EMS Spinal Assessment and Precautions
|
|
|
- June Nichols
- 5 years ago
- Views:
Transcription

1 EMS Spinal Assessment and Precautions Adapted from a presentation prepared by Chelsea C. White IV, MD, NREMT-P Medical Director, Bernalillo County Fire Department Robert M. Domeier, MD, EMS Medical Director, Washtenaw/Livingston Medical Control Authority


2 Latest Spinal Injury Guidelines In July, 2013, NAEMSP and ACS-COT released a joint position paper on EMS Spinal Precautions and the Use of the Long Backboard Highlights: Utilization of backboards for spinal immobilization during transport should be judicious, so that the potential benefits outweigh the risks
3 Latest Clinical Guidelines Highlights: Patients with penetrating trauma to the head, neck, or torso and no evidence of spinal injury should not be immobilized on a backboard Spinal precautions can be maintained by application of a rigid cervical collar and securing the patient to the EMS stretcher, and may be most appropriate for: Patients who are found to be ambulatory at the scene Patients who must be transported for a protracted time, particularly prior to interfacility transfer
4



5 Backboards have been a part of EMS since the beginning! Spinal immobilization a key feature of early Emergency Medical Technician training

6 1960s: Growing Awareness of Spinal Injuries The most frequently mishandled injuries, made worse by hasty and rough movement from a vehicle or other accident scene, are fractures of the spine and the femur. J.D. Farrington, MD, from DEATH IN A DITCH, American College of Surgeons, 1967

7 Early Spinal Injury Research A 1963 survey of a large series of patients with fatal injuries treated at the Edinburgh Royal Infirmary showed that 25% of fatal complications occurred during the period between the accident and arrival in the ED A community depends on the expertise of its emergency personnel to correctly manage high risk crises and potentiate recovery
 had incontrovertible evidence of delayed paralysis, attributed to either pre- or in-hospital inept handling Authors suspected but could not prove that a larger number undoubtedly suffered this")
8 Early Spinal Injury Research A 1965 retrospective study of 958 spinal cord injury patients in Toronto attempted to quantify serious cord damage due to inept handling of the patients Only 29 patients (3%) had incontrovertible evidence of delayed paralysis, attributed to either pre- or in-hospital inept handling Authors suspected but could not prove that a larger number undoubtedly suffered this fate

9 Birth of Spinal Immobilization In 1966, USAF Col. L. C. Kossuth first described the use of the long backboard to move a victim from the vehicle with a minimum of additional trauma Such movement was to occur with due regard to maximum gentleness

10

11 Backboards Cause Pain 1989 study of 170 trauma victims eventually discharged from a major ED showed a significant reduction in c- and l- spine pain when patients were allowed off the boards 21% had cervical P/T on the board but not off suggested that the immobilization process or the boards themselves cause pain that otherwise would not be there 1993 study caused 100% of 21 healthy volunteers to report pain within 30 minutes of being strapped to a backboard Headache, sacral, lumbar, and mandibular pain most common
12 Backboards Cause Pressure Sores A prospective study at Charity Hospital 1988 of the association between immobilization in the immediate postinjury period and the development of pressure ulcers in spinal cordinjured patients Time on the spinal board was significantly associated with ulcers developing within 8 days

13 Backboards Cause Pressure Sores A 1995 study at Methodist Hospital of Indiana measured the interface (contact) pressures over bony prominences of 20 patients on wooden backboards over 80 minutes Interface pressure > 32 mm Hg causes capillaries collapse, resulting in ischemia and pressure ulceration. This study measured mean interface pressures as high as 149 mm Hg at the sacrum, 59 mm Hg at occiput, and 51 mm Hg at heels

14 Backboards Create Respiratory Compromise 1987 study at Beaumont Hospital of healthy, backboarded males concluded that backboard straps significantly decrease pulmonary function Similar study 1999 showed 15% respiratory restriction in backboarded adult subjects Pediatric study in 1991 showed decreased FVC in children due to backboard straps

15 5 year retrospective chart review at University of New Mexico and University of Malaysia hospitals All 454 patients with acute spinal cord injuries included during the 5 year study period None of the 120 U. Malaysia patients were immobilized All 334 U. of NM patients were immobilized in the field Hospitals and treatment otherwise equivalent Results: 2x MORE neurologic disability in the University of New Mexico patients

16 How well do we immobilize anyway? Convenience sample of 50 low acuity backboarded subjects at one Level 1 ED 30% had at least 1 point where a strap or tape did not secure the head 70% had 1 strap with >4 cm slack 12% had all 4 straps with >4 cm slack at 4 cm, movement in any direction along the board is both possible and probable A well secured head and mobile body creates moment arm about the neck
, regardless of a backboard or")
17 Backboards don t make patients lie still A violent or agitated patient is going to fight against a backboard, threatening his/her spine A cooperative patient is going to lie still when asked (or if it hurts to move), regardless of a backboard or straps
18 C-Spine imaging in the ED By the late 1980s, physicians realized that some patients with neck pain did not need x- rays to rule out spine injury Several studies showed that patients could be clinically cleared without exposing them to radiation

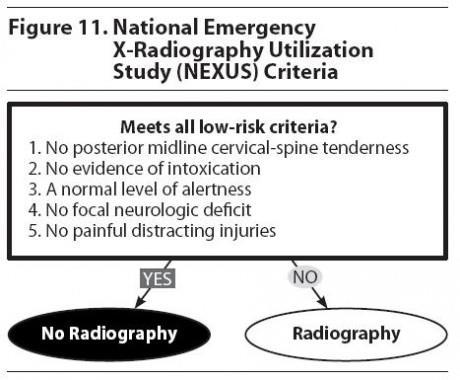
19 NEXUS and Canadian C-Spine rules These were the two major studies showing the safety of clinical spine clearance by emergency physicians NEXUS = National Emergency X-Radiography Utilization Group, formed to reduce patient exposure to x-rays Canadian C-Spine rule developed for similar reasons
20

21
22 Selective Spinal Immobilization Multiple studies in the late 1990s showed the safety of field spinal clearance by EMS providers These studies showed that EMS providers were able to apply NEXUS and CCR criteria in the field Goal was to reduce the amount of patients transported on backboards

