Eric Magrum PT, DPT, OCS, FAAOMPT Orthopaedic Manual Physical Therapy Series Charlottesville
|
|
|
- Ferdinand Hutchinson
- 5 years ago
- Views:
Transcription



1 SHOULDER CASE 1 Eric Magrum PT, DPT, OCS, FAAOMPT Orthopaedic Manual Physical Therapy Series Charlottesville Reproduction Without Consent 1

2 Prevalence Shoulder pain 2 nd to LBP prevalence MSK 44-60% Shoulder = IMP Reproduction Without Consent 2



3 Less Prevalent 2018 Shoulder Pain Reproduction Without Consent 3


4 Impingement Syndrome Cluster of signs/symptoms Location Anterior Superior (SA), Posterior Superior (Internal) Chronic bursitis RC tendinitis RTC Partial thickness Tear Cause Compression-Primary vs. Instability-Secondary Direct Compression of RTC Tendons, Biceps Tendon, SA bursa Primary Impingement Between the Humeral Head and the overlying anterior 1/3 of the Acromion, Coracoacromial ligament, Coracoid or AC joint Reproduction Without Consent 4
")
5 Characteristics of Primary Impingement > 50 yo Age related degenerative changes Mechanical compromise of the subacromial space DJD - AC joint? Bursal side RTC pathology - controversy Subacromial osteophytic changes SA Bursitis RTC tendinitis/tendinosis - atrophy/weakness LH Biceps tendinitis Scapular Dyskinesis (poor posture) Secondary IMP - Sub Acromial Reproduction Without Consent 5
6 Secondary Impingement Underlying instability of the GH joint Laxity of capsular ligaments and labrum, in throwing or overhead activities can lead to anterior instability of the GH joint Increased humeral head translation, the Biceps/RTC Tendon can become impinged secondary to the ensuing instability Dynamic stabilizing functions of the rotator cuff are diminished from fatigue, intrinsic overload and subsequent tendon injury Characteristics of Secondary Impingement Patients < 50 yo Pain is anterior or anterolateral Typically associated with repetitive overhead use Rarely night pain, unless chronic? Bursal vs Articular side RTC pathology Attenuation of the static stabilizers leads to fatigue of the dynamic stabilizers and subsequent anterior subluxation Cycle Reproduction Without Consent 6


7 Silent Subluxation Cycle RTC Pathology Repetitive Micro Trauma Fatigue RTC/Scapular Stabilizers Secondary IMP Increased Ant Translation/Superior Migration Internal IMP Posterior Post aspect Supraspinatus IMP Between Greater Tuberosity & Posterior Superior 90 ABD/ER Articular RTC tears Reproduction Without Consent 7
8 Cools A M et al. Br J Sports Med 2008;42: Reproduction Without Consent 8

9 Impingement Lesions Rotator Cuff Pathology Progressive stages (Neer) Stage 1 Edema and hemorrhage result from excessive overhead use: Tendinitis < 25 yo Stage 2 Fibrosis and Tendinosis - Bursa/RTC following repeated episodes of mechanical inflammation: Tendinopathy yo Stage 3 Bone spurs and incomplete and complete RTC/LHB tears : Partial RTC tear > 40 yo TendinOPATHY NOT Tendonitis Absence of inflammatory cell infiltrate and biochemical mediators Cellular activation with an increase in cell numbers Increase in Ground substance Collagen Disorganization Neovascularization Reproduction Without Consent 9



10 Reproduction Without Consent 10

11 Proposed Tendinopathy Etiology Mechanical Inability of the tendon to respond to increasing loads over time may lead to tendon failure and degeneration Vascular Decreased vascular supply to certain areas of the tendon causes vascular compromise, pain, inferior healing response progressing to degeneration and tearing Neural Potential of the nervous system, most notably the proinflammatory mediator substance P, to contribute to the presence of painful symptoms with tendon degeneration Mechanical - Collagen Degeneration Absence normal inflammatory response Disordered Healing Response Increased Type III Thinner, weaker, disorganized matrix Imbalance of MMPs & TIMPs Extra cellular remodeling enzymes Reproduction Without Consent 11


12 Watershed area Relative Vascular - Critical Zone Hypovascularity Controversy Relative to arm position Poor Healing Response Neurogenic Inflammation = Pain Chronic painful Tendon No Inflammation Increased neurotransmitters of pain Substance P Glutamate Reproduction Without Consent 12


13 Intrinsic/Extrinsic Factors Extrinsic factors Soft tissue impingement Bony impingement Training errors - Overuse Intrinsic Factors Aging Vascular supply Nutrition Genetics Tensile load Under stimulation may be as damaging as overstimulation Reproduction Without Consent 13


14 Reproduction Without Consent 14

 + Manual")

15 Function Pain Strength Findings/Conclusions: Exercise is effective as treatment for reduction in pain Kuhn JE JSES 2009 Recommend 2-3 x/week prescribed exercise (RTC strengthening + Scapular stabilization) + Manual Therapy Progress to home program when Manual Therapy no longer indicated Reproduction Without Consent 15



16 Reproduction Without Consent 16



17 Treatment- RTC Tendinopathy Manual Therapy + Exercise has proved beneficial for RTC tendinopathy > Exercise alone Manual Therapy addresses Extrinsic factors Exercise may address the intrinsic factor of blood flow. Eccentrics help by increasing tenocyte production and normalizing tendon structure Lack of quality studies reporting similar benefits in RTC tendinopathy Hallmark of Tendonopathy Management Progressive Tendon Loading Treatment- RTC Tendinopathy Reproduction Without Consent 17
 NSAIDs/ice Active Rest Manual Therapy Scapular mobs,")

18 Initial Goals: Education Anatomy/pathology Posture (Scapular positioning) NSAIDs/ice Active Rest Manual Therapy Scapular mobs, GH mobs Decrease Superior/Anterior Translation RTC activation Compression Depression Scapular stabilization IMP Reproduction Without Consent 18



19 Glenohumeral Inferior Glide Glenohumeral Inferior Glide Prone end ROM Reproduction Without Consent 19







20 Glenohumeral - Posterior Glide Reproduction Without Consent 20

21 Reproduction Without Consent 21


22 Scapular Observation Static Resting position Hands on Hips 90 ABD Active Elevation Flexion, Scaption, ABD 3-5 reps Loaded - (3-5# weights) Observe for Abnormal Mechanics Asymmetry Eccentric phase Reproduction Without Consent 22


23 Type I: Abnormal static scapular position and/or dynamic scapular motion characterized by Medial border prominence Excessive Scapular ER RTC IMP Type II: Inferior angle prominence and/or early scapular elevation or shrugging on arm elevation Excessive Ant Tilt GH Instability Change in glenoid position Type III: Excessive Upward Rotation Rapid downward rotation during arm lowering RTC weakness Muscle imbalance force couple Scapulothoracic Assessment Physiological Motion : Elevation - Depression Reproduction Without Consent 23

24 Scapulothoracic Assessment Physiological Motion : Protraction - Retraction Scapulothoracic Accessory Motion Distraction Upward/Downward Rotation Internal/External Rotation Anterior/Posterior Tilt Reproduction Without Consent 24


25 Scapulothoracic Accessory Motion Distraction Scapulothoracic Accessory Motion Internal/External Rotation Reproduction Without Consent 25


26 Scapulothoracic Accessory Motion Anterior/Posterior Tilt Scapulothoracic Accessory Motion Upward/Downward Rotation Reproduction Without Consent 26
 Test = Painful arc of impingement symptoms are relieved and the arc of motion is increased.")
: Supraspinatus strength is increased or the symptoms relieved in the retracted")
27 Scapular Dyskinesis Scapula Assist Test Pt : Standing Active Elevation PT : Gentle pressure to assist scapular upward rotation and posterior tilt (+) Test = Painful arc of impingement symptoms are relieved and the arc of motion is increased. Scapular Dyskinesis Scapula Relocation Test Pt: Standing Full Can Supraspinatus test position Test: Resist Full Can Stabilize Scapula in retracted position; re test resisted Supraspinatus (+): Supraspinatus strength is increased or the symptoms relieved in the retracted position Reproduction Without Consent 27

