R. Frank Henn III, MD. Associate Professor Chief of Sports Medicine Residency Program Director
|
|
|
- Adrian Porter
- 5 years ago
- Views:
Transcription

1 R. Frank Henn III, MD Associate Professor Chief of Sports Medicine Residency Program Director

2 Disclosures No financial relationships to disclose

3 1. Labral anatomy 2. Adaptations of the throwing shoulder 3. GIRD 4. SLAP lesions 5. PASTA lesions 6. Spinoglenoid notch cysts

4 Fibrocartilage tissue along rim of glenoid Deepens socket and stabilizes the humeral head Anatomic variability anterosuperiorly Cooper JBJS 1992 Galinat CORR 1989


5 More complex and variable anatomy meniscoid, edge vs recessed origin Origin of long head of biceps variations Supraglenoid tubercle superior labrum


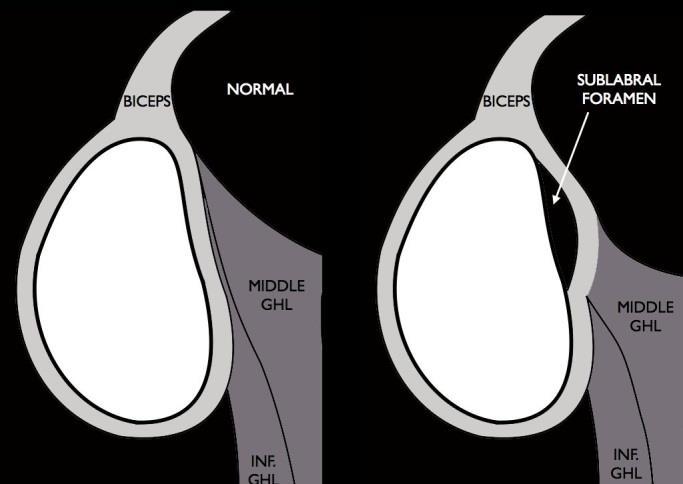
6 Sublabral foramen Bufford Complex NO labrum Cord-liked MGHL


7 Adaptation that predates humans Survival benefit Deadly with minimal risk to the thrower Refined in humans


8 Selection pressure continues Majority of us do not depend on throwing



9 Throwers have distinct demands on the upper extremity Pitchers are the most well studied Principals apply to any throwing Most principals apply to any overhead athlete




10 Linear velocity Running start Rotational Convert torque to linear velocity (Legs/hips/trunk) Height Throw downhill

11 Power/Velocity comes from the kinetic chain Upper extremity musculature least important primarily accuracy and control Disruption to the kinetic chain (e.g. hip injury) can put increased stress on the upper extremity pushing
 Increased abducted")

12 Anatomic adaptations Increased humeral retroversion (~15 deg) Increased abducted external rotation Decreased abducted internal rotation Unchanged total arc of motion

13 Crockett et al. AJSM 2002


 Kids do NOT get SLAP")
14 Shoulder and elbow injuries are associated with high pitch counts, curve balls, and poor mechanics Little League Shoulder Physeal stress fracture (widening) Kids do NOT get SLAP tears Treatment = rest

15 Prevention Limit pitch counts with appropriate rest Age 7-8: 50 pitches per game Age 9-10: 75 pitches per game Age 11-12: 85 pitches per game Age 13-16: 95 pitches per game

16 Mean 10 deg loss of abducted internal rotation for 24 hours after pitching (Reinold AJSM 2010) Probable teres minor tightness from deceleration stress Progress to contracture of posterior inferior capsule
17 GIRD (Glenohumeral internal rotation deficit) > 20 degree difference in abducted internal rotation Loss of over 5 degrees of total arc of motion Increased risk of injury (Wilk AJSM 2011)

18 GIRD accentuates stress on the superior labrum at risk shoulder Altered glenohumeral mechanics Treatment: Capsular stretching

19 Andrews AJSM 1985 Superior labral lesions in throwing athletes Synder Arthroscopy / 700 arthroscopies retrospectively evaluated Injury of the superior labrum begins posteriorly and extends anteriorly, stopping before or at the mid-glenoid notch and including the "anchor" of the biceps tendon to the labrum SLAP Superior Labrum Anterior Posterior

20 Synder Arthroscopy 1990 Type I: Frayed or degenerated labrum Type II: Detachment of superior labrum & biceps from glenoid rim Type III: bucket-handle labral tear with intact biceps anchor Type IV: bucket-handle labral tear that extends into biceps tendon

21 Degenerative Altered glenohumeral mechanics rotator cuff tears, arthritis, throwing Traumatic Compression Fall on outstretched hand Tension Traction on the arm Recurrent anterior dislocations

22 Peel-back of the labrum medially and posteriorly Internal impingement of the greater tuberosity against the posterosuperior glenoid


23 Normal impingement that predisposes to pathology with repetitive insult Articular sided rotator cuff tears Glenoid retroversion may protect Sweitzer et al. Arthroscopy 2012

24 Multiple in-vitro studies demonstrate increased humeral head translations with unstable SLAP tears microinstability Radosky MW AJSM 1994 Panossian VR. JSES 2005 Uggen C Arthrscopy 2009 Chhadia AM. Arthroscopy 2010 Abnormal EMG during tackling Horsley IG. J Orthop Surg Res


25 Variable history Variable history of trauma Throwers: pain with throwing Pain is typically posterior Mechanical symptoms are unusual but suggestive of unstable flap Night pain and resting pain is atypical
26 No examination findings are reliably diagnostic >10 special physical examination tests described O Brien Active Compression Test Best sensitivity (67%) Yergason s Test Best specificity (95%) Hegedus Br J Sports Med 2012

27 Comprehensive shoulder examination Scapular thoracic mechanics SICK scapula Shoulder ptosis, inferior medial border prominence, coracoid pain, dyskinesia Bicipital groove tenderness Rotator cuff strength Spinoglenoid notch cyst infraspinatus weakness Weakness in external rotation with the arm adducted



28 Xays MRI Intra-articular contrast controversial Increased sensitivity, decreased specificity Paralabral cyst is pathognomonic of labral tear ABER: Abduction and External Rotation

29 Non-operative treatment 3 months of directed rehabilitation program Scapular strengthing Capsular stretching Dynamic stabilizations Throwing mechanics intra-articular corticosteroid injection Operative Compressive paralabral cyst, mechanical symptoms
30 Predictors of Failure of Nonoperative Treatment Jang et al. JSES % successful with nonoperative treatment (45 of 63) Multivariable analysis of treatment failure Overhead activity (OR 19.1) History of Trauma (OR 9.8)

31 Determined by stability of the biceps origin If biceps is stable, then debride (types 1 & 3) If biceps unstable, stabilize (types 2 & 4) Poor results with debridement of unstable lesions Good intra and inter-observer reliability of the Synder classification with respect to treatment decisions Gobezie AJSM 2008


32 SLAP repair Prepare glenoid (shaver) Accessory portal Rotator interval Portal of Wilmington Place anchors 1 anchor double loaded 2 anchors single loaded Suture-passer to shuttle sutures Posterior to biceps origin Simple or mattress

33 Biceps Tenodesis/Tenotomy Biceps tendinopathy, poor tissue quality Concomitant Rotator Cuff Repair Caution in throwers (no pitchers) Boileau et al. AJSM 2009 Cohort study SLAP repair: Constant score 83, 2 of 10 returned to sport. Tenodesis: Constant score 89, 14 of 15 returned to sport

34 83% good-to-excellent results 73% return to play Only 63% of overhead athletes returned to previous level of play Postoperative stiffness after SLAP repair is a concern


