Working with The Shoulder
|
|
|
- Alban Ryan
- 6 years ago
- Views:
Transcription

1 Working with The Shoulder Plus BONUS Stretching! Dr Bryan Hawley DC
2 Housekeeping Recording will be sent out tomorrow Certificates Questions All presented today is based off OUR OWN CLINIC system Lets begin copy right 2010 Dr Bryan Hawley
3 Shoulder pain is extremely common in fact it is the 2 nd most common complaint Difficult joint to examine Multi directional ROM Must make an accurate dx of the cause of the symptoms (look for the root cause) in order for it not to keep reoccurring

4 Anatomy Glenohumeral Joint- ball and socket synovial type of joint Highly dependent and guarded by muscles and ligaments When relaxed the head of the humerus is centered in the glenoid cavity Rotator Cuff mm plays vital role in stability and support

5 Pectoral/Shoulder girdle muscles from the back

6 Pectoral/Shoulder girdle muscles from the front

7

8
9 Clinical Presentation Usually effects persons in the age from and mostly females Slight wasting of muscular tissue surrounding the joint with palpable tendernes Pain is gradual in onset External rotation is most inhibited of the ROM
10 Common Shoulder Injuries Impingement Syndrome Rotator Cuff Sprain Strain Rotator Cuff Tear Glenoid labral Tear Tendonitis Bursitis AC Separation Adhesive Capsulitis (Frozen Shoulder)
11 Shoulder Exam This topic is broken down into general shoulder exam inspection palpation ROM neurovascular exam impingement tests rotator cuff tests labral injury tests biceps injuries tests AC joint instability Other, Radiology
12 Acromioclavicular (AC) Joint Distraction Test Acromioclavicular (AC) Shear Test Adson s Maneuver Allen Test Anterior Drawer Test Apley s Scratch Test Apprehension Test Brachial Plexus Stretch Test Biceps Load Test Clunk Test Crank Test Cross-Over Impingement Test Drop Arm Test Empty Can (Supraspinatus) Test Feagin Test French Horn Test Gerber s Lift Off Test Grind Test Hawkins Test / Hawkins-Kennedy Impingement Test Jobe Relocation Test Load and Shift Test Orthopedic Special Tests for the Shoulder Girdle Ludington s Sign Neer Impingement Test O Brien s Test Pectoralis Major Contracture Test Piano Key Sign Posterior Drawer Test Roos Test Shoulder Abduction Test Speed s Test / Speed s Maneuver Sternoclavicular (SC) Joint Stress Test Sulcus Sign Yergason s Test Yocum Test
13 Impingement Tests Neer Impingement Sign indicative of impingement as well as many other causes of shoulder pain/focal abnormalities (stiffness, OA, instability, bone lesions); note you must have full range of motion for "positive" finding. technique use one hand to prevent motion of the scapula while raising the arm of the patient with the other hand in forced elevation (somewhere between flexion and abduction) eliciting pain (positive test) as the greater tuberosity impinges against the acromion (between ) Hawkins Sign positive with impingement technique performed by flexing shoulder to 90, flex elbow to 90, and forcibly internally rotate driving the greater tuberosity farther under the CA ligament. test for impingement. Jobe s Test positive with supraspinatus weakness and or impingement technique abduct arm to 90, angle forward 30 (bringing it into the scapular plane), and internally rotate (thumb pointing to floor). then press down on arm while patient attempts to maintain position testing for weakness or pain. Internal Impingement patient supine, abduct affected side to 90 and maximally externally rotate (throwing position-late cocking phase) with extension. If this maneuver reproduces pain experienced during throwing (posteriorly located) considered it is considered positive. Further confirmed with relief upon performing relocation test. Reperform test in Abduction/max. ER with elbow in front of plane of body and pain disappears.
14 Rotator Cuff Tests Subscapularis Strength is tested comparing both sides by having patient keep elbow at sides in 90 of flexion test ability to internally rotate against resistance. Internal Rotation Lag Sign this tests is the most sensitive and specific test for subscapularis pathology. technique stand behind patient, flex elbow to 90, hold shoulder at 20 elevation and 20 extension. Internally rotate shoulder to near maximum holding the wrist by passively lifting the dorsum of the hand away from the lumbar spine then supporting the elbow, tell patient to maintain position and release the wrist while looking for a lag. Increased Passive ER a person with a subscapularis tear may have increased Passive ER rotation when compared to contralateral side Lift Off Test more accurate for inferior portion of subscapularis. technique hand brought around back to region of lumbar spine, palm facing outward; Test patient s ability to lift hand away from back (internal rotation). Inability to do this indicates subscapularis pathology. Is confounded by other muscles. More accurate if the tested hand can reach the contralateral scapula. Belly Press test positive with subscapularis pathology more accurate for superior portion of subscapularis technique patient presses abdomen with palm of hand, maintaining shoulder in internal rotation. If elbow drops back (does not remain in front of trunk)
15 Supraspinatus tests Supraspinatus Strength Jobe s Test strength is assessed using Jobe s Test (see below) pain with this test is indicative of a subacromial bursitis/irritation not necessarily a supra tear. Only considered positive for tear with a true drop arm. i.e. arm is brought to 90 and literally falls down. tests for supraspinatus weakness and/or impingement technique abduct arm to 90, angle forward 30 (bringing it into the scapular plane), and internally rotate (thumb pointing to floor). Then press down on arm while patient attempts to maintain position testing for weakness or pain. Drop Sign tests for function/integrity of supraspinatus technique passively elevate arm in scapular plan to 90. Then ask the patient to slowly lower the arm. The test is positive when weakness or pain causes them to drop the arm to their side.
16 Infraspinatus Infraspinatus Strength external rotation strength tested while the arm is in neutral abduction/adduction External Rotation Lag Sign positive when the arm starts to drift into internal rotation technique passively flex the elbow to 90 degrees, holding wrist to rotate the shoulder to maximal external rotation. Tell the patient to hold the arm in that externally rotated position. If the arm starts to drift into internal rotation, it is positive.
17 Teres Minor Teres Minor Strength external rotation tested with the arm held in 90 degrees of abduction Hornblower's sign positive if the arm falls into internal rotation it may represent teres minor pathology technique bring the shoulder to 90 degrees of abduction, 90 degrees of external rotation and ask the patient to hold this position
18 AC joint Tests Acromioclavicular joint tenderness tenderness with palpation of the acromioclavicular joint Cross-Body Adduction positive when there is pain in the AC joint technique patient forward elevates the arm to 90 degrees and actively adducts the arm across the body. Obrien's Test (Active Compression test) positive when there is pain "superficial" over the AC joint while the forearm is pronated but not when the forearm is supinated Technique patient forward flexes the affected arm to 90 degrees while keeping the elbow fully extended. The arm is then adducted degrees across the body. The patient then pronates the forearm so the thumb is pointing down. The examiner applies downward force to the wrist while the arm is in this position while the patient resists. The patient then supinates the forearm so the palm is up and the examiner once again applies force to the wrist while the patient resists.

19 Drop-arm test Abduct the patient's shoulder to 90 and ask the patient to lower the arm side in the same arc of movement. Severe pain or inability of the patient to return the arm to the side slowly indicates a positive test result.a positive result indicates a rotator cuff tear.

20 Neer impingement test The shoulder is forcibly forward flexed and internally rotated, causing the greater tuberosity to jam against the anterior inferior surface of the acromion. Pain reflects a positive test result and indicates an overuse injury to the supraspinatus muscle and possibly to the biceps tendon indicative of impingement as well as many other causes of shoulder pain/focal abnormalities (stiffness, OA, instability, bone lesions); note you must have full range of motion for "positive" finding. technique use one hand to prevent motion of the scapula while raising the arm of the patient with the other hand in forced elevation (somewhere between flexion and abduction) eliciting pain (positive test) as the greater tuberosity impinges against the acromion (between )

21 Hawkins-Kennedy impingement test With force internally rotate the shoulder. Pain indicates a positive test result and is due to supraspinatus tendon and greater tuberosity impingement under the coracoacromial ligament and coracoid process.


22 Apprehension test Abduct the arm 90 and fully externally rotate while placing anteriorly directed force on the posterior humeral head from behind. The patient becomes apprehensive and resists further motion if chronic anterior instability is present.

