Therapeu(c Hypothermia: The Status of its Use for Hypoxic-Ischemic Encephalopathy (HIE)
|
|
|
- Leslie Hall
- 5 years ago
- Views:
Transcription
 Abbot R. Laptook, M.")

1 Therapeu(c Hypothermia: The Status of its Use for Hypoxic-Ischemic Encephalopathy (HIE) Abbot R. Laptook, M.D. Medical Director, NICU Women and Infants Hospital of RI Professor of Pediatrics Alpert Medical School of Brown University
2 Disclosure Speaker: Abbot Laptook 1. Dr. Laptook has no financial relahonships to disclose or conflicts of Interest to resolve. Any real or apparent conflicts of interest related to the content of this presentahon have been resolved. 2. This presentahon will not involve discussion of unapproved or off-label, experimental or inveshgahonal use of a drug.
3 Objec(ves Current status of hypothermia treatment for HIE NICHD workshops/cofn: research gaps Evidence for target temperature Evidence for durahon of cooling Evidence for Hme of inihahon Evidence for use in premature infants Evidence for use in mild encephalopathy
4 Components of a Hypothermia Regimen Time of inihahon DuraHon of cooling Temperature depth Rate of rewarming Method of cooling Body cooling Head cooling Phases of Hypothermia Tx InducHon Maintenance Rewarming
5 Parameters of Hypothermia Regimens Used in Clinical Trials Hypothermia Regimen GestaHonal age 36 weeks Encephalopathy IniHaHon age Mode of cooling Target Temperature DuraHon of hypothermia Rewarming rate Moderate or severe < 6 hours Body or head 33.5 o C or 34.5 o C 72 hours 0.5 o C hour
6 Clinical Trials of Therapeu(c Hypothermia for Newborn HIE Trial Year Cooled (n) Control (n) CoolCap NICHD TOBY Chinese European ICE Lancet 2005;365: NEJM 2005;353: NEJM 2009;361: J Pediatrics 2010;157: Pediatrics 2010;126:e Arch Pediatr Adol Med 2011;165:
7 Primary Outcome in Therapeu(c Hypothermia Trials in Newborns Death or disability assessed at 18 months Disability: typically severe GMFCS: Index of motor disability/cerebral palsy Developmental delay < 2 SDs Bayley Scales of Infant Development MDI Griffiths assessment Gesell Child Development Age Scale Blindness Deafness
8 Death or Disability among Infants with HIE at 18 months treated with Hypothermia or Usual Care < 6 hours Cooling Hypothermia Usual Care RR 95% CI SelecHve Head n % outcome n % outcome Body Jacobs, SE et al, Cochrane Database of SystemaHc Reviews, 2013



9 J Pediatr, 2006: 148: Research Gaps v Long term safety/efficacy v Optimizing cooling v Value in preterm infants J Pediatr, 2011: 159: v Biomarkers for prognosis v Organized dissemination v Low resource countries v Adjunctive therapies Pediatrics 2014:133: v Evidence based practice v Comprehensive care v Out-reach education v Role of research
10 NICHD Neonatal Research Network: Studies of Knowledge Gaps for Hypothermia Treatment of Encephalopathy Long term outcome following hypothermia Benefit to a lower target temperature Benefit to longer cooling Benefit for later inihahon of cooling Benefit for cooling preterm infants
11 6-7 Year Outcome Following Hypothermia for Encephalopathy: NRN Trial % Hypothermia n=97 1 o outcome* Death or IQ < 70 2 o outcomes Control n=93 RR (95%CI) p value ( ).06 Death ( ).04 Survivors IQ < ( ).51 Disabling CP ( ).28 * Primary outcome available for 190 of 208 NICHD trial enrollees (91%) Shankaran et al, NEJM 2012;366:
12 6-7 Year Outcome Following Hypothermia for Encephalopathy: TOBY Trial N, (%) Hypothermia n=163 1 o outcome* Survival with IQ 85 2 o outcomes Control n=162 RR (95%CI) p value 75/145 (52) 52/132 (39) 1.31 ( ).04 Death 47/163 (29) 79/162 (30).95 ( ).81 Survivors IQ 85 75/98 (77) 52/83 (63) 1.22 ( ).05 Disabling CP 21/98 (21) 31/86 (36).59 ( ).03 * IQ scores could not be determined: Hypothermia group: 18 Control group: 30 Azzopardi D et al, NEJM 2014:371:
13 Evidence for a Target Temperature of 33.5 o C
14 Target Temperature: Neuroprotection in Newborn/Fetal Animals with Delayed Cooling Model Age Temperature Site Temperature Decrement Δ T Reference Rat 7d Rectal o C 7 o C Peds Res 2002;51:354 Pigs 48hrs Tympanic o C 4 o C Peds Res 1997;41:505 Pigs 7d Rectal o C 2.5 o C Peds Res 1997;42:17 Fetal lambs d Extra-dural o C 6.7 o C JCI 1997;99:248 Neuroprotection: associated with a spectrum of in temperature
15 Target Temperature: Clinical Trials Should it be: An absolute temperature Change in temperature from baseline Trade off for the target temperature: Extent of neuroprotection vs harm of a lower temperature
16 Hypothermia Treatment in Newborns with Encephalopathy: Pilot Trials Gunn et al 1 Head cooling + minimal body cooling (72 hrs) Randomization T: 37.0 o C (n=10), 36.3±.2 o C (n=6), 35.7±.2 o C (n=6) Thoresen et al 2 Head cooling + body cooling (72 hrs) T: o C (n=6) Body cooling (72 hrs), T: o C (n=3) Shankaran et al 3 Body cooling (72 hrs) Randomization T: 37.0 o C (n=10), 34.5 o C (n=9) Conclusions: modest cooling is feasible and safe 1 Pediatrics 1998; 102: Pediatrics 2000; 106:92-99 Pediatrics 2002; 110:

17 Use of Lower Temperatures for Therapeutic Hypothermia: Feasibility Retrospective Safety assessment v Control group, n=11 v o C, n=10 v o C, n=18 No differences in safety endpoints Compagnoni G et al, Neonatology 2008; 93:230
18 Evidence for 72 hour duration of Cooling
19 Duration of Hypothermia: Neuroprotection in Adult/Newborn/Fetal Animals with Cooling Adult rodents (gerbils, rats) 1-3 Ischemia models (global or focal) duration of cooling (immediate or delayed) brain injury Rat pups 4 Hypoxia-ischemia model duration of cooling (immediate) brain injury Fetal sheep 5 Ischemia model (global) Epileptiform activity triggered with stopping cooling at 48 hrs compared to 72 hrs. 1 Carroll et al, Met Brain Dis 1992;7:45 2 Colbourne et al, Brain Res 1994; 654:265 3 Yanamoto et al, Brain Res 1996;718:207 4 Sirimanne et al, Ped Res 199 6; 39: Gunn et al, JCI 1997; 99:

20 Temporal Profile of the Mechanisms of Brain Injury Ferriero DM, NEJM 2004;351:1985
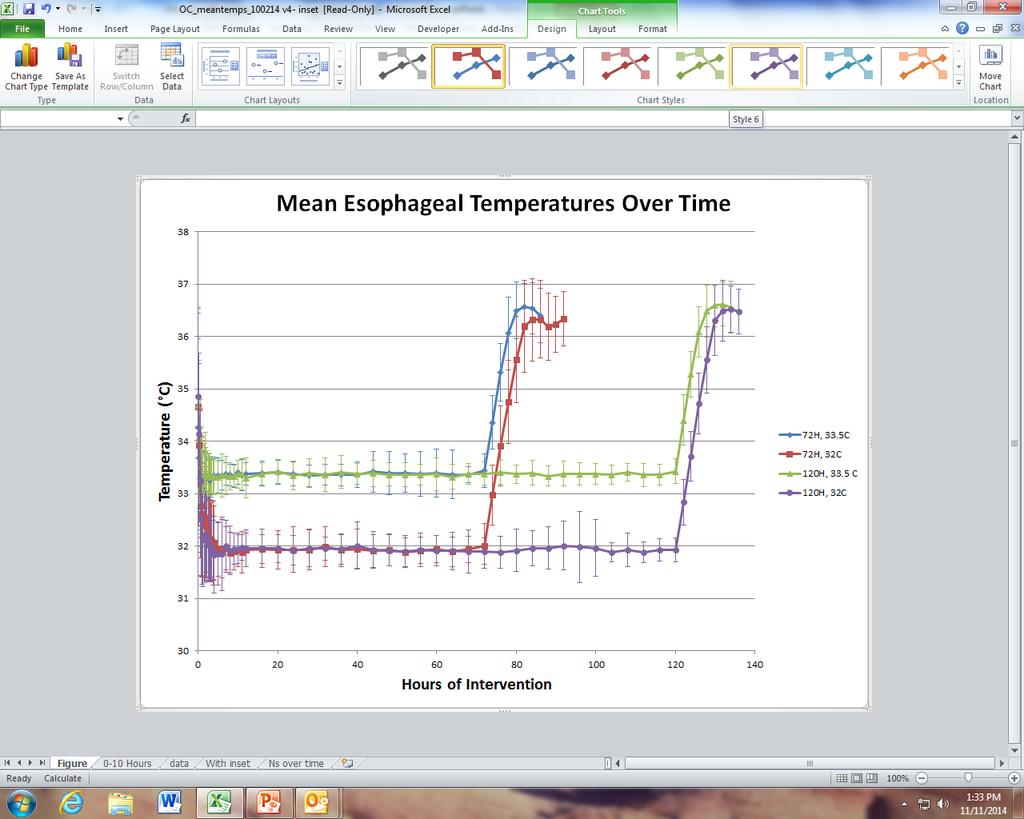
21 Refining Hypothermia: Op(mizing Cooling RCT (NCT ) P: Newborn infants with moderate or severe HIE at < 6 hours of age I: Cooling to 32 o C or cooling for 120 hours C: Cooling to 33.5 o C or cooling for 72 hours O: Death or disability T: months Factorial 2 x 2 design (assumes no interachon) 33.5 o C 72 hours 32.0 o C 72 hours Dura(on(n=363) 72 hr 33.5 o C 120 hours 32.0 o C 120 hours 120 hr Depth (n=363) 33.5 o C 32.0 o C
22
23 Trial Closure v Trial was stopped amer enrollment of 364 infants v Death up to 18 months of age 33.5 C for 72 h: 9% 32.0 C for 72 h: 18% 33.5 C for 120 h: 19% 32.0 C for 120 h: 19% v CondiHonal fuhlity analysis: probability of detechng a significant treatment benefit of longer or deeper cooling for inhospital mortality was < 2% v An interachon was present (p=.05)
24 Outcome of Deeper Cooling: 33.5 o C vs 32.0 o C Dura(on 72 hrs 72 hrs RR ǂ 95% CI Depth 33.5 o C 32.0 o C n Death or disability* 29% 35% Death 9% 18% Disability* 23% 20% Disabling Cerebral Palsy 16% 14% * Disability was moderate or severe in extent ǂ adjusted for level of encephalopathy and center Shankaran S, PAS 2016
25 Outcome of Longer Cooling: 72 vs 120 hours Dura(on 72 hrs 120 hrs RR ǂ 95% CI Depth 33.5 o C 33.5 o C n Death or disability* 29% 34% Death 9% 19% Disability* 23% 19% Disabling Cerebral Palsy 16% 12% * Disability was moderate or severe in extent ǂ adjusted for level of encephalopathy and center Shankaran S, PAS 2016