35 Partial articular supraspinatus tendon avulsion Capsular injury Can occur in isolation or with concomitant SLAP

36 Nonoperative Operative Debridement if <50% of the thickness Repair Take down to full thickness and repair Trans-tendon repair Good long term results (Synder et al. Arthroscopy 2013)


 External")
37 Paralabral cyst from a SLAP tear can compress the suprascapular nerve in the spinoglenoid notch Can denervate the infraspinatus (neurogenic edema) External rotation weakness and pain




38 SLAP Repair with or without decompression Good results with both Kim et al. JSES 2012
I (and/or my co-authors) have something to disclose.
 have something to disclose.") Shoulder Anatomy And Biomechanics Nikhil N Verma, MD Director of Sports Medicine Professor, Department of Orthopedics Rush University Team Physician, Chicago White Sox and Bulls I (and/or my co-authors)
Shoulder Anatomy And Biomechanics Nikhil N Verma, MD Director of Sports Medicine Professor, Department of Orthopedics Rush University Team Physician, Chicago White Sox and Bulls I (and/or my co-authors)
Superior Labral Pathology in Throwers
 Superior Labral Pathology in Throwers Disclosures Available via AAOS website None relevant to this presentation L. Pearce McCarty, III M.D. Team Physician, Minnesota Twins Chairman, Orthopedic Surgery,
Superior Labral Pathology in Throwers Disclosures Available via AAOS website None relevant to this presentation L. Pearce McCarty, III M.D. Team Physician, Minnesota Twins Chairman, Orthopedic Surgery,
Throwing Injuries and Prevention: The Physical Therapy Perspective
 Throwing Injuries and Prevention: The Physical Therapy Perspective Andrew M Jordan, PT, DPT, OCS Staff Physical Therapist, Cayuga Medical Center Physical Therapy and Sports Medicine ajordan@cayugamed.org
Throwing Injuries and Prevention: The Physical Therapy Perspective Andrew M Jordan, PT, DPT, OCS Staff Physical Therapist, Cayuga Medical Center Physical Therapy and Sports Medicine ajordan@cayugamed.org
SLAP Lesions Assessment & Treatment
 SLAP Lesions Assessment & Treatment Kevin E. Wilk,, PT, DPT Glenoid Labral Lesions Introduction Common injury - difficult to diagnose May occur in isolation or in combination SLAP lesions: Snyder: Arthroscopy
SLAP Lesions Assessment & Treatment Kevin E. Wilk,, PT, DPT Glenoid Labral Lesions Introduction Common injury - difficult to diagnose May occur in isolation or in combination SLAP lesions: Snyder: Arthroscopy
ANATOMY / BIOMECHANICS LONG HEAD OF BICEPS ATTACHES AT THE SUPERIOR GLENOIDAL TUBERCLE WITH THE LABRUM FIBROCARTILAGINOUS TISSUE IF THERE IS A TORN SU
 SLAP LESIONS Management Of Glenoid Labrum Injuries INTRODUCTION First described by Andrews AJSM 85 Throwers 60% Normal Variants Sublabral Foramen Buford Complex Meniscoid Snyder Arth. 1990 termed SLAP
SLAP LESIONS Management Of Glenoid Labrum Injuries INTRODUCTION First described by Andrews AJSM 85 Throwers 60% Normal Variants Sublabral Foramen Buford Complex Meniscoid Snyder Arth. 1990 termed SLAP
SLAP Repairs Versus Biceps Tenodesis in Athletes 15 min
 SLAP Repairs Versus Biceps Tenodesis in Athletes 15 min Power Points Not all SLAP tears need surgery Preservation of Native Anatomy GOAL Not all labral repairs are equal Kinetic chain MUST be addressed
SLAP Repairs Versus Biceps Tenodesis in Athletes 15 min Power Points Not all SLAP tears need surgery Preservation of Native Anatomy GOAL Not all labral repairs are equal Kinetic chain MUST be addressed
Sports Medicine: Shoulder Arthrography. Christine B. Chung, M.D. Professor of Radiology Musculoskeletal Division UCSD and VA Healthcare System
 Sports Medicine: Shoulder Arthrography Christine B. Chung, M.D. Professor of Radiology Musculoskeletal Division UCSD and VA Healthcare System Disclosure Off-label use for gadolinium Pediatric Sports Injuries
Sports Medicine: Shoulder Arthrography Christine B. Chung, M.D. Professor of Radiology Musculoskeletal Division UCSD and VA Healthcare System Disclosure Off-label use for gadolinium Pediatric Sports Injuries
MRI of the Shoulder What to look for and how to find it? Dr. Eric Handley Musculoskeletal Radiologist Cherry Creek Imaging
 MRI of the Shoulder What to look for and how to find it? Dr. Eric Handley Musculoskeletal Radiologist Cherry Creek Imaging MRI of the Shoulder Benefits of Ultrasound: * Dynamic * Interactive real time
MRI of the Shoulder What to look for and how to find it? Dr. Eric Handley Musculoskeletal Radiologist Cherry Creek Imaging MRI of the Shoulder Benefits of Ultrasound: * Dynamic * Interactive real time
The ball-and-socket articulation at the glenohumeral joint is between the convex
 SLAP Lesion Repair Emily Cotey, Emily Hurysz, and Patrick Schroeder Abstract SLAP lesion, which stands for Superior Labrum Anterior and Posterior, is a detachment tear of the superior labrum that originates
SLAP Lesion Repair Emily Cotey, Emily Hurysz, and Patrick Schroeder Abstract SLAP lesion, which stands for Superior Labrum Anterior and Posterior, is a detachment tear of the superior labrum that originates
significant increase of glenohumeral translation at middle and lower elevation angles [6].
![significant increase of glenohumeral translation at middle and lower elevation angles [6].](/thumbs/94/120620199.jpg "significant increase of glenohumeral translation at middle and lower elevation angles [6].") significant increase of glenohumeral translation at middle and lower elevation angles [6]. Two types of injury mechanisms have been postulated for superior labral tears. 1. Traction injury : Chronic repetitive
significant increase of glenohumeral translation at middle and lower elevation angles [6]. Two types of injury mechanisms have been postulated for superior labral tears. 1. Traction injury : Chronic repetitive
Type II SLAP lesions are created when the biceps anchor has pulled away from the glenoid attachment.
 Arthroscopic Superior Labral (SLAP) Repair Protocol-Type II, IV, and Complex Tears The intent of this protocol is to provide the clinician with a guideline of the post-operative rehabilitation course of
Arthroscopic Superior Labral (SLAP) Repair Protocol-Type II, IV, and Complex Tears The intent of this protocol is to provide the clinician with a guideline of the post-operative rehabilitation course of
Shoulder Instability. Fig 1: Intact labrum and biceps tendon
 Shoulder Instability What is it? The shoulder joint is a ball and socket joint, with the humeral head (upper arm bone) as the ball and the glenoid as the socket. The glenoid (socket) is a shallow bone
Shoulder Instability What is it? The shoulder joint is a ball and socket joint, with the humeral head (upper arm bone) as the ball and the glenoid as the socket. The glenoid (socket) is a shallow bone
Arthroscopic Labral Repair Protocol-Type II, IV, and Complex Tears:
 Arthroscopic Labral Repair Protocol-Type II, IV, and Complex Tears: The intent of this protocol is to provide the clinician with a guideline of the postoperative rehabilitation course of a patient that
