Evaluation and Management of Scapular Dysfunction
|
|
|
- Susanna Turner
- 5 years ago
- Views:
Transcription



 Interspinous Ligs (Kellgren; Feinstein) Facet joint (Dwyer) Lev Scap (Travell)")

 => pain & function Identified impairments")

1 Evaluation and Management of Scapular Dysfunction Phil McClure PT, PhD Goals of this presentation Relevance of scapular dysfunction to common shoulder pathologies rmal scapular motion & function Key examination techniques to identify scapular dysfunction Key treatment concepts and techniques to address scapular dysfunction Why all the fuss about the scapula? Is it a direct source of symptoms? Rarely Scapular pain: think cervical spine first Scapular Dysfunction The Big Picture Scapular Dysfunction Something not working correctly Medical Diagnosis or Physical Impairment? Who cares? IV disc (Cloward) Interspinous Ligs (Kellgren; Feinstein) Facet joint (Dwyer) Lev Scap (Travell) Scapular Dysfunction The Big Picture Medical diagnosis RC tendinopathy/tear, instability, SLAP, frozen shoulder helps direct general course of care and prognosis does not dictate specific rehab As therapists, we treat physical impairments identified through an examination Assumption : improving impairments (strength, ROM, motor control, posture etc) => pain & function Identified impairments dictate specific rehab Scapular Dysfunction The Big Picture Scapular Dysfunction is an Impairment Abnormal motion or posture, weakness, tightness t a medical diagnosis Shoulder Impingement/ RC tendinopathy is the most common medical diagnosis potentially influenced by scapular dysfunction SLAP injuries, instability, frozen shoulder may also be related 1







2 Scapular Dysfunction Is it related to common shoulder pathologies? Maybe Subacromial Impingement Abnormal motion leads to decrease in subacromial space => impingement/tendinopathy Abnormal motion / posture results in inefficiency and overuse of rot cuff => impingement/tendinopathy Rot cuff may be the victim but scap dysfunction may be culprit True evidence directly linking scapular dysfunction with impingement is lacking Rotator Cuff / Impingement 2nd Level Shoulder Classification Specific Exam Key Positive: impingement signs Painful arc Pain w/ isom resist Weakness Atrophy Key negative: Sig loss of motion Instability signs Common Shoulder Diagnoses Frozen Shoulder Key Positive: Spontaneous progressive pain Loss of motion in multiple planes Pain at end-range Key negative: rmal motion Age < 40 Glenohumeral Instability Key Positive: Age usu < 40 Hx disloc / sublux Apprehension Generalized laxity Key negative: hx disloc apprehension Other GH Arthritis Fractures AC jt Neural Entrap Myofascial Fibromyalgia Post-Op Red Flag Conditions Scapula Dysfunction Is it related to common shoulder pathologies? Maybe Frozen Shoulder Compensatory early/excessive scapular motion has been identified May be difficult to unlearn SLAP / GH Instability Unstable or malpositioned scapula may lead to over stress of labrum and GH capsular structures, especially overhead sports Cause or Effect? Base for UE function Mobility Requirement for proper positioning: maintain length-tension relationship for GH muscles maintain GH stability during UE task by following the humerus Stability Requirement: base for force generation through UE The Scapula Functional Role The Scapula rmal Motion Is it as simple as 2:1? 30 o 60 o 2


: 269-277, 2001 Subjects Eight")


 motion Three")

3 Direct Three-Dimensional Measurement of Scapular Kinematics. McClure PW, Karduna AR, Michener LA, Sennett BJ. Journal of Shoulder and Elbow Surgery 10(3): , 2001 Subjects Eight healthy volunteers One patient with impingement syndrome Protocol/Data Analysis 2 bone pins inserted directly into scapula Mount sensors and set up coordinate systems Flexion, Scaption, IR/ER@90 Continuous (dynamic) motion Three trials - averaged and interpolated Scapular Rotations Clavicular Rotations (also Scapular Translation) Ludewig 2009 JBJS Scapular Plane Elevation: Scap Upward Rot Mean = 50 o 3






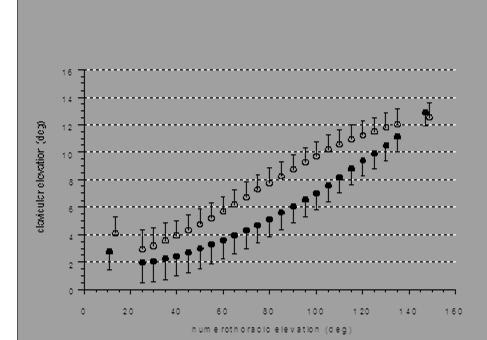
4 Scapular Plane Elevation: Scap Posterior Tilting Mean = 30 o Scapular Plane Elevation: Scap Ext Rot Mean = 24.0 o Scapular Plane Elevation: Clavicular Elevation Mean=10 o 4




 with specific manual muscle Determine corrective strategies Triceps (long head) testing Determine source of deficit Neural injury")
 Classifying scapular motion: the scapula dyskinesis test (SDT) (McClure et al.")
 dyskinesis: mild/questionable evidence of abnormality, not consistently present Obvious (O) dyskinesis: striking, clearly apparent abnormalities, evident on at")
5 Scapular Plane Elevation: Clavicular Retraction Protraction Mean=21 o Shoulder Girdle Motion Retraction Four Articulations Glenohumeral Scapulothoracic Acromioclavicular Sternoclavicular Clav Retract Is Scapular Dyskinesis Present? Visual observation during flexion and abduction with and without resistance If negative, consider testing under fatiguing conditions Continue Shoulder Exam Scapular dysfunction unlikely From: McClure PW, Sciascia AD, Uhl TL. Are symptoms changed with manual correction? Scapular Reposition/Retraction Test Scapular Examination pp35 51 In Scapular Assistance Test Disorders of the Scapula and Other corrections of scapular malposition Their Role in Shoulder Injury. Verbal/Manual Cueing to correct position/motion Kibler WB, Sciascia AD eds. Springer 2017 Identify tissue source of dysfunction to guide appropriate intervention Soft tissue tightness: Poor Muscle Performance Test Specific Structures Readily correctable with cueing and conscious effort? Axioscapular Muscles Glenohumeral Capsule and Muscles Pectoralis minor Posterior capsule Levator scapulae Inferior capsule Rhomboids Infraspinatus / teres minor True muscle weakness Motor Control Deficit Latissimus dorsi / teres major Determine deficit(s) with specific manual muscle Determine corrective strategies Triceps (long head) testing Determine source of deficit Neural injury (usually more profund weakness, more rapid onset) Disuse (less profound weakness, slower more Modified from Cools et al., 2014, Br J Sports Med chronic onset ) Classifying scapular motion: the scapula dyskinesis test (SDT) (McClure et al. JAT, 2009 Tate et al, JAT, 2009) 5 repetitions: Flexion (weighted) Abduction (weighted) Rate scapular motion on each test as: rmal (N) motion: no evidence of abnormality Medial border and inferior angle relatively flat Subtle (S) dyskinesis: mild/questionable evidence of abnormality, not consistently present Obvious (O) dyskinesis: striking, clearly apparent abnormalities, evident on at least 3/5 trials Winging 1 or greater displacement of scapula from thorax Dysrhythmia Dyskinesis: Winging Movement of medial border and/or inferior angle away from the thorax, becoming more prominent during arm motion with a sulcus/gap between the scapula and the thorax: 1 is considered abnormal May be unilateral or bilateral Picture: Posterior view of winging Dyskinesis: Dysrhythmia Describes a lack of smooth scapulohumeral rhythm A hitch or a jump in the otherwise smooth motion. (Kibler, 2003) Most common pattern is early/excessive scapular elevation (shrug) Another common pattern: rapid downward rotation during lowering (dump) Picture: Example of shrug during arm raising Picture: Superior view of winging Picture: Dumping during arm lowering 5
 5# if150")







6 Winging Dysrhythmia: Dumping Scapula Dyskinesis Test 5 repetitions flexion abduction Weight (if able) 5# if150 lbs or > 3# if <150 lbs Look for Winging (1 or >) Dysrhythmia Grade rmal Subtle Obvious ** Symptom Altering Tests Modified Scapular Assistance Test Posteriorly tilt and upwardly rotate scapula (Rabin et al, 2006) JOSPT 08 Scapula Reposition Test Tate, McClure et al, JOSPT, 2008 Purpose Jobe with scapula reposition test (Tate et al, 2008) SRT Reduce pain? Increase elevation force? Overhead athletes (N=142) Symptomatic Asymptomatic Grasp scapula medial to the lateral aspect of acromion with fingers on clavicle/acjt and palm on scapular spine Forearm is obliquely angled toward inferior angle for additional support Apply moderate posterior tilting and external rotation force Passively elevate arm and repeat Jobe test Document pain (NRS 0-10) Lateral aspect of acromion 6





