Determining causation of traumatic versus preexisting. conditions. David Fisher, Ph.D., ABPP, LP Chairman of the Board PsyBar, LLC
|
|
|
- Sheryl Short
- 6 years ago
- Views:
Transcription

1 Determining causation of traumatic versus preexisting psychological conditions David Fisher, Ph.D., ABPP, LP Chairman of the Board PsyBar, LLC
2 Part 1: First steps to determine causation
3 Information to gather prior to psychological/psychiatric evaluation All prior psychological/psychiatric evaluations Collateral contact information (doctors, supervisors, etc.) Raw test data and raw test protocols mailed directly from the past psychologist to the IME psychologist/psychiatrist (They relate to assessing validity and duration of the problems)
4 Information to gather prior to psychological/psychiatric evaluation Relevant medical information such as neuroimaging studies, physicals Past psychiatric/psychological treatment records for as far back in time as possible
5 Part 2: Neuropsychological IMES:


6 Neuropsychology: Includes the assessment of cognitive abilities with a combination of objective procedures as well as largely subjective observations.
7 Neuropsychological assessment used when: There is a trauma, injury or disease causing: Cognitive difficulties Physical functioning problems (e.g. fatigue, perceptual problems) Emotional problems

8 Neuropsychological assessment used even if: Neurological or other evaluations do not show problems (MRI,CT etc. show structure, not function).
9 Neuropsychological assessment used even if: There is no impairment in cognitive functioning that would be obvious to a physician.
10 A good evaluation to determine functioning and causation will include: Extensive interview with the patient (2-31/2 hours) with an additional 4 to 10 hours of testing. Collateral interviews with spouse, employer, and / or others (often used in tx settings)
11 A good evaluation to determine functioning and causation will contain a range of tests measuring: Intellectual abilities Memory Motor speed and coordination Naming skills & verbal fluency
12 A good evaluation to determine functioning and causation will include: Attention Executive Processing speed Personality traits & mood Truthfulness, motivation and effort/malingering
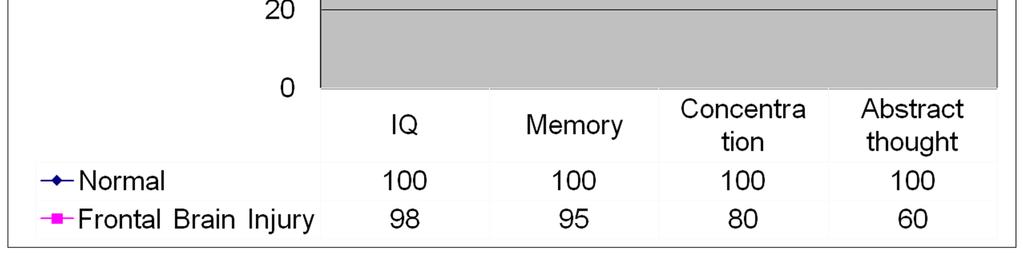
13 In a normal individual with no brain damage: The measurement of different cognitive abilities should result in test scores that are roughly equivalent to each other.
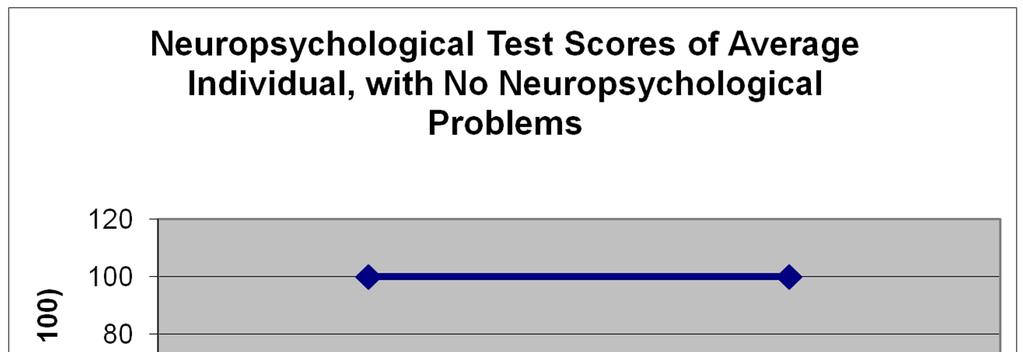
14
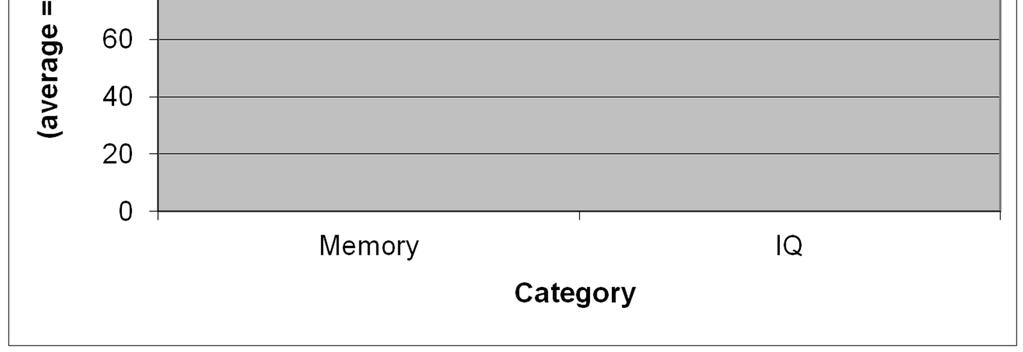
15 IQ usually remains stable after injury, while other tests might not. Full Scale IQ scores tend to be largely unaffected by most brain injuries. Scores on other psychological test scores frequently decline.
16
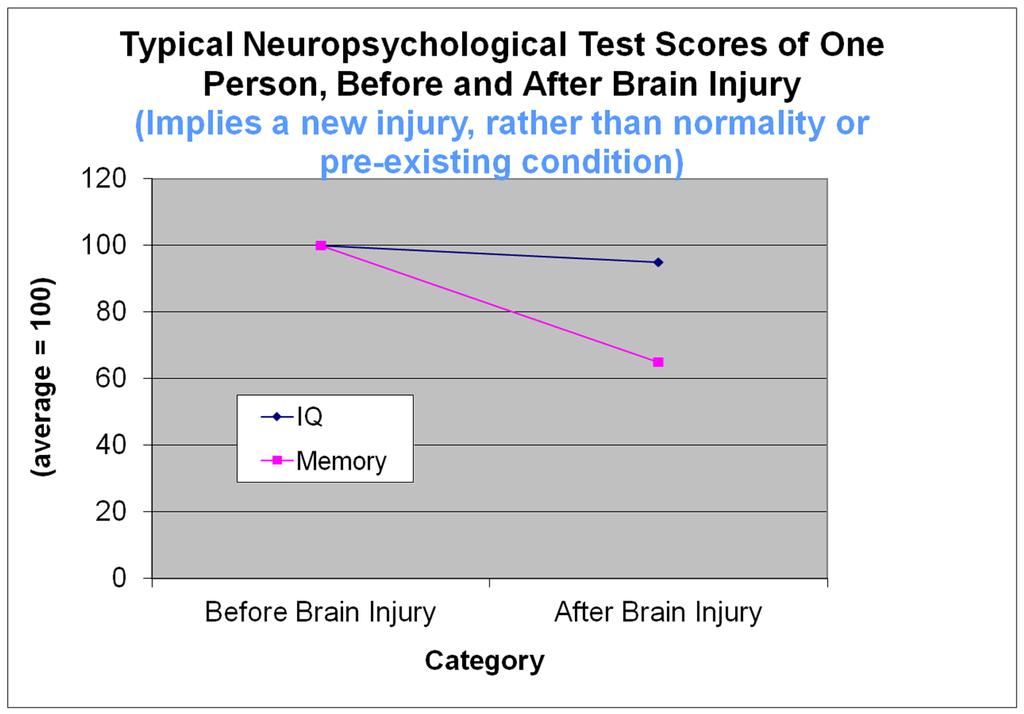
17 Injuries to the front part of the brain can cause problems with: The ability to understand abstract concepts Concentration The ability to form memories Personality changes

18 Phineas Gage (1848 injury)
19
20 The previous graph implies acquired, rather than normality or a pre-existing condition because the scores: Are consistent with a frontal injury, rather than with a normal medical history Severely depressed people often have worrisome problems with more effortful memory tasks. (If this were due to longer term depression, rather than a recent frontal injury, with some the score would be low)
21 Often pre-existing psychological vs. acquired brain injury: Inconsistency from one evaluation to the next and problems worsen during times of emotional stress Inconsistency from one conceptually similar test to the next
22 Determining deception by comparisons to prior scores: Person with brain injury: Scores show rapid recovery in first 4 months after injury. Recovery very slow after 1.5 years. (If we don t see these patterns it could be pre-existing or something else)
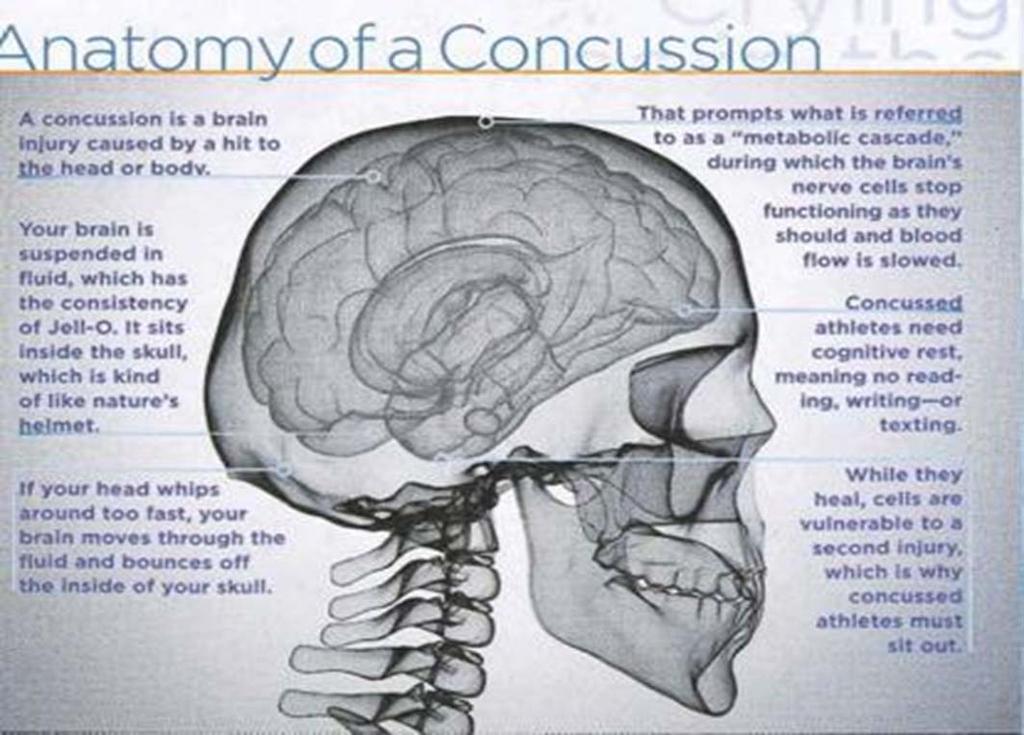
23 Mild Traumatic Brain injury:
24 Lots of misinformation:
25 Clinical presentation Recent head trauma, often with no loss of consciousness Memory, concentration, irritability, decline in work performance, depression and anxiety Collateral sources confirm behavior change Nobody can find anything physically wrong Seem clinically identical to people with more severe TBI
26 Defining MTBI without LOC Alteration in mental status Confusion or amnesia Delayed verbal/motor responding Difficulty focusing attention Disorientation Slurred/incoherent speech Gross motor incoordination American Academy of Neurology Guidelines for Management of Sport Concussion
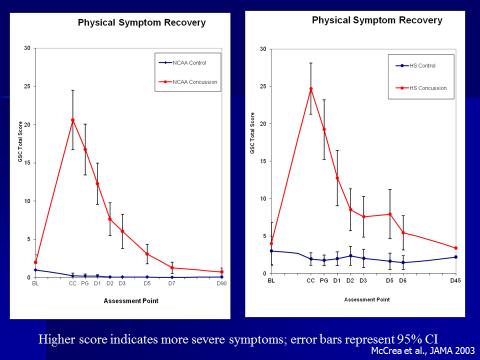
27 Participants NCAA Concussion Study (4, 251 college athletes) Concussion Prevention Initiative-CPI (9,094 high school/college athletes) Project Sideline (3,279 high school athletes) Pre-post measures Less concern about litigation bias
28
29 Physical Symptoms: Summary Most severe immediately following injury, measurable improvement within hours Gradual improvement occurs up to ~7 days Headache tends to remain the longest, may be primary in clinical management
30
31 Cognitive Symptoms Most severe immediately following injury, measurable improvement within hours Gradual improvement occurs up to ~7 days for most individuals Memory most susceptible to change but shows complete recovery within days Frank cognitive abnormalities are not common
32 Misattribution: PCS Sx are present in numerous groups resulting in attribution problems, sometimes to pre-existing issues College Students Chronic Pain Pts. Depressed Pts. Personal Injury Claimants (non TBI) Headache Dizziness Irritability Memory Problems 36% 18% 36% 17% 42% 80% 67% 49% 33% 63% 37% 20% 52% 25% 54% 77% 41% 63% 46% 71% MTBI 42% 26% 28% 36% 25% Concentratio nproblems
33 $64,000 questions: Have symptoms worsened with time? Are symptoms more persistent than expected with this diagnosis? Inconsistency from one evaluation to the next and problems worsen during times of emotional stress
34 If yes, then... Assess for complicating factors, including pre-existing conditions. Depression (Adjustment Reaction, Major Depressive Episode) Posttraumatic Stress Disorder (PTSD) Somatic Disorders Malingering
