11. Spinal cord injury
|
|
|
- Gerald Carter
- 5 years ago
- Views:
Transcription
1 11. Spinal cord injury Introduction Always think spinal (vertebral) and/or spinal cord injury (SCI) in children with trauma. Remember SCIWORA cord injury may be present without abnormalities on routine X-rays. All children with possible spinal cord injury in Yorkshire & Humber should be referred to the Major Trauma Centre (MTC). The MTC will organise registration on a national database nww.scireferrals.nhs.uk and appropriate multi-disciplinary input as required from intensive care, neurosurgery, orthopaedics, urology, respiratory and rehabilitation. Think Spinal Cord Injury if A child complains of back or neck pain and appears to be guarding their back or neck The child complains of sensory changes or loss such as numbness or tingling The child is unable to pass urine The child has difficulty moving any part of their arms or legs There is pre-existing pathology In general, spinal injuries should be suspected in all children who have been involved in: A road traffic accident A fall or jump from a height An accident resulting in impact or crush injuries An accident resulting in multiple trauma An accident resulting in the patient losing consciousness Following an injury, the potential for a spinal cord injury to exist must be considered. Children may present with full movement and sensation of all four limbs; however, they may have a vertebral fracture and, if handled incorrectly, the spinal cord may be damaged and the results could be devastating. Immediate management of traumatic SCI (actual or suspected) Approach to initial assessment Initial assessment is the standard c-abc approach as per APLS / ATLS guidelines : Control massive haemorrhage Airway with cervical spine control Breathing with ventilation support Circulation with haemorrhage control Disability AVPU, posture and pupils Exposure with temperature control c-abc is the priority, with protection of any potential unstable fracture. The secondary survey is of greater importance in a patient with impaired sensation.
2 Spinal Shock At the acute stage there may be total, flaccid paralysis of all skeletal muscle and loss of all spinal reflexes below the level of the lesion. This is referred to as spinal shock. It may last from several hours to several weeks depending on the severity. Airway and Cervical Spine Control In any injury the airway can become compromised. The spine should be kept in alignment at all times. Place the patient in the neutral supine position Look for evidence of airway obstruction or compromise Use a jaw thrust NOT head tilt / chin lift Minimise any movement of the cervical spine Consider use of an airway adjunct (NOT nasopharyngeal in head injured patients) Seek early help from the most experienced anaesthetist available Refer to the section on emergency anaesthesia. Breathing The risk of deteriorating respiratory function is extremely high. In cervical and high thoracic injuries the nerves to the intercostal muscles are paralysed, reducing the ability to breathe effectively. In high cervical lesions the diaphragm may also be affected (C3/4/5). In these high lesions the most affected function is coughing. Patients with very high lesions are breathing with the diaphragm only and have no effective cough at all. Look at the rate and depth of respirations Look for shallow or abdominal breathing, asymmetry, or paradoxical breathing Slowing down respirations, grunting and desaturation in oxygen are worrying signs There may be evidence of aspiration or consolidation Have a low threshold for intubation and ventilation prior to transport to the MTC Circulation Neurogenic (spinal) shock is the body's response to the sudden loss of sympathetic control. It occurs in cervical and high thoracic lesions (above T6). Incomplete injuries may not display these signs. Due to lack of vasomotor control significant hypotension results. Bradycardia occurs as a result of unopposed effects of the vagus nerve. A lower mean blood pressure may be compatible with good urinary output and cannot be used as sole indicator of perfusion. However, hypovolaemic shock may also be present and other injuries may escape detection in the cord injured patient with sensory deprivation. Keep patient supine and monitor for hypotension and bradycardia Abnormal vaso-vagal response can occur through stimulation such as rapid changes in body positioning, i.e. log rolling quickly, tracheal suctioning, or passing a gastric tube. Maintain a normotensive mean pressure and an adequate urinary output for age and size (2 ml/kg/h for infants <1 year old, 1 ml/kg/h for children 1-12 years old, and 0.5ml/kg/h over 12 years old) Page 2
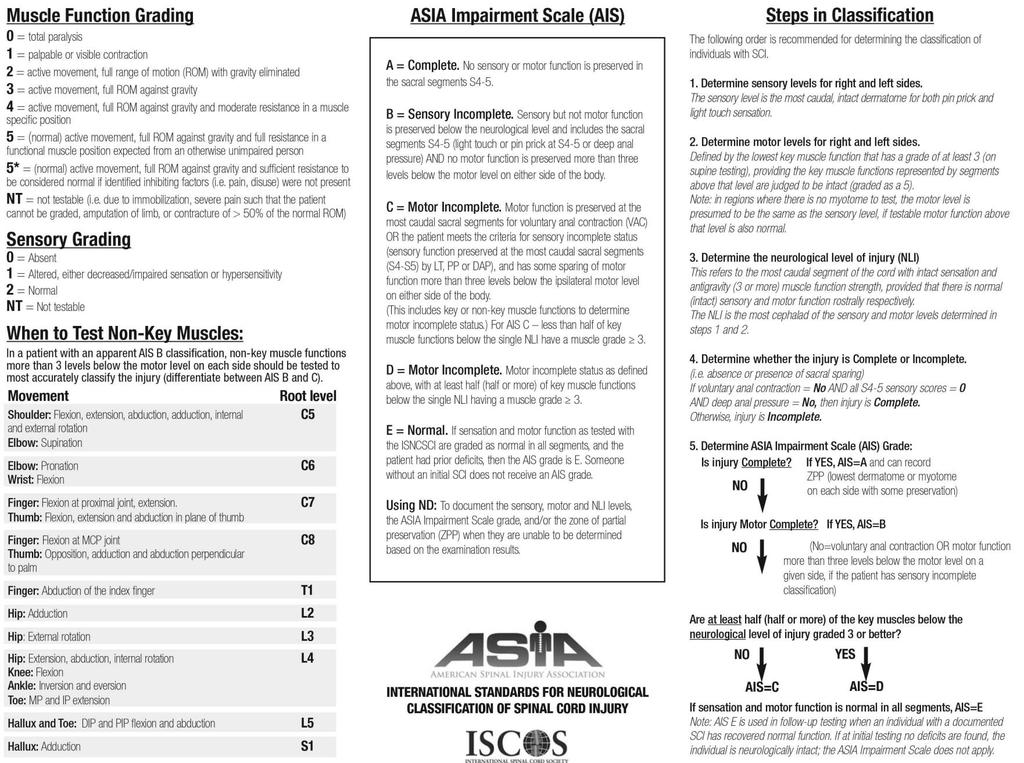
3 Administer IV bolus fluids as needed plus maintenance. However be careful not to give too much fluid - this may precipitate cardiac failure and pulmonary oedema. Inotropes may be necessary to maintain the blood pressure CVP monitoring can be helpful Problematic bradycardia usually resolves over a few days. Pacemakers can cause management complications in the long term and should be avoided where possible There is a high incidence of cardiac contusion in patients with thoracic injuries with a potential for arrhythmias Neurological Assessment (all cases) Careful neurological assessment is absolutely essential for patient with spinal cord pathology. This is very difficult to perform in young children, and in any child when frightened and distressed. In the first hours and days following injury the neurological level may change. An extension of the lesion by one or even two levels may be observed and it is critical that any change is monitored, to prevent any avoidable deterioration of neurological deficit. Although the gold standard expects neurological observations should be performed at two hourly intervals this is not feasible in young children. Concentrating on a few key points may give better results in combination with attempting to establish level with MRI scan. At the site of cord injury there will be a zone of critical ischaemia. This zone may expand with poor oxygen saturation or poor perfusion. Patients with high lesions have poor autonomic vascular control and postural hypotension may be severe and significant. In the acute phase of the injury, postural hypotension may expand the zone of critical ischaemia. Neurological examination should be undertaken by an experienced member of the medical team using the standardised examination recording chart published by the American Spinal Injuries Association (ASIA Chart, Appendix 6). Mark the sensory level on the patient as this is very useful in subsequent review. A change from an accurately recorded level may allow diagnosis of potential complications, e.g., epidural haematoma, over distraction when using skull traction. In the period of spinal shock formal classification of the injury is not possible. Sacral segments have great prognostic significance for recovery as well as bowel and bladder management. Careful examination of perianal sensation, deep anal pressure, tone, and voluntary anal contraction is important but not usually possible in younger children and has to be considered for each child as the information may be extremely unreliable. If not performed the reason for this should be documented for each individual. Spinal surgery may be contemplated. If spinal surgery is undertaken the ASIA Chart must be carefully completed both prior to surgery and post-operatively. Remember this is, however, less reliable in the presence of spinal shock. Steroid Therapy Post Injury There have been no clinical trials in children and no evidence that high dose steroids have any place in the management of acute traumatic spinal injured children. Page 3
