Joint Injection Workshop
|
|
|
- Madeleine Wilkinson
- 5 years ago
- Views:
Transcription
1 Joint Injection Workshop Annual Clinical Day in Family Medicine May 13, 2015 Dr. Vikram Dalal MD CCFP(EM) FCFP Dr. Bryan Lemenchick MD CCFP DipSportMed
2 Faculty / Presenter Disclosure Faculty: Dr. Vikram Dalal Relationship with Commercial Interstes: NONE
3 Faculty / Presenter Disclosure Faculty: Dr. Bryan Lemenchick Relationship with Commercial Interstes: NONE
4 Disclosure of Commercial Support This program has received NO financial support This program has received IN-KIND support from Tribute Pharmaceuticals in the form of injection models Potential Conflict(s) of interest: NONE
5 Mitigating Potential Bias NOT APPLICABLE
6 Objectives To Educate Family Physicians on Evidence base for injection therapy The drugs used The bony landmarks for common joint/bursa/soft tissue injections Correct techniques to do joint injections
7 What Providers Need to Know About Joint Injection and Aspiration Relatively simple procedure Complications are rare Injection/arthrocentesis can provide diagnosis, pain relief, reduce joint damage - Liquid biopsy of joint - Useful information can be provided by relatively inexpensive tests - Can help differentiate inflammatory from noninflammatory arthritis Judicious use of anesthetics and steroids may be safer than systemic medications Summary: There are often more reasons for doing than not
8 Indications for Joint Injection /Aspiration Diagnostic: Acute inflammatory arthritis (24-48hrs) in a patient who has never had these symptoms before Acute effusion in the setting of fever, chills, or presence of infection at another site Acute effusion in the setting of trauma Prior to committing patients to long-term, expensive or toxic therapy Therapeutic: To facilitate a more tolerable musculoskeletal exam (ie pain control) To suppress inflammation in one or two isolated joints Adjuvant therapy to a few joints resistant to systemic therapy To facilitate a rehabilitative physical therapy program To support a patient with active joint inflammation pending the effects of systemic therapy To remove exudative fluid from a septic joint To relieve pain in a swollen joint
9 Conditions Likely to be Improved by Joint or Periarticular Injections Rheumatoid arthritis Seronegative spondyloarthropathies Crystal induced arthritis Carpal tunnel Bursitis Tenosynovitis / tendinosis Adhesive capsulitis Osteoarthritis
10 Contraindications to Joint Injection/Aspiration Absolute: - Sepsis / Cellulitis - Hypersensitivity - Fracture - Arthroplasty - Previous severe steroid flare - Reluctant patient - Uninformed patient - Injection into critical wt bearing tendons Relative: - Uncontrolled Diabetes - Immunosuppression - Bleeding disorder - Anticoagulants* - > 3 prev. steroid injection in a major wt bearing joint within the preceding year - Excessive anxiety - Prosthetic Joint *Therapeutic INR okay, NOACs variable but okay (Ahmed 2012)





11 Technique: Equipment
12 Technique: Preparation - Discuss with patient option of injection and alternative treatments applicable to condition - Obtain informed consent - Check names on consent and expiration dates - Place in comfortable position - Define / mark anatomy
 - Isopropyl alcohol similar to")
 - Inject using Aseptic Technique - Confident Approach - Stretch skin - Needle")
13 Technique: Site Prep - Skin Preparation - Infection is rare - Reported incidence unknown, but varies from 1:3,000 to 1:50,000 (Baima, J, 2008) - Isopropyl alcohol similar to chlorhexidine in killing skin flora (Cawley et al., 1992) - Inject using Aseptic Technique - Confident Approach - Stretch skin - Needle insertion depending on site and type of injection
14 Technique: Aftercare - Avoid excessive activities for hours - Gradual return - Apply ice for min, 2-3 times/day - NSAIDS / Acetaminophen for first hours (PRN) - Watch for steroid flare - +/- Follow-up
15 Steroid Use Commonly used in ambulatory care settings by family doctors, orthopedic surgeons, and rheumatologists Conditions warranting injection (Hill JJ (1989); McNabb J (2010)) - Epicondylitis (93%) - Shoulder Pathologies (91%) - Greater trochanteric bursitis (91%) - De Quervain s tendinopathy (87%) - Bicipital tendonitis (81%) - Osteoarthritis (knee) (92%)

16 Corticosteroid Function - Corticosteroids have anti-inflammatory and immunosuppressive effect (Pekarek et al, 2011) - Alter movement and function of leukocytes - Reduce vascular permeability in inflamed areas - Reduce prostaglandin synthesis Serve to reduce erythema, swelling, heat, and tenderness of inflamed joints Also increase the viscosity and hyaluronate concentration in synovial fluid
17 Steroids - Physiology - Stabilizes lysosomal membranes of inflammatory cells - Decreases local vascular permeability - Alters neutrophil chemotaxis and function - Passes through cell membranes and binds to nuclear steroid receptors - Where they influence RNA transcription and subsequent protein production
18 Guide to Glucocorticoids for Intra-articular and Soft tissue Injections
19 The Drugs Few studies have assessed the comparative efficacy of different corticosteroid injections for various articular and peri-articular disorders Physician s choice of specific corticosteroid for injection is linked to the region where the physician was trained, as opposed to specific evidence based practice (Wittich et al., 2009) What we know: Triamcinolone hexacetonide had faster pain relief than methylprednisolone for knee RA at day 7 and knee OA at 3 weeks; both had similar long term efficacy (Garg et al., 2014) Triamcinolone acetate and methylprednisolone seem to have similar efficacy for knee and shoulder injections (Garg et al., 2014)


20 Local Anesthetics Typically a local anesthetic agent is combined with steroid agents 1. Analgesia: - Decrease nerve conduction through the blockade of sodium channels, which disrupts axonal nerve conduction Lidocaine: - Rapid onset (minutes) - Short duration (60-90 min) Bupivicaine - Slower onset (30 min) - Longer duration 96-8 hours) Buffering: - Sodium bicarbonate 2. Diagnostic: - pain relief confirms pathology and correct administration 3. Volume Distribution / Dilutional: - dilutes the steroid (reduced chance skin atrophy) - increases the distribution of the agent to the treated area
21 What Patients (and Providers) Need to Know About Joint Injection and Aspiration Relief will typically last weeks or longer No ligamentous or tendon structure should be injected directly Activity modification following injections of steroid is uncertain Maximal number of injections and the required period between injections have not been determined (Nichols, A (2005); Pfenninger, JL (2010))
, depigmenation (0.8%), localized erythema and warmth (0.7%), and facial flushing (0.")
 - Post injection flare (2-5%) Infection 18/250,000 injections (0.")