 Disuse (less profound weakness, slower more chronic onset ) Scapular Muscle Weakness Key Muscles Serratus Anterior Middle Trapezius Lower")
7 Results: Pain provocation and strength Pain with impingement test 1 positive impingement test in 98/142 athletes With SRT 46/98 athletes had 1pt or more in pain Strength 26-29% significant increase in strength Relevance of SRT identify those in whom scapular interventions are indicated Can also use a dynamometer for SRT Modified Scapula Assistance Test (Rabin et al, 2006) Pain rating during scaption or sagittal plane elevation /10 Stabilize the upper scapular border into mild retraction From: McClure PW, Sciascia AD, Uhl TL. Scapular Examination pp35 51 In Disorders of the Scapula and Their Role in Shoulder Injury. Kibler WB, Sciascia AD eds. Springer 2017 Is Scapular Dyskinesis Present? Visual observation during flexion and abduction with and without resistance If negative, consider testing under fatiguing conditions Are symptoms changed with manual correction? Scapular Reposition/Retraction Test Scapular Assistance Test Other corrections of scapular malposition Verbal/Manual Cueing to correct position/motion Identify tissue source of dysfunction to guide appropriate intervention Continue Shoulder Exam Scapular dysfunction unlikely Heal of other hand over inferior angle with fingers wrapped around thorax to assist upward rotation during elevation Pain rating /10 ** Soft tissue tightness: Test Specific Structures Axioscapular Muscles Glenohumeral Capsule and Muscles Pectoralis minor Posterior capsule Levator scapulae Inferior capsule Rhomboids Infraspinatus / teres minor Latissimus dorsi / teres major Triceps (long head) Modified from Cools et al., 2014, Br J Sports Med Poor Muscle Performance Readily correctable with cueing and conscious effort? True muscle weakness Motor Control Deficit Determine deficit(s) with specific manual muscle Determine corrective strategies testing Determine source of deficit Neural injury (usually more profund weakness, more rapid onset) Disuse (less profound weakness, slower more chronic onset ) Scapular Muscle Weakness Key Muscles Serratus Anterior Middle Trapezius Lower Trapezius Serratus Muscle Test Highest ms activity: Flexion or scapular plane elevation and resist shoulder elevation Resisting protraction: does not elicit as much as SA emg activity 7






 with specific manual muscle Determine corrective")

 on involved side Measure and palpate lower ribs for elevation during")
8 Strength: Serratus anterior Strength: Middle Trapezius Patient seated, no back support Arm flexed to 125 o Apply downward resistance just proximal to patient s elbow Monitor inferior angle of scapula and grade based on ability of serratus to hold upward rotation rmal strength ** Prone Horizontal abduction with thumb pointed superiorly Apply downward resistance just proximal to patient s elbow Stabilize thorax Monitor medial border of scapula, grade on ability to maintain retraction rmal strength ** HOME EXAMINATION INTERVENTION Reduced strength HOME EXAMINATION INTERVENTION Reduced strength Strength: Lower Trapezius Prone Arm elevated overhead in line with lower trapezius Apply downward resistance just proximal to patient s elbow Stabilize thorax Monitor medial border of scapula, grade on ability to maintain retraction rmal strength ** Is Scapular Dyskinesis Present? Visual observation during flexion and abduction with and without resistance If negative, consider testing under fatiguing conditions Continue Shoulder Exam Scapular dysfunction unlikely From: McClure PW, Sciascia AD, Uhl TL. Are symptoms changed with manual correction? Scapular Reposition/Retraction Test Scapular Examination pp35 51 In Scapular Assistance Test Disorders of the Scapula and Other corrections of scapular malposition Their Role in Shoulder Injury. Verbal/Manual Cueing to correct position/motion Kibler WB, Sciascia AD eds. Springer 2017 Identify tissue source of dysfunction to guide appropriate intervention Soft tissue tightness: Poor Muscle Performance Test Specific Structures Readily correctable with cueing and conscious effort? Axioscapular Muscles Glenohumeral Capsule and Muscles Pectoralis minor Posterior capsule Levator scapulae Inferior capsule Rhomboids Infraspinatus / teres minor True muscle weakness Motor Control Deficit Latissimus dorsi / teres major Determine deficit(s) with specific manual muscle Determine corrective strategies Triceps (long head) testing Determine source of deficit Neural injury (usually more profund weakness, more rapid onset) Disuse (less profound weakness, slower more Modified from Cools et al., 2014, Br J Sports Med chronic onset ) Reduced strength Pectoralis Minor length Forward shoulders/protracted scapulae rmal: posterior acromial heights = bilaterally or involved side is lower Reduced: acromion is significantly higher (>1cm) on involved side Measure and palpate lower ribs for elevation during passive shoulder flexion Reduced resting pec minor length on right Are they a problem? Solem-Bertoft anterior opening of subacromial space narrowed with protracted vs retracted position Reduced pec minor length (Borstadt, 2005) Reduced posterior tipping at 90, 120 elevation Reduced external rotation during abduction 30, 60, 90 deg Significance: reduce the subacromial space 8

 Loss of internal rotation (GIRD) May cause scapula to rotate or")

 PROM: Horizontal adduction Myers, AJSM")

 -typical measure is 95 o Restricted HOME EXAMINATION INTERVENTION rkin,1995 rmal")
 and shoulder neutral Reduced = obviously decreased (10 o or")

 with elbow flexed vs extended B A Reduced triceps length indicated by")
9 Shoulder ROM, Posterior Capsule Length Posterior Capsule (Harryman, 1990) increased posterior shoulder tightness HH sup translation & ed GH IR AROM decreased subacromial space mechanical compression of SA tissues Posterior Capsule tightness Superior migration of humerus with posterior capsule tightness (Harryman,1990 ) Loss of internal rotation (GIRD) May cause scapula to rotate or protract excessively during follow-through (add/ir) Throwing Swinging PROM: Internal Rotation 90 abduction Supine Humerus 90 abduction, elbow flexed 90 Fulcrum at olecranon process Stationary arm perpendicular to floor Align moveable arm with ulnar styloid End the movement when the acromion elevates anteriorly (beyond dashed line in top picture) PROM: Horizontal adduction Myers, AJSM 2007 Supine squeeze shoulder blades together PT stabilizes scapula into maximal retraction using thenar eminance against lateral scapular border Passively horizontally adduct humerus to end range Rate Restricted = adduction less than sagittal plane (90 o ) rmal = adduction beyond sagittal plane (90 o) -typical measure is 95 o Restricted HOME EXAMINATION INTERVENTION rkin,1995 rmal Latissimus Dorsi Length (Sahrmann, 2002) Shoulder flexion hips extended (lat on slack) shoulder neutral vs hips flexed (back flat) and shoulder neutral Reduced = obviously decreased (10 o or more) shoulder flexion with the hips flexed, back flat, shoulder ER rmal = grossly equal or greater flexion A B Reduced latissimus length indicated by obviously decreased flexion in B compared to A Triceps Length rmal: flexion ROM is same with elbow flexed and extended Reduced: flexion ROM is less ( 10 o ) with elbow flexed vs extended B A Reduced triceps length indicated by obviously decreased flexion in B compared to A 9
 Flex +/- wt Abd +/- wt SRT (Scap Reposition Test) Empty can w/wo scap")
 Use if elevation is painful Assist scap upward rot during painful elevation movement Strength Assessment Mid trap Low trap Serr Ant Post Capsule")




10 Thoracic Intervertebral Mobility: Spring Testing over spinous processes Maitland, 2000, Cleland et al, 2007 Based on examiners perception of mobility at a level relative to those above and below and examiner s experience and perception of normal Hypomobile Hypermobile Practice: Examination SDT (Scap Dyskinesis Test) Flex +/- wt Abd +/- wt SRT (Scap Reposition Test) Empty can w/wo scap stabilization? Pain reduced? Obvious strength increase SAT (Scap Assist Test) Use if elevation is painful Assist scap upward rot during painful elevation movement Strength Assessment Mid trap Low trap Serr Ant Post Capsule Tightness IR at 90 degrees Horiz Adduction with scap blocked Pec minor tight? Coracoid ht supine, palpate ribs during arm elevation Shdr depressed standing? Latissimus Dorsi tight? Triceps tight? Treatment If TIGHT => Stretch Scapula mobs Pec minor Post capsule Thoracic spine mobilization/thrust IF WEAK => Re educate proper motor control strengthen if true weakness Tape / Brace / NMES (adjunct) Activity Modification Is Scapular Dyskinesis Present? Visual observation during flexion and abduction with and without resistance If negative, consider testing under fatiguing conditions Continue Shoulder Exam Scapular dysfunction unlikely From: McClure PW, Sciascia AD, Uhl TL. Are symptoms changed with manual correction? Scapular Reposition/Retraction Test Scapular Examination pp35 51 In Scapular Assistance Test Disorders of the Scapula and Other corrections of scapular malposition Their Role in Shoulder Injury. Verbal/Manual Cueing to correct position/motion Kibler WB, Sciascia AD eds. Springer 2017 Identify tissue source of dysfunction to guide appropriate intervention Soft tissue tightness: Poor Muscle Performance Test Specific Structures Readily correctable with cueing and conscious effort? Axioscapular Muscles Glenohumeral Capsule and Muscles Pectoralis minor Posterior capsule Levator scapulae Inferior capsule Rhomboids Infraspinatus / teres minor True muscle weakness Motor Control Deficit Latissimus dorsi / teres major Determine deficit(s) with specific manual muscle Determine corrective strategies Triceps (long head) testing Determine source of deficit Neural injury (usually more profund weakness, more rapid onset) Disuse (less profound weakness, slower more Modified from Cools et al., 2014, Br J Sports Med chronic onset ) Pec Minor Stretching Posterior Capsule stretching Passive Posterior glides supine Posterior/inferior glides sidelying arm behind back Horizontal adduction (block scapula) 10