4 Transfer to the Regional Spinal Centre Decisions regarding transfer should be made by senior staff in both the transferring and receiving paediatric units. The Major Trauma Networks have agreed an immediate transfer policy regarding patient referrals to the Major Trauma Centre see Section 3. The referring team may require clinical advice regarding stabilization and transfer. This may be facilitated by Embrace via the conference call system. When transport is provided by the referring hospital team the principles of safe transfer should be followed please refer to Section 19. Special considerations in SCI: The transferring team should have the skills and equipment to manage deterioration on route A properly immobilised spinal injured patient can be transferred at normal road speeds - sudden acceleration and deceleration should be avoided Pay attention to pressure areas and skin care Handling the Child and Young Person with a traumatic SCI Patients are usually transferred into Emergency Departments on a scoop stretcher. Transfer onto an appropriate support surface MUST be undertaken at the earliest possible opportunity. In the Emergency Department this will be onto a sheet over a vacuum mattress on a standard padded tipping trolley. Ensure sufficient personnel are available for continued maintenance of spinal alignment. Ensure all head huggers and straps are removed before transfer. No log roll is required to be removed from a scoop stretcher as the two sides can be split and removed laterally. When moving a child, avoid shearing their skin against the underlying surface. If a patient presents on a long spinal board extrication device, to ensure that total protection and alignment of the spine is maintained, to allow the patient to be moved, the recommended technique which can be applied is the logroll. It is vital that staff are trained in the technique of log rolling and that the person at the head end takes the lead. The log roll may be used in combination with Patslide and sliding sheets. APLS and NICE guidance has moved away from the application of hard cervical collars towards use of manual in-line stabilisation as first choice, followed by use of sand bags and tape only, often in conjunction with a vacuum mattress. If a patient presents to the ED with a hard cervical collar in situ, it will be removed during the primary survey. Patients with acute spinal cord injury must be nursed flat initially. Elevation of the whole body up to 15 degrees may assist ventilation. Pressure reducing dynamic air mattresses are contraindicated in unstable injuries and turning regime should be initiated to prevent pressure ulceration. Skull traction in children must be reviewed on an individual case basis as in young children the majority of injuries are unstable in traction. Children cannot be transferred in traction. Page 4
5 Imaging Most paediatric major trauma patients do not require spinal imaging of any form. In cases where risk of or clinical suspicion for vertebral fracture exists, regional Trauma Network guidance should be followed on which patients require spinal imaging see Section 17. Spinal Surgery Spinal surgery comprises two components; decompression of the neural tissues and reduction and stabilisation of the spine. Conservative management is also appropriate in some injuries. The role of decompression in the management of patients with spinal cord injury has yet to be fully determined. The only definite indication for decompression and stabilisation is progressive neurological deterioration. Benefits and risks of surgery should be evaluated and discussed at the specialist centre by an experienced spinal surgeon. Page 5
6 Appendix 6 Page 6
7 Page 7
SPINE EVALUATION AND CLEARANCE Basic Principles
 SPINE EVALUATION AND CLEARANCE Basic Principles General 1. Entire spine is immobilized during primary survey. 2. Radiographic clearance of the spine is not required before emergent surgical procedures.
SPINE EVALUATION AND CLEARANCE Basic Principles General 1. Entire spine is immobilized during primary survey. 2. Radiographic clearance of the spine is not required before emergent surgical procedures.
North West London Trauma Network Spinal Pathway and Protocols
 North West London Trauma Network Spinal Pathway and Protocols 1. Spinal Clearance in the Trauma Patient Inclusions: All trauma patients who are not alert and orientated, unable to cooperate (including
North West London Trauma Network Spinal Pathway and Protocols 1. Spinal Clearance in the Trauma Patient Inclusions: All trauma patients who are not alert and orientated, unable to cooperate (including
SPINAL CORD INJURIES DR. F. DE V. THERON MUELMED/PAH HOSPITAL SPINAL UNIT 2012
 SPINAL CORD INJURIES DR. F. DE V. THERON MUELMED/PAH HOSPITAL SPINAL UNIT 2012 INTRODUCTION Mortal condition recognised since antiquity First described in the Edwin Smith papyrus 2500BC An ailment not
SPINAL CORD INJURIES DR. F. DE V. THERON MUELMED/PAH HOSPITAL SPINAL UNIT 2012 INTRODUCTION Mortal condition recognised since antiquity First described in the Edwin Smith papyrus 2500BC An ailment not
10. Severe traumatic brain injury also see flow chart Appendix 5
 10. Severe traumatic brain injury also see flow chart Appendix 5 Introduction Severe traumatic brain injury (TBI) is the leading cause of death in children in the UK, accounting for 15% of deaths in 1-15
10. Severe traumatic brain injury also see flow chart Appendix 5 Introduction Severe traumatic brain injury (TBI) is the leading cause of death in children in the UK, accounting for 15% of deaths in 1-15
European Resuscitation Council
 European Resuscitation Council Incidence of Trauma in Childhood Leading cause of death and disability in children older than one year all over the world Structured approach Primary survey and resuscitation
European Resuscitation Council Incidence of Trauma in Childhood Leading cause of death and disability in children older than one year all over the world Structured approach Primary survey and resuscitation
Chapter 32. Injuries to the Spine by Pearson Education, Inc. Upper Saddle River, New Jersey
 Chapter Injuries to the Spine Topics Anatomy and physiology of the spine Spinal injuries Guidelines for immobilization Special considerations Enrichment Introduction Injuries to the spine are among the
Chapter Injuries to the Spine Topics Anatomy and physiology of the spine Spinal injuries Guidelines for immobilization Special considerations Enrichment Introduction Injuries to the spine are among the
Chapter 32. Objectives. Objectives 01/09/2013. Spinal Column and Spinal Cord Trauma
 Chapter 32 Spinal Column and Spinal Cord Trauma Prehospital Emergency Care, Ninth Edition Joseph J. Mistovich Keith J. Karren Copyright 2010 by Pearson Education, Inc. All rights reserved. Objectives 1.
Chapter 32 Spinal Column and Spinal Cord Trauma Prehospital Emergency Care, Ninth Edition Joseph J. Mistovich Keith J. Karren Copyright 2010 by Pearson Education, Inc. All rights reserved. Objectives 1.