23 This REDUCED backboard use Backboard use has decreased significantly BUT, patients with positive spinal assessments still ride on backboards Many of these patients do not actually have spinal injury
24 Goal: protect unstable spine fractures without causing new problems Backboards have been proven to cause: Pain Pressure sores Respiratory compromise Backboards have NOT been shown to prevent: Spinal movement Further neurologic injury
25 Recommendation Best available evidence supports removing patients from backboards as soon as possible, even if spinal injury is suspected This already happens in most EDs shortly after a backboarded patient arrives Given the similarities between an ambulance cot and an ED cot, patients with suspected spinal injury should be removed from the backboard once safely on the ambulance cot
26 How do we protect the spine of a patient who MAY have a spine injury without the risks of a backboard?
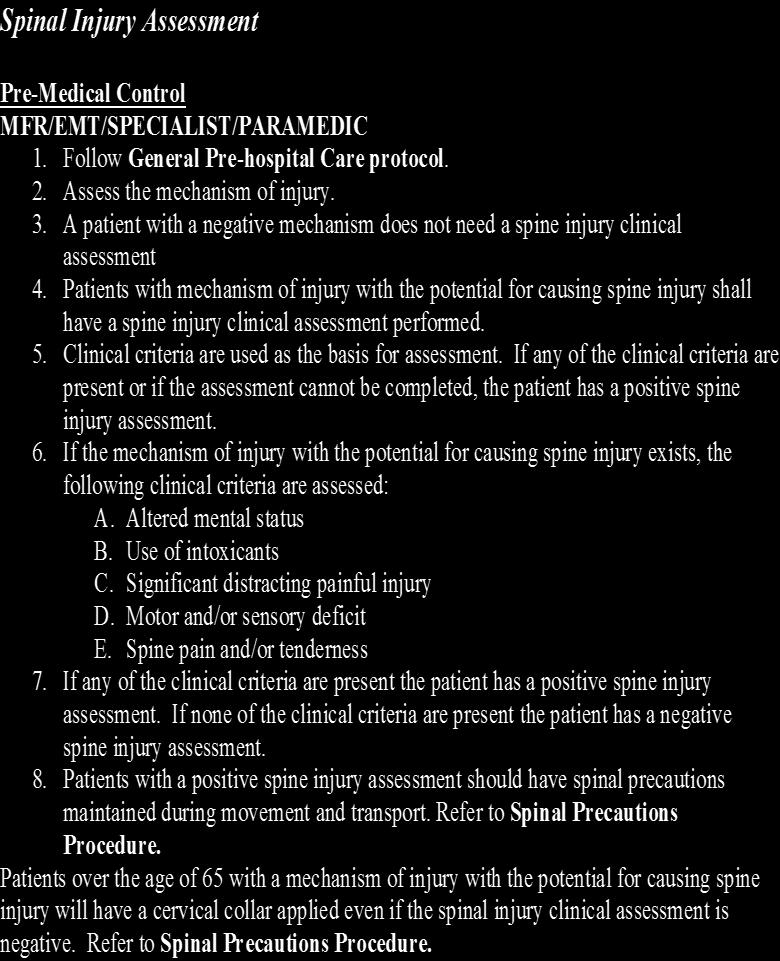
27 Spinal Injury Assessment NEW Michigan Protocol for Spine Injury Assessment: Pre-Medical Control MFR/EMT/SPECIALIST/PARAMEDIC 1. Follow General Pre-hospital Care protocol. 2. Assess the mechanism of injury. 3. A patient with a negative mechanism does not need a spine injury clinical assessment 4. Patients with mechanism of injury with the potential for causing spine injury shall have a spine injury clinical assessment performed. 5. Clinical criteria are used as the basis for assessment. If any of the clinical criteria are present or if the assessment cannot be completed, the patient has a positive spine injury assessment. 6. If the mechanism of injury with the potential for causing spine injury exists, the following clinical criteria are assessed: A. Altered mental status B. Use of intoxicants C. Significant distracting painful injury D. Motor and/or sensory deficit E. Spine pain and/or tenderness 7. If any of the clinical criteria are present the patient has a positive spine injury assessment. If none of the clinical criteria are present the patient has a negative spine injury assessment. 8. Patients with a positive spine injury assessment should have spinal precautions maintained during movement and transport. Refer to Spinal Precautions Procedure. Patients over the age of 65 with a mechanism of injury with the potential for causing spine injury will have a cervical collar applied even if the spinal injury clinical assessment is negative. Refer to Spinal Precautions Procedure.
28 Spinal Injury Assessment Pre-Medical Control MFR/EMT/SPECIALIST/PARAMEDIC 1. Follow General Pre-hospital Care protocol. 2. Assess the mechanism of injury. 3. A patient with a negative mechanism does not need a spine injury clinical assessment 4. Patients with mechanism of injury with the potential for causing spine injury shall have a spine injury clinical assessment performed. 5. Clinical criteria are used as the basis for assessment. If any of the clinical criteria are present or if the assessment cannot be completed, the patient has a positive spine injury assessment. 6. If the mechanism of injury with the potential for causing spine injury exists, the following clinical criteria are assessed: A. Altered mental status B. Use of intoxicants C. Significant distracting painful injury D. Motor and/or sensory deficit E. Spine pain and/or tenderness 7. If any of the clinical criteria are present the patient has a positive spine injury assessment. If none of the clinical criteria are present the patient has a negative spine injury assessment. 8. Patients with a positive spine injury assessment should have spinal precautions maintained during movement and transport. Refer to Spinal Precautions Procedure. Patients over the age of 65 with a mechanism of injury with the potential for causing spine injury will have a cervical collar applied even if the spinal injury clinical assessment is negative. Refer to Spinal Precautions Procedure. If mechanism exists for spinal injury: Examples: Fall Motor vehicle crash Assault with significant head, neck, or back trauma Anything else that could cause spinal injury
29 Spinal Injury Assessment Pre-Medical Control MFR/EMT/SPECIALIST/PARAMEDIC 1. Follow General Pre-hospital Care protocol. 2. Assess the mechanism of injury. 3. A patient with a negative mechanism does not need a spine injury clinical assessment 4. Patients with mechanism of injury with the potential for causing spine injury shall have a spine injury clinical assessment performed. 5. Clinical criteria are used as the basis for assessment. If any of the clinical criteria are present or if the assessment cannot be completed, the patient has a positive spine injury assessment. 6. If the mechanism of injury with the potential for causing spine injury exists, the following clinical criteria are assessed: A. Altered mental status B. Use of intoxicants C. Significant distracting painful injury D. Motor and/or sensory deficit E. Spine pain and/or tenderness 7. If any of the clinical criteria are present the patient has a positive spine injury assessment. If none of the clinical criteria are present the patient has a negative spine injury assessment. 8. Patients with a positive spine injury assessment should have spinal precautions maintained during movement and transport. Refer to Spinal Precautions Procedure. Patients over the age of 65 with a mechanism of injury with the potential for causing spine injury will have a cervical collar applied even if the spinal injury clinical assessment is negative. Refer to Spinal Precautions Procedure. Perform Spinal Assessment 6.A-C. Evaluate if the patient can give a reliable exam: Look for: Are they altered? Are they intoxicated? Are they distracted by other injury?
30 Spinal Injury Assessment Pre-Medical Control MFR/EMT/SPECIALIST/PARAMEDIC 1. Follow General Pre-hospital Care protocol. 2. Assess the mechanism of injury. 3. A patient with a negative mechanism does not need a spine injury clinical assessment 4. Patients with mechanism of injury with the potential for causing spine injury shall have a spine injury clinical assessment performed. 5. Clinical criteria are used as the basis for assessment. If any of the clinical criteria are present or if the assessment cannot be completed, the patient has a positive spine injury assessment. 6. If the mechanism of injury with the potential for causing spine injury exists, the following clinical criteria are assessed: A. Altered mental status B. Use of intoxicants C. Significant distracting painful injury D. Motor and/or sensory deficit E. Spine pain and/or tenderness 7. If any of the clinical criteria are present the patient has a positive spine injury assessment. If none of the clinical criteria are present the patient has a negative spine injury assessment. 8. Patients with a positive spine injury assessment should have spinal precautions maintained during movement and transport. Refer to Spinal Precautions Procedure. Patients over the age of 65 with a mechanism of injury with the potential for causing spine injury will have a cervical collar applied even if the spinal injury clinical assessment is negative. Refer to Spinal Precautions Procedure. Perform Spinal Injury Assessment Any unexplained focal motor or sensory neurologic deficit Pain or tenderness in posterior midline over spine

31 Positive Spinal Assessment

32 POSITIVE SPINAL ASSESSMENT means there is a POSSIBILITY for SPINE and/or SPINAL CORD INJURY Spinal Precautions Procedure should be followed

