MNT for ESLSD. Presented by AEYSHA NASIR
|
|
|
- Chester Hardy
- 5 years ago
- Views:
Transcription
1 MNT for ESLSD Presented by AEYSHA NASIR
2 Where is the Liver? Upper right quadrant, beneath the diaphragm Largest internal organ Weighs ~ 1500 grams
3 Liver Functions Stores glucose as glycogen or releases glycogen in response to blood sugar levels Break down lipids (bile) Break down proteins into ammonia Produces blood proteins (albumin, prothrombin, fibrinogen) Detoxifies blood of alcohol Secretes drugs such as antibiotics into bile Inactivates thyroid and steroid hormones Secretes bilirubin (left over pigment from break down of hemoglobin)

4 Liver Functions (cont d) Stores Vitamin A, B12, D, E and K Stores iron and copper Remove old blood cells and some bacteria from blood Activates Vitamin D produced by the skin

5 ESLD Chronic liver failure, also called end-stage liver disease, progresses over months, years, or decades. Most often, chronic liver failure is the result of cirrhosis, a condition in which scar tissue replaces healthy liver tissue until the liver cannot function adequately. Patients with abnormal liver function who develop ascites, variceal hemorrhage, hepatic encephalopathy, or renal impairment are considered to have end-stage liver disease (ESLD)
6 Complications of ESLD
7 Hepatic encephalopathy Hepatic encephalopathy is defined as a complex neuropsychiatric syndrome marked by personality changes, intellectual impairment, and an altered level of consciousness Hepatic encephalopathy is associated with hepatocyte loss and dysfunction, and portosystemic shunting, which allow nitrogenous substances derived from the gut to adversely affect brain function It is a common and distressing complication, developing in 30% to 45% of patients with decompensated cirrhosis
8 Hepatic encephalopathy resulting from cirrhosis is classified according to the severity of clinical manifestations, the time course, and the presence of precipitating factors In the past, a diet high in animal protein was implicated in worsening serum ammonia levels and the symptoms of HE. However, many patients with ESLD have proteincalorie malnutrition, and protein restriction is generally not recommended ( Canadian Family Physician, janvier 2016)
9 Spontaneous bacterial peritonitis Spontaneous bacterial peritonitis is defined as an ascitic fluid infection with a polymorpho nuclear cell count of 250 cell/mm3 or greater and an ascitic fluid culture positive for bacteria, in the absence of a surgically treatable source. Spontaneous bacterial peritonitis is the most common and severe infection in patients with cirrhosis: up to 30% of patients with cirrhosis develop SBP,11 with a mortality rate ranging between 30% and 50% (canadian physician society 2016)
10 Primary prophylaxis of SBP has been associated with a decreased risk of bacterial infection and decreased mortality in patients considered to be at high risk of SBP, which includes patients with a history of variceal bleeding or ascites fluid protein levels below 1.0 g/dl (canadian physician society 2016)
11 Esophageal varices Esophageal varices, a direct consequence of increased portal pressure, are a common complication of cirrhosis, and their presence correlates with the severity of liver disease. Approximately 50% of patients with cirrhosis develop esophageal varices, and of these onethird will develop a variceal bleed.19 With any episode of active bleeding, there is a 30% chance of mortality and a 70% risk of hemorrhage recurrence within 1 year (canadian physician society 2016)
12 liver inflammation pain liver necrosis nausea vomiting anorexia constipation Wt loss fatigue nutrition metabolism portal pressure venous pressure hypoglycemia ascites splenomegaly anemia leukopenia edema EV hormone metabolism bilirubin metabolism total liver failure HE coma death thrombocytopenia erectile dysfunction menstrual disorders jaundice bilirubinemia urobilingen intestinal bile clay-colored stool dark urine bleeding Vit. K absorption
13 Nutritional Concerns
14 In CLD there occurs a decrease in branched chain aminoacids/aromatic amino acids (BCAA/AAA) ratio, as observed in sepsis or major trauma During overnight fast, keto-genesis and gluconeogenesis are increased (lipids represent75% of the calories expended during this period), causing an increased AA consumption by the muscles This condition is also observed in healthy subjects after 3 days of fasting, but in cirrhosis, this process is accelerated
15 Pancreatic dysfunction, increased lipolysis, fatty acids oxidation and ketogenesis lead to a reduction of plasma triglycerides, phospholipids, cholesterol, apoproteins and polyunsaturated fatty acids This decrease is proportional to the severity of the liver disease and the degree of mal-nutrition, and is associated with decreased survival and is considered an independent predictor of mortality in cirrhosis
16 Micronutrient deficits are prevalent as well.deficiency of water-soluble vitamins, especially group B vitamins, is common in cirrhosis Deficiency of fat-soluble vitamins has been reported, in the presence of steatorrhea associated with cholestasis and in the bile salt deficiency
17 Thiamine deficiency is quite common Decreased intake, absorption and hepatic reserves may contribute to it Alcohol intake also reduces intestinal absorption of thiamine and pre-vents metabolization in its active substrate. Thiamine deficiency may lead to Wernicke encephalopathy and Korsakoff dementia
18 Vitamin B12 deficiency is mainly related to the decrease of its liver reserves. Serum levels may be increased, but tis-sue levels are decreased deficiency is associated with anemia, glossitis and neurological symptoms Folic acid deficiency develops faster in cirrhotic patients due to decreased hepatic storage levels
19 Retinol deficiency is related with decreased absorption and impaired hepatic mobilization It can cause dermatitis, night blindness or photophobia and increased risk of neoplastic disorders, including hepatocellular carcinoma A retrospective study reported that the majority of liver disease patients being considered for liver transplantation present with vitamin A and D deficiencies Because high doses of vitamin A are potentially hepatotoxic, care must be taken to avoid excessive supplementation
20 Vitamin K deficiency is caused by decreased liver storage levels and is associated with increased risk of bleeding
21 Vitamin D deficiency results from ingest reduction, decreased absorption (due to cholestatic disease or portal hypertension enteropathy) Since vitamin D is hydroxylated in the liver to produce calcidiol, patients with severe parenchymal or obstructive hepatic disease may have reduced production of this metabolite The majority of the liver must be dysfunctional before calcidiol synthesis is reduced. Thus, these patients rarely manifest biochemical or histological evidence of osteomalacia, unless concomitant nutritional deficiency or interruption of the enterohepatic circulation occurs. Extremely low serum levels of vitamin D are associated with increased mortality in patients with chronic liver disease
22 Zinc and selenium deficiency have been described inpatients with alcoholic and non-alcoholic liver disease. Zinc deficiency is caused by intake reduction (to which contributes a diet with restriction of animal origin protein), impaired intestinal absorption and treatment with diuretics This deficiency may increase ammonia levels in circulation, increasing the risk of HE and may also induce anorexia, dysfunction of the immune system and dysgeusia, which further decreases its intake
23
24 Inadequate nutrients intake was seen under a variety of reasons, such as loss of appetite caused by tristimania, anorexia, drug side effects and satiety caused by less gastrointestinal peristalsis and gastric restrictive expansion caused by large volume ascites In addition, acute gastroesophageal varicose hemorrhage followed by long time fasting is also common in clinical practice ( Plauth 2017)
25 Professor Plauth pointed out in a research that many clinicians make a prescription of low protein diet to avoid encephalopathy, which leads to deterioration of nutritional status. However, it is not necessary and lack of being evidence-based in most cases (plauth 2017) One other important factor is the presence of impaired absorption function due to portal hypertension, which frequently accompanied with portal hypertensive gastrointestinal disease or peptic ulcer disease.
26 Under this condition, there is gradually arising impaired absorption of fat-soluble vitamins such as A, D, E and K, intestinal mucosal atrophy and conditional bacterial infections, followed by hypercatabolic status and higher mortality Finally, iatrogenic factors such as the multiple hospitalizations, pending examinations and procedures (e.g., paracentesis) should not be ignored as well

27
28 Etiologies of Malnutrition in Cirrhosis Decreased Intake Anorexia Early satiety Ascites Altered mental status/encephalopathy Frequent hospitalizations Decreased Absorption Inadequate bile flow Bacterial overgrowth Pancreatic insufficiency Metabolic alterations Iatrogenic Factors Overzealous dietary restrictions Frequent Paracentesis Diuresis (micronutrient losses) Lactulose therapy Used with permission from the University of Virginia Health System Nutrition Support Traineeship Syllabus
29 Nutritional Assessment
30 Assessment of nutritional status For complete assessment of nutritional status information, three important parameters required are: Energy balance Body composition Tissue function
31 Energy Balance A systematic dietary recall obtained by a skilled dietitian will provide adequate information in most cases. For hospitalized patients, a food diary should be completed, weighing the food consumed, and appropriate tables for food composition should be used for calculation of proportions of different nutrients.