Introduction to Emergency Medical Care 1
 Introduction to Emergency Medical Care 1 OBJECTIVES 31.1 Define key terms introduced in this chapter. Slides 13 15, 17, 19, 28 31.2 Describe the components and function of the nervous system and the anatomy
Introduction to Emergency Medical Care 1 OBJECTIVES 31.1 Define key terms introduced in this chapter. Slides 13 15, 17, 19, 28 31.2 Describe the components and function of the nervous system and the anatomy
MEDICAL CONTROL POLICY STATEMENT/ADVISORY. Re: Spinal Injury Assessment & Spinal Precautions Procedure
 MEDICAL CONTROL POLICY STATEMENT/ADVISORY No. 2015-01 Date: January 20, 2015 Re: Spinal Injury Assessment & Spinal Precautions Procedure Office of the Medical Director Noel Wagner, MD, NREMT-P 1000 Houghton
MEDICAL CONTROL POLICY STATEMENT/ADVISORY No. 2015-01 Date: January 20, 2015 Re: Spinal Injury Assessment & Spinal Precautions Procedure Office of the Medical Director Noel Wagner, MD, NREMT-P 1000 Houghton
Injuries to the Head and Spine
 Injuries to the Head and Spine Anatomy Review Skull Protects the brain Made up of several bones with seam like sutures Regions of the scalp-frontal, occipital, parietal, temporal Bones of face Orbits Mandible
Injuries to the Head and Spine Anatomy Review Skull Protects the brain Made up of several bones with seam like sutures Regions of the scalp-frontal, occipital, parietal, temporal Bones of face Orbits Mandible
Heidi Lako-Adamson, MD, NRP, FAEMS FM Ambulance and Sanford EMS Education Medical Director
 Heidi Lako-Adamson, MD, NRP, FAEMS FM Ambulance and Sanford EMS Education Medical Director Spinal cord injury statistics. Definition of spinal motion restriction. Difference between spinal motion restriction
Heidi Lako-Adamson, MD, NRP, FAEMS FM Ambulance and Sanford EMS Education Medical Director Spinal cord injury statistics. Definition of spinal motion restriction. Difference between spinal motion restriction
Acute spinal cord injury
 Acute spinal cord injury Thakul Oearsakul Songklanagarind hospital Hat Yai Songkhla Introduction New SCI 10000-12000 cases Approximately 4.0-5.3 per 100000 population Common causes of traumatic SCI :Motor
Acute spinal cord injury Thakul Oearsakul Songklanagarind hospital Hat Yai Songkhla Introduction New SCI 10000-12000 cases Approximately 4.0-5.3 per 100000 population Common causes of traumatic SCI :Motor
Selective Spine Assessment & Spinal Motion Restriction
 Selective Spine Assessment & Spinal Motion Restriction Supersedes: 02-09-15 Effective: 10-20-15 Spinal cord injury may be the result of direct blunt and/or penetrating trauma, compression forces (axial
Selective Spine Assessment & Spinal Motion Restriction Supersedes: 02-09-15 Effective: 10-20-15 Spinal cord injury may be the result of direct blunt and/or penetrating trauma, compression forces (axial
Overview. Overview. Chapter 30. Injuries to the Head and Spine 9/11/2012. Review of the Nervous and Skeletal Systems. Devices for Immobilization
 Chapter 30 Injuries to the Head and Spine Slide 1 Overview Review of the Nervous and Skeletal Systems The Nervous System The Skeletal System Devices for Immobilization Cervical Spine Short Backboards Long
Chapter 30 Injuries to the Head and Spine Slide 1 Overview Review of the Nervous and Skeletal Systems The Nervous System The Skeletal System Devices for Immobilization Cervical Spine Short Backboards Long
Indications for cervical spine immobilisation: -
 Paediatric Trauma Cervical Spine Guidelines UHW Traumatic injuries of the cervical spine (C-spine) are uncommon in children. However, it is safer assume there is a cervical spine injury until examination
Paediatric Trauma Cervical Spine Guidelines UHW Traumatic injuries of the cervical spine (C-spine) are uncommon in children. However, it is safer assume there is a cervical spine injury until examination
Emergency First Response (EFR) Assessment Sheets September 2011
 Assessment Sheets September 2011") Emergency First Response () Assessment Sheets September 2011 Airway Management & Ventilation Current Version: Version 2 (Sep 2011) Airway Management & Ventilation TRAUMA JAW THRUST 1 Hand position 2 Perform
Emergency First Response () Assessment Sheets September 2011 Airway Management & Ventilation Current Version: Version 2 (Sep 2011) Airway Management & Ventilation TRAUMA JAW THRUST 1 Hand position 2 Perform
Post-Anesthesia Care In the ICU
 Post-Anesthesia Care In the ICU The following is based on current research and regional standards of care. At completion you will be able to identify Basic equipment needed at the bedside. Aldrete scoring
Post-Anesthesia Care In the ICU The following is based on current research and regional standards of care. At completion you will be able to identify Basic equipment needed at the bedside. Aldrete scoring
Emergency First Response (EFR) Skills Assessment Sheets V4 June 2017
 Skills Assessment Sheets V4 June 2017") Emergency First Response () Skills Assessment Sheets V4 June 2017 Airway management & ventilation Airway management & ventilation Trauma jaw thrust 1 Hand positions 2 Perform jaw thrust / mouth open 3
Emergency First Response () Skills Assessment Sheets V4 June 2017 Airway management & ventilation Airway management & ventilation Trauma jaw thrust 1 Hand positions 2 Perform jaw thrust / mouth open 3
Daniel A. Beals MD, FACS, FAAP Pediatric Surgery and Urology Community Medical Center Associate Professor of Surgery and Pediatrics University of
 Daniel A. Beals MD, FACS, FAAP Pediatric Surgery and Urology Community Medical Center Associate Professor of Surgery and Pediatrics University of Washington Seattle Children s Hospital Objectives Define
Daniel A. Beals MD, FACS, FAAP Pediatric Surgery and Urology Community Medical Center Associate Professor of Surgery and Pediatrics University of Washington Seattle Children s Hospital Objectives Define
1. Spinal cord injury mild flexion-extension whiplash ~ complete transection with permanent quadriplegia
 Wk 5. Management of Clients with Neurologic Trauma 1. Spinal cord injury mild flexion-extension whiplash ~ complete transection with permanent quadriplegia most common in cervical, lower thoracic-upper
Wk 5. Management of Clients with Neurologic Trauma 1. Spinal cord injury mild flexion-extension whiplash ~ complete transection with permanent quadriplegia most common in cervical, lower thoracic-upper
Spinal Cord Injuries: The Basics. Kadre Sneddon POS Rounds October 1, 2003
 Spinal Cord Injuries: The Basics Kadre Sneddon POS Rounds October 1, 2003 Anatomy Dorsal columntouch, vibration Corticospinal tract- UMN Anterior horn-lmn Spinothalamic tractpain, temperature (contralateral)
Spinal Cord Injuries: The Basics Kadre Sneddon POS Rounds October 1, 2003 Anatomy Dorsal columntouch, vibration Corticospinal tract- UMN Anterior horn-lmn Spinothalamic tractpain, temperature (contralateral)
10O SPLINTING OF INJURIES ADULT & PEDIATRIC. 10Oa: Axial/Spine with Selective Spinal Motion Restriction Adult & Pediatric:
 10O SPLINTING OF INJURIES ADULT & PEDIATRIC EMERGENCY MEDICAL RESPONDER EMT EMT-INTERMEDIATE 85 ADVANCED EMT PARAMEDIC 10Oa: Axial/Spine with Selective Spinal Motion Restriction Adult & Pediatric: Many