28 Static Neutral, 45, 90 degrees Specific plane of dysfunction Dynamic Active Elevation Flexion Specific plane of dysfunction Loaded Physiological Motions Retraction/Protraction Depression/Elevation Accessory Motions Distraction Upward/Downward Rotation Anterior/Posterior Tilt Internal/External Rotation Special Tests Scapular Assist Test Scapular Retraction Test Scapular Assess: Lab Reproduction Without Consent 28




29 Changes in static posture Significant Incr flexion, scaption Increased elevation ROM prior to onset pain Reproduction Without Consent 29






30 Thoracic Extension Thoracic Mobilization/Manipulation Reproduction Without Consent 30



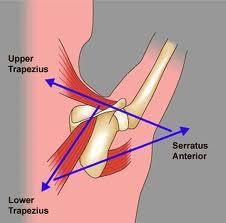
31 Upper Quarter Crossed Syndrome Facilitated/Short Upper Trap/Levator Scapulae Pecs Inhibited/Weak Scapular Retractors Mid/Low Trap Rhomboids Serratus Ant Deep Neck Flexors STM: Upper Trap, Levator, Scaleni Subscapularis Reproduction Without Consent 31




32 Pec Minor Restore Force Couple - Timing Reproduction Without Consent 32


33 Timing deficits - Improved with feedback/exercise CONCLUSIONS: Conscious correction of scapular orientation during the prone extension and side-lying external rotation exercise can be used to increase the activation level in the 3 sections of the trapezius in overhead athletes with scapular dyskinesis. Reproduction Without Consent 33



34 Visual, Auditory, Kinesthetic Cues Anterior-tilted Scapula Gently bring the tip of your shoulder blade toward your spine Downwardly Rotated Scapula Gently lift the top of the shoulder Protracted Scapula Gently spread the front of your shoulder apart to draw your shoulder blade toward midline Low Row Isometric Inferior Glide Reproduction Without Consent 34







35 Squat and Reach H i g h L o w R o w Reproduction Without Consent 35

36 Kinetic Chain Functions Using integrated programs of muscle activation to temporarily link multiple body segments into one functional segment to decrease the degrees of freedom in the entire motion Providing a stable proximal base for distal arm mobility Maximizing force development in the large muscles of the core and transferring it to the hand Producing interactive moments at distal joints that develop more force and energy than the joint itself could develop and decrease the magnitude of the applied loads at the distal joint Producing torques that decrease deceleration forces Reproduction Without Consent 36


37 Kinetic Chain Proximal-to-distal sequencing of velocity, energy, and forces 54% of the total force generated in the tennis serve are created by the lower legs, hip, and trunk Forces that are generated in the proximal segments have to be transferred efficiently to the shoulder Kinetic Chain This can be accomplished most efficiently through the stable and controlled platform of the scapula The entire arm rotates as a unit around the stable base of the Glenoid Reproduction Without Consent 37



38 McMullen J Ath Train 2000 Contralateral step up with Ipsilateral reach Hip EXT Trunk EXT Thoracic EXT Scapular upward rotation GH Elevation Functional Position with all CKC Reproduction Without Consent 38



39 Shoulder Dump Contralateral Hip/Trunk Flexion Rotation Weight shift to ipsilateral leg; Trunk Extension/Rotation Scapular Retraction GH ER Reciprocal Thoracic EXT Sternal Lift Scapular Retraction- Depression Avoid Lumbar Hyper EXT Reproduction Without Consent 39



40 Lateral Lunge Eccentric Scapular Protraction Weight shift to outside leg Scapular Retraction-Depression Elbow to Back Hip pocket Clavicle retraction, Upward rotation, Post tilt * Scapular ER, Upward rotation, Retraction, Post tilt * Greatest Upward Rotation Upward rotation, Posterior Tilt. High Upper/Mid Trap * Scapular ER, Upward rotation, Retraction, Post tilt * 50% MVIC Lower Trap Best LT/UT ratio JOSPT 2010 Reproduction Without Consent 40




41 Moderate amount Posterior RTC EMG Lower Trapezius EMG activity Minimal Upper Trapezius activity Highest ratio of lower Trapezius to Upper Trapezius activity McCabe NAJSPT 2007 Overhead Shrug: High UT/Lower Levator Overhead Retraction/Lift: High Mid/Lower Trap Reproduction Without Consent 41





42 High SA, Low UT Reproduction Without Consent 42

43 Cools AM AJSM 2007 Highest LT/MT : UT Ratio Reproduction Without Consent 43


44 Reproduction Without Consent 44
45 Reproduction Without Consent 45

46 Rehab Factors Post RTC Repair Surgical Approach Open, Mini-open, Arthroscopic Size of Tear Small (<1 cm) Medium (1-3 cm) Large (3-5 cm) Massive (> 5 cm) Tissue Quality Good Poor Fixation Single, Double Row Tear Location Supra/Infraspinatus Subscapularis Type of Tear Crescent, U, L shaped? retracted Mechanism Traumatic; Degenerative Surgical Timing Immediate; Delayed Surrounding RTC Tissue Quality Patient General Health DM, smoker Access to care/rehab Physician Philosophical approach Conservative vs. Aggressive Ghodadra JOSPT 2009 Reproduction Without Consent 46