35 Part 3: Validity

36
37 Definition of malingering: For an external goal, an individual deliberately fabricates a symptom.
38 Attribution of problems Attributing an illness or symptom to the wrong cause is also a type of malingering. Sometimes seen in workers compensation claims.
39 Rates of malingering/ exaggeration of cognitive impairment: Personal Injury: 29% Disability: 30% Fibromyalgia/CFS 35% Chronic fatigue: 35% Chronic pain: 31% Mild head injury: 39% Mittenberg, W., Patton, C., Canyock, E..M., & Condit, D.C. (2002) Base Rates of malingering and symptom exaggeration. Journal of clinical and Experimental Neuropsychology. 24,
40 Can have both cognitive impairment and deception Most claimants probably accurately report their psychiatric symptoms. Gilding the lily for insurance reimbursement. Tough for IME examiners to see genuinely impaired people who exaggerate.
41 Can have both cognitive impairment and defensiveness Embarrassment about brain injury or other problems. Claimants might conceal the true cause of their problems, such as a brain injury, out of embarrassment
42 False appearance of defensiveness Brain injury (many don t realize the extent of their injuries). Importance of collateral interviews, objective psychological testing, careful records review, and observation. (Often critical in determining new versus preexisting)
43 Clinical Judgment/ intuitional perspective I ve evaluated thousands of patients over 30 years and I know a faker when I see one. Why do I need psychological tests?
44 Clinical judgment/ intuitional perspective Myth: With an interview, a psychologist or psychiatrist, using many years of clinical knowledge, can consistently identify those individuals who are deceptive.
45 Clinical judgment/ intuitional perspective Fact: There is little, if any, credible evidence that experienced mental health professionals are able, across a variety of situations, to reliably identify deception using clinical judgment alone.
46 Treating doctors: Assumption of truthfulness from their patients. Don t necessarily develop the skills to assess this according to forensic standards.
47 Objective testing: Over a hundred years of research on objective psychological testing has demonstrated that it can often measure skills and behavior more accurately than can the most skilled clinicians.



48 Objective psychological testing is often critical in resolving these claims
49 Objective testing: Usually desirable for the psychologist or psychiatrist to rely in part on objective psychological test results to assess deception and determine the onset of the problems.
50 Test of Memory Malingering 15 minutes long and requires claimant to remember simple drawings Claimants who are not putting forth full effort receives scores lower than those obtained by patients with genuine neuropsychological problems Correct classification rate is approximately 80%
51 Validity Indicator Profile Sophisticated computer-scored test Cannot be used with individuals who are severely cognitive impaired Both verbal and visual portions Approximately 77% correct classification rate
52 How to ask questions about causation and validity: Avoid leading questions. Unintentionally, Independent Examiners might be influenced by leading questions Even when Independent Examiners impartially answer leading questions, those responses are vulnerable to challenges during litigation.
53 Referral question Rather than directly asking about malingering: Please explain how your sources of evidence above are consistent or inconsistent with each other. For example, is the examinee self-report consistent with your observations and with test data? (Questions PsyBar )
54 Tests designed to help assess for deception of psychological symptoms, such as depression and anxiety:
55 MMPI-2 and MMPI-2-RF Revised throughout the 1980s Examines validity of reports of psychological disturbance (not specifically designed to evaluate truthfulness regarding neuropsychological dysfunction Evaluates areas such as depression, anxiety, attitude towards work and psychotherapy, tendency to report physical problems when under emotional stress, and self-confidence.
56 MMPI-2 and MMPI-2-RF Also useful in detecting defensiveness, or downplaying the severity of symptoms.


57 MMPI-2 and MMPI-2-RF Gold standard
58 MMPI-II Not specifically designed for medical populations Contains some of the best (sub) tests to assess malingering of psychiatric problems. Can over-estimate psychological problems in medical patients
59 To compensate for the MMPI s shortcoming, objectively compare claimant s psychiatric distress and other complaints to those of others who are undergoing physical rehabilitation using the BHI-2:
60 Battery for Health Improvement 2 Compares claimant to many people with substantiated physical problems and to healthy individuals. Does not overpathologize what is normal for medical patients. Has measures of validity. (Measures symptom minimization and magnification). 217 items
61 Battery for Health Improvement 2 measures affective factors: Depression Anxiety Hostility
62 Battery for Health Improvement 2 measures character factors: Borderline (a range of personality disorders) (Often pre-existing) Symptom Dependency (use of symptoms for secondary gain) (Sometimes pre-existing) Chronic Maladjustment (Often pre-existing) Perseverance Substance Abuse (claimant report only)
63 Battery for Health Improvement 2 measures psychosocial factors: Family Dysfunction (identifies potentially enabling tendencies that might undermine functionality) Job Dissatisfaction (avoidance might be source of secondary gain) Doctor Dissatisfaction
64 Battery for Health Improvement 2 measures general Physical symptoms: Somatic Complaints (Somatic preoccupation often preexisting) Pain Complaints (Claimants perception of pain in 10 body areas often pre-existing) Functional Complaints (Claimants perception of own limitations) Muscular Bracing (Claimant perception of muscular tightness)
65 Structured Interview of Reported symptoms (1992) Designed to assess feigning (The deliberate production of psychological symptoms. The purpose, or goal, is not known).