")
11 Stretching for Post Shoulder Tightness Lack of evidence related to interventions for tightness stretching methods Horizontal adduction Horizontal adduction with scapula stabilized by PT Wilk et al, 2002 AJSM Internal Rotation Stretch Wilk et al, 2002 AJSM Sidelying IR with stabilized scapula Kibler AJSM 2003 Sleeper stretch vs horizontal adduction (McClure et al, JOSPT, 2009) Cross-Body Stretch Using your hand, grab your arm just above the elbow, gently pull your arm across your body in front of you until you feel a stretch. 5 x 30 seconds daily and log performance Sleeper Stretch Lie on your side with your arm out to the side, elbow bent. Use your arm to slowly push your forearm toward the floor/bed until you feel a stretch. 5 x 30 seconds daily and log performance < NS NS paired t-tests performed by group and side * All changes significant (p <.01) except SS control side ST Mobilization From: McClure PW, Sciascia AD, Uhl TL. Scapular Examination pp35 51 In Disorders of the Scapula and Their Role in Shoulder Injury. Kibler WB, Sciascia AD eds. Springer 2017 Is Scapular Dyskinesis Present? Visual observation during flexion and abduction with and without resistance If negative, consider testing under fatiguing conditions Are symptoms changed with manual correction? Scapular Reposition/Retraction Test Scapular Assistance Test Other corrections of scapular malposition Verbal/Manual Cueing to correct position/motion Continue Shoulder Exam Scapular dysfunction unlikely Identify tissue source of dysfunction to guide appropriate intervention Soft tissue tightness: Test Specific Structures Poor Muscle Performance Superior/Inferior Protraction/Retraction Distraction Axioscapular Muscles Glenohumeral Capsule and Muscles Pectoralis minor Posterior capsule Levator scapulae Inferior capsule Rhomboids Infraspinatus / teres minor Latissimus dorsi / teres major Triceps (long head) Modified from Cools et al., 2014, Br J Sports Med Readily correctable with cueing and conscious effort? True muscle weakness Motor Control Deficit Determine deficit(s) with specific manual muscle Determine corrective strategies testing Determine source of deficit Neural injury (usually more profund weakness, more rapid onset) Disuse (less profound weakness, slower more chronic onset ) 11




















12 Scapular Exercise: EARLY PHASE Scapular Exercise: MIDDLE PHASE Scapular Exercise: LATE PHASE Surface EMG analysis of Ex for trapezius and serratus anterior (Ekstrom, 2004) N=30 healthy subjects Which exercises elicit greatest emg? Middle trap: overhead arm raise in line w/l trap & horizontal ext w/ ER ( T and Y ) Lower trap: overhead arm raise in line w/l trap Alternate: prone ER w/ 90 abd???indications Serratus anterior: scaption > 120 & combined flexion, horiz. flexion and ER Using E-stim for NM Re-education T 12






 Taping/bracing S3")
13 Y Flexion, horizontal flexion, external rotation Based on Ekstrom 2003 Relative Balance of Serratus Anterior and Upper Trapezius Muscle Activity During Push-up Exercises Muscle Activity During Push-up Exercises Plus maneuver: palsy vs motor control deficit Scapular Exercise Principles Quality vs Quantity GH range limited to where scap control is achieved and maintained CKC or OKC? Trunk motion to facilitate scap motion Multiple planes (safer => more challenging) Taping/bracing S3 Brace Alignmed 13