10O SPLINTING OF INJURIES ADULT & PEDIATRIC EMERGENCY MEDICAL RESPONDER EMT EMT-INTERMEDIATE 85 ADVANCED EMT PARAMEDIC 10Oa: Axial/Spine with Selective Spinal Motion Restriction Adult & Pediatric: Many
SPINAL IMMOBILIZATION
 Spinal Immobilization Decision Assessment Recent studies have shown an increase in mortality for patients with isolated penetrating trauma who are spinally immobilized. Therefore spinal immobilization
Spinal Immobilization Decision Assessment Recent studies have shown an increase in mortality for patients with isolated penetrating trauma who are spinally immobilized. Therefore spinal immobilization
Shenandoah Co. Fire & Rescue. Injuries to. and Spine. December EMS Training Bill Streett Training Section Chief
 Shenandoah Co. Fire & Rescue Injuries to the Head and Spine December EMS Training Bill Streett Training Section Chief C.E. Card Information BLS Providers 2 Cards / Provider Category 1 Course # Blank Topic#
Shenandoah Co. Fire & Rescue Injuries to the Head and Spine December EMS Training Bill Streett Training Section Chief C.E. Card Information BLS Providers 2 Cards / Provider Category 1 Course # Blank Topic#
Spinal injury. Structure of the spine
 Spinal injury Structure of the spine Some understanding of the structure of the spine (spinal column) and the spinal cord is important as it helps your Neurosurgeon explain about the part of the spine
Spinal injury Structure of the spine Some understanding of the structure of the spine (spinal column) and the spinal cord is important as it helps your Neurosurgeon explain about the part of the spine
CHANHASSEN FIRE DEPARTMENT MEDICAL / RESCUE SKILLS
 CHANHASSEN FIRE DEPARTMENT MEDICAL / RESCUE SKILLS PRACTICAL STATIONS CHANHASSEN FIRE DEPARTMENT MEDICAL / RESCUE SKILLS 1. CARDIAC ARREST MANAGEMENT 2. AIRWAY & RESPIRATORY MANAGEMENT 3. SPINAL IMMOBILIZATION
CHANHASSEN FIRE DEPARTMENT MEDICAL / RESCUE SKILLS PRACTICAL STATIONS CHANHASSEN FIRE DEPARTMENT MEDICAL / RESCUE SKILLS 1. CARDIAC ARREST MANAGEMENT 2. AIRWAY & RESPIRATORY MANAGEMENT 3. SPINAL IMMOBILIZATION
Trauma Life Support Pre-Hospital (TLS-P) Preparatory Materials
 Preparatory Materials") Trauma Life Support Pre-Hospital (TLS-P) Preparatory Materials 1 1. A high-risk bodily fluid for spreading infection is blood. 2. Items that can reduce the spread of infection include masks, gloves, and
Trauma Life Support Pre-Hospital (TLS-P) Preparatory Materials 1 1. A high-risk bodily fluid for spreading infection is blood. 2. Items that can reduce the spread of infection include masks, gloves, and
BUKU PANDUAN INSTRUKTUR SKILLS LEARNING SISTEM EMERGENSI DAN TRAUMATOLOGI STABILISASI DAN TRANSPORTASI
 BUKU PANDUAN INSTRUKTUR SKILLS LEARNING SISTEM EMERGENSI DAN TRAUMATOLOGI STABILISASI DAN TRANSPORTASI KOORDINATOR SKILLS LAB SISTEM EMERGENSI DAN TRAUMATAOLOGI FAKULTAS KEDOKTERAN UNIVERSITAS HASANUDDIN
BUKU PANDUAN INSTRUKTUR SKILLS LEARNING SISTEM EMERGENSI DAN TRAUMATOLOGI STABILISASI DAN TRANSPORTASI KOORDINATOR SKILLS LAB SISTEM EMERGENSI DAN TRAUMATAOLOGI FAKULTAS KEDOKTERAN UNIVERSITAS HASANUDDIN
Acute Neurosurgical Emergency Transfer [see also CATS SOP neurosurgical]
![Acute Neurosurgical Emergency Transfer [see also CATS SOP neurosurgical]](/thumbs/87/96512765.jpg "Acute Neurosurgical Emergency Transfer [see also CATS SOP neurosurgical]") Children s Acute Transport Service Clinical Guidelines Acute Neurosurgical Emergency Transfer [see also CATS SOP neurosurgical] Document Control Information Author D Lutman Author Position Head of Clinical
Children s Acute Transport Service Clinical Guidelines Acute Neurosurgical Emergency Transfer [see also CATS SOP neurosurgical] Document Control Information Author D Lutman Author Position Head of Clinical
Emergency Room Resuscitation of the Unstable Trauma Patient
 Emergency Room Resuscitation of the Unstable Trauma Patient Goals of trauma resuscitation Maintain: Systemic oxygenation Systemic perfusion Neurologic function Approach to unstable trauma patient Primary
Emergency Room Resuscitation of the Unstable Trauma Patient Goals of trauma resuscitation Maintain: Systemic oxygenation Systemic perfusion Neurologic function Approach to unstable trauma patient Primary
West Yorkshire Major Trauma Operational Delivery Network (WYMTN) Management of Spinal Injuries
 Management of Spinal Injuries") West Yorkshire Major Trauma Operational Delivery Network (WYMTN) Management of Spinal Injuries Contents Introduction... 2 Background... 2 WYMTN Pathways for the initial management of patients with spinal
West Yorkshire Major Trauma Operational Delivery Network (WYMTN) Management of Spinal Injuries Contents Introduction... 2 Background... 2 WYMTN Pathways for the initial management of patients with spinal
THE MANAGEMENT OF CHILDREN WITH SPINAL CORD INJURIES. Advice for Major Trauma Networks and SCI Centres On the Development of Joint Protocols
 THE MANAGEMENT OF CHILDREN WITH SPINAL CORD INJURIES Advice for Major Trauma Networks and SCI Centres On the Development of Joint Protocols With Advice for Clinicians in Acute Hospitals Approved by the
THE MANAGEMENT OF CHILDREN WITH SPINAL CORD INJURIES Advice for Major Trauma Networks and SCI Centres On the Development of Joint Protocols With Advice for Clinicians in Acute Hospitals Approved by the
What to expect following spinal cord injury. Information for patients Therapy Services
 What to expect following spinal cord injury Information for patients Therapy Services Introduction This leaflet aims to explain what spinal cord injury is and what to expect over the next few months. What
What to expect following spinal cord injury Information for patients Therapy Services Introduction This leaflet aims to explain what spinal cord injury is and what to expect over the next few months. What
EMS Spinal Assessment and Precautions
 EMS Spinal Assessment and Precautions Adapted from a presentation prepared by Chelsea C. White IV, MD, NREMT-P Medical Director, Bernalillo County Fire Department Robert M. Domeier, MD, EMS Medical Director,
EMS Spinal Assessment and Precautions Adapted from a presentation prepared by Chelsea C. White IV, MD, NREMT-P Medical Director, Bernalillo County Fire Department Robert M. Domeier, MD, EMS Medical Director,
Blunt Chest Trauma (Rib Fracture) Management Guideline
 Management Guideline") Blunt Chest Trauma (Rib Fracture) Management Guideline Midlands Critical Care, Trauma and Burns Networks Network: Midlands Trauma Networks Publication: Document purpose: Trauma Guidelines Document name:
Blunt Chest Trauma (Rib Fracture) Management Guideline Midlands Critical Care, Trauma and Burns Networks Network: Midlands Trauma Networks Publication: Document purpose: Trauma Guidelines Document name:
Emergency Care Progress Log
 Emergency Care Progress Log For further details on the National Occupational Competencies for EMRs, please visit www.paramedic.ca. Check off each skill once successfully demonstrated the Instructor. All
Emergency Care Progress Log For further details on the National Occupational Competencies for EMRs, please visit www.paramedic.ca. Check off each skill once successfully demonstrated the Instructor. All
