Mississippi Newborn Screening Guide for Healthcare Providers
|
|
|
- Gwenda Ray
- 6 years ago
- Views:
Transcription



1 Mississippi Newborn Screening Guide for Healthcare Providers Mississippi State Department of Health Office of Child & Adolescent Health Bureau of Genetic Services October 2015
2 TABLE OF CONTENTS Introduction... 1 What is Newborn Screening?... 1 Who should be Screened?... 1 Newborn Screening Panel... 1 Mississippi Genetic Newborn Screening Panel... 2 Point-of-Service Screening... 1 Tips For Collection... 3 Instructions For Dried Blood Spot Card (DBS) Completion... 4 Critical Congenital Heart Disease (CCHD)... 7 Hearing Screening... 7 Specimen Collection... 8 Problems with Specimen Collection Specimen Collection/Transfers Specimen Collection/Transfusions Screening for CCHD Hospital Hearing Screening Dried Blood Spot Card How to Order Dried Blood Spot Cards Newborn Screening Results Unacceptable or Inconclusive Results Immediate Follow-Up Of Abnormal or Presumptive Positive Results Immediate Follow-Up Of Abnormal or Presumptive Positive Result After Hours/Weekends Appendices... 17
3 INTRODUCTION The purpose of this newborn screening guide is to provide information and assistance to healthcare professionals participating in the newborn screening process in Mississippi. We hope that the information in this guide is helpful. Contact the Newborn Screening Program at with questions or comments regarding newborn screening. WHAT IS NEWBORN SCREENING? Newborn Screening is a public health service completed prior to a newborn being discharged from the delivering facility to assist in identification of certain serious or life-threatening conditions. The screening provides early detection of numerous disorders so that timely treatment can be initiated and long-term sequelae minimized. Long-term sequelae may include organ damage, developmental delay, or death if left undiagnosed and untreated. WHO SHOULD BE SCREENED? Sections and of the Mississippi Code of 1972 require all newborns born in Mississippi to be screened prior to discharge from the hospital regardless of the age of the newborn or the feeding status. Parents of newborns who object on grounds that the screening conflicts with their religious practices are exempt from screening, but they are required to sign a refusal form stating their understanding of this process. NEWBORN SCREENING PANEL The Mississippi State Department of Health (MSDH) contracts with an outside laboratory to perform newborn screening blood spot testing and, when indicated, second tier DNA testing for some disorders. Evaluation and confirmatory testing is performed at a tertiary care center by medical subspecialists. Page 2 lists the diseases/disorders screened for in Mississippi by the blood spot test. POINT-OF-SERVICE SCREENING Point-of-service tests for newborns include early hearing and critical congenital heart disease (CCHD) screening. These screens do not involve dried blood spots and are non-invasive tests to screen for hearing loss and certain cardiac defects that may require further medical intervention. 1
4 MISSISSIPPI GENETIC NEWBORN SCREENING PANEL Core Condition Propionic acidemia Methylmalonic acidemia (methylmalonyl-coa mutase) Methylmalonic acidemia (cobalamin disorders) Isovaleric acidemia 3-Methylcrotonyl-CoA carboxylase deficiency 3-Hydroxy-3-methyglutaric aciduria Holocarboxylase synthase deficiency ß-Ketothiolase deficiency Glutaric acidemia type I Carnitine uptake defect/carnitine transport defect Medium-chain acyl-coa dehydrogenase deficiency Very long-chain acyl-coa dehydrogenase deficiency Long-chain L-3 hydroxyacyl-coa dehydrogenase deficiency Trifunctional protein deficiency Argininosuccinic aciduria Citrullinemia, type I Maple syrup urine disease Homocystinuria Classic phenylketonuria Tyrosinemia, type I Primary congenital hypothyroidism Congenital adrenal hyperplasia S,S disease (Sickle cell anemia) Secondary Condition Methylmalonic acidemia with homocystinuria Malonic acidemia Isobutyrylglycinuria 2-Methylbutyrylglycinuria 3-Methylglutaconic aciduria 2-Methyl-3-hydroxybutyric aciduria Short-chain acyl-coa dehydrogenase deficiency Medium/short-chain L-3-hydroxyacl-CoA dehydrogenase deficiency Glutaric acidemia type II Medium-chain ketoacyl-coa thiolase deficiency 2,4 Dienoyl-CoA reductase deficiency Carnitine palmitoyltransferase type I deficiency Carnitine palmitoyltransferase type II deficiency Carnitine acylcarnitine translocase deficiency Argininemia Citrullinemia, type II Hypermethioninemia Benign hyperphenylalaninemia Biopterin defect in cofactor biosynthesis Biopterin defect in cofactor regeneration Tyrosinemia, type II Tyrosinemia, type III Various other hemoglobinopathies S, βeta-thalassemia Galactoepimerase deficiency S,C disease Biotinidase deficiency Galactokinase deficiency T-cell related lymphocyte deficiencies Cystic fibrosis Classic galactosemia Severe Combined Immunodeficiences 2
5 TIPS FOR COLLECTION All birthing hospitals are required to collect a newborn screening specimen (blood spot test) on each newborn before discharge from the hospital or transfer to a facility for higher level care, regardless of age or the feeding status. In order to expedite screen results, always follow the steps below: Scheduling: The ideal time for specimen collection is hours after birth. If discharged prior to 24 hours of age, collect the specimen as close to discharge as possible, and collect a repeat specimen at approximately 48 hours of age. Critically ill infants should be screened by hours of age. Technique: Fill out the specimen card completely. Collect the specimen correctly (see Appendix A). Fill each of the circles on the filter paper with a single, free-flowing drop of blood. Do not layer successive drops of blood. Apply the blood to only one side of the filter paper. Make sure the blood has saturated through to the back of the paper. Handling: Air dry on a flat surface for 3-4 hours. Do not heat, stack, or allow blood spots on the filter paper to touch other surfaces during the drying process. Air-dried specimens should be refrigerated until shipped. Send specimens daily, via the overnight courier service provided. The Screening Laboratory has arranged courier services with UPS. Note: The Complete View Solution (ICVS) is a secure Web-based shipping application that has been customized to accommodate the facility s unique business requirements. Please see UPS - ICVS Training User Guide for instructions. Mississippi law requires all newborns born in Mississippi to be screened prior to discharge from the hospital regardless of the age of the newborn or the feeding status. Parents of newborns who object on the grounds that the screening conflicts with their religious practices are exempt from screening but are required to sign a refusal form stating their understanding of this process (see Appendix B). Send a copy of this form to MSDH Newborn Screening Program. 3
6 INSTRUCTIONS FOR DRIED BLOOD SPOT CARD (DBS) COMPLETION Results may be delayed for screening specimens submitted with incomplete information. ALWAYS check the specimen card expiration date located on the far left side of the filter paper, next to the hour glass, noted by the year and date. Expired cards are not acceptable. All information must be legible. TOP LINE First Specimen If it is the first newborn screening specimen (dried blood spot) collected on the infant, place an X in the blank provided. Home Birth If the newborn was born at home, place an X in the blank provided. Repeat Specimen If the test is a repeat newborn screening specimen collected on the infant, place an X in the blank provided. Repeat Specimen Reason Put an X by the appropriate reason for a repeat Specimen; < 24 hr, Unsatisfactory, Abnormal, Transfused, Inconclusive. REQUIRED INFANT INFORMATION Infant s Last/First Name Write infant s name in order as shown: Last name, first name, previous last name. Ensure the name is spelled correctly. If the infant s first name is not available, put last name, followed by Boy/Girl. (Example: Smith, Baby Boy). Previous Last Name If the infant s last name is different from the name given at birth, indicate the previous/original name in the blank provided. (Smith, John; Brown, Boy). Birth Date Write the date of birth using numbers only in the blank provided. (Example: December 25, 2002, will appear as ). Time of Birth Write the time of birth using Military Time Only in the blank provided. (Example: 2:30 p.m. will appear as 1430). Date Collected Write the date the specimen was collected using numbers only in the blank provided. (Example: December 2, 2003, will appear as ). Time Collected Write the time the specimen was collected using Military Time Only in the blank provided. (Example: 8:00 p.m. will appear as 2000). Birth Write an X in the blank provided. (EXAMPLE: in the case of twins/triplets, write an X to indicate the birth order of the infant to indicate A or B). For triplets or more use #3 blank and indicate C, D, or E as necessary. Hospital of Birth Code or Health Department Code Write the hospital code/health Department code in the appropriate blank provided. Note: If the infant is born in the same hospital in which 4
7 the specimen is collected, then both the hospital of birth code and hospital collected code will be the same. If the infant is born in one hospital, but transferred to another hospital prior to the specimen being collected, the hospital collection code will be different from that of the hospital of birth. When the specimen is collected or repeated by the Health Department, the Health Department county code is entered into the Health Department collected blank. Medical Record Number Write the infant s medical record number in the blank provided. Transferred If the infant has been transferred to another facility, check yes and write the name of the facility in the space provided. Physician s Name Write the name and contact information of the healthcare professional who will be providing local medical care for the infant in the blank provided. In the event of a homebirth, provide the name of the midwife or person attending the homebirth, with contact information. Additional Information Use these lines to provide the following information: Collection of a Pre transfusion specimen Infant is Adopted (give the name and address of the adoption agency, attorney or physician handling the adoption.) Infant discharged/ expired from the hospital prior to newborn screening collection. Incarceration if mother will return to an incarceration facility, write INMATE and to whom the infant has been discharged and the contact information. Submitter Name/Address Write the name and address of the hospital/health Department (submitter) in the blank provided. Specimen Collected By Write initials of person collecting specimen in the blank provided. Sex Write an X in the appropriate blank provided. Race Write an X in the appropriate blank provided. Ethnicity Write an X in the appropriate blank provided. Transfused Collect specimen PRIOR to transfusion if at all possible. Provide the date and time of the last transfusion for each specimen collected in the space provided (Example: December 15, 2002, at 10:00 a.m. will appear as /1000.) Note: Ideal collection time: hours of age Transfusion required > 24 hours of age: Collect specimen prior to transfusion. Transfusion required < 24 hours of age: Collect specimen prior to transfusion and 2-4 days after the transfusion. Transfusion required but no specimen collected prior to transfusion: Collect specimen 2-4 days, 2-4 weeks, and > 90 days after transfusion 5