66 Personality Assessment Inventory (PAI) Well researched and designed test Not used as frequently as the MMPI-2 Has standardized cut-off scales for feigning.
67 Tests designed to help assess for deception of cognitive symptoms, such as problems with memory and concentration
68 TOMM 15 minutes long and requires claimant to remember simple drawings Claimants who are not putting forth full effort receives scores lower than those obtained by patients with genuine neuropsychological problems Easily hand scored Classification rate approximately 80%
69 Validity Indicator Profile (1997) Sophisticated computer-scored test Assesses suboptimal effort. Cannot be used with individuals who are severely cognitive impaired Both verbal and visual portions. Approximately 77% correct classification rate.
70 When does it make sense to use more than one test to evaluate deception? Usually, as multiple validity tests recommended throughout long assessments.
71 How to request Specific Psychological Tests Very diplomatically Don t tell the psychologist what to do Focus more on defining the problem to be answered and working with the psychologist about the best tests to use Very complex process, taking into consideration test validity/reliability, examinee age, sex, capabilities, etc.
72
73
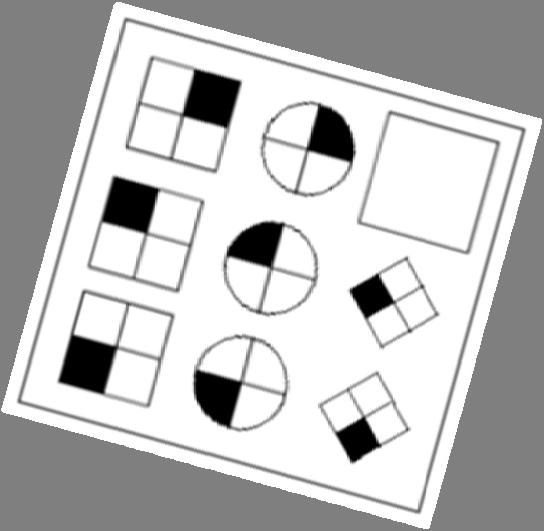
74 Projective tests that, when used alone, might confuse issue of traumatic vs. preexisting: Rorschach ( Inkblots ) TAT (Telling stories about pictures) House-tree Person ( Draw a house, a tree, and a person ) Incomplete Sentences (e.g. When I was young, my mother used to. )
75
76 PsyBar LLC 6600 France Avenue South #640 Minneapolis, MN
77 Where are your employees located?
Donald A. Davidoff, Ph.D., ABPDC Chief, Neuropsychology Department, McLean Hospital Assistant Professor of Psychology, Harvard Medical School
 Donald A. Davidoff, Ph.D., ABPDC Chief, Neuropsychology Department, McLean Hospital Assistant Professor of Psychology, Harvard Medical School Interests: Adult/Geriatric/Forensic Neuropsychology ddavidoff@mclean.harvard.edu
Donald A. Davidoff, Ph.D., ABPDC Chief, Neuropsychology Department, McLean Hospital Assistant Professor of Psychology, Harvard Medical School Interests: Adult/Geriatric/Forensic Neuropsychology ddavidoff@mclean.harvard.edu
The Components of an Objective IME
 The Components of an Objective IME Presented By: Lee H. Doppelt, PhD Brought to you by: Today s Topics Appropriate and ethical communication with IME providers IME providers standards of conduct requirement
The Components of an Objective IME Presented By: Lee H. Doppelt, PhD Brought to you by: Today s Topics Appropriate and ethical communication with IME providers IME providers standards of conduct requirement
VA/DoD Clinical Practice Guideline for the Management of Concussion/mTBI
 VA/DoD Clinical Practice Guideline for the Management of Concussion/mTBI Chief, Evidence-Based Practice US Army Medical Command Clinical Program Specialist Office of Performance and Quality Improvement
VA/DoD Clinical Practice Guideline for the Management of Concussion/mTBI Chief, Evidence-Based Practice US Army Medical Command Clinical Program Specialist Office of Performance and Quality Improvement
Adult Neuropsychological Issues: Impact on Intellectual Functioning and Return to Work. Kenneth Perrine, Ph.D., ABPP-CN Weill Cornell Medical College
 Adult Neuropsychological Issues: Impact on Intellectual Functioning and Return to Work Kenneth Perrine, Ph.D., ABPP-CN Weill Cornell Medical College Disclosures I receive compensation from the New York
Adult Neuropsychological Issues: Impact on Intellectual Functioning and Return to Work Kenneth Perrine, Ph.D., ABPP-CN Weill Cornell Medical College Disclosures I receive compensation from the New York
Neuropsychological Assessment: Applications to the Work Setting
 : Applications to the Work Setting! Arlin Pachet, Ph.D, R.Psych., ABPP Board Certified Clinical Neuropsychologist! September 30, 2014 1 Presentation Objectives! (NPA) overview What is an NPA? What is a
: Applications to the Work Setting! Arlin Pachet, Ph.D, R.Psych., ABPP Board Certified Clinical Neuropsychologist! September 30, 2014 1 Presentation Objectives! (NPA) overview What is an NPA? What is a
Community Partnerships for Youth Concussion Care: Power of the Medical Neighborhood
 Community Partnerships for Youth Concussion Care: Power of the Medical Neighborhood Gerard A. Gioia, Ph.D. Pediatric Neuropsychologist Chief, Division of Pediatric Neuropsychology Director, Safe Concussion
Community Partnerships for Youth Concussion Care: Power of the Medical Neighborhood Gerard A. Gioia, Ph.D. Pediatric Neuropsychologist Chief, Division of Pediatric Neuropsychology Director, Safe Concussion
Malingering (AADEP Position Paper) The gross volitional exaggeration or fabrication of symptoms/dysfunction for the purpose of obtaining substantial m
 The gross volitional exaggeration or fabrication of symptoms/dysfunction for the purpose of obtaining substantial m") Malingering in Pain Management Gerald M. Aronoff, M.D. Medical Director, Carolina Pain Associates, Charlotte, NC, USA General Principles Treating physician vs IME physician Subjective history is not fact
Malingering in Pain Management Gerald M. Aronoff, M.D. Medical Director, Carolina Pain Associates, Charlotte, NC, USA General Principles Treating physician vs IME physician Subjective history is not fact
Brain-based disorders in children, teens, and young adults: When to know there is a problem and what to do
 Brain-based disorders in children, teens, and young adults: When to know there is a problem and what to do Timothy A. Fratto, Ph.D. Neuropsychology Associates of Fairfax What is Neuropsychology? The study
Brain-based disorders in children, teens, and young adults: When to know there is a problem and what to do Timothy A. Fratto, Ph.D. Neuropsychology Associates of Fairfax What is Neuropsychology? The study
Mild Traumatic Brain Injury in Sports, Daily Life, and Military Service
 Mild Traumatic Brain Injury in Sports, Daily Life, and Military Service Grant L. Iverson, Ph.D. Professor, Department of Physical Medicine and Rehabilitation, Harvard Medical School; Director, MassGeneral
Mild Traumatic Brain Injury in Sports, Daily Life, and Military Service Grant L. Iverson, Ph.D. Professor, Department of Physical Medicine and Rehabilitation, Harvard Medical School; Director, MassGeneral
Pediatric Traumatic Brain Injury. Seth Warschausky, PhD Department of Physical Medicine and Rehabilitation University of Michigan
 Pediatric Traumatic Brain Injury Seth Warschausky, PhD Department of Physical Medicine and Rehabilitation University of Michigan Modules Module 1: Overview Module 2: Cognitive and Academic Needs Module
Pediatric Traumatic Brain Injury Seth Warschausky, PhD Department of Physical Medicine and Rehabilitation University of Michigan Modules Module 1: Overview Module 2: Cognitive and Academic Needs Module
Dr. Paul Comper. Toronto Rehabilitation Institute. with PIA LAW
 with PIA LAW and Toronto ABI Network Dr. Paul Comper Toronto Rehabilitation Institute Dr. Paul Comper is a clinical neuropsychologist at the Toronto Rehabilitation Institute University Health Network,
with PIA LAW and Toronto ABI Network Dr. Paul Comper Toronto Rehabilitation Institute Dr. Paul Comper is a clinical neuropsychologist at the Toronto Rehabilitation Institute University Health Network,
Optimizing Concussion Recovery: The Role of Education and Expectancy Effects
 Rehabilitation Institute of Michigan Optimizing Concussion Recovery: The Role of Education and Expectancy Effects Robin Hanks, Ph.D., ABPP Chief of Rehabilitation Psychology and Neuropsychology Professor
Rehabilitation Institute of Michigan Optimizing Concussion Recovery: The Role of Education and Expectancy Effects Robin Hanks, Ph.D., ABPP Chief of Rehabilitation Psychology and Neuropsychology Professor
What s Wrong With My Client: Understanding Psychological Testing in Order to Work Effectively With Your Expert
 What s Wrong With My Client: Understanding Psychological Testing in Order to Work Effectively With Your Expert Common Standardized, Norm Referenced Psychological Tests: Diagnostic ( Personality ) Tests:
What s Wrong With My Client: Understanding Psychological Testing in Order to Work Effectively With Your Expert Common Standardized, Norm Referenced Psychological Tests: Diagnostic ( Personality ) Tests:
Health Psychology and Medical Communication. 1.Health Psychology: a domain of interference between Medicine and Psychosocial Sciences
 Health Psychology and Medical Communication 1.Health Psychology: a domain of interference between Medicine and Psychosocial Sciences 1 Fields of Medical Psychology Health Psychology Psychological mechanisms