14 Scapular Taping Treatment Summary & Practice Stretching Post capsule PecMinor C-spine / T-spine Strengthening Motor control vs strength SA, LT Core and whole body patterns Cuff strengthening also effects scapula Taping / Bracing Adjunct to facilitate painfree exercise Thank you Phil McClure PT, PhD, FAPTA Professor, Arcadia University mcclurep@arcadia.edu 14
Describe methods to evaluate for scapular. Perform a scapular dyskinesis examination. With humeral elevation, the scapula:
 Describe methods to evaluate for scapular dyskinesis Perform a scapular dyskinesis examination Lori Michener, PhD, PT, ATC Virginia Commonwealth University Richmond, VA Ant / Post Tilting Internal / External
Describe methods to evaluate for scapular dyskinesis Perform a scapular dyskinesis examination Lori Michener, PhD, PT, ATC Virginia Commonwealth University Richmond, VA Ant / Post Tilting Internal / External
Returning the Shoulder Back to Optimal Function. Scapula. Clavicle. Humerus. Bones of the Shoulder (Osteology) Joints of the Shoulder (Arthrology)
 Joints of the Shoulder (Arthrology)") Returning the Shoulder Back to Optimal Function Sternum Clavicle Ribs Scapula Humerus Bones of the Shoulder (Osteology) By Rick Kaselj Clavicle Scapula Medial Left Anterior Clavicle Inferior View 20 degree
Returning the Shoulder Back to Optimal Function Sternum Clavicle Ribs Scapula Humerus Bones of the Shoulder (Osteology) By Rick Kaselj Clavicle Scapula Medial Left Anterior Clavicle Inferior View 20 degree
IMPINGEMENT-TESTSTESTS
 «thinking about.» DIFFERENTIAL DIAGNOSIS: Looking for the causes of Which special tests do you use in your shoulder examination? Ann Cools, PT, PhD Ghent University - Belgium Dept of Rehabilitation Sciences
«thinking about.» DIFFERENTIAL DIAGNOSIS: Looking for the causes of Which special tests do you use in your shoulder examination? Ann Cools, PT, PhD Ghent University - Belgium Dept of Rehabilitation Sciences
Lab Workbook. ANATOMY Manual Muscle Testing Lower Trapezius Patient: prone
 ANATOMY Manual Muscle Testing Lower Trapezius Patient: prone Lab Workbook Fixation: place on hand below the scapula on the opposite side Test: adduction and depression of the scapula with lateral rotation
ANATOMY Manual Muscle Testing Lower Trapezius Patient: prone Lab Workbook Fixation: place on hand below the scapula on the opposite side Test: adduction and depression of the scapula with lateral rotation
Joint G*H. Joint S*C. Joint A*C. Labrum. Humerus. Sternum. Scapula. Clavicle. Thorax. Articulation. Scapulo- Thoracic
 A*C Joint Scapulo- Thoracic Articulation Thorax Sternum Clavicle Scapula Humerus S*C Joint G*H Joint Labrum AC Ligaments SC Ligaments SC JOINT AC Coracoacromial GH GH Ligament Complex Coracoclavicular
A*C Joint Scapulo- Thoracic Articulation Thorax Sternum Clavicle Scapula Humerus S*C Joint G*H Joint Labrum AC Ligaments SC Ligaments SC JOINT AC Coracoacromial GH GH Ligament Complex Coracoclavicular
11/6/2013. Keely Behning, PT, SCS, ATC MNPTA Fall Conference November 16, 2013
 Keely Behning, PT, SCS, ATC MNPTA Fall Conference November 16, 2013 Upon completion of this course, attendees should be able to: Understand pertinent anatomy and biomechanics as they relate to specific
Keely Behning, PT, SCS, ATC MNPTA Fall Conference November 16, 2013 Upon completion of this course, attendees should be able to: Understand pertinent anatomy and biomechanics as they relate to specific
REMINDER. Obtain medical clearance and physician s release prior to beginning an exercise program for clients with medical or orthopedic concerns
 Understanding Shoulder Dysfunction REMINDER Obtain medical clearance and physician s release prior to beginning an exercise program for clients with medical or orthopedic concerns What is a healthy shoulder?
Understanding Shoulder Dysfunction REMINDER Obtain medical clearance and physician s release prior to beginning an exercise program for clients with medical or orthopedic concerns What is a healthy shoulder?
Physical Examination of the Shoulder
 General setup Patient will be examined in both the seated and supine position so exam table needed 360 degree access to patient Expose neck and both shoulders (for comparison); female in gown or sports
General setup Patient will be examined in both the seated and supine position so exam table needed 360 degree access to patient Expose neck and both shoulders (for comparison); female in gown or sports
DIFFERENTIAL DIAGNOSIS: Looking for the causes of impingement
 DIFFERENTIAL DIAGNOSIS: Looking for the causes of Ann Cools, PT, PhD Ghent University - Belgium Dept of Rehabilitation Sciences & Physiotherapy Ann.Cools@UGent.be «thinking about.» Which special tests
DIFFERENTIAL DIAGNOSIS: Looking for the causes of Ann Cools, PT, PhD Ghent University - Belgium Dept of Rehabilitation Sciences & Physiotherapy Ann.Cools@UGent.be «thinking about.» Which special tests
SHOULDER PAIN LESSONS FROM THE SPORTS FIELD MOVEMENT RESTRICTIONS. Steve McCaig
 SHOULDER PAIN LESSONS FROM THE SPORTS FIELD MOVEMENT RESTRICTIONS 1 Steve McCaig Senior Physiotherapist England Development Programme, ECB, Loughborough, United Kingdom Throwing High forces upper limb
SHOULDER PAIN LESSONS FROM THE SPORTS FIELD MOVEMENT RESTRICTIONS 1 Steve McCaig Senior Physiotherapist England Development Programme, ECB, Loughborough, United Kingdom Throwing High forces upper limb
WEEKEND 2 Shoulder. Shoulder Active Range of Motion Assessment
 Virginia Orthopedic Manual Physical Therapy Institute - 2016 Technique Manual WEEKEND 2 Shoulder Shoulder Active Range of Motion Assessment - Patient Positioning: Standing, appropriately undressed so that
Virginia Orthopedic Manual Physical Therapy Institute - 2016 Technique Manual WEEKEND 2 Shoulder Shoulder Active Range of Motion Assessment - Patient Positioning: Standing, appropriately undressed so that
Structure and Function of the Bones and Joints of the Shoulder Girdle
 Structure and Function of the Bones and Joints of the Shoulder Girdle LEARNING OBJECTIVES: At the end of this laboratory exercise the student will be able to: Palpate the important skeletal landmarks of
Structure and Function of the Bones and Joints of the Shoulder Girdle LEARNING OBJECTIVES: At the end of this laboratory exercise the student will be able to: Palpate the important skeletal landmarks of
REMINDER. an exercise program. Senior Fitness Obtain medical clearance and physician s release prior to beginning
 Functional Forever: Exercise for Independent Living REMINDER Obtain medical clearance and physician s release prior to beginning an exercise program for clients with medical or orthopedic concerns. What
Functional Forever: Exercise for Independent Living REMINDER Obtain medical clearance and physician s release prior to beginning an exercise program for clients with medical or orthopedic concerns. What
Shoulder: Clinical Anatomy, Kinematics & Biomechanics
 Shoulder: Clinical Anatomy, Kinematics & Biomechanics Dr. Alex K C Poon Department of Orthopaedics & Traumatology Pamela Youde Nethersole Eastern Hospital Clinical Anatomy the application of anatomy to
Shoulder: Clinical Anatomy, Kinematics & Biomechanics Dr. Alex K C Poon Department of Orthopaedics & Traumatology Pamela Youde Nethersole Eastern Hospital Clinical Anatomy the application of anatomy to
SHOULDER REHABILITATION PART II
 SHOULDER REHABILITATION PART II Ann Cools, PT, PhD Ghent University - Belgium Dept of Rehabilitation Sciences & Physiotherapy Ann.Cools@UGent.be Shoulder rehab course level I Shoulder pathology and clinical
SHOULDER REHABILITATION PART II Ann Cools, PT, PhD Ghent University - Belgium Dept of Rehabilitation Sciences & Physiotherapy Ann.Cools@UGent.be Shoulder rehab course level I Shoulder pathology and clinical
Secrets and Staples of Training the Athletic Shoulder
 Secrets and Staples of Training the Athletic Shoulder Eric Beard Corrective Exercise Specialist Athletic Performance Enhancement Specialist EricBeard.com AthleticShoulder.com Presentation Overview Rationale
Secrets and Staples of Training the Athletic Shoulder Eric Beard Corrective Exercise Specialist Athletic Performance Enhancement Specialist EricBeard.com AthleticShoulder.com Presentation Overview Rationale
MLT Muscle(s) Patient Position Therapist position Stabilization Limb Position Picture Put biceps on slack by bending elbow.
 Patient Position Therapist position Stabilization Limb Position Picture Put biceps on slack by bending elbow.") MLT Muscle(s) Patient Position Therapist position Stabilization Limb Position Picture Put biceps on slack by bending elbow. Pectoralis Minor Supine, arm at side, elbows extended, supinated Head of Table
MLT Muscle(s) Patient Position Therapist position Stabilization Limb Position Picture Put biceps on slack by bending elbow. Pectoralis Minor Supine, arm at side, elbows extended, supinated Head of Table
Scapular Dyskinesis. Orthopaedic Update 2018 April 15, Peter Tang, MD, MPH, FAOA
 Scapular Dyskinesis Orthopaedic Update 2018 April 15, 2018 Peter Tang, MD, MPH, FAOA Director Center for Brachial Plexus and Nerve Injury Program Director Hand, Upper Extremity & Microvascular Surgery
Scapular Dyskinesis Orthopaedic Update 2018 April 15, 2018 Peter Tang, MD, MPH, FAOA Director Center for Brachial Plexus and Nerve Injury Program Director Hand, Upper Extremity & Microvascular Surgery
The Shoulder. Anatomy and Injuries PSK 4U Unit 3, Day 4
 The Shoulder Anatomy and Injuries PSK 4U Unit 3, Day 4 Shoulder Girdle Shoulder Complex is the most mobile joint in the body. Scapula Clavicle Sternum Humerus Rib cage/thorax Shoulder Girdle It also includes
The Shoulder Anatomy and Injuries PSK 4U Unit 3, Day 4 Shoulder Girdle Shoulder Complex is the most mobile joint in the body. Scapula Clavicle Sternum Humerus Rib cage/thorax Shoulder Girdle It also includes
Shoulder Joint Examination. Shoulder Joint Examination. Inspection. Inspection Palpation Movement. Look Feel Move
