Prof. Dr. Birgit Castelein
|
|
|
- Frank Daniel
- 6 years ago
- Views:
Transcription
1 Annual meeting of the Danish Society for Surgery of the shoulder and of the elbow April Aarhus, Denmark Prof. Dr. Birgit Castelein



2



3 PhD: Analysis of recruitment of the superficial and deep scapular muscles in patients with chronic shoulder or neck pain, and implications for rehabilitation exercises Professor at our department Physiotherapy and Rehabilitation Sciences : Rehabilitation of the Upper Limb
4 Overview 1. Analysis of recruitment of the superficial and deep scapular muscles in patients with chronic shoulder or neck pain, and implications for rehabilitation exercises 2. Shoulder impingement: can one label satisfy everything? 3. Central pain processing in shoulder pain 4. Progression in biceps load during rehabilitation exercises 5. The influence of induced shoulder muscle pain on rotator cuff and scapulothoracic muscle activity during elevation of the arm.
5 Overview 1. Analysis of recruitment of the superficial and deep scapular muscles in patients with chronic shoulder or neck pain, and implications for rehabilitation exercises 2. Shoulder impingement: can one label satisfy everything? 3. Central pain processing in shoulder pain 4. Progression in biceps load during rehabilitation exercises 5. The influence of induced shoulder muscle pain on rotator cuff and scapulothoracic muscle activity during elevation of the arm.

6



7 Movements of the scapula: * TRANSLATION Elevation Depression Protraction Retraction * ROTATION Upward rotation Downward rotation Anterior tilt Posterior tilt Internal rotation External rotation
8 ROTATION 8

9 UPWARD ROTATION INTRODUCTION BODY DISCUSSION CONCLUSION

10 DOWNWARD ROTATION INTRODUCTION BODY DISCUSSION CONCLUSION



11

12 SCAPULAR MOVEMENT DURING ELEVATION OF THE ARM: 1) UPWARD ROTATION 2) POSTERIOR TILT 3) INTERNAL/EXTERNAL ROTATION Braman et al. 2009, Ludewig et al. 2009, McClure et al. 2001, Kibler and McMullen, 2003



13 TRAPEZIUS PECTORALIS MINOR RHOMBOIDS SERRATUS ANTERIOR LEVATOR SCAPULAE 13

14 Upper Trapezius Upper Trapezius
15 Middle Trapezius INTRODUCTION BODY DISCUSSION CONCLUSION
16 Lower Trapezius Lower Trapezius INTRODUCTION BODY DISCUSSION CONCLUSION

17 Serratus Anterior INTRODUCTION BODY DISCUSSION CONCLUSION

18 Trapezius Serratus Anterior
19 Pectoralis Minor Rhomboid Major Levator Scapulae INFLUENCE THE POSITION AND MOVEMENT OF THE SCAPULA 19


20 Pectoralis Minor Levator Scapulae Rhomboids 20




21 PECTORALIS MINOR RHOMBOID MAJOR LEVATOR SCAPULAE - MAY INFLUENCE THE POSITION AND MOVEMENT OF THE SCAPULA - MAY HINDER NORMAL SCAPULAR MOVEMENT IN CASE OF TIGHTNESS OR HYPERACTIIVTY 21
22 OPTIMAL FUNCTION SCAPULA: is necessary for optimal function of the shoulder/neck region (central link between shoulder and neck) Disturbances in the function of the scapular muscles can induce mechanical load on the shoulder and on the neck region (Trapezius & Levator Scapulae) 22

 Patients with idiopathic")
23 DYSFUNCTION OF THE SCAPULA = SCAPULAR DYSKINESIS Patients with shoulder pain (subacromial pain syndrome) Patients with idiopathic neck pain 23
 UPWARD ROTATION POSTERIOR TILT INTERNAL")

24 DYSFUNCTION OF THE SCAPULA = SCAPULAR DYSKINESIS CHRONIC SHOULDER PAIN (impingement) UPWARD ROTATION POSTERIOR TILT INTERNAL ROTATION/ EXTERNAL ROTATION * Ludewig & Reynolds 2009 * Struyf et al * Timmons et al * Ratcliffe et al * Sousa et al
 * Helgadottir et al. 2010 * Van Dillen et al. 2007 * Ha et al. 2011 * Lluch et al.")
25 DYSFUNCTION OF THE SCAPULA = SCAPULAR DYSKINESIS CHRONIC IDIOPATHIC NECK PAIN s INITIAL EVIDENCE OF ALTERATIONS IN SCAPULAR POSITION/MOVEMENT (similar to alterations seen in patients with shoulder pain) * Helgadottir et al * Van Dillen et al * Ha et al * Lluch et al

26 DYSFUNCTION OF THE SCAPULA = SCAPULAR DYSKINESIS Pain Soft tissue tightness Muscle fatigue Cervical and thoracic posture Muscle activation/strength 26



27 - ALTERATIONS IN SCAPULOTHORACIC MUSCLE ACTIVITY: UPPER TRAPEZIUS or MIDDLE TRAPEZIUS LOWER TRAPEZIUS SERRATUS ANTERIOR Struyf et al. 2014, Sousa et al DEEPER LYING MUSCLES??? PECTORALIS MINOR RHOMBOID MAJOR LEVATOR SCAPULAE
28 - ALTERATIONS IN SCAPULOTHORACIC MUSCLE ACTIVITY: UPPER TRAPEZIUS or Falla et al. 2004, Johnston et al. 2008a, Johnston et al. 2008b MT, LT, SA??? Deeper lying muscles??? PECTORALIS MINOR RHOMBOID MAJOR LEVATOR SCAPULAE
29 Training the scapulothoracic muscles : symptoms (De Mey et al. 2012, Mulligan et al. 2016, Baskurt et al. 2011, Struyf et al. 2013, Moezy et al. 2014, Andersen et al. 2014) 29
30 SHOULDER PAIN: De Mey et al : 6-week scapular training in overhead athletes with SIS: - improved scapular muscle recruitment (decreased Trapezius muscle activation and decreased UT/SA ratio during a similar arm elevation task) - significant functional improvement and less pain. Baskurt et al. 2011: compared (1) stretching and strengthening exercises and (2) scapular stabilization exercises in patients with SIS - pain, ROM, muscle strength, joint position sense, scapular dysfunction and quality of life improved in both groups after treatment. - improvements in muscle strength, joint position sense and scapular dysfunction: significantly larger with the scapular stabilization exercises. Moezy et al. 2014: compared (1) scapular stabilization exercise therapy and (2) physical therapy in patients with SIS - Scapular stabilization exercise: superior in decreasing pain, improving scapular protraction, improving head and back posture and increasing shoulder mobility. Mulligan et al. 2016: 4 weeks scapular stabilization exercises in patients with SIS - decreased significantly the pain score & improved significantly the shoulder function Struyf et al.2013: compared (1) scapular-focused treatment (including stretching, scapular motor control training and passive manual mobilization) and (2) a control therapy (stretching, muscle friction and eccentric rotator cuff training) in patients with SIS An important treatment effect in favor of scapular-focused treatment was found in self-reported disability, and also in pain during the Neer, Hawkins and Empty can test. In addition, the scapular focused treatment demonstrated an improvement in self-experienced pain at rest, whereas the control group did not change. * 30
31 NECK PAIN: Andersen et al compared (1) intensive scapular function training with exercises and (2) control therapy in patients with chronic non-specific neck/shoulder pain - reducing pain and increasing shoulder elevation strength 31
32 Training the scapulothoracic muscles : symptoms (De Mey et al. 2012, Mulligan et al. 2016, Baskurt et al. 2011, Struyf et al. 2013, Moezy et al. 2014, Andersen et al. 2014) Choice of an exercise? Based upon the assumed effect of the exercise on the muscle activation Based upon the knowledge of the superficial lying scapulothoracic muscles Deeper lying muscle activity???? 32

33 Deeper lying muscle activity - in patient populations - during different exercises
34 Part 1: SUPERFICIAL AND DEEPER LYING SCAPULOTHORACIC MUSCLE ACTIVITY IN PATIENTS WITH SHOULDER AND NECK PAIN Part 2: SCAPULOTHORACIC MUSCLE ACTIVITY DURING DIFFERENT EXERCISES COMMONLY USED IN SCAPULR REHABILITATION PROGRAMS



35 - ELECTROMYOGRAPHY OF THE SCAPULOTHORACIC MUSCLES: - SURFACE EMG ELECTRODES: TRAPEZIUS & SERRATUS ANTERIOR - FINE-WIRE EMG ELECTRODES: PECTORALIS MINOR, LEVATOR SCAPULAE & RHOMBOID - DOMINANT SIDE OF THE SUBJECT * PATIENTS WITH IMPINGEMENT SYMPTOMS * PATIENTS WITH IDIOPATHIC NECK PAIN * HEALTHY CONTROLS
36 Part 1: SUPERFICIAL AND DEEPER LYING SCAPULOTHORACIC MUSCLE ACTIVITY IN PATIENTS WITH SHOULDER PAIN

37 37
 HEALTHY CONTROLS (matched")


38 17 ( ) PATIENTS WITH SHOULDER IMPINGEMENT SYMPTOMS 20 ( ) HEALTHY CONTROLS (matched for age, weight and height) 7 SCAPULOTHORACIC MUSCLES: UT MT LT SA LS Pm RM 3 ELEVATION TASKS IN THE SCAPULAR PLANE SCAPTION TOWEL WALL SLIDE BILATERAL ELEVATION WITH EXTERNAL ROTATION
39 39
40 PECTORALIS MINOR 40

41 41
42
43 19 ( ) patients with idiopathic neck pain 19 ( ) healthy controls (matched for gender, age, weight and height) Presence / absence of scapular dyskinesis 7 scapulothoracic muscles: UT MT LT SA LS Pm RM Scaption Towel Wall Slide
44 *Patients with idiopathic neck pain: Pm activity during the towel wall slide in comparison with healthy controls *Patients with idiopathic neck pain and scapular dyskinesis: MT activity in comparison with healthy controls with scapular dyskinesis
45 Part 2: SCAPULOTHORACIC MUSCLE ACTIVITY DURING DIFFERENT EXERCISES COMMONLY USED IN SCAPULAR REHABILITATION PROGRAMS
46
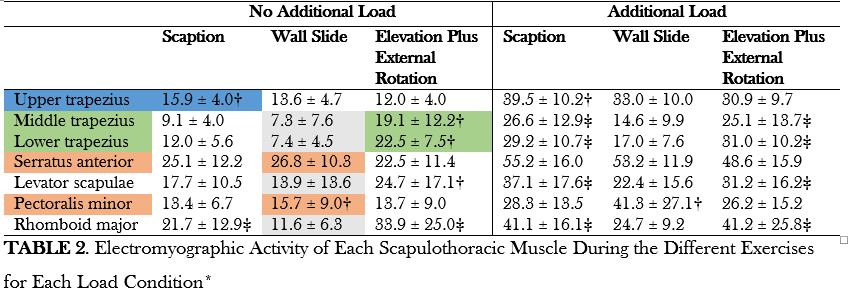
47 21 HEALTHY SUBJECTS (10, 11 ) MUSCLES: UT, MT, LT, SA, Pm, LS & RM 3 ELEVATION EXERCISES, with and without load SCAPTION TOWEL WALL SLIDE ELEVATION WITH EXTERNAL ROTATION
48 BACKGROUND: Sdfqdsf MATERIALS & METHODS: RESULTS & CONCLUSION
49 49

50 - The SA has a critical role in stabilizing the scapula against the thorax + contributes to the movement of the scapula during elevation - Research has linked shoulder disorders to impairments of the SA activation => Exercises that target SA in the rehabilitation: Protraction Exercises - Pm: synergist during protraction exercises BUT: also downward rotation & depression - Overuse of Pm: malaligned scapula TO WHAT EXTENT IS THE Pm ACTIVATED DURING SA EXERCISES?