47 Reproduction Without Consent 47
REMINDER. an exercise program. Senior Fitness Obtain medical clearance and physician s release prior to beginning
 Functional Forever: Exercise for Independent Living REMINDER Obtain medical clearance and physician s release prior to beginning an exercise program for clients with medical or orthopedic concerns. What
Functional Forever: Exercise for Independent Living REMINDER Obtain medical clearance and physician s release prior to beginning an exercise program for clients with medical or orthopedic concerns. What
Returning the Shoulder Back to Optimal Function. Scapula. Clavicle. Humerus. Bones of the Shoulder (Osteology) Joints of the Shoulder (Arthrology)
 Joints of the Shoulder (Arthrology)") Returning the Shoulder Back to Optimal Function Sternum Clavicle Ribs Scapula Humerus Bones of the Shoulder (Osteology) By Rick Kaselj Clavicle Scapula Medial Left Anterior Clavicle Inferior View 20 degree
Returning the Shoulder Back to Optimal Function Sternum Clavicle Ribs Scapula Humerus Bones of the Shoulder (Osteology) By Rick Kaselj Clavicle Scapula Medial Left Anterior Clavicle Inferior View 20 degree
REMINDER. Obtain medical clearance and physician s release prior to beginning an exercise program for clients with medical or orthopedic concerns
 Understanding Shoulder Dysfunction REMINDER Obtain medical clearance and physician s release prior to beginning an exercise program for clients with medical or orthopedic concerns What is a healthy shoulder?
Understanding Shoulder Dysfunction REMINDER Obtain medical clearance and physician s release prior to beginning an exercise program for clients with medical or orthopedic concerns What is a healthy shoulder?
Tendinosis & Subacromial Impingement Syndrome. Gene Desepoli, LMT, D.C.
 Tendinosis & Subacromial Impingement Syndrome Gene Desepoli, LMT, D.C. What is the shoulder joint? Shoulder joint or shoulder region? There is an interrelatedness of all moving parts of the shoulder and
Tendinosis & Subacromial Impingement Syndrome Gene Desepoli, LMT, D.C. What is the shoulder joint? Shoulder joint or shoulder region? There is an interrelatedness of all moving parts of the shoulder and
Joint G*H. Joint S*C. Joint A*C. Labrum. Humerus. Sternum. Scapula. Clavicle. Thorax. Articulation. Scapulo- Thoracic
 A*C Joint Scapulo- Thoracic Articulation Thorax Sternum Clavicle Scapula Humerus S*C Joint G*H Joint Labrum AC Ligaments SC Ligaments SC JOINT AC Coracoacromial GH GH Ligament Complex Coracoclavicular
A*C Joint Scapulo- Thoracic Articulation Thorax Sternum Clavicle Scapula Humerus S*C Joint G*H Joint Labrum AC Ligaments SC Ligaments SC JOINT AC Coracoacromial GH GH Ligament Complex Coracoclavicular
ROTATOR CUFF DISORDERS/IMPINGEMENT
 ROTATOR CUFF DISORDERS/IMPINGEMENT Dr.KN Subramanian M.Ch Orth., FRCS (Tr & Orth), CCT Orth(UK) Consultant Orthopaedic Surgeon, Special interest: Orthopaedic Sports Injury, Shoulder and Knee Surgery, SPARSH
ROTATOR CUFF DISORDERS/IMPINGEMENT Dr.KN Subramanian M.Ch Orth., FRCS (Tr & Orth), CCT Orth(UK) Consultant Orthopaedic Surgeon, Special interest: Orthopaedic Sports Injury, Shoulder and Knee Surgery, SPARSH
Theodore B. Shybut, M.D.
 Theodore B. Shybut, M.D. Orthopedics and Sports Medicine 7200 Cambridge St. #10A Houston, Texas 77030 Non-operative Shoulder Rehabilitation Protocol Basic shoulder program for: o Scapular Dyskinesis (proximally
Theodore B. Shybut, M.D. Orthopedics and Sports Medicine 7200 Cambridge St. #10A Houston, Texas 77030 Non-operative Shoulder Rehabilitation Protocol Basic shoulder program for: o Scapular Dyskinesis (proximally
Rehabilitation Guidelines for Large Rotator Cuff Repair
 Rehabilitation Guidelines for Large Rotator Cuff Repair The true shoulder joint is called the glenohumeral joint and consists humeral head and the glenoid. It is a ball and socket joint. Anatomy of the
Rehabilitation Guidelines for Large Rotator Cuff Repair The true shoulder joint is called the glenohumeral joint and consists humeral head and the glenoid. It is a ball and socket joint. Anatomy of the
Rehabilitation of Overhead Shoulder Injuries
 Rehabilitation of Overhead Shoulder Injuries 16 th Annual Primary Care Orthopaedic & Sports Medicine Symposium January 29, 2016 Jeremy Sherman, PT, MPT Disclosures No financial disclosures to note. Jeremy
Rehabilitation of Overhead Shoulder Injuries 16 th Annual Primary Care Orthopaedic & Sports Medicine Symposium January 29, 2016 Jeremy Sherman, PT, MPT Disclosures No financial disclosures to note. Jeremy
TIPS FOR SUCCESSFUL SHOULDER TREATMENT. In Service Training 16 th May 2014
 TIPS FOR SUCCESSFUL SHOULDER TREATMENT In Service Training 16 th May 2014 Training day aims to address: Controversies of impingement syndrome diagnosis Controversies of MRI/USS imaging Clinical diagnosis
TIPS FOR SUCCESSFUL SHOULDER TREATMENT In Service Training 16 th May 2014 Training day aims to address: Controversies of impingement syndrome diagnosis Controversies of MRI/USS imaging Clinical diagnosis
Throwing Athlete Rehabilitation. Brett Schulz LAT/CMSS Sport and Spine Physical Therapy
 Throwing Athlete Rehabilitation Brett Schulz LAT/CMSS Sport and Spine Physical Therapy Disclosure No conflicts to disclose Throwing Athlete Dilemma The shoulder must have enough range of motion to allow
Throwing Athlete Rehabilitation Brett Schulz LAT/CMSS Sport and Spine Physical Therapy Disclosure No conflicts to disclose Throwing Athlete Dilemma The shoulder must have enough range of motion to allow
Secrets and Staples of Training the Athletic Shoulder
 Secrets and Staples of Training the Athletic Shoulder Eric Beard Corrective Exercise Specialist Athletic Performance Enhancement Specialist EricBeard.com AthleticShoulder.com Presentation Overview Rationale
Secrets and Staples of Training the Athletic Shoulder Eric Beard Corrective Exercise Specialist Athletic Performance Enhancement Specialist EricBeard.com AthleticShoulder.com Presentation Overview Rationale
Physical Examination of the Shoulder
 General setup Patient will be examined in both the seated and supine position so exam table needed 360 degree access to patient Expose neck and both shoulders (for comparison); female in gown or sports
General setup Patient will be examined in both the seated and supine position so exam table needed 360 degree access to patient Expose neck and both shoulders (for comparison); female in gown or sports
Shoulder Joint Examination. Shoulder Joint Examination. Inspection. Inspection Palpation Movement. Look Feel Move
 Shoulder Joint Examination History Cuff Examination Instability Examination AC Joint Examination Biceps Tendon Examination Superior Labrum Examination Shoulder Joint Examination Inspection Palpation Movement
Shoulder Joint Examination History Cuff Examination Instability Examination AC Joint Examination Biceps Tendon Examination Superior Labrum Examination Shoulder Joint Examination Inspection Palpation Movement
Eric Magrum PT, DPT, OCS, FAAOMPT Orthopaedic Manual Physical Therapy Series Charlottesville
 SHOULDER EXAM Eric Magrum PT, DPT, OCS, FAAOMPT Orthopaedic Manual Physical Therapy Series Charlottesville 2017-2018 Reproduction Without Consent 1 Subjective History: Interrogate with Empathy Age Hand
SHOULDER EXAM Eric Magrum PT, DPT, OCS, FAAOMPT Orthopaedic Manual Physical Therapy Series Charlottesville 2017-2018 Reproduction Without Consent 1 Subjective History: Interrogate with Empathy Age Hand
SHOULDER EXAM. Differential Diagnosis
 SHOULDER EXAM Eric Magrum PT, DPT, OCS, FAAOMPT Orthopaedic Manual Physical Therapy Series Charlottesville 2017-2018 Subjective History: Interrogate with Empathy Age Hand Dominance Symptom onset Pain description
SHOULDER EXAM Eric Magrum PT, DPT, OCS, FAAOMPT Orthopaedic Manual Physical Therapy Series Charlottesville 2017-2018 Subjective History: Interrogate with Empathy Age Hand Dominance Symptom onset Pain description