8 Note: Anticoagulants should not be used in the collection of newborn screening specimens. In cases where it is unavoidable, only heparin should be used and its presence in the sample should be noted on the filter paper. Gestation/Infant s Age Write the gestational age of the infant at birth and the age of the infant at the time of collection in the blank provided. Birth Weight Write the infant s weight in grams, At the Time of Birth in the blank provided. If specimen is collected > 14 days of age, write current weight in grams. Feeding Write an X in the appropriate blank provided, indicating the infant s feeding status at the time of collection. More than one blank may be marked if appropriate. Meconium Ileus Check the blank, if appropriate, to indicate the presence of a meconium ileus. MOTHER S INFORMATION Mother s Current Last/First Name Write mother s full name, as specified at time of delivery in the blank provided (Example: Smith, Caroline). Enter the mother s maiden name in the space provided. (Note: If the infant is ADOPTED, do not give the birth mother s information. In the case of ADOPTION, this area should reflect the name of the agency, physician, or attorney handling the adoption.) Mother s Date of Birth Write mother s date of birth using numbers only in the blank provided. (Example: December 25, 1983, will appear as ). Address/Phone Number Write the physical street address (Do Not Give P.O. Box), and/or apartment number, as well as the city, state, and zip code in the blanks provided. Write the telephone number or emergency contact number where a voic /message can be accepted, in the blanks provided. (Note: In the case of ADOPTION, give the agency, physician or attorney name, address and phone number handling the adoption in the blanks provided.) Medicaid Number/Mother s Social Security Number Write mother s Medicaid number, if it applies, and Social Security number in the blanks provided. County of Residence Write the county two - digit code where the infant resides in the space provided (Example Hinds County/25). Note: In the event an infant is a Drop Off Baby, assign the baby a name. The date the baby was dropped at the hospital should be used as the date of birth, and the approximate time the baby was left should be used as the time of birth, unless other information is known to the hospital. The hospital code should be entered in the space provided for the hospital of birth and hospital collected. In the box provided for Physician s Name, note the emergency medical services provider. This will allow for adequate follow-up/tracking in the event of an abnormal or positive newborn screen. 6
9 CRITICAL CONGENITAL HEART DISEASE (CCHD) In the spaces provided, write the date/time the initial pulse ox screening was performed. If pulse ox was not performed, indicate the reason why. In the appropriate space, indicate the pulse oximetry screening outcome passed or a failed screen. Indicate if an echocardiogram was performed. DO NOT delay sending the dried blood spot specimen to the screening lab to provide CCHD screening data. Complete the Delayed Screening Form and mail or FAX the delayed CCHD screening data to the newborn screening program. (See Delayed CCHD screening form APPENDIX G) HEARING SCREENING This section of the newborn screening form should be completed by the hospital of birth prior to discharge. Check the appropriate test performed, i.e., ABR/OAE, and the appropriate result for each ear, i.e., pass/refer. If the hearing screening is not performed, leave this section blank. DO NOT delay sending the dried blood spot specimen to the screening lab to provide hearing screening data. OFFICE MECHANICS/FILING/RETENTION: The yellow NCR copy of the dried blood spot card should be kept by the submitting hospital of birth/county Health Department to ensure the results are received by the submitting hospital or county Health Department. Once the newborn screen result is received, the yellow copy can be destroyed. The electronic copy/hard copy of the newborn screening result should be filed in the infant s electronic medical record/paper medical record and retained according to hospital/county Health Department policy. 7
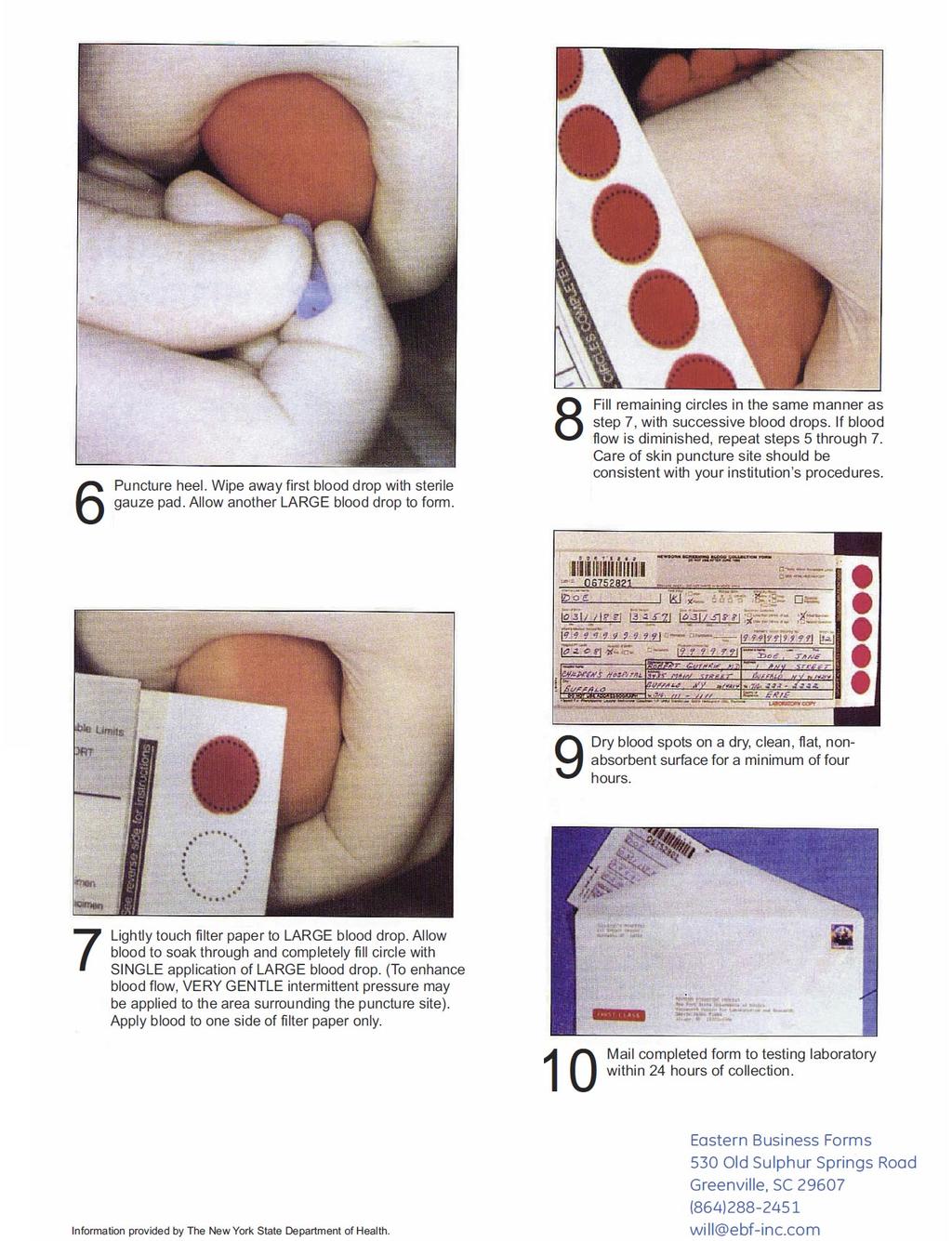
10 SPECIMEN COLLECTION SUPPLIES FOR SPECIMEN COLLECTION Dried Blood Spot Card (DBS card) Soap and water Cotton balls soaked with 70% isopropyl alcohol (also the alcohol prep, which is likely used in most facilities) Dry cotton balls Sterile gauze pad Heel Warmer (if available); Lancet SPECIMEN COLLECTION PROCEDURE 1. Recommended site: The least hazardous sites for heel puncture are medial to a line drawn posteriorly from the middle of the big toe to the heel, or a similar line drawn on the other side extending from between the 4th and 5th toe to the heel. Refer to Blood Specimen Collection and Handling Procedure for the shaded areas demarcating preferred puncture sites (see Appendix A). 2. Thoroughly wash the puncture site with soap and water. 3. Disinfect the skin with 70% isopropyl alcohol. Vigorous rubbing during this step may help stimulate blood flow to the area. Allow time to air dry. 4. Puncture the skin in one continuous motion using the Lancet. (Avoid the use of long tip lancets which may damage the heel bone.) 5. Wipe away and discard the first drop of blood since it may be contaminated by disinfectant or tissue fluid. 6. Allow a second drop to form from a spontaneous free flow of blood. 7. Expose the filter paper end of the DBS card. Touch the filter paper to the drop of blood, as close to the center of the circle as possible. Observing from the opposite side, allow the blood spot to enlarge until the circle is completely filled. There should only be a single application of the filter paper to the blood spot for each circle. (No dabbling of filter paper to the heel; this will cause an overlay of blood, which may cause inaccurate results.) 8. Once the blood collection is completed, press a sterile gauze pad to the puncture site until the bleeding has stopped. 9. Dry the blood spots on a level, nonabsorptive surface, away from the direct sunlight, and at room temperature for at least four hours. DBS cards should not be stacked while the 8
11 filter paper specimens are exposed. After drying, rewrap the filter paper with the cover sheet to its original position to protect the specimen. 10. IMPORTANT: All information requested on the DBS card should be completed. Failure to complete critical information such as the infant s last name, the date and time of birth, and the date and time of collection will cause the specimen to be rejected by the screening laboratory and necessitate a repeat specimen collection on the infant by the originator of the specimen. 11. The DBS card should be mailed within 24 hours of collection to the screening laboratory utilizing the overnight courier service. 9
12 PROBLEMS WITH SPECIMEN COLLECTION Dilution or contamination of the blood spot may occur due to the following errors: Failure to wipe off the alcohol residue Failure to discard the first drop of blood that forms, since it may be contaminated with alcohol or tissue fluids Milking the puncture site to stimulate bleeding, which can dilute the blood with tissue fluid Touching the blood spot circles before or after filling, which can contaminate the spots with perspiration and/or oil from fingertips Allowing blood spots to be contaminated by contact with water, feeding formulas, or antiseptics The blood may be unevenly distributed on the filter paper due to the following errors: The repeated touching of the filter paper to small drops of blood in an attempt to fill a circle. This will result in areas overfilled due to layering one drop over a partially dried drop and some areas contain no blood at all. A mottled appearance will occur if the filter paper is not soaked through, front to back. Overfilling the circles causes the center of the circle to be supersaturated. This may cause inaccurate test results. Blood collected in capillary tubes and used to fill the circles. There is a chance of the capillary tube scratching the surface of the filter paper, which may alter the thickness in that area. 10
13 SPECIMEN COLLECTION/TRANSFERS Optimal time for specimen collection is hours after birth. In the event of pending transfer to a facility for higher level of care, collect the newborn screen specimen prior to transfer, if possible. If DBS specimen is not collected prior to transfer, indicate on the DBS card that the infant has been transferred; provide the name of the facility where newborn is transferred. Mail the DBS card with no blood on it to: MSDH Genetics Program P.O. Box 1700 Jackson, MS SPECIMEN COLLECTION/TRANSFUSIONS Optimal time for specimen collection is hours after birth. If an infant is discharged before 24 hours of age or transferred to another facility for higher level of care, the specimen must be collected before discharge to assure that the infant is in the system. It is also recommended that the specimen is collected before a blood transfusion, if possible. Ideal collection time: hours of age Transfusion required at > 24 hours of age: collect specimen prior to transfusion Transfusion required < 24 hours of age: collect specimen prior to transfusion and 2 4 days after the transfusion Transfusion required but no specimen collected prior to transfusion: collect specimen 2 4 days, 2 4 weeks and > 90 days after transfusion 11
14 SCREENING FOR CCHD Annually, approximately 8 in every 1,000 babies are born with congenital heart disease (CHD) in the United States. CHD occurs when an infant is born with an abnormal structure of the heart, creating abnormal blood flow patterns. Critical congenital heart disease (CCHD) is a more serious group of heart defects that occurs in approximately 25% of CHD cases, and is one of the leading causes of infant death. Pulse oximetry, or pulse ox, is a simple non-invasive screening test that detects low oxygen levels in the blood and may help to diagnose critical CHD before babies are discharged from the hospital. CCHD screening should be performed before discharge from the nursery, after the infant turns 24 hours of age, and ideally between 24 to 48 hours. If the infant was born prematurely, screening should be performed when medically appropriate. If early discharge is planned, screening should occur as late as possible prior to discharge. Pulse ox screening should be performed while the infant is in the nursery, before discharge at a time when the infant is quiet, warm, and on room air. The pulse ox test should be performed on the right hand and one foot. In many centers a convenient time for the pulse ox screening to be completed is in conjunction with the hearing screen. HOSPITAL HEARING SCREENING All hospitals that deliver babies are equipped with newborn hearing screening equipment. Every baby (unless otherwise medically indicated) should have at least one hearing screen test documented on the dried blood spot card prior to submission. The first screen is completed shortly after birth when the baby is quiet. The second screen is completed prior to discharge if the baby refers in either ear on the first screen. Both ears are to be rescreened. If the baby refers in either ear during the first and/or second screens, an appointment is made by staff at the birthing hospital for an outpatient screen and documented in the medical record. Both ears are to be rescreened. In the spaces provided, check the appropriate test box and the ear screened (L or R). In the appropriate space, indicate the result pass or refer. 12

15 DRIED BLOOD SPOT CARD HOW TO ORDER DRIED BLOOD SPOT CARDS To order Newborn Screening Pamphlets and dried blood spot cards complete a Newborn Screening Supply Form and fax to or call (See Appendix C.) 13
16 NEWBORN SCREENING RESULTS The screening laboratory provides results to the birthing hospitals to file in the infant s medical record. Birthing hospitals can also obtain newborn screening results for specimens submitted by their facility by accessing Information@PerkinElmer.com. To request a User Access Form call PerkinElmer Genetics at In addition, all results are electronically downloaded into the Mississippi State Department of Health s Newborn Screening Program system. Primary care providers can obtain a copy of the newborn screening results from the hospital of birth by faxing a written request (Request For Newborn Screening Results / Dried Blood Spot Card Form see Appendix D) to the Newborn Screening Program (NBS) at or call the NBS Program at for questions Monday Friday, 8 am 5 pm. The following information is needed to provide newborn screen results: Name Sex Date of birth Mother s name Hospital of birth Parents should ask their baby s physician about the Newborn Screening results at the first well baby checkup. For more information on what parents should know about newborn screening and FAQs. (See Appendices E and F.) UNACCEPTABLE OR INCONCLUSIVE RESULTS The NBS Program coordinates repeat specimen collection for unacceptable or inconclusive test results. Repeat specimen collection is addressed by the hospital of birth or the Health Department in the county of residence. 14