 Shoulder Joint Examination History Cuff Examination Instability Examination AC Joint Examination Biceps Tendon Examination Superior Labrum Examination Shoulder Joint Examination Inspection Palpation Movement
Shoulder Joint Examination History Cuff Examination Instability Examination AC Joint Examination Biceps Tendon Examination Superior Labrum Examination Shoulder Joint Examination Inspection Palpation Movement
Shoulder Impingement Rehabilitation Recommendations
 Shoulder Impingement Rehabilitation Recommendations The following protocol can be utilized for conservative care of shoulder impingement as well as post- operative subacromial decompression (SAD) surgery.
Shoulder Impingement Rehabilitation Recommendations The following protocol can be utilized for conservative care of shoulder impingement as well as post- operative subacromial decompression (SAD) surgery.
Throwing Athlete Rehabilitation. Brett Schulz LAT/CMSS Sport and Spine Physical Therapy
 Throwing Athlete Rehabilitation Brett Schulz LAT/CMSS Sport and Spine Physical Therapy Disclosure No conflicts to disclose Throwing Athlete Dilemma The shoulder must have enough range of motion to allow
Throwing Athlete Rehabilitation Brett Schulz LAT/CMSS Sport and Spine Physical Therapy Disclosure No conflicts to disclose Throwing Athlete Dilemma The shoulder must have enough range of motion to allow
Continuing Education: Shoulder Stability
 Continuing Education: Shoulder Stability Anatomy & Kinesiology: The GHJ consists of the articulation of three bones: the scapula, clavicle and humerus. The scapula has three protrusions: the coracoid,
Continuing Education: Shoulder Stability Anatomy & Kinesiology: The GHJ consists of the articulation of three bones: the scapula, clavicle and humerus. The scapula has three protrusions: the coracoid,
Rehabilitation Guidelines for Labral/Bankert Repair
 Rehabilitation Guidelines for Labral/Bankert Repair The true shoulder joint is called the glenohumeral joint and consists humeral head and the glenoid. It is a ball and socket joint. Anatomy of the Shoulder
Rehabilitation Guidelines for Labral/Bankert Repair The true shoulder joint is called the glenohumeral joint and consists humeral head and the glenoid. It is a ball and socket joint. Anatomy of the Shoulder
Rehabilitation of Overhead Shoulder Injuries
 Rehabilitation of Overhead Shoulder Injuries 16 th Annual Primary Care Orthopaedic & Sports Medicine Symposium January 29, 2016 Jeremy Sherman, PT, MPT Disclosures No financial disclosures to note. Jeremy
Rehabilitation of Overhead Shoulder Injuries 16 th Annual Primary Care Orthopaedic & Sports Medicine Symposium January 29, 2016 Jeremy Sherman, PT, MPT Disclosures No financial disclosures to note. Jeremy
RN(EC) ENC(C) GNC(C) MN ACNP *** MECHANISM OF INJURY.. MOST IMPORTANT ***
 ENC(C) GNC(C) MN ACNP *** MECHANISM OF INJURY.. MOST IMPORTANT ***") HISTORY *** MECHANISM OF INJURY.. MOST IMPORTANT *** Age - Certain conditions are more prevalent in particular age groups (i.e. Full rotator cuff tears are more common over the age of 45, traumatic injuries
HISTORY *** MECHANISM OF INJURY.. MOST IMPORTANT *** Age - Certain conditions are more prevalent in particular age groups (i.e. Full rotator cuff tears are more common over the age of 45, traumatic injuries
Joint Range of Motion Assessment Techniques. Presentation Created by Ken Baldwin, M.Ed Copyright
 Joint Range of Motion Assessment Techniques Presentation Created by Ken Baldwin, M.Ed Copyright 2001-2006 Objectives Understand how joint range of motion & goniometric assessment is an important component
Joint Range of Motion Assessment Techniques Presentation Created by Ken Baldwin, M.Ed Copyright 2001-2006 Objectives Understand how joint range of motion & goniometric assessment is an important component
Disclosures. Training for the Scapulothoracic Joint and Thoracic Spine. Scapular Muscles Stabilization & Rotation 9/7/2018
 Disclosures Training for the Scapulothoracic Joint and Thoracic Spine mtrigger Litecure Russ Paine, PT Director -UT Physicians Sportsmedicine Rehabilitation Houston, Texas 21 academic institutions 14 hospitals
Disclosures Training for the Scapulothoracic Joint and Thoracic Spine mtrigger Litecure Russ Paine, PT Director -UT Physicians Sportsmedicine Rehabilitation Houston, Texas 21 academic institutions 14 hospitals
Evaluation & Treatment of the Scapula in Athletes: How Important is the Scapula Kevin E Wilk, PT, DPT,FAPTA
 Evaluation & Treatment of the Scapula in Athletes: How Important is the Scapula Kevin E Wilk, PT, DPT,FAPTA Kevin E Wilk, PT, DPT,FAPTA 2016 Baseball Sports Medicine Conference Faculty Disclosure: Theralase
Evaluation & Treatment of the Scapula in Athletes: How Important is the Scapula Kevin E Wilk, PT, DPT,FAPTA Kevin E Wilk, PT, DPT,FAPTA 2016 Baseball Sports Medicine Conference Faculty Disclosure: Theralase
Background. Background. Movement Examination. Movement Examination. MSI Scapular Diagnoses Lecture October 2016
 MSI Scapular Diagnoses Lecture October 2016 Diagnosis and Treatment of Movement System Impairment Syndromes of the Shoulder: Scapular Diagnoses Shirley Sahrmann, PhD, PT, FAPTA and Associates Developed
MSI Scapular Diagnoses Lecture October 2016 Diagnosis and Treatment of Movement System Impairment Syndromes of the Shoulder: Scapular Diagnoses Shirley Sahrmann, PhD, PT, FAPTA and Associates Developed
Active-Assisted Stretches
 1 Active-Assisted Stretches Adequate flexibility is fundamental to a functional musculoskeletal system which represents the foundation of movement efficiency. Therefore a commitment toward appropriate
1 Active-Assisted Stretches Adequate flexibility is fundamental to a functional musculoskeletal system which represents the foundation of movement efficiency. Therefore a commitment toward appropriate
Anterior Stabilization of the Shoulder: Distal Tibial Allograft
 Anterior Stabilization of the Shoulder: Distal Tibial Allograft Name: Diagnosis: Date: Date of Surgery: Phase I Immediate Post Surgical Phase (approximately Weeks 1-3) Minimize shoulder pain and inflammatory
Anterior Stabilization of the Shoulder: Distal Tibial Allograft Name: Diagnosis: Date: Date of Surgery: Phase I Immediate Post Surgical Phase (approximately Weeks 1-3) Minimize shoulder pain and inflammatory
Phase I : Immediate Postoperative Phase- Protected Motion. (0-2 Weeks)
") Phase I : Immediate Postoperative Phase- Protected Motion (0-2 Weeks) Appointments Progression Criteria 2 weeks after surgery Rehabilitation appointments begin within 7-10 days of surgery, continue 1-2
Phase I : Immediate Postoperative Phase- Protected Motion (0-2 Weeks) Appointments Progression Criteria 2 weeks after surgery Rehabilitation appointments begin within 7-10 days of surgery, continue 1-2
Addressing Core and Balance Deficits to Maximize Return to Sport in Overhead Athletes
 Addressing Core and Balance Deficits to Maximize Return to Sport in Overhead Athletes Meg Jacobs P.T. Momentum Physical Therapy and Sports Rehab Hands on care for faster results www.wegetyouhealthy.com
Addressing Core and Balance Deficits to Maximize Return to Sport in Overhead Athletes Meg Jacobs P.T. Momentum Physical Therapy and Sports Rehab Hands on care for faster results www.wegetyouhealthy.com
REHABILITATION GUIDELINES FOR ANTERIOR SHOULDER RECONSTRUCTION WITH BANKART REPAIR
 REHABILITATION GUIDELINES FOR ANTERIOR SHOULDER RECONSTRUCTION WITH BANKART REPAIR The rehabilitation guidelines are presented in a criterion based progression. General time frames are given for reference
REHABILITATION GUIDELINES FOR ANTERIOR SHOULDER RECONSTRUCTION WITH BANKART REPAIR The rehabilitation guidelines are presented in a criterion based progression. General time frames are given for reference
S3 EFFECTIVE FOR SHOULDER PATHOLOGIES -Dr. Steven Smith
 S3 EFFECTIVE FOR SHOULDER PATHOLOGIES -Dr. Steven Smith Introduction: Scapular function and its role in shoulder biomechanics has gained increased notoriety in the pathogenesis of shoulder dysfunction
S3 EFFECTIVE FOR SHOULDER PATHOLOGIES -Dr. Steven Smith Introduction: Scapular function and its role in shoulder biomechanics has gained increased notoriety in the pathogenesis of shoulder dysfunction
REHABILITATION GUIDELINES FOR ARTHROSCOPIC CAPSULAR SHIFT
 REHABILITATION GUIDELINES FOR ARTHROSCOPIC CAPSULAR SHIFT The rehabilitation guidelines are presented in a criterion based progression. General time frames are given for reference to the average, but individual
REHABILITATION GUIDELINES FOR ARTHROSCOPIC CAPSULAR SHIFT The rehabilitation guidelines are presented in a criterion based progression. General time frames are given for reference to the average, but individual
INSTRUCTION MANUAL FOR THE FLEXTEND AC Exercise System for The Acromioclavicular (AC) / Shoulder Joint
 / Shoulder Joint") INSTRUCTION MANUAL FOR THE FLEXTEND AC Exercise System for The Acromioclavicular (AC) / Shoulder Joint FLEXTEND -AC: Congratulations! You have chosen to use the FLEXTEND -AC Upper Extremity Training System,
INSTRUCTION MANUAL FOR THE FLEXTEND AC Exercise System for The Acromioclavicular (AC) / Shoulder Joint FLEXTEND -AC: Congratulations! You have chosen to use the FLEXTEND -AC Upper Extremity Training System,
ORTHOPEDIC AND SPORTS MEDICINE CENTER
 ORTHOPEDIC AND SPORTS MEDICINE CENTER SPORTS MEDICINE DIVISION COMBINED REHAB PROTOCOLS AAMC ORTHOPEDIC AND SPORTS MEDICINE SPECIALISTS Office: (410) 268-8862 Fax: (410) 268-0380 Rotator Cuff Repair Rehab
ORTHOPEDIC AND SPORTS MEDICINE CENTER SPORTS MEDICINE DIVISION COMBINED REHAB PROTOCOLS AAMC ORTHOPEDIC AND SPORTS MEDICINE SPECIALISTS Office: (410) 268-8862 Fax: (410) 268-0380 Rotator Cuff Repair Rehab
Nonoperative Treatment For Rotator Cuff Tendinitis/ Partial Thickness Tear Dr. Trueblood