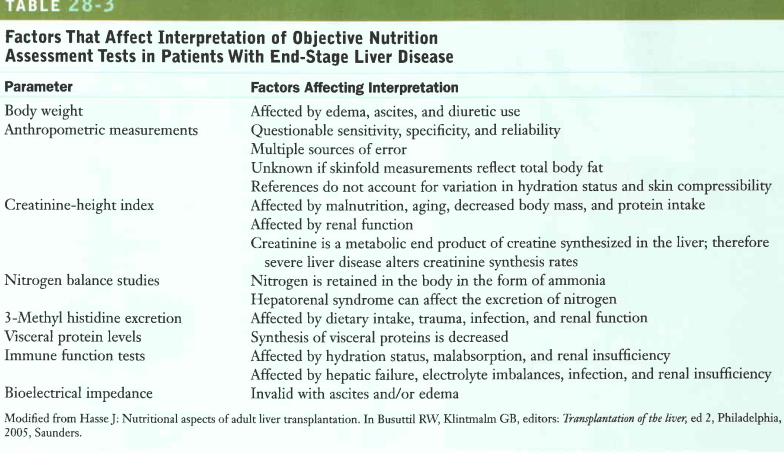
32 Body Composition Body composition of cirrhotic patients is assessed by indirect techniques, such as anthropometry, urinary creatinine excretion It would be desirable to directly assess fat mass and fat free mass components, total body water, extracellular water and body cell or muscle mass.
33 Anthropometry is the accurate tool to detect the protein depleted status of cirrhotic patients. Skinfold anthropometry is the best indirect method of assessing body fat stores in these patients. The value of urinary creatinine excretion also helps to estimate muscle or body cell mass as creatine is synthesized by the liver. Elevation in serum creatinine is a common laboratory finding for patients with cirrhosis and can indicate the presence of either an acute kidney injury (AKI) or chronic kidney disease (CKD)

34 Tissue function Circulating concentrations of many visceral plasma proteins (albumin, prealbumin, retin01-binding protein) are highly affected by the presence of liver disease, excessive alcohol consumption and inflammatory states Immune status, which is often considered a functional test of malnutrition, may be affected by hypersplenism, abnormal immunologic reactivity and alcohol abuse At present, total lymphocyte count and CD8 cell count seem to be of prognostic value in malnourished patients with alcoholic liver disease In nutrition intervention trials, results from lymphocyte PHA stimulation index or skin anergy test were not useful for the detection of nutritional changes. ( ESPEN)

35 Subjective Global Assessment
36
37 Conclusion Based on expert consensus, a dry weight or usual weight be used instead of actual weight in predictive equations to determine energy and protein in patients with cirrhosis and hepatic failure, due to complications of ascites, intravascular volume depletion, edema, portal hypertension, and hypo albuminemia ASPEN 2016 suggest that nutrition regimens avoid restricting protein in patients with liver failure, using the same recommendations as for other critically ill patients ( Aspen 2016)

38 Nutrition in the Management of ESLD and its Complications

39 Nutrition in the Management of ESLD and its Complications
40 Nutrition in the complications of ESLD Calories (Cal) Fat Protein (PT) Carbohydrate (CHO) Sodium (Na) Fluid Vitamins
41 Total Cal= kcal/kg Fat=30-35% of total Cal PT=1g/kg/d ( g/kg) (Aspen 2016) ESPEN Consensus group : req g/kg/d low PT diet may worsen HE Plauth et al. 2017
42 Nutritional Management of HE Historical treatment theories Protein Restriction BCAA supplementation Goals of MNT Treatment of PCM associated with ESLD
43 Historical Treatment Theories: Protein Restriction Studies in early 1950 s showed cirrhotic pts given nitrogenous substances developed hepatic precoma Led to introduction of protein restriction Began with 20-40g protein/day Increased by 10g increments q3-5 days as tolerated with clinical recovery Upper limit of g/kg Was thought sufficient to achieve positive nitrogen balance Lack of Valid Evidence Efficacy of restriction never proven within controlled trial
44 Dispelling the Myth Normal Protein Diet for Episodic Hepatic Encephalopathy Cordoba et al. J Hepatol Objective: To test safety of normal-protein diets Randomized, controlled trial in 20 cirrhotic patients with HE 10 patients subjected to protein restriction, followed by progressive increments No protein first 3 days, increasing q3days until 1.2g/kg daily for last 2 days 10 patients followed normal protein diet (1.2g/kg) Both groups received equal calories
45 Dispelling the Myth Results On days 2 and 14: Similar protein synthesis among both groups Protein breakdown higher in low-protein group Conclusion No significant differences in course of hepatic encephalopathy Greater protein breakdown in protein-restricted subjects
46 Protein and HE Considerations Presence of malnutrition in pts with cirrhosis and ESLD clearly established No valid clinical evidence supporting protein restriction in pts with acute HE Higher protein intake required in CHE to maintain positive nitrogen balance Protein intake < 40g/day contributes to malnutrition and worsening HE Increased endogenous protein breakdown NH3 Susceptibiliy to infection increases under such catabolic conditions
47 Proteins Proteins should not be restricted in patients with liver disease unless they become protein intolerant due to encephalopathy Protein intake should be in the range of g/kg/day ( ASPEN 2016, Plauth 2017)
48 [ Proteins. Cont Several studies have shown that a daily protein supply of g/kg/day may be sufficient to prevent negative N 2 balance in cirrhosis With mild stress, this has to increase to 1.5 g/kg/day, and with acute exacerbations of hepatitis or decompensation to 2.0 g/kg/day
49 Proteins. Cont Special attention should be paid to patients on betablockers for prevention of variceal bleeding Beta-blockers increase protein oxidation (an alternative method of protein metabolism without energy production), and may increase protein requirement. patients on propranolol should be placed on the higher end of the protein intake.
50 BCAA Supplementation Effective or Not?
51 Branched Chain Amino Acids (BCAA) Valine Leucine Isoleucine Important fuel sources for skeletal muscle during periods of metabolic stress Metabolized in muscle & brain, not liver -promote protein synthesis -suppress protein catabolism -substrates for gluconeogenesis Catabolized to L-alanine and L-glutamine in skeletal muscle
52 BCAAs in cirrhosis with acute encephalopathy 7 controlled studies BCAAs group v.s. glucose or non selective AA soln. or lipid groups BCAAs was gave for 2-6 d Post treatment observation period : 4-16 d 201(BCAAs) v.s. 179(isocaloric group) No statistically significant in survival Riggio et al Wahren et al Michel et al Cerra et al Fiaccadori et al Strauss et al Vilstrup et al. 1990
53 Certainly BCAAs don t worsen encephalopathy and may be safely used to maintain an adequate PT intake in subjects at risk of altered mental state BCAAs may be easily used as energy sources, thus improving nitrogen balance and have a beneficial on anorexia. Plauth et al. 2017
54 A multicenter, randomized study, > 1 yr, 174 p t (a) BCAA supplementation group (b) maltodextrins group (equicaloric) (c) lactoalbumin group (equicaloric/nitrogenous) Non-BCAA group
55

56 Long term BCAA supplementation increases survival time and prevents to decrease hospital admission rates.
57 BCAA-enriched formulations can be useful in p t who are intolerant to PT and malnourished, which can improve PT synthesis and reduce post injury catabolism. Nompleggi and Bonkovsky 2014
58 BCAA-enriched soln. increased serum alb. also reduced morbidity and improved the quality of life. BCAAs strongly activate mtor signaling in liver, which is the cellular nutrition sensor for PT translation initiation. Poon et al, 2014 Nishitani et al, 2014
59 ASPEN 2016 There is no evidence to suggest that a formulation enriched in BCAA improves patient outcomes compared with standard whole-protein formulations in critically ill patients with liver disease. The rationale for use of BCAAs in the treatment of hepatic encephalopathy in liver failure is based on their reduced concentrations in liver failure, competing for binding sites in the central nervous system with aromatic amino acids, and their stimulatory effect on ammonia detoxification to glutamine
60 Findings from randomized outpatient trials suggest that long-term (12 and 24 months) nutrition supplementation with oral BCAA granules may be useful in slowing the progression of hepatic disease and/or failure and prolonging event-free surviva In patients with hepatic encephalopathy already receiving first-line therapy (antibiotics and lactulose), there is no evidence to date that adding BCAAs will further improve mental status or coma grade (ASPEN 2016)
61 Caffeine s Effect Caffeine is present in coffee, tea, chocolate, cola, and some over-the-counter medications Caffeine is metabolized through the liver. However caffeine itself is not directly harmful to the liver Some people may experience a rapid heartbeat and/or palpitations from caffeine consumption Excessive intake of caffeine in patients with chronic liver disease at increased risk for osteoporosis and bone fractures
62 Na Restriction For mobilization of ascites, Na has to be restricted to less than the daily losses. If patients have high urinary Na and are able to excrete a water load, they will respond to Na restriction alone, and will lose g fluid for every gram Na deficit. A no added salt regimen together with avoiding salty food will result in a diet containing 50 meq Na daily
63 Fluid Restriction Fluid restriction of all patients with ascites is inappropriate. Patients should drink, but not to excess. Water restriction to treat hyponatremia is indicated only if this is severe. Fluid restriction to less than 1 liter daily is justified only in hyponatremic patients, and only when the serum Na drops below 120 meq/l.

