Sexual Dysfunction Caused by Cancer Treatments Issues in Men. Dr Christopher Love
|
|
|
- Alice Daniels
- 5 years ago
- Views:
Transcription
1 Sexual Dysfunction Caused by Cancer Treatments Issues in Men Dr Christopher Love Urological and Prosthetic Surgeon Bayside Urology 66 Balcombe Rd., Mentone Men s Health Melbourne Level M 233 Collins St., Melbourne 1800 DRLOVE
 Penile Rehabilitation 5) Treating Established Erectile")
2 1) Incidence and types of sexual dysfunction 2) Factors causing sexual dysfunction 3) Prostate cancer associated dysfunctions, particularly erectile dysfunction 4) Penile Rehabilitation 5) Treating Established Erectile Dysfunction
3 Incidence of Sexual Dysfunction in Cancer Treatment Many types of cancer and cancer therapies are frequently associated with sexual dysfunction Estimates range from % of patients Derogatis LR, Kourlesis SM. CA Cancer J Clin 31 (1) ; 46 50, 1981
4 Incidence of Sexual Dysfunction in Cancer Treatment Most of the published information relates to women who have breast or gynaecological cancers, or men who have prostate cancer Less is known about how other types of cancer affect sexuality
5 The Most Common Problems The most common sexual problems for people with cancer are: Decreased libido (men and women) Erectile Dysfunction Dyspareunia Ejaculation changes and failure to reach orgasm (men) Changes in genital sensation and failure to reach orgasm (women) Schover LR, Montague DK, Lakin MM. Cancer: Principles and Practice of Oncology, 5 th Ed, pp Lippincott-Raven Publishers 1997
6 The Impact of Sexual Dysfunction Unlike many other physiological side-effects of cancer treatment, sexual dysfunction does not tend to resolve, and has influences on cancerfree quality of life (1) Erectile dysfunction is an important issue for patients who have undergone radical prostatectomy. Urologists tend to underestimate patient s distress and their desire for early treatment (2) 1. Litwin MS, Hayes RD et al. JAMA 273 (2); , Chartier-Kastler,E. J Sex Med 2008; 5:
 ED has a significant negative impact on the patient s quality of life and self esteem (2) 1. Burnett A. et al.")
7 Impact of Post-Operative Erectile Dysfunction Erectile function is precipitously, severely and extendedly lost following this and other pelvic surgeries causing significant emotional and psychological distress for many men and their partners (1) ED has a significant negative impact on the patient s quality of life and self esteem (2) 1. Burnett A. et al. J Sex Med 2008; 5 : Mulhall J.P. J Sex Med 2008: 5 (supp): 197
8 Factors Causing Sexual Dysfunction Sexual dysfunction, as it relates to cancer treatments, may be multifactorial, with both physiological and psychological factors contributing to its development. Doctors and patients tend to focus on the medication-intensive treatment of the cancer itself, and perhaps less on the quality of life side-effects. Cakar B, Karaca B, Uslu R. J BUON. 18 (4); Oct Dec 2013
9 Factors Causing Sexual Dysfunction Physiological factors: Functional damage, fatigue, pain and pain medications Testosterone levels affected by many chronic illnesses and some medications Cancer therapies such as surgery, chemotherapy, hormone therapy, radiation therapy and bonemarrow transplant may all have direct physiological impact on sexual function Watson M, Wheatley K et al. Cancer 86(7):
10 Factors Causing Sexual Dysfunction Psychological factors: Misbeliefs about origin of the cancer Guilt related to those misbeliefs Co-existing depression Changes in body image Stresses to relationships secondary to cancer diagnosis and treatment Schover LR, Montague DK, Lakin MM. Cancer: Principles and Practice of Oncology, 5 th Ed, pp Lippincott-Raven Publishers 1997
11 Therapy Related Factors - Surgery Many surgical treatments for cancer have a direct physiological effect on sexual function This applies particularly to surgery for breast cancer, gynaecological cancer, rectal cancer, prostate cancer, testicular cancer and penile cancer, with potential vascular, nerve and end organ damage Common predictors of post-operative sexual function include age, pre-treatment sexual function, tumour location, tumour size, and extent of surgical resection.
12 Therapy Related Factors Chemotherapy Loss of libido and decreased frequency of intercourse are noted in many patients undergoing chemotherapy, and are probably related to general side-effects of the treatment, like nausea, fatigue, diarrhoea, mucositis, altered sense of taste and smell, alopecia, all possibly leading to the patient feeling asexual. Chemotherapy agents rarely play a role in the development of erectile dysfunction or ejaculatory problems, but some can interfere with testosterone production Gradishai WJ and Schilsky Rl. Crit Rev Oncol Haematol 8(2): , 1988
13 Therapy Related Factors Radiotherapy As with chemotherapy, general side-effects like fatigue and changes in bladder and bowel function may play a role in loss of libido Pelvic nerves or vessels may be damaged ED Prostate scarred no semen Time course is different- The ED takes longer to happen with radiation than surgery, suggesting gradual arterial insufficiency But by 3yrs minimal difference in incidence of ED between radiation and surgery
14 Therapy Related Factors Hormone Therapy The hormone therapy used in prostate cancer, aiming to reduce circulating androgens as low as possible, will result in loss of libido, erectile dysfunction and possibly difficulty achieving orgasm in most men Strategies, including delayed commencement of therapy, intermittent hormone therapy, or alternatives like finasteride and androgen-receptor blocker combinations, have been tried to minimise side-effects. Potasky Al et al. J Natl Cancer Inst 94(6):
15 Prostate Cancer Surgery Associated Problems RADICAL PROSTATECTOMY (open / laparoscopic / robotic) (There is no difference in these side effects no matter which surgical technique is used) 1-5 % - severe incontinence and 5-15 % - mild stress incontinence during physical exertion Erectile dysfunction occurs in up to 85 % of men after a radical prostatectomy Penile shortening or curvature is reported Ejaculation is not possible after RP as the ejaculatory glands have been removed. Anorgasmia, or painful orgasm have both been reported Climacturia loss of urine with climax Bladder neck scarring 2-10% Bowel injury <1% Psychological distress anxiety, depression, loss of self-esteem, don t feel like a man anymore, quality of life reduced.
16 Post-prostatectomy Sexual Dysfunction other than ED Orgasm changes Orgasmic pain reported in 14% of men after radical prostatectomy Thought to be associated with bladder neck and pelvic floor spasm, as many cases are helped by selective alpha-blocker Tamsulosin (1) 37% prevalence of complete absence of orgasm, as well as of decreased orgasm intensity (2) But orgasmic function tends to improve linearly over 48 months after radical prostatectomy. Absence of seminal vesicle and prostatic contractions may account for less satisfying orgasms. There is no effective treatment to allow return to baseline function Urine Leak with Climax (climacturia) Up to 20 % of men Behavioural therapy decrease fluid intake, empty bladder before sex Mechanical therapy condom, constriction ring Surgery urethral slings, particularly urethral re-positioning or elongating slings 1. Barnas J, Parker M, Guhring P et al. Eur Urol 2005; 47 (3): Barnas JL, Pierpaoli S, et al. BJU Int 2004; 94:
17 Post prostatectomy Sexual Dysfunction other than ED Loss of Penile Length 71% of men report this after radical prostatectomy > 1.5 cm length loss in 48% of men at 3 months (1) Thought to be related to Fibrosis, following on from hypoxia and an increase in fibrogenic cytokines like TGF-beta 1, leading to increased collagen deposition Sympathetic hyperinnervation as neuropraxia improves, sympathetic nerves recover quicker, causing an increase in sympathetic tone and therefore decreased distensibility and relaxation of corpora Neuropraxia may also contribute to smooth muscle degeneration in the penis 1. Munding M D, Wessells HB, Dalkin BL. Urology 2001; 58 (4):
")

18 Erectile Dysfunction (ED) is just a part of Sexual Dysfunction (SD) SD ED
19 The scope of the ED problem Disparate rates of erectile dysfunction ranging from 20 90% in various studies 1 Prostate Cancer Outcome Study 2 Looks at the changes in erectile function for up to 5 years post-operatively Pre-Op 6 months 12 months 24 months 60 months 1213 patients. Based on self reported erections firm enough for intercourse 81% 9% 17% 22% 28% Back to Baseline at 24 months 3 - Same erections as before surgery (without medication) 16% who had normal function pre-op, and only 5% if over age Burnett A.L. et al J Urol 2007; 178: Penson et al. J Urol 2008; 5: Mulhall et al J Sex Med 2013; 10:
20 The Nature of Erectile Dysfunction After Radical Prostatectomy Very common early after surgery Generally improves with time Improved surgical techniques have helped ( nerve sparing ) - but not as much as expected Can keep improving for 36 months in some cases BUT If nothing happening at 6-12 months unlikely to recover
21 Prostate Cancer Surgery Improvements in surgical technique have lead to improved long-term cure (1) and significantly better continence rates (2) after surgery. This has increased the attention given to, and perhaps the significance of, erectile dysfunction after surgery. 1. Han M et al Urol Clin North Am 2001; 28: Catalona W.J. et al J Urol 1999; 162: 433