Review shoulder anatomy Review the physical exam of the shoulder Discuss some common causes of acute shoulder pain Discuss some common causes of
 Review shoulder anatomy Review the physical exam of the shoulder Discuss some common causes of acute shoulder pain Discuss some common causes of chronic shoulder pain Review with some case questions Bones:
Review shoulder anatomy Review the physical exam of the shoulder Discuss some common causes of acute shoulder pain Discuss some common causes of chronic shoulder pain Review with some case questions Bones:
Disclosures. Training for the Scapulothoracic Joint and Thoracic Spine. Scapular Muscles Stabilization & Rotation 9/7/2018
 Disclosures Training for the Scapulothoracic Joint and Thoracic Spine mtrigger Litecure Russ Paine, PT Director -UT Physicians Sportsmedicine Rehabilitation Houston, Texas 21 academic institutions 14 hospitals
Disclosures Training for the Scapulothoracic Joint and Thoracic Spine mtrigger Litecure Russ Paine, PT Director -UT Physicians Sportsmedicine Rehabilitation Houston, Texas 21 academic institutions 14 hospitals
The Shoulder. Anatomy and Injuries PSK 4U Unit 3, Day 4
 The Shoulder Anatomy and Injuries PSK 4U Unit 3, Day 4 Shoulder Girdle Shoulder Complex is the most mobile joint in the body. Scapula Clavicle Sternum Humerus Rib cage/thorax Shoulder Girdle It also includes
The Shoulder Anatomy and Injuries PSK 4U Unit 3, Day 4 Shoulder Girdle Shoulder Complex is the most mobile joint in the body. Scapula Clavicle Sternum Humerus Rib cage/thorax Shoulder Girdle It also includes
DIFFERENTIAL DIAGNOSIS: Looking for the causes of impingement
 DIFFERENTIAL DIAGNOSIS: Looking for the causes of Ann Cools, PT, PhD Ghent University - Belgium Dept of Rehabilitation Sciences & Physiotherapy Ann.Cools@UGent.be «thinking about.» Which special tests
DIFFERENTIAL DIAGNOSIS: Looking for the causes of Ann Cools, PT, PhD Ghent University - Belgium Dept of Rehabilitation Sciences & Physiotherapy Ann.Cools@UGent.be «thinking about.» Which special tests
Shoulder: Clinical Anatomy, Kinematics & Biomechanics
 Shoulder: Clinical Anatomy, Kinematics & Biomechanics Dr. Alex K C Poon Department of Orthopaedics & Traumatology Pamela Youde Nethersole Eastern Hospital Clinical Anatomy the application of anatomy to
Shoulder: Clinical Anatomy, Kinematics & Biomechanics Dr. Alex K C Poon Department of Orthopaedics & Traumatology Pamela Youde Nethersole Eastern Hospital Clinical Anatomy the application of anatomy to
11/6/2013. Keely Behning, PT, SCS, ATC MNPTA Fall Conference November 16, 2013
 Keely Behning, PT, SCS, ATC MNPTA Fall Conference November 16, 2013 Upon completion of this course, attendees should be able to: Understand pertinent anatomy and biomechanics as they relate to specific
Keely Behning, PT, SCS, ATC MNPTA Fall Conference November 16, 2013 Upon completion of this course, attendees should be able to: Understand pertinent anatomy and biomechanics as they relate to specific
WEEKEND 2 Shoulder. Shoulder Active Range of Motion Assessment
 Virginia Orthopedic Manual Physical Therapy Institute - 2016 Technique Manual WEEKEND 2 Shoulder Shoulder Active Range of Motion Assessment - Patient Positioning: Standing, appropriately undressed so that
Virginia Orthopedic Manual Physical Therapy Institute - 2016 Technique Manual WEEKEND 2 Shoulder Shoulder Active Range of Motion Assessment - Patient Positioning: Standing, appropriately undressed so that
IMPINGEMENT-TESTSTESTS
 «thinking about.» DIFFERENTIAL DIAGNOSIS: Looking for the causes of Which special tests do you use in your shoulder examination? Ann Cools, PT, PhD Ghent University - Belgium Dept of Rehabilitation Sciences
«thinking about.» DIFFERENTIAL DIAGNOSIS: Looking for the causes of Which special tests do you use in your shoulder examination? Ann Cools, PT, PhD Ghent University - Belgium Dept of Rehabilitation Sciences
SHOULDER PAIN LESSONS FROM THE SPORTS FIELD MOVEMENT RESTRICTIONS. Steve McCaig
 SHOULDER PAIN LESSONS FROM THE SPORTS FIELD MOVEMENT RESTRICTIONS 1 Steve McCaig Senior Physiotherapist England Development Programme, ECB, Loughborough, United Kingdom Throwing High forces upper limb
SHOULDER PAIN LESSONS FROM THE SPORTS FIELD MOVEMENT RESTRICTIONS 1 Steve McCaig Senior Physiotherapist England Development Programme, ECB, Loughborough, United Kingdom Throwing High forces upper limb
Rehabilitation Guidelines for Labral/Bankert Repair
 Rehabilitation Guidelines for Labral/Bankert Repair The true shoulder joint is called the glenohumeral joint and consists humeral head and the glenoid. It is a ball and socket joint. Anatomy of the Shoulder
Rehabilitation Guidelines for Labral/Bankert Repair The true shoulder joint is called the glenohumeral joint and consists humeral head and the glenoid. It is a ball and socket joint. Anatomy of the Shoulder
SHOULDER PROBLEMS & ARTHROSCOPIC MANAGEMENT
 SHOULDER PROBLEMS & ARTHROSCOPIC MANAGEMENT DR.SHEKHAR SRIVASTAV Sr. Consultant-KNEE & SHOULDER Arthroscopy Sant Parmanand Hospital,Delhi Peculiarities of Shoulder Elegant piece of machinery It has the
SHOULDER PROBLEMS & ARTHROSCOPIC MANAGEMENT DR.SHEKHAR SRIVASTAV Sr. Consultant-KNEE & SHOULDER Arthroscopy Sant Parmanand Hospital,Delhi Peculiarities of Shoulder Elegant piece of machinery It has the
Conservative Management of Rotator Cuff Pathology
 Conservative Management of Rotator Cuff Pathology Dustin Maracle, PT, DPT, MS, SCS, COMT, CSCS APTA Board Certified Sports Specialist Clinical Director/Co-Owner: Lattimore Physical Therapy Presentation
Conservative Management of Rotator Cuff Pathology Dustin Maracle, PT, DPT, MS, SCS, COMT, CSCS APTA Board Certified Sports Specialist Clinical Director/Co-Owner: Lattimore Physical Therapy Presentation
Acromioplasty. Surgical Indications and Considerations
 1 Acromioplasty Surgical Indications and Considerations Anatomical Considerations: Any abnormality that disrupts the intricate relationship within the subacromial space may lead to impingement. Both intrinsic
1 Acromioplasty Surgical Indications and Considerations Anatomical Considerations: Any abnormality that disrupts the intricate relationship within the subacromial space may lead to impingement. Both intrinsic
Nonoperative Treatment For Rotator Cuff Tendinitis/ Partial Thickness Tear Dr. Trueblood
 Nonoperative Treatment For Rotator Cuff Tendinitis/ Partial Thickness Tear Dr. Trueblood Relieving Pain Patients who present with SIS will have shoulder pain that is exacerbated with overhead activities.
Nonoperative Treatment For Rotator Cuff Tendinitis/ Partial Thickness Tear Dr. Trueblood Relieving Pain Patients who present with SIS will have shoulder pain that is exacerbated with overhead activities.
Lab Workbook. ANATOMY Manual Muscle Testing Lower Trapezius Patient: prone
 ANATOMY Manual Muscle Testing Lower Trapezius Patient: prone Lab Workbook Fixation: place on hand below the scapula on the opposite side Test: adduction and depression of the scapula with lateral rotation
ANATOMY Manual Muscle Testing Lower Trapezius Patient: prone Lab Workbook Fixation: place on hand below the scapula on the opposite side Test: adduction and depression of the scapula with lateral rotation
Shoulder joint Assessment and General View
 Shoulder joint Assessment and General View Done by; Mshari S. Alghadier BSc Physical Therapy RHPT 366 m.alghadier@sau.edu.sa http://faculty.sau.edu.sa/m.alghadier/ Functional anatomy The shoulder contains
Shoulder joint Assessment and General View Done by; Mshari S. Alghadier BSc Physical Therapy RHPT 366 m.alghadier@sau.edu.sa http://faculty.sau.edu.sa/m.alghadier/ Functional anatomy The shoulder contains
1. The coordinated action of a scapular upward rotation and humeral abduction is known as the:
 1 1. The coordinated action of a scapular upward rotation and humeral abduction is known as the: a. Carrying angle of the arm b. Scapulohumeral rhythm c. Glenohumeral capsular pattern d. Abduction resistance