23 Coracoid impingement syndrome is a less common cause of shoulder pain. Symptoms are presumed to occur when the subscapularis tendon impinges between the coracoid and lesser tuberosity of the humerus.
24 Where is the pain coming from? Rotator cuff? Bursa (bursitis) Glenohumeral disorders (capsulitis, frozen shoulder), arthritis Acromioclavicular pathology Trauma (minor dislocation) Referred, neck and upper back pain Fibromyalgia Internal disorders (lung malignancy cardiovascular)


25 Typical Gen Shoulder TPs
26 Adhesive Capsulitis Frozen Shoulder Syndrome Disorder in which the shoulder capsule becomes inflames and stiff greatly restricting the normal ROM Unless trauma is present the etiology is mostly unknown Progressive pain and increasing stiffness which sometimes will resolve spontaneously after 18 month Pain is worse at night and shoulder movement is severely restricted
27 Rehab of Frozen Shoulder Phase1 This phase is usually the most painful phase of frozen shoulder treatment and movement becomes gradually more and more difficult. The aim of the following treatments and exercises is to help control pain and maintain movement in the shoulder joint. Electrotherapy modalities such as ultrasound, TENS and laser treatment may all help reduce pain and inflammation. Massage and Trigger Point work for surrounding muscles combined w passive ROM Phase 2 Mobility exercises such as pendulums and wand exercises should be continued. Frozen shoulder stretching exercises for the chest muscles and muscles at the back of the shoulder should also be maintained. Strengthening exercises for frozen shoulder can be performed to maintain muscle strength. Isometric or static contractions are exercises needing no joint movement and can be done without worrying about movement in the shoulder. Phase 3 Mobility exercises and stretches can become more aggressive, but should still be within the boundaries of pain. Aim to restore full mobility in the shoulder joint. Strengthening exercises can progress from isometric or static contractions, to exercises using a resistance band, then eventually free weights or weight machines.

28 Impingement syndrome This occurs when the space between the humeral head and the acromion above becomes narrowed The three things that usually get pinched are 1. Joint capsule itself 2. Tendons of the rotator cuff muscles 3. Bursa sac This can create either a bursitis or tendonitis depending on the Structures involved. Overhead usage workers and athletes are more likely to have Issues such as this Approx 1/3 of shoulder problems are due to impingement

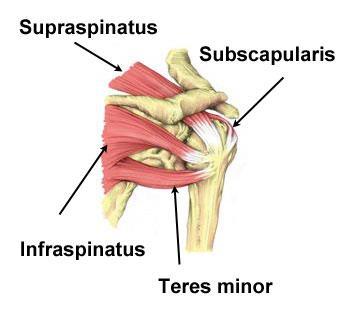
29 Rotator Cuff Muscles SITS
30
31 Rotator Cuff Injuries Tendinitis: Tendons in your rotator cuff can become inflamed due to overuse or overload, especially in athletes who perform a lot of overhead activities. In some people, the space where the rotator cuff resides can be narrowed due to the shape of different shoulder bones, including the outside end of the collarbone or shoulder blade. Bursitis: The fluid-filled sac (bursa) between your shoulder joint and rotator cuff tendons can become irritated and Strain or tear: Left untreated, tendinitis can weaken a tendon and lead to chronic tendon degeneration or to a tendon tear. Stress from overuse also can cause a shoulder tendon or muscle to tear.
32 Rotator Cuff Tear A ripping of one or more of the tendons Result when a sudden eccentric force applied to the rotator cuff resulting in failure of the tendon. Uncommon under the age of 40 but strains do occur. In the population over 40 years of age, supraspinatus tears occur and less commonly, infraspinatus tears. Tears in the subscapularis tendon are uncommon and are often the result of a shoulder dislocation.

33 Rotator Cuff Tears YOUNG PERSON Usually is more due to a traumatic type injury from a hanging or falling on an outstretched arm A person can have a chronic injury such as a repetitive stress syndrome that can lead to a tear OLDER PERSON It is more likely due to loss of elasticity within the muscle and tendon which can result in A tear from doing basic everyday activities.
34 Causes of RT Tears Repetitive stress: Repetitive overhead movement of your arms can stress your rotator cuff muscles and tendons, causing inflammation and eventually tearing. This occurs often in athletes, especially baseball pitchers and tennis players. It's also common among people in the building trades, such as painters and carpenters Impingement: Falls or incorrect throwing techniques or arm movements and weak shoulder muscles may cause the arm bone to move up and trap the tendon. This may also happen in persons who over-train or have a sudden change in arm or shoulder activity. Normal wear and tear: The rotator cuff tendons can degenerate due to ages (starting around the age of 40). This can cause a breakdown of fibrous protein (collagen) in the cuff's tendons and muscles. Calcium deposits: Calcium may deposit in the tendons due to decreased oxygen and poor blood supply. These deposits may cause irritation and inflammation
35 Causes Cont. Poor posture: When you slouch your neck and shoulders forward, the space where the rotator cuff muscles reside can become smaller. This can allow a muscle or tendon to become pinched under your shoulder bones, including your collarbone, especially during overhead activities, Falling: Using your arm to break a fall or falling on your arm can bruise or tear a rotator cuff tendon or muscle. Lifting or Pulling: Lifting an object that's too heavy, or doing so improperly (especially overhead) can strain or tear your tendons or muscles. Pulling something, such as an archery bow of too heavy poundage, may cause an injury.
36 Rotator Cuff Tears Symptoms Atrophy of the muscles around the shoulder Pain when someone else lifts the arm Pain when lowering the arm from a fully raised position Weakness when moving the arm Crackling or grinding sensation when arm is passively moved With a partial tear the person will feel pain but still have normal ROM With a complete tear there is pain but not normal ROM Overhead motions are most difficult A shoulder shrugging motion is present


37

38
39 Tendinitis of the Supraspinatus Sup Tendinitis is a common condition of the shoulder that causes anterior shoulder pain Present usually in abduction The painful arc is between 60 and 90 deg of abduction. Pt usually starts leaning body away from arc to avoid excessive abduction Pain sleeping on the affected side Catching of the shoulder during use Pain on BOTH AROM and PROM Palpable tenderness

40 Supraspinatous Tendinitis Test With pt seated abduct the arm to 90 deg against resistance POS pain or weakness over the insertion of the Supraspinatous tendon may indicate tendinitis or tear Pain over the deltoid mm may indicate a strained medial or anterior deltoid mm. Watch for pt leaning away sign as well. Always perform on the non involved side first to get a baseline ROM and resistance pressure Apley ScratchTest With pt seated place hand of affected shoulder behind head to touch the upper part of the back. POS indicates tendinitis of the tendons of the supraspinatous tendon
41 Bursitis The subacromial bursa overlies the rotator cuff tendons Bursitis is associated with tendinitis of the of the adjacent supraspinatus tendon Causes of bursitis are trauma, overuse, multiple traumas, improper executed activity Clinical Signs and Symptoms Anterloateral shoulder pain Pain sleeping on affected side Stiffness Pain on AROM and PROM

42 Glenoid Labrum The glenoid Labrum is a ring of cartilage attached to the margin of the Glenoid cavity of the scapula This labrum acts to keep the humeral head positioned on the glenoid by blocking Unwanted movement.
 part of the labrum is injured Injuries to the superior labrum can be caused by acute trauma or by repetitive shoulder motion.")
43 A SLAP tear is an injury to the labrum of the shoulder, which is the ring of cartilage that surrounds the socket of the shoulder joint. The term SLAP stands for Superior Labrum Anterior and Posterior. In a SLAP injury, the top (superior) part of the labrum is injured Injuries to the superior labrum can be caused by acute trauma or by repetitive shoulder motion. An acute SLAP injury may result from: A motor vehicle accident A fall onto an outstretched arm Forceful pulling on the arm, such as when trying to catch a heavy object Rapid or forceful movement of the arm when it is above the level of the shoulder Shoulder dislocation People who participate in repetitive overhead sports, such as throwing athletes or weightlifters, can experience labrum tears as a result of repeated shoulder motion.
44 3 Main types of instability 1.Anterior 2.Posterior 3.Multi Directional

45

46 Posterior Instability 5% of cases Painful arc (PROM and AROM) if dislocated Feeling of shoulder slippage Apprehension on any movement Crepitus on movement Increase shoulder girth if dislocated TEST Pt is supine, forward flex and internally rotate the shoulder. Apply an ant-post pressure on the elbow POS Pain or apprehension on the pts face.


47 Shoulder Drawer Sign Manually assessing translation the examiner places hand on upper humeral while stabilizing at the distal end and checks for excessive movement. This can also be done sitting as well with placing hand on scapula and posterior shoulder for support while moving the humeral head. Apprehension test modified Pt arm is placed in abduction, extension, and external rotation while stressing it in anterior translocation. If patient becomes apprehensive or reports pain this is a pos finding.
, backward (posterior), or downward (inferior) direction.")
48 What is Multidirectional Instability of the Shoulder? MDI of the shoulder is defined as generalized laxity (looseness) of the joint due to increased mobility and joint weakness. The shoulder joint may "slip" in and out of its socket in a forward (anterior), backward (posterior), or downward (inferior) direction. This "laxity" may be exaggerated in people who participate in activities that require repeated overhead movement of the arm, such as baseball pitchers or swimmers. The most common cause of MDI is overuse of the shoulder or repetitive stress.