26 Outcome of Longer and Deeper Cooling: 33.5 o C/72 hrs vs 32.0 o C/120 hrs Dura(on 72 hrs 120 hrs RR ǂ 95% CI Depth 33.5 o C 32.0 o C n Death or disability* 29% 28% Death 9% 19% Disability* 23% 11% Disabling Cerebral Palsy 16% 8% * Disability was moderate or severe in extent ǂ adjusted for level of encephalopathy and center Shankaran S, PAS 2016

27 Lessons From the Op(mizing Cooling Trial (JAMA 2014; 312: ) Among term infants with HIE, longer cooling was not superior to usual durahon and deeper cooling was not superior to usual depth of cooling Avoid drims in adherence to established protocols based on randomized trials Whole body cooling regimens: Target Tes of 33.5 o C for 72 hours
28 Evidence for Cooling beyond 6 hours of age
29 Time of Ini(a(on of Hypothermia: Dura(on of Therapeu(c Window JCI 1997:99;248 Ped 1998:102;1098 Ped Res 1999:46;274
30 Hypothermia Ini(ated at 8.5 hours ajer Brain Ischemia in Fetal Sheep (Late) Sham cooling: n = 13 Cooling: n = 5 IntervenHon for 72 hr Outcome at 5 d Neuronal loss score, p=.11, NS 90.3±4.5% vs 82.0±9.0% p=.03 p=.06 Gunn AJ et al, Pediatr Res 1999; 46(3):
31 Implementa(on of Therapeu(c Hypothermia in the UK DistribuHon of cooling centers in the UK PLoS One 2012;7;e38504 TOBY registry, Dec 2006-July 2011, n= hrs: 9-10% > 12hrs: 2.2%
32 Ra(onale to Study Ini(a(on of Hypothermia Ajer 6 hours of Age Available data: Does not exclude the possibility of benefit when hypothermia is inihated amer 6 hours Clinical rahonale: Timing of fetal hypoxia-ischemia may not be accurate Some infants manifest symptoms at > 6 hours Geographic constraints PracHce creep in the absence of evidence
33 The Late Hypothermia RCT (NCT ) P: Infants 36 wks with moderate or severe HIE who are between 6-24 hours of age I: Cooling to 33.5 o C (Tes) for 96 hours C: Maintenance of Tes at 37.0 o C ( o C) O: Death or disability T: months Laptook et al, PAS 2017
34 Sample Size Considera(ons Frequen6st analysis: probability of the observed data or more extreme data if the null hypothesis is true Primary outcome: 60%, 10% absolute reduchon (17% RR) 392 infants per group Bayesian analysis: probability that the hypothesis is true based on the observed data A formal method to assess the range of treatment effects compahble with the best available evidence and eshmate the probability of a benefit Recommended for trials with limited sample size Provides useful data even when a definihve result is unlikely
35 Sample Size and Pre-specified Analyses Bayesian analysis: pre-specified Sample size, N=168, pre-defined Largest feasible number of infants that could be studied EsHmated from the NRN 1 st hypothermia trial 1 and reports 2 of progression from stage 1 to 2 or 3 Primary analyses adjusted for level of encephalopathy and age at randomizahon P values: provided for descriphve stahshcs and components of the primary outcome 1 NEJM 2005;353: Pediatrics2003;111:351
 Area under the curve which lies < RR 1.")
36 Bayesian Analysis Prior distribu6on Observed data Posterior distribu6on: Point eshmate 95% credible intervals Probability of posterior treatment benefit (P-TB) Area under the curve which lies < RR 1.0
37 Posterior Probability of Reduced Death or Disability with Late Hypothermia: Neutral Prior Death or mod/sev disability Cooled (n=78) Non-cooled (n=79) Neutral prior n % n % arr, 95% credible intervals ( ) P-TB RR< arr: Adjusted for level of encephalopathy and age at randomizahon
38 Posterior Probability of Treatment Benefit (P-TB): Secondary Outcomes using a Neutral Prior Cooled (n=78) Non-cooled (n=79) Neutral prior n % n % arr, 95% credible intervals P-TB RR<1.0 Death ( ) Severe disability ( ) Moderate disability arr: Adjusted for level of encephalopathy and age at randomizahon
39 Other Outcomes Among Survivors Cooled (n=69) Non-cooled (n=70) p value n X±sd or % n X±sd, or % Age at FU ± ± 3.83 Bayley cognihve < X±sd ± ± Cerebral Palsy Moderate Severe
40 Conclusions: Late Hypothermia Trial Bayesian analysis suggests a possible treatment benefit but is not conclusive 76% likelihood of reduced death or disability 3 in 4 chance of treatment benefit compared to the neutral prior (2 in 4 chance) What is the minimum probability of benefit that jushfies a treatment? Outcome involved PotenHal harm The results should not delay efforts to recognize HIE early and inihate hypothermia within 6 h of birth
41 Evidence for Cooling Infants < 36 Weeks GestaHon
42 Therapeu(c Hypothermia for Infants < 36 weeks Gesta(on Limited data on efficacy and safety: RCT 1,2 : 7 infants with outcome (all weeks) Registry Data 3,4 : VON and TOBY 3-6% of infants being cooled: no outcome data Single center 5 : wks (n=31) vs 39.3±.8 wks (n=32) RetrospecHve, all cooled, PT deaths/complicahons > term No follow-up Single center 6 : wks (n=31), no comparison group 17% IVH, FU (75%), death or disability 65% 1 Pediatr Neurol 2005;32:11 2 Arch Pediatr Adolesc Med, 2011;165:692 3 PLOS One, 2012;e PAS, 2013, abstract J Peds 2017; 183: Herrera PAS 2017
43 Preterm Hypothermia RCT (NCT ) P: Infants wks with moderate or severe HIE who are between 6-24 hours of age I: Cooling to 33.5 o C (Tes) for 72 hours C: Maintenance of Tes at 37.0 o C ( o C) O: Death or disability T: months Sample size: 168, current enrollment: 63 FrequenHst and Bayesian analyses


44 Preterm Hypothermia Trial v Safety and efficacy
45 Should Infants with Mild HIE Receive ExisHng data: Hypothermia Treatment? Adverse outcomes among some infants not meehng cooling criteria 1 Center reports: Similar frequency of MRI abnormalihes among mild and moderate HIE 2,3 California: 50% of mild HIE are cooled (CPQCC & CPTS) 4 5 yr outcome: FSIQ normal but.5 SD < controls 5 Data quality All retrospechve reports No criteria to diagnose mild encephalopathy No follow-up except for reference 5 No randomized controlled trials 1 J Peds 2013; 162:35-41, 2 Am J Perinatol 2016; 33: , 3 J Peds 2017 epub 4 J Peds 2014; 165: , 5 Pediatrics 2016; 138: e
46 Prospec(ve Research on Infants with Mild Encephalopathy: The PRIME Study Hypothesis: 20% of infants evaluated at < 6 hours for hypothermia with exam abnormalihes but not meehng criteria for treatment will have neurological dysfunchon ObservaHonal cohort 6 centers: McGill University, WIH/Brown, UTSW, WSU, Mahidol University, Imperial College Primary outcome: Abnormality of any of the following: MRI, aeeg or neurological exam at discharge Secondary outcome: Neurodevelopmental outcome at 18 months Sample size: 54 Santa Anna, G et al, PAS 2016
47 PRIME Study: Short Term Outcomes Neurodevelopment at 18 months in progress Outcome Results (n=54) Abnormality of aeeg, MRI or discharge exam 28 (54%) Abnormal aeeg 4 (7%) Abnormal MRI 9 (17%) Abnormal discharge exam 22 (41%)
48 Clinical Implica(ons: Use an Evidenced Based Approach to Therapeu(c Hypothermia Structured program Establish screening guidelines for pahent criteria Train transport teams RecogniHon of encephalopathy Temperature control on transport Cooling regimen Start at < 6 hours; consider late cooling Cool for 72 hours Use a core temperature of 33.5 o C for whole body cooling Use a controlled rate of increasing temperature (0.5 o C/hour) Ensure follow-up Monitor for late complicahons (eg, subcutaneous fat necrosis) Program to assess neurodevelopment
