Clinical Nutrition. part II
|
|
|
- Felicia James
- 5 years ago
- Views:
Transcription
1 Clinical Nutrition part II Jacek Szopinski MD. PhD Department of General Surgery and Transplantology Collegium Medicum in Bydgoszczy, Nicolaus Copernicus University in Torun, Poland
2 How much energy? 35 kcal/kg IBW 30 kcal/kg IBW 25 kcal/kg IBW 20 kcal/kg IBW Obesity Perioperatively Burns Sepsis Repeted surgery GI fistula Severe malnutrition
3 What is nutrition support? An alternate means of providing nutrients to people who cannot eat any or enough food When is it needed? Illness resulting in inability to take in adequate nutrients by mouth Illness or surgery that results in malfunctioning gastrointestinal tract Two types: Enteral nutrition Parenteral nutrition
4 Nutrition route ENTERAL route always preferable unless contraindications: mechanical ileus, severe shock (non-stabilized), bowel ischemia (even suspected only) IF the enteral route NOT POSSIBLE or at least 60% of daily energy intake can not be acheived -> MIXED ENTERAL AND PARENTERAL NUTRITION PARENTERAL route alone
5 Methods of enteral feeding Sip feeding Tube feeding Nasoenteral tube Tube enterostomy Percuteneous endoscopic jejunostomy (PEG) Fine catheter needle jejunostomy



6 Sip feeding / oral nutritional supplements (ONS)
7 Oral nutritional supplements protein rich (ie. Nutridrink Protein 125 ml) before major non cancer surgery (2x daily/ 5 x days) with immunonutrition (i.e. Cubitan, Impact Enteral) contain: ARG, GLU, nucleotides (2x daily / 5-7 days)
8 Enteral feeding If the gut works use it Nasogastric (NG) Nasojejunal (NJ) Percutaneous Endoscopic Gastrostomy (PEG) Percutaneous Endoscopic Jejunostomy (PEJ) Radiologically Inserted Gastrostomy (RIG) Surgical Gastrostomy Surgical Jejunostomy (JEJ)


9 Nasoenteric tube

10 PEG or G-tube


11 PEG (Percutaneous Endoscopic Gastrostomy)

12 G-tube (gastric tube)
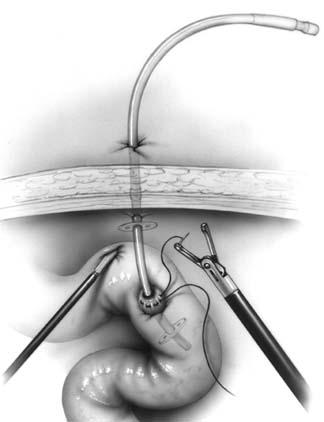

13 Microjejunostomy
14 1. Whole protein formulae (polymeric) - contain intact proteins, and usually include lipids in the form of long chain triglycerides (LCTs), and carbohydrates predominantly as maltodextrins; - require relatively normal gastrointestinal function for digestion and absorption, but can be used successfully in up to 95% of patients on artificial enteral nutrition; - nutrients are not hydrolysed - osmolality reasonably close to the physiological level (about 200 to 350 mosmol/kg). 2. Peptide based formulae (oligomeric) - partially "pre-digested" and are thus more easily absorbed than whole protein formulae. - contain nitrogen predominantly in peptide form (chains of 2-50 amino acids). - lipids are provided at least in part as MCTs, since these also are more readily digested and absorbed. 3. Free amino acid formulae (monomeric) contain single amino acids as the nitrogen source; very few indications for their use, since oligopeptides are generally better absorbed than free amino acids and combine this with lower osmolality.
15 EN Standard formula standard energy kcal / ml low energy < 0. 9 high energy > 1. 2

16 Indications for monomeric formulae Some forms of congenital metabolic disease, Severe allergy to dietary protein, Nutritional treatment of Crohn's disease
17 Enteral formulae Protein sources for the whole protein formulae are mostly milk proteins such as casein, often together with soy proteins. In peptide-based formulae hydrolysates of soy, lactalbumin, gelatine and/or whey are used. Amino acid-based formulae contain free amino acids, and accordingly do not contain glutamine, because this amino acid is not stable in its free state. Fat sources in standard formulae are predominantly mixtures of oils that are high in polyunsaturated ω-6 fatty acids, such as sunflower, soy, safflower and corn oils. Recently, with increasing awareness of the positive effects of the ω-3 fatty acids, canola oil has been added to many formulae, and sometimes fish oils are added. Medium chain triglycerides (MCT) derived from coconut oil form part of several formulae. Peptide-based and elemental preparations often contain dominant amounts of MCTs, on the basis that they do not require bile salts or pancreatic lipase prior to absorption, and that they bypass the lymphatic system with direct uptake into the portal circulation. Self-evidently the MCTs do not contain any essential fatty acids, and a minimum of 5% polyunsaturated fatty acids is added to any such mixture in order to ensure that the formula is nutritionally complete.
18 Carbohydrate sources are predominantly partial enzymatic hydrolysates of corn starch (maltodextrins with at least 10 glucose molecules). Some formulae, especially those intended for oral use, may contain small amounts of sucrose as this increases palatability. Some whole protein formulae may also contain starch. Minerals, vitamins and trace elements are added, usually to meet 100% of each RDA in the volume of the formula required to yield 1500 kcal.
19 EN formulae generally do not contain lactose, cholesterol, purines, or gluten This is achieved by careful choice of the base materials rather than through technical elimination processes. Cholesterol, for example, is avoided by the selection of plant oils as the predominant lipid sources. Purines are absent from the principal macro-ingredients (such as milk and soy). Gluten content is minimised by the choice of corn-derived carbohydrates. The protein component of most enteral products is added in highly concentrated powder form, usually with a protein fraction of about 85%; this helps to ensure that only negligible amounts of lactose remain despite the use of milk. Enteral formulae are therefore safe for patients with primary or secondary lactose intolerance, coeliac disease, and appropriate for use in those with gout or hypercholesterolaemia. Despite their use of manipulated products, enteral formulae are still based on natural components mainly using common high quality staples. Emphasising their artificiality is no more logical than in respect of regular supermarket foods (such as milk desserts), and may be counterproductive when encouraging their use by patients.
20 Short-Term vs. Long-Term Tube Feeding Access No standard of care for cut-off time between short-term and long-term access However, if patient is expected to require nutrition support longer than 6-8 weeks, longterm access should be considered
21 Complications of Enteral Nutrition Support Aspiration Nausea and vomiting (delayed gastric emptying) Malabsorption (hyperosmolarity) steatorrhea, diarrhea (most frequent)
22 Parenteral Nutrition This is administering nutrients through the vein AIO ( All in One method) Two types: Peripheral Central
23 Indications for Total Parenteral Nutrition (TPN) All severely ill patients where GIT is not available for feeding. Protein calorie malnutrition Intra-abdominal sepsis Sever trauma It is used when the GIT is blocked, short, fistulated, inflamed or cannot cope with demands.
24 Indications for Total Parenteral Nutrition (TPN) GIT is: Blocked - Gastric outlet obstruction Short - Short bowel syndrom Fistulated - proximal enterocutaneous fistula. Inflamed inflammatory bowel disease Unable to cope severe trauma

25 Central vein access

26

27 Central vein access The end of the catheter lower 1/3 vena cava upper 1/3 right atrium X-ray!


28 CVC port Ceramic base Silicone membrane (up to 2000 injections)
29 Proteins amino acids always 8 obligatory amino acids: (izo, leu, liz, met, fen, tre, try, wal) + non obligatory amino acids total amount: g/l daily requirement for healthy adults: 0.75 /kg BW daily requirement for patients: / kg BW
30 Carbohydrates Glucose one of 2 main energy sources (4 kcal/g) usually % of energy lowers the level of gluconeogenesis, regulates metabolism of amino acids and lipids Max dose 5 mg/kg/min produced CO2 RQ (Respiratory Quotient) = used O2 RQ glucose = 1.0 RQ lipids = 0.7 Maintain plasma glucose < 150 mg/dl
31 Lipids soybean fatty acids (LCT) source of energy (1 g = 9 kcal) and obligatory fatty acids (linoleic acid, alpha-linolenic acid) phospholipids structure of the cell membrane % energy 0.1 g/kg/h (LCT) or 0.15 g/ kg/ h (MCT/LCT) stop infusion if hipertrigliceridemia (> 350 mg/dl) able to modify inflammation: MCT, olive oil, fish oil
32 Vitamins 9 water soluable vitamins + 4 lipid soluable obligatory for metabolism of proteins, lipids and carbohydrates coenzymes, regulatory functions, antioxidants for free radicals ALL vitamins should be given from the very begining (50% pts shortage of vitamins D, folic acid, E, A, H) administration of some vitamins modifies the need for others (ie. C -- B2 i B12) Solutions: Soluvit, Cernevit (water sol.) Vitalipid (lipid sol.)
