Eric Magrum PT, DPT, OCS, FAAOMPT Orthopaedic Manual Physical Therapy Series Charlottesville
|
|
|
- Stanley Hampton
- 5 years ago
- Views:
Transcription


1 SHOULDER CASE 3 Eric Magrum PT, DPT, OCS, FAAOMPT Orthopaedic Manual Physical Therapy Series Charlottesville Reproduction Without Consent 1

2 Reproduction Without Consent 2
 Instability - Load and")

3 Instability - Sulcus Sign Multidirectional instability Sitting: Arm in Neutral Inferior Traction on humerus at elbow Test Distance between inferior acromium, superior aspect humeral head Graded: (cm displacement) Instability - Load and Shift Pt: Seated/Supine Test : Humeral head is loaded to centre it congruently within the glenoid fossa; then manually shifted anteriorly and posteriorly, relative to the glenoid fossa. (+) Laxity/Subluxation over glenoid rim Reproduction Without Consent 3


4 Instability (Posterior)- Posterior Subluxation (Jerk) Test Posterior instability Pt: Sitting Test: Scapular plane, IR, Flexion; Posteriorly directed force. Bring humerus into Horizontal ADD (+/-) ER (+) Test : Clunk as posterior subluxation is reproduced Instability - Apprehension Pt: Supine 90 ABD, Maximal ER Contact: Posterior aspect GH Test : Anterior force at end ROM ER (+) Apprehension > Pain Reproduction Without Consent 4
 Reduction in Pain/Apprehension;")


5 Pt: Supine 90 ABD, maximal ER Instability - Relocation Contact: Anterior aspect GH Test: Posterior force to humeral head at end ROM ER (+) Reduction in Pain/Apprehension; Increased ER TUBS: Glenohumeral Instability Traumatic - Significant traumatic event Unilateral / Unidirectional instability Bankart lesion Anterior Inferior Labrum Surgery required to stabilize the GH joint AMBRI A traumatic Multidirectional Instability Bilateral Rehabilitation Inferior Capsular Shift, Rotator Interval closure Reproduction Without Consent 5


 Neuromuscular")


6 MDI Etiology : Multifactorial Anatomic Distended inferior pouch and a wide rotator interval Global increase in capsular volume, resulting in overall laxity Pathologic changes with degenerative Labrum and Bankart lesions Biochemical Capsule has alterations in type and quantity of collagen Collagen Disorders (Ehlers-Danlos) Neuromuscular Repeated micro trauma (athletes) - Repetitive overhead use Cumulative into global laxity Labral pathology Laxity Instability Adaptive for Sport,? pathological Strength Neuromuscular control» Rotator cuff» Scapular stabilizers Reproduction Without Consent 6


7 Traumatic Anterior Dislocation Anteroinferiorly displaced humeral head stretches the capsuloligamentous components Detachment of the anterior-inferior labrum - Bankartnkart Hill Sachs lesions (SLAP) lesions Capsular tears Rotator cuff tears Glenoid rim fractures Boone JL BJSM 2010 Reproduction Without Consent 7

8 Acute Dislocation Young patients (<24 years) 97% : Bankart lesions 89% : Hill Sachs lesions 10% incidence of SLAP lesions No rotator cuff tears Progressive labral-ligamentous injury and degeneration with increasing episodes of dislocation Postoperative arthritis correlated with an increased number of dislocations Reoccurrence rates: 72 95% < 20 yo 70 82% yo Boone JL BJSM % >50 yo Acute Dislocation - Recommendations Young patients (15 25 years) Early Surgical Repair Shown to reduce their recurrence rate from 80 90% to 3 15% and improve overall quality of life Patients aged years Initial trial of non-operative management Risk of re-dislocation is much lower at 20 30% Patients >40 yo Typically manage them non-operatively Low recurrence rate of 10 15% Address associated injuries RTC tears Bone defects Neurological injury Handoll HH Cochrane Database Syst Rev 2004 Reproduction Without Consent 8



 2.")
9 Recurrent Instability Males 3.2 x > likely < 40 year olds 13.5 x > likely Greater Tuberosity Fx 7 x < likely Hyperlaxity (Beighton) 2.7 x > likely Patterson WH JBJS 2010 Reproduction Without Consent 9




10 Gaunt BC JOSPT 2010 Gaunt BC JOSPT 2010 Reproduction Without Consent 10


11 Post OP Guidelines: Bankart Phase 1 : Healing (0-6 weeks) Education Immobilization 0-4 weeks Strict ROM Guidelines Scapular stabilization Submax RTC isometrics AAROM Wand, Pulley, Table step back Post OP Guidelines: Bankart Phase 2 : Controlled Loading (6-12 weeks) Education Progress ROM to Full gradually - Guidelines Scapular Stabilization Post Capsule mobility - prn RTC NM control Low weight/high Reps Avoid compensations Reproduction Without Consent 11
12 Post OP Guidelines: Bankart Phase 3 : Normalize Strength, Power, Endurance Function (12-24 weeks) Full ROM all planes Gradual stresses to ant capsule Multiplanar mvts Progressive weight bearing Plyometrics Sport/Work specific strengthening Reproduction Without Consent 12
 mechanical signs/sx Bucket-handle tear of from a Type III or Type IV SLAP lesion (+) LR : 2.44 (-) LR : 0.")
13 Inferior Capsular Shift AMBRI Pt : Sitting or Supine Scaption 160 degrees Axial load with humeral internal <-> external rotation (+) pain with external rotation (+) mechanical signs/sx Bucket-handle tear of from a Type III or Type IV SLAP lesion (+) LR : 2.44 (-) LR : 0.51 SLAP - Crank Test Reproduction Without Consent 13
 Horizontal ADD with a posterosuperior directed force (posterior labral) Pt stand/sit Hands")

14 Labral: Compression-Rotation Test Glenohumeral joint long axis compression with rotation (+) Provocation: Grind the labrum between the glenoid and the humeral head degrees Variations Horizontal ABD with an anterosuperior directed force (anterosuperior labral lesions) Horizontal ADD with a posterosuperior directed force (posterior labral) Pt stand/sit Hands on hips, thumbs pointing posteriorly PT: Stabilize scapula posteriorly, over anterior acromium. SLAP - Anterior Slide Test Opposite hand posterior aspect elbow. Anterior, superior force through elbow. (+) Test: mechanical signs/sxs ( clicking ); reproduction of sxs Anterior, superior humeral head translation stress superior labrum; traction biceps tendon Reproduction Without Consent 14
 Pain/mechanical signs as superior labrum peeled")
: P!")
15 SLAP Biceps Load II Pt Supine arm ABD to 120 degrees, maximal ER, elbow flexed to 90, supination Test Resist elbow flexion (+) Pain/mechanical signs as superior labrum peeled off glenoid SLAP Biceps involvement Speed s Test Pt : Seated Elbow extended, full supination Test : Resist flexion 0-60 degrees (+): P! bicepital groove Reproduction Without Consent 15
 reproduce Pain (+) LR : 8.83 (-) LR : 0.")
 mechanical symptoms, posterior joint pain (+) LR : 31.57 (-) LR : 0.")
16 SLAP Passive Distraction Test Shoulder Flexed to 150 degrees Elbow extended, Forearm supinated Test: Forearm pronation (+) reproduce Pain (+) LR : 8.83 (-) LR : 0.50 SLAP - Dynamic Labral Shear Test Passive ABD to 120 degrees Full ER at 90 degrees Shoulder lowered 120 to 60 degrees (+) mechanical symptoms, posterior joint pain (+) LR : (-) LR : 0.29 Reproduction Without Consent 16
 AC - Incr superior P!")
 Relocation Test (+) Active Compression Test (+) LR : 4.56 (-) LR 0.")
17 AC/Labral - O Brien Test/Active Compression Pt : Standing flexed to 90 degrees, 15 degrees Horiz ADD, full IR (pronation) Resist flexion pronated Repeat in full supination (+) AC - Incr superior P! (+) Labral Incr deep non specific shoulder pain (+) Pain Decreased Pain (+) LR (SLAP) : 1.06 (-) LR : (SLAP) : 0.89 Test Cluster Labral Tear (+) Relocation Test (+) Active Compression Test (+) LR : 4.56 (-) LR 0.65 (+) Relocation Test (+) Apprehension Test (+) LR : 5.43 (-) LR : 0.67 Reproduction Without Consent 17


18 AC Posterior Shear Compression Paxinos Test Pt: Seated, UE neutral PT: Standing perpendicular to shoulder Anterior hand contact distal Clavicle Posterior hand stabilize posterior Acromium Assess: Posterior glide Clavicle on Acromium Shear/Compression; Provoke Sxs Reproduction Without Consent 18
 Overhead")
19 5 SLAP tests O Brien s Dynamic Labral Shear Test Speed s Biceps Load II Labral Tension MRI Confirmed Arthroscopically None provided diagnostic utility Stand alone Clustered 56% Concomitant findings Biceps Load II test demonstrated utility in identifying patients with a SLAP-only lesion, with a PPV = 26 Choosing which SLAP test Subjective Exam should guide your Objective Exam (1) Overhead Athletes that present with peel-back lesions (2) Compression injuries from someone that falls onto an outstretched arm or on the side of the shoulder. This will compress and sheer the labrum, similar to a meniscus tear (3) Traction injuries from a sudden eccentric biceps contraction (least common) Peel-Back Injury: Biceps Load II Crank Compression Injury: Active Compression Compression Rotation Passive Distraction Dynamic Labral Shear Traction Injury: Speed s Active Compression Reproduction Without Consent 19



