Clinical Masqueraders: Pediatric and Binocular Vision Cases That Aren t What They Appear Katie S. Connolly, OD, FAAO Don W. Lyon, OD, MS, FAAO
|
|
|
- Darrell Jackson
- 5 years ago
- Views:
Transcription
1 Clinical Masqueraders: Pediatric and Binocular Vision Cases That Aren t What They Appear Katie S. Connolly, OD, FAAO Don W. Lyon, OD, MS, FAAO Please silence all mobile devices and remove items from chairs so others can sit. Unauthorized recording of this session is prohibited.
2 Disclosure Statement: Nothing to disclose
3 Patient 1: 11 Year Old Caucasian Male Long Time Patient Seen Since Age 4 Cc Routine Exam Mother and patient so not have any complaints, no medications, no reported health problems VA 20/20 Distance and Near All BV testing normal Pupils normal APD Low hyperopic prescription External health normal OU Internal health..


4 Baseline OCT This is the previous patient, similar appearance with this patient
5 REFER Letter to Pediatrician indicating diagnosis and need for MRI and possible Lumbar Puncture Pediatrician wanted patient seen by ophthalmologist before heading down that route Patient saw OMD who agreed with diagnosis of Papilledema and sent off to neuro for appointment 3 months later received MRI, which was normal, and subsequent LP Opening pressure >580mm Dx Pseudo tumor Started Diamox Patient does not fit typical clinical picture: Male Overweight, 284 lbs. at Neuro appt



6 Repeat OCTs Baseline 2 months 3 months 5 months
7 Repeat Visual Fields
8 Patient is now 15 years old Still being followed by Neuro PCP wanted patient followed by OMD, mother refused stayed with us Continuous contact between Neuro and us on overall health and visual system Case complicated by additional health issues, Sleep Apnea, DM type 1.5, HTN, gaining weight Long term patient
9 Clinical Pearls Not all conditions follow the typical clinical picture Order the test(s) you are comfortable with, refer when needed Stand your ground on your concerns and Dx
10 Patient 2 10 year old Caucasian Male Patient here for routine comprehensive eye exam. LEE 1 year, Diagnosed with unspecified amblyopia. No treatment beyond habitual Rx, RTC 1 year. Short stature, hearing aid in left ear. No medications Results from previous exam VA 20/25 OD, 20/80 OS, Cover test orthophoric HAB Rx OD x025, OS x005 Ocular health normal Results from Current exam VA 20/25 OD, 20/200 OS, Cover test 15pd LXT Distance Stereo, -global, 400 local HAB Rx OD x025, OS x005 Ocular health


11 Patient 2 10 year old Caucasian Male 0.1/0.1 double ring sign mild vessel tortuosity 0.05/0.05 double ring, marked vessel tortuosity
12 Patient 2 10 year old Caucasian Male Diagnosis: NOT unspecified amblyopia If you do not know the reason for loss of visual acuity, diagnose Unspecified visual loss H54.7 To diagnose amblyopia, must have association, refractive, strabismic, form deprivation Bilateral optic nerve hypoplasia, (OS>OD) with reduced visual acuity. Order MRI, will call parents with the results.
13 Patient 2 10 year old Caucasian Male The patient was referred to his Pediatrician and to Pediatric Endocrinology. Patient was started on growth hormones. Since patient had constant exotropia patching was initiated to see if visual acuity could be improved in left eye patient lost to follow-up. Clinical Pearls Forget Unspecified Amblyopia is a diagnosis, DO NOT USE IT Cases with bilateral optic nerve hypoplasia imaging should be considered Cases with associated risk factor(s) for amblyopia and ocular health problem, visual acuity still may be improved through traditional amblyopic treatments.

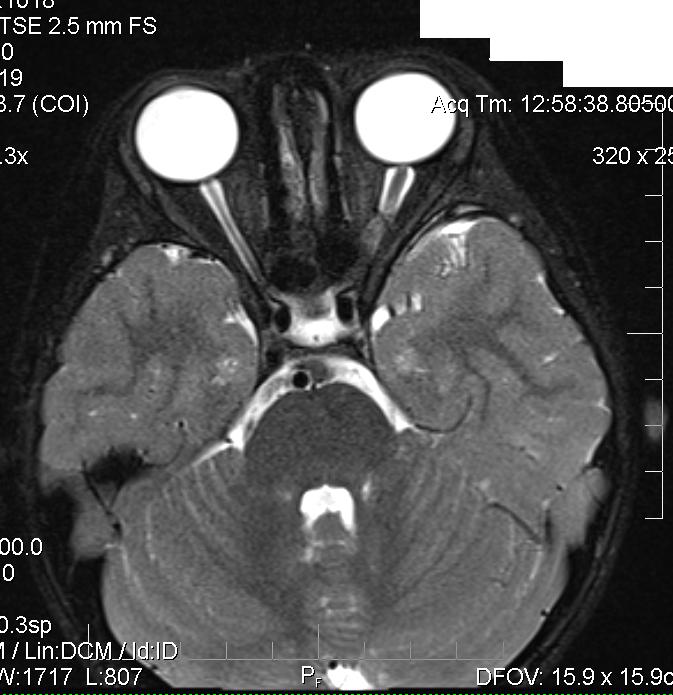
14 Patient 2 10 year old Caucasian Male Results of MRI atrophy of the left and possibly right optic nerve along with a deficient septum pellucidum (SP) anteriorly. These results are suggestive of Septo-Optic Dysplasia, [DeMorsier s Syndrome] Axial flair image demonstrating absence of the septum pellucidum. uhrad.com-neurology Imaging Teaching Files
15 Septo-Optic Dysplasia A congenital malformation characterized by: optic nerve hypoplasia (ONH) Absence of the septum pellucidum Pituitary hormone deficiencies. 30% of patients will have all three findings Additional clinical signs may include Strabismus Nystagmus Decreased visual acuity

16 Patient 3: 6 Year Old Caucasian Female Referral for strabismus and amblyopia Previous visual acuity: 20/60 OD 20/20 OS Unremarkable systemic health, no allergies, no medications Normal birth and development
17 Patient 3: Entrance Evaluation Visual acuity (adhesive patch, single surround): 20/300 OD 20/20 OS No stereo, constant right eye suppression 30 PD right exotropia distance and near
18 Health/Refractive Error Anterior unremarkable Posterior unremarkable ONHs well perfused, symmetric in size Macula flat with foveal reflex Cycloplegic Retinoscopy: OD: x180 OS: x180

19 Assessment and Plan Assessment: Strabismic Amblyopia, right eye Plan Extensive education Rx patching OS 4-6 hours per day Referral to peds ophthalmology per parent request
20 Summary of Visits VA OD VA OS Plan 4 months 20/320 20/16 Up patching to 6 hrs/day 8.5 months 20/250 20/16 Cont patching 6 hrs/day. Consult with Ophthalmology. Order MRI.


21 MRI Results
22 Management Pearls Sit back and look at the big picture Don t forget about relative amblyopia Keep the pediatrician in the loop Be clear in your notes to ophthalmology
 CT Ortho, but marked occlusion preference noted Bruckner Whiter, brighter reflex OS Stereo no measurable stereo Pupils, EOM normal Anterior Health normal")
23 Patient 4: 5 year old African American Male Parents concerned with a white flash seen in photographs for the last eight months No medical conditions, normal birth, no medications Clinical exam VA 20/20 OD 20/150 OS, (with eccentric viewing) CT Ortho, but marked occlusion preference noted Bruckner Whiter, brighter reflex OS Stereo no measurable stereo Pupils, EOM normal Anterior Health normal OD, OS
24 Patient 4: Internal Assessment Internal Health OD normal 0.3 CD, well perfused OS Initial Dx Coat s Disease, refer to Riley for FA and Treatment



25 Coats FA

26 Coat s Clinical Pearl One of the most litigious diagnoses for OD, OMD, pediatricians Can be misdiagnosed as amblyopia Can be misdiagnosed as retinoblastoma Prompt treatment needed to hopefully achieve good visual prognosis
27 Patient 5: 9 Month Old Referral from pediatrician Abnormal esotropia OS, x 2 months, worsening White pupil in pictures Able to grab toys and spot people across the room

28 Patient 5: 9 Month Old Initial Visit VAs: 20/63 OU, strong occlusion preference 10 PD Intermittent left esotropia Anterior Chamber Angles: 4+ OD, 1+ OS