22 What Patients (and Providers) Need to Know about Joint Injections *Dietzel, D (2004); Nepple J (2009); Wang AA (2006); Pfenninger JL (2010) In a meta-analysis summarizing 25+ studies, a 5.5% complication rate noted - Most common side effects included skin atrophy (2.4%), depigmenation (0.8%), localized erythema and warmth (0.7%), and facial flushing (0.6%) - Post-injection pain was noted in up to 9% of patients - Prolonged and repeated usage may increase the risk of complications and systemic side effects (hence at times limited to 3 injections within 12 months) - Post injection flare (2-5%) Infection 18/250,000 injections (0.072%) In diabetic patients, hyperglycemia has been shown to persists up to 5 days after single soft tissue injection
23 Typical Injection/Aspiration Procedure Determine the medical diagnosis and consider relevant differential diagnosis Discuss the proposed procedure and alternatives with the patient Obtain written informed consent from the patient Collect and prepare the required materials Correctly position the patient for the procedure Identify and mark the anatomic landmarks and injection site with ink Do not allow the patient to move the affected area from the time that the marks are placed until after the procedure is completed Press firmly on the skin with the retracted tip of a ballpoint pen to further identify the injection site Prepare the site for injection by cleansing with a topical antimicrobial agene (providine-iodine and/or alcohol swab) If using providine, allow to dry for full antibacterial effect Provide local anesthesia as indicated***
24 Typical Injection/Aspiration Procedure Using the no-touch technique, introduce the needle at the injection site and advance into the treatment area Aspirate fluid (optional) using a 18 or 20-g needle and send it for laboratory examination if indicated If injecting corticosteroid immediately following aspiration, do not remove the needle from the joint or bursa; In this case, grasp the needle hub firmly (with hemostat clamp if necessary), twist off the original syringe, and then immediately attach the second syringe that contains the corticosteroid Always aspirate before injection to avoid intravascular administration Inject corticosteroid solution into the treatment area - If not aspirating then use 25-g needle - Do not inject the medication against resistance Withdraw the needle Apply direct pressure over the injection site with a gauze pad Apply an adhesive dressing Provide the patient with specific post-injection instructions

25 Shoulder Complex - A complicated anatomical and biomechanical joint - Actually multiple joints - Static and dynamic stabilizers - Bursitis, tendinosis, adhesive capsulitis, impingement syndrome, calcific tendinopathy
: - 1cc (40mg) depomedrol + 2cc xylocaine AC Joint (Attic): - 1cc (40mg) depomedrol + 1cc")
26 Shoulder Complex Anatomy: No major arteries or nerves in the technique Examples: GH Joint (Ground Floor): cc (40-80mg) depomedrol + 3-4cc xylocaine Subacromial bursa (First Floor): - 1cc (40mg) depomedrol + 2cc xylocaine AC Joint (Attic): - 1cc (40mg) depomedrol + 1cc xylocaine
27 Shoulder Glenohumeral joint The Ground Floor

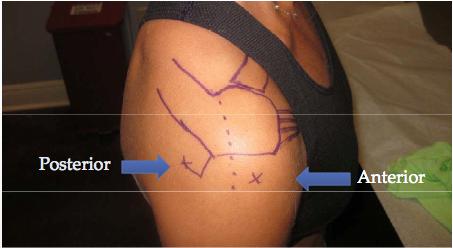
28 Shoulder Subacromial Bursa (1 st Floor)


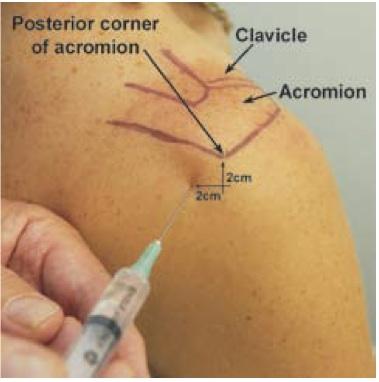
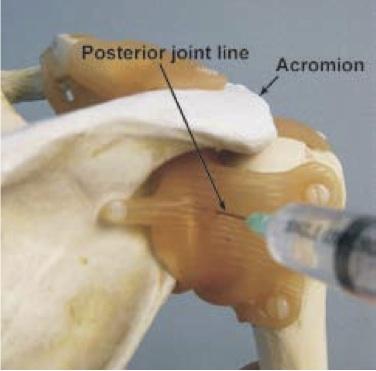
29 Shoulder - The AC joint (The Attic)
 - Approaches: - Anterior - Medial Retropatellar - Lateral Retropatellar - Suprapatellar (done for suprapatellar effusions) Example: - 1cc (40mg) Depomedrol + 4 cc")
30 Knee Injections - OA, RA, Gout, Synovitis, Meniscal Tear, Effusion, Pain - Anatomy: Large Joint / No major arteries or nerves - Can improve patient s symptoms for up to 3 weeks with NNT of 3 or 4 (Roskos, 2005) - Approaches: - Anterior - Medial Retropatellar - Lateral Retropatellar - Suprapatellar (done for suprapatellar effusions) Example: - 1cc (40mg) Depomedrol + 4 cc lidocaine



31 Knee Lateral Retropatellar - Keep knee straight - Palpate the upper and lower pole of the patella - Lateral access point: within the lateral retropatellar space in line with the junction of the upper and middle thirds of the patella - Apply pressure on the patella medially and with knee extended advance the needle medially and a bit inferiorly while holding the needle horizontally


 advance the needle laterally while holding the needle")
32 Knee Medial Retropatellar - Keep knee straight / extended - Palpate the upper and lower pole of the patella - Medial access point: At medial parapatellar groove underneath the patella, in line with the half-way point between the superior and inferior poles of the patella - Apply pressure on the patella laterally and with knee extended (to open the patella medially) advance the needle laterally while holding the needle horizontally


; locate")


33 Knee - Anterior or Infrapatellar Approach (Lateral side) - Flex at 30 or 90 degrees - Locate the patellar tendon, move about 1cm laterally (or medially); locate tibial plateau and move 1cm superiorly and palpate slight depression - Mark the site - Direct needle perpendicular to knee towards the center of the knee





34 Knee - Superolateral Approach - Palpate superolateral and lateral edges of patella with patient supine and leg straight - Mark the lines (red) - Aspirate for effusion (compression of the opposite side of the joint may aid in arthrocentesis) - Can use same needle if using aspiration and injection (steroid or viscosupplementation)



 -")
35 Ankle Joint Positioning: - Sitting or supine - Knee flexed at 90o with leg either hanging or bent with heel resting against the stretcher - Plantar flexion of the ankle against minimal ankle dorsiflexion by the pateint helps define the anatomy Indications: Diagnostic: - Evaluation of arthiritis (monoarticular or septic) - Evaluation of joint effusion - Evaluation of crystal arthropathy - Identification of intra articular fracture Therapeutic: - Relief of pain by aspirating effusions or blood - Injection of medications (corticosteroids, antibiotics, anesthetics) - Drainage of septic effusion
36 References Sims SE, Miller K, Elfar JC, Hammert WC. Non-surgical treatment of lateral epicondylitis: a systematic review of randomized controlled trials. Hand (2014); 9: Krogh TP, Bartels EM, Ellingsen T, Stengaard-Pedersen K, Buchbinder R, Fredberg U, Bliddal H, Christensen R. Comparative effectiveness of injection therapies in lateral epicondylitis: a systematic review and network meta-analysis of randomized controlled trials. Am J Sports Med Jun;41(6): Smidt N, van der Windt DA, Assendelft WJ, Devillé WL, Korthals-de Bos IB, Bouter LM. Corticosteroid injections, physiotherapy, or a wait-and-see policy for lateral epicondylitis: a randomised controlled trial. Lancet Feb 23;359(9307): Wittich CM, Ficalora RD, Mason TG, Beckman TJ. Musculoskeletal injection. Mayo Clin Proc Sep;84(9): Garg N1, Perry L, Deodhar A. Intra-articular and soft tissue injections, a systematic review of relative efficacy of various corticosteroids. Clin Rheumatol Dec;33(12): Brinks A, van Rijn RM, Willemsen SP, Bohnen AM, Verhaar JA, Koes BW, Bierma-Zeinstra SM. Corticosteroid injections for greater trochanteric pain syndrome: a randomized controlled trial in primary care. Ann Fam Med May-Jun;9(3): Cawley PJ, Morris IM. A study to compare the efficacy of two methods of skin preparation prior to joint injection. Br J Rheumatol. 1992;31: Pekarek B, Osher L, Buck S, Bowen M. Intra-articular corticosteroid injections: a critical literature review with up-to-date findings. Foot (Edinb) Jun;21(2): Pensak MJ, Bayron J, Wolf JM. Current treatment of de Quervain tendinopathy. J Hand Surg Am Nov;38(11): Baima J., Zacharia, I. Clean versus sterile technique for common joint injections: A review from the psysiatry prerspective Curr Rev Musculoskelet Med 2008 Jun;1(2): Hill JJ Jr, Trapp RG, Colliver JA: Survey on the use of corticosteroid injections by orthopaedists. Contemp Orthop 1989;18: McNabb, James. A Practical Guide to Joint & Soft Tissue Injection & Aspiration. 2nd Ed.LWW; 2010.
37 References Nichols, AW. Complications associated With the Use of Corticosteroids in the Treatment of Athletic Injuries. Clin J Sport Med (2005); 15:E370 Pfenninger JL. Procedures for Primary Care Physicians. St. Louis: Mosby, 2010 Dietzel DP, Hedlund EC Injections and return to play. Curr Sports Med Rep (2004) Dec; 3(6): Nepple JJ, Matava MJ. Soft Tissue Injections in the athlete Sports Health: A multidisciplinary Approach (2009) Sep;1(5): Wang AA, Hutchinson DT. The effect of corticosteroid in injection for trigger finger on blood glucose level in diabetic patient. J Hand Surg Am (2006) Jul-Aug; 31(6): Ahmed I, Gerner E Safety of arthrocentesis and joint injection in patients receiving anticoagulation at therapeutic levels. Am J Med (2012) Mar; 125(3):265-9.