Arthroscopic Labral Repair Protocol-Type II, IV, and Complex Tears: The intent of this protocol is to provide the clinician with a guideline of the postoperative rehabilitation course of a patient that
SHOULDER ANATOMY Karl Wieser, MD Department of Orthopedics, University of Zurich, Balgrist, Switzerland
 20th Course in Shoulder Surgery Balgrist SHOULDER ANATOMY Karl Wieser, MD Department of Orthopedics, University of Zurich, Balgrist, Switzerland www.balgrist.ch ANATOMY OVERVIEW courtesy of Georg Lajtai
20th Course in Shoulder Surgery Balgrist SHOULDER ANATOMY Karl Wieser, MD Department of Orthopedics, University of Zurich, Balgrist, Switzerland www.balgrist.ch ANATOMY OVERVIEW courtesy of Georg Lajtai
Common Shoulder Injuries in the Throwing Athlete: Amateur to Professional
 Common Shoulder Injuries in the Throwing Athlete: Amateur to Professional Steven B. Cohen, MD Associate Professor: Dept Orthopedic Surgery / Rothman Institute Asst Team Physician Philadelphia Phillies
Common Shoulder Injuries in the Throwing Athlete: Amateur to Professional Steven B. Cohen, MD Associate Professor: Dept Orthopedic Surgery / Rothman Institute Asst Team Physician Philadelphia Phillies
SLAP Lesions of the Shoulder
 Arthroscopy: The Journal of Arthroscopic and Related Surgery 6(4):21&279 Published by Raven Press, Ltd. Q 1990 Arthroscopy Association of North America SLAP Lesions of the Shoulder Stephen J. Snyder, M.D.,
Arthroscopy: The Journal of Arthroscopic and Related Surgery 6(4):21&279 Published by Raven Press, Ltd. Q 1990 Arthroscopy Association of North America SLAP Lesions of the Shoulder Stephen J. Snyder, M.D.,
Disclosure 11/14/2016. Partial Thickness Rotator Cuff Tears in the Throwing Athlete. Partial Thickness Rotator Cuff Tears. Neal S. ElAttrache, M.D.
 Partial Thickness Rotator Cuff Tears in the Throwing Athlete Neal S. ElAttrache, M.D. Disclosure I, Neal ElAttrache, or a family member(s), have relevant financial relationships to be discussed, directly
Partial Thickness Rotator Cuff Tears in the Throwing Athlete Neal S. ElAttrache, M.D. Disclosure I, Neal ElAttrache, or a family member(s), have relevant financial relationships to be discussed, directly
Labral Tears. Fig 1: Intact labrum and biceps tendon
 Labral Tears What is it? The shoulder joint is a ball and socket joint, with the humeral head (upper arm bone) as the ball and the glenoid as the socket. The glenoid (socket) is a shallow bone that is
Labral Tears What is it? The shoulder joint is a ball and socket joint, with the humeral head (upper arm bone) as the ball and the glenoid as the socket. The glenoid (socket) is a shallow bone that is
Upper Extremity Injuries in Youth Baseball: Causes and Prevention
 Upper Extremity Injuries in Youth Baseball: Causes and Prevention Biomechanics Throwing a baseball is an unnatural movement Excessively high forces are generated at the elbow and shoulder Throwing requires
Upper Extremity Injuries in Youth Baseball: Causes and Prevention Biomechanics Throwing a baseball is an unnatural movement Excessively high forces are generated at the elbow and shoulder Throwing requires
11/6/2013. Keely Behning, PT, SCS, ATC MNPTA Fall Conference November 16, 2013
 Keely Behning, PT, SCS, ATC MNPTA Fall Conference November 16, 2013 Upon completion of this course, attendees should be able to: Understand pertinent anatomy and biomechanics as they relate to specific
Keely Behning, PT, SCS, ATC MNPTA Fall Conference November 16, 2013 Upon completion of this course, attendees should be able to: Understand pertinent anatomy and biomechanics as they relate to specific
FUNCTIONAL ANATOMY OF SHOULDER JOINT
 FUNCTIONAL ANATOMY OF SHOULDER JOINT ARTICULATION Articulation is between: The rounded head of the Glenoid cavity humerus and The shallow, pear-shaped glenoid cavity of the scapula. 2 The articular surfaces
FUNCTIONAL ANATOMY OF SHOULDER JOINT ARTICULATION Articulation is between: The rounded head of the Glenoid cavity humerus and The shallow, pear-shaped glenoid cavity of the scapula. 2 The articular surfaces
POSTERIOR INSTABILITY OF THE SHOULDER Vasu Pai
 POSTERIOR INSTABILITY OF THE SHOULDER Vasu Pai Posterior instability is less common among cases of shoulder instability, accounting for 2% to 10% of all cases of instability. More common in sporting groups:
POSTERIOR INSTABILITY OF THE SHOULDER Vasu Pai Posterior instability is less common among cases of shoulder instability, accounting for 2% to 10% of all cases of instability. More common in sporting groups:
Suprascapular Nerve: How to identify when it is a problem and what to do? Speaker Disclosure
 Suprascapular Nerve: How to identify when it is a problem and what to do? Eric C. McCarty, MD Associate Professor Chief of Sports Medicine and Shoulder Surgery University of Colorado School of Medicine
Suprascapular Nerve: How to identify when it is a problem and what to do? Eric C. McCarty, MD Associate Professor Chief of Sports Medicine and Shoulder Surgery University of Colorado School of Medicine
Introduction & Question 1
 Page 1 of 7 www.medscape.com To Print: Click your browser's PRINT button. NOTE: To view the article with Web enhancements, go to: http://www.medscape.com/viewarticle/424981 Case Q & A Shoulder Pain, Part
Page 1 of 7 www.medscape.com To Print: Click your browser's PRINT button. NOTE: To view the article with Web enhancements, go to: http://www.medscape.com/viewarticle/424981 Case Q & A Shoulder Pain, Part
Rehabilitation Guidelines for Labral/Bankert Repair
 Rehabilitation Guidelines for Labral/Bankert Repair The true shoulder joint is called the glenohumeral joint and consists humeral head and the glenoid. It is a ball and socket joint. Anatomy of the Shoulder
Rehabilitation Guidelines for Labral/Bankert Repair The true shoulder joint is called the glenohumeral joint and consists humeral head and the glenoid. It is a ball and socket joint. Anatomy of the Shoulder
The Shoulder. Jill Inouye Primary Care Sports Medicine Family Medicine Resident School February 26, 2014
 The Shoulder Jill Inouye Primary Care Sports Medicine Family Medicine Resident School February 26, 2014 Objectives Review shoulder anatomy Explain and demonstrate shoulder physical exam Diagnosis and management
The Shoulder Jill Inouye Primary Care Sports Medicine Family Medicine Resident School February 26, 2014 Objectives Review shoulder anatomy Explain and demonstrate shoulder physical exam Diagnosis and management
SUPERIOR LABRAL TEARS: Fact or Fiction?
 SUPERIOR LABRAL TEARS: Michael G. Ciccotti, MD The Everett J. and Marian Gordon Professor of Orthopaedics Chief, Division of Sports Medicine Rothman Institute Head Team Physician, Philadelphia Phillies
SUPERIOR LABRAL TEARS: Michael G. Ciccotti, MD The Everett J. and Marian Gordon Professor of Orthopaedics Chief, Division of Sports Medicine Rothman Institute Head Team Physician, Philadelphia Phillies