29 Left Eye



30 Right Eye



31 MRI
32 Prevalence/Genetics Most common eye cancer of childhood Requires mutation in both RB1 genes Bilateral 40% of cases Assumed hereditary/germline Unilateral 60% of cases Majority sporadic Detection 2/3 are diagnosed by 2 years of age
33 Treatment Chemotherapy OD: red diode and argon laser on new tumors and those not regressing OS: No anterior chamber infiltration, No optic nerve infiltration, eventual enucleation
34 Management Pearls Always dilate children, ensure you see the entire posterior pole If you want something done quickly, call Use these cases to educate those around you about what you do
35 Patient 6: 27 Year Old Caucasian Male This primary care exam Complaint of decreased vision and a shadow on his right side that seemed to be worsening or creeping into his central vision Was in for regular exam, the year before he had been diagnosed with Microtropia OS and resultant amblyopia 4 BO test was inconclusive at time of examination FDT had scattered defects Referred to BV/Peds for assessment of Microtrope with suggested 24-2 HVF due to the FDT findings.
36 Binocular Assessment VA 20/30 OD, 20/70 OS (was 20/50 previous year) CT 4 EP Dist. and Near NPC BON Pupils Grade 1 APD OS Color 10/10 OD, 9/10 OS Stereo 20 arc Ref X070 OD X105 OS External health Normal Internal health normal Versions smooth and full MEM OD, OS 4-Base Out inconclusive Worth Dot inconsistent results


37 Visual Field Results
38 Assessment and Plan 1. Vision loss unknown origin, results either inconclusive or inconsistent with diagnosis of amblyopia 2. Patient education that vision loss may be organic in nature. Recommended MRI. Patient does not have medical insurance and needs to discuss costs with wife prior to referral. Educated further on possible severity and not being imaged or further tested. Gave patient information on Volunteers in Medicine program. Patient called next day agreeing and MRI was scheduled.

39 MRI Results Pituitary prolactinoma, (18mmX23mmX18mm)with severe cisternal optic nerve and chiasmal compression. Subacute hemorrhagic components along left anterior border. Tumoral involvement left cavernous sinus. Referral to neurologist made
40 Neurologist Report 1. Neuro report indicated that patient detailed having problems with his left eye since childhood, told was a bad test taker for visual fields. 2. Discussed treatment options, decision was made to monitor and treat underlying condition by decreasing amount of prolactin in the body


41 MRI Comparison August 2011 November 2013


42 Follow-Up Patient has returned twice since the diagnosis of pituitary tumor. BVA 20/20 OD 20/25 OS Patient expressed this is the best vision he s had Still on medication to control levels to stop tumor from enlarging
43 Clinical Pearls 1. Functional Amblyopia vs. Organic Vision Loss 2. Children as poor test takers on Visual Fields
44 Case 7: 18 yo Caucasian Female Presents due to blurred vision OU, x 2 weeks, distance, when starting College for the 1 st time, worsens throughout the day as she transitions from distance to near more Test Visual Acuity Entrance Testing Cover Test Result 20/20 OD/OS PERRLA SAFE Matrix Clear Ortho at distance 2^ Esophoria at near NRA/PRA +1.25/-2.00 Amplitude of Accomm Vergence Ranges Ocular Health Age appropriate Reduced BO at near Unremarkable Macula flat, +FLR 0.20 C/D with good color
45 Case 7: Follow-up Now complaining of diplopia X 2 weeks, constant, worst in left gaze Associated droopy right upper eye lid x 1.5 weeks Associated mild headaches, behind right eye x 1 month Mild blur at distance now constant, worst in the left eye
46 Case 7: Follow-up Test Visual Acuity Pupils EOMS Result 20/20 OD, OS with contact lenses Intermittent anisocoria OD>OS, reactive pupils Restriction of the right eye in superior left gaze (up and in) Cover Test Red Lens Test Anterior Seg Posterior Seg 15^ RXT 7^ RHypoT at dist/near Exo and right hypo, worst in up and left gaze 5 mm right ptosis Macula flat with +FLR, Optic nerves well perfused with C/D of 0.20 OD, OS


47


48
49 Giant Cell Tumor 1. Rare, benign primary bone tumor 2. Locally aggressive % of all benign bone tumors, usually in the epiphysis of long bones 4. 2% of cases present in the skull Ethmoid, temporal and sphenoid bones most commonly 5. Causes osteolytic bone destruction by formation of osteoclasts 6. Diagnosed via microscopic analysis after biopsy
50 Case 7: Resolution of Case 1. Underwent transphenoid approach resection 2 weeks after diagnosis treatments of proton beam radiation due to incomplete resection 3. 4 injections of Denosumab 4. Diplopia fully resolved, stable 2 years later, monitored every 3-6 months with MRI
51 Case 8: 58 yo Caucasian Male 1. Referred for diplopia Onset 5 days prior, horizontal, bilateral, worst when driving, worsening 2. Previous Evaluation: (3 days prior) 8^ LET distance/near Full EOMs, diplopia in right gaze Normal pupils/confrontations 0.25/0.25 C/Ds with good color and distinct marings 3. H/O high cholesterol. Taking Simvastatin
52 Case 8: Initial Visit Testing: Visual Acuity: 20/25 OD/OS EOMs: unable to abduct OD, full OS CT: 20^ RET distance and near Subjective prism eval: 20^ BO distance None for 20 cm and closer Red Lens Over OD IOP, Ocular Health unremarkable R Gaze