64 Sarah Haynes 2015
65 The management of perioperative nutrition in patients with end stage liver disease undergoing liver transplantation
66 The prevalence of glucose intolerance and insulin resistance is seen in the population of ESLD patients. Many could develop the hepatic diabetes. Overnight fasting, hepatic glycogen stores are depleted in patients with ESLD, presenting increased gluconeogenesis from amino acids and increased lipid peroxidation. At this time, fat becomes their main substrate for energy. As the result, the mobilization of amino acids from the skeletal muscles and visceral proteins is active, demonstrating muscle depletion and decrease in subcutaneous fat
67 Perioperative maintenance of normoglycemia is frequently emphasized to improve surgical outcomes and may be quite important factor to prevent surgical site infection. A research found that surgical site infections were reduced in patients whose HbA1c was <7% (10) HepatoBiliary Surg Nutr 2015
68 adequate preoperative nutritional support ( 7 d) is beneficial to patients with a nutrition risk score (NRS) score at least 5 The ability of oral intake is connected with postoperative mortality. In addition, body mass index (BMI) should be obtained from patient s height and weight. BMI of <18.5 kg/m 2 or the 15th percentile for arm anthropometric measurements often were considered be malnutrition in this population. However, BMI can be inaccurate in the condition of fluid retention or edema
69 Surgery has been associated with hypermetabolism in reported literatures and guidelines The formula of 25 kcal/kg ideal body weight provides an approximate estimate of daily energy requirements. Under conditions of severe stress, requirements may approach 30 kcal/kg ideal body weight and a protein intake of 1.5 g/kg ideal body weight (or approximately 20% of total energy requirements) is generally effective to limit nitrogen losses. Some studies suggest that the degree of hypermetabolism is on average not more than % of predicted, and should not be furnished more than kcal/kg daily in the acute phase of critical severe illness HepatoBiliary Surg Nutr 2015
70 mixed-fuel system of both carbohydrate and fat is suggested to provide energy in post-olt period. Usually, 70% of non-protein calories are given as carbohydrates during this phase. In a study of patients in a surgical critical care unit, either 30 kcal/kg adjusted body weight or the REE calculated from the Harris Benedict equation multiplied by 1.5 adequately predicts the nutritional requirements of critically ill surgery HepatoBiliary Surg Nutr 2015
71 Additional several meta-analysis show more clearly the evidence of feeding started within h of surgery. Recent clinical trial performed in 346 liver transplant patients has gotten a conclusion that Bacterial sepsis occurred in 5.9% of patients who received tube feeding within 48 hours of surgery compared with 21% in patients who started tube feeding after 48 hours HepatoBiliary Surg Nutr 2015
72 for those patients in hemodynamic instability requiring vasopressor agents, once the hemodynamic is stable for more than 24 hours and bowl function is in recovery, feeding should commence from at ml/h rate with a progressive increase to reach the full goal within 2-3 days of post-operation exception of contraindication for enteral nutrition HepatoBiliary Surg Nutr 2015

73
74 Thank you
NUTRITIONAL OPTIMIZATION IN PRE LIVER TRANSPLANT PATIENTS
 NUTRITIONAL OPTIMIZATION IN PRE LIVER TRANSPLANT PATIENTS ACHIEVING NUTRITIONAL ADEQUACY Dr N MURUGAN Consultant Hepatologist Apollo Hospitals Chennai NUTRITION IN LIVER FAILURE extent of problem and consequences
NUTRITIONAL OPTIMIZATION IN PRE LIVER TRANSPLANT PATIENTS ACHIEVING NUTRITIONAL ADEQUACY Dr N MURUGAN Consultant Hepatologist Apollo Hospitals Chennai NUTRITION IN LIVER FAILURE extent of problem and consequences
Luis S. Marsano, MD Professor of Medicine Division of Gastroenterology, Hepatology and Nutrition University of Louisville and Louisville VAMC 2015
 Luis S. Marsano, MD Professor of Medicine Division of Gastroenterology, Hepatology and Nutrition University of Louisville and Louisville VAMC 2015 Protein-calorie malnutrition (PCM) is extremely common
Luis S. Marsano, MD Professor of Medicine Division of Gastroenterology, Hepatology and Nutrition University of Louisville and Louisville VAMC 2015 Protein-calorie malnutrition (PCM) is extremely common
Nutritional Issues In Advanced Liver Disease. Corrie Clark, RDN, LD
 Nutritional Issues In Advanced Liver Disease Corrie Clark, RDN, LD Objectives List specific points to keep in mind when assessing the nutritional status of patients with advanced liver disease. Describe
Nutritional Issues In Advanced Liver Disease Corrie Clark, RDN, LD Objectives List specific points to keep in mind when assessing the nutritional status of patients with advanced liver disease. Describe
Nutrition Management of End- Stage Liver Failure
 Nutrition Management of End- Stage Liver Failure Krystel Ouaijan, RDN, MSc Nutrition Support Dietitian in Saint George Hospital UMC PhD in University of Geneva Just few questions https://www.mentimeter.com/s/c1c1be18dc2
Nutrition Management of End- Stage Liver Failure Krystel Ouaijan, RDN, MSc Nutrition Support Dietitian in Saint George Hospital UMC PhD in University of Geneva Just few questions https://www.mentimeter.com/s/c1c1be18dc2
Nutritional Issues in Cholestatic Disease
 THE HOSPITAL FOR SICK CHILDREN Nutritional Issues in Cholestatic Disease NASPGHAN-CPNP Joint Session Binita M. Kamath, MBBChir MRCP MTR Associate Professor Division of Gastroenterology, Hepatology and
THE HOSPITAL FOR SICK CHILDREN Nutritional Issues in Cholestatic Disease NASPGHAN-CPNP Joint Session Binita M. Kamath, MBBChir MRCP MTR Associate Professor Division of Gastroenterology, Hepatology and
LIVER CIRRHOSIS. The liver extracts nutrients from the blood and processes them for later use.
 LIVER CIRRHOSIS William Sanchez, M.D. & Jayant A. Talwalkar, M.D., M.P.H. Advanced Liver Disease Study Group Miles and Shirley Fiterman Center for Digestive Diseases Mayo College of Medicine Rochester,
LIVER CIRRHOSIS William Sanchez, M.D. & Jayant A. Talwalkar, M.D., M.P.H. Advanced Liver Disease Study Group Miles and Shirley Fiterman Center for Digestive Diseases Mayo College of Medicine Rochester,
Nutrition in Liver Disease An overview of the EASL Clinical Practice Guidelines
 Nutrition in Liver Disease An overview of the EASL Clinical Practice Guidelines Marike Bauermeister Registered Dietitian Wits Donald Gordon Medical Centre Malnutrition Malnutrition is a complication in
Nutrition in Liver Disease An overview of the EASL Clinical Practice Guidelines Marike Bauermeister Registered Dietitian Wits Donald Gordon Medical Centre Malnutrition Malnutrition is a complication in
By; Ashraf El Houfi MD MS (pulmonology) MRCP (UK) FRCP (London) EDIC Consultant ICU Dubai Hospital
 MRCP (UK) FRCP (London) EDIC Consultant ICU Dubai Hospital") By; Ashraf El Houfi MD MS (pulmonology) MRCP (UK) FRCP (London) EDIC Consultant ICU Dubai Hospital Introduction The significance of nutrition in hospital setting (especially the ICU) cannot be overstated.
By; Ashraf El Houfi MD MS (pulmonology) MRCP (UK) FRCP (London) EDIC Consultant ICU Dubai Hospital Introduction The significance of nutrition in hospital setting (especially the ICU) cannot be overstated.
Case Study BMIs in the range of are considered overweight. Therefore, F.V. s usual BMI indicates that she was overweight.
 Morgan McFarlane February 26 th, 2013 HHP 439 Professor White Case Study 7.10 1. What is your interpretation of F.V. s clinical data? F.V. s clinical data includes chronic abdominal pain, loose stools,
Morgan McFarlane February 26 th, 2013 HHP 439 Professor White Case Study 7.10 1. What is your interpretation of F.V. s clinical data? F.V. s clinical data includes chronic abdominal pain, loose stools,
Intradialytic Parenteral Nutrition in Hemodialysis Patients. Hamdy Amin, Pharm.D., MBA, BCNSP Riyadh, Saudi Arabia
 Intradialytic Parenteral Nutrition in Hemodialysis Patients Hamdy Amin, Pharm.D., MBA, BCNSP Riyadh, Saudi Arabia Disclosure Information Intradialytic Parenteral Nutrition in Hemodialysis Patients Hamdy
Intradialytic Parenteral Nutrition in Hemodialysis Patients Hamdy Amin, Pharm.D., MBA, BCNSP Riyadh, Saudi Arabia Disclosure Information Intradialytic Parenteral Nutrition in Hemodialysis Patients Hamdy
Evidence Analysis Library Research Project
 Evidence Analysis Library Research Project EAL question: What is the evidence to support the use of supplementing BCAA in patients with cirrhosis to 1) prevent further liver damage or improve liver function;
Evidence Analysis Library Research Project EAL question: What is the evidence to support the use of supplementing BCAA in patients with cirrhosis to 1) prevent further liver damage or improve liver function;
Role of Nutritional Support in the Treatment of Alcoholic Liver Disease
 Riunione Monotematica AISF Alcoholic Liver Disease: The New Challenge Roma, 4-6 Ottobre 2017 Role of Nutritional Support in the Treatment of Alcoholic Liver Disease Esmeralda Capristo Divisione di Patologie
Riunione Monotematica AISF Alcoholic Liver Disease: The New Challenge Roma, 4-6 Ottobre 2017 Role of Nutritional Support in the Treatment of Alcoholic Liver Disease Esmeralda Capristo Divisione di Patologie
Nutrition. Chapter 45. Reada Almashagba
 Nutrition Chapter 45 1 Nutrition: - Nutrient are organic substances found in food and are required for body function - No one food provide all essential nutrient Major function of nutrition: providing
Nutrition Chapter 45 1 Nutrition: - Nutrient are organic substances found in food and are required for body function - No one food provide all essential nutrient Major function of nutrition: providing
Clinical Manifestations. Principles of Nutrition Assessment. Significance of nutritional assessment. Nutrition Deficiency States.