22 Neurovascular Bundles

23 Nerve-sparing technique
24 The question about ED after prostate surgery Why have we not seen, despite meticulous nerve-sparing techniques, the same improvement in post-operative potency rates that have now become normal for continence after radical prostatectomy?
25 The ongoing surgical problem Even in nerve sparing surgery, manipulation, traction and stretching of the cavernous nerves occurs, resulting in some degree of neuropraxia. Neuropraxia itself results in structural changes in the penis including vascular, neural and cavernous smooth muscle changes (1) 1.Blaya R. and Mulhall J.P. AUA Update 2008; 27: Lesson 36
26 The ongoing surgical problem 2 Even with good surgical technique there may be possible vascular damage to functional accessory pudendal arteries (1) Added to this, the chronic lack of erections secondary to the neuropraxia results in failure of cavernosal oxygenation with the potential for further structural damage (2) 1. Rogers C.G. et al Urology 2004; 64: Moreland R.B. Int J Imp Res 1998; 10:
27 The ongoing surgical problem 3 Clinical manifestations of these changes may be 1. corporal veno-occlusive dysfunction(cvod) (1) 2. shrinkage and atrophy of the penis (2) 3. the development of Peyronie s like plaques and curvatures (3) 1. Ferrini M. et al J Sex Med 2009; 6: Savoie M et al J Urol 2003; 169: Cianco S.J. et al BJU Int 2000; 85:
28 How the penis becomes erect: Cavernosal Artery Tunica albuginea Subtunical venules Corpora cavernosum - Smooth muscle and vascular spaces
29 How the penis becomes erect: FLACCID ERECT 1 Dilation of cavernosal artery and increased arterial inflow 2 Engorgement of corpora cavernosum with blood, and relaxation of smooth muscle 3 Passive occlusion of sub-tunical venules against tunica 4 Intra-cavernosal pressure rises and rigidity occurs


30 Nerve Damage Neuropraxia This may eventually recover in months No signal to penis to become engorged Poor Erections Minimal blood flow = hypoxia Venous leak Fibrosis and poor compliance of penis Permanent ED Penile shortening
31 Basic Science Injury Mechanisms Apoptosis Denervation of the rat penis leads to apoptosis of corporal bodies (1) Penile apoptosis as early as 1 day after cavernous nerve ablation. Most apoptosis directly under tunica albuginea (2) Cavernous nerve crush injury model causes apoptosis in both smooth muscle and endothelium (3) 1.Klein L.T. et al J Urol 1997;158: User H.M. et al J Urol 2003; 169: Mullerad M. et al J Sex Med 2006; 3: 77-83
32 Basic Science Injury Mechanisms Fibrosis Neuropraxia results in alterations in smooth muscle collagen ratios (1) Neuropraxia causes upregulation of fibrogenic cytokines such as TGF-beta1, which increases collagen types I and III synthesis (1) Cavernous nerve injury results in endothelial cell retraction (2) 1. Leungwattanakij S. et al J Androl 2003; 24: Klein L.T. et al J Urol 1997; 158:
33 Basic Science Injury Mechanisms Cavernosal Deoxygenation Low oxygen tensions upregulate fibrogenic cytokines, such as TGF-beta1, resulting in increased fibrosis (1) Oxygenation upregulates the production of endogenous prostanoids as well as camp (1) Prostanoids such as PGE1, inhibit TGF-beta1 activity and reduce collagen production (2) Prostanoids are protective for smooth muscle (1) 1. Moreland R.B. et al Am J Physiol Heart Circ 2001; 281: H552 H Moreland R.B. et al Int J Impot Res 1998; 10:
34 Basic Science Injury Mechanisms Venous Leak If corporeal smooth muscle fails to expand, some or all of the sub-tunical venules are left in a non-compressed state, leading to venous leakage Corporeal smooth muscle fails to expand most commonly due to adrenaline, and structural changes such as fibrosis
35 Signal transduction pathways Adapted from Lue T. N Engl J Med 2000; 342:
36 Basic Science Injury Mechanisms Venous Leak Venous leak occurs once smooth muscle content in the penis drops below 40% (1) Collagen deposition in erectile tissues increases markedly as early as 2 months after surgery (2) Haemodynamic studies show that more than half the men with ED after radical prostate surgery have venous leakage, and the incidence of venous leakage increases with time from surgery, particularly after four months (3) 1. Nehra A et al J Urol 1996; 156: Iacono F et al J Urol 2005; 173: Mulhall J.P. et al Int J Imp Res 1996; 8: 91-94


37


38

39 Penile Rehabilitation Use of any medication or device, after pelvic surgery, to maximise the recovery of erectile function Concept: Improve oxygen to penile tissues Protection of the cells lining the blood spaces Prevent cavernosal nerve injury-induced structure changes Penile rehabilitation is an assortment of strategies directed towards preventing the structural alterations in the penis, whilst the nerve damage resolves, and therefore restoring penile health after radical prostatectomy
40 Penile Rehabilitation We think most nerve damage, with good surgical technique, will eventually recover, but will the penis still work by the time the nerves have healed? We now understand that regular erections are important for the health of the penis stretching of elastic tissues, fresh blood and oxygen to keep the penis healthy. If you don t use it you lose it When there are no erections for a time, irreversible structural damage occurs in the penis.
41 Basic Science Possible Repair Mechanisms Prostaglandin PGE1 may promote the recovery of erectile function by the promotion of cavernosal oxygenation levels By stimulating the formation of adenyl cyclase, PGE1 increases the concentration of camp within smooth muscle cells. Ruis Rubio J.L. et al J Urol 2004; 171:
42 Basic Science Possible Repair Mechanisms PDE5 inhibitors stimulate smooth muscle cell replacement via a cgmp mechanism and reduce collagen synthesis via protein kinase G activation If PGE5 inhibitors can induce cavernosal oxygenation in the absence of erection, they may function as endothelial protectants and preserve smooth muscle Kovanecz I et al BJU Int 2007; 101:
43 Evidence Supporting Penile Rehabilitation Animal Data Sildenafil shows significant improvement in intra-cavernosal /mean arterial pressure ratio (ICP/MAP) in rats commencing on the day of cavernous nerve injury Sildenafil treatment in rats having cavernous nerve injuries resulted in preservation of corporeal smooth muscle content, better endothelial factors, reduced apoptosis and increased phosphorylation of AKT and enos, both critical to endothelial function for penile erection Mulhall J.P. et al J Sex Med 2008; 5:
44 Evidence Supporting Penile Rehabilitation Animal Data Vardenafil prevents fibrosis and loss of corporeal smooth muscle after bilateral cavernous nerve resection in rats. This may be by vasoactive effector stimulatory mechanisms (1) PDE5 inhibitors work by anti-oxidative mechanisms (2) Statin therapy may improve penile endothelial function (2) 1. Ferrini M.G et al Urology 2006; 68: DeYoung L.X. et al Int J Imp Res 2003; 15:
45 Evidence Supporting Penile Rehabilitation Human Data Intracavernous PGE1 three times a week for 12 weeks post RP. At 6 months 67% of treatment group had erections sufficient for intercourse compared to 20% of untreated group (1) Corporeal biopsies at time of RP and 6 months later shows that Sildenafil treated patients showed histopathological evidence of preservation of smooth muscle content compared to untreated patients (2) 1. Montorsi F et al J Urol 1997; 158: Schwartz E.J. et al J Urol 2004; 171:
46 Evidence Supporting Penile Rehabilitation Human Data Randomised, placebo controlled trial of Sildenafil nightly from 4 weeks to 36 weeks 27% of patients receiving Sildenafil demonstrated return of spontaneous erectile function compared to 4% in the placebo group at 48 weeks A subset of these patients had nocturnal penile tumescence and rigidity studies pre- and post operatively, showing a gradual dose-dependent improvement in the treatment group Padma Nathan H. et al Int J Imp Res 2008; 20:
47 Other Strategies for Penile Rehabilitation Vacuum Device Therapy daily use for men wishing to preserve penile length (1) Early use of VCD facilitated preservation of penile length and girth (2) Trans-urethral PGE1 (MUSE) 3 times a week for 9 months post-operatively. Only 68% completed the study. (3) 40% in treatment group had return of natural erections compared to 11% in observation group (3) 1. Dalkin B.L. and Christopher B.A. Int J Imp Res 2007; 19: Raina R et al J Sex Med 2008; 5(Supp 1): Raina R. et al BJU Int 2007; 100:





48 Nerve Damage
49 Penile Rehabilitation does it work? Penile Rehabilitation Treatment Options (alone or in combination) Oral Medications (PDE-5) Vacuum Erection Device (VEDs) Intraurethral Suppository Intracorporeal Injections Sildenafil 25 mg daily (Bannowsky 2008) Sildenafil 50 or 100 mg daily (McCullough 2008) VED (Raina 2006) Urethral Suppository (Raina 2007) Intracorporeal Injection (Montorsi 1997) Intracorporeal Injection or sildenafil 100 mg (Mulhall 2005) Rehabilitation Control 11/23 (47%) 5/18 (28%) 10/35 (28%) 1/19 (5%) 10/60 (17%) 4/35 (11%) 21/38 (55%) 4/35 (11%) 8/12 (67%) 3/15 (20%) 30/58 (52%) 14/74 (19%)
50 Current Role of Penile Rehabilitation Arguments For Mechanisms for protection of endothelial function and smooth muscle are known Animal models of chronic dosing with PDE5 i demonstrate improvements Human data point to improvement Argument against Present human studies have significant limitations and many lack Level 1 evidence Cost of rehabilitation at least $ 120+ per month (? for how long)
51 Cost - Effectiveness Penile rehabilitation was found to be not cost-effective when compared to other therapeutic options Simultaneous penile prosthesis implantation at the time of radical prostatectomy appears to be the most cost-effective treatment option Hellstrom W.J.G. et al J Sex Med 2008; 5 (supp 1): 4-41
52 Penile Rehabilitation Programme Mulhall - MSKCC 1. Low dose PDE5 nightly for two weeks pre-op. 2. Two weeks post op commence nightly low dose PDE5 6 nights/ week and weekly maximal dose PDE5 with sexual stimulation 3. If responding (erectile activity) at 6 weeks, continue maximum dose two nights a week and low dose other five nights 4. If not responding then PGE1 twice weekly and low dose PDE5 other nights until response 5. +/- use of vacuum-erection device
53 PREVENTION OF POST PROSTATECTOMY ED Be aged less than 60 Don t have any ED before prostate cancer treatment Don t have diabetes, cholesterol issues, high blood pressure Have a motivated partner Don t be overweight Don t be a smoker Pick your surgeon rather than the surgical technique Meticulous dissection nerve sparing Surgeon experience is important Start a Penile Rehabilitation programme