Diagnosis and Treatment of Common Shoulder Disorders
 Diagnosis and Treatment of Common Shoulder Disorders NAOEM Oct 14 th, 2017 Michael Codsi, M.D. www.drcodsi.com Learning Objectives SLAP tears diagnosis, imaging and treatment How to diagnose rotator cuff
Diagnosis and Treatment of Common Shoulder Disorders NAOEM Oct 14 th, 2017 Michael Codsi, M.D. www.drcodsi.com Learning Objectives SLAP tears diagnosis, imaging and treatment How to diagnose rotator cuff
Double bucket handle tears of the superior labrum
 Case Report http://dx.doi.org/10.14517/aosm13013 pissn 2289-005X eissn 2289-0068 Double bucket handle tears of the superior labrum Dong-Soo Kim, Kyoung-Jin Park, Yong-Min Kim, Eui-Sung Choi, Hyun-Chul
Case Report http://dx.doi.org/10.14517/aosm13013 pissn 2289-005X eissn 2289-0068 Double bucket handle tears of the superior labrum Dong-Soo Kim, Kyoung-Jin Park, Yong-Min Kim, Eui-Sung Choi, Hyun-Chul
Review shoulder anatomy Review the physical exam of the shoulder Discuss some common causes of acute shoulder pain Discuss some common causes of
 Review shoulder anatomy Review the physical exam of the shoulder Discuss some common causes of acute shoulder pain Discuss some common causes of chronic shoulder pain Review with some case questions Bones:
Review shoulder anatomy Review the physical exam of the shoulder Discuss some common causes of acute shoulder pain Discuss some common causes of chronic shoulder pain Review with some case questions Bones:
Lawrence Gulotta Gillian Lieberman, MD October Gillian Lieberman, MD. Shoulder Imaging. Lawrence V. Gulotta, HMS IV 10/16/02
 October 2002 Shoulder Imaging Lawrence V. Gulotta, HMS IV 10/16/02 Goals Review Anatomy of the Shoulder -Dynamic Stabilizers -> Rotator Cuff -Static Stabilizers -> Labrum and Capsule Systematic Approach
October 2002 Shoulder Imaging Lawrence V. Gulotta, HMS IV 10/16/02 Goals Review Anatomy of the Shoulder -Dynamic Stabilizers -> Rotator Cuff -Static Stabilizers -> Labrum and Capsule Systematic Approach
Anatomy GH Joint. Glenohumeral Instability. Components of Stability. Components of Stability 7/7/2017. AllinaHealthSystem
 Glenohumeral Instability Dr. John Steubs Allina Sports Medicine Conference July 7, 2017 Anatomy GH Joint Teardrop or oval shape Inherently unstable Golf ball and tee analogy Stabilizers Static Dynamic
Glenohumeral Instability Dr. John Steubs Allina Sports Medicine Conference July 7, 2017 Anatomy GH Joint Teardrop or oval shape Inherently unstable Golf ball and tee analogy Stabilizers Static Dynamic
Shoulder Injuries: Treatments that Work, Do Not Work, and When ENOUGH is Enough? Mark Ganjianpour, M.D. Beverly Hills, CA April 20, 2012
 Shoulder Injuries: Treatments that Work, Do Not Work, and When ENOUGH is Enough? Mark Ganjianpour, M.D. Beverly Hills, CA April 20, 2012 Multiaxial ball and socket Little Inherent Instability Glenohumeral
Shoulder Injuries: Treatments that Work, Do Not Work, and When ENOUGH is Enough? Mark Ganjianpour, M.D. Beverly Hills, CA April 20, 2012 Multiaxial ball and socket Little Inherent Instability Glenohumeral
Management of Anterior Shoulder Instability
 Management of Anterior Shoulder Instability Angelo J. Colosimo, MD Head Orthopaedic Surgeon University of Cincinnati Athletics Director of Sports Medicine University of Cincinnati Medical Center Associate
Management of Anterior Shoulder Instability Angelo J. Colosimo, MD Head Orthopaedic Surgeon University of Cincinnati Athletics Director of Sports Medicine University of Cincinnati Medical Center Associate
Position Statement. Journal of Athletic Training 209
 Journal of Athletic Training 2018;53(3):209 229 doi: 10.4085/1062-6050-59-16 Ó by the National Athletic Trainers Association, Inc www.natajournals.org Position Statement National Athletic Trainers Association
Journal of Athletic Training 2018;53(3):209 229 doi: 10.4085/1062-6050-59-16 Ó by the National Athletic Trainers Association, Inc www.natajournals.org Position Statement National Athletic Trainers Association
SLAP Lesions Rehabilitation Concepts
 SLAP Lesions Rehabilitation Concepts Kevin E. Wilk, PT, DPT, FAPTA Glenoid Labral Lesions Introduction Classification of SLAP tears Andrews & Carson: AJSM 85 Snyder: Arthroscopy 90 (Type I IV) Maffet et
SLAP Lesions Rehabilitation Concepts Kevin E. Wilk, PT, DPT, FAPTA Glenoid Labral Lesions Introduction Classification of SLAP tears Andrews & Carson: AJSM 85 Snyder: Arthroscopy 90 (Type I IV) Maffet et
The Cryo/Cuff provides two functions: 1. Compression - to keep swelling down. 2. Ice Therapy - to keep swelling down and to help minimize pain. Patien
 The Cryo/Cuff provides two functions: 1. Compression - to keep swelling down. 2. Ice Therapy - to keep swelling down and to help minimize pain. Patients, for the most part, experience less pain and/or
The Cryo/Cuff provides two functions: 1. Compression - to keep swelling down. 2. Ice Therapy - to keep swelling down and to help minimize pain. Patients, for the most part, experience less pain and/or
APPENDIX: The Houston Astros Stretching Program
 Vol. 35, No. 4, 2007 Glenohumeral Internal Rotation Deficits 1 APPENDIX: The Houston Astros Stretching Program Our Flexibility program consists of 5 positions. Four of the 5 have 2 variations of each position.
Vol. 35, No. 4, 2007 Glenohumeral Internal Rotation Deficits 1 APPENDIX: The Houston Astros Stretching Program Our Flexibility program consists of 5 positions. Four of the 5 have 2 variations of each position.
11/15/2017. Biceps Lesions. Highgate Private Hospital (Whittington Health NHS Trust) E: LHB Anatomy.
 E: LHB Anatomy.") Biceps Lesions Mr Omar Haddo (Consultant Orthopaedic Surgeon MBBS, BmedSci, FRCS(Orth) ) Highgate Private Hospital (Whittington Health NHS Trust) E: admin@denovomedic.co.uk LHB Anatomy Arise from superior
Biceps Lesions Mr Omar Haddo (Consultant Orthopaedic Surgeon MBBS, BmedSci, FRCS(Orth) ) Highgate Private Hospital (Whittington Health NHS Trust) E: admin@denovomedic.co.uk LHB Anatomy Arise from superior
DK7215-Levine-ch12_R2_211106
 12 Arthroscopic Rotator Interval Closure Andreas H. Gomoll Department of Orthopedic Surgery, Brigham and Women s Hospital, Harvard Medical School, Boston, Massachusetts, U.S.A. Brian J. Cole Departments
12 Arthroscopic Rotator Interval Closure Andreas H. Gomoll Department of Orthopedic Surgery, Brigham and Women s Hospital, Harvard Medical School, Boston, Massachusetts, U.S.A. Brian J. Cole Departments
Advances in Rehabilitation of the Throwing Athlete
 Advances in Rehabilitation of the Throwing Athlete Introduction It is a "whipping" action that brings the hand and eventually the ball to a speed of 90 to 100 mph. Elite level is 87 MPH (Football is 55
Advances in Rehabilitation of the Throwing Athlete Introduction It is a "whipping" action that brings the hand and eventually the ball to a speed of 90 to 100 mph. Elite level is 87 MPH (Football is 55
Shoulder Arthroscopy Lab Manual