33 Electrolytes All electrolytes should be administered to fulfil daily requirements and losts The amino acids solutions contain electrolytes Can be added separately if necessary NaCl, KCl, CaCl2, Ca gluconate, Phosphate Solutions: Glycophos, Addiphos Limitted amout in the All in One bags!!!


34 AIO ( All in One bags)
35 AIO 1+ ions: Na + K < 130 mmol/l 2+ ions: Ca + Mg < 8 mmol/l CAN (Critical Aggregation Number a maximal concentration of cations above which the aggregation of lipid particles can occur 1+ ions + 64 x 2+ ions x 3+ ions < 600 /l CaHPO4 - unsoluable Ca3PO4 - unsoluable 2+ ions => 60x more destabilizing effect of a monovalent ions

36
37 Precipitation of Calcium Hydrogen Phosphate. The sediment is deposited when the product of concentration of Ca2+ and ions is above 72 mmol2/l. Many other factors such as ph and the content of the mixture, the way it was prepared, and storage conditions may affect the solubility of CaHPO4. Currently, the risk of precipitation of CaHPO4 can be eliminated by the use of organic calcium salts such as gluconates and glycerophosphate which do not dissociate in aqueous solutions Inactivation of Vitamins, as They Are Highly Susceptible to Degradation. Parenteral nutrition generally contains vitamins at the minimal concentrations necessary for the body function. Sometimes the clinical state of the patient requires additional supplementation with high doses of some vitamins: vitamin B1 in severe malnutrition or vitamin C in patients with increased cell catabolism. Inactivation of vitamins may follow many mechanisms: photolysis of vitamin A and B1, oxidation of vitamin C, reduction of vitamin B1, or adsorption of vitamin A onto the surface of the container
38 Immunonutrition Recently - some advantages of specific components for patients survival and lowering the number of complications (several trials, some still ongoing) glutamine, arginine, nukcleotydes, ώ- 3 fatty acids GLUTAMINE (Dipeptiven) elevating the number and activity of limphocytes and the cytotoxic activity of mononuclears; obligatory AA for fast proliferating cells strong indications (grade A) in severe burn and trauma daily dose in critically ill: 0,3-0,6 g/kg OMEGA 3 FATTY ACIDS (Omegaven) immunosupresive effect (lower cytokine production, lower the expression of Tcell activating receptors) lower inflammatory response (support CARS) max 30 % of daily lipid
39 PPN vs. TPN TPN (total parenteral nutrition) High glucose concentration (15%-25% final dextrose concentration) Provides a hyperosmolar formulation ( mosm/l) Must be delivered into a large-diameter vein through central line. PPN (peripheral parenteral nutrition) Similar nutrient components as TPN, but lower concentration (5%-10% final dextrose concentration) Osmolarity < 900 mosm/l (maximum tolerated by a peripheral vein) May be delivered into a peripheral vein Because of lower concentration, large fluid volumes are needed to provide a comparable calorie and protein dose as TPN (practically up to 2000 kcal/24h)
40 Administration of the Nutrient Solution The hypertonic solution is given at a constant rate per day (usually 1-1.5liters in 1st 24hrs then 1liter 12hourly x 48hrs increasing up to 2.5liters/day gradually to avoid hyperosmolarity problems.
41 Parenteral Nutrition Monitoring Check daily electrolytes and adjust TPN/PPN electrolyte additives accordingly Check accu-check glucose q 6 hours (regular insulin may be added to TPN/PPN bag for glucose control as needed) Non-diabetics or NIDDM: start with half of the previous day s sliding scale insulin requirement in TPN/PPN bag and increase daily in the same manner until target glucose is reached IDDM: start with 0.1 units regular insulin per gram of dextrose in TPN/PPN, then increase daily by half of the previous day s sliding scale insulin requirement Check triglyceride level within 24 hours of starting TPN/PPN If TG > mg/dl, lipid infusion should be significantly reduced or discontinued Consider adding carnitine 1 gram daily to TPN/PPN to improve lipid metabolism ~100 grams fat per week is needed to prevent essential fatty acid deficiency
42 Parenteral Nutrition Monitoring (continued) Acid/base balance Adjust TPN/PPN anion concentration to maintain proper acid/base balance Increase/decrease chloride content as needed Since bicarbonate is unstable in TPN/PPN preparations, the precursor acetate is used; adjust acetate content as needed
43 Complications of Parenteral Nutrition Hepatic steatosis (PNALD) May occur within 1-2 weeks after starting PN May be associated with fatty liver infiltration Usually is benign, transient, and reversible in patients on short-term PN and typically resolves in days Limiting fat content of PN and cycling PN over 12 hours is needed to control steatosis in long-term PN patients
44 Complications of Parenteral Nutrition Support (continued) Cholestasis May occur 2-6 weeks after starting PN Indicated by progressive increase in TBili and an elevated serum alkaline phosphatase Occurs because there are no intestinal nutrients to stimulate hepatic bile flow Trophic enteral feeding to stimulate the gallbladder can be helpful in reducing/preventing cholestasis Gastrointestinal atrophy Lack of enteral stimulation is associated with villus hypoplasia, colonic mucosal atrophy, decreased gastric function, impaired GI immunity, bacterial overgrowth, and bacterial translocation Trophic enteral feeding to minimize/prevent GI atrophy
45 Benefits of Enteral Nutrition Over Parenteral Nutrition Cost Tube feeding cost ~ $10-20 per day TPN costs up to $100 or more per day! Maintains integrity of the gut Tube feeding preserves intestinal function; it is more physiologic TPN may be associated with gut atrophy Less infection Enteral feeding very small risk of infection and may prevent bacterial translocation across the gut wall TPN high risk/incidence of infection and sepsis
46 Refeeding Syndrome the metabolic and physiologic consequences of depletion, repletion, compartmental shifts, and interrelationships of phosphorus, potassium, and magnesium Severe drop in serum electrolyte levels resulting from intracellular electrolyte movement when energy is provided after a period of starvation (usually > 7-10 days) Physiologic and metabolic sequelae may include: EKG changes, hypotension, arrhythmia, cardiac arrest Weakness, paralysis Respiratory depression Ketoacidosis / metabolic acidosis
47 Refeeding Syndrome (continued) Prevention and Therapy Correct electrolyte abnormalities before starting nutrition support Continue to monitor serum electrolytes after nutrition support begins and replete aggressively Initiate nutrition support at low rate/concentration (~ 50% of estimated needs) and advance to goal slowly in patients who are at high risk
48 Consequences of Over-feeding Risks associated with over-feeding: Hyperglycemia Hepatic dysfunction from fatty infiltration Respiratory acidosis from increased CO2 production Difficulty weaning from the ventilator Risks associated with under-feeding: Depressed ventilatory drive Decreased respiratory muscle function Impaired immune function Increased infection
49 Thank you
Methods of Nutrition Support KNH 406
 Methods of Nutrition Support KNH 406 Malnutrition 30 50% of hospitalized patients 95% of nursing home patients Resulting in reduced quality of life & increased health care costs May be remedied by providing
Methods of Nutrition Support KNH 406 Malnutrition 30 50% of hospitalized patients 95% of nursing home patients Resulting in reduced quality of life & increased health care costs May be remedied by providing
Parenteral and Enteral Nutrition
 Parenteral and Enteral Nutrition Audis Bethea, Pharm.D. Assistant Professor Therapeutics I December 5 & 9, 2003 Parenteral Nutrition Definition process of supplying nutrients via the intravenous route
Parenteral and Enteral Nutrition Audis Bethea, Pharm.D. Assistant Professor Therapeutics I December 5 & 9, 2003 Parenteral Nutrition Definition process of supplying nutrients via the intravenous route
Nutritional intervention in hospitalised paediatric patients. Dr Y.K.Amdekar
 Nutritional intervention in hospitalised paediatric patients Dr Y.K.Amdekar Back to basics Suboptimal nutrient intake is always dangerous in health and more so in disease to feed or not to feed is it a
Nutritional intervention in hospitalised paediatric patients Dr Y.K.Amdekar Back to basics Suboptimal nutrient intake is always dangerous in health and more so in disease to feed or not to feed is it a
PARENTERAL NUTRITION
 PARENTERAL NUTRITION DEFINITION Parenteral nutrition [(PN) or total parenteral nutrition (TPN)] is the intravenous infusion of some or all nutrients for tissue maintenance, metabolic requirements and growth