33 Michigan Spinal Precautions Procedure

34 Michigan Spinal Precautions Procedure
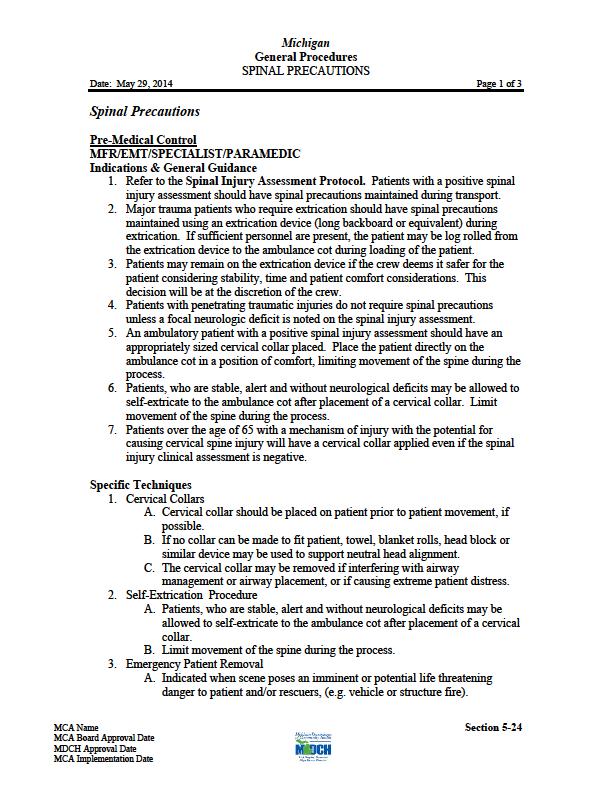
35 Spinal Precautions Procedure Indications & General Guidance 1. Refer to the Spinal Injury Assessment Protocol. Patients with a positive spinal injury assessment should have spinal precautions maintained during transport. 2. Major trauma patients who require extrication should have spinal precautions maintained using an extrication device (long backboard or equivalent) during extrication. If sufficient personnel are present, the patient may be log rolled from the extrication device to the ambulance cot during loading of the patient. 3. Patients may remain on the extrication device if the crew deems it safer for the patient considering stability, time and patient comfort considerations. This decision will be at the discretion of the crew. Notes: 1. Patients with a positive spinal injury assessment should have spinal precaution maintained 2. Log roll patients to the ambulance cot when possible 3. EMS crews may keep the patient on the extrication device for transport as needed. It may be quicker to log roll the patient onto the ambulance cot than to secure the patient to the extrication device (backboard) and then the cot.
36 Spinal Precautions Procedure Indications & General Guidance 4. Patients with penetrating traumatic injuries do not require spinal precautions unless a focal neurologic deficit is noted on the spinal injury assessment. 5. An ambulatory patient with a positive spinal injury assessment should have an appropriately sized cervical collar placed. Place the patient directly on the ambulance cot in a position of comfort, limiting movement of the spine during the process. 6. Patients, who are stable, alert and without neurological deficits may be allowed to self-extricate to the ambulance cot after placement of a cervical collar. Limit movement of the spine during the process. Notes: 4. Penetrating trauma patients do not require spinal precautions. If a neurologic deficit is noted maintain spinal precautions but no backboard is needed. 5. For ambulatory patients with a positive assessment place a collar and put the patient on the ambulance cot. No standing takedowns. 6. Patients may self-extricate when possible. Patients who self extricate have less cervical motion than when extricated by rescuers.
37 Spinal Precautions Procedure Indications & General Guidance 7. Patients over the age of 65 with a mechanism of injury with the potential for causing cervical spine injury will have a cervical collar applied even if the spinal injury clinical assessment is negative. Notes: 7. Place the patient over 65 with a potential mechanism and negative injury assessment in a collar in a position of comfort Why? Our spinal assessment tool the same one we have used for years to decide whether or not to backboard is not 100% accurate (but it is very close) Most of the false negatives are in patients >65
38 Spinal Precautions Procedure Specific Techniques 1. Cervical Collars A. Cervical collar should be placed on patient prior to patient movement, if possible. B. If no collar can be made to fit patient, towel, blanket rolls, head block or similar device may be used to support neutral head alignment. C. The cervical collar may be removed if interfering with airway management or airway placement, or if causing extreme patient distress. 2. Self-Extrication Procedure A. Patients, who are stable, alert and without neurological deficits may be allowed to self-extricate to the ambulance cot after placement of a cervical collar. B. Limit movement of the spine during the process. 3. Emergency Patient Removal A. Indicated when scene poses an imminent or potential life threatening danger to patient and/or rescuers, (e.g. vehicle or structure fire). B. Remove the patient from danger while best attempt is made to maintain spinal precautions. C. Rapid Extrication is indicated when patient condition is unstable (i.e.: airway or breathing compromise, shock, unconsciousness, or need for immediate intervention). 4. Long Extrication Device (e.g. long Backboard, scoop stretcher, basket stretcher) A. Indicated when patient requires spinal precautions and the patient condition prevents self-extrication. B. Patient's head and cervical spine should be manually stabilized. C. Rescuers should place the patient in a stable, neutral position where space is created to place backboard or other long extrication device in position near the patient. D. Move the patient to supine position on the long extrication device. E. The patient is secured to the device with torso straps applied before head stabilization. F. Head stabilization material should be placed to allow for movement of the lower jaw to facilitate possible airway management. G. The extrication device is used to move the patient to the ambulance cot.
39 Spinal Precautions Procedure Specific Techniques 5. Log Roll Procedure A. Cervical collar should be placed when indicated. B. Place the backboard or equivalent behind the patient. C. Patient is log rolled, maintaining neutral alignment of spine and extremities. D. Log roll procedure requires 2 or more personnel in contact with the patient. E. If log roll is not possible, patient should be moved to board or equivalent while attempting to maintain neutral alignment spinal precautions. F. Patient is secured to the backboard or equivalent for movement to the ambulance cot. G. Head stabilization materials such as foam pads, blanket rolls may be used to prevent lateral motion. Pad under the head when feasible. H. If sufficient personnel are present, the patient should be log rolled from the extrication device to the ambulance cot during loading of the patient. I. When log roll on to the ambulance cot is impractical, secure the patient to the extrication device and ambulance cot for transport. 6. Spinal Precautions A. Once the patient is placed on the ambulance cot, if no extrication device is still in place, secure the patient with seatbelts in a supine position, or in position of comfort if a supine position is not tolerated. B. Head may be supported with head block or similar device to prevent rotation if needed. Padding should be placed under the head when practical. Do not tape the head to the ambulance cot.
40 Spinal Precautions Procedure Special Considerations 1. Hypoventilation is likely to occur with spinal cord injury above the diaphragm. Quality of ventilation should be monitored closely with support offered early. 2. Spinal/neurogenic shock may result from high spinal cord injury. Monitor patient for signs of shock. Refer to Shock Protocol. 3. Spinal precautions in the patient wearing a helmet should be according to the Helmet Removal Procedure. 4. Manual spinal precautions in the obtunded patient must be initiated and continued until the patient is secured to the ambulance cot. 5. Patients who are markedly agitated, combative or confused may not be able to follow commands and cooperate with minimizing spinal movement. Rigid immobilization should be avoided if it contributes to patient combativeness. Patients may remain on the backboard if the crew deems it safer for the patient, and this will be at the discretion of the crew.
41 Spinal Precautions Procedure Special Considerations 6. Manual in line stabilization must be used during any procedure that risks head or neck movement, such as endotracheal intubation. If manual cervical stabilization is hampering efforts to intubate the patient, the neck should be allowed to move as needed to secure the airway. An unsecured airway is a greater danger to the patient than a spinal fracture. 7. Document spinal precautions techniques utilized. 8. Document the patient s neurologic status before and after establishing spinal precautions when possible. 9. Pediatric Patients and Car Seats: a. Infants restrained in a rear-facing car seat may be immobilized and extricated in the car seat. The child may remain in the car seat if the immobilization is secure and his/her condition allows (no signs of respiratory distress or shock). b. Children restrained in a car seat (with a high back) may be immobilized and extricated in the car seat; however, once removed from the vehicle, the child should have spinal precautions maintained as for an adult. c. Children restrained in a booster seat (without a back) need to be extricated and immobilized following standard procedures.