 Shoulder Arthroscopy Lab Manual Dalhousie University Orthopaedic Program May 5, 2017 Skills Centre OBJECTIVES 1. Demonstrate a competent understanding of the arthroscopic anatomy and biomechanics of the
Shoulder Arthroscopy Lab Manual Dalhousie University Orthopaedic Program May 5, 2017 Skills Centre OBJECTIVES 1. Demonstrate a competent understanding of the arthroscopic anatomy and biomechanics of the
Suprascapular Nerve Entrapment: Technique for Arthroscopic Release
 Techniques in Shoulder and Elbow Surgery 7(2):000 000, 2006 R E V I E W Suprascapular Nerve Entrapment: Technique for Arthroscopic Release Peter J. Millett, MD, MSc Steadman Hawkins Clinic, Vail, CO Harvard
Techniques in Shoulder and Elbow Surgery 7(2):000 000, 2006 R E V I E W Suprascapular Nerve Entrapment: Technique for Arthroscopic Release Peter J. Millett, MD, MSc Steadman Hawkins Clinic, Vail, CO Harvard
Disclosures 7/25/2018. SLAP Tears In Overhead Athletes: Should We Be Fixing Them? How Do We Fix Them?
 SLAP Tears In Overhead Athletes: Should We Be Fixing Them? How Do We Fix Them? Michael T. Freehill M.D. Associate Professor of Orthopaedic Surgery University of Michigan 10th Annual Detroit Regional Sports
SLAP Tears In Overhead Athletes: Should We Be Fixing Them? How Do We Fix Them? Michael T. Freehill M.D. Associate Professor of Orthopaedic Surgery University of Michigan 10th Annual Detroit Regional Sports
Rehabilitation Guidelines for Anterior Shoulder Reconstruction with Arthroscopic Bankart Repair
 UW HEALTH SPORTS REHABILITATION Rehabilitation Guidelines for Anterior Shoulder Reconstruction with Arthroscopic Bankart Repair The anatomic configuration of the shoulder joint (glenohumeral joint) is
UW HEALTH SPORTS REHABILITATION Rehabilitation Guidelines for Anterior Shoulder Reconstruction with Arthroscopic Bankart Repair The anatomic configuration of the shoulder joint (glenohumeral joint) is
Patient ID. Case Conference. Physical Examination. Image examination. Treatment 2011/6/16
 Patient ID Case Conference R3 高逢駿 VS 徐郭堯 55 y/o female C.C.: recurrent right shoulder dislocation noted since falling down injury 2 years ago Came to ER because of dislocation for many times due to minor
Patient ID Case Conference R3 高逢駿 VS 徐郭堯 55 y/o female C.C.: recurrent right shoulder dislocation noted since falling down injury 2 years ago Came to ER because of dislocation for many times due to minor
Shoulder Injuries. Glenoid labrum injuries. SLAP Lesions
 Shoulder Injuries functional anatomy clinical perspective impingement rotator cuff injuries glenoid labrum injuries dislocation Glenoid labrum injuries SLAP lesions stable or unstable traction/compression
Shoulder Injuries functional anatomy clinical perspective impingement rotator cuff injuries glenoid labrum injuries dislocation Glenoid labrum injuries SLAP lesions stable or unstable traction/compression
SHOULDER PROBLEMS & ARTHROSCOPIC MANAGEMENT
 SHOULDER PROBLEMS & ARTHROSCOPIC MANAGEMENT DR.SHEKHAR SRIVASTAV Sr. Consultant-KNEE & SHOULDER Arthroscopy Sant Parmanand Hospital,Delhi Peculiarities of Shoulder Elegant piece of machinery It has the
SHOULDER PROBLEMS & ARTHROSCOPIC MANAGEMENT DR.SHEKHAR SRIVASTAV Sr. Consultant-KNEE & SHOULDER Arthroscopy Sant Parmanand Hospital,Delhi Peculiarities of Shoulder Elegant piece of machinery It has the
MUSCLES OF SHOULDER REGION
 Dr Jamila EL Medany OBJECTIVES At the end of the lecture, students should: List the name of muscles of the shoulder region. Describe the anatomy of muscles of shoulder region regarding: attachments of
Dr Jamila EL Medany OBJECTIVES At the end of the lecture, students should: List the name of muscles of the shoulder region. Describe the anatomy of muscles of shoulder region regarding: attachments of
Arm Pain in Throwing Athletes. Eric N. Hoeper, MD Primary Care Sports Medicine NorthShore University HealthSystem
 Arm Pain in Throwing Athletes Eric N. Hoeper, MD Primary Care Sports Medicine NorthShore University HealthSystem I have no potential conflicts of interest to declare. What s the Big Deal? Between 26% and
Arm Pain in Throwing Athletes Eric N. Hoeper, MD Primary Care Sports Medicine NorthShore University HealthSystem I have no potential conflicts of interest to declare. What s the Big Deal? Between 26% and
Shoulder Joint Examination. Shoulder Joint Examination. Inspection. Inspection Palpation Movement. Look Feel Move
 Shoulder Joint Examination History Cuff Examination Instability Examination AC Joint Examination Biceps Tendon Examination Superior Labrum Examination Shoulder Joint Examination Inspection Palpation Movement
Shoulder Joint Examination History Cuff Examination Instability Examination AC Joint Examination Biceps Tendon Examination Superior Labrum Examination Shoulder Joint Examination Inspection Palpation Movement
The suction cup mechanism is enhanced by the slightly negative intra articular pressure within the joint.
 SHOULDER INSTABILITY Stability A. The stability of the shoulder is improved by depth of the glenoid. This is determined by: 1. Osseous glenoid, 2. Articular cartilage of the glenoid, which is thicker at
SHOULDER INSTABILITY Stability A. The stability of the shoulder is improved by depth of the glenoid. This is determined by: 1. Osseous glenoid, 2. Articular cartilage of the glenoid, which is thicker at
WEEKEND 2 Shoulder. Shoulder Active Range of Motion Assessment
 Virginia Orthopedic Manual Physical Therapy Institute - 2016 Technique Manual WEEKEND 2 Shoulder Shoulder Active Range of Motion Assessment - Patient Positioning: Standing, appropriately undressed so that
Virginia Orthopedic Manual Physical Therapy Institute - 2016 Technique Manual WEEKEND 2 Shoulder Shoulder Active Range of Motion Assessment - Patient Positioning: Standing, appropriately undressed so that
Shoulder Labral Tear and Shoulder Dislocation
 Shoulder Labral Tear and Shoulder Dislocation The shoulder joint is a ball and socket joint with tremendous flexibility and range of motion. The ball is the humeral head while the socket is the glenoid.
Shoulder Labral Tear and Shoulder Dislocation The shoulder joint is a ball and socket joint with tremendous flexibility and range of motion. The ball is the humeral head while the socket is the glenoid.
The Shoulder. Anatomy and Injuries PSK 4U Unit 3, Day 4
 The Shoulder Anatomy and Injuries PSK 4U Unit 3, Day 4 Shoulder Girdle Shoulder Complex is the most mobile joint in the body. Scapula Clavicle Sternum Humerus Rib cage/thorax Shoulder Girdle It also includes
The Shoulder Anatomy and Injuries PSK 4U Unit 3, Day 4 Shoulder Girdle Shoulder Complex is the most mobile joint in the body. Scapula Clavicle Sternum Humerus Rib cage/thorax Shoulder Girdle It also includes
Technique For SLAP Repair in 2016
 Technique For SLAP Repair in 2016 Eric J. Strauss MD Division of Sports Medicine NYU Hospital for Joint Diseases Hospital for Joint Diseases Department of Orthopaedic Surgery Disclosures Joint Restoration