PARENTERAL NUTRITION DEFINITION Parenteral nutrition [(PN) or total parenteral nutrition (TPN)] is the intravenous infusion of some or all nutrients for tissue maintenance, metabolic requirements and growth
Short Bowel Syndrome: Medical management
 Short Bowel Syndrome: Medical management La Sindrome dell'intestino Corto in età pediatrica Brescia 18 marzo 2011 Jon A.Vanderhoof, M.D. Division of Pediatric GI Harvard Medical School Children s Hospital,
Short Bowel Syndrome: Medical management La Sindrome dell'intestino Corto in età pediatrica Brescia 18 marzo 2011 Jon A.Vanderhoof, M.D. Division of Pediatric GI Harvard Medical School Children s Hospital,
Nutrition and Medicine, 2006 Tufts University School of Medicine Nutrition and Acute Illness: Learning Objectives
 Nutrition and Medicine, 2006 Tufts University School of Medicine Nutrition and Acute Illness: Learning Objectives Margo N. Woods, D.Sc. 1. Define protein-calorie, or protein-energy malnutrition (PEM) and
Nutrition and Medicine, 2006 Tufts University School of Medicine Nutrition and Acute Illness: Learning Objectives Margo N. Woods, D.Sc. 1. Define protein-calorie, or protein-energy malnutrition (PEM) and
Substrates in clinical nutrition Ilze Jagmane
 Substrates in clinical nutrition Ilze Jagmane Latvian Society of Parenteral and Enteral Nutrition September, 2013 Introduction Food contains one or more of the following nutrients: Water Carbohydrate Lipids
Substrates in clinical nutrition Ilze Jagmane Latvian Society of Parenteral and Enteral Nutrition September, 2013 Introduction Food contains one or more of the following nutrients: Water Carbohydrate Lipids
Chapter 16 Nutrition, Fluids and Electrolytes, and Acid-Base Balance Nutrition Nutrients Water o Functions Promotes metabolic processes Transporter
 Chapter 16 Nutrition, Fluids and Electrolytes, and Acid-Base Balance Nutrition Nutrients Water o Functions Promotes metabolic processes Transporter for nutrients and wastes Lubricant Insulator and shock
Chapter 16 Nutrition, Fluids and Electrolytes, and Acid-Base Balance Nutrition Nutrients Water o Functions Promotes metabolic processes Transporter for nutrients and wastes Lubricant Insulator and shock
Enteral Nutrition: Whom, Why, When, What and Where to Feed?
 Meier RF, Reddy BR, Soeters PB (eds): The Importance of Nutrition as an Integral Part of Disease Management. Nestlé Nutr Inst Workshop Ser, vol 82, pp 53 59, (DOI: 10.1159/000382002) Nestec Ltd., Vevey/S.
Meier RF, Reddy BR, Soeters PB (eds): The Importance of Nutrition as an Integral Part of Disease Management. Nestlé Nutr Inst Workshop Ser, vol 82, pp 53 59, (DOI: 10.1159/000382002) Nestec Ltd., Vevey/S.
Intensive Care Nutrition. Dr Alan Race BSc(Hons) PhD FRCA
 PhD FRCA") Intensive Care Nutrition Dr Alan Race BSc(Hons) PhD FRCA Objectives 1. What examiners say 2. Definition 3. Assessment 4. Requirements 5. Types of delivery 6. CALORIES Trial 7. Timing 8. Immunomodulation
Intensive Care Nutrition Dr Alan Race BSc(Hons) PhD FRCA Objectives 1. What examiners say 2. Definition 3. Assessment 4. Requirements 5. Types of delivery 6. CALORIES Trial 7. Timing 8. Immunomodulation
Nutrition care plan for surgical patients. Objectives
 Slide 1 Nutrition care plan for surgical patients Surgical Nutrition Training Module Level 1 Philippine Society of General Surgeons Committee on Surgical Training In this session we will discuss the most
Slide 1 Nutrition care plan for surgical patients Surgical Nutrition Training Module Level 1 Philippine Society of General Surgeons Committee on Surgical Training In this session we will discuss the most
Nutrition Services at a glance
 Nutrition Services at a glance Ragini Raghuveer, MS, RD, LD/N Systems Clinical Nutrition Manager Linette De Armas, RD, LD/N Clinical Dietitian Melissa Lorenzo, RD, LD/N Clinical Dietitian 1 Learning Objectives
Nutrition Services at a glance Ragini Raghuveer, MS, RD, LD/N Systems Clinical Nutrition Manager Linette De Armas, RD, LD/N Clinical Dietitian Melissa Lorenzo, RD, LD/N Clinical Dietitian 1 Learning Objectives
Effect of changing lipid formulation in Parenteral Nutrition in the Newborn Experimental Pathology BSc
 Effect of changing lipid formulation in Parenteral Nutrition in the Newborn Experimental Pathology BSc Word count: 6939 0 CONTENTS Abstract...2 Acknowledgements...3 Introduction...4 Materials and Methods...11
Effect of changing lipid formulation in Parenteral Nutrition in the Newborn Experimental Pathology BSc Word count: 6939 0 CONTENTS Abstract...2 Acknowledgements...3 Introduction...4 Materials and Methods...11
ICU NUTRITION UPDATE : ESPEN GUIDELINES Mirey Karavetian Assistant Professor Zayed University
 ICU NUTRITION UPDATE : ESPEN GUIDELINES 2018 Mirey Karavetian Assistant Professor Zayed University http://www.espen.org/files/espen- Guidelines/ESPEN_Guideline_on_clinical_nutrition_in_-ICU.pdf Medical
ICU NUTRITION UPDATE : ESPEN GUIDELINES 2018 Mirey Karavetian Assistant Professor Zayed University http://www.espen.org/files/espen- Guidelines/ESPEN_Guideline_on_clinical_nutrition_in_-ICU.pdf Medical
Nutritional Management in Enterocutaneous fistula Dr Deepak Govil
 Nutritional Management in Enterocutaneous fistula Dr Deepak Govil MS, PhD (GI Surgery) Senior Consultant Surgical Gastroenterology Indraprastha Apollo Hospital New Delhi What is enterocutaneous fistula
Nutritional Management in Enterocutaneous fistula Dr Deepak Govil MS, PhD (GI Surgery) Senior Consultant Surgical Gastroenterology Indraprastha Apollo Hospital New Delhi What is enterocutaneous fistula
Nutrition Support Calculations Brianne Squires
 Nutrition Support Calculations Brianne Squires 1. Determine the following for Ensure at 68 ml/hour (Note: when working with volumes of formula for enteral formula, it is expressed in total volume/ml not
Nutrition Support Calculations Brianne Squires 1. Determine the following for Ensure at 68 ml/hour (Note: when working with volumes of formula for enteral formula, it is expressed in total volume/ml not
Total Parenteral Nutrition and Enteral Nutrition in the Home. Original Policy Date 12:2013
 MP 1.02.01 Total Parenteral Nutrition and Enteral Nutrition in the Home Medical Policy Section Durable Medical Equipment Issue Original Policy Date Last Review Status/Date Return to Medical Policy Index
MP 1.02.01 Total Parenteral Nutrition and Enteral Nutrition in the Home Medical Policy Section Durable Medical Equipment Issue Original Policy Date Last Review Status/Date Return to Medical Policy Index
L.Mageswary Dietitian Hospital Selayang
 L.Mageswary Dietitian Hospital Selayang 14 15 AUG ASMIC 2015 Learning Objectives 1. To understand the importance of nutrition support in ICU 2. To know the right time to feed 3. To understand the indications
L.Mageswary Dietitian Hospital Selayang 14 15 AUG ASMIC 2015 Learning Objectives 1. To understand the importance of nutrition support in ICU 2. To know the right time to feed 3. To understand the indications
ENTERAL NUTRITION IN THE CRITICALLY ILL
 ENTERAL NUTRITION IN THE CRITICALLY ILL 1 Ebb phase Flow phase acute response (catabolic) adoptive response (anabolic) 2 3 Metabolic Response to Stress (catabolic phase) Glucose and Protein Metabolism
ENTERAL NUTRITION IN THE CRITICALLY ILL 1 Ebb phase Flow phase acute response (catabolic) adoptive response (anabolic) 2 3 Metabolic Response to Stress (catabolic phase) Glucose and Protein Metabolism
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Acetate, in pediatric surgical patients, 525 526 Acute respiratory distress syndrome (ARDS), immune-modulating nutrition in, 584 585 Aerobic
Index Note: Page numbers of article titles are in boldface type. A Acetate, in pediatric surgical patients, 525 526 Acute respiratory distress syndrome (ARDS), immune-modulating nutrition in, 584 585 Aerobic
ESPEN Congress Florence 2008
 ESPEN Congress Florence 2008 PN Guidelines presentation PN Guidelines in pancreas diseases L. Gianotti (Italy) ESPEN Guidelines on Parenteral Nutrition: Pancreas L.Gianotti, R.Meier, D.N.Lobo, C.Bassi,
ESPEN Congress Florence 2008 PN Guidelines presentation PN Guidelines in pancreas diseases L. Gianotti (Italy) ESPEN Guidelines on Parenteral Nutrition: Pancreas L.Gianotti, R.Meier, D.N.Lobo, C.Bassi,
Introduction to Clinical Nutrition
 M-III Introduction to Clinical Nutrition Donald F. Kirby, MD Chief, Section of Nutrition Division of Gastroenterology 1 Things We Take for Granted Air to Breathe Death Taxes Another Admission Our Next
M-III Introduction to Clinical Nutrition Donald F. Kirby, MD Chief, Section of Nutrition Division of Gastroenterology 1 Things We Take for Granted Air to Breathe Death Taxes Another Admission Our Next
Who Needs Parenteral Nutrition? Is Parenteral Nutrition An Appropriate Intervention?