Health Psychology and Medical Communication 1.Health Psychology: a domain of interference between Medicine and Psychosocial Sciences 1 Fields of Medical Psychology Health Psychology Psychological mechanisms
Mild Traumatic Brain Injury (mtbi): An Occupational Dilemma
: An Occupational Dilemma") Mild Traumatic Brain Injury (mtbi): An Occupational Dilemma William H. Cann, MD MPH Occupational Medicine Trainee Occupational Medicine Trainee University of Washington Disclosures None This presentation
Mild Traumatic Brain Injury (mtbi): An Occupational Dilemma William H. Cann, MD MPH Occupational Medicine Trainee Occupational Medicine Trainee University of Washington Disclosures None This presentation
02/07/2016. Relationship Status Never Married. Race White
 Profile Report PATIENT INFORMATION Patient Identification Number: 12345 Patient Name (Optional) Gender Male Age 55 Pain Diagnostic Category Back Injury Date of Injury (Optional) 11/15/2011 Test Date 02/07/2016
Profile Report PATIENT INFORMATION Patient Identification Number: 12345 Patient Name (Optional) Gender Male Age 55 Pain Diagnostic Category Back Injury Date of Injury (Optional) 11/15/2011 Test Date 02/07/2016
GEPIC. An Introduction to Guide for the Evaluation of Psychiatric Impairment for Clinicians. Dr Michael Duke Senior Forensic Psychiatrist
 GEPIC An Introduction to Guide for the Evaluation of Psychiatric Impairment for Clinicians Dr Michael Duke Senior Forensic Psychiatrist What is psychiatric impairment? A psychiatric impairment is any loss
GEPIC An Introduction to Guide for the Evaluation of Psychiatric Impairment for Clinicians Dr Michael Duke Senior Forensic Psychiatrist What is psychiatric impairment? A psychiatric impairment is any loss
Chapter 5 - Somatic Symptom, Dissociative, and Factitious Disorders
 Chapter 5 - Somatic Symptom, Dissociative, and Factitious Disorders SOMATIC SYMPTOM AND RELATED DISORDERS -Physical symptoms (eg. pain) or concerns about an illness cannot be explained by a medical or
Chapter 5 - Somatic Symptom, Dissociative, and Factitious Disorders SOMATIC SYMPTOM AND RELATED DISORDERS -Physical symptoms (eg. pain) or concerns about an illness cannot be explained by a medical or
Outline. Dr. Robert G. Kaplan Kaplan Consulting & Counseling, Inc.
 Dr. Robert G. Kaplan Kaplan Consulting & Counseling, Inc. 3401 Enterprise Pkwy., Ste. 340 Beachwood, Ohio 44122-7340 Call: 216-766-5743 Fax: 217-937-0187 Email: RKaplan@KaplanCC.com Internet: WWW.KaplanCC.com
Dr. Robert G. Kaplan Kaplan Consulting & Counseling, Inc. 3401 Enterprise Pkwy., Ste. 340 Beachwood, Ohio 44122-7340 Call: 216-766-5743 Fax: 217-937-0187 Email: RKaplan@KaplanCC.com Internet: WWW.KaplanCC.com
Introduction To Mild TBI. Not Just Less Severe But Different
 Introduction To Mild TBI Not Just Less Severe But Different Purpose Provide a discussion of issues related to diagnostic criteria for mild brain injury and concussion To present incidence data on MTBI
Introduction To Mild TBI Not Just Less Severe But Different Purpose Provide a discussion of issues related to diagnostic criteria for mild brain injury and concussion To present incidence data on MTBI
The Neuropsychological Impairment Scale (NIS) Self-Report Form
 Self-Report Form") The Neuropsychological Impairment Scale (NIS) Self-Report Form A WPS TEST REPORT by William E O Donnell, PhD, MPH Copyright 1999 by Western Psychological Services wwwwpspublishcom Version 1110 ID Number:
The Neuropsychological Impairment Scale (NIS) Self-Report Form A WPS TEST REPORT by William E O Donnell, PhD, MPH Copyright 1999 by Western Psychological Services wwwwpspublishcom Version 1110 ID Number:
Many people are confused about what Social Security benefits might be available to them. Here are answers to frequently asked questions.
 Many people are confused about what Social Security benefits might be available to them. Here are answers to frequently asked questions. What is the difference between SSI and SSDI? SSDI or Social Security
Many people are confused about what Social Security benefits might be available to them. Here are answers to frequently asked questions. What is the difference between SSI and SSDI? SSDI or Social Security
Using Neuropsychological Experts. Elizabeth L. Leonard, PhD
 Using Neuropsychological Experts Elizabeth L. Leonard, PhD Prepared for Advocate. Arizona Association for Justice/Arizona Trial Lawyers Association. September, 2011 Neurocognitive Associates 9813 North
Using Neuropsychological Experts Elizabeth L. Leonard, PhD Prepared for Advocate. Arizona Association for Justice/Arizona Trial Lawyers Association. September, 2011 Neurocognitive Associates 9813 North
Prolonged Issues with Cognitive Function. Julie Miller, Psy.D., ABPP-CN Neuropsychologist Wallace-Kettering Neuroscience Institute
 Prolonged Issues with Cognitive Function Julie Miller, Psy.D., ABPP-CN Neuropsychologist Wallace-Kettering Neuroscience Institute Presentation Outline Basics of human brain development Vulnerability of
Prolonged Issues with Cognitive Function Julie Miller, Psy.D., ABPP-CN Neuropsychologist Wallace-Kettering Neuroscience Institute Presentation Outline Basics of human brain development Vulnerability of
Functional Assessment of Depression and Anxiety Disorders Relevant to Work Requirements
 Functional Assessment of Depression and Anxiety Disorders Relevant to Work Requirements Paul S. Appelbaum, MD Dollard Professor of Psychiatry, Medicine & Law Columbia University Overview Depression and
Functional Assessment of Depression and Anxiety Disorders Relevant to Work Requirements Paul S. Appelbaum, MD Dollard Professor of Psychiatry, Medicine & Law Columbia University Overview Depression and
PEDIATRIC SPORTS RELATED CONCUSSIONS
 Anna Mazur, PhD PEDIATRIC SPORTS RELATED CONCUSSIONS Disclosure No financial interests or funding 1 Presentation Outline Prevalence Predicting recovery: Post Traumatic Amnesia and Loss of Consciousness
Anna Mazur, PhD PEDIATRIC SPORTS RELATED CONCUSSIONS Disclosure No financial interests or funding 1 Presentation Outline Prevalence Predicting recovery: Post Traumatic Amnesia and Loss of Consciousness
Concussions and Mild Traumatic Brain Injury
 Concussions and Mild Traumatic Brain Injury Nancy Mann, MD, Paradigm Medical Director Fellow, American Academy of Physical Medicine and Rehabilitation Nancy Mann, MD Specializes in traumatic brain injury
Concussions and Mild Traumatic Brain Injury Nancy Mann, MD, Paradigm Medical Director Fellow, American Academy of Physical Medicine and Rehabilitation Nancy Mann, MD Specializes in traumatic brain injury
Psychosocial Impact of Concussions
 Psychosocial Impact of Concussions Tammy Miller, COTA/L, MHS, CBIS, CCM Jillian Jones, DPT, CBIS, CCI Definition A concussion is an injury that affects the way the brain works or functions. It is also
Psychosocial Impact of Concussions Tammy Miller, COTA/L, MHS, CBIS, CCM Jillian Jones, DPT, CBIS, CCI Definition A concussion is an injury that affects the way the brain works or functions. It is also
Lecture Outline Signs and symptoms in psychiatry Adjustment Disorders Other conditions that may be a focus of clinical attention
 V Codes & Adjustment Disorders Cornelia Pinnell, Ph.D. Argosy University/Phoenix Lecture Outline Signs and symptoms in psychiatry Adjustment Disorders Other conditions that may be a focus of clinical attention
V Codes & Adjustment Disorders Cornelia Pinnell, Ph.D. Argosy University/Phoenix Lecture Outline Signs and symptoms in psychiatry Adjustment Disorders Other conditions that may be a focus of clinical attention
Ronette Goodwin, Ph.D. Forensic and Psychological Experts, Inc Crenshaw Blvd. #179 Torrance, CA (866)
") Ronette Goodwin, Ph.D. Forensic and Psychological Experts, Inc. 2390 Crenshaw Blvd. #179 Torrance, CA. 90501 (866) 853-0056 goodwindoc@aol.com ACADEMIC BACKGROUND August 2001 Harbor UCLA Medical Center,
Ronette Goodwin, Ph.D. Forensic and Psychological Experts, Inc. 2390 Crenshaw Blvd. #179 Torrance, CA. 90501 (866) 853-0056 goodwindoc@aol.com ACADEMIC BACKGROUND August 2001 Harbor UCLA Medical Center,
Neuropsychological Sequale of Mild Traumatic Brain Injury. Professor Magdalena Mateo. Megan Healy
 Neuropsychological Sequale of Mild Traumatic Brain Injury Professor Magdalena Mateo Megan Healy Abstract: Studies have proven that mild traumatic brain injuries (MTBI), commonly known as concussions, can
Neuropsychological Sequale of Mild Traumatic Brain Injury Professor Magdalena Mateo Megan Healy Abstract: Studies have proven that mild traumatic brain injuries (MTBI), commonly known as concussions, can
Neuropsychological Testing (NPT)