 Clinical Manifestations Principles of Nutrition Assessment Audis Bethea, Pharm.D. Assistant Professor Therapeutics I December 5 & 9, 2003 Impaired cellular immunity Impaired wound healing End organ dysfunction
Clinical Manifestations Principles of Nutrition Assessment Audis Bethea, Pharm.D. Assistant Professor Therapeutics I December 5 & 9, 2003 Impaired cellular immunity Impaired wound healing End organ dysfunction
Critical Care case Study: Nutritional Management in the care of Decompensated Cirrhosis and ascites
 Critical Care case Study: Nutritional Management in the care of Decompensated Cirrhosis and ascites Click Becky Schneider to edit Master subtitle style August 2012 Overview Decompensated cirrhosis (ETOH-related),
Critical Care case Study: Nutritional Management in the care of Decompensated Cirrhosis and ascites Click Becky Schneider to edit Master subtitle style August 2012 Overview Decompensated cirrhosis (ETOH-related),
Nutritional Demands of Disease and Trauma
 al Demands of Disease and Trauma Lecture 89 Medical School al Requirements Based on needs to support optimal physiological function Are changed by disease or injury metabolism is altered to prevent further
al Demands of Disease and Trauma Lecture 89 Medical School al Requirements Based on needs to support optimal physiological function Are changed by disease or injury metabolism is altered to prevent further
Neoplastic Disease KNH 406
 Neoplastic Disease KNH 406 Cancer Carcinogenesis - Etiology Genes may be affected by antioxidants, soy, protein, fat, kcal, alcohol Nutritional genomics study of genetic variations that cause different
Neoplastic Disease KNH 406 Cancer Carcinogenesis - Etiology Genes may be affected by antioxidants, soy, protein, fat, kcal, alcohol Nutritional genomics study of genetic variations that cause different
WEEK. MPharm Programme. Liver Biochemistry. Slide 1 of 49 MPHM14 Liver Biochemistry
 MPharm Programme Liver Biochemistry Slide 1 of 49 MPHM Liver Biochemistry Learning Outcomes Assess and evaluate the signs and symptoms of illness Assess and critically appraise a patients medication regimen,
MPharm Programme Liver Biochemistry Slide 1 of 49 MPHM Liver Biochemistry Learning Outcomes Assess and evaluate the signs and symptoms of illness Assess and critically appraise a patients medication regimen,
Nutritional assessments and diagnosis of digestive disorders
 Nutritional assessments and diagnosis of digestive disorders AASER ABDELAZIM Assistant professor of Medical Biochemistry Zagazig University, Egypt University of Bisha, KSA aaserabdelazim@yahoo.com 7 Mal
Nutritional assessments and diagnosis of digestive disorders AASER ABDELAZIM Assistant professor of Medical Biochemistry Zagazig University, Egypt University of Bisha, KSA aaserabdelazim@yahoo.com 7 Mal
following the last documented transfusion; thereafter, evaluate the residual impairment(s).
.") Adult Listings 5.01 Category of Impairments, Digestive System 5.02 Gastrointestinal hemorrhaging from any cause, requiring blood transfusion (with or without hospitalization) of at least 2 units of blood
Adult Listings 5.01 Category of Impairments, Digestive System 5.02 Gastrointestinal hemorrhaging from any cause, requiring blood transfusion (with or without hospitalization) of at least 2 units of blood
Management of Alcoholic Liver Disease. Hafez Fakheri Professor of medicine, Sari, Iran
 Management of Alcoholic Liver Disease Hafez Fakheri Professor of medicine, Sari, Iran Alcoholic Hepatitis Scores DF = (4.6 x [ PT- control PT]) + (bili ) MELD = 10 * ((0.957 * ln(cr)) + (0.378 * ln(bil))
Management of Alcoholic Liver Disease Hafez Fakheri Professor of medicine, Sari, Iran Alcoholic Hepatitis Scores DF = (4.6 x [ PT- control PT]) + (bili ) MELD = 10 * ((0.957 * ln(cr)) + (0.378 * ln(bil))
NUTRITION PLANNING FOR PRE AND POST LIVER TRANSPLANT DAPHNEE.D.K HEAD DEPARTMENT OF DIETETICS APOLLO HOSPITALS (MAIN) CHENNAI
 CHENNAI") NUTRITION PLANNING FOR PRE AND POST LIVER TRANSPLANT DAPHNEE.D.K HEAD DEPARTMENT OF DIETETICS APOLLO HOSPITALS (MAIN) CHENNAI PRE - OPERATIVE Case Presentation Name: Mr. XXX Age: 51yrs Sex: Male No. of
NUTRITION PLANNING FOR PRE AND POST LIVER TRANSPLANT DAPHNEE.D.K HEAD DEPARTMENT OF DIETETICS APOLLO HOSPITALS (MAIN) CHENNAI PRE - OPERATIVE Case Presentation Name: Mr. XXX Age: 51yrs Sex: Male No. of
Nutritional Demands of Disease and Trauma
 Nutritional Demands of Disease and Trauma Lecture 89 2000 Northwestern University Medical School Nutritional Requirements Based on needs to support optimal physiological function Are changed by disease
Nutritional Demands of Disease and Trauma Lecture 89 2000 Northwestern University Medical School Nutritional Requirements Based on needs to support optimal physiological function Are changed by disease
ENTERAL NUTRITION IN THE CRITICALLY ILL
 ENTERAL NUTRITION IN THE CRITICALLY ILL 1 Ebb phase Flow phase acute response (catabolic) adoptive response (anabolic) 2 3 Metabolic Response to Stress (catabolic phase) Glucose and Protein Metabolism
ENTERAL NUTRITION IN THE CRITICALLY ILL 1 Ebb phase Flow phase acute response (catabolic) adoptive response (anabolic) 2 3 Metabolic Response to Stress (catabolic phase) Glucose and Protein Metabolism
Alpha-1 Antitrypsin Deficiency: Liver Disease
 Alpha-1 Antitrypsin Deficiency: Liver Disease Who is at risk to develop Alpha-1 liver disease? Alpha-1 liver disease may affect children and adults who have abnormal Alpha-1 antitrypsin genes. Keys to
Alpha-1 Antitrypsin Deficiency: Liver Disease Who is at risk to develop Alpha-1 liver disease? Alpha-1 liver disease may affect children and adults who have abnormal Alpha-1 antitrypsin genes. Keys to
Controversies in Management of Portal Hypertension and Cirrhosis Complications in the Transplant Candidate
 Controversies in Management of Portal Hypertension and Cirrhosis Complications in the Transplant Candidate Patrick Northup, MD, FAASLD, FACG Medical Director, Liver Transplantation University of Virginia
Controversies in Management of Portal Hypertension and Cirrhosis Complications in the Transplant Candidate Patrick Northup, MD, FAASLD, FACG Medical Director, Liver Transplantation University of Virginia
Nutritional Pathology SCBM341: General Pathology
 Nutritional Pathology SCBM341: General Pathology Assistance Professor Amornrat N.Jensen, Ph.D. Department of Pathobiology School of Science, Mahidol University amornrat.nar@mahidol.ac.th Nutrients: Chemicals
Nutritional Pathology SCBM341: General Pathology Assistance Professor Amornrat N.Jensen, Ph.D. Department of Pathobiology School of Science, Mahidol University amornrat.nar@mahidol.ac.th Nutrients: Chemicals
Renal Care and Liver Disease: Disease Trajectory and Hospice Eligibility
 Renal Care and Liver Disease: Disease Trajectory and Hospice Eligibility Terri L. Maxwell PhD, APRN VP, Strategic Initiatives Weatherbee Resources/HEN Course Materials & Disclosure Course materials including
Renal Care and Liver Disease: Disease Trajectory and Hospice Eligibility Terri L. Maxwell PhD, APRN VP, Strategic Initiatives Weatherbee Resources/HEN Course Materials & Disclosure Course materials including
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Accelerated intravascular coagulation and fibrinolysis (AICF) in liver disease, 390 391 Acid suppression in liver disease, 403 404 ACLF.
Index Note: Page numbers of article titles are in boldface type. A Accelerated intravascular coagulation and fibrinolysis (AICF) in liver disease, 390 391 Acid suppression in liver disease, 403 404 ACLF.