49 Thank You Any questions?
TOO COOL OR NOT TOO COOL- THERAPEUTIC HYPOTHERMIA IN THE ICU SCCM TX 2017 TED WU MD PEDIATRIC CRITICAL CARE UNIVERSITY OF TEXAS HEALTH SAN ANTONIO
 TOO COOL OR NOT TOO COOL- THERAPEUTIC HYPOTHERMIA IN THE ICU SCCM TX 2017 TED WU MD PEDIATRIC CRITICAL CARE UNIVERSITY OF TEXAS HEALTH SAN ANTONIO DISCLOSURE I have no relationships with commercial companies
TOO COOL OR NOT TOO COOL- THERAPEUTIC HYPOTHERMIA IN THE ICU SCCM TX 2017 TED WU MD PEDIATRIC CRITICAL CARE UNIVERSITY OF TEXAS HEALTH SAN ANTONIO DISCLOSURE I have no relationships with commercial companies
Queen Charlotte Hospital
 Queen Charlotte Hospital Neuroprotection for neonatal encephalopathy Neonatal encephalopathy accounts for 1 million deaths worldwide and even greater numbers of disabled survivors In countries with
Queen Charlotte Hospital Neuroprotection for neonatal encephalopathy Neonatal encephalopathy accounts for 1 million deaths worldwide and even greater numbers of disabled survivors In countries with
Objectives. Birth Depression Management. Birth Depression Terms
 Objectives Birth Depression Management Regional Perinatal Outreach Program 2016 Understand the terms and the clinical characteristics of birth depression. Be familiar with the evidence behind therapeutic
Objectives Birth Depression Management Regional Perinatal Outreach Program 2016 Understand the terms and the clinical characteristics of birth depression. Be familiar with the evidence behind therapeutic
COOLING FOR HYPOXIC ISCHEMIC ENCEPHALOPATHY
 COOLING FOR HYPOXIC ISCHEMIC ENCEPHALOPATHY Roger F. Soll H. Wallace Professor of Neonatology University of Vermont 19 th International Symposium on Neonatology Sao Paulo, Brazil DISCLOSURE Roger F. Soll
COOLING FOR HYPOXIC ISCHEMIC ENCEPHALOPATHY Roger F. Soll H. Wallace Professor of Neonatology University of Vermont 19 th International Symposium on Neonatology Sao Paulo, Brazil DISCLOSURE Roger F. Soll
Neonatal Therapeutic Hypothermia. A Wasunna Professor of Neonatal Medicine and Pediatrics School of Medicine, University of Nairobi
 Neonatal Therapeutic Hypothermia A Wasunna Professor of Neonatal Medicine and Pediatrics School of Medicine, University of Nairobi Definition of Perinatal Asphyxia *No agreed universal definition ACOG/AAP
Neonatal Therapeutic Hypothermia A Wasunna Professor of Neonatal Medicine and Pediatrics School of Medicine, University of Nairobi Definition of Perinatal Asphyxia *No agreed universal definition ACOG/AAP
Disclosures. Objectives. Definition: HIE. HIE: Incidence. Impact 9/10/2018. Hypoxic Ischemic Encephalopathy in the Neonate
 Disclosures Hypoxic Ischemic Encephalopathy in the Neonate No relevant financial relationships or conflicts of interest to disclose Franscesca Miquel-Verges MD 2018 Review therapies currently under research
Disclosures Hypoxic Ischemic Encephalopathy in the Neonate No relevant financial relationships or conflicts of interest to disclose Franscesca Miquel-Verges MD 2018 Review therapies currently under research
No social problems noted No past med hx Mother had spontaneous rupture of fetal membranes SB born on Needed to be resuscitated at birth
 No social problems noted No past med hx Mother had spontaneous rupture of fetal membranes SB born on 9-16-2011 Needed to be resuscitated at birth (included assisted vent) Had generalized edema and possible
No social problems noted No past med hx Mother had spontaneous rupture of fetal membranes SB born on 9-16-2011 Needed to be resuscitated at birth (included assisted vent) Had generalized edema and possible
Perinatal asphyxia: Pathophysiology and therapy
 Perinatal asphyxia: Pathophysiology and therapy Peter Davis Melbourne Australia With thanks to Dr Sue Jacobs Moderate or severe HIE Complicates ~1/1000 term live births: Mortality: >25% Major neurological
Perinatal asphyxia: Pathophysiology and therapy Peter Davis Melbourne Australia With thanks to Dr Sue Jacobs Moderate or severe HIE Complicates ~1/1000 term live births: Mortality: >25% Major neurological
Predicting Outcomes in HIE. Naaz Merchant Consultant Neonatologist Beds & Herts Meeting 17/03/2016
 Predicting Outcomes in HIE Naaz Merchant Consultant Neonatologist Beds & Herts Meeting 17/03/2016 Interactive please! Case 1 Term, 3.5 kg Antenatal: Breech Labour/Delivery: Em CS failure to progress, mec
Predicting Outcomes in HIE Naaz Merchant Consultant Neonatologist Beds & Herts Meeting 17/03/2016 Interactive please! Case 1 Term, 3.5 kg Antenatal: Breech Labour/Delivery: Em CS failure to progress, mec
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE INTERVENTIONAL PROCEDURES PROGRAMME Interventional procedure overview of therapeutic hypothermia with intracorporeal temperature monitoring for hypoxic
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE INTERVENTIONAL PROCEDURES PROGRAMME Interventional procedure overview of therapeutic hypothermia with intracorporeal temperature monitoring for hypoxic
PEER REVIEW HISTORY ARTICLE DETAILS TITLE (PROVISIONAL)
") PEER REVIEW HISTORY BMJ Paediatrics Open publishes all reviews undertaken for accepted manuscripts. Reviewers are asked to complete a checklist review form and are provided with free text boxes to elaborate
PEER REVIEW HISTORY BMJ Paediatrics Open publishes all reviews undertaken for accepted manuscripts. Reviewers are asked to complete a checklist review form and are provided with free text boxes to elaborate
Too or Too Cold. Too Cold...Too Hot...Just Right. Temperature Control in Newborns. Temperature Balance in Newborns. Basics in the Delivery Room
 Too or Too Cold Neonatology Rediscovers Temperature Control Advances and Controversies in Clinical Pediatrics May 31, 2007 Terri A. Slagle Neonatology, CPMC Too Cold...Too Hot...Just Right Too Cold = Issues
Too or Too Cold Neonatology Rediscovers Temperature Control Advances and Controversies in Clinical Pediatrics May 31, 2007 Terri A. Slagle Neonatology, CPMC Too Cold...Too Hot...Just Right Too Cold = Issues
Principal Investigator: Abbot Laptook. Final July 31, Version: 1.0
 Evaluation of Systemic Hypothermia Initiated After 6 Hours of Age in Infants 36 Weeks Gestation with Hypoxic-Ischemic Encephalopathy: A Bayesian Evaluation (Late Hypothermia Study for HIE) Principal Investigator:
Evaluation of Systemic Hypothermia Initiated After 6 Hours of Age in Infants 36 Weeks Gestation with Hypoxic-Ischemic Encephalopathy: A Bayesian Evaluation (Late Hypothermia Study for HIE) Principal Investigator:
Hazards and Benefits of Postnatal Steroids. David J. Burchfield, MD Professor and Chief, Neonatology University of Florida
 Hazards and Benefits of Postnatal Steroids David J. Burchfield, MD Professor and Chief, Neonatology University of Florida Disclosures I have no financial affiliations or relationships to disclose. I will
Hazards and Benefits of Postnatal Steroids David J. Burchfield, MD Professor and Chief, Neonatology University of Florida Disclosures I have no financial affiliations or relationships to disclose. I will
Insults to the Developing Brain & Effect on Neurodevelopmental Outcomes
 Insults to the Developing Brain & Effect on Neurodevelopmental Outcomes Ira Adams-Chapman, MD Assistant Professor of Pediatrics Director, Developmental Progress Clinic Emory University School of Medicine
Insults to the Developing Brain & Effect on Neurodevelopmental Outcomes Ira Adams-Chapman, MD Assistant Professor of Pediatrics Director, Developmental Progress Clinic Emory University School of Medicine
Rango de saturacion de oxigeno: Cual es la evidencia?
