Joint Injection Workshop ACP Scientific Meeting February 28, Andrea M. Barker, MPAS, PA C Michael J. Battistone, MD
|
|
|
- Maria Barber
- 6 years ago
- Views:
Transcription
1 Joint Injection Workshop ACP Scientific Meeting February 28, 2015 Andrea M. Barker, MPAS, PA C Michael J. Battistone, MD
2 Workshop Schedule 1:00 1:15 A Practical Approach to the Shoulder Exam 1:15 1:40 Arthrocentesis and Steroid Injections of the Knee and Shoulder 1:40 1:45 Transition 1:45 2:05 Hands on Session I* Shoulder Exams Knee Injections 2:05 2:25 Hands on Session II* Shoulder Exams Knee Injections * Joint Injection simulators are available during this time
3
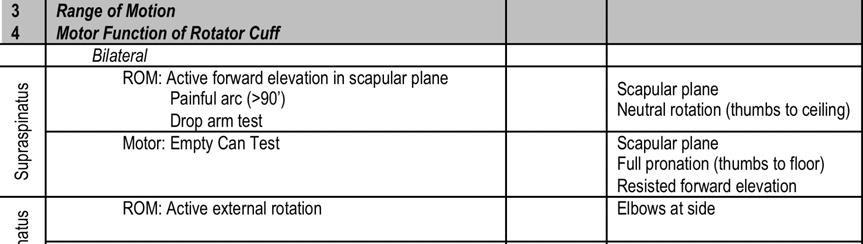
4 Examination Performed Technique Adequate FROM BEHIND 1 Observation Adequate exposure General Scapular winging Observe as they disrobe for degree of discomfort Symmetry, scars, skin lesions, erythema, edema, atrophy Patient raises arms bilaterally Wall press 2 Palpation Bilateral Sternoclavicular joint Acromioclavicular joint Biceps tendon Lateral shoulder Inferior to acromion FACING PATIENT 3 Range of Motion 4 Motor Function of Rotator Cuff Bilateral ROM: Active forward elevation in scapular plane Painful arc (>90 ) Drop arm test Motor: Empty Can Test Supraspinatus Infraspinatus ROM: Active external rotation Motor: Active external rotation against resistance Scapular plane Neutral rotation (thumbs to ceiling) Scapular plane Full pronation (thumbs to floor) Resisted forward elevation Elbows at side Elbows at side Start with hands near midline Subscapularis Teres Minor Unilateral Motor: Belly Press Test Hand on abdomen Elbow anterior to midline Examiner pulls at forearm Watch for elbow to drop ROM: Active internal rotation along spine Observe patient from behind Motor: Lift Off Test ROM: Active external rotation with 90 shoulder abduction and 90 elbow flexion Hand at lumbar spine Actively lifts off back against resistance 90' shoulder abduction 90' elbow flexion Thumb points posterior Motor: Hornblower s Test External rotation as above against resistance Note: check passive range of motion if active is limited. This will identify mechanical block of motion versus shoulder weakness
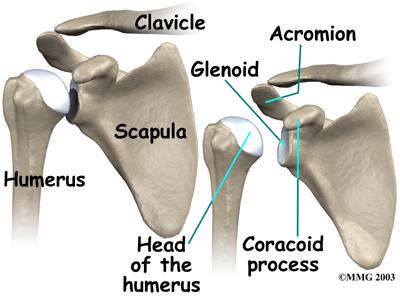
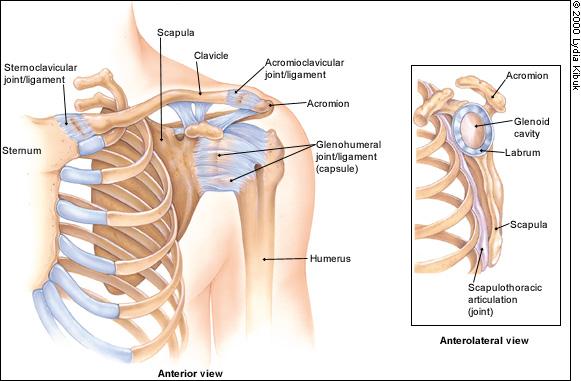
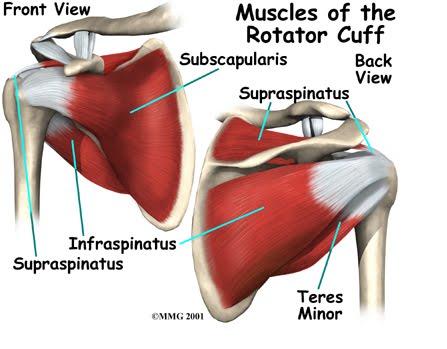
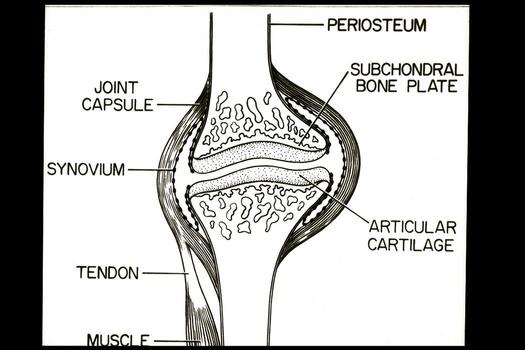
5 Anatomy
6
7
8
9 5 Components of Shoulder Exam 1. Observation 2. Palpation 3. Range of Motion 4. Motor Function of the Rotator Cuff 5. Provocative Testing ADEQUATE EXPOSURE!!!


10 1. Observation Symmetry Skin lesions/scars Erythema Scapular winging Atrophy
11 2. Palpation Bilateral palpation from behind patient SC joint AC joint Biceps tendon (long head) Subacromial space (lateral and posterolateral) Note locations of tenderness to help guide examination
12
13 Start with active ROM and perform passive ROM if active is limited 4. Motor Function of Rotator Cuff Monitor each maneuver for pain as well as strength Pain but normal strength: tendonitis or partialthickness tear Pain with weakness: concern for full thickness tear Compare strength with unaffected side
 Drop Arm")
14 Supraspinatus Abduction Forward elevation ROM: Active forward elevation in scapular plane Bilateral Elbows extended Thumbs to ceiling Painful Arc (pain >90 0 ABD) Drop Arm Test
 Elbows extended Downward pressure by examiner 90 or")
15 Supraspinatus Abduction Forward elevation Motor: Empty Can Test Bilateral Internal rotation (thumbs toward floor) Elbows extended Downward pressure by examiner 90 or lower


16 Infraspinatus ROM: External rotation Bilateral Elbows at side, 90 degrees of flexion Examine for symmetry

17 Infraspinatus External rotation Motor: external rotation test Bilateral Elbows at side, 90 degrees of flexion Hands near midline Examiner resists ER


18 Subscapularis Internal rotation Motor: Belly Press Test Unilateral Elbow anterior to midline Examiner attempts pull arm off abdomen at the wrist


19 Subscapularis Internal rotation ROM: Internal rotation along spine Unilateral Repeat on unaffected side for comparison

20 Subscapularis Internal rotation Motor: Lift off Test Unilateral Dorsum of hand against lumbar spine Patient attempts to lift hand off back against resistance Resistance applied at wrist



21 Teres Minor External rotation ROM: External rotation in abduction Unilateral 90 degrees shoulder abduction 90 degrees elbow flexion Thumb toward ceiling Patient attempts ER hitchhiking

22 Teres Minor External rotation Motor: Hornblower s Test Unilateral 90 degrees shoulder abduction 90 degrees elbow flexion End position of ROM test Examiner resists ER
23 5 Provocative Testing Impingement Testing Hawkin s Test Neer s Test Biceps Testing Speed s Test AC Joint Testing Yergeson s Test Cross-arm Test Shoulder 90' abduction Scapular plane 90' elbow flexion Internal rotation + horizontal adduction Elbow extended Full pronation Maximal passive forward elevation of shoulder with scapular stabilization 60' forward elevation Hand in supination 20-30' elbow flexion Apply downward pressure to forearm Elbow at side, 90' flexion Palm in supination Resisted supination Active horizontal adduction

24 Subacromial Impingement Area between humeral head and acromion Narrowed space Bony changes Acromion type AC spurs Cuff arthropathy Soft tissue swelling Bursa Rotator cuff



25 Subacromial Impingement Testing Hawkin s Test Passive 90 abduction, 90 elbow flexion Scapular plane Maximal internal rotation Neer s Test Passive Elbow extended Pronation Sagittal plane Near to the ear