Benefits of Aspiration and Injection JOINT INJECTIONS. Injection Indications. Mechanism of Action 1/11/2016
 Benefits of Aspiration and Injection JOINT INJECTIONS Mark Niedfeldt, M.D. Medical College of Wisconsin Decrease or resolution of pain Decrease or resolution of inflammation Decrease or resolution of effusion
Benefits of Aspiration and Injection JOINT INJECTIONS Mark Niedfeldt, M.D. Medical College of Wisconsin Decrease or resolution of pain Decrease or resolution of inflammation Decrease or resolution of effusion
KAPA 2017 Musculoskeletal Aspiration and Injection Workshop. W. Scott Black, MD Physician Assistant Studies Program University of Kentucky
 KAPA 2017 Musculoskeletal Aspiration and Injection Workshop W. Scott Black, MD Physician Assistant Studies Program University of Kentucky Aspiration Relatively quick and inexpensive Can be performed in
KAPA 2017 Musculoskeletal Aspiration and Injection Workshop W. Scott Black, MD Physician Assistant Studies Program University of Kentucky Aspiration Relatively quick and inexpensive Can be performed in
GP practical procedures Joint and soft tissue injections. Dr Monica Gupta Dr Hilary Wilson Dr John Hunter
 GP practical procedures Joint and soft tissue injections Dr Monica Gupta Dr Hilary Wilson Dr John Hunter Outline of talk Acute mono arthritis Pros & Cons of injections Regional problems Shoulder Knee Soft
GP practical procedures Joint and soft tissue injections Dr Monica Gupta Dr Hilary Wilson Dr John Hunter Outline of talk Acute mono arthritis Pros & Cons of injections Regional problems Shoulder Knee Soft
Aspiration, Intra-articular and Soft Tissue Injections. MR KEWAL SINGH, MS(orth), FRCS(Eng)
, FRCS(Eng)") Aspiration, Intra-articular and Soft Tissue Injections MR KEWAL SINGH, MS(orth), FRCS(Eng) Indications for Aspiration Haemarthrosis Septic arthritis Symptomatic relief of a large effusion Crystal-induced
Aspiration, Intra-articular and Soft Tissue Injections MR KEWAL SINGH, MS(orth), FRCS(Eng) Indications for Aspiration Haemarthrosis Septic arthritis Symptomatic relief of a large effusion Crystal-induced
Subacromial Bursa Injection
 Subacromial Bursa Injection 5 cc syringe, 21 gauge 1.5 inch needle 1% lidocaine - 4cc 40mg triamcinolone - 1 cc of 40mg/ml identify site-seat the patient with weight of arm hanging down, palpate the lateral
Subacromial Bursa Injection 5 cc syringe, 21 gauge 1.5 inch needle 1% lidocaine - 4cc 40mg triamcinolone - 1 cc of 40mg/ml identify site-seat the patient with weight of arm hanging down, palpate the lateral
ORTHOPEDIC PRIMARY CARE Joint Injections in Primary Care. Jackson Orthopaedic Foundation
 ORTHOPEDIC PRIMARY CARE Joint Injections in Primary Care Jackson Orthopaedic Foundation Joint Injections in Primary Care Kathleen A. Geier, DNP, NP, ONC A.J. Benham, DNP, NP, ONC kgeier@jacksonortho.org
ORTHOPEDIC PRIMARY CARE Joint Injections in Primary Care Jackson Orthopaedic Foundation Joint Injections in Primary Care Kathleen A. Geier, DNP, NP, ONC A.J. Benham, DNP, NP, ONC kgeier@jacksonortho.org
Live On Screen: Knee Injections ABCs of Musculoskeletal Care. Knee aspiration. Objectives. I have no disclosures.
 I have no disclosures. Live On Screen: Knee Injections ABCs of Musculoskeletal Care Carlin Senter, MD Primary Care Sports Medicine Departments of Medicine and Orthopaedics December 11, 2015 Objectives
I have no disclosures. Live On Screen: Knee Injections ABCs of Musculoskeletal Care Carlin Senter, MD Primary Care Sports Medicine Departments of Medicine and Orthopaedics December 11, 2015 Objectives
ORTHOPAEDIC INJECTION AND ASPIRATION TECHNIQUES
 ORTHOPAEDIC INJECTION AND ASPIRATION TECHNIQUES OAAPN October 20, 2016 David H. Sohn, JD MD Chief, Shoulder and Sports Medicine University of Toledo Medical Center When to aspirate? To rule out infection
ORTHOPAEDIC INJECTION AND ASPIRATION TECHNIQUES OAAPN October 20, 2016 David H. Sohn, JD MD Chief, Shoulder and Sports Medicine University of Toledo Medical Center When to aspirate? To rule out infection
Injections of the Joints & Soft Tissues. Matthew Kanaan DO, MS
 Injections of the Joints & Soft Tissues Matthew Kanaan DO, MS Outline / Goals! Injection basics (risks, contraindications, supplies )! Upper extremity Injections! HANDS ON - Simulated needle w/ marking
Injections of the Joints & Soft Tissues Matthew Kanaan DO, MS Outline / Goals! Injection basics (risks, contraindications, supplies )! Upper extremity Injections! HANDS ON - Simulated needle w/ marking
Hands on - Steroid Injections. Jan Schulz, MD Associate professor of medicine McGill University
 Hands on - Steroid Injections Jan Schulz, MD Associate professor of medicine McGill University Disclosures Abbott Pharmaceuticals Amgen Roche Bristol-Myers Squibb Janssen Ortho Novartis Adult Rheumatology
Hands on - Steroid Injections Jan Schulz, MD Associate professor of medicine McGill University Disclosures Abbott Pharmaceuticals Amgen Roche Bristol-Myers Squibb Janssen Ortho Novartis Adult Rheumatology
Musculoskeletal corticosteroid use:
 Musculoskeletal corticosteroid use: Types, Indications, Contraindications, Equivalent doses, Frequency of use and Adverse effects. Dr Jide Olubaniyi MBBS, FRCR Dr Sean Crowther MB BCh, MRCS, FRCR Dr Sukhvinder
Musculoskeletal corticosteroid use: Types, Indications, Contraindications, Equivalent doses, Frequency of use and Adverse effects. Dr Jide Olubaniyi MBBS, FRCR Dr Sean Crowther MB BCh, MRCS, FRCR Dr Sukhvinder
How to Do a Subacromial Shoulder Injection
 How to Do a Subacromial Shoulder Injection UCSF Primary Care Sports Medicine Conference 2018 Carlin Senter, MD Associate Professor Co-Director UCSF Sports Concussion Program Primary Care Sports Medicine
How to Do a Subacromial Shoulder Injection UCSF Primary Care Sports Medicine Conference 2018 Carlin Senter, MD Associate Professor Co-Director UCSF Sports Concussion Program Primary Care Sports Medicine
9/25/2014. Ricki Loar, Ph.D., APN, FNP-BC, GNP-BC. Disclosure: No Disclosures. Strategic Nurse Practitioner Solutions, LLC
 Ricki Loar, Ph.D., APN, FNP-BC, GNP-BC 1 Dr. Ricki S. Loar, Ph.D., FNP-BC, GNP-BC Clinical Director, Be Well Partners in Health Nurse Practitioner, South Naperville Family Practice Faculty, Advanced Practice
Ricki Loar, Ph.D., APN, FNP-BC, GNP-BC 1 Dr. Ricki S. Loar, Ph.D., FNP-BC, GNP-BC Clinical Director, Be Well Partners in Health Nurse Practitioner, South Naperville Family Practice Faculty, Advanced Practice
Professor Lisa Stamp
 Professor Lisa Stamp Rheumatologist University of Otago, Christchurch 8:30-9:25 WS #65: Joint Injection Techniques 9:35-10:30 WS #75: Joint Injection Techniques (Repeated) Joint/soft tissue corticosteroid
Professor Lisa Stamp Rheumatologist University of Otago, Christchurch 8:30-9:25 WS #65: Joint Injection Techniques 9:35-10:30 WS #75: Joint Injection Techniques (Repeated) Joint/soft tissue corticosteroid
Workshop Hands on - Steroid Injections. Michael Stein MDCM, FRCP(C) Date: Nov
 Date: Nov") Workshop Hands on - Steroid Injections Michael Stein MDCM, FRCP(C) Date: Nov 26 2018 Disclosure of Commercial Support This program has received no financial support Faculty/Presenter Disclosures I am a
Workshop Hands on - Steroid Injections Michael Stein MDCM, FRCP(C) Date: Nov 26 2018 Disclosure of Commercial Support This program has received no financial support Faculty/Presenter Disclosures I am a
JOINT INJECTIONS AJ DURFEE PA-C CHRIS MAYBERRY PA-C
 JOINT INJECTIONS AJ DURFEE PA-C Worked with sports group in San Diego for 7 ½ years Worked for Kaiser Orthopedics since 2011 I grew up in San Diego CHRIS MAYBERRY PA-C 1 XAVIER VALDEZ Grew up in Texas
JOINT INJECTIONS AJ DURFEE PA-C Worked with sports group in San Diego for 7 ½ years Worked for Kaiser Orthopedics since 2011 I grew up in San Diego CHRIS MAYBERRY PA-C 1 XAVIER VALDEZ Grew up in Texas
Introduction to Ultrasound Guided Shoulder Injections. Alison Hall Consultant Sonographer Keele University Cannock Chase Hospital
 Introduction to Ultrasound Guided Shoulder Injections Alison Hall Consultant Sonographer Keele University Cannock Chase Hospital Safe Robust Aim: to provide a service that is Cost effective To enable patients
Introduction to Ultrasound Guided Shoulder Injections Alison Hall Consultant Sonographer Keele University Cannock Chase Hospital Safe Robust Aim: to provide a service that is Cost effective To enable patients
Office Knee Injections
 CME Workshop Office Knee Injections Step By Step Prem Sequeira, MD, CCFP Presented at Family Medicine Potpourri, Memorial University of Newfoundland Corticosteroid injections can give dramatic and long-lasting
CME Workshop Office Knee Injections Step By Step Prem Sequeira, MD, CCFP Presented at Family Medicine Potpourri, Memorial University of Newfoundland Corticosteroid injections can give dramatic and long-lasting
BATES VISUAL GUIDE TO PHYSICAL EXAMINATION. OSCE 4: Knee Pain
 BATES VISUAL GUIDE TO PHYSICAL EXAMINATION OSCE 4: Knee Pain This video format is designed to help you prepare for objective structured clinical examinations, or OSCEs. You are going to observe and participate
BATES VISUAL GUIDE TO PHYSICAL EXAMINATION OSCE 4: Knee Pain This video format is designed to help you prepare for objective structured clinical examinations, or OSCEs. You are going to observe and participate
Evidence Based Approach to Shoulder Injections
 Evidence Based Approach to Shoulder Injections Bradley Sandella, DO Christiana Care Sports Medicine Joseph Straight, MD First State Orthopaedics Objectives Relevant Anatomy Indications for injections Injection
Evidence Based Approach to Shoulder Injections Bradley Sandella, DO Christiana Care Sports Medicine Joseph Straight, MD First State Orthopaedics Objectives Relevant Anatomy Indications for injections Injection
Ankle Arthroscopy.