To see a description of the Academy Recommendation Rating Scheme (Strong, Fair, Weak, Consensus, Insufficient Evidence) visit the EAL.
 visit the EAL.") WWW.ANDEAL.ORG HEART FAILURE HF: EXECUTIVE SUMMARY OF RECOMMENDATIONS (2017) Executive Summary of Recommendations Below are the major recommendations and ratings for the Academy of Nutrition and Dietetics
WWW.ANDEAL.ORG HEART FAILURE HF: EXECUTIVE SUMMARY OF RECOMMENDATIONS (2017) Executive Summary of Recommendations Below are the major recommendations and ratings for the Academy of Nutrition and Dietetics
Practical recommendations for the post-bariatric surgery medical management
 Practical recommendations for the post-bariatric surgery medical management Dr L. Favre CHUV Sce Endocrinologie, diabétologie et métabolisme 26.04.2018 Bariatric surgery in Switzerland Multidisciplinary
Practical recommendations for the post-bariatric surgery medical management Dr L. Favre CHUV Sce Endocrinologie, diabétologie et métabolisme 26.04.2018 Bariatric surgery in Switzerland Multidisciplinary
Hepatic Encephalopathy
 Hepatic Encephalopathy John Barber UMassMedical Student, Class of 2019 www.12daysinmarch.com Outline Overview Normal Physiology Pathology Symptoms Diagnosis Treatment Overview Ammonia (NH 3 ) is a byproduct
Hepatic Encephalopathy John Barber UMassMedical Student, Class of 2019 www.12daysinmarch.com Outline Overview Normal Physiology Pathology Symptoms Diagnosis Treatment Overview Ammonia (NH 3 ) is a byproduct
Management of Chronic Liver Failure/Cirrhosis Complications in Hospitals. By: Dr. Kevin Dolehide
 Management of Chronic Liver Failure/Cirrhosis Complications in Hospitals By: Dr. Kevin Dolehide Overview DX Cirrhosis and Prognosis Compensated Decompensated Complications Of Cirrhosis Management Of Complications
Management of Chronic Liver Failure/Cirrhosis Complications in Hospitals By: Dr. Kevin Dolehide Overview DX Cirrhosis and Prognosis Compensated Decompensated Complications Of Cirrhosis Management Of Complications
Esophageal Cancer Treated with Surgery and Radiation Case Study (Evaluation and ADIME Note)
") Esophageal Cancer Treated with Surgery and Radiation Case Study (Evaluation and ADIME Note) Nutritional care plan: N.S. is a 58 yr old male. His serum albumin is below normal with a value of 3.1L (9/5)
Esophageal Cancer Treated with Surgery and Radiation Case Study (Evaluation and ADIME Note) Nutritional care plan: N.S. is a 58 yr old male. His serum albumin is below normal with a value of 3.1L (9/5)
Chronic Hepatic Disease
 Chronic Hepatic Disease 10 th Leading Cause of Death Liver Functions Energy Metabolism Protein Synthesis Solubilization, Transport, and Storage Protects and Clears drugs, damaged cells Causes of Liver
Chronic Hepatic Disease 10 th Leading Cause of Death Liver Functions Energy Metabolism Protein Synthesis Solubilization, Transport, and Storage Protects and Clears drugs, damaged cells Causes of Liver
Introduction to Clinical Nutrition
 M-III Introduction to Clinical Nutrition Donald F. Kirby, MD Chief, Section of Nutrition Division of Gastroenterology 1 Things We Take for Granted Air to Breathe Death Taxes Another Admission Our Next
M-III Introduction to Clinical Nutrition Donald F. Kirby, MD Chief, Section of Nutrition Division of Gastroenterology 1 Things We Take for Granted Air to Breathe Death Taxes Another Admission Our Next
SUPPLEMENTATION ANALYSIS
 SUPPLEMENTATION ANALYSIS WHAT IS CYCLING? Cycling is the process of alternating between supplements and ingredients to maximise results. WHY IS CYCLING IMPORTANT? Everytime you take a drug, medication
SUPPLEMENTATION ANALYSIS WHAT IS CYCLING? Cycling is the process of alternating between supplements and ingredients to maximise results. WHY IS CYCLING IMPORTANT? Everytime you take a drug, medication
Laboratory assessment of nutritional status in children
 Laboratory assessment of nutritional status in children Dr O Kiabilua Block 10 Chemical Pathology department University of Pretoria Malnutrition CHO, proteins, lipids,vitamins, mineral and trace elements
Laboratory assessment of nutritional status in children Dr O Kiabilua Block 10 Chemical Pathology department University of Pretoria Malnutrition CHO, proteins, lipids,vitamins, mineral and trace elements
Alcoholic Liver Disease: A Nutrition Focused Approach to Treatment. By Laura Johnson Montana State Dietetic Intern
 Alcoholic Liver Disease: A Nutrition Focused Approach to Treatment By Laura Johnson Montana State Dietetic Intern OBJECTIVES 1. UNDERSTAND HOW MALNUTRITION IS RELATED TO CIRRHOSIS 2. LEARN AT LEAST ONE
Alcoholic Liver Disease: A Nutrition Focused Approach to Treatment By Laura Johnson Montana State Dietetic Intern OBJECTIVES 1. UNDERSTAND HOW MALNUTRITION IS RELATED TO CIRRHOSIS 2. LEARN AT LEAST ONE
Assessment and monitoring of CKD stages 1-3
 Assessment and monitoring of CKD stages 1-3 Annual Paediatric Nephrouroradiology and Network Symposium 2014 Pearl Pugh Paediatric Renal Dietitian Nottingham Children s Hospital Goals of Dietetic Management
Assessment and monitoring of CKD stages 1-3 Annual Paediatric Nephrouroradiology and Network Symposium 2014 Pearl Pugh Paediatric Renal Dietitian Nottingham Children s Hospital Goals of Dietetic Management
Liver Disease / Pancreatitis Case Study
 Name: Sari Bornstein Liver Disease / Pancreatitis Case Study (Adapted from Clinical Nutrition Case Studies, by Wayne Billon) Mr. G is a 56 yo construction worker. He is recently divorced with three children
Name: Sari Bornstein Liver Disease / Pancreatitis Case Study (Adapted from Clinical Nutrition Case Studies, by Wayne Billon) Mr. G is a 56 yo construction worker. He is recently divorced with three children
Providing Optimal Nutritional Support on the ICU common problems and practical solutions. Pete Turner Specialist Nutritional Support Dietitian
 Providing Optimal Nutritional Support on the ICU common problems and practical solutions Pete Turner Specialist Nutritional Support Dietitian ICU Nutritional Support ACCEPT study showed improved ICU survival
Providing Optimal Nutritional Support on the ICU common problems and practical solutions Pete Turner Specialist Nutritional Support Dietitian ICU Nutritional Support ACCEPT study showed improved ICU survival
Index. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Abdominal pain, enteral therapy in acute pancreatitis and, 812 Abscess(es), pancreatic, nutritional support for, 814 815 Acute Physiology and
Note: Page numbers of article titles are in boldface type. A Abdominal pain, enteral therapy in acute pancreatitis and, 812 Abscess(es), pancreatic, nutritional support for, 814 815 Acute Physiology and
IFA Sports Nutrition Certification Test Answer Form
 IFA Sports Nutrition Certification Test Answer Form In order to receive your certification card, take the following test and mail this single page answer sheet in with your check or money order in US funds.
IFA Sports Nutrition Certification Test Answer Form In order to receive your certification card, take the following test and mail this single page answer sheet in with your check or money order in US funds.
Nutrition and Medicine, 2006 Tufts University School of Medicine Nutrition and Acute Illness: Learning Objectives
 Nutrition and Medicine, 2006 Tufts University School of Medicine Nutrition and Acute Illness: Learning Objectives Margo N. Woods, D.Sc. 1. Define protein-calorie, or protein-energy malnutrition (PEM) and
Nutrition and Medicine, 2006 Tufts University School of Medicine Nutrition and Acute Illness: Learning Objectives Margo N. Woods, D.Sc. 1. Define protein-calorie, or protein-energy malnutrition (PEM) and
THE LIVER AND THE GUT
 THE LIVER AND THE GUT Liver & Gut A quintessential relationship One does not work well without the other There is a continuous bidirectional communication between these organs through the bile, hormones,
THE LIVER AND THE GUT Liver & Gut A quintessential relationship One does not work well without the other There is a continuous bidirectional communication between these organs through the bile, hormones,
Biochemical parameters
 Biochemical parameters Urea The liver produces urea if amino acids break down. Urea production is bigger after a protein rich meal and when endogenous catabolism is increased (infections, internal bleedings,
Biochemical parameters Urea The liver produces urea if amino acids break down. Urea production is bigger after a protein rich meal and when endogenous catabolism is increased (infections, internal bleedings,
Slide 1 THE LIVER AND THE GUT. Slide 2 Liver & Gut. Slide 3 Gut Health For Detoxing
 Slide 1 THE LIVER AND THE GUT Slide 2 Liver & Gut A quintessential relationship One does not work well without the other There is a continuous bidirectional communication between these organs through the
Slide 1 THE LIVER AND THE GUT Slide 2 Liver & Gut A quintessential relationship One does not work well without the other There is a continuous bidirectional communication between these organs through the
Gastroenterology and Feeding Issues in Fanconi Anemia
 Gastroenterology and Feeding Issues in Fanconi Anemia Sarah Jane Schwarzenberg, MD Pediatric Gastroenterology, Hepatology and Nutrition August 12, 2012 GI problems in FA 5% have gastrointestinal tract
Gastroenterology and Feeding Issues in Fanconi Anemia Sarah Jane Schwarzenberg, MD Pediatric Gastroenterology, Hepatology and Nutrition August 12, 2012 GI problems in FA 5% have gastrointestinal tract
ICU NUTRITION UPDATE : ESPEN GUIDELINES Mirey Karavetian Assistant Professor Zayed University
 ICU NUTRITION UPDATE : ESPEN GUIDELINES 2018 Mirey Karavetian Assistant Professor Zayed University http://www.espen.org/files/espen- Guidelines/ESPEN_Guideline_on_clinical_nutrition_in_-ICU.pdf Medical
ICU NUTRITION UPDATE : ESPEN GUIDELINES 2018 Mirey Karavetian Assistant Professor Zayed University http://www.espen.org/files/espen- Guidelines/ESPEN_Guideline_on_clinical_nutrition_in_-ICU.pdf Medical
LLL Session - Nutritional support in renal disease
 ESPEN Congress Leipzig 2013 LLL Session - Nutritional support in renal disease Peritoneal dialysis D. Teta (CH) Nutrition Support in Patients undergoing Peritoneal Dialysis (PD) Congress ESPEN, Leipzig
ESPEN Congress Leipzig 2013 LLL Session - Nutritional support in renal disease Peritoneal dialysis D. Teta (CH) Nutrition Support in Patients undergoing Peritoneal Dialysis (PD) Congress ESPEN, Leipzig
Copyright 2014 ChaBiotech. All Rights Reserved. 차의과학대학교분당차병원소화기내과이주호, MD, PhD
 Copyright 2014 ChaBiotech. All Rights Reserved. 차의과학대학교분당차병원소화기내과이주호, MD, PhD Contents 1. Prevalence of Malnutrition in End Stage Liver Disease 2. Assessment of Malnutrition in Liver cirrhosis 3. Prognosis
Copyright 2014 ChaBiotech. All Rights Reserved. 차의과학대학교분당차병원소화기내과이주호, MD, PhD Contents 1. Prevalence of Malnutrition in End Stage Liver Disease 2. Assessment of Malnutrition in Liver cirrhosis 3. Prognosis
The patient s cirrhosis is most likely caused from her Hepatitis C diagnosis.