")

49 At Home Exercises for shoulder instability Shoulder instability is relatively common condition characterized by loosening of the connective tissue (ligaments and joint capsule) surrounding the shoulder joint therefore enabling the bones forming the joint to move excessively on each other.

50

51

52

53
54

55

56


57 Stretching the Sup.

58 The End, Thank you Recording will be sent out tomorrow Certificates Questions All presented today is based off OUR OWN CLINIC system Lets begin copy right 2010 Dr Bryan Hawley
Physical Examination of the Shoulder
 General setup Patient will be examined in both the seated and supine position so exam table needed 360 degree access to patient Expose neck and both shoulders (for comparison); female in gown or sports
General setup Patient will be examined in both the seated and supine position so exam table needed 360 degree access to patient Expose neck and both shoulders (for comparison); female in gown or sports
Review shoulder anatomy Review the physical exam of the shoulder Discuss some common causes of acute shoulder pain Discuss some common causes of
 Review shoulder anatomy Review the physical exam of the shoulder Discuss some common causes of acute shoulder pain Discuss some common causes of chronic shoulder pain Review with some case questions Bones:
Review shoulder anatomy Review the physical exam of the shoulder Discuss some common causes of acute shoulder pain Discuss some common causes of chronic shoulder pain Review with some case questions Bones:
Shoulder joint Assessment and General View
 Shoulder joint Assessment and General View Done by; Mshari S. Alghadier BSc Physical Therapy RHPT 366 m.alghadier@sau.edu.sa http://faculty.sau.edu.sa/m.alghadier/ Functional anatomy The shoulder contains
Shoulder joint Assessment and General View Done by; Mshari S. Alghadier BSc Physical Therapy RHPT 366 m.alghadier@sau.edu.sa http://faculty.sau.edu.sa/m.alghadier/ Functional anatomy The shoulder contains
Shoulder Joint Examination. Shoulder Joint Examination. Inspection. Inspection Palpation Movement. Look Feel Move
 Shoulder Joint Examination History Cuff Examination Instability Examination AC Joint Examination Biceps Tendon Examination Superior Labrum Examination Shoulder Joint Examination Inspection Palpation Movement
Shoulder Joint Examination History Cuff Examination Instability Examination AC Joint Examination Biceps Tendon Examination Superior Labrum Examination Shoulder Joint Examination Inspection Palpation Movement
SHOULDER PAIN. A Real Pain in the Neck. Michael Wolk, MD Northeastern Rehabilitation Associates October 31, 2017
 SHOULDER PAIN A Real Pain in the Neck Michael Wolk, MD Northeastern Rehabilitation Associates October 31, 2017 THE SHOULDER JOINT (S) 1. glenohumeral 2. suprahumeral 3. acromioclavicular 4. scapulocostal
SHOULDER PAIN A Real Pain in the Neck Michael Wolk, MD Northeastern Rehabilitation Associates October 31, 2017 THE SHOULDER JOINT (S) 1. glenohumeral 2. suprahumeral 3. acromioclavicular 4. scapulocostal
The Shoulder. Anatomy and Injuries PSK 4U Unit 3, Day 4
 The Shoulder Anatomy and Injuries PSK 4U Unit 3, Day 4 Shoulder Girdle Shoulder Complex is the most mobile joint in the body. Scapula Clavicle Sternum Humerus Rib cage/thorax Shoulder Girdle It also includes
The Shoulder Anatomy and Injuries PSK 4U Unit 3, Day 4 Shoulder Girdle Shoulder Complex is the most mobile joint in the body. Scapula Clavicle Sternum Humerus Rib cage/thorax Shoulder Girdle It also includes
Shoulder Labral Tear and Shoulder Dislocation
 Shoulder Labral Tear and Shoulder Dislocation The shoulder joint is a ball and socket joint with tremendous flexibility and range of motion. The ball is the humeral head while the socket is the glenoid.
Shoulder Labral Tear and Shoulder Dislocation The shoulder joint is a ball and socket joint with tremendous flexibility and range of motion. The ball is the humeral head while the socket is the glenoid.
Joint G*H. Joint S*C. Joint A*C. Labrum. Humerus. Sternum. Scapula. Clavicle. Thorax. Articulation. Scapulo- Thoracic
 A*C Joint Scapulo- Thoracic Articulation Thorax Sternum Clavicle Scapula Humerus S*C Joint G*H Joint Labrum AC Ligaments SC Ligaments SC JOINT AC Coracoacromial GH GH Ligament Complex Coracoclavicular
A*C Joint Scapulo- Thoracic Articulation Thorax Sternum Clavicle Scapula Humerus S*C Joint G*H Joint Labrum AC Ligaments SC Ligaments SC JOINT AC Coracoacromial GH GH Ligament Complex Coracoclavicular
RN(EC) ENC(C) GNC(C) MN ACNP *** MECHANISM OF INJURY.. MOST IMPORTANT ***
 ENC(C) GNC(C) MN ACNP *** MECHANISM OF INJURY.. MOST IMPORTANT ***") HISTORY *** MECHANISM OF INJURY.. MOST IMPORTANT *** Age - Certain conditions are more prevalent in particular age groups (i.e. Full rotator cuff tears are more common over the age of 45, traumatic injuries
HISTORY *** MECHANISM OF INJURY.. MOST IMPORTANT *** Age - Certain conditions are more prevalent in particular age groups (i.e. Full rotator cuff tears are more common over the age of 45, traumatic injuries
Anatomical Considerations/ Pathophysiology The shoulder is the most mobile joint in the body. : Three bones:
 Introduction Musculoskeletal training is generally underrepresented in medical training and residency curriculums. There is a general deficit in musculoskeletal knowledge amongst current medical students,
Introduction Musculoskeletal training is generally underrepresented in medical training and residency curriculums. There is a general deficit in musculoskeletal knowledge amongst current medical students,
Mastering the Musculoskeletal Exam UCSF Essentials of Women s Health July 7, 2016 Carlin Senter, M.D. Henry Crevensten, M.D.
 Mastering the Musculoskeletal Exam UCSF Essentials of Women s Health July 7, 2016 Carlin Senter, M.D. Henry Crevensten, M.D. I have nothing to disclose Outline Knee exam Shoulder exam Knee Anatomy The
Mastering the Musculoskeletal Exam UCSF Essentials of Women s Health July 7, 2016 Carlin Senter, M.D. Henry Crevensten, M.D. I have nothing to disclose Outline Knee exam Shoulder exam Knee Anatomy The
Shoulder examination. P Sripathi Rao Arthroscopy & Sports Injuries Unit Dean, Kasturba Medical College
 Shoulder examination P Sripathi Rao Arthroscopy & Sports Injuries Unit Dean, Kasturba Medical College Manipal University, Manipal Common symptoms Tingling Numbness Pain Loss of movements Weakness Approach
Shoulder examination P Sripathi Rao Arthroscopy & Sports Injuries Unit Dean, Kasturba Medical College Manipal University, Manipal Common symptoms Tingling Numbness Pain Loss of movements Weakness Approach
The Shoulder. By Patrick Ryan, Bobby Law, Jack Beaty, Alex Newhouse and Chuck Nelson
 The Shoulder By Patrick Ryan, Bobby Law, Jack Beaty, Alex Newhouse and Chuck Nelson Learning Objectives/Agenda Review the anatomy of the shoulder Describe the main diseases of the shoulder Describe the
The Shoulder By Patrick Ryan, Bobby Law, Jack Beaty, Alex Newhouse and Chuck Nelson Learning Objectives/Agenda Review the anatomy of the shoulder Describe the main diseases of the shoulder Describe the
WEEKEND 2 Shoulder. Shoulder Active Range of Motion Assessment
 Virginia Orthopedic Manual Physical Therapy Institute - 2016 Technique Manual WEEKEND 2 Shoulder Shoulder Active Range of Motion Assessment - Patient Positioning: Standing, appropriately undressed so that
Virginia Orthopedic Manual Physical Therapy Institute - 2016 Technique Manual WEEKEND 2 Shoulder Shoulder Active Range of Motion Assessment - Patient Positioning: Standing, appropriately undressed so that
The Shoulder Complex. Anatomy. Articulations 12/11/2017. Oak Ridge High School Conroe, Texas. Clavicle Collar Bone Scapula Shoulder Blade Humerus
 The Shoulder Complex Oak Ridge High School Conroe, Texas Anatomy Clavicle Collar Bone Scapula Shoulder Blade Humerus Articulations Sternoclavicular SC joint. Sternum and Clavicle. Acromioclavicular AC