54
55 Potential options: 1 st Line: Oral Medications 2 nd Line: Vacuum Erection Devices Penile injections 3 rd Line: Penile prostheses (implant)
 Efficacious but less likely in")
56 Safe (Viagra 1998, Cialis and Levitra 2003) Easily accessible Easily taken (oral) Efficacious but less likely in post-prostatectomy


57 Phosphodiesterase 5 inhibitors (PDE5s) in Penile Rehabilitation? Protect smooth muscle and endothelial cells? Minimise fibrosis? Help nocturnal blood flow and erections NANC
 >1 time and type 3.Must know side effects Headache, facial flushing, stuffy nose (<10%) Indigestion, blue tinge (V) Temporary 4.")
58 Dr Love s Medication Musts 1.Must know the potential benefit and limitations Need to be able to get some erections on your own Not a magic pill 2.Must take them as directed Dose Timing (V) >1 time and type 3.Must know side effects Headache, facial flushing, stuffy nose (<10%) Indigestion, blue tinge (V) Temporary 4.Must NOT take Nitrate medication 5.Must not buy off the internet

59

60




61 Vacuum Erection Device (VED) in Penile Rehabilitation Keep penis stretched? More blood into penis
62 Seems great No drugs Works One off cost

63 Blue Cold Painful Hinge effect Tedious Interrupts the flow of things

64


65 Intracavernosal injections in Penile Rehabilitation Cross-section of the shaft of the penis Midline Vasoactive drug injected directly into the corpus away from the midline Corpus cavernosum A way of getting an erection and keeping the penis stretched Fresh blood into penis If you use it you are less likely to lose it
66 Many men who try it continue in the long term* Simple Effective Cheap Minimal discomfort Very few serious side effects * When adhere to secrets of success

67 Education 2 x sessions Tiny needle Less sensitive area Small dose increments Support 24 hr Involve partner
 Travel Just cant")
68 Painful Prolonged erection (priapism) May not work leaky valve venous leak Problems with dexterity/limited eyesight (partner) Travel Just cant do it

69 What If Penile Rehabilitation Doesn t Work? Eventually, if erections are not recovering, or are insufficient for penetrative intercourse, decisions will need to be made. When is the right time? What is the right next step?
70 Penile Prostheses Paired inflatable inner tubes inserted surgically into the penis. Ideal for men who have tried other treatments without success On the market for 40 years 30,000 penile implants per year 1 Over 450,000 implants to date 2 High patient and partner satisfaction 3 1 Millenium Research Group. US Markets for Urological Devices May "Penile Prosthesis." The Sexual Medicine Web Site European Society for Sexual Medicine. 23 Jan 3 Levine LA, Estrada CR, Morgentaler A.. J Urol Sep;166(3):932-7
 The")
 The pump (placed within")
71 Penile Prosthesis The cylinders (placed within the penis) The reservoir (placed within the abdomen) The pump (placed within the scrotum)

72
73 Proven Benefits of Penile Implants Achieve an erection easily and maintain it as long as required Looks and feels like a normal penis Erection hard enough for penetration and allows you to complete sexual intercourse 1 Easy to use Sensation, orgasm same as before Dependable, works every time Restores spontaneity 30 minute operation Usually one night stay in hospital 1 "Benefits of Penile Implants." Erectile Dysfunction Institute Erectile Dysfunction Institute. 23 Jan
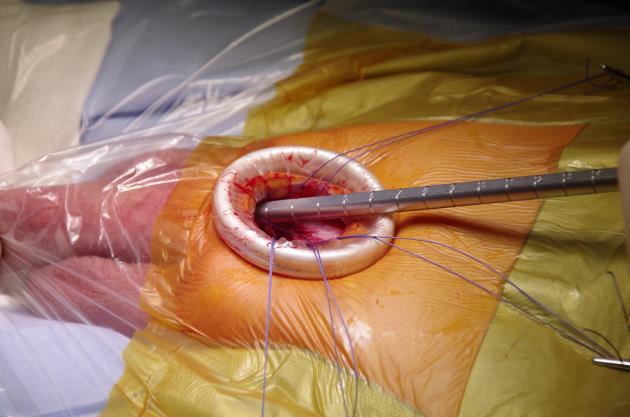




74 Penile Prosthesis Minimally Invasive Surgery




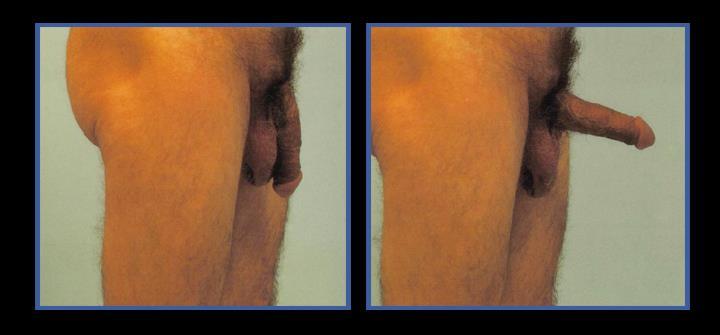
75 The Results of Penile Implant Surgery

76 Penile prosthesis - satisfaction Series of approx men and their partners ~90% said they were satisfied ~80% of partners were satisfied ~85% said they would have the operation again ~85% would recommend it to a friend 80 % 60% 40 % 20 % Carson C, Mulcahy J et al Penile Implant Oral Medication Penile Injections
")
77 Why such high patient and partner satisfaction rates? Works! Quick to inflate seconds Concealed Confidence Spontaneous Preserves sensation and orgasm(s) Individually tailored Age is no barrier
78 However, there are some aspects that concern patients about penile implants. Requires surgery Risk of surgical complications which may include infection(< 1%) Cost may be prohibitive without insurance Possible discomfort or pain from use Non-reversible There may be mechanical failures which may require revision surgery (< 5% at 10 years) Requires some manual dexterity
79 1. Sexual Dysfunction is common after prostate cancer, and other cancer treatments 2. SD is not just ED 3. Check testosterone 4. Penile rehabilitation 5. Numerous treatments available for established ED 6. Each have their own benefits, limitations and side effects 7. 1 st, 2 nd, 3 rd line treatments Increasingly effective Penile Prosthesis has the highest satisfaction rate