 Rango de saturacion de oxigeno: Cual es la evidencia? Wally Carlo, M.D. University of Alabama at Birmingham Department of Pediatrics Division of Neonatology wcarlo@peds.uab.edu 1 2 Stevie Wonder 4 Objectives
Rango de saturacion de oxigeno: Cual es la evidencia? Wally Carlo, M.D. University of Alabama at Birmingham Department of Pediatrics Division of Neonatology wcarlo@peds.uab.edu 1 2 Stevie Wonder 4 Objectives
Neurodevelopmental Follow Up After Therapeutic Hypothermia for Perinatal Asphyxia
 ORIGINAL PAPER doi: 10.5455/medarh.2015.69.362-366 Med Arh. 2015 Dec; 69(6): 362-366 Received: August 25th 2015 Accepted: November 05th 2015 2015 Smail Zubcevic, Suada Heljic, Feriha Catibusic, Sajra Uzicanin,
ORIGINAL PAPER doi: 10.5455/medarh.2015.69.362-366 Med Arh. 2015 Dec; 69(6): 362-366 Received: August 25th 2015 Accepted: November 05th 2015 2015 Smail Zubcevic, Suada Heljic, Feriha Catibusic, Sajra Uzicanin,
From NICU to the Community. General Practitioners Study Day October 18 th 2014
 From NICU to the Community General Practitioners Study Day October 18 th 2014 News in Neonatology Therapeutic hypothermia CPAP vs ventilation Palivizumab RSV prophylaxis Feeding post discharge Universal
From NICU to the Community General Practitioners Study Day October 18 th 2014 News in Neonatology Therapeutic hypothermia CPAP vs ventilation Palivizumab RSV prophylaxis Feeding post discharge Universal
No Disclosures or Conflicts of Interest. Objectives. Overview. Therapeutic Hypothermia and other Potential Neuroprotective Strategies for HIE
 Therapeutic Hypothermia and other Potential Neuroprotective Strategies for HIE Alexis Davis, M.D. Medical Director, Neonatal Intensive Care Unit Lucile Packard Children s Hospital Clinical Associate Professor
Therapeutic Hypothermia and other Potential Neuroprotective Strategies for HIE Alexis Davis, M.D. Medical Director, Neonatal Intensive Care Unit Lucile Packard Children s Hospital Clinical Associate Professor
Prematurity as a Risk Factor for ASD. Disclaimer
 Prematurity as a Risk Factor for ASD Angela M. Montgomery, MD, MSEd Assistant Professor of Pediatrics (Neonatology) Director, Yale NICU GRAD Program Suzanne L. Macari, PhD Research Scientist, Child Study
Prematurity as a Risk Factor for ASD Angela M. Montgomery, MD, MSEd Assistant Professor of Pediatrics (Neonatology) Director, Yale NICU GRAD Program Suzanne L. Macari, PhD Research Scientist, Child Study
Correlation of Neurodevelopmental Outcome and brain MRI/EEG findings in term HIE infants
 Correlation of Neurodevelopmental Outcome and brain MRI/EEG findings in term HIE infants Ajou University School of Medicine Department of Pediatrics Moon Sung Park M.D. Hee Cheol Jo, M.D., Jang Hoon Lee,
Correlation of Neurodevelopmental Outcome and brain MRI/EEG findings in term HIE infants Ajou University School of Medicine Department of Pediatrics Moon Sung Park M.D. Hee Cheol Jo, M.D., Jang Hoon Lee,
Newborn Hypoxic Ischemic Brain Injury. Hisham Dahmoush, MBBCh FRCR Lucile Packard Children s Hospital at Stanford
 Newborn Hypoxic Ischemic Brain Injury Hisham Dahmoush, MBBCh FRCR Lucile Packard Children s Hospital at Stanford NO DISCLOSURES INTRODUCTION Neonatal hypoxic-ischemic encephalopathy (HIE) is a major cause
Newborn Hypoxic Ischemic Brain Injury Hisham Dahmoush, MBBCh FRCR Lucile Packard Children s Hospital at Stanford NO DISCLOSURES INTRODUCTION Neonatal hypoxic-ischemic encephalopathy (HIE) is a major cause
When? Incidence of neonatal seizures in a NICU population The incidence of seizures is higher in the neonatal period than in any other age group.
 Incidence of neonatal seizures in a NICU population The incidence of seizures is higher in the neonatal period than in any other age group. Standard EEG 2,3% 8.6% Standard EEG + aeeg Scher MS et al; Pediatrics
Incidence of neonatal seizures in a NICU population The incidence of seizures is higher in the neonatal period than in any other age group. Standard EEG 2,3% 8.6% Standard EEG + aeeg Scher MS et al; Pediatrics
Moving beyond therapeutic hypothermia
 Moving beyond therapeutic hypothermia #swaps2017 #foamneo @elisasmit_neo Elisa Smit, MD MRCPCH Consultant Neonatologist Cardiff and Vale University Health Board Honorary Researcher Neonatal Neuroscience
Moving beyond therapeutic hypothermia #swaps2017 #foamneo @elisasmit_neo Elisa Smit, MD MRCPCH Consultant Neonatologist Cardiff and Vale University Health Board Honorary Researcher Neonatal Neuroscience
Too Cool? Hypoxic Ischemic Encephalopathy and Therapeutic Hypothermia. Lauren Sacco DNP, ARNP, NNP-BC
 Too Cool? Hypoxic Ischemic Encephalopathy and Therapeutic Hypothermia Lauren Sacco DNP, ARNP, NNP-BC Pathophysiology of HIE Occurs in two energy failure phases: First phase happens during the initial insult
Too Cool? Hypoxic Ischemic Encephalopathy and Therapeutic Hypothermia Lauren Sacco DNP, ARNP, NNP-BC Pathophysiology of HIE Occurs in two energy failure phases: First phase happens during the initial insult
Noah Hillman M.D. IPOKRaTES Conference Guadalajaira, Mexico August 23, 2018
 Postnatal Steroids Use for Bronchopulmonary Dysplasia in 2018 + = Noah Hillman M.D. IPOKRaTES Conference Guadalajaira, Mexico August 23, 2018 AAP Policy Statement - 2002 This statement is intended for
Postnatal Steroids Use for Bronchopulmonary Dysplasia in 2018 + = Noah Hillman M.D. IPOKRaTES Conference Guadalajaira, Mexico August 23, 2018 AAP Policy Statement - 2002 This statement is intended for
University of Bristol - Explore Bristol Research
 Elstad, M., Liu, X., & Thoresen, M. (2016). Heart rate response to therapeutic hypothermia in infants with hypoxic-ischaemic encephalopathy. Resuscitation, 106, 53-57. DOI: 10.1016/j.resuscitation.2016.06.023
Elstad, M., Liu, X., & Thoresen, M. (2016). Heart rate response to therapeutic hypothermia in infants with hypoxic-ischaemic encephalopathy. Resuscitation, 106, 53-57. DOI: 10.1016/j.resuscitation.2016.06.023
Hypothermia: Neuroprotective Treatment of Hypoxic-Ischemic Encephalopathy. Serious perinatal asphyxia. Therapeutic hypothermia
 Therapeutic hypothermia Hypothermia: Neuroprotective Treatment of Hypoxic-Ischemic Encephalopathy Background of hypothermia Clinical application Floris Groenendaal Department of Neonatology Complications
Therapeutic hypothermia Hypothermia: Neuroprotective Treatment of Hypoxic-Ischemic Encephalopathy Background of hypothermia Clinical application Floris Groenendaal Department of Neonatology Complications
Review Article Current Controversies in Newer Therapies to Treat Birth Asphyxia
 International Pediatrics Volume 2011, Article ID 848413, 5 pages doi:10.1155/2011/848413 Review Article Current Controversies in Newer Therapies to Treat Birth Asphyxia Pia Wintermark Division of Newborn
International Pediatrics Volume 2011, Article ID 848413, 5 pages doi:10.1155/2011/848413 Review Article Current Controversies in Newer Therapies to Treat Birth Asphyxia Pia Wintermark Division of Newborn
NEONATOLOGY GIVES BACK WHAT OBSTETRICS TAKE AWAY. It is well-known that hypoxic and/or ischemic events during labor and
 NEONATOLOGY GIVES BACK WHAT OBSTETRICS TAKE AWAY I. Introduction It is well-known that hypoxic and/or ischemic events during labor and delivery can cause injury to the baby's brain. The mechanisms at first
NEONATOLOGY GIVES BACK WHAT OBSTETRICS TAKE AWAY I. Introduction It is well-known that hypoxic and/or ischemic events during labor and delivery can cause injury to the baby's brain. The mechanisms at first
Initiation of passive cooling at referring centre is most predictive of achieving early therapeutic hypothermia in asphyxiated newborns
 Paediatrics & Child Health, 2017, 264 268 doi: 10.1093/pch/pxx062 Original Article Advance Access publication 23 May 2017 Original Article Initiation of passive cooling at referring centre is most predictive
Paediatrics & Child Health, 2017, 264 268 doi: 10.1093/pch/pxx062 Original Article Advance Access publication 23 May 2017 Original Article Initiation of passive cooling at referring centre is most predictive
Dysphagia in Encephalopathic Neonates Treated with Hypothermia
 Dysphagia in Encephalopathic Neonates Treated with Hypothermia A thesis submitted to the University of Arizona College of Medicine -- Phoenix in partial fulfillment of the requirements for the degree of
Dysphagia in Encephalopathic Neonates Treated with Hypothermia A thesis submitted to the University of Arizona College of Medicine -- Phoenix in partial fulfillment of the requirements for the degree of
Prognosis in. Encephalopathy. Hypoxic-Ischemic. Özge Aydemİr MD
 Prognosis in Hypoxic-Ischemic Encephalopathy Özge Aydemİr MD Major problems we have to face while caring infants with HIE are; Øto provide families with reliable information about outcome. Øto decide how
Prognosis in Hypoxic-Ischemic Encephalopathy Özge Aydemİr MD Major problems we have to face while caring infants with HIE are; Øto provide families with reliable information about outcome. Øto decide how
BMC Pediatrics. Open Access. Abstract
 BMC Pediatrics BioMed Central Research article A systematic review of cooling for neuroprotection in neonates with hypoxic ischemic encephalopathy are we there yet? Sven M Schulzke* 1,2, Shripada Rao 1
BMC Pediatrics BioMed Central Research article A systematic review of cooling for neuroprotection in neonates with hypoxic ischemic encephalopathy are we there yet? Sven M Schulzke* 1,2, Shripada Rao 1
Number: Policy *Please see amendment for Pennsylvania Medicaid at the end of this CPB.