53 Case 8: Initial Evaluation 1. Assessment: 2. Plan: Cranial Nerve VI Palsy, Right side Fit pt with 20 PD Fresnel over right lens for driving Contact PCP via phone to discuss ordering lab work/imaging.
54 Case 8: Lab Work/MRI 1. Basic Metabolic Profile Sodium, Potassium, Chloride BUN, Creatinine, Calcium Anion Gap Osmolality, Calc GFR Hgb A1C 5. MRI? If less than 45 yo Between and no vasculopathic risk Pain, papilledema, bilateral or h/o cancer 2. CBC with platelets 3. Full neuro evaluation 4. Additional lab work? ESR/CRP RPR, Lyme Titer, FTA-ABS
55 Case 8: Resolution of Case 1. Lab work unremarkable 2. MRI unremarkable 3. Diagnosis?? Idiopathic viral?? 4. Slowly reduced prism over first year for driving. Now wearing 8^ BO for driving and none for other activities
56 Case 8: Management Pearls 1. Don t be afraid to assist the PCP with what to order 2. Their knowledge on the subject could be variable 3. Keep them informed on the health of the ONH Helps determine need for imaging and certain lab work 4. If unable to efficiently and effectively work with the PCP, order yourself. 5. Consider Fresnel prisms for specific tasks
Amblyopia 101: How to use Current Amblyopia Research in Clinical Practice
 Amblyopia 101: How to use Current Amblyopia Research in Clinical Practice Valerie M. Kattouf O.D. Chief, Pediatric/Binocular Vision Service FAAO, FCOVD Illinois College of Optometry Associate Professor
Amblyopia 101: How to use Current Amblyopia Research in Clinical Practice Valerie M. Kattouf O.D. Chief, Pediatric/Binocular Vision Service FAAO, FCOVD Illinois College of Optometry Associate Professor
Amblyopia Definition 9/25/2017. Strabismic Amblyopia. Amblyopia 101: How to use Current Amblyopia Research in Clinical Practice
 Amblyopia 101: How to use Current Amblyopia Research in Clinical Practice Valerie M. Kattouf O.D. Chief, Pediatric/Binocular Vision Service FAAO, FCOVD Illinois College of Optometry Associate Professor
Amblyopia 101: How to use Current Amblyopia Research in Clinical Practice Valerie M. Kattouf O.D. Chief, Pediatric/Binocular Vision Service FAAO, FCOVD Illinois College of Optometry Associate Professor
2. The clinician will know how to manage common pediatric ocular diseases
 Ida Chung, OD, MSHE, FCOVD, FAAO Western University College of Optometry Associate Professor/Assistant Dean of Learning 309 E. Second Street, Pomona, CA 91766 Office: 909 938 4140 Email: ichung@westernu.edu
Ida Chung, OD, MSHE, FCOVD, FAAO Western University College of Optometry Associate Professor/Assistant Dean of Learning 309 E. Second Street, Pomona, CA 91766 Office: 909 938 4140 Email: ichung@westernu.edu
Case Example BE 6 year old male
 Goals for this lecture Understand how to properly diagnose amblyopia Understand how to utilize patching and atropine in therapy Learn about the role of vision therapy Amblyopia: To See or Not To See Discuss
Goals for this lecture Understand how to properly diagnose amblyopia Understand how to utilize patching and atropine in therapy Learn about the role of vision therapy Amblyopia: To See or Not To See Discuss
Clinical Pearls: Infant vision examination Deborah Orel-Bixler, PhD, OD University of California, Berkeley School of Optometry
 Clinical Pearls: Infant vision examination Deborah Orel-Bixler, PhD, OD University of California, Berkeley School of Optometry Recommended ages for examinations Recommended populations Recommendations
Clinical Pearls: Infant vision examination Deborah Orel-Bixler, PhD, OD University of California, Berkeley School of Optometry Recommended ages for examinations Recommended populations Recommendations
Management of Diplopia Indiana Optometric Association Annual Convention April 2018 Kristine B. Hopkins, OD, MSPH, FAAO
 Management of Diplopia Indiana Optometric Association Annual Convention April 2018 Kristine B. Hopkins, OD, MSPH, FAAO For patients with diplopia, the clinician must differentiate monocular from binocular
Management of Diplopia Indiana Optometric Association Annual Convention April 2018 Kristine B. Hopkins, OD, MSPH, FAAO For patients with diplopia, the clinician must differentiate monocular from binocular
Pediatric Clinical Pearls. Valerie M. Kattouf O.D., FAAO, FCOVD Illinois College of Optometry Chicago, IL
 Pediatric Clinical Pearls Valerie M. Kattouf O.D., FAAO, FCOVD Illinois College of Optometry Chicago, IL Pediatric Clinical Pearls Collecting exam data / Modification of exam techniques Determining the
Pediatric Clinical Pearls Valerie M. Kattouf O.D., FAAO, FCOVD Illinois College of Optometry Chicago, IL Pediatric Clinical Pearls Collecting exam data / Modification of exam techniques Determining the
The Management of Infant Aphakia
 The Management of Infant Aphakia Christina Twardowski O.D., FAAO Please silence all mobile devices and remove items from chairs so others can sit. Unauthorized recording of this session is prohibited.
The Management of Infant Aphakia Christina Twardowski O.D., FAAO Please silence all mobile devices and remove items from chairs so others can sit. Unauthorized recording of this session is prohibited.
How would you explain and how would you get informed consent?
 Q: Picture of child with esotropia, Primary, left + right gaze does not abduct either eye What is DDx? How would you examine ptn? How would you differentiate between bilateral 6 th and cross fixation?
Q: Picture of child with esotropia, Primary, left + right gaze does not abduct either eye What is DDx? How would you examine ptn? How would you differentiate between bilateral 6 th and cross fixation?
Ocular Manifestations of Systemic Disease: Grand Rounds Kimberly K. Reed, O.D., FAAO
 Ocular Manifestations of Systemic Disease: Grand Rounds Kimberly K. Reed, O.D., FAAO Course description: This course describes several ocular presentations that result from a systemic disease or condition.
Ocular Manifestations of Systemic Disease: Grand Rounds Kimberly K. Reed, O.D., FAAO Course description: This course describes several ocular presentations that result from a systemic disease or condition.
Evidence-Based Refractive Prescribing for Pediatric Patients
 Evidence-Based Refractive Prescribing for Pediatric Patients Graham B. Erickson, OD, FAAO, FCOVD Pacific University College of Optometry Dr. Erickson has no financial interests to disclose Overview Of
Evidence-Based Refractive Prescribing for Pediatric Patients Graham B. Erickson, OD, FAAO, FCOVD Pacific University College of Optometry Dr. Erickson has no financial interests to disclose Overview Of
Complicated Refractive Cases and their Management
 Complicated Refractive Cases and their Management COPE 42302-GO Kristin Anderson, OD, FAAO Complicated Refractive Cases and Prescribing Considerations Kristin K. Anderson, OD Professor Southern College
Complicated Refractive Cases and their Management COPE 42302-GO Kristin Anderson, OD, FAAO Complicated Refractive Cases and Prescribing Considerations Kristin K. Anderson, OD Professor Southern College
How Strongly Do You Feel That This Patient Has Glaucoma? % % % % %
 My Favorite Cases Anthony B. Litwak, OD, FAAO VA Medical Center Baltimore, Maryland Dr. Litwak is a speaker and on advisory boards for Alcon and Zeiss Meditek CASE CR 35 yohf Neg PMH +FOH mother and grandmother
My Favorite Cases Anthony B. Litwak, OD, FAAO VA Medical Center Baltimore, Maryland Dr. Litwak is a speaker and on advisory boards for Alcon and Zeiss Meditek CASE CR 35 yohf Neg PMH +FOH mother and grandmother
My Favourite Cases Anthony B. Litwak, OD, FAAO VA Medical Center Baltimore, MD
 My Favourite Cases Anthony B. Litwak, OD, FAAO VA Medical Center Baltimore, MD Dr. Litwak is a speaker and on advisory boards for Alcon and Zeiss Meditek CASE CR! 35 YOHF! Neg PMH! +FOH mother and grandmother
My Favourite Cases Anthony B. Litwak, OD, FAAO VA Medical Center Baltimore, MD Dr. Litwak is a speaker and on advisory boards for Alcon and Zeiss Meditek CASE CR! 35 YOHF! Neg PMH! +FOH mother and grandmother
Financial Disclosures. Amblyopia: What the Studies Show. Acknowledgements. Development of PEDIG. PEDIG Protocols. Amblyopia Treatment Dogma Pre-ATS
 Amblyopia: What the Studies Show Zachary S. McCarty, OD Financial Disclosures Acknowledgements Development of PEDIG PEDIG is a network dedicated to conducting multi-center studies in strabismus, amblyopia,
