daily activities