 Who Needs Parenteral Nutrition? 1 Is Parenteral Nutrition An Appropriate Intervention? Key questions to ask with initial consultation Can the gastrointestinal (GI) tract be utilized? Can the GI tract be
Who Needs Parenteral Nutrition? 1 Is Parenteral Nutrition An Appropriate Intervention? Key questions to ask with initial consultation Can the gastrointestinal (GI) tract be utilized? Can the GI tract be
The Role of Parenteral Nutrition. in PEDIATRIC INTENSIVE CARE UNIT. Dzulfikar DLH. Pediatric Emergency and Intensive Care Unit
 The Role of Parenteral Nutrition in PEDIATRIC INTENSIVE CARE UNIT Dzulfikar DLH Pediatric Emergency and Intensive Care Unit Department of Child Health, Faculty of Medicine Universitas Padjajaran, Hasan
The Role of Parenteral Nutrition in PEDIATRIC INTENSIVE CARE UNIT Dzulfikar DLH Pediatric Emergency and Intensive Care Unit Department of Child Health, Faculty of Medicine Universitas Padjajaran, Hasan
Major Case Study: Enteral and Parenteral Nutrition Due 2/13/15 60 points. Ht: 5 11 Current wt: 156 # UBW: 167 # Serum albumin: 3.
 Name: Wan yi Wang Major Case Study: Enteral and Parenteral Nutrition Due 2/13/15 60 points Mr. R, a 35 yo drug user, is hospitalized after a motor vehicle accident (MVA). He is currently suffering from
Name: Wan yi Wang Major Case Study: Enteral and Parenteral Nutrition Due 2/13/15 60 points Mr. R, a 35 yo drug user, is hospitalized after a motor vehicle accident (MVA). He is currently suffering from
Vanderbilt University Medical Center Trauma ICU Nutrition Management Guidelines
 Vanderbilt University Medical Center Trauma ICU Nutrition Management Guidelines Trauma Critical Care Nutrition Guidelines Clinical judgment may supersede guidelines as patient circumstances warrant ASSESSMENT
Vanderbilt University Medical Center Trauma ICU Nutrition Management Guidelines Trauma Critical Care Nutrition Guidelines Clinical judgment may supersede guidelines as patient circumstances warrant ASSESSMENT
Major Case Study: Enteral and Parenteral Nutrition
 Major Case Study: Enteral and Parenteral Nutrition Mr. R, a 35 yo drug user, is hospitalized after a motor vehicle accident (MVA). He is currently suffering from a severe concussion and lapses of consciousness,
Major Case Study: Enteral and Parenteral Nutrition Mr. R, a 35 yo drug user, is hospitalized after a motor vehicle accident (MVA). He is currently suffering from a severe concussion and lapses of consciousness,
Drug Shortages with Parenteral Nutrition
 Drug Shortages with Parenteral Nutrition Carol J Rollins, MS, RD, PharmD, BCNSP Coordinator, Nutrition Support Team The University of Arizona Medical Center www.nutritioncare.org Conflict of Interest None
Drug Shortages with Parenteral Nutrition Carol J Rollins, MS, RD, PharmD, BCNSP Coordinator, Nutrition Support Team The University of Arizona Medical Center www.nutritioncare.org Conflict of Interest None
Parenteral Nutrition Audis Bethea, Pharm.D. Assistant Professor Therapeutics I. December 5 & 9, 2003
 Parenteral Nutrition Audis Bethea, Pharm.D. Assistant Professor Therapeutics I December 5 & 9, 2003 Required readings Mattox TW. Parenteral nutrition. Dipiro JT, Talbert RL, Yee CG, et al., eds. Pharmacotherapy:
Parenteral Nutrition Audis Bethea, Pharm.D. Assistant Professor Therapeutics I December 5 & 9, 2003 Required readings Mattox TW. Parenteral nutrition. Dipiro JT, Talbert RL, Yee CG, et al., eds. Pharmacotherapy:
Scott A. Lynch, MD, MPH,FAAFP Assistant Professor
 Scott A. Lynch, MD, MPH,FAAFP Assistant Professor Lynch.Scott@mayo.edu 2015 MFMER 3543652-1 Nutrition in the Hospital Mayo School of Continuous Professional Development 2nd Annual Inpatient Medicine for
Scott A. Lynch, MD, MPH,FAAFP Assistant Professor Lynch.Scott@mayo.edu 2015 MFMER 3543652-1 Nutrition in the Hospital Mayo School of Continuous Professional Development 2nd Annual Inpatient Medicine for
Index. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Abdominal pain, enteral therapy in acute pancreatitis and, 812 Abscess(es), pancreatic, nutritional support for, 814 815 Acute Physiology and
Note: Page numbers of article titles are in boldface type. A Abdominal pain, enteral therapy in acute pancreatitis and, 812 Abscess(es), pancreatic, nutritional support for, 814 815 Acute Physiology and
Nutritional Support For The Critical Patient Andrea Collins, BBA, LVT, VTS (ECC)
") Nutritional Support For The Critical Patient Andrea Collins, BBA, LVT, VTS (ECC) TOPICS PART 1 Importance Indications for support Nutritional assessment Energy requirements The plan Enteral/Parenteral
Nutritional Support For The Critical Patient Andrea Collins, BBA, LVT, VTS (ECC) TOPICS PART 1 Importance Indications for support Nutritional assessment Energy requirements The plan Enteral/Parenteral
ESPEN Congress The Hague 2017
 ESPEN Congress The Hague 2017 Meeting nutritional needs of acute care patients Feeding acute pancreatitis patients J. Luttikhold (NL) FEEDING ACUTE PANCREATITIS PATIENTS Joanna Luttikhold, MD PhD Registrar
ESPEN Congress The Hague 2017 Meeting nutritional needs of acute care patients Feeding acute pancreatitis patients J. Luttikhold (NL) FEEDING ACUTE PANCREATITIS PATIENTS Joanna Luttikhold, MD PhD Registrar
Nutrition. By Dr. Ali Saleh 2/27/2014 1
 Nutrition By Dr. Ali Saleh 2/27/2014 1 Nutrition Functions of nutrients: Providing energy for body processes and movement. Providing structural material for body tissues. Regulating body processes. 2/27/2014
Nutrition By Dr. Ali Saleh 2/27/2014 1 Nutrition Functions of nutrients: Providing energy for body processes and movement. Providing structural material for body tissues. Regulating body processes. 2/27/2014
EU RISK MANAGEMENT PLAN (EU RMP) Nutriflex Omega peri emulsion for infusion , version 1.1