51 26 HEALTHY SUBJECTS(15, 11 ) MUSCLES: SERRATUS ANTERIOR & PECTORALIS MINOR 3 PROTRACTION EXERCISES Serratus Punch Modified Push-Up Plus Wall Version Modified Push-Up Plus Floor Version
52 * During the Serratus Punch: SA activity significantly higher than Pm activity Pectoralis Minor: * Serratus Anterior:
53 CONCENTRIC PHASE OF THE PROTRACTION EXERCISES CONCENTRIC ECCENTRIC

54 - In patients with scapular dysfunction: often imbalance between upward rotators & downward rotators => can cause abnormalities in coordinated scapular rotation - Exercises with focus on activation of upward rotators while minimizing the activation of the downward rotators - Shrug exercises are often recommended to activate muscles that produce upward rotation, but little information is available on the activity of the downward rotators during shrugging exercises
55 26 HEALTHY SUBJECTS(15, 11 ) MEDIAL SCAPULAR MUSCLES: UT, LS, MT, RM & LT 3 EXERCISES: SHRUG SHRUG OVERHEAD RETRACTION OVERHEAD
56 Similar UT Similar UT Similar UT LS & RM MT, LT & RM
57 Alterations in scapulothoracic muscle activity can be present in patients with shoulder or neck pain: REHABILITATION
58 RESEARCH & CLINICAL PRACTICE: - MIDDLE TRAPEZIUS, LOWER TRAPEZIUS, SERRATUS ANTERIOR: ACTIVATION - PECTORALIS MINOR: AVOID ACTIVATION - LEVATOR SCAPULAE, RHOMBOID MAJOR & UPPER TRAPEZIUS:???? - LEVATOR SCAPULAE: clinical experience: overactive & shortened - RHOMBOID MAJOR - UPPER TRAPEZIUS SPECIFIC NEEDS AND MUSCLE DYSFUNCTIONS MAY VARY BETWEEN INDIVIDUALS CLINICAL EXAMINATION: CRUCIAL TO FIND POSSIBLE MUSCLE DYSFUNCTION AND INDIVIDU-SPECIFIC REHABILITATION PROGRAM
59 SCAPULA properly positioned? - Clinical tools? Struyf et al. 2014: Clinical assessment of the scapula: a review of the literature 59

60 60
61 SCAPULA properly positioned? - CLINICAL TOOLS? Struyf et al. 2014: Clinical assessment of the scapula: a review of the literature Overview of different reliable clinical tools for both static and dynamic positioning of the scapula, but no real cut-off value NO CONSENSUS -> it is up to the clinician to decide when scapular dysfunction or scapular muscle dysfunction is present 61
62 Current recommendation? => SCAPULAR DYSKINESIS TEST clinical observation of the medial and inferior scapular borders for winging or medial border prominence, lack a smooth coordinated movement as exemplified by early scapular elevation or shrugging during ascending arm forward flexion, and rapid downward rotation during arm lowering from full flexion. YES or NO 62

63 63
64 Role of scapular dyskinesis? - Scapular dyskinesis can be present in overhead athletes too - 3 prospective studies (Clarsen et al. 2014, Kawasaki et al. 2012, McKenna et al ): - Association between scapular dysfunction and development shoulder pain - 2 prospective studies (Myers et al. 2013, Struyf et al. 2014) - No association between scapular dysfunction and development of shoulder pain 64
65 Prospective studies 1) Kawasaki et al. (2012) showed that scapular dyskinesis, based on visual observation, is a risk factor for shoulder pain during the season in professional rugby players. 2) Myers et al. (2013) reported that scapular dysfunction, identified during preseason screening, could not be established as a prospective risk factor for throwing-related upper extremity injuries in high school baseball players. 3) Shitara et al. (2015) did also not identify scapular dyskinesis as a risk factor for shoulder and elbow injuries in high school baseball pitchers. 4) Clarsen et al. (2014) showed that obvious scapular dyskinesis is a risk factor for shoulder injuries among elite male handball players. 5) A prospective study of Struyf et al. (2014) investigated possible scapular related risk factors for developing shoulder pain. It was found that scapular characteristics could not predict the development of shoulder pain in the overhead athlete population. 65
66 Presence of scapular dyskinesis: contributing factor to the symptoms of the patient? SYMPTOM ALTERATION TESTS: = identify if scapular dyskinesis is driving symptoms by manually correcting the scapula during provocation testing *Scapular Assistance Test (SAT) *Scapular Retraction Test (SRT) *(Shoulder symptom modification procedure (SSMP)) 66

67 SCAPULAR ASSISTANCE TEST 67

68 SCAPULAR RETRACTION TEST 68

69 If there is a relation between scapula and symptoms Inclusion in the rehabilitation 69
70 70
71 71

72 Stretching Pectoralis Minor 72

73 Stretching Levator Scapulae 73

74 Stretching Trapezius pars descendens 74


75 Stretching Posterior Capsule 75

76 76
77 77

78 78
79 TRAINING => CRUCIAL TO SELECT THE MOST APPROPRIATE EXERCISE ACCORDING TO THE INDIVIDUAL PRESENTATION OF THE PATIENT => RECOMMENDATIONS FOR EXERCISES Clinical Examination Inspection Palpation Manual Muscle Testing Symptom alteration tests Etc.
80 In the past: Choice for exercises based upon knowledge from Trapezius and Serratus Anterior Now: Take into account the activity of the deeper lying muscles also!! 80
81 Focus Upper Trapezius: Promote activation of UT (upward rotation) Avoid activation of UT (muscle is too active) 81
 Clinically: downward rotation of the scapula")
82 Focus Upper Trapezius: Promote activation of UT (upward rotation) Clinically: downward rotation of the scapula 82
83 Focus Upper Trapezius: Promote activation UT (upward rotation) Clinically: downward rotation of the scapula => exercises with focus on upward rotation with minimal activation of downward rotators = SHRUGOVERHEAD 83
84 Focus Upper Trapezius: Avoid activation UT (muscle is already too active) Clinically: shrugging sign * TOWEL WALL SLIDE *ELEVATION WITH EXTERNAL ROTATION 84


85 Ratio s: - Between Trapezius en Serratus Anterior: * low UT/SA: elbow push-up/prone bridging serratus punch supine serratus punch in GKK (bench slide). 85
86 Focus Serratus Anterior: Promote activation SA Clinically: internal rotation of the scapula, prominence medial borderr (scapula alata of winging) or prominent angulus inferior or excessive anterior tilting Exercises with focus on SA: Serratus punch > push-up floor > push-up wall 86
87 Focus Serratus Anterior: Promote activation SA Clinically: internal rotation of the scapula, prominence medial borderr (scapula alata of winging) or prominent angulus inferior or excessive anterior tilting Exercises with focus on SA: Serratus punch > push-up floor > push-up wall Exercises with low Pm/SA ratio: SERRATUS PUNCH 87
88 Ratio s: - Between different parts of Trapezius: Low UT/MT & UT/LT Sidelying forward flexion Prone horizontal abduction with external rotation Sidelying External Rotation Prone Extension 89
89 Focus Rhomboid: Promote activation RM: elevation with external rotation Avoid activation RM: towel wall slide 90

90 High UT Low LS ShrugOverhead

91 Towel Wall Slide Prone bridging/ Elbow Push-Up High SA Low UT Bilateral Elevation with External Rotation Serratus Punch Supine

92 High LT Low Pm Bilateral Elevation with External Rotation



93 High SA Low Pm Serratus Punch

94 Bilateral Elevation with External Rotation High MT High LT Low UT Sidelying forward flexion Prone horizontal abduction with external rotation Sidelying External Rotation Prone Extension
95 CONCLUSION - ALTERATIONS IN SCAPULOTHORACIC MUSCLE ACTIVITY CAN BE PRESENT IN PATIENTS WITH SHOULDER AND NECK PAIN + POSSIBLE ROLE PECTORALIS MINOR - CRUCIAL TO SELECT THE MOST APPROPRIATE EXERCISE ACCORDING TO THE SPECIFIC NEEDS/INDIVIDUAL PRESENTATION OF THE PATIENT
96 Overview 1. Analysis of recruitment of the superficial and deep scapular muscles in patients with chronic shoulder or neck pain, and implications for rehabilitation exercises 2. Shoulder impingement: can one label satisfy everything? 3. Central pain processing in shoulder pain 4. Progression in biceps load during rehabilitation exercises 5. The influence of induced shoulder muscle pain on rotator cuff and scapulothoracic muscle activity during elevation of the arm.