 Ankle Arthroscopy Key words: Ankle pain, ankle arthroscopy, ankle sprain, ankle stiffness, day case surgery, articular cartilage, chondral injury, chondral defect, anti-inflammatory medication Our understanding
Ankle Arthroscopy Key words: Ankle pain, ankle arthroscopy, ankle sprain, ankle stiffness, day case surgery, articular cartilage, chondral injury, chondral defect, anti-inflammatory medication Our understanding
Pragmatic use of US in intraarticular and periarticular procedures
 Pragmatic use of US in intraarticular and periarticular procedures Plovdiv, 13. January 2018 Dr. med. Giorgio Tamborrini-Schütz www.irheuma.com member of the EULAR Network of Imaging Training Centres Ulrasound
Pragmatic use of US in intraarticular and periarticular procedures Plovdiv, 13. January 2018 Dr. med. Giorgio Tamborrini-Schütz www.irheuma.com member of the EULAR Network of Imaging Training Centres Ulrasound
Rheumatology & Immunology. Regional pain syndromes to be covered today. Some definitions. Tendinitis. Bursitis. History. History. Exam.
 Rheumatology & Immunology Some problems are difficult, but diagnosing and treating soft tissue syndromes are not! Soft tissue syndromes one of the most common reasons patients present to their doctor.
Rheumatology & Immunology Some problems are difficult, but diagnosing and treating soft tissue syndromes are not! Soft tissue syndromes one of the most common reasons patients present to their doctor.
Joint Injection Challenge The art of good injection therapy is to place the appropriate amount of the appropriate medication into the exact site of th
 The Art of the Injection By Jon C. Brillhart PA-C Daivd Lannik MD Portsmouth Orthopedics, Inc Joint Injection Challenge The art of good injection therapy is to place the appropriate amount of the appropriate
The Art of the Injection By Jon C. Brillhart PA-C Daivd Lannik MD Portsmouth Orthopedics, Inc Joint Injection Challenge The art of good injection therapy is to place the appropriate amount of the appropriate
Soft Tissue Rheumatism. Elinor Mody, MD Chief, Division of Rheumatology Reliant Medical Group
 Soft Tissue Rheumatism Elinor Mody, MD Chief, Division of Rheumatology Reliant Medical Group Some problems are difficult, but diagnosing and treating most causes of joint pain are not! Common areas of
Soft Tissue Rheumatism Elinor Mody, MD Chief, Division of Rheumatology Reliant Medical Group Some problems are difficult, but diagnosing and treating most causes of joint pain are not! Common areas of
Focal Knee Swelling Clinical Presentation
 Focal Knee Swelling Clinical Presentation referral for MSK Triage History and Examination Baker's Cyst Medial or Lateral Focal Swelling Consider meniscal Cysts Bursitis Refer for Weight Bearing X-ray AP
Focal Knee Swelling Clinical Presentation referral for MSK Triage History and Examination Baker's Cyst Medial or Lateral Focal Swelling Consider meniscal Cysts Bursitis Refer for Weight Bearing X-ray AP
HANDS ON: Knee Evaluation J. Scott Delaney MD, FRCPC, FACEP, CSPQ
 HANDS ON: Knee Evaluation J. Scott Delaney MD, FRCPC, FACEP, CSPQ FACULTY DISCLOSURE Dr. Delaney has no affiliation with the manufacturer of any commercial product or provider of any commercial service
HANDS ON: Knee Evaluation J. Scott Delaney MD, FRCPC, FACEP, CSPQ FACULTY DISCLOSURE Dr. Delaney has no affiliation with the manufacturer of any commercial product or provider of any commercial service
SMF PCP Treatment & Referral Guideline Orthopedics Developed February 1, 2003 Revised: October, 2011
 SUTTER MEDICAL FOUNDATION (SMF) 2800 L Street, 7 th Floor Sacramento, CA 95816 SMF PCP Treatment & Referral Guideline Orthopedics Developed February 1, 2003 Revised: October, 2011 I. Shoulder Pain...Page
SUTTER MEDICAL FOUNDATION (SMF) 2800 L Street, 7 th Floor Sacramento, CA 95816 SMF PCP Treatment & Referral Guideline Orthopedics Developed February 1, 2003 Revised: October, 2011 I. Shoulder Pain...Page
Title: EZ-IO. Effective Date: January SOG Number: EMS Rescinds:
 S O G Title: EZ-IO Effective Date: January 2010 SOG Number: EMS - 25 Rescinds: Scope: Providers Authorized are AIC s in the following certifications EMT-I and EMT-P who have been trained and cleared by
S O G Title: EZ-IO Effective Date: January 2010 SOG Number: EMS - 25 Rescinds: Scope: Providers Authorized are AIC s in the following certifications EMT-I and EMT-P who have been trained and cleared by
ORTHOPEDIC OFFICE INTERVENTIONS. Objectives of this discussion. Why me? By Steve Benz M.D.
 ORTHOPEDIC OFFICE INTERVENTIONS By Steve Benz M.D. Objectives of this discussion Learn about injections and castings that you can perform in your clinic setting. Learn about the agents that you can inject.
ORTHOPEDIC OFFICE INTERVENTIONS By Steve Benz M.D. Objectives of this discussion Learn about injections and castings that you can perform in your clinic setting. Learn about the agents that you can inject.
