NATIONAL CLINICAL GUIDELINE INVESTIGATION AND MANAGEMENT OVARIAN CYSTS IN POSTMENOPAUSAL WOMEN
|
|
|
- Elmer Harrison
- 6 years ago
- Views:
Transcription

1 NATIONAL CLINICAL GUIDELINE INVESTIGATION AND MANAGEMENT OF OVARIAN CYSTS IN POSTMENOPAUSAL WOMEN Institute of Obstetricians and Gynaecologists, Royal College of Physicians of Ireland and the Clinical Strategy and Programmes Division, Health Service Executive Version 1.1 Publication date: Sept 2016 Guideline no: 39 Revision date: Sept 2019
2 Contents 1. Revision History Key Recommendations Purpose and Scope Background and Introduction Methodology Clinical Guideline on Ovarian Cysts in Postmenopausal Women References Implementation Strategy Qualifying Statement Appendices
3 1. Revision History Version No. Date Modified By Description /9/16 Vicky O Dwyer 2. Key Recommendations Women with a postmenopausal ovarian cyst should have a CA 125 level and transvaginal ultrasound performed. Women with a postmenopausal ovarian cyst should have a risk of malignancy index calculated to decide on management. Simple, unilateral ovarian cysts, <5 cm in diameter can be managed conservatively with monitoring of CA 125 level and ultrasound surveillance. Aspiration is not recommended for management of postmenopausal ovarian cysts. Laparoscopic oophorectomy is appropriate management for women with a low risk of malignancy index who do not fit the criteria for conservative management. This may be performed by a general gynaecologist. Consider performing salpingectomy or bilateral salpingo-oophorectomy for women undergoing laparoscopic management of postmenopausal ovarian cysts. Women with a moderate risk of malignancy index should undergo laparoscopic bilateral salpingo-oophorectomy. Women with a moderate or high risk of malignancy index should be managed by a gynaecological oncologist in a cancer centre. 3
4 3. Purpose and Scope The purpose of this guideline is to provide information for healthcare professionals on the investigation and management of ovarian cysts in postmenopausal women. The guideline is intended to be used by healthcare professionals working in the area of women s health, which includes gynaecologists, nurse sonographers, radiographers, radiologists and general practitioners. This guideline aids clinical judgement and does not replace it. In individual cases a gynaecologist may, after careful consideration, decide not to follow the guideline if it is deemed to be in the best interests of the woman. 4. Background and Introduction The cornerstone of management of postmenopausal ovarian cysts is identification and treatment of ovarian malignancy in the appropriate setting. Ovarian cancer is the fifth commonest malignancy in women. It usually occurs in women after the age of 50 years. Ovarian cancer often presents late, (stage 3-4), with a high mortality rate. Management of postmenopausal cysts includes surveillance and surgery, which may be performed by either a general gynaecologist or by a gynaecological oncologist in a cancer centre depending on the risk of malignancy. Risk factors for ovarian cancer include: prolonged exposure to Estrogen, for example, early menarche and late menopause polycystic ovarian syndrome nulliparity genetic mutations; BRCA 1, BRCA 2; Lynch syndrome personal history of breast cancer family history of breast or ovarian cancer obesity smoking 4
5 never having used the oral contraceptive pill fertility treatment hormone replacement therapy 5. Methodology This guideline was written after Medline, EMBASE and Cochrane Database of Systematic Reviews were searched using the terms menopause, ovarian cyst, ovarian mass and ovarian cancer. Searches were limited to humans and restricted to the titles of English language articles published between August 1992 and August Relevant meta-analyses, systematic reviews, intervention and observational studies were reviewed. The principal guideline developer was Dr Vicky O Dwyer. The guideline was reviewed by: Dr William Boyd (Gynaecologist, Rotunda), Dr Donal O Brien (Obstetrician, NMH), Dr Tom D Arcy (Obstetrician & Gynaecologist, CWIUH), Dr Michael Gannon (Obstetrician & Gynaecologist, Mullingar), Dr Matt Hewitt (Obstetrician & Gynaecologist, CUMH), Dr John Bermingham (Obstetrician, Waterford), Dr Katharine Astbury (Obstetrician & Gynaecologist, Galway), Dr Ulrich Bartels (Obstetrician & Gynaecologist, Mayo General). 5
6 6. Clinical Guideline on Ovarian Cysts in Postmenopausal Women 6.1 Investigation - CA125 and ultrasound To decide on the appropriate management of a postmenopausal ovarian cyst it is necessary to firstly estimate the risk that the cyst is malignant (Curtin 1994). This involves checking a serum CA125 and performing an ultrasound. CA125 is raised in over 80% of ovarian cancers and, if a cut-off of 30 u/ml is used, the test has a sensitivity of 81% and specificity of 75% (Jacobs et al, 1990). However, CA125 will only be raised in 50% of stage 1 ovarian cancers. Ultrasound is also well established, achieving a sensitivity of 89% and specificity of 73% when using a morphology index (DePriest et al, 1994). Ovarian cysts should normally be assessed using transvaginal ultrasound, as this appears to provide more detail and greater sensitivity than transabdominal ultrasound (Leibmann et al, 1988). Larger cysts may also need to be assessed by transabdominal ultrasound. The roles of magnetic resonance imaging (MRI), computed tomography (CT) and positron emission tomography (PET), in the diagnosis of ovarian cancer have yet to be clearly established (Kurtz et al, 1999; Grab et al 2000). These imaging modalities are generally used for staging once a cytological or histological diagnosis of cancer has been made. 6.2 Risk of malignancy index Risk of malignancy index should be used to decide which women are managed by a general gynaecologist, or by a gynaecological oncologist in a cancer centre. The best prognosis for women with ovarian cancer is obtained if a laparotomy and full staging procedure is carried out by a gynaecological oncologist. (Junor et al, 1999) RMI = U x M x CA125 6
7 U = 0 (for ultrasound score of 0); U = 1 (for ultrasound score of 1); U = 3 (for ultrasound score of 2 5). Ultrasound scans are scored one point for each of the following characteristics: multilocular cyst bilateral lesions evidence of solid areas evidence of metastases presence of ascites M = 1 for premenopausal women and 3 for postmenopausal women CA125 is serum CA125 measurement in u/ml 6.3 Management of ovarian cysts Management of postmenopausal ovarian cysts includes both surveillance and surgery Conservative management Simple, unilateral ovarian cysts, less than 5 cm in diameter, have a low risk of malignancy. In the presence of a normal serum CA125 level, they can be managed conservatively (Goldstein et al, 1989). The risk of malignancy for these type of cysts is less than 1%. Over 50% of these cysts will resolve spontaneously within three months, Thus, it is reasonable to manage these cysts conservatively, with a follow-up ultrasound scan in three months (Oveles et al, 2002). Persistent ovarian cysts should be reviewed at 3 months and then every 6 months thereafter on a selected basis. The American College of Obstetrics and Gynecology (ACOG) recommends annual transvaginal ultrasounds for 3 years and CA 125 for 5 years from diagnosis (Farghaly, 2014). This is due to the fact that postmenopausal simple unilocular ovarian cysts are common, have low malignant potential and are likely to remain stable or resolve without surgical intervention (Nardo et al, 2003). An increase in cyst size or rising CA 125 level should prompt the clinician to consider surgical management. 7
8 6.3.2 Surgical management Aspiration Cytological examination of ovarian cyst fluid is poor at distinguishing between benign and malignant tumours, with sensitivities in most studies of around 25%. Cyst rupture in the setting of unexpected malignancy results in upstaging and an adverse effect on survival rates. Aspiration, therefore, has no role in the management of ovarian cysts in postmenopausal women. Laparoscopic oophorectomy It is recommended that a risk of malignancy index should be used to select women for laparoscopic surgery. The laparoscopic management of benign adnexal masses is well established. However, when managing ovarian cysts in postmenopausal women, it should be remembered that the main reason for operating is to exclude an ovarian malignancy. If an ovarian malignancy is present then the appropriate management in the postmenopausal woman is to perform a laparotomy and a total abdominal hysterectomy, bilateral salpingooophorectomy, infracolic omentectomy, pelvic washings +/- appendicectomy. The laparoscopic approach should, therefore, be reserved for those women who are not eligible for conservative management but still have a relatively low risk of malignancy. In a postmenopausal woman, the appropriate laparoscopic treatment for an ovarian cyst, which is not suitable for conservative management, is oophorectomy, with removal of the ovary intact in a bag without cyst rupture into the peritoneal cavity. Robotic assisted laparoscopic management An alternative to traditional laparoscopic surgery is robotic assisted laparoscopic surgery. A recent American study reviewed these two methods of management of presumed benign ovarian masses and it found that the traditional laparoscopic approach was preferable to robotic surgery due to quicker operating time. There was no difference in complications or length of hospital stay between the two groups (Khlouly et al, 2014). Laparoscopic salpingectomy Recently it has been suggested that ovarian carcinomas, which are most commonly high-grade serous carcinomas, arise from high-grade intraepithelial 8