42

43

44
45 Questions?
MEDICAL CONTROL POLICY STATEMENT/ADVISORY. Re: Spinal Injury Assessment & Spinal Precautions Procedure
 MEDICAL CONTROL POLICY STATEMENT/ADVISORY No. 2015-01 Date: January 20, 2015 Re: Spinal Injury Assessment & Spinal Precautions Procedure Office of the Medical Director Noel Wagner, MD, NREMT-P 1000 Houghton
MEDICAL CONTROL POLICY STATEMENT/ADVISORY No. 2015-01 Date: January 20, 2015 Re: Spinal Injury Assessment & Spinal Precautions Procedure Office of the Medical Director Noel Wagner, MD, NREMT-P 1000 Houghton
7/15/2016 ALL TIED UP. Spinal Immobilization; The most up to date recommendations following trauma. Kelly Miller RN, CFRN, EMT, CMTE
 ALL TIED UP Spinal Immobilization; The most up to date recommendations following trauma. Kelly Miller RN, CFRN, EMT, CMTE Objectives Understand where the past 30 years of pre-hospital spinal immobilization
ALL TIED UP Spinal Immobilization; The most up to date recommendations following trauma. Kelly Miller RN, CFRN, EMT, CMTE Objectives Understand where the past 30 years of pre-hospital spinal immobilization
Heidi Lako-Adamson, MD, NRP, FAEMS FM Ambulance and Sanford EMS Education Medical Director
 Heidi Lako-Adamson, MD, NRP, FAEMS FM Ambulance and Sanford EMS Education Medical Director Spinal cord injury statistics. Definition of spinal motion restriction. Difference between spinal motion restriction
Heidi Lako-Adamson, MD, NRP, FAEMS FM Ambulance and Sanford EMS Education Medical Director Spinal cord injury statistics. Definition of spinal motion restriction. Difference between spinal motion restriction
10O SPLINTING OF INJURIES ADULT & PEDIATRIC. 10Oa: Axial/Spine with Selective Spinal Motion Restriction Adult & Pediatric:
 10O SPLINTING OF INJURIES ADULT & PEDIATRIC EMERGENCY MEDICAL RESPONDER EMT EMT-INTERMEDIATE 85 ADVANCED EMT PARAMEDIC 10Oa: Axial/Spine with Selective Spinal Motion Restriction Adult & Pediatric: Many
10O SPLINTING OF INJURIES ADULT & PEDIATRIC EMERGENCY MEDICAL RESPONDER EMT EMT-INTERMEDIATE 85 ADVANCED EMT PARAMEDIC 10Oa: Axial/Spine with Selective Spinal Motion Restriction Adult & Pediatric: Many
Selective Spine Assessment & Spinal Motion Restriction
 Selective Spine Assessment & Spinal Motion Restriction Supersedes: 02-09-15 Effective: 10-20-15 Spinal cord injury may be the result of direct blunt and/or penetrating trauma, compression forces (axial
Selective Spine Assessment & Spinal Motion Restriction Supersedes: 02-09-15 Effective: 10-20-15 Spinal cord injury may be the result of direct blunt and/or penetrating trauma, compression forces (axial
SPINAL IMMOBILIZATION
 Spinal Immobilization Decision Assessment Recent studies have shown an increase in mortality for patients with isolated penetrating trauma who are spinally immobilized. Therefore spinal immobilization
Spinal Immobilization Decision Assessment Recent studies have shown an increase in mortality for patients with isolated penetrating trauma who are spinally immobilized. Therefore spinal immobilization
Introduction. Objectives C-Spine: Where Are We Now? NAEMSP Medical Director Course 1/9/2013
 NAEMSP Medical Director Course 1/9/2013 Objectives C-Spine: Where Are We Now? Robert M. Domeier, MD EMS Medical Director Washtenaw/Livingston Medical Control Authority Department of Emergency Medicine
NAEMSP Medical Director Course 1/9/2013 Objectives C-Spine: Where Are We Now? Robert M. Domeier, MD EMS Medical Director Washtenaw/Livingston Medical Control Authority Department of Emergency Medicine
INTERNATIONAL TRAUMA LIFE SUPPORT
 INTERNATIONAL TRAUMA LIFE SUPPORT LONG BACKBOARD USE FOR SPINAL MOTION RESTRICTION OF THE TRAUMA PATIENT The guidelines and references contained in this document are current as of the date of publication
INTERNATIONAL TRAUMA LIFE SUPPORT LONG BACKBOARD USE FOR SPINAL MOTION RESTRICTION OF THE TRAUMA PATIENT The guidelines and references contained in this document are current as of the date of publication
Controversies in Spinal Immobilization
 Controversies in Spinal Immobilization Ken Berumen, BSN, MD, FACEP Medical Director El Paso Fire Department Medical Director Emergency Services District #1 Network Director EM Sierra Providence Health
Controversies in Spinal Immobilization Ken Berumen, BSN, MD, FACEP Medical Director El Paso Fire Department Medical Director Emergency Services District #1 Network Director EM Sierra Providence Health
XXX Spinal Motion Restriction
 Nor-Cal EMS Policy & Procedure Manual NAME OF MODULE XXX Purpose: The purpose of this protocol is to protect patients with signs and symptoms of spinal injuries and those who have the potential for spinal
Nor-Cal EMS Policy & Procedure Manual NAME OF MODULE XXX Purpose: The purpose of this protocol is to protect patients with signs and symptoms of spinal injuries and those who have the potential for spinal
Overview. Overview. Chapter 30. Injuries to the Head and Spine 9/11/2012. Review of the Nervous and Skeletal Systems. Devices for Immobilization
 Chapter 30 Injuries to the Head and Spine Slide 1 Overview Review of the Nervous and Skeletal Systems The Nervous System The Skeletal System Devices for Immobilization Cervical Spine Short Backboards Long
Chapter 30 Injuries to the Head and Spine Slide 1 Overview Review of the Nervous and Skeletal Systems The Nervous System The Skeletal System Devices for Immobilization Cervical Spine Short Backboards Long
NEW SPINAL PRECAUTION STANDARDS
 NEW SPINAL PRECAUTION STANDARDS July 31, 2015 Dane Van Horn B.S., CCEMT-P Field Supervisor - Life EMS Ambulance Disclosure I have no relevant financial relationships or conflicts of interest to disclose
NEW SPINAL PRECAUTION STANDARDS July 31, 2015 Dane Van Horn B.S., CCEMT-P Field Supervisor - Life EMS Ambulance Disclosure I have no relevant financial relationships or conflicts of interest to disclose
Shenandoah Co. Fire & Rescue. Injuries to. and Spine. December EMS Training Bill Streett Training Section Chief
 Shenandoah Co. Fire & Rescue Injuries to the Head and Spine December EMS Training Bill Streett Training Section Chief C.E. Card Information BLS Providers 2 Cards / Provider Category 1 Course # Blank Topic#
Shenandoah Co. Fire & Rescue Injuries to the Head and Spine December EMS Training Bill Streett Training Section Chief C.E. Card Information BLS Providers 2 Cards / Provider Category 1 Course # Blank Topic#
To protect patients exhibiting signs and symptoms of spinal injuries and those who have the potential for spinal injuries.
 POLICY T1 SPINAL MOTION RESTRICTION Effective Date: January 1, 2017 Last Review Date: January 1, 2017 New Policy Next Review Date: January 2019 Purpose: To protect patients exhibiting signs and symptoms
POLICY T1 SPINAL MOTION RESTRICTION Effective Date: January 1, 2017 Last Review Date: January 1, 2017 New Policy Next Review Date: January 2019 Purpose: To protect patients exhibiting signs and symptoms
Chapter 32. Objectives. Objectives 01/09/2013. Spinal Column and Spinal Cord Trauma
 Chapter 32 Spinal Column and Spinal Cord Trauma Prehospital Emergency Care, Ninth Edition Joseph J. Mistovich Keith J. Karren Copyright 2010 by Pearson Education, Inc. All rights reserved. Objectives 1.
Chapter 32 Spinal Column and Spinal Cord Trauma Prehospital Emergency Care, Ninth Edition Joseph J. Mistovich Keith J. Karren Copyright 2010 by Pearson Education, Inc. All rights reserved. Objectives 1.
Injuries to the Head and Spine
 Injuries to the Head and Spine Anatomy Review Skull Protects the brain Made up of several bones with seam like sutures Regions of the scalp-frontal, occipital, parietal, temporal Bones of face Orbits Mandible
Injuries to the Head and Spine Anatomy Review Skull Protects the brain Made up of several bones with seam like sutures Regions of the scalp-frontal, occipital, parietal, temporal Bones of face Orbits Mandible
4/19/2017. Prehospital Spinal Care: Then. Prehospital Spinal Care: Then. Prehospital Spinal Care: Then. Prehospital Spinal Care: Then. Why Immobilize?
 Management of Cervical Spine Injuries and Athletic Equipment Removal Gianluca Del Rossi, PhD, ATC Prehospital Spinal Care: Then While the exact origins of backboards in EMS are unclear, noted trauma surgeon
Management of Cervical Spine Injuries and Athletic Equipment Removal Gianluca Del Rossi, PhD, ATC Prehospital Spinal Care: Then While the exact origins of backboards in EMS are unclear, noted trauma surgeon
Evaluation and Stabilization of the Athlete with Possible Spine Injury
 Evaluation and Stabilization of the Athlete with Possible Spine Injury Jeffrey H. Bohmer, MD, FACEP Emergency Physician Northwestern Medicine Central DuPage Hospital June 12, 2015 Introduction Goals: 1.
Evaluation and Stabilization of the Athlete with Possible Spine Injury Jeffrey H. Bohmer, MD, FACEP Emergency Physician Northwestern Medicine Central DuPage Hospital June 12, 2015 Introduction Goals: 1.
To Backboard or Not To Backboard? Selective Spinal Immobilization
 To Backboard or Not To Backboard? Selective Spinal Immobilization Will Smith, MD, EMT-P Medical Director Grand Teton National Park and Jackson Hole Fire/EMS, Jackson, WY www.wildmedconsulting.com Objectives
To Backboard or Not To Backboard? Selective Spinal Immobilization Will Smith, MD, EMT-P Medical Director Grand Teton National Park and Jackson Hole Fire/EMS, Jackson, WY www.wildmedconsulting.com Objectives
Indications for cervical spine immobilisation: -
 Paediatric Trauma Cervical Spine Guidelines UHW Traumatic injuries of the cervical spine (C-spine) are uncommon in children. However, it is safer assume there is a cervical spine injury until examination