Amblyopia: What the Studies Show Zachary S. McCarty, OD Financial Disclosures Acknowledgements Development of PEDIG PEDIG is a network dedicated to conducting multi-center studies in strabismus, amblyopia,
Controversies in Pediatric Refractive Development Timothy Hug, OD, FAAO
 Controversies in Pediatric Refractive Development Timothy Hug, OD, FAAO Please silence all mobile devices and remove items from chairs so others can sit. Unauthorized recording of this session is prohibited
Controversies in Pediatric Refractive Development Timothy Hug, OD, FAAO Please silence all mobile devices and remove items from chairs so others can sit. Unauthorized recording of this session is prohibited
This 3-year-old presented with an alternating esotropia of two-month duration. Her initial
 Management of Significant Refractive Error Abstract: This case report is of a child who was referred to me by a practicing optometrist. This 3-year-old presented with an alternating esotropia of two-month
Management of Significant Refractive Error Abstract: This case report is of a child who was referred to me by a practicing optometrist. This 3-year-old presented with an alternating esotropia of two-month
10/4/2016. Organic (systemic) Form deprivation (structural) Strabismic Refractive Isometric Anisometric
 Form deprivation (structural) Strabismic Refractive Isometric Anisometric") Marc B. Taub, OD, MS, FAAO, FCOVD Chief, Vision Therapy and Rehabilitation Southern College of Optometry Editor in Chief, Optometry & Visual Performance A difference in the VA of the two eyes of at least
Marc B. Taub, OD, MS, FAAO, FCOVD Chief, Vision Therapy and Rehabilitation Southern College of Optometry Editor in Chief, Optometry & Visual Performance A difference in the VA of the two eyes of at least
Re-Double. Ron Teed, M.D. 12 January 2007 Vanderbilt Eye Institute. Alfred Bielschowsky
 Re-Double Ron Teed, M.D. 12 January 2007 Vanderbilt Eye Institute Alfred Bielschowsky Patient History I cc: vertical binocular diplopia 63 yo male with 4 week history of diplopia; first intermittent, then
Re-Double Ron Teed, M.D. 12 January 2007 Vanderbilt Eye Institute Alfred Bielschowsky Patient History I cc: vertical binocular diplopia 63 yo male with 4 week history of diplopia; first intermittent, then
Neuro-Ocular Grand Rounds
 Neuro-Ocular Grand Rounds Anthony B. Litwak,OD, FAAO VA Medical Center Baltimore, Maryland Dr. Litwak is on the speaker and advisory boards for Alcon and Zeiss Meditek COMMON OPTIC NEUROPATHIES THAT CAN
Neuro-Ocular Grand Rounds Anthony B. Litwak,OD, FAAO VA Medical Center Baltimore, Maryland Dr. Litwak is on the speaker and advisory boards for Alcon and Zeiss Meditek COMMON OPTIC NEUROPATHIES THAT CAN
My Doc told me I needed an eye exam because.. Bruce Onofrey, OD, RPh, FAAO Professor, U. Houston UEI
 My Doc told me I needed an eye exam because.. Bruce Onofrey, OD, RPh, FAAO eyedoc3@aol.com Professor, U. Houston UEI Drugs can blind you (the patient) Cataract Glaucoma Uveitis Dry eye Macular disease
My Doc told me I needed an eye exam because.. Bruce Onofrey, OD, RPh, FAAO eyedoc3@aol.com Professor, U. Houston UEI Drugs can blind you (the patient) Cataract Glaucoma Uveitis Dry eye Macular disease
The WORST-CASE SCENARIO Survival Handbook
 The WORST-CASE SCENARIO Survival Handbook I certify: I have no proprietary interest in the tested product I have no equity interest or significant payments by the sponsor of a covered study Lecture content
The WORST-CASE SCENARIO Survival Handbook I certify: I have no proprietary interest in the tested product I have no equity interest or significant payments by the sponsor of a covered study Lecture content
Neuro-Ocular Grand Rounds Anthony B. Litwak,OD, FAAO VA Medical Center Baltimore, Maryland
 Neuro-Ocular Grand Rounds Anthony B. Litwak,OD, FAAO VA Medical Center Baltimore, Maryland Dr. Litwak is on the speaker and advisory boards for Alcon and Zeiss Meditek COMMON OPTIC NEUROPATHIES THAT CAN
Neuro-Ocular Grand Rounds Anthony B. Litwak,OD, FAAO VA Medical Center Baltimore, Maryland Dr. Litwak is on the speaker and advisory boards for Alcon and Zeiss Meditek COMMON OPTIC NEUROPATHIES THAT CAN
ASSESSING THE EYES. Structures. Eyelids Extraocularmuscles Eyelashes Lacrimal glands: Lacrimal ducts Cornea Conjunctiva Sclera Pupils Iris.
 ASSESSING THE EYES Structures External Eyelids Extraocularmuscles Eyelashes Lacrimal glands: Lacrimal ducts Cornea Conjunctiva Sclera Pupils Iris 1 2 Structures Internal Optic disc Physiological cup Retinal
ASSESSING THE EYES Structures External Eyelids Extraocularmuscles Eyelashes Lacrimal glands: Lacrimal ducts Cornea Conjunctiva Sclera Pupils Iris 1 2 Structures Internal Optic disc Physiological cup Retinal
No Financial Interest
 Pituitary Apoplexy Michael Vaphiades, D.O. Professor Department of Ophthalmology, Neurology, Neurosurgery University of Alabama at Birmingham, Birmingham, AL No Financial Interest N E U R O L O G I C
Pituitary Apoplexy Michael Vaphiades, D.O. Professor Department of Ophthalmology, Neurology, Neurosurgery University of Alabama at Birmingham, Birmingham, AL No Financial Interest N E U R O L O G I C
Tiffany L. Kruger, D.O. Children s Hospital of Michigan Wayne State University/Kresge Eye Institute
 Pediatric Cases Nt Not To Be Missed Tiffany L. Kruger, D.O. Pediatric Ophthalmology Fellow Children s Hospital of Michigan Wayne State University/Kresge Eye Institute Case Presentation CC: Left eye turns
Pediatric Cases Nt Not To Be Missed Tiffany L. Kruger, D.O. Pediatric Ophthalmology Fellow Children s Hospital of Michigan Wayne State University/Kresge Eye Institute Case Presentation CC: Left eye turns
Pediatric Headaches: Is It Their Eyes? Catherine McDaniel, OD, MS, FAAO
 Pediatric Headaches: Is It Their Eyes? Catherine McDaniel, OD, MS, FAAO Please silence all mobile devices and remove items from chairs so others can sit. Unauthorized recording of this session is prohibited.
Pediatric Headaches: Is It Their Eyes? Catherine McDaniel, OD, MS, FAAO Please silence all mobile devices and remove items from chairs so others can sit. Unauthorized recording of this session is prohibited.
Reena Patel, OD, FAAO
 Reena Patel, OD, FAAO 5 to 10% of all preschool-aged children o Significant refractive error o Amblyopia Poor vision o Strabismus Misalignment of the eyes Myopia o nearsightedness Hyperopia o farsightedness
Reena Patel, OD, FAAO 5 to 10% of all preschool-aged children o Significant refractive error o Amblyopia Poor vision o Strabismus Misalignment of the eyes Myopia o nearsightedness Hyperopia o farsightedness
4/28/2014. Reena Patel, OD, FAAO. 5 to 10% of all preschool-aged children. Myopia. Hyperopia. Astigmatism. High refractive error
 5 to 10% of all preschool-aged children o Significant refractive error o Amblyopia Poor vision Reena Patel, OD, FAAO Misalignment of the eyes Myopia o nearsightedness Hyperopia o farsightedness Inward
5 to 10% of all preschool-aged children o Significant refractive error o Amblyopia Poor vision Reena Patel, OD, FAAO Misalignment of the eyes Myopia o nearsightedness Hyperopia o farsightedness Inward
Unilateral Optic Nerve Hypoplasia in a patient desiring surgical treatment for exotropia
 Unilateral Optic Nerve Hypoplasia in a patient desiring surgical treatment for exotropia Michael S. Floyd, MD, Christy Benson, and Susannah Q. Longmuir, MD June 13, 2011 Chief Complaint: 17- year- old
Unilateral Optic Nerve Hypoplasia in a patient desiring surgical treatment for exotropia Michael S. Floyd, MD, Christy Benson, and Susannah Q. Longmuir, MD June 13, 2011 Chief Complaint: 17- year- old
Author: Ida Lucy Iacobucci, 2015
 Author: Ida Lucy Iacobucci, 2015 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution-NonCommercial-Share Alike 4.0 License: http://creativecommons.org/licenses/by-nc-sa/4.0/
Author: Ida Lucy Iacobucci, 2015 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution-NonCommercial-Share Alike 4.0 License: http://creativecommons.org/licenses/by-nc-sa/4.0/
Carotid Cavernous Fistula
 Chief Complaint: Double vision. Carotid Cavernous Fistula Alex W. Cohen, MD, PhD; Richard Allen, MD, PhD May 14, 2010 History of Present Illness: A 46 year old female patient presented to the Oculoplastics