9 serous carcinomas in the fallopian tube which then spread to the ovary. This is in contrast to the original theory that all ovarian cancer develops from a surface lesion of the ovary which then undergoes metaplastic change and develops into a stromal cancer. (Kirman & Shih, 2010). Therefore, it has been suggested that prophylactic salpingectomy should be performed as a risk reducing procedure in addition to oophorectomy. In a Canadian study, salpingectomy for sterilisation or at the time of hysterectomy was found to be a safe procedure with no increase in operating time, blood transfusion or other peri/postoperative complications (McAlpine et al, 2014). Laparoscopic bilateral salpingo-oophrectomy The clinician should consider bilateral salpingo-oophorectomy (BSO) as an alternative to oophorectomy to reduce the chance of further benign or malignant ovarian cysts and need for further surgery. Laparoscopic BSO should also be performed in women with a moderate risk of malignancy index. These women should have their surgery performed by a gynaecological oncologist in a cancer centre. Women at intermediate risk undergoing laparoscopic oophorectomy should be counselled preoperatively that a full staging laparotomy will be required if evidence of malignancy is revealed. Surgery of suspected ovarian malignancy If an ovarian cancer is discovered at surgery or on histology, a subsequent full staging procedure is likely to be required. A full staging procedure should also be performed for women with a high risk of malignancy index. This includes a midline laparotomy, cytology (either ascites or pelvic washings), hysterectomy, bilateral salpingo-oophorectomy and infracolic omentectomy. Biopsies should be taken from suspicious areas and bilateral selective pelvic and para-aortic lymphadenectomy performed. Appendicectomy is performed in all suspected mucinous cystadenocarcinomas. 9
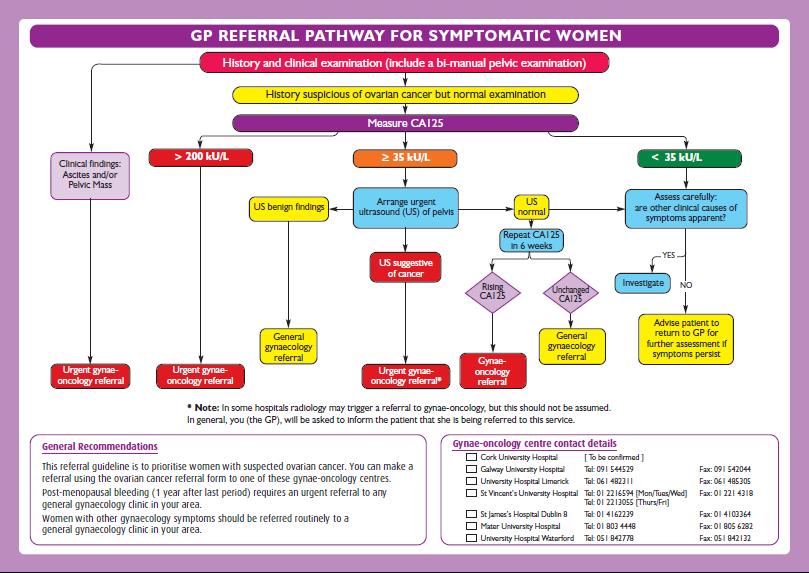
10 6.4 Management algorithm Low risk Management in a general gynaecology unit. Simple cysts less than 5 cm in diameter with a normal serum CA125 level may be managed conservatively. Conservative management should include ultrasound scans and serum CA125 measurement every three months for two years. If the cyst does not fit the above criteria or if the woman requests surgery then laparoscopic oophorectomy is acceptable. Moderate risk Management in a cancer centre by a gynaecological oncologist. Laparoscopic bilateral salpingo-oophorectomy is acceptable in selected cases. If a malignancy is discovered then a full staging procedure should be undertaken. High risk Management in a cancer centre by a gynaecological oncologist. GP referral pathway for symptomatic high risk women Appendix 1 Appendix 2 10
11 7. References Curtin JP (1994) Management of the adnexal mass. Gynecologic Oncology, 55(3 Pt 2): S42-6. DePriest PD, Varner E, Powell J, Fried A, Puls L, Higgins R, et al. (1994) The efficacy of a sonographic morphology index in identifying ovarian cancer: a multi-institutional investigation. Gynecologic Oncology, 55: El Khouly N I, Barr R L, Kim B B et al. (2014) Comparison of robotic-assisted and conventional laparoscopy in the management of adnexal masses. Journal of Minimally Invasive Gynecology, 21(6): Farghaly SA. (2014) Current diagnosis and management of ovarian cysts. Clinical and Experimental Obstetrics and Gynecology. 41(6):609-12, Goldstein SR, Subramanyam B, Snyder JR et al. (1989) The postmenopausal cystic adnexal mass: the potential role of ultrasound in conservative management. Obstetrics & Gynecology, Jan;73(1):8-10. Grab D, Flock F, Stohr I et al. (2000). Classification of asymptomatic adnexal masses by ultrasound, magnetic resonance imaging, and positron emission tomography. Gynecologic Oncology, 77: Jacobs I, Oram D, Fairbanks J et al. (1990) A risk of malignancy index incorporating CA125, ultrasound and menopausal status for the accurate preoperative diagnosis of ovarian cancer. BJOG, 97: Junor EJ, Hole DJ, McNulty L et al. (1999) Specialist gynaecologists and survival outcome in ovarian cancer: a Scottish national study of 1866 patients. BJOG, 106:
12 Kurman RJ, Shih LM. (2010) The Origin and Pathogenesis of Epithelial Ovarian Cancer- a Proposed Unifying Theory. The American Journal of Surgical Pathology, 21 (3): Kurtz AB, Tsimikas JV, Tempany CM et al. (1999) Diagnosis and staging of ovarian cancer: comparative values of Doppler and conventional US, CT, and MR imaging correlated with surgery and histopathologic analysis: report of the Radiology Diagnostic Oncology Group'. Radiology, 212: Leibman AJ, Kruse B, McSweeney MB. (1988) Transvaginal sonography: comparison with transabdominal sonography in the diagnosis of pelvic Masses. American Journal of Roentgenology, 151: McAlpine JN, Hanley MMM, Tone AA et al. (2014) Opportunistic salpingectomy: uptake, risks, and complications of a regional initiative for ovarian cancer prevention. American Journal of Obstetrics & Gynecology, 210 (5): 471 Nardo LG, Kroon ND, Reginald PW. (2003) Persistent Unilocular Ovarian Cysts in a General Population of Postmenopausal Women: Is There a Place for Expectant Management? Obstetrics & Gynecology, 102 (3): Oyelese Y, Kueck AS, Barter JF et al. (2002) Asymptomatic postmenopausal simple ovarian cyst. Obstetrical & Gynecological Survey, 57(12): Implementation Strategy Distribution of guideline to all members of the Institute and to all maternity units. Distribution to the Directorate of the Acute Hospitals for dissemination through line management in all acute hospitals. Implementation through HSE Obstetrics and Gynaecology Programme local implementation boards. Distribution to other interested parties and professional bodies. 12
13 9. Qualifying Statement These guidelines have been prepared to promote and facilitate standardisation and consistency of practice, using a multidisciplinary approach. Clinical material offered in this guideline does not replace or remove clinical judgement or the professional care and duty necessary for each pregnant woman. Clinical care carried out in accordance with this guideline should be provided within the context of locally available resources and expertise. This Guideline does not address all elements of standard practice and assumes that individual clinicians are responsible for: Discussing care with women in an environment that is appropriate and which enables respectful confidential discussion. Advising women of their choices and ensure informed consent is obtained. Meeting all legislative requirements and maintaining standards of professional conduct. Applying standard precautions and additional precautions, as necessary, when delivering care. Documenting all care in accordance with local and mandatory requirements. 13
14 10. Appendices

15 Appendix 1: Ovarian cancer GP referral for symptomatic women 15
16 16

17 Appendix 2: National Ovarian Cancer GP Referral for symptomatic women 17
Clinical guideline Published: 27 April 2011 nice.org.uk/guidance/cg122
 Ovarian cancer: recognition and initial management Clinical guideline Published: 27 April 2011 nice.org.uk/guidance/cg122 NICE 2018. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Ovarian cancer: recognition and initial management Clinical guideline Published: 27 April 2011 nice.org.uk/guidance/cg122 NICE 2018. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
LAPAROSCOPY and OVARIAN CANCER
 LAPAROSCOPY and OVARIAN CANCER J. DAUPLAT Clermont-Ferrand France UNIVERSITÉ D'AUVERGNE CLERMONT 1 1 - PROPHYLACTIC OOPHORECTOMY 2 - DIAGNOSIS 3 - EARLY STAGES : STAGING 4 - ADVANCED STAGES - ASSESSMENT
LAPAROSCOPY and OVARIAN CANCER J. DAUPLAT Clermont-Ferrand France UNIVERSITÉ D'AUVERGNE CLERMONT 1 1 - PROPHYLACTIC OOPHORECTOMY 2 - DIAGNOSIS 3 - EARLY STAGES : STAGING 4 - ADVANCED STAGES - ASSESSMENT
BRCA mutation carrier patient: How to manage?