97 Shoulder impingement: can one label satisfy everything?
98 99


99 Subacromial Impingement Syndrome (Neer) diagnostic: structural impingement of the structures in the subacromial space controversial: does not fully explain the mechanism Impingement related shoulder pain = Impingement = cluster of symptoms and possible mechanism for pain, rather than pathoanatomic diagnose itself


100 SURGERY VERSUS PHYSIOTHERAPY Structural anatomy, pathoanatomical diagnostic labels Movement-related impairments (motor control, soft tissue strength, flexibility, functional osteokinematics and arthrokinematics)
101 SIS as diagnostic label Diagnostic labels based on tissue-specific pathology fail to accurately classify the patient into subgroups for clinical decision making
102 SIS as subacromial conflict Subacromial Pain Syndrome

103 Discussion on terminoloy: Subacromial pain syndrome Rotator cuff disease Anterolateral shoulder pain or shoulder pain of unknown aetiology => no single label to satisfy everyone and everything

104 Abandon perfect name for the problem & umbrella terminology Shoulder pain can be caused by several mechanisms: Bursa, rotator cuff, tendon failure, central sensitisation, muscle imbalances etc. No single label to cover all the mechanisms and pathologies associated with pain of the subacromial region

105 Non-traumatic shoulder pain is multifactoral We should not try to put all patients under the same umbrella the umbrella will never be big enough to keep every-one out of the rain Better to create several umbrellas to put our patients under and keep them dry

106 Classifying patients into subcategories like: flexibility deficits versus muscle dysfunction, high versus low irritability glenohumeral versus scapulothoracic impairment, strength deficits versus motor control impairment Etc. Labelling of patients, but also individually based approach
107 Overview 1. Analysis of recruitment of the superficial and deep scapular muscles in patients with chronic shoulder or neck pain, and implications for rehabilitation exercises 2. Shoulder impingement: can one label satisfy everything? 3. Central pain processing in shoulder pain 4. Progression in biceps load during rehabilitation exercises 5. The influence of induced shoulder muscle pain on rotator cuff and scapulothoracic muscle activity during elevation of the arm.



108 Central pain processing in shoulder pain? Despite the large group of individuals seeking for primary-care services, about 50% of patients with shoulder pain still report persistent pain after 12 months. Chronic shoulder pain often cannot be explained by an obvious anatomic defect or tissue damage
109 Central sensitization: = An amplification of neural signaling within the central nervous system that elicits pain hypersensitivity => minimal tissue damage or sensory input without tissue damage can be sufficient to trigger pain Sensitivity of the tissues can be altered within the injured area (primary hyperalgesia) but also in the adjacent, uninjured tissue (secondary hyperalgesia) Central sensitisation has already been found in various chronic pain populations including: Chronic Whiplash, Fibromyalgia, Carpal Tunnel Syndrome, Osteoarthritis, Tensiontype headache, temporomandibular joint pain


110 Central sensitization might play a role in a subgroup of these shoulder patients. Conclusion: In patients with musculoskeletal shoulder pain, there is involvement of the central nervous system

111 Conclusion: Although peripheral mechanisms are involved, hypersensitivity of the central nervous system plays a role in a subgroup within the shoulder pain population.
112 Evaluation of CS? No golden standard! Quantitative sensory testing Pain pressure tresholds Conditioned pain modulation Exercise-induced endogenous analgesia

113 Central sensitisation manifests itself at different degrees over a continuum from none at all to severe
114 Some evidence that psychological factors could be associated with prognosis of CSP Reilingh et al. (2008) Rheumatology investigated the course and prognosis of shoulder pain in the 6 first months after presentation to the GP. Predictors of a better outcome for CSP were lower scores on pain catastrophising and higher baseline pain intensity. Gill et al. (2013) ACR examined which factors are predictive of incident, recurrent or resolved shoulder pain in a community-based sample from the general population. Findings showed how recurrent shoulder pain was associated with depressive symptoms. Chester et al. (2016) BJSM aimed to identify which baseline patient and clinical characteristics are associated with a better outcome, 6 weeks and 6 months after starting a course of physiotherapy for shoulder pain. In this study, higher patient expectation of complete recovery compared to slight improvement because of physiotherapy and higher pain self-efficacy were associated with patient-rated outcomes. => psychological factors could play a role in people with shoulder pain and favour the perpetuation of chronic shoulder pain

115 Overview different questionnaires: Kinesiophobia and pain-related fear FACS: Fear Avoidance Components Scale Pain Catastrophizing PCS: Pain Catastrophising Scale Anxiety and Depression HADS: Hospital Anxiety and Depression Scale Patient expectations of recovery scale: How likely is it that within the next 3 months you will have resumed some form of recovery?
116 similar clinical presentation equal pain processing mechanisms underlying their symptoms => could explain why some patients fail to recover after standard treatment directed at peripheral targets.
117 Clinicians should be encouraged to identify patients with chronic shoulder pain who show psychological symptoms (beliefs, attitudes, expectations) in the preliminary assessment possibility to consider other therapeutic interventions rather than physical therapies for chronic shoulder pain





118 Pain neuroscience education => decreasing hyperexcitability of the central nervous system
119 Overview 1. Analysis of recruitment of the superficial and deep scapular muscles in patients with chronic shoulder or neck pain, and implications for rehabilitation exercises 2. Shoulder impingement: can one label satisfy everything? 3. Central pain processing in shoulder pain 4. Progression in biceps load during rehabilitation exercises 5. The influence of induced shoulder muscle pain on rotator cuff and scapulothoracic muscle activity during elevation of the arm.
120 Progression in biceps load during rehabilitation exercises => Help for the clinician for the nonoperative and postoperative treatment of biceps-related disorders and superior labrum anterior-posterior (SLAP) lesions in overhead athletes

121



122 SCAPULOTHORACIC MUSCLE GROUP

123 GLENOHUMERAL MUSCLE GROUP

124 BICEPS BRACHII


125 FUNCTIONAL DIAGONALS

126 EMG-measurements 1. UT 2. MT 3. LT 4. SA 5. AD 6. PD 7. BB 8. TB
127 (Cools et al. AJSM 2014)
128 <20% MVC: low activity 20-50%MVC: moderate >50%MVC: high activity Moderate: forward flexion in supination full can elbow flexion in forearm supi (Cools et al. AJSM 2014)
129 (Cools et al. AJSM 2014)
130 (Cools et al. AJSM 2014)
131 Exercises targeting the Trapezius result in less loads on the biceps muscle compared with exercises for the SA => might be preferred before SA training in patients with biceps-related pathological lesions.
132 (Cools et al. AJSM 2014)
133
134

135 (Cools et al. AJSM 2014)
136 Results? Effects of these exercises in patients with biceps related pathology? High level activity in biceps during exercises? A Cools SLAP 2016

137 Follow up study 2016 Exercise UT MT LT SA BB TB No. Mean SD Mean SD Mean SD Mean SD Mean SD Mean SD



138 139




139




140
141 Exercise UT MT LT SA BB TB No. Mean SD Mean SD Mean SD Mean SD Mean SD Mean SD <20% MVC: low activity 20-50%MVC: moderate >50%MVC: high activity
142 No % MVIC
143 No % MVIC
144 No % MVIC
145 No % MVIC Functionally contracting (elbow flexion in supination) the biceps muscle from an elongated position (shoulder in extension)
146 No % MVIC High velocity, explosive exercise
147 No % MVIC High velocity, explosive exercise
148 CONCLUSION Study describes a continuum of exercises with an increasing level of EMG activity in the BB Exercises targeting the Trapezius resulted in less loads on the biceps compared with exercises for the SA

149 Overview 1. Analysis of recruitment of the superficial and deep scapular muscles in patients with chronic shoulder or neck pain, and implications for rehabilitation exercises 2. Shoulder impingement: can one label satisfy everything? 3. Central pain processing in shoulder pain 4. Progression in biceps load during rehabilitation exercises 5. The influence of induced shoulder muscle pain on rotator cuff and scapulothoracic muscle activity during elevation of the arm.
150 151
151 CAUSE CONSEQUENCE? PAIN ALTERED MUSCLE RECRUITMENT 152
152 Experimental pain injection a bolus of 1 ml of hypertonic saline (5%) into the SS of the dominant arm the distribution of pain after the injection; similar to that described in patients with SIS. 153
153 EVALUATION OF THE EFFECT OF EXPERIMENTAL SHOULDER PAIN ON THE ACTIVITY OF THE GLENOHUMERAL AND SCAPULOTHORACIC MUSCLES DURING THE PERFORMANCE OF AN ELEVATION TASK IN THE SCAPULAR PLANE 154
154 Muscle functional MRI - Non invasive technique based on the differences in water relaxation values (T2 relaxation of the muscles) of the muscles - Activity of the muscles: acute activity-induced increase in T2 relaxation times => The shifts in T2 values upon exercise relate to the amount of work performed by the muscle 155


155 156


156 Exercise 157
157 METHODS - 25 healthy individuals, performing elevation in the scapular plane (3 sets of 10 reps) - Tested under 2 conditions: first without pain and then with experimental shoulder pain 158

158 Exercise MR image at rest Exercise MRI image while having muscle pain MRI image 159
159 Scans were obtained at 4 different levels, parallel to: C6-C7 T2-T3 T3-T4 T6-T7 160
160 Figure 1 Region of interest (red outline) for the upper trapezius (UT) muscle in the T2-weighted (T2 map) image at the level parallel to C6-C7. 161
 muscles in the T2-weighted (T2 map) image at the level parallel to")
161 Figure 2 Region of interest (red outline) for the supraspinatus (SS) and middle trapezius (MT) muscles in the T2-weighted (T2 map) image at the level parallel to T2-T3. 162
 muscles in the T2-weighted (T2 map) image at the level parallel")
162 Figure 3 Region of interest (red outline) for the subscapularis (SUB) and infraspinatus (IS) muscles in the T2-weighted (T2 map) image at the level parallel to T3-T4. 163
163 Figure 4 Region of interest (red outline) for the serratus anterior (SA) and lower trapezius (LT) muscle in the T2-weighted (T2 map) image at the level parallel to T6-T7. 164
164 165