Chief Complaint: Double vision. Carotid Cavernous Fistula Alex W. Cohen, MD, PhD; Richard Allen, MD, PhD May 14, 2010 History of Present Illness: A 46 year old female patient presented to the Oculoplastics
Author: Ida Lucy Iacobucci, 2015
 Author: Ida Lucy Iacobucci, 2015 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution-NonCommercial-Share Alike 4.0 License: http://creativecommons.org/licenses/by-nc-sa/4.0/
Author: Ida Lucy Iacobucci, 2015 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution-NonCommercial-Share Alike 4.0 License: http://creativecommons.org/licenses/by-nc-sa/4.0/
Communicating with patients about alternative therapies: A case of optic nerve hypoplasia
 Communicating with patients about alternative therapies: A case of optic nerve hypoplasia Chief Complaint:14 year old male with poor vision since birth History of Present Illness: An otherwise healthy
Communicating with patients about alternative therapies: A case of optic nerve hypoplasia Chief Complaint:14 year old male with poor vision since birth History of Present Illness: An otherwise healthy
INFANTILE EXOTROPIA. Lionel Kowal
 INFANTILE EXOTROPIA Lionel Kowal INFANTILE XT Usage often imprecise Variation in definitions number of investigators? onset day 1 of life? constant / intermittent Any / large angle? Associated systemic
INFANTILE EXOTROPIA Lionel Kowal INFANTILE XT Usage often imprecise Variation in definitions number of investigators? onset day 1 of life? constant / intermittent Any / large angle? Associated systemic
Learn Connect Succeed. JCAHPO Regional Meetings 2017
 Learn Connect Succeed JCAHPO Regional Meetings 2017 NO FINANCIAL DISCLOSURES Technician s Role in Neuro-Ophthalmology Workup Beth Koch COT, ROUB Cleveland 9/16/2017 What Tests Are You Expected To Perform?
Learn Connect Succeed JCAHPO Regional Meetings 2017 NO FINANCIAL DISCLOSURES Technician s Role in Neuro-Ophthalmology Workup Beth Koch COT, ROUB Cleveland 9/16/2017 What Tests Are You Expected To Perform?
Help! My Baby s Eyes Are Crossed (or Something!)
") Help! My Baby s Eyes Are Crossed (or Something!) Madhuri Chilakapati, MD Ophthalmology Chief Complaint My baby has a lazy eye The eyes move funny The eyes don t move together The eyes get stuck The eyes
Help! My Baby s Eyes Are Crossed (or Something!) Madhuri Chilakapati, MD Ophthalmology Chief Complaint My baby has a lazy eye The eyes move funny The eyes don t move together The eyes get stuck The eyes
OPHTHALMOLOGIC PEARLS FOR THE NON- OPHTHALMOLOGIST. David G. Gross D.O. Deen-Gross Eye Centers Merrillville-Hobart Deengrosseye.
 OPHTHALMOLOGIC PEARLS FOR THE NON- OPHTHALMOLOGIST David G. Gross D.O. Deen-Gross Eye Centers Merrillville-Hobart Deengrosseye.com A FEW OF THE AREAS WE WILL DISCUSS Red Eye Glaucoma Neuro ophthalmic tid
OPHTHALMOLOGIC PEARLS FOR THE NON- OPHTHALMOLOGIST David G. Gross D.O. Deen-Gross Eye Centers Merrillville-Hobart Deengrosseye.com A FEW OF THE AREAS WE WILL DISCUSS Red Eye Glaucoma Neuro ophthalmic tid
Financial Disclosures
 Update on Amblyopia Treatment: Evidence-based Practice Financial Disclosures No financial interests directly related to this presentation Yi Pang, O.D., Ph.D. Professor Illinois College of Optometry 2018
Update on Amblyopia Treatment: Evidence-based Practice Financial Disclosures No financial interests directly related to this presentation Yi Pang, O.D., Ph.D. Professor Illinois College of Optometry 2018
RETINOSCOPY HANDBOOK FOR CLINICIANS
 RETINOSCOPY HANDBOOK FOR CLINICIANS Author: Sarah Wassnig B.Optom(OcTher), MPH New England College of Optometry created this handbook for the use of Orbis International trainees. This publication is the
RETINOSCOPY HANDBOOK FOR CLINICIANS Author: Sarah Wassnig B.Optom(OcTher), MPH New England College of Optometry created this handbook for the use of Orbis International trainees. This publication is the
Von Noorden defines amblyopia
 MEDULLATED NERVE FIBERS CONFOUNDING OR CONTRIBUTING TO AMBLYOPIA ACASE REPORT AND REVIEW Marie I. Bodack, O.D. Abstract Medullated, or myelinated nerve fibers affect between 0.57 to 1% of the population.
MEDULLATED NERVE FIBERS CONFOUNDING OR CONTRIBUTING TO AMBLYOPIA ACASE REPORT AND REVIEW Marie I. Bodack, O.D. Abstract Medullated, or myelinated nerve fibers affect between 0.57 to 1% of the population.
A Curious Case of Bilateral Optic Disc Edema Brittney Dautremont, DO, MPH
 A Curious Case of Bilateral Optic Disc Edema Brittney Dautremont, DO, MPH PGY2 Ophthalmology Resident Grandview Medical Center Dayton, OH CASE PRESENTATION 51 year old white female presenting with blurred
A Curious Case of Bilateral Optic Disc Edema Brittney Dautremont, DO, MPH PGY2 Ophthalmology Resident Grandview Medical Center Dayton, OH CASE PRESENTATION 51 year old white female presenting with blurred
Optometric Care of Children with Developmental Disabilities Kia B. Eldred, OD, FAAO Diplomate in Low Vision
 Optometric Care of Children with Developmental Disabilities Kia B. Eldred, OD, FAAO Diplomate in Low Vision kia.eldred@va.gov 1. Demographics Who is the Developmentally Delayed child? The child who is
Optometric Care of Children with Developmental Disabilities Kia B. Eldred, OD, FAAO Diplomate in Low Vision kia.eldred@va.gov 1. Demographics Who is the Developmentally Delayed child? The child who is
Shedding Light on Pediatric Cataracts. Kimberly G. Yen, MD Associate Professor of Ophthalmology Texas Children s Hospital
 Shedding Light on Pediatric Cataracts Kimberly G. Yen, MD Associate Professor of Ophthalmology Texas Children s Hospital A newborn infant presents with bilateral white cataracts. What is the best age to
Shedding Light on Pediatric Cataracts Kimberly G. Yen, MD Associate Professor of Ophthalmology Texas Children s Hospital A newborn infant presents with bilateral white cataracts. What is the best age to
OCT : retinal layers. Extraocular muscles. History. Central vs Peripheral vision. History: Temporal course. Optical Coherence Tomography (OCT)
") Optical Coherence Tomography (OCT) OCT : retinal layers 7 Central vs Peripheral vision Extraocular muscles RPE E Peripheral Vision: Rods (95 million) 30% Ganglion cells Central Vision: Cones (5 million)
Optical Coherence Tomography (OCT) OCT : retinal layers 7 Central vs Peripheral vision Extraocular muscles RPE E Peripheral Vision: Rods (95 million) 30% Ganglion cells Central Vision: Cones (5 million)
Case #1: 68 M with floaters OS
 Case #1: 68 M with floaters OS Point-of-Care Ocular Sonography for the Emergency Department Nate Teismann MD Dept of Emergency Medicine, UCSF Topics in EM 2012 Acute onset of dark spots in L eye 2 days
Case #1: 68 M with floaters OS Point-of-Care Ocular Sonography for the Emergency Department Nate Teismann MD Dept of Emergency Medicine, UCSF Topics in EM 2012 Acute onset of dark spots in L eye 2 days
Paediatric Ophthalmology Assessment. Justin Mora 2017
 Paediatric Ophthalmology Assessment Justin Mora 2017 History Visual developmental milestones Aware of people in the room, reaching for objects, following toys, alignment should be central and stable
Paediatric Ophthalmology Assessment Justin Mora 2017 History Visual developmental milestones Aware of people in the room, reaching for objects, following toys, alignment should be central and stable
DIAGNOSIS? CASE NUMBER ONE CONVERGENCE DIFFICIENCIES. Children vs. Adults. Insufficiency vs. Paralysis CONVERGENCE INSUFFICIENCY
 CONVERGENCE DIFFICIENCIES Children vs. Adults Insufficiency vs. Paralysis CASE NUMBER ONE DIAGNOSIS? 8 year boy referred from school- headaches, reading difficulties and blurred vision MY EXAMINATION 20/20-
CONVERGENCE DIFFICIENCIES Children vs. Adults Insufficiency vs. Paralysis CASE NUMBER ONE DIAGNOSIS? 8 year boy referred from school- headaches, reading difficulties and blurred vision MY EXAMINATION 20/20-
Children's Eye Assessment
 Children's Eye Assessment Dr Antony Bedggood, Children s Specialist Centre Paediatric Ophthalmologist, Cataract & Strabismus Surgeon Why kids need early referral Children s eye problems are often subtle:
Children's Eye Assessment Dr Antony Bedggood, Children s Specialist Centre Paediatric Ophthalmologist, Cataract & Strabismus Surgeon Why kids need early referral Children s eye problems are often subtle:
Article. Reverse-Engineering of Hyperopic Anisometropic Refractive Amblyopia. Leonard J. Press, OD, FAAO, FCOVD; Daniel J.
 Article Reverse-Engineering of Hyperopic Anisometropic Refractive Amblyopia Leonard J. Press, OD, FAAO, FCOVD; Daniel J. Press, OD, FCOVD Private Practice, Fair Lawn, NJ Abstract Background. Uncompensated
Article Reverse-Engineering of Hyperopic Anisometropic Refractive Amblyopia Leonard J. Press, OD, FAAO, FCOVD; Daniel J. Press, OD, FCOVD Private Practice, Fair Lawn, NJ Abstract Background. Uncompensated
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 Sensorimotor and Neurobehavioral Status Exams Page 1 of 5 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Sensorimotor and Neurobehavioral Status Exams for Optometric
Sensorimotor and Neurobehavioral Status Exams Page 1 of 5 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Sensorimotor and Neurobehavioral Status Exams for Optometric
Mom, There s Something Wrong With My Eye
 Mom, There s Something Wrong With My Eye Veeral Shah MD, PHD Texas Children's Hospital Most Common Issues Seen by the Pediatrician Emergent Ocular Issues Seen by the Pediatrician 1 What does this baby
Mom, There s Something Wrong With My Eye Veeral Shah MD, PHD Texas Children's Hospital Most Common Issues Seen by the Pediatrician Emergent Ocular Issues Seen by the Pediatrician 1 What does this baby
Neuro Ocular Grand Rounds Anthony B. Litwak, OD, FAAO VA Medical Center Baltimore, MD
 Neuro Ocular Grand Rounds Anthony B. Litwak, OD, FAAO VA Medical Center Baltimore, MD 58 YOWM! C/O I think there is something wrong with my vision, but I m not sure what it is.! +PMH for HTN, atrial fibrillation,
Neuro Ocular Grand Rounds Anthony B. Litwak, OD, FAAO VA Medical Center Baltimore, MD 58 YOWM! C/O I think there is something wrong with my vision, but I m not sure what it is.! +PMH for HTN, atrial fibrillation,
Incorporation of Vision Therapy into Daily Practice. Vision Therapy Services in a Primary Care Practice. Considerations. Management Considerations
 Incorporation of Vision Therapy into Daily Practice Vision Therapy Services in a Primary Care Practice Graham Erickson, OD, FAAO, FCOVD Pacific University College of Optometry Adequate data Consultation
Incorporation of Vision Therapy into Daily Practice Vision Therapy Services in a Primary Care Practice Graham Erickson, OD, FAAO, FCOVD Pacific University College of Optometry Adequate data Consultation
Picture of patient with apparent lid retraction and poor elevation. Shows you Orbital CT-Scan with muscle involvement including IR and asks is this
 NEUROLOGY Q: MENINGIOMAS AND SKULL (*2) Real skull is given, and you are asked to point to tuberculum sella What kind of meningioma occurs at this location? Where is the anterior clinoid process? Where
NEUROLOGY Q: MENINGIOMAS AND SKULL (*2) Real skull is given, and you are asked to point to tuberculum sella What kind of meningioma occurs at this location? Where is the anterior clinoid process? Where
Neuro-imaging for the Ophthalmologist. Karl C. Golnik, MD, MEd University of Cincinnati & The Cincinnati Eye Institute
 Neuro-imaging for the Ophthalmologist Karl C. Golnik, MD, MEd University of Cincinnati & The Cincinnati Eye Institute Neuro-ophthalmology is that subspecialty where the diagnosis is made upon reinterpretation
Neuro-imaging for the Ophthalmologist Karl C. Golnik, MD, MEd University of Cincinnati & The Cincinnati Eye Institute Neuro-ophthalmology is that subspecialty where the diagnosis is made upon reinterpretation
12/2/16. Ways to differentiate:
 Nate Lighthizer, O.D., F.A.A.O. Assistant Dean for Clinical Care Services Director of CE Chief of Specialty Care Clinics Chief of Electrodiagnostics Clinic Oklahoma College of Optometry lighthiz@nsuok.edu
Nate Lighthizer, O.D., F.A.A.O. Assistant Dean for Clinical Care Services Director of CE Chief of Specialty Care Clinics Chief of Electrodiagnostics Clinic Oklahoma College of Optometry lighthiz@nsuok.edu
University Journal of Surgery and Surgical Specialities
 University Journal of Surgery and Surgical Specialities Volume 1 Issue 1 2015 PARINAUD'S SYNDROME A CASE REPORT Basker K Shubha Raguram K Stanley Medical College Introduction: Gaze palsies are a group
University Journal of Surgery and Surgical Specialities Volume 1 Issue 1 2015 PARINAUD'S SYNDROME A CASE REPORT Basker K Shubha Raguram K Stanley Medical College Introduction: Gaze palsies are a group
The Royal College of Ophthalmologists. Parent Information Squint/Strabismus
 Parent Information Squint/Strabismus This leaflet is designed to answer some of the general queries relating to squint in childhood. The Children s Eye Care Team An OPHTHALMOLOGIST is a doctor who specialises
Parent Information Squint/Strabismus This leaflet is designed to answer some of the general queries relating to squint in childhood. The Children s Eye Care Team An OPHTHALMOLOGIST is a doctor who specialises
Is this glaucoma? Leo Semes, OD Michael Chaglasian, OD Danica Marrelli, OD. Optometry s Meeting 2015 Seattle, WA
 Is this glaucoma? Leo Semes, OD Michael Chaglasian, OD Danica Marrelli, OD Optometry s Meeting 2015 Seattle, WA Case 1. 54 WM Engineer is referred to UAB Eye Care as a glaucoma suspect. Mild myopic refractive
Is this glaucoma? Leo Semes, OD Michael Chaglasian, OD Danica Marrelli, OD Optometry s Meeting 2015 Seattle, WA Case 1. 54 WM Engineer is referred to UAB Eye Care as a glaucoma suspect. Mild myopic refractive
REMEMBER SOMETIMES TO PARENTS THE SKY IS FALLING!!! AND SOMETIMES IT IS, AND OTHER TIMES IT IS SOMETHING VERY SIMPLE
 PEDIATRIC MASQUERADERS CONFLICTS AND ACKNOWLEDGMENTS NO CONFLICTS. ALL MEDICATIONS DISCUSSED ARE WHAT I TYPICALLY USE IN CLINICAL PRACTICE. THERE ARE MANY APPROPRIATE MEDICATIONS THAT I WILL NOT MENTION.
PEDIATRIC MASQUERADERS CONFLICTS AND ACKNOWLEDGMENTS NO CONFLICTS. ALL MEDICATIONS DISCUSSED ARE WHAT I TYPICALLY USE IN CLINICAL PRACTICE. THERE ARE MANY APPROPRIATE MEDICATIONS THAT I WILL NOT MENTION.
Pearls for the Refractive Technician Fadiah Alkhawaldeh, IMBA, COT, ROUB
 Pearls for the Refractive Technician Fadiah Alkhawaldeh, IMBA, COT, ROUB Cleveland Clinic Cole Eye Institute OOS, Columbus, OH February, 2014 alkhawf@ccf.org NO FINANCIAL DISCLOSURES A Puzzle of an Eye
Pearls for the Refractive Technician Fadiah Alkhawaldeh, IMBA, COT, ROUB Cleveland Clinic Cole Eye Institute OOS, Columbus, OH February, 2014 alkhawf@ccf.org NO FINANCIAL DISCLOSURES A Puzzle of an Eye
Double Vision as a Presenting Symptom in Adults Without Acquired or Long- Standing Strabismus
 Double Vision as a Presenting Symptom in Adults Without Acquired or Long- Standing Strabismus Sara Shippman, C.O. Larisa Heiser, C.O. Kenneth R. Cohen, M.D., F.A.C.S. Lisabeth Hall, M.D. ABSTRACT Background:
Double Vision as a Presenting Symptom in Adults Without Acquired or Long- Standing Strabismus Sara Shippman, C.O. Larisa Heiser, C.O. Kenneth R. Cohen, M.D., F.A.C.S. Lisabeth Hall, M.D. ABSTRACT Background:
Objectives. Unexplained Vision Loss: Where Do I Go From Here. History. History. Drug Induced Vision Loss
 Objectives Unexplained Vision Loss: Where Do I Go From Here Denise Goodwin, OD, FAAO Coordinator, Neuro-ophthalmic Disease Clinic Pacific University College of Optometry goodwin@pacificu.edu Know the importance
Objectives Unexplained Vision Loss: Where Do I Go From Here Denise Goodwin, OD, FAAO Coordinator, Neuro-ophthalmic Disease Clinic Pacific University College of Optometry goodwin@pacificu.edu Know the importance
Strabismus. A.Medghalchi,M.D Assistant professor of ophthalmology Gilan medical science university
 Strabismus A.Medghalchi,M.D Assistant professor of ophthalmology Gilan medical science university ۳ Anatomy Of The EOM s Six Extraocular muscles surround eye: Medial Rectus Lateral Rectus Superior Rectus
Strabismus A.Medghalchi,M.D Assistant professor of ophthalmology Gilan medical science university ۳ Anatomy Of The EOM s Six Extraocular muscles surround eye: Medial Rectus Lateral Rectus Superior Rectus
Diabetes & Your Eyes
 Diabetes & Your Eyes Diabetes is a disease that occurs when the pancreas does not secrete enough insulin or the body is unable to process it properly. Insulin is the hormone that regulates the level of