80 ED is important even in nature

81 Thank you DRLOVE ( )
Management of Post-Prostatectomy Urinary Incontinence and Sexual Dysfunction
 Management of Post-Prostatectomy Urinary Incontinence and Sexual Dysfunction Robert C. Eyre, MD, FACS Associate Clinical Professor of Surgery (Urology) Harvard Medical School Post-prostatectomy Incontinence
Management of Post-Prostatectomy Urinary Incontinence and Sexual Dysfunction Robert C. Eyre, MD, FACS Associate Clinical Professor of Surgery (Urology) Harvard Medical School Post-prostatectomy Incontinence
ERECTION MISDIRECTION: PENILE REHABILITATION & TREATMENTS FOR ERECTILE DYSFUNCTION. Gregory Harochaw Pharmacy Manager Tache Pharmacy (204)
") ERECTION MISDIRECTION: PENILE REHABILITATION & TREATMENTS FOR ERECTILE DYSFUNCTION Gregory Harochaw Pharmacy Manager Tache Pharmacy (204) 233-3469 Nerve Function After careful prostatectomy where the erectile
ERECTION MISDIRECTION: PENILE REHABILITATION & TREATMENTS FOR ERECTILE DYSFUNCTION Gregory Harochaw Pharmacy Manager Tache Pharmacy (204) 233-3469 Nerve Function After careful prostatectomy where the erectile
Managing Symptoms after Prostate Cancer Sexual Side Effects. Changes in a man s sex life are common and can be managed.
 Managing Symptoms after Prostate Cancer Sexual Side Effects Changes in a man s sex life are common and can be managed. Prostate cancer and its treatment often bring changes in a man s sex life, especially
Managing Symptoms after Prostate Cancer Sexual Side Effects Changes in a man s sex life are common and can be managed. Prostate cancer and its treatment often bring changes in a man s sex life, especially
MANAGEMENT UPDATE , LLC MedReviews
 MANAGEMENT UPDATE 2013 MedReviews, LLC rostate cancer is the most common cancer in men over the age of 50 years. 1 When patients undergo a radical prostatectomy (RP), there is a risk of postoperative erectile
MANAGEMENT UPDATE 2013 MedReviews, LLC rostate cancer is the most common cancer in men over the age of 50 years. 1 When patients undergo a radical prostatectomy (RP), there is a risk of postoperative erectile
Erectile Dysfunction and the Prostate Cancer Patient
 BAUN & Prostate cancer UK Erectile Dysfunction Study Day Erectile Dysfunction and the Prostate Cancer Patient Lorraine Montgomery Specialist Nurse Practitioner Urology Queen Elizabeth Hospital Gateshead
BAUN & Prostate cancer UK Erectile Dysfunction Study Day Erectile Dysfunction and the Prostate Cancer Patient Lorraine Montgomery Specialist Nurse Practitioner Urology Queen Elizabeth Hospital Gateshead
Managing Symptoms after Prostate Cancer Sexual Side Effects for Gay and Bisexual Men Changes in a man s sex life are common and can be managed.
 Managing Symptoms after Prostate Cancer Sexual Side Effects for Gay and Bisexual Men Changes in a man s sex life are common and can be managed. Even without prostate cancer, getting older can cause changes
Managing Symptoms after Prostate Cancer Sexual Side Effects for Gay and Bisexual Men Changes in a man s sex life are common and can be managed. Even without prostate cancer, getting older can cause changes
13-Oct-15 ERECTILE DYSFUNCTION. Urology Subdepartement dr. Mintohardjo Naval Hospital dr. Isdiyanto Septiadi, Sp.U
 ERECTILE DYSFUNCTION Urology Subdepartement dr. Mintohardjo Naval Hospital dr. Isdiyanto Septiadi, Sp.U 1 2 3 So what is impotence or erectile dysfunction..? The persistent inability to achieve or maintain
ERECTILE DYSFUNCTION Urology Subdepartement dr. Mintohardjo Naval Hospital dr. Isdiyanto Septiadi, Sp.U 1 2 3 So what is impotence or erectile dysfunction..? The persistent inability to achieve or maintain
A Proposed Study of Hyperbaric Oxygen Therapy Following Radical Prostatectomy: Effects on Erectile Dysfunction
 A Proposed Study of Hyperbaric Oxygen Therapy Following Radical Prostatectomy: Effects on Erectile Dysfunction Anthony J. Bella MD, FRCSC Division of Urology, Department of Surgery and Department of Neuroscience
A Proposed Study of Hyperbaric Oxygen Therapy Following Radical Prostatectomy: Effects on Erectile Dysfunction Anthony J. Bella MD, FRCSC Division of Urology, Department of Surgery and Department of Neuroscience
MALE SEXUAL DYSFUNCTION. Urology Division, Surgery Department Medical Faculty, University of Sumatera Utara
 MALE SEXUAL DYSFUNCTION Urology Division, Surgery Department Medical Faculty, University of Sumatera Utara DEFINITION The inability to achieve a satisfactory sexual relationship May involve : - inadequacy
MALE SEXUAL DYSFUNCTION Urology Division, Surgery Department Medical Faculty, University of Sumatera Utara DEFINITION The inability to achieve a satisfactory sexual relationship May involve : - inadequacy
Review Article Penile Rehabilitation Therapy with PDE-V Inhibitors Following Radical Prostatectomy: Proceed with Caution
 Advances in Urology Volume 2009, Article ID 852437, 4 pages doi:10.1155/2009/852437 Review Article Penile Rehabilitation Therapy with PDE-V Inhibitors Following Radical Prostatectomy: Proceed with Caution
Advances in Urology Volume 2009, Article ID 852437, 4 pages doi:10.1155/2009/852437 Review Article Penile Rehabilitation Therapy with PDE-V Inhibitors Following Radical Prostatectomy: Proceed with Caution
Managing Erectile Dysfunction
 Managing Erectile Dysfunction Lewis E. Harpster MD, FACS Urology of Central PA 4/23/16 1 Objectives 1. Review physiologic mechanism of erection 2. Discuss medical management of ED 3. Discuss surgical management
Managing Erectile Dysfunction Lewis E. Harpster MD, FACS Urology of Central PA 4/23/16 1 Objectives 1. Review physiologic mechanism of erection 2. Discuss medical management of ED 3. Discuss surgical management
Jan Farrell. Nurse Consultant Urology Department of Urology Rotherham General Hospital NHS FT
 Jan Farrell Nurse Consultant Urology Department of Urology Rotherham General Hospital NHS FT Aims of session To promote discussion / interaction Opportunity to discuss with peers Promote learning / share
Jan Farrell Nurse Consultant Urology Department of Urology Rotherham General Hospital NHS FT Aims of session To promote discussion / interaction Opportunity to discuss with peers Promote learning / share
Erectile Dysfunction; It s Not Just About Sex
 Erectile Dysfunction; It s Not Just About Sex Disclosures Conflict of interest: I am not paid by Boston Scientific but once in a while they buy me a tasty meal. I do routinely use their products without
Erectile Dysfunction; It s Not Just About Sex Disclosures Conflict of interest: I am not paid by Boston Scientific but once in a while they buy me a tasty meal. I do routinely use their products without
Sidney Glina Faculdade de Medicina do ABC Instituto H. Ellis Editor-in-Chief of the International Brazilian Journal of Urology
 Sidney Glina Faculdade de Medicina do ABC Instituto H. Ellis Editor-in-Chief of the International Brazilian Journal of Urology (www.intbrazjurol.com.br) glinas@terra.com.br Conflict of Interest: In the
Sidney Glina Faculdade de Medicina do ABC Instituto H. Ellis Editor-in-Chief of the International Brazilian Journal of Urology (www.intbrazjurol.com.br) glinas@terra.com.br Conflict of Interest: In the
Jan Farrell Nurse Consultant Urological Services Department of Urology Rotherham General Hospital NHS FT
 Jan Farrell Nurse Consultant Urological Services Department of Urology Rotherham General Hospital NHS FT Aims of session To promote discussion / interaction Opportunity to discuss with peers Promote learning
Jan Farrell Nurse Consultant Urological Services Department of Urology Rotherham General Hospital NHS FT Aims of session To promote discussion / interaction Opportunity to discuss with peers Promote learning
Mr PHIP No. 6 Sexual function after treatment for prostate cancer
 Mr PHIP No. 6 Sexual function after treatment for prostate cancer Mr Phip There is a wide variability in sexual function as men grow older; however a gradual decline is normal. Key points Normal sexual
Mr PHIP No. 6 Sexual function after treatment for prostate cancer Mr Phip There is a wide variability in sexual function as men grow older; however a gradual decline is normal. Key points Normal sexual
Disclosure Slide. Dr Michael Gillman IMPOTENCE ERECTILE DIFFICULTIES. Do Men Really Care??? 15/10/2014 ASSESSMENT OF ERECTILE DYSFUNCTION
 ASSESSMENT OF ERECTILE DYSFUNCTION Dr Michael Gillman St Andrews Hospital North St Specialist Suites Mater Hospital 3 rd Floor Mater Private Clinic Wesley Hospital Suite 5 Level 9 Evan Thomson Bld Cleveland-
ASSESSMENT OF ERECTILE DYSFUNCTION Dr Michael Gillman St Andrews Hospital North St Specialist Suites Mater Hospital 3 rd Floor Mater Private Clinic Wesley Hospital Suite 5 Level 9 Evan Thomson Bld Cleveland-
Diagnosis and management of sexual dysfunction. Dr Chris Simpson Consultant Psychiatrist
 Diagnosis and management of sexual dysfunction Dr Chris Simpson Consultant Psychiatrist What are we talking about? Male Erectile dysfunction Premature ejaculation Delayed ejaculation Sexual aversion Paraphilia
Diagnosis and management of sexual dysfunction Dr Chris Simpson Consultant Psychiatrist What are we talking about? Male Erectile dysfunction Premature ejaculation Delayed ejaculation Sexual aversion Paraphilia
Penile implants What to expect and how to prepare
 Penile implants What to expect and how to prepare Penile implants can restore erectile function. Explore your choices and find out what to expect from this procedure. Penile implants are artificial devices
Penile implants What to expect and how to prepare Penile implants can restore erectile function. Explore your choices and find out what to expect from this procedure. Penile implants are artificial devices
Erectile Dysfunction (ED) Shawn McGee M.D. CentraCare Adult and Pediatric Urology January 30 th, 2016