Management of Severe Traumatic Brain Injury
 Guideline for North Bristol Trust Management of Severe Traumatic Brain Injury This guideline describes the following: Initial assessment and management of the patient with head injury Indications for CT
Guideline for North Bristol Trust Management of Severe Traumatic Brain Injury This guideline describes the following: Initial assessment and management of the patient with head injury Indications for CT
ITLS Pediatric Provider Course Advanced Pre-Test
 ITLS Pediatric Provider Course Advanced Pre-Test 1. You arrive at the scene of a motor vehicle crash and are directed to evaluate a child who was in one of the vehicles. The patient appears to be a child
ITLS Pediatric Provider Course Advanced Pre-Test 1. You arrive at the scene of a motor vehicle crash and are directed to evaluate a child who was in one of the vehicles. The patient appears to be a child
Major Trauma Scenarios. Ballarat Health Services Emergency Medicine Training Hub
 Major Trauma Scenarios Ballarat Health Services Emergency Medicine Training Hub Trauma Scenario 1 You receive a phone call from the ambulance service. They have a 27 yr old male involved in a MCA, he is
Major Trauma Scenarios Ballarat Health Services Emergency Medicine Training Hub Trauma Scenario 1 You receive a phone call from the ambulance service. They have a 27 yr old male involved in a MCA, he is
XXX Spinal Motion Restriction
 Nor-Cal EMS Policy & Procedure Manual NAME OF MODULE XXX Purpose: The purpose of this protocol is to protect patients with signs and symptoms of spinal injuries and those who have the potential for spinal
Nor-Cal EMS Policy & Procedure Manual NAME OF MODULE XXX Purpose: The purpose of this protocol is to protect patients with signs and symptoms of spinal injuries and those who have the potential for spinal
Chapter 24 Spinal Trauma Introduction to Spinal Injuries (1 of 2) Annually 15,000 permanent spinal cord injuries Commonly men years old
 Annually 15,000 permanent spinal cord injuries Commonly men years old") 1 2 3 4 5 6 7 Chapter 24 Spinal Trauma Introduction to Spinal Injuries (1 of 2) Annually 15,000 permanent spinal cord injuries Commonly men 16-30 years old Mechanism of Injury: Vehicle crashes: 48% : 21%
1 2 3 4 5 6 7 Chapter 24 Spinal Trauma Introduction to Spinal Injuries (1 of 2) Annually 15,000 permanent spinal cord injuries Commonly men 16-30 years old Mechanism of Injury: Vehicle crashes: 48% : 21%
Airway and Ventilation. Emergency Medical Response
 Airway and Ventilation Lesson 14: Airway and Ventilation You Are the Emergency Medical Responder Your medical emergency response team has been called to the fitness center by building security on a report
Airway and Ventilation Lesson 14: Airway and Ventilation You Are the Emergency Medical Responder Your medical emergency response team has been called to the fitness center by building security on a report
ITLS Pediatric Provider Course Basic Pre-Test
 ITLS Pediatric Provider Course Basic Pre-Test 1. You arrive at the scene of a motor vehicle collision and are directed to evaluate a child who was in one of the vehicles. The patient appears to be a child
ITLS Pediatric Provider Course Basic Pre-Test 1. You arrive at the scene of a motor vehicle collision and are directed to evaluate a child who was in one of the vehicles. The patient appears to be a child
The Management of the Patient with an Acute Spinal Cord Injury D. J. Brown
 The Management of the Patient 1 Associate Prof. Director Victorian Spinal Cord Service Austin Health Melbourne, Victoria, Australia 2 3 Continuity of care A prevention C triage / transfer U emergency /
The Management of the Patient 1 Associate Prof. Director Victorian Spinal Cord Service Austin Health Melbourne, Victoria, Australia 2 3 Continuity of care A prevention C triage / transfer U emergency /
Anatomy and Physiology. The airways can be divided in to parts namely: The upper airway. The lower airway.
 Airway management Anatomy and Physiology The airways can be divided in to parts namely: The upper airway. The lower airway. Non-instrumental airway management Head Tilt and Chin Lift Jaw Thrust Advanced
Airway management Anatomy and Physiology The airways can be divided in to parts namely: The upper airway. The lower airway. Non-instrumental airway management Head Tilt and Chin Lift Jaw Thrust Advanced
Injuries to the Head and Spine From Bradys Emergency Care 10 th Edition
 Injuries to the Head and Spine From Bradys Emergency Care 10 th Edition 1. When performing the four-rescuer log roll, which responder pulls the board into position? A.) Head B.) Waist C.) Knee D.) Shoulder
Injuries to the Head and Spine From Bradys Emergency Care 10 th Edition 1. When performing the four-rescuer log roll, which responder pulls the board into position? A.) Head B.) Waist C.) Knee D.) Shoulder
Competency Log Professional Responder Courses
 Competency Log Professional Responder Courses Check off each competency once successfully demonstrated. This log may be used as a support tool when teaching a Professional Responder course. Refer to the
Competency Log Professional Responder Courses Check off each competency once successfully demonstrated. This log may be used as a support tool when teaching a Professional Responder course. Refer to the
Controversies in Spinal Immobilization
 Controversies in Spinal Immobilization Ken Berumen, BSN, MD, FACEP Medical Director El Paso Fire Department Medical Director Emergency Services District #1 Network Director EM Sierra Providence Health
Controversies in Spinal Immobilization Ken Berumen, BSN, MD, FACEP Medical Director El Paso Fire Department Medical Director Emergency Services District #1 Network Director EM Sierra Providence Health
CERVICAL SPINE TIPS A
 CERVICAL SPINE TIPS A Musculoskeletal Approach to managing Neck Pain An ALGORITHM, as a management guide Rick Bernau & Ian Wallbridge June 2010 THE PROCESS An interactive approach to the management of
CERVICAL SPINE TIPS A Musculoskeletal Approach to managing Neck Pain An ALGORITHM, as a management guide Rick Bernau & Ian Wallbridge June 2010 THE PROCESS An interactive approach to the management of
AIRWAY MANAGEMENT AND VENTILATION
 AIRWAY MANAGEMENT AND VENTILATION D1 AIRWAY MANAGEMENT AND VENTILATION Basic airway management and ventilation The laryngeal mask airway and Combitube Advanced techniques of airway management D2 Basic
AIRWAY MANAGEMENT AND VENTILATION D1 AIRWAY MANAGEMENT AND VENTILATION Basic airway management and ventilation The laryngeal mask airway and Combitube Advanced techniques of airway management D2 Basic
DOCUMENT CONTROL PAGE
 DOCUMENT CONTROL PAGE Title Title: UNDERGOING SPINAL DEFORMITY SURGERY Version: 2 Reference Number: Supersedes Supersedes: all other versions Description of Amendment(s): Revision of analgesia requirements
DOCUMENT CONTROL PAGE Title Title: UNDERGOING SPINAL DEFORMITY SURGERY Version: 2 Reference Number: Supersedes Supersedes: all other versions Description of Amendment(s): Revision of analgesia requirements
Spinal or Suspected Spinal, Injury: Logrolling Technique with C- Spine Precautions