 Lisa Nguyen Medical Nutrition Therapy March 18, 2013 Cirrhosis of the Liver with Resulting Hepatic Encephalopathy 1. The liver is an extremely complex organ that as a particularly important role in nutrient
Lisa Nguyen Medical Nutrition Therapy March 18, 2013 Cirrhosis of the Liver with Resulting Hepatic Encephalopathy 1. The liver is an extremely complex organ that as a particularly important role in nutrient
Surgical Nutrition for the Cardiothoracic Patient. Stephanie Kunioki RD, CNSC, LD Memorial Hermann TMC
 Surgical Nutrition for the Cardiothoracic Patient Stephanie Kunioki RD, CNSC, LD Memorial Hermann TMC Financial Disclosures NONE Declared PROPER NUTRITION Surgical Effects on Nutrition Intake & Status
Surgical Nutrition for the Cardiothoracic Patient Stephanie Kunioki RD, CNSC, LD Memorial Hermann TMC Financial Disclosures NONE Declared PROPER NUTRITION Surgical Effects on Nutrition Intake & Status
Ascites Management. Atif Zaman, MD MPH Oregon Health & Science University Professor of Medicine Division of Gastroenterology and Hepatology
 Ascites Management Atif Zaman, MD MPH Oregon Health & Science University Professor of Medicine Division of Gastroenterology and Hepatology Disclosure 1. The speaker Atif Zaman, MD MPH have no relevant
Ascites Management Atif Zaman, MD MPH Oregon Health & Science University Professor of Medicine Division of Gastroenterology and Hepatology Disclosure 1. The speaker Atif Zaman, MD MPH have no relevant
UNIVERSITY OF PNG SCHOOL OF MEDICINE AND HEALTH SCIENCES DIVISION OF BASIC MEDICAL SCIENCES Discipline of Biochemistry and Molecular Biology
 UNIVERSITY OF PNG SCHOOL OF MEDICINE AND HEALTH SCIENCES DIVISION OF BASIC MEDICAL SCIENCES Discipline of Biochemistry and Molecular Biology 1 PBL SEMINAR ACUTE & CHRONIC ETHANOL EFFECTS An Overview Sites
UNIVERSITY OF PNG SCHOOL OF MEDICINE AND HEALTH SCIENCES DIVISION OF BASIC MEDICAL SCIENCES Discipline of Biochemistry and Molecular Biology 1 PBL SEMINAR ACUTE & CHRONIC ETHANOL EFFECTS An Overview Sites
Metabolic diseases of the liver
 Metabolic diseases of the liver Central role in metabolism Causes and mechanisms of dysfunction Clinical patterns of metabolic disease Clinical approach to problem-solving Specific disorders Liver s central
Metabolic diseases of the liver Central role in metabolism Causes and mechanisms of dysfunction Clinical patterns of metabolic disease Clinical approach to problem-solving Specific disorders Liver s central
EDUCATION PRACTICE. Management of Refractory Ascites. Clinical Scenario. The Problem
 CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2005;3:1187 1191 EDUCATION PRACTICE Management of Refractory Ascites ANDRÉS CÁRDENAS and PERE GINÈS Liver Unit, Institute of Digestive Diseases, Hospital Clínic,
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2005;3:1187 1191 EDUCATION PRACTICE Management of Refractory Ascites ANDRÉS CÁRDENAS and PERE GINÈS Liver Unit, Institute of Digestive Diseases, Hospital Clínic,
Liver Disease. By: Michael Martins
 Liver Disease By: Michael Martins Recently I have been getting a flurry of patients that have some serious liver complications. This week s literature review will be the dental management of the patients
Liver Disease By: Michael Martins Recently I have been getting a flurry of patients that have some serious liver complications. This week s literature review will be the dental management of the patients
Routine Clinic Lab Studies
 Routine Lab Studies Routine Clinic Lab Studies With all lab studies, a Tacrolimus level will be obtained. These drug levels are routinely assessed to ensure that there is enough or not too much anti-rejection
Routine Lab Studies Routine Clinic Lab Studies With all lab studies, a Tacrolimus level will be obtained. These drug levels are routinely assessed to ensure that there is enough or not too much anti-rejection
Nutrition and Liver Diseases. Carla Vartanian
 Nutrition and Liver Diseases Carla Vartanian Functions of the Liver The liver is the main metabolic organ in the body and weighs about 1.5 kg. Only 10-20% of functioning liver is required to sustain life.
Nutrition and Liver Diseases Carla Vartanian Functions of the Liver The liver is the main metabolic organ in the body and weighs about 1.5 kg. Only 10-20% of functioning liver is required to sustain life.