165 166

166 167

167 ROLE OF M. INFRASPINATUS - stabilizes the humeral head during arm elevation - depresses humeral head to avoid contact and impact with coracoacromial arch INHIBITION OF INFRASPINATUS? => Inefficient humeral head depression during humeral elevation leading to shoulder impingement 168
168 Acute experimental pain? different from chronic pain or acute traumatic pain 169
169 CONCLUSION Acute experimental shoulder pain has an inhibitory effect on the activity of the IS (reduction in T2 shift) during elevation of the arm Possible implications: rotator cuff muscle function (IS) should be a consideration in the early managing of patients with shoulder pain 170
170 Any questions? 171
SHOULDER REHABILITATION PART II
 SHOULDER REHABILITATION PART II Ann Cools, PT, PhD Ghent University - Belgium Dept of Rehabilitation Sciences & Physiotherapy Ann.Cools@UGent.be Shoulder rehab course level I Shoulder pathology and clinical
SHOULDER REHABILITATION PART II Ann Cools, PT, PhD Ghent University - Belgium Dept of Rehabilitation Sciences & Physiotherapy Ann.Cools@UGent.be Shoulder rehab course level I Shoulder pathology and clinical
REMINDER. an exercise program. Senior Fitness Obtain medical clearance and physician s release prior to beginning
 Functional Forever: Exercise for Independent Living REMINDER Obtain medical clearance and physician s release prior to beginning an exercise program for clients with medical or orthopedic concerns. What
Functional Forever: Exercise for Independent Living REMINDER Obtain medical clearance and physician s release prior to beginning an exercise program for clients with medical or orthopedic concerns. What
Returning the Shoulder Back to Optimal Function. Scapula. Clavicle. Humerus. Bones of the Shoulder (Osteology) Joints of the Shoulder (Arthrology)
 Joints of the Shoulder (Arthrology)") Returning the Shoulder Back to Optimal Function Sternum Clavicle Ribs Scapula Humerus Bones of the Shoulder (Osteology) By Rick Kaselj Clavicle Scapula Medial Left Anterior Clavicle Inferior View 20 degree
Returning the Shoulder Back to Optimal Function Sternum Clavicle Ribs Scapula Humerus Bones of the Shoulder (Osteology) By Rick Kaselj Clavicle Scapula Medial Left Anterior Clavicle Inferior View 20 degree
REMINDER. Obtain medical clearance and physician s release prior to beginning an exercise program for clients with medical or orthopedic concerns
 Understanding Shoulder Dysfunction REMINDER Obtain medical clearance and physician s release prior to beginning an exercise program for clients with medical or orthopedic concerns What is a healthy shoulder?
Understanding Shoulder Dysfunction REMINDER Obtain medical clearance and physician s release prior to beginning an exercise program for clients with medical or orthopedic concerns What is a healthy shoulder?
APPENDIX: The Houston Astros Stretching Program
 Vol. 35, No. 4, 2007 Glenohumeral Internal Rotation Deficits 1 APPENDIX: The Houston Astros Stretching Program Our Flexibility program consists of 5 positions. Four of the 5 have 2 variations of each position.
Vol. 35, No. 4, 2007 Glenohumeral Internal Rotation Deficits 1 APPENDIX: The Houston Astros Stretching Program Our Flexibility program consists of 5 positions. Four of the 5 have 2 variations of each position.
Review shoulder anatomy Review the physical exam of the shoulder Discuss some common causes of acute shoulder pain Discuss some common causes of
 Review shoulder anatomy Review the physical exam of the shoulder Discuss some common causes of acute shoulder pain Discuss some common causes of chronic shoulder pain Review with some case questions Bones:
Review shoulder anatomy Review the physical exam of the shoulder Discuss some common causes of acute shoulder pain Discuss some common causes of chronic shoulder pain Review with some case questions Bones:
Throwing Athlete Rehabilitation. Brett Schulz LAT/CMSS Sport and Spine Physical Therapy
 Throwing Athlete Rehabilitation Brett Schulz LAT/CMSS Sport and Spine Physical Therapy Disclosure No conflicts to disclose Throwing Athlete Dilemma The shoulder must have enough range of motion to allow
Throwing Athlete Rehabilitation Brett Schulz LAT/CMSS Sport and Spine Physical Therapy Disclosure No conflicts to disclose Throwing Athlete Dilemma The shoulder must have enough range of motion to allow
Secrets and Staples of Training the Athletic Shoulder
 Secrets and Staples of Training the Athletic Shoulder Eric Beard Corrective Exercise Specialist Athletic Performance Enhancement Specialist EricBeard.com AthleticShoulder.com Presentation Overview Rationale
Secrets and Staples of Training the Athletic Shoulder Eric Beard Corrective Exercise Specialist Athletic Performance Enhancement Specialist EricBeard.com AthleticShoulder.com Presentation Overview Rationale
Tendinosis & Subacromial Impingement Syndrome. Gene Desepoli, LMT, D.C.
 Tendinosis & Subacromial Impingement Syndrome Gene Desepoli, LMT, D.C. What is the shoulder joint? Shoulder joint or shoulder region? There is an interrelatedness of all moving parts of the shoulder and
Tendinosis & Subacromial Impingement Syndrome Gene Desepoli, LMT, D.C. What is the shoulder joint? Shoulder joint or shoulder region? There is an interrelatedness of all moving parts of the shoulder and
DIFFERENTIAL DIAGNOSIS: Looking for the causes of impingement
 DIFFERENTIAL DIAGNOSIS: Looking for the causes of Ann Cools, PT, PhD Ghent University - Belgium Dept of Rehabilitation Sciences & Physiotherapy Ann.Cools@UGent.be «thinking about.» Which special tests
DIFFERENTIAL DIAGNOSIS: Looking for the causes of Ann Cools, PT, PhD Ghent University - Belgium Dept of Rehabilitation Sciences & Physiotherapy Ann.Cools@UGent.be «thinking about.» Which special tests
Describe methods to evaluate for scapular. Perform a scapular dyskinesis examination. With humeral elevation, the scapula:
 Describe methods to evaluate for scapular dyskinesis Perform a scapular dyskinesis examination Lori Michener, PhD, PT, ATC Virginia Commonwealth University Richmond, VA Ant / Post Tilting Internal / External
Describe methods to evaluate for scapular dyskinesis Perform a scapular dyskinesis examination Lori Michener, PhD, PT, ATC Virginia Commonwealth University Richmond, VA Ant / Post Tilting Internal / External
Shoulder Joint Examination. Shoulder Joint Examination. Inspection. Inspection Palpation Movement. Look Feel Move
 Shoulder Joint Examination History Cuff Examination Instability Examination AC Joint Examination Biceps Tendon Examination Superior Labrum Examination Shoulder Joint Examination Inspection Palpation Movement
Shoulder Joint Examination History Cuff Examination Instability Examination AC Joint Examination Biceps Tendon Examination Superior Labrum Examination Shoulder Joint Examination Inspection Palpation Movement
Rehabilitation of Overhead Shoulder Injuries
 Rehabilitation of Overhead Shoulder Injuries 16 th Annual Primary Care Orthopaedic & Sports Medicine Symposium January 29, 2016 Jeremy Sherman, PT, MPT Disclosures No financial disclosures to note. Jeremy
Rehabilitation of Overhead Shoulder Injuries 16 th Annual Primary Care Orthopaedic & Sports Medicine Symposium January 29, 2016 Jeremy Sherman, PT, MPT Disclosures No financial disclosures to note. Jeremy
Lab Workbook. ANATOMY Manual Muscle Testing Lower Trapezius Patient: prone
 ANATOMY Manual Muscle Testing Lower Trapezius Patient: prone Lab Workbook Fixation: place on hand below the scapula on the opposite side Test: adduction and depression of the scapula with lateral rotation
ANATOMY Manual Muscle Testing Lower Trapezius Patient: prone Lab Workbook Fixation: place on hand below the scapula on the opposite side Test: adduction and depression of the scapula with lateral rotation
Musculoskeletal dysfunctions associated with swimmer s shoulder
 Musculoskeletal dysfunctions associated with swimmer s shoulder SURPRISING? Control Strength Endurance Mobility Elite swimmers: 14km/day 2500 shoulder revolution/day 16 000 shoulder revolutions/week Shoulder
Musculoskeletal dysfunctions associated with swimmer s shoulder SURPRISING? Control Strength Endurance Mobility Elite swimmers: 14km/day 2500 shoulder revolution/day 16 000 shoulder revolutions/week Shoulder
IMPINGEMENT-TESTSTESTS
 «thinking about.» DIFFERENTIAL DIAGNOSIS: Looking for the causes of Which special tests do you use in your shoulder examination? Ann Cools, PT, PhD Ghent University - Belgium Dept of Rehabilitation Sciences
«thinking about.» DIFFERENTIAL DIAGNOSIS: Looking for the causes of Which special tests do you use in your shoulder examination? Ann Cools, PT, PhD Ghent University - Belgium Dept of Rehabilitation Sciences
11/6/2013. Keely Behning, PT, SCS, ATC MNPTA Fall Conference November 16, 2013
 Keely Behning, PT, SCS, ATC MNPTA Fall Conference November 16, 2013 Upon completion of this course, attendees should be able to: Understand pertinent anatomy and biomechanics as they relate to specific
Keely Behning, PT, SCS, ATC MNPTA Fall Conference November 16, 2013 Upon completion of this course, attendees should be able to: Understand pertinent anatomy and biomechanics as they relate to specific
Joint G*H. Joint S*C. Joint A*C. Labrum. Humerus. Sternum. Scapula. Clavicle. Thorax. Articulation. Scapulo- Thoracic
 A*C Joint Scapulo- Thoracic Articulation Thorax Sternum Clavicle Scapula Humerus S*C Joint G*H Joint Labrum AC Ligaments SC Ligaments SC JOINT AC Coracoacromial GH GH Ligament Complex Coracoclavicular
A*C Joint Scapulo- Thoracic Articulation Thorax Sternum Clavicle Scapula Humerus S*C Joint G*H Joint Labrum AC Ligaments SC Ligaments SC JOINT AC Coracoacromial GH GH Ligament Complex Coracoclavicular
Shoulder: Clinical Anatomy, Kinematics & Biomechanics
 Shoulder: Clinical Anatomy, Kinematics & Biomechanics Dr. Alex K C Poon Department of Orthopaedics & Traumatology Pamela Youde Nethersole Eastern Hospital Clinical Anatomy the application of anatomy to