 BRCA mutation carrier patient: How to manage? Clinical Case Presentation Katarzyna Sosińska-Mielcarek Department of Oncology and Radiotherapy University Clinical Center Gdansk, Poland esmo.org DISCLOSURE
BRCA mutation carrier patient: How to manage? Clinical Case Presentation Katarzyna Sosińska-Mielcarek Department of Oncology and Radiotherapy University Clinical Center Gdansk, Poland esmo.org DISCLOSURE
Ask the Experts Obstetrics & Gynecology
 1 Management of the Adnexal Mass James H. Liu, MD, and Kristine M. Zanotti, MD June 2011 Volume 117 Issue 6 Pages 1413 28 Click Here to Read the Full Article Questions written by: Rini Banerjee Ratan,
1 Management of the Adnexal Mass James H. Liu, MD, and Kristine M. Zanotti, MD June 2011 Volume 117 Issue 6 Pages 1413 28 Click Here to Read the Full Article Questions written by: Rini Banerjee Ratan,
Clinical Audit Data: 01 October 2015 to 30 September West of Scotland Cancer Network. Gynaecological Cancer Managed Clinical Network
 Gynaecological Cancer Managed Clinical Network Audit Report Ovarian Cancer Quality Performance Indicators Cervical Cancer Quality Performance Indicators Endometrial Cancer Quality Performance Indicators
Gynaecological Cancer Managed Clinical Network Audit Report Ovarian Cancer Quality Performance Indicators Cervical Cancer Quality Performance Indicators Endometrial Cancer Quality Performance Indicators
Chapter 2: Initial treatment for endometrial cancer (including histologic variant type)
") Chapter 2: Initial treatment for endometrial cancer (including histologic variant type) CQ01 Which surgical techniques for hysterectomy are recommended for patients considered to be stage I preoperatively?
Chapter 2: Initial treatment for endometrial cancer (including histologic variant type) CQ01 Which surgical techniques for hysterectomy are recommended for patients considered to be stage I preoperatively?
CA125 in the diagnosis of ovarian cancer: the art in medicine
 CA125 in the diagnosis of ovarian cancer: the art in medicine Dr Marcia Hall Consultant Medical Oncology Mount Vernon Cancer Centre Hillingdon Hospital Wexham Park Hospital Epidemiology Ovarian cancer
CA125 in the diagnosis of ovarian cancer: the art in medicine Dr Marcia Hall Consultant Medical Oncology Mount Vernon Cancer Centre Hillingdon Hospital Wexham Park Hospital Epidemiology Ovarian cancer
Ovarian cancer. Quick reference guide. Issue date: April The recognition and initial management of ovarian cancer
 Issue date: April 2011 Ovarian cancer The recognition and initial management of ovarian cancer Developed by the National Collaborating Centre for Cancer About this booklet This is aquick reference guide
Issue date: April 2011 Ovarian cancer The recognition and initial management of ovarian cancer Developed by the National Collaborating Centre for Cancer About this booklet This is aquick reference guide
Multimodal approach to predict ovarian malignancy prior to laparoscopy
 2017; 3(2): 149-153 ISSN Print: 2394-7500 ISSN Online: 2394-5869 Impact Factor: 5.2 IJAR 2017; 3(2): 149-153 www.allresearchjournal.com Received: 24-12-2016 Accepted: 25-01-2017 Dr. Juhi Bhatti Dr. Shriraj
2017; 3(2): 149-153 ISSN Print: 2394-7500 ISSN Online: 2394-5869 Impact Factor: 5.2 IJAR 2017; 3(2): 149-153 www.allresearchjournal.com Received: 24-12-2016 Accepted: 25-01-2017 Dr. Juhi Bhatti Dr. Shriraj
One of the commonest gynecological cancers,especially in white Americans.
 Gynaecology Dr. Rozhan Lecture 6 CARCINOMA OF THE ENDOMETRIUM One of the commonest gynecological cancers,especially in white Americans. It is a disease of postmenopausal women with a peak incidence in
Gynaecology Dr. Rozhan Lecture 6 CARCINOMA OF THE ENDOMETRIUM One of the commonest gynecological cancers,especially in white Americans. It is a disease of postmenopausal women with a peak incidence in
Hereditary Breast and Ovarian Cancer (HBOC) Information for individuals and families
 Information for individuals and families") Hereditary Breast and Ovarian Cancer (HBOC) Information for individuals and families What is Hereditary Breast and Ovarian Cancer (HBOC)? Hereditary Breast and Ovarian Cancer is a genetic condition which
Hereditary Breast and Ovarian Cancer (HBOC) Information for individuals and families What is Hereditary Breast and Ovarian Cancer (HBOC)? Hereditary Breast and Ovarian Cancer is a genetic condition which
Title of Guideline (must include the word Guideline (not protocol, policy, procedure etc)
") Title of Guideline (must include the word Guideline (not protocol, policy, procedure etc) Author: Contact Name and Job Title Directorate & Speciality Assessment, referral and initial management of ultrasound
Title of Guideline (must include the word Guideline (not protocol, policy, procedure etc) Author: Contact Name and Job Title Directorate & Speciality Assessment, referral and initial management of ultrasound
David Nunns on behalf of the Gynae Guidelines Group Date:
 Title of Guideline (must include the word Guideline (not protocol, policy, procedure etc) Borderline tumours of the ovary management and follow-up Author: Contact Name and Job Title Directorate & Speciality
Title of Guideline (must include the word Guideline (not protocol, policy, procedure etc) Borderline tumours of the ovary management and follow-up Author: Contact Name and Job Title Directorate & Speciality
SIGN 135 Management of epithelial ovarian cancer. A national clinical guideline June Evidence
 SIGN 135 Management of epithelial ovarian cancer A national clinical guideline June 2018 Evidence KEY TO EVIDENCE STATEMENTS AND GRADES OF RECOMMENDATIONS LEVELS OF EVIDENCE 1 ++ High quality meta-analyses,
SIGN 135 Management of epithelial ovarian cancer A national clinical guideline June 2018 Evidence KEY TO EVIDENCE STATEMENTS AND GRADES OF RECOMMENDATIONS LEVELS OF EVIDENCE 1 ++ High quality meta-analyses,
Gynaecological cancers. Mr Vivek Nama MD MRCOG Consultant Gynaecological Oncologist
 Gynaecological cancers Mr Vivek Nama MD MRCOG Consultant Gynaecological Oncologist Gynaecological cancers Why do we need 2 week wait? Early/timely diagnosis of cancer Possibly less invasive treatment and
Gynaecological cancers Mr Vivek Nama MD MRCOG Consultant Gynaecological Oncologist Gynaecological cancers Why do we need 2 week wait? Early/timely diagnosis of cancer Possibly less invasive treatment and
Borderline Ovarian Tumours. Andreas Obermair Brisbane
 Borderline Ovarian Tumours Andreas Obermair Brisbane Definition First described in 1929 Cellular features of malignancy Cellular atypia Mitotic activity No stromal invasion An entity per se??? (or precursor
Borderline Ovarian Tumours Andreas Obermair Brisbane Definition First described in 1929 Cellular features of malignancy Cellular atypia Mitotic activity No stromal invasion An entity per se??? (or precursor
Sarah Burton. Lead Gynae Oncology Nurse Specialist Cancer Care Cymru
 Sarah Burton Lead Gynae Oncology Nurse Specialist Cancer Care Cymru Gynaecological Cancers Cervical Cancers Risk factors Presentation Early sexual activity Multiple sexual partners Smoking Human Papiloma
Sarah Burton Lead Gynae Oncology Nurse Specialist Cancer Care Cymru Gynaecological Cancers Cervical Cancers Risk factors Presentation Early sexual activity Multiple sexual partners Smoking Human Papiloma
FAQ-Protocol 3. BRCA mutation carrier guidelines Frequently asked questions
 ULast updated: 09/02/2015 Protocol 3 BRCA mutation carrier guidelines Frequently asked questions UQ: How accurate are the remaining lifetime and 5 year breast cancer risks in the table? These figures are
ULast updated: 09/02/2015 Protocol 3 BRCA mutation carrier guidelines Frequently asked questions UQ: How accurate are the remaining lifetime and 5 year breast cancer risks in the table? These figures are