Clinical Presentation. Medial or Lateral Focal Swelling Consider meniscal Cysts. Click for more info. Osteoarthritis confirmed. Osteoarthritis pathway
 Focal Knee Swelling Information for GPs who refer into PAH Spinal and knee MRIs should only be requested as a pre-cursor to surgery. Clinical Presentation If you think a patient requires an MRI as there
Focal Knee Swelling Information for GPs who refer into PAH Spinal and knee MRIs should only be requested as a pre-cursor to surgery. Clinical Presentation If you think a patient requires an MRI as there
Musculoskeletal Examination Benchmarks
 Musculoskeletal Examination Benchmarks _ The approach to examining the musculoskeletal system is the same no matter what joint or limb is being examined. The affected and contralateral region should both
Musculoskeletal Examination Benchmarks _ The approach to examining the musculoskeletal system is the same no matter what joint or limb is being examined. The affected and contralateral region should both
Nursing Management: Musculoskeletal Trauma and Orthopedic Surgery. By: Aun Lauriz E. Macuja SAC_SN4
 Nursing Management: Musculoskeletal Trauma and Orthopedic Surgery By: Aun Lauriz E. Macuja SAC_SN4 The most common cause of musculoskeletal injuries is a traumatic event resulting in fracture, dislocation,
Nursing Management: Musculoskeletal Trauma and Orthopedic Surgery By: Aun Lauriz E. Macuja SAC_SN4 The most common cause of musculoskeletal injuries is a traumatic event resulting in fracture, dislocation,
Evaluation of the Knee and Shoulder
 Evaluation of the Knee and Shoulder Karen J. Boselli, MD Northeast Regional Nurse Practitioner Conference May 2018 Knee Overview History Examination Top 5 diagnoses When to image When to refer Pain most
Evaluation of the Knee and Shoulder Karen J. Boselli, MD Northeast Regional Nurse Practitioner Conference May 2018 Knee Overview History Examination Top 5 diagnoses When to image When to refer Pain most
Joint Injections. AJ Durfee PA-C. Course Objectives. Jerry Hizon,MD, FAAFP,CAQSM
 Jerry Hizon,MD, FAAFP,CAQSM Joint Injections OUCH Sports Med Ctr Team Doctor, SD Chargers (NFL) Temecula Valley High School Assist. Clinical Professor, University of California, San Diego Mayor of Temecula
Jerry Hizon,MD, FAAFP,CAQSM Joint Injections OUCH Sports Med Ctr Team Doctor, SD Chargers (NFL) Temecula Valley High School Assist. Clinical Professor, University of California, San Diego Mayor of Temecula
Joint Injection Workshop ACP Scientific Meeting February 28, Andrea M. Barker, MPAS, PA C Michael J. Battistone, MD
 Joint Injection Workshop ACP Scientific Meeting February 28, 2015 Andrea M. Barker, MPAS, PA C Michael J. Battistone, MD Workshop Schedule 1:00 1:15 A Practical Approach to the Shoulder Exam 1:15 1:40
Joint Injection Workshop ACP Scientific Meeting February 28, 2015 Andrea M. Barker, MPAS, PA C Michael J. Battistone, MD Workshop Schedule 1:00 1:15 A Practical Approach to the Shoulder Exam 1:15 1:40
What is Medial Plica Syndrome?
 What is Medial Plica Syndrome? It is a congenital disorder in which the thin wall of fibrous tissue extends from the synovial capsule of the knee. Pain usually occurs when the synovial capsule becomes
What is Medial Plica Syndrome? It is a congenital disorder in which the thin wall of fibrous tissue extends from the synovial capsule of the knee. Pain usually occurs when the synovial capsule becomes
CLINICAL PRESENTATION AND RADIOLOGY QUIZ QUESTION
 Donald L. Renfrew, MD Radiology Associates of the Fox Valley, 333 N. Commercial Street, Suite 100, Neenah, WI 54956 12/01/2012 Radiology Quiz of the Week # 101 Page 1 CLINICAL PRESENTATION AND RADIOLOGY
Donald L. Renfrew, MD Radiology Associates of the Fox Valley, 333 N. Commercial Street, Suite 100, Neenah, WI 54956 12/01/2012 Radiology Quiz of the Week # 101 Page 1 CLINICAL PRESENTATION AND RADIOLOGY
Welcome to the: Orthopaedic Opinion Online Website The website for the answer to all your Orthopaedic Questions
 Welcome to the: Orthopaedic Opinion Online Website The website for the answer to all your Orthopaedic Questions Orthopaedic Opinion Online is a website designed to provide information to patients who have
Welcome to the: Orthopaedic Opinion Online Website The website for the answer to all your Orthopaedic Questions Orthopaedic Opinion Online is a website designed to provide information to patients who have
Elbow. Chapter 2 LISTEN. Mechanism of Injury (If Applicable) Pain
 Pain") Chapter 2 Elbow LISTEN Mechanism of Injury (If Applicable) Patient usually remembers their position at the time of injury Certain mechanisms of injury result in characteristic patterns Fall on outstretched
Chapter 2 Elbow LISTEN Mechanism of Injury (If Applicable) Patient usually remembers their position at the time of injury Certain mechanisms of injury result in characteristic patterns Fall on outstretched
Preliminary Report Choosing Wisely Identifying Musculoskeletal Interventions with Limited Levels of Efficacy in the Shoulder & Elbow.
 Preliminary Report Choosing Wisely Identifying Musculoskeletal Interventions with Limited Levels of Efficacy in the Shoulder & Elbow. Prepared for The Canadian Orthopaedic Association Contents Executive
Preliminary Report Choosing Wisely Identifying Musculoskeletal Interventions with Limited Levels of Efficacy in the Shoulder & Elbow. Prepared for The Canadian Orthopaedic Association Contents Executive
The right medicine, in the right quantity, in the right place, at the right time.
 Ian Reilly FCPodS DMS Consultant Podiatric Surgeon Injection therapy (IT) for the treatment of joint pain has been performed for many years using different substances Compounds such as sodium bicarbonate,
Ian Reilly FCPodS DMS Consultant Podiatric Surgeon Injection therapy (IT) for the treatment of joint pain has been performed for many years using different substances Compounds such as sodium bicarbonate,
Musculoskeletal Referral Guidelines
 Musculoskeletal Referral Guidelines Introduction These guidelines have been developed to provide an integrated musculoskeletal service. They are based on reasonable clinical practice and will initially
Musculoskeletal Referral Guidelines Introduction These guidelines have been developed to provide an integrated musculoskeletal service. They are based on reasonable clinical practice and will initially
Larry Rosenberger, CNP
 Larry Rosenberger, APRN CNP Julie Melendez, APRN CNP Larry Rosenberger, CNP Northwest Ohio Orthopedics and Sports Medicine Findlay, Ohio lrosenberger@nwoortho.com 419 233 2215 Julie Melendez, CNP Northwest
Larry Rosenberger, APRN CNP Julie Melendez, APRN CNP Larry Rosenberger, CNP Northwest Ohio Orthopedics and Sports Medicine Findlay, Ohio lrosenberger@nwoortho.com 419 233 2215 Julie Melendez, CNP Northwest
Outline. Knee Anatomy. Physical Exam Skills and Office Procedures in Orthopaedics. The quadriceps muscles extend the knee 7/23/2013
 Physical Exam Skills and Office Procedures in Orthopaedics Outline Knee exam Knee aspiration and injection Shoulder exam Subacromial bursa injection UCSF Essentials of Primary Care August 14, 2012 Carlin
Physical Exam Skills and Office Procedures in Orthopaedics Outline Knee exam Knee aspiration and injection Shoulder exam Subacromial bursa injection UCSF Essentials of Primary Care August 14, 2012 Carlin
Diagnosis & Nonoperative Treatment of the Osteoarthritic Knee. Randall R Wroble MD Orthopedic One Columbus OH
 Diagnosis & Nonoperative Treatment of the Osteoarthritic Knee Randall R Wroble MD Orthopedic One Columbus OH There are 2 things a good doctor does First Step: Finds out what's wrong Second step Makes the
Diagnosis & Nonoperative Treatment of the Osteoarthritic Knee Randall R Wroble MD Orthopedic One Columbus OH There are 2 things a good doctor does First Step: Finds out what's wrong Second step Makes the
Evaluation of the Hip and Knee
 Evaluation of the Hip and Knee Causes of hip pain RA Osteoarthritis Psoriatic arthritis Septic arthritis Bursitis Hip fx Labral tear Tendinitis Referred back pain Cancer AVN Legg-Calve-Perthes Paget's
Evaluation of the Hip and Knee Causes of hip pain RA Osteoarthritis Psoriatic arthritis Septic arthritis Bursitis Hip fx Labral tear Tendinitis Referred back pain Cancer AVN Legg-Calve-Perthes Paget's
Checklist for Physical Examination of the Knee Muscuoskeletal Block -- Chris McGrew MD, Andrew Ashbaugh DO
 Checklist for Physical Examination of the Knee Muscuoskeletal Block -- Chris McGrew MD, Andrew Ashbaugh DO This handout is for use as a rough guide and study aid. Your instructor may perform certain maneuvers
Checklist for Physical Examination of the Knee Muscuoskeletal Block -- Chris McGrew MD, Andrew Ashbaugh DO This handout is for use as a rough guide and study aid. Your instructor may perform certain maneuvers
Regional Pain. Rheumatologist, Manipal Hospital ChanRe Rheumatology and Immunology Center, Bengaluru
 Regional Pain Dr. B. G. Dharmanand M.D., D.M. (Rheumatology) Rheumatologist, Manipal Hospital ChanRe Rheumatology and Immunology Center, Bengaluru Dharmanand B.G. Regional Pain In Wagh S. (Ed). Rheumatology
Regional Pain Dr. B. G. Dharmanand M.D., D.M. (Rheumatology) Rheumatologist, Manipal Hospital ChanRe Rheumatology and Immunology Center, Bengaluru Dharmanand B.G. Regional Pain In Wagh S. (Ed). Rheumatology
SMALL GROUP SESSION 16 January 8 th or 10 th Shoulder pain case/ Touch workshop/ Upper and Lower Extremity Examination
 SMALL GROUP SESSION 16 January 8 th or 10 th Shoulder pain case/ Touch workshop/ Upper and Lower Extremity Examination Suggested Readings: Opatrny L. The Healing Touch. Ann Int Med 2002; 137:1003. http://www.annals.org/cgi/reprint/137/12/1003.pdf
SMALL GROUP SESSION 16 January 8 th or 10 th Shoulder pain case/ Touch workshop/ Upper and Lower Extremity Examination Suggested Readings: Opatrny L. The Healing Touch. Ann Int Med 2002; 137:1003. http://www.annals.org/cgi/reprint/137/12/1003.pdf
APPENDIX EZ IO ADULT INTRAOSSEOUS INFUSION. Purpose: To establish guidelines for the insertion of an intraosseous catheter for patients > 40 kgs.