Shoulder: Clinical Anatomy, Kinematics & Biomechanics Dr. Alex K C Poon Department of Orthopaedics & Traumatology Pamela Youde Nethersole Eastern Hospital Clinical Anatomy the application of anatomy to
Core deconditioning Smoking Outpatient Phase 1 ROM Other
 whereby the ball does not stay properly centered in the shoulder socket during shoulder movement. This condition may be associated with impingement of the rotator cuff on the acromion bone and coracoacromial
whereby the ball does not stay properly centered in the shoulder socket during shoulder movement. This condition may be associated with impingement of the rotator cuff on the acromion bone and coracoacromial
Get Rhythm or what s the link between scapular dyskinesis and Algorithm?
 Get Rhythm or what s the link between scapular dyskinesis and Algorithm? Rehabilitation of scapular dyskinesis: from the office worker to the elite overhead athlete Adapted Critical appraised Paper and
Get Rhythm or what s the link between scapular dyskinesis and Algorithm? Rehabilitation of scapular dyskinesis: from the office worker to the elite overhead athlete Adapted Critical appraised Paper and
ER + IR = Total Motion
 Treating the Thrower s Shoulder Michael M. Reinold, PT, DPT, ATC, CSCS Introduction Common site of injury» Repetitive forces / stresses Tremendous joint forces» Anterior shear forces 1-1.5 1.5 X BW» Distraction
Treating the Thrower s Shoulder Michael M. Reinold, PT, DPT, ATC, CSCS Introduction Common site of injury» Repetitive forces / stresses Tremendous joint forces» Anterior shear forces 1-1.5 1.5 X BW» Distraction
CLINICAL EXAMINATION OF THE SHOULDER JOINT 대한신경근골격연구회 분당제생병원재활의학과 박준성
 CLINICAL EXAMINATION OF THE SHOULDER JOINT 대한신경근골격연구회 분당제생병원재활의학과 박준성 Clinical Examination of the Shoulder Good history, full clinical examination Detailed knowledge of the anatomy solve the majority of
CLINICAL EXAMINATION OF THE SHOULDER JOINT 대한신경근골격연구회 분당제생병원재활의학과 박준성 Clinical Examination of the Shoulder Good history, full clinical examination Detailed knowledge of the anatomy solve the majority of
Labral Tears. Fig 1: Intact labrum and biceps tendon
 Labral Tears What is it? The shoulder joint is a ball and socket joint, with the humeral head (upper arm bone) as the ball and the glenoid as the socket. The glenoid (socket) is a shallow bone that is
Labral Tears What is it? The shoulder joint is a ball and socket joint, with the humeral head (upper arm bone) as the ball and the glenoid as the socket. The glenoid (socket) is a shallow bone that is
Strength and muscle activity of shoulder external rotation of subjects with and
 Strength and muscle activity of shoulder external rotation of subjects with and without scapular dyskinesis DAISUKE UGA, RPT, MS 1,2), RIE NAKAZAWA, RPT, PhD 2), MASAAKI SAKAMOTO, RPT, PhD 2) 1) Jobu Hospital
Strength and muscle activity of shoulder external rotation of subjects with and without scapular dyskinesis DAISUKE UGA, RPT, MS 1,2), RIE NAKAZAWA, RPT, PhD 2), MASAAKI SAKAMOTO, RPT, PhD 2) 1) Jobu Hospital
Management of Shoulder Pain in Persons with SCI
 www.fisiokinesiterapia.biz Management of Shoulder Pain in Persons with SCI Research Program Development from a Clinical Perspective Identification of the problem Identification of potential cause Development
www.fisiokinesiterapia.biz Management of Shoulder Pain in Persons with SCI Research Program Development from a Clinical Perspective Identification of the problem Identification of potential cause Development
Continuing Education: Shoulder Stability
 Continuing Education: Shoulder Stability Anatomy & Kinesiology: The GHJ consists of the articulation of three bones: the scapula, clavicle and humerus. The scapula has three protrusions: the coracoid,
Continuing Education: Shoulder Stability Anatomy & Kinesiology: The GHJ consists of the articulation of three bones: the scapula, clavicle and humerus. The scapula has three protrusions: the coracoid,
SLAP LESION REPAIR PROTOCOL
 SLAP LESION REPAIR PROTOCOL Clarkstown Division This rehabilitation protocol has been developed for the patient following a SLAP (Superior Labrum Anterior Posterior) repair. It is extremely important to
SLAP LESION REPAIR PROTOCOL Clarkstown Division This rehabilitation protocol has been developed for the patient following a SLAP (Superior Labrum Anterior Posterior) repair. It is extremely important to
Rehabilitation Guidelines for Labral/Bankert Repair
 Rehabilitation Guidelines for Labral/Bankert Repair The true shoulder joint is called the glenohumeral joint and consists humeral head and the glenoid. It is a ball and socket joint. Anatomy of the Shoulder
Rehabilitation Guidelines for Labral/Bankert Repair The true shoulder joint is called the glenohumeral joint and consists humeral head and the glenoid. It is a ball and socket joint. Anatomy of the Shoulder
Nonoperative Treatment For Rotator Cuff Tendinitis/ Partial Thickness Tear Dr. Trueblood
 Nonoperative Treatment For Rotator Cuff Tendinitis/ Partial Thickness Tear Dr. Trueblood Relieving Pain Patients who present with SIS will have shoulder pain that is exacerbated with overhead activities.
Nonoperative Treatment For Rotator Cuff Tendinitis/ Partial Thickness Tear Dr. Trueblood Relieving Pain Patients who present with SIS will have shoulder pain that is exacerbated with overhead activities.
[12]. 100 subjects. The sampling method used was purposive sampling. Fifty gymers and fifty matched non gymers were
![[12]. 100 subjects. The sampling method used was purposive sampling. Fifty gymers and fifty matched non gymers were](/thumbs/90/103918912.jpg "[12]. 100 subjects. The sampling method used was purposive sampling. Fifty gymers and fifty matched non gymers were") To Study the Prevalence of Scapular Dyskinesia in Gymers and Non Gymers Divya Khare 1, Supriya Vinay Deshmukh 2 Associate Professor, Physiotherapy Department, Ayushman College, Bhopal [Madhya Pradesh],
To Study the Prevalence of Scapular Dyskinesia in Gymers and Non Gymers Divya Khare 1, Supriya Vinay Deshmukh 2 Associate Professor, Physiotherapy Department, Ayushman College, Bhopal [Madhya Pradesh],
The Shoulder. Anatomy and Injuries PSK 4U Unit 3, Day 4
 The Shoulder Anatomy and Injuries PSK 4U Unit 3, Day 4 Shoulder Girdle Shoulder Complex is the most mobile joint in the body. Scapula Clavicle Sternum Humerus Rib cage/thorax Shoulder Girdle It also includes
The Shoulder Anatomy and Injuries PSK 4U Unit 3, Day 4 Shoulder Girdle Shoulder Complex is the most mobile joint in the body. Scapula Clavicle Sternum Humerus Rib cage/thorax Shoulder Girdle It also includes
Disclosures. Training for the Scapulothoracic Joint and Thoracic Spine. Scapular Muscles Stabilization & Rotation 9/7/2018
 Disclosures Training for the Scapulothoracic Joint and Thoracic Spine mtrigger Litecure Russ Paine, PT Director -UT Physicians Sportsmedicine Rehabilitation Houston, Texas 21 academic institutions 14 hospitals
Disclosures Training for the Scapulothoracic Joint and Thoracic Spine mtrigger Litecure Russ Paine, PT Director -UT Physicians Sportsmedicine Rehabilitation Houston, Texas 21 academic institutions 14 hospitals
INSTRUCTION MANUAL FOR THE FLEXTEND AC Exercise System for The Acromioclavicular (AC) / Shoulder Joint
 / Shoulder Joint") INSTRUCTION MANUAL FOR THE FLEXTEND AC Exercise System for The Acromioclavicular (AC) / Shoulder Joint FLEXTEND -AC: Congratulations! You have chosen to use the FLEXTEND -AC Upper Extremity Training System,
INSTRUCTION MANUAL FOR THE FLEXTEND AC Exercise System for The Acromioclavicular (AC) / Shoulder Joint FLEXTEND -AC: Congratulations! You have chosen to use the FLEXTEND -AC Upper Extremity Training System,
SLAP LESION REPAIR PROTOCOL Dr. Steven Flores
 SLAP LESION REPAIR PROTOCOL Dr. Steven Flores This rehabilitation protocol has been developed for the patient following a SLAP (Superior Labrum Anterior Posterior) repair. It is extremely important to
SLAP LESION REPAIR PROTOCOL Dr. Steven Flores This rehabilitation protocol has been developed for the patient following a SLAP (Superior Labrum Anterior Posterior) repair. It is extremely important to
Orthopedic Physical Assessment with Special Tests Shoulder
 Orthopedic Physical Assessment with Special Tests Shoulder COURSE DESCRIPTION Detailed video demonstrations of tests and procedures common in musculoskeletal assessment are supplemented by high-quality
Orthopedic Physical Assessment with Special Tests Shoulder COURSE DESCRIPTION Detailed video demonstrations of tests and procedures common in musculoskeletal assessment are supplemented by high-quality
Physical Examination of the Shoulder
 General setup Patient will be examined in both the seated and supine position so exam table needed 360 degree access to patient Expose neck and both shoulders (for comparison); female in gown or sports
General setup Patient will be examined in both the seated and supine position so exam table needed 360 degree access to patient Expose neck and both shoulders (for comparison); female in gown or sports
Overuse Injuries. Overuse injury defined. Overuse Injuries
 Overuse Injuries Lisa DeStefano, DO Associate Professor and Chair Department of Osteopathic Manipulative Medicine College of Osteopathic Medicine Michigan State University Overuse injury defined Overuse
Overuse Injuries Lisa DeStefano, DO Associate Professor and Chair Department of Osteopathic Manipulative Medicine College of Osteopathic Medicine Michigan State University Overuse injury defined Overuse
Evaluation & Treatment of the Scapula in Athletes: How Important is the Scapula Kevin E Wilk, PT, DPT,FAPTA
 Evaluation & Treatment of the Scapula in Athletes: How Important is the Scapula Kevin E Wilk, PT, DPT,FAPTA Kevin E Wilk, PT, DPT,FAPTA 2016 Baseball Sports Medicine Conference Faculty Disclosure: Theralase