Surgery to Reduce the Risk of Ovarian Cancer. Information for Women at Increased Risk
 Surgery to Reduce the Risk of Ovarian Cancer Information for Women at Increased Risk Centre for Genetics Education NSW Health 2017 The Centre for Genetics Education NSW Health Level 5 2C Herbert St St
Surgery to Reduce the Risk of Ovarian Cancer Information for Women at Increased Risk Centre for Genetics Education NSW Health 2017 The Centre for Genetics Education NSW Health Level 5 2C Herbert St St
Menopause and Cancer risk; What to do overcome the risks? Fatih DURMUŞOĞLU,M.D
 Menopause and Cancer risk; What to do overcome the risks? Fatih DURMUŞOĞLU,M.D Menopause and Cancer How does menopause affect a woman s cancer risk? Ø Menopause does not cause cancer.but risk of developing
Menopause and Cancer risk; What to do overcome the risks? Fatih DURMUŞOĞLU,M.D Menopause and Cancer How does menopause affect a woman s cancer risk? Ø Menopause does not cause cancer.but risk of developing
Risk of Malignancy Index in the Preoperative Evaluation of Patients with Adnexal Masses among Women of Perimenopausal and Postmenopausal Age Group
 IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 17, Issue 9 Ver. 8 (September. 2018), PP 20-25 www.iosrjournals.org Risk of Malignancy Index in the Preoperative
IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 17, Issue 9 Ver. 8 (September. 2018), PP 20-25 www.iosrjournals.org Risk of Malignancy Index in the Preoperative
OVARIAN CARCINOMA Immune Therapy. Antibodies to CA-125 (Ovarex) Vaccine therapy
 Vaccine therapy") OVARIAN CARCINOMA Immune Therapy Antibodies to CA-125 (Ovarex) Vaccine therapy OVARIAN CARCINOMA Targeted Therapy Bevacizumab (Avastin): GOG- 218 Anti-VEGF, angiogenesis inhibitor TLK 286 (Telcyta): Glutathione
OVARIAN CARCINOMA Immune Therapy Antibodies to CA-125 (Ovarex) Vaccine therapy OVARIAN CARCINOMA Targeted Therapy Bevacizumab (Avastin): GOG- 218 Anti-VEGF, angiogenesis inhibitor TLK 286 (Telcyta): Glutathione
Tumori eredofamiliari: sorveglianza di donne ad alto rischio
 Tumori eredofamiliari: sorveglianza di donne ad alto rischio 14/01/2018 Dott Matteo Generali AUSL Modena Carpi U.O. Ostetricia e Ginecologia Screening for gynaecologic cancer in genetically predisposed
Tumori eredofamiliari: sorveglianza di donne ad alto rischio 14/01/2018 Dott Matteo Generali AUSL Modena Carpi U.O. Ostetricia e Ginecologia Screening for gynaecologic cancer in genetically predisposed
6 Week Course Agenda. Today s Agenda. Ovarian Cancer: Risk Factors. Winning the War 11/30/2016 on Women s Cancer Gynecologic Cancer Prevention
 6 Week Course Agenda Winning the War 11/30/2016 on Women s Cancer Gynecologic Cancer Prevention Lee-may Chen, MD Director, Division of Gynecologic Oncology Professor Department of Obstetrics, Gynecology
6 Week Course Agenda Winning the War 11/30/2016 on Women s Cancer Gynecologic Cancer Prevention Lee-may Chen, MD Director, Division of Gynecologic Oncology Professor Department of Obstetrics, Gynecology
Focus on... Ovarian cancer. HE4 & ROMA score
 Focus on... Ovarian cancer HE4 & ROMA score Ovarian cancer in the world* Accounting for around 4% of all cancers diagnosed in women The estimated World age-standardised incidence rate for the more developed
Focus on... Ovarian cancer HE4 & ROMA score Ovarian cancer in the world* Accounting for around 4% of all cancers diagnosed in women The estimated World age-standardised incidence rate for the more developed
Case Scenario 1. Pathology report Specimen from mediastinoscopy Final Diagnosis : Metastatic small cell carcinoma with residual lymphatic tissue
 Case Scenario 1 Oncology Consult: Patient is a 51-year-old male with history of T4N3 squamous cell carcinoma of tonsil status post concurrent chemoradiation finished in October two years ago. He was hospitalized
Case Scenario 1 Oncology Consult: Patient is a 51-year-old male with history of T4N3 squamous cell carcinoma of tonsil status post concurrent chemoradiation finished in October two years ago. He was hospitalized
General history. Basic Data : Age :62y/o Date of admitted: Married status : Married
 General history Basic Data : Age :62y/o Date of admitted:940510 Married status : Married General history Chief Complain : bilateral ovarian cyst incidentally being found out during pap smear. Present Illness
General history Basic Data : Age :62y/o Date of admitted:940510 Married status : Married General history Chief Complain : bilateral ovarian cyst incidentally being found out during pap smear. Present Illness
Index. B Bilateral salpingo-oophorectomy (BSO), 69
, 69") A Advanced stage endometrial cancer diagnosis, 92 lymph node metastasis, 92 multivariate analysis, 92 myometrial invasion, 92 prognostic factors FIGO stage, 94 histological grade, 94, 95 histologic cell
A Advanced stage endometrial cancer diagnosis, 92 lymph node metastasis, 92 multivariate analysis, 92 myometrial invasion, 92 prognostic factors FIGO stage, 94 histological grade, 94, 95 histologic cell
Audit Report Report of the 2012 Clinical Audit Data
 Gynaecological Cancer Managed Clinical Network Audit Report Report of the 2012 Clinical Audit Data Nadeem Siddiqui Consultant Gynaecological Oncologist MCN Clinical Lead Kevin Campbell MCN Manager Julie
Gynaecological Cancer Managed Clinical Network Audit Report Report of the 2012 Clinical Audit Data Nadeem Siddiqui Consultant Gynaecological Oncologist MCN Clinical Lead Kevin Campbell MCN Manager Julie
GYNECOLOGIC MALIGNANCIES: Ovarian Cancer
 GYNECOLOGIC MALIGNANCIES: Ovarian Cancer KRISTEN STARBUCK, MD ROSWELL PARK CANCER INSTITUTE DEPARTMENT OF SURGERY DIVISION OF GYNECOLOGIC ONCOLOGY APRIL 19 TH, 2018 Objectives Basic Cancer Statistics Discuss
GYNECOLOGIC MALIGNANCIES: Ovarian Cancer KRISTEN STARBUCK, MD ROSWELL PARK CANCER INSTITUTE DEPARTMENT OF SURGERY DIVISION OF GYNECOLOGIC ONCOLOGY APRIL 19 TH, 2018 Objectives Basic Cancer Statistics Discuss
Ovarian, Peritoneal, and Fallopian Tube Epithelial Cancer (OPT)
") Ovarian, Peritoneal, and Fallopian Tube Epithelial Cancer (OPT) ACOG District II 2 Learning Objectives At the end of this clinical presentation, obstetrician gynecologists and other women s health care
Ovarian, Peritoneal, and Fallopian Tube Epithelial Cancer (OPT) ACOG District II 2 Learning Objectives At the end of this clinical presentation, obstetrician gynecologists and other women s health care
EDUCATIONAL COMMENTARY CA 125. Learning Outcomes
 EDUCATIONAL COMMENTARY CA 125 Learning Outcomes Upon completion of this exercise, participants will be able to: discuss the use of CA 125 levels in monitoring patients undergoing treatment for ovarian
EDUCATIONAL COMMENTARY CA 125 Learning Outcomes Upon completion of this exercise, participants will be able to: discuss the use of CA 125 levels in monitoring patients undergoing treatment for ovarian
SCREENING FOR OVARIAN CANCER DR MACİT ARVAS
 SCREENING FOR OVARIAN CANCER DR MACİT ARVAS Ovarian cancer is the leading cause of death from gynecologic malignancy In 2008, ovarian cancer was the seventh common cancer in women worldwide There were
SCREENING FOR OVARIAN CANCER DR MACİT ARVAS Ovarian cancer is the leading cause of death from gynecologic malignancy In 2008, ovarian cancer was the seventh common cancer in women worldwide There were
Audit Report Report of the 2010 Clinical Audit Data
 Gynaecological Cancer Managed Clinical Network Audit Report Report of the Clinical Audit Data Nick Reed Consultant Clinical Oncologist MCN Clinical Lead (Joint) Nadeem Siddiqui Consultant Gynaecological
Gynaecological Cancer Managed Clinical Network Audit Report Report of the Clinical Audit Data Nick Reed Consultant Clinical Oncologist MCN Clinical Lead (Joint) Nadeem Siddiqui Consultant Gynaecological
MPH Quiz. 1. How many primaries are present based on this pathology report? 2. What rule is this based on?