17 IMMEDIATE FOLLOW-UP OF ABNORMAL OR PRESUMPTIVE POSITIVE RESULTS All abnormal or presumptive positive screening results are reported to the NBS Program by the screening laboratory. If the infant is a hospital inpatient, the attending physician is notified of the results. If the infant has been discharged, the primary care physician of record is notified of the screen results. A disease-specific American College of Medical Genetics (ACMG) ACTion sheet is provided to the notified physician. The ACMG ACTion sheet provides a brief overview of the condition description, differential diagnosis, diagnostic evaluation, and course of action which can be used in conjunction with a consultation of a tertiary care specialist ( Once the primary care physician of record is notified of the screening results, the NBS Program may facilitate a referral to the tertiary care specialist as requested by the physician. Diagnosis will require an evaluation and confirmatory testing. Evaluation and treatment may require ongoing clinic visits with the appropriate clinical provider. (See Appendix I.) 15
18 IMMEDIATE FOLLOW-UP OF ABNORMAL OR PRESUMPTIVE POSITIVE RESULT AFTER HOURS/WEEKENDS After normal business hours, which includes weekends and holidays, abnormal or presumptive positive screening results are reported to the NBS Program staff. The NBS Program staff who is on-call immediately contacts the hospital of birth and the on-call physician. The results are given to the physician via telephone with instructions on how to access the ACMG website ( for a disease specific ACTion sheet, and also how to contact the appropriate specialist (see Appendix I). The next business day, a copy of the newborn screening result will be faxed to the hospital of birth and the physician of record. 16
19 APPENDICES A. Neonatal Screening: Blood Specimen Collection and Handling Procedure..18 B. Refusal of Newborn Screening Form...22 C. Newborn Screening Supply Form...23 D. Request for Newborn Screening Results / Dried Blood Spot Card..24 E. What Parents Should Know About Newborn Screening 25 F. Newborn Screening in Mississippi: Frequently Asked Questions.26 G. CCHD Delayed Screen Reporting Form...28 H. CCHD Failed Screen Reporting Form 29 I. Tertiary Care Center...31 J. Mississippi Newborn Screening Flow Chart.33 17

20
21
22 APPENDIX B Refusal of Newborn Screening Parent(s) are allowed to refuse the newborn screening test for their infant only if their religious beliefs and practices do not allow testing. When a parent refuses the newborn screening test, staff should: Give parent a copy of the Newborn Screening pamphlet and discuss the significance of the NBS test. Ask for a signed statement from parent stating refusal to have baby screened for these very serious conditions (See example : Genetic Services Newborn Screening Refusal) Place signed form or statement in the baby's hospital medical record, and send a copy of the signed/witnessed form to the MS Newborn Screening Program. Mailing Address: MSDH Genetics Program P.O. Box 1700 Jackson, MS Fax Number:
23 APPENDIX B Sample Newborn Screening Refusal Form Patient s Name Date of Birth Mother s Name Hospital Person(s) Counseled Date I, have been counseled on the importance of Newborn (Parent s Name) Screening tests and have received literature on Newborn Screening. I do understand that the Mississippi state law requires every baby to be screened between hours of birth. I understand that appropriate screening can allow for early detection, treatment, and follow- up. Many of these disorders may cause life-threatening medical conditions, mental retardation or even death, and many of these serious consequences can be lessened with timely medical intervention. However, due to my religious beliefs, I decline to have these tests performed on my child. Signed Witnessed 22
24 APPENDIX C NEWBORN SCREENING SUPPLY FORM Fax completed request to the Newborn Screening Program Requested by: ATTN: Date: Ship to: Telephone Number: Description Quantity Requested Quantity Shipped Newborn Screening Dried Blood Spot Cards Filter Paper Newborn Screening Pamphlet(#5198 English) Newborn Screening Pamphlet (#5198 Spanish) Screening for Critical Congenital Heart Defects 5 Things to Know About Congenital Heart Defects What Does A Safe Sleep Environment Look Like (#5404 English) What Does A Safe Sleep Environment Look Like (#5404S Spanish) Baby s Safe Sleep Crib Checklist (# 5400 English) Newborn Hearing Screening What to Expect (#5272 English) Newborn Hearing Screening What to Expect (#5272S Spanish) Newborn/Infant Hearing Screening Report (#288) Infant Hearing Screening Log (#291) Infant Hearing Screening Log/ Data Summary (#81) Disk Mailers Newborn Hearing Screening/ Pass Card (Yellow & Green) Newborn Hearing Screening/ Refer Card (Yellow & Red) Supplier Use Only Filled by: Date: Mail or FAX request to the below address, Attn: Genetic Services, fax to or call East Woodrow Wilson Post Office Box 1700 Jackson, MS HLTHY4U Equal Opportunity in Employment/Services Revised Date: February
25 APPENDIX D REQUEST FOR NEWBORN SCREENING RESULTS / DRIED BLOOD SPOT CARD Phone (601) Fax (601) PLEASE PRINT LEGIBLY. ILLEGIBLE AND INCOMPLETE REQUEST WILL BE RETURNED TO SENDER. TYPE OF REQUEST: Newborn Screening Results Dried Blood Spot Card REASON FOR REQUEST: Parent Request Primary Care Provider/Pediatrician Recent Death Other: Family History REQUESTOR S REQUIRED INFORMATION Name of Facility: Date: Contact Person: Requestor Name: Facility Address: Telephone ( ) Fax # ( ) Child s Name (at birth) Last First Middle Initial Child s Date of Birth: Sex: Male Female Indeterminate (Circle One) Mother s Name: Mother s Address: Mother s DOB: County of residence at birth: If child has a different last name than above please list below: CONFIDENTIALITY NOTE: This information has been disclosed to you from records whose confidentiality is protected. Statutes/Regulations prohibit you from making further disclosures other than treatment, payment or health care operation, without the specific written authorization of the person to whom it pertains, or as otherwise permitted by such regulations. Bureau of Genetic Services 570 East Woodrow Wilson Post Office Box 1700 Jackson, MS HLTHY4U Equal Opportunity in Employment/Services 24



26 What Parents Should Know About Newborn Screening All babies born in Mississippi are required by law to have a blood sample collected after birth to screen for a number of genetic disorders. Babies with genetic disorders may look healthy at birth, yet be at risk for serious health problems. Serious health problems may be prevented if these disorders are identified as soon as possible after birth. You will receive a pamphlet about newborn screening before you and your baby are discharged from the hospital. Twenty-four to forty-eight hours after your baby s birth, a nurse or laboratory technician will draw a few drops of blood from your baby s heel. He or she will then send it to a laboratory for testing. Both you and your baby s physician will be notified if the screening indicates that further follow-up is needed, and a copy of the screening results will be sent to the hospital where your baby was born. These results will be included in your baby s medical record. Ask your baby s physician about the newborn screening results at your first well baby checkup. Occasionally a second screening is required to confirm test results. If your baby requires a second screening, it should be done as soon as possible. Your local county health department will contact you if rescreening is necessary. To help with prompt notification, be sure to provide the name of your baby s doctor, your physical address and a telephone number before hospital discharge. If you have any further questions about newborn screening, talk with your obstetrician and your baby s physician. You may also contact the Mississippi State Department of Health Newborn Screening Program at or HLTHY4U ( ). You may also visit the Mississippi State Department of Health s website at Also available in Spanish MISSISSIPPI STATE DEPARTMENT OF HEALTH
27 APPENDIX F NEWBORN SCREENING IN MISSISSIPPI FREQUENTLY ASKED QUESTIONS What is Newborn Screening? Newborn screening refers to a dried blood spot screening test that is performed on babies before they are discharged from the hospital. The screen is done before discharge to identify babies who may be at risk for a condition with serious effects who might not otherwise be detected for several days, months, or even years. Only additional testing (diagnostic and/or confirmatory testing) can tell if the baby has a disorder. Why should my baby have the screening? The conditions for which babies will be screened are individually rare. However, some are very serious and can result in mental retardation, other serious medical problems, and/or death if not treated appropriately. Babies with these conditions often appear normal at birth. The newborn screen helps to identify babies who need medical treatment, such as medications or special diets. Newborn screening may not always detect a disorder. If your baby does not seem well, talk to your baby s physician as soon as possible. My baby looks healthy. Is this screen still necessary? Yes! Most babies with a condition found by newborn screening show no signs of the condition right after birth. However, babies with a condition will need special medical care and the screen can usually identify these babies before they become sick. Do I need to give permission for my baby to be screened for these conditions? No. The state law (MS Statute ) states that all babies born in Mississippi must be screened prior to discharge from the hospital unless your religious beliefs and practices do not allow this testing. May I refuse the screening test? As a parent, you may refuse newborn screening only if your religious beliefs and practices do not allow this testing. If you refuse to have the screen performed on your baby, you will be asked to sign a form (Newborn Screening Refusal) stating you refused to have your baby screened for these very serious conditions. This form will go in your baby s hospital medical record. Is there a fee for the screening test? A fee is billed to the hospital where your baby was born for the screen. What conditions are currently screened for in Mississippi? Mississippi Genetic Newborn Screening Panel 26
28 APPENDIX F When and how is the screening test done? The screening specimen is usually collected between hours of age. A few drops of blood are taken by pricking the baby s heel and dropping blood onto a special screening card and shipped to the screening laboratory. Will I be told the newborn screen test results? Results are mailed to the hospital of birth. The physician of record is notified of any abnormal screen results by the Mississippi State Department of Health. It is very important that the hospital have the parent s correct last name, physical address, and a working telephone number. Your baby s physician can request the screen result from the hospital or call the Mississippi State Department of Health s Genetic Services Program for the screen results. Ask your baby s physician about the screen results at the first well baby checkup. If a repeat screen is requested, does it mean my baby may have a condition? No. There are several reasons why a repeat screen may be needed. If the screen is done incorrectly and is not okay for testing, a second test (repeat) is needed. If a screen is collected too early, a repeat screen is needed. A retest for these reasons simply means another sample is needed. If the first screen was abnormal for one of the conditions, a second test or a confirmatory test may be required. An abnormal screening result does not mean that your baby has a problem. The screening test does not say yes or no to whether your baby has a condition. It identifies a few babies who may need more specific testing. A confirmatory test may say yes or no to whether or not your child has a condition. Can these conditions be cured? Currently, there is no known cure for these conditions. The serious effects of these conditions can be lessened if a special diet, medical treatment, or other intervention is started early. If my baby has one of these conditions, does it mean my future children will also be affected? Your doctor can discuss this with you or refer you to a genetic specialist. These specialists have information about the specific condition and how it is inherited. They can help explain the potential risk for your future children. 27