 Number: 0812 Policy *Please see amendment for Pennsylvania Medicaid at the end of this CPB. Aetna considers total body cooling (TBC, also known as whole body cooling) and/or selective head cooling (SHC)
Number: 0812 Policy *Please see amendment for Pennsylvania Medicaid at the end of this CPB. Aetna considers total body cooling (TBC, also known as whole body cooling) and/or selective head cooling (SHC)
Neuroimaging updates on neonatal hypoxic ischemic injury and hypothermia
 Neuroimaging updates on neonatal hypoxic ischemic injury and hypothermia Fabio Triulzi Neuroradiology Dept. Cà Granda Foundation Ospedale Maggiore Policlinico Università degli Studi, Milan ITALY Term Neonate
Neuroimaging updates on neonatal hypoxic ischemic injury and hypothermia Fabio Triulzi Neuroradiology Dept. Cà Granda Foundation Ospedale Maggiore Policlinico Università degli Studi, Milan ITALY Term Neonate
Wales Neonatal Network Guideline Guideline for the management of Infants with Moderate or Severe Perinatal Asphyxia requiring cooling.
 Guideline for the management of Infants with Moderate or Severe Perinatal Asphyxia requiring cooling. (Including flowchart for infants fulfilling A criteria or A and B criteria only) Perinatal asphyxia
Guideline for the management of Infants with Moderate or Severe Perinatal Asphyxia requiring cooling. (Including flowchart for infants fulfilling A criteria or A and B criteria only) Perinatal asphyxia
Early Accurate Diagnosis & Early Intervention for Cerebral Palsy INTERNATIONAL RECOMMENDATIONS
 Early Accurate Diagnosis & Early Intervention for Cerebral Palsy INTERNATIONAL RECOMMENDATIONS Professor Iona Novak Cerebral Palsy Alliance Australia Neuroplasticity is fundamentally why we believe in
Early Accurate Diagnosis & Early Intervention for Cerebral Palsy INTERNATIONAL RECOMMENDATIONS Professor Iona Novak Cerebral Palsy Alliance Australia Neuroplasticity is fundamentally why we believe in
Is It Possible to Prevent Necrotizing Enterocolitis?
 Is It Possible to Prevent Necrotizing Enterocolitis? Ravi Mangal Patel, MD MSc Associate Professor of Pediatrics Emory University School of Medicine, Atlanta, GA, USA @institutopgg @ravimpatelmd Disclosures
Is It Possible to Prevent Necrotizing Enterocolitis? Ravi Mangal Patel, MD MSc Associate Professor of Pediatrics Emory University School of Medicine, Atlanta, GA, USA @institutopgg @ravimpatelmd Disclosures
Therapeutic hypothermia for hypoxic ischemic encephalopathy using low-technology methods: A systematic review and meta-analysis
 Therapeutic hypothermia for hypoxic ischemic encephalopathy using low-technology methods: A systematic review and meta-analysis Rossouw G 1, Irlam J 2, Horn AR 1 1)Division of Neonatal Medicine, Department
Therapeutic hypothermia for hypoxic ischemic encephalopathy using low-technology methods: A systematic review and meta-analysis Rossouw G 1, Irlam J 2, Horn AR 1 1)Division of Neonatal Medicine, Department
Predicting outcome using neonatal MRI in preterm infants. Manon Benders, neonatologist. Summer Conference on Neonatology in Provence
 Predicting outcome using neonatal MRI in preterm infants Manon Benders, neonatologist Summer Conference on Neonatology in Provence Avignon, France, 6 th - 9 th September 2017 the human brain the third
Predicting outcome using neonatal MRI in preterm infants Manon Benders, neonatologist Summer Conference on Neonatology in Provence Avignon, France, 6 th - 9 th September 2017 the human brain the third
Serum Lactate, Brain Magnetic Resonance Imaging and Outcome of Neonatal Hypoxic Ischemic Encephalopathy after Therapeutic Hypothermia
 Pediatrics and Neonatology (2016) 57, 35e40 Available online at www.sciencedirect.com ScienceDirect journal homepage: http://www.pediatr-neonatol.com ORIGINAL ARTICLE Serum Lactate, Brain Magnetic Resonance
Pediatrics and Neonatology (2016) 57, 35e40 Available online at www.sciencedirect.com ScienceDirect journal homepage: http://www.pediatr-neonatol.com ORIGINAL ARTICLE Serum Lactate, Brain Magnetic Resonance
REVIEW ARTICLE. Mohamed A. Tagin, MB BCh; Christy G. Woolcott, PhD; Michael J. Vincer, MD; Robin K. Whyte, MB; Dora A. Stinson, MD
 REVIEW ARTICLE ONLINE FIRST JOURNAL CLUB for Neonatal Hypoxic Ischemic Encephalopathy Scan for Author Audio Interview An Updated Systematic Review and Meta-analysis Mohamed A. Tagin, MB BCh; Christy G.
REVIEW ARTICLE ONLINE FIRST JOURNAL CLUB for Neonatal Hypoxic Ischemic Encephalopathy Scan for Author Audio Interview An Updated Systematic Review and Meta-analysis Mohamed A. Tagin, MB BCh; Christy G.
be able to identify newer adjunct therapies for management of infants with HIE.
 A7a Beyond Hypothermia: Emerging Therapies for Neuroprotection Rajan Wadhawan, MD, MMM, CPE, FAAP Chief of Neonatology Walt Disney Pavilion, Florida Hospital for Children Orlando, FL The speaker has signed
A7a Beyond Hypothermia: Emerging Therapies for Neuroprotection Rajan Wadhawan, MD, MMM, CPE, FAAP Chief of Neonatology Walt Disney Pavilion, Florida Hospital for Children Orlando, FL The speaker has signed
Pathophysiology Review. Hypoxic-Ischemic Encephalopathy & Therapeutic Hypothermia. Objectives. What is Hypoxic-Ischemic Encephalopathy?
 Hypoxic-Ischemic Encephalopathy & Therapeutic Hypothermia Nancy Couto Nurse Practitioner, NICU London Health Sciences Centre, Children s Hospital nancy.couto@lhsc.on.ca 2014 12 17 Objectives Review Pathophysiology
Hypoxic-Ischemic Encephalopathy & Therapeutic Hypothermia Nancy Couto Nurse Practitioner, NICU London Health Sciences Centre, Children s Hospital nancy.couto@lhsc.on.ca 2014 12 17 Objectives Review Pathophysiology
Imaging the Premature Brain- New Knowledge
 Imaging the Premature Brain- New Knowledge Stein Magnus Aukland Haukeland University Hospital University of Bergen NORWAY No disclosure Imaging modalities O Skull X-ray O Computer Tomography O Cerebral
Imaging the Premature Brain- New Knowledge Stein Magnus Aukland Haukeland University Hospital University of Bergen NORWAY No disclosure Imaging modalities O Skull X-ray O Computer Tomography O Cerebral
Running head: THERAPEUTIC HYPOTHERMIA AND TRANSPORT 1
 Running head: THERAPEUTIC HYPOTHERMIA AND TRANSPORT 1 Therapeutic Hypothermia for Neonatal Encephalopathy: Preparation for Transport to Cooling Center Teresa Z. Baker, DNP-S Annie L. Addison, FNP-S NURS
Running head: THERAPEUTIC HYPOTHERMIA AND TRANSPORT 1 Therapeutic Hypothermia for Neonatal Encephalopathy: Preparation for Transport to Cooling Center Teresa Z. Baker, DNP-S Annie L. Addison, FNP-S NURS
1/29/2014. Kimberly Johnson Hatchett, MD PGY-4 11/15/13
 Kimberly Johnson Hatchett, MD PGY-4 11/15/13 History of Present Illness 14 month old previously healthy infant boy presented via EMS after being found by his mother to be breathing loudly and non-responsive.
Kimberly Johnson Hatchett, MD PGY-4 11/15/13 History of Present Illness 14 month old previously healthy infant boy presented via EMS after being found by his mother to be breathing loudly and non-responsive.
Inclusion criteria for cooling: Babies should be assessed for 3 criteria: A, B and C. See Appendix 1 for a decision making flowchart.