26 Biceps Tendinopathy Testing Speed s Test 60 forward elevation elbow flexion Downward pressure at forearm Yergason s Test Elbow at side, 90 flexion Palm in supination Examiner attempts to pronate
27 Acromioclavicular Joint Testing Cross arm Test 90 forward elevation Maximal horizontal adduction Pain must be localized to AC joint for test to be positive
 Elbow extension/wrist flexion/finger extension (C7) Finger flexion/thumb abduction (C8) Reflexes Biceps (C5, C6) Brachioradialis (C6) Triceps (C7, C8) Sensation Deltoid (C5) Radial")
28 Neurologic Testing Spurling s Test Slight neck extension Rotation toward affected shoulder Axial load Neurologic Testing Motor Shoulder abduction, forearm supination (C5) Elbow flexion, wrist extension (C6) Elbow extension/wrist flexion/finger extension (C7) Finger flexion/thumb abduction (C8) Reflexes Biceps (C5, C6) Brachioradialis (C6) Triceps (C7, C8) Sensation Deltoid (C5) Radial aspect of arm/hand, thumb (C6) 3 rd digit (C7) Ulnar aspect of arm/hand and 5 th digit (C8)
29 Arthrocentesis and Corticosteroid Injections of the Knee and Shoulder

30 Am I Ready? Do I have a good indication? Do the risks outweigh the benefits? What size needle and syringe will I use? What medications do I want to use? Will I anesthetize the skin? Which approach is most reliable and least painful? What will be considered a successful outcome? What can I tell the patient to expect during & after?
31 Overview Contraindications/risks to corticosteroid (CS) injections Preparation prior to procedure Intra articular (IA) knee injection Indications Approach Patient positioning + procedure Subacromial (SA) injection of the shoulder Indications Approach Patient positioning + procedure
32 Contraindications/Cautions Prosthetic joint Recent surgical procedure involving the joint Joint surgery anticipated in the next 3 months Overlying cellulitis Supratherapeutic anticoagulation Medication allergies Suboptimal response to prior injection If concern for septic arthritis, contact orthopedics or rheumatology
33 Do Risks Outweigh Benefits? Significant Risks and Complications Infection 1 Post injection flare Bleeding Increase in blood glucose Lack of response/no improvement 2 Things to Consider Tendon rupture Skin atrophy/hypopigmentation Suppression of the hypothalamic pituitary axis
34 Pre Procedure Checklist 1. Informed consent 2. Documentation plan 3. Supplies prepared
35 Supplies KEY: Be consistent with needle gauge and syringe size This produces consistent resistance during injections; increased resistance suggests injection of medications into soft tissue/tendon

36 21 Gauge 1.5 Inch Needle + 10cc Syringe Recommended for SA and IA injections Fast delivery, can still feel resistance Can be used for aspiration 18 gauge needle cc syringe Aspiration of large effusion or hemarthrosis

37 Medications Use single dose vials when possible 3,4
38 Anesthetics: Lidocaine + Bupivacaine Mix in syringe with CS Dilution and dispersion of steroid Decrease risk post injection flare, local atrophy Fast onset with lidocaine (1 2cc total) Facilitates diagnosis Long duration with bupivacaine (1 2cc total) Bridges gap with onset of CS
39 Should I Anesthetize the Skin? Local anesthetic not necessary or recommended More painful Limits feedback on accuracy of needle placement Ethyl chloride spray not recommended KEY: Get needle through skin quickly and deliberately
40 Which Corticosteroid Should be Used? No large RCTs comparing various preparations American College of Rheumatology Survey 5 Triamcinolone acetonide (Kenalog) in the West Methylprednisolone (Depo Medrol) in the East Both agents comparable for SA shoulder injection 6 Both may have less chance of post injection flare
41 Body Area Specific Location Corticosteroid Dosing Recommendation (Methylprednisolone equivalent) Shoulder Subacromial 40mg Glenohumeral joint Acromioclavicular joint 40 80mg 20mg Knee Intra articular 40 80mg Hip Pre patellar bursa Pes anserine bursa Greater trochanteric bursa/area General rule for methylprednisolone equivalent: 120mg in 1day 160mg in 4 weeks 20 40mg 20mg 20 40mg
42 Process of Drawing up Medication Open 10cc syringe and attach 18 gauge needle Open medication vials and wipe tops with chlorhexidine Draw medication into syringe; start with multi dose Cap 18 gauge needle but don t remove from syringe Open gauze and bandage, set near patient
43 Ready For Procedure Pre procedure checklist imed Consent Out of OR Time Out Note Supplies prepared and near patient Marking injection site Sterile prep No touch technique

44 Retractable pen Marking the Site
45 Sterile Prep Chlorhexidine over iodine 7 Must be mechanical scrub 2 swabs, 30 seconds each Silver dollar area

46 No Touch Technique Use final prep to confirm location & hand placement Non sterile gloves Indentation remains

47 Intra articular Knee Injection Indications Approach Patient Positioning Procedure Checklist
48 Do I Have a Good Indication for a Knee Aspiration and/or Injection? OA ACR conditionally recommends 8 AAOS inconclusive 9 Degenerative meniscus tear Known inflammatory disease with exacerbation Question of inflammatory disease needing confirmation of crystals Avoid in younger patients/those with normal cartilage


49 Approach to Knee Injection Flexed Knee Anteromedial joint line Anterolateral joint line Extended Knee Lateral midpatellar Superolateral patellar
50 Accuracy Review Flexed Knee Anterolateral joint line 67 71% Anteromedial joint line 72 75% Extended Knee Lateral midpatellar 85 93% Superolateral patellar 87 91% Improved accuracy Effusion present Provider experience Recommend when starting out to pick one technique and use the same approach every time
51
52 Sagittal Knee `
53 Axial Knee
54 Recommendations 1 st choice Superolateral patellar or lateral midpatellar Improved accuracy Potentially less painful Alternate Anterolateral or anteromedial joint line When body habitus limits landmarks in extension Severe PF OA with large lateral patellar osteophytes
 Elevate patient to place entry site at eye")
55 Patient Positioning Supine Bridge from pelvis to ankle Maximal tolerated hyperextension* Point toes and patella to ceiling Keep quadriceps relaxed (may require additional person to stabilize the foot) Elevate patient to place entry site at eye level
56 Procedure 1. Identify the upper 1/3 of patella 2. Displace and tilt lateral edge of patella 3. Find entry point: soft indentation just posterior to lateral patellar edge 4. Needle entry: 1. Perpendicular to femur 2. Parallel to ground





57 Procedure 1. Identify the upper 1/3 of patella 2. Displace patella lateral and tilt lateral edge up 3. ID entry point: soft indentation just posterior to lateral patellar edge 4. Needle entry: Perpendicular to femur + parallel to ground 5. Insert needle quickly through skin, then slowly advance through synovium (0.5 to 1 in)
58 Knee Injection Summary: Superolateral or lateral midpatellar approach Positioning Maximal hyperextension Toes to ceiling Relax quads Eye level Procedure Upper 1/3 of patella Displace and tilt Perpendicular to femur Parallel to ground
59 Subacromial Shoulder Injection Indications Approach Patient Positioning Procedure Checklist
60 Do I Have a Good Indication for Subacromial Injection of the Shoulder? Impingement Syndrome/SA bursitis Rotator cuff tendinitis/partial thickness tear Failed conservative management Inoperable full thickness rotator cuff tear Rotator cuff arthropathy Get both SA and GH areas Not indicated for primary GH OA No connection unless full thickness tear
61 Subacromial Injections

62 Approach Posterior Lateral
63 Patient Positioning Patient seated Arm hanging at side, relaxed Provider stands behind patient Injection site at eye level