The Shoulder Complex Oak Ridge High School Conroe, Texas Anatomy Clavicle Collar Bone Scapula Shoulder Blade Humerus Articulations Sternoclavicular SC joint. Sternum and Clavicle. Acromioclavicular AC
Rehabilitation Guidelines for Shoulder Arthroscopy
 Rehabilitation Guidelines for Shoulder Arthroscopy The true shoulder joint is called the glenohumeral joint and consists humeral head and the glenoid. It is a ball and socket joint. Anatomy of the Shoulder
Rehabilitation Guidelines for Shoulder Arthroscopy The true shoulder joint is called the glenohumeral joint and consists humeral head and the glenoid. It is a ball and socket joint. Anatomy of the Shoulder
FUNCTIONAL ANATOMY OF SHOULDER JOINT
 FUNCTIONAL ANATOMY OF SHOULDER JOINT ARTICULATION Articulation is between: The rounded head of the Glenoid cavity humerus and The shallow, pear-shaped glenoid cavity of the scapula. 2 The articular surfaces
FUNCTIONAL ANATOMY OF SHOULDER JOINT ARTICULATION Articulation is between: The rounded head of the Glenoid cavity humerus and The shallow, pear-shaped glenoid cavity of the scapula. 2 The articular surfaces
Rehabilitation Guidelines for Large Rotator Cuff Repair
 Rehabilitation Guidelines for Large Rotator Cuff Repair The true shoulder joint is called the glenohumeral joint and consists humeral head and the glenoid. It is a ball and socket joint. Anatomy of the
Rehabilitation Guidelines for Large Rotator Cuff Repair The true shoulder joint is called the glenohumeral joint and consists humeral head and the glenoid. It is a ball and socket joint. Anatomy of the
Rehabilitation Guidelines for Labral/Bankert Repair
 Rehabilitation Guidelines for Labral/Bankert Repair The true shoulder joint is called the glenohumeral joint and consists humeral head and the glenoid. It is a ball and socket joint. Anatomy of the Shoulder
Rehabilitation Guidelines for Labral/Bankert Repair The true shoulder joint is called the glenohumeral joint and consists humeral head and the glenoid. It is a ball and socket joint. Anatomy of the Shoulder
Tendinosis & Subacromial Impingement Syndrome. Gene Desepoli, LMT, D.C.
 Tendinosis & Subacromial Impingement Syndrome Gene Desepoli, LMT, D.C. What is the shoulder joint? Shoulder joint or shoulder region? There is an interrelatedness of all moving parts of the shoulder and
Tendinosis & Subacromial Impingement Syndrome Gene Desepoli, LMT, D.C. What is the shoulder joint? Shoulder joint or shoulder region? There is an interrelatedness of all moving parts of the shoulder and
Shoulder and Elbow ORTHOPAEDIC SYPMPOSIUM APRIL 8, 2017 DANIEL DOTY MD
 Shoulder and Elbow ORTHOPAEDIC SYPMPOSIUM APRIL 8, 2017 DANIEL DOTY MD Shoulder Articulations Glenohumeral Joint 2/3 total arc of motion Shallow Ball and Socket Joint Allows for excellent ROM Requires
Shoulder and Elbow ORTHOPAEDIC SYPMPOSIUM APRIL 8, 2017 DANIEL DOTY MD Shoulder Articulations Glenohumeral Joint 2/3 total arc of motion Shallow Ball and Socket Joint Allows for excellent ROM Requires
EVALUATION OF ACUTE SHOULDER INJURIES. Douglas J. Moran, MD Orthopaedic Sports Medicine
 EVALUATION OF ACUTE SHOULDER INJURIES Douglas J. Moran, MD Orthopaedic Sports Medicine DISCLOSURES None of the planners or presenters of this session have disclosed any conflict or commercial interest
EVALUATION OF ACUTE SHOULDER INJURIES Douglas J. Moran, MD Orthopaedic Sports Medicine DISCLOSURES None of the planners or presenters of this session have disclosed any conflict or commercial interest
Table 17: Provocative tests performed in a neutral shoulder position, i.e. the arm is at the patient s side.
 Page 1 of 1 Table 17: Provocative tests performed in a neutral shoulder position, i.e. the arm is at the patient s side. Description Click Image Positive Indicator Study Painful Arc of Abduction Also reported
Page 1 of 1 Table 17: Provocative tests performed in a neutral shoulder position, i.e. the arm is at the patient s side. Description Click Image Positive Indicator Study Painful Arc of Abduction Also reported
Orthopedic Physical Assessment with Special Tests Shoulder
 Orthopedic Physical Assessment with Special Tests Shoulder COURSE DESCRIPTION Detailed video demonstrations of tests and procedures common in musculoskeletal assessment are supplemented by high-quality
Orthopedic Physical Assessment with Special Tests Shoulder COURSE DESCRIPTION Detailed video demonstrations of tests and procedures common in musculoskeletal assessment are supplemented by high-quality
Shoulder Instability. Fig 1: Intact labrum and biceps tendon
 Shoulder Instability What is it? The shoulder joint is a ball and socket joint, with the humeral head (upper arm bone) as the ball and the glenoid as the socket. The glenoid (socket) is a shallow bone
Shoulder Instability What is it? The shoulder joint is a ball and socket joint, with the humeral head (upper arm bone) as the ball and the glenoid as the socket. The glenoid (socket) is a shallow bone
Labral Tears. Fig 1: Intact labrum and biceps tendon
 Labral Tears What is it? The shoulder joint is a ball and socket joint, with the humeral head (upper arm bone) as the ball and the glenoid as the socket. The glenoid (socket) is a shallow bone that is
Labral Tears What is it? The shoulder joint is a ball and socket joint, with the humeral head (upper arm bone) as the ball and the glenoid as the socket. The glenoid (socket) is a shallow bone that is
Shoulder Pain
 www.fisiokinesiterapia.biz Shoulder Pain Outline Shoulder Anatomy and Biomechanics Patient History and Pain Patterns Etiology and Differential Diagnoses Physical Examination Stepwise Clinical Approach
www.fisiokinesiterapia.biz Shoulder Pain Outline Shoulder Anatomy and Biomechanics Patient History and Pain Patterns Etiology and Differential Diagnoses Physical Examination Stepwise Clinical Approach
Pearson Education Limited Edinburgh Gate Harlow Essex CM20 2JE England and Associated Companies throughout the world
 Pearson Education Limited Edinburgh Gate Harlow Essex CM20 2JE England and Associated Companies throughout the world Visit us on the World Wide Web at: www.pearsoned.co.uk Pearson Education Limited 2014
Pearson Education Limited Edinburgh Gate Harlow Essex CM20 2JE England and Associated Companies throughout the world Visit us on the World Wide Web at: www.pearsoned.co.uk Pearson Education Limited 2014
MUSCLES OF SHOULDER REGION
 Dr Jamila EL Medany OBJECTIVES At the end of the lecture, students should: List the name of muscles of the shoulder region. Describe the anatomy of muscles of shoulder region regarding: attachments of
Dr Jamila EL Medany OBJECTIVES At the end of the lecture, students should: List the name of muscles of the shoulder region. Describe the anatomy of muscles of shoulder region regarding: attachments of
1-Apley scratch test.
 1-Apley scratch test. The patient attempts to touch the opposite scapula to test range of motion of the shoulder. 1-Testing abduction and external rotation( +ve sign touch the opposite scapula, -ve sign
1-Apley scratch test. The patient attempts to touch the opposite scapula to test range of motion of the shoulder. 1-Testing abduction and external rotation( +ve sign touch the opposite scapula, -ve sign
C. Christopher Smith, M.D. Associate Professor of Medicine Harvard Medical School Beth Israel Deaconess Medical Center
 Evaluation and Treatment of the Painful Shoulder in the Primary Care Setting C. Christopher Smith, M.D. Associate Professor of Medicine Harvard Medical School Beth Israel Deaconess Medical Center A 65-year-old
Evaluation and Treatment of the Painful Shoulder in the Primary Care Setting C. Christopher Smith, M.D. Associate Professor of Medicine Harvard Medical School Beth Israel Deaconess Medical Center A 65-year-old
Stefan C Muzin, MD PM&R Attending Physician, Beth Israel Deaconess Medical Center, Harvard Medical School Onsite Physiatrist, GE Aviation, Lynn, MA
 Stefan C Muzin, MD PM&R Attending Physician, Beth Israel Deaconess Medical Center, Harvard Medical School Onsite Physiatrist, GE Aviation, Lynn, MA Consultant, OEHN (Occupational and Environmental Network)