 APPENDIX EZ IO ADULT INTRAOSSEOUS INFUSION Purpose: To establish guidelines for the insertion of an intraosseous catheter for patients > 40 kgs. Indications: Any Adult patient (>40 kg) for whom you are
APPENDIX EZ IO ADULT INTRAOSSEOUS INFUSION Purpose: To establish guidelines for the insertion of an intraosseous catheter for patients > 40 kgs. Indications: Any Adult patient (>40 kg) for whom you are
Intraosseous Vascular Access. Dr Merl & Dr Veera
 Intraosseous Vascular Access Dr Merl & Dr Veera INDICATIONS The EZ-IO can be used for adult and pediatric patients, Is indicated any time vascular access is difficult to obtain Can be in emergent, urgent,
Intraosseous Vascular Access Dr Merl & Dr Veera INDICATIONS The EZ-IO can be used for adult and pediatric patients, Is indicated any time vascular access is difficult to obtain Can be in emergent, urgent,
MUSCULOSKELETAL DISORDERS: THE BIGGEST JOB SAFETY PROBLEM. What Are Musculoskeletal Disorders
 MUSCULOSKELETAL DISORDERS: THE BIGGEST JOB SAFETY PROBLEM What Are Musculoskeletal Disorders Every year more than 1.8 million workers in the United States suffer painful back and repetitive strain injuries,
MUSCULOSKELETAL DISORDERS: THE BIGGEST JOB SAFETY PROBLEM What Are Musculoskeletal Disorders Every year more than 1.8 million workers in the United States suffer painful back and repetitive strain injuries,
The Joints are Painful & Swollen: Do I give Steroids? Dr Tom Kennedy
 The Joints are Painful & Swollen: Do I give Steroids? Dr Tom Kennedy Learning Objectives When to use an acute rheumatology service Appropriate use of steroids by condition Injection or Oral or Intramuscular
The Joints are Painful & Swollen: Do I give Steroids? Dr Tom Kennedy Learning Objectives When to use an acute rheumatology service Appropriate use of steroids by condition Injection or Oral or Intramuscular
SARASOTA MEMORIAL HOSPITAL. NURSING PROCEDURE INTRAOSSEOUS NEEDLE: INSERTION, CARE, AND REMOVAL (inv08) 12/18 12/18 1 of 7 RESPONSIBILITY:
 12/18 12/18 1 of 7 RESPONSIBILITY:") SARASOTA MEMORIAL HOSPITAL TITLE: ISSUED FOR: NURSING PROCEDURE INTRAOSSEOUS NEEDLE: INSERTION, CARE, AND REMOVAL (inv08) Nursing DATE: REVIEWED: PAGES: 12/18 12/18 1 of 7 RESPONSIBILITY: PS1094 Insertion-
SARASOTA MEMORIAL HOSPITAL TITLE: ISSUED FOR: NURSING PROCEDURE INTRAOSSEOUS NEEDLE: INSERTION, CARE, AND REMOVAL (inv08) Nursing DATE: REVIEWED: PAGES: 12/18 12/18 1 of 7 RESPONSIBILITY: PS1094 Insertion-
Please differentiate an internal derangement from an external knee injury.
 Knee Orthopaedic Tests Sports and Knee Injuries James J. Lehman, DC, MBA, DABCO University of Bridgeport College of Chiropractic Knee Injury Strain, Sprain, Internal Derangement Anatomy of the Knee Please
Knee Orthopaedic Tests Sports and Knee Injuries James J. Lehman, DC, MBA, DABCO University of Bridgeport College of Chiropractic Knee Injury Strain, Sprain, Internal Derangement Anatomy of the Knee Please
Practical guide to joint and soft tissue injection techniques James Galloway MRCP and Marwan Bukhari PhD, FRCP
 Practical guide to joint and soft tissue injection techniques James Galloway MRCP and Marwan Bukhari PhD, FRCP Figure 1. The authors encourage a medial approach to injection of the knee joint; a combination
Practical guide to joint and soft tissue injection techniques James Galloway MRCP and Marwan Bukhari PhD, FRCP Figure 1. The authors encourage a medial approach to injection of the knee joint; a combination
Trigger Finger and Trigger Thumb A Patient's Guide to Trigger Finger & Trigger Thumb
 Trigger Finger and Trigger Thumb A Patient's Guide to Trigger Finger & Trigger Thumb Introduction Trigger finger and trigger thumb are conditions affecting the movement of the tendons as they bend the
Trigger Finger and Trigger Thumb A Patient's Guide to Trigger Finger & Trigger Thumb Introduction Trigger finger and trigger thumb are conditions affecting the movement of the tendons as they bend the
SHOULDER PATIENTS. Diagnostic Shoulder Arthroscopy Technique Guide
 SHOULDER PATIENTS Diagnostic Shoulder Arthroscopy Technique Guide mi-eye 2 Indications for Use The mi-eye 2 system is indicated for use in diagnostic and operative arthroscopic and endoscopic procedures
SHOULDER PATIENTS Diagnostic Shoulder Arthroscopy Technique Guide mi-eye 2 Indications for Use The mi-eye 2 system is indicated for use in diagnostic and operative arthroscopic and endoscopic procedures
ANTERIOR KNEE PAIN. Expected Outcome. Causes
 Montefiore Pediatric Orthopedic and Scoliosis Center Children s Hospital at Montefiore Norman Otsuka MD Eric Fornari MD Jacob Schulz MD Jaime Gomez MD Christine Moloney PA 3400 Bainbridge Avenue, 6 th
Montefiore Pediatric Orthopedic and Scoliosis Center Children s Hospital at Montefiore Norman Otsuka MD Eric Fornari MD Jacob Schulz MD Jaime Gomez MD Christine Moloney PA 3400 Bainbridge Avenue, 6 th
Ultrasound Guided Injections
 Ultrasound Guided Injection Technique More accurate injections Better Results! 1 Benefits: Increased Level of Certainty ie : really know how accurate PRP/Prolotherapy Avoid damage to articular cartilage
Ultrasound Guided Injection Technique More accurate injections Better Results! 1 Benefits: Increased Level of Certainty ie : really know how accurate PRP/Prolotherapy Avoid damage to articular cartilage
Joel S Sellers, DO, FAOASM CAQSM, RMSK
 Joel S Sellers, DO, FAOASM CAQSM, RMSK This is a sports slide of an Olympic wrestler Chris Taylor 1 This is a Sports Illustrated slide of jockey Johnny Sellers This is a slide of Coach Jim Sellers 2 This
Joel S Sellers, DO, FAOASM CAQSM, RMSK This is a sports slide of an Olympic wrestler Chris Taylor 1 This is a Sports Illustrated slide of jockey Johnny Sellers This is a slide of Coach Jim Sellers 2 This
Ultrasound Guided Genicular Nerve Block-A Motor Sparing Technique for the Treatment of Acute and Chronic Knee Pain
 International Journal of Anesthesiology Research, 2015, 3, 37-43 37 Ultrasound Guided Genicular Nerve Block-A Motor Sparing Technique for the Treatment of Acute and Chronic Knee Pain Michael Meng 1, Reid
International Journal of Anesthesiology Research, 2015, 3, 37-43 37 Ultrasound Guided Genicular Nerve Block-A Motor Sparing Technique for the Treatment of Acute and Chronic Knee Pain Michael Meng 1, Reid
Trauma & Orthopaedic Undergraduate Syllabus
 Trauma & Orthopaedic Undergraduate Syllabus Introduction The purpose of this document is to provide a recommended syllabus for medical students in Trauma & Orthopaedics (T&0). It should help students on
Trauma & Orthopaedic Undergraduate Syllabus Introduction The purpose of this document is to provide a recommended syllabus for medical students in Trauma & Orthopaedics (T&0). It should help students on
Dr. K. Brindha, M.D PG ESI PGIMSR, K.K Nagar, Chennai
 Dr. K. Brindha, M.D PG ESI PGIMSR, K.K Nagar, Chennai Case History 9 year old boy presented with a 3 week history of: Swelling of major lower limb joints Progression was additive (right ankle followed
Dr. K. Brindha, M.D PG ESI PGIMSR, K.K Nagar, Chennai Case History 9 year old boy presented with a 3 week history of: Swelling of major lower limb joints Progression was additive (right ankle followed
ATI Skills Modules Checklist for Central Venous Access Devices
 For faculty use only Educator s name Score Date ATI Skills Modules Checklist for Central Venous Access Devices Student s name Date Verify order Patient record Assess for procedure need Identify, gather,
For faculty use only Educator s name Score Date ATI Skills Modules Checklist for Central Venous Access Devices Student s name Date Verify order Patient record Assess for procedure need Identify, gather,
A guide to joint and soft ti s su e corti co s teroid injecti on. Pa rt 1: gen eral principles and the k n ee
 Me d i c i n etoday Pe e r R e v i e w e d Practical procedures A guide to joint and soft ti s su e corti co s teroid injecti on. Pa rt 1: gen eral principles and the k n ee ARVIN KUMAR DAMODARAN BSc,