 Nonoperative Treatment For Rotator Cuff Tendinitis/ Partial Thickness Tear Dr. Trueblood Relieving Pain Patients who present with SIS will have shoulder pain that is exacerbated with overhead activities.
Nonoperative Treatment For Rotator Cuff Tendinitis/ Partial Thickness Tear Dr. Trueblood Relieving Pain Patients who present with SIS will have shoulder pain that is exacerbated with overhead activities.
Core deconditioning Smoking Outpatient Phase 1 ROM Other
 whereby the ball does not stay properly centered in the shoulder socket during shoulder movement. This condition may be associated with impingement of the rotator cuff on the acromion bone and coracoacromial
whereby the ball does not stay properly centered in the shoulder socket during shoulder movement. This condition may be associated with impingement of the rotator cuff on the acromion bone and coracoacromial
PHASE I (Begin PT 3-5 days post-op) DOS:
 DOS:") REHABILITATION GUIDELINES FOR POSTERIOR SHOULDER RECONSTRUCTION +/- LABRAL REPAIRS The rehabilitation guidelines are presented in a criterion based progression. General time frames are given for reference
REHABILITATION GUIDELINES FOR POSTERIOR SHOULDER RECONSTRUCTION +/- LABRAL REPAIRS The rehabilitation guidelines are presented in a criterion based progression. General time frames are given for reference
Shoulder Biomechanics
 Shoulder Biomechanics Lecture originally developed by Bryan Morrison, Ph.D. candidate Arizona State University Fall 2000 1 Outline Anatomy Biomechanics Problems 2 Shoulder Complex Greatest Greatest Predisposition
Shoulder Biomechanics Lecture originally developed by Bryan Morrison, Ph.D. candidate Arizona State University Fall 2000 1 Outline Anatomy Biomechanics Problems 2 Shoulder Complex Greatest Greatest Predisposition
Scapular Assessment & Dyskinesis: What s Relevant?
 Scapular Assessment & Dyskinesis: What s Relevant? Jesse Awenus PT, MSc.PT, Dip.Manip.PT, FCAMPT, Cert. DN Registered Physiotherapist Director of Rehabilitation at Synergy Sports Medicine & Rehabilitation
Scapular Assessment & Dyskinesis: What s Relevant? Jesse Awenus PT, MSc.PT, Dip.Manip.PT, FCAMPT, Cert. DN Registered Physiotherapist Director of Rehabilitation at Synergy Sports Medicine & Rehabilitation
Overuse Injuries. Overuse injury defined. Overuse Injuries
 Overuse Injuries Lisa DeStefano, DO Associate Professor and Chair Department of Osteopathic Manipulative Medicine College of Osteopathic Medicine Michigan State University Overuse injury defined Overuse
Overuse Injuries Lisa DeStefano, DO Associate Professor and Chair Department of Osteopathic Manipulative Medicine College of Osteopathic Medicine Michigan State University Overuse injury defined Overuse
Conservative Massive Rotator Cuff Tear Protocol
 SPORTS & ORTHOPAEDIC SPECIALISTS Conservative Massive Rotator Cuff Tear Protocol 3-4 visits over 4-6 weeks Emphasis is on AAROM and a high repetition, low weight free weight program Emphasize improved
SPORTS & ORTHOPAEDIC SPECIALISTS Conservative Massive Rotator Cuff Tear Protocol 3-4 visits over 4-6 weeks Emphasis is on AAROM and a high repetition, low weight free weight program Emphasize improved
SHOULDER TO SHOULDER The Range Of Possibilities
 mouse click to advance the slides SHOULDER TO SHOULDER The Range Of Possibilities HATHA YOGA Hatha yoga asanas Take the shoulders through every possible range of motion in both weight-bearing and relatively
mouse click to advance the slides SHOULDER TO SHOULDER The Range Of Possibilities HATHA YOGA Hatha yoga asanas Take the shoulders through every possible range of motion in both weight-bearing and relatively
[12]. 100 subjects. The sampling method used was purposive sampling. Fifty gymers and fifty matched non gymers were
![[12]. 100 subjects. The sampling method used was purposive sampling. Fifty gymers and fifty matched non gymers were](/thumbs/90/103918912.jpg "[12]. 100 subjects. The sampling method used was purposive sampling. Fifty gymers and fifty matched non gymers were") To Study the Prevalence of Scapular Dyskinesia in Gymers and Non Gymers Divya Khare 1, Supriya Vinay Deshmukh 2 Associate Professor, Physiotherapy Department, Ayushman College, Bhopal [Madhya Pradesh],
To Study the Prevalence of Scapular Dyskinesia in Gymers and Non Gymers Divya Khare 1, Supriya Vinay Deshmukh 2 Associate Professor, Physiotherapy Department, Ayushman College, Bhopal [Madhya Pradesh],
Conservative Posterior Capsular Instability Protocol
 SPORTS & ORTHOPAEDIC SPECIALISTS Conservative Posterior Capsular Instability Protocol 4-6 visits over 6 weeks Primary instability often experiences secondary impingement. Therefore, to treat posterior
SPORTS & ORTHOPAEDIC SPECIALISTS Conservative Posterior Capsular Instability Protocol 4-6 visits over 6 weeks Primary instability often experiences secondary impingement. Therefore, to treat posterior
D: Doorway Stretch E: Towel Stretch for Pectoralis Minor Blackburn Exercises: 6 Positions A: Prone Horizontal Abduction (Neutral)
") D: Doorway Stretch Bring your shoulder into a horizontal position out to your side (abduction) and flex your elbow 90û Place your elbow against the edge of a doorway Lead forward and downwards with your
D: Doorway Stretch Bring your shoulder into a horizontal position out to your side (abduction) and flex your elbow 90û Place your elbow against the edge of a doorway Lead forward and downwards with your
Clinical Assessment of Scapular Motion
 Clinical Assessment of Scapular Motion BRADY L. TRIPP, MEd, ATC, and TIM L. UHL, PhD, ATC, PT University of Kentucky Key Points Many athletic therapists appreciate the role that scapular function plays
Clinical Assessment of Scapular Motion BRADY L. TRIPP, MEd, ATC, and TIM L. UHL, PhD, ATC, PT University of Kentucky Key Points Many athletic therapists appreciate the role that scapular function plays
CLINICAL EXAMINATION OF THE SHOULDER JOINT 대한신경근골격연구회 분당제생병원재활의학과 박준성
 CLINICAL EXAMINATION OF THE SHOULDER JOINT 대한신경근골격연구회 분당제생병원재활의학과 박준성 Clinical Examination of the Shoulder Good history, full clinical examination Detailed knowledge of the anatomy solve the majority of
CLINICAL EXAMINATION OF THE SHOULDER JOINT 대한신경근골격연구회 분당제생병원재활의학과 박준성 Clinical Examination of the Shoulder Good history, full clinical examination Detailed knowledge of the anatomy solve the majority of
Theodore B. Shybut, M.D.
 Theodore B. Shybut, M.D. Orthopedics and Sports Medicine 7200 Cambridge St. #10A Houston, Texas 77030 Non-operative Shoulder Rehabilitation Protocol Basic shoulder program for: o Scapular Dyskinesis (proximally
Theodore B. Shybut, M.D. Orthopedics and Sports Medicine 7200 Cambridge St. #10A Houston, Texas 77030 Non-operative Shoulder Rehabilitation Protocol Basic shoulder program for: o Scapular Dyskinesis (proximally
Anterior Stabilization of the Shoulder: Latarjet Protocol
 Robert K. Fullick, MD 6400 Fannin Street, Suite 1700 Houston, Texas 77030 Ph.: 713-486-7543 / Fx.: 713-486-5549 Anterior Stabilization of the Shoulder: Latarjet Protocol The intent of this protocol is
Robert K. Fullick, MD 6400 Fannin Street, Suite 1700 Houston, Texas 77030 Ph.: 713-486-7543 / Fx.: 713-486-5549 Anterior Stabilization of the Shoulder: Latarjet Protocol The intent of this protocol is
Rotator Cuff Repair Protocol for tear involving Subscapularis Tendon with or without Pectoralis Major Tendon Transfer
 Rotator Cuff Repair Protocol for tear involving Subscapularis Tendon with or without Pectoralis Major Tendon Transfer D. WATTS, MD Precautions: BASIS Tendon healing back to bone is a slow process that
Rotator Cuff Repair Protocol for tear involving Subscapularis Tendon with or without Pectoralis Major Tendon Transfer D. WATTS, MD Precautions: BASIS Tendon healing back to bone is a slow process that
Anatomical Considerations/ Pathophysiology The shoulder is the most mobile joint in the body. : Three bones:
 Introduction Musculoskeletal training is generally underrepresented in medical training and residency curriculums. There is a general deficit in musculoskeletal knowledge amongst current medical students,
Introduction Musculoskeletal training is generally underrepresented in medical training and residency curriculums. There is a general deficit in musculoskeletal knowledge amongst current medical students,
Latarjet Repair Rehabilitation Protocol
 General Notes: As tolerated should be understood to include with safety for the reconstruction/repair; a sudden increase in pain, swelling, or other undesirable factors are indicators that you are doing
General Notes: As tolerated should be understood to include with safety for the reconstruction/repair; a sudden increase in pain, swelling, or other undesirable factors are indicators that you are doing
REHABILITATION GUIDELINES FOR SUBSCAPULARIS (+/- SUBACROMIAL DECOMPRESSION) Dr. Carson
 Dr. Carson") REHABILITATION GUIDELINES FOR SUBSCAPULARIS (+/- SUBACROMIAL DECOMPRESSION) Dr. Carson The rehabilitation guidelines are presented in a criterion based progression. General time frames are given for reference
REHABILITATION GUIDELINES FOR SUBSCAPULARIS (+/- SUBACROMIAL DECOMPRESSION) Dr. Carson The rehabilitation guidelines are presented in a criterion based progression. General time frames are given for reference
Throwing Injuries and Prevention: The Physical Therapy Perspective
 Throwing Injuries and Prevention: The Physical Therapy Perspective Andrew M Jordan, PT, DPT, OCS Staff Physical Therapist, Cayuga Medical Center Physical Therapy and Sports Medicine ajordan@cayugamed.org
Throwing Injuries and Prevention: The Physical Therapy Perspective Andrew M Jordan, PT, DPT, OCS Staff Physical Therapist, Cayuga Medical Center Physical Therapy and Sports Medicine ajordan@cayugamed.org
RHS 221 Manual Muscle Testing Theory 1 hour practical 2 hours Dr. Ali Aldali, MS, PT Tel# Department of Physical Therapy King Saud University
 1 RHS 221 Manual Muscle Testing Theory 1 hour practical 2 hours Dr. Ali Aldali, MS, PT Tel# 4693601 Department of Physical Therapy King Saud University 2 The scapulae lie against the thorax approximately