1 1. The coordinated action of a scapular upward rotation and humeral abduction is known as the: a. Carrying angle of the arm b. Scapulohumeral rhythm c. Glenohumeral capsular pattern d. Abduction resistance
Definition. Compressive load of structures between the acromion and acromial arch (coracoacromial ligament) and the head of humerus.
 and the head of humerus.") Definition Compressive load of structures between the acromion and acromial arch (coracoacromial ligament) and the head of humerus. Definition Many shoulder pathologies can involve a degree of impingement.
Definition Compressive load of structures between the acromion and acromial arch (coracoacromial ligament) and the head of humerus. Definition Many shoulder pathologies can involve a degree of impingement.
SHOULDER REHABILITATION PART II
 SHOULDER REHABILITATION PART II Ann Cools, PT, PhD Ghent University - Belgium Dept of Rehabilitation Sciences & Physiotherapy Ann.Cools@UGent.be Shoulder rehab course level I Shoulder pathology and clinical
SHOULDER REHABILITATION PART II Ann Cools, PT, PhD Ghent University - Belgium Dept of Rehabilitation Sciences & Physiotherapy Ann.Cools@UGent.be Shoulder rehab course level I Shoulder pathology and clinical
Continuing Education: Shoulder Stability
 Continuing Education: Shoulder Stability Anatomy & Kinesiology: The GHJ consists of the articulation of three bones: the scapula, clavicle and humerus. The scapula has three protrusions: the coracoid,
Continuing Education: Shoulder Stability Anatomy & Kinesiology: The GHJ consists of the articulation of three bones: the scapula, clavicle and humerus. The scapula has three protrusions: the coracoid,
Shoulder Biomechanics
 Shoulder Biomechanics Lecture originally developed by Bryan Morrison, Ph.D. candidate Arizona State University Fall 2000 1 Outline Anatomy Biomechanics Problems 2 Shoulder Complex Greatest Greatest Predisposition
Shoulder Biomechanics Lecture originally developed by Bryan Morrison, Ph.D. candidate Arizona State University Fall 2000 1 Outline Anatomy Biomechanics Problems 2 Shoulder Complex Greatest Greatest Predisposition
Exploring the Rotator Cuff
 Exploring the Rotator Cuff Improving one s performance in sports and daily activity is a factor of neuromuscular efficiency and metabolic enhancements. To attain proficiency, reaction force must be effectively
Exploring the Rotator Cuff Improving one s performance in sports and daily activity is a factor of neuromuscular efficiency and metabolic enhancements. To attain proficiency, reaction force must be effectively
Rotator Cuff Repair Protocol for tear involving Subscapularis Tendon with or without Pectoralis Major Tendon Transfer
 Rotator Cuff Repair Protocol for tear involving Subscapularis Tendon with or without Pectoralis Major Tendon Transfer D. WATTS, MD Precautions: BASIS Tendon healing back to bone is a slow process that
Rotator Cuff Repair Protocol for tear involving Subscapularis Tendon with or without Pectoralis Major Tendon Transfer D. WATTS, MD Precautions: BASIS Tendon healing back to bone is a slow process that
Nonoperative Treatment of Subacromial Impingement Rehabilitation Protocol
 Therapist Nonoperative Treatment of Subacromial Impingement Rehabilitation Protocol Subacromial impingement is a chronic inflammatory process produced as one of the Rotator Cuff Muscle the and the Subdeltoid
Therapist Nonoperative Treatment of Subacromial Impingement Rehabilitation Protocol Subacromial impingement is a chronic inflammatory process produced as one of the Rotator Cuff Muscle the and the Subdeltoid
Stefan C Muzin, MD PM&R Attending Physician, Beth Israel Deaconess Medical Center, Harvard Medical School Onsite Physiatrist, GE Aviation, Lynn, MA
 Stefan C Muzin, MD PM&R Attending Physician, Beth Israel Deaconess Medical Center, Harvard Medical School Onsite Physiatrist, GE Aviation, Lynn, MA Consultant, OEHN (Occupational and Environmental Network)
Stefan C Muzin, MD PM&R Attending Physician, Beth Israel Deaconess Medical Center, Harvard Medical School Onsite Physiatrist, GE Aviation, Lynn, MA Consultant, OEHN (Occupational and Environmental Network)
Overuse Injuries. Overuse injury defined. Overuse Injuries
 Overuse Injuries Lisa DeStefano, DO Associate Professor and Chair Department of Osteopathic Manipulative Medicine College of Osteopathic Medicine Michigan State University Overuse injury defined Overuse
Overuse Injuries Lisa DeStefano, DO Associate Professor and Chair Department of Osteopathic Manipulative Medicine College of Osteopathic Medicine Michigan State University Overuse injury defined Overuse
Vol 3, 2008 CEC ARTICLE: Special Medical Conditions Part 2: Shoulder Maintenance and Rehab C. Eggers
 Vol 3, 2008 CEC ARTICLE: Special Medical Conditions Part 2: Shoulder Maintenance and Rehab C. Eggers SHOULDER GIRDLE STABILIZATION Knowledge of the anatomy and biomechanics of the shoulder girdle is essential
Vol 3, 2008 CEC ARTICLE: Special Medical Conditions Part 2: Shoulder Maintenance and Rehab C. Eggers SHOULDER GIRDLE STABILIZATION Knowledge of the anatomy and biomechanics of the shoulder girdle is essential
Throwing Injuries and Prevention: The Physical Therapy Perspective
 Throwing Injuries and Prevention: The Physical Therapy Perspective Andrew M Jordan, PT, DPT, OCS Staff Physical Therapist, Cayuga Medical Center Physical Therapy and Sports Medicine ajordan@cayugamed.org
Throwing Injuries and Prevention: The Physical Therapy Perspective Andrew M Jordan, PT, DPT, OCS Staff Physical Therapist, Cayuga Medical Center Physical Therapy and Sports Medicine ajordan@cayugamed.org
Small Rotator Cuff Repair
 Small Rotator Cuff Repair 1. Defined a. Surgical repair of the rotator cuff (most commonly supraspinatus muscle) utilizing sutures b. May be done arthroscopically or open. c. May be done in conjunction
Small Rotator Cuff Repair 1. Defined a. Surgical repair of the rotator cuff (most commonly supraspinatus muscle) utilizing sutures b. May be done arthroscopically or open. c. May be done in conjunction
Large/Massive Rotator Cuff Repair
 Large/Massive Rotator Cuff Repair 1. Defined a. Suturing of tears within the rotator cuff (most commonly supraspinatus muscle). Massive RCR usually involve more than the supraspinatus. b. May be done arthroscopically
Large/Massive Rotator Cuff Repair 1. Defined a. Suturing of tears within the rotator cuff (most commonly supraspinatus muscle). Massive RCR usually involve more than the supraspinatus. b. May be done arthroscopically
Shoulder Impingement Rehabilitation Recommendations
 Shoulder Impingement Rehabilitation Recommendations The following protocol can be utilized for conservative care of shoulder impingement as well as post- operative subacromial decompression (SAD) surgery.
Shoulder Impingement Rehabilitation Recommendations The following protocol can be utilized for conservative care of shoulder impingement as well as post- operative subacromial decompression (SAD) surgery.
Scapular and Deltoid Regions
 M1 Gross and Developmental Anatomy Scapular and Deltoid Regions Dr. Peters 1 Outline I. Skeleton of the Shoulder and Attachment of the Upper Extremity to Trunk II. Positions and Movements of the Scapula
M1 Gross and Developmental Anatomy Scapular and Deltoid Regions Dr. Peters 1 Outline I. Skeleton of the Shoulder and Attachment of the Upper Extremity to Trunk II. Positions and Movements of the Scapula
OBJECTIVES. Therapists Management of Shoulder Instability SHOULDER STABILITY SHOULDER STABILITY WHAT IS SHOULDER INSTABILITY? SHOULDER INSTABILITY
 Therapists Management of Shoulder Instability Brian G. Leggin, PT, DPT, OCS Lead Therapist, Penn Therapy and Fitness at Valley Forge Adjunct Assistant Professor, Department of Orthopaedics, University