 31% exhibited a combined anterior and superior lesion")
20 Dodson CC JOSPT 2009 Type I SLAP lesions Isolated fraying of the superior labrum with a firm attachment of the labrum to the glenoid Degenerative? Normal finding Type II SLAP lesions Detachment of the superior labrum and the origin of the tendon of the long head of the biceps brachii from the glenoid resulting in instability of the bicepslabral anchor Most common Three distinct sub-categories of type II SLAP lesions 37% presented with an anterosuperior lesion(traumatic) 31% with a posterosuperior lesion (overhead athletes ) 31% exhibited a combined anterior and superior lesion Reproduction Without Consent 20

21 Type III SLAP lesions Bucket-handle tear of the labrum with an intact biceps insertion The labrum tears and flips into the joint similar to a meniscal tear Type IV SLAP lesions Bucket-handle tear of the labrum involving the biceps tendon Instability of the bicepslabrum anchor is also present Mechanism - SLAP Traumatic Compression of the superior joint surfaces superimposed with subluxation of the humeral head FOOSH Bracing oneself during a motor vehicle accident Direct blows Falling onto the point of the shoulder Forceful traction injuries of the upper extremity Repetitive Overhead Use Throwing Athletes High Eccentric activity of the biceps brachii during the arm deceleration and follow-through phases of the overhead throw Peel back mechanism Reproduction Without Consent 21
 Partial")
22 Shoulder in a position of ABD and maximal EXT ROT Rotation produces a twist at the base of the biceps Torsional force to the anchor Peel Back SLAP lesions Combination biceps activity during deceleration may serve to weaken the bicepslabrum complex Torsional peel back force may result in the posterosuperior detachment of the labral anchor Concomitant Injuries 45% (73% pitchers) Partial thickness RTC tear (supraspinatus) 11% Complete RTC tear 22% Bankart lesion Type I RTC pathology Type III/IV Instability Type II Older Patients = RTC pathology Younger = Anterior instability SLAP Reproduction Without Consent 22

23 Glenoid Labral Tears: Presentation Hx repetitive overhead / long head biceps eccentrics Sx with arm in overhead position Deep, Non-specific post shoulder ache Mechanical signs/sxs: painful or non-painful pop/catch/click Hx of dislocation / subluxation C/o instability Click/catch may be reproduced w/ special tests Additional Dx?: Impingement, GH instability, RTC tear Reproduction Without Consent 23

24 Dodson CC JOSPT 2009 Reproduction Without Consent 24



25 Circle Concept of Stability Balance of Passive/Dynamic Restraints Ligamentous lesion on one side of the joint capsule may result in shifting loads to the opposite side of the capsule permitting the humeral head to subluxate or dislocate Loss of IR of the throwing shoulder of 20 or more as compared with the non throwing shoulder = GIRD TRM in the throwing shoulders of professional baseball pitchers is within 5 of the non throwing shoulder Reproduction Without Consent 25



26 Assessment of GIRD: Glenohumeral internal rotation is measured with the patient in supine position, the shoulder abducted 90, and the scapula stabilised against the table Cools A M BJSM 2008 Causes of GIRD Osseous Capsular contracture Muscular (ER) tightness Scapular positioning Posture Reproduction Without Consent 26

27 GIRD is a loss of IR ROM in the presence of a loss of TRM Loss of side-to-side IR is actually a normal anatomical variation in overhead athletes and should not be considered pathological GIRD unless there is a subsequent loss of total rotational motion in the dominant arm as well. GIRD = (Side-to-side difference in ER) + (Side-to-side difference in IR) Player 1 = (D ER 120 deg ND ER 100 deg = +20 deg ER) + (D IR 60 deg ND IR 80 deg = -20 deg IR) = 0 deg Loss of 20 degrees this is not pathological GIRD because total motion is the same bilaterally Player 2 = (D ER 120 deg ND ER 100 deg = +20 deg ER) + (D IR 35 deg ND IR 80 deg = -45 deg IR) = -25 deg GIRD This represents a pathological GIRD because both IR and total rotational motion are limited Reproduction Without Consent 27


28 Reproduction Without Consent 28


29 Reproduction Without Consent 29


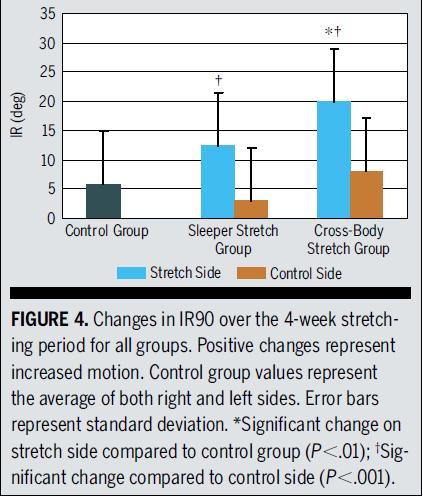
30 McClure JOSPT 2007 Reproduction Without Consent 30





31 ¼ Rotation back Contract relax Elbow up on towel to increase post capsule stretch Reproduction Without Consent 31


32 Performing the Sleeper Stretch Correctly Scapula position Roll onto your side and make sure that your scapula is retracted; lie mostly on your rib cage and the outside border of your scapula Shoulder position Roll backwards so you body is facing upward at close to a 45 degree angle - into the scapular plane that stretches more of the posterior musculature. Intensity Gently push down until you feel a MILD stretch and hold for 30 seconds. The goal is to feel a mild stretch in the back of your shoulder. Do this gently for a few reps MikeReinold.com Performing the Cross Body Horiz ADD Stretch Correctly ¼ Rotation back to stabilize scapula Pull into Horizontal ADD Restrict ER Contract Relax Horiz ABD EXT ROT Reproduction Without Consent 32



33 STM to Posterior RTC Teres STM with active elevation Reproduction Without Consent 33

34 LAB Cross Body stretch MET Sleeper stretch STM post RTC Self STM post RTC Reproduction Without Consent 34

35 Key Factors in the Rehabilitation of Shoulder Instability Chronicity of Shoulder Instability Degree of Shoulder Instability Concomitant Pathology Direction of Shoulder Instability Neuromuscular Control Pre-Injury Activity Level Reproduction Without Consent 35





36 Reproduction Without Consent 36





37 Squat and Reach High Row Low Row Reproduction Without Consent 37



38 Reproduction Without Consent 38
 Rehab: Restore")
39 Treatment Principles Proprioception Kinesthesia Joint reposition sense Progress to fatigued proprioception training Injury to static restraints alters sensorimotor response Functional Instability Altered Proprioception/Kinesthesia Patients with instability CNS processing alterations Bilateral deficit Pain affects proprioception Muscle activation dysfunction (RTC co contraction) Rehab: Restore RTC co contraction Perturbations Plyometrics CKC Myers JB Man Ther 2006 Reproduction Without Consent 39





40 Proprioception Ther Ex Sport Specific Training Neuromuscular Re-Education Unconscious Incompetence Conscious Incompetence Conscious Competence Unconscious Competence Reproduction Without Consent 40



41 Sports Health 2014 Virag B Hand Entry Resist upward force of water Max elevation angle Scapular dyskinesia = IMP Peak Serratus activity Upward Scapular rotation Reproduction Without Consent 41


42 Sports Health 2014 Virag B Reproduction Without Consent 42


43 Reproduction Without Consent 43


44 Mid Pull through Pull body over stable UE Scapular dyskinesia = IMP High Elbow increased surface area INT ROT GH; not Scapula Stable Scapula Reproduction Without Consent 44


45 Sports Health 2014 Virag B Reproduction Without Consent 45


46 Reproduction Without Consent 46


47 Primary Ant IMP Recovery Secondary Post IMP laxity ER strength ER Endurance Scapular retraction/posterior tilt Reproduction Without Consent 47


48 Sports Health 2014 Virag B Reproduction Without Consent 48


49 Reproduction Without Consent 49

50 IR/ER tubing at 0 of abduction seated on stability ball Full can seated on stability ball Lateral raise to 90 of abduction seated on stability ball Side-lying external rotation (plank) T raises prone on stability ball Y raises prone on stability ball Phys Sp Med 2011_Wilk KE Prone row into ER on stability ball Lower Trapezius 5 Series Phys Sp Med 2011_Wilk KE Shoulder extension in ER seated on stability ball Shoulder extension at 45 in ER seated on stability ball Standing wall circle slides Standing low row Standing table press-downs with scapular depression Biceps curls/triceps extensions seated on stability ball Wrist flexion/extension and supination/pronation Reproduction Without Consent 50