1 RHS 221 Manual Muscle Testing Theory 1 hour practical 2 hours Dr. Ali Aldali, MS, PT Tel# 4693601 Department of Physical Therapy King Saud University 2 The scapulae lie against the thorax approximately
Current concepts: scapular dyskinesis
 Current concepts: scapular dyskinesis W Ben Kibler, Aaron Sciascia Shoulder Center of Kentucky, Lexington, Kentucky, USA Correspondence to Aaron Sciascia, Shoulder Center of Kentucky, 700 Bob- O-Link,
Current concepts: scapular dyskinesis W Ben Kibler, Aaron Sciascia Shoulder Center of Kentucky, Lexington, Kentucky, USA Correspondence to Aaron Sciascia, Shoulder Center of Kentucky, 700 Bob- O-Link,
MOON SHOULDER GROUP NONOPERATIVE TREATMENT OF ROTATOR CUFF TENDONOPATHY PHYSICAL THERAPY GUIDELINES
 MOON SHOULDER GROUP NONOPERATIVE TREATMENT OF ROTATOR CUFF TENDONOPATHY PHYSICAL THERAPY GUIDELINES From: Kuhn JE. Exercise in the treatment of rotator cuff impingement. A systematic review and synthesized
MOON SHOULDER GROUP NONOPERATIVE TREATMENT OF ROTATOR CUFF TENDONOPATHY PHYSICAL THERAPY GUIDELINES From: Kuhn JE. Exercise in the treatment of rotator cuff impingement. A systematic review and synthesized
Mercer County Community College Donna Doulong March 8, 2013
 Mercer County Community College Donna Doulong March 8, 2013 Why strengthen the scapular muscles? The scapular thoracic articulation is the true core of the upper extremity. (Shankman & Manske, 2011, p.
Mercer County Community College Donna Doulong March 8, 2013 Why strengthen the scapular muscles? The scapular thoracic articulation is the true core of the upper extremity. (Shankman & Manske, 2011, p.
Orthopedic Physical Assessment with Special Tests Shoulder
 Orthopedic Physical Assessment with Special Tests Shoulder COURSE DESCRIPTION Detailed video demonstrations of tests and procedures common in musculoskeletal assessment are supplemented by high-quality
Orthopedic Physical Assessment with Special Tests Shoulder COURSE DESCRIPTION Detailed video demonstrations of tests and procedures common in musculoskeletal assessment are supplemented by high-quality
SLAP Lesion Type II Repair Rehabilitation Program
 SLAP Lesion Type II Repair Rehabilitation Program The GLSM SLAP Type II Repair Rehabilitation Program is an evidence-based and soft tissue healing dependent program allowing patients to progress to vocational
SLAP Lesion Type II Repair Rehabilitation Program The GLSM SLAP Type II Repair Rehabilitation Program is an evidence-based and soft tissue healing dependent program allowing patients to progress to vocational
Rehabilitation after Arthroscopic Posterior Bankart Repair
 Rehabilitation after Arthroscopic Posterior Bankart Repair Phase 1: 0 to 2 weeks after surgery POSTOPERATIVE INSTRUCTIONS You will wake up in the operating room. A sling and an ice pack will be in place.
Rehabilitation after Arthroscopic Posterior Bankart Repair Phase 1: 0 to 2 weeks after surgery POSTOPERATIVE INSTRUCTIONS You will wake up in the operating room. A sling and an ice pack will be in place.
Treatment of the Shoulder Girdle for Functional Outcomes. Postural Alignment and it s Effect on the Shoulder Girdle. Left Anterior Rotation of Pelvis
 Treatment of the Shoulder Girdle for Functional Outcomes Gail Ritchie, OTR/L Postural Alignment and it s Effect on the Shoulder Girdle Floating system Relies on the alignment of the axial skeleton Left
Treatment of the Shoulder Girdle for Functional Outcomes Gail Ritchie, OTR/L Postural Alignment and it s Effect on the Shoulder Girdle Floating system Relies on the alignment of the axial skeleton Left
Scapular function and dysfunction
 Scapular function and dysfunction - Impingement - Muscle detachment W. Ben Kibler, MD Medical director FUNCTION IMPINGEMENT REVISITED Is impingement always a diagnosis- isolated description of pathology
Scapular function and dysfunction - Impingement - Muscle detachment W. Ben Kibler, MD Medical director FUNCTION IMPINGEMENT REVISITED Is impingement always a diagnosis- isolated description of pathology
Ms. Ruth A. Delaney, MB BCh BAO, MMedSc, MRCS
 Ms. Ruth A. Delaney, MB BCh BAO, MMedSc, MRCS Consultant Orthopaedic Surgeon, Shoulder Specialist. +353 1 5262335 ruthdelaney@sportssurgeryclinic.com Modified from the protocol developed at Boston Shoulder
Ms. Ruth A. Delaney, MB BCh BAO, MMedSc, MRCS Consultant Orthopaedic Surgeon, Shoulder Specialist. +353 1 5262335 ruthdelaney@sportssurgeryclinic.com Modified from the protocol developed at Boston Shoulder
Breakout Session #7: Manual therapy for shoulder pain and limited mobility
 Northwestern University Feinberg School of Medicine Breakout Session #7: Manual therapy for shoulder pain and limited mobility @Amee_S Objectives 1. Demonstrate the examination procedures and describe
Northwestern University Feinberg School of Medicine Breakout Session #7: Manual therapy for shoulder pain and limited mobility @Amee_S Objectives 1. Demonstrate the examination procedures and describe
Affiliations. Scapular Stabilization in the Overhead Athlete. COI Disclosure Information. Greetings Commonwealth of Kentucky 6/10/2015
 Scapular Stabilization in the Overhead Athlete Tim L. Uhl PhD ATC PT FNATA Division of Athletic Training Department of Rehabilitation Sciences College of Health Sciences University of Kentucky COI Disclosure
Scapular Stabilization in the Overhead Athlete Tim L. Uhl PhD ATC PT FNATA Division of Athletic Training Department of Rehabilitation Sciences College of Health Sciences University of Kentucky COI Disclosure
Cervico-Thoracic Management Exercise and Manual Therapy. Deep Neck Flexor Training. Deep Neck Flexor Training. FPTA Spring 2011 Eric Chaconas 1
 Cervico-Thoracic Management Exercise and Manual Therapy Eric Chaconas PT, DPT, CSCS, FAAOMPT Deep Neck Flexor Training Evidence of dysfunction in the longus coli and longus capitus. Chronic Neck Pain Idiopathic
Cervico-Thoracic Management Exercise and Manual Therapy Eric Chaconas PT, DPT, CSCS, FAAOMPT Deep Neck Flexor Training Evidence of dysfunction in the longus coli and longus capitus. Chronic Neck Pain Idiopathic
OrthoCarolina. Arthroscopic SLAP Lesion (Type II) Repair Protocol
 Repair Protocol") OrthoCarolina Arthroscopic SLAP Lesion (Type II) Repair Protocol Surgical Overview: SLAP, which stands for superior labrum anterior to posterior, lesions are labral detachments that originate posterior
OrthoCarolina Arthroscopic SLAP Lesion (Type II) Repair Protocol Surgical Overview: SLAP, which stands for superior labrum anterior to posterior, lesions are labral detachments that originate posterior
Shoulder and Elbow ORTHOPAEDIC SYPMPOSIUM APRIL 8, 2017 DANIEL DOTY MD
 Shoulder and Elbow ORTHOPAEDIC SYPMPOSIUM APRIL 8, 2017 DANIEL DOTY MD Shoulder Articulations Glenohumeral Joint 2/3 total arc of motion Shallow Ball and Socket Joint Allows for excellent ROM Requires
Shoulder and Elbow ORTHOPAEDIC SYPMPOSIUM APRIL 8, 2017 DANIEL DOTY MD Shoulder Articulations Glenohumeral Joint 2/3 total arc of motion Shallow Ball and Socket Joint Allows for excellent ROM Requires
Rotator Cuff and Shoulder Conditioning Program
 Rotator Cuff and Shoulder Conditioning Program Purpose of Program After an injury or surgery, an exercise conditioning program will help you return to daily activities and enjoy a more active, healthy
Rotator Cuff and Shoulder Conditioning Program Purpose of Program After an injury or surgery, an exercise conditioning program will help you return to daily activities and enjoy a more active, healthy
Biceps Tenodesis Protocol
 Biceps Tenodesis Protocol A biceps tenodesis procedure involves cutting of the long head of the biceps just prior to its insertion on the superior labrum and then anchoring the tendon along its anatomical
Biceps Tenodesis Protocol A biceps tenodesis procedure involves cutting of the long head of the biceps just prior to its insertion on the superior labrum and then anchoring the tendon along its anatomical
The SUPPORT Trial: SUbacromial impingement syndrome and Pain: a randomised controlled trial Of exercise and injection
 The SUPPORT Trial: SUbacromial impingement syndrome and Pain: a randomised controlled trial Of exercise and injection SUPPORT Physiotherapy Intervention Training Manual Authors: Sue Jackson (SJ) Julie
The SUPPORT Trial: SUbacromial impingement syndrome and Pain: a randomised controlled trial Of exercise and injection SUPPORT Physiotherapy Intervention Training Manual Authors: Sue Jackson (SJ) Julie
Presented by Matt Repa ATC,CES
 Presented by Matt Repa ATC,CES mrepa@ibji.com Illinois Bone & Joint Institute CSL Symposium 1/11/11 } Throwing is a very complex and dynamic activity. } As clinicians, how can we step in and make a difference?
Presented by Matt Repa ATC,CES mrepa@ibji.com Illinois Bone & Joint Institute CSL Symposium 1/11/11 } Throwing is a very complex and dynamic activity. } As clinicians, how can we step in and make a difference?
Conservative Multi-Directional Capsular Instability Protocol
 SPORTS & ORTHOPAEDIC SPECIALISTS 8100 W. 78 th Street Edina, MN 55439 952-946-9777 www.womensorthocenter.com Conservative Multi-Directional Capsular Instability Protocol 4-6 visits over 6 weeks Primary
SPORTS & ORTHOPAEDIC SPECIALISTS 8100 W. 78 th Street Edina, MN 55439 952-946-9777 www.womensorthocenter.com Conservative Multi-Directional Capsular Instability Protocol 4-6 visits over 6 weeks Primary
ARTHROSCOPIC DECOMPRESSION PROTOCOL Dr. Steven Flores
 ARTHROSCOPIC DECOMPRESSION PROTOCOL Dr. Steven Flores This rehabilitation protocol has been developed for the patient following an arthroscopic decompression surgical procedure. The arthroscopic decompression
ARTHROSCOPIC DECOMPRESSION PROTOCOL Dr. Steven Flores This rehabilitation protocol has been developed for the patient following an arthroscopic decompression surgical procedure. The arthroscopic decompression