64 1. Identify anterior and posterior acromion 2. Note angle of acromion 3. Find entry point: 1 cm inferior and medial to posterior corner 4. Needle entry: Parallel to acromion angle Saggital plane 5. Insert needle in. Tip under mid to anterior acromion Procedure
65 Troubleshooting Always aspirate before injecting If resistance encountered: First, rotate needle 180 degrees Next, withdraw few millimeters Finally, withdraw a few more millimeters and redirect slope of needle by 5 10 degrees
66 Documentation Requirements See handout
 Order")
67 Synovial Fluid Analysis Purple top tube Cell count and differential Crystal analysis Original syringe with cap Gram stain and culture Label each tube Patient name SSN Date/time collected Location ( Right knee ) Order number
68 Summary Recommendations 21 gauge 1.5 inch needle with 10cc syringe Medications (can be used for both procedures): 1cc = 40mg methylprednisolone or equivalent 2cc 0.1% lidocaine 2cc 0.5% bupivicaine Do not anesthetize the skin Prep skin with chlorhexidine Use the no touch technique Position patient with entry site at eye level Use same approach for each procedure
69 1. Geirsson AJ, Statkevicius S, Víkingsson A. Septic arthritis in Iceland : increasing incidence due to iatrogenic infections. Ann Rheum Dis 2008; 67: Gaffney K, Ledingham J, Perry JD. Intra articular triamcinolone hexacetonide in knee osteoarthritis: factors influencing the clinical response. Ann Rheum Dis 1995; 54: Kirschke DL, Jones TF, Stratton CW, et al. Outbreak of joint and soft tissue infections associated with injections from a multiple dose medication vial. Clin Infect Dis 2003; 36: Motamedifar M, Askarian M. The prevalence of multidose vial contamination by aerobic bacteria in a major teaching hospital, Shiraz, Iran, Am J Infect Control 2009; 37: Centeno LM, Moore ME. Preferred intraarticular corticosteroids and associated practice: a survey of members of the American College of Rheumatology. Arthritis Care Res 1994; 7: Mod Rheumatol. 2009;19(2): doi: /s x. Epub 2008 Nov 22. need full citation PMID Mimoz O, Karim A, Mercat A, et al. Chlorhexidine compared with povidone iodine as skin preparation before blood culture. A randomized, controlled trial. Ann Intern Med 1999; 131: Recommendations for the medical management of osteoarthritis of the hip and knee: 2000 update. American College of Rheumatology Subcommittee on Osteoarthritis Guidelines. Arthritis Rheum Sep;43(9): Brown GA. AAOS clinical practice guideline: treatment of osteoarthritis of the knee: evidence based guideline, 2nd edition. J Am Acad Orthop Surg Sep;21(9): Hermans J, Bierma Zeinstra SM, Bos PK, Verhaar JA, Reijman M. The most accurate approach for intra articular needle placement in the knee joint: a systematic review. Semin Arthritis Rheum 2011;41: Jackson DW, Evans NA, Thomas BM. Accuracy of needle placement into the intra articular space of the knee. JBJS 2002; 84(9): Maricar N, Parks MJ, Callaghan MJ, et al. Where and how to inject the knee a systematic review. Semin Arthritis Rheum 2013 Oct; 43(2):
Physical Examination of the Shoulder
 General setup Patient will be examined in both the seated and supine position so exam table needed 360 degree access to patient Expose neck and both shoulders (for comparison); female in gown or sports
General setup Patient will be examined in both the seated and supine position so exam table needed 360 degree access to patient Expose neck and both shoulders (for comparison); female in gown or sports
Subacromial Bursa Injection
 Subacromial Bursa Injection 5 cc syringe, 21 gauge 1.5 inch needle 1% lidocaine - 4cc 40mg triamcinolone - 1 cc of 40mg/ml identify site-seat the patient with weight of arm hanging down, palpate the lateral
Subacromial Bursa Injection 5 cc syringe, 21 gauge 1.5 inch needle 1% lidocaine - 4cc 40mg triamcinolone - 1 cc of 40mg/ml identify site-seat the patient with weight of arm hanging down, palpate the lateral
Benefits of Aspiration and Injection JOINT INJECTIONS. Injection Indications. Mechanism of Action 1/11/2016
 Benefits of Aspiration and Injection JOINT INJECTIONS Mark Niedfeldt, M.D. Medical College of Wisconsin Decrease or resolution of pain Decrease or resolution of inflammation Decrease or resolution of effusion
Benefits of Aspiration and Injection JOINT INJECTIONS Mark Niedfeldt, M.D. Medical College of Wisconsin Decrease or resolution of pain Decrease or resolution of inflammation Decrease or resolution of effusion
Outline. Knee Anatomy. Physical Exam Skills and Office Procedures in Orthopaedics. The quadriceps muscles extend the knee 7/23/2013
 Physical Exam Skills and Office Procedures in Orthopaedics Outline Knee exam Knee aspiration and injection Shoulder exam Subacromial bursa injection UCSF Essentials of Primary Care August 14, 2012 Carlin
Physical Exam Skills and Office Procedures in Orthopaedics Outline Knee exam Knee aspiration and injection Shoulder exam Subacromial bursa injection UCSF Essentials of Primary Care August 14, 2012 Carlin
Mastering the Musculoskeletal Exam UCSF Essentials of Women s Health July 7, 2016 Carlin Senter, M.D. Henry Crevensten, M.D.
 Mastering the Musculoskeletal Exam UCSF Essentials of Women s Health July 7, 2016 Carlin Senter, M.D. Henry Crevensten, M.D. I have nothing to disclose Outline Knee exam Shoulder exam Knee Anatomy The
Mastering the Musculoskeletal Exam UCSF Essentials of Women s Health July 7, 2016 Carlin Senter, M.D. Henry Crevensten, M.D. I have nothing to disclose Outline Knee exam Shoulder exam Knee Anatomy The
Injections of the Joints & Soft Tissues. Matthew Kanaan DO, MS
 Injections of the Joints & Soft Tissues Matthew Kanaan DO, MS Outline / Goals! Injection basics (risks, contraindications, supplies )! Upper extremity Injections! HANDS ON - Simulated needle w/ marking
Injections of the Joints & Soft Tissues Matthew Kanaan DO, MS Outline / Goals! Injection basics (risks, contraindications, supplies )! Upper extremity Injections! HANDS ON - Simulated needle w/ marking
How to Do a Subacromial Shoulder Injection
 How to Do a Subacromial Shoulder Injection UCSF Primary Care Sports Medicine Conference 2018 Carlin Senter, MD Associate Professor Co-Director UCSF Sports Concussion Program Primary Care Sports Medicine
How to Do a Subacromial Shoulder Injection UCSF Primary Care Sports Medicine Conference 2018 Carlin Senter, MD Associate Professor Co-Director UCSF Sports Concussion Program Primary Care Sports Medicine
The examination of the painful knee. Maja K Artandi, MD, FACP Clinical Associate Professor of Medicine Stanford University
 The examination of the painful knee Maja K Artandi, MD, FACP Clinical Associate Professor of Medicine Stanford University Objectives of the talk By the end of this talk you will know The important anatomy
The examination of the painful knee Maja K Artandi, MD, FACP Clinical Associate Professor of Medicine Stanford University Objectives of the talk By the end of this talk you will know The important anatomy
ORTHOPAEDIC INJECTION AND ASPIRATION TECHNIQUES
 ORTHOPAEDIC INJECTION AND ASPIRATION TECHNIQUES OAAPN October 20, 2016 David H. Sohn, JD MD Chief, Shoulder and Sports Medicine University of Toledo Medical Center When to aspirate? To rule out infection
ORTHOPAEDIC INJECTION AND ASPIRATION TECHNIQUES OAAPN October 20, 2016 David H. Sohn, JD MD Chief, Shoulder and Sports Medicine University of Toledo Medical Center When to aspirate? To rule out infection
Shoulder Joint Examination. Shoulder Joint Examination. Inspection. Inspection Palpation Movement. Look Feel Move
 Shoulder Joint Examination History Cuff Examination Instability Examination AC Joint Examination Biceps Tendon Examination Superior Labrum Examination Shoulder Joint Examination Inspection Palpation Movement
Shoulder Joint Examination History Cuff Examination Instability Examination AC Joint Examination Biceps Tendon Examination Superior Labrum Examination Shoulder Joint Examination Inspection Palpation Movement
Musculoskeletal Examination Benchmarks
 Musculoskeletal Examination Benchmarks _ The approach to examining the musculoskeletal system is the same no matter what joint or limb is being examined. The affected and contralateral region should both
Musculoskeletal Examination Benchmarks _ The approach to examining the musculoskeletal system is the same no matter what joint or limb is being examined. The affected and contralateral region should both
Diagnostic and Management Approach to the Painful Shoulder