Technique For SLAP Repair in 2016 Eric J. Strauss MD Division of Sports Medicine NYU Hospital for Joint Diseases Hospital for Joint Diseases Department of Orthopaedic Surgery Disclosures Joint Restoration
The glenohumeral joint has a unique anatomic configuration
 Imaging of Glenohumeral Instability Timothy G. Sanders, MD,*, Michael Zlatkin, MD,*, and Justin Montgomery, MD The glenohumeral joint has a unique anatomic configuration designed to maximize the positioning
Imaging of Glenohumeral Instability Timothy G. Sanders, MD,*, Michael Zlatkin, MD,*, and Justin Montgomery, MD The glenohumeral joint has a unique anatomic configuration designed to maximize the positioning
Disclosure 8/10/2016. SLAP Or Biceps: Repair or Tenodesis? Royalties/Stock Options: Smith and Nephew, Omeros, Minivasive
 SLAP Or Biceps: Repair or Tenodesis? Nikhil N. Verma MD Director Sports Medicine Professor, Orthopedic Surgery Rush University Medical Center Midwest Orthopaedics at Rush Disclosure Royalties/Stock Options:
SLAP Or Biceps: Repair or Tenodesis? Nikhil N. Verma MD Director Sports Medicine Professor, Orthopedic Surgery Rush University Medical Center Midwest Orthopaedics at Rush Disclosure Royalties/Stock Options:
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Abduction pillow, ultrasling, 880, 881, 882, 883 Adolescents, shoulder instability in. See Shoulder, instability of, pediatric and adolescent.
Index Note: Page numbers of article titles are in boldface type. A Abduction pillow, ultrasling, 880, 881, 882, 883 Adolescents, shoulder instability in. See Shoulder, instability of, pediatric and adolescent.
Management of Massive/Revision Rotator Cuff Tears
 Management of Massive/Revision Rotator Cuff Tears Nikhil N. Verma MD, Director Sports Medicine, Rush University Medical Center, Midwest Orthopedics at Rush, Chicago, IL nverma@rushortho.com I. Anatomy
Management of Massive/Revision Rotator Cuff Tears Nikhil N. Verma MD, Director Sports Medicine, Rush University Medical Center, Midwest Orthopedics at Rush, Chicago, IL nverma@rushortho.com I. Anatomy
Rotator Cuff Repair TRENDS OF REPAIRS. Evolution of Arthroscopic Repair. Shoulder Girdle. Rotator Cuff Repair 8/29/2013
 Rotator Cuff Repair Indications, Patient Selection, Outcomes James C. Vailas, M.D. New Hampshire Orthopaedic Center September 14, 2013 New Hampshire Musculoskeletal Institute 20 th Annual Symposium Evolution
Rotator Cuff Repair Indications, Patient Selection, Outcomes James C. Vailas, M.D. New Hampshire Orthopaedic Center September 14, 2013 New Hampshire Musculoskeletal Institute 20 th Annual Symposium Evolution
Christopher A Brown, MD Sports Medicine Orthopedist. Duke Orthopedic Residency Sports Medicine Fellowship Stanford
 Christopher A Brown, MD Sports Medicine Orthopedist Duke Orthopedic Residency Sports Medicine Fellowship Stanford Office Geneva Newark Opening Canandaigua and Penfield Topics Of Discussion Shoulder dislocation
Christopher A Brown, MD Sports Medicine Orthopedist Duke Orthopedic Residency Sports Medicine Fellowship Stanford Office Geneva Newark Opening Canandaigua and Penfield Topics Of Discussion Shoulder dislocation
Glenohumeral Joint Instability. Static Stabilizers of the GHJ. Static Stabilizers of the GHJ. Static Stabilizers of the GHJ
 1 Glenohumeral Joint Instability GHJ Joint Stability: Or Lack Thereof! Christine B. Chung, M.D. Assistant Professor of Radiology Musculoskeletal Division UCSD and VA Healthcare System Static Stabilizers
1 Glenohumeral Joint Instability GHJ Joint Stability: Or Lack Thereof! Christine B. Chung, M.D. Assistant Professor of Radiology Musculoskeletal Division UCSD and VA Healthcare System Static Stabilizers
SHOULDER INSTABILITY
 SHOULDER INSTABILITY Dr.KN Subramanian M.Ch Orth., FRCS (Tr & Orth), CCT Orth(UK) Consultant Orthopaedic Surgeon, Special interest: Orthopaedic Sports Injury, Shoulder and Knee Surgery, SPARSH Hospital
SHOULDER INSTABILITY Dr.KN Subramanian M.Ch Orth., FRCS (Tr & Orth), CCT Orth(UK) Consultant Orthopaedic Surgeon, Special interest: Orthopaedic Sports Injury, Shoulder and Knee Surgery, SPARSH Hospital
Intern Arthroscopy Course 2015 Shoulder Arthroscopy Cases
 Intern Arthroscopy Course 2015 Shoulder Arthroscopy Cases Mary Lloyd Ireland, M.D. University of Kentucky Dept. of Orthopaedic Surgery & Sports Medicine Lexington, KY Broken screw s/p Bristow procedure
Intern Arthroscopy Course 2015 Shoulder Arthroscopy Cases Mary Lloyd Ireland, M.D. University of Kentucky Dept. of Orthopaedic Surgery & Sports Medicine Lexington, KY Broken screw s/p Bristow procedure
Injury to the superior labrum i.e. superior labral anterior
 Original Article Correlation of the slap lesion with lesions of the medial sheath of the biceps tendon and intra-articular subscapularis tendon William F Bennett Abstract Background: Superior labral anterior
Original Article Correlation of the slap lesion with lesions of the medial sheath of the biceps tendon and intra-articular subscapularis tendon William F Bennett Abstract Background: Superior labral anterior
Supplemental Video Available at
 Current Concepts in the Recognition and Treatment of Superior Labral (SLAP) Lesions Kevin E. Wilk, DPT 1 Michael M. Reinold, DPT, ATC, CSCS 2 Jeffrey R. Dugas, MD 3 Christopher A. Arrigo, PT, MS 4 Michael
Current Concepts in the Recognition and Treatment of Superior Labral (SLAP) Lesions Kevin E. Wilk, DPT 1 Michael M. Reinold, DPT, ATC, CSCS 2 Jeffrey R. Dugas, MD 3 Christopher A. Arrigo, PT, MS 4 Michael
Common Surgical Shoulder Injury Repairs
 Common Surgical Shoulder Injury Repairs Mr Ilia Elkinson BHB, MBChB, FRACS (Ortho), FNZOA Orthopaedic and Upper Limb Surgeon Bowen Hospital Wellington Hospital Objectives Review pertinent anatomy of the
Common Surgical Shoulder Injury Repairs Mr Ilia Elkinson BHB, MBChB, FRACS (Ortho), FNZOA Orthopaedic and Upper Limb Surgeon Bowen Hospital Wellington Hospital Objectives Review pertinent anatomy of the
Throwing Athlete Rehabilitation. Brett Schulz LAT/CMSS Sport and Spine Physical Therapy
 Throwing Athlete Rehabilitation Brett Schulz LAT/CMSS Sport and Spine Physical Therapy Disclosure No conflicts to disclose Throwing Athlete Dilemma The shoulder must have enough range of motion to allow
Throwing Athlete Rehabilitation Brett Schulz LAT/CMSS Sport and Spine Physical Therapy Disclosure No conflicts to disclose Throwing Athlete Dilemma The shoulder must have enough range of motion to allow
P.O. Box Sierra Park Road Mammoth Lakes, CA Orthopedic Surgery & Sports Medicine
 P.O. Box 660 85 Sierra Park Road Mammoth Lakes, CA 93546 SHOULDER: Instability Dislocation Labral Tears The shoulder is the most mobile joint in the body, but to have this amount of motion, it is also
P.O. Box 660 85 Sierra Park Road Mammoth Lakes, CA 93546 SHOULDER: Instability Dislocation Labral Tears The shoulder is the most mobile joint in the body, but to have this amount of motion, it is also
Rehabilitation of Overhead Shoulder Injuries