Evaluation & Treatment of the Scapula in Athletes: How Important is the Scapula Kevin E Wilk, PT, DPT,FAPTA Kevin E Wilk, PT, DPT,FAPTA 2016 Baseball Sports Medicine Conference Faculty Disclosure: Theralase
S p o r t s & O r t h o p a e d i c S p e c i a l i s t s A n t e r i o r I n s t a b i l i t y P r o t o c o l
 S p o r t s & O r t h o p a e d i c S p e c i a l i s t s This protocol provides appropriate guidelines for the rehabilitation of patients with anterior instability. The protocol draws evidence from the
S p o r t s & O r t h o p a e d i c S p e c i a l i s t s This protocol provides appropriate guidelines for the rehabilitation of patients with anterior instability. The protocol draws evidence from the
TIPS FOR SUCCESSFUL SHOULDER TREATMENT. In Service Training 16 th May 2014
 TIPS FOR SUCCESSFUL SHOULDER TREATMENT In Service Training 16 th May 2014 Training day aims to address: Controversies of impingement syndrome diagnosis Controversies of MRI/USS imaging Clinical diagnosis
TIPS FOR SUCCESSFUL SHOULDER TREATMENT In Service Training 16 th May 2014 Training day aims to address: Controversies of impingement syndrome diagnosis Controversies of MRI/USS imaging Clinical diagnosis
A science-based protocol for the conservative and postoperative treatment of SLAP LESIONS & BICEPS PATHOLOGY
 A science-based protocol for the conservative and postoperative treatment of SLAP LESIONS & BICEPS PATHOLOGY Prof dr Ann Cools, PT, PhD Dept Rehab. Sciences & Physiotherapy Ghent University, Belgium From
A science-based protocol for the conservative and postoperative treatment of SLAP LESIONS & BICEPS PATHOLOGY Prof dr Ann Cools, PT, PhD Dept Rehab. Sciences & Physiotherapy Ghent University, Belgium From
Burwood Road, Concord 160 Belmore Road, Randwick
 www.orthosports.com.au 47 49 Burwood Road, Concord 160 Belmore Road, Randwick Conservative management of subacromial pathology Mel Cusi MBBS, Cert Sp Med, FACSP, FFSEM (UK) Presenting symptoms Shoulder
www.orthosports.com.au 47 49 Burwood Road, Concord 160 Belmore Road, Randwick Conservative management of subacromial pathology Mel Cusi MBBS, Cert Sp Med, FACSP, FFSEM (UK) Presenting symptoms Shoulder
Shoulder Instability. Fig 1: Intact labrum and biceps tendon
 Shoulder Instability What is it? The shoulder joint is a ball and socket joint, with the humeral head (upper arm bone) as the ball and the glenoid as the socket. The glenoid (socket) is a shallow bone
Shoulder Instability What is it? The shoulder joint is a ball and socket joint, with the humeral head (upper arm bone) as the ball and the glenoid as the socket. The glenoid (socket) is a shallow bone
Vol 3, 2008 CEC ARTICLE: Special Medical Conditions Part 2: Shoulder Maintenance and Rehab C. Eggers
 Vol 3, 2008 CEC ARTICLE: Special Medical Conditions Part 2: Shoulder Maintenance and Rehab C. Eggers SHOULDER GIRDLE STABILIZATION Knowledge of the anatomy and biomechanics of the shoulder girdle is essential
Vol 3, 2008 CEC ARTICLE: Special Medical Conditions Part 2: Shoulder Maintenance and Rehab C. Eggers SHOULDER GIRDLE STABILIZATION Knowledge of the anatomy and biomechanics of the shoulder girdle is essential
Conservative Massive Rotator Cuff Tear Protocol
 SPORTS & ORTHOPAEDIC SPECIALISTS Conservative Massive Rotator Cuff Tear Protocol 3-4 visits over 4-6 weeks Emphasis is on AAROM and a high repetition, low weight free weight program Emphasize improved
SPORTS & ORTHOPAEDIC SPECIALISTS Conservative Massive Rotator Cuff Tear Protocol 3-4 visits over 4-6 weeks Emphasis is on AAROM and a high repetition, low weight free weight program Emphasize improved
Scapular and Deltoid Regions
 M1 Gross and Developmental Anatomy Scapular and Deltoid Regions Dr. Peters 1 Outline I. Skeleton of the Shoulder and Attachment of the Upper Extremity to Trunk II. Positions and Movements of the Scapula
M1 Gross and Developmental Anatomy Scapular and Deltoid Regions Dr. Peters 1 Outline I. Skeleton of the Shoulder and Attachment of the Upper Extremity to Trunk II. Positions and Movements of the Scapula
Biceps Tenodesis Protocol
 Biceps Tenodesis Protocol A biceps tenodesis procedure involves cutting of the long head of the biceps just prior to its insertion on the superior labrum and then anchoring the tendon along its anatomical
Biceps Tenodesis Protocol A biceps tenodesis procedure involves cutting of the long head of the biceps just prior to its insertion on the superior labrum and then anchoring the tendon along its anatomical
RN(EC) ENC(C) GNC(C) MN ACNP *** MECHANISM OF INJURY.. MOST IMPORTANT ***
 ENC(C) GNC(C) MN ACNP *** MECHANISM OF INJURY.. MOST IMPORTANT ***") HISTORY *** MECHANISM OF INJURY.. MOST IMPORTANT *** Age - Certain conditions are more prevalent in particular age groups (i.e. Full rotator cuff tears are more common over the age of 45, traumatic injuries
HISTORY *** MECHANISM OF INJURY.. MOST IMPORTANT *** Age - Certain conditions are more prevalent in particular age groups (i.e. Full rotator cuff tears are more common over the age of 45, traumatic injuries
Shoulder Impingement Rehabilitation Recommendations
 Shoulder Impingement Rehabilitation Recommendations The following protocol can be utilized for conservative care of shoulder impingement as well as post- operative subacromial decompression (SAD) surgery.
Shoulder Impingement Rehabilitation Recommendations The following protocol can be utilized for conservative care of shoulder impingement as well as post- operative subacromial decompression (SAD) surgery.
FUNCTIONAL ANATOMY OF SHOULDER JOINT
 FUNCTIONAL ANATOMY OF SHOULDER JOINT ARTICULATION Articulation is between: The rounded head of the Glenoid cavity humerus and The shallow, pear-shaped glenoid cavity of the scapula. 2 The articular surfaces
FUNCTIONAL ANATOMY OF SHOULDER JOINT ARTICULATION Articulation is between: The rounded head of the Glenoid cavity humerus and The shallow, pear-shaped glenoid cavity of the scapula. 2 The articular surfaces
Rotator Cuff Repair Protocol for tear involving Subscapularis Tendon with or without Pectoralis Major Tendon Transfer
 Rotator Cuff Repair Protocol for tear involving Subscapularis Tendon with or without Pectoralis Major Tendon Transfer D. WATTS, MD Precautions: BASIS Tendon healing back to bone is a slow process that
Rotator Cuff Repair Protocol for tear involving Subscapularis Tendon with or without Pectoralis Major Tendon Transfer D. WATTS, MD Precautions: BASIS Tendon healing back to bone is a slow process that
Scapular Assessment & Dyskinesis: What s Relevant?
 Scapular Assessment & Dyskinesis: What s Relevant? Jesse Awenus PT, MSc.PT, Dip.Manip.PT, FCAMPT, Cert. DN Registered Physiotherapist Director of Rehabilitation at Synergy Sports Medicine & Rehabilitation
Scapular Assessment & Dyskinesis: What s Relevant? Jesse Awenus PT, MSc.PT, Dip.Manip.PT, FCAMPT, Cert. DN Registered Physiotherapist Director of Rehabilitation at Synergy Sports Medicine & Rehabilitation
Disclosure/Objectives. Movement System Diagnostic Classification for the Painful Shoulder. Pathoanatomic Diagnostic Labels. Why Classify?
 Movement System Diagnostic Classification for the Painful Shoulder Paula M Ludewig, PhD, PT, FAPTA Divisions of Physical Therapy & Rehabilitation Science Department of Rehabilitation Medicine Allina Health
Movement System Diagnostic Classification for the Painful Shoulder Paula M Ludewig, PhD, PT, FAPTA Divisions of Physical Therapy & Rehabilitation Science Department of Rehabilitation Medicine Allina Health
Scapular Dyskinesis. Orthopaedic Update 2018 April 15, Peter Tang, MD, MPH, FAOA
 Scapular Dyskinesis Orthopaedic Update 2018 April 15, 2018 Peter Tang, MD, MPH, FAOA Director Center for Brachial Plexus and Nerve Injury Program Director Hand, Upper Extremity & Microvascular Surgery
Scapular Dyskinesis Orthopaedic Update 2018 April 15, 2018 Peter Tang, MD, MPH, FAOA Director Center for Brachial Plexus and Nerve Injury Program Director Hand, Upper Extremity & Microvascular Surgery
Shoulder Biomechanics
 Shoulder Biomechanics Lecture originally developed by Bryan Morrison, Ph.D. candidate Arizona State University Fall 2000 1 Outline Anatomy Biomechanics Problems 2 Shoulder Complex Greatest Greatest Predisposition
Shoulder Biomechanics Lecture originally developed by Bryan Morrison, Ph.D. candidate Arizona State University Fall 2000 1 Outline Anatomy Biomechanics Problems 2 Shoulder Complex Greatest Greatest Predisposition
Theodore B. Shybut, M.D.
 Theodore B. Shybut, M.D. Orthopedics and Sports Medicine 7200 Cambridge St. #10A Houston, Texas 77030 Non-operative Shoulder Rehabilitation Protocol Basic shoulder program for: o Scapular Dyskinesis (proximally
Theodore B. Shybut, M.D. Orthopedics and Sports Medicine 7200 Cambridge St. #10A Houston, Texas 77030 Non-operative Shoulder Rehabilitation Protocol Basic shoulder program for: o Scapular Dyskinesis (proximally
2015 OPSC Annual Convention. syllabus. February 4-8, 2015 Hyatt Regency Mission Bay San Diego, California
 2015 OPSC Annual Convention syllabus February 4-8, 2015 Hyatt Regency Mission Bay San Diego, California THURSDAY, FEBRUARY 5, 2015: 3:30pm - 4:30pm The Shoulder: 2 View or Not 2 View * Presented by Alexandra
2015 OPSC Annual Convention syllabus February 4-8, 2015 Hyatt Regency Mission Bay San Diego, California THURSDAY, FEBRUARY 5, 2015: 3:30pm - 4:30pm The Shoulder: 2 View or Not 2 View * Presented by Alexandra
Anterior Stabilization of the Shoulder: Distal Tibial Allograft
 Anterior Stabilization of the Shoulder: Distal Tibial Allograft Name: Diagnosis: Date: Date of Surgery: Phase I Immediate Post Surgical Phase (approximately Weeks 1-3) Minimize shoulder pain and inflammatory
Anterior Stabilization of the Shoulder: Distal Tibial Allograft Name: Diagnosis: Date: Date of Surgery: Phase I Immediate Post Surgical Phase (approximately Weeks 1-3) Minimize shoulder pain and inflammatory