 Diagnostic and Management Approach to the Painful Shoulder Introduction What conditions causing shoulder pain commonly present in General Practice? Subacromial impingement Rotator cuff tears AC joint pathology
Diagnostic and Management Approach to the Painful Shoulder Introduction What conditions causing shoulder pain commonly present in General Practice? Subacromial impingement Rotator cuff tears AC joint pathology
Evidence Based Approach to Shoulder Injections
 Evidence Based Approach to Shoulder Injections Bradley Sandella, DO Christiana Care Sports Medicine Joseph Straight, MD First State Orthopaedics Objectives Relevant Anatomy Indications for injections Injection
Evidence Based Approach to Shoulder Injections Bradley Sandella, DO Christiana Care Sports Medicine Joseph Straight, MD First State Orthopaedics Objectives Relevant Anatomy Indications for injections Injection
RN(EC) ENC(C) GNC(C) MN ACNP *** MECHANISM OF INJURY.. MOST IMPORTANT ***
 ENC(C) GNC(C) MN ACNP *** MECHANISM OF INJURY.. MOST IMPORTANT ***") HISTORY *** MECHANISM OF INJURY.. MOST IMPORTANT *** Age - Certain conditions are more prevalent in particular age groups (i.e. Full rotator cuff tears are more common over the age of 45, traumatic injuries
HISTORY *** MECHANISM OF INJURY.. MOST IMPORTANT *** Age - Certain conditions are more prevalent in particular age groups (i.e. Full rotator cuff tears are more common over the age of 45, traumatic injuries
Soft Tissue Rheumatism. Elinor Mody, MD Chief, Division of Rheumatology Reliant Medical Group
 Soft Tissue Rheumatism Elinor Mody, MD Chief, Division of Rheumatology Reliant Medical Group Some problems are difficult, but diagnosing and treating most causes of joint pain are not! Common areas of
Soft Tissue Rheumatism Elinor Mody, MD Chief, Division of Rheumatology Reliant Medical Group Some problems are difficult, but diagnosing and treating most causes of joint pain are not! Common areas of
SHOULDER PAIN. A Real Pain in the Neck. Michael Wolk, MD Northeastern Rehabilitation Associates October 31, 2017
 SHOULDER PAIN A Real Pain in the Neck Michael Wolk, MD Northeastern Rehabilitation Associates October 31, 2017 THE SHOULDER JOINT (S) 1. glenohumeral 2. suprahumeral 3. acromioclavicular 4. scapulocostal
SHOULDER PAIN A Real Pain in the Neck Michael Wolk, MD Northeastern Rehabilitation Associates October 31, 2017 THE SHOULDER JOINT (S) 1. glenohumeral 2. suprahumeral 3. acromioclavicular 4. scapulocostal
KAPA 2017 Musculoskeletal Aspiration and Injection Workshop. W. Scott Black, MD Physician Assistant Studies Program University of Kentucky
 KAPA 2017 Musculoskeletal Aspiration and Injection Workshop W. Scott Black, MD Physician Assistant Studies Program University of Kentucky Aspiration Relatively quick and inexpensive Can be performed in
KAPA 2017 Musculoskeletal Aspiration and Injection Workshop W. Scott Black, MD Physician Assistant Studies Program University of Kentucky Aspiration Relatively quick and inexpensive Can be performed in
Hands on - Steroid Injections. Jan Schulz, MD Associate professor of medicine McGill University
 Hands on - Steroid Injections Jan Schulz, MD Associate professor of medicine McGill University Disclosures Abbott Pharmaceuticals Amgen Roche Bristol-Myers Squibb Janssen Ortho Novartis Adult Rheumatology
Hands on - Steroid Injections Jan Schulz, MD Associate professor of medicine McGill University Disclosures Abbott Pharmaceuticals Amgen Roche Bristol-Myers Squibb Janssen Ortho Novartis Adult Rheumatology
Review shoulder anatomy Review the physical exam of the shoulder Discuss some common causes of acute shoulder pain Discuss some common causes of
 Review shoulder anatomy Review the physical exam of the shoulder Discuss some common causes of acute shoulder pain Discuss some common causes of chronic shoulder pain Review with some case questions Bones:
Review shoulder anatomy Review the physical exam of the shoulder Discuss some common causes of acute shoulder pain Discuss some common causes of chronic shoulder pain Review with some case questions Bones:
Aspiration, Intra-articular and Soft Tissue Injections. MR KEWAL SINGH, MS(orth), FRCS(Eng)
, FRCS(Eng)") Aspiration, Intra-articular and Soft Tissue Injections MR KEWAL SINGH, MS(orth), FRCS(Eng) Indications for Aspiration Haemarthrosis Septic arthritis Symptomatic relief of a large effusion Crystal-induced
Aspiration, Intra-articular and Soft Tissue Injections MR KEWAL SINGH, MS(orth), FRCS(Eng) Indications for Aspiration Haemarthrosis Septic arthritis Symptomatic relief of a large effusion Crystal-induced
Elbow. Chapter 2 LISTEN. Mechanism of Injury (If Applicable) Pain
 Pain") Chapter 2 Elbow LISTEN Mechanism of Injury (If Applicable) Patient usually remembers their position at the time of injury Certain mechanisms of injury result in characteristic patterns Fall on outstretched
Chapter 2 Elbow LISTEN Mechanism of Injury (If Applicable) Patient usually remembers their position at the time of injury Certain mechanisms of injury result in characteristic patterns Fall on outstretched
Workshop Hands on - Steroid Injections. Michael Stein MDCM, FRCP(C) Date: Nov
 Date: Nov") Workshop Hands on - Steroid Injections Michael Stein MDCM, FRCP(C) Date: Nov 26 2018 Disclosure of Commercial Support This program has received no financial support Faculty/Presenter Disclosures I am a
Workshop Hands on - Steroid Injections Michael Stein MDCM, FRCP(C) Date: Nov 26 2018 Disclosure of Commercial Support This program has received no financial support Faculty/Presenter Disclosures I am a
2015 OPSC Annual Convention. syllabus. February 4-8, 2015 Hyatt Regency Mission Bay San Diego, California
 2015 OPSC Annual Convention syllabus February 4-8, 2015 Hyatt Regency Mission Bay San Diego, California THURSDAY, FEBRUARY 5, 2015: 3:30pm - 4:30pm The Shoulder: 2 View or Not 2 View * Presented by Alexandra
2015 OPSC Annual Convention syllabus February 4-8, 2015 Hyatt Regency Mission Bay San Diego, California THURSDAY, FEBRUARY 5, 2015: 3:30pm - 4:30pm The Shoulder: 2 View or Not 2 View * Presented by Alexandra
Anatomical Considerations/ Pathophysiology The shoulder is the most mobile joint in the body. : Three bones:
 Introduction Musculoskeletal training is generally underrepresented in medical training and residency curriculums. There is a general deficit in musculoskeletal knowledge amongst current medical students,
Introduction Musculoskeletal training is generally underrepresented in medical training and residency curriculums. There is a general deficit in musculoskeletal knowledge amongst current medical students,
JOINT INJECTIONS AJ DURFEE PA-C CHRIS MAYBERRY PA-C
 JOINT INJECTIONS AJ DURFEE PA-C Worked with sports group in San Diego for 7 ½ years Worked for Kaiser Orthopedics since 2011 I grew up in San Diego CHRIS MAYBERRY PA-C 1 XAVIER VALDEZ Grew up in Texas
JOINT INJECTIONS AJ DURFEE PA-C Worked with sports group in San Diego for 7 ½ years Worked for Kaiser Orthopedics since 2011 I grew up in San Diego CHRIS MAYBERRY PA-C 1 XAVIER VALDEZ Grew up in Texas
C. Christopher Smith, M.D. Associate Professor of Medicine Harvard Medical School Beth Israel Deaconess Medical Center
 Evaluation and Treatment of the Painful Shoulder in the Primary Care Setting C. Christopher Smith, M.D. Associate Professor of Medicine Harvard Medical School Beth Israel Deaconess Medical Center A 65-year-old
Evaluation and Treatment of the Painful Shoulder in the Primary Care Setting C. Christopher Smith, M.D. Associate Professor of Medicine Harvard Medical School Beth Israel Deaconess Medical Center A 65-year-old
Returning the Shoulder Back to Optimal Function. Scapula. Clavicle. Humerus. Bones of the Shoulder (Osteology) Joints of the Shoulder (Arthrology)
 Joints of the Shoulder (Arthrology)") Returning the Shoulder Back to Optimal Function Sternum Clavicle Ribs Scapula Humerus Bones of the Shoulder (Osteology) By Rick Kaselj Clavicle Scapula Medial Left Anterior Clavicle Inferior View 20 degree
Returning the Shoulder Back to Optimal Function Sternum Clavicle Ribs Scapula Humerus Bones of the Shoulder (Osteology) By Rick Kaselj Clavicle Scapula Medial Left Anterior Clavicle Inferior View 20 degree
Musculoskeletal Ultrasound. Technical Guidelines SHOULDER
 Musculoskeletal Ultrasound Technical Guidelines SHOULDER 1 Although patient s positioning for shoulder US varies widely across different Countries and Institutions reflecting multifaceted opinions and
Musculoskeletal Ultrasound Technical Guidelines SHOULDER 1 Although patient s positioning for shoulder US varies widely across different Countries and Institutions reflecting multifaceted opinions and