51 Reproduction Without Consent 51


52 Reproduction Without Consent 52
Orthopaedic Manual Physical Therapy Series Orthopaedic Manual Physical Therapy Series
 SHOULDER CASE3 Eric Magrum PT, DPT, OCS, FAAOMPT Orthopaedic Manual Physical Therapy Series Charlottesville 2017-2018 Reproduction Without Consent 1 Instability - Sulcus Sign Instability - Load and Shift
SHOULDER CASE3 Eric Magrum PT, DPT, OCS, FAAOMPT Orthopaedic Manual Physical Therapy Series Charlottesville 2017-2018 Reproduction Without Consent 1 Instability - Sulcus Sign Instability - Load and Shift
WEEKEND 2 Shoulder. Shoulder Active Range of Motion Assessment
 Virginia Orthopedic Manual Physical Therapy Institute - 2016 Technique Manual WEEKEND 2 Shoulder Shoulder Active Range of Motion Assessment - Patient Positioning: Standing, appropriately undressed so that
Virginia Orthopedic Manual Physical Therapy Institute - 2016 Technique Manual WEEKEND 2 Shoulder Shoulder Active Range of Motion Assessment - Patient Positioning: Standing, appropriately undressed so that
Eric Magrum PT, DPT, OCS, FAAOMPT Orthopaedic Manual Physical Therapy Series Charlottesville
 SHOULDER EXAM Eric Magrum PT, DPT, OCS, FAAOMPT Orthopaedic Manual Physical Therapy Series Charlottesville 2017-2018 Reproduction Without Consent 1 Subjective History: Interrogate with Empathy Age Hand
SHOULDER EXAM Eric Magrum PT, DPT, OCS, FAAOMPT Orthopaedic Manual Physical Therapy Series Charlottesville 2017-2018 Reproduction Without Consent 1 Subjective History: Interrogate with Empathy Age Hand
SHOULDER EXAM. Differential Diagnosis
 SHOULDER EXAM Eric Magrum PT, DPT, OCS, FAAOMPT Orthopaedic Manual Physical Therapy Series Charlottesville 2017-2018 Subjective History: Interrogate with Empathy Age Hand Dominance Symptom onset Pain description
SHOULDER EXAM Eric Magrum PT, DPT, OCS, FAAOMPT Orthopaedic Manual Physical Therapy Series Charlottesville 2017-2018 Subjective History: Interrogate with Empathy Age Hand Dominance Symptom onset Pain description
SHOULDER INSTABILITY
 SHOULDER INSTABILITY Dr.KN Subramanian M.Ch Orth., FRCS (Tr & Orth), CCT Orth(UK) Consultant Orthopaedic Surgeon, Special interest: Orthopaedic Sports Injury, Shoulder and Knee Surgery, SPARSH Hospital
SHOULDER INSTABILITY Dr.KN Subramanian M.Ch Orth., FRCS (Tr & Orth), CCT Orth(UK) Consultant Orthopaedic Surgeon, Special interest: Orthopaedic Sports Injury, Shoulder and Knee Surgery, SPARSH Hospital
Rehabilitation Guidelines for Labral/Bankert Repair
 Rehabilitation Guidelines for Labral/Bankert Repair The true shoulder joint is called the glenohumeral joint and consists humeral head and the glenoid. It is a ball and socket joint. Anatomy of the Shoulder
Rehabilitation Guidelines for Labral/Bankert Repair The true shoulder joint is called the glenohumeral joint and consists humeral head and the glenoid. It is a ball and socket joint. Anatomy of the Shoulder
Type II SLAP lesions are created when the biceps anchor has pulled away from the glenoid attachment.
 Arthroscopic Superior Labral (SLAP) Repair Protocol-Type II, IV, and Complex Tears The intent of this protocol is to provide the clinician with a guideline of the post-operative rehabilitation course of
Arthroscopic Superior Labral (SLAP) Repair Protocol-Type II, IV, and Complex Tears The intent of this protocol is to provide the clinician with a guideline of the post-operative rehabilitation course of
OBJECTIVES. Therapists Management of Shoulder Instability SHOULDER STABILITY SHOULDER STABILITY WHAT IS SHOULDER INSTABILITY? SHOULDER INSTABILITY
 Therapists Management of Shoulder Instability Brian G. Leggin, PT, DPT, OCS Lead Therapist, Penn Therapy and Fitness at Valley Forge Adjunct Assistant Professor, Department of Orthopaedics, University
Therapists Management of Shoulder Instability Brian G. Leggin, PT, DPT, OCS Lead Therapist, Penn Therapy and Fitness at Valley Forge Adjunct Assistant Professor, Department of Orthopaedics, University
Arthroscopic Labral Repair Protocol-Type II, IV, and Complex Tears:
 Arthroscopic Labral Repair Protocol-Type II, IV, and Complex Tears: The intent of this protocol is to provide the clinician with a guideline of the postoperative rehabilitation course of a patient that
Arthroscopic Labral Repair Protocol-Type II, IV, and Complex Tears: The intent of this protocol is to provide the clinician with a guideline of the postoperative rehabilitation course of a patient that
Rehabilitation Protocol: Arthroscopic Anterior Capsulolabral Repair of the Shoulder - Bankart Repair Rehabilitation Guidelines
 Rehabilitation Protocol: Arthroscopic Anterior Capsulolabral Repair of the Shoulder - Bankart Repair Rehabilitation Guidelines Department of Orthopaedic Surgery Lahey Hospital & Medical Center, Burlington
Rehabilitation Protocol: Arthroscopic Anterior Capsulolabral Repair of the Shoulder - Bankart Repair Rehabilitation Guidelines Department of Orthopaedic Surgery Lahey Hospital & Medical Center, Burlington
SLAP Lesions Assessment & Treatment
 SLAP Lesions Assessment & Treatment Kevin E. Wilk,, PT, DPT Glenoid Labral Lesions Introduction Common injury - difficult to diagnose May occur in isolation or in combination SLAP lesions: Snyder: Arthroscopy
SLAP Lesions Assessment & Treatment Kevin E. Wilk,, PT, DPT Glenoid Labral Lesions Introduction Common injury - difficult to diagnose May occur in isolation or in combination SLAP lesions: Snyder: Arthroscopy
Shoulder Instability. Fig 1: Intact labrum and biceps tendon
 Shoulder Instability What is it? The shoulder joint is a ball and socket joint, with the humeral head (upper arm bone) as the ball and the glenoid as the socket. The glenoid (socket) is a shallow bone
Shoulder Instability What is it? The shoulder joint is a ball and socket joint, with the humeral head (upper arm bone) as the ball and the glenoid as the socket. The glenoid (socket) is a shallow bone
OrthoCarolina. Arthroscopic SLAP Lesion (Type II) Repair Protocol
 Repair Protocol") OrthoCarolina Arthroscopic SLAP Lesion (Type II) Repair Protocol Surgical Overview: SLAP, which stands for superior labrum anterior to posterior, lesions are labral detachments that originate posterior
OrthoCarolina Arthroscopic SLAP Lesion (Type II) Repair Protocol Surgical Overview: SLAP, which stands for superior labrum anterior to posterior, lesions are labral detachments that originate posterior
Aquatic Exercise. Rehabilitation after the SLAP lesion repair. I. Anatomy & Function SLAP 의가장흔한손상기전. Anatomy of the Shoulder (I)
") Aquatic Exercise Rehabilitation after the SLAP lesion repair Sports Medicine Clinic Sky 임승길 ATC 2 SLAP 의가장흔한손상기전 SLAP Superior Labrum Anterior to Posterior 1. Compression force Attempting to catch a heavy
Aquatic Exercise Rehabilitation after the SLAP lesion repair Sports Medicine Clinic Sky 임승길 ATC 2 SLAP 의가장흔한손상기전 SLAP Superior Labrum Anterior to Posterior 1. Compression force Attempting to catch a heavy
Phase I : Immediate Postoperative Phase- Protected Motion. (0-2 Weeks)
") Phase I : Immediate Postoperative Phase- Protected Motion (0-2 Weeks) Appointments Progression Criteria 2 weeks after surgery Rehabilitation appointments begin within 7-10 days of surgery, continue 1-2
Phase I : Immediate Postoperative Phase- Protected Motion (0-2 Weeks) Appointments Progression Criteria 2 weeks after surgery Rehabilitation appointments begin within 7-10 days of surgery, continue 1-2
Rehabilitation Guidelines for Anterior Shoulder Reconstruction with Arthroscopic Bankart Repair
 UW HEALTH SPORTS REHABILITATION Rehabilitation Guidelines for Anterior Shoulder Reconstruction with Arthroscopic Bankart Repair The anatomic configuration of the shoulder joint (glenohumeral joint) is
UW HEALTH SPORTS REHABILITATION Rehabilitation Guidelines for Anterior Shoulder Reconstruction with Arthroscopic Bankart Repair The anatomic configuration of the shoulder joint (glenohumeral joint) is
Nonoperative Treatment For Rotator Cuff Tendinitis/ Partial Thickness Tear Dr. Trueblood