 Shawn McGee M.D. CentraCare Adult and Pediatric Urology January 30 th, 2016") Erectile Dysfunction (ED) Shawn McGee M.D. CentraCare Adult and Pediatric Urology January 30 th, 2016 Erectile dysfunction: The inability to attain or maintain penile erection sufficient for satisfactory
Erectile Dysfunction (ED) Shawn McGee M.D. CentraCare Adult and Pediatric Urology January 30 th, 2016 Erectile dysfunction: The inability to attain or maintain penile erection sufficient for satisfactory
Medicines Q&As. Date prepared: November 2016
 Q&A 128.3 What is the rationale and evidence for the use of phosphodiesterase-5 inhibitors as supportive therapy to rehabilitate Erectile Function after nerve sparing radical prostatectomy? Summary Prepared
Q&A 128.3 What is the rationale and evidence for the use of phosphodiesterase-5 inhibitors as supportive therapy to rehabilitate Erectile Function after nerve sparing radical prostatectomy? Summary Prepared
Review Article Overview of Contemporary Penile Rehabilitation Therapies
 Hindawi Publishing Corporation Advances in Urology Volume 2008, Article ID 481218, 6 pages doi:10.1155/2008/481218 Review Article Overview of Contemporary Penile Rehabilitation Therapies Peter Hinh and
Hindawi Publishing Corporation Advances in Urology Volume 2008, Article ID 481218, 6 pages doi:10.1155/2008/481218 Review Article Overview of Contemporary Penile Rehabilitation Therapies Peter Hinh and
Evidence Review for Surrey Prescribing Clinical Network. Treatment: Oral and non-oral combination therapy for erectile dysfunction
 Evidence Review for Surrey Prescribing Clinical Network Treatment: Oral and non-oral combination therapy for erectile dysfunction Prepared by: Linda Honey Topic Submitted by: Prescribing Clinical Network
Evidence Review for Surrey Prescribing Clinical Network Treatment: Oral and non-oral combination therapy for erectile dysfunction Prepared by: Linda Honey Topic Submitted by: Prescribing Clinical Network
, David Stultz, MD. Erectile Dysfunction. David Stultz, MD September 10, 2001
 Erectile Dysfunction David Stultz, MD September 10, 2001 Case Presentation A 66 year old male presents to your office requesting Viagra. He states that for the past year he has had difficulty forming
Erectile Dysfunction David Stultz, MD September 10, 2001 Case Presentation A 66 year old male presents to your office requesting Viagra. He states that for the past year he has had difficulty forming
Penile Rehabilitation after Radical Prostatectomy
 Penile Rehabilitation after Radical Prostatectomy The PRO Position John P. Mulhall MD MSc FECSM FACS Director, Sexual & Reproductive Medicine Program Urology Service Memorial Sloan Kettering Cancer Center
Penile Rehabilitation after Radical Prostatectomy The PRO Position John P. Mulhall MD MSc FECSM FACS Director, Sexual & Reproductive Medicine Program Urology Service Memorial Sloan Kettering Cancer Center
ASSESSMENT OF PREMATURE EJACULATION AND ERECTILE DYSFUNCTION
 ASSESSMENT OF PREMATURE EJACULATION AND ERECTILE DYSFUNCTION Dr Michael Gillman St Andrews Hospital Wickham Terrace Spring Hill Mater Private Clinic, South Brisbane Shore St West Medical Centre, Cleveland
ASSESSMENT OF PREMATURE EJACULATION AND ERECTILE DYSFUNCTION Dr Michael Gillman St Andrews Hospital Wickham Terrace Spring Hill Mater Private Clinic, South Brisbane Shore St West Medical Centre, Cleveland
Penile rehabilitation after radical prostatectomy: patients attitude and feasibility in China
 Original Article Penile rehabilitation after radical prostatectomy: patients attitude and feasibility in China Yi-Jun Shen 1,2, Jian Li 1,2, Ding-Wei Ye 1,2 1 Department of Urology, Fudan University Shanghai
Original Article Penile rehabilitation after radical prostatectomy: patients attitude and feasibility in China Yi-Jun Shen 1,2, Jian Li 1,2, Ding-Wei Ye 1,2 1 Department of Urology, Fudan University Shanghai
SEXUAL HEALTH. Erectile Dysfunction
 SEXUAL HEALTH Erectile Dysfunction Don t Let Erectile Dysfunction Keep You from a Satisfying Sex Life. What Is Erectile Dysfunction or ED? Who Gets ED? Men who have ED have a problem getting or keeping
SEXUAL HEALTH Erectile Dysfunction Don t Let Erectile Dysfunction Keep You from a Satisfying Sex Life. What Is Erectile Dysfunction or ED? Who Gets ED? Men who have ED have a problem getting or keeping
Schemi terapeutici complessi per la gestione della disfunzione erettile post trattamento del carcinoma prostatico: non solo PDE5i
 Schemi terapeutici complessi per la gestione della disfunzione erettile post trattamento del carcinoma prostatico: non solo PDE5i M. Lazzeri MD-PhD Department of Urology Ist. Clinico Humanitas IRCCS Schema
Schemi terapeutici complessi per la gestione della disfunzione erettile post trattamento del carcinoma prostatico: non solo PDE5i M. Lazzeri MD-PhD Department of Urology Ist. Clinico Humanitas IRCCS Schema
Penile Rehabilitation After Radical Prostatectomy: Important Therapy or Wishful Thinking?
 MANAGEMENT UPDATE Penile Rehabilitation After Radical Prostatectomy: Important Therapy or Wishful Thinking? Joseph E. Dall Era, MD, Jesse N. Mills, MD, Hari K. Koul, MD, Randall B. Meacham, MD Division
MANAGEMENT UPDATE Penile Rehabilitation After Radical Prostatectomy: Important Therapy or Wishful Thinking? Joseph E. Dall Era, MD, Jesse N. Mills, MD, Hari K. Koul, MD, Randall B. Meacham, MD Division
Erectile Dysfunction: A Primer for Primary Care Providers
 Erectile Dysfunction: A Primer for Primary Care Providers Jeanne Martin, DNP, ANP-BC Objectives 1. Understand the definition, incidence and prevalence of Erectile Dysfunction in the U.S. 2. Understand
Erectile Dysfunction: A Primer for Primary Care Providers Jeanne Martin, DNP, ANP-BC Objectives 1. Understand the definition, incidence and prevalence of Erectile Dysfunction in the U.S. 2. Understand
THE FACTS ABOUT MEN S SEXUAL HEALTH
 Come in and experience the Chesapeake Urology difference. Call 877-422-8237 to make an appointment with a urologist today or visit www.chesapeakeurology.com to learn more about our specialized care for
Come in and experience the Chesapeake Urology difference. Call 877-422-8237 to make an appointment with a urologist today or visit www.chesapeakeurology.com to learn more about our specialized care for
Sexual Issues following Prostate Cancer Treatments. Seacourses December 30, 2017 January 6, 2018 Dr. Stacy Elliott
 Sexual Issues following Prostate Cancer Treatments Seacourses December 30, 2017 January 6, 2018 Dr. Stacy Elliott Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be
Sexual Issues following Prostate Cancer Treatments Seacourses December 30, 2017 January 6, 2018 Dr. Stacy Elliott Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be
Erectile Dysfunction Case Study 2. Medical Student Case-Based Learning
 Erectile Dysfunction Case Study 2 Medical Student Case-Based Learning The Case of Mr. Power s Limp Mojo Mr. Powers develops erectile dysfunction after his radical prostatectomy for prostate cancer. You
Erectile Dysfunction Case Study 2 Medical Student Case-Based Learning The Case of Mr. Power s Limp Mojo Mr. Powers develops erectile dysfunction after his radical prostatectomy for prostate cancer. You
About Erectile Dysfunction. Causes, self-test and treatment
 About Erectile Dysfunction Causes, self-test and treatment 2015 One Way S.r.l. All rights reserved. Gift copy for physicians. Illustrated by Davide Ceccon With an unrestricted grant from Recordati About
About Erectile Dysfunction Causes, self-test and treatment 2015 One Way S.r.l. All rights reserved. Gift copy for physicians. Illustrated by Davide Ceccon With an unrestricted grant from Recordati About
Moving Beyond Cancer To A New Normal in Intimacy For Men & Their Partners. Presented by Mary Ellen West, RN, MN, CNM AASECT Certified Sex Counselor
 Moving Beyond Cancer To A New Normal in Intimacy For Men & Their Partners Presented by Mary Ellen West, RN, MN, CNM AASECT Certified Sex Counselor WHO Definition of Sexuality Central aspect of being human
Moving Beyond Cancer To A New Normal in Intimacy For Men & Their Partners Presented by Mary Ellen West, RN, MN, CNM AASECT Certified Sex Counselor WHO Definition of Sexuality Central aspect of being human
Questions & Answers about Sexuality and Intimacy after Bladder Cancer. Part III: Causes and Treatments for Sexual Dysfunction
 Questions & Answers about Sexuality and Intimacy after Bladder Cancer A Valentine's chat with Dr. Trinity Bivalacqua Monday, February 13, 2017 Part III: Causes and Treatments for Sexual Dysfunction Presented
Questions & Answers about Sexuality and Intimacy after Bladder Cancer A Valentine's chat with Dr. Trinity Bivalacqua Monday, February 13, 2017 Part III: Causes and Treatments for Sexual Dysfunction Presented
Canadian Undergraduate Urology Curriculum (CanUUC): Erectile Dysfunction
: Erectile Dysfunction") Canadian Undergraduate Urology Curriculum (CanUUC): Erectile Dysfunction Last reviewed July 2014 Objectives 1. Define erectile dysfunction 2. List and classify the risk factors for erectile dysfunction
Canadian Undergraduate Urology Curriculum (CanUUC): Erectile Dysfunction Last reviewed July 2014 Objectives 1. Define erectile dysfunction 2. List and classify the risk factors for erectile dysfunction
Recovery of erectile function after nerve-sparing radical prostatectomy: improvement with nightly low-dose sildenafil
 Sexual Medicine RECOVERY OF ERECTILE FUNCTION AFTER NERVE-SPARING RP WITH NIGHTLY LOW-DOSE SILDENAFIL BANNOWSKY et al. Associate Editor Michael G. Wyllie Editorial Board Ian Eardley, UK Jean Fourcroy,
Sexual Medicine RECOVERY OF ERECTILE FUNCTION AFTER NERVE-SPARING RP WITH NIGHTLY LOW-DOSE SILDENAFIL BANNOWSKY et al. Associate Editor Michael G. Wyllie Editorial Board Ian Eardley, UK Jean Fourcroy,
Long-term efficacy and compliance of intracorporeal (IC) injection for erectile dysfunction following radical prostatectomy: SHIM (IIEF-5) analysis