Exploring the Rotator Cuff
 Exploring the Rotator Cuff Improving one s performance in sports and daily activity is a factor of neuromuscular efficiency and metabolic enhancements. To attain proficiency, reaction force must be effectively
Exploring the Rotator Cuff Improving one s performance in sports and daily activity is a factor of neuromuscular efficiency and metabolic enhancements. To attain proficiency, reaction force must be effectively
Structure and Function of the Bones and Joints of the Shoulder Girdle
 Structure and Function of the Bones and Joints of the Shoulder Girdle LEARNING OBJECTIVES: At the end of this laboratory exercise the student will be able to: Palpate the important skeletal landmarks of
Structure and Function of the Bones and Joints of the Shoulder Girdle LEARNING OBJECTIVES: At the end of this laboratory exercise the student will be able to: Palpate the important skeletal landmarks of
Active-Assisted Stretches
 1 Active-Assisted Stretches Adequate flexibility is fundamental to a functional musculoskeletal system which represents the foundation of movement efficiency. Therefore a commitment toward appropriate
1 Active-Assisted Stretches Adequate flexibility is fundamental to a functional musculoskeletal system which represents the foundation of movement efficiency. Therefore a commitment toward appropriate
Eric Magrum PT, DPT, OCS, FAAOMPT Orthopaedic Manual Physical Therapy Series Charlottesville
 SHOULDER CASE 1 Eric Magrum PT, DPT, OCS, FAAOMPT Orthopaedic Manual Physical Therapy Series Charlottesville 2017-2018 Reproduction Without Consent 1 Prevalence Shoulder pain 2 nd to LBP prevalence MSK
SHOULDER CASE 1 Eric Magrum PT, DPT, OCS, FAAOMPT Orthopaedic Manual Physical Therapy Series Charlottesville 2017-2018 Reproduction Without Consent 1 Prevalence Shoulder pain 2 nd to LBP prevalence MSK
P ERFORMANCE CONDITIONING. Inside the Bermuda Triangle of Chronic Shoulder and Elbow Pain- Part IV
 P ERFORMANCE VOLLEYBALL CONDITIONING A NEWSLETTER DEDICATED TO IMPROVING VOLLEYBALL PLAYERS www.performancecondition.com/volleyball Inside the Bermuda Triangle of Chronic Shoulder and Elbow Pain- Part
P ERFORMANCE VOLLEYBALL CONDITIONING A NEWSLETTER DEDICATED TO IMPROVING VOLLEYBALL PLAYERS www.performancecondition.com/volleyball Inside the Bermuda Triangle of Chronic Shoulder and Elbow Pain- Part
Bradley C. Carofino, M.D. Shoulder Specialist 230 Clearfield Avenue, Suite 124 Virginia Beach, Virginia Phone
 Subpectoral Bicep Tenodesis Protocol (Spreadsheet) Weeks 1-2 Modalities Treatment Restrictions Goals No active elbow flexion (6weeks) Full PROM shoulder and elbow PROM: Shoulder, elbow, forearm No active
Subpectoral Bicep Tenodesis Protocol (Spreadsheet) Weeks 1-2 Modalities Treatment Restrictions Goals No active elbow flexion (6weeks) Full PROM shoulder and elbow PROM: Shoulder, elbow, forearm No active
Conservative Posterior Capsular Instability Protocol
 SPORTS & ORTHOPAEDIC SPECIALISTS Conservative Posterior Capsular Instability Protocol 4-6 visits over 6 weeks Primary instability often experiences secondary impingement. Therefore, to treat posterior
SPORTS & ORTHOPAEDIC SPECIALISTS Conservative Posterior Capsular Instability Protocol 4-6 visits over 6 weeks Primary instability often experiences secondary impingement. Therefore, to treat posterior
WEEKEND THREE HOMEWORK
 WEEKEND THREE HOMEWORK READING ASSIGNMENTS Salvo Massage Therapy Principles and Practice 4 th Edition Muscolino The Muscular System Manual Muscolino The Muscle and Bone Palpation Manual Ch. 19 Skeletal
WEEKEND THREE HOMEWORK READING ASSIGNMENTS Salvo Massage Therapy Principles and Practice 4 th Edition Muscolino The Muscular System Manual Muscolino The Muscle and Bone Palpation Manual Ch. 19 Skeletal
MOON SHOULDER GROUP NONOPERATIVE TREATMENT OF ROTATOR CUFF TENDONOPATHY PHYSICAL THERAPY GUIDELINES
 MOON SHOULDER GROUP NONOPERATIVE TREATMENT OF ROTATOR CUFF TENDONOPATHY PHYSICAL THERAPY GUIDELINES From: Kuhn JE. Exercise in the treatment of rotator cuff impingement. A systematic review and synthesized
MOON SHOULDER GROUP NONOPERATIVE TREATMENT OF ROTATOR CUFF TENDONOPATHY PHYSICAL THERAPY GUIDELINES From: Kuhn JE. Exercise in the treatment of rotator cuff impingement. A systematic review and synthesized
Diagnostic and Management Approach to the Painful Shoulder
 Diagnostic and Management Approach to the Painful Shoulder Introduction What conditions causing shoulder pain commonly present in General Practice? Subacromial impingement Rotator cuff tears AC joint pathology
Diagnostic and Management Approach to the Painful Shoulder Introduction What conditions causing shoulder pain commonly present in General Practice? Subacromial impingement Rotator cuff tears AC joint pathology
Integrating Sensorimotor Control Into Rehabilitation
 Integrating Sensorimotor Control Into Rehabilitation BRADY L. TRIPP, PhD, LAT, ATC Florida International University Key Points As evidence accumulates, so does our appreciation of the integral roles that
Integrating Sensorimotor Control Into Rehabilitation BRADY L. TRIPP, PhD, LAT, ATC Florida International University Key Points As evidence accumulates, so does our appreciation of the integral roles that
Acute Orthopaedic Injuries Developing a Diagnostic Approach to the Shoulder
 Acute Orthopaedic Injuries Developing a Diagnostic Approach to the Shoulder WWW.FISIOKINESITERAPIA.BIZ Overview To be able to quickly categorize shoulder injuries To take appropriate history and conduct
Acute Orthopaedic Injuries Developing a Diagnostic Approach to the Shoulder WWW.FISIOKINESITERAPIA.BIZ Overview To be able to quickly categorize shoulder injuries To take appropriate history and conduct
Clinical examination of the shoulder girdle
 Clinical of the shoulder girdle CHAPTER CONTENTS Symptoms referred to the shoulder girdle........ e72 Symptoms referred from the shoulder girdle...... e72 History........................... e72 Inspection.........................
Clinical of the shoulder girdle CHAPTER CONTENTS Symptoms referred to the shoulder girdle........ e72 Symptoms referred from the shoulder girdle...... e72 History........................... e72 Inspection.........................
Exercise for Reducing Neck Pain and Enhancing Dynamic Stability.
 Exercise for Reducing Neck Pain and Enhancing Dynamic Stability www.fisiokinesiterapia.biz Presentation Outline Compare/Contrast Lumbar Exercise Literature to Cervical Spine Discuss Neck Musculature and
Exercise for Reducing Neck Pain and Enhancing Dynamic Stability www.fisiokinesiterapia.biz Presentation Outline Compare/Contrast Lumbar Exercise Literature to Cervical Spine Discuss Neck Musculature and
SHOULDER INJURY PREVENTION FOR CLIMBERS - INTERVENTION BOOKLET
 2018 SHOULDER INJURY PREVENTION FOR CLIMBERS - INTERVENTION BOOKLET MÁRIA DANCSÓ INJURY PREVENTION Why? How? Shoulder injuries can cause pain, reduced function and prolonged periods away from the training.
2018 SHOULDER INJURY PREVENTION FOR CLIMBERS - INTERVENTION BOOKLET MÁRIA DANCSÓ INJURY PREVENTION Why? How? Shoulder injuries can cause pain, reduced function and prolonged periods away from the training.
Unit 8 SPECIFIC SPORTS INJURIES Upper Extremity Case Study
 Unit 8 SPECIFIC SPORTS INJURIES Upper Extremity Case Study Swimming Shoulder Pain Identifying the Source By Tamara Stelting, ATC As swimming season kicks into gear, many shoulders will start feeling fatigued
Unit 8 SPECIFIC SPORTS INJURIES Upper Extremity Case Study Swimming Shoulder Pain Identifying the Source By Tamara Stelting, ATC As swimming season kicks into gear, many shoulders will start feeling fatigued
Anterior Stabilization of the Shoulder: Latarjet Protocol
 Robert K. Fullick, MD 6400 Fannin Street, Suite 1700 Houston, Texas 77030 Ph.: 713-486-7543 / Fx.: 713-486-5549 Anterior Stabilization of the Shoulder: Latarjet Protocol The intent of this protocol is
Robert K. Fullick, MD 6400 Fannin Street, Suite 1700 Houston, Texas 77030 Ph.: 713-486-7543 / Fx.: 713-486-5549 Anterior Stabilization of the Shoulder: Latarjet Protocol The intent of this protocol is
Conservative Multi-Directional Capsular Instability Protocol
 SPORTS & ORTHOPAEDIC SPECIALISTS 8100 W. 78 th Street Edina, MN 55439 952-946-9777 www.womensorthocenter.com Conservative Multi-Directional Capsular Instability Protocol 4-6 visits over 6 weeks Primary
SPORTS & ORTHOPAEDIC SPECIALISTS 8100 W. 78 th Street Edina, MN 55439 952-946-9777 www.womensorthocenter.com Conservative Multi-Directional Capsular Instability Protocol 4-6 visits over 6 weeks Primary
BASIC ORTHOPEDIC ASSESSMENT Muscle and Joint Testing
 BASIC ORTHOPEDIC ASSESSMENT Muscle and Joint Testing The following tests are for the purpose of determining relative shortening, restriction or bind of muscle tissues. In this context the term bind in
BASIC ORTHOPEDIC ASSESSMENT Muscle and Joint Testing The following tests are for the purpose of determining relative shortening, restriction or bind of muscle tissues. In this context the term bind in
Welcome to. Not to be copied without the express permission of EDUCATA. Copyright 2014 EDUCATA. All rights reserved. 1. How to Navigate EDUCATA
 Welcome to Copyright 2014 EDUCATA. This presentation is not to be copied in whole or in part without the express permission of EDUCATA. How to Navigate EDUCATA The Shoulder Complex Mechanics, Muscle Function
Welcome to Copyright 2014 EDUCATA. This presentation is not to be copied in whole or in part without the express permission of EDUCATA. How to Navigate EDUCATA The Shoulder Complex Mechanics, Muscle Function
Cervical Radiculopathy: My 32 Year-Old Cyclist is Nervous What do I do on the initial visit?
 Cervical Radiculopathy: My 32 Year-Old Cyclist is Nervous What do I do on the initial visit? Scott D Boden, MD The Emory Spine Center Atlanta, Georgia History of Trauma? 2 History of Trauma? 3 Sometimes