") Neuropsychological Testing (NPT) POLICY Psychological testing (96101-03) refers to a series of tests used to evaluate and treat an individual with emotional, psychiatric, neuropsychiatric, personality
Neuropsychological Testing (NPT) POLICY Psychological testing (96101-03) refers to a series of tests used to evaluate and treat an individual with emotional, psychiatric, neuropsychiatric, personality
Manual. Manual. Report Manual. Battery for Health Improvement 2. Daniel Bruns, PsyD, & John Mark Disorbio, EdD
 Battery for Health Improvement 2 Daniel Bruns, PsyD, & John Mark Disorbio, EdD Battery for Health Improvement 2 Manual Medical Daniel Bruns, PsyD, Intervention & John Mark Disorbio, EdD Risk (MIR) Report
Battery for Health Improvement 2 Daniel Bruns, PsyD, & John Mark Disorbio, EdD Battery for Health Improvement 2 Manual Medical Daniel Bruns, PsyD, Intervention & John Mark Disorbio, EdD Risk (MIR) Report
New Criteria for Posttraumatic Stress Disorder in DSM-5: Implications for Causality
 New Criteria for Posttraumatic Stress Disorder in DSM-5: Implications for Causality Paul A. Arbisi, Ph.D. ABAP, ABPP. Staff Psychologist Minneapolis VA Medical Center Professor Departments of Psychiatry
New Criteria for Posttraumatic Stress Disorder in DSM-5: Implications for Causality Paul A. Arbisi, Ph.D. ABAP, ABPP. Staff Psychologist Minneapolis VA Medical Center Professor Departments of Psychiatry
Emotional Symptoms in Athletes With PCS. David Westerdahl, MD FAAFP Cleveland Clinic Florida 6/24/2012
 Emotional Symptoms in Athletes With PCS David Westerdahl, MD FAAFP Cleveland Clinic Florida 6/24/2012 Objectives Discuss Post-Concussion symptoms and functional problems Identify pre-injury factors that
Emotional Symptoms in Athletes With PCS David Westerdahl, MD FAAFP Cleveland Clinic Florida 6/24/2012 Objectives Discuss Post-Concussion symptoms and functional problems Identify pre-injury factors that
Disclosures. Objectives 2/15/2014. Wright, Concussion Assessment, Management and Return to Sports
 Concussion Assessment, Management and Return to Sports Wendy L. Wright, MS, APRN, FNP, FAANP Adult/Family Nurse Practitioner Owner Wright & Associates Family Healthcare Amherst Owner Wright & Associates
Concussion Assessment, Management and Return to Sports Wendy L. Wright, MS, APRN, FNP, FAANP Adult/Family Nurse Practitioner Owner Wright & Associates Family Healthcare Amherst Owner Wright & Associates
THE WETC PSYCHOLOGY NEWSLETTER
 Forty Tough Deposition Questions for Psych AME s & PQME s Forty Tough Deposition Questions for Psych AME s & PQME s THE WETC PSYCHOLOGY NEWSLETTER Dr. Bruce Leckart Westwood Evaluation & Treatment Center
Forty Tough Deposition Questions for Psych AME s & PQME s Forty Tough Deposition Questions for Psych AME s & PQME s THE WETC PSYCHOLOGY NEWSLETTER Dr. Bruce Leckart Westwood Evaluation & Treatment Center
Practical Neuropsychology for the NZ setting; from Assessment Planning to Formulation of Practical Recommendations. Dr Susan Shaw
 Practical Neuropsychology for the NZ setting; from Assessment Planning to Formulation of Practical Recommendations. Dr Susan Shaw Outline This workshop is based upon practical experience Includes what
Practical Neuropsychology for the NZ setting; from Assessment Planning to Formulation of Practical Recommendations. Dr Susan Shaw Outline This workshop is based upon practical experience Includes what
Interpretive Report. Client Information
 Interpretive Report Developed by Michelle R. Widows, PhD, Glenn P. Smith, PhD, and PAR Staff Client Information Client name: Sample Client Client ID: SIMS Test date: 08/12/2013 Date of birth: 02/03/1975
Interpretive Report Developed by Michelle R. Widows, PhD, Glenn P. Smith, PhD, and PAR Staff Client Information Client name: Sample Client Client ID: SIMS Test date: 08/12/2013 Date of birth: 02/03/1975
Neuropsychology of TBI & PTSD
 Neuropsychology of TBI & PTSD George S. Serna, Ph.D. Louis Stokes VA Medical Center TBI: The Signature Injury of the Iraq/Afghanistan War Veteran? 19% - 30% of OEF/OIF veterans reported some level of TBI
Neuropsychology of TBI & PTSD George S. Serna, Ph.D. Louis Stokes VA Medical Center TBI: The Signature Injury of the Iraq/Afghanistan War Veteran? 19% - 30% of OEF/OIF veterans reported some level of TBI
Somatization. Could the patient be suffering with a psychosomatic illness? Awesome article series read! Somatization. Somatization.
 What will you do and how will you feel when you have patients who repeatedly present with unexplained physical complaints that defy your best diagnostic and therapeutic efforts? Awesome article series
What will you do and how will you feel when you have patients who repeatedly present with unexplained physical complaints that defy your best diagnostic and therapeutic efforts? Awesome article series
Relevant Listings for Evaluating Traumatic Brain Injury at Step 3 of the Sequential Evaluation
 Relevant Listings for Evaluating Traumatic Brain Injury at Step 3 of the Sequential Evaluation I. Neurological Disorders Revised Medical Criteria for Evaluating Neurological Disorders went into effect
Relevant Listings for Evaluating Traumatic Brain Injury at Step 3 of the Sequential Evaluation I. Neurological Disorders Revised Medical Criteria for Evaluating Neurological Disorders went into effect
THE WETC PSYCHOLOGY NEWSLETTER
 THE WETC PSYCHOLOGY NEWSLETTER Dr. Bruce Leckart "Find the Truth, Tell the Story" Westwood Evaluation & Treatment Center 11340 Olympic Blvd., Suite 303, Los Angeles, CA 90064 310-444-3154, DrLeckartWETC@gmail.com,
THE WETC PSYCHOLOGY NEWSLETTER Dr. Bruce Leckart "Find the Truth, Tell the Story" Westwood Evaluation & Treatment Center 11340 Olympic Blvd., Suite 303, Los Angeles, CA 90064 310-444-3154, DrLeckartWETC@gmail.com,
Traumatic Brain Injury. By Laura Gomez, LCSW
 Traumatic Brain Injury By Laura Gomez, LCSW Objectives Briefly describe TBI, and its incidence, severity, and treatments Describe the VHA system of specialized TBI care for active duty and veterans Describe
Traumatic Brain Injury By Laura Gomez, LCSW Objectives Briefly describe TBI, and its incidence, severity, and treatments Describe the VHA system of specialized TBI care for active duty and veterans Describe
Award Number: W81XWH
 AD Award Number: W81XWH-08-2-0050 TITLE: PT073853: Mild TBI Following Exposure to Explosive Devices: Device Characteristics, Neuropsychological Functioning, and Symptoms of Post-Traumatic Stress Disorder
AD Award Number: W81XWH-08-2-0050 TITLE: PT073853: Mild TBI Following Exposure to Explosive Devices: Device Characteristics, Neuropsychological Functioning, and Symptoms of Post-Traumatic Stress Disorder
Commentary on Delis and Wetter, Cogniform disorder and cogniform condition: Proposed diagnoses for excessive cognitive symptoms
 Archives of Clinical Neuropsychology 22 (2007) 683 687 Abstract Commentary Commentary on Delis and Wetter, Cogniform disorder and cogniform condition: Proposed diagnoses for excessive cognitive symptoms
Archives of Clinical Neuropsychology 22 (2007) 683 687 Abstract Commentary Commentary on Delis and Wetter, Cogniform disorder and cogniform condition: Proposed diagnoses for excessive cognitive symptoms
Kristine Burkman, Ph.D. Staff Psychologist San Francisco VA Medical Center
 Kristine Burkman, Ph.D. Staff Psychologist San Francisco VA Medical Center ASAM Disclosure of Relevant Financial Relationships Content of Activity: ASAM Medical Scientific Conference 2013 Name Commercial
Kristine Burkman, Ph.D. Staff Psychologist San Francisco VA Medical Center ASAM Disclosure of Relevant Financial Relationships Content of Activity: ASAM Medical Scientific Conference 2013 Name Commercial
DBQ Initial Evaluation of Residuals of Traumatic Brain Injury (I-TBI) Disability
 Disability") DBQ Initial Evaluation of Residuals of Traumatic Brain Injury (I-TBI) Disability Name of patient/veteran: SSN: SECTION I 1. Diagnosis Does the Veteran now have or has he/she ever had a traumatic brain
DBQ Initial Evaluation of Residuals of Traumatic Brain Injury (I-TBI) Disability Name of patient/veteran: SSN: SECTION I 1. Diagnosis Does the Veteran now have or has he/she ever had a traumatic brain
insight. Psychological tests to help support your work with medical patients
 insight. Psychological tests to help support your work with medical patients C O M P R E H E N S I V E Shedding light on important issues Sometimes a closer view is all you need to find the answers you
insight. Psychological tests to help support your work with medical patients C O M P R E H E N S I V E Shedding light on important issues Sometimes a closer view is all you need to find the answers you
Biopsychosocial Characteristics of Somatoform Disorders