 Nonoperative Treatment For Rotator Cuff Tendinitis/ Partial Thickness Tear Dr. Trueblood Relieving Pain Patients who present with SIS will have shoulder pain that is exacerbated with overhead activities.
Nonoperative Treatment For Rotator Cuff Tendinitis/ Partial Thickness Tear Dr. Trueblood Relieving Pain Patients who present with SIS will have shoulder pain that is exacerbated with overhead activities.
SHOULDER DISLOCATION & INSTABILITY Rehabilitation Considerations
 SHOULDER DISLOCATION & INSTABILITY Rehabilitation Considerations Meagan Pehnke, MS, OTR/L, CHT, CLT March 1 st, 2019 Philadelphia Surgery & Rehabilitation of the Hand: Pediatric Pre-course OUTLINE Discuss
SHOULDER DISLOCATION & INSTABILITY Rehabilitation Considerations Meagan Pehnke, MS, OTR/L, CHT, CLT March 1 st, 2019 Philadelphia Surgery & Rehabilitation of the Hand: Pediatric Pre-course OUTLINE Discuss
Rehabilitation of Overhead Shoulder Injuries
 Rehabilitation of Overhead Shoulder Injuries 16 th Annual Primary Care Orthopaedic & Sports Medicine Symposium January 29, 2016 Jeremy Sherman, PT, MPT Disclosures No financial disclosures to note. Jeremy
Rehabilitation of Overhead Shoulder Injuries 16 th Annual Primary Care Orthopaedic & Sports Medicine Symposium January 29, 2016 Jeremy Sherman, PT, MPT Disclosures No financial disclosures to note. Jeremy
DIFFERENTIAL DIAGNOSIS: Looking for the causes of impingement
 DIFFERENTIAL DIAGNOSIS: Looking for the causes of Ann Cools, PT, PhD Ghent University - Belgium Dept of Rehabilitation Sciences & Physiotherapy Ann.Cools@UGent.be «thinking about.» Which special tests
DIFFERENTIAL DIAGNOSIS: Looking for the causes of Ann Cools, PT, PhD Ghent University - Belgium Dept of Rehabilitation Sciences & Physiotherapy Ann.Cools@UGent.be «thinking about.» Which special tests
REMINDER. Obtain medical clearance and physician s release prior to beginning an exercise program for clients with medical or orthopedic concerns
 Understanding Shoulder Dysfunction REMINDER Obtain medical clearance and physician s release prior to beginning an exercise program for clients with medical or orthopedic concerns What is a healthy shoulder?
Understanding Shoulder Dysfunction REMINDER Obtain medical clearance and physician s release prior to beginning an exercise program for clients with medical or orthopedic concerns What is a healthy shoulder?
Patient ID. Case Conference. Physical Examination. Image examination. Treatment 2011/6/16
 Patient ID Case Conference R3 高逢駿 VS 徐郭堯 55 y/o female C.C.: recurrent right shoulder dislocation noted since falling down injury 2 years ago Came to ER because of dislocation for many times due to minor
Patient ID Case Conference R3 高逢駿 VS 徐郭堯 55 y/o female C.C.: recurrent right shoulder dislocation noted since falling down injury 2 years ago Came to ER because of dislocation for many times due to minor
Rehabilitation Guidelines for Anterior Shoulder Reconstruction with Open Bankart Repair
 UW HEALTH SPORTS REHABILITATION Rehabilitation Guidelines for Anterior Shoulder Reconstruction with Open Bankart Repair The anatomic configuration of the shoulder joint (glenohumeral joint) is often compared
UW HEALTH SPORTS REHABILITATION Rehabilitation Guidelines for Anterior Shoulder Reconstruction with Open Bankart Repair The anatomic configuration of the shoulder joint (glenohumeral joint) is often compared
SLAP LESION REPAIR PROTOCOL
 SLAP LESION REPAIR PROTOCOL Clarkstown Division This rehabilitation protocol has been developed for the patient following a SLAP (Superior Labrum Anterior Posterior) repair. It is extremely important to
SLAP LESION REPAIR PROTOCOL Clarkstown Division This rehabilitation protocol has been developed for the patient following a SLAP (Superior Labrum Anterior Posterior) repair. It is extremely important to
Rehabilitation Guidelines for Large Rotator Cuff Repair
 Rehabilitation Guidelines for Large Rotator Cuff Repair The true shoulder joint is called the glenohumeral joint and consists humeral head and the glenoid. It is a ball and socket joint. Anatomy of the
Rehabilitation Guidelines for Large Rotator Cuff Repair The true shoulder joint is called the glenohumeral joint and consists humeral head and the glenoid. It is a ball and socket joint. Anatomy of the
Glenohumeral Joint Instability: An Athlete s Perspective
 Anatomic Considerations Glenohumeral Joint Instability: An Athlete s Perspective Michael D. Loeb, MD Texas Orthopedics, Sports Medicine, and Rehabilitation Associates Austin, Texas Static Stabilizers Osseous
Anatomic Considerations Glenohumeral Joint Instability: An Athlete s Perspective Michael D. Loeb, MD Texas Orthopedics, Sports Medicine, and Rehabilitation Associates Austin, Texas Static Stabilizers Osseous
SHOULDER PAIN LESSONS FROM THE SPORTS FIELD MOVEMENT RESTRICTIONS. Steve McCaig
 SHOULDER PAIN LESSONS FROM THE SPORTS FIELD MOVEMENT RESTRICTIONS 1 Steve McCaig Senior Physiotherapist England Development Programme, ECB, Loughborough, United Kingdom Throwing High forces upper limb
SHOULDER PAIN LESSONS FROM THE SPORTS FIELD MOVEMENT RESTRICTIONS 1 Steve McCaig Senior Physiotherapist England Development Programme, ECB, Loughborough, United Kingdom Throwing High forces upper limb
Physical Examination of the Shoulder
 General setup Patient will be examined in both the seated and supine position so exam table needed 360 degree access to patient Expose neck and both shoulders (for comparison); female in gown or sports
General setup Patient will be examined in both the seated and supine position so exam table needed 360 degree access to patient Expose neck and both shoulders (for comparison); female in gown or sports
Shoulder Impingement Rehabilitation Recommendations
 Shoulder Impingement Rehabilitation Recommendations The following protocol can be utilized for conservative care of shoulder impingement as well as post- operative subacromial decompression (SAD) surgery.
Shoulder Impingement Rehabilitation Recommendations The following protocol can be utilized for conservative care of shoulder impingement as well as post- operative subacromial decompression (SAD) surgery.
SLAP LESION REPAIR PROTOCOL Dr. Steven Flores
 SLAP LESION REPAIR PROTOCOL Dr. Steven Flores This rehabilitation protocol has been developed for the patient following a SLAP (Superior Labrum Anterior Posterior) repair. It is extremely important to
SLAP LESION REPAIR PROTOCOL Dr. Steven Flores This rehabilitation protocol has been developed for the patient following a SLAP (Superior Labrum Anterior Posterior) repair. It is extremely important to
Throwing Athlete Rehabilitation. Brett Schulz LAT/CMSS Sport and Spine Physical Therapy
 Throwing Athlete Rehabilitation Brett Schulz LAT/CMSS Sport and Spine Physical Therapy Disclosure No conflicts to disclose Throwing Athlete Dilemma The shoulder must have enough range of motion to allow
Throwing Athlete Rehabilitation Brett Schulz LAT/CMSS Sport and Spine Physical Therapy Disclosure No conflicts to disclose Throwing Athlete Dilemma The shoulder must have enough range of motion to allow
Arthroscopic Bankart Repair Rehabilitation Protocol Dr. Mark Adickes
 Arthroscopic Bankart Repair Rehabilitation Protocol Dr. Mark Adickes Introduction: This rehabilitation protocol has been developed for the patient following an arthroscopic Bankart (anteroinferior labral
Arthroscopic Bankart Repair Rehabilitation Protocol Dr. Mark Adickes Introduction: This rehabilitation protocol has been developed for the patient following an arthroscopic Bankart (anteroinferior labral
Anatomy GH Joint. Glenohumeral Instability. Components of Stability. Components of Stability 7/7/2017. AllinaHealthSystem
 Glenohumeral Instability Dr. John Steubs Allina Sports Medicine Conference July 7, 2017 Anatomy GH Joint Teardrop or oval shape Inherently unstable Golf ball and tee analogy Stabilizers Static Dynamic
Glenohumeral Instability Dr. John Steubs Allina Sports Medicine Conference July 7, 2017 Anatomy GH Joint Teardrop or oval shape Inherently unstable Golf ball and tee analogy Stabilizers Static Dynamic