Diabetes & Your Eyes Diabetes is a disease that occurs when the pancreas does not secrete enough insulin or the body is unable to process it properly. Insulin is the hormone that regulates the level of
Disclosure Ocular Anatomy and Motility
 Disclosure Ocular Anatomy and Motility Jenean Carlton BA, ABOC, NCLC President, Carlton & Associates, LLC Carlton and Associates, LLC provides communications and educational materials for the optical industry
Disclosure Ocular Anatomy and Motility Jenean Carlton BA, ABOC, NCLC President, Carlton & Associates, LLC Carlton and Associates, LLC provides communications and educational materials for the optical industry
Five diagnoses you cannot afford to miss. I will not be discussing any off label uses of drugs
 Five diagnoses you cannot afford to miss Andrew G. Lee, MD Chair Ophthalmology, Houston Methodist Hospital, Professor of Ophthalmology, Neurology, & Neurosurgery, Weill Cornell Medical College; Adjunct
Five diagnoses you cannot afford to miss Andrew G. Lee, MD Chair Ophthalmology, Houston Methodist Hospital, Professor of Ophthalmology, Neurology, & Neurosurgery, Weill Cornell Medical College; Adjunct
Dr Casey Ung. Ophthalmologist Dunedin Hospital Eye Clinic Marinoto Clinic & Specialists Dunedin
 Dr Casey Ung Ophthalmologist Dunedin Hospital Eye Clinic Marinoto Clinic & Specialists Dunedin 8:30-9:25 WS #140: Paediatric Ophthalmology 9:35-10:30 WS #150: Paediatric Ophthalmology (Repeated) Paediatric
Dr Casey Ung Ophthalmologist Dunedin Hospital Eye Clinic Marinoto Clinic & Specialists Dunedin 8:30-9:25 WS #140: Paediatric Ophthalmology 9:35-10:30 WS #150: Paediatric Ophthalmology (Repeated) Paediatric
Comparison of management options for scleral buckle exposure
 Comparison of management options for scleral buckle exposure Abstract: Scleral buckling is a technique used for repair of rhegmatogenous retinal detachment in eyes with retinal breaks. This report demonstrates
Comparison of management options for scleral buckle exposure Abstract: Scleral buckling is a technique used for repair of rhegmatogenous retinal detachment in eyes with retinal breaks. This report demonstrates
Glaucoma. Cornea. Iris
 Glaucoma Introduction Glaucoma is a group of eye diseases that can lead to blindness if not treated. Openangle glaucoma, the most common form of glaucoma, affects about 3 million Americans. Half of those
Glaucoma Introduction Glaucoma is a group of eye diseases that can lead to blindness if not treated. Openangle glaucoma, the most common form of glaucoma, affects about 3 million Americans. Half of those
Open Access Journal of Ophthalmology
 Esotropia Anurag Narula 1 * and Shilpa Singh 2 1Safdarjung Hospital, VMMC, India 2Visitech Eye Centre, India *Corresponding author: Anurag Narula, Consultant, Safdarjung Hospital, Vardhman Short Communication
Esotropia Anurag Narula 1 * and Shilpa Singh 2 1Safdarjung Hospital, VMMC, India 2Visitech Eye Centre, India *Corresponding author: Anurag Narula, Consultant, Safdarjung Hospital, Vardhman Short Communication
Pediatric Ophthalmology. Strabismus
 Pediatric Ophthalmology Strabismus Strabismus is an eye alignment condition when both eyes do not look at the same point at the same time. Strabismus most often begins in early childhood. It is sometimes
Pediatric Ophthalmology Strabismus Strabismus is an eye alignment condition when both eyes do not look at the same point at the same time. Strabismus most often begins in early childhood. It is sometimes
Esotropia - Exotropia. Carlos Eduardo Solarte MD. MPH Assistant Clinical Professor Director Residency Program Ophthalmology
 Esotropia - Exotropia Carlos Eduardo Solarte MD. MPH Assistant Clinical Professor Director Residency Program Ophthalmology Financial Disclosure and Source I have no actual or potential financial interest
Esotropia - Exotropia Carlos Eduardo Solarte MD. MPH Assistant Clinical Professor Director Residency Program Ophthalmology Financial Disclosure and Source I have no actual or potential financial interest
Neuro-Ophthalmic Masqueraders
 Neuro-Ophthalmic Masqueraders Leonid Skorin, Jr., OD, DO, MS, FAAO, FAOCO Mayo Clinic Health System in Albert Lea Denise Goodwin, OD, FAAO Pacific University College of Optometry Please silence all mobile
Neuro-Ophthalmic Masqueraders Leonid Skorin, Jr., OD, DO, MS, FAAO, FAOCO Mayo Clinic Health System in Albert Lea Denise Goodwin, OD, FAAO Pacific University College of Optometry Please silence all mobile
Visual Impairment & Eye Health in Children. Susan Cotter, OD, MS So CA College of Optometry Marshall B Ketchum University Fullerton, CA
 Visual Impairment & Eye Health in Children Susan Cotter, OD, MS So CA College of Optometry Marshall B Ketchum University Fullerton, CA Consequences of Childhood VI Social Emotional Physical Educational
Visual Impairment & Eye Health in Children Susan Cotter, OD, MS So CA College of Optometry Marshall B Ketchum University Fullerton, CA Consequences of Childhood VI Social Emotional Physical Educational
Unexplained visual loss in seven easy steps
 Unexplained visual loss in seven easy steps Andrew G. Lee, MD Chair Ophthalmology, Houston Methodist Hospital, Professor, Weill Cornell MC; Adjunct Professor, Baylor COM, U Iowa, UTMB Galveston, UT MD
Unexplained visual loss in seven easy steps Andrew G. Lee, MD Chair Ophthalmology, Houston Methodist Hospital, Professor, Weill Cornell MC; Adjunct Professor, Baylor COM, U Iowa, UTMB Galveston, UT MD
Scleral Lenses: How do you know what is best
 Scleral Lenses: How do you know what is best Alan Kwok, OD, FAAO, FSLS Tar Vaz, OD, FAAO Please silence all mobile devices and remove items from chairs so others can sit. Unauthorized recording of this
Scleral Lenses: How do you know what is best Alan Kwok, OD, FAAO, FSLS Tar Vaz, OD, FAAO Please silence all mobile devices and remove items from chairs so others can sit. Unauthorized recording of this
A Case of Carotid-Cavernous Fistula
 A Case of Carotid-Cavernous Fistula By : Mohamed Elkhawaga 2 nd Year Resident of Ophthalmology Alexandria University A 19 year old male patient came to our outpatient clinic, complaining of : -Severe conjunctival
A Case of Carotid-Cavernous Fistula By : Mohamed Elkhawaga 2 nd Year Resident of Ophthalmology Alexandria University A 19 year old male patient came to our outpatient clinic, complaining of : -Severe conjunctival
DISCLOSURE: What to do? 2/22/2016
 DISCLOSURE: Dr. Joseph Sowka is a member of the Speakers Bureau for Alcon Laboratories, and Carl Zeiss Meditec. He is on the advisory boards for Alcon, Zeiss, and Allergan. He is a consultant for Alcon.
DISCLOSURE: Dr. Joseph Sowka is a member of the Speakers Bureau for Alcon Laboratories, and Carl Zeiss Meditec. He is on the advisory boards for Alcon, Zeiss, and Allergan. He is a consultant for Alcon.
Notes compiled for Pediatrics. Ophthalmology. (Med I, Block 5, OP)
") Notes compiled for Pediatrics Ophthalmology (Med I, Block 5, OP) Amblyopia and Strabismus University of Manitoba Faculty of Medicine MedII/OP7 Dr. P. Shuckett 2008-09 Objectives: 1. To state how to measure
Notes compiled for Pediatrics Ophthalmology (Med I, Block 5, OP) Amblyopia and Strabismus University of Manitoba Faculty of Medicine MedII/OP7 Dr. P. Shuckett 2008-09 Objectives: 1. To state how to measure
Recurrent intraocular hemorrhage secondary to cataract wound neovascularization (Swan Syndrome)
") Recurrent intraocular hemorrhage secondary to cataract wound neovascularization (Swan Syndrome) John J. Chen MD, PhD; Young H. Kwon MD, PhD August 6, 2012 Chief complaint: Recurrent vitreous hemorrhage,
Recurrent intraocular hemorrhage secondary to cataract wound neovascularization (Swan Syndrome) John J. Chen MD, PhD; Young H. Kwon MD, PhD August 6, 2012 Chief complaint: Recurrent vitreous hemorrhage,
Overview INTRODUCTION 3/15/2018. Headache Emergencies. Other way to differentiate between them? Is there an easy way to differentiate between them?
 Overview Headache Emergencies Primary versus Secondary headache disorder Red flags 4 cases of unusual headache emergencies Disclaimer: we will not talk about brain bleed as patients usually go the ED.
Overview Headache Emergencies Primary versus Secondary headache disorder Red flags 4 cases of unusual headache emergencies Disclaimer: we will not talk about brain bleed as patients usually go the ED.