 Contemporary Psychiatric-Mental Health Nursing Chapter 19 Somatoform and Sleep Disorders Biopsychosocial Characteristics of Somatoform Disorders Unconscious transformation of emotions into physical symptoms
Contemporary Psychiatric-Mental Health Nursing Chapter 19 Somatoform and Sleep Disorders Biopsychosocial Characteristics of Somatoform Disorders Unconscious transformation of emotions into physical symptoms
Multiple Choice Questions
 Multiple Choice Questions Which one of these represents intrinsic motivation? (A) Trophies (B) Medals (C) Enjoyment of the activity (D) Money Which one of these represents extrinsic motivation? (A) High
Multiple Choice Questions Which one of these represents intrinsic motivation? (A) Trophies (B) Medals (C) Enjoyment of the activity (D) Money Which one of these represents extrinsic motivation? (A) High
The DSM-5 Draft: Critique and Recommendations
 The DSM-5 Draft: Critique and Recommendations Psychological Injury and Law ISSN 1938-971X Volume 3 Number 4 Psychol. Inj. and Law (2010) 3:320-322 DOI 10.1007/s12207-010-9091- y 1 23 Your article is protected
The DSM-5 Draft: Critique and Recommendations Psychological Injury and Law ISSN 1938-971X Volume 3 Number 4 Psychol. Inj. and Law (2010) 3:320-322 DOI 10.1007/s12207-010-9091- y 1 23 Your article is protected
Assessment: Interviews, Tests, Techniques. Clinical Psychology Lectures
 Lecture 6 Assessment: Interviews, Tests, Techniques Clinical Psychology Lectures Psychodiagnostic Assessment Also termed: personality assessment, diagnostic assessment, pretreatment assessments or psychological
Lecture 6 Assessment: Interviews, Tests, Techniques Clinical Psychology Lectures Psychodiagnostic Assessment Also termed: personality assessment, diagnostic assessment, pretreatment assessments or psychological
Review Evaluation of Residuals of Traumatic Brain Injury (R-TBI) Disability Benefits Questionnaire * Internal VA or DoD Use Only*
 Disability Benefits Questionnaire * Internal VA or DoD Use Only*") Review Evaluation of Residuals of Traumatic Brain Injury (R-TBI) Disability Benefits Questionnaire * Internal VA or DoD Use Only* Name of patient/veteran: SSN: Your patient is applying to the U. S. Department
Review Evaluation of Residuals of Traumatic Brain Injury (R-TBI) Disability Benefits Questionnaire * Internal VA or DoD Use Only* Name of patient/veteran: SSN: Your patient is applying to the U. S. Department
Mild TBI (Concussion) Not Just Less Severe But Different
 Not Just Less Severe But Different") Mild TBI (Concussion) Not Just Less Severe But Different Disclosures Funded research: 1. NIH: RO1 Physiology of concussion 2016-2021, Co-PI, $2,000,000 2. American Medical Society of Sports Medicine: RCT
Mild TBI (Concussion) Not Just Less Severe But Different Disclosures Funded research: 1. NIH: RO1 Physiology of concussion 2016-2021, Co-PI, $2,000,000 2. American Medical Society of Sports Medicine: RCT
The unexamined lie is a lie worth fibbing Neuropsychological malingering and the Word Memory Test
 Archives of Clinical Neuropsychology 17 (2002) 709 714 The unexamined lie is a lie worth fibbing Neuropsychological malingering and the Word Memory Test David E. Hartman Private Practice/Chicago Medical
Archives of Clinical Neuropsychology 17 (2002) 709 714 The unexamined lie is a lie worth fibbing Neuropsychological malingering and the Word Memory Test David E. Hartman Private Practice/Chicago Medical
Chapter Three BRIDGE TO THE PSYCHOPATHOLOGIES
 Chapter Three BRIDGE TO THE PSYCHOPATHOLOGIES Developmental Psychopathology: From Infancy through Adolescence, 5 th edition By Charles Wenar and Patricia Kerig When do behaviors or issues become pathologies?
Chapter Three BRIDGE TO THE PSYCHOPATHOLOGIES Developmental Psychopathology: From Infancy through Adolescence, 5 th edition By Charles Wenar and Patricia Kerig When do behaviors or issues become pathologies?
Other Disorders Myers for AP Module 69
 1 Other s Myers for AP Module 69 Describe the general characteristics of somatic symptom disorders. How does culture influence people s expression of physical complaints? Compare the symptoms of conversion
1 Other s Myers for AP Module 69 Describe the general characteristics of somatic symptom disorders. How does culture influence people s expression of physical complaints? Compare the symptoms of conversion
Dr. JoAnne Savoie, L.Psyc. Clinical Neuropsychologist Stan Cassidy Center for Rehabilitation Fredericton, NB. October 16, 2012
 Dr. JoAnne Savoie, L.Psyc. Clinical Neuropsychologist Stan Cassidy Center for Rehabilitation Fredericton, NB October 16, 2012 Risk factors for concussion Players at all levels are at risk 5-10% of athletes
Dr. JoAnne Savoie, L.Psyc. Clinical Neuropsychologist Stan Cassidy Center for Rehabilitation Fredericton, NB October 16, 2012 Risk factors for concussion Players at all levels are at risk 5-10% of athletes
The Albany Consistency Index for the Test of Memory Malingering
 Archives of Clinical Neuropsychology 27 (2012) 1 9 The Albany Consistency Index for the Test of Memory Malingering Jessica H. Gunner 1, *, Andrea S. Miele 1, Julie K. Lynch 2, Robert J. McCaffrey 1,2 1
Archives of Clinical Neuropsychology 27 (2012) 1 9 The Albany Consistency Index for the Test of Memory Malingering Jessica H. Gunner 1, *, Andrea S. Miele 1, Julie K. Lynch 2, Robert J. McCaffrey 1,2 1
A Comparison of Two BHI Measures of Faking
 Paper Presentation to the American Psychological Association 2000 National Convention A Comparison of Two BHI Measures of Faking Daniel Bruns, PsyD Health Psychology Associates Greeley, Colorado www.healthpsych.com
Paper Presentation to the American Psychological Association 2000 National Convention A Comparison of Two BHI Measures of Faking Daniel Bruns, PsyD Health Psychology Associates Greeley, Colorado www.healthpsych.com
PSYCHOTROPIC MEDICATION AND THE WORKPLACE. Dr. Marty Ewer 295 Fullarton Road Parkside
 PSYCHOTROPIC MEDICATION AND THE WORKPLACE Dr. Marty Ewer 295 Fullarton Road Parkside 5063 82999281 Introduction Depression and anxiety commonly occur in people who work. The World Health Organization has
PSYCHOTROPIC MEDICATION AND THE WORKPLACE Dr. Marty Ewer 295 Fullarton Road Parkside 5063 82999281 Introduction Depression and anxiety commonly occur in people who work. The World Health Organization has
BACKGROUND HISTORY QUESTIONNAIRE
 BACKGROUND HISTORY QUESTIONNAIRE Name: Sex M F Address: Home Number: Work Number: Cell Number: Email: SSN: Name and Address of Employer: Date of Birth: Age: Ethnicity: Referred By: Referral Question or
BACKGROUND HISTORY QUESTIONNAIRE Name: Sex M F Address: Home Number: Work Number: Cell Number: Email: SSN: Name and Address of Employer: Date of Birth: Age: Ethnicity: Referred By: Referral Question or
Outline. A brief history of concussion 4/25/2018. Understanding the Impact of Concussions: From Injury through Recovery
 Understanding the Impact of Concussions: From Injury through Recovery Luke C. Henry, PhD Clinical Neuropsychologist UPMC Department of Neurological Surgery 05.04.2018 Concussions Brief history Definition
Understanding the Impact of Concussions: From Injury through Recovery Luke C. Henry, PhD Clinical Neuropsychologist UPMC Department of Neurological Surgery 05.04.2018 Concussions Brief history Definition
Malingering in the Primary Care Setting. Jeremy Di Bari, DVM, MD M elissa Arthur, PhD
 Malingering in the Primary Care Setting Jeremy Di Bari, DVM, MD M elissa Arthur, PhD Simulation of Illness Both malingering and factitious disorder involve simulating an illness Malingering Illness falsification
Malingering in the Primary Care Setting Jeremy Di Bari, DVM, MD M elissa Arthur, PhD Simulation of Illness Both malingering and factitious disorder involve simulating an illness Malingering Illness falsification
Brain Concussion: A Stealth Injury. Christine Schulman, RN, MS, CNS, CCRN Trauma & Critical Care CNS Legacy Health, Portland, Oregon Director, AACN
 Brain Concussion: A Stealth Injury Christine Schulman, RN, MS, CNS, CCRN Trauma & Critical Care CNS Legacy Health, Portland, Oregon Director, AACN Legacy Emanuel Medical Center Portland, Oregon Disclosures
Brain Concussion: A Stealth Injury Christine Schulman, RN, MS, CNS, CCRN Trauma & Critical Care CNS Legacy Health, Portland, Oregon Director, AACN Legacy Emanuel Medical Center Portland, Oregon Disclosures
Changes, Challenges and Solutions: Overcoming Cognitive Deficits after TBI Sarah West, Ph.D. Hollee Stamper, LCSW, CBIS
 Changes, Challenges and Solutions: Overcoming Cognitive Deficits after TBI Sarah West, Ph.D. Hollee Stamper, LCSW, CBIS Learning Objectives 1. Be able to describe the characteristics of brain injury 2.