1. Occupation; Right or left handed, Age
 SHOULDER HISTORY 1. Occupation; Right or left handed, Age 2. Pain: Site. Any referred pain to the deltoid insertion Any localizing pain at Acromio-clavicular joint How long? Continuous or not Night pain
SHOULDER HISTORY 1. Occupation; Right or left handed, Age 2. Pain: Site. Any referred pain to the deltoid insertion Any localizing pain at Acromio-clavicular joint How long? Continuous or not Night pain
Joint G*H. Joint S*C. Joint A*C. Labrum. Humerus. Sternum. Scapula. Clavicle. Thorax. Articulation. Scapulo- Thoracic
 A*C Joint Scapulo- Thoracic Articulation Thorax Sternum Clavicle Scapula Humerus S*C Joint G*H Joint Labrum AC Ligaments SC Ligaments SC JOINT AC Coracoacromial GH GH Ligament Complex Coracoclavicular
A*C Joint Scapulo- Thoracic Articulation Thorax Sternum Clavicle Scapula Humerus S*C Joint G*H Joint Labrum AC Ligaments SC Ligaments SC JOINT AC Coracoacromial GH GH Ligament Complex Coracoclavicular
Introduction to Ultrasound Guided Shoulder Injections. Alison Hall Consultant Sonographer Keele University Cannock Chase Hospital
 Introduction to Ultrasound Guided Shoulder Injections Alison Hall Consultant Sonographer Keele University Cannock Chase Hospital Safe Robust Aim: to provide a service that is Cost effective To enable patients
Introduction to Ultrasound Guided Shoulder Injections Alison Hall Consultant Sonographer Keele University Cannock Chase Hospital Safe Robust Aim: to provide a service that is Cost effective To enable patients
Lab Workbook. ANATOMY Manual Muscle Testing Lower Trapezius Patient: prone
 ANATOMY Manual Muscle Testing Lower Trapezius Patient: prone Lab Workbook Fixation: place on hand below the scapula on the opposite side Test: adduction and depression of the scapula with lateral rotation
ANATOMY Manual Muscle Testing Lower Trapezius Patient: prone Lab Workbook Fixation: place on hand below the scapula on the opposite side Test: adduction and depression of the scapula with lateral rotation
Musculoskeletal Examination
 Musculoskeletal Examination Statement of Goals Know how to perform a complete musculoskeletal examination. Learning Objectives A. Describe the anatomy of the musculoskeletal system including the bony structures,
Musculoskeletal Examination Statement of Goals Know how to perform a complete musculoskeletal examination. Learning Objectives A. Describe the anatomy of the musculoskeletal system including the bony structures,
WEEKEND 2 Shoulder. Shoulder Active Range of Motion Assessment
 Virginia Orthopedic Manual Physical Therapy Institute - 2016 Technique Manual WEEKEND 2 Shoulder Shoulder Active Range of Motion Assessment - Patient Positioning: Standing, appropriately undressed so that
Virginia Orthopedic Manual Physical Therapy Institute - 2016 Technique Manual WEEKEND 2 Shoulder Shoulder Active Range of Motion Assessment - Patient Positioning: Standing, appropriately undressed so that
Live On Screen: Knee Injections ABCs of Musculoskeletal Care. Knee aspiration. Objectives. I have no disclosures.
 I have no disclosures. Live On Screen: Knee Injections ABCs of Musculoskeletal Care Carlin Senter, MD Primary Care Sports Medicine Departments of Medicine and Orthopaedics December 11, 2015 Objectives
I have no disclosures. Live On Screen: Knee Injections ABCs of Musculoskeletal Care Carlin Senter, MD Primary Care Sports Medicine Departments of Medicine and Orthopaedics December 11, 2015 Objectives
Evaluating shoulder injuries in primary care Bethany Reed, MSn, AGPCNP-BC One Medical Group
 Evaluating shoulder injuries in primary care Bethany Reed, MSn, AGPCNP-BC One Medical Group Disclosures There has been no commercial support or sponsorship for this program. The planners and presenters
Evaluating shoulder injuries in primary care Bethany Reed, MSn, AGPCNP-BC One Medical Group Disclosures There has been no commercial support or sponsorship for this program. The planners and presenters
Disclaimer. Evaluation & Treatment of Shoulder and Elbow Pain in the Adult Patient. Objectives. Anatomy
 Evaluation & Treatment of Shoulder and Elbow Pain in the Adult Patient William T. Crowe, RN-C, FNP, MSN, MBA Disclaimer! I, William T Crowe, have relevant financial relationships to be discussed, directly
Evaluation & Treatment of Shoulder and Elbow Pain in the Adult Patient William T. Crowe, RN-C, FNP, MSN, MBA Disclaimer! I, William T Crowe, have relevant financial relationships to be discussed, directly
The Shoulder. Anatomy and Injuries PSK 4U Unit 3, Day 4
 The Shoulder Anatomy and Injuries PSK 4U Unit 3, Day 4 Shoulder Girdle Shoulder Complex is the most mobile joint in the body. Scapula Clavicle Sternum Humerus Rib cage/thorax Shoulder Girdle It also includes
The Shoulder Anatomy and Injuries PSK 4U Unit 3, Day 4 Shoulder Girdle Shoulder Complex is the most mobile joint in the body. Scapula Clavicle Sternum Humerus Rib cage/thorax Shoulder Girdle It also includes
Elbow. Chapter 2 LISTEN. Mechanism of Injury (If Applicable) Pain
 Pain") Preface The first decade of the twenty-first century has witnessed the continuation of an explosion in our knowledge and understanding of all aspects of disease. Accompanying this has been the increasing
Preface The first decade of the twenty-first century has witnessed the continuation of an explosion in our knowledge and understanding of all aspects of disease. Accompanying this has been the increasing
Joint Range of Motion Assessment Techniques. Presentation Created by Ken Baldwin, M.Ed Copyright
 Joint Range of Motion Assessment Techniques Presentation Created by Ken Baldwin, M.Ed Copyright 2001-2006 Objectives Understand how joint range of motion & goniometric assessment is an important component
Joint Range of Motion Assessment Techniques Presentation Created by Ken Baldwin, M.Ed Copyright 2001-2006 Objectives Understand how joint range of motion & goniometric assessment is an important component
GP practical procedures Joint and soft tissue injections. Dr Monica Gupta Dr Hilary Wilson Dr John Hunter
 GP practical procedures Joint and soft tissue injections Dr Monica Gupta Dr Hilary Wilson Dr John Hunter Outline of talk Acute mono arthritis Pros & Cons of injections Regional problems Shoulder Knee Soft
GP practical procedures Joint and soft tissue injections Dr Monica Gupta Dr Hilary Wilson Dr John Hunter Outline of talk Acute mono arthritis Pros & Cons of injections Regional problems Shoulder Knee Soft
Sick Call Screener Course
 Sick Call Screener Course Musculoskeletal System Upper Extremities (2.7) 2.7-2-1 Enabling Objectives 1.46 Utilize the knowledge of musculoskeletal system anatomy while assessing a patient with a musculoskeletal
Sick Call Screener Course Musculoskeletal System Upper Extremities (2.7) 2.7-2-1 Enabling Objectives 1.46 Utilize the knowledge of musculoskeletal system anatomy while assessing a patient with a musculoskeletal
Evaluation of the Knee and Shoulder
 Evaluation of the Knee and Shoulder Karen J. Boselli, MD Northeast Regional Nurse Practitioner Conference May 2018 Knee Overview History Examination Top 5 diagnoses When to image When to refer Pain most
Evaluation of the Knee and Shoulder Karen J. Boselli, MD Northeast Regional Nurse Practitioner Conference May 2018 Knee Overview History Examination Top 5 diagnoses When to image When to refer Pain most
Subacromial Impingement (diagnostic methods )
") Subacromial Impingement (diagnostic methods ) M.N. Naderi Fellowship in shoulder and arthroscopic surgery Neer : Definition Impingement on the tendinous portion of the rotator cuff by the coracoacromial
Subacromial Impingement (diagnostic methods ) M.N. Naderi Fellowship in shoulder and arthroscopic surgery Neer : Definition Impingement on the tendinous portion of the rotator cuff by the coracoacromial
PRIMARY CARE EXAMINATION OF KEY JOINTS. Thomas M. Howard, MD, FACSM FFPC Sports Medicine
 PRIMARY CARE EXAMINATION OF KEY JOINTS Thomas M. Howard, MD, FACSM FFPC Sports Medicine General exam principles: Expose entire joint and opposite limb for comparison Have a Differential Diagnosis Exam
PRIMARY CARE EXAMINATION OF KEY JOINTS Thomas M. Howard, MD, FACSM FFPC Sports Medicine General exam principles: Expose entire joint and opposite limb for comparison Have a Differential Diagnosis Exam
Shoulder joint Assessment and General View
 Shoulder joint Assessment and General View Done by; Mshari S. Alghadier BSc Physical Therapy RHPT 366 m.alghadier@sau.edu.sa http://faculty.sau.edu.sa/m.alghadier/ Functional anatomy The shoulder contains