Paediatric Trauma Cervical Spine Guidelines UHW Traumatic injuries of the cervical spine (C-spine) are uncommon in children. However, it is safer assume there is a cervical spine injury until examination
Position Statement for the Management of Patients with Potential Spinal Injuries
 Office of the Medical Director San Antonio Fire Department and UT Health San Antonio Dept. of Emergency Health Sciences Position Statement for the Management of Patients with Potential Spinal Injuries
Office of the Medical Director San Antonio Fire Department and UT Health San Antonio Dept. of Emergency Health Sciences Position Statement for the Management of Patients with Potential Spinal Injuries
TALK TRAUMA Clearing the C-Spine. David Ouellette
 TALK TRAUMA 2011 Clearing the C-Spine David Ouellette Case #1 - Mother / Daughter MVC 34 y/o female Dangerous mechanism CHI Mumbling incoherently Femur # - distracting injury ETOH - 22 9 y/o female Dangerous
TALK TRAUMA 2011 Clearing the C-Spine David Ouellette Case #1 - Mother / Daughter MVC 34 y/o female Dangerous mechanism CHI Mumbling incoherently Femur # - distracting injury ETOH - 22 9 y/o female Dangerous
Chapter 32. Injuries to the Spine by Pearson Education, Inc. Upper Saddle River, New Jersey
 Chapter Injuries to the Spine Topics Anatomy and physiology of the spine Spinal injuries Guidelines for immobilization Special considerations Enrichment Introduction Injuries to the spine are among the
Chapter Injuries to the Spine Topics Anatomy and physiology of the spine Spinal injuries Guidelines for immobilization Special considerations Enrichment Introduction Injuries to the spine are among the
Northwest Community EMS System Continuing Education Class Credit Questions for October 2014 Spine Motion Restriction (Didactic)
") Northwest Community EMS System Continuing Education Class Credit Questions for October 2014 Spine Motion Restriction (Didactic) Name (PRINT): Date submitted: Affiliation: Rating: [ ] Complete [ ] Incomplete
Northwest Community EMS System Continuing Education Class Credit Questions for October 2014 Spine Motion Restriction (Didactic) Name (PRINT): Date submitted: Affiliation: Rating: [ ] Complete [ ] Incomplete
Follow your protocols!
 By Will Dunn, BA, NRP, CCEMTP & Myles Sibley, BA, NREMT P Eagle County Paramedic Services, Eagle County, CO. FIELD ASSESSMENT AND TREATMENT OF CLOSED HEAD AND SPINAL INJURY Follow your protocols! Objectives
By Will Dunn, BA, NRP, CCEMTP & Myles Sibley, BA, NREMT P Eagle County Paramedic Services, Eagle County, CO. FIELD ASSESSMENT AND TREATMENT OF CLOSED HEAD AND SPINAL INJURY Follow your protocols! Objectives
Introduction to Emergency Medical Care 1
 Introduction to Emergency Medical Care 1 OBJECTIVES 31.1 Define key terms introduced in this chapter. Slides 13 15, 17, 19, 28 31.2 Describe the components and function of the nervous system and the anatomy
Introduction to Emergency Medical Care 1 OBJECTIVES 31.1 Define key terms introduced in this chapter. Slides 13 15, 17, 19, 28 31.2 Describe the components and function of the nervous system and the anatomy
Episode 66 Backboard and Collar Nightmares from EMU Conference. The Risks Associated with Backboard & Collar
 However, backboards and collars are not without risk: Episode 66 Backboard and Collar Nightmares from EMU Conference With Dr. Kylie Bosman Prepared by Dr., edited by Dr. Kylie Bosman & Anton Helman, May
However, backboards and collars are not without risk: Episode 66 Backboard and Collar Nightmares from EMU Conference With Dr. Kylie Bosman Prepared by Dr., edited by Dr. Kylie Bosman & Anton Helman, May
GOALS: To be able to assure proper patient selection in spinal motion restriction
 CLINICAL STANDARD OF PRACTICE APPROVED BY: MAB MEDICAL DIRECTOR: Dr. James Cameron REVIEW DATE: April 16, 2014 REVIEWED: REVISED: February 18, 2015 TITLE: Pre-hospital spinal motion restriction (Revised
CLINICAL STANDARD OF PRACTICE APPROVED BY: MAB MEDICAL DIRECTOR: Dr. James Cameron REVIEW DATE: April 16, 2014 REVIEWED: REVISED: February 18, 2015 TITLE: Pre-hospital spinal motion restriction (Revised
MEMORANDUM Date: To: From: Subject:
 COUNTY OF EL DORADO HEALTH & HUMAN SERVICES BOARD OF SUPERVISORS Director Chris Weston Program Manager II 931 Spring Street Placerville, CA 95667 530-621-6100 Phone / 530-295-2501 Fax 1360 Johnson Boulevard,
COUNTY OF EL DORADO HEALTH & HUMAN SERVICES BOARD OF SUPERVISORS Director Chris Weston Program Manager II 931 Spring Street Placerville, CA 95667 530-621-6100 Phone / 530-295-2501 Fax 1360 Johnson Boulevard,
Restore adequate respiratory and circulatory conditions. Reduce pain
 Pre-hospital management of the trauma patient is best performed by an integrated team focused on minimizing the time from injury to definitive care at an appropriate trauma center. Dispatchers, first responders,
Pre-hospital management of the trauma patient is best performed by an integrated team focused on minimizing the time from injury to definitive care at an appropriate trauma center. Dispatchers, first responders,
Pre-hospital Response to Trauma and Brain Injury. Hans Notenboom, M.D. Asst. Medical Director Sacred Heart Medical Center
 Pre-hospital Response to Trauma and Brain Injury Hans Notenboom, M.D. Asst. Medical Director Sacred Heart Medical Center Traumatic Brain Injury is Common 235,000 Americans hospitalized for non-fatal TBI
Pre-hospital Response to Trauma and Brain Injury Hans Notenboom, M.D. Asst. Medical Director Sacred Heart Medical Center Traumatic Brain Injury is Common 235,000 Americans hospitalized for non-fatal TBI
Injuries to the Head and Spine From Bradys Emergency Care 10 th Edition
 Injuries to the Head and Spine From Bradys Emergency Care 10 th Edition 1. When performing the four-rescuer log roll, which responder pulls the board into position? A.) Head B.) Waist C.) Knee D.) Shoulder
Injuries to the Head and Spine From Bradys Emergency Care 10 th Edition 1. When performing the four-rescuer log roll, which responder pulls the board into position? A.) Head B.) Waist C.) Knee D.) Shoulder
Cervical Spine Precautions A quick review. By Joseph Lewis, M.D. Medical Director, Honolulu EMS Board Certified in Emergency Medicine
 Cervical Spine Precautions A quick review By Joseph Lewis, M.D. Medical Director, Honolulu EMS Board Certified in Emergency Medicine 1 Goals of this Cervical Spine Immobilization In-service Learn Objectives:
Cervical Spine Precautions A quick review By Joseph Lewis, M.D. Medical Director, Honolulu EMS Board Certified in Emergency Medicine 1 Goals of this Cervical Spine Immobilization In-service Learn Objectives:
Pre-hospital Spinal Motion Restriction Standard update. Presented by: Dr. Tatiana Jevremovic CCFP (EM)(SEM), Dip.
(SEM), Dip.") Pre-hospital Spinal Motion Restriction Standard update Presented by: Dr. Tatiana Jevremovic CCFP (EM)(SEM), Dip. Sport Med (CASEM) Dr. Thomas J. Pashby What is happening Pre-hospital Spinal Motion Restriction
Pre-hospital Spinal Motion Restriction Standard update Presented by: Dr. Tatiana Jevremovic CCFP (EM)(SEM), Dip. Sport Med (CASEM) Dr. Thomas J. Pashby What is happening Pre-hospital Spinal Motion Restriction
Every day thousands of people become the accidental victims of trauma.
 Aurora Health Care South Region EMS 2010 2 nd Quarter CE Packet Spinal Cord Trauma Every day thousands of people become the accidental victims of trauma. Approximately 43,000 people die in motor vehicle
Aurora Health Care South Region EMS 2010 2 nd Quarter CE Packet Spinal Cord Trauma Every day thousands of people become the accidental victims of trauma. Approximately 43,000 people die in motor vehicle
By: Kurt Bloomstrand, MD. EMS Medical Director
 By: Kurt Bloomstrand, MD EMS Medical Director Review anatomy and physiology List the mechanisms of injury that cause a high index of suspicion for the possibility of spine injury Discuss historical perspectives
By: Kurt Bloomstrand, MD EMS Medical Director Review anatomy and physiology List the mechanisms of injury that cause a high index of suspicion for the possibility of spine injury Discuss historical perspectives
Cervical Spine Injury Guidelines
 6/15/2018 Cervical Spine Injury Guidelines Benjamin Oshlag, MD, CAQSM Assistant Professor of Emergency Medicine Assistant Professor of Sports Medicine Columbia University Medical Center Nothing to Disclose
6/15/2018 Cervical Spine Injury Guidelines Benjamin Oshlag, MD, CAQSM Assistant Professor of Emergency Medicine Assistant Professor of Sports Medicine Columbia University Medical Center Nothing to Disclose
Lifting and Moving Patients
 1. Which of the following factors should be considered before lifting any patient? a. The weight of the patient b. Your physical limitations c. Communications 2. When lifting a patient, a basic principle
1. Which of the following factors should be considered before lifting any patient? a. The weight of the patient b. Your physical limitations c. Communications 2. When lifting a patient, a basic principle
To Backboard or Not To Backboard, That is the Question? Selective Spinal Immobilization
 To Backboard or Not To Backboard, That is the Question? Selective Spinal Immobilization Will Smith, MD, NREMT-P Medical Director, Jackson Hole Fire/EMS, Grand Teton National Park Emergency Medicine, St.
To Backboard or Not To Backboard, That is the Question? Selective Spinal Immobilization Will Smith, MD, NREMT-P Medical Director, Jackson Hole Fire/EMS, Grand Teton National Park Emergency Medicine, St.
Position Statement from the National Ski Patrol Medical Advisory Committee on the Selective Use of Backboards for Possible Spinal Injuries