 Nutriflex Omega peri emulsion for infusion , version 1.1") EU RISK MANAGEMENT PLAN (EU RMP) Nutriflex Omega peri emulsion for infusion 13.7.2015, version 1.1 III.1. Elements for a Public Summary III.1.1. Overview of disease epidemiology Patients may need parenteral
EU RISK MANAGEMENT PLAN (EU RMP) Nutriflex Omega peri emulsion for infusion 13.7.2015, version 1.1 III.1. Elements for a Public Summary III.1.1. Overview of disease epidemiology Patients may need parenteral
Nutritional assessments and diagnosis of digestive disorders
 Nutritional assessments and diagnosis of digestive disorders AASER ABDELAZIM Assistant professor of Medical Biochemistry Zagazig University, Egypt University of Bisha, KSA aaserabdelazim@yahoo.com 7 Mal
Nutritional assessments and diagnosis of digestive disorders AASER ABDELAZIM Assistant professor of Medical Biochemistry Zagazig University, Egypt University of Bisha, KSA aaserabdelazim@yahoo.com 7 Mal
Current concepts in Critical Care Nutrition
 Current concepts in Critical Care Nutrition Dr.N.Ramakrishnan AB (Int Med), AB (Crit Care), MMM, FACP, FCCP, FCCM Director, Critical Care Services Apollo Hospitals, Chennai Objectives Why? Enteral or Parenteral
Current concepts in Critical Care Nutrition Dr.N.Ramakrishnan AB (Int Med), AB (Crit Care), MMM, FACP, FCCP, FCCM Director, Critical Care Services Apollo Hospitals, Chennai Objectives Why? Enteral or Parenteral
Product Information: Pivot 1.5 Cal
 Product Information: Pivot 1.5 Cal 1 of 5 PIVOT 1.5 CAL is a very-high-protein, calorically dense, immune-supporting, hydrolyzed, peptide-based enteral formula for use in metabolically stressed, immunosuppressed
Product Information: Pivot 1.5 Cal 1 of 5 PIVOT 1.5 CAL is a very-high-protein, calorically dense, immune-supporting, hydrolyzed, peptide-based enteral formula for use in metabolically stressed, immunosuppressed
Product Category: Pivot 1.5 Cal
 Product Category: Pivot 1.5 Cal Pivot 1.5 Cal Updated 4/8/2014 Product Information: Pivot 1.5 Cal 1 of 6 PIVOT 1.5 CAL is designed for metabolically stressed surgical, trauma, burn, and head and neck cancer
Product Category: Pivot 1.5 Cal Pivot 1.5 Cal Updated 4/8/2014 Product Information: Pivot 1.5 Cal 1 of 6 PIVOT 1.5 CAL is designed for metabolically stressed surgical, trauma, burn, and head and neck cancer
Product Category: Pulmocare
 Product Category: Pulmocare Pulmocare Updated 4/8/2014 Product Information: Pulmocare 1 of 5 PULMOCARE is designed for people with chronic obstructive pulmonary disease (COPD), cystic fibrosis, or respiratory
Product Category: Pulmocare Pulmocare Updated 4/8/2014 Product Information: Pulmocare 1 of 5 PULMOCARE is designed for people with chronic obstructive pulmonary disease (COPD), cystic fibrosis, or respiratory
Product Segments. Medical Nutrition. General Nutrition. Wellness Nutrition. Sports Nutrition. And Many More..
 Product Segments Medical Nutrition General Nutrition Diabetic Nutrition, Renal Nutrition, Cancer Nutrition, Critical Care Nutrition, Hepatic Nutrition, Bone Health Nutrition, MCT & Fibers Balanced Nutrition,
Product Segments Medical Nutrition General Nutrition Diabetic Nutrition, Renal Nutrition, Cancer Nutrition, Critical Care Nutrition, Hepatic Nutrition, Bone Health Nutrition, MCT & Fibers Balanced Nutrition,
Product Information: PediaSure Peptide 1.5 Cal
 Product Information: PediaSure Peptide 1.5 Cal 1 of 5 PEDIASURE PEPTIDE 1.5 is a nutritionally complete, peptide-based formula for the nutritional needs of children 1-13 years with malabsorption, maldigestion,
Product Information: PediaSure Peptide 1.5 Cal 1 of 5 PEDIASURE PEPTIDE 1.5 is a nutritionally complete, peptide-based formula for the nutritional needs of children 1-13 years with malabsorption, maldigestion,
Nutrition care plan. Components and development
 Nutrition care plan Components and development Objectives To define the nutrition care plan To present the components of the nutrition care plan To discuss the different approaches in determining the contents
Nutrition care plan Components and development Objectives To define the nutrition care plan To present the components of the nutrition care plan To discuss the different approaches in determining the contents
Nutrition Support. John Cha Department of Surgery DHMC/UCHSC
 Nutrition Support John Cha Department of Surgery DHMC/UCHSC Overview Why? When? How much? What route? Fancy stuff: enhanced nutrition Advantages of Nutrition Decreased catabolism Improved wound healing
Nutrition Support John Cha Department of Surgery DHMC/UCHSC Overview Why? When? How much? What route? Fancy stuff: enhanced nutrition Advantages of Nutrition Decreased catabolism Improved wound healing
MCT AND THE ROLES NUTRITION
 MCT AND THE ROLES NUTRITION Nguyen Hoang Nhut Hoa Department of Nutrition Children's Hospital 2 OBJECTIVES Structure Absorption and metabolic Effects of MCT in the treatment of certain diseases Demand
MCT AND THE ROLES NUTRITION Nguyen Hoang Nhut Hoa Department of Nutrition Children's Hospital 2 OBJECTIVES Structure Absorption and metabolic Effects of MCT in the treatment of certain diseases Demand
Nutritional Information
 Nutritional Information Honest Milk Step 1 Infant Formula Milk-based Infant Formula Milk powder for Infants 0-12 Months Indication Honest Milk Step 1 Infant Formula Milk Powder Includes Natural Defense
Nutritional Information Honest Milk Step 1 Infant Formula Milk-based Infant Formula Milk powder for Infants 0-12 Months Indication Honest Milk Step 1 Infant Formula Milk Powder Includes Natural Defense
Nutrition Management in GI Diseases
 Nutrition Management in GI Diseases Aryono Hendarto MD Nutrition & Metabolic Diseases Division Department of Child Health Cipto Mangunkusumo Hospital University of Indonesia 1 Patient s Care 1. Drugs 2.
Nutrition Management in GI Diseases Aryono Hendarto MD Nutrition & Metabolic Diseases Division Department of Child Health Cipto Mangunkusumo Hospital University of Indonesia 1 Patient s Care 1. Drugs 2.