 MPH Quiz Case 1 Surgical Pathology from hysterectomy performed July 11, 2007 Final Diagnosis: Uterus, resection: Endometrioid adenocarcinoma, Grade 1 involving most of endometrium, myometrial invasion
MPH Quiz Case 1 Surgical Pathology from hysterectomy performed July 11, 2007 Final Diagnosis: Uterus, resection: Endometrioid adenocarcinoma, Grade 1 involving most of endometrium, myometrial invasion
Triage of Ovarian Masses. Andreas Obermair Brisbane
 Triage of Ovarian Masses Andreas Obermair Brisbane Why Triage? In ovarian cancer, best outcomes for patients can be achieved when patients are treated in tertiary centres by a multidisciplinary team led
Triage of Ovarian Masses Andreas Obermair Brisbane Why Triage? In ovarian cancer, best outcomes for patients can be achieved when patients are treated in tertiary centres by a multidisciplinary team led
FDG-PET Findings in an Ovarian Endometrioma: A Case Report
 FDG-PET Findings in an Ovarian Endometrioma: A Case Report Jia-Huei Lin 1, Victor Chit-kheng Kok 2, Jian-Chiou Su 3 1 Department of Nuclear medicine, Kuang Tien General Hospital, Sha-Lu, Taichung, Taiwan
FDG-PET Findings in an Ovarian Endometrioma: A Case Report Jia-Huei Lin 1, Victor Chit-kheng Kok 2, Jian-Chiou Su 3 1 Department of Nuclear medicine, Kuang Tien General Hospital, Sha-Lu, Taichung, Taiwan
Article begins on next page
 Pseudopapillary Granulosa Cell Tumor: A Case of This Rare Subtype Rutgers University has made this article freely available. Please share how this access benefits you. Your story matters. [https://rucore.libraries.rutgers.edu/rutgers-lib/50622/story/]
Pseudopapillary Granulosa Cell Tumor: A Case of This Rare Subtype Rutgers University has made this article freely available. Please share how this access benefits you. Your story matters. [https://rucore.libraries.rutgers.edu/rutgers-lib/50622/story/]
4:00 into mp3 file Huang_342831_5_v1.mp3
 Support for Yale Cancer Answers comes from AstraZeneca, providing important treatment options for women living with advanced ovarian cancer. Learn more at astrazeneca-us.com. Welcome to Yale Cancer Answers
Support for Yale Cancer Answers comes from AstraZeneca, providing important treatment options for women living with advanced ovarian cancer. Learn more at astrazeneca-us.com. Welcome to Yale Cancer Answers
North of Scotland Cancer Network Clinical Management Guideline for Cancer of the Ovary
 North of Scotland Cancer Network Cancer of the Ovary Based on WOSCAN CMG with further extensive consultation within NOSCAN UNCONTROLLED WHEN PRINTED DOCUMENT CONTROL Prepared by NOSCAN Gynaecology Cancer
North of Scotland Cancer Network Cancer of the Ovary Based on WOSCAN CMG with further extensive consultation within NOSCAN UNCONTROLLED WHEN PRINTED DOCUMENT CONTROL Prepared by NOSCAN Gynaecology Cancer
Is It Time To Implement Ovarian Cancer Screening?
 Is It Time To Implement Ovarian Cancer Screening? Prof Dr Samet Topuz Istanbul Medıcal Faculty Department Of Obstetrics and Gynecology ESGO Prevention in Gynaecological Malignancies September 08 2016 Antalya
Is It Time To Implement Ovarian Cancer Screening? Prof Dr Samet Topuz Istanbul Medıcal Faculty Department Of Obstetrics and Gynecology ESGO Prevention in Gynaecological Malignancies September 08 2016 Antalya
Shared Care Pathway for Soft Tissue Sarcomas Presenting to Site Specialised MDTs. Gynaecological sarcomas Version 1
 Shared Care Pathway for Soft Tissue Sarcomas Presenting to Site Specialised MDTs Gynaecological sarcomas Version 1 Background This guidance is to provide direction for the management of patients with sarcomas
Shared Care Pathway for Soft Tissue Sarcomas Presenting to Site Specialised MDTs Gynaecological sarcomas Version 1 Background This guidance is to provide direction for the management of patients with sarcomas
Please complete prior to the webinar. HOSPITAL REGISTRY WEBINAR FEMALE REPRODUCTIVE SYSTEM EXERCISES CASE 1: FEMALE REPRODUCTIVE
 Please complete prior to the webinar. HOSPITAL REGISTRY WEBINAR FEMALE REPRODUCTIVE SYSTEM EXERCISES PHYSICAL EXAMINATION CASE 1: FEMALE REPRODUCTIVE 3/5 Patient presents through the emergency room with
Please complete prior to the webinar. HOSPITAL REGISTRY WEBINAR FEMALE REPRODUCTIVE SYSTEM EXERCISES PHYSICAL EXAMINATION CASE 1: FEMALE REPRODUCTIVE 3/5 Patient presents through the emergency room with
They are updated regularly as new NICE guidance is published. To view the latest version of this NICE Pathway see:
 bring together everything NICE says on a topic in an interactive flowchart. are interactive and designed to be used online. They are updated regularly as new NICE guidance is published. To view the latest
bring together everything NICE says on a topic in an interactive flowchart. are interactive and designed to be used online. They are updated regularly as new NICE guidance is published. To view the latest
Gynecologic Cancers are many diseases. Gynecologic Cancers in the Age of Precision Medicine Advances in Internal Medicine. Speaker Disclosure:
 Gynecologic Cancer Care in the Age of Precision Medicine Gynecologic Cancers in the Age of Precision Medicine Advances in Internal Medicine Lee-may Chen, MD Department of Obstetrics, Gynecology & Reproductive
Gynecologic Cancer Care in the Age of Precision Medicine Gynecologic Cancers in the Age of Precision Medicine Advances in Internal Medicine Lee-may Chen, MD Department of Obstetrics, Gynecology & Reproductive
Title of Guideline (must include the word Guideline not protocol, policy, procedure etc)
") Title of Guideline (must include the word Guideline not protocol, policy, procedure etc) Author: Contact Name and Job Title Directorate & Speciality Assessment, referral and initial management of ultrasound
Title of Guideline (must include the word Guideline not protocol, policy, procedure etc) Author: Contact Name and Job Title Directorate & Speciality Assessment, referral and initial management of ultrasound
Gynecologic Cancers are many diseases. Speaker Disclosure: Gynecologic Cancer Care in the Age of Precision Medicine. Controversies in Women s Health
 Gynecologic Cancer Care in the Age of Precision Medicine Gynecologic Cancers in the Age of Precision Medicine Controversies in Women s Health Lee-may Chen, MD Department of Obstetrics, Gynecology & Reproductive
Gynecologic Cancer Care in the Age of Precision Medicine Gynecologic Cancers in the Age of Precision Medicine Controversies in Women s Health Lee-may Chen, MD Department of Obstetrics, Gynecology & Reproductive
Screening and prevention of ovarian cancer
 Chapter 2 Screening and prevention of ovarian cancer Prevention of ovarian carcinoma Oral contraceptive pills Use of oral contraceptive pills (OCPs) has been associated with a significant reduction in
Chapter 2 Screening and prevention of ovarian cancer Prevention of ovarian carcinoma Oral contraceptive pills Use of oral contraceptive pills (OCPs) has been associated with a significant reduction in
CASE STUDY. Presented by: Jessica Pizzo. CFCC Sonography student Class of 2018
 CASE STUDY Presented by: Jessica Pizzo CFCC Sonography student Class of 2018 Case Presentation April 4, 2017 56 yr old woman presented to ED with lower abdominal pain & swelling, along with constipation.
CASE STUDY Presented by: Jessica Pizzo CFCC Sonography student Class of 2018 Case Presentation April 4, 2017 56 yr old woman presented to ED with lower abdominal pain & swelling, along with constipation.
3 Summary of clinical applications and limitations of measurements
 CA125 (serum) 1 Name and description of analyte 1.1 Name of analyte Cancer Antigen 125 (CA125) 1.2 Alternative names Mucin-16 1.3 NLMC code To follow 1.4 Description of analyte CA125 is an antigenic determinant
CA125 (serum) 1 Name and description of analyte 1.1 Name of analyte Cancer Antigen 125 (CA125) 1.2 Alternative names Mucin-16 1.3 NLMC code To follow 1.4 Description of analyte CA125 is an antigenic determinant
What is the gynecologist s role in the care of BRCA previvors?
 What is the gynecologist s role in the care of BRCA previvors? Here, your patient s options for surgery and your best options for her follow-up care and ongoing surveillance OBG Manag. Sept 2013;25(9):10-14.
What is the gynecologist s role in the care of BRCA previvors? Here, your patient s options for surgery and your best options for her follow-up care and ongoing surveillance OBG Manag. Sept 2013;25(9):10-14.