 Position Statement from the National Ski Patrol Medical Advisory Committee on the Selective Use of Backboards for Possible Spinal Injuries Approved by the NSP Medical Committee 3/8/ 2017 Approved by the
Position Statement from the National Ski Patrol Medical Advisory Committee on the Selective Use of Backboards for Possible Spinal Injuries Approved by the NSP Medical Committee 3/8/ 2017 Approved by the
3/14/2014 USED TO BE SIMPLE.. TO IMMOBILIZE OR NOT TO IMMOBILIZE.THAT IS THE QUESTION THE PROBLEM OLD THINKING
 USED TO BE SIMPLE.. TO IMMOBILIZE OR NOT TO IMMOBILIZE.THAT IS THE QUESTION Immobilization following injury used to be a simple decision--but no one was thinking. Up to 5 million people per year receive
USED TO BE SIMPLE.. TO IMMOBILIZE OR NOT TO IMMOBILIZE.THAT IS THE QUESTION Immobilization following injury used to be a simple decision--but no one was thinking. Up to 5 million people per year receive
PRE-HOSPITAL PATIENT CARE PROTOCOLS BASIC LIFE SUPPORT/ADVANCED LIFE SUPPORT
 PRE-HOSPITAL PATIENT CARE PROTOCOLS BASIC LIFE SUPPORT/ADVANCED LIFE SUPPORT Board Approved June 2007 Revised December 2009 Revised July 2011 Revised June 2015 435 Hunter Street Fredericksburg, VA 22401
PRE-HOSPITAL PATIENT CARE PROTOCOLS BASIC LIFE SUPPORT/ADVANCED LIFE SUPPORT Board Approved June 2007 Revised December 2009 Revised July 2011 Revised June 2015 435 Hunter Street Fredericksburg, VA 22401
Chapter 24 Spinal Trauma Introduction to Spinal Injuries (1 of 2) Annually 15,000 permanent spinal cord injuries Commonly men years old
 Annually 15,000 permanent spinal cord injuries Commonly men years old") 1 2 3 4 5 6 7 Chapter 24 Spinal Trauma Introduction to Spinal Injuries (1 of 2) Annually 15,000 permanent spinal cord injuries Commonly men 16-30 years old Mechanism of Injury: Vehicle crashes: 48% : 21%
1 2 3 4 5 6 7 Chapter 24 Spinal Trauma Introduction to Spinal Injuries (1 of 2) Annually 15,000 permanent spinal cord injuries Commonly men 16-30 years old Mechanism of Injury: Vehicle crashes: 48% : 21%
SPINE EVALUATION AND CLEARANCE Basic Principles
 SPINE EVALUATION AND CLEARANCE Basic Principles General 1. Entire spine is immobilized during primary survey. 2. Radiographic clearance of the spine is not required before emergent surgical procedures.
SPINE EVALUATION AND CLEARANCE Basic Principles General 1. Entire spine is immobilized during primary survey. 2. Radiographic clearance of the spine is not required before emergent surgical procedures.
Objective 1 Review Research on spine injuries and evaluation standards.
 To Backboard or Not To Backboard? Spinal Clearance Protocols Will Smith, MD, NREMT-P Medical Director, Jackson Hole Fire/EMS, Grand Teton National Park Wilderness and Emergency Medicine Consulting (WEMC),
To Backboard or Not To Backboard? Spinal Clearance Protocols Will Smith, MD, NREMT-P Medical Director, Jackson Hole Fire/EMS, Grand Teton National Park Wilderness and Emergency Medicine Consulting (WEMC),
EMS Update Spinal Motion Restriction Training
 EMS Update Spinal Motion Restriction Training 700-M11 Spinal Motion Restriction Spinal Motion Restriction, also called SMR Formally known as Spinal Immobilization or C-Spine Effective February 9, 2016
EMS Update Spinal Motion Restriction Training 700-M11 Spinal Motion Restriction Spinal Motion Restriction, also called SMR Formally known as Spinal Immobilization or C-Spine Effective February 9, 2016
Spinal, or Suspected Spinal Injury
 Approved by: Spinal, or Suspected Spinal Injury Vice President and Chief Medical Officer; and Vice President and Chief Operating Officer Corporate Policy & Procedures Manual Number: VII-B-150 Date Approved
Approved by: Spinal, or Suspected Spinal Injury Vice President and Chief Medical Officer; and Vice President and Chief Operating Officer Corporate Policy & Procedures Manual Number: VII-B-150 Date Approved
Steve Blados M.Ed., NRP Linda Gibbens, M.S., ATC, LAT
 Steve Blados M.Ed., NRP Linda Gibbens, M.S., ATC, LAT The National Athletic Trainers Association has updated the recommendations pertaining to equipment removal of injured players when spinal immobilization
Steve Blados M.Ed., NRP Linda Gibbens, M.S., ATC, LAT The National Athletic Trainers Association has updated the recommendations pertaining to equipment removal of injured players when spinal immobilization
The Assessment & Management of Spine & Spinal Cord Injuries in the Field:
 The Assessment & Management of Spine & Spinal Cord Injuries in the Field: Where We Started, Where We are Now, & Why WMTC Wilderness Medicine Training Center International Paul Nicolazzo Director Wilderness
The Assessment & Management of Spine & Spinal Cord Injuries in the Field: Where We Started, Where We are Now, & Why WMTC Wilderness Medicine Training Center International Paul Nicolazzo Director Wilderness
Trauma Life Support Pre-Hospital (TLS-P) Preparatory Materials
 Preparatory Materials") Trauma Life Support Pre-Hospital (TLS-P) Preparatory Materials 1 1. A high-risk bodily fluid for spreading infection is blood. 2. Items that can reduce the spread of infection include masks, gloves, and
Trauma Life Support Pre-Hospital (TLS-P) Preparatory Materials 1 1. A high-risk bodily fluid for spreading infection is blood. 2. Items that can reduce the spread of infection include masks, gloves, and
11. Spinal cord injury
 11. Spinal cord injury Introduction Always think spinal (vertebral) and/or spinal cord injury (SCI) in children with trauma. Remember SCIWORA cord injury may be present without abnormalities on routine
11. Spinal cord injury Introduction Always think spinal (vertebral) and/or spinal cord injury (SCI) in children with trauma. Remember SCIWORA cord injury may be present without abnormalities on routine
IRECA BLS Challenge 2015 Scenario 1
 Scenario 1 Team Name Team Number Captain Name Judge 1 # Judge 2 # JUDGE S SHEET Overview: This scenario challenges the competitors to use basic triage techniques and then to do the most good for the most
Scenario 1 Team Name Team Number Captain Name Judge 1 # Judge 2 # JUDGE S SHEET Overview: This scenario challenges the competitors to use basic triage techniques and then to do the most good for the most
ITLS Pediatric Provider Course Advanced Pre-Test
 ITLS Pediatric Provider Course Advanced Pre-Test 1. You arrive at the scene of a motor vehicle crash and are directed to evaluate a child who was in one of the vehicles. The patient appears to be a child
ITLS Pediatric Provider Course Advanced Pre-Test 1. You arrive at the scene of a motor vehicle crash and are directed to evaluate a child who was in one of the vehicles. The patient appears to be a child
Spinal or Suspected Spinal, Injury: Logrolling Technique with C- Spine Precautions
 Approved by: Spinal or Suspected Spinal, Injury: Logrolling Technique with C- Spine Precautions Vice President and Chief Medical Officer; and Vice President and Chief Operating Officer Corporate Policy
Approved by: Spinal or Suspected Spinal, Injury: Logrolling Technique with C- Spine Precautions Vice President and Chief Medical Officer; and Vice President and Chief Operating Officer Corporate Policy
STOP THE MADDNESS! 4/19/2012. Mechanism of Injury A historical review of bad advice and dangerous dogma
 OBJECTIVES Discuss the inherent inaccuracy of using mechanism of injury as the primary indicator leading to spinal immobilization. STOP THE MADDNESS! Jim Morrissey, EMT-P Alameda County EMS PHCC FBI Tactical
OBJECTIVES Discuss the inherent inaccuracy of using mechanism of injury as the primary indicator leading to spinal immobilization. STOP THE MADDNESS! Jim Morrissey, EMT-P Alameda County EMS PHCC FBI Tactical
North West London Trauma Network Spinal Pathway and Protocols
 North West London Trauma Network Spinal Pathway and Protocols 1. Spinal Clearance in the Trauma Patient Inclusions: All trauma patients who are not alert and orientated, unable to cooperate (including
North West London Trauma Network Spinal Pathway and Protocols 1. Spinal Clearance in the Trauma Patient Inclusions: All trauma patients who are not alert and orientated, unable to cooperate (including
Chapter 26 Head and Spine Trauma The Nervous System The nervous system controls virtually all of our body activities including reflex, voluntary and
 1 2 3 4 5 Chapter 26 Head and Spine Trauma The Nervous System The nervous system controls virtually all of our body activities including reflex, voluntary and involuntary activities Voluntary activities
1 2 3 4 5 Chapter 26 Head and Spine Trauma The Nervous System The nervous system controls virtually all of our body activities including reflex, voluntary and involuntary activities Voluntary activities
Cervical Collar Policy 2010
 Cervical Collar Policy 2010 Version 1 For implementation in 2011 1 P a g e Introduction The Australian Rugby League is committed in providing the best possible care for all players who play the game of
Cervical Collar Policy 2010 Version 1 For implementation in 2011 1 P a g e Introduction The Australian Rugby League is committed in providing the best possible care for all players who play the game of
EMS SKILL NEUROLOGICAL EMERGENCY / SPINAL MOTION RESTRICTION (SMR) VEST TYPE EXTRICATION DEVICE FOR THE SEATED PATIENT
 VEST TYPE EXTRICATION DEVICE FOR THE SEATED PATIENT") EMS SKILL NEUROLOGICAL EMERGENCY / SPINAL MOTION RESTRICTION (SMR) VEST TYPE EXTRICATION DEVICE FOR THE SEATED PATIENT PERFORMANCE OBJECTIVES Demonstrate competency in performing and directing team members