 Rehabilitation of Overhead Shoulder Injuries 16 th Annual Primary Care Orthopaedic & Sports Medicine Symposium January 29, 2016 Jeremy Sherman, PT, MPT Disclosures No financial disclosures to note. Jeremy
Rehabilitation of Overhead Shoulder Injuries 16 th Annual Primary Care Orthopaedic & Sports Medicine Symposium January 29, 2016 Jeremy Sherman, PT, MPT Disclosures No financial disclosures to note. Jeremy
Bryan L Reuss MD. Objectives: Orlando Orthopaedic Center Orlando, FL
 Bryan L Reuss MD Orlando Orthopaedic Center Orlando, FL breuss@mac.com Dr. Reuss earned his B.A. in Biology from the University of Kansas and his M.D. degree with Honors from the University of Nebraska
Bryan L Reuss MD Orlando Orthopaedic Center Orlando, FL breuss@mac.com Dr. Reuss earned his B.A. in Biology from the University of Kansas and his M.D. degree with Honors from the University of Nebraska
DIFFERENTIAL DIAGNOSIS: Looking for the causes of impingement
 DIFFERENTIAL DIAGNOSIS: Looking for the causes of Ann Cools, PT, PhD Ghent University - Belgium Dept of Rehabilitation Sciences & Physiotherapy Ann.Cools@UGent.be «thinking about.» Which special tests
DIFFERENTIAL DIAGNOSIS: Looking for the causes of Ann Cools, PT, PhD Ghent University - Belgium Dept of Rehabilitation Sciences & Physiotherapy Ann.Cools@UGent.be «thinking about.» Which special tests
RECURRENT SHOULDER DISLOCATIONS WITH ABSENT LABRUM
 RECURRENT SHOULDER DISLOCATIONS WITH ABSENT LABRUM D R. A M R I S H K R. J H A M S ( O R T H O ) A S S I S T A N T P R O F E S S O R M E D I C A L C O L L E G E, K O L K A T A LABRUM Function as a chock-block,
RECURRENT SHOULDER DISLOCATIONS WITH ABSENT LABRUM D R. A M R I S H K R. J H A M S ( O R T H O ) A S S I S T A N T P R O F E S S O R M E D I C A L C O L L E G E, K O L K A T A LABRUM Function as a chock-block,
Acromioplasty. Surgical Indications and Considerations
 1 Acromioplasty Surgical Indications and Considerations Anatomical Considerations: Any abnormality that disrupts the intricate relationship within the subacromial space may lead to impingement. Both intrinsic
1 Acromioplasty Surgical Indications and Considerations Anatomical Considerations: Any abnormality that disrupts the intricate relationship within the subacromial space may lead to impingement. Both intrinsic
An analysis of 140 injuries to the superior glenoid labrum
 ORIGINAL ARTICLES An analysis of 140 injuries to the superior glenoid labrum Stephen J. Snyder, MD, Michael P. Banas, MD, and Ronald P. Karzel, MD, Van Nuys, Calif. Between 1985 and 1993 140 injuries of
ORIGINAL ARTICLES An analysis of 140 injuries to the superior glenoid labrum Stephen J. Snyder, MD, Michael P. Banas, MD, and Ronald P. Karzel, MD, Van Nuys, Calif. Between 1985 and 1993 140 injuries of
Rotator cuff injuries are commonly attributed to repetitive
 [ Orthopaedics ] Massive Rotator Cuff Tear in an Adolescent Athlete: A Case Report Kimberly A. Turman, MD,* Mark W. Anderson, MD, and Mark D. Miller, MD Full-thickness rotator cuff tears in the young athlete
[ Orthopaedics ] Massive Rotator Cuff Tear in an Adolescent Athlete: A Case Report Kimberly A. Turman, MD,* Mark W. Anderson, MD, and Mark D. Miller, MD Full-thickness rotator cuff tears in the young athlete
Rehabilitation Guidelines for Biceps Tenodesis with Hardware Fixation
 UW HEALTH SPORTS REHABILITATION Rehabilitation Guidelines for Biceps Tenodesis with Hardware Fixation The shoulder has two primary joints. One part of the shoulder blade, called the glenoid fossa forms
UW HEALTH SPORTS REHABILITATION Rehabilitation Guidelines for Biceps Tenodesis with Hardware Fixation The shoulder has two primary joints. One part of the shoulder blade, called the glenoid fossa forms
The overhead throwing motion is a highly skilled movement
 KEVIN E. WILK, PT, DPT¹ MD² DPT³ MD 4 MD 4 MD 5 Shoulder Injuries in the Overhead Athlete The overhead throwing motion is a highly skilled movement performed at extremely high velocity, which requires
KEVIN E. WILK, PT, DPT¹ MD² DPT³ MD 4 MD 4 MD 5 Shoulder Injuries in the Overhead Athlete The overhead throwing motion is a highly skilled movement performed at extremely high velocity, which requires
FAI syndrome with or without labral tear.
 Case This 16-year-old female, soccer athlete was treated for pain in the right groin previously. Now has acute onset of pain in the left hip. The pain was in the groin that was worse with activities. Diagnosis
Case This 16-year-old female, soccer athlete was treated for pain in the right groin previously. Now has acute onset of pain in the left hip. The pain was in the groin that was worse with activities. Diagnosis
Rehabilitation Guidelines for Anterior Shoulder Reconstruction with Open Bankart Repair
 UW HEALTH SPORTS REHABILITATION Rehabilitation Guidelines for Anterior Shoulder Reconstruction with Open Bankart Repair The anatomic configuration of the shoulder joint (glenohumeral joint) is often compared
UW HEALTH SPORTS REHABILITATION Rehabilitation Guidelines for Anterior Shoulder Reconstruction with Open Bankart Repair The anatomic configuration of the shoulder joint (glenohumeral joint) is often compared
Anatomical Considerations/ Pathophysiology The shoulder is the most mobile joint in the body. : Three bones:
 Introduction Musculoskeletal training is generally underrepresented in medical training and residency curriculums. There is a general deficit in musculoskeletal knowledge amongst current medical students,
Introduction Musculoskeletal training is generally underrepresented in medical training and residency curriculums. There is a general deficit in musculoskeletal knowledge amongst current medical students,
ER + IR = Total Motion
 Treating the Thrower s Shoulder Michael M. Reinold, PT, DPT, ATC, CSCS Introduction Common site of injury» Repetitive forces / stresses Tremendous joint forces» Anterior shear forces 1-1.5 1.5 X BW» Distraction
Treating the Thrower s Shoulder Michael M. Reinold, PT, DPT, ATC, CSCS Introduction Common site of injury» Repetitive forces / stresses Tremendous joint forces» Anterior shear forces 1-1.5 1.5 X BW» Distraction
SHOULDER INSTABILITY
 SHOULDER INSTABILITY Your shoulder is the most flexible joint in your body, allowing you to throw fastballs, lift a heavy suitcase, scratch your back, and reach in almost any direction. Your shoulder joint
SHOULDER INSTABILITY Your shoulder is the most flexible joint in your body, allowing you to throw fastballs, lift a heavy suitcase, scratch your back, and reach in almost any direction. Your shoulder joint
Rehabilitation Guidelines for Shoulder Arthroscopy
 Rehabilitation Guidelines for Shoulder Arthroscopy The true shoulder joint is called the glenohumeral joint and consists humeral head and the glenoid. It is a ball and socket joint. Anatomy of the Shoulder
Rehabilitation Guidelines for Shoulder Arthroscopy The true shoulder joint is called the glenohumeral joint and consists humeral head and the glenoid. It is a ball and socket joint. Anatomy of the Shoulder
APPROPRIATE USE GUIDELINES