Shoulder joint Assessment and General View Done by; Mshari S. Alghadier BSc Physical Therapy RHPT 366 m.alghadier@sau.edu.sa http://faculty.sau.edu.sa/m.alghadier/ Functional anatomy The shoulder contains
Physical examination protocol in the study of VPT and nerve conduction in working women with and without chronic pain
 Physical examination protocol in the study of VPT and nerve conduction in working women with and without chronic pain ID number General health OK Affected Height cm Weight kg Heart OK Arrhythmia Murmurs
Physical examination protocol in the study of VPT and nerve conduction in working women with and without chronic pain ID number General health OK Affected Height cm Weight kg Heart OK Arrhythmia Murmurs
MLT Muscle(s) Patient Position Therapist position Stabilization Limb Position Picture Put biceps on slack by bending elbow.
 Patient Position Therapist position Stabilization Limb Position Picture Put biceps on slack by bending elbow.") MLT Muscle(s) Patient Position Therapist position Stabilization Limb Position Picture Put biceps on slack by bending elbow. Pectoralis Minor Supine, arm at side, elbows extended, supinated Head of Table
MLT Muscle(s) Patient Position Therapist position Stabilization Limb Position Picture Put biceps on slack by bending elbow. Pectoralis Minor Supine, arm at side, elbows extended, supinated Head of Table
The Shoulder Complex. Anatomy. Articulations 12/11/2017. Oak Ridge High School Conroe, Texas. Clavicle Collar Bone Scapula Shoulder Blade Humerus
 The Shoulder Complex Oak Ridge High School Conroe, Texas Anatomy Clavicle Collar Bone Scapula Shoulder Blade Humerus Articulations Sternoclavicular SC joint. Sternum and Clavicle. Acromioclavicular AC
The Shoulder Complex Oak Ridge High School Conroe, Texas Anatomy Clavicle Collar Bone Scapula Shoulder Blade Humerus Articulations Sternoclavicular SC joint. Sternum and Clavicle. Acromioclavicular AC
Stefan C Muzin, MD PM&R Attending Physician, Beth Israel Deaconess Medical Center, Harvard Medical School Onsite Physiatrist, GE Aviation, Lynn, MA
 Stefan C Muzin, MD PM&R Attending Physician, Beth Israel Deaconess Medical Center, Harvard Medical School Onsite Physiatrist, GE Aviation, Lynn, MA Consultant, OEHN (Occupational and Environmental Network)
Stefan C Muzin, MD PM&R Attending Physician, Beth Israel Deaconess Medical Center, Harvard Medical School Onsite Physiatrist, GE Aviation, Lynn, MA Consultant, OEHN (Occupational and Environmental Network)
IFAST Assessment. Name: Date: Sport: Review Health Risk Assessment on initial consult form. List Client Goals (what brings you here?
 IFAST Assessment Name: Date: Sport: Review Health Risk Assessment on initial consult form List Client Goals (what brings you here?) Cardiovascular Measurements Blood Pressure Resting Heart Rate Body Composition
IFAST Assessment Name: Date: Sport: Review Health Risk Assessment on initial consult form List Client Goals (what brings you here?) Cardiovascular Measurements Blood Pressure Resting Heart Rate Body Composition
The Language of Anatomy. (Anatomical Terminology)
") The Language of Anatomy (Anatomical Terminology) Terms of Position The anatomical position is a fixed position of the body (cadaver) taken as if the body is standing (erect) looking forward with the upper
The Language of Anatomy (Anatomical Terminology) Terms of Position The anatomical position is a fixed position of the body (cadaver) taken as if the body is standing (erect) looking forward with the upper
Table 17: Provocative tests performed in a neutral shoulder position, i.e. the arm is at the patient s side.
 Page 1 of 1 Table 17: Provocative tests performed in a neutral shoulder position, i.e. the arm is at the patient s side. Description Click Image Positive Indicator Study Painful Arc of Abduction Also reported
Page 1 of 1 Table 17: Provocative tests performed in a neutral shoulder position, i.e. the arm is at the patient s side. Description Click Image Positive Indicator Study Painful Arc of Abduction Also reported
SMALL GROUP SESSION 16 January 8 th or 10 th Shoulder pain case/ Touch workshop/ Upper and Lower Extremity Examination
 SMALL GROUP SESSION 16 January 8 th or 10 th Shoulder pain case/ Touch workshop/ Upper and Lower Extremity Examination Suggested Readings: Opatrny L. The Healing Touch. Ann Int Med 2002; 137:1003. http://www.annals.org/cgi/reprint/137/12/1003.pdf
SMALL GROUP SESSION 16 January 8 th or 10 th Shoulder pain case/ Touch workshop/ Upper and Lower Extremity Examination Suggested Readings: Opatrny L. The Healing Touch. Ann Int Med 2002; 137:1003. http://www.annals.org/cgi/reprint/137/12/1003.pdf
OMT Without An OMT Table Workshop. Dennis Dowling, DO FAAO Ann Habenicht, DO FAAO FACOFP
 OMT Without An OMT Table Workshop Dennis Dowling, DO FAAO Ann Habenicht, DO FAAO FACOFP Cervical Somatic Dysfunction (C5 SR RR) - Seated 1. Patient position: seated. 2. Physician position: standing facing
OMT Without An OMT Table Workshop Dennis Dowling, DO FAAO Ann Habenicht, DO FAAO FACOFP Cervical Somatic Dysfunction (C5 SR RR) - Seated 1. Patient position: seated. 2. Physician position: standing facing
Shoulder and Elbow ORTHOPAEDIC SYPMPOSIUM APRIL 8, 2017 DANIEL DOTY MD
 Shoulder and Elbow ORTHOPAEDIC SYPMPOSIUM APRIL 8, 2017 DANIEL DOTY MD Shoulder Articulations Glenohumeral Joint 2/3 total arc of motion Shallow Ball and Socket Joint Allows for excellent ROM Requires
Shoulder and Elbow ORTHOPAEDIC SYPMPOSIUM APRIL 8, 2017 DANIEL DOTY MD Shoulder Articulations Glenohumeral Joint 2/3 total arc of motion Shallow Ball and Socket Joint Allows for excellent ROM Requires
Physical Capability Exam Testing Protocol
 Test Duration: ~ min Physical Capability Exam Testing Protocol Pinch Gauge Grip Dynamometer Inclinometer Stop Watch Lift Box Table Weight Plates (5 lbs., lbs., lbs., 50 lbs., 0 lbs.) Physical Capability
Test Duration: ~ min Physical Capability Exam Testing Protocol Pinch Gauge Grip Dynamometer Inclinometer Stop Watch Lift Box Table Weight Plates (5 lbs., lbs., lbs., 50 lbs., 0 lbs.) Physical Capability
Inhibition Associated with somatic dysfunctions, no matter which components are impaired Implies consideration of all components in treatment planning
 Somatic Dysfunction Impaired or altered function of related components of the somatic system including the skeletal, arthrodial, myofascial structures and their related vascular, lymphatic and neural elements.
Somatic Dysfunction Impaired or altered function of related components of the somatic system including the skeletal, arthrodial, myofascial structures and their related vascular, lymphatic and neural elements.
79b Orthopedic Massage: Technique Demo and Practice! Rotator Cuff and Carpal Tunnel!
 79b Orthopedic Massage: Technique Demo and Practice! Rotator Cuff and Carpal Tunnel! 79b Orthopedic Massage: Technique Demo and Practice! Rotator Cuff and Carpal Tunnel! Class Outline" 5 minutes" "Attendance,
79b Orthopedic Massage: Technique Demo and Practice! Rotator Cuff and Carpal Tunnel! 79b Orthopedic Massage: Technique Demo and Practice! Rotator Cuff and Carpal Tunnel! Class Outline" 5 minutes" "Attendance,
Functional Movement Test. Deep Squat
 Functional Movement Test Put simply, the FMS is a ranking and grading system that documents movement patterns that are key to normal function. By screening these patterns, the FMS readily identifies functional
Functional Movement Test Put simply, the FMS is a ranking and grading system that documents movement patterns that are key to normal function. By screening these patterns, the FMS readily identifies functional
The Shoulder. Jennifer R Marks, MD
 The Shoulder Jennifer R Marks, MD Shoulder Anatomy Skeletal & ligamentous components: The joint is comprised of a confluence of Scapula Clavicle Humerus https://www.shoulderdoc.co.uk/article/ http/ www.shoulderdoc.co.uk/article/117777
The Shoulder Jennifer R Marks, MD Shoulder Anatomy Skeletal & ligamentous components: The joint is comprised of a confluence of Scapula Clavicle Humerus https://www.shoulderdoc.co.uk/article/ http/ www.shoulderdoc.co.uk/article/117777
FUNCTIONAL ANATOMY OF SHOULDER JOINT
 FUNCTIONAL ANATOMY OF SHOULDER JOINT ARTICULATION Articulation is between: The rounded head of the Glenoid cavity humerus and The shallow, pear-shaped glenoid cavity of the scapula. 2 The articular surfaces
FUNCTIONAL ANATOMY OF SHOULDER JOINT ARTICULATION Articulation is between: The rounded head of the Glenoid cavity humerus and The shallow, pear-shaped glenoid cavity of the scapula. 2 The articular surfaces