R. Frank Henn III, MD. Associate Professor Chief of Sports Medicine Residency Program Director
 R. Frank Henn III, MD Associate Professor Chief of Sports Medicine Residency Program Director Disclosures No financial relationships to disclose 1. Labral anatomy 2. Adaptations of the throwing shoulder
R. Frank Henn III, MD Associate Professor Chief of Sports Medicine Residency Program Director Disclosures No financial relationships to disclose 1. Labral anatomy 2. Adaptations of the throwing shoulder
IMPINGEMENT-TESTSTESTS
 «thinking about.» DIFFERENTIAL DIAGNOSIS: Looking for the causes of Which special tests do you use in your shoulder examination? Ann Cools, PT, PhD Ghent University - Belgium Dept of Rehabilitation Sciences
«thinking about.» DIFFERENTIAL DIAGNOSIS: Looking for the causes of Which special tests do you use in your shoulder examination? Ann Cools, PT, PhD Ghent University - Belgium Dept of Rehabilitation Sciences
11/6/2013. Keely Behning, PT, SCS, ATC MNPTA Fall Conference November 16, 2013
 Keely Behning, PT, SCS, ATC MNPTA Fall Conference November 16, 2013 Upon completion of this course, attendees should be able to: Understand pertinent anatomy and biomechanics as they relate to specific
Keely Behning, PT, SCS, ATC MNPTA Fall Conference November 16, 2013 Upon completion of this course, attendees should be able to: Understand pertinent anatomy and biomechanics as they relate to specific
Review shoulder anatomy Review the physical exam of the shoulder Discuss some common causes of acute shoulder pain Discuss some common causes of
 Review shoulder anatomy Review the physical exam of the shoulder Discuss some common causes of acute shoulder pain Discuss some common causes of chronic shoulder pain Review with some case questions Bones:
Review shoulder anatomy Review the physical exam of the shoulder Discuss some common causes of acute shoulder pain Discuss some common causes of chronic shoulder pain Review with some case questions Bones:
Biceps Tenodesis Protocol
 Biceps Tenodesis Protocol A biceps tenodesis procedure involves cutting of the long head of the biceps just prior to its insertion on the superior labrum and then anchoring the tendon along its anatomical
Biceps Tenodesis Protocol A biceps tenodesis procedure involves cutting of the long head of the biceps just prior to its insertion on the superior labrum and then anchoring the tendon along its anatomical
The ball-and-socket articulation at the glenohumeral joint is between the convex
 SLAP Lesion Repair Emily Cotey, Emily Hurysz, and Patrick Schroeder Abstract SLAP lesion, which stands for Superior Labrum Anterior and Posterior, is a detachment tear of the superior labrum that originates
SLAP Lesion Repair Emily Cotey, Emily Hurysz, and Patrick Schroeder Abstract SLAP lesion, which stands for Superior Labrum Anterior and Posterior, is a detachment tear of the superior labrum that originates
SLAP Lesions in High Demand Performers Randy Schwartxberg, MD
 SLAP Lesions in High Demand Performers Randy Schwartxberg, MD How does this impact Cirque? Our challenge Return to prior form Training sessions 10 shows per week Cirque Medical Set-up Team Physician Orthopaedic
SLAP Lesions in High Demand Performers Randy Schwartxberg, MD How does this impact Cirque? Our challenge Return to prior form Training sessions 10 shows per week Cirque Medical Set-up Team Physician Orthopaedic
Superior Labrum Repair Protocol - SLAP
 Superior Labrum Repair Protocol - SLAP Stage I (0-4 weeks): Key Goals: Protect the newly repaired shoulder. Allow for decreased inflammation and healing. Maintain elbow, wrist and hand function. Maintain
Superior Labrum Repair Protocol - SLAP Stage I (0-4 weeks): Key Goals: Protect the newly repaired shoulder. Allow for decreased inflammation and healing. Maintain elbow, wrist and hand function. Maintain
Rehabilitation Guidelines for Open Latarjet Anterior Shoulder Stabilization
 UW HEALTH SPORTS REHABILITATION Rehabilitation Guidelines for Open Latarjet Anterior Shoulder Stabilization The anatomic configuration of the shoulder joint (glenohumeral joint) is often compared to a
UW HEALTH SPORTS REHABILITATION Rehabilitation Guidelines for Open Latarjet Anterior Shoulder Stabilization The anatomic configuration of the shoulder joint (glenohumeral joint) is often compared to a
ANTERIOR SHOULDER STABILIZATION CLINICAL PRACTICE GUIDELINE
 ANTERIOR SHOULDER STABILIZATION CLINICAL PRACTICE GUIDELINE Background Ohio State s Anterior Shoulder Stabilization Rehabilitation Guideline is to be utilized following open or arthroscopic anterior shoulder
ANTERIOR SHOULDER STABILIZATION CLINICAL PRACTICE GUIDELINE Background Ohio State s Anterior Shoulder Stabilization Rehabilitation Guideline is to be utilized following open or arthroscopic anterior shoulder
REHABILITATION GUIDELINES FOR ANTERIOR SHOULDER RECONSTRUCTION WITH BANKART REPAIR
 REHABILITATION GUIDELINES FOR ANTERIOR SHOULDER RECONSTRUCTION WITH BANKART REPAIR The rehabilitation guidelines are presented in a criterion based progression. General time frames are given for reference
REHABILITATION GUIDELINES FOR ANTERIOR SHOULDER RECONSTRUCTION WITH BANKART REPAIR The rehabilitation guidelines are presented in a criterion based progression. General time frames are given for reference
Labral Tears. Fig 1: Intact labrum and biceps tendon
 Labral Tears What is it? The shoulder joint is a ball and socket joint, with the humeral head (upper arm bone) as the ball and the glenoid as the socket. The glenoid (socket) is a shallow bone that is
Labral Tears What is it? The shoulder joint is a ball and socket joint, with the humeral head (upper arm bone) as the ball and the glenoid as the socket. The glenoid (socket) is a shallow bone that is
Rehabilitation Guidelines for Arthroscopic Capsular Shift
 UW HEALTH SPORTS REHABILITATION Rehabilitation Guidelines for Arthroscopic Capsular Shift The anatomic configuration of the shoulder joint (glenohumeral joint) is often compared to a golf ball on a tee.
UW HEALTH SPORTS REHABILITATION Rehabilitation Guidelines for Arthroscopic Capsular Shift The anatomic configuration of the shoulder joint (glenohumeral joint) is often compared to a golf ball on a tee.
4/12/2016. Goals. Anatomy. Basic Anatomy. Biomechanics. Function. Traumatic Rupture of Proximal Biceps: In-season Rehabilitation and Management
 Goals Traumatic Rupture of Proximal Biceps: In-season Rehabilitation and Management Thomas F. LaPorta, MD To understand the anatomy of the biceps at the shoulder To present the mechanism, signs and symptoms,
Goals Traumatic Rupture of Proximal Biceps: In-season Rehabilitation and Management Thomas F. LaPorta, MD To understand the anatomy of the biceps at the shoulder To present the mechanism, signs and symptoms,
Arthroscopic SLAP Lesion Repair Rehabilitation Guideline
 Arthroscopic SLAP Lesion Repair Rehabilitation Guideline This rehabilitation program is designed to return the individual to their activities as quickly and safely as possible. It is designed for rehabilitation
Arthroscopic SLAP Lesion Repair Rehabilitation Guideline This rehabilitation program is designed to return the individual to their activities as quickly and safely as possible. It is designed for rehabilitation
Shoulder and Elbow ORTHOPAEDIC SYPMPOSIUM APRIL 8, 2017 DANIEL DOTY MD
 Shoulder and Elbow ORTHOPAEDIC SYPMPOSIUM APRIL 8, 2017 DANIEL DOTY MD Shoulder Articulations Glenohumeral Joint 2/3 total arc of motion Shallow Ball and Socket Joint Allows for excellent ROM Requires
Shoulder and Elbow ORTHOPAEDIC SYPMPOSIUM APRIL 8, 2017 DANIEL DOTY MD Shoulder Articulations Glenohumeral Joint 2/3 total arc of motion Shallow Ball and Socket Joint Allows for excellent ROM Requires
Returning the Shoulder Back to Optimal Function. Scapula. Clavicle. Humerus. Bones of the Shoulder (Osteology) Joints of the Shoulder (Arthrology)
 Joints of the Shoulder (Arthrology)") Returning the Shoulder Back to Optimal Function Sternum Clavicle Ribs Scapula Humerus Bones of the Shoulder (Osteology) By Rick Kaselj Clavicle Scapula Medial Left Anterior Clavicle Inferior View 20 degree