Consent Advice No. XX (Joint with BSGE) Peer Review Draft Spring Morcellation for Laparoscopic Myomectomy or Hysterectomy
 Peer Review Draft Spring Morcellation for Laparoscopic Myomectomy or Hysterectomy") 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 Consent Advice No. XX (Joint with BSGE) Peer Review Draft
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 Consent Advice No. XX (Joint with BSGE) Peer Review Draft
CLINICAL PRESENTATION AND RADIOLOGY QUIZ QUESTION
 Donald L. Renfrew, MD Radiology Associates of the Fox Valley, 333 N. Commercial Street, Suite 100, Neenah, WI 54956 2/12/2011 Radiology Quiz of the Week # 7 Page 1 CLINICAL PRESENTATION AND RADIOLOGY QUIZ
Donald L. Renfrew, MD Radiology Associates of the Fox Valley, 333 N. Commercial Street, Suite 100, Neenah, WI 54956 2/12/2011 Radiology Quiz of the Week # 7 Page 1 CLINICAL PRESENTATION AND RADIOLOGY QUIZ
Surgery to reduce the risk of ovarian cancer
 Surgery to reduce the risk of ovarian cancer INFORMATION FOR PATIENTS This leaflet is designed to answer questions you may have about surgery to reduce your risk of ovarian cancer. You may be considering
Surgery to reduce the risk of ovarian cancer INFORMATION FOR PATIENTS This leaflet is designed to answer questions you may have about surgery to reduce your risk of ovarian cancer. You may be considering
Ovarian cancer. The recognition and initial management of ovarian cancer. Issued: April NICE clinical guideline 122. guidance.nice.org.
 Ovarian cancer The recognition and initial management of ovarian cancer Issued: April 2011 NICE clinical guideline 122 guidance.nice.org.uk/cg122 NICE has accredited the process used by the Centre for
Ovarian cancer The recognition and initial management of ovarian cancer Issued: April 2011 NICE clinical guideline 122 guidance.nice.org.uk/cg122 NICE has accredited the process used by the Centre for
Squamous cell carcinoma arising in a dermoid cyst of the ovary: a case series
 DOI: 10.1111/j.1471-0528.2007.01478.x www.blackwellpublishing.com/bjog Gynaecological oncology Squamous cell carcinoma arising in a dermoid cyst of the ovary: a case series JL Hurwitz, a A Fenton, a WG
DOI: 10.1111/j.1471-0528.2007.01478.x www.blackwellpublishing.com/bjog Gynaecological oncology Squamous cell carcinoma arising in a dermoid cyst of the ovary: a case series JL Hurwitz, a A Fenton, a WG
OVARIAN CANCER Updates in Screening, Early Detection and Prevention
 UW MEDICINE SUSAN PATRICIA TECK MEMORIAL LECTURE October 2017 OVARIAN CANCER Updates in Screening, Early Detection and Prevention BARBARA GOFF, MD Seattle Gynecologic Society March 2018 OVARIAN CANCER
UW MEDICINE SUSAN PATRICIA TECK MEMORIAL LECTURE October 2017 OVARIAN CANCER Updates in Screening, Early Detection and Prevention BARBARA GOFF, MD Seattle Gynecologic Society March 2018 OVARIAN CANCER
Ovarian Cancer Includes Epithelial, Fallopian Tube, Primary Peritoneal Cancer, and Ovarian Germ Cell Tumors
 Ovarian Cancer Includes Epithelial, Fallopian Tube, Primary Peritoneal Cancer, and Ovarian Germ Cell Tumors Overview Ovarian epithelial cancer, fallopian tube cancer, and primary peritoneal cancer are
Ovarian Cancer Includes Epithelial, Fallopian Tube, Primary Peritoneal Cancer, and Ovarian Germ Cell Tumors Overview Ovarian epithelial cancer, fallopian tube cancer, and primary peritoneal cancer are
Endometriosis Information Leaflet
 Endometriosis Information Leaflet What is Endometriosis? Endometriosis is a condition where tissue similar to the lining of the womb (endometrium) is found outside the womb. About 1 out of 10 women of
Endometriosis Information Leaflet What is Endometriosis? Endometriosis is a condition where tissue similar to the lining of the womb (endometrium) is found outside the womb. About 1 out of 10 women of
Epithelial Ovarian Cancer
 Epithelial Ovarian Cancer GYNE/ONC Practice Guideline Dr. Alex Hammond Dr. Ian Kerr Dr. Akira Sugimoto Dr. Stephen Welch Kay Faroni Christine Gawlik Kerri Thornton Approval Date: This guideline is a statement
Epithelial Ovarian Cancer GYNE/ONC Practice Guideline Dr. Alex Hammond Dr. Ian Kerr Dr. Akira Sugimoto Dr. Stephen Welch Kay Faroni Christine Gawlik Kerri Thornton Approval Date: This guideline is a statement
CAN TV U/S REDUCE THE
 CAN TV U/S REDUCE THE NEED FOR SURGERY IN GYNECOLOGY? Steven R. Goldstein, M.D. Professor of Obstetrics & Gynecology New York University it School of fmedicine i Director of Gynecologic Ultrasound Co-Director
CAN TV U/S REDUCE THE NEED FOR SURGERY IN GYNECOLOGY? Steven R. Goldstein, M.D. Professor of Obstetrics & Gynecology New York University it School of fmedicine i Director of Gynecologic Ultrasound Co-Director
Clinical guideline Published: 25 June 2013 nice.org.uk/guidance/cg164
 Familial breast cancer: classification, care and managing breast cancer and related risks in people with a family history of breast cancer Clinical guideline Published: 25 June 2013 nice.org.uk/guidance/cg164
Familial breast cancer: classification, care and managing breast cancer and related risks in people with a family history of breast cancer Clinical guideline Published: 25 June 2013 nice.org.uk/guidance/cg164
Clinical guideline Published: 27 April 2011 nice.org.uk/guidance/cg122
 Ovarian cancer: recognition and initial management Clinical guideline Published: 27 April 2011 nice.org.uk/guidance/cg122 NICE 2011. All rights reserved. Your responsibility The recommendations in this
Ovarian cancer: recognition and initial management Clinical guideline Published: 27 April 2011 nice.org.uk/guidance/cg122 NICE 2011. All rights reserved. Your responsibility The recommendations in this
بسم هللا الرحمن الرحيم. Prof soha Talaat
 بسم هللا الرحمن الرحيم Ovarian tumors The leading indication for gynecologic surgery. Preoperative characterization of complex solid and cystic adnexal masses is crucial for informing patients about possible
بسم هللا الرحمن الرحيم Ovarian tumors The leading indication for gynecologic surgery. Preoperative characterization of complex solid and cystic adnexal masses is crucial for informing patients about possible
Epithelial ovarian cancer
 Scottish Intercollegiate Guidelines Net work 75 Epithelial ovarian cancer A na tion al clinical guideline 1 Introduction 1 2 Screening and the role of prophylactic oophorectomy 3 3 Diagnosis 6 4 Surgical
Scottish Intercollegiate Guidelines Net work 75 Epithelial ovarian cancer A na tion al clinical guideline 1 Introduction 1 2 Screening and the role of prophylactic oophorectomy 3 3 Diagnosis 6 4 Surgical
Partners: Introductions: Dr. Carolyn Johnston Deanna Cosens & Ann Garvin. Ovarian Cancer and Primary Care July 16, :00 9:00am EST 7/16/2014
 Welcome To The Webinar Technical Support Ovarian Cancer and Primary Care July 16, 2014 8:00 9:00am EST In order to hear the presentation please call 1 (626) 544-0058, access code 167-314-644, followed
Welcome To The Webinar Technical Support Ovarian Cancer and Primary Care July 16, 2014 8:00 9:00am EST In order to hear the presentation please call 1 (626) 544-0058, access code 167-314-644, followed
What You Need to Know About Ovarian Cancer
 What You Need to Know About Ovarian Cancer About Us The Rhode Island Ovarian Cancer Alliance (RIOCA) was formed in honor and memory of Jessica Morris. Jessica was diagnosed with Stage IIIC Ovarian Cancer
What You Need to Know About Ovarian Cancer About Us The Rhode Island Ovarian Cancer Alliance (RIOCA) was formed in honor and memory of Jessica Morris. Jessica was diagnosed with Stage IIIC Ovarian Cancer
X-Plain Ovarian Cancer Reference Summary
 X-Plain Ovarian Cancer Reference Summary Introduction Ovarian cancer is fairly rare. Ovarian cancer usually occurs in women who are over 50 years old and it may sometimes be hereditary. This reference
X-Plain Ovarian Cancer Reference Summary Introduction Ovarian cancer is fairly rare. Ovarian cancer usually occurs in women who are over 50 years old and it may sometimes be hereditary. This reference
American Journal of Oral Medicine and Radiology
 American Journal of Oral Medicine and Radiology e - ISSN - XXXX-XXXX ISSN - 2394-7721 Journal homepage: www.mcmed.us/journal/ajomr ULTRASONOGRAPHIC EVALUATION OF ADNEXAL MASSES Nageswar Rao* Professor,
American Journal of Oral Medicine and Radiology e - ISSN - XXXX-XXXX ISSN - 2394-7721 Journal homepage: www.mcmed.us/journal/ajomr ULTRASONOGRAPHIC EVALUATION OF ADNEXAL MASSES Nageswar Rao* Professor,
Ovarian Cancer Quality Performance Indicators