 Approved by: Spinal or Suspected Spinal, Injury: Logrolling Technique with C- Spine Precautions Vice President and Chief Medical Officer; and Vice President and Chief Operating Officer Corporate Policy
Approved by: Spinal or Suspected Spinal, Injury: Logrolling Technique with C- Spine Precautions Vice President and Chief Medical Officer; and Vice President and Chief Operating Officer Corporate Policy
2017 Northern Mine Rescue Contest Written Exam (First Aid Competition)
") 2017 Northern Mine Rescue Contest Written Exam (First Aid Competition) 2017 2010 June 5, 2017 Findley Lake, New York 2017 Northern Mine Rescue Contest Written Exam First Aid Competition Directions: Fill
2017 Northern Mine Rescue Contest Written Exam (First Aid Competition) 2017 2010 June 5, 2017 Findley Lake, New York 2017 Northern Mine Rescue Contest Written Exam First Aid Competition Directions: Fill
Shepherd Center: A Catastrophic Care Hospital. The Jane Woodruff Pavilion
 Shepherd Center: A Catastrophic Care Hospital The Jane Woodruff Pavilion Acute Management of SCI & Prevention of Secondary Complications Joycelyn Craig, BSN, RN, CRRN SCI Nurse Education Manager FACTS
Shepherd Center: A Catastrophic Care Hospital The Jane Woodruff Pavilion Acute Management of SCI & Prevention of Secondary Complications Joycelyn Craig, BSN, RN, CRRN SCI Nurse Education Manager FACTS
TEACHING BASIC LIFE SUPPORT (& ALS)
") TEACHING BASIC LIFE SUPPORT (& ALS) Anton Koželj, R.N., B. Sc., lecturer Faculty of Health Sciences, University of Maribor Žitna ulica 15, 2000 Maribor, Slovenia Fact s To know-how to perform basic life
TEACHING BASIC LIFE SUPPORT (& ALS) Anton Koželj, R.N., B. Sc., lecturer Faculty of Health Sciences, University of Maribor Žitna ulica 15, 2000 Maribor, Slovenia Fact s To know-how to perform basic life
Level 5 Paramedic Primary Skills
 Title: Paramedic Primary Assessment Sheets V-4 Page: 1 of 15 Owner: LD Approved by: Examination Quality Group Approval date: March 2017 PHECC National Qualification in Emergency Medical Technology (NQEMT)
Title: Paramedic Primary Assessment Sheets V-4 Page: 1 of 15 Owner: LD Approved by: Examination Quality Group Approval date: March 2017 PHECC National Qualification in Emergency Medical Technology (NQEMT)
ABCDE HOW TO RECOGNISE AND TREAT THE SERIOUSLY ILL CHILD
 ABCDE HOW TO RECOGNISE AND TREAT THE SERIOUSLY ILL CHILD A B C D E Possible Problems Airway obstruction Partial or complete Foreign body Secretions/blood/vomit Infection Swelling e.g. anaphylaxis trauma
ABCDE HOW TO RECOGNISE AND TREAT THE SERIOUSLY ILL CHILD A B C D E Possible Problems Airway obstruction Partial or complete Foreign body Secretions/blood/vomit Infection Swelling e.g. anaphylaxis trauma
Other methods for maintaining the airway (not definitive airway as still unprotected):
:") Page 56 Where anaesthetic skills and drugs are available, endotracheal intubation is the preferred method of securing a definitive airway. This technique comprises: rapid sequence induction of anaesthesia
Page 56 Where anaesthetic skills and drugs are available, endotracheal intubation is the preferred method of securing a definitive airway. This technique comprises: rapid sequence induction of anaesthesia
Management of Spinal Cord Injury outside of a specialist Spinal Injuries Centre The Derby Experience
 Management of Spinal Cord Injury outside of a specialist Spinal Injuries Centre The Derby Experience Sharon Budd Trauma Nurse Derby Hospitals NHS Foundation Trust Learning Outcomes To understand the role
Management of Spinal Cord Injury outside of a specialist Spinal Injuries Centre The Derby Experience Sharon Budd Trauma Nurse Derby Hospitals NHS Foundation Trust Learning Outcomes To understand the role
Care of the Deteriorating Patient in Recovery NADIA TICEHURST : CLINICAL NURSE EDUCATOR PERI ANAESTHETICS BENDIGO HEALTH
 Care of the Deteriorating Patient in Recovery NADIA TICEHURST : CLINICAL NURSE EDUCATOR PERI ANAESTHETICS BENDIGO HEALTH Intended learning outcomes Describe the components of a comprehensive clinician
Care of the Deteriorating Patient in Recovery NADIA TICEHURST : CLINICAL NURSE EDUCATOR PERI ANAESTHETICS BENDIGO HEALTH Intended learning outcomes Describe the components of a comprehensive clinician
Cervical Collar Policy 2010
 Cervical Collar Policy 2010 Version 1 For implementation in 2011 1 P a g e Introduction The Australian Rugby League is committed in providing the best possible care for all players who play the game of
Cervical Collar Policy 2010 Version 1 For implementation in 2011 1 P a g e Introduction The Australian Rugby League is committed in providing the best possible care for all players who play the game of
Chapter 26 Head and Spine Trauma The Nervous System The nervous system controls virtually all of our body activities including reflex, voluntary and
 1 2 3 4 5 Chapter 26 Head and Spine Trauma The Nervous System The nervous system controls virtually all of our body activities including reflex, voluntary and involuntary activities Voluntary activities
1 2 3 4 5 Chapter 26 Head and Spine Trauma The Nervous System The nervous system controls virtually all of our body activities including reflex, voluntary and involuntary activities Voluntary activities
Spinal cord compression
 Spinal cord compression Urology Department Patient Information Leaflet Introduction If you have been diagnosed with cancer, you need to know about spinal cord compression and the warning signs. This leaflet
Spinal cord compression Urology Department Patient Information Leaflet Introduction If you have been diagnosed with cancer, you need to know about spinal cord compression and the warning signs. This leaflet
Suspected spinal cord compression form
 Suspected spinal cord compression form Enter this form into the notes at the appropriate date in the Progress / Evaluation sheets. Please copy this form to Lisa Lewis, Medical PA (ext 4551), for audit
Suspected spinal cord compression form Enter this form into the notes at the appropriate date in the Progress / Evaluation sheets. Please copy this form to Lisa Lewis, Medical PA (ext 4551), for audit
Appendix (i) The ABCDE approach to the sick patient
 The ABCDE approach to the sick patient") Appendix (i) The ABCDE approach to the sick patient This appendix and the one following provide guidance on the initial approach and management of common medical emergencies which may arise in general
Appendix (i) The ABCDE approach to the sick patient This appendix and the one following provide guidance on the initial approach and management of common medical emergencies which may arise in general
Examples EMERGENCY SITUATIONS IN SPORTS
 Examples EMERGENCY SITUATIONS IN SPORTS Dr Kaspar Rõivassepp Orthopedic surgeon (North Estonian Medical Centre, Estonian Football Association) 23.08.2015 IX Baltic Sports Medicine Conference The most serious
Examples EMERGENCY SITUATIONS IN SPORTS Dr Kaspar Rõivassepp Orthopedic surgeon (North Estonian Medical Centre, Estonian Football Association) 23.08.2015 IX Baltic Sports Medicine Conference The most serious
Activity Three: Where s the Bleeding?