 Guideline for the management of Infants with Moderate or Severe Perinatal Asphyxia requiring cooling. (Including flowchart for infants fulfilling A criteria or A and B criteria only) Perinatal asphyxia
Guideline for the management of Infants with Moderate or Severe Perinatal Asphyxia requiring cooling. (Including flowchart for infants fulfilling A criteria or A and B criteria only) Perinatal asphyxia
Management of Neonatal Seizures
 Management of Neonatal Seizures Manal E. Moustafa Assistant Professor of Pediatric Neurology and Epilepsy Children s Healthcare of Atlanta/Emory University Disclosures I have none! 1 Objectives Recognition
Management of Neonatal Seizures Manal E. Moustafa Assistant Professor of Pediatric Neurology and Epilepsy Children s Healthcare of Atlanta/Emory University Disclosures I have none! 1 Objectives Recognition
Natalia Gorelik 1, Ricardo Faingold 2, Alan Daneman 3, Monica Epelman 3,4. Original Article
 Original Article Intraventricular hemorrhage in term neonates with hypoxicischemic encephalopathy: a comparison study between neonates treated with and without hypothermia Natalia Gorelik 1, Ricardo Faingold
Original Article Intraventricular hemorrhage in term neonates with hypoxicischemic encephalopathy: a comparison study between neonates treated with and without hypothermia Natalia Gorelik 1, Ricardo Faingold
Effect of ALlopurinol in addition to hypothermia for hypoxic-ischemic Brain Injury on Neurocognitive Outcome. Axel Franz, Tübingen
 Effect of ALlopurinol in addition to hypothermia for hypoxic-ischemic Brain Injury on Neurocognitive Outcome Axel Franz, Tübingen Hypoxic-ischemic encephalopathy 1-2 / 1000 newborn suffer from moderate
Effect of ALlopurinol in addition to hypothermia for hypoxic-ischemic Brain Injury on Neurocognitive Outcome Axel Franz, Tübingen Hypoxic-ischemic encephalopathy 1-2 / 1000 newborn suffer from moderate
Life Goes On: High Risk Infant Follow up & Early Intervention. Learning Objectives. Why Do We Need HRIF? 6/7/2013. Outcome studies
 Life Goes On: High Risk Infant Follow up & Early Intervention Anne DeBattista RN, MS, CPNP, CPMHS, PhD(c) Developmental Behavioral Pediatrics Lucile Packard Children s Hospital Learning Objectives Describe
Life Goes On: High Risk Infant Follow up & Early Intervention Anne DeBattista RN, MS, CPNP, CPMHS, PhD(c) Developmental Behavioral Pediatrics Lucile Packard Children s Hospital Learning Objectives Describe
Patent Ductus Arteriosus: Philosophy or Pathology?
 Patent Ductus Arteriosus: Philosophy or Pathology? Disclosure Ray Sato, MD is a speaker for Prolacta Biosciences, Inc. This presentation will discuss off-label uses of acetaminophen and ibuprofen. RAY
Patent Ductus Arteriosus: Philosophy or Pathology? Disclosure Ray Sato, MD is a speaker for Prolacta Biosciences, Inc. This presentation will discuss off-label uses of acetaminophen and ibuprofen. RAY
Planning Committee: Jeffery D. Horbar, MD, Madge E. Buus-Frank, RN, MS, APRN-BC, FAAN, Roger F. Soll, MD
 Title of Program: What has Cochrane Neonatal Done For Babies? Speakers/Moderators: Roger F. Soll, MD Planning Committee: Jeffery D. Horbar, MD, Madge E. Buus-Frank, RN, MS, APRN-BC, FAAN, Roger F. Soll,
Title of Program: What has Cochrane Neonatal Done For Babies? Speakers/Moderators: Roger F. Soll, MD Planning Committee: Jeffery D. Horbar, MD, Madge E. Buus-Frank, RN, MS, APRN-BC, FAAN, Roger F. Soll,
Birth Asphyxia. Perinatal Depression. Birth Asphyxia. Risk Factors maternal. Risk Factors fetal. Risk Factors Intrapartum 2/12/2011
 Birth Asphyxia Perinatal Depression Sara Brown, ARNP Children s Hospital and Regional Medical Center May occur in utero, during labor/delivery or during the neonatal period Condition of impaired blood
Birth Asphyxia Perinatal Depression Sara Brown, ARNP Children s Hospital and Regional Medical Center May occur in utero, during labor/delivery or during the neonatal period Condition of impaired blood
Therapeutic Cooling after Perinatal Asphyxia. Case presentation. Case: seizure and Rx cooling effects
 Therapeutic Cooling after Perinatal Asphyxia Thomas K. Shimotake, MD Assistant Professor of Pediatrics Co-Director, Neurointensive Care Nursery Benioff Children s Hospital University of California San
Therapeutic Cooling after Perinatal Asphyxia Thomas K. Shimotake, MD Assistant Professor of Pediatrics Co-Director, Neurointensive Care Nursery Benioff Children s Hospital University of California San
AMERICAN COLLEGE OF SURGEONS CRITICAL CARE REVIEW COURSE 2012 HOT TOPICS IN PEDIATRIC CRITICAL CARE
 AMERICAN COLLEGE OF SURGEONS CRITICAL CARE REVIEW COURSE 2012 HOT TOPICS IN PEDIATRIC CRITICAL CARE Karyn L. Butler, MD, FACS, FCCM Chief, Surgical Critical Care Hartford Hospital / University of Connecticut
AMERICAN COLLEGE OF SURGEONS CRITICAL CARE REVIEW COURSE 2012 HOT TOPICS IN PEDIATRIC CRITICAL CARE Karyn L. Butler, MD, FACS, FCCM Chief, Surgical Critical Care Hartford Hospital / University of Connecticut
ETIOLOGY AND PATHOGENESIS OF HYPOXIC-ISCHEMIC ENCEPHALOPATHY
 ETIOLOGY AND PATHOGENESIS OF HYPOXIC-ISCHEMIC ENCEPHALOPATHY HYPOXIC-ISCHEMIC ENCEPHALOPATHY Hypoxic-İschemic Encephalopathy Encephalopathy due to hypoxic-ischemic injury [Hypoxic-ischemic encephalopathy
ETIOLOGY AND PATHOGENESIS OF HYPOXIC-ISCHEMIC ENCEPHALOPATHY HYPOXIC-ISCHEMIC ENCEPHALOPATHY Hypoxic-İschemic Encephalopathy Encephalopathy due to hypoxic-ischemic injury [Hypoxic-ischemic encephalopathy
GS3. Understanding How to Use Statistics to Evaluate an Article. Session Summary. Session Objectives. References. Session Outline
 GS3 Understanding How to Use Statistics to Evaluate an Article Reese H. Clark, MD Director of Research Pediatrix Medical Group Neonatologist Greenville Memorial Hospital, Greenville, SC The speaker has
GS3 Understanding How to Use Statistics to Evaluate an Article Reese H. Clark, MD Director of Research Pediatrix Medical Group Neonatologist Greenville Memorial Hospital, Greenville, SC The speaker has
DOWNLOAD OR READ : PERINATAL EVENTS AND BRAIN DAMAGE IN SURVIVING CHILDREN BASED ON PAPERS PRESENTED AT AN INTERNATIONA PDF EBOOK EPUB MOBI
 DOWNLOAD OR READ : PERINATAL EVENTS AND BRAIN DAMAGE IN SURVIVING CHILDREN BASED ON PAPERS PRESENTED AT AN INTERNATIONA PDF EBOOK EPUB MOBI Page 1 Page 2 perinatal events and brain damage in surviving
DOWNLOAD OR READ : PERINATAL EVENTS AND BRAIN DAMAGE IN SURVIVING CHILDREN BASED ON PAPERS PRESENTED AT AN INTERNATIONA PDF EBOOK EPUB MOBI Page 1 Page 2 perinatal events and brain damage in surviving
The Basics. Editorial Team. Editorial Team 9/28/2017
 Title of Program: What has Cochrane Neonatal Done For Babies? Speakers/Moderators: Roger F. Soll, MD Planning Committee: Jeffery D. Horbar, MD, Madge E. Buus-Frank, RN, MS, APRN-BC, FAAN, Roger F. Soll,
Title of Program: What has Cochrane Neonatal Done For Babies? Speakers/Moderators: Roger F. Soll, MD Planning Committee: Jeffery D. Horbar, MD, Madge E. Buus-Frank, RN, MS, APRN-BC, FAAN, Roger F. Soll,
Kimberly M. Thornton, 1,2 Hongying Dai, 3 Seth Septer, 2,4 and Joshua E. Petrikin 1,2. 1. Introduction
 International Pediatrics, Article ID 643689, 7 pages http://dx.doi.org/10.1155/2014/643689 Research Article Effects of Whole Body Therapeutic Hypothermia on Gastrointestinal Morbidity and Feeding Tolerance
International Pediatrics, Article ID 643689, 7 pages http://dx.doi.org/10.1155/2014/643689 Research Article Effects of Whole Body Therapeutic Hypothermia on Gastrointestinal Morbidity and Feeding Tolerance
Perlman J, Clinics Perinatol 2006; 33: Underlying causal pathways. Antenatal Intrapartum Postpartum. Acute near total asphyxia
 Perlman J, Clinics Perinatol 2006; 33:335-353 Underlying causal pathways Antenatal Intrapartum Postpartum Acute injury Subacute injury Associated problem Reduced fetal movements Placental insufficiency
Perlman J, Clinics Perinatol 2006; 33:335-353 Underlying causal pathways Antenatal Intrapartum Postpartum Acute injury Subacute injury Associated problem Reduced fetal movements Placental insufficiency
Postnatal growth failure Causes, consequences and prevention
 Postnatal growth failure Causes, consequences and prevention Bielsko March 9, 2014 Ekhard E. Ziegler, M.D. Fomon Infant Nutrition Unit University of Iowa 1995; 26-29 weeks gestation NICHD Growth Observational
Postnatal growth failure Causes, consequences and prevention Bielsko March 9, 2014 Ekhard E. Ziegler, M.D. Fomon Infant Nutrition Unit University of Iowa 1995; 26-29 weeks gestation NICHD Growth Observational
Ipotermia terapeutica nel bambino: manca l evidenza?