Cervical Radiculopathy: My 32 Year-Old Cyclist is Nervous What do I do on the initial visit? Scott D Boden, MD The Emory Spine Center Atlanta, Georgia History of Trauma? 2 History of Trauma? 3 Sometimes
Anatomical Considerations/ Pathophysiology The shoulder is the most mobile joint in the body. : Three bones:
 Introduction Musculoskeletal training is generally underrepresented in medical training and residency curriculums. There is a general deficit in musculoskeletal knowledge amongst current medical students,
Introduction Musculoskeletal training is generally underrepresented in medical training and residency curriculums. There is a general deficit in musculoskeletal knowledge amongst current medical students,
Throwing Injuries and Prevention: The Physical Therapy Perspective
 Throwing Injuries and Prevention: The Physical Therapy Perspective Andrew M Jordan, PT, DPT, OCS Staff Physical Therapist, Cayuga Medical Center Physical Therapy and Sports Medicine ajordan@cayugamed.org
Throwing Injuries and Prevention: The Physical Therapy Perspective Andrew M Jordan, PT, DPT, OCS Staff Physical Therapist, Cayuga Medical Center Physical Therapy and Sports Medicine ajordan@cayugamed.org
Phase I : Immediate Postoperative Phase- Protected Motion. (0-2 Weeks)
") Phase I : Immediate Postoperative Phase- Protected Motion (0-2 Weeks) Appointments Progression Criteria 2 weeks after surgery Rehabilitation appointments begin within 7-10 days of surgery, continue 1-2
Phase I : Immediate Postoperative Phase- Protected Motion (0-2 Weeks) Appointments Progression Criteria 2 weeks after surgery Rehabilitation appointments begin within 7-10 days of surgery, continue 1-2
The Shoulder Complex. Anatomy. Articulations 12/11/2017. Oak Ridge High School Conroe, Texas. Clavicle Collar Bone Scapula Shoulder Blade Humerus
 The Shoulder Complex Oak Ridge High School Conroe, Texas Anatomy Clavicle Collar Bone Scapula Shoulder Blade Humerus Articulations Sternoclavicular SC joint. Sternum and Clavicle. Acromioclavicular AC
The Shoulder Complex Oak Ridge High School Conroe, Texas Anatomy Clavicle Collar Bone Scapula Shoulder Blade Humerus Articulations Sternoclavicular SC joint. Sternum and Clavicle. Acromioclavicular AC
Shoulder Injury Evaluation.
 Shoulder Injury Evaluation www.fisiokinesiterapia.biz Basic Anatomy & Kinesiology 3 Bone Structures Clavicle Scapula Humerus Evaluation Principles Always follow a standard progression Determine the target
Shoulder Injury Evaluation www.fisiokinesiterapia.biz Basic Anatomy & Kinesiology 3 Bone Structures Clavicle Scapula Humerus Evaluation Principles Always follow a standard progression Determine the target
Rehabilitation Guidelines for Large Rotator Cuff Repair
 Rehabilitation Guidelines for Large Rotator Cuff Repair The true shoulder joint is called the glenohumeral joint and consists humeral head and the glenoid. It is a ball and socket joint. Anatomy of the
Rehabilitation Guidelines for Large Rotator Cuff Repair The true shoulder joint is called the glenohumeral joint and consists humeral head and the glenoid. It is a ball and socket joint. Anatomy of the
Today s session. Common Problems in Rehab. UPPER BODY REHAB ESSENTIALS TIM KEELEY FILEX 2012
 Tim Keeley B.Phty, Cred.MDT, APA Principal Physiotherapist physiofitness.com.au facebook.com/physiofitness Today s session Essential list for the upper body Rehab starting point Focussing on activation,
Tim Keeley B.Phty, Cred.MDT, APA Principal Physiotherapist physiofitness.com.au facebook.com/physiofitness Today s session Essential list for the upper body Rehab starting point Focussing on activation,
Shoulder Injuries. Glenoid labrum injuries. SLAP Lesions
 Shoulder Injuries functional anatomy clinical perspective impingement rotator cuff injuries glenoid labrum injuries dislocation Glenoid labrum injuries SLAP lesions stable or unstable traction/compression
Shoulder Injuries functional anatomy clinical perspective impingement rotator cuff injuries glenoid labrum injuries dislocation Glenoid labrum injuries SLAP lesions stable or unstable traction/compression
The SUPPORT Trial: SUbacromial impingement syndrome and Pain: a randomised controlled trial Of exercise and injection
 The SUPPORT Trial: SUbacromial impingement syndrome and Pain: a randomised controlled trial Of exercise and injection SUPPORT Physiotherapy Intervention Training Manual Authors: Sue Jackson (SJ) Julie
The SUPPORT Trial: SUbacromial impingement syndrome and Pain: a randomised controlled trial Of exercise and injection SUPPORT Physiotherapy Intervention Training Manual Authors: Sue Jackson (SJ) Julie
SHOULDER PAIN LESSONS FROM THE SPORTS FIELD MOVEMENT RESTRICTIONS. Steve McCaig
 SHOULDER PAIN LESSONS FROM THE SPORTS FIELD MOVEMENT RESTRICTIONS 1 Steve McCaig Senior Physiotherapist England Development Programme, ECB, Loughborough, United Kingdom Throwing High forces upper limb
SHOULDER PAIN LESSONS FROM THE SPORTS FIELD MOVEMENT RESTRICTIONS 1 Steve McCaig Senior Physiotherapist England Development Programme, ECB, Loughborough, United Kingdom Throwing High forces upper limb
Upper Cross Syndrome: Assessment & Management in Family Practice HKDU Symposium Dec 2014
 Upper Cross Syndrome: Assessment & Management in Family Practice HKDU Symposium Dec 2014 Dr. Ngai Ho Yin Allen Family Medicine Specialist PGDipMusculoskeletal Medicine MBBS(HK), DCH(London), DFM(CUHK),
Upper Cross Syndrome: Assessment & Management in Family Practice HKDU Symposium Dec 2014 Dr. Ngai Ho Yin Allen Family Medicine Specialist PGDipMusculoskeletal Medicine MBBS(HK), DCH(London), DFM(CUHK),
ARTHROSCOPIC DECOMPRESSION PROTOCOL Dr. Steven Flores
 ARTHROSCOPIC DECOMPRESSION PROTOCOL Dr. Steven Flores This rehabilitation protocol has been developed for the patient following an arthroscopic decompression surgical procedure. The arthroscopic decompression
ARTHROSCOPIC DECOMPRESSION PROTOCOL Dr. Steven Flores This rehabilitation protocol has been developed for the patient following an arthroscopic decompression surgical procedure. The arthroscopic decompression
Evaluating shoulder injuries in primary care Bethany Reed, MSn, AGPCNP-BC One Medical Group
 Evaluating shoulder injuries in primary care Bethany Reed, MSn, AGPCNP-BC One Medical Group Disclosures There has been no commercial support or sponsorship for this program. The planners and presenters
Evaluating shoulder injuries in primary care Bethany Reed, MSn, AGPCNP-BC One Medical Group Disclosures There has been no commercial support or sponsorship for this program. The planners and presenters
Scapular function and dysfunction
 Scapular function and dysfunction - Impingement - Muscle detachment W. Ben Kibler, MD Medical director FUNCTION IMPINGEMENT REVISITED Is impingement always a diagnosis- isolated description of pathology
Scapular function and dysfunction - Impingement - Muscle detachment W. Ben Kibler, MD Medical director FUNCTION IMPINGEMENT REVISITED Is impingement always a diagnosis- isolated description of pathology
Biceps Tenotomy Protocol
 Biceps Tenotomy Protocol A biceps tenotomy procedure involves cutting of the long head of the biceps just prior to its insertion on the superior labrum. A biceps tenotomy is typically done when there is
Biceps Tenotomy Protocol A biceps tenotomy procedure involves cutting of the long head of the biceps just prior to its insertion on the superior labrum. A biceps tenotomy is typically done when there is
Biceps Tenodesis Protocol
 Robert K. Fullick, MD 6400 Fannin Street, Suite 1700 Houston, Texas 77030 Ph.: 713-486-7543 / Fx.: 713-486-5549 Biceps Tenodesis Protocol The intent of this protocol is to provide the clinician with a
Robert K. Fullick, MD 6400 Fannin Street, Suite 1700 Houston, Texas 77030 Ph.: 713-486-7543 / Fx.: 713-486-5549 Biceps Tenodesis Protocol The intent of this protocol is to provide the clinician with a
Using the Research to Improve our Management of Shoulder Pain. Ian Horsley PhD,MMACP, MCSP Technical Lead Physiotherapist (Upper Limb) EIS
 EIS") Using the Research to Improve our Management of Shoulder Pain Ian Horsley PhD,MMACP, MCSP Technical Lead Physiotherapist (Upper Limb) EIS Outline What do we call it? How can we reliably assess it? What
Using the Research to Improve our Management of Shoulder Pain Ian Horsley PhD,MMACP, MCSP Technical Lead Physiotherapist (Upper Limb) EIS Outline What do we call it? How can we reliably assess it? What
STEP #1: Anatomy STEP #2: Awareness STEP #3: Action
 Stabilize the Scapula in Three Easy Steps by NFPT Idea World 2016: Session 611 Saturday July 16th 7:30-9:20am Beverly Hosford, MA STEP #1: Anatomy STEP #2: Awareness STEP #3: Action 1. Anatomy *Memorize
Stabilize the Scapula in Three Easy Steps by NFPT Idea World 2016: Session 611 Saturday July 16th 7:30-9:20am Beverly Hosford, MA STEP #1: Anatomy STEP #2: Awareness STEP #3: Action 1. Anatomy *Memorize
Ms. Ruth A. Delaney, MB BCh BAO, MMedSc, MRCS
 Ms. Ruth A. Delaney, MB BCh BAO, MMedSc, MRCS Consultant Orthopaedic Surgeon, Shoulder Specialist. +353 1 5262335 ruthdelaney@sportssurgeryclinic.com Modified from the protocol developed at Boston Shoulder
Ms. Ruth A. Delaney, MB BCh BAO, MMedSc, MRCS Consultant Orthopaedic Surgeon, Shoulder Specialist. +353 1 5262335 ruthdelaney@sportssurgeryclinic.com Modified from the protocol developed at Boston Shoulder
Post-Operative Instructions Glenoid Reconstruction using Fresh Distal Tibial Allograft
 Day of Surgery Post-Operative Instructions Glenoid Reconstruction using Fresh Distal Tibial Allograft A. Relax. Diet as tolerated. B. Icing is important for the first 5-7 days post-op. While the post-op
Day of Surgery Post-Operative Instructions Glenoid Reconstruction using Fresh Distal Tibial Allograft A. Relax. Diet as tolerated. B. Icing is important for the first 5-7 days post-op. While the post-op