World Health Organization. Western Pacific Region
 Basic modules for hepatitis 1 Basic Module 1 Liver anatomy and physiology 2 Position of liver Midline Located in right upper abdomen Protected by the right rib cage Right upper Measures: 12 15 cm in vertical
Basic modules for hepatitis 1 Basic Module 1 Liver anatomy and physiology 2 Position of liver Midline Located in right upper abdomen Protected by the right rib cage Right upper Measures: 12 15 cm in vertical
Interpreting Liver Function Tests
 PSH Clinical Guidelines Statement 2017 Interpreting Liver Function Tests Dr. Asad A Chaudhry Consultant Hepatologist, Chaudhry Hospital, Gujranwala, Pakistan. Liver function tests (LFTs) generally refer
PSH Clinical Guidelines Statement 2017 Interpreting Liver Function Tests Dr. Asad A Chaudhry Consultant Hepatologist, Chaudhry Hospital, Gujranwala, Pakistan. Liver function tests (LFTs) generally refer
KETOGENIC DIET ISMAIL HALAHLEH, MSC. نقیب اخصاي یي التغذیة الفلسطینیین
 KETOGENIC DIET ISMAIL HALAHLEH, MSC. نقیب اخصاي یي التغذیة الفلسطینیین INTRODUCTION WHAT IS KETOGENIC DIET???? KETOGENIC DIET The ketogenic diet (KD) is a diet that is high in fat, low in carbohydrate,
KETOGENIC DIET ISMAIL HALAHLEH, MSC. نقیب اخصاي یي التغذیة الفلسطینیین INTRODUCTION WHAT IS KETOGENIC DIET???? KETOGENIC DIET The ketogenic diet (KD) is a diet that is high in fat, low in carbohydrate,
Liver failure &portal hypertension
 Liver failure &portal hypertension Objectives: by the end of this lecture each student should be able to : Diagnose liver failure (acute or chronic) List the causes of acute liver failure Diagnose and
Liver failure &portal hypertension Objectives: by the end of this lecture each student should be able to : Diagnose liver failure (acute or chronic) List the causes of acute liver failure Diagnose and
Optimizing Physical Performance: The Science of Supplementation
 Optimizing Physical Performance: The Science of Supplementation There are many different supplements marketed as performance enhancers in the world of sports nutrition. With athletes trying to find an
Optimizing Physical Performance: The Science of Supplementation There are many different supplements marketed as performance enhancers in the world of sports nutrition. With athletes trying to find an
Nutrition and Dietetics in the Normal Patient
 Nutrition and Dietetics in the Normal Patient Study Aims Definition Malnutrition Actual body weight Ideal body weight Predicted body weight Nutritional assessement Calculation of nutritional needs Complications
Nutrition and Dietetics in the Normal Patient Study Aims Definition Malnutrition Actual body weight Ideal body weight Predicted body weight Nutritional assessement Calculation of nutritional needs Complications
ESPEN Congress Copenhagen 2016
 ESPEN Congress Copenhagen 2016 THE DIVERSITY OF OBESITY MALNUTRITION IN THE OBESE R. Barazzoni (IT) Malnutrition in the obese patient Rocco Barazzoni Dept of Medical, Surgical and Health Sciences University
ESPEN Congress Copenhagen 2016 THE DIVERSITY OF OBESITY MALNUTRITION IN THE OBESE R. Barazzoni (IT) Malnutrition in the obese patient Rocco Barazzoni Dept of Medical, Surgical and Health Sciences University
Etiology of liver cirrhosis
 Liver cirrhosis 1 Liver cirrhosis Liver cirrhosis is the progressive replacement of normal hepatic cells by fibrous scar tissue, This scarring is accompanied by the loss of viable hepatocytes, which are
Liver cirrhosis 1 Liver cirrhosis Liver cirrhosis is the progressive replacement of normal hepatic cells by fibrous scar tissue, This scarring is accompanied by the loss of viable hepatocytes, which are
Feeding the septic patient How and when? Masterclass ICU nurses
 Feeding the septic patient How and when? Masterclass ICU nurses Case Male, 60 - No PMH - L 1.74 m and W 85 kg Pneumococcal pneumonia Stable hemodynamics - No AKI MV in prone position (PEEP 16 - FiO2 60%)
Feeding the septic patient How and when? Masterclass ICU nurses Case Male, 60 - No PMH - L 1.74 m and W 85 kg Pneumococcal pneumonia Stable hemodynamics - No AKI MV in prone position (PEEP 16 - FiO2 60%)
Substrates in clinical nutrition Ilze Jagmane
 Substrates in clinical nutrition Ilze Jagmane Latvian Society of Parenteral and Enteral Nutrition September, 2013 Introduction Food contains one or more of the following nutrients: Water Carbohydrate Lipids
Substrates in clinical nutrition Ilze Jagmane Latvian Society of Parenteral and Enteral Nutrition September, 2013 Introduction Food contains one or more of the following nutrients: Water Carbohydrate Lipids
Management of Ascites and Hepatorenal Syndrome. Florence Wong University of Toronto. June 4, /16/ Gore & Associates: Consultancy
 Management of Ascites and Hepatorenal Syndrome Florence Wong University of Toronto June 4, 2016 6/16/2016 1 Disclosures Gore & Associates: Consultancy Sequana Medical: Research Funding Mallinckrodt Pharmaceutical:
Management of Ascites and Hepatorenal Syndrome Florence Wong University of Toronto June 4, 2016 6/16/2016 1 Disclosures Gore & Associates: Consultancy Sequana Medical: Research Funding Mallinckrodt Pharmaceutical:
Ingvar Bosaeus, MD, Sahlgrenska University Hospital, Goteborg, Sweden
 Cachexia in Cancer Ingvar Bosaeus, MD, Sahlgrenska University Hospital, Goteborg, Sweden Severe, progressive malnutrition and wasting often is seen in advanced cancer, with weight loss long associated
Cachexia in Cancer Ingvar Bosaeus, MD, Sahlgrenska University Hospital, Goteborg, Sweden Severe, progressive malnutrition and wasting often is seen in advanced cancer, with weight loss long associated
ESPEN Congress Florence 2008
 ESPEN Congress Florence 2008 PN Guidelines presentation PN Guidelines in pancreas diseases L. Gianotti (Italy) ESPEN Guidelines on Parenteral Nutrition: Pancreas L.Gianotti, R.Meier, D.N.Lobo, C.Bassi,
ESPEN Congress Florence 2008 PN Guidelines presentation PN Guidelines in pancreas diseases L. Gianotti (Italy) ESPEN Guidelines on Parenteral Nutrition: Pancreas L.Gianotti, R.Meier, D.N.Lobo, C.Bassi,
Clinician Blood Panel Results
 Page 1 of 7 Blood Panel - Markers Out of Range and Patterns (Pattern: proprietary formula using one or more Blood Markers) Blood Panel: Check for Markers that are out of Lab Range ***NOTE*** Only one supplement
Page 1 of 7 Blood Panel - Markers Out of Range and Patterns (Pattern: proprietary formula using one or more Blood Markers) Blood Panel: Check for Markers that are out of Lab Range ***NOTE*** Only one supplement
Nutritional Management of Criticallly Ill Patients with Acute Kidney Injury
 Nutritional Management of Criticallly Ill Patients with Acute Kidney Injury 3 rd International Conference of European Renal Nutrition Working Group of ERA-EDTA T. Alp Ikizler, MD Catherine McLaughlin-Hakim
Nutritional Management of Criticallly Ill Patients with Acute Kidney Injury 3 rd International Conference of European Renal Nutrition Working Group of ERA-EDTA T. Alp Ikizler, MD Catherine McLaughlin-Hakim
CASE STUDY ON INPATIENT MALNUTRITION DISCUSSION
 CASE STUDY ON INPATIENT MALNUTRITION Elena Kret-Sudjian MD, PhD, UC Davis Medical Center A 59 year-old white man with a history of diabetes, severe PVD, CKD IV, chronic hepatitis C admitted for non-healing
CASE STUDY ON INPATIENT MALNUTRITION Elena Kret-Sudjian MD, PhD, UC Davis Medical Center A 59 year-old white man with a history of diabetes, severe PVD, CKD IV, chronic hepatitis C admitted for non-healing
4/3/2014. Elizabeth Thompson, PharmD April Understand the importance of the liver and basic physiology.
 Liver Disease Elizabeth Thompson, PharmD thompse@sarmc.org April 2014 Objectives Understand the importance of the liver and basic physiology. Review hepatic disorders Recognize liver function scoring systems
Liver Disease Elizabeth Thompson, PharmD thompse@sarmc.org April 2014 Objectives Understand the importance of the liver and basic physiology. Review hepatic disorders Recognize liver function scoring systems
Pharmaconutrition in PICU. Gan Chin Seng Paediatric Intensivist UMMC
 Pharmaconutrition in PICU Gan Chin Seng Paediatric Intensivist UMMC Pharmaconutrition in Critical Care Unit Gan Chin Seng Paediatric Intensivist UMMC Definition New concept Treatment with specific nutrients
Pharmaconutrition in PICU Gan Chin Seng Paediatric Intensivist UMMC Pharmaconutrition in Critical Care Unit Gan Chin Seng Paediatric Intensivist UMMC Definition New concept Treatment with specific nutrients
Nutritional physiology of the critically ill patient
 Section 1 General Concepts Nutritional physiology of the critically ill patient David C. Frankenfield 1 Introduction Nutritional physiology refers to the role of food and nutrition in the function of the
Section 1 General Concepts Nutritional physiology of the critically ill patient David C. Frankenfield 1 Introduction Nutritional physiology refers to the role of food and nutrition in the function of the
LESSON 2.4 WORKBOOK. Part two: Glucose homeostasis in the blood Un-Storing energy
 DEFINITIONS OF TERMS Fasting A state of abstinence from all food or drinks that provide calories. For a complete list of defined terms, see the Glossary. LESSON 2.4 WORKBOOK Part two: Glucose homeostasis