80b Orthopedic Massage: Technique Review and Practice! Rotator Cuff and Carpal Tunnel!
 80b Orthopedic Massage: Technique Review and Practice! Rotator Cuff and Carpal Tunnel! 80b Orthopedic Massage: Technique Review and Practice! Rotator Cuff and Carpal Tunnel! Class Outline 5 minutes Attendance,
80b Orthopedic Massage: Technique Review and Practice! Rotator Cuff and Carpal Tunnel! 80b Orthopedic Massage: Technique Review and Practice! Rotator Cuff and Carpal Tunnel! Class Outline 5 minutes Attendance,
Proteus XR/f Patient positioning guide
 Proteus XR/f Patient positioning guide PROTEUS XR/F Now a single digital x-ray room accommodates nearly all your radiographic studies. With extended tube coverage and wireless detectors, Proteus XR/f gives
Proteus XR/f Patient positioning guide PROTEUS XR/F Now a single digital x-ray room accommodates nearly all your radiographic studies. With extended tube coverage and wireless detectors, Proteus XR/f gives
Rotator Cuff and Shoulder Conditioning Program
 Rotator Cuff and Shoulder Conditioning Program Purpose of Program After an injury or surgery, an exercise conditioning program will help you return to daily activities and enjoy a more active, healthy
Rotator Cuff and Shoulder Conditioning Program Purpose of Program After an injury or surgery, an exercise conditioning program will help you return to daily activities and enjoy a more active, healthy
The Shoulder. By Patrick Ryan, Bobby Law, Jack Beaty, Alex Newhouse and Chuck Nelson
 The Shoulder By Patrick Ryan, Bobby Law, Jack Beaty, Alex Newhouse and Chuck Nelson Learning Objectives/Agenda Review the anatomy of the shoulder Describe the main diseases of the shoulder Describe the
The Shoulder By Patrick Ryan, Bobby Law, Jack Beaty, Alex Newhouse and Chuck Nelson Learning Objectives/Agenda Review the anatomy of the shoulder Describe the main diseases of the shoulder Describe the
UPPER EXTREMITY INJURIES. Recognizing common injuries to the upper extremity
 UPPER EXTREMITY INJURIES Recognizing common injuries to the upper extremity ANATOMY BONES Clavicle Scapula Spine of the scapula Acromion process Glenoid fossa/cavity Humerus Epicondyles ANATOMY BONES Ulna
UPPER EXTREMITY INJURIES Recognizing common injuries to the upper extremity ANATOMY BONES Clavicle Scapula Spine of the scapula Acromion process Glenoid fossa/cavity Humerus Epicondyles ANATOMY BONES Ulna
1-Apley scratch test.
 1-Apley scratch test. The patient attempts to touch the opposite scapula to test range of motion of the shoulder. 1-Testing abduction and external rotation( +ve sign touch the opposite scapula, -ve sign
1-Apley scratch test. The patient attempts to touch the opposite scapula to test range of motion of the shoulder. 1-Testing abduction and external rotation( +ve sign touch the opposite scapula, -ve sign
Types of Body Movements
 Types of Body Movements Bởi: OpenStaxCollege Synovial joints allow the body a tremendous range of movements. Each movement at a synovial joint results from the contraction or relaxation of the muscles
Types of Body Movements Bởi: OpenStaxCollege Synovial joints allow the body a tremendous range of movements. Each movement at a synovial joint results from the contraction or relaxation of the muscles
9/25/2014. Ricki Loar, Ph.D., APN, FNP-BC, GNP-BC. Disclosure: No Disclosures. Strategic Nurse Practitioner Solutions, LLC
 Ricki Loar, Ph.D., APN, FNP-BC, GNP-BC 1 Dr. Ricki S. Loar, Ph.D., FNP-BC, GNP-BC Clinical Director, Be Well Partners in Health Nurse Practitioner, South Naperville Family Practice Faculty, Advanced Practice
Ricki Loar, Ph.D., APN, FNP-BC, GNP-BC 1 Dr. Ricki S. Loar, Ph.D., FNP-BC, GNP-BC Clinical Director, Be Well Partners in Health Nurse Practitioner, South Naperville Family Practice Faculty, Advanced Practice
Ultrasound-Guided Shoulder Injections 인제대학교일산백병원 재활의학과 임길병
 Ultrasound-Guided Shoulder Injections 인제대학교일산백병원 재활의학과 임길병 How to improve needle visibility Advantages of Ultrasound in Procedures Real-time imaging Avoids radiation exposure But, interventions without
Ultrasound-Guided Shoulder Injections 인제대학교일산백병원 재활의학과 임길병 How to improve needle visibility Advantages of Ultrasound in Procedures Real-time imaging Avoids radiation exposure But, interventions without
SHOULDER PATIENTS. Diagnostic Shoulder Arthroscopy Technique Guide
 SHOULDER PATIENTS Diagnostic Shoulder Arthroscopy Technique Guide mi-eye 2 Indications for Use The mi-eye 2 system is indicated for use in diagnostic and operative arthroscopic and endoscopic procedures
SHOULDER PATIENTS Diagnostic Shoulder Arthroscopy Technique Guide mi-eye 2 Indications for Use The mi-eye 2 system is indicated for use in diagnostic and operative arthroscopic and endoscopic procedures
CLINICAL EXAMINATION OF THE SHOULDER JOINT 대한신경근골격연구회 분당제생병원재활의학과 박준성
 CLINICAL EXAMINATION OF THE SHOULDER JOINT 대한신경근골격연구회 분당제생병원재활의학과 박준성 Clinical Examination of the Shoulder Good history, full clinical examination Detailed knowledge of the anatomy solve the majority of
CLINICAL EXAMINATION OF THE SHOULDER JOINT 대한신경근골격연구회 분당제생병원재활의학과 박준성 Clinical Examination of the Shoulder Good history, full clinical examination Detailed knowledge of the anatomy solve the majority of
Cervical Radiculopathy: My 32 Year-Old Cyclist is Nervous What do I do on the initial visit?
 Cervical Radiculopathy: My 32 Year-Old Cyclist is Nervous What do I do on the initial visit? Scott D Boden, MD The Emory Spine Center Atlanta, Georgia History of Trauma? 2 History of Trauma? 3 Sometimes
Cervical Radiculopathy: My 32 Year-Old Cyclist is Nervous What do I do on the initial visit? Scott D Boden, MD The Emory Spine Center Atlanta, Georgia History of Trauma? 2 History of Trauma? 3 Sometimes
Shoulder: Clinical Anatomy, Kinematics & Biomechanics
 Shoulder: Clinical Anatomy, Kinematics & Biomechanics Dr. Alex K C Poon Department of Orthopaedics & Traumatology Pamela Youde Nethersole Eastern Hospital Clinical Anatomy the application of anatomy to
Shoulder: Clinical Anatomy, Kinematics & Biomechanics Dr. Alex K C Poon Department of Orthopaedics & Traumatology Pamela Youde Nethersole Eastern Hospital Clinical Anatomy the application of anatomy to
Monster Walk Stand with your feet slightly closer than shoulder-width apart in an athletic stance. Loop an elastic band around your ankles.
 Off-season Lower-Body Tennis Exercises Research conducted on elite tennis players shows that lower-body strength is the same on both the left and right sides. Therefore, lower-body training for tennis
Off-season Lower-Body Tennis Exercises Research conducted on elite tennis players shows that lower-body strength is the same on both the left and right sides. Therefore, lower-body training for tennis
Body Organizations Flashcards
 1. What are the two main regions of the body? 2. What three structures are in the Axial Region? 1. Axial Region (Goes down midline of the body) 2. Appendicular Region (limbs) 3. Axial Region (Goes down
1. What are the two main regions of the body? 2. What three structures are in the Axial Region? 1. Axial Region (Goes down midline of the body) 2. Appendicular Region (limbs) 3. Axial Region (Goes down
Work-related shoulder pain
 Work-related shoulder pain Stadler Kirsten M.B., Ch.B. (1987) (Pret), M. Med. (Orthop) (1998) (Stell.), Orthopaedic Surgeon, Room 333, Louis Leipoldt Medical Centre, Broadway Street, Bellville Cape Town
Work-related shoulder pain Stadler Kirsten M.B., Ch.B. (1987) (Pret), M. Med. (Orthop) (1998) (Stell.), Orthopaedic Surgeon, Room 333, Louis Leipoldt Medical Centre, Broadway Street, Bellville Cape Town
Checklist for Physical Examination of the Knee Muscuoskeletal Block -- Chris McGrew MD, Andrew Ashbaugh DO
 Checklist for Physical Examination of the Knee Muscuoskeletal Block -- Chris McGrew MD, Andrew Ashbaugh DO This handout is for use as a rough guide and study aid. Your instructor may perform certain maneuvers
Checklist for Physical Examination of the Knee Muscuoskeletal Block -- Chris McGrew MD, Andrew Ashbaugh DO This handout is for use as a rough guide and study aid. Your instructor may perform certain maneuvers
The Shoulder. Systematically scanning the shoulder provides extremely useful diagnostic information. The Shoulder
 1 ! The most ACCESSIBLE to sonographic exam! The most MOBILE and VULNERABLE extremity AND Systematically scanning the shoulder provides extremely useful diagnostic information! The Goal for this section
1 ! The most ACCESSIBLE to sonographic exam! The most MOBILE and VULNERABLE extremity AND Systematically scanning the shoulder provides extremely useful diagnostic information! The Goal for this section