29 APPENDIX G CCHD DELAYED SCREEN REPORTING FORM Utilize this form if the CCHD pulse oximetry screen was not completed prior to the submission of the newborn screening dried blood spot card. Newborn Demographic Information: First Name: Last Name: Birth Last Name: DOB (mm/dd/yyyy): Sex: Male Female Time of birth: Indeterminate (Circle One) Gestational age at birth (weeks): Birth weight (grams): Medical Record Number: Mother Demographic Information: First Name: Last Name: DOB (mm/dd/yyyy): Address: City: State: Zip: Delayed Screening Information: Date of initial pulse ox screening for CCHD: Military Time: If not performed, indicate the reason: (required field) Refused On O2 Other Expired Transferred Echocardiogram performed? Yes No Unsure Final Result of the CCHD Screen: Pass (Negative) Fail (Positive) Person completing form: Print Name Title: Date Completed: Phone Number: Facility Name: Mississippi State Department of Health Revised 7/10/15 Form 150
30 APPENDIX H CCHD FAILED SCREEN REPORTING FORM Utilize this form if the CCHD pulse oximetry screen was failed. Newborn Demographic Information: First Name: Last Name: Birth Last Name: DOB (mm/dd/yyyy): Sex: Male Female Time of birth: Indeterminate (Circle One) Gestational age at birth (weeks): Birth weight (grams): Medical Record Number: Mother Demographic Information: First Name: Last Name: DOB (mm/dd/yyyy): Address: City: State: Zip: Failed Screening Information: Date of initial pulse ox screening for CCHD: Was a prenatal ultrasound performed? (Circle one) Military Time: Yes No Unsure First Pulse Ox Screen Saturation Results Second Pulse Ox Screen (if indicated) Saturation Results Third Pulse Ox Screen (if indicated) Saturation Results Right hand % % % Foot % % % Screening Information Age (in hours) Was an echocardiogram performed? (Circle one) Yes No Unsure If yes date: Facility Name: Was the patient transferred? (Circle one) Yes If yes Where? (Facility name): No Date of transfer: Comment sections on back Mississippi State Department of Health Revised 7/10/15 Form 143
31 Reason for failed screen. What is the final diagnosis that explains the failed pulse oximetry screening? Cardiac Defects (check all that apply): Aortic Arch Atresia Aortic Arch Hypoplasia Coarctation of the Aorta Double-outlet Right Ventricle Ebstein Anomaly Hypoplastic Left Heart Syndrome Interrupted Aortic Arch Pulmonary Atresia, intact septum Pulmonary Stenosis Single Ventricle Tetrology of Fallot Total Anomalous Pulmonary Venous Return Transposition of the Great Arteries Tricuspid Atresia Truncus Arterious Ventricular Septal Defect Other Cardiac Defect(s) Describe: Non-Cardiac Explanation: Normal evaluation after failed screen Explanation: Pending diagnosis Explain: Person completing form: Print Name Title: Date Completed: Facility Name: Phone Number: Mississippi State Department of Health Revised 7/10/15 Form 143
32 APPENDIX I University of Mississippi Medical Center Jackson, Mississippi TERTIARY CARE CENTER Amino Acid Disorders, Organic Acid and Fatty Acid Disorders Clinic Staff University Medical Center Omar Ali Abdul-Rahman, MD University of Mississippi Health Care Brian Kirmse, MD Pediatric Medical Genetics Julie Kaplan, MD 2500 North State Street Jennifer Cook, CNP Jackson, MS Leslie Berryhill, R.D. LD Emergency after hours: (Page metabolic/newborn screening physician) Phone No Pager No Fax No Endocrine Disorders Clinic University Medical Center University of Mississippi Health Care Pediatric Endocrine Clinic 2500 North State Street Jackson, MS Emergency after hours: (Page pediatric endocrine/newborn screening physician) Staff George Moll, MD Michael Torchinksy, MD Naznin Dixit, MD Simeen Pasha, MD Phone No FAX No
33 APPENDIX I University of Mississippi Medical Center Jackson, Mississippi TERTIARY CARE CENTER (continued) Cystic Fibrosis Clinic Staff University Medical Center J. Marc Majure, M.D David Josey, M.D. University of Mississippi Health Care Lynn Walker, M.D. Pediatric Pulmonary Clinic 2500 North State Street Jackson, MS Phone No Emergency after hours: FAX No (Page pediatric pulmonary /newborn screening physician) Pediatric Allergy/Immunology Clinic University Medical Center University of Mississippi Health Center Pediatric Allergy/Immunology 2500 North State Street Jackson, MS Emergency after hours: (Page pediatric allergy/immunology) Pediatric Hematology/Sickle Cell Disease Clinic University Medical Center University of Mississippi Health Care Pediatric Hematology 2500 North State Street Jackson, MS Emergency after hours: (Page pediatric hematology/sickle cell/ newborn screening physician) Staff Anne Yates, MD Ray Rodriquez, MD Nina Dave, MD Phone No FAX # Staff Gail Megason, MD Betsy Herrington, MD Cathy Gordon, MD Suvankar Majumdar, MD Amy Forsythe, CFNP Tobi Breland, CFNP Phone No FAX No Out of state tertiary centers will be identified upon request of providers/family. 32


34 APPENDIX J MISSISSIPPI NEWBORN SCREENING FLOW CHART Newborn screening specimen collected hours of age Newborn screening specimen sent to PerkinElmer Genetics Results electronically downloaded to Mississippi database and electronically available to submitting hospitals Normal Repeat newborn screening required* Inconclusive and/or presumptive positive newborn screening result PerkinElmer reports results to submitting hospital to file in infant medical record Infant inpatient hospital collects repeat specimen Infant at home County health department collects repeat specimen Infant inpatient attending physician notified by newborn screening staff Infant at home Repeat newborn screening results reported to hospital Repeat newborn screening results reported to county health department and hospital Attending physician discusses evaluation and treatment with appropriate subspecialist District Genetic/CMP coordinator contacts primary care provider and facilitates tertiary care and interagency referrals The flow chart above explains the path of a screening specimen from collection to results. This process includes birthing hospitals, the newborn screening laboratory, newborn screening staff, primary care providers, and tertiary care centers. * Reasons for a repeat newborn screening include, but are not limited to, specimen quantity insufficient for testing, specimen appears diluted or contaminated, and specimen exhibits serum rings. 33
(f) "Birthing center" means any facility that is licensed by the Georgia Department of Community Health as a birthing center;
 Birthing center means any facility that is licensed by the Georgia Department of Community Health as a birthing center;") Ga. Comp. R. & Regs. r. 511-5-5-.02 Definitions Rule 511-5-5-.02. Definitions (a) "Abnormal test result" is a test result from blood testing or physiologic monitoring that is outside the screening limits
Ga. Comp. R. & Regs. r. 511-5-5-.02 Definitions Rule 511-5-5-.02. Definitions (a) "Abnormal test result" is a test result from blood testing or physiologic monitoring that is outside the screening limits
For Your Baby s Health Department of Health
 Newborn Screening For Your Baby s Health Department of Health Why is my baby tested? To help make sure your baby will be as healthy as possible. The blood test provides important information about your
Newborn Screening For Your Baby s Health Department of Health Why is my baby tested? To help make sure your baby will be as healthy as possible. The blood test provides important information about your
Newborn Screening: Train the Trainer PPT Questions
 Newborn Screening: Train the Trainer PPT Questions Bloodspot Screening Purpose 1. How many possible hidden disorders does the Oklahoma Newborn Screening Program screen for? A. >10 B. >20 C. >30 D. >40
Newborn Screening: Train the Trainer PPT Questions Bloodspot Screening Purpose 1. How many possible hidden disorders does the Oklahoma Newborn Screening Program screen for? A. >10 B. >20 C. >30 D. >40
Newborn Screening in Washington State Saving lives with a simple blood spot
 Newborn Screening in Washington State Saving lives with a simple blood spot Ashleigh Ragsdale, MPH Gauri Gupta, MScPH Objectives Newborn Screening Overview Process and Law Completing Collection Cards Video
Newborn Screening in Washington State Saving lives with a simple blood spot Ashleigh Ragsdale, MPH Gauri Gupta, MScPH Objectives Newborn Screening Overview Process and Law Completing Collection Cards Video
[R23-13-MET/HRG] STATE OF RHODE ISLAND AND PROVIDENCE PLANTATIONS DEPARTMENT OF HEALTH. February October October 1992 (E) September 1995
![[R23-13-MET/HRG] STATE OF RHODE ISLAND AND PROVIDENCE PLANTATIONS DEPARTMENT OF HEALTH. February October October 1992 (E) September 1995](/thumbs/95/122505027.jpg "[R23-13-MET/HRG] STATE OF RHODE ISLAND AND PROVIDENCE PLANTATIONS DEPARTMENT OF HEALTH. February October October 1992 (E) September 1995") RULES AND REGULATIONS PERTAINING TO THE NEWBORN METABOLIC, ENDOCRINE, AND HEMOGLOBINOPATHY SCREENING PROGRAM AND THE NEWBORN HEARING LOSS SCREENING PROGRAM [R23-13-MET/HRG] STATE OF RHODE ISLAND AND PROVIDENCE
RULES AND REGULATIONS PERTAINING TO THE NEWBORN METABOLIC, ENDOCRINE, AND HEMOGLOBINOPATHY SCREENING PROGRAM AND THE NEWBORN HEARING LOSS SCREENING PROGRAM [R23-13-MET/HRG] STATE OF RHODE ISLAND AND PROVIDENCE
Title: Assessing Recommendations Related To Timeliness of Newborn Screening
 Title: Assessing Recommendations Related To Timeliness of Newborn Screening Purpose: In January 2014, the Secretary s Discretionary Advisory Committee on Heritable Diseases on Newborns and Children (Committee)
Title: Assessing Recommendations Related To Timeliness of Newborn Screening Purpose: In January 2014, the Secretary s Discretionary Advisory Committee on Heritable Diseases on Newborns and Children (Committee)
NEWBORN METABOLIC SCREEN, MINNESOTA
 Lab Dept: Test Name: Chemistry NEWBORN METABOLIC SCREEN, MINNESOTA General Information Lab Order Codes: Synonyms: CPT Codes: Test Includes: PKUN Newborn Screen for Hyopothyroidism, Phenylketonuria (PKU),
Lab Dept: Test Name: Chemistry NEWBORN METABOLIC SCREEN, MINNESOTA General Information Lab Order Codes: Synonyms: CPT Codes: Test Includes: PKUN Newborn Screen for Hyopothyroidism, Phenylketonuria (PKU),
Overview of Newborn Screening, Potential Uses of Residual Dried Blood Spots, and Protection of Privacy
 Overview of Newborn Screening, Potential Uses of Residual Dried Blood Spots, and Protection of Privacy Alan R. Fleischman, M.D. Senior Vice President and Medical Director Chair, Federal Advisory Committee,
Overview of Newborn Screening, Potential Uses of Residual Dried Blood Spots, and Protection of Privacy Alan R. Fleischman, M.D. Senior Vice President and Medical Director Chair, Federal Advisory Committee,
Attachment 1. Newborn Screening Program Description
 Attachment 1 Newborn Screening Program Description The core mission of Texas Newborn Screening Program is to save children s lives through the early detection of life-threatening disorders. 34 Newborn
Attachment 1 Newborn Screening Program Description The core mission of Texas Newborn Screening Program is to save children s lives through the early detection of life-threatening disorders. 34 Newborn
Newborn Screening in Manitoba. Information for Health Care Providers
 Newborn Screening in Manitoba Information for Health Care Providers Newborn screening: a healthy start leads to a healthier life Health care professionals have provided newborn screening for phenylketonuria
Newborn Screening in Manitoba Information for Health Care Providers Newborn screening: a healthy start leads to a healthier life Health care professionals have provided newborn screening for phenylketonuria
NEWBORN SCREENING. in Massachusetts: Answers for You and Your Baby. University of Massachusetts Medical School
 University of Massachusetts Medical School NEWBORN SCREENING in Massachusetts: Answers for You and Your Baby New England Newborn Screening Program Biotech 4, 2nd Floor UMass Medical School 377 Plantation
University of Massachusetts Medical School NEWBORN SCREENING in Massachusetts: Answers for You and Your Baby New England Newborn Screening Program Biotech 4, 2nd Floor UMass Medical School 377 Plantation
Newborn Screening: Focus on Treatment
 Newborn Screening: Focus on Treatment Alan R. Fleischman, M.D. Senior Vice President and Medical Director March of Dimes National Conference of State Legislatures July 21, 2008 Newborn Screening: A Public
Newborn Screening: Focus on Treatment Alan R. Fleischman, M.D. Senior Vice President and Medical Director March of Dimes National Conference of State Legislatures July 21, 2008 Newborn Screening: A Public
Positive Newborn Screens: What do you do next?