Stefan C Muzin, MD PM&R Attending Physician, Beth Israel Deaconess Medical Center, Harvard Medical School Onsite Physiatrist, GE Aviation, Lynn, MA Consultant, OEHN (Occupational and Environmental Network)
Shoulder Injury Evaluation.
 Shoulder Injury Evaluation www.fisiokinesiterapia.biz Basic Anatomy & Kinesiology 3 Bone Structures Clavicle Scapula Humerus Evaluation Principles Always follow a standard progression Determine the target
Shoulder Injury Evaluation www.fisiokinesiterapia.biz Basic Anatomy & Kinesiology 3 Bone Structures Clavicle Scapula Humerus Evaluation Principles Always follow a standard progression Determine the target
The examination of the painful knee. Maja K Artandi, MD, FACP Clinical Associate Professor of Medicine Stanford University
 The examination of the painful knee Maja K Artandi, MD, FACP Clinical Associate Professor of Medicine Stanford University Objectives of the talk By the end of this talk you will know The important anatomy
The examination of the painful knee Maja K Artandi, MD, FACP Clinical Associate Professor of Medicine Stanford University Objectives of the talk By the end of this talk you will know The important anatomy
Mr. Siva Chandrasekaran Orthopaedic Surgeon MBBS MSpMed MPhil (surg) FRACS. Rotator Cuff Tears
 FRACS. Rotator Cuff Tears") Rotator Cuff Tears A rotator cuff tear is a common cause of pain and disability among adults. A torn rotator cuff will weaken your shoulder. This means that many daily activities, like combing your hair
Rotator Cuff Tears A rotator cuff tear is a common cause of pain and disability among adults. A torn rotator cuff will weaken your shoulder. This means that many daily activities, like combing your hair
The Shoulder. Jill Inouye Primary Care Sports Medicine Family Medicine Resident School February 26, 2014
 The Shoulder Jill Inouye Primary Care Sports Medicine Family Medicine Resident School February 26, 2014 Objectives Review shoulder anatomy Explain and demonstrate shoulder physical exam Diagnosis and management
The Shoulder Jill Inouye Primary Care Sports Medicine Family Medicine Resident School February 26, 2014 Objectives Review shoulder anatomy Explain and demonstrate shoulder physical exam Diagnosis and management
SHOULDER IMPINGEMENT / ROTATOR CUFF TENDONITIS / SUBACROMIAL BURSITIS
 SHOULDER IMPINGEMENT / ROTATOR CUFF TENDONITIS / SUBACROMIAL BURSITIS The terms impingement, rotator cuff tendonitis, and subacromial bursitis, all refer to a spectrum of the same condition. Anatomy The
SHOULDER IMPINGEMENT / ROTATOR CUFF TENDONITIS / SUBACROMIAL BURSITIS The terms impingement, rotator cuff tendonitis, and subacromial bursitis, all refer to a spectrum of the same condition. Anatomy The
Upper Extremity Injuries in Youth Baseball: Causes and Prevention
 Upper Extremity Injuries in Youth Baseball: Causes and Prevention Biomechanics Throwing a baseball is an unnatural movement Excessively high forces are generated at the elbow and shoulder Throwing requires
Upper Extremity Injuries in Youth Baseball: Causes and Prevention Biomechanics Throwing a baseball is an unnatural movement Excessively high forces are generated at the elbow and shoulder Throwing requires
1. Occupation; Right or left handed, Age
 SHOULDER HISTORY 1. Occupation; Right or left handed, Age 2. Pain: Site. Any referred pain to the deltoid insertion Any localizing pain at Acromio-clavicular joint How long? Continuous or not Night pain
SHOULDER HISTORY 1. Occupation; Right or left handed, Age 2. Pain: Site. Any referred pain to the deltoid insertion Any localizing pain at Acromio-clavicular joint How long? Continuous or not Night pain
Returning the Shoulder Back to Optimal Function. Scapula. Clavicle. Humerus. Bones of the Shoulder (Osteology) Joints of the Shoulder (Arthrology)
 Joints of the Shoulder (Arthrology)") Returning the Shoulder Back to Optimal Function Sternum Clavicle Ribs Scapula Humerus Bones of the Shoulder (Osteology) By Rick Kaselj Clavicle Scapula Medial Left Anterior Clavicle Inferior View 20 degree
Returning the Shoulder Back to Optimal Function Sternum Clavicle Ribs Scapula Humerus Bones of the Shoulder (Osteology) By Rick Kaselj Clavicle Scapula Medial Left Anterior Clavicle Inferior View 20 degree
Soft Tissue Rheumatism. Elinor Mody, MD Chief, Division of Rheumatology Reliant Medical Group
 Soft Tissue Rheumatism Elinor Mody, MD Chief, Division of Rheumatology Reliant Medical Group Some problems are difficult, but diagnosing and treating most causes of joint pain are not! Common areas of
Soft Tissue Rheumatism Elinor Mody, MD Chief, Division of Rheumatology Reliant Medical Group Some problems are difficult, but diagnosing and treating most causes of joint pain are not! Common areas of
Vol 3, 2008 CEC ARTICLE: Special Medical Conditions Part 2: Shoulder Maintenance and Rehab C. Eggers
 Vol 3, 2008 CEC ARTICLE: Special Medical Conditions Part 2: Shoulder Maintenance and Rehab C. Eggers SHOULDER GIRDLE STABILIZATION Knowledge of the anatomy and biomechanics of the shoulder girdle is essential
Vol 3, 2008 CEC ARTICLE: Special Medical Conditions Part 2: Shoulder Maintenance and Rehab C. Eggers SHOULDER GIRDLE STABILIZATION Knowledge of the anatomy and biomechanics of the shoulder girdle is essential
Lab Workbook. ANATOMY Manual Muscle Testing Lower Trapezius Patient: prone
 ANATOMY Manual Muscle Testing Lower Trapezius Patient: prone Lab Workbook Fixation: place on hand below the scapula on the opposite side Test: adduction and depression of the scapula with lateral rotation
ANATOMY Manual Muscle Testing Lower Trapezius Patient: prone Lab Workbook Fixation: place on hand below the scapula on the opposite side Test: adduction and depression of the scapula with lateral rotation
ROTATOR CUFF INJURIES / IMPINGEMENT SYNDROME
 ROTATOR CUFF INJURIES / IMPINGEMENT SYNDROME Shoulder injuries are common in patients across all ages, from young, athletic people to the aging population. Two of the most common problems occur in the
ROTATOR CUFF INJURIES / IMPINGEMENT SYNDROME Shoulder injuries are common in patients across all ages, from young, athletic people to the aging population. Two of the most common problems occur in the
Diagnostic and Management Approach to the Painful Shoulder
 Diagnostic and Management Approach to the Painful Shoulder Introduction What conditions causing shoulder pain commonly present in General Practice? Subacromial impingement Rotator cuff tears AC joint pathology
Diagnostic and Management Approach to the Painful Shoulder Introduction What conditions causing shoulder pain commonly present in General Practice? Subacromial impingement Rotator cuff tears AC joint pathology
Shoulder Pain: Diagnosis and Management
 Shoulder Pain: Diagnosis and Management Thomas J. Gill, M.D. Director, Boston Sports Medicine and Research Institute Associate Professor of Orthopedic Surgery Tufts Medical School www.bostonsportsmedicine.com
Shoulder Pain: Diagnosis and Management Thomas J. Gill, M.D. Director, Boston Sports Medicine and Research Institute Associate Professor of Orthopedic Surgery Tufts Medical School www.bostonsportsmedicine.com
The Cryo/Cuff provides two functions: 1. Compression - to keep swelling down. 2. Ice Therapy - to keep swelling down and to help minimize pain. Patien
 The Cryo/Cuff provides two functions: 1. Compression - to keep swelling down. 2. Ice Therapy - to keep swelling down and to help minimize pain. Patients, for the most part, experience less pain and/or
The Cryo/Cuff provides two functions: 1. Compression - to keep swelling down. 2. Ice Therapy - to keep swelling down and to help minimize pain. Patients, for the most part, experience less pain and/or
CLINICAL EXAMINATION OF THE SHOULDER JOINT 대한신경근골격연구회 분당제생병원재활의학과 박준성
 CLINICAL EXAMINATION OF THE SHOULDER JOINT 대한신경근골격연구회 분당제생병원재활의학과 박준성 Clinical Examination of the Shoulder Good history, full clinical examination Detailed knowledge of the anatomy solve the majority of