Conservative Massive Rotator Cuff Tear Protocol
 SPORTS & ORTHOPAEDIC SPECIALISTS Conservative Massive Rotator Cuff Tear Protocol 3-4 visits over 4-6 weeks Emphasis is on AAROM and a high repetition, low weight free weight program Emphasize improved
SPORTS & ORTHOPAEDIC SPECIALISTS Conservative Massive Rotator Cuff Tear Protocol 3-4 visits over 4-6 weeks Emphasis is on AAROM and a high repetition, low weight free weight program Emphasize improved
ROTATOR CUFF DISORDERS/IMPINGEMENT
 ROTATOR CUFF DISORDERS/IMPINGEMENT Dr.KN Subramanian M.Ch Orth., FRCS (Tr & Orth), CCT Orth(UK) Consultant Orthopaedic Surgeon, Special interest: Orthopaedic Sports Injury, Shoulder and Knee Surgery, SPARSH
ROTATOR CUFF DISORDERS/IMPINGEMENT Dr.KN Subramanian M.Ch Orth., FRCS (Tr & Orth), CCT Orth(UK) Consultant Orthopaedic Surgeon, Special interest: Orthopaedic Sports Injury, Shoulder and Knee Surgery, SPARSH
Terms of Movements by Prof. Dr. Muhammad Imran Qureshi
 Terms of Movements by Prof. Dr. Muhammad Imran Qureshi Three systems of the body work in coordination to perform various movements of the body. These are: A System of Bones (Osteology), A System of Muscles
Terms of Movements by Prof. Dr. Muhammad Imran Qureshi Three systems of the body work in coordination to perform various movements of the body. These are: A System of Bones (Osteology), A System of Muscles
Connects arm to thorax 3 joints. Glenohumeral joint Acromioclavicular joint Sternoclavicular joint
 Connects arm to thorax 3 joints Glenohumeral joint Acromioclavicular joint Sternoclavicular joint Scapula Elevation Depression Protraction (abduction) Retraction (adduction) Downward Rotation Upward Rotation
Connects arm to thorax 3 joints Glenohumeral joint Acromioclavicular joint Sternoclavicular joint Scapula Elevation Depression Protraction (abduction) Retraction (adduction) Downward Rotation Upward Rotation
Chapter 6 part 2. Skeletal Muscles of the Body
 Chapter 6 part 2 Skeletal Muscles of the Body Basic Principles 600 + muscles in the human body (you are required to learn 45, lucky kids)! Skeletal Muscles pull on bones Origin of a muscle = point of attachment
Chapter 6 part 2 Skeletal Muscles of the Body Basic Principles 600 + muscles in the human body (you are required to learn 45, lucky kids)! Skeletal Muscles pull on bones Origin of a muscle = point of attachment
Shoulder Pain
 www.fisiokinesiterapia.biz Shoulder Pain Outline Shoulder Anatomy and Biomechanics Patient History and Pain Patterns Etiology and Differential Diagnoses Physical Examination Stepwise Clinical Approach
www.fisiokinesiterapia.biz Shoulder Pain Outline Shoulder Anatomy and Biomechanics Patient History and Pain Patterns Etiology and Differential Diagnoses Physical Examination Stepwise Clinical Approach
BASIC ORTHOPEDIC ASSESSMENT Muscle and Joint Testing
 BASIC ORTHOPEDIC ASSESSMENT Muscle and Joint Testing The following tests are for the purpose of determining relative shortening, restriction or bind of muscle tissues. In this context the term bind in
BASIC ORTHOPEDIC ASSESSMENT Muscle and Joint Testing The following tests are for the purpose of determining relative shortening, restriction or bind of muscle tissues. In this context the term bind in
ORTHOPEDIC PRIMARY CARE Joint Injections in Primary Care. Jackson Orthopaedic Foundation
 ORTHOPEDIC PRIMARY CARE Joint Injections in Primary Care Jackson Orthopaedic Foundation Joint Injections in Primary Care Kathleen A. Geier, DNP, NP, ONC A.J. Benham, DNP, NP, ONC kgeier@jacksonortho.org
ORTHOPEDIC PRIMARY CARE Joint Injections in Primary Care Jackson Orthopaedic Foundation Joint Injections in Primary Care Kathleen A. Geier, DNP, NP, ONC A.J. Benham, DNP, NP, ONC kgeier@jacksonortho.org
Pearson Education Limited Edinburgh Gate Harlow Essex CM20 2JE England and Associated Companies throughout the world
 Pearson Education Limited Edinburgh Gate Harlow Essex CM20 2JE England and Associated Companies throughout the world Visit us on the World Wide Web at: www.pearsoned.co.uk Pearson Education Limited 2014
Pearson Education Limited Edinburgh Gate Harlow Essex CM20 2JE England and Associated Companies throughout the world Visit us on the World Wide Web at: www.pearsoned.co.uk Pearson Education Limited 2014
Continuing Education: Shoulder Stability
 Continuing Education: Shoulder Stability Anatomy & Kinesiology: The GHJ consists of the articulation of three bones: the scapula, clavicle and humerus. The scapula has three protrusions: the coracoid,
Continuing Education: Shoulder Stability Anatomy & Kinesiology: The GHJ consists of the articulation of three bones: the scapula, clavicle and humerus. The scapula has three protrusions: the coracoid,
Working with The Shoulder
 Working with The Shoulder Plus BONUS Stretching! Dr Bryan Hawley DC Housekeeping Recording will be sent out tomorrow Certificates Questions All presented today is based off OUR OWN CLINIC system Email
Working with The Shoulder Plus BONUS Stretching! Dr Bryan Hawley DC Housekeeping Recording will be sent out tomorrow Certificates Questions All presented today is based off OUR OWN CLINIC system Email
Ultrasound Guided Injections
 Ultrasound Guided Injection Technique More accurate injections Better Results! 1 Benefits: Increased Level of Certainty ie : really know how accurate PRP/Prolotherapy Avoid damage to articular cartilage
Ultrasound Guided Injection Technique More accurate injections Better Results! 1 Benefits: Increased Level of Certainty ie : really know how accurate PRP/Prolotherapy Avoid damage to articular cartilage
Body Planes & Positions
 Learning Objectives Objective 1: Identify and utilize anatomical positions, planes, and directional terms. Demonstrate what anatomical position is and how it is used to reference the body. Distinguish
Learning Objectives Objective 1: Identify and utilize anatomical positions, planes, and directional terms. Demonstrate what anatomical position is and how it is used to reference the body. Distinguish
Professor Lisa Stamp
 Professor Lisa Stamp Rheumatologist University of Otago, Christchurch 8:30-9:25 WS #65: Joint Injection Techniques 9:35-10:30 WS #75: Joint Injection Techniques (Repeated) Joint/soft tissue corticosteroid
Professor Lisa Stamp Rheumatologist University of Otago, Christchurch 8:30-9:25 WS #65: Joint Injection Techniques 9:35-10:30 WS #75: Joint Injection Techniques (Repeated) Joint/soft tissue corticosteroid
Shoulder vs Neck Pathology. Goal: Simplify Evaluation of the Painful Shoulder. Shoulder: Bony Anatomy Three major bones. Shoulder Disorders: Overview
 Goal: Simplify Evaluation of the Painful Shoulder Can be challenging Overlapping diagnoses Multiple complaints - Neck - Shoulder - Back - Arm Shoulder vs Neck Pathology Very common to have neck pain with
Goal: Simplify Evaluation of the Painful Shoulder Can be challenging Overlapping diagnoses Multiple complaints - Neck - Shoulder - Back - Arm Shoulder vs Neck Pathology Very common to have neck pain with
P V S MEMORIAL HOSPITAL LTD.
 SHOULDER XRAYS Instability Series o True AP (Grashey s) o Axillary o Stryker Notch view o True AP in Internal rotation o Scapular Y view o West Point view for Bony Bankart ( looks like modif axillary view)
SHOULDER XRAYS Instability Series o True AP (Grashey s) o Axillary o Stryker Notch view o True AP in Internal rotation o Scapular Y view o West Point view for Bony Bankart ( looks like modif axillary view)
Evidence- Based Examination of the Shoulder Presented by Eric Hegedus, PT, DPT, MHSC, OCS, CSCS Practice Sessions/Skill Check- offs
 Evidence- Based Examination of the Shoulder Practice Session & Skills Check- offs Evidence- Based Examination of the Shoulder Presented by Eric Hegedus, PT, DPT, MHSC, OCS, CSCS Practice Sessions/Skill
Evidence- Based Examination of the Shoulder Practice Session & Skills Check- offs Evidence- Based Examination of the Shoulder Presented by Eric Hegedus, PT, DPT, MHSC, OCS, CSCS Practice Sessions/Skill
Physical Exam. Jared Van Der Beek. Basics To Remember. Know the anatomy and how the muscles function.
 Physical Exam Jared Van Der Beek Jared@physio-puncture.com 1 Basics To Remember Know the anatomy and how the muscles function. Know what the special tests are looking for and understand why they are positive.
Physical Exam Jared Van Der Beek Jared@physio-puncture.com 1 Basics To Remember Know the anatomy and how the muscles function. Know what the special tests are looking for and understand why they are positive.