 Activity Three: Where s the Bleeding? There are five main sites of potentially fatal bleeding in trauma, remembered by the phrase on the floor and four more. On the floor refers to losing blood externally
Activity Three: Where s the Bleeding? There are five main sites of potentially fatal bleeding in trauma, remembered by the phrase on the floor and four more. On the floor refers to losing blood externally
RESPIRATORY COMPLICATIONS AFTER SCI
 SHEPHERD.ORG RESPIRATORY COMPLICATIONS AFTER SCI NORMA I RIVERA, RRT, RCP RESPIRATORY EDUCATOR SHEPHERD CENTER 2020 Peachtree Road, NW, Atlanta, GA 30309-1465 404-352-2020 DISCLOSURE STATEMENT I have no
SHEPHERD.ORG RESPIRATORY COMPLICATIONS AFTER SCI NORMA I RIVERA, RRT, RCP RESPIRATORY EDUCATOR SHEPHERD CENTER 2020 Peachtree Road, NW, Atlanta, GA 30309-1465 404-352-2020 DISCLOSURE STATEMENT I have no
Pediatric Patients. BCFPD Paramedic Education Program. EMS Education Paramedic Level
 Pediatric Patients BCFPD Program Basic Considerations Much of the initial patient assessment can be done during visual examination of the scene. Involve the caregiver or parent as much as possible. Allow
Pediatric Patients BCFPD Program Basic Considerations Much of the initial patient assessment can be done during visual examination of the scene. Involve the caregiver or parent as much as possible. Allow
Spinal Trauma. Dr T G Kruger
 Spinal Trauma Dr T G Kruger Epidemiology Spine injury in 6% of trauma patients Multiple levels involved in 20% of cases 80% of spinal cord injury patients have concurrent other system injuries 41% have
Spinal Trauma Dr T G Kruger Epidemiology Spine injury in 6% of trauma patients Multiple levels involved in 20% of cases 80% of spinal cord injury patients have concurrent other system injuries 41% have
Fractures of the Thoracic and Lumbar Spine
 A spinal fracture is a serious injury. Nader M. Hebela, MD Fellow of the American Academy of Orthopaedic Surgeons http://orthodoc.aaos.org/hebela Cleveland Clinic Abu Dhabi Cleveland Clinic Abu Dhabi Neurological
A spinal fracture is a serious injury. Nader M. Hebela, MD Fellow of the American Academy of Orthopaedic Surgeons http://orthodoc.aaos.org/hebela Cleveland Clinic Abu Dhabi Cleveland Clinic Abu Dhabi Neurological
Spinal Trauma. General Rehabilitation of Patient with Spinal Trauma. Common Spinal Injuries. Important Anatomical Structures at each Vertebral Level
 Asian Association for Dynamic Osteosynthesis Workshop on Management of Spinal Trauma 22 April 2007 (Sunday) Orthopaedic Learning Centre, PWH, Shatin, Hong Kong General Rehabilitation of Patient with Spinal
Asian Association for Dynamic Osteosynthesis Workshop on Management of Spinal Trauma 22 April 2007 (Sunday) Orthopaedic Learning Centre, PWH, Shatin, Hong Kong General Rehabilitation of Patient with Spinal
1. In a rear-impact motor vehicle crash, which area of the spine is most susceptible to injury? A. Cervical B. Thoracic C. Lumbar D.
 1. In a rear-impact motor vehicle crash, which area of the spine is most susceptible to injury? A. Cervical B. Thoracic C. Lumbar D. Sacral-coccygeal 2. A 36-year-old male sustains blunt force thoracic
1. In a rear-impact motor vehicle crash, which area of the spine is most susceptible to injury? A. Cervical B. Thoracic C. Lumbar D. Sacral-coccygeal 2. A 36-year-old male sustains blunt force thoracic
Restore adequate respiratory and circulatory conditions. Reduce pain
 Pre-hospital management of the trauma patient is best performed by an integrated team focused on minimizing the time from injury to definitive care at an appropriate trauma center. Dispatchers, first responders,
Pre-hospital management of the trauma patient is best performed by an integrated team focused on minimizing the time from injury to definitive care at an appropriate trauma center. Dispatchers, first responders,
Pulmonary Rehabilitation in Acute Spinal Cord Injury. Jatuporn Jatutawanit Physical therapist, Physical therapy unit, Prince of songkla university
 Pulmonary Rehabilitation in Acute Spinal Cord Injury Jatuporn Jatutawanit Physical therapist, Physical therapy unit, Prince of songkla university Causes of spinal cord injury Traumatic injury Motor vehicle
Pulmonary Rehabilitation in Acute Spinal Cord Injury Jatuporn Jatutawanit Physical therapist, Physical therapy unit, Prince of songkla university Causes of spinal cord injury Traumatic injury Motor vehicle
Competency Statement: Manoeuvring an In-Patient with a Spinal or Suspected Spinal Injury.
 Competency Statement: Manoeuvring an In-Patient with a Spinal or Suspected Spinal Injury. 1 st Level 2 nd Level 3 rd level 4 th level Competently participate as part of the manoeuvring team; To turn (Log
Competency Statement: Manoeuvring an In-Patient with a Spinal or Suspected Spinal Injury. 1 st Level 2 nd Level 3 rd level 4 th level Competently participate as part of the manoeuvring team; To turn (Log
1 Chapter 40 Advanced Airway Management 2 Advanced Airway Management The advanced airway management techniques discussed in this chapter are to
 1 Chapter 40 Advanced Airway Management 2 Advanced Airway Management The advanced airway management techniques discussed in this chapter are to introduce the EMT-B student to these procedures only. In
1 Chapter 40 Advanced Airway Management 2 Advanced Airway Management The advanced airway management techniques discussed in this chapter are to introduce the EMT-B student to these procedures only. In
Chapter 40 Advanced Airway Management
 1 2 3 4 5 Chapter 40 Advanced Airway Management Advanced Airway Management The advanced airway management techniques discussed in this chapter are to introduce the EMT-B student to these procedures only.
1 2 3 4 5 Chapter 40 Advanced Airway Management Advanced Airway Management The advanced airway management techniques discussed in this chapter are to introduce the EMT-B student to these procedures only.
Competency Indicators Pediatrics Registered Nurse
 Hospital Logo Competency Indicators Pediatrics Registered Nurse mployee Name: Review Key: = ducation Session valuation Key: Able to perform & document A: Airway assessment: mployee Describes unique airway
Hospital Logo Competency Indicators Pediatrics Registered Nurse mployee Name: Review Key: = ducation Session valuation Key: Able to perform & document A: Airway assessment: mployee Describes unique airway
HeartCode PALS. PALS Actions Overview > Legend. Contents
 HeartCode PALS PALS Actions Overview > Legend Action buttons (round buttons) Clicking a round button initiates an action. Clicking this button, for example, checks the child s carotid pulse. Menu buttons
HeartCode PALS PALS Actions Overview > Legend Action buttons (round buttons) Clicking a round button initiates an action. Clicking this button, for example, checks the child s carotid pulse. Menu buttons
Acute to Rehab Spinal Cord Injuries Anna Brown CNC, Certificate SCI Nursing, Grad Dip Rehabilitation Studies, La Trobe
 Acute to Rehab Spinal Cord Injuries Anna Brown CNC, Certificate SCI Nursing, Grad Dip Rehabilitation Studies, La Trobe Victorian Spinal Cord Service Austin Health SCI Acute to Rehab Let the rollercoaster
Acute to Rehab Spinal Cord Injuries Anna Brown CNC, Certificate SCI Nursing, Grad Dip Rehabilitation Studies, La Trobe Victorian Spinal Cord Service Austin Health SCI Acute to Rehab Let the rollercoaster
MULTIPLE CHOICE. Choose the one alternative that best completes the statement or answers the question.
 EPC Ch 24 Quiz w-key Name MULTIPLE CHOICE. Choose the one alternative that best completes the statement or answers the question. 1) Which of the following best explains the presentation and prognosis of
EPC Ch 24 Quiz w-key Name MULTIPLE CHOICE. Choose the one alternative that best completes the statement or answers the question. 1) Which of the following best explains the presentation and prognosis of
Scope of Practice Athletic Rehabilitation Therapist, Certified (A.R.T.C.)
") Scope of Practice Athletic Rehabilitation Therapist, Certified (A.R.T.C.) An Athletic Rehabilitation Therapist Certified (A.R.T.C) is an autonomous health care practitioner to whom members of the public
Scope of Practice Athletic Rehabilitation Therapist, Certified (A.R.T.C.) An Athletic Rehabilitation Therapist Certified (A.R.T.C) is an autonomous health care practitioner to whom members of the public
3/10/17 Spinal a Injury 1
 Spinal Injury 1 'Paralysed' Watmough vows he'll have the backbone for Game Two after treatment for neck injury Watmough will have cortisone injected into his spine this morning to speed up the recovery
Spinal Injury 1 'Paralysed' Watmough vows he'll have the backbone for Game Two after treatment for neck injury Watmough will have cortisone injected into his spine this morning to speed up the recovery
Surgery. Conus medullaris and Cauda Equina Syndromes. Anatomy. See online here
 Surgery Conus medullaris and Cauda Equina Syndromes See online here Conus medullaris and cauda equina syndromes are spinal cord injuries that involve injury to the lumbosacral segment of the spinal cord.