CLINICAL EXAMINATION OF THE SHOULDER JOINT 대한신경근골격연구회 분당제생병원재활의학과 박준성 Clinical Examination of the Shoulder Good history, full clinical examination Detailed knowledge of the anatomy solve the majority of
The Shoulder. Jennifer R Marks, MD
 The Shoulder Jennifer R Marks, MD Shoulder Anatomy Skeletal & ligamentous components: The joint is comprised of a confluence of Scapula Clavicle Humerus https://www.shoulderdoc.co.uk/article/ http/ www.shoulderdoc.co.uk/article/117777
The Shoulder Jennifer R Marks, MD Shoulder Anatomy Skeletal & ligamentous components: The joint is comprised of a confluence of Scapula Clavicle Humerus https://www.shoulderdoc.co.uk/article/ http/ www.shoulderdoc.co.uk/article/117777
ROTATOR CUFF TENDONITIS
 Daniel P. Duggan, D.O. The Sports Clinic 23961 Calle de la Magdalena, Suite 229 Laguna Hills, CA 92653 Phone: (949) 581-7001 Fax: (949) 581-8410 http://orthodoc.aaos.org/danielduggando The shoulder is
Daniel P. Duggan, D.O. The Sports Clinic 23961 Calle de la Magdalena, Suite 229 Laguna Hills, CA 92653 Phone: (949) 581-7001 Fax: (949) 581-8410 http://orthodoc.aaos.org/danielduggando The shoulder is
Chronic Shoulder Disorders
 Chronic Shoulder Disorders Dr. Mustafa Elsingergy Consultant orthopedic surgeon Dallah Hospita Prof. Mamoun Kremli Almaarefa Medical College Contents INTRINSIC Shoulder Pain Due to causes in the shoulder
Chronic Shoulder Disorders Dr. Mustafa Elsingergy Consultant orthopedic surgeon Dallah Hospita Prof. Mamoun Kremli Almaarefa Medical College Contents INTRINSIC Shoulder Pain Due to causes in the shoulder
Recurrent Shoulder Dislocation.
 Recurrent Shoulder Dislocation www.fisiokinesiterapia.biz Anatomy of the Shoulder Shoulder Dislocations Case Study Rehabilitation Pick List Anatomy of the Shoulder Articulations Sternoclavicular Acromioclavicular
Recurrent Shoulder Dislocation www.fisiokinesiterapia.biz Anatomy of the Shoulder Shoulder Dislocations Case Study Rehabilitation Pick List Anatomy of the Shoulder Articulations Sternoclavicular Acromioclavicular
SHOULDER INSTABILITY
 SHOULDER INSTABILITY Your shoulder is the most flexible joint in your body, allowing you to throw fastballs, lift a heavy suitcase, scratch your back, and reach in almost any direction. Your shoulder joint
SHOULDER INSTABILITY Your shoulder is the most flexible joint in your body, allowing you to throw fastballs, lift a heavy suitcase, scratch your back, and reach in almost any direction. Your shoulder joint
Rotator Cuff Tears. Anatomy. Description
 Rotator Cuff Tears A rotator cuff tear is a common cause of pain and disability among adults. In 2008, close to 2 million people in the United States went to their doctors because of a rotator cuff problem.
Rotator Cuff Tears A rotator cuff tear is a common cause of pain and disability among adults. In 2008, close to 2 million people in the United States went to their doctors because of a rotator cuff problem.
Sick Call Screener Course
 Sick Call Screener Course Musculoskeletal System Upper Extremities (2.7) 2.7-2-1 Enabling Objectives 1.46 Utilize the knowledge of musculoskeletal system anatomy while assessing a patient with a musculoskeletal
Sick Call Screener Course Musculoskeletal System Upper Extremities (2.7) 2.7-2-1 Enabling Objectives 1.46 Utilize the knowledge of musculoskeletal system anatomy while assessing a patient with a musculoskeletal
Disclaimer. Evaluation & Treatment of Shoulder and Elbow Pain in the Adult Patient. Objectives. Anatomy
 Evaluation & Treatment of Shoulder and Elbow Pain in the Adult Patient William T. Crowe, RN-C, FNP, MSN, MBA Disclaimer! I, William T Crowe, have relevant financial relationships to be discussed, directly
Evaluation & Treatment of Shoulder and Elbow Pain in the Adult Patient William T. Crowe, RN-C, FNP, MSN, MBA Disclaimer! I, William T Crowe, have relevant financial relationships to be discussed, directly
Anatomy Your shoulder is made up of three bones: your upper arm bone (humerus), your shoulder blade (scapula), and your collarbone (clavicle).
, your shoulder blade (scapula), and your collarbone (clavicle).") Shoulder Impingement/Rotator Cuff Tendinitis One of the most common physical complaints is shoulder pain. Your shoulder is made up of several joints combined with tendons and muscles that allow a great
Shoulder Impingement/Rotator Cuff Tendinitis One of the most common physical complaints is shoulder pain. Your shoulder is made up of several joints combined with tendons and muscles that allow a great
.org. Rotator Cuff Tears. Anatomy. Description
 Rotator Cuff Tears Page ( 1 ) A rotator cuff tear is a common cause of pain and disability among adults. In 2008, close to 2 million people in the United States went to their doctors because of a rotator
Rotator Cuff Tears Page ( 1 ) A rotator cuff tear is a common cause of pain and disability among adults. In 2008, close to 2 million people in the United States went to their doctors because of a rotator
ANATOMY / BIOMECHANICS LONG HEAD OF BICEPS ATTACHES AT THE SUPERIOR GLENOIDAL TUBERCLE WITH THE LABRUM FIBROCARTILAGINOUS TISSUE IF THERE IS A TORN SU
 SLAP LESIONS Management Of Glenoid Labrum Injuries INTRODUCTION First described by Andrews AJSM 85 Throwers 60% Normal Variants Sublabral Foramen Buford Complex Meniscoid Snyder Arth. 1990 termed SLAP
SLAP LESIONS Management Of Glenoid Labrum Injuries INTRODUCTION First described by Andrews AJSM 85 Throwers 60% Normal Variants Sublabral Foramen Buford Complex Meniscoid Snyder Arth. 1990 termed SLAP
Rehabilitation Guidelines for Shoulder Arthroscopy
 UW HEALTH SPORTS REHABILITATION Rehabilitation Guidelines for Shoulder Arthroscopy Front View Acromion Supraspinatus Back View Supraspinatus Long head of bicep Type I Infraspinatus Short head of bicep
UW HEALTH SPORTS REHABILITATION Rehabilitation Guidelines for Shoulder Arthroscopy Front View Acromion Supraspinatus Back View Supraspinatus Long head of bicep Type I Infraspinatus Short head of bicep
Biceps Tenodesis Protocol
 Biceps Tenodesis Protocol A biceps tenodesis procedure involves cutting of the long head of the biceps just prior to its insertion on the superior labrum and then anchoring the tendon along its anatomical
Biceps Tenodesis Protocol A biceps tenodesis procedure involves cutting of the long head of the biceps just prior to its insertion on the superior labrum and then anchoring the tendon along its anatomical
Shoulder Impingement Rehabilitation Recommendations
 Shoulder Impingement Rehabilitation Recommendations The following protocol can be utilized for conservative care of shoulder impingement as well as post- operative subacromial decompression (SAD) surgery.
Shoulder Impingement Rehabilitation Recommendations The following protocol can be utilized for conservative care of shoulder impingement as well as post- operative subacromial decompression (SAD) surgery.
Shoulder Exam Break-out with Case Highlights. Teri Metcalf McCambridge, MD, FAAP, CAQSM Assistant Professor of Pediatrics and Orthopedics University
 Shoulder Exam Break-out with Case Highlights. Teri Metcalf McCambridge, MD, FAAP, CAQSM Assistant Professor of Pediatrics and Orthopedics University of Maryland School of Medicine Faculty Disclosure Information
Shoulder Exam Break-out with Case Highlights. Teri Metcalf McCambridge, MD, FAAP, CAQSM Assistant Professor of Pediatrics and Orthopedics University of Maryland School of Medicine Faculty Disclosure Information
Structure and Function of the Bones and Joints of the Shoulder Girdle
 Structure and Function of the Bones and Joints of the Shoulder Girdle LEARNING OBJECTIVES: At the end of this laboratory exercise the student will be able to: Palpate the important skeletal landmarks of
Structure and Function of the Bones and Joints of the Shoulder Girdle LEARNING OBJECTIVES: At the end of this laboratory exercise the student will be able to: Palpate the important skeletal landmarks of
REMINDER. an exercise program. Senior Fitness Obtain medical clearance and physician s release prior to beginning