EMS SKILL NEUROLOGICAL EMERGENCY / SPINAL MOTION RESTRICTION (SMR) VEST TYPE EXTRICATION DEVICE FOR THE SEATED PATIENT PERFORMANCE OBJECTIVES Demonstrate competency in performing and directing team members
ADMINISTRATIVE REQUIREMENT MANUAL EFFECTIVE DATE
 PURPOSE: I. To establish the minimum requirements for a first responder training course in first aid, which all first responders must take, in order to meet the requirements of M.G.L. c. 111, 201 and 105
PURPOSE: I. To establish the minimum requirements for a first responder training course in first aid, which all first responders must take, in order to meet the requirements of M.G.L. c. 111, 201 and 105
Fractures of the Thoracic and Lumbar Spine
 A spinal fracture is a serious injury. Nader M. Hebela, MD Fellow of the American Academy of Orthopaedic Surgeons http://orthodoc.aaos.org/hebela Cleveland Clinic Abu Dhabi Cleveland Clinic Abu Dhabi Neurological
A spinal fracture is a serious injury. Nader M. Hebela, MD Fellow of the American Academy of Orthopaedic Surgeons http://orthodoc.aaos.org/hebela Cleveland Clinic Abu Dhabi Cleveland Clinic Abu Dhabi Neurological
Hatfield & McCoy Mine Safety Competition First-Aid Contest JULY 15, Page 1
 Hatfield & McCoy Mine Safety Competition First-Aid Contest JULY 15, 2014 Page 1 PROBLEM Billy is a maintenance person that has been conducting clean-up and service duties on the number one conveyor belt
Hatfield & McCoy Mine Safety Competition First-Aid Contest JULY 15, 2014 Page 1 PROBLEM Billy is a maintenance person that has been conducting clean-up and service duties on the number one conveyor belt
Chapter 5. Learning Objectives. Learning Objectives 9/18/2012. Lifting and Moving Patients. Define body mechanics
 Chapter 5 Lifting and Moving Patients Learning Objectives Define body mechanics Discuss guidelines/safety precautions to follow when lifting patient Explain rationale for properly lifting/moving patients
Chapter 5 Lifting and Moving Patients Learning Objectives Define body mechanics Discuss guidelines/safety precautions to follow when lifting patient Explain rationale for properly lifting/moving patients
ITLS Pediatric Provider Course Basic Pre-Test
 ITLS Pediatric Provider Course Basic Pre-Test 1. You arrive at the scene of a motor vehicle collision and are directed to evaluate a child who was in one of the vehicles. The patient appears to be a child
ITLS Pediatric Provider Course Basic Pre-Test 1. You arrive at the scene of a motor vehicle collision and are directed to evaluate a child who was in one of the vehicles. The patient appears to be a child
MASSACHUSETTS DEPARTMENT OF PUBLIC HEALTH OFFICE OF EMERGENCY MEDICAL SERVICES Basic EMT Practical Examination Cardiac Arrest Management
 Basic EMT Practical Examination 6.0 - Cardiac Arrest Management Station 1 RESUSCITATION & DEFIBRILLATION No Point WHILE FUNCTIONING AS FIRST RESCUER: Point 1. Verbalizes or takes body substance isolation
Basic EMT Practical Examination 6.0 - Cardiac Arrest Management Station 1 RESUSCITATION & DEFIBRILLATION No Point WHILE FUNCTIONING AS FIRST RESCUER: Point 1. Verbalizes or takes body substance isolation
CHANHASSEN FIRE DEPARTMENT MEDICAL / RESCUE SKILLS
 CHANHASSEN FIRE DEPARTMENT MEDICAL / RESCUE SKILLS PRACTICAL STATIONS CHANHASSEN FIRE DEPARTMENT MEDICAL / RESCUE SKILLS 1. CARDIAC ARREST MANAGEMENT 2. AIRWAY & RESPIRATORY MANAGEMENT 3. SPINAL IMMOBILIZATION
CHANHASSEN FIRE DEPARTMENT MEDICAL / RESCUE SKILLS PRACTICAL STATIONS CHANHASSEN FIRE DEPARTMENT MEDICAL / RESCUE SKILLS 1. CARDIAC ARREST MANAGEMENT 2. AIRWAY & RESPIRATORY MANAGEMENT 3. SPINAL IMMOBILIZATION
Time Equals Neurons - Spinal Cord Injury Management in the first 4 Hours
 Time Equals Neurons - Spinal Cord Injury Management in the first 4 Hours William D. Whetstone M.D. Clinical Professor UCSF Department of Emergency Medicine SFGH ED Center for Neuro-Critical Emergencies
Time Equals Neurons - Spinal Cord Injury Management in the first 4 Hours William D. Whetstone M.D. Clinical Professor UCSF Department of Emergency Medicine SFGH ED Center for Neuro-Critical Emergencies
MULTIPLE CHOICE. Choose the one alternative that best completes the statement or answers the question.
 EPC Ch 24 Quiz w-key Name MULTIPLE CHOICE. Choose the one alternative that best completes the statement or answers the question. 1) Which of the following best explains the presentation and prognosis of
EPC Ch 24 Quiz w-key Name MULTIPLE CHOICE. Choose the one alternative that best completes the statement or answers the question. 1) Which of the following best explains the presentation and prognosis of
Spinal injury. Structure of the spine
 Spinal injury Structure of the spine Some understanding of the structure of the spine (spinal column) and the spinal cord is important as it helps your Neurosurgeon explain about the part of the spine
Spinal injury Structure of the spine Some understanding of the structure of the spine (spinal column) and the spinal cord is important as it helps your Neurosurgeon explain about the part of the spine
Pediatric Trauma Cases
 Pediatric Trauma Cases QPEM 2018 Barbara Blackie, MD, MEd, FRCPC DISCLOSURE I do not have any relevant financial relationship with commercial interest to disclose. Learning Objectives -Manage interactive
Pediatric Trauma Cases QPEM 2018 Barbara Blackie, MD, MEd, FRCPC DISCLOSURE I do not have any relevant financial relationship with commercial interest to disclose. Learning Objectives -Manage interactive
Selective Spinal Immobilization
 Selective Spinal Immobilization Objectives Understand the background of spinal immobilization. Understand the rationale for developing a current selective spinal immobilization protocol. Review the data
Selective Spinal Immobilization Objectives Understand the background of spinal immobilization. Understand the rationale for developing a current selective spinal immobilization protocol. Review the data
ESCAMBIA COUNTY TRAUMA TRANSPORT
 TRAUMA ALERT CRITERIA are established state mandated criteria. ADULT TRAUMA ALERT CRITERIA (Physical and anatomical characteristics of a person 16 years of age or older) Any 1 of the following: 1. Airway:
TRAUMA ALERT CRITERIA are established state mandated criteria. ADULT TRAUMA ALERT CRITERIA (Physical and anatomical characteristics of a person 16 years of age or older) Any 1 of the following: 1. Airway:
Code3 Conference October 24, 2014
 Code3 Conference October 24, 2014 Disclaimer Out of hospital providers should follow local protocol at all times. Which Patient Need Spinal Immobilization? History of Spinal Immobilization A thorough search
Code3 Conference October 24, 2014 Disclaimer Out of hospital providers should follow local protocol at all times. Which Patient Need Spinal Immobilization? History of Spinal Immobilization A thorough search
Pre-hospital Trauma Life Support. Rattiya Banjungam Emergency Physician, Khon Kaen Hospital
 Pre-hospital Trauma Life Support Rattiya Banjungam Emergency Physician, Khon Kaen Hospital Golden principles of Prehospital Trauma Care Golden Hour There is a golden hour if you are critically injured,
Pre-hospital Trauma Life Support Rattiya Banjungam Emergency Physician, Khon Kaen Hospital Golden principles of Prehospital Trauma Care Golden Hour There is a golden hour if you are critically injured,
CERVICAL SPINE CLEARANCE
 DISCLAIMER: These guidelines were prepared by the Department of Surgical Education, Orlando Regional Medical Center. They are intended to serve as a general statement regarding appropriate patient care
DISCLAIMER: These guidelines were prepared by the Department of Surgical Education, Orlando Regional Medical Center. They are intended to serve as a general statement regarding appropriate patient care
SEMINOLE COUNTY EMS PROVISIONAL EMT SKILLS VERIFICATION
 The following individual has completed the Seminole County EMS Provisional EMT Skills Verification check in the following areas: Oxygen, Airway and Ventilation Skills ALS Assistance Trauma Management Medical
The following individual has completed the Seminole County EMS Provisional EMT Skills Verification check in the following areas: Oxygen, Airway and Ventilation Skills ALS Assistance Trauma Management Medical
Chapter 8 - Lifting and Moving Patients
 1 Chapter 8 Lifting and Moving Patients 2 3 4 5 6 7 8 9 National EMS Education Standard Competencies EMS Operations Knowledge of operational roles and responsibilities to ensure patient, public, and personnel
1 Chapter 8 Lifting and Moving Patients 2 3 4 5 6 7 8 9 National EMS Education Standard Competencies EMS Operations Knowledge of operational roles and responsibilities to ensure patient, public, and personnel
Vacuum Immobilisation Mattress (VIM) Research Studies
 Research Studies") Please Note: All studies below compare the Vacuum Mattress against a flat Long Spine Board. No studies currently exist comparing the Vacuum Mattress against a curved Long Spine Board. Curved devices are
Please Note: All studies below compare the Vacuum Mattress against a flat Long Spine Board. No studies currently exist comparing the Vacuum Mattress against a curved Long Spine Board. Curved devices are
Pediatric Prehospital Protocols Grant Cervical Spine Immoblization Evidence-Based Practice Summary
 Pediatric Prehospital Protocols Grant Cervical Spine Immoblization Evidence-Based Practice Summary Evidence-Based Practice Summary prepared by Elizabeth Crabtree, MPH, Research Specialist and Quinn Franklin,
Pediatric Prehospital Protocols Grant Cervical Spine Immoblization Evidence-Based Practice Summary Evidence-Based Practice Summary prepared by Elizabeth Crabtree, MPH, Research Specialist and Quinn Franklin,