Surgery Conus medullaris and Cauda Equina Syndromes See online here Conus medullaris and cauda equina syndromes are spinal cord injuries that involve injury to the lumbosacral segment of the spinal cord.
PRE-HOSPITAL EMERGENCY CARE COURSE.
 PRE-HOSPITAL EMERGENCY CARE COURSE www.basics.org.uk Chest Assessment & Management BASICS Education March 2016 Objectives To understand the importance of oxygenation and ventilation To be able to describe
PRE-HOSPITAL EMERGENCY CARE COURSE www.basics.org.uk Chest Assessment & Management BASICS Education March 2016 Objectives To understand the importance of oxygenation and ventilation To be able to describe
Title Protocol for the management of suspected cauda equine syndrome & decompensating spinal stenosis at NDDH
 Document Control Title Protocol for the management of suspected cauda equine syndrome & decompensating spinal stenosis at NDDH Author Author s job title Consultant T&O Directorate Scheduled Care Department
Document Control Title Protocol for the management of suspected cauda equine syndrome & decompensating spinal stenosis at NDDH Author Author s job title Consultant T&O Directorate Scheduled Care Department
Brain and Central Nervous System Cancers
 Brain and Central Nervous System Cancers NICE guidance link: https://www.nice.org.uk/guidance/ta121 Clinical presentation of brain tumours History and Examination Consider immediate referral Management
Brain and Central Nervous System Cancers NICE guidance link: https://www.nice.org.uk/guidance/ta121 Clinical presentation of brain tumours History and Examination Consider immediate referral Management
Ligamentous Integrity in Spinal Cord Injury without Radiographic Abnormality. Dr Anria Horn Dr Stewart Dix-Peek
 Ligamentous Integrity in Spinal Cord Injury without Radiographic Abnormality Dr Anria Horn Dr Stewart Dix-Peek Introduction Spinal Cord Injury Without Radiographic Abnormality SCIWORA Pang, Wilberger 1982
Ligamentous Integrity in Spinal Cord Injury without Radiographic Abnormality Dr Anria Horn Dr Stewart Dix-Peek Introduction Spinal Cord Injury Without Radiographic Abnormality SCIWORA Pang, Wilberger 1982
Trauma CT Scanning Protocol
 Northern Trauma Network Trauma CT Scanning Protocol Background Whole body CT (WBCT) has assumed a pivotal position in trauma management. UK trauma is typically described as blunt and blind i.e. blunt trauma
Northern Trauma Network Trauma CT Scanning Protocol Background Whole body CT (WBCT) has assumed a pivotal position in trauma management. UK trauma is typically described as blunt and blind i.e. blunt trauma
Yaniv Berliner EMS STABILIZATION
 Yaniv Berliner EMS STABILIZATION Scene survey EMS must first evaluate the safety of the scene. Downed power lines, fire, traffic Is there a need for specialized equipment for extrication. Is there a need
Yaniv Berliner EMS STABILIZATION Scene survey EMS must first evaluate the safety of the scene. Downed power lines, fire, traffic Is there a need for specialized equipment for extrication. Is there a need
CHEST INJURY PULMONARY CONTUSION
 CHEST INJURY PULMONARY CONTUSION Introduction Pulmonary contusion refers to blunt traumatic lung parenchymal injury which results in oedema and haemorrhaging into alveolar spaces. It may also result in
CHEST INJURY PULMONARY CONTUSION Introduction Pulmonary contusion refers to blunt traumatic lung parenchymal injury which results in oedema and haemorrhaging into alveolar spaces. It may also result in
A Patient s Guide to Burners and Stingers
 A Patient s Guide to Burners and Stingers 763 Larkfield Road 2nd Floor Commack, NY 11725 Phone: (631) 462-2225 Fax: (631) 462-2240 DISCLAIMER: The information in this booklet is compiled from a variety
A Patient s Guide to Burners and Stingers 763 Larkfield Road 2nd Floor Commack, NY 11725 Phone: (631) 462-2225 Fax: (631) 462-2240 DISCLAIMER: The information in this booklet is compiled from a variety
Paediatric Trauma. A/Prof Drew Richardson. The Canberra Hospital May MB BS (Hons) FACEM Grad CertHE MD
 FACEM Grad CertHE MD") Paediatric Trauma A/Prof Drew Richardson MB BS (Hons) FACEM Grad CertHE MD The Canberra Hospital May 2013 Objectives Identify unique anatomic and physiologic characteristics of injured children Describe
Paediatric Trauma A/Prof Drew Richardson MB BS (Hons) FACEM Grad CertHE MD The Canberra Hospital May 2013 Objectives Identify unique anatomic and physiologic characteristics of injured children Describe
Head injuries. Severity of head injuries
 Head injuries ED Teaching day 23 rd October Severity of head injuries Minor GCS 14-15 Must not have any of the following: Amnesia 10min Neurological sign or symptom Skull fracture (clinically or radiologically)
Head injuries ED Teaching day 23 rd October Severity of head injuries Minor GCS 14-15 Must not have any of the following: Amnesia 10min Neurological sign or symptom Skull fracture (clinically or radiologically)
PRE-HOSPITAL PATIENT CARE PROTOCOLS BASIC LIFE SUPPORT/ADVANCED LIFE SUPPORT
 PRE-HOSPITAL PATIENT CARE PROTOCOLS BASIC LIFE SUPPORT/ADVANCED LIFE SUPPORT Board Approved June 2007 Revised December 2009 Revised July 2011 Revised June 2015 435 Hunter Street Fredericksburg, VA 22401
PRE-HOSPITAL PATIENT CARE PROTOCOLS BASIC LIFE SUPPORT/ADVANCED LIFE SUPPORT Board Approved June 2007 Revised December 2009 Revised July 2011 Revised June 2015 435 Hunter Street Fredericksburg, VA 22401
4/19/2017. Prehospital Spinal Care: Then. Prehospital Spinal Care: Then. Prehospital Spinal Care: Then. Prehospital Spinal Care: Then. Why Immobilize?
 Management of Cervical Spine Injuries and Athletic Equipment Removal Gianluca Del Rossi, PhD, ATC Prehospital Spinal Care: Then While the exact origins of backboards in EMS are unclear, noted trauma surgeon
Management of Cervical Spine Injuries and Athletic Equipment Removal Gianluca Del Rossi, PhD, ATC Prehospital Spinal Care: Then While the exact origins of backboards in EMS are unclear, noted trauma surgeon
CORE STANDARDS STANDARDS USED IN TARN REPORTS
 CORE STANDARDS Time to CT Scan BEST PRACTICE TARIFF SECTION 4.10 MAJOR TRAUMA 7 If the patient is admitted directly to the MTC or transferred as an emergency, the patient must be received by a trauma team
CORE STANDARDS Time to CT Scan BEST PRACTICE TARIFF SECTION 4.10 MAJOR TRAUMA 7 If the patient is admitted directly to the MTC or transferred as an emergency, the patient must be received by a trauma team
Time Equals Neurons - Spinal Cord Injury Management in the first 4 Hours
 Time Equals Neurons - Spinal Cord Injury Management in the first 4 Hours William D. Whetstone M.D. Clinical Professor UCSF Department of Emergency Medicine SFGH ED Center for Neuro-Critical Emergencies
Time Equals Neurons - Spinal Cord Injury Management in the first 4 Hours William D. Whetstone M.D. Clinical Professor UCSF Department of Emergency Medicine SFGH ED Center for Neuro-Critical Emergencies