 Ovarian Cancer Quality Performance Indicators Patients diagnosed between October 2013 and September 2016 Publication date 20 February 2018 An Official Statistics publication for Scotland This is an Official
Ovarian Cancer Quality Performance Indicators Patients diagnosed between October 2013 and September 2016 Publication date 20 February 2018 An Official Statistics publication for Scotland This is an Official
Inherited Ovarian Cancer Diagnosis and Prevention
 Inherited Ovarian Cancer Diagnosis and Prevention Dr. Jacob Korach - Deputy director Gynecologic Oncology (past chair - Israeli Society of Gynecologic Oncology) Prof. Eitan Friedman - Head, Oncogenetics
Inherited Ovarian Cancer Diagnosis and Prevention Dr. Jacob Korach - Deputy director Gynecologic Oncology (past chair - Israeli Society of Gynecologic Oncology) Prof. Eitan Friedman - Head, Oncogenetics
Case 1. Gynaecology Case Presentation. Objectives. Disclosures 22/10/ year old female Clinical history: Assess right ovarian cyst
 Gynaecology Case Presentation Organ Imaging 2016 University of Toronto Sarah Johnson 39 year old female Clinical history: Assess right ovarian cyst Clinically diagnosed endometriosis Started fertility
Gynaecology Case Presentation Organ Imaging 2016 University of Toronto Sarah Johnson 39 year old female Clinical history: Assess right ovarian cyst Clinically diagnosed endometriosis Started fertility
FDG-PET value in deep endometriosis
 Gynecol Surg (2011) 8:305 309 DOI 10.1007/s10397-010-0652-6 ORIGINAL ARTICLE FDG-PET value in deep endometriosis A. Setubal & S. Maia & C. Lowenthal & Z. Sidiropoulou Received: 3 December 2010 / Accepted:
Gynecol Surg (2011) 8:305 309 DOI 10.1007/s10397-010-0652-6 ORIGINAL ARTICLE FDG-PET value in deep endometriosis A. Setubal & S. Maia & C. Lowenthal & Z. Sidiropoulou Received: 3 December 2010 / Accepted:
Policy #: 259 Latest Review Date: November 2009
 Name of Policy: Prophylactic Oophorectomy Policy #: 259 Latest Review Date: November 2009 Category: Surgery Policy Grade: Active Policy but no longer scheduled for regular literature reviews and updates.
Name of Policy: Prophylactic Oophorectomy Policy #: 259 Latest Review Date: November 2009 Category: Surgery Policy Grade: Active Policy but no longer scheduled for regular literature reviews and updates.
Gynaecological Oncology Cases
 Gynaecological Oncology Cases 1. Tamoxifen and the endometrium 2. Cancer and the older woman Dr Julie M Lamont Consultant Gynaecological Oncologist Epworth Freemasons Hospital 21 st April 2015 Mrs FS 66
Gynaecological Oncology Cases 1. Tamoxifen and the endometrium 2. Cancer and the older woman Dr Julie M Lamont Consultant Gynaecological Oncologist Epworth Freemasons Hospital 21 st April 2015 Mrs FS 66
Coversheet for Network Site Specific Group Agreed Documentation
 Coversheet for Network Site Specific Group Agreed Documentation This sheet is to accompany all documentation agreed by Pan Birmingham Cancer Network Site Specific Groups. This will assist the Network Governance
Coversheet for Network Site Specific Group Agreed Documentation This sheet is to accompany all documentation agreed by Pan Birmingham Cancer Network Site Specific Groups. This will assist the Network Governance
Screening Postmenopausal Women for Ovarian Cancer
 Evidence Summary Report 4-6a IN REVIEW A Quality Initiative of the Program in Evidence-based Care (PEBC), Cancer Care Ontario (CCO) Screening Postmenopausal Women for Ovarian Cancer M. Fung Kee Fung, P.
Evidence Summary Report 4-6a IN REVIEW A Quality Initiative of the Program in Evidence-based Care (PEBC), Cancer Care Ontario (CCO) Screening Postmenopausal Women for Ovarian Cancer M. Fung Kee Fung, P.
Ovarian Cancer Causes, Risk Factors, and Prevention
 Ovarian Cancer Causes, Risk Factors, and Prevention Risk Factors A risk factor is anything that affects your chance of getting a disease such as cancer. Learn more about the risk factors for ovarian cancer.
Ovarian Cancer Causes, Risk Factors, and Prevention Risk Factors A risk factor is anything that affects your chance of getting a disease such as cancer. Learn more about the risk factors for ovarian cancer.
OVARIAN CANCER STATISTICS
 bioprognos OncoOVARIAN Dx Non-invasive blood test useful to suggest a possible diagnosis in patients with suspected malignancy in the ovarians, reduce inappropriate diagnostic tests, days of hospitalization,
bioprognos OncoOVARIAN Dx Non-invasive blood test useful to suggest a possible diagnosis in patients with suspected malignancy in the ovarians, reduce inappropriate diagnostic tests, days of hospitalization,
Ovarian Cancer Quality Performance Indicators (QPI) Comparative Report
 Comparative Report") SOUTH EAST SCOTLAND CANCER NETWORK (SCAN) PROSPECTIVE CANCER AUDIT Ovarian Cancer Quality Performance Indicators (QPI) Comparative Report Dr Cameron Martin, SCAN Lead Ovarian Cancer Clinician Dr Scott
SOUTH EAST SCOTLAND CANCER NETWORK (SCAN) PROSPECTIVE CANCER AUDIT Ovarian Cancer Quality Performance Indicators (QPI) Comparative Report Dr Cameron Martin, SCAN Lead Ovarian Cancer Clinician Dr Scott
Ovarian cancer the need for change in service delivery in Northern Ireland
 The Ulster Medical Ovarian Journal, cancer Volume the need 72, for No. change 2, pp. in 93-97, service November delivery in 2003. Northern Ireland 93 Ovarian cancer the need for change in service delivery
The Ulster Medical Ovarian Journal, cancer Volume the need 72, for No. change 2, pp. in 93-97, service November delivery in 2003. Northern Ireland 93 Ovarian cancer the need for change in service delivery
patient education Fact Sheet PFS007: BRCA1 and BRCA2 Mutations MARCH 2015
 patient education Fact Sheet PFS007: BRCA1 and BRCA2 Mutations MARCH 2015 BRCA1 and BRCA2 Mutations Cancer is a complex disease thought to be caused by several different factors. A few types of cancer
patient education Fact Sheet PFS007: BRCA1 and BRCA2 Mutations MARCH 2015 BRCA1 and BRCA2 Mutations Cancer is a complex disease thought to be caused by several different factors. A few types of cancer
Unexpected Gynecologic Findings at Laparotomy. Susan A. Davidson, MD University of Colorado, Denver School of Medicine
 Unexpected Gynecologic Findings at Laparotomy Susan A. Davidson, MD University of Colorado, Denver School of Medicine Adnexal Mass: Gyn Etiologies Uterine Leiomyomas Pregnancy Malignancy Tubal Pregnancy
Unexpected Gynecologic Findings at Laparotomy Susan A. Davidson, MD University of Colorado, Denver School of Medicine Adnexal Mass: Gyn Etiologies Uterine Leiomyomas Pregnancy Malignancy Tubal Pregnancy
Jill Stopfer, MS, CGC Abramson Cancer Center University of Pennsylvania
 Jill Stopfer, MS, CGC Abramson Cancer Center University of Pennsylvania Aging Family history Early menarche Late menopause Nulliparity Estrogen / Progesterone use after menopause More than two alcoholic
Jill Stopfer, MS, CGC Abramson Cancer Center University of Pennsylvania Aging Family history Early menarche Late menopause Nulliparity Estrogen / Progesterone use after menopause More than two alcoholic
North of Scotland Cancer Network Clinical Management Guideline for Endometrial Cancer
 THIS DOCUMENT North of Scotland Cancer Network Clinical Management Guideline for Endometrial Cancer Based on WOSCAN CMG with further extensive consultation within NOSCAN UNCONTROLLED WHEN PRINTED DOCUMENT
THIS DOCUMENT North of Scotland Cancer Network Clinical Management Guideline for Endometrial Cancer Based on WOSCAN CMG with further extensive consultation within NOSCAN UNCONTROLLED WHEN PRINTED DOCUMENT
New York Science Journal 2017;10(3) Mahmoud Sayed El Edessy, Hesham Saleh mohammed, and Abd Alsttar Alwaziry
 Mahmoud Sayed El Edessy, Hesham Saleh mohammed, and Abd Alsttar Alwaziry") Edessy ovarian cancer score (EOCS) in prediction of malignant ovarian masses Mahmoud Sayed El Edessy, Hesham Saleh mohammed, and Abd Alsttar Alwaziry Obstetrics and Gynecology Department, Al Azhar University,
Edessy ovarian cancer score (EOCS) in prediction of malignant ovarian masses Mahmoud Sayed El Edessy, Hesham Saleh mohammed, and Abd Alsttar Alwaziry Obstetrics and Gynecology Department, Al Azhar University,
Endometrial Cancer. Incidence. Types 3/25/2019
 Endometrial Cancer J. Anthony Rakowski DO, FACOOG MSU SCS Board Review Coarse Incidence 53,630 new cases yearly 8,590 deaths yearly 4 th most common malignancy in women worldwide Most common GYN malignancy
Endometrial Cancer J. Anthony Rakowski DO, FACOOG MSU SCS Board Review Coarse Incidence 53,630 new cases yearly 8,590 deaths yearly 4 th most common malignancy in women worldwide Most common GYN malignancy
Oophorectomy or salpingectomy which makes more sense?