 Functional Forever: Exercise for Independent Living REMINDER Obtain medical clearance and physician s release prior to beginning an exercise program for clients with medical or orthopedic concerns. What
Functional Forever: Exercise for Independent Living REMINDER Obtain medical clearance and physician s release prior to beginning an exercise program for clients with medical or orthopedic concerns. What
Evaluating shoulder injuries in primary care Bethany Reed, MSn, AGPCNP-BC One Medical Group
 Evaluating shoulder injuries in primary care Bethany Reed, MSn, AGPCNP-BC One Medical Group Disclosures There has been no commercial support or sponsorship for this program. The planners and presenters
Evaluating shoulder injuries in primary care Bethany Reed, MSn, AGPCNP-BC One Medical Group Disclosures There has been no commercial support or sponsorship for this program. The planners and presenters
UPPER EXTREMITY INJURIES. Recognizing common injuries to the upper extremity
 UPPER EXTREMITY INJURIES Recognizing common injuries to the upper extremity ANATOMY BONES Clavicle Scapula Spine of the scapula Acromion process Glenoid fossa/cavity Humerus Epicondyles ANATOMY BONES Ulna
UPPER EXTREMITY INJURIES Recognizing common injuries to the upper extremity ANATOMY BONES Clavicle Scapula Spine of the scapula Acromion process Glenoid fossa/cavity Humerus Epicondyles ANATOMY BONES Ulna
DIFFERENTIAL DIAGNOSIS: Looking for the causes of impingement
 DIFFERENTIAL DIAGNOSIS: Looking for the causes of Ann Cools, PT, PhD Ghent University - Belgium Dept of Rehabilitation Sciences & Physiotherapy Ann.Cools@UGent.be «thinking about.» Which special tests
DIFFERENTIAL DIAGNOSIS: Looking for the causes of Ann Cools, PT, PhD Ghent University - Belgium Dept of Rehabilitation Sciences & Physiotherapy Ann.Cools@UGent.be «thinking about.» Which special tests
Gross Anatomy Questions That Should be Answerable After October 27, 2017
 Gross Anatomy Questions That Should be Answerable After October 27, 2017 1. The inferior angle of the scapula of a woman who was recently in an automobile accident seems to protrude making a ridge beneath
Gross Anatomy Questions That Should be Answerable After October 27, 2017 1. The inferior angle of the scapula of a woman who was recently in an automobile accident seems to protrude making a ridge beneath
Evidence- Based Examination of the Shoulder Presented by Eric Hegedus, PT, DPT, MHSC, OCS, CSCS Practice Sessions/Skill Check- offs
 Evidence- Based Examination of the Shoulder Practice Session & Skills Check- offs Evidence- Based Examination of the Shoulder Presented by Eric Hegedus, PT, DPT, MHSC, OCS, CSCS Practice Sessions/Skill
Evidence- Based Examination of the Shoulder Practice Session & Skills Check- offs Evidence- Based Examination of the Shoulder Presented by Eric Hegedus, PT, DPT, MHSC, OCS, CSCS Practice Sessions/Skill
Evaluation of the Knee and Shoulder
 Evaluation of the Knee and Shoulder Karen J. Boselli, MD Northeast Regional Nurse Practitioner Conference May 2018 Knee Overview History Examination Top 5 diagnoses When to image When to refer Pain most
Evaluation of the Knee and Shoulder Karen J. Boselli, MD Northeast Regional Nurse Practitioner Conference May 2018 Knee Overview History Examination Top 5 diagnoses When to image When to refer Pain most
Connects arm to thorax 3 joints. Glenohumeral joint Acromioclavicular joint Sternoclavicular joint
 Connects arm to thorax 3 joints Glenohumeral joint Acromioclavicular joint Sternoclavicular joint Scapula Elevation Depression Protraction (abduction) Retraction (adduction) Downward Rotation Upward Rotation
Connects arm to thorax 3 joints Glenohumeral joint Acromioclavicular joint Sternoclavicular joint Scapula Elevation Depression Protraction (abduction) Retraction (adduction) Downward Rotation Upward Rotation
Musculoskeletal Ultrasound. Technical Guidelines SHOULDER
 Musculoskeletal Ultrasound Technical Guidelines SHOULDER 1 Although patient s positioning for shoulder US varies widely across different Countries and Institutions reflecting multifaceted opinions and
Musculoskeletal Ultrasound Technical Guidelines SHOULDER 1 Although patient s positioning for shoulder US varies widely across different Countries and Institutions reflecting multifaceted opinions and
Anterior Stabilization of the Shoulder: Distal Tibial Allograft
 Anterior Stabilization of the Shoulder: Distal Tibial Allograft Name: Diagnosis: Date: Date of Surgery: Phase I Immediate Post Surgical Phase (approximately Weeks 1-3) Minimize shoulder pain and inflammatory
Anterior Stabilization of the Shoulder: Distal Tibial Allograft Name: Diagnosis: Date: Date of Surgery: Phase I Immediate Post Surgical Phase (approximately Weeks 1-3) Minimize shoulder pain and inflammatory
SHOULDER PROBLEMS & ARTHROSCOPIC MANAGEMENT
 SHOULDER PROBLEMS & ARTHROSCOPIC MANAGEMENT DR.SHEKHAR SRIVASTAV Sr. Consultant-KNEE & SHOULDER Arthroscopy Sant Parmanand Hospital,Delhi Peculiarities of Shoulder Elegant piece of machinery It has the
SHOULDER PROBLEMS & ARTHROSCOPIC MANAGEMENT DR.SHEKHAR SRIVASTAV Sr. Consultant-KNEE & SHOULDER Arthroscopy Sant Parmanand Hospital,Delhi Peculiarities of Shoulder Elegant piece of machinery It has the
ACTIVE AGING.
 Shoulder Pain Rehabilitation Protocol Rotator Cuff Syndrome Shoulder impingement The Resistance Chair Solution Shoulder Impingement a. Shoulder impingement is one of the most common causes of shoulder
Shoulder Pain Rehabilitation Protocol Rotator Cuff Syndrome Shoulder impingement The Resistance Chair Solution Shoulder Impingement a. Shoulder impingement is one of the most common causes of shoulder
Frozen Shoulder Syndrome Rehabilitation Using the Resistance Chair
 Frozen Shoulder Syndrome Rehabilitation Using the Resistance Chair General Information Frozen shoulder is a condition where the shoulder joint (glenohumeral joint) gradually becomes stiff, resulting in
Frozen Shoulder Syndrome Rehabilitation Using the Resistance Chair General Information Frozen shoulder is a condition where the shoulder joint (glenohumeral joint) gradually becomes stiff, resulting in
Scapular and Deltoid Regions
 M1 Gross and Developmental Anatomy Scapular and Deltoid Regions Dr. Peters 1 Outline I. Skeleton of the Shoulder and Attachment of the Upper Extremity to Trunk II. Positions and Movements of the Scapula
M1 Gross and Developmental Anatomy Scapular and Deltoid Regions Dr. Peters 1 Outline I. Skeleton of the Shoulder and Attachment of the Upper Extremity to Trunk II. Positions and Movements of the Scapula
REMINDER. Obtain medical clearance and physician s release prior to beginning an exercise program for clients with medical or orthopedic concerns
 Understanding Shoulder Dysfunction REMINDER Obtain medical clearance and physician s release prior to beginning an exercise program for clients with medical or orthopedic concerns What is a healthy shoulder?
Understanding Shoulder Dysfunction REMINDER Obtain medical clearance and physician s release prior to beginning an exercise program for clients with medical or orthopedic concerns What is a healthy shoulder?
2015 OPSC Annual Convention. syllabus. February 4-8, 2015 Hyatt Regency Mission Bay San Diego, California
 2015 OPSC Annual Convention syllabus February 4-8, 2015 Hyatt Regency Mission Bay San Diego, California THURSDAY, FEBRUARY 5, 2015: 3:30pm - 4:30pm The Shoulder: 2 View or Not 2 View * Presented by Alexandra
2015 OPSC Annual Convention syllabus February 4-8, 2015 Hyatt Regency Mission Bay San Diego, California THURSDAY, FEBRUARY 5, 2015: 3:30pm - 4:30pm The Shoulder: 2 View or Not 2 View * Presented by Alexandra
Exploring the Rotator Cuff
 Exploring the Rotator Cuff Improving one s performance in sports and daily activity is a factor of neuromuscular efficiency and metabolic enhancements. To attain proficiency, reaction force must be effectively