Returning the Shoulder Back to Optimal Function Sternum Clavicle Ribs Scapula Humerus Bones of the Shoulder (Osteology) By Rick Kaselj Clavicle Scapula Medial Left Anterior Clavicle Inferior View 20 degree
REHABILITATION GUIDELINES FOR ARTHROSCOPIC CAPSULAR SHIFT
 REHABILITATION GUIDELINES FOR ARTHROSCOPIC CAPSULAR SHIFT The rehabilitation guidelines are presented in a criterion based progression. General time frames are given for reference to the average, but individual
REHABILITATION GUIDELINES FOR ARTHROSCOPIC CAPSULAR SHIFT The rehabilitation guidelines are presented in a criterion based progression. General time frames are given for reference to the average, but individual
ORTHOPEDIC AND SPORTS MEDICINE CENTER
 ORTHOPEDIC AND SPORTS MEDICINE CENTER SPORTS MEDICINE DIVISION COMBINED REHAB PROTOCOLS AAMC ORTHOPEDIC AND SPORTS MEDICINE SPECIALISTS Office: (410) 268-8862 Fax: (410) 268-0380 Rotator Cuff Repair Rehab
ORTHOPEDIC AND SPORTS MEDICINE CENTER SPORTS MEDICINE DIVISION COMBINED REHAB PROTOCOLS AAMC ORTHOPEDIC AND SPORTS MEDICINE SPECIALISTS Office: (410) 268-8862 Fax: (410) 268-0380 Rotator Cuff Repair Rehab
SUPERIOR LABRAL REPAIRS
 LOURDES MEDICAL ASSOCIATES Sean Mc Millan, DO Director of Orthopaedic Sports Medicine & Arthroscopy 2103 Burlington-Mount Holly Rd Burlington, NJ 08016 (609) 747-9200 (office) (609) 747-1408 (fax) http://orthodoc.aaos.org/drmcmillan
LOURDES MEDICAL ASSOCIATES Sean Mc Millan, DO Director of Orthopaedic Sports Medicine & Arthroscopy 2103 Burlington-Mount Holly Rd Burlington, NJ 08016 (609) 747-9200 (office) (609) 747-1408 (fax) http://orthodoc.aaos.org/drmcmillan
The Management of Shoulder Instability. By Debbie Prince Clinical Shoulder Specialist
 The Management of Shoulder Instability By Debbie Prince Clinical Shoulder Specialist Shoulder Dislocation The most common joint dislocation Traumatic Instability, highest incidence in males aged 21 to
The Management of Shoulder Instability By Debbie Prince Clinical Shoulder Specialist Shoulder Dislocation The most common joint dislocation Traumatic Instability, highest incidence in males aged 21 to
Diagnosis: ( LEFT / RIGHT ) Shoulder Instability / SLAP Tear
 Shoulder Instability / SLAP Tear") UCLA OUTPATIENT REHABILITATION SERVICES! SANTA MONICA! WESTWOOD 1000 Veteran Ave., A level Phone: (310) 794-1323 Fax: (310) 794-1457 1260 15 th St, Ste. 900 Phone: (310) 319-4646 Fax: (310) 319-2269 FOR
UCLA OUTPATIENT REHABILITATION SERVICES! SANTA MONICA! WESTWOOD 1000 Veteran Ave., A level Phone: (310) 794-1323 Fax: (310) 794-1457 1260 15 th St, Ste. 900 Phone: (310) 319-4646 Fax: (310) 319-2269 FOR
Recurrent Shoulder Dislocation.
 Recurrent Shoulder Dislocation www.fisiokinesiterapia.biz Anatomy of the Shoulder Shoulder Dislocations Case Study Rehabilitation Pick List Anatomy of the Shoulder Articulations Sternoclavicular Acromioclavicular
Recurrent Shoulder Dislocation www.fisiokinesiterapia.biz Anatomy of the Shoulder Shoulder Dislocations Case Study Rehabilitation Pick List Anatomy of the Shoulder Articulations Sternoclavicular Acromioclavicular
Shoulder: Clinical Anatomy, Kinematics & Biomechanics
 Shoulder: Clinical Anatomy, Kinematics & Biomechanics Dr. Alex K C Poon Department of Orthopaedics & Traumatology Pamela Youde Nethersole Eastern Hospital Clinical Anatomy the application of anatomy to
Shoulder: Clinical Anatomy, Kinematics & Biomechanics Dr. Alex K C Poon Department of Orthopaedics & Traumatology Pamela Youde Nethersole Eastern Hospital Clinical Anatomy the application of anatomy to
Latarjet Repair Rehabilitation Protocol
 General Notes: As tolerated should be understood to include with safety for the reconstruction/repair; a sudden increase in pain, swelling, or other undesirable factors are indicators that you are doing
General Notes: As tolerated should be understood to include with safety for the reconstruction/repair; a sudden increase in pain, swelling, or other undesirable factors are indicators that you are doing
ER + IR = Total Motion
 Treating the Thrower s Shoulder Michael M. Reinold, PT, DPT, ATC, CSCS Introduction Common site of injury» Repetitive forces / stresses Tremendous joint forces» Anterior shear forces 1-1.5 1.5 X BW» Distraction
Treating the Thrower s Shoulder Michael M. Reinold, PT, DPT, ATC, CSCS Introduction Common site of injury» Repetitive forces / stresses Tremendous joint forces» Anterior shear forces 1-1.5 1.5 X BW» Distraction
Arthroscopic Anterior Stabilization Rehab
 Arthroscopic Anterior Stabilization Rehab Phase I (0-3weeks) Sling immobilization-md directed Codmans/Pendulum exercises Wrist/Elbow ROM Gripping exercises FF-AAROM (supine)-limit to 90 o ER to 0 o Sub
Arthroscopic Anterior Stabilization Rehab Phase I (0-3weeks) Sling immobilization-md directed Codmans/Pendulum exercises Wrist/Elbow ROM Gripping exercises FF-AAROM (supine)-limit to 90 o ER to 0 o Sub
Shoulder Joint Examination. Shoulder Joint Examination. Inspection. Inspection Palpation Movement. Look Feel Move
 Shoulder Joint Examination History Cuff Examination Instability Examination AC Joint Examination Biceps Tendon Examination Superior Labrum Examination Shoulder Joint Examination Inspection Palpation Movement
Shoulder Joint Examination History Cuff Examination Instability Examination AC Joint Examination Biceps Tendon Examination Superior Labrum Examination Shoulder Joint Examination Inspection Palpation Movement
Rehabilitation after Arthroscopic Posterior Bankart Repair
 Rehabilitation after Arthroscopic Posterior Bankart Repair Phase 1: 0 to 2 weeks after surgery POSTOPERATIVE INSTRUCTIONS You will wake up in the operating room. A sling and an ice pack will be in place.
Rehabilitation after Arthroscopic Posterior Bankart Repair Phase 1: 0 to 2 weeks after surgery POSTOPERATIVE INSTRUCTIONS You will wake up in the operating room. A sling and an ice pack will be in place.
ROTATOR CUFF REPAIR REHAB PROTOCOL
 Jayesh K. Patel, M.D. Trinity Clinic Orthopaedic and Sports Medicine 1327 Troup Hwy Tyler, TX 75701 (903) 510-8840 ROTATOR CUFF REPAIR REHAB PROTOCOL This rehabilitation protocol has been developed for
Jayesh K. Patel, M.D. Trinity Clinic Orthopaedic and Sports Medicine 1327 Troup Hwy Tyler, TX 75701 (903) 510-8840 ROTATOR CUFF REPAIR REHAB PROTOCOL This rehabilitation protocol has been developed for
BANKART REPAIR PROTOCOL
 BANKART REPAIR PROTOCOL Clarkstown Division This rehabilitation protocol has been developed for the patient following Bankart surgical procedure for anterior shoulder instability. The protocol is divided
BANKART REPAIR PROTOCOL Clarkstown Division This rehabilitation protocol has been developed for the patient following Bankart surgical procedure for anterior shoulder instability. The protocol is divided
Evidence- Based Examination of the Shoulder Presented by Eric Hegedus, PT, DPT, MHSC, OCS, CSCS Practice Sessions/Skill Check- offs
 Evidence- Based Examination of the Shoulder Practice Session & Skills Check- offs Evidence- Based Examination of the Shoulder Presented by Eric Hegedus, PT, DPT, MHSC, OCS, CSCS Practice Sessions/Skill
Evidence- Based Examination of the Shoulder Practice Session & Skills Check- offs Evidence- Based Examination of the Shoulder Presented by Eric Hegedus, PT, DPT, MHSC, OCS, CSCS Practice Sessions/Skill
Lab Workbook. ANATOMY Manual Muscle Testing Lower Trapezius Patient: prone
 ANATOMY Manual Muscle Testing Lower Trapezius Patient: prone Lab Workbook Fixation: place on hand below the scapula on the opposite side Test: adduction and depression of the scapula with lateral rotation
ANATOMY Manual Muscle Testing Lower Trapezius Patient: prone Lab Workbook Fixation: place on hand below the scapula on the opposite side Test: adduction and depression of the scapula with lateral rotation
Biceps Tenotomy Protocol
 Biceps Tenotomy Protocol A biceps tenotomy procedure involves cutting of the long head of the biceps just prior to its insertion on the superior labrum. A biceps tenotomy is typically done when there is