Changes, Challenges and Solutions: Overcoming Cognitive Deficits after TBI Sarah West, Ph.D. Hollee Stamper, LCSW, CBIS Learning Objectives 1. Be able to describe the characteristics of brain injury 2.
Background 6/24/2014. Validity Testing in Pediatric Populations. Michael Kirkwood, PhD, ABPP/CN. Conflict of Interest Statement
 Validity Testing in Pediatric Populations Michael Kirkwood, PhD, ABPP/CN Background Board Certified Clinical Neuropsychologist at Children s Hospital Colorado Exclusively pediatric-focused Patient work
Validity Testing in Pediatric Populations Michael Kirkwood, PhD, ABPP/CN Background Board Certified Clinical Neuropsychologist at Children s Hospital Colorado Exclusively pediatric-focused Patient work
Plan for Today. Brain Injury: 8/4/2017. Effective Services for People Living with Brain Injury. What is it & what causes it?
 Effective Services for People Living with Brain Injury Jean Capler, MSW, LSW Local Support Network Leader The Rehabilitation Hospital of Indiana Department of Resource Facilitation Plan for Today Brain
Effective Services for People Living with Brain Injury Jean Capler, MSW, LSW Local Support Network Leader The Rehabilitation Hospital of Indiana Department of Resource Facilitation Plan for Today Brain
1/22/2015. Contemporary Psychiatric-Mental Health Nursing Third Edition. Theories: Dissociative Disorders. Theories: Dissociative Disorders (cont'd)
") Contemporary Psychiatric-Mental Health Nursing Third Edition CHAPTER 19 Dissociative, Somatoform, and Factitious Disorders Theories: Dissociative Disorders Biological factors Serotonin Limbic system Physical
Contemporary Psychiatric-Mental Health Nursing Third Edition CHAPTER 19 Dissociative, Somatoform, and Factitious Disorders Theories: Dissociative Disorders Biological factors Serotonin Limbic system Physical
1. Injury Description
 ACUTE CONCUSSION EVALUATION (ACE) Physician/Clinician Office Version Gerard Gioia, PhD 1 & Micky Collins, PhD 2 1 Children's National Medical Center 2 University of Pittsburgh Medical Center Patient Name
ACUTE CONCUSSION EVALUATION (ACE) Physician/Clinician Office Version Gerard Gioia, PhD 1 & Micky Collins, PhD 2 1 Children's National Medical Center 2 University of Pittsburgh Medical Center Patient Name
Somatization,Somatoform disorders, and functional somatic syndromes: Prepared by Dr John Potokar Senior Lecturer Liaison Psychiatry UOB
 Somatization,Somatoform disorders, and functional somatic syndromes: Prepared by Dr John Potokar Senior Lecturer Liaison Psychiatry UOB Topic relevant to all clinical disciplines in medicine/surgery/primary
Somatization,Somatoform disorders, and functional somatic syndromes: Prepared by Dr John Potokar Senior Lecturer Liaison Psychiatry UOB Topic relevant to all clinical disciplines in medicine/surgery/primary
Scoring the BBHI 2 Standardized Treatment Risk Scores
 Scoring the BBHI 2 Standardized Treatment Risk Scores 2013 by Daniel Bruns, PsyD and John Mark Disorbio, EdD v 9 Patient Name: Date: Referring Physician: Proposed Treatment: Risk Score Findings Raw Score
Scoring the BBHI 2 Standardized Treatment Risk Scores 2013 by Daniel Bruns, PsyD and John Mark Disorbio, EdD v 9 Patient Name: Date: Referring Physician: Proposed Treatment: Risk Score Findings Raw Score
10/23/2018. What is a Concussion? Understand What is a concussion? Learn typical signs and symptoms and red flags
 Maria Chininis, Sports Medicine and Concussion Institute Understand What is a concussion? Learn typical signs and symptoms and red flags Understand trajectories that affect concussion recovery What is
Maria Chininis, Sports Medicine and Concussion Institute Understand What is a concussion? Learn typical signs and symptoms and red flags Understand trajectories that affect concussion recovery What is
A Healthy Brain. An Injured Brain
 A Healthy Brain Before we can understand what happens when a brain is injured, we must realize what a healthy brain is made of and what it does. The brain is enclosed inside the skull. The skull acts as
A Healthy Brain Before we can understand what happens when a brain is injured, we must realize what a healthy brain is made of and what it does. The brain is enclosed inside the skull. The skull acts as
Departmental Concussion Guidelines
 Concussion Plan Departmental Concussion Guidelines The following guidelines have been developed in accordance with Alabama A&M s Mission Statement and service goal of providing quality healthcare services
Concussion Plan Departmental Concussion Guidelines The following guidelines have been developed in accordance with Alabama A&M s Mission Statement and service goal of providing quality healthcare services
Screening and Assessment
 Screening and Assessment Screening and assessment are two different ways to obtain mental health and substance use information about youth. Screening is typically a brief procedure, performed by non-mental-health
Screening and Assessment Screening and assessment are two different ways to obtain mental health and substance use information about youth. Screening is typically a brief procedure, performed by non-mental-health
Demystifying the Neuropsychological Evaluation Report. Clinical Neuropsychologist 17 March 2017 Program Director, Neurobehavioral Program
 Demystifying the Neuropsychological Evaluation Report Jennifer R. Cromer, PhD BIAC Annual Conference Clinical Neuropsychologist 17 March 2017 Program Director, Neurobehavioral Program 84% of neuropsychologists
Demystifying the Neuropsychological Evaluation Report Jennifer R. Cromer, PhD BIAC Annual Conference Clinical Neuropsychologist 17 March 2017 Program Director, Neurobehavioral Program 84% of neuropsychologists
University of Notre Dame Sports Medicine Department Intercollegiate Athletics Concussion Management Plan
 ! Purpose: University of Notre Dame Sports Medicine Department Intercollegiate Athletics Concussion Management Plan Head injuries can pose a significant health risk for student-athletes competing in intercollegiate
! Purpose: University of Notre Dame Sports Medicine Department Intercollegiate Athletics Concussion Management Plan Head injuries can pose a significant health risk for student-athletes competing in intercollegiate
Evaluation of PTSD with Dissociative or Recovered Memory Clients and Plaintiffs
 Evaluation of PTSD with Dissociative or Recovered Memory Clients and Plaintiffs Constance J Dalenberg, Ph.D. Alliant International University Aall Why should the evaluation be different than for PTSD in
Evaluation of PTSD with Dissociative or Recovered Memory Clients and Plaintiffs Constance J Dalenberg, Ph.D. Alliant International University Aall Why should the evaluation be different than for PTSD in
G. FUNCTIONAL MEMORY AND COGNITION ASSESSMENT 100
 G. FUNCTIONAL MEMORY AND COGNITION ASSESSMENT 100 1. Check if any of the following exist: 1000 Learning disability 105 Communication, sensory or motor disabilities 110 Diagnosed Traumatic Brain Injury
G. FUNCTIONAL MEMORY AND COGNITION ASSESSMENT 100 1. Check if any of the following exist: 1000 Learning disability 105 Communication, sensory or motor disabilities 110 Diagnosed Traumatic Brain Injury
Copyright 2009 ACNN 1
 1 The focus of this information is children who have previously been evaluated and have an established diagnosis of concussion. The information contained herein is not intended for acute concussion management.
1 The focus of this information is children who have previously been evaluated and have an established diagnosis of concussion. The information contained herein is not intended for acute concussion management.