 Oophorectomy or salpingectomy which makes more sense? During hysterectomy for benign indications, many surgeons routinely remove the ovaries to prevent cancer. Here s what we know about this practice.
Oophorectomy or salpingectomy which makes more sense? During hysterectomy for benign indications, many surgeons routinely remove the ovaries to prevent cancer. Here s what we know about this practice.
--- or not, and do we need to come up with newer strategies for ovarian cancer screening.
 My name is Dr. Karen Lu and I am a Professor of Gynecologic Oncology at the University of Texas MD Anderson Cancer Center. I also serve as Co-Medical Director for Clinical Cancer Genetics. I m going to
My name is Dr. Karen Lu and I am a Professor of Gynecologic Oncology at the University of Texas MD Anderson Cancer Center. I also serve as Co-Medical Director for Clinical Cancer Genetics. I m going to
A new scoring model for characterization of adnexal masses based on two-dimensional gray-scale and colour Doppler sonographic features
 FVV in ObGyn, 2014, 6 (2): 68-74 Original paper A new scoring model for characterization of adnexal masses based on two-dimensional gray-scale and colour Doppler sonographic features Ahmed M. Abbas, Kamal
FVV in ObGyn, 2014, 6 (2): 68-74 Original paper A new scoring model for characterization of adnexal masses based on two-dimensional gray-scale and colour Doppler sonographic features Ahmed M. Abbas, Kamal
This information explains the advice about familial breast cancer (breast cancer in the family) that is set out in NICE guideline CG164.
 that is set out in NICE guideline CG164.") Familial breast cancer (breast cancer in the family) Information for the public Published: 1 June 2013 nice.org.uk About this information NICE guidelines provide advice on the care and support that should
Familial breast cancer (breast cancer in the family) Information for the public Published: 1 June 2013 nice.org.uk About this information NICE guidelines provide advice on the care and support that should
Cancer arising from Endometriosis and Its Clinical implications
 Cancer arising from Endometriosis and Its Clinical implications 1) Nezhat F, Cohen C, Rahaman J, Gretz H, Cole P, Kalir T. Comparative immunohistochemical studies of bcl-2 and p53 proteins in benign
Cancer arising from Endometriosis and Its Clinical implications 1) Nezhat F, Cohen C, Rahaman J, Gretz H, Cole P, Kalir T. Comparative immunohistochemical studies of bcl-2 and p53 proteins in benign
Metastatic Colonic Adenocarcinoma Simulating Primary Ovarian Neoplasm in Transvaginal Doppler Sonography
 J Clin Ultrasound 22:121-125, February 1994 0 1994 by John Wiley & Sons, Inc. CCC 0091-2751/94/020121-05 Case Report Metastatic Colonic Adenocarcinoma Simulating Primary Ovarian Neoplasm in Transvaginal
J Clin Ultrasound 22:121-125, February 1994 0 1994 by John Wiley & Sons, Inc. CCC 0091-2751/94/020121-05 Case Report Metastatic Colonic Adenocarcinoma Simulating Primary Ovarian Neoplasm in Transvaginal
Diagnostics guidance Published: 15 November 2017 nice.org.uk/guidance/dg31
 Tests in secondary care to identify people at high risk of ovarian cancer Diagnostics guidance Published: 15 November 2017 nice.org.uk/guidance/dg31 NICE 2017. All rights reserved. Subject to Notice of
Tests in secondary care to identify people at high risk of ovarian cancer Diagnostics guidance Published: 15 November 2017 nice.org.uk/guidance/dg31 NICE 2017. All rights reserved. Subject to Notice of
Ovarian Tumors. Andrea Hayes-Jordan MD FACS, FAAP Section Chief, Pediatric Surgery/Surgical Onc. UT MD Anderson Cancer Center
 Ovarian Tumors Andrea Hayes-Jordan MD FACS, FAAP Section Chief, Pediatric Surgery/Surgical Onc. UT MD Anderson Cancer Center Case 13yo female with abdominal pain Ultrasound shows huge ovarian mass Surgeon
Ovarian Tumors Andrea Hayes-Jordan MD FACS, FAAP Section Chief, Pediatric Surgery/Surgical Onc. UT MD Anderson Cancer Center Case 13yo female with abdominal pain Ultrasound shows huge ovarian mass Surgeon
Gestione dei tumori borderline iniziali e avanzati nelle donne in età fertile
 Gestione dei tumori borderline iniziali e avanzati nelle donne in età fertile Pierandrea De Iaco pierandrea.deiaco@aosp.bo.it SSD ONCOLOGIA GINECOLOGICA AOU SANT ORSOLA-MALPIGHI BOLOGNA Borderline ovarian
Gestione dei tumori borderline iniziali e avanzati nelle donne in età fertile Pierandrea De Iaco pierandrea.deiaco@aosp.bo.it SSD ONCOLOGIA GINECOLOGICA AOU SANT ORSOLA-MALPIGHI BOLOGNA Borderline ovarian
Guideline for the Assessment, Management and Referral of Patients with Suspected Ovarian Cancer
 Guideline for the Assessment, Management and Referral of Patients with Suspected Ovarian Cancer Version History Version Date Summary of Change/Process 2.0 February Endorsed by the Governance Committee
Guideline for the Assessment, Management and Referral of Patients with Suspected Ovarian Cancer Version History Version Date Summary of Change/Process 2.0 February Endorsed by the Governance Committee
Pathology of Ovarian Tumours. Dr. Jyothi Ranganathan MD ( Path) AFMC Pune PDCC (Cytopathology) PGI Chandigarh
 AFMC Pune PDCC (Cytopathology) PGI Chandigarh") Pathology of Ovarian Tumours Dr. Jyothi Ranganathan MD ( Path) AFMC Pune PDCC (Cytopathology) PGI Chandigarh Outline Incidence Risk factors Classification Pathology of tumours Tumour markers Prevention
Pathology of Ovarian Tumours Dr. Jyothi Ranganathan MD ( Path) AFMC Pune PDCC (Cytopathology) PGI Chandigarh Outline Incidence Risk factors Classification Pathology of tumours Tumour markers Prevention
IOTA and Models for Screening for Ovarian Cancer
 IOTA and Models for Screening for Ovarian Cancer Hennie Botha MARCH 2017 T H IG PY R O C F O SP EA KE R Silent Killer to Whispering Disease Listening to your body.. new, persistent, and increases in severity
IOTA and Models for Screening for Ovarian Cancer Hennie Botha MARCH 2017 T H IG PY R O C F O SP EA KE R Silent Killer to Whispering Disease Listening to your body.. new, persistent, and increases in severity
SURGICAL MANAGEMENT OF EPITHELIAL OVARIAN CANCER PARSGO, MARRAKECH 2018
 SURGICAL MANAGEMENT OF EPITHELIAL OVARIAN CANCER SURGERY SERVICE FOR GYNECOLOGIC AND BREAST C ANCER CENTER MOHAMED VI FOR C ANCER TREATMENT CASABLANCA, MOROCCO PARSGO, MARRAKECH 2018 5th female cancer
SURGICAL MANAGEMENT OF EPITHELIAL OVARIAN CANCER SURGERY SERVICE FOR GYNECOLOGIC AND BREAST C ANCER CENTER MOHAMED VI FOR C ANCER TREATMENT CASABLANCA, MOROCCO PARSGO, MARRAKECH 2018 5th female cancer