 Positive Newborn Screens: What do you do next? James B. Gibson, MD, Ph.D. Biochemical Geneticist at Specially for Children Clinical Associate Professor of Pediatrics UTHSCSA Carla R. Scott, MD Pediatric
Positive Newborn Screens: What do you do next? James B. Gibson, MD, Ph.D. Biochemical Geneticist at Specially for Children Clinical Associate Professor of Pediatrics UTHSCSA Carla R. Scott, MD Pediatric
Screening for Critical Congenital Heart Disease
 Screening for Critical Congenital Heart Disease Caroline K. Lee, MD Pediatric Cardiology Disclosures I have no relevant financial relationships or conflicts of interest 1 Most Common Birth Defect Most
Screening for Critical Congenital Heart Disease Caroline K. Lee, MD Pediatric Cardiology Disclosures I have no relevant financial relationships or conflicts of interest 1 Most Common Birth Defect Most
MISSOURI DEPARTMENT OF HEALTH AND SENIOR SERVICES
 NEWBORN SCREENING Protecting your newborn MISSOURI DEPARTMENT OF HEALTH AND SENIOR SERVICES [ 1 ] NEWBORN SCREENING [ 2 ] FREQUENTLY ASKED QUESTIONS [ 4 ] DISORDERS INCLUDED IN NEWBORN SCREENING [ 12 ]
NEWBORN SCREENING Protecting your newborn MISSOURI DEPARTMENT OF HEALTH AND SENIOR SERVICES [ 1 ] NEWBORN SCREENING [ 2 ] FREQUENTLY ASKED QUESTIONS [ 4 ] DISORDERS INCLUDED IN NEWBORN SCREENING [ 12 ]
HA Convention 2016 Master course How to Handle Abnormal Newborn Metabolic Screening Results Causes, Management and Follow up
 HA Convention 2016 Master course How to Handle Abnormal Newborn Metabolic Screening Results Causes, Management and Follow up Dr. Josephine Chong Clinical Professional Consultant Centre of Inborn Errors
HA Convention 2016 Master course How to Handle Abnormal Newborn Metabolic Screening Results Causes, Management and Follow up Dr. Josephine Chong Clinical Professional Consultant Centre of Inborn Errors
Standard of Newborn Care in the Age of Birth Plans. Stephanie Deal, MD Tiffany McKee-Garrett, MD
 Standard of Newborn Care in the Age of Birth Plans Stephanie Deal, MD Tiffany McKee-Garrett, MD Disclosure We have no relevant financial relationships with the manufacturers(s) of any commercial products(s)
Standard of Newborn Care in the Age of Birth Plans Stephanie Deal, MD Tiffany McKee-Garrett, MD Disclosure We have no relevant financial relationships with the manufacturers(s) of any commercial products(s)
Mississippi Newborn Screening Report
 Mississippi Newborn Screening Report 2011-2016 Introduction The primary goal of the Newborn Screening Program is to screen every infant born in the state and refer infants with abnormal results to appropriate
Mississippi Newborn Screening Report 2011-2016 Introduction The primary goal of the Newborn Screening Program is to screen every infant born in the state and refer infants with abnormal results to appropriate
Newborn Bloodspot Screening Information for parents
 Newborn Bloodspot Screening Information for parents You will be offered a bloodspot screening test for your newborn baby for several rare but serious conditions. The sample for this test is usually taken
Newborn Bloodspot Screening Information for parents You will be offered a bloodspot screening test for your newborn baby for several rare but serious conditions. The sample for this test is usually taken
Considerations in Choosing Screening Conditions: One (US) Approach
 Approach") 22 Plenary Considerations in Choosing Screening Conditions: One (US) Approach Bradford L Therrell Jr, 1,2 MS, PhD Abstract The lack of a national policy on newborn screening (NBS) in the United States
22 Plenary Considerations in Choosing Screening Conditions: One (US) Approach Bradford L Therrell Jr, 1,2 MS, PhD Abstract The lack of a national policy on newborn screening (NBS) in the United States
Routine Newborn Screening, Testing the Newborn Inherited Metabolic Disorders Update August 2015
 Routine Newborn Screening, Testing the Newborn Inherited Metabolic Disorders Update August 2015 Metabolic birth defects can cause physical problems, mental retardation and, in some cases, death. It is
Routine Newborn Screening, Testing the Newborn Inherited Metabolic Disorders Update August 2015 Metabolic birth defects can cause physical problems, mental retardation and, in some cases, death. It is
Newborn Bloodspot Screening Information for parents
 Newborn Bloodspot Screening Information for parents You will be offered a bloodspot screening test for your newborn baby for several rare but serious conditions. The sample for this test is usually taken
Newborn Bloodspot Screening Information for parents You will be offered a bloodspot screening test for your newborn baby for several rare but serious conditions. The sample for this test is usually taken
TIMELINESS OF NEWBORN SCREENING: RECOMMENDATIONS FROM ADVISORY COMMITTEE ON HERITABLE DISORDERS IN NEWBORNS AND CHILDREN
 TIMELINESS OF NEWBORN SCREENING: RECOMMENDATIONS FROM ADVISORY COMMITTEE ON HERITABLE DISORDERS IN NEWBORNS AND CHILDREN Susan Tanksley, PhD May 19, 2015 TIMELINESS - BACKGROUND In order to effectively
TIMELINESS OF NEWBORN SCREENING: RECOMMENDATIONS FROM ADVISORY COMMITTEE ON HERITABLE DISORDERS IN NEWBORNS AND CHILDREN Susan Tanksley, PhD May 19, 2015 TIMELINESS - BACKGROUND In order to effectively
NEWBORN SCREENING. health.mo.gov/newbornscreening MISSOURI DEPARTMENT OF HEALTH AND SENIOR SERVICES
 NEWBORN SCREENING health.mo.gov/newbornscreening MISSOURI DEPARTMENT OF HEALTH AND SENIOR SERVICES Table of Contents NEWBORN SCREENING...1 FREQUENTLY ASKED QUESTIONS...2 DISORDERS INCLUDED IN NEWBORN SCREENING...4
NEWBORN SCREENING health.mo.gov/newbornscreening MISSOURI DEPARTMENT OF HEALTH AND SENIOR SERVICES Table of Contents NEWBORN SCREENING...1 FREQUENTLY ASKED QUESTIONS...2 DISORDERS INCLUDED IN NEWBORN SCREENING...4
A Guide for Prenatal Educators
 A Guide for Prenatal Educators Why Teach Newborn Screening This booklet is designed to make it easy for you, a prenatal educator, to effectively inform expectant parents about newborn screening. All of
A Guide for Prenatal Educators Why Teach Newborn Screening This booklet is designed to make it easy for you, a prenatal educator, to effectively inform expectant parents about newborn screening. All of
2015 Annual Report for New Mexico s Newborn Screening (NBS) Program
 Program") 2015 Annual Report for New Mexico s Newborn Screening (NBS) Program Sawyer-A Family s Story Inside this Edition A Family Story......1 Why Screen....4 When to Screen...4 What is NBS....5 Screened Conditions..5
2015 Annual Report for New Mexico s Newborn Screening (NBS) Program Sawyer-A Family s Story Inside this Edition A Family Story......1 Why Screen....4 When to Screen...4 What is NBS....5 Screened Conditions..5
Health Chapter ALABAMA STATE BOARD OF HEALTH ALABAMA DEPARTMENT OF PUBLIC HEALTH BUREAU OF FAMILY HEALTH SERVICES ADMINISTRATIVE CODE
 ALABAMA STATE BOARD OF HEALTH ALABAMA DEPARTMENT OF PUBLIC HEALTH BUREAU OF FAMILY HEALTH SERVICES ADMINISTRATIVE CODE CHAPTER 420-10-1 CARE AND TREATMENT OF INFANTS IDENTIFIED THROUGH THE NEWBORN SCREENING
ALABAMA STATE BOARD OF HEALTH ALABAMA DEPARTMENT OF PUBLIC HEALTH BUREAU OF FAMILY HEALTH SERVICES ADMINISTRATIVE CODE CHAPTER 420-10-1 CARE AND TREATMENT OF INFANTS IDENTIFIED THROUGH THE NEWBORN SCREENING
Blood Lead Filter Paper Collection. Regional Pathology Services University of Nebraska Medical Center
 Blood Lead Filter Paper Collection Regional Pathology Services University of Nebraska Medical Center 800.334.0459 Overview Use capillary blood from heel or finger stick Fill in three circles (two circles
Blood Lead Filter Paper Collection Regional Pathology Services University of Nebraska Medical Center 800.334.0459 Overview Use capillary blood from heel or finger stick Fill in three circles (two circles
Assessing Mothers Knowledge of the Wisconsin Newborn Screening Program. Sara Wolfgram UW Master of Public Health Symposium August 11, 2006
 Assessing Mothers Knowledge of the Wisconsin Newborn Screening Program Sara Wolfgram UW Master of Public Health Symposium August 11, 2006 Background Wisconsin Newborn Screening (NBS): Began in 1965 Heel
Assessing Mothers Knowledge of the Wisconsin Newborn Screening Program Sara Wolfgram UW Master of Public Health Symposium August 11, 2006 Background Wisconsin Newborn Screening (NBS): Began in 1965 Heel
Newborn Screening Manual
 Newborn Screening Manual A GUIDE FOR NEWBORN CARE PROVIDERS N ONATAL Newborn Screening Manual: A guide for newborn care providers This manual was created by Newborn Screening Ontario (NSO) as a comprehensive
Newborn Screening Manual A GUIDE FOR NEWBORN CARE PROVIDERS N ONATAL Newborn Screening Manual: A guide for newborn care providers This manual was created by Newborn Screening Ontario (NSO) as a comprehensive
What Makes a Satisfactory Newborn Screen Sample?
 What Makes a Satisfactory Newborn Screen Sample? Feb 21, 2013 Christine McRoberts Newborn Screening Ontario One of the challenges the Newborn screening Ontario program (NSO) faces every day is the receipt
What Makes a Satisfactory Newborn Screen Sample? Feb 21, 2013 Christine McRoberts Newborn Screening Ontario One of the challenges the Newborn screening Ontario program (NSO) faces every day is the receipt
Newborn Screening. Helping babies start life healthy. Minnesota Newborn Screening Program
 Newborn Screening Helping babies start life healthy Minnesota Newborn Screening Program What is newborn screening? Newborn screening is a set of three tests that check babies for serious, rare conditions.
Newborn Screening Helping babies start life healthy Minnesota Newborn Screening Program What is newborn screening? Newborn screening is a set of three tests that check babies for serious, rare conditions.