Exploring the Rotator Cuff Improving one s performance in sports and daily activity is a factor of neuromuscular efficiency and metabolic enhancements. To attain proficiency, reaction force must be effectively
Biceps Tenotomy Protocol
 Biceps Tenotomy Protocol A biceps tenotomy procedure involves cutting of the long head of the biceps just prior to its insertion on the superior labrum. A biceps tenotomy is typically done when there is
Biceps Tenotomy Protocol A biceps tenotomy procedure involves cutting of the long head of the biceps just prior to its insertion on the superior labrum. A biceps tenotomy is typically done when there is
Chiropractic Healthcare
 ebook 2 Chiropractic Healthcare Four symptoms explained Introduction 3 Chapter 1 Carpal Tunnel Syndrome 4 Chapter 2 Common Shoulder Pain Issues 8 Chapter 3 Headaches and Chiropractic Care 14 Chapter 4
ebook 2 Chiropractic Healthcare Four symptoms explained Introduction 3 Chapter 1 Carpal Tunnel Syndrome 4 Chapter 2 Common Shoulder Pain Issues 8 Chapter 3 Headaches and Chiropractic Care 14 Chapter 4
I (and/or my co-authors) have something to disclose.
 have something to disclose.") Shoulder Anatomy And Biomechanics Nikhil N Verma, MD Director of Sports Medicine Professor, Department of Orthopedics Rush University Team Physician, Chicago White Sox and Bulls I (and/or my co-authors)
Shoulder Anatomy And Biomechanics Nikhil N Verma, MD Director of Sports Medicine Professor, Department of Orthopedics Rush University Team Physician, Chicago White Sox and Bulls I (and/or my co-authors)
Shoulder Trauma (Fractures and Dislocations)
") Shoulder Trauma (Fractures and Dislocations) Trauma to the shoulder is common. Injuries range from a separated shoulder resulting from a fall onto the shoulder to a high-speed car accident that fractures
Shoulder Trauma (Fractures and Dislocations) Trauma to the shoulder is common. Injuries range from a separated shoulder resulting from a fall onto the shoulder to a high-speed car accident that fractures
IMPINGEMENT-TESTSTESTS
 «thinking about.» DIFFERENTIAL DIAGNOSIS: Looking for the causes of Which special tests do you use in your shoulder examination? Ann Cools, PT, PhD Ghent University - Belgium Dept of Rehabilitation Sciences
«thinking about.» DIFFERENTIAL DIAGNOSIS: Looking for the causes of Which special tests do you use in your shoulder examination? Ann Cools, PT, PhD Ghent University - Belgium Dept of Rehabilitation Sciences
Philip Bayliss St Albans Osteopathy
 Philip Bayliss St Albans Osteopathy 43 Thames Street, St Albans, Christchurch 8013 Phone: (03) 356 1353 Website: philip-bayliss.com Subacromial (Shoulder) Bursitis 1 Experts estimate that 65% of people
Philip Bayliss St Albans Osteopathy 43 Thames Street, St Albans, Christchurch 8013 Phone: (03) 356 1353 Website: philip-bayliss.com Subacromial (Shoulder) Bursitis 1 Experts estimate that 65% of people
The Upper Limb II. Anatomy RHS 241 Lecture 11 Dr. Einas Al-Eisa
 The Upper Limb II Anatomy RHS 241 Lecture 11 Dr. Einas Al-Eisa Sternoclavicular joint Double joint.? Each side separated by intercalating articular disc Grasp the mid-portion of your clavicle on one side
The Upper Limb II Anatomy RHS 241 Lecture 11 Dr. Einas Al-Eisa Sternoclavicular joint Double joint.? Each side separated by intercalating articular disc Grasp the mid-portion of your clavicle on one side
Ms. Ruth A. Delaney, MB BCh BAO, MMedSc, MRCS
 Ms. Ruth A. Delaney, MB BCh BAO, MMedSc, MRCS Consultant Orthopaedic Surgeon, Shoulder Specialist. +353 1 5262335 ruthdelaney@sportssurgeryclinic.com Modified from the protocol developed at Boston Shoulder
Ms. Ruth A. Delaney, MB BCh BAO, MMedSc, MRCS Consultant Orthopaedic Surgeon, Shoulder Specialist. +353 1 5262335 ruthdelaney@sportssurgeryclinic.com Modified from the protocol developed at Boston Shoulder
Musculoskeletal Examination Benchmarks
 Musculoskeletal Examination Benchmarks _ The approach to examining the musculoskeletal system is the same no matter what joint or limb is being examined. The affected and contralateral region should both
Musculoskeletal Examination Benchmarks _ The approach to examining the musculoskeletal system is the same no matter what joint or limb is being examined. The affected and contralateral region should both
Evaluation of Shoulder Pain Tim Garner, PT, OCS. Disclaimer
 Evaluation of Shoulder Pain Tim Garner, PT, OCS Disclaimer I do not have any relevant financial relationships to be discussed, directly or indirectly, referred to or illustrated, with or without recognition
Evaluation of Shoulder Pain Tim Garner, PT, OCS Disclaimer I do not have any relevant financial relationships to be discussed, directly or indirectly, referred to or illustrated, with or without recognition
SUPERIOR LABRAL REPAIRS
 LOURDES MEDICAL ASSOCIATES Sean Mc Millan, DO Director of Orthopaedic Sports Medicine & Arthroscopy 2103 Burlington-Mount Holly Rd Burlington, NJ 08016 (609) 747-9200 (office) (609) 747-1408 (fax) http://orthodoc.aaos.org/drmcmillan
LOURDES MEDICAL ASSOCIATES Sean Mc Millan, DO Director of Orthopaedic Sports Medicine & Arthroscopy 2103 Burlington-Mount Holly Rd Burlington, NJ 08016 (609) 747-9200 (office) (609) 747-1408 (fax) http://orthodoc.aaos.org/drmcmillan
Rehabilitation of Overhead Shoulder Injuries
 Rehabilitation of Overhead Shoulder Injuries 16 th Annual Primary Care Orthopaedic & Sports Medicine Symposium January 29, 2016 Jeremy Sherman, PT, MPT Disclosures No financial disclosures to note. Jeremy
Rehabilitation of Overhead Shoulder Injuries 16 th Annual Primary Care Orthopaedic & Sports Medicine Symposium January 29, 2016 Jeremy Sherman, PT, MPT Disclosures No financial disclosures to note. Jeremy
Distal Biceps Repair/Reconstruction Protocol
 SPORTS & ORTHOPAEDIC SPECIALISTS Distal Biceps Repair/Reconstruction Protocol 6-10 visits over 4-6 months Maintain shoulder ROM while immobilized during early phase of healing During recovery, pulling
SPORTS & ORTHOPAEDIC SPECIALISTS Distal Biceps Repair/Reconstruction Protocol 6-10 visits over 4-6 months Maintain shoulder ROM while immobilized during early phase of healing During recovery, pulling
OCCUPATIONAL SHOULDER DISORDERS
 OCCUPATIONAL SHOULDER DISORDERS Mark A. Greenfield D.O., F.A.O.A.O. Orthopaedic Surgery May 13, 2016 CREDENTIALS Orthopaedic Surgeon Fellowship Trained Board Certified Licensed to practice in AZ Published
OCCUPATIONAL SHOULDER DISORDERS Mark A. Greenfield D.O., F.A.O.A.O. Orthopaedic Surgery May 13, 2016 CREDENTIALS Orthopaedic Surgeon Fellowship Trained Board Certified Licensed to practice in AZ Published
SHOULDER JOINT ANATOMY AND KINESIOLOGY
 SHOULDER JOINT ANATOMY AND KINESIOLOGY SHOULDER JOINT ANATOMY AND KINESIOLOGY The shoulder joint, also called the glenohumeral joint, consists of the scapula and humerus. The motions of the shoulder joint
SHOULDER JOINT ANATOMY AND KINESIOLOGY SHOULDER JOINT ANATOMY AND KINESIOLOGY The shoulder joint, also called the glenohumeral joint, consists of the scapula and humerus. The motions of the shoulder joint
Nonoperative Treatment For Rotator Cuff Tendinitis/ Partial Thickness Tear Dr. Trueblood
 Nonoperative Treatment For Rotator Cuff Tendinitis/ Partial Thickness Tear Dr. Trueblood Relieving Pain Patients who present with SIS will have shoulder pain that is exacerbated with overhead activities.
Nonoperative Treatment For Rotator Cuff Tendinitis/ Partial Thickness Tear Dr. Trueblood Relieving Pain Patients who present with SIS will have shoulder pain that is exacerbated with overhead activities.
INSTRUCTION MANUAL FOR THE FLEXTEND AC Exercise System for The Acromioclavicular (AC) / Shoulder Joint
 / Shoulder Joint") INSTRUCTION MANUAL FOR THE FLEXTEND AC Exercise System for The Acromioclavicular (AC) / Shoulder Joint FLEXTEND -AC: Congratulations! You have chosen to use the FLEXTEND -AC Upper Extremity Training System,
INSTRUCTION MANUAL FOR THE FLEXTEND AC Exercise System for The Acromioclavicular (AC) / Shoulder Joint FLEXTEND -AC: Congratulations! You have chosen to use the FLEXTEND -AC Upper Extremity Training System,