 Ipotermia terapeutica nel bambino: manca l evidenza? Andrea Moscatelli UOSD Terapia Intensiva Neonatale e Pediatrica Dipartimento Integrato di Alta Intensita` di Cura e Chirurgia Istituto Giannina Gaslini
Ipotermia terapeutica nel bambino: manca l evidenza? Andrea Moscatelli UOSD Terapia Intensiva Neonatale e Pediatrica Dipartimento Integrato di Alta Intensita` di Cura e Chirurgia Istituto Giannina Gaslini
Respiratory Management and Outcome of Preterm Infants
 Respiratory Management and Outcome of Preterm Infants 6 th Annual Care Of The Sick Newborn Conference Shu Wu, MD. Department of Pediatrics Division of Neonatology University of Miami School of Medicine
Respiratory Management and Outcome of Preterm Infants 6 th Annual Care Of The Sick Newborn Conference Shu Wu, MD. Department of Pediatrics Division of Neonatology University of Miami School of Medicine
Swiss neonatal network and Follow up Group
 Swiss neonatal network and Follow up Group March 2011 Barbara Brotschi and Cornelia Hagmann Hypoxic ischaemic encephalopathy Neonatal encephalopathy due to perinatal hypoxiaischaemia: clinically defined
Swiss neonatal network and Follow up Group March 2011 Barbara Brotschi and Cornelia Hagmann Hypoxic ischaemic encephalopathy Neonatal encephalopathy due to perinatal hypoxiaischaemia: clinically defined
Effects of Hypothermia for Perinatal Asphyxia on Childhood Outcomes
 The new england journal of medicine original article Effects of Hypothermia for Perinatal Asphyxia on Childhood Outcomes Denis Azzopardi, M.D., Brenda Strohm, R.N., Neil Marlow, D.M., Peter Brocklehurst,
The new england journal of medicine original article Effects of Hypothermia for Perinatal Asphyxia on Childhood Outcomes Denis Azzopardi, M.D., Brenda Strohm, R.N., Neil Marlow, D.M., Peter Brocklehurst,
TLC March 27, Shawn Hollinger-Neonatal Fellow CHEO
 TLC March 27, 2013 Presented/Prepared by: Shawn Hollinger, PGY5 Neonatal-Perinatal Medicine Resident - University of Ottawa With slides/images from Dr. Brigitte Lemyre Associate Professor of Pediatrics
TLC March 27, 2013 Presented/Prepared by: Shawn Hollinger, PGY5 Neonatal-Perinatal Medicine Resident - University of Ottawa With slides/images from Dr. Brigitte Lemyre Associate Professor of Pediatrics
The Pharmacokinetics of Antiepileptics Drugs in Neonates with Hypoxic Ischemic Encephalopathy
 The Pharmacokinetics of Antiepileptics Drugs in Neonates with Hypoxic Ischemic Encephalopathy KELIANA O MARA, PHARMD FLORIDA NEONATAL NEUROLOGIC NETWORK STATE MEETING Objectives Describe seizures in hypoxic
The Pharmacokinetics of Antiepileptics Drugs in Neonates with Hypoxic Ischemic Encephalopathy KELIANA O MARA, PHARMD FLORIDA NEONATAL NEUROLOGIC NETWORK STATE MEETING Objectives Describe seizures in hypoxic
Amgen (Europe) GmbH, Zug, Switzerland, 2 Amgen GmbH, Munich, Germany, 3
 GmbH, Zug, Switzerland, 2 Amgen GmbH, Munich, Germany, 3") Occurrence of skeletal-related events (SRE) in pa9ents with solid tumors (ST): early versus late ini9a9on of SRE preventa9ve agents (SPA) Intorcia M 1, Hohmann D 2, Giannopoulou C 1, Ansorge S 3, Diel
Occurrence of skeletal-related events (SRE) in pa9ents with solid tumors (ST): early versus late ini9a9on of SRE preventa9ve agents (SPA) Intorcia M 1, Hohmann D 2, Giannopoulou C 1, Ansorge S 3, Diel
REVIEW ARTICLE. Hypothermia to Treat Neonatal Hypoxic Ischemic Encephalopathy
 REVIEW ARTICLE Hypothermia to Treat Neonatal Hypoxic Ischemic Encephalopathy Systematic Review Prakesh S. Shah, MD, MSc, FRCPC; Arne Ohlsson, FRCPC, MSc; Max Perlman, FRCPC Objectives: To systematically
REVIEW ARTICLE Hypothermia to Treat Neonatal Hypoxic Ischemic Encephalopathy Systematic Review Prakesh S. Shah, MD, MSc, FRCPC; Arne Ohlsson, FRCPC, MSc; Max Perlman, FRCPC Objectives: To systematically
Hypoxic-Ischemic Encephalopathy. TW de Witt University of Pretoria Department of Paediatrics Neonatology
 Hypoxic-Ischemic Encephalopathy TW de Witt University of Pretoria Department of Paediatrics Neonatology Background HIE remains a serious condition that causes significant mortality and longterm morbidity.
Hypoxic-Ischemic Encephalopathy TW de Witt University of Pretoria Department of Paediatrics Neonatology Background HIE remains a serious condition that causes significant mortality and longterm morbidity.
Epoetin Alfa for Neuroprotection in Hypoxic Ischemic Encephalopathy: Incredibly Promising or Sub-Par?
 Epoetin Alfa for Neuroprotection in Hypoxic Ischemic Encephalopathy: Incredibly Promising or Sub-Par? Erin Hohenstein, PharmD PGY-1 Pharmacy Resident The Children s Hospital of San Antonio Division of
Epoetin Alfa for Neuroprotection in Hypoxic Ischemic Encephalopathy: Incredibly Promising or Sub-Par? Erin Hohenstein, PharmD PGY-1 Pharmacy Resident The Children s Hospital of San Antonio Division of
Study of role of MRI brain in evaluation of hypoxic ischemic encephalopathy
 Original article: Study of role of MRI brain in evaluation of hypoxic ischemic encephalopathy *Dr Harshad Bhagat, ** Dr Ravindra Kawade, ***Dr Y.P.Sachdev *Junior Resident, Department Of Radiodiagnosis,
Original article: Study of role of MRI brain in evaluation of hypoxic ischemic encephalopathy *Dr Harshad Bhagat, ** Dr Ravindra Kawade, ***Dr Y.P.Sachdev *Junior Resident, Department Of Radiodiagnosis,
Benefits of Caffeine Citrate: Neurodevelopmental Outcomes of ELBW Infants
 St. Catherine University SOPHIA Master of Arts in Nursing Theses Nursing 12-2011 Benefits of Caffeine Citrate: Neurodevelopmental Outcomes of ELBW Infants Teri Johnson St. Catherine University Follow this
St. Catherine University SOPHIA Master of Arts in Nursing Theses Nursing 12-2011 Benefits of Caffeine Citrate: Neurodevelopmental Outcomes of ELBW Infants Teri Johnson St. Catherine University Follow this
PedsCases Podcast Scripts
 PedsCases Podcast Scripts This is a text version of a podcast from Pedscases.com on Hypoxic Ischemic Encephalopathy. These podcasts are designed to give medical students an overview of key topics in pediatrics.
PedsCases Podcast Scripts This is a text version of a podcast from Pedscases.com on Hypoxic Ischemic Encephalopathy. These podcasts are designed to give medical students an overview of key topics in pediatrics.
Total Body Cooling & Hypoxic Ischemic Encephalopathy in the Neonate Kaleidoscope 2017
 Total Body Cooling & Hypoxic Ischemic Encephalopathy in the Neonate Kaleidoscope 2017 LEIGH ANN CATES PHD, APRN, NNP -BC, RRT-NPS, CHSE N E O N ATA L N U R S E P R A C T I T I O N E R - T E X A S C H I
Total Body Cooling & Hypoxic Ischemic Encephalopathy in the Neonate Kaleidoscope 2017 LEIGH ANN CATES PHD, APRN, NNP -BC, RRT-NPS, CHSE N E O N ATA L N U R S E P R A C T I T I O N E R - T E X A S C H I
Lesson learnt from big trials. Sung Phil Chung, MD Gangnam Severance Hospital, Yonsei Univ.