DEFINITIONS OF TERMS Fasting A state of abstinence from all food or drinks that provide calories. For a complete list of defined terms, see the Glossary. LESSON 2.4 WORKBOOK Part two: Glucose homeostasis
Intensive Care Nutrition. Dr Alan Race BSc(Hons) PhD FRCA
 PhD FRCA") Intensive Care Nutrition Dr Alan Race BSc(Hons) PhD FRCA Objectives 1. What examiners say 2. Definition 3. Assessment 4. Requirements 5. Types of delivery 6. CALORIES Trial 7. Timing 8. Immunomodulation
Intensive Care Nutrition Dr Alan Race BSc(Hons) PhD FRCA Objectives 1. What examiners say 2. Definition 3. Assessment 4. Requirements 5. Types of delivery 6. CALORIES Trial 7. Timing 8. Immunomodulation
PARENTERAL NUTRITION
 PARENTERAL NUTRITION DEFINITION Parenteral nutrition [(PN) or total parenteral nutrition (TPN)] is the intravenous infusion of some or all nutrients for tissue maintenance, metabolic requirements and growth
PARENTERAL NUTRITION DEFINITION Parenteral nutrition [(PN) or total parenteral nutrition (TPN)] is the intravenous infusion of some or all nutrients for tissue maintenance, metabolic requirements and growth
Chronic Kidney Disease
 Chronic Kidney Disease Chronic Kidney Disease (CKD) Guideline (2010) Chronic Kidney Disease CKD: Executive Summary of Recommendations (2010) Executive Summary of Recommendations Below are the major recommendations
Chronic Kidney Disease Chronic Kidney Disease (CKD) Guideline (2010) Chronic Kidney Disease CKD: Executive Summary of Recommendations (2010) Executive Summary of Recommendations Below are the major recommendations
Management of Cirrhosis Related Complications
 Management of Cirrhosis Related Complications Ke-Qin Hu, MD, FAASLD Professor of Clinical Medicine Director of Hepatology University of California, Irvine Disclosure I have no disclosure related to this
Management of Cirrhosis Related Complications Ke-Qin Hu, MD, FAASLD Professor of Clinical Medicine Director of Hepatology University of California, Irvine Disclosure I have no disclosure related to this
Adams Memorial Hospital Decatur, Indiana EXPLANATION OF LABORATORY TESTS
 Adams Memorial Hospital Decatur, Indiana EXPLANATION OF LABORATORY TESTS Your health is important to us! The test descriptions listed below are for educational purposes only. Laboratory test interpretation
Adams Memorial Hospital Decatur, Indiana EXPLANATION OF LABORATORY TESTS Your health is important to us! The test descriptions listed below are for educational purposes only. Laboratory test interpretation
Medicines for Chronic Liver Disease
 UW MEDICINE PATIENT EDUCATION Medicines for Chronic Liver Disease Treating common conditions This handout gives basic information about how the liver works and what happens during liver failure. It describes
UW MEDICINE PATIENT EDUCATION Medicines for Chronic Liver Disease Treating common conditions This handout gives basic information about how the liver works and what happens during liver failure. It describes
Shyana Sadiq DFM 484: MNT Case Study 33: Esophageal Cancer Treated with Surgery and Radiation 10/14/2013
 Shyana Sadiq DFM 484: MNT Case Study 33: Esophageal Cancer Treated with Surgery and Radiation 10/14/2013 I. Understanding the Disease and Pathophysiology 1. Mr. Seyer has been diagnosed with adenocarcinoma
Shyana Sadiq DFM 484: MNT Case Study 33: Esophageal Cancer Treated with Surgery and Radiation 10/14/2013 I. Understanding the Disease and Pathophysiology 1. Mr. Seyer has been diagnosed with adenocarcinoma
Nutritional intervention in hospitalised paediatric patients. Dr Y.K.Amdekar
 Nutritional intervention in hospitalised paediatric patients Dr Y.K.Amdekar Back to basics Suboptimal nutrient intake is always dangerous in health and more so in disease to feed or not to feed is it a
Nutritional intervention in hospitalised paediatric patients Dr Y.K.Amdekar Back to basics Suboptimal nutrient intake is always dangerous in health and more so in disease to feed or not to feed is it a
Role of Branched Chain Amino Acids in Hepatic Encephalopathy
 ORIGINAL ARTICLE (APMC 378) DOI: 10.29054/APMC/17.378 Role of Branched Chain Amino Acids in Hepatic Encephalopathy Umair Ahmed, Aamir Shaukat, Hooria Aamir, Awais Ahmed ABSTRACT Introduction: Hepatic encephalopathy
ORIGINAL ARTICLE (APMC 378) DOI: 10.29054/APMC/17.378 Role of Branched Chain Amino Acids in Hepatic Encephalopathy Umair Ahmed, Aamir Shaukat, Hooria Aamir, Awais Ahmed ABSTRACT Introduction: Hepatic encephalopathy
VITAMIN BASICS VITAMIN WHAT IT DOES TOO LITTLE TOO MUCH SOURCES. Night blindness Total blindness Reduced resistance to infection Can lead to death
 VITAMIN BASICS VITAMIN WHAT IT DOES TOO LITTLE TOO MUCH SOURCES Fat-Soluble Vitamin A Maintains vision Maintains epithelial tissues (skin) Develops immune cells Bone growth Night blindness Total blindness
VITAMIN BASICS VITAMIN WHAT IT DOES TOO LITTLE TOO MUCH SOURCES Fat-Soluble Vitamin A Maintains vision Maintains epithelial tissues (skin) Develops immune cells Bone growth Night blindness Total blindness
Gastrointestinal, Hepatic, and Nutritional Challenges in FA
 Gastrointestinal, Hepatic, and Nutritional Challenges in FA Sarah Jane Schwarzenberg, MD Pediatric Gastroenterology, Hepatology and Nutrition June 29, 2014 GI problems in FA 5% have gastrointestinal tract
Gastrointestinal, Hepatic, and Nutritional Challenges in FA Sarah Jane Schwarzenberg, MD Pediatric Gastroenterology, Hepatology and Nutrition June 29, 2014 GI problems in FA 5% have gastrointestinal tract
Physiological Role: B-vitamins are coenzymes of many enzymes systems of body metabolism. Thiamine {B 1 }
 Food Constituents [continued] Micronutrients B-Vitamins The B group of vitamin {water soluble} includes: Thiamine: vitamin B 1, ant beriberi vitamin. Riboflavin: vitamin B 2. Niacin: nicotinic acid, PP
Food Constituents [continued] Micronutrients B-Vitamins The B group of vitamin {water soluble} includes: Thiamine: vitamin B 1, ant beriberi vitamin. Riboflavin: vitamin B 2. Niacin: nicotinic acid, PP
HEPATIC ENCEPHALOPATHY(HE) AND NUTRITIONAL SUPPORT. Jin-Woo Lee, MD,PhD. Division of Hepatology Inha University Hospital
 AND NUTRITIONAL SUPPORT. Jin-Woo Lee, MD,PhD. Division of Hepatology Inha University Hospital") HEPATIC ENCEPHALOPATHY(HE) AND NUTRITIONAL SUPPORT Jin-Woo Lee, MD,PhD. Division of Hepatology Inha University Hospital Contents 1. Definition and causes of HE 2. Diagnosis and treatment of HE 3. Malnutriton
HEPATIC ENCEPHALOPATHY(HE) AND NUTRITIONAL SUPPORT Jin-Woo Lee, MD,PhD. Division of Hepatology Inha University Hospital Contents 1. Definition and causes of HE 2. Diagnosis and treatment of HE 3. Malnutriton
BETA-BLOCKERS IN CIRRHOSIS.PRO.
 BETA-BLOCKERS IN CIRRHOSIS.PRO. Angela Puente Sánchez. MD PhD Hepatology Unit. Gastroenterology department Marques de Valdecilla University Hospital. Santander INTRODUCTION. Natural history of cirrhosis
BETA-BLOCKERS IN CIRRHOSIS.PRO. Angela Puente Sánchez. MD PhD Hepatology Unit. Gastroenterology department Marques de Valdecilla University Hospital. Santander INTRODUCTION. Natural history of cirrhosis
MALIGNANT CACHEXIA (CACHEXIA ANOREXIA SYNDROME): Overview
: Overview") MALIGNANT CACHEXIA (CACHEXIA ANOREXIA SYNDROME): Overview UNIVERSITY OF PNG SCHOOL OF MEDICINE AND HEALTH SCIENCES DISCIPLINE OF BIOCHEMISTRY & MOLECULAR BIOLOGY PBL MBBS II SEMINAR VJ Temple 1 Cachexia:
MALIGNANT CACHEXIA (CACHEXIA ANOREXIA SYNDROME): Overview UNIVERSITY OF PNG SCHOOL OF MEDICINE AND HEALTH SCIENCES DISCIPLINE OF BIOCHEMISTRY & MOLECULAR BIOLOGY PBL MBBS II SEMINAR VJ Temple 1 Cachexia:
CHAPTER 1. Alcoholic Liver Disease
 CHAPTER 1 Alcoholic Liver Disease Major Lesions of Alcoholic Liver Disease Alcoholic fatty liver - >90% of binge and chronic drinkers Alcoholic hepatitis precursor of cirrhosis Alcoholic cirrhosis end
CHAPTER 1 Alcoholic Liver Disease Major Lesions of Alcoholic Liver Disease Alcoholic fatty liver - >90% of binge and chronic drinkers Alcoholic hepatitis precursor of cirrhosis Alcoholic cirrhosis end
MANAGEMENT OF LIVER CIRRHOSIS: PRACTICE ESSENTIALS AND PATIENT SELF-MANAGEMENT
 MANAGEMENT OF LIVER CIRRHOSIS: PRACTICE ESSENTIALS AND PATIENT SELF-MANAGEMENT Sherona Bau, ACNP The Pfleger Liver Institute 200 UCLA Medical Plaza, Suite 214 Los Angeles, CA 90095 September 30, 2017 I
MANAGEMENT OF LIVER CIRRHOSIS: PRACTICE ESSENTIALS AND PATIENT SELF-MANAGEMENT Sherona Bau, ACNP The Pfleger Liver Institute 200 UCLA Medical Plaza, Suite 214 Los Angeles, CA 90095 September 30, 2017 I
Nutritional Support in Liver Diseases Topic 13
 Nutritional Support in Liver Diseases Topic 13 Module 13.2 Nutritional Support in Chronic Liver Disease Learning Objectives Mathias Plauth, Chair Department of Internal Medicine, Community Hospital Dessau,
Nutritional Support in Liver Diseases Topic 13 Module 13.2 Nutritional Support in Chronic Liver Disease Learning Objectives Mathias Plauth, Chair Department of Internal Medicine, Community Hospital Dessau,
KEY INDICATORS OF NUTRITION RISK
 NUTRITION TOOLS KEY INDICATORS OF Consumes fewer than 2 servings of fruit or fruit juice per day. Consumes fewer than 3 servings of vegetables per day. Food Choices Fruits and vegetables provide dietary
NUTRITION TOOLS KEY INDICATORS OF Consumes fewer than 2 servings of fruit or fruit juice per day. Consumes fewer than 3 servings of vegetables per day. Food Choices Fruits and vegetables provide dietary