Nutrition Therapy. Medical Coverage Policy Enteral/Parenteral EFFECTIVE DATE: POLICY LAST UPDATED: 11/20/2018 OVERVIEW
 Medical Coverage Policy Enteral/Parenteral Nutrition Therapy EFFECTIVE DATE: 01 20 2007 POLICY LAST UPDATED: 11/20/2018 OVERVIEW This policy describes the reimbursement for enteral and parenteral nutrition
Medical Coverage Policy Enteral/Parenteral Nutrition Therapy EFFECTIVE DATE: 01 20 2007 POLICY LAST UPDATED: 11/20/2018 OVERVIEW This policy describes the reimbursement for enteral and parenteral nutrition
Nutrients. Nutrition. Carbohydrates. - ex. Carbs, Fats, Protein, Water. - ex. vitamins, minerals
 Nutrients Nutrition Introduction elements and compounds an organism needs but can not manufacture itself 6 Basic Nutrients carbohydrates fats proteins water vitamins minerals Macronutrients supply energy
Nutrients Nutrition Introduction elements and compounds an organism needs but can not manufacture itself 6 Basic Nutrients carbohydrates fats proteins water vitamins minerals Macronutrients supply energy
PAEDIATRIC PARENTERAL NUTRITION - INDIAN CONTEXT. Dr. Sarath Gopalan
 PAEDIATRIC PARENTERAL NUTRITION - INDIAN CONTEXT Dr. Sarath Gopalan Senior Consultant in Pediatric Gastroenterology, Hepatology Indraprastha Apollo Hospital, New Delhi PN DELIVERY CENTRAL PERIPHERAL
PAEDIATRIC PARENTERAL NUTRITION - INDIAN CONTEXT Dr. Sarath Gopalan Senior Consultant in Pediatric Gastroenterology, Hepatology Indraprastha Apollo Hospital, New Delhi PN DELIVERY CENTRAL PERIPHERAL
TOTAL PARENTERAL NUTRITION
 TOTAL PARENTERAL NUTRITION Indication See algorithm. Timing Start TPN as indicated on algorithm 1. There is no need to build up TPN volume. The volume of TPN (including lipids) should equate to the total
TOTAL PARENTERAL NUTRITION Indication See algorithm. Timing Start TPN as indicated on algorithm 1. There is no need to build up TPN volume. The volume of TPN (including lipids) should equate to the total
Product Information: EleCare Jr
 Product Information: EleCare Jr 1 of 5 A 30 Cal/fl oz, nutritionally complete amino acid-based medical food for children age 1 and older who cannot tolerate intact or hydrolyzed protein. EleCare Jr is
Product Information: EleCare Jr 1 of 5 A 30 Cal/fl oz, nutritionally complete amino acid-based medical food for children age 1 and older who cannot tolerate intact or hydrolyzed protein. EleCare Jr is
Product Information: EleCare (for Infants)
") 1 of 5 Product Information: 2 of 5 A 20 Cal/fl oz, nutritionally complete amino acid-based formula for infants who cannot tolerate intact or hydrolyzed protein. EleCare is indicated for the dietary management
1 of 5 Product Information: 2 of 5 A 20 Cal/fl oz, nutritionally complete amino acid-based formula for infants who cannot tolerate intact or hydrolyzed protein. EleCare is indicated for the dietary management
Nutritional Demands of Disease and Trauma
 al Demands of Disease and Trauma Lecture 89 Medical School al Requirements Based on needs to support optimal physiological function Are changed by disease or injury metabolism is altered to prevent further
al Demands of Disease and Trauma Lecture 89 Medical School al Requirements Based on needs to support optimal physiological function Are changed by disease or injury metabolism is altered to prevent further
CHILDREN: NUTRITIONALS Prescription Required Provided by the Wisconsin WIC Program to Children (1 through 4 Years of Age)
") P-40077C (03/2016) CHILDREN: NUTRITIONALS Prescription Required Provided by the Wisconsin WIC Program to Children (1 through 4 Years of Age) A Prescription, for treatment of a diagnosed medical condition,
P-40077C (03/2016) CHILDREN: NUTRITIONALS Prescription Required Provided by the Wisconsin WIC Program to Children (1 through 4 Years of Age) A Prescription, for treatment of a diagnosed medical condition,
Product Category: Perative
 Product Category: Perative Perative Updated 4/8/2014 Product Information: Perative 1 of 5 PERATIVE is designed for metabolically stressed patients who can benefit from an enteral formula supplemented with
Product Category: Perative Perative Updated 4/8/2014 Product Information: Perative 1 of 5 PERATIVE is designed for metabolically stressed patients who can benefit from an enteral formula supplemented with
MEDICAL POLICY: Enteral and Parenteral Nutrition
 POLICY: PG0114 ORIGINAL EFFECTIVE: 02/15/07 LAST REVIEW: 08/14/18 MEDICAL POLICY: Enteral and Parenteral Nutrition GUIDELINES This policy does not certify benefits or authorization of benefits, which is
POLICY: PG0114 ORIGINAL EFFECTIVE: 02/15/07 LAST REVIEW: 08/14/18 MEDICAL POLICY: Enteral and Parenteral Nutrition GUIDELINES This policy does not certify benefits or authorization of benefits, which is
Nutritional Issues in Cholestatic Disease
 THE HOSPITAL FOR SICK CHILDREN Nutritional Issues in Cholestatic Disease NASPGHAN-CPNP Joint Session Binita M. Kamath, MBBChir MRCP MTR Associate Professor Division of Gastroenterology, Hepatology and
THE HOSPITAL FOR SICK CHILDREN Nutritional Issues in Cholestatic Disease NASPGHAN-CPNP Joint Session Binita M. Kamath, MBBChir MRCP MTR Associate Professor Division of Gastroenterology, Hepatology and
Nutrition Support in Children. Lyon 21 sept 2013
 Nutrition Support in Children Lyon 21 sept 2013 Malnutrition : why detecting it in children? Alters cognitive development (observational or interventional studies) Responsible for prolongation of hospitalisation
Nutrition Support in Children Lyon 21 sept 2013 Malnutrition : why detecting it in children? Alters cognitive development (observational or interventional studies) Responsible for prolongation of hospitalisation
Nutrition and Energy 1
 Nutrition and Energy 1 Food Energy The ingestion of food serves two primary functions: 1. it provides a source of energy 2. it provides raw materials the animal is unable to manufacture for itself. 2 Basal
Nutrition and Energy 1 Food Energy The ingestion of food serves two primary functions: 1. it provides a source of energy 2. it provides raw materials the animal is unable to manufacture for itself. 2 Basal
Enteral and parenteral nutrition in GI failure and short bowel syndrome
 Enteral and parenteral nutrition in GI failure and short bowel syndrome Alastair Forbes University College London Intestinal failure Inadequate functional intestine to allow health to be maintained by
Enteral and parenteral nutrition in GI failure and short bowel syndrome Alastair Forbes University College London Intestinal failure Inadequate functional intestine to allow health to be maintained by
Small Bowel Obstruction after operation in a severely malnourished man. By: Ms Bounmark Phoumesy
 Small Bowel Obstruction after operation in a severely malnourished man By: Ms Bounmark Phoumesy Normal length of GI tract Normal length(achieved by age 9) Small bowel 600cm (Men: 630 cm; Women: 592 cm)
Small Bowel Obstruction after operation in a severely malnourished man By: Ms Bounmark Phoumesy Normal length of GI tract Normal length(achieved by age 9) Small bowel 600cm (Men: 630 cm; Women: 592 cm)
Product Information: Pivot 1.5 Cal
 Product Information: Pivot 1.5 Cal 1 of 5 PIVOT 1.5 CAL is designed for metabolically stressed surgical, trauma, burn, or head and neck cancer patients who could benefit from an immune modulating enteral
Product Information: Pivot 1.5 Cal 1 of 5 PIVOT 1.5 CAL is designed for metabolically stressed surgical, trauma, burn, or head and neck cancer patients who could benefit from an immune modulating enteral
PAEDIATRIC PARENTERAL NUTRITION. Ezatul Mazuin Ayla binti Mamdooh Waffa Hospital Sultanah Aminah