Therapists Management of Shoulder Instability Brian G. Leggin, PT, DPT, OCS Lead Therapist, Penn Therapy and Fitness at Valley Forge Adjunct Assistant Professor, Department of Orthopaedics, University
Shoulder Injuries. Glenoid labrum injuries. SLAP Lesions
 Shoulder Injuries functional anatomy clinical perspective impingement rotator cuff injuries glenoid labrum injuries dislocation Glenoid labrum injuries SLAP lesions stable or unstable traction/compression
Shoulder Injuries functional anatomy clinical perspective impingement rotator cuff injuries glenoid labrum injuries dislocation Glenoid labrum injuries SLAP lesions stable or unstable traction/compression
Structure and Function of the Bones and Joints of the Shoulder Girdle
 Structure and Function of the Bones and Joints of the Shoulder Girdle LEARNING OBJECTIVES: At the end of this laboratory exercise the student will be able to: Palpate the important skeletal landmarks of
Structure and Function of the Bones and Joints of the Shoulder Girdle LEARNING OBJECTIVES: At the end of this laboratory exercise the student will be able to: Palpate the important skeletal landmarks of
Scapular Dyskinesis. Orthopaedic Update 2018 April 15, Peter Tang, MD, MPH, FAOA
 Scapular Dyskinesis Orthopaedic Update 2018 April 15, 2018 Peter Tang, MD, MPH, FAOA Director Center for Brachial Plexus and Nerve Injury Program Director Hand, Upper Extremity & Microvascular Surgery
Scapular Dyskinesis Orthopaedic Update 2018 April 15, 2018 Peter Tang, MD, MPH, FAOA Director Center for Brachial Plexus and Nerve Injury Program Director Hand, Upper Extremity & Microvascular Surgery
Upper Limb Biomechanics SCHOOL OF HUMAN MOVEMENT STUDIES
 Upper Limb Biomechanics Phases of throwing motion 1. Wind up Starts: initiate first movement Ends: lead leg is lifted & throwing hand removed from glove COG raised 2. Early Cocking Start: lead leg is lifted
Upper Limb Biomechanics Phases of throwing motion 1. Wind up Starts: initiate first movement Ends: lead leg is lifted & throwing hand removed from glove COG raised 2. Early Cocking Start: lead leg is lifted
Burwood Road, Concord 160 Belmore Road, Randwick
 www.orthosports.com.au 47 49 Burwood Road, Concord 160 Belmore Road, Randwick Conservative management of subacromial pathology Mel Cusi MBBS, Cert Sp Med, FACSP, FFSEM (UK) Presenting symptoms Shoulder
www.orthosports.com.au 47 49 Burwood Road, Concord 160 Belmore Road, Randwick Conservative management of subacromial pathology Mel Cusi MBBS, Cert Sp Med, FACSP, FFSEM (UK) Presenting symptoms Shoulder
Rehabilitation Guidelines for Shoulder Arthroscopy
 Rehabilitation Guidelines for Shoulder Arthroscopy The true shoulder joint is called the glenohumeral joint and consists humeral head and the glenoid. It is a ball and socket joint. Anatomy of the Shoulder
Rehabilitation Guidelines for Shoulder Arthroscopy The true shoulder joint is called the glenohumeral joint and consists humeral head and the glenoid. It is a ball and socket joint. Anatomy of the Shoulder
Rehabilitation Protocol: Massive Rotator Cuff Tear Repair
 Rehabilitation Protocol: Massive Rotator Cuff Tear Repair Department of Orthopaedic Surgery Lahey Hospital & Medical Center, Burlington 781-744-8650 Lahey Outpatient Center, Lexington 781-372-7020 Lahey
Rehabilitation Protocol: Massive Rotator Cuff Tear Repair Department of Orthopaedic Surgery Lahey Hospital & Medical Center, Burlington 781-744-8650 Lahey Outpatient Center, Lexington 781-372-7020 Lahey
Shoulder and Elbow ORTHOPAEDIC SYPMPOSIUM APRIL 8, 2017 DANIEL DOTY MD
 Shoulder and Elbow ORTHOPAEDIC SYPMPOSIUM APRIL 8, 2017 DANIEL DOTY MD Shoulder Articulations Glenohumeral Joint 2/3 total arc of motion Shallow Ball and Socket Joint Allows for excellent ROM Requires
Shoulder and Elbow ORTHOPAEDIC SYPMPOSIUM APRIL 8, 2017 DANIEL DOTY MD Shoulder Articulations Glenohumeral Joint 2/3 total arc of motion Shallow Ball and Socket Joint Allows for excellent ROM Requires
Dr. Stefan C. Muzin, MD PM&R Beth Israel Deaconess Medical Center Harvard Medical School Consultant, GE Aviation, OEHN.
 Dr. Stefan C. Muzin, MD PM&R Beth Israel Deaconess Medical Center Harvard Medical School Consultant, GE Aviation, OEHN Work Related Workshop WorkInjuries Related Injuries Workshop Think of the Big Picture
Dr. Stefan C. Muzin, MD PM&R Beth Israel Deaconess Medical Center Harvard Medical School Consultant, GE Aviation, OEHN Work Related Workshop WorkInjuries Related Injuries Workshop Think of the Big Picture
Today s session. Common Problems in Rehab. UPPER BODY REHAB ESSENTIALS TIM KEELEY FILEX 2012
 Tim Keeley B.Phty, Cred.MDT, APA Principal Physiotherapist physiofitness.com.au facebook.com/physiofitness Today s session Essential list for the upper body Rehab starting point Focussing on activation,
Tim Keeley B.Phty, Cred.MDT, APA Principal Physiotherapist physiofitness.com.au facebook.com/physiofitness Today s session Essential list for the upper body Rehab starting point Focussing on activation,
Rehabilitation Protocol: Arthroscopic Anterior Capsulolabral Repair of the Shoulder - Bankart Repair Rehabilitation Guidelines
 Rehabilitation Protocol: Arthroscopic Anterior Capsulolabral Repair of the Shoulder - Bankart Repair Rehabilitation Guidelines Department of Orthopaedic Surgery Lahey Hospital & Medical Center, Burlington
Rehabilitation Protocol: Arthroscopic Anterior Capsulolabral Repair of the Shoulder - Bankart Repair Rehabilitation Guidelines Department of Orthopaedic Surgery Lahey Hospital & Medical Center, Burlington
Mercer County Community College Donna Doulong March 8, 2013
 Mercer County Community College Donna Doulong March 8, 2013 Why strengthen the scapular muscles? The scapular thoracic articulation is the true core of the upper extremity. (Shankman & Manske, 2011, p.
Mercer County Community College Donna Doulong March 8, 2013 Why strengthen the scapular muscles? The scapular thoracic articulation is the true core of the upper extremity. (Shankman & Manske, 2011, p.
Anterior Stabilization of the Shoulder: Distal Tibial Allograft
 Anterior Stabilization of the Shoulder: Distal Tibial Allograft Name: Diagnosis: Date: Date of Surgery: Phase I Immediate Post Surgical Phase (approximately Weeks 1-3) Minimize shoulder pain and inflammatory
Anterior Stabilization of the Shoulder: Distal Tibial Allograft Name: Diagnosis: Date: Date of Surgery: Phase I Immediate Post Surgical Phase (approximately Weeks 1-3) Minimize shoulder pain and inflammatory
REHABILITATION GUIDELINES FOR ROTATOR CUFF REPAIR FOR TYPE II TEARS (MASSIVE)(+/- SUBACROMIAL DECOMPRESSION)
(+/- SUBACROMIAL DECOMPRESSION)") REHABILITATION GUIDELINES FOR ROTATOR CUFF REPAIR FOR TYPE II TEARS (MASSIVE)(+/- SUBACROMIAL DECOMPRESSION) The rehabilitation guidelines are presented in a criterion based progression. General time frames
REHABILITATION GUIDELINES FOR ROTATOR CUFF REPAIR FOR TYPE II TEARS (MASSIVE)(+/- SUBACROMIAL DECOMPRESSION) The rehabilitation guidelines are presented in a criterion based progression. General time frames
Phase I : Immediate Postoperative Phase- Protected Motion. (0-2 Weeks)
") Phase I : Immediate Postoperative Phase- Protected Motion (0-2 Weeks) Appointments Progression Criteria 2 weeks after surgery Rehabilitation appointments begin within 7-10 days of surgery, continue 1-2
Phase I : Immediate Postoperative Phase- Protected Motion (0-2 Weeks) Appointments Progression Criteria 2 weeks after surgery Rehabilitation appointments begin within 7-10 days of surgery, continue 1-2
The Shoulder Complex. Anatomy. Articulations 12/11/2017. Oak Ridge High School Conroe, Texas. Clavicle Collar Bone Scapula Shoulder Blade Humerus
 The Shoulder Complex Oak Ridge High School Conroe, Texas Anatomy Clavicle Collar Bone Scapula Shoulder Blade Humerus Articulations Sternoclavicular SC joint. Sternum and Clavicle. Acromioclavicular AC
The Shoulder Complex Oak Ridge High School Conroe, Texas Anatomy Clavicle Collar Bone Scapula Shoulder Blade Humerus Articulations Sternoclavicular SC joint. Sternum and Clavicle. Acromioclavicular AC