 Lesson learnt from big trials Sung Phil Chung, MD Gangnam Severance Hospital, Yonsei Univ. Trend of cardiac arrest research 1400 1200 1000 800 600 400 200 0 2008 2009 2010 2011 2012 2013 2014 2015 2016
Lesson learnt from big trials Sung Phil Chung, MD Gangnam Severance Hospital, Yonsei Univ. Trend of cardiac arrest research 1400 1200 1000 800 600 400 200 0 2008 2009 2010 2011 2012 2013 2014 2015 2016
UK cooling TOBY. register. UK TOBY Cooling Register Protocol
 UK cooling TOBY register UK TOBY Cooling Register Protocol Version 3, 11th June 2007 1 Contents 1. Background 2 1.1 Perinatal asphyxial encephalopathy 2 1.2 Pathogenesis of perinatal asphyxial encephalopathy
UK cooling TOBY register UK TOBY Cooling Register Protocol Version 3, 11th June 2007 1 Contents 1. Background 2 1.1 Perinatal asphyxial encephalopathy 2 1.2 Pathogenesis of perinatal asphyxial encephalopathy
Case Presentations. Anamika B. Mukherjee, MD September 13, 2017
 Case Presentations Anamika B. Mukherjee, MD September 13, 2017 Nothing to disclose Disclosures Learning Objectives Use the CPQCC Toolkit for therapeutic hypothermia to apply the guidelines for screening
Case Presentations Anamika B. Mukherjee, MD September 13, 2017 Nothing to disclose Disclosures Learning Objectives Use the CPQCC Toolkit for therapeutic hypothermia to apply the guidelines for screening
Seizure burden and neurodevelopmental outcome in neonates with hypoxic ischemic encephalopathy
 DEVELOPMENTAL MEDICINE & CHILD NEUROLOGY ORIGINAL ARTICLE Seizure burden and neurodevelopmental outcome in neonates with hypoxic ischemic encephalopathy LIUDMILA KHAROSHANKAYA 1,2 NATHAN J STEVENSON 1
DEVELOPMENTAL MEDICINE & CHILD NEUROLOGY ORIGINAL ARTICLE Seizure burden and neurodevelopmental outcome in neonates with hypoxic ischemic encephalopathy LIUDMILA KHAROSHANKAYA 1,2 NATHAN J STEVENSON 1
Outcomes of Infants with Neonatal Abstinence Syndrome
 Outcomes of Infants with Neonatal Abstinence Syndrome Caroline O. Chua, MD, FAAP Medical Director, Division of Neonatology Director, Neonatal Follow Up Clinic Nemours Children s Hospital Orlando, Florida
Outcomes of Infants with Neonatal Abstinence Syndrome Caroline O. Chua, MD, FAAP Medical Director, Division of Neonatology Director, Neonatal Follow Up Clinic Nemours Children s Hospital Orlando, Florida
Outcome of infants with hypoxic ischemic encephalopathy treated with brain hypothermia
 bs_bs_banner doi:10.1111/jog.12520 J. Obstet. Gynaecol. Res. Vol. 41, No. 2: 229 237, February 2015 Outcome of infants with hypoxic ischemic encephalopathy treated with brain hypothermia Takuya Tokuhisa
bs_bs_banner doi:10.1111/jog.12520 J. Obstet. Gynaecol. Res. Vol. 41, No. 2: 229 237, February 2015 Outcome of infants with hypoxic ischemic encephalopathy treated with brain hypothermia Takuya Tokuhisa
Neonatal Encephalopathy: Treatment With Hypothermia Seetha Shankaran. DOI: /neo.11-2-e85
 Neonatal Encephalopathy: Treatment With Hypothermia Seetha Shankaran NeoReviews 2010;11;e85-e92 DOI: 10.1542/neo.11-2-e85 The online version of this article, along with updated information and services,
Neonatal Encephalopathy: Treatment With Hypothermia Seetha Shankaran NeoReviews 2010;11;e85-e92 DOI: 10.1542/neo.11-2-e85 The online version of this article, along with updated information and services,
Therapeutic hypothermia in neonatal asphyxia
 FVV IN OBGYN, 2012, 4 (2): 133-139 New perspective Therapeutic hypothermia in neonatal asphyxia L. CORNETTE Head Department Neonatology, AZ Sint Jan Brugge-Oostende AV Ruddershove 10, 8000 Brugge, Belgium.
FVV IN OBGYN, 2012, 4 (2): 133-139 New perspective Therapeutic hypothermia in neonatal asphyxia L. CORNETTE Head Department Neonatology, AZ Sint Jan Brugge-Oostende AV Ruddershove 10, 8000 Brugge, Belgium.
CEREBRAL FUNCTION MONITORING
 CEREBRAL FUNCTION MONITORING Introduction and Definitions The term amplitude integrated electroencephalography (aeeg) is used to denote a method for electro-cortical monitoring whereas cerebral function
CEREBRAL FUNCTION MONITORING Introduction and Definitions The term amplitude integrated electroencephalography (aeeg) is used to denote a method for electro-cortical monitoring whereas cerebral function
Imaging findings in neonates with hypoxic-ischaemic encephalopathy and terapeutic hypothermia.
 Imaging findings in neonates with hypoxic-ischaemic encephalopathy and terapeutic hypothermia. Poster No.: C-1577 Congress: ECR 2014 Type: Scientific Exhibit Authors: S. Manso Garcia, M. J. Velasco Marcos,
Imaging findings in neonates with hypoxic-ischaemic encephalopathy and terapeutic hypothermia. Poster No.: C-1577 Congress: ECR 2014 Type: Scientific Exhibit Authors: S. Manso Garcia, M. J. Velasco Marcos,
Discriminating ability of the Infant Neurological International Battery
 Discriminating ability of the Infant Neurological International Battery (Infanib) for the neurological outcome of high-risk infants in a cohort of 5857 low birth weight infants followed during their irst
Discriminating ability of the Infant Neurological International Battery (Infanib) for the neurological outcome of high-risk infants in a cohort of 5857 low birth weight infants followed during their irst
12/7/2011. JDBP 32,6, July/August011468July/August011
 Easy (?) as 1,2,3: Issues in Developmental Follow UP of NICU GRADS Martin T. Hoffman, MD Dept. of Pediatrics University at Buffalo School of Medicine and Biomedical Science Women and Children s Hospital
Easy (?) as 1,2,3: Issues in Developmental Follow UP of NICU GRADS Martin T. Hoffman, MD Dept. of Pediatrics University at Buffalo School of Medicine and Biomedical Science Women and Children s Hospital
Approach to the Child with Developmental Delay
 Approach to the Child with Developmental Delay Arwa Nasir Department of Pediatrics University of Nebraska Medical Center DISCLOSURE DECLARATION Approach to the Child with Developmental Delay Arwa Nasir
Approach to the Child with Developmental Delay Arwa Nasir Department of Pediatrics University of Nebraska Medical Center DISCLOSURE DECLARATION Approach to the Child with Developmental Delay Arwa Nasir
Therapeutic Hypothermia
 Objectives Overview Therapeutic Hypothermia Nerissa U. Ko, MD, MAS UCSF Department of Neurology Critical Care Medicine and Trauma June 4, 2011 Hypothermia as a neuroprotectant Proven indications: Adult
Objectives Overview Therapeutic Hypothermia Nerissa U. Ko, MD, MAS UCSF Department of Neurology Critical Care Medicine and Trauma June 4, 2011 Hypothermia as a neuroprotectant Proven indications: Adult
Brain injury and Resuscitation! Turning Back the Clock!
 Brain injury and Resuscitation! Turning Back the Clock! Dec 2008 Patrick J McNamara Learning Objectives Understand the benefits of Hypothermia and how it works? Identify patients who may benefit from treatment.
Brain injury and Resuscitation! Turning Back the Clock! Dec 2008 Patrick J McNamara Learning Objectives Understand the benefits of Hypothermia and how it works? Identify patients who may benefit from treatment.
The NeuroNICU From Concept to Clinical Service. MJ Harbert, MD Co-Director, NeuroNICU Service Rady Children s Hospital San Diego
 The NeuroNICU From Concept to Clinical Service MJ Harbert, MD Co-Director, NeuroNICU Service Rady Children s Hospital San Diego What is a NeuroNICU? Collaboration between Neonatology and Neurology Neonatal
The NeuroNICU From Concept to Clinical Service MJ Harbert, MD Co-Director, NeuroNICU Service Rady Children s Hospital San Diego What is a NeuroNICU? Collaboration between Neonatology and Neurology Neonatal
Temperature Correction of Blood Gas Measurements during Therapeutic Hypothermia: Is it Time to Chill Out?
 Temperature Correction of Blood Gas Measurements during Therapeutic Hypothermia: Is it Time to Chill Out? Dr. Elizabeth Zorn Dr. Gwenyth Fischer Dr. Martha Lyon Disclosures (ML) Speaking Honoraria Radiometer
Temperature Correction of Blood Gas Measurements during Therapeutic Hypothermia: Is it Time to Chill Out? Dr. Elizabeth Zorn Dr. Gwenyth Fischer Dr. Martha Lyon Disclosures (ML) Speaking Honoraria Radiometer
State of Florida Hypothermia Protocol. Michael D. Weiss, M.D. Associate Professor of Pediatrics Division of Neonatology
 State of Florida Hypothermia Protocol Michael D. Weiss, M.D. Associate Professor of Pediatrics Division of Neonatology I. Entry Criteria 1. Gestational Age greater than or equal to 35 weeks gestation
State of Florida Hypothermia Protocol Michael D. Weiss, M.D. Associate Professor of Pediatrics Division of Neonatology I. Entry Criteria 1. Gestational Age greater than or equal to 35 weeks gestation
An Update on Caffeine Therapy
 An Update on Caffeine Therapy Emory University School of Medicine Atlanta, GA Wally Carlo, MD University of Alabama at Birmingham Department of Pediatrics Division of Neonatology wcarlo@peds.uab.edu Objectives
An Update on Caffeine Therapy Emory University School of Medicine Atlanta, GA Wally Carlo, MD University of Alabama at Birmingham Department of Pediatrics Division of Neonatology wcarlo@peds.uab.edu Objectives
Objectives. Apnea Definition and Pitfalls. Pathophysiology of Apnea. Apnea of Prematurity and hypoxemia episodes 5/18/2015
 Apnea of Prematurity and hypoxemia episodes Deepak Jain MD Care of Sick Newborn Conference May 2015 Objectives Differentiating between apnea and hypoxemia episodes. Pathophysiology Diagnosis of apnea and
Apnea of Prematurity and hypoxemia episodes Deepak Jain MD Care of Sick Newborn Conference May 2015 Objectives Differentiating between apnea and hypoxemia episodes. Pathophysiology Diagnosis of apnea and
Infant Nutrition & Growth to Optimize Outcome Fauzia Shakeel, MD
 Infant Nutrition & Growth to Optimize Outcome Fauzia Shakeel, MD Neonatologist All Children s Hospital / Johns Hopkins Medicine Affiliate Assistant Professor, University of South Florida September 2014
Infant Nutrition & Growth to Optimize Outcome Fauzia Shakeel, MD Neonatologist All Children s Hospital / Johns Hopkins Medicine Affiliate Assistant Professor, University of South Florida September 2014