 injection for erectile dysfunction following radical prostatectomy: SHIM (IIEF-5) analysis") (2003) 15, 318 322 & 2003 Nature Publishing Group All rights reserved 0955-9930/03 $25.00 www.nature.com/ijir Long-term efficacy and compliance of intracorporeal (IC) injection for erectile dysfunction
(2003) 15, 318 322 & 2003 Nature Publishing Group All rights reserved 0955-9930/03 $25.00 www.nature.com/ijir Long-term efficacy and compliance of intracorporeal (IC) injection for erectile dysfunction
Life after prostate cancer End your frustration. Restore your normalcy. Renew your confidence. Take the next step
 Take the next step Visit EDCure.org to: Take the online ED quiz and get your customized treatment results Find an ED specialist in your area Register for free educational seminars to learn more about treatment
Take the next step Visit EDCure.org to: Take the online ED quiz and get your customized treatment results Find an ED specialist in your area Register for free educational seminars to learn more about treatment
Information for Patients. Priapism. English
 Information for Patients Priapism English Table of contents What is priapism?... 3 What causes priapism?... 3 Diagnosing priapism... 3 Treating priapism... 4 Conservative, first- and second-line treatments...
Information for Patients Priapism English Table of contents What is priapism?... 3 What causes priapism?... 3 Diagnosing priapism... 3 Treating priapism... 4 Conservative, first- and second-line treatments...
GUIDELINES ON ERECTILE DYSFUNCTION
 16 GUIDELINES ON ERECTILE DYSFUNCTION E. Wespes (chairman), E. Amar, D. Hatzichristou, Dr. F. Montorsi, J. Pryor, Y. Vardi Eur Urol 2002;41:1-5 1. Background, definition and classification Male erectile
16 GUIDELINES ON ERECTILE DYSFUNCTION E. Wespes (chairman), E. Amar, D. Hatzichristou, Dr. F. Montorsi, J. Pryor, Y. Vardi Eur Urol 2002;41:1-5 1. Background, definition and classification Male erectile
LONG-TERM INTRACAVERNOUS THERAPY RESPONDERS CAN POTENTIALLY SWITCH TO SILDENAFIL CITRATE AFTER RADICAL PROSTATECTOMY
 ADULT UROLOGY LONG-TERM INTRACAVERNOUS THERAPY RESPONDERS CAN POTENTIALLY SWITCH TO SILDENAFIL CITRATE AFTER RADICAL PROSTATECTOMY RUPESH RAINA, MILTON M. LAKIN, ASHOK AGARWAL, SANDRA AUSMUNDSON, DROGO
ADULT UROLOGY LONG-TERM INTRACAVERNOUS THERAPY RESPONDERS CAN POTENTIALLY SWITCH TO SILDENAFIL CITRATE AFTER RADICAL PROSTATECTOMY RUPESH RAINA, MILTON M. LAKIN, ASHOK AGARWAL, SANDRA AUSMUNDSON, DROGO
Erectile dysfunction. By Anas Hindawi Supervised by Dr Khalid AL Sayyid
 Erectile dysfunction By Anas Hindawi Supervised by Dr Khalid AL Sayyid ED is the persistent/recurrent inability to attain and/or maintain a penile erection rigid enough for satisfactory sexual intercourse
Erectile dysfunction By Anas Hindawi Supervised by Dr Khalid AL Sayyid ED is the persistent/recurrent inability to attain and/or maintain a penile erection rigid enough for satisfactory sexual intercourse
Opinion: Yes. PDE-5 inhibitors should be used post radical prostatectomy as erection function rehabilitation?
 Difference of opinion Vol. 43 (3): 385-389, May - June, 2017 doi: 10.1590/S1677-5538.IBJU.2017.03.03 PDE-5 inhibitors should be used post radical prostatectomy as erection function rehabilitation? Opinion:
Difference of opinion Vol. 43 (3): 385-389, May - June, 2017 doi: 10.1590/S1677-5538.IBJU.2017.03.03 PDE-5 inhibitors should be used post radical prostatectomy as erection function rehabilitation? Opinion:
Erectile Dysfunction
 Erectile Dysfunction WWW.RN.ORG Reviewed May, 2017, Expires May, 2019 Provider Information and Specifics available on our Website Unauthorized Distribution Prohibited 2017 RN.ORG, S.A., RN.ORG, LLC Erectile
Erectile Dysfunction WWW.RN.ORG Reviewed May, 2017, Expires May, 2019 Provider Information and Specifics available on our Website Unauthorized Distribution Prohibited 2017 RN.ORG, S.A., RN.ORG, LLC Erectile
ERECTILE DYSFUNCTION TREATMENTS
 ERECTILE DYSFUNCTION TREATMENTS Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Medical Coverage
ERECTILE DYSFUNCTION TREATMENTS Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Medical Coverage
Erectile Dysfunction National Kidney and Urologic Diseases Information Clearinghouse
 Erectile Dysfunction National Kidney and Urologic Diseases Information Clearinghouse National Institute of Diabetes and Digestive and Kidney Diseases NATIONAL INSTITUTES OF HEALTH U.S. Department of Health
Erectile Dysfunction National Kidney and Urologic Diseases Information Clearinghouse National Institute of Diabetes and Digestive and Kidney Diseases NATIONAL INSTITUTES OF HEALTH U.S. Department of Health
Patient Information ERECTILE DYSFUNCTION. Department of Urology
 ERECTILE DYSFUNCTION What is erectile dysfunction? Erectile dysfunction (impotence) is the inability to get or keep an erection sufficient for sexual intercourse. One in ten men (10%) suffer from impotence
ERECTILE DYSFUNCTION What is erectile dysfunction? Erectile dysfunction (impotence) is the inability to get or keep an erection sufficient for sexual intercourse. One in ten men (10%) suffer from impotence
Prostate cancer. Treatments Side effects and management in the community setting
 Prostate cancer Treatments Side effects and management in the community setting Kristoffer Ohlin CNS Urology Janice Minter Lead Cancer Nurse St George s Hospital Agenda Prostate cancer treatments Radiotherapy
Prostate cancer Treatments Side effects and management in the community setting Kristoffer Ohlin CNS Urology Janice Minter Lead Cancer Nurse St George s Hospital Agenda Prostate cancer treatments Radiotherapy
Quality of life issues after treatment for prostate cancer
 Quality of life issues after treatment for prostate cancer Christopher Saigal MD, MPH Associate Professor, UCLA Department of Urology Definition of Health not merely the absence of disease or infirmity,
Quality of life issues after treatment for prostate cancer Christopher Saigal MD, MPH Associate Professor, UCLA Department of Urology Definition of Health not merely the absence of disease or infirmity,
response to MUSE was 70% in the office setting, compared to a 57% success rate when used at home.
 Original Article EARLY USE OF MUSE AFTER RP RAINA et al. The early use of transurethral alprostadil after radical prostatectomy potentially facilitates an earlier return of erectile function and successful
Original Article EARLY USE OF MUSE AFTER RP RAINA et al. The early use of transurethral alprostadil after radical prostatectomy potentially facilitates an earlier return of erectile function and successful
for ED and LUTS/BPH Pierre Sarkis, M.D. Assistant Professor Fellow of the European Board of Urology
 Tadalafil 5 mg once daily for ED and LUTS/BPH Pierre Sarkis, M.D. Assistant Professor Fellow of the European Board of Urology Why this conference? Not promotional but educational The pharmacist regularly
Tadalafil 5 mg once daily for ED and LUTS/BPH Pierre Sarkis, M.D. Assistant Professor Fellow of the European Board of Urology Why this conference? Not promotional but educational The pharmacist regularly
Preserved Postoperative Penile Size Correlates Well with Maintained Erectile Function after Bilateral Nerve-Sparing Radical Retropubic Prostatectomy
 european urology 52 (2007) 702 707 available at www.sciencedirect.com journal homepage: www.europeanurology.com Prostate Cancer Preserved Postoperative Penile Size Correlates Well with Maintained Erectile
european urology 52 (2007) 702 707 available at www.sciencedirect.com journal homepage: www.europeanurology.com Prostate Cancer Preserved Postoperative Penile Size Correlates Well with Maintained Erectile
Life after prostate cancer. End your frustration. Restore your normalcy. Renew your confidence. Erectile dysfunction and male incontinence
 Life after prostate cancer End your frustration. Restore your normalcy. Renew your confidence. Erectile dysfunction and male incontinence Welcome This brochure is designed to help you learn more about
Life after prostate cancer End your frustration. Restore your normalcy. Renew your confidence. Erectile dysfunction and male incontinence Welcome This brochure is designed to help you learn more about
Prospective analysis of penile length changes after radical prostatectomy
 Prospective analysis of penile length changes after radical prostatectomy Boback M. Berookhim, Christian J. Nelson*, Brian Kunzel, John P. Mulhall and Joseph B. Narus Male Sexual and Reproductive Medicine
Prospective analysis of penile length changes after radical prostatectomy Boback M. Berookhim, Christian J. Nelson*, Brian Kunzel, John P. Mulhall and Joseph B. Narus Male Sexual and Reproductive Medicine
Male Sexuality and Cancer. Anne Katz, PhD, RN CancerCare Manitoba August 29, 2012
 Male Sexuality and Cancer Anne Katz, PhD, RN CancerCare Manitoba August 29, 2012 Objectives! Recognize the sexual side effects of treatment for cancer in men! Discuss treatment modalities for these problems!
Male Sexuality and Cancer Anne Katz, PhD, RN CancerCare Manitoba August 29, 2012 Objectives! Recognize the sexual side effects of treatment for cancer in men! Discuss treatment modalities for these problems!
Sexual Function for Men with Spinal Cord Injury
 Sexual Function for Men with Spinal Cord Injury A spinal cord injury (SCI) affects a man's sexuality both physically and psychologically. The type and level of injury both can play a role on the impact
Sexual Function for Men with Spinal Cord Injury A spinal cord injury (SCI) affects a man's sexuality both physically and psychologically. The type and level of injury both can play a role on the impact
Is This Really a Fair Debate? 2013 MFMER slide-2