SHOULDER DISLOCATION & INSTABILITY Rehabilitation Considerations
 SHOULDER DISLOCATION & INSTABILITY Rehabilitation Considerations Meagan Pehnke, MS, OTR/L, CHT, CLT March 1 st, 2019 Philadelphia Surgery & Rehabilitation of the Hand: Pediatric Pre-course OUTLINE Discuss
SHOULDER DISLOCATION & INSTABILITY Rehabilitation Considerations Meagan Pehnke, MS, OTR/L, CHT, CLT March 1 st, 2019 Philadelphia Surgery & Rehabilitation of the Hand: Pediatric Pre-course OUTLINE Discuss
I (and/or my co-authors) have something to disclose.
 have something to disclose.") Shoulder Anatomy And Biomechanics Nikhil N Verma, MD Director of Sports Medicine Professor, Department of Orthopedics Rush University Team Physician, Chicago White Sox and Bulls I (and/or my co-authors)
Shoulder Anatomy And Biomechanics Nikhil N Verma, MD Director of Sports Medicine Professor, Department of Orthopedics Rush University Team Physician, Chicago White Sox and Bulls I (and/or my co-authors)
Core deconditioning Smoking Outpatient Phase 1 ROM Other
 whereby the ball does not stay properly centered in the shoulder socket during shoulder movement. This condition may be associated with impingement of the rotator cuff on the acromion bone and coracoacromial
whereby the ball does not stay properly centered in the shoulder socket during shoulder movement. This condition may be associated with impingement of the rotator cuff on the acromion bone and coracoacromial
Welcome to. Not to be copied without the express permission of EDUCATA. Copyright 2014 EDUCATA. All rights reserved. 1. How to Navigate EDUCATA
 Welcome to Copyright 2014 EDUCATA. This presentation is not to be copied in whole or in part without the express permission of EDUCATA. How to Navigate EDUCATA The Shoulder Complex Mechanics, Muscle Function
Welcome to Copyright 2014 EDUCATA. This presentation is not to be copied in whole or in part without the express permission of EDUCATA. How to Navigate EDUCATA The Shoulder Complex Mechanics, Muscle Function
Exercises to restore range of movement: Rotation
 Exercises to restore range of movement: Rotation Start position: Sitting upright with your back supported in a chair. Position your head so it is evenly balanced, looking forward. Avoid allowing your head
Exercises to restore range of movement: Rotation Start position: Sitting upright with your back supported in a chair. Position your head so it is evenly balanced, looking forward. Avoid allowing your head
Chronic Shoulder Disorders
 Chronic Shoulder Disorders Dr. Mustafa Elsingergy Consultant orthopedic surgeon Dallah Hospita Prof. Mamoun Kremli Almaarefa Medical College Contents INTRINSIC Shoulder Pain Due to causes in the shoulder
Chronic Shoulder Disorders Dr. Mustafa Elsingergy Consultant orthopedic surgeon Dallah Hospita Prof. Mamoun Kremli Almaarefa Medical College Contents INTRINSIC Shoulder Pain Due to causes in the shoulder
Shoulder Labral Tear and Shoulder Dislocation
 Shoulder Labral Tear and Shoulder Dislocation The shoulder joint is a ball and socket joint with tremendous flexibility and range of motion. The ball is the humeral head while the socket is the glenoid.
Shoulder Labral Tear and Shoulder Dislocation The shoulder joint is a ball and socket joint with tremendous flexibility and range of motion. The ball is the humeral head while the socket is the glenoid.
ER + IR = Total Motion
 Treating the Thrower s Shoulder Michael M. Reinold, PT, DPT, ATC, CSCS Introduction Common site of injury» Repetitive forces / stresses Tremendous joint forces» Anterior shear forces 1-1.5 1.5 X BW» Distraction
Treating the Thrower s Shoulder Michael M. Reinold, PT, DPT, ATC, CSCS Introduction Common site of injury» Repetitive forces / stresses Tremendous joint forces» Anterior shear forces 1-1.5 1.5 X BW» Distraction
UNDERSTANDING YOUR SHOULDERS
 It is a widely known fact that the shoulder is one of the body s most mobile joints. Unfortunately this mobility comes at a cost. With its high degree of mobility, stability is often compromised. This
It is a widely known fact that the shoulder is one of the body s most mobile joints. Unfortunately this mobility comes at a cost. With its high degree of mobility, stability is often compromised. This
Rotator Cuff Tendinopathy
 Differential Diagnosis of Rotator Cuff Disease Director of Clinical Outcomes and Research Director University of Southern California; Los Angeles, CA lmichene@pt.usc.edu http://pt.usc.edu/coor/ Rotator
Differential Diagnosis of Rotator Cuff Disease Director of Clinical Outcomes and Research Director University of Southern California; Los Angeles, CA lmichene@pt.usc.edu http://pt.usc.edu/coor/ Rotator
S p o r t s & O r t h o p a e d i c S p e c i a l i s t s A n t e r i o r I n s t a b i l i t y P r o t o c o l
 S p o r t s & O r t h o p a e d i c S p e c i a l i s t s This protocol provides appropriate guidelines for the rehabilitation of patients with anterior instability. The protocol draws evidence from the
S p o r t s & O r t h o p a e d i c S p e c i a l i s t s This protocol provides appropriate guidelines for the rehabilitation of patients with anterior instability. The protocol draws evidence from the
CLINICAL EXAMINATION OF THE SHOULDER JOINT 대한신경근골격연구회 분당제생병원재활의학과 박준성
 CLINICAL EXAMINATION OF THE SHOULDER JOINT 대한신경근골격연구회 분당제생병원재활의학과 박준성 Clinical Examination of the Shoulder Good history, full clinical examination Detailed knowledge of the anatomy solve the majority of
CLINICAL EXAMINATION OF THE SHOULDER JOINT 대한신경근골격연구회 분당제생병원재활의학과 박준성 Clinical Examination of the Shoulder Good history, full clinical examination Detailed knowledge of the anatomy solve the majority of
THE OLDER TENNIS AND GOLF ATHLETE: INJURY MANAGEMENT AND PREVENTION
 THE OLDER TENNIS AND GOLF ATHLETE: INJURY MANAGEMENT AND PREVENTION William Micheo, MD Professor and Chairman Physical Medicine, Rehabilitation, and Sports Medicine Department University of Puerto Rico
THE OLDER TENNIS AND GOLF ATHLETE: INJURY MANAGEMENT AND PREVENTION William Micheo, MD Professor and Chairman Physical Medicine, Rehabilitation, and Sports Medicine Department University of Puerto Rico
Common Surgical Shoulder Injury Repairs
 Common Surgical Shoulder Injury Repairs Mr Ilia Elkinson BHB, MBChB, FRACS (Ortho), FNZOA Orthopaedic and Upper Limb Surgeon Bowen Hospital Wellington Hospital Objectives Review pertinent anatomy of the
Common Surgical Shoulder Injury Repairs Mr Ilia Elkinson BHB, MBChB, FRACS (Ortho), FNZOA Orthopaedic and Upper Limb Surgeon Bowen Hospital Wellington Hospital Objectives Review pertinent anatomy of the
ROTATOR CUFF TENDONITIS
 Daniel P. Duggan, D.O. The Sports Clinic 23961 Calle de la Magdalena, Suite 229 Laguna Hills, CA 92653 Phone: (949) 581-7001 Fax: (949) 581-8410 http://orthodoc.aaos.org/danielduggando The shoulder is
Daniel P. Duggan, D.O. The Sports Clinic 23961 Calle de la Magdalena, Suite 229 Laguna Hills, CA 92653 Phone: (949) 581-7001 Fax: (949) 581-8410 http://orthodoc.aaos.org/danielduggando The shoulder is
8/8/2017. Partial Rotator Cuff Tears. Disclosures. Prevalence. Geoffrey S. Van Thiel, MD/MBA OrthoIllinois
 Partial Rotator Cuff Tears Geoffrey S. Van Thiel, MD/MBA OrthoIllinois Associate Professor Rush University Medical Center Associate Professor University of Illinois Team Physician US National Soccer Team
Partial Rotator Cuff Tears Geoffrey S. Van Thiel, MD/MBA OrthoIllinois Associate Professor Rush University Medical Center Associate Professor University of Illinois Team Physician US National Soccer Team
Dr. Denard s Rehabilitation Protocols Arthroscopic Shoulder Surgery
 2780 E. Barnett Rd Medford, OR 97530 541-779-6250 Dr. Denard s Rehabilitation Protocols Arthroscopic Shoulder Surgery These rehabilitation protocols are based on current studies detailing healing time