11/27/2012. Objectives. What is Critical Congenital Heart Disease?
 Screening for Critical Congenital Heart Disease in the Apparently Healthy Newborn A presentation of Texas Pulse Oximetry Project: A Joint Educational Initiative of The University of Texas Health Science
Screening for Critical Congenital Heart Disease in the Apparently Healthy Newborn A presentation of Texas Pulse Oximetry Project: A Joint Educational Initiative of The University of Texas Health Science
GUIDE TO NEWBORN SCREENING PROGRAMME
 \ GUIDE TO NEWBORN SCREENING PROGRAMME 1 MEDILAB PROFILE MEDILAB, the leading independent provider of Clinical Laboratory Diagnostic Services in Cyprus, was established in 1980 by Mr. C. Pavlides and has
\ GUIDE TO NEWBORN SCREENING PROGRAMME 1 MEDILAB PROFILE MEDILAB, the leading independent provider of Clinical Laboratory Diagnostic Services in Cyprus, was established in 1980 by Mr. C. Pavlides and has
Annual Report Calendar Year 2015
 Annual Report Calendar Year 2015 Page 1 of 19 Contents 1. SAMPLE VOLUMES IN 2015...3 1.1 SCREENING SAMPLES...3 1.1.1 INFANTS SCREENED...3 1.1.2 DECLINED/DEFERRED TESTING...4 1.1.3 MISSED SCREENS...5 1.2
Annual Report Calendar Year 2015 Page 1 of 19 Contents 1. SAMPLE VOLUMES IN 2015...3 1.1 SCREENING SAMPLES...3 1.1.1 INFANTS SCREENED...3 1.1.2 DECLINED/DEFERRED TESTING...4 1.1.3 MISSED SCREENS...5 1.2
For the Ongoing Management of Babies under 1 year old.
 Pathway Author: Nicy Turney, Senior Nurse Professional Lead, Health Visiting 19.06.17 For the Ongoing Management of Babies under 1 year old. Check Health Records (CHR) to undertake daily checks to identify:
Pathway Author: Nicy Turney, Senior Nurse Professional Lead, Health Visiting 19.06.17 For the Ongoing Management of Babies under 1 year old. Check Health Records (CHR) to undertake daily checks to identify:
SUNY Downstate Medical Center -University Hospital of Brooklyn Network Department of Pathology Policy and Procedure
 SUNY Downstate Medical Center -University Hospital of Brooklyn Network Department of Pathology Policy and Procedure Subject: NEWBORN SCREENING FOR METABOLIC DEFICIENCIES Prepared By: Yolaine Henry Edit
SUNY Downstate Medical Center -University Hospital of Brooklyn Network Department of Pathology Policy and Procedure Subject: NEWBORN SCREENING FOR METABOLIC DEFICIENCIES Prepared By: Yolaine Henry Edit
Assessing the follow-up of BART hemoglobin reported by the Wisconsin Newborn Screening Laboratory
 Assessing the follow-up of BART hemoglobin reported by the Wisconsin Newborn Screening Laboratory Bao Yang MPH Candidate Background The Wisconsin Newborn Screening (NBS) Laboratory screens 70,000 babies
Assessing the follow-up of BART hemoglobin reported by the Wisconsin Newborn Screening Laboratory Bao Yang MPH Candidate Background The Wisconsin Newborn Screening (NBS) Laboratory screens 70,000 babies
NEWBORN SCREENING. in Massachusetts: Information for You and Your Baby. University of Massachusetts Medical School
 University of Massachusetts Medical School NEWBORN SCREENING in Massachusetts: Information for You and Your Baby New England Newborn Screening Program Biotech 4, 2nd Floor UMass Medical School 377 Plantation
University of Massachusetts Medical School NEWBORN SCREENING in Massachusetts: Information for You and Your Baby New England Newborn Screening Program Biotech 4, 2nd Floor UMass Medical School 377 Plantation
Beyond the case for NBS in South Africa. Chris Vorster 28/05/2016
 Beyond the case for NBS in South Africa Chris Vorster 28/05/2016 The case for NBS in SA Economic justification Cost Utility analysis = Cost/QALY GDP/Capita Immediate implementation (WHO) Political justification
Beyond the case for NBS in South Africa Chris Vorster 28/05/2016 The case for NBS in SA Economic justification Cost Utility analysis = Cost/QALY GDP/Capita Immediate implementation (WHO) Political justification
Newborn Genetic Testing & Surveillance System
 Georgia Newborn Genetic Testing & Surveillance System State GA Statute/ Rule STATUTE: Chapter 1 Chapter 2 Chapter 12 Title 33 Chapter 54 RULE: 290-5-.02 and 290-5- 24 Language Specific to Genetic Testing
Georgia Newborn Genetic Testing & Surveillance System State GA Statute/ Rule STATUTE: Chapter 1 Chapter 2 Chapter 12 Title 33 Chapter 54 RULE: 290-5-.02 and 290-5- 24 Language Specific to Genetic Testing
Further expansion of the neonatal screening panel in the Netherlands
 Further expansion of the neonatal screening panel in the Netherlands J.Gerard Loeber APHL-NBSGT, St.Louis (MO), USA 290216 Population Area Newborns 6.01 million 0.35:1 16.8 million 180,693 sq km 4.3:1
Further expansion of the neonatal screening panel in the Netherlands J.Gerard Loeber APHL-NBSGT, St.Louis (MO), USA 290216 Population Area Newborns 6.01 million 0.35:1 16.8 million 180,693 sq km 4.3:1
Newborn Bloodspot Screening (NBS) Training for Health Visitors. December 2017
 Training for Health Visitors. December 2017") Newborn Bloodspot Screening (NBS) Training for Health Visitors www.newbornbloodspotscreening.wales.nhs.uk December 2017 Aims To enable you to gain a clear understanding of the following: Aim and rationale
Newborn Bloodspot Screening (NBS) Training for Health Visitors www.newbornbloodspotscreening.wales.nhs.uk December 2017 Aims To enable you to gain a clear understanding of the following: Aim and rationale
NEWBORN SCREENING in Massachusetts: Answers for you and your baby
 NEWBORN SCREENING in Massachusetts: Answers for you and your baby The New England Newborn Screening Program University of Massachusetts Medical School 305 South St. Jamaica Plain, MA 02130 617-983-6300
NEWBORN SCREENING in Massachusetts: Answers for you and your baby The New England Newborn Screening Program University of Massachusetts Medical School 305 South St. Jamaica Plain, MA 02130 617-983-6300
The Fetal Cardiology Program
 The Fetal Cardiology Program at Texas Children s Fetal Center About the program Since the 1980s, Texas Children s Fetal Cardiology Program has provided comprehensive fetal cardiac care to expecting families
The Fetal Cardiology Program at Texas Children s Fetal Center About the program Since the 1980s, Texas Children s Fetal Cardiology Program has provided comprehensive fetal cardiac care to expecting families
Collection of Dried Blood Spots from Infants for Diagnosis of HIV by DNA PCR. MOH Regional Trainings March 2013
 Collection of Dried Blood Spots from Infants for Diagnosis of HIV by DNA MOH Regional Trainings March 2013 Outline Introduce DBS testing Rationale Testing algorithm Sample collection, storage and transportation
Collection of Dried Blood Spots from Infants for Diagnosis of HIV by DNA MOH Regional Trainings March 2013 Outline Introduce DBS testing Rationale Testing algorithm Sample collection, storage and transportation
Most common is the congenital adrenogenital syndrome (AGS) or congenital adrenal hyperplasia (CAH) due to 21-hydroxylase deficiency.
 or congenital adrenal hyperplasia (CAH) due to 21-hydroxylase deficiency.") Newborn Screening Examination parameters: TSH-neonatal (hypothyreosis), 17-OH progesterone (AGS), galactose (galactosemia), galactose-uridyl transferase (galacto semia), biotinidase (biotinidase ), phenylalanine
Newborn Screening Examination parameters: TSH-neonatal (hypothyreosis), 17-OH progesterone (AGS), galactose (galactosemia), galactose-uridyl transferase (galacto semia), biotinidase (biotinidase ), phenylalanine
MEDICAL COVERAGE GUIDELINES ORIGINAL EFFECTIVE DATE: 12/19/17 SECTION: MEDICINE LAST REVIEW DATE: LAST CRITERIA REVISION DATE: ARCHIVE DATE:
 MEDICAL FOODS Non-Discrimination Statement and Multi-Language Interpreter Services information are located at the end of this document. Coverage for services, procedures, medical devices and drugs are
MEDICAL FOODS Non-Discrimination Statement and Multi-Language Interpreter Services information are located at the end of this document. Coverage for services, procedures, medical devices and drugs are
The Compelling Benefits of Routine 2 nd NBS: A Fifteen-Year Review in Washington State. Saving lives with a simple blood spot
 The Compelling Benefits of Routine 2 nd NBS: A Fifteen-Year Review in Washington State Caroline T. Nucup-Villaruz, MD Primary Author NBS Consultant - Disorder FU Santosh Shaunak Co-Author & Presenter Laboratory
The Compelling Benefits of Routine 2 nd NBS: A Fifteen-Year Review in Washington State Caroline T. Nucup-Villaruz, MD Primary Author NBS Consultant - Disorder FU Santosh Shaunak Co-Author & Presenter Laboratory
Russell-Silver syndrome (RSS)
") GENETIC DIAGNOSTIC LABORATORY Russell-Silver syndrome (RSS) Background: Russell-Silver syndrome (RSS, OMIM 103280, 180860) is a growth disorder characterized by intrauterine and postnatal growth retardation,
GENETIC DIAGNOSTIC LABORATORY Russell-Silver syndrome (RSS) Background: Russell-Silver syndrome (RSS, OMIM 103280, 180860) is a growth disorder characterized by intrauterine and postnatal growth retardation,
Hypertrophy of liver Neonatal hypoglycemia Omphalocele Large for gestational age Other:
 REQUEST FOR BECKWITH-WIEDEMANN SYNDROME (BWS) TESTING Please provide the following information. We cannot perform your test without ALL of this information. PLEASE PRINT ALL ANSWERS PATIENT INFORMATION
REQUEST FOR BECKWITH-WIEDEMANN SYNDROME (BWS) TESTING Please provide the following information. We cannot perform your test without ALL of this information. PLEASE PRINT ALL ANSWERS PATIENT INFORMATION
Early Intervention: The Importance of Newborn Screening
 Early Intervention: The Importance of Newborn Screening July is the 50 th anniversary of screening newborns for genetic, endocrine and metabolic diseases. Missouri Kids Count is celebrating one of our
Early Intervention: The Importance of Newborn Screening July is the 50 th anniversary of screening newborns for genetic, endocrine and metabolic diseases. Missouri Kids Count is celebrating one of our
Newborn Metabolic Screening Programme Annual Report
 Newborn Metabolic Screening Programme Annual Report January to December 2015 Disclaimer This publication reports on information provided to the Ministry of Health by the Auckland District Health Board.
Newborn Metabolic Screening Programme Annual Report January to December 2015 Disclaimer This publication reports on information provided to the Ministry of Health by the Auckland District Health Board.