ARTICLE. Cyclotherapy as a Technique to Expedite the Treatment of Hyperopic Amblyopia
 ARTICLE Cyclotherapy as a Technique to Expedite the Treatment of Hyperopic Amblyopia Lily Zhu-Tam, OD, FAAO, Bronx-Lebanon Hospital Center, Bronx, New York Francesca Kim, OD, Northwell Health, Long Island,
ARTICLE Cyclotherapy as a Technique to Expedite the Treatment of Hyperopic Amblyopia Lily Zhu-Tam, OD, FAAO, Bronx-Lebanon Hospital Center, Bronx, New York Francesca Kim, OD, Northwell Health, Long Island,
Diagnosis and Management of Refractive Error in Infants & Young Children A Current Perspective
 Diagnosis and Management of Refractive Error in Infants & Young Children A Current Perspective Susan A. Cotter, OD, MS, FAAO SCCO at Marshall B Ketchum University Tawna L. Roberts, OD, PhD, FAAO Akron
Diagnosis and Management of Refractive Error in Infants & Young Children A Current Perspective Susan A. Cotter, OD, MS, FAAO SCCO at Marshall B Ketchum University Tawna L. Roberts, OD, PhD, FAAO Akron
Early detection of Retinoblastoma in children. Max Mantik
 Early detection of Retinoblastoma in children Max Mantik Introduction The most common primary intraocular malignancy of childhood 10 to 15 % of cancers that occur within the first year of life Typical
Early detection of Retinoblastoma in children Max Mantik Introduction The most common primary intraocular malignancy of childhood 10 to 15 % of cancers that occur within the first year of life Typical
Financial Disclosures
 Retinoblastoma Management: Update Jesse L. Berry, MD Associate Director, Ocular Oncology Service Associate Program Director USC/CHLA, Keck School of Medicine Financial Disclosures Research Support: Bright
Retinoblastoma Management: Update Jesse L. Berry, MD Associate Director, Ocular Oncology Service Associate Program Director USC/CHLA, Keck School of Medicine Financial Disclosures Research Support: Bright
Phone Triage for Optometric Staff ???????? CHEMICAL BURN CHEMICAL BURN
 Phone Triage for Optometric Staff There are very few ocular emergencies that you will have to deal with in practice, but it is imperative that you be able to Michelle Welch, O.D. NSU Oklahoma College of
Phone Triage for Optometric Staff There are very few ocular emergencies that you will have to deal with in practice, but it is imperative that you be able to Michelle Welch, O.D. NSU Oklahoma College of
Optic Disc: Anatomy, Variants, Unusual discs. Kathleen B. Digre, MD Professor Neurology, Ophthalmology
 Optic Disc: Anatomy, Variants, Unusual discs Kathleen B. Digre, MD Professor Neurology, Ophthalmology THE OPHTHALMOSCOPE DIRECT OPHTHALMOSCOPY Jan Purkinje 1823 Hermann von Helmholtz 1851 Hand held ophthalmoscope
Optic Disc: Anatomy, Variants, Unusual discs Kathleen B. Digre, MD Professor Neurology, Ophthalmology THE OPHTHALMOSCOPE DIRECT OPHTHALMOSCOPY Jan Purkinje 1823 Hermann von Helmholtz 1851 Hand held ophthalmoscope
Midbrain Infarction Causing Diplopia and Atypical Neurological Symptoms: An Abducens Palsy Review
 Midbrain Infarction Causing Diplopia and Atypical Neurological Symptoms: An Abducens Palsy Review A 68 year old white male reports distance horizontal diplopia immediately following a cerebrovascular accident.
Midbrain Infarction Causing Diplopia and Atypical Neurological Symptoms: An Abducens Palsy Review A 68 year old white male reports distance horizontal diplopia immediately following a cerebrovascular accident.
Clinical Study Early Results of Slanted Recession of the Lateral Rectus Muscle for Intermittent Exotropia with Convergence Insufficiency
 Ophthalmology Volume 2015, Article ID 380467, 5 pages http://dx.doi.org/10.1155/2015/380467 Clinical Study Early Results of Slanted Recession of the Lateral Rectus Muscle for Intermittent Exotropia with
Ophthalmology Volume 2015, Article ID 380467, 5 pages http://dx.doi.org/10.1155/2015/380467 Clinical Study Early Results of Slanted Recession of the Lateral Rectus Muscle for Intermittent Exotropia with
INTRODUCTION TO BINOCULAR VISION TESTING: LECTURE 1
 INTRODUCTION TO BINOCULAR VISION TESTING: LECTURE 1 Dr Hilary Gaiser OD, MSc Assistant Professor of Optometry New England College of Optometry This presentation has been created for Orbis International
INTRODUCTION TO BINOCULAR VISION TESTING: LECTURE 1 Dr Hilary Gaiser OD, MSc Assistant Professor of Optometry New England College of Optometry This presentation has been created for Orbis International
Ocular Pathology I 6234_16385 Rm HBSB 203-E 1:00-3:00pm. Tonya G. Ketcham, OD, PhD , RM 2113
 Ocular Pathology I 6234_16385 Rm HBSB 203-E 1:00-3:00pm Tonya G. Ketcham, OD, PhD tketcham@optometry.uh.edu 3-1799, RM 2113 Course Syllabus Course Description To describe normal anomalies and pathologic
Ocular Pathology I 6234_16385 Rm HBSB 203-E 1:00-3:00pm Tonya G. Ketcham, OD, PhD tketcham@optometry.uh.edu 3-1799, RM 2113 Course Syllabus Course Description To describe normal anomalies and pathologic
Evaluation of ONH Pallor in Glaucoma Patients and Suspects. Leticia Rousso, O.D. Joseph Sowka, O.D
 Evaluation of ONH Pallor in Glaucoma Patients and Suspects Leticia Rousso, O.D Joseph Sowka, O.D I. Abstract This case report will evaluate a young glaucoma suspect with unilateral sectoral optic nerve
Evaluation of ONH Pallor in Glaucoma Patients and Suspects Leticia Rousso, O.D Joseph Sowka, O.D I. Abstract This case report will evaluate a young glaucoma suspect with unilateral sectoral optic nerve
Supplementary Online Content
 Supplementary Online Content Gao TY, Guo CX, Babu RJ, et al; the BRAVO Study Team. Effectiveness of a binocular video game vs placebo video game for improving visual functions in older children, teenagers,
Supplementary Online Content Gao TY, Guo CX, Babu RJ, et al; the BRAVO Study Team. Effectiveness of a binocular video game vs placebo video game for improving visual functions in older children, teenagers,
Neuro Op Grand Rounds: Fields and Diplopia Utah Optometric Association June 2018
 Disclosures Neuro Op Grand Rounds: Fields and Diplopia Utah Optometric Association June 2018 I have received honorarium from the following: Glaukos CE in Italy Heidelberg Engineering Review of Optometry
Disclosures Neuro Op Grand Rounds: Fields and Diplopia Utah Optometric Association June 2018 I have received honorarium from the following: Glaukos CE in Italy Heidelberg Engineering Review of Optometry
n Early Detection/Prevention/Treatment n Vision loss n Loss of binocularity n Eye health n Visual system plasticity
 The ABC s of Stress-Free Eye Care for Infants & Young Children Patient photos removed from slides for handout Rationale for Examination Early Detection/Prevention/Treatment Vision loss Loss of binocularity
The ABC s of Stress-Free Eye Care for Infants & Young Children Patient photos removed from slides for handout Rationale for Examination Early Detection/Prevention/Treatment Vision loss Loss of binocularity
Case Follow Up. Sepi Jooniani PGY-1
 Case Follow Up Sepi Jooniani PGY-1 Triage 54 year old M Pt presents to prelim states noticed today he had reddness to eyes, states worse in R eye. Pt denies any pain or itching. No further complaints.
Case Follow Up Sepi Jooniani PGY-1 Triage 54 year old M Pt presents to prelim states noticed today he had reddness to eyes, states worse in R eye. Pt denies any pain or itching. No further complaints.
Visual Fields A Road Map to Management.
 Visual Fields A Road Map to Management. Disclosures Dr. Beth Steele Company Position Received Optos Advisory Board Honorarium Med Op Consultant Honorarium Beth A. Steele, OD, FAAO bsteele@uab.edu FACTS
Visual Fields A Road Map to Management. Disclosures Dr. Beth Steele Company Position Received Optos Advisory Board Honorarium Med Op Consultant Honorarium Beth A. Steele, OD, FAAO bsteele@uab.edu FACTS
Think Outside the Box. Strabismus & Amblyopia. Prescribing. Amblyopia 5/9/2017. Goals of today s lecture: Kacie Monroe, OD, FCOVD. Peripheral Movement
 Think Outside the Box Strabismus & Kacie Monroe, OD, FCOVD Goals of today s lecture: Define success in treatment Determine the best path to get there Spoiler: it may not be what you think Provide specific
Think Outside the Box Strabismus & Kacie Monroe, OD, FCOVD Goals of today s lecture: Define success in treatment Determine the best path to get there Spoiler: it may not be what you think Provide specific