 Sex Rehab after Radical Prostatectomy: Is it Really Justified? Con Position Landon Trost, MD Assistant Professor of Urology Mayo Clinic, Rochester, MN ISSM 16 th World Meeting on Sexual Medicine October
Sex Rehab after Radical Prostatectomy: Is it Really Justified? Con Position Landon Trost, MD Assistant Professor of Urology Mayo Clinic, Rochester, MN ISSM 16 th World Meeting on Sexual Medicine October
SEXUAL RELATIONSHIPS AND FERTILITY FOLLOWING SPINAL CORD INJURY
 NATIONAL SPINAL INJURIES CENTRE STOKE MANDEVILLE HOSPITAL A HANDOUT PREPARED FOR PATIENTS BY SPINAL OUTPATIENT SERVICES SEXUAL RELATIONSHIPS AND FERTILITY FOLLOWING SPINAL CORD INJURY Mary Leonard, RGN.
NATIONAL SPINAL INJURIES CENTRE STOKE MANDEVILLE HOSPITAL A HANDOUT PREPARED FOR PATIENTS BY SPINAL OUTPATIENT SERVICES SEXUAL RELATIONSHIPS AND FERTILITY FOLLOWING SPINAL CORD INJURY Mary Leonard, RGN.
Clinic for urology, pediatric urology and andrology. Penile diseases. Dr. Arne Hauptmann
 Clinic for urology, pediatric urology and andrology JUSTUS- LIEBIG UNVERISTY GIESSEN Penile diseases Dr. Arne Hauptmann Clinic for urology, pediatric urology and andrology University Giessen und Marburg
Clinic for urology, pediatric urology and andrology JUSTUS- LIEBIG UNVERISTY GIESSEN Penile diseases Dr. Arne Hauptmann Clinic for urology, pediatric urology and andrology University Giessen und Marburg
Understanding Men s Sexuality and Intimacy After Bladder Cancer Webinar. Part III: Treatments for Improvement
 Understanding Men s Sexuality and Intimacy After Bladder Cancer Webinar Tuesday December 8, 2015 Part III: Treatments for Improvement Presented by Section A: Medical and behavioral treatments to improve
Understanding Men s Sexuality and Intimacy After Bladder Cancer Webinar Tuesday December 8, 2015 Part III: Treatments for Improvement Presented by Section A: Medical and behavioral treatments to improve
ERECTILE DYSFUNCTION. & Current Therapies. GP Conference, Rotorua 7-10 June 2012
 ERECTILE DYSFUNCTION & Current Therapies GP Conference, Rotorua 7-10 June 2012 Jan Burns & Annie Woodsford Jan: EN, RCpN, BHSc, RPN (USA),MHSc, Member of the Sexual Medicine Society Urology Nurse Specialist
ERECTILE DYSFUNCTION & Current Therapies GP Conference, Rotorua 7-10 June 2012 Jan Burns & Annie Woodsford Jan: EN, RCpN, BHSc, RPN (USA),MHSc, Member of the Sexual Medicine Society Urology Nurse Specialist
GUIDELINES ON ERECTILE DYSFUNCTION
 GUIDELINES ON ERECTILE DYSFUNCTION (Text updated March 2005) E. Wespes (chairman), E. Amar, D. Hatzichristou, K. Hatzimouratidis, F. Montorsi, J. Pryor, Y. Vardi 88 Erectile Dysfunction Eur Urol 2001;40:97-101
GUIDELINES ON ERECTILE DYSFUNCTION (Text updated March 2005) E. Wespes (chairman), E. Amar, D. Hatzichristou, K. Hatzimouratidis, F. Montorsi, J. Pryor, Y. Vardi 88 Erectile Dysfunction Eur Urol 2001;40:97-101
Immediate penile prosthesis insertion after failed T shunt and snake maneuver in patient with prolonged priapism
 Immediate penile prosthesis insertion after failed T shunt and snake maneuver in patient with prolonged priapism Evangelos Zacharakis PhD, FRCS, FECSM, FEAA Consultant Urological Surgeon St Peter s Anrology
Immediate penile prosthesis insertion after failed T shunt and snake maneuver in patient with prolonged priapism Evangelos Zacharakis PhD, FRCS, FECSM, FEAA Consultant Urological Surgeon St Peter s Anrology
DATE BIO# NAME: Last First Middle REFERRING PHYSICIAN NAME: REFERRING PHYSICIAN SPECIALTY (Urologist, Internist, etc.): PRIMARY CARE PHYSICIAN NAME:
: PRIMARY CARE PHYSICIAN NAME:") DATE BIO# ERECTILE DYSFUNCTION QUESTIONNAIRE NAME: Last First Middle BIRTHDATE: OCCUPATION: REFERRING PHYSICIAN NAME: REFERRING PHYSICIAN SPECIALTY (Urologist, Internist, etc.): PRIMARY CARE PHYSICIAN
DATE BIO# ERECTILE DYSFUNCTION QUESTIONNAIRE NAME: Last First Middle BIRTHDATE: OCCUPATION: REFERRING PHYSICIAN NAME: REFERRING PHYSICIAN SPECIALTY (Urologist, Internist, etc.): PRIMARY CARE PHYSICIAN
Molecular Mechanisms of Vacuum Therapy in Penile Rehabilitation: A Novel Animal Study
 EUROPEAN UROLOGY 58 (2010) 773 780 available at www.sciencedirect.com journal homepage: www.europeanurology.com Sexual Medicine Molecular Mechanisms of Vacuum Therapy in Penile Rehabilitation: A Novel
EUROPEAN UROLOGY 58 (2010) 773 780 available at www.sciencedirect.com journal homepage: www.europeanurology.com Sexual Medicine Molecular Mechanisms of Vacuum Therapy in Penile Rehabilitation: A Novel
Managing the Patient with Erectile Dysfunction: What Would You Do?
 Managing the Patient with Erectile Dysfunction: What Would You Do? Florida A & M University College of Pharmacy and Pharmaceutical Sciences 42 nd Annual Clinical Symposium Wayne A. Sampson, M.D. Cross
Managing the Patient with Erectile Dysfunction: What Would You Do? Florida A & M University College of Pharmacy and Pharmaceutical Sciences 42 nd Annual Clinical Symposium Wayne A. Sampson, M.D. Cross
Phosphodiesterase Type 5 Inhibitors Quantity Limit Program Summary
 Phosphodiesterase Type 5 Inhibitors Quantity Limit Program Summary FDA APPROVED INDICATIONS AND DOSAGE 1-4,23 Agent FDA Approved Dosage and Administration Indication Cialis (tadalafil) (ED) ED; As needed:
Phosphodiesterase Type 5 Inhibitors Quantity Limit Program Summary FDA APPROVED INDICATIONS AND DOSAGE 1-4,23 Agent FDA Approved Dosage and Administration Indication Cialis (tadalafil) (ED) ED; As needed:
Peyronie s Disease and Erectile Dysfunction: A New Perspective-What Every Urologist and Man Should Know About Peyronie s Disease
 Peyronie s Disease and Erectile Dysfunction: A New Perspective-What Every Urologist and Man Should Know About Peyronie s Disease Commentary Drogo K. Montague Center for Genitourinary Reconstruction, Glickman
Peyronie s Disease and Erectile Dysfunction: A New Perspective-What Every Urologist and Man Should Know About Peyronie s Disease Commentary Drogo K. Montague Center for Genitourinary Reconstruction, Glickman
Physiology and disturbances of sexual functions Prof. Jolanta Słowikowska-Hilczer, M.D., Ph.D.
 Physiology and disturbances of sexual functions Prof. Jolanta Słowikowska-Hilczer, M.D., Ph.D. Department of Andrology and Reproductive Endocrinology Medical University of Łódź, Poland SEXUALITY Sexuality
Physiology and disturbances of sexual functions Prof. Jolanta Słowikowska-Hilczer, M.D., Ph.D. Department of Andrology and Reproductive Endocrinology Medical University of Łódź, Poland SEXUALITY Sexuality
LONG-TERM EFFECT OF SILDENAFIL CITRATE ON ERECTILE DYSFUNCTION AFTER RADICAL PROSTATECTOMY: 3-YEAR FOLLOW-UP
 ADULT UROLOGY LONG-TERM EFFECT OF SILDENAFIL CITRATE ON ERECTILE DYSFUNCTION AFTER RADICAL PROSTATECTOMY: 3-YEAR FOLLOW-UP RUPESH RAINA, MILTON M. LAKIN, ASHOK AGARWAL, RAKESH SHARMA, KUSH K. GOYAL, DROGO
ADULT UROLOGY LONG-TERM EFFECT OF SILDENAFIL CITRATE ON ERECTILE DYSFUNCTION AFTER RADICAL PROSTATECTOMY: 3-YEAR FOLLOW-UP RUPESH RAINA, MILTON M. LAKIN, ASHOK AGARWAL, RAKESH SHARMA, KUSH K. GOYAL, DROGO
Strategies for preventing erectile dysfunction induced by radical prostatectomy
 Contemporary Urology Archive November 2002 Strategies for preventing erectile dysfunction induced by radical prostatectomy By Edward D. Kim, MD Despite refinements in technique, erectile dysfunction remains
Contemporary Urology Archive November 2002 Strategies for preventing erectile dysfunction induced by radical prostatectomy By Edward D. Kim, MD Despite refinements in technique, erectile dysfunction remains
Managing the Impact of Prostate Cancer Treatments on Sexual Function & Intimacy. Christine Zarowski, RN BSN Sexual Health Clinician
 Managing the Impact of Prostate Cancer Treatments on Sexual Function & Intimacy Christine Zarowski, RN BSN Sexual Health Clinician OVERVIEW 1) What is normal male sexual function? 2) Erectile dysfunction
Managing the Impact of Prostate Cancer Treatments on Sexual Function & Intimacy Christine Zarowski, RN BSN Sexual Health Clinician OVERVIEW 1) What is normal male sexual function? 2) Erectile dysfunction
UNDERSTANDING PEYRONIE S DISEASE
 Learn more about Peyronie s disease and how Chesapeake Urology s Men s Sexual Health specialists can help restore your quality of life. Call 877-422-8237 to schedule an appointment with a urologist or
Learn more about Peyronie s disease and how Chesapeake Urology s Men s Sexual Health specialists can help restore your quality of life. Call 877-422-8237 to schedule an appointment with a urologist or
Clinical Policy Title: Penile implant after prostate cancer surgery
 Clinical Policy Title: Penile implant after prostate cancer surgery Clinical Policy Number: 13.03.06 Effective Date: October 1, 2017 Initial Review Date: September 21, 2017 Most Recent Review Date: October
Clinical Policy Title: Penile implant after prostate cancer surgery Clinical Policy Number: 13.03.06 Effective Date: October 1, 2017 Initial Review Date: September 21, 2017 Most Recent Review Date: October
Gerald Brock Professor of Surgery University of Western Ontario
 Treatment Induced Erectile Dysfunction Gerald Brock Professor of Surgery University of Western Ontario 1 1 2 Should you believe in Rehab? 3 3 Should you believe in Rehab? Avoidance Education related to
Treatment Induced Erectile Dysfunction Gerald Brock Professor of Surgery University of Western Ontario 1 1 2 Should you believe in Rehab? 3 3 Should you believe in Rehab? Avoidance Education related to
National Kidney and Urologic Diseases Information Clearinghouse
 Erectile Dysfunction National Kidney and Urologic Diseases Information Clearinghouse What is erectile dysfunction (ED)? Erectile dysfunction is a condition in which a man is unable to get or keep an erection
Erectile Dysfunction National Kidney and Urologic Diseases Information Clearinghouse What is erectile dysfunction (ED)? Erectile dysfunction is a condition in which a man is unable to get or keep an erection
Sexual function and dysfunction in men