 PAEDIATRIC PARENTERAL NUTRITION Ezatul Mazuin Ayla binti Mamdooh Waffa Hospital Sultanah Aminah Johor Bahru Malnutrition INTRODUCTION pathologic state of varying severity with clinical features caused
PAEDIATRIC PARENTERAL NUTRITION Ezatul Mazuin Ayla binti Mamdooh Waffa Hospital Sultanah Aminah Johor Bahru Malnutrition INTRODUCTION pathologic state of varying severity with clinical features caused
Małgorzata Łyszkowska
 Małgorzata Łyszkowska Department of Paediatric Surgery and Organ Transplantation The Children s Memorial Health Institute, Warsaw Poland Baltic Club 13-14.09.2013 Distinction Between Parenteral Nutrition
Małgorzata Łyszkowska Department of Paediatric Surgery and Organ Transplantation The Children s Memorial Health Institute, Warsaw Poland Baltic Club 13-14.09.2013 Distinction Between Parenteral Nutrition
Electrolytes Solution
 Electrolytes Solution Substances that are not dissociated in solution are called nonelectrolytes, and those with varying degrees of dissociation are called electrolytes. Urea and dextrose are examples
Electrolytes Solution Substances that are not dissociated in solution are called nonelectrolytes, and those with varying degrees of dissociation are called electrolytes. Urea and dextrose are examples
Amino Acids and Sorbitol injection with/without Electrolytes NIRMIN *
 For the use of a registered medical practitioner or a Hospital or a Laboratory only Amino Acids and Sorbitol injection with/without Electrolytes NIRMIN * DESCRIPTION: NIRMIN * is a clear, colourless injection
For the use of a registered medical practitioner or a Hospital or a Laboratory only Amino Acids and Sorbitol injection with/without Electrolytes NIRMIN * DESCRIPTION: NIRMIN * is a clear, colourless injection
Product Category: EleCare
 EleCare Product Category: EleCare EleCare (for Infants) Updated 4/28/2016 Product Information: EleCare (for Infants) 1 of 4 A 20 Cal/fl oz, nutritionally complete amino acid-based formula for infants who
EleCare Product Category: EleCare EleCare (for Infants) Updated 4/28/2016 Product Information: EleCare (for Infants) 1 of 4 A 20 Cal/fl oz, nutritionally complete amino acid-based formula for infants who
SUMMARY OF PRODUCT CHARACTERISTICS. Synthamin 14, 8.5% Amino Acid Intravenous Infusion
 SUMMARY OF PRODUCT CHARACTERISTICS 1. NAME OF THE MEDICINAL PRODUCT Synthamin 14, 8.5% Amino Acid Intravenous Infusion 2. QUALITATIVE AND QUANTITATIVE COMPOSITION L-Leucine Ph. Eur 0.620% w/v L-Isoleucine
SUMMARY OF PRODUCT CHARACTERISTICS 1. NAME OF THE MEDICINAL PRODUCT Synthamin 14, 8.5% Amino Acid Intravenous Infusion 2. QUALITATIVE AND QUANTITATIVE COMPOSITION L-Leucine Ph. Eur 0.620% w/v L-Isoleucine
Lipids Types, Food Sources, Functions
 Lipids Types, Food Sources, Functions What Are Lipids? Lipids Diverse group of molecules that are insoluble in water Fats The lipid content of diets and foods 1 Lipids in Body Cells and Tissues Types of
Lipids Types, Food Sources, Functions What Are Lipids? Lipids Diverse group of molecules that are insoluble in water Fats The lipid content of diets and foods 1 Lipids in Body Cells and Tissues Types of
Amanda Hernandez FND Parenteral Nutrition Worksheet October 26, 2011
 Amanda Hernandez FND 430-001 Parenteral Nutrition Worksheet October 26, 2011 1. HP needs TPN because he has short bowel syndrome and his GI tract is not functional. His entire jejunum was and proximal
Amanda Hernandez FND 430-001 Parenteral Nutrition Worksheet October 26, 2011 1. HP needs TPN because he has short bowel syndrome and his GI tract is not functional. His entire jejunum was and proximal
Intestinal Rehabilitation and Transplantation
 Intestinal Rehabilitation and Transplantation Joel Lim, MD Associate Professor of Pediatrics Children s Mercy Hospital University of Missouri in Kansas City Objective: Intestinal Failure/Short Bowel Syndrome
Intestinal Rehabilitation and Transplantation Joel Lim, MD Associate Professor of Pediatrics Children s Mercy Hospital University of Missouri in Kansas City Objective: Intestinal Failure/Short Bowel Syndrome
Product Category: Promote
 Product Category: Promote Promote Promote with Fiber Updated 4/28/2016 Very-High-Protein Nutrition Product Information: Promote 1 of 5 Very-High-Protein Nutrition PROMOTE is a complete, balanced, very-high-protein
Product Category: Promote Promote Promote with Fiber Updated 4/28/2016 Very-High-Protein Nutrition Product Information: Promote 1 of 5 Very-High-Protein Nutrition PROMOTE is a complete, balanced, very-high-protein
Product Information: Vital AF 1.2 Cal
 Product Information: Vital AF 1.2 Cal 1 of 5 VITAL AF 1.2 CAL is Advanced Formula therapeutic nutrition with ingredients to help manage inflammation and symptoms of GI intolerance. For tube or oral feeding.
Product Information: Vital AF 1.2 Cal 1 of 5 VITAL AF 1.2 CAL is Advanced Formula therapeutic nutrition with ingredients to help manage inflammation and symptoms of GI intolerance. For tube or oral feeding.
Product Information: Similac Expert Care Alimentum
 Product Information: Similac Expert Care Alimentum 1 of 6 A nutritionally complete, hypoallergenic formula for infants, including those with colic symptoms due to protein sensitivity. A supplemental beverage
Product Information: Similac Expert Care Alimentum 1 of 6 A nutritionally complete, hypoallergenic formula for infants, including those with colic symptoms due to protein sensitivity. A supplemental beverage
Digestion and Absorption
 Digestion and Absorption Digestion and Absorption Digestion is a process essential for the conversion of food into a small and simple form. Mechanical digestion by mastication and swallowing Chemical digestion
Digestion and Absorption Digestion and Absorption Digestion is a process essential for the conversion of food into a small and simple form. Mechanical digestion by mastication and swallowing Chemical digestion
Parenteral Nutrition in IBD: Any indication?
 Parenteral Nutrition in IBD: Any indication? Name: Institution: Marianna Arvanitakis Erasme University Hospital, Brussels, Belgium Clinical case 42 year old male Crohn s disease since he was 16 years old
Parenteral Nutrition in IBD: Any indication? Name: Institution: Marianna Arvanitakis Erasme University Hospital, Brussels, Belgium Clinical case 42 year old male Crohn s disease since he was 16 years old
Breast Milk. Composition of Breast Milk
 Breast Milk Composition of Breast Milk Knowledge of the biological composition and constituents of breast milk are critical to the dietitian, because they form the rationale for effective practice in both
Breast Milk Composition of Breast Milk Knowledge of the biological composition and constituents of breast milk are critical to the dietitian, because they form the rationale for effective practice in both
Product Information: TwoCal HN
 Product Information: TwoCal HN 1 of 5 TWOCAL HN is a nutritionally complete, high-calorie formula designed to meet the increased protein and calorie needs of stressed patients and patients requiring low-volume
Product Information: TwoCal HN 1 of 5 TWOCAL HN is a nutritionally complete, high-calorie formula designed to meet the increased protein and calorie needs of stressed patients and patients requiring low-volume
Inflammatory Bowel Disease
 + Inflammatory Bowel Disease Christina Kalafsky, Dietetic Intern University of Maryland College Park Children s National Medical Center Case Study January 31, 2014 + Outline n Inflammatory Bowel Disease
+ Inflammatory Bowel Disease Christina Kalafsky, Dietetic Intern University of Maryland College Park Children s National Medical Center Case Study January 31, 2014 + Outline n Inflammatory Bowel Disease
Case Study BMIs in the range of are considered overweight. Therefore, F.V. s usual BMI indicates that she was overweight.