PAEDIATRIC PROVIDER INITIATED TESTING AND COUNSELLING
 PAEDIATRIC PROVIDER INITIATED TESTING AND COUNSELLING This checklist is offered as an aid to support supervision and quality assurance for paediatric PITC services. Through observation, interviews and
PAEDIATRIC PROVIDER INITIATED TESTING AND COUNSELLING This checklist is offered as an aid to support supervision and quality assurance for paediatric PITC services. Through observation, interviews and
9.Pediatric Procedures
 9.Pediatric Procedures A. Introduction 1. Pediatric blood collection may be by skin puncture or venipuncture. 2. Skill in pediatric phlebotomy is gained by knowledge of special collection equipment, observation
9.Pediatric Procedures A. Introduction 1. Pediatric blood collection may be by skin puncture or venipuncture. 2. Skill in pediatric phlebotomy is gained by knowledge of special collection equipment, observation
RESULTS REPORTING MANUAL. Hospital Births Newborn Screening Program June 2016
 RESULTS REPORTING MANUAL Hospital Births Newborn Screening Program June 2016 CONTENTS GETTING STARTED... 1 Summary... 1 Logging In... 1 Access For New Hires... 2 Reporting Parental Refusals... 3 Adding
RESULTS REPORTING MANUAL Hospital Births Newborn Screening Program June 2016 CONTENTS GETTING STARTED... 1 Summary... 1 Logging In... 1 Access For New Hires... 2 Reporting Parental Refusals... 3 Adding
Annual Report Calendar Year 2014
 Annual Report Calendar Year 2014 1 Contents 1. SAMPLE VOLUMES IN 2014...4 1.1 SCREENING SAMPLES...4 1.1.1 INFANTS SCREENED...4 1.1.2 DECLINED/DEFERRED TESTING...5 1.1.3 MISSED SCREENS...6 1.2 NON-SCREENING
Annual Report Calendar Year 2014 1 Contents 1. SAMPLE VOLUMES IN 2014...4 1.1 SCREENING SAMPLES...4 1.1.1 INFANTS SCREENED...4 1.1.2 DECLINED/DEFERRED TESTING...5 1.1.3 MISSED SCREENS...6 1.2 NON-SCREENING
CCHD Screening with Pulse Oximetry: A Success Story!
 CCHD Screening with Pulse Oximetry: A Success Story! Nicole Spillane, MD Associate Director of Neonatology, HackensackUMC Hackensack Meridian Health Objective Recognize the contribution of pulse oximetry
CCHD Screening with Pulse Oximetry: A Success Story! Nicole Spillane, MD Associate Director of Neonatology, HackensackUMC Hackensack Meridian Health Objective Recognize the contribution of pulse oximetry
Safety Regulations and Procedures Occupational Health Bloodborne Pathogens Exposure Control Plan S80.10, updated, May Contains information for:
 APPENDIX A Safety Regulations and Procedures Occupational Health Bloodborne Pathogens Exposure Control Plan S80.10, updated, May 2018 BLOODBORNE PATHOGEN EXPOSURE INCIDENT PACKET Contains information for:
APPENDIX A Safety Regulations and Procedures Occupational Health Bloodborne Pathogens Exposure Control Plan S80.10, updated, May 2018 BLOODBORNE PATHOGEN EXPOSURE INCIDENT PACKET Contains information for:
Green Amber Red Assurance Level
 A re-audit of the turnaround time of samples for the Sickle Cell and Thalassaemia Newborn Screening Programme, in the Manchester Newborn Screening Laboratory Clinical Audit Report May 2014 Clinical Audit
A re-audit of the turnaround time of samples for the Sickle Cell and Thalassaemia Newborn Screening Programme, in the Manchester Newborn Screening Laboratory Clinical Audit Report May 2014 Clinical Audit
How to Recognize a Suspected Cardiac Defect in the Neonate
 Neonatal Nursing Education Brief: How to Recognize a Suspected Cardiac Defect in the Neonate https://www.seattlechildrens.org/healthcareprofessionals/education/continuing-medical-nursing-education/neonatalnursing-education-briefs/
Neonatal Nursing Education Brief: How to Recognize a Suspected Cardiac Defect in the Neonate https://www.seattlechildrens.org/healthcareprofessionals/education/continuing-medical-nursing-education/neonatalnursing-education-briefs/
Employee Benefits & Executive Compensation ADVISORY
 Employee Benefits & Executive Compensation ADVISORY July 27, 2010 Agencies Outline Preventive Care Coverage Requirements under PPACA The Departments of Health and Human Services (HHS), Treasury and Labor
Employee Benefits & Executive Compensation ADVISORY July 27, 2010 Agencies Outline Preventive Care Coverage Requirements under PPACA The Departments of Health and Human Services (HHS), Treasury and Labor
Newborn bloodspot testing
 Policy HUMAN GENETICS SOCIETY OF AUSTRALASIA ARBN. 076 130 937 (Incorporated Under the Associations Incorporation Act) The liability of members is limited RACP, 145 Macquarie Street, Sydney NSW 2000, Australia
Policy HUMAN GENETICS SOCIETY OF AUSTRALASIA ARBN. 076 130 937 (Incorporated Under the Associations Incorporation Act) The liability of members is limited RACP, 145 Macquarie Street, Sydney NSW 2000, Australia
Newborn Screening: Blood Spot Disorders
 Newborn Screening: Blood Spot Disorders Arizona s Newborn Screening Program Program Overview Panel of Disorders Disorder Descriptions Program Components Hospitals ADHS Lab ADHS Follow-up ADHS Billing Medical
Newborn Screening: Blood Spot Disorders Arizona s Newborn Screening Program Program Overview Panel of Disorders Disorder Descriptions Program Components Hospitals ADHS Lab ADHS Follow-up ADHS Billing Medical
Newborn Screen & Development Facts about the genetic diseases new since March 2006 (Excluding Cystic Fibrosis)
") Newborn Screen & Development Facts about the genetic diseases new since March 2006 (Excluding Cystic Fibrosis) 1) Argininosuccinic acidemia (ASA) a) Incidence: ~1 in 70,000 b) Deficiency in an enzyme of
Newborn Screen & Development Facts about the genetic diseases new since March 2006 (Excluding Cystic Fibrosis) 1) Argininosuccinic acidemia (ASA) a) Incidence: ~1 in 70,000 b) Deficiency in an enzyme of
5. Hospitals will provide the family with a copy of the Michigans Community Program: Information for Parents (MDCH /01). Copies can be ordered,
. Copies can be ordered,") GUIDELINES FOR HEARING SCREENING A goal of newborn hearing screening is to ensure that all newborns receive a hearing screen before discharge from the hospital or before one month of age. All hospitals
GUIDELINES FOR HEARING SCREENING A goal of newborn hearing screening is to ensure that all newborns receive a hearing screen before discharge from the hospital or before one month of age. All hospitals
Lab Guide 2019 Metabolic Section Lab Guide
 Lab Guide 2019 Metabolic Section Lab Guide Quantitative Amino acids Plasma Plasma. Container/Tube: Preferred EDTA, Place immediately in ice. Acceptable: lithium heparin, sodium heparin. Patient preparation:
Lab Guide 2019 Metabolic Section Lab Guide Quantitative Amino acids Plasma Plasma. Container/Tube: Preferred EDTA, Place immediately in ice. Acceptable: lithium heparin, sodium heparin. Patient preparation:
MNSCREEN TRAINING MANUAL Hospital Births Newborn Screening Program October 2015
 MNSCREEN TRAINING MANUAL Hospital Births Newborn Screening Program October 2015 CONTENTS PART 1: GETTING STARTED... 2 Logging In... 2 Access for New Hires... 2 Reporting Refusals... 3 Adding Patient Records...
MNSCREEN TRAINING MANUAL Hospital Births Newborn Screening Program October 2015 CONTENTS PART 1: GETTING STARTED... 2 Logging In... 2 Access for New Hires... 2 Reporting Refusals... 3 Adding Patient Records...
What s new in newborn screening?
 PERSPECTIVE What s new in newborn screening? Bradford L Therrell Jr 1,2, Colleen Buechner 1,2, Michele A Lloyd-Puryear 3,4, Peter C van Dyck 3,5 & Marie Y Mann 3,6 Author for correspondence 1 National
PERSPECTIVE What s new in newborn screening? Bradford L Therrell Jr 1,2, Colleen Buechner 1,2, Michele A Lloyd-Puryear 3,4, Peter C van Dyck 3,5 & Marie Y Mann 3,6 Author for correspondence 1 National
Information for health professionals
 Introduction of a new screening test for newborn babies in Wales Newborn bloodspot screening for Medium chain acyl-coa dehydrogenase deficiency (MCADD) Newborn bloodspot screening for MCADD is being introduced
Introduction of a new screening test for newborn babies in Wales Newborn bloodspot screening for Medium chain acyl-coa dehydrogenase deficiency (MCADD) Newborn bloodspot screening for MCADD is being introduced
LOUISIANA MEDICAID PROGRAM ISSUED: 09/28/12 REPLACED: 02/01/12 CHAPTER 5: PROFESSIONAL SERVICES SECTION 5.1: COVERED SERVICES PAGE(S) 7
 7") Early and Periodic Screening, Diagnosis and Treatment (EPSDT) Medicaid recipients under 21 years of age are entitled to receive all medically necessary health care, diagnostic services, treatment and other
Early and Periodic Screening, Diagnosis and Treatment (EPSDT) Medicaid recipients under 21 years of age are entitled to receive all medically necessary health care, diagnostic services, treatment and other
Information for health professionals
 Changes to the Newborn Bloodspot Screening Policy for Congenital Hypothyroidism (CHT) in Preterm Babies A UK policy change has been agreed that will mean changes to: which preterm babies require second
Changes to the Newborn Bloodspot Screening Policy for Congenital Hypothyroidism (CHT) in Preterm Babies A UK policy change has been agreed that will mean changes to: which preterm babies require second
Pulse Oximetry Screening in Newborns to Enhance the Detection Of Critical Congenital Heart Disease. Frequently Asked Questions
 Pulse Oximetry Screening in Newborns to Enhance the Detection Of Critical Congenital Heart Disease Frequently Asked Questions Current Recommendation: The current recommendation from the Canadian Cardiovascular
Pulse Oximetry Screening in Newborns to Enhance the Detection Of Critical Congenital Heart Disease Frequently Asked Questions Current Recommendation: The current recommendation from the Canadian Cardiovascular
Newborn Metabolic Screening Programme. Annual Report
 Newborn Metabolic Screening Programme Annual Report January to December 2016 1 Disclaimer This publication reports on information provided to the Ministry of Health by the Auckland District Health Board.
Newborn Metabolic Screening Programme Annual Report January to December 2016 1 Disclaimer This publication reports on information provided to the Ministry of Health by the Auckland District Health Board.