Me d i c i n etoday Pe e r R e v i e w e d Practical procedures A guide to joint and soft ti s su e corti co s teroid injecti on. Pa rt 1: gen eral principles and the k n ee ARVIN KUMAR DAMODARAN BSc,
ARROW EZ-IO Intraosseous Vascular Access System Procedure Template
 ARROW EZ-IO Intraosseous Vascular Access System Procedure Template PURPOSE To provide procedural guidance for establishment of intraosseous vascular access using the ARROW EZ-IO Intraosseous Vascular Access
ARROW EZ-IO Intraosseous Vascular Access System Procedure Template PURPOSE To provide procedural guidance for establishment of intraosseous vascular access using the ARROW EZ-IO Intraosseous Vascular Access
SOFT TISSUE KNEE INJURIES
 SOFT TISSUE KNEE INJURIES Soft tissue injuries of the knee commonly occur in all sports or in any activity that requires sudden changes in activity or movement. The knee is a complex joint and any injury
SOFT TISSUE KNEE INJURIES Soft tissue injuries of the knee commonly occur in all sports or in any activity that requires sudden changes in activity or movement. The knee is a complex joint and any injury
ELENI ANDIPA General Hospital of Athens G. Gennimatas
 ELENI ANDIPA General Hospital of Athens G. Gennimatas Technological advances over the last years have caused a dramatic improvement in ultrasound quality and resolution An established imaging modality
ELENI ANDIPA General Hospital of Athens G. Gennimatas Technological advances over the last years have caused a dramatic improvement in ultrasound quality and resolution An established imaging modality
limbsandthings.com Knee Aspiration & Injection Trainer with Ultrasound Capability User Guide For more skills training products visit
 Knee Aspiration & Injection Trainer with Ultrasound Capability Product No: 70103 User Guide For more skills training products visit limbsandthings.com Limbs & Things Ltd. Sussex Street, St Philips Bristol,
Knee Aspiration & Injection Trainer with Ultrasound Capability Product No: 70103 User Guide For more skills training products visit limbsandthings.com Limbs & Things Ltd. Sussex Street, St Philips Bristol,
Tarsal Tunnel Syndrome
 43 Thames Street, St Albans, Christchurch 8013 Phone: (03) 356 1353. Website: philip-bayliss.com Tarsal Tunnel Syndrome The foot is subjected to forces hundreds of times the bodyweight, thousands of times
43 Thames Street, St Albans, Christchurch 8013 Phone: (03) 356 1353. Website: philip-bayliss.com Tarsal Tunnel Syndrome The foot is subjected to forces hundreds of times the bodyweight, thousands of times
Kineto. Orthopaedics & Rehabilitation Products
 Member of Vincent Medical Holdings Limited Kineto Orthopaedics & Rehabilitation Products Our orthopaedic and rehabilitation products comprise of a variety of adjustable rehabilitation braces for support,
Member of Vincent Medical Holdings Limited Kineto Orthopaedics & Rehabilitation Products Our orthopaedic and rehabilitation products comprise of a variety of adjustable rehabilitation braces for support,
Bursitis. Other joints are found between the different bones of your fingers and toes. You also have joints that allow your vertebrae to move.
 Bursitis Introduction Bursitis is a common condition that causes swelling around muscles and bones. It happens most often in the shoulder, elbow, hip, or knee. Bursitis is usually caused by overusing a
Bursitis Introduction Bursitis is a common condition that causes swelling around muscles and bones. It happens most often in the shoulder, elbow, hip, or knee. Bursitis is usually caused by overusing a
Ultrasound in Rheumatology
 Arthritis Research UK Primary Care Centre Winner of a Queen s Anniversary Prize For Higher and Further Education 2009 Ultrasound in Rheumatology Alison Hall Consultant MSK Sonographer/Research Fellow Primary
Arthritis Research UK Primary Care Centre Winner of a Queen s Anniversary Prize For Higher and Further Education 2009 Ultrasound in Rheumatology Alison Hall Consultant MSK Sonographer/Research Fellow Primary
Anatomy Your shoulder is made up of three bones: your upper arm bone (humerus), your shoulder blade (scapula), and your collarbone (clavicle).
, your shoulder blade (scapula), and your collarbone (clavicle).") Shoulder Impingement/Rotator Cuff Tendinitis One of the most common physical complaints is shoulder pain. Your shoulder is made up of several joints combined with tendons and muscles that allow a great
Shoulder Impingement/Rotator Cuff Tendinitis One of the most common physical complaints is shoulder pain. Your shoulder is made up of several joints combined with tendons and muscles that allow a great
ACPOMIT Conference 2013 Workshop: Hand and Wrist
 ACPOMIT Conference 2013 Workshop: Hand and Wrist Sarah Turner, MCSP, Clinical Specialist in Hand Therapy Grad Dip Injection Therapy Workshop! Trigger Finger! OA 1 st CMC joint! De Quervain s Tenosynovitis!
ACPOMIT Conference 2013 Workshop: Hand and Wrist Sarah Turner, MCSP, Clinical Specialist in Hand Therapy Grad Dip Injection Therapy Workshop! Trigger Finger! OA 1 st CMC joint! De Quervain s Tenosynovitis!
MEDIAL HEAD GASTROCNEMIUS TEAR (Tennis Leg)
") MEDIAL HEAD GASTROCNEMIUS TEAR (Tennis Leg) Description Expected Outcome Medial head gastrocnemius tear is a strain of the inner part (medial head) of the major calf muscle (gastrocnemius muscle). Muscle
MEDIAL HEAD GASTROCNEMIUS TEAR (Tennis Leg) Description Expected Outcome Medial head gastrocnemius tear is a strain of the inner part (medial head) of the major calf muscle (gastrocnemius muscle). Muscle
LOW LEVEL LASER THERAPY TREATMENT RECOMMENDATIONS FOR TREATMENT WITH THE LASERNEEDLE TOUCH
 LOW LEVEL LASER THERAPY TREATMENT RECOMMENDATIONS FOR TREATMENT WITH THE LASERNEEDLE TOUCH INTRODUCTION & GENERAL INFORMATION For over 12 years, LASERNEEDLE has been working on the development and manufacture
LOW LEVEL LASER THERAPY TREATMENT RECOMMENDATIONS FOR TREATMENT WITH THE LASERNEEDLE TOUCH INTRODUCTION & GENERAL INFORMATION For over 12 years, LASERNEEDLE has been working on the development and manufacture
Key words: Laser, sprain, strain, lameness, tendon
 MLS Master Class - Veterinary Imaging Presented by CelticSMR Ltd Free Phone (UK): 0800 279 9050 International: +44 (0) 1646 603150 AUTHOR DETAILS Carl Gorman BVSc MRCVS PUBLISHER DETAILS Mike Howe B Vet
MLS Master Class - Veterinary Imaging Presented by CelticSMR Ltd Free Phone (UK): 0800 279 9050 International: +44 (0) 1646 603150 AUTHOR DETAILS Carl Gorman BVSc MRCVS PUBLISHER DETAILS Mike Howe B Vet
Musculoskeletal Examination
 Musculoskeletal Examination Statement of Goals Know how to perform a complete musculoskeletal examination. Learning Objectives A. Describe the anatomy of the musculoskeletal system including the bony structures,
Musculoskeletal Examination Statement of Goals Know how to perform a complete musculoskeletal examination. Learning Objectives A. Describe the anatomy of the musculoskeletal system including the bony structures,
APPROPRIATE USE GUIDELINES
 APPROPRIATE USE GUIDELINES Appropriateness of Advanced Imaging Procedures (MRI, CT, Bone Scan/PET) in Patients with Shoulder Pain CDI QUALITY INSTITUTE: PROVIDER LED ENTITY (PLE) Compiled by Rob Liddell,
APPROPRIATE USE GUIDELINES Appropriateness of Advanced Imaging Procedures (MRI, CT, Bone Scan/PET) in Patients with Shoulder Pain CDI QUALITY INSTITUTE: PROVIDER LED ENTITY (PLE) Compiled by Rob Liddell,
ANTERIOR ANKLE IMPINGEMENT
 ANTERIOR ANKLE IMPINGEMENT Description Possible Complications Pinching of bone or soft tissue, including scar tissue, at the Frequent recurrence of symptoms, resulting in chronically front of the ankle
ANTERIOR ANKLE IMPINGEMENT Description Possible Complications Pinching of bone or soft tissue, including scar tissue, at the Frequent recurrence of symptoms, resulting in chronically front of the ankle
ASSESSMENT AND MANAGEMENT OF THE KNEE AND LOWER LIMB.