Creating and Maintaining a Safe and Comfortable Home
 Creating and Maintaining a Safe and Comfortable Home Crisis Prevention and Management Training for Limited Mental Health Assisted Living Facility Staff Program Manager and Trainer MARGO FLEISHER Acknowledgements
Creating and Maintaining a Safe and Comfortable Home Crisis Prevention and Management Training for Limited Mental Health Assisted Living Facility Staff Program Manager and Trainer MARGO FLEISHER Acknowledgements
Language After Traumatic Brain Injury
 Chapter 7 Language After Traumatic Brain Injury 10/24/05 COMD 326, Chpt. 7 1 1 10/24/05 COMD 326, Chpt. 7 2 http://www.californiaspinalinjurylawyer.com/images/tbi.jpg 2 TBI http://www.conleygriggs.com/traumatic_brain_injury.shtml
Chapter 7 Language After Traumatic Brain Injury 10/24/05 COMD 326, Chpt. 7 1 1 10/24/05 COMD 326, Chpt. 7 2 http://www.californiaspinalinjurylawyer.com/images/tbi.jpg 2 TBI http://www.conleygriggs.com/traumatic_brain_injury.shtml
Kendra L. Bryant, Ph.D., ABPP- Clinical Neuropsychology EDUCATION Northeastern University Boston College Wellesley College:
 Kendra L. Bryant, Ph.D., ABPP- Clinical Neuropsychology Board Certified by the American Board of Professional Psychology in Clinical Neuropsychology Licensed Psychologist: State of Maine (#PS1009) Neuropsychology
Kendra L. Bryant, Ph.D., ABPP- Clinical Neuropsychology Board Certified by the American Board of Professional Psychology in Clinical Neuropsychology Licensed Psychologist: State of Maine (#PS1009) Neuropsychology
Psychological Disorders: More Than Everyday Problems 14 /
 Psychological Disorders: More Than Everyday Problems 14 / Psychological Disorder(p.630) The presence of a constellation of symptoms that create significant distress; impair work, school, family, relationships,
Psychological Disorders: More Than Everyday Problems 14 / Psychological Disorder(p.630) The presence of a constellation of symptoms that create significant distress; impair work, school, family, relationships,
The ABCs of Dementia Diagnosis
 The ABCs of Dementia Diagnosis Dr. Robin Heinrichs, Ph.D., ABPP Board Certified Clinical Neuropsychologist Associate Professor, Psychiatry & Behavioral Sciences Director of Neuropsychology Training What
The ABCs of Dementia Diagnosis Dr. Robin Heinrichs, Ph.D., ABPP Board Certified Clinical Neuropsychologist Associate Professor, Psychiatry & Behavioral Sciences Director of Neuropsychology Training What
PTSD and TBI. Rita Wood, Psy.D. Assistant Chief of VA Police Aaron Yoder
 PTSD and TBI Rita Wood, Psy.D. Assistant Chief of VA Police Aaron Yoder Outline Prevalence of Post Traumatic Stress Disorder What is a traumatic event? Acute Stress Disorder (ASD) Risk Factors for PTSD
PTSD and TBI Rita Wood, Psy.D. Assistant Chief of VA Police Aaron Yoder Outline Prevalence of Post Traumatic Stress Disorder What is a traumatic event? Acute Stress Disorder (ASD) Risk Factors for PTSD
WakeMed Health & Hospitals
 WakeMed Health & Hospitals The Power to Heal. A Passion for Care. WakeMed Health & Hospitals Raleigh, North Carolina Traumatic Brain Injury December 4th, 2012 Laurie Leach, Ph.D., FACPN Director of Neuropsychology
WakeMed Health & Hospitals The Power to Heal. A Passion for Care. WakeMed Health & Hospitals Raleigh, North Carolina Traumatic Brain Injury December 4th, 2012 Laurie Leach, Ph.D., FACPN Director of Neuropsychology
Handling Challenges & Changes after TBI
 Handling Challenges & Changes after TBI Quick Facts about Traumatic Brain Injury (TBI) The CDC reports that roughly 2.5 million Americans have a TBI each year The most common causes are: falls, motor vehicle
Handling Challenges & Changes after TBI Quick Facts about Traumatic Brain Injury (TBI) The CDC reports that roughly 2.5 million Americans have a TBI each year The most common causes are: falls, motor vehicle
IT S ALL IN YOUR HEAD!
 IT S ALL IN YOUR HEAD! CARING FOR CONCUSSIONS IN YOUR COMMUNITY Stephen K Stacey, DO CPT, MC, USA OUTLINE Definition Epidemiology Diagnosis Evaluation Recovery Sequelae Prevention Resources for providers
IT S ALL IN YOUR HEAD! CARING FOR CONCUSSIONS IN YOUR COMMUNITY Stephen K Stacey, DO CPT, MC, USA OUTLINE Definition Epidemiology Diagnosis Evaluation Recovery Sequelae Prevention Resources for providers
Neuropsychological Testing in Occupational Medicine
 Neuropsychological Testing in Occupational Medicine When is a referral appropriate and what will neuropsychological testing offer? Nancy Fiedler, Ph.D. Rutgers, The State University of New Jersey Objectives
Neuropsychological Testing in Occupational Medicine When is a referral appropriate and what will neuropsychological testing offer? Nancy Fiedler, Ph.D. Rutgers, The State University of New Jersey Objectives
Guideline for Concussion/Mild Traumatic Brain Injury and Persistent Symptoms. Patient Version
 Guideline for Concussion/Mild Traumatic Brain Injury and Persistent Symptoms 3 rd Edition - for adults, +18 years of age Patient Version This guideline has been created to help with management of concussion/mild
Guideline for Concussion/Mild Traumatic Brain Injury and Persistent Symptoms 3 rd Edition - for adults, +18 years of age Patient Version This guideline has been created to help with management of concussion/mild
The Role of Psychological Factors in Muscle Tension Dysphonia
 The Role of Psychological Factors in Muscle Tension Dysphonia Sheri L. Goldstrohm, Ph.D. University of Pittsburgh Medial Center Background To speak, one requires an organic apparatus capable of producing
The Role of Psychological Factors in Muscle Tension Dysphonia Sheri L. Goldstrohm, Ph.D. University of Pittsburgh Medial Center Background To speak, one requires an organic apparatus capable of producing
11/21/2007. Introduction to Psychological and Psychiatric Disorders. James M. Rice, RhD, CLCP Medical Psychology Associates, PC
 Introduction to Psychological and Psychiatric Disorders James M. Rice, RhD, CLCP Medical Psychology Associates, PC Goals of this lecture/presentation To discuss, review, and understand the DSM IV multiaxial
Introduction to Psychological and Psychiatric Disorders James M. Rice, RhD, CLCP Medical Psychology Associates, PC Goals of this lecture/presentation To discuss, review, and understand the DSM IV multiaxial
Lost in Psychiatry: Addressing Brain Injury in a Psychiatric Hospital Population
 Lost in Psychiatry: Addressing Brain Injury in a Psychiatric Hospital Population Ron Broughton, M.Ed., L.P.C. Chief Clinical Officer Brookhaven Hospital Tulsa, Oklahoma Objectives 1. Learn methods used
Lost in Psychiatry: Addressing Brain Injury in a Psychiatric Hospital Population Ron Broughton, M.Ed., L.P.C. Chief Clinical Officer Brookhaven Hospital Tulsa, Oklahoma Objectives 1. Learn methods used
Comparison of Male and Female Response Behaviour on Minnesota Multiphasic Personality Inventory-2
 Comparison of Male and Female Response Behaviour on Minnesota Multiphasic Personality Inventory-2 Dr. Hayfa Tayseer Elbokai & Dr. Aziz Ahmad Alrhamneh Special Education Dep., Al- Balqa' Applied University,
Comparison of Male and Female Response Behaviour on Minnesota Multiphasic Personality Inventory-2 Dr. Hayfa Tayseer Elbokai & Dr. Aziz Ahmad Alrhamneh Special Education Dep., Al- Balqa' Applied University,
Violent Ideation in Medical Patients in Four Insurance Systems
 Paper Presentation to the American Psychological Association 1998 National Convention Violent Ideation in Medical Patients in Four Insurance Systems by Daniel Bruns, PsyD Health Psychology Associates Greeley,
Paper Presentation to the American Psychological Association 1998 National Convention Violent Ideation in Medical Patients in Four Insurance Systems by Daniel Bruns, PsyD Health Psychology Associates Greeley,
Anxiety disorders part II
 Anxiety disorders part II OBSESSIVE-COMPULSIVE DISORDER obsession a recurrent and intrusive thought, feeling, idea, or sensation compulsion a conscious, standarized, recurring pattern of behavior, such
Anxiety disorders part II OBSESSIVE-COMPULSIVE DISORDER obsession a recurrent and intrusive thought, feeling, idea, or sensation compulsion a conscious, standarized, recurring pattern of behavior, such
Date of Onset is defined as the first day the claimant meets the definition of disability as defined in the Act and regulations.
 THESE ARE THE FORMS I USE THIS IS NOT LEGAL ADVICE AND INTENDED TO SUPPLEMENT YOUR PARTICULAR FACTUAL SITUATION ONLY It is crucial you educate yourself on the Social Security Regulations that define and
THESE ARE THE FORMS I USE THIS IS NOT LEGAL ADVICE AND INTENDED TO SUPPLEMENT YOUR PARTICULAR FACTUAL SITUATION ONLY It is crucial you educate yourself on the Social Security Regulations that define and