 APPROPRIATE USE GUIDELINES Appropriateness of Advanced Imaging Procedures (MRI, CT, Bone Scan/PET) in Patients with Shoulder Pain CDI QUALITY INSTITUTE: PROVIDER LED ENTITY (PLE) Compiled by Rob Liddell,
APPROPRIATE USE GUIDELINES Appropriateness of Advanced Imaging Procedures (MRI, CT, Bone Scan/PET) in Patients with Shoulder Pain CDI QUALITY INSTITUTE: PROVIDER LED ENTITY (PLE) Compiled by Rob Liddell,
Partial Thickness Rotator Cuff Tears: All-Inside Repair of PASTA Lesions in Athletes
 Partial Thickness Rotator Cuff Tears: All-Inside Repair of PASTA Lesions in Athletes Thomas M. DeBerardino, MD Associate Professor, UConn Health Center Team Physician, Orthopaedic Consultant UConn Huskie
Partial Thickness Rotator Cuff Tears: All-Inside Repair of PASTA Lesions in Athletes Thomas M. DeBerardino, MD Associate Professor, UConn Health Center Team Physician, Orthopaedic Consultant UConn Huskie
A comparison of the immediate effects of muscle energy technique and joint mobilizations on posterior shoulder tightness in youth throwing athletes
 Illinois State University ISU ReD: Research and edata Theses and Dissertations 11-7-2016 A comparison of the immediate effects of muscle energy technique and joint mobilizations on posterior shoulder tightness
Illinois State University ISU ReD: Research and edata Theses and Dissertations 11-7-2016 A comparison of the immediate effects of muscle energy technique and joint mobilizations on posterior shoulder tightness
Anatomy of the Shoulder Girdle. Prof Oluwadiya Kehinde FMCS (Orthop)
") Anatomy of the Shoulder Girdle Prof Oluwadiya Kehinde FMCS (Orthop) www.oluwadiya.com Bony Anatomy Shoulder Complex: Sternum(manubrium) Clavicle Scapula Proximal humerus Manubrium Sterni Upper part of
Anatomy of the Shoulder Girdle Prof Oluwadiya Kehinde FMCS (Orthop) www.oluwadiya.com Bony Anatomy Shoulder Complex: Sternum(manubrium) Clavicle Scapula Proximal humerus Manubrium Sterni Upper part of
Page 1. Shoulder Injuries in Sports.
 www.schulterteam.ch Shoulder Injuries in Sports Matthias A Zumstein Shoulder, Elbow and Orthopaedic Sports Medicine Department of Orthopedic Surgery and Traumatology University of Berne, Switzerland matthias.zumstein@insel.ch
www.schulterteam.ch Shoulder Injuries in Sports Matthias A Zumstein Shoulder, Elbow and Orthopaedic Sports Medicine Department of Orthopedic Surgery and Traumatology University of Berne, Switzerland matthias.zumstein@insel.ch
Index. radiologic.theclinics.com. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Acromioclavicular joint injuries in football players, 318, 319 ALPSA. See Anterior labroligamentous periosteal sleeve avulsion. Anterior
Index Note: Page numbers of article titles are in boldface type. A Acromioclavicular joint injuries in football players, 318, 319 ALPSA. See Anterior labroligamentous periosteal sleeve avulsion. Anterior
Considerations 3/9/2018. Asheesh Bedi, MD. I have no disclosures or conflicts of interest related to the content of this presentation.
 Radiological Assessment of the Rotator Cuff What predicts outcomes? Asheesh Bedi, MD Harold and Helen W. Gehring Professor Chief, Sports Medicine & Shoulder Surgery MedSport, Department of Orthopedic Surgery
Radiological Assessment of the Rotator Cuff What predicts outcomes? Asheesh Bedi, MD Harold and Helen W. Gehring Professor Chief, Sports Medicine & Shoulder Surgery MedSport, Department of Orthopedic Surgery
Aquatic Exercise. Rehabilitation after the SLAP lesion repair. I. Anatomy & Function SLAP 의가장흔한손상기전. Anatomy of the Shoulder (I)
") Aquatic Exercise Rehabilitation after the SLAP lesion repair Sports Medicine Clinic Sky 임승길 ATC 2 SLAP 의가장흔한손상기전 SLAP Superior Labrum Anterior to Posterior 1. Compression force Attempting to catch a heavy
Aquatic Exercise Rehabilitation after the SLAP lesion repair Sports Medicine Clinic Sky 임승길 ATC 2 SLAP 의가장흔한손상기전 SLAP Superior Labrum Anterior to Posterior 1. Compression force Attempting to catch a heavy
MR Arthrography of the Shoulder - A Beginner's Guide
 MR Arthrography of the Shoulder - A Beginner's Guide Poster No.: C-1034 Congress: ECR 2011 Type: Educational Exhibit Authors: A. Jain, S. Connolly; Prescot/UK Keywords: Pathology, Arthrography, MR, Musculoskeletal
MR Arthrography of the Shoulder - A Beginner's Guide Poster No.: C-1034 Congress: ECR 2011 Type: Educational Exhibit Authors: A. Jain, S. Connolly; Prescot/UK Keywords: Pathology, Arthrography, MR, Musculoskeletal
This presentation is the intellectual property of the author. Contact them at for permission to reprint and/or distribute.
 January 19, 2012 John W. Hinchey, MD Dept of Orthopaedic Surgery Shoulder & Elbow Service This live activity is designated for a maximum of 1 AMA PRA Category 1 Credit tm. Physicians should claim only
January 19, 2012 John W. Hinchey, MD Dept of Orthopaedic Surgery Shoulder & Elbow Service This live activity is designated for a maximum of 1 AMA PRA Category 1 Credit tm. Physicians should claim only
Arthroscopic fixation of isolated type II SLAP lesions using a two-portal technique
 Acta Orthop. Belg., 2011, 77, 160-166 ORIGINAL STUDY Arthroscopic fixation of isolated type II SLAP lesions using a two-portal technique Aristotelis KAisiDis, Panagiotis PAntOs, Horst HEGER, Dimitrios
Acta Orthop. Belg., 2011, 77, 160-166 ORIGINAL STUDY Arthroscopic fixation of isolated type II SLAP lesions using a two-portal technique Aristotelis KAisiDis, Panagiotis PAntOs, Horst HEGER, Dimitrios
Mastering the Musculoskeletal Exam UCSF Essentials of Women s Health July 7, 2016 Carlin Senter, M.D. Henry Crevensten, M.D.
 Mastering the Musculoskeletal Exam UCSF Essentials of Women s Health July 7, 2016 Carlin Senter, M.D. Henry Crevensten, M.D. I have nothing to disclose Outline Knee exam Shoulder exam Knee Anatomy The
Mastering the Musculoskeletal Exam UCSF Essentials of Women s Health July 7, 2016 Carlin Senter, M.D. Henry Crevensten, M.D. I have nothing to disclose Outline Knee exam Shoulder exam Knee Anatomy The
The shoulder girdle consists of the glenohumeral, acromioclavicular, sternoclavicular and scapulothoracic joints
 Anatomy of Shoulder Girdle The shoulder girdle consists of the glenohumeral, acromioclavicular, sternoclavicular and scapulothoracic joints Glenohumeral Joint A ball and socket synoval joint with a large
Anatomy of Shoulder Girdle The shoulder girdle consists of the glenohumeral, acromioclavicular, sternoclavicular and scapulothoracic joints Glenohumeral Joint A ball and socket synoval joint with a large
Anterior shoulder instability: Evaluation using MR arthrography.
 Anterior shoulder instability: Evaluation using MR arthrography. Poster No.: C-2407 Congress: ECR 2016 Type: Educational Exhibit Authors: C. Lord, I. Katsimilis, N. Purohit, V. T. Skiadas; Southampton/UK
Anterior shoulder instability: Evaluation using MR arthrography. Poster No.: C-2407 Congress: ECR 2016 Type: Educational Exhibit Authors: C. Lord, I. Katsimilis, N. Purohit, V. T. Skiadas; Southampton/UK