Newborn screening project at departments of genetics and endocrinology SGPGIMS, Lucknow
 Newborn screening project at departments of genetics and endocrinology SGPGIMS, Lucknow Population based newborn screening (NBS) is being carried out in developed nations for the last 40 years. It aims
Newborn screening project at departments of genetics and endocrinology SGPGIMS, Lucknow Population based newborn screening (NBS) is being carried out in developed nations for the last 40 years. It aims
NEWBORN SCREENING PRENATAL CURRICULUM
 NEWBORN SCREENING PRENATAL CURRICULUM GOAL 1: Explain why newborn screening is important GOAL 2: How newborn screening is performed GOAL 3: The newborn screening test results GOAL 4: Follow-up to newborn
NEWBORN SCREENING PRENATAL CURRICULUM GOAL 1: Explain why newborn screening is important GOAL 2: How newborn screening is performed GOAL 3: The newborn screening test results GOAL 4: Follow-up to newborn
Sending and Receiving Newborn Screening Results in Indiana: The HIE Perspective
 Sending and Receiving Newborn Screening Results in Indiana: The HIE Perspective Shaun Grannis, MD, MS FAAFP, Regenstrief Bob Bowman, MS, MA, MS, ISDH Nov 2, 2010 What we ll cover Health Information Exchange
Sending and Receiving Newborn Screening Results in Indiana: The HIE Perspective Shaun Grannis, MD, MS FAAFP, Regenstrief Bob Bowman, MS, MA, MS, ISDH Nov 2, 2010 What we ll cover Health Information Exchange
The Fetal Care Center at NewYork-Presbyterian/ Weill Cornell Medicine
 The Fetal Care Center at NewYork-Presbyterian/ Weill Cornell Medicine Prompt and Personalized Care for Women with Complex Pregnancies A Team of Experts additional training in maternal and fetal complications
The Fetal Care Center at NewYork-Presbyterian/ Weill Cornell Medicine Prompt and Personalized Care for Women with Complex Pregnancies A Team of Experts additional training in maternal and fetal complications
5/22/2013. Alan Zuckerman 1, Swapna Abhyankar 1, Tiffany Colarusso 2, Richard Olney 2, Kristin Burns 3, Marci Sontag 4
 Alan Zuckerman 1, Swapna Abhyankar 1, Tiffany Colarusso 2, Richard Olney 2, Kristin Burns 3, Marci Sontag 4 1 National Library of Medicine, NIH, Bethesda, MD, USA, 2 Centers for Disease Control and Prevention,
Alan Zuckerman 1, Swapna Abhyankar 1, Tiffany Colarusso 2, Richard Olney 2, Kristin Burns 3, Marci Sontag 4 1 National Library of Medicine, NIH, Bethesda, MD, USA, 2 Centers for Disease Control and Prevention,
Objectives. Prenatal Diagnosis of Critical Congenital Heart Disease. The Law. Disclosure. Dylan s Story
 Keeping the Beat: Pediatric Cardiac Screening and Management of Congenital Heart Disease Prenatal Diagnosis of Critical Congenital Heart Disease Robert Koppel, MD Neonatal/Perinatal Medicine, Pediatrics
Keeping the Beat: Pediatric Cardiac Screening and Management of Congenital Heart Disease Prenatal Diagnosis of Critical Congenital Heart Disease Robert Koppel, MD Neonatal/Perinatal Medicine, Pediatrics
Influenza-Associated Pediatric Mortality rev Jan 2018
 rev Jan 2018 Infectious Agent Influenza A, B or C virus BASIC EPIDEMIOLOGY Transmission Transmission occurs via droplet spread. After a person infected with influenza coughs, sneezes, or talks, influenza
rev Jan 2018 Infectious Agent Influenza A, B or C virus BASIC EPIDEMIOLOGY Transmission Transmission occurs via droplet spread. After a person infected with influenza coughs, sneezes, or talks, influenza
APPENDIX C: LEAD SCREENING
 CHILDREN S SERVICES HANDBOOK APPENDIX C: LEAD SCREENING C.1 Blood Lead Screening Procedures and Follow-up Testing......................... C-338 C.2 Symptoms of Lead Poisoning...................................................
CHILDREN S SERVICES HANDBOOK APPENDIX C: LEAD SCREENING C.1 Blood Lead Screening Procedures and Follow-up Testing......................... C-338 C.2 Symptoms of Lead Poisoning...................................................
Management of Central Venous Access Devices. Blood Glucose Monitoring
 Management of Central Venous Access Devices Blood Glucose Monitoring Purpose To provide education on the standard of care regarding the use and monitoring of the Accu- Chek Blood glucose machine, including
Management of Central Venous Access Devices Blood Glucose Monitoring Purpose To provide education on the standard of care regarding the use and monitoring of the Accu- Chek Blood glucose machine, including
Newborn Screening: What s New?
 Newborn Screening: What s New? Patricia M. Jones, PhD (Department of Pathology, University of Texas Southwestern Medical Center and Children s Medical Center of Dallas, Dallas, TX) DOI: 10.1309/LMOOXWVPSM5FC3B6
Newborn Screening: What s New? Patricia M. Jones, PhD (Department of Pathology, University of Texas Southwestern Medical Center and Children s Medical Center of Dallas, Dallas, TX) DOI: 10.1309/LMOOXWVPSM5FC3B6
Newborn Metabolic Screening Programme
 Newborn Metabolic Screening Programme Annual Report January to December 2017 Released 2018 health.govt.nz Disclaimer This publication reports on information provided to the Ministry of Health by the Auckland
Newborn Metabolic Screening Programme Annual Report January to December 2017 Released 2018 health.govt.nz Disclaimer This publication reports on information provided to the Ministry of Health by the Auckland
MI Newborn Screening Program: An Overview of Follow-up & Case Management for Sickle Cell Conditions
 Michigan Department of Community Health MI Newborn Screening Program: An Overview of Follow-up & Case Management for Sickle Cell Conditions Dominic Smith, MSA - Linda Carter, BSW - Ben Frazier, BSW - Ruth
Michigan Department of Community Health MI Newborn Screening Program: An Overview of Follow-up & Case Management for Sickle Cell Conditions Dominic Smith, MSA - Linda Carter, BSW - Ben Frazier, BSW - Ruth
Screening Newborns for Congenital Disorders
 Screening Newborns for Congenital Disorders Gary L. Hoffman, BS; Ronald H. Laessig, PhD ABSTRACT The Newborn Screening Laboratory at the Wisconsin State Laboratory of Hygiene (WSLH) tests all newborn babies
Screening Newborns for Congenital Disorders Gary L. Hoffman, BS; Ronald H. Laessig, PhD ABSTRACT The Newborn Screening Laboratory at the Wisconsin State Laboratory of Hygiene (WSLH) tests all newborn babies
DR. MORLEY SLUTSKY WORK RELATED HEARING LOSS EVALUATIONS SCHEDULING: (800) FAX: (888)
 FAX: (888)") Dear Patient: DR. MORLEY SLUTSKY WORK RELATED HEARING LOSS EVALUATIONS SCHEDULING: (800) 990-7924 FAX: (888) 418-7997 WWW.HEAREXAMS.COM Here are a few things to check prior to coming to the appointment
Dear Patient: DR. MORLEY SLUTSKY WORK RELATED HEARING LOSS EVALUATIONS SCHEDULING: (800) 990-7924 FAX: (888) 418-7997 WWW.HEAREXAMS.COM Here are a few things to check prior to coming to the appointment
Congenital Hypothyroidism Referral Guidelines for Newborn Bloodspot Screening Wales
 Congenital Hypothyroidism Referral Guidelines for Newborn Bloodspot Screening Wales September 2014 Version 1 Based on the CHT initial Clinical Referral Standards and Guidelines in the UK [www.newbornbloodspot.screening.nhs.uk/cht]
Congenital Hypothyroidism Referral Guidelines for Newborn Bloodspot Screening Wales September 2014 Version 1 Based on the CHT initial Clinical Referral Standards and Guidelines in the UK [www.newbornbloodspot.screening.nhs.uk/cht]
Testing for Genetic Disorders that Cause Brain Damage
 STO-132 Testing for Genetic Disorders that Cause Brain Damage Part 1: Newborn Screening Tests Matt is watching his twins, Anna and Cody, in the newborn nursery. The nurse pokes the babies heels, collects
STO-132 Testing for Genetic Disorders that Cause Brain Damage Part 1: Newborn Screening Tests Matt is watching his twins, Anna and Cody, in the newborn nursery. The nurse pokes the babies heels, collects
Solution Title: CONGENITAL HEART DISEASE SCREENING IN THE NEWBORN
 Institutional Affiliation: ANNE ARUNDEL MEDICAL CENTER Solution Title: CONGENITAL HEART DISEASE SCREENING IN THE NEWBORN Program/Project Description Congenital heart defects in general, and newborn screening
Institutional Affiliation: ANNE ARUNDEL MEDICAL CENTER Solution Title: CONGENITAL HEART DISEASE SCREENING IN THE NEWBORN Program/Project Description Congenital heart defects in general, and newborn screening
Appendix C NEWBORN HEARING SCREENING PROJECT
 Appendix C NEWBORN HEARING SCREENING PROJECT I. WEST VIRGINIA STATE LAW All newborns born in the State of West Virginia must be screened for hearing impairment as required in WV Code 16-22A and 16-1-7,
Appendix C NEWBORN HEARING SCREENING PROJECT I. WEST VIRGINIA STATE LAW All newborns born in the State of West Virginia must be screened for hearing impairment as required in WV Code 16-22A and 16-1-7,
Improving Communication of Negative Newborn Screening Results. Whitney Thompson MPhil Amy Gaviglio MS, CGC Susan Berry MD
 Improving Communication of Negative Newborn Screening Results Whitney Thompson MPhil Amy Gaviglio MS, CGC Susan Berry MD Positive newborn blood spot results in MN Presumptive positive and borderline results
Improving Communication of Negative Newborn Screening Results Whitney Thompson MPhil Amy Gaviglio MS, CGC Susan Berry MD Positive newborn blood spot results in MN Presumptive positive and borderline results
BASE 24-HOUR URINE COLLECTION LITHOLINK CORE LAB
 CHAPTER 34. BASE 24-HOUR URINE COLLECTION LITHOLINK CORE LAB 34.1 Background Participants who are enrolled in the CKD BASE Study will collect urine over a 24-hour period at B0, W12 and W28. A 50 ml tube
CHAPTER 34. BASE 24-HOUR URINE COLLECTION LITHOLINK CORE LAB 34.1 Background Participants who are enrolled in the CKD BASE Study will collect urine over a 24-hour period at B0, W12 and W28. A 50 ml tube
Cardiology Competency Based Goals and Objectives
 Cardiology Competency Based Goals and Objectives COMPETENCY 1. Patient Care. Provide family centered patient care that is developmentally and age appropriate, compassionate, and effective for the treatment
Cardiology Competency Based Goals and Objectives COMPETENCY 1. Patient Care. Provide family centered patient care that is developmentally and age appropriate, compassionate, and effective for the treatment
Newborn Blood Spot Screening Service. Information for Users
 Newborn Blood Spot Screening Service Information for Users Newborn Blood Spot user Handbook v1 Page 1 14/07/2016 Content s Laboratory Information... 3 The Service... 3 Laboratory Mission Statement... 3
Newborn Blood Spot Screening Service Information for Users Newborn Blood Spot user Handbook v1 Page 1 14/07/2016 Content s Laboratory Information... 3 The Service... 3 Laboratory Mission Statement... 3
Congenital Heart Disease. CCCHD In WI. Critical Congenital Heart Disease. Why Screen? 4/20/2018. Early Detection = Better Outcomes
 Congenital Heart Disease A Positive Screen? What Does it Mean? A Review of Pulse Oximetry Screening for Critical Congenital Heart Disease Elizabeth Goetz MD MPH 8-10/1000 livebirths 3% of all infant mortality
Congenital Heart Disease A Positive Screen? What Does it Mean? A Review of Pulse Oximetry Screening for Critical Congenital Heart Disease Elizabeth Goetz MD MPH 8-10/1000 livebirths 3% of all infant mortality
Organic Acid Disorders
 Genetic Fact Sheets for Parents Organic Acid Disorders Screening, Technology, and Research in Genetics is a multi-state project to improve information about the financial, ethical, legal, and social issues
Genetic Fact Sheets for Parents Organic Acid Disorders Screening, Technology, and Research in Genetics is a multi-state project to improve information about the financial, ethical, legal, and social issues
HIV Testing in Children
 Module 6 HIV Testing in Children Total Module Time: 185 minutes (3 hours, 5 minutes) Learning Objectives After completing this module, participants will be able to: Understand the procedure for collecting
Module 6 HIV Testing in Children Total Module Time: 185 minutes (3 hours, 5 minutes) Learning Objectives After completing this module, participants will be able to: Understand the procedure for collecting
Northwestern University Department of Urology CONSENT FORM AND AUTHORIZATION FOR RESEARCH
 Northwestern University Department of Urology CONSENT FORM AND AUTHORIZATION FOR RESEARCH Project Title: Genetics of Prostate Cancer Principal Investigator or Faculty Advisor: William J. Catalona, M.D.
Northwestern University Department of Urology CONSENT FORM AND AUTHORIZATION FOR RESEARCH Project Title: Genetics of Prostate Cancer Principal Investigator or Faculty Advisor: William J. Catalona, M.D.