Yoga Straps for Scapular Strength
 ACE Pro Source Yoga Straps for Scapular Strength By Elizabeth R. Kovar M.A. In a well-rounded yoga practice, it is important to demonstrate scapular or shoulder blade strength. For some people, however,
ACE Pro Source Yoga Straps for Scapular Strength By Elizabeth R. Kovar M.A. In a well-rounded yoga practice, it is important to demonstrate scapular or shoulder blade strength. For some people, however,
Clinical examination of the shoulder girdle
 Clinical of the shoulder girdle CHAPTER CONTENTS Symptoms referred to the shoulder girdle........ e72 Symptoms referred from the shoulder girdle...... e72 History........................... e72 Inspection.........................
Clinical of the shoulder girdle CHAPTER CONTENTS Symptoms referred to the shoulder girdle........ e72 Symptoms referred from the shoulder girdle...... e72 History........................... e72 Inspection.........................
Review shoulder anatomy Review the physical exam of the shoulder Discuss some common causes of acute shoulder pain Discuss some common causes of
 Review shoulder anatomy Review the physical exam of the shoulder Discuss some common causes of acute shoulder pain Discuss some common causes of chronic shoulder pain Review with some case questions Bones:
Review shoulder anatomy Review the physical exam of the shoulder Discuss some common causes of acute shoulder pain Discuss some common causes of chronic shoulder pain Review with some case questions Bones:
Scapular and Deltoid Regions
 M1 Gross and Developmental Anatomy Scapular and Deltoid Regions Dr. Peters 1 Outline I. Skeleton of the Shoulder and Attachment of the Upper Extremity to Trunk II. Positions and Movements of the Scapula
M1 Gross and Developmental Anatomy Scapular and Deltoid Regions Dr. Peters 1 Outline I. Skeleton of the Shoulder and Attachment of the Upper Extremity to Trunk II. Positions and Movements of the Scapula
Bradley C. Carofino, M.D. Shoulder Specialist 230 Clearfield Avenue, Suite 124 Virginia Beach, Virginia Phone
 Subpectoral Bicep Tenodesis Protocol (Spreadsheet) Weeks 1-2 Modalities Treatment Restrictions Goals No active elbow flexion (6weeks) Full PROM shoulder and elbow PROM: Shoulder, elbow, forearm No active
Subpectoral Bicep Tenodesis Protocol (Spreadsheet) Weeks 1-2 Modalities Treatment Restrictions Goals No active elbow flexion (6weeks) Full PROM shoulder and elbow PROM: Shoulder, elbow, forearm No active
SLAP LESION REPAIR PROTOCOL
 SLAP LESION REPAIR PROTOCOL Clarkstown Division This rehabilitation protocol has been developed for the patient following a SLAP (Superior Labrum Anterior Posterior) repair. It is extremely important to
SLAP LESION REPAIR PROTOCOL Clarkstown Division This rehabilitation protocol has been developed for the patient following a SLAP (Superior Labrum Anterior Posterior) repair. It is extremely important to
REHABILITATION GUIDELINES FOR ROTATOR CUFF REPAIR FOR TYPE II TEARS (MASSIVE)(+/- SUBACROMIAL DECOMPRESSION)
(+/- SUBACROMIAL DECOMPRESSION)") REHABILITATION GUIDELINES FOR ROTATOR CUFF REPAIR FOR TYPE II TEARS (MASSIVE)(+/- SUBACROMIAL DECOMPRESSION) The rehabilitation guidelines are presented in a criterion based progression. General time frames
REHABILITATION GUIDELINES FOR ROTATOR CUFF REPAIR FOR TYPE II TEARS (MASSIVE)(+/- SUBACROMIAL DECOMPRESSION) The rehabilitation guidelines are presented in a criterion based progression. General time frames
SHOULDER PAIN. A Real Pain in the Neck. Michael Wolk, MD Northeastern Rehabilitation Associates October 31, 2017
 SHOULDER PAIN A Real Pain in the Neck Michael Wolk, MD Northeastern Rehabilitation Associates October 31, 2017 THE SHOULDER JOINT (S) 1. glenohumeral 2. suprahumeral 3. acromioclavicular 4. scapulocostal
SHOULDER PAIN A Real Pain in the Neck Michael Wolk, MD Northeastern Rehabilitation Associates October 31, 2017 THE SHOULDER JOINT (S) 1. glenohumeral 2. suprahumeral 3. acromioclavicular 4. scapulocostal
Arthroscopic SLAP Repair Protocol
 SPORTS & ORTHOPAEDIC SPECIALISTS Arthroscopic SLAP Repair Protocol 6-8 visits over 12 weeks Emphasis is on AAROM and a high repetition, low weight free weight program Address posterior capsular tightness
SPORTS & ORTHOPAEDIC SPECIALISTS Arthroscopic SLAP Repair Protocol 6-8 visits over 12 weeks Emphasis is on AAROM and a high repetition, low weight free weight program Address posterior capsular tightness
[ CLINICAL COMMENTARY ]
![[ CLINICAL COMMENTARY ]](/thumbs/75/72029404.jpg "[ CLINICAL COMMENTARY ]") PAULA M. LUDEWIG, PT, PhD¹ PT, PhD² The Association of Scapular Kinematics and Glenohumeral Joint Pathologies houlder pain and associated glenohumeral joint movement dysfunctions are common and debilitating
PAULA M. LUDEWIG, PT, PhD¹ PT, PhD² The Association of Scapular Kinematics and Glenohumeral Joint Pathologies houlder pain and associated glenohumeral joint movement dysfunctions are common and debilitating
Superior Labrum Repair Protocol - SLAP
 Superior Labrum Repair Protocol - SLAP Stage I (0-4 weeks): Key Goals: Protect the newly repaired shoulder. Allow for decreased inflammation and healing. Maintain elbow, wrist and hand function. Maintain
Superior Labrum Repair Protocol - SLAP Stage I (0-4 weeks): Key Goals: Protect the newly repaired shoulder. Allow for decreased inflammation and healing. Maintain elbow, wrist and hand function. Maintain
Biceps Tenotomy Protocol
 Biceps Tenotomy Protocol A biceps tenotomy procedure involves cutting of the long head of the biceps just prior to its insertion on the superior labrum. A biceps tenotomy is typically done when there is
Biceps Tenotomy Protocol A biceps tenotomy procedure involves cutting of the long head of the biceps just prior to its insertion on the superior labrum. A biceps tenotomy is typically done when there is
Cross Country Education Leading the Way in Continuing Education and Professional Development.
 Manual Therapy Exercises for the Shoulder To comply with professional boards/associations standards: I declare that I or my family do not have any financial relationship in any amount, occurring in the
Manual Therapy Exercises for the Shoulder To comply with professional boards/associations standards: I declare that I or my family do not have any financial relationship in any amount, occurring in the
Anatomy of the Shoulder Girdle. Prof Oluwadiya Kehinde FMCS (Orthop)
") Anatomy of the Shoulder Girdle Prof Oluwadiya Kehinde FMCS (Orthop) www.oluwadiya.com Bony Anatomy Shoulder Complex: Sternum(manubrium) Clavicle Scapula Proximal humerus Manubrium Sterni Upper part of
Anatomy of the Shoulder Girdle Prof Oluwadiya Kehinde FMCS (Orthop) www.oluwadiya.com Bony Anatomy Shoulder Complex: Sternum(manubrium) Clavicle Scapula Proximal humerus Manubrium Sterni Upper part of
Sterile gauze used at incision site. Check brace for rubbing or irritation. Compression garment at elbow to be used with physician s authorization
 ULNAR COLLATERAL LIGAMENT RECONSTRUCTION GUIDELINE Functional Outcome Measure KJOC (Appendix 1) should be completed at initial evaluation and at all identified times through guideline, Phase 1 Immediate
ULNAR COLLATERAL LIGAMENT RECONSTRUCTION GUIDELINE Functional Outcome Measure KJOC (Appendix 1) should be completed at initial evaluation and at all identified times through guideline, Phase 1 Immediate
Welcome to. Not to be copied without the express permission of EDUCATA. Copyright 2014 EDUCATA. All rights reserved. 1. How to Navigate EDUCATA
 Welcome to Copyright 2014 EDUCATA. This presentation is not to be copied in whole or in part without the express permission of EDUCATA. How to Navigate EDUCATA The Shoulder Complex Mechanics, Muscle Function
Welcome to Copyright 2014 EDUCATA. This presentation is not to be copied in whole or in part without the express permission of EDUCATA. How to Navigate EDUCATA The Shoulder Complex Mechanics, Muscle Function
Tendinosis & Subacromial Impingement Syndrome. Gene Desepoli, LMT, D.C.
 Tendinosis & Subacromial Impingement Syndrome Gene Desepoli, LMT, D.C. What is the shoulder joint? Shoulder joint or shoulder region? There is an interrelatedness of all moving parts of the shoulder and
Tendinosis & Subacromial Impingement Syndrome Gene Desepoli, LMT, D.C. What is the shoulder joint? Shoulder joint or shoulder region? There is an interrelatedness of all moving parts of the shoulder and
Today s Shoulder. Session 108: Glenohumeral Stabilization For True Upper Extremity Function
 To comply with professional boards/associations standards: I declare that I (or my family) do not have a financial relationship in any amount, occurring in the last 12 months with a commercial interest
To comply with professional boards/associations standards: I declare that I (or my family) do not have a financial relationship in any amount, occurring in the last 12 months with a commercial interest
Rehabilitation Protocol: Arthroscopic Anterior Capsulolabral Repair of the Shoulder - Bankart Repair Rehabilitation Guidelines
 Rehabilitation Protocol: Arthroscopic Anterior Capsulolabral Repair of the Shoulder - Bankart Repair Rehabilitation Guidelines Department of Orthopaedic Surgery Lahey Hospital & Medical Center, Burlington
Rehabilitation Protocol: Arthroscopic Anterior Capsulolabral Repair of the Shoulder - Bankart Repair Rehabilitation Guidelines Department of Orthopaedic Surgery Lahey Hospital & Medical Center, Burlington
Prater Chiropractic Wellness Center 903 W. South St. Kalamazoo, MI PH: (269)
") Purpose of Program After an injury or surgery, an exercise conditioning program will help you return to daily activities and enjoy a more active, healthy lifestyle. Following a well-structured conditioning
Purpose of Program After an injury or surgery, an exercise conditioning program will help you return to daily activities and enjoy a more active, healthy lifestyle. Following a well-structured conditioning