 Georges A. de Boccard,, M.D. Consultant Urologist F.E.B.U. Sexual function and dysfunction in men Geneva Foundation for Medical Education and Research Training Course in Reproductive Health / Sexual Health
Georges A. de Boccard,, M.D. Consultant Urologist F.E.B.U. Sexual function and dysfunction in men Geneva Foundation for Medical Education and Research Training Course in Reproductive Health / Sexual Health
MEDICAL POLICY SUBJECT: ERECTILE DYSFUNCTION. POLICY NUMBER: CATEGORY: Miscellaneous
 MEDICAL POLICY PAGE: 1 OF: 8 If the member's subscriber contract excludes coverage for a specific service it is not covered under that contract. In such cases, medical policy criteria are not applied.
MEDICAL POLICY PAGE: 1 OF: 8 If the member's subscriber contract excludes coverage for a specific service it is not covered under that contract. In such cases, medical policy criteria are not applied.
Friday, 11 January 13. Sexual Anatomy
 Friday, 11 January 13 Sexual Anatomy Friday, 11 January 13 Friday, 11 January 13 Friday, 11 January 13 Friday, 11 January 13 Fallopian Tube Ovary Uterus Bladder Cervix Pubic bone Clitoris Urethra Rectum
Friday, 11 January 13 Sexual Anatomy Friday, 11 January 13 Friday, 11 January 13 Friday, 11 January 13 Friday, 11 January 13 Fallopian Tube Ovary Uterus Bladder Cervix Pubic bone Clitoris Urethra Rectum
ED treatments: PDE5 inhibitors, injections and vacuum devices
 ED treatments: PDE5 inhibitors, injections and vacuum devices Martin Steggall Clinical Nurse Specialist (Erectile Dysfunction and Premature Ejaculation) Barts Health NHS Trust; Associate Dean, Director
ED treatments: PDE5 inhibitors, injections and vacuum devices Martin Steggall Clinical Nurse Specialist (Erectile Dysfunction and Premature Ejaculation) Barts Health NHS Trust; Associate Dean, Director
Sexual Anatomy. Monday, 30 March 2009
 Sexual Anatomy 1 2 3 Fallopian Tube Ovary Uterus Bladder Cervix Pubic bone Clitoris Urethra Rectum Vagina Anus G Spot 4 Variety of Vulvae 5 Bladder Corpus Cavernosum Rectum Seminal Vesicle Prostate Glans
Sexual Anatomy 1 2 3 Fallopian Tube Ovary Uterus Bladder Cervix Pubic bone Clitoris Urethra Rectum Vagina Anus G Spot 4 Variety of Vulvae 5 Bladder Corpus Cavernosum Rectum Seminal Vesicle Prostate Glans
Male Pelvic Health following Pelvic Surgery
 Male Pelvic Health following Pelvic Surgery Radical Pelvic Surgery Associated Sexual Dysfunction Pathophysiology Post Radical Prostatectomy (RP) Sexual Dysfunctions Erectile dysfunction (ED) Anejaculation
Male Pelvic Health following Pelvic Surgery Radical Pelvic Surgery Associated Sexual Dysfunction Pathophysiology Post Radical Prostatectomy (RP) Sexual Dysfunctions Erectile dysfunction (ED) Anejaculation
Symptom management for prostate cancer Contents
 13 11 20 Information and support Symptom management for prostate cancer Contents Urinary problems Erection problems Other changes to sexuality Restoring your sex life Other side effects Information last
13 11 20 Information and support Symptom management for prostate cancer Contents Urinary problems Erection problems Other changes to sexuality Restoring your sex life Other side effects Information last
Sexuality for the Man With Cancer Cancer, sex, and sexuality
 Sexuality for the Man With Cancer Cancer, sex, and sexuality When you first learned you had cancer, you probably thought mostly about survival. But after awhile, other questions may have started coming
Sexuality for the Man With Cancer Cancer, sex, and sexuality When you first learned you had cancer, you probably thought mostly about survival. But after awhile, other questions may have started coming
MMM. Topic The use of Tadalafil 5mg daily for the treatment of BPH-LUTS
 Dr Tan & Partners MMM Vol. 1 No. 1 Morbidity & Mortality Meeting 14 th November 2014 Introduction Topic The use of Tadalafil 5mg daily for the treatment of BPH-LUTS Tadalafil 5mg daily is a well established
Dr Tan & Partners MMM Vol. 1 No. 1 Morbidity & Mortality Meeting 14 th November 2014 Introduction Topic The use of Tadalafil 5mg daily for the treatment of BPH-LUTS Tadalafil 5mg daily is a well established
Find your ED cure End your frustration. Renew your confidence. Feel complete. Take the next steps. Erectile dysfunction and heart disease
 Take the next steps Visit your general practitioner or cardiologist to learn more about your risk for cardiovascular disease. Visit EDCure.org to: Take the online ED quiz and get your customized treatment
Take the next steps Visit your general practitioner or cardiologist to learn more about your risk for cardiovascular disease. Visit EDCure.org to: Take the online ED quiz and get your customized treatment
Prostate cancer and your sex life
 Prostate cancer and your sex life 2 Prostate cancer and your sex lfe About this booklet This booklet is for men and their partners who want to know how prostate cancer and its treatment can affect their
Prostate cancer and your sex life 2 Prostate cancer and your sex lfe About this booklet This booklet is for men and their partners who want to know how prostate cancer and its treatment can affect their
Erectile Dysfunction (ED) or Impotence
 or Impotence") Erectile Dysfunction (ED) or Impotence Introduction Impotence is a consistent inability to sustain an erection sufficient for sexual intercourse. Medical professionals often use the term "erectile dysfunction"
Erectile Dysfunction (ED) or Impotence Introduction Impotence is a consistent inability to sustain an erection sufficient for sexual intercourse. Medical professionals often use the term "erectile dysfunction"
GUIDELINES ON PRIAPISM
 GUIDELINES ON PRIAPISM (Text update March 2015) A. Salonia, I. Eardley, F. Giuliano, I. Moncada, K. Hatzimouratidis Eur Urol 2014 Feb;65(2):480-9 Introduction Priapism is a pathological condition representing
GUIDELINES ON PRIAPISM (Text update March 2015) A. Salonia, I. Eardley, F. Giuliano, I. Moncada, K. Hatzimouratidis Eur Urol 2014 Feb;65(2):480-9 Introduction Priapism is a pathological condition representing
Symptom Management. Sexual Health Information for Men with Cancer
 Symptom Management Sexual Health Information for Men with Cancer Table of Contents 3 The Male Reproductive System 5 Managing Erection Problems Vacuum Erection Devices................... 9 Oral Medicine
Symptom Management Sexual Health Information for Men with Cancer Table of Contents 3 The Male Reproductive System 5 Managing Erection Problems Vacuum Erection Devices................... 9 Oral Medicine
QUESTIONS TO ASK A UROLOGIST
 QUESTIONS TO ASK A UROLOGIST For the patient: You should review these questions and determine if the answers would satisfy a better understanding of what to expect and ease your concerns. If there are
QUESTIONS TO ASK A UROLOGIST For the patient: You should review these questions and determine if the answers would satisfy a better understanding of what to expect and ease your concerns. If there are
Sexual Health after Spinal Cord Injury
 Authors: SCIRE Community Team Reviewed by: Lesley Houle, RN and Rachel Nicoletti, RN(C), BSN Last updated: June 12, 2018 Sexual health changes are common after spinal cord injury (SCI). This page provides
Authors: SCIRE Community Team Reviewed by: Lesley Houle, RN and Rachel Nicoletti, RN(C), BSN Last updated: June 12, 2018 Sexual health changes are common after spinal cord injury (SCI). This page provides
SURGERY FOR PEYRONIE S DISEASE. PEYRONIE S DISEASE WITHOUT IMPOTENCE Exposure and Mobilization of Dorsal Nerves and Vessels
 SURGERY FOR 25 PEYRONIE S DISEASE PEYRONIE S DISEASE WITHOUT Exposure and Mobilization of Dorsal Nerves and Vessels FIG. 25-1. Most surgeons use a degloving procedure via a circumferential skin incision
SURGERY FOR 25 PEYRONIE S DISEASE PEYRONIE S DISEASE WITHOUT Exposure and Mobilization of Dorsal Nerves and Vessels FIG. 25-1. Most surgeons use a degloving procedure via a circumferential skin incision
MODULE 4: ERECTILE DYSFUNCTION
 MODULE 4: ERECTILE DYSFUNCTION KEYWORDS: Erectile dysfunction, phosphodiesterase inhibitors, sexual dysfunction LEARNING OBJECTIVES At the end of this clerkship, the medical student will be able to: 1.
MODULE 4: ERECTILE DYSFUNCTION KEYWORDS: Erectile dysfunction, phosphodiesterase inhibitors, sexual dysfunction LEARNING OBJECTIVES At the end of this clerkship, the medical student will be able to: 1.
Understanding your treatment options for male stress urinary incontinence and erectile dysfunction
 Understanding your treatment options for male stress urinary incontinence and erectile dysfunction Male Stress Urinary Incontinence and Erectile Dysfunction What causes male stress urinary incontinence
Understanding your treatment options for male stress urinary incontinence and erectile dysfunction Male Stress Urinary Incontinence and Erectile Dysfunction What causes male stress urinary incontinence
Erectile Dysfunction Prior Authorization with Quantity Limit Criteria Program Summary
 Prior Authorization with Quantity Limit Criteria Program Summary Objective The intent of the prior authorization (PA) program for (ED) is to ensure appropriate selection of patients for treatment according
Prior Authorization with Quantity Limit Criteria Program Summary Objective The intent of the prior authorization (PA) program for (ED) is to ensure appropriate selection of patients for treatment according
Diagnosis and management of Peyronie s disease: an evidence-based review
 18 Diagnosis and management of Peyronie s disease: an evidence-based review ERIC CHUNG Peyronie s disease presents a considerable therapeutic dilemma because of an incomplete understanding of the pathophysiology
18 Diagnosis and management of Peyronie s disease: an evidence-based review ERIC CHUNG Peyronie s disease presents a considerable therapeutic dilemma because of an incomplete understanding of the pathophysiology