Acute spinal cord injury
 Acute spinal cord injury Thakul Oearsakul Songklanagarind hospital Hat Yai Songkhla Introduction New SCI 10000-12000 cases Approximately 4.0-5.3 per 100000 population Common causes of traumatic SCI :Motor
Acute spinal cord injury Thakul Oearsakul Songklanagarind hospital Hat Yai Songkhla Introduction New SCI 10000-12000 cases Approximately 4.0-5.3 per 100000 population Common causes of traumatic SCI :Motor
Northwest Community EMS System Feb 2018 CE: Multiple Patient Incidents/ChemPack Intro Credit Questions
 Northwest Community EMS System Feb 2018 CE: Multiple Patient Incidents/ChemPack Intro Credit Questions Name: EMS Agency/hospital: EMSC/Educator reviewer: Date submitted: Credit awarded (date): Returned
Northwest Community EMS System Feb 2018 CE: Multiple Patient Incidents/ChemPack Intro Credit Questions Name: EMS Agency/hospital: EMSC/Educator reviewer: Date submitted: Credit awarded (date): Returned
Pediatric Cardiac Arrest General
 Date: November 15, 2012 Page 1 of 5 Pediatric Cardiac Arrest General This protocol should be followed for all pediatric cardiac arrests. If an arrest is of a known traumatic origin refer to the Dead on
Date: November 15, 2012 Page 1 of 5 Pediatric Cardiac Arrest General This protocol should be followed for all pediatric cardiac arrests. If an arrest is of a known traumatic origin refer to the Dead on
STAYTON FIRE DISTRICT PROTOCOL QUIZ
 STAYTON FIRE DISTRICT PROTOCOL QUIZ Name 1. Please list the appropriate EMS Level for each of the Scope of Practice items below EMR Emergency Medical Responder B Basic Conduct primary and secondary patient
STAYTON FIRE DISTRICT PROTOCOL QUIZ Name 1. Please list the appropriate EMS Level for each of the Scope of Practice items below EMR Emergency Medical Responder B Basic Conduct primary and secondary patient
Running head: SPINAL IMMOBILIZATION AND PRESSURE ULCERS 1
 Running head: SPINAL IMMOBILIZATION AND PRESSURE ULCERS 1 Evidence Based Practice Critically Appraised Topic Spinal Immobilization & Pressure Ulcers Amy Gotvaslee, RN, FNP-S University of Mary SPINAL IMMOBILIZATION
Running head: SPINAL IMMOBILIZATION AND PRESSURE ULCERS 1 Evidence Based Practice Critically Appraised Topic Spinal Immobilization & Pressure Ulcers Amy Gotvaslee, RN, FNP-S University of Mary SPINAL IMMOBILIZATION
Pediatric Sports Emergencies. Asthma
 Pediatric Sports Emergencies Michele Kirk, MD JPS Sports Medicine Fellowship TCU Team Physician Two underlying factors: Inflammation Asthma Chronic Leads to structural changes Increase in airway smooth
Pediatric Sports Emergencies Michele Kirk, MD JPS Sports Medicine Fellowship TCU Team Physician Two underlying factors: Inflammation Asthma Chronic Leads to structural changes Increase in airway smooth
of Trauma Assembly 27 th Page 1
 Eastern Association for the Surgery of Trauma 27 th Annual Scientific Assembly Sunrise Session 08 To Scan or Not To Scan Thatt is the Question January 16, 2014 Waldorf Astoria Naples Naples, Floridaa Page
Eastern Association for the Surgery of Trauma 27 th Annual Scientific Assembly Sunrise Session 08 To Scan or Not To Scan Thatt is the Question January 16, 2014 Waldorf Astoria Naples Naples, Floridaa Page
Yaniv Berliner EMS STABILIZATION
 Yaniv Berliner EMS STABILIZATION Scene survey EMS must first evaluate the safety of the scene. Downed power lines, fire, traffic Is there a need for specialized equipment for extrication. Is there a need
Yaniv Berliner EMS STABILIZATION Scene survey EMS must first evaluate the safety of the scene. Downed power lines, fire, traffic Is there a need for specialized equipment for extrication. Is there a need
EMS 202: Emergency Medical Technician Course Schedule
 0- Aug EMS 0: Emergency Medical Technician Course Schedule (Section 111 - Tuesday/Thursday Mornings) ***UNLESS OTHERWISE STATED, ALL ASSIGNMENTS ARE DUE ON THE NEXT DAY OF CLASS*** **IT IS STRONGLY SUGGESTED
0- Aug EMS 0: Emergency Medical Technician Course Schedule (Section 111 - Tuesday/Thursday Mornings) ***UNLESS OTHERWISE STATED, ALL ASSIGNMENTS ARE DUE ON THE NEXT DAY OF CLASS*** **IT IS STRONGLY SUGGESTED
Emergency Care Progress Log
 Emergency Care Progress Log For further details on the National Occupational Competencies for EMRs, please visit www.paramedic.ca. Check off each skill once successfully demonstrated the Instructor. All
Emergency Care Progress Log For further details on the National Occupational Competencies for EMRs, please visit www.paramedic.ca. Check off each skill once successfully demonstrated the Instructor. All
SCIWORA Rozlyn McTeer BSN, RN, CEN Pediatric Trauma Coordinator Trauma Services OBJECTIVES DEFINITION 11/8/2017. Identify SCIWORA.
 SCIWORA Rozlyn McTeer BSN, RN, CEN Pediatric Trauma Coordinator Trauma Services Identify SCIWORA. OBJECTIVES Identify the population at risk. To identify anatomic and physiologic reasons for SCIWORA. To
SCIWORA Rozlyn McTeer BSN, RN, CEN Pediatric Trauma Coordinator Trauma Services Identify SCIWORA. OBJECTIVES Identify the population at risk. To identify anatomic and physiologic reasons for SCIWORA. To
BUKU PANDUAN INSTRUKTUR SKILLS LEARNING SISTEM EMERGENSI DAN TRAUMATOLOGI STABILISASI DAN TRANSPORTASI
 BUKU PANDUAN INSTRUKTUR SKILLS LEARNING SISTEM EMERGENSI DAN TRAUMATOLOGI STABILISASI DAN TRANSPORTASI KOORDINATOR SKILLS LAB SISTEM EMERGENSI DAN TRAUMATAOLOGI FAKULTAS KEDOKTERAN UNIVERSITAS HASANUDDIN
BUKU PANDUAN INSTRUKTUR SKILLS LEARNING SISTEM EMERGENSI DAN TRAUMATOLOGI STABILISASI DAN TRANSPORTASI KOORDINATOR SKILLS LAB SISTEM EMERGENSI DAN TRAUMATAOLOGI FAKULTAS KEDOKTERAN UNIVERSITAS HASANUDDIN
Kinetic Energy Energy in Motion KE = Mass (weight) X Velocity (speed)² 2 Double Weight = Energy Double Speed = Energy IS THE GREATEST DETERMINANT
 X Velocity (speed)² 2 Double Weight = Energy Double Speed = Energy IS THE GREATEST DETERMINANT") 1 Chapter 17 Blunt Trauma 2 Introduction to Blunt Trauma Most common cause of trauma death and disability exchange between an object and the human body, without intrusion through the skin 3 Blunt trauma
1 Chapter 17 Blunt Trauma 2 Introduction to Blunt Trauma Most common cause of trauma death and disability exchange between an object and the human body, without intrusion through the skin 3 Blunt trauma
3/10/17 Spinal a Injury 1
 Spinal Injury 1 'Paralysed' Watmough vows he'll have the backbone for Game Two after treatment for neck injury Watmough will have cortisone injected into his spine this morning to speed up the recovery
Spinal Injury 1 'Paralysed' Watmough vows he'll have the backbone for Game Two after treatment for neck injury Watmough will have cortisone injected into his spine this morning to speed up the recovery
Chapter 7 EMERGENCY PLAN AND INITIAL INJURY EVALUATION
 Chapter 7 EMERGENCY PLAN AND INITIAL INJURY EVALUATION Major Concepts. Proper planning of an emergency response is essential for appropriate first aid management of an injury. Anything that can be done
Chapter 7 EMERGENCY PLAN AND INITIAL INJURY EVALUATION Major Concepts. Proper planning of an emergency response is essential for appropriate first aid management of an injury. Anything that can be done
Chapter 12. Learning Objectives. Learning Objectives 9/11/2012. Musculoskeletal Injuries
 Chapter 12 Musculoskeletal Injuries Learning Objectives Describe the anatomy and function of the musculoskeletal system Demonstrate the assessment and management of a patient with a suspected musculoskeletal
Chapter 12 Musculoskeletal Injuries Learning Objectives Describe the anatomy and function of the musculoskeletal system Demonstrate the assessment and management of a patient with a suspected musculoskeletal
EMS 202: Emergency Medical Technician Course Schedule
 19- Aug EMS 0: Emergency Medical Technician Course Schedule Section 109 Monday/Wednesday Mornings ***UNLESS OTHERWISE STATED, ALL ASSIGNMENTS ARE DUE ON THE NEXT DAY OF CLASS*** **IT IS STRONGLY SUGGESTED
19- Aug EMS 0: Emergency Medical Technician Course Schedule Section 109 Monday/Wednesday Mornings ***UNLESS OTHERWISE STATED, ALL ASSIGNMENTS ARE DUE ON THE NEXT DAY OF CLASS*** **IT IS STRONGLY SUGGESTED
TITLE: Vacuum Boards for Spinal Motion Restriction: Clinical Effectiveness
 TITLE: Vacuum Boards for Spinal Motion Restriction: Clinical Effectiveness DATE: 14 October 2008 RESEARCH QUESTION: What are the clinical benefits and harms of using vacuum boards for spinal motion restriction?
TITLE: Vacuum Boards for Spinal Motion Restriction: Clinical Effectiveness DATE: 14 October 2008 RESEARCH QUESTION: What are the clinical benefits and harms of using vacuum boards for spinal motion restriction?
TRAUMA PATIENT ASSESSMENT
 SECTION: Adult Trauma Emergencies PROTOCOL TITLE: Injury General Trauma Management REVISED: 06/2015 OVERVIEW Each year, one out of three Americans sustains a traumatic injury. Trauma is a major cause of
SECTION: Adult Trauma Emergencies PROTOCOL TITLE: Injury General Trauma Management REVISED: 06/2015 OVERVIEW Each year, one out of three Americans sustains a traumatic injury. Trauma is a major cause of
Daniel A. Beals MD, FACS, FAAP Pediatric Surgery and Urology Community Medical Center Associate Professor of Surgery and Pediatrics University of
 Daniel A. Beals MD, FACS, FAAP Pediatric Surgery and Urology Community Medical Center Associate Professor of Surgery and Pediatrics University of Washington Seattle Children s Hospital Objectives Define
Daniel A. Beals MD, FACS, FAAP Pediatric Surgery and Urology Community Medical Center Associate Professor of Surgery and Pediatrics University of Washington Seattle Children s Hospital Objectives Define