Biceps Tenotomy Protocol A biceps tenotomy procedure involves cutting of the long head of the biceps just prior to its insertion on the superior labrum. A biceps tenotomy is typically done when there is
EBP - An Examination of Special Tests for the Shoulder- Module 8 Exam
 We recommend that you download and print this exam to use as a worksheet. As you study the course material, add your answers to the worksheet. After studying, you will submit the answers. After you submit
We recommend that you download and print this exam to use as a worksheet. As you study the course material, add your answers to the worksheet. After studying, you will submit the answers. After you submit
Anterior Stabilization of the Shoulder: Distal Tibial Allograft
 Anterior Stabilization of the Shoulder: Distal Tibial Allograft Name: Diagnosis: Date: Date of Surgery: Phase I Immediate Post Surgical Phase (approximately Weeks 1-3) Minimize shoulder pain and inflammatory
Anterior Stabilization of the Shoulder: Distal Tibial Allograft Name: Diagnosis: Date: Date of Surgery: Phase I Immediate Post Surgical Phase (approximately Weeks 1-3) Minimize shoulder pain and inflammatory
Rehabilitation Protocol: Massive Rotator Cuff Tear Repair
 Rehabilitation Protocol: Massive Rotator Cuff Tear Repair Department of Orthopaedic Surgery Lahey Hospital & Medical Center, Burlington 781-744-8650 Lahey Outpatient Center, Lexington 781-372-7020 Lahey
Rehabilitation Protocol: Massive Rotator Cuff Tear Repair Department of Orthopaedic Surgery Lahey Hospital & Medical Center, Burlington 781-744-8650 Lahey Outpatient Center, Lexington 781-372-7020 Lahey
Arthroscopic SLAP Repair Protocol
 SPORTS & ORTHOPAEDIC SPECIALISTS Arthroscopic SLAP Repair Protocol 6-8 visits over 12 weeks Emphasis is on AAROM and a high repetition, low weight free weight program Address posterior capsular tightness
SPORTS & ORTHOPAEDIC SPECIALISTS Arthroscopic SLAP Repair Protocol 6-8 visits over 12 weeks Emphasis is on AAROM and a high repetition, low weight free weight program Address posterior capsular tightness
Shoulder Instability and Tendon Injuries
 Shoulder Instability and Tendon Injuries Shoulder Update Spire Hospital Leeds November 2017 Simon Boyle Consultant Shoulder and Elbow Surgeon Simon Boyle York and Leeds Nuffield Trained in Yorkshire, Annecy,
Shoulder Instability and Tendon Injuries Shoulder Update Spire Hospital Leeds November 2017 Simon Boyle Consultant Shoulder and Elbow Surgeon Simon Boyle York and Leeds Nuffield Trained in Yorkshire, Annecy,
Arthroscopic Labrum Repair of the Shoulder (SLAP)
") Anatomy Arthroscopic Labrum Repair of the Shoulder (SLAP) The shoulder joint involves three bones: the scapula (shoulder blade), the clavicle (collarbone) and the humerus (upper arm bone). The humeral
Anatomy Arthroscopic Labrum Repair of the Shoulder (SLAP) The shoulder joint involves three bones: the scapula (shoulder blade), the clavicle (collarbone) and the humerus (upper arm bone). The humeral
Shoulder Arthroscopy with Posterior Labral Repair Rehabilitation Protocol
 General Notes: As tolerated should be understood to include with safety for the surgical procedure; a sudden increase in pain, swelling, or other undesirable factors are indicators that you are doing too
General Notes: As tolerated should be understood to include with safety for the surgical procedure; a sudden increase in pain, swelling, or other undesirable factors are indicators that you are doing too
Management of Anterior Shoulder Instability
 Management of Anterior Shoulder Instability Angelo J. Colosimo, MD Head Orthopaedic Surgeon University of Cincinnati Athletics Director of Sports Medicine University of Cincinnati Medical Center Associate
Management of Anterior Shoulder Instability Angelo J. Colosimo, MD Head Orthopaedic Surgeon University of Cincinnati Athletics Director of Sports Medicine University of Cincinnati Medical Center Associate
Biceps Tenodesis Protocol
 Robert K. Fullick, MD 6400 Fannin Street, Suite 1700 Houston, Texas 77030 Ph.: 713-486-7543 / Fx.: 713-486-5549 Biceps Tenodesis Protocol The intent of this protocol is to provide the clinician with a
Robert K. Fullick, MD 6400 Fannin Street, Suite 1700 Houston, Texas 77030 Ph.: 713-486-7543 / Fx.: 713-486-5549 Biceps Tenodesis Protocol The intent of this protocol is to provide the clinician with a
Bankart/ Anterior Capsulorrhaphy Repair Protocol
 SPORTS & ORTHOPAEDIC SPECIALISTS Bankart/ Anterior Capsulorrhaphy Repair Protocol 6-8 visits over 12 weeks Emphasis is on AAROM and a high repetition, low weight free weight program Address posterior capsular
SPORTS & ORTHOPAEDIC SPECIALISTS Bankart/ Anterior Capsulorrhaphy Repair Protocol 6-8 visits over 12 weeks Emphasis is on AAROM and a high repetition, low weight free weight program Address posterior capsular
PHASE I (Begin PT 3-5 days post-op) DOS:
 DOS:") REHABILITATION GUIDELINES FOR POSTERIOR SHOULDER RECONSTRUCTION +/- LABRAL REPAIRS The rehabilitation guidelines are presented in a criterion based progression. General time frames are given for reference
REHABILITATION GUIDELINES FOR POSTERIOR SHOULDER RECONSTRUCTION +/- LABRAL REPAIRS The rehabilitation guidelines are presented in a criterion based progression. General time frames are given for reference
Superior Labral Pathology in Throwers
 Superior Labral Pathology in Throwers Disclosures Available via AAOS website None relevant to this presentation L. Pearce McCarty, III M.D. Team Physician, Minnesota Twins Chairman, Orthopedic Surgery,
Superior Labral Pathology in Throwers Disclosures Available via AAOS website None relevant to this presentation L. Pearce McCarty, III M.D. Team Physician, Minnesota Twins Chairman, Orthopedic Surgery,
SMALL-MEDIUM ROTATOR CUFF REPAIR GUIDELINE
 SMALL-MEDIUM ROTATOR CUFF REPAIR GUIDELINE The rotator cuff is responsible for stabilization and active movement of the glenohumeral joint. An acute or overuse injury may cause the rotator cuff to be injured
SMALL-MEDIUM ROTATOR CUFF REPAIR GUIDELINE The rotator cuff is responsible for stabilization and active movement of the glenohumeral joint. An acute or overuse injury may cause the rotator cuff to be injured
Throwing Injuries and Prevention: The Physical Therapy Perspective
 Throwing Injuries and Prevention: The Physical Therapy Perspective Andrew M Jordan, PT, DPT, OCS Staff Physical Therapist, Cayuga Medical Center Physical Therapy and Sports Medicine ajordan@cayugamed.org
Throwing Injuries and Prevention: The Physical Therapy Perspective Andrew M Jordan, PT, DPT, OCS Staff Physical Therapist, Cayuga Medical Center Physical Therapy and Sports Medicine ajordan@cayugamed.org
Biceps Tenotomy Protocol
 Department of Rehabilitation Services Physical Therapy The intent of this protocol is to provide the clinician with a guideline of the postoperative rehabilitation course of a patient that has undergone
Department of Rehabilitation Services Physical Therapy The intent of this protocol is to provide the clinician with a guideline of the postoperative rehabilitation course of a patient that has undergone
Mark Adickes, M.D. Orthopedics and Sports Medicine 7200 Cambridge St. #10A Houston, Texas Phone: Fax:
 Mark Adickes, M.D. Orthopedics and Sports Medicine 7200 Cambridge St. #10A Houston, Texas 77030 Phone: 713-986-6016 Fax: 713-986-5411 Pectoralis Major Tendon Repair The pectoralis major is a thick, fan-shaped
Mark Adickes, M.D. Orthopedics and Sports Medicine 7200 Cambridge St. #10A Houston, Texas 77030 Phone: 713-986-6016 Fax: 713-986-5411 Pectoralis Major Tendon Repair The pectoralis major is a thick, fan-shaped
The Shoulder. Anatomy and Injuries PSK 4U Unit 3, Day 4
 The Shoulder Anatomy and Injuries PSK 4U Unit 3, Day 4 Shoulder Girdle Shoulder Complex is the most mobile joint in the body. Scapula Clavicle Sternum Humerus Rib cage/thorax Shoulder Girdle It also includes