 Morgan McFarlane February 26 th, 2013 HHP 439 Professor White Case Study 7.10 1. What is your interpretation of F.V. s clinical data? F.V. s clinical data includes chronic abdominal pain, loose stools,
Morgan McFarlane February 26 th, 2013 HHP 439 Professor White Case Study 7.10 1. What is your interpretation of F.V. s clinical data? F.V. s clinical data includes chronic abdominal pain, loose stools,
LITTLE TREASURE. Premium Australian Made Powdered Milk Products
 LITTLE TREASURE Premium Australian Made Powdered Milk Products Little Treasure Infant Formula and other Milk Powder products. Made in Australia to the highest possible standard, using milk from Australian
LITTLE TREASURE Premium Australian Made Powdered Milk Products Little Treasure Infant Formula and other Milk Powder products. Made in Australia to the highest possible standard, using milk from Australian
Product Information: PediaSure (Institutional)
") Product Information: PediaSure (Institutional) 1 of 5 PediaSure is a source of complete, balanced nutrition especially designed for children 1 to 13 years of age. May be used as the sole source of nutrition
Product Information: PediaSure (Institutional) 1 of 5 PediaSure is a source of complete, balanced nutrition especially designed for children 1 to 13 years of age. May be used as the sole source of nutrition
Human milk. The Gold Standard. Human milk. Human milk. Human milk. Human milk. 3 Types of Human Milk 4/23/2015
 The Gold Standard Defining characteristic of the class Mammalian Ability to produce designed specifically to nourish the young It is a unique complex fluid with a species specific composition It is the
The Gold Standard Defining characteristic of the class Mammalian Ability to produce designed specifically to nourish the young It is a unique complex fluid with a species specific composition It is the
Principles of nutrition in the preterm infant. Importance of nutrition: Undernutrition is very common in VLBW infants
 Principles of nutrition in the preterm infant Dr. S. Navarro-Psihas Pädiatrie IV, Klinik für Neonatologie Medizinische Universität Innsbruck Importance of nutrition: Undernutrition is very common in VLBW
Principles of nutrition in the preterm infant Dr. S. Navarro-Psihas Pädiatrie IV, Klinik für Neonatologie Medizinische Universität Innsbruck Importance of nutrition: Undernutrition is very common in VLBW
TRANSPARENCY COMMITTEE OPINION. 19 March Date of the Marketing Authorisation (national procedure): 18 December 1997
: 18 December 1997") The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 19 March 2008 INTRALIPIDE 20 PER CENT, emulsion for infusion 100 ml in Excel container (PE/PP) (CIP: 355 096-5) 250
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 19 March 2008 INTRALIPIDE 20 PER CENT, emulsion for infusion 100 ml in Excel container (PE/PP) (CIP: 355 096-5) 250
Nutrition Basics. Chapter McGraw-Hill Higher Education. All rights reserved.
 Nutrition Basics Chapter 12 1 The Body s Nutritional Requirements Essential nutrients The Six Essential Nutrients: Proteins, Fats, Carbohydrates, Vitamins, Minerals, Water Defined as : Nutrients one must
Nutrition Basics Chapter 12 1 The Body s Nutritional Requirements Essential nutrients The Six Essential Nutrients: Proteins, Fats, Carbohydrates, Vitamins, Minerals, Water Defined as : Nutrients one must
Nutrition in the premie World
 SURVIVAL AND GROWTH NUTRITION ESSENTIALS Nutrition in the premie World DR VISH SUBRAMANIAN MD MRCP (UK) FAAP NEONATAL CRITICAL CARE MERCY CHILDRENS HOSPITAL., SPRINGFIELD MO Prematurity Nutritional Requirements
SURVIVAL AND GROWTH NUTRITION ESSENTIALS Nutrition in the premie World DR VISH SUBRAMANIAN MD MRCP (UK) FAAP NEONATAL CRITICAL CARE MERCY CHILDRENS HOSPITAL., SPRINGFIELD MO Prematurity Nutritional Requirements
STRATEGIES TO IMPROVE ENTERAL FEEDING TOLERANCE. IS IT WORTH IT? ENGELA FRANCIS RD(SA)
") STRATEGIES TO IMPROVE ENTERAL FEEDING TOLERANCE. IS IT WORTH IT? ENGELA FRANCIS RD(SA) DEFINITION OF ENTERAL FEEDING INTOLERANCE Gastrointestinal feeding intolerance are usually defined as: High gastric
STRATEGIES TO IMPROVE ENTERAL FEEDING TOLERANCE. IS IT WORTH IT? ENGELA FRANCIS RD(SA) DEFINITION OF ENTERAL FEEDING INTOLERANCE Gastrointestinal feeding intolerance are usually defined as: High gastric
Product Information: TwoCal HN
 Product Information: TwoCal HN 1 of 5 TWOCAL HN Calorie and Protein Dense Nutrition with FOS is a nutritionally complete, high-calorie liquid food for stressed patients and those requiring low-volume feedings.
Product Information: TwoCal HN 1 of 5 TWOCAL HN Calorie and Protein Dense Nutrition with FOS is a nutritionally complete, high-calorie liquid food for stressed patients and those requiring low-volume feedings.
List of Topics and Modules (2012)
") List of Topics and Modules (202) Code Title Credits for Live course Topic 0 Introduction to Clinical Nutrition EDU T0 M 0. Introduction to clinical nutrition support Topic Metabolism of Metabolism of Macronutrients,
List of Topics and Modules (202) Code Title Credits for Live course Topic 0 Introduction to Clinical Nutrition EDU T0 M 0. Introduction to clinical nutrition support Topic Metabolism of Metabolism of Macronutrients,
3.9 Carbohydrates. Provide building materials and energy storage. Are molecules that contain carbon, hydrogen and oxygen in a 1:2:1 ratio
 3.9 Carbohydrates Provide building materials and energy storage Are molecules that contain carbon, hydrogen and oxygen in a 1:2:1 ratio Are of two main types Simple carbohydrates Complex carbohydrates
3.9 Carbohydrates Provide building materials and energy storage Are molecules that contain carbon, hydrogen and oxygen in a 1:2:1 ratio Are of two main types Simple carbohydrates Complex carbohydrates
Intradialytic Parenteral Nutrition in Hemodialysis Patients. Hamdy Amin, Pharm.D., MBA, BCNSP Riyadh, Saudi Arabia
 Intradialytic Parenteral Nutrition in Hemodialysis Patients Hamdy Amin, Pharm.D., MBA, BCNSP Riyadh, Saudi Arabia Disclosure Information Intradialytic Parenteral Nutrition in Hemodialysis Patients Hamdy
Intradialytic Parenteral Nutrition in Hemodialysis Patients Hamdy Amin, Pharm.D., MBA, BCNSP Riyadh, Saudi Arabia Disclosure Information Intradialytic Parenteral Nutrition in Hemodialysis Patients Hamdy
Surgical Nutrition for the Cardiothoracic Patient. Stephanie Kunioki RD, CNSC, LD Memorial Hermann TMC
 Surgical Nutrition for the Cardiothoracic Patient Stephanie Kunioki RD, CNSC, LD Memorial Hermann TMC Financial Disclosures NONE Declared PROPER NUTRITION Surgical Effects on Nutrition Intake & Status
Surgical Nutrition for the Cardiothoracic Patient Stephanie Kunioki RD, CNSC, LD Memorial Hermann TMC Financial Disclosures NONE Declared PROPER NUTRITION Surgical Effects on Nutrition Intake & Status
PARENTAL NUTRITION SUPPORT. Dr Rezzan Khan Consultant Nutritionist Shifa International Hospital
 PARENTAL NUTRITION SUPPORT Dr Rezzan Khan Consultant Nutritionist Shifa International Hospital Objectives Explain the indications and contraindications of PN Describe the types of PN How to set PN Explain
PARENTAL NUTRITION SUPPORT Dr Rezzan Khan Consultant Nutritionist Shifa International Hospital Objectives Explain the indications and contraindications of PN Describe the types of PN How to set PN Explain
What s s up with Omegaven????? Kathleen Gura PharmD Children s s Hospital Boston
 What s s up with Omegaven????? Kathleen Gura PharmD Children s s Hospital Boston Disclosures Funding : March of Dimes FDA Orphan Drug Grants Program NIH Children s s Hospital Surgical Foundation Patent
What s s up with Omegaven????? Kathleen Gura PharmD Children s s Hospital Boston Disclosures Funding : March of Dimes FDA Orphan Drug Grants Program NIH Children s s Hospital Surgical Foundation Patent
Product Information: Glucerna 1.2 Cal
 Product Information: Glucerna 1.2 Cal 1 of 5 GLUCERNA 1.2 CAL is a calorically dense formula that has CarbSteady, including low glycemic carbohydrates clinically shown to help minimize blood glucose response.
Product Information: Glucerna 1.2 Cal 1 of 5 GLUCERNA 1.2 CAL is a calorically dense formula that has CarbSteady, including low glycemic carbohydrates clinically shown to help minimize blood glucose response.
Advances in intestinal Rehabilitation Susan Hill Gastroenterology Consultant
 Advances in intestinal Rehabilitation Susan Hill Gastroenterology Consultant 2 Indication for intravenous nutrition/pn: Intestinal Failure Inability to maintain weight and growth despite adequate enteral
Advances in intestinal Rehabilitation Susan Hill Gastroenterology Consultant 2 Indication for intravenous nutrition/pn: Intestinal Failure Inability to maintain weight and growth despite adequate enteral