2780 E. Barnett Rd Medford, OR 97530 541-779-6250 Dr. Denard s Rehabilitation Protocols Arthroscopic Shoulder Surgery These rehabilitation protocols are based on current studies detailing healing time
Management of Shoulder Pain in Persons with SCI
 www.fisiokinesiterapia.biz Management of Shoulder Pain in Persons with SCI Research Program Development from a Clinical Perspective Identification of the problem Identification of potential cause Development
www.fisiokinesiterapia.biz Management of Shoulder Pain in Persons with SCI Research Program Development from a Clinical Perspective Identification of the problem Identification of potential cause Development
SHOULDER IMPINGEMENT / ROTATOR CUFF TENDONITIS / SUBACROMIAL BURSITIS
 SHOULDER IMPINGEMENT / ROTATOR CUFF TENDONITIS / SUBACROMIAL BURSITIS The terms impingement, rotator cuff tendonitis, and subacromial bursitis, all refer to a spectrum of the same condition. Anatomy The
SHOULDER IMPINGEMENT / ROTATOR CUFF TENDONITIS / SUBACROMIAL BURSITIS The terms impingement, rotator cuff tendonitis, and subacromial bursitis, all refer to a spectrum of the same condition. Anatomy The
Incorporating OMM to Enhance Your Clinical Practice Osteopathic diagnosis and approach to the upper extremity
 Incorporating OMM to Enhance Your Clinical Practice Osteopathic diagnosis and approach to the upper extremity Sheldon C. Yao, D.O. Acting Department Chair March 1, 2013 Clinical significance Upper extremity
Incorporating OMM to Enhance Your Clinical Practice Osteopathic diagnosis and approach to the upper extremity Sheldon C. Yao, D.O. Acting Department Chair March 1, 2013 Clinical significance Upper extremity
Shoulder examination. P Sripathi Rao Arthroscopy & Sports Injuries Unit Dean, Kasturba Medical College
 Shoulder examination P Sripathi Rao Arthroscopy & Sports Injuries Unit Dean, Kasturba Medical College Manipal University, Manipal Common symptoms Tingling Numbness Pain Loss of movements Weakness Approach
Shoulder examination P Sripathi Rao Arthroscopy & Sports Injuries Unit Dean, Kasturba Medical College Manipal University, Manipal Common symptoms Tingling Numbness Pain Loss of movements Weakness Approach
Upper Extremity Injuries in Youth Baseball: Causes and Prevention
 Upper Extremity Injuries in Youth Baseball: Causes and Prevention Biomechanics Throwing a baseball is an unnatural movement Excessively high forces are generated at the elbow and shoulder Throwing requires
Upper Extremity Injuries in Youth Baseball: Causes and Prevention Biomechanics Throwing a baseball is an unnatural movement Excessively high forces are generated at the elbow and shoulder Throwing requires
Shoulder Injuries: Treatments that Work, Do Not Work, and When ENOUGH is Enough? Mark Ganjianpour, M.D. Beverly Hills, CA April 20, 2012
 Shoulder Injuries: Treatments that Work, Do Not Work, and When ENOUGH is Enough? Mark Ganjianpour, M.D. Beverly Hills, CA April 20, 2012 Multiaxial ball and socket Little Inherent Instability Glenohumeral
Shoulder Injuries: Treatments that Work, Do Not Work, and When ENOUGH is Enough? Mark Ganjianpour, M.D. Beverly Hills, CA April 20, 2012 Multiaxial ball and socket Little Inherent Instability Glenohumeral
Anatomical Considerations/ Pathophysiology The shoulder is the most mobile joint in the body. : Three bones:
 Introduction Musculoskeletal training is generally underrepresented in medical training and residency curriculums. There is a general deficit in musculoskeletal knowledge amongst current medical students,
Introduction Musculoskeletal training is generally underrepresented in medical training and residency curriculums. There is a general deficit in musculoskeletal knowledge amongst current medical students,
Eric Magrum PT, DPT, OCS, FAAOMPT Orthopaedic Manual Physical Therapy Series Charlottesville
 SHOULDER CASE 3 Eric Magrum PT, DPT, OCS, FAAOMPT Orthopaedic Manual Physical Therapy Series Charlottesville 2017-2018 Reproduction Without Consent 1 Reproduction Without Consent 2 Instability - Sulcus
SHOULDER CASE 3 Eric Magrum PT, DPT, OCS, FAAOMPT Orthopaedic Manual Physical Therapy Series Charlottesville 2017-2018 Reproduction Without Consent 1 Reproduction Without Consent 2 Instability - Sulcus
Active-Assisted Stretches
 1 Active-Assisted Stretches Adequate flexibility is fundamental to a functional musculoskeletal system which represents the foundation of movement efficiency. Therefore a commitment toward appropriate
1 Active-Assisted Stretches Adequate flexibility is fundamental to a functional musculoskeletal system which represents the foundation of movement efficiency. Therefore a commitment toward appropriate
Orthopaedic Manual Physical Therapy Series Orthopaedic Manual Physical Therapy Series
 SHOULDER CASE3 Eric Magrum PT, DPT, OCS, FAAOMPT Orthopaedic Manual Physical Therapy Series Charlottesville 2017-2018 Reproduction Without Consent 1 Instability - Sulcus Sign Instability - Load and Shift
SHOULDER CASE3 Eric Magrum PT, DPT, OCS, FAAOMPT Orthopaedic Manual Physical Therapy Series Charlottesville 2017-2018 Reproduction Without Consent 1 Instability - Sulcus Sign Instability - Load and Shift
FUNCTIONAL ANATOMY OF SHOULDER JOINT
 FUNCTIONAL ANATOMY OF SHOULDER JOINT ARTICULATION Articulation is between: The rounded head of the Glenoid cavity humerus and The shallow, pear-shaped glenoid cavity of the scapula. 2 The articular surfaces
FUNCTIONAL ANATOMY OF SHOULDER JOINT ARTICULATION Articulation is between: The rounded head of the Glenoid cavity humerus and The shallow, pear-shaped glenoid cavity of the scapula. 2 The articular surfaces
REHABILITATION GUIDELINES FOR ARTHROSCOPIC CAPSULAR SHIFT
 REHABILITATION GUIDELINES FOR ARTHROSCOPIC CAPSULAR SHIFT The rehabilitation guidelines are presented in a criterion based progression. General time frames are given for reference to the average, but individual
REHABILITATION GUIDELINES FOR ARTHROSCOPIC CAPSULAR SHIFT The rehabilitation guidelines are presented in a criterion based progression. General time frames are given for reference to the average, but individual
Breakout Session #7: Manual therapy for shoulder pain and limited mobility
 Northwestern University Feinberg School of Medicine Breakout Session #7: Manual therapy for shoulder pain and limited mobility @Amee_S Objectives 1. Demonstrate the examination procedures and describe
Northwestern University Feinberg School of Medicine Breakout Session #7: Manual therapy for shoulder pain and limited mobility @Amee_S Objectives 1. Demonstrate the examination procedures and describe
Rehabilitation for MDI in the Female Athlete. John Dale PT, DPT, SCS, ATC, CSCS Andrew Naylor PT, DPT, SCS
 Rehabilitation for MDI in the Female Athlete John Dale PT, DPT, SCS, ATC, CSCS Andrew Naylor PT, DPT, SCS Disclosure No relevant financial relationship exists Session Learning Objectives Discuss etiology
Rehabilitation for MDI in the Female Athlete John Dale PT, DPT, SCS, ATC, CSCS Andrew Naylor PT, DPT, SCS Disclosure No relevant financial relationship exists Session Learning Objectives Discuss etiology
Prof. Dr. Birgit Castelein
 Annual meeting of the Danish Society for Surgery of the shoulder and of the elbow April 21 2017 Aarhus, Denmark Prof. Dr. Birgit Castelein Birgit.Castelein@ugent.be PhD: Analysis of recruitment of the
Annual meeting of the Danish Society for Surgery of the shoulder and of the elbow April 21 2017 Aarhus, Denmark Prof. Dr. Birgit Castelein Birgit.Castelein@ugent.be PhD: Analysis of recruitment of the
Anterior Stabilization of the Shoulder: Latarjet Protocol
 Robert K. Fullick, MD 6400 Fannin Street, Suite 1700 Houston, Texas 77030 Ph.: 713-486-7543 / Fx.: 713-486-5549 Anterior Stabilization of the Shoulder: Latarjet Protocol The intent of this protocol is
Robert K. Fullick, MD 6400 Fannin Street, Suite 1700 Houston, Texas 77030 Ph.: 713-486-7543 / Fx.: 713-486-5549 Anterior Stabilization of the Shoulder: Latarjet Protocol The intent of this protocol is