The Shoulder Anatomy and Injuries PSK 4U Unit 3, Day 4 Shoulder Girdle Shoulder Complex is the most mobile joint in the body. Scapula Clavicle Sternum Humerus Rib cage/thorax Shoulder Girdle It also includes
Rehabilitation for MDI in the Female Athlete. John Dale PT, DPT, SCS, ATC, CSCS Andrew Naylor PT, DPT, SCS
 Rehabilitation for MDI in the Female Athlete John Dale PT, DPT, SCS, ATC, CSCS Andrew Naylor PT, DPT, SCS Disclosure No relevant financial relationship exists Session Learning Objectives Discuss etiology
Rehabilitation for MDI in the Female Athlete John Dale PT, DPT, SCS, ATC, CSCS Andrew Naylor PT, DPT, SCS Disclosure No relevant financial relationship exists Session Learning Objectives Discuss etiology
PROM is not stretching!
 Dx: o Right o Left Shoulder Replacement/Hemiarthroplasty Rehab Date of Surgery: Patient Name: PT/OT: Please evaluate and treat. Follow attached protocol. 2-3 x per week x 6 weeks. Signature/Date: The intent
Dx: o Right o Left Shoulder Replacement/Hemiarthroplasty Rehab Date of Surgery: Patient Name: PT/OT: Please evaluate and treat. Follow attached protocol. 2-3 x per week x 6 weeks. Signature/Date: The intent
SHOULDER PAIN. A Real Pain in the Neck. Michael Wolk, MD Northeastern Rehabilitation Associates October 31, 2017
 SHOULDER PAIN A Real Pain in the Neck Michael Wolk, MD Northeastern Rehabilitation Associates October 31, 2017 THE SHOULDER JOINT (S) 1. glenohumeral 2. suprahumeral 3. acromioclavicular 4. scapulocostal
SHOULDER PAIN A Real Pain in the Neck Michael Wolk, MD Northeastern Rehabilitation Associates October 31, 2017 THE SHOULDER JOINT (S) 1. glenohumeral 2. suprahumeral 3. acromioclavicular 4. scapulocostal
Reverse Bankart/Posterior Capsulorrhaphy Repair Protocol
 + SPORTS & ORTHOPAEDIC SPECIALISTS 8100 W. 78 th Street Edina, MN 55439 952-946-9777 www.womensorthocenter.com Reverse Bankart/Posterior Capsulorrhaphy Repair Protocol 6-10 visits over 16 weeks Emphasis
+ SPORTS & ORTHOPAEDIC SPECIALISTS 8100 W. 78 th Street Edina, MN 55439 952-946-9777 www.womensorthocenter.com Reverse Bankart/Posterior Capsulorrhaphy Repair Protocol 6-10 visits over 16 weeks Emphasis
Conservative Massive Rotator Cuff Tear Protocol
 SPORTS & ORTHOPAEDIC SPECIALISTS Conservative Massive Rotator Cuff Tear Protocol 3-4 visits over 4-6 weeks Emphasis is on AAROM and a high repetition, low weight free weight program Emphasize improved
SPORTS & ORTHOPAEDIC SPECIALISTS Conservative Massive Rotator Cuff Tear Protocol 3-4 visits over 4-6 weeks Emphasis is on AAROM and a high repetition, low weight free weight program Emphasize improved
THERMAL - ASSISTED CAPSULORRAPHY With or without SLAP Repair
 THERMAL - ASSISTED CAPSULORRAPHY With or without SLAP Repair **It is important for the clinician to determine the capsular response to the heat probe. Patients that have excessive ROM early in the rehab
THERMAL - ASSISTED CAPSULORRAPHY With or without SLAP Repair **It is important for the clinician to determine the capsular response to the heat probe. Patients that have excessive ROM early in the rehab
Supplemental Video Available at
 Current Concepts in the Recognition and Treatment of Superior Labral (SLAP) Lesions Kevin E. Wilk, DPT 1 Michael M. Reinold, DPT, ATC, CSCS 2 Jeffrey R. Dugas, MD 3 Christopher A. Arrigo, PT, MS 4 Michael
Current Concepts in the Recognition and Treatment of Superior Labral (SLAP) Lesions Kevin E. Wilk, DPT 1 Michael M. Reinold, DPT, ATC, CSCS 2 Jeffrey R. Dugas, MD 3 Christopher A. Arrigo, PT, MS 4 Michael
Rotator Cuff Repair Protocol for tear involving Subscapularis Tendon with or without Pectoralis Major Tendon Transfer
 Rotator Cuff Repair Protocol for tear involving Subscapularis Tendon with or without Pectoralis Major Tendon Transfer D. WATTS, MD Precautions: BASIS Tendon healing back to bone is a slow process that
Rotator Cuff Repair Protocol for tear involving Subscapularis Tendon with or without Pectoralis Major Tendon Transfer D. WATTS, MD Precautions: BASIS Tendon healing back to bone is a slow process that
REMINDER. an exercise program. Senior Fitness Obtain medical clearance and physician s release prior to beginning
 Functional Forever: Exercise for Independent Living REMINDER Obtain medical clearance and physician s release prior to beginning an exercise program for clients with medical or orthopedic concerns. What
Functional Forever: Exercise for Independent Living REMINDER Obtain medical clearance and physician s release prior to beginning an exercise program for clients with medical or orthopedic concerns. What
Anterior Stabilization of the Shoulder: Latarjet Protocol
 Robert K. Fullick, MD 6400 Fannin Street, Suite 1700 Houston, Texas 77030 Ph.: 713-486-7543 / Fx.: 713-486-5549 Anterior Stabilization of the Shoulder: Latarjet Protocol The intent of this protocol is
Robert K. Fullick, MD 6400 Fannin Street, Suite 1700 Houston, Texas 77030 Ph.: 713-486-7543 / Fx.: 713-486-5549 Anterior Stabilization of the Shoulder: Latarjet Protocol The intent of this protocol is
Bradley C. Carofino, M.D. Shoulder Specialist 230 Clearfield Avenue, Suite 124 Virginia Beach, Virginia Phone
 Subpectoral Bicep Tenodesis Protocol (Spreadsheet) Weeks 1-2 Modalities Treatment Restrictions Goals No active elbow flexion (6weeks) Full PROM shoulder and elbow PROM: Shoulder, elbow, forearm No active
Subpectoral Bicep Tenodesis Protocol (Spreadsheet) Weeks 1-2 Modalities Treatment Restrictions Goals No active elbow flexion (6weeks) Full PROM shoulder and elbow PROM: Shoulder, elbow, forearm No active
Theodore B. Shybut, M.D. Orthopedics and Sports Medicine 7200 Cambridge St. #10A Houston, Texas Phone: Fax:
 Theodore B. Shybut, M.D. Orthopedics and Sports Medicine 7200 Cambridge St. #10A Houston, Texas 77030 Phone: 713-986-5590 Fax: 713-986-5521 ROTATOR CUFF REPAIR PROTOCOL This rehabilitation protocol has
Theodore B. Shybut, M.D. Orthopedics and Sports Medicine 7200 Cambridge St. #10A Houston, Texas 77030 Phone: 713-986-5590 Fax: 713-986-5521 ROTATOR CUFF REPAIR PROTOCOL This rehabilitation protocol has
Intern Arthroscopy Course 2015 Shoulder Arthroscopy Cases
 Intern Arthroscopy Course 2015 Shoulder Arthroscopy Cases Mary Lloyd Ireland, M.D. University of Kentucky Dept. of Orthopaedic Surgery & Sports Medicine Lexington, KY Broken screw s/p Bristow procedure
Intern Arthroscopy Course 2015 Shoulder Arthroscopy Cases Mary Lloyd Ireland, M.D. University of Kentucky Dept. of Orthopaedic Surgery & Sports Medicine Lexington, KY Broken screw s/p Bristow procedure
ANATOMY / BIOMECHANICS LONG HEAD OF BICEPS ATTACHES AT THE SUPERIOR GLENOIDAL TUBERCLE WITH THE LABRUM FIBROCARTILAGINOUS TISSUE IF THERE IS A TORN SU
 SLAP LESIONS Management Of Glenoid Labrum Injuries INTRODUCTION First described by Andrews AJSM 85 Throwers 60% Normal Variants Sublabral Foramen Buford Complex Meniscoid Snyder Arth. 1990 termed SLAP
SLAP LESIONS Management Of Glenoid Labrum Injuries INTRODUCTION First described by Andrews AJSM 85 Throwers 60% Normal Variants Sublabral Foramen Buford Complex Meniscoid Snyder Arth. 1990 termed SLAP
Addressing Core and Balance Deficits to Maximize Return to Sport in Overhead Athletes
 Addressing Core and Balance Deficits to Maximize Return to Sport in Overhead Athletes Meg Jacobs P.T. Momentum Physical Therapy and Sports Rehab Hands on care for faster results www.wegetyouhealthy.com
Addressing Core and Balance Deficits to Maximize Return to Sport in Overhead Athletes Meg Jacobs P.T. Momentum Physical Therapy and Sports Rehab Hands on care for faster results www.wegetyouhealthy.com
REHABILITATION GUIDELINES FOR SUBSCAPULARIS (+/- SUBACROMIAL DECOMPRESSION) Dr. Carson
 Dr. Carson") REHABILITATION GUIDELINES FOR SUBSCAPULARIS (+/- SUBACROMIAL DECOMPRESSION) Dr. Carson The rehabilitation guidelines are presented in a criterion based progression. General time frames are given for reference
REHABILITATION GUIDELINES FOR SUBSCAPULARIS (+/- SUBACROMIAL DECOMPRESSION) Dr. Carson The rehabilitation guidelines are presented in a criterion based progression. General time frames are given for reference