 ASSESSMENT AND MANAGEMENT OF THE KNEE AND LOWER LIMB www.fisiokinesiterapia.biz Overview History Examination X-rays Fractures and Dislocations. Soft Tissue Injuries Other Knee/Lower limb Problems Anatomy
ASSESSMENT AND MANAGEMENT OF THE KNEE AND LOWER LIMB www.fisiokinesiterapia.biz Overview History Examination X-rays Fractures and Dislocations. Soft Tissue Injuries Other Knee/Lower limb Problems Anatomy
Trigger Finger Release
 Trigger Finger Release Trigger finger, also known as stenosing tenosynovitis, occurs when one of the tendons responsible for bending a finger or the thumb develops a thickening, known as a nodule, and
Trigger Finger Release Trigger finger, also known as stenosing tenosynovitis, occurs when one of the tendons responsible for bending a finger or the thumb develops a thickening, known as a nodule, and
ACL Athletic Career. ACL Rupture - Warning Features Intensive pain Immediate swelling Locking Feel a Pop Dead leg Cannot continue to play
 FIMS Ambassador Tour to Eastern Europe, 2004 Belgrade, Serbia Montenegro Acute Knee Injuries - Controversies and Challenges Professor KM Chan OBE, JP President of FIMS Belgrade ACL Athletic Career ACL
FIMS Ambassador Tour to Eastern Europe, 2004 Belgrade, Serbia Montenegro Acute Knee Injuries - Controversies and Challenges Professor KM Chan OBE, JP President of FIMS Belgrade ACL Athletic Career ACL
Sick Call Screener Course
 Sick Call Screener Course Musculoskeletal System Upper Extremities (2.7) 2.7-2-1 Enabling Objectives 1.46 Utilize the knowledge of musculoskeletal system anatomy while assessing a patient with a musculoskeletal
Sick Call Screener Course Musculoskeletal System Upper Extremities (2.7) 2.7-2-1 Enabling Objectives 1.46 Utilize the knowledge of musculoskeletal system anatomy while assessing a patient with a musculoskeletal
What is arthroscopy? Normal knee anatomy
 What is arthroscopy? Arthroscopy is a common surgical procedure for examining and repairing the inside of your knee. It is a minimally invasive surgical procedure which uses an Arthroscope and other specialized
What is arthroscopy? Arthroscopy is a common surgical procedure for examining and repairing the inside of your knee. It is a minimally invasive surgical procedure which uses an Arthroscope and other specialized
Heel Pain DISCLOSURES. John Tennity, D.P.M. I have no financial disclosures or conflicts of interest
 Heel Pain John Tennity, D.P.M. DISCLOSURES I have no financial disclosures or conflicts of interest 1 What is the Most Common Form of Heel Pain? A. Neurologic B. Arthritic C. Mechanical D. Traumatic 2
Heel Pain John Tennity, D.P.M. DISCLOSURES I have no financial disclosures or conflicts of interest 1 What is the Most Common Form of Heel Pain? A. Neurologic B. Arthritic C. Mechanical D. Traumatic 2
An older systematic review looked at the evidence behind the best approach to evaluate acute knee pain in primary care (Ann Int Med.2003;139:575).
.") There is so much we don't know in medicine that could make a difference, and often we focus on the big things, and the little things get forgotten. To highlight some smaller but important issues, we've
There is so much we don't know in medicine that could make a difference, and often we focus on the big things, and the little things get forgotten. To highlight some smaller but important issues, we've
Musculoskeletal Ultrasound: Basics, Utility, and Clinical Applications
 Musculoskeletal Ultrasound: Basics, Utility, and Clinical Applications Andrew Lavigne, MD, FRCPC Physical Medicine and Rehabilitation CSCN Diplomat (EMG) Dip Sport Medicine Eugene Maida, MD, PGY-4 Resident
Musculoskeletal Ultrasound: Basics, Utility, and Clinical Applications Andrew Lavigne, MD, FRCPC Physical Medicine and Rehabilitation CSCN Diplomat (EMG) Dip Sport Medicine Eugene Maida, MD, PGY-4 Resident
A Patient s Guide to Tendonitis. Foot and Ankle Center of Massachusetts, P.C.
 A Patient s Guide to Tendonitis Welcome to Foot and Ankle Center of Massachusetts, where we believe in accelerating your learning curve with educational materials that are clearly written and professionally
A Patient s Guide to Tendonitis Welcome to Foot and Ankle Center of Massachusetts, where we believe in accelerating your learning curve with educational materials that are clearly written and professionally
Official reprint from UpToDate UpToDate
 UpToDate L* & Official reprint from UpToDate www.uptodate.com 2012 UpToDate The content on the UpToDate website is not intended nor recommended as a substitute for medical advice, diagnosis, or treatment.
UpToDate L* & Official reprint from UpToDate www.uptodate.com 2012 UpToDate The content on the UpToDate website is not intended nor recommended as a substitute for medical advice, diagnosis, or treatment.
Ultrasound of the Knee
 Ultrasound of the Knee Jon A. Jacobson, M.D. Professor of Radiology Director, Division of Musculoskeletal Radiology University of Michigan Disclosures: Consultant: Bioclinica Book Royalties: Elsevier Advisory
Ultrasound of the Knee Jon A. Jacobson, M.D. Professor of Radiology Director, Division of Musculoskeletal Radiology University of Michigan Disclosures: Consultant: Bioclinica Book Royalties: Elsevier Advisory
Elbow. Chapter 2 LISTEN. Mechanism of Injury (If Applicable) Pain
 Pain") Preface The first decade of the twenty-first century has witnessed the continuation of an explosion in our knowledge and understanding of all aspects of disease. Accompanying this has been the increasing
Preface The first decade of the twenty-first century has witnessed the continuation of an explosion in our knowledge and understanding of all aspects of disease. Accompanying this has been the increasing
Interventional Pain Management Newsletters
 Interventional Pain Management Newsletters Ultrasound- guided percutaneous injection of lateral epicondylitis Ultrasound guided percutaneous injection of lateral epicondylitis ( tennis elbow ) is a well-
Interventional Pain Management Newsletters Ultrasound- guided percutaneous injection of lateral epicondylitis Ultrasound guided percutaneous injection of lateral epicondylitis ( tennis elbow ) is a well-
emoryhealthcare.org/ortho
 COMMON SOCCER INJURIES Oluseun A. Olufade, MD Assistant Professor, Department of Orthopedics and PM&R 1/7/18 GOALS Discuss top soccer injuries and treatment strategies Simplify hip and groin injuries in
COMMON SOCCER INJURIES Oluseun A. Olufade, MD Assistant Professor, Department of Orthopedics and PM&R 1/7/18 GOALS Discuss top soccer injuries and treatment strategies Simplify hip and groin injuries in
Philip Bayliss St Albans Osteopathy
 Philip Bayliss St Albans Osteopathy 43 Thames Street, St Albans, Christchurch 8013 Phone: (03) 356 1353 Website: philip-bayliss.com Subacromial (Shoulder) Bursitis 1 Experts estimate that 65% of people
Philip Bayliss St Albans Osteopathy 43 Thames Street, St Albans, Christchurch 8013 Phone: (03) 356 1353 Website: philip-bayliss.com Subacromial (Shoulder) Bursitis 1 Experts estimate that 65% of people