The "Inner vs. Outer Solutions" By David D. Burns, MD*
|
|
|
- Patrick Armstrong
- 6 years ago
- Views:
Transcription
1 Page 1 The "Inner vs. Outer Solutions" By David D. Burns, MD* When we are criticized by a patient, friend, or family member, or get negative feedback on during a role play, it s easy to feel anxious and spaced out, or ashamed or annoyed. We may get flooded with all kinds of negative emotions. This makes it far more difficult to respond skillfully, using the Five Secrets of Effective Communication. The Five Secrets represent the outward solution, because that s how you convert a failed relationship or conflict into a vastly improved, trusting relationship. But your own use of the Daily Mood Log will be the key to the inner solution. A colleague might tell you that you got a "B" or a "C" in a role-play, and that while you did certain things really nicely, you made some errors and there is room for improvement. For example, you may be told that you did not acknowledge the patient's anger during the role-play, or did not really grasp or disarm the essence of the patient's criticism, or did not use an "I Feel" statement. These are errors we all tend to make, and these would be some specific areas you can focus on if you want to improve your interpersonal skills. For example, you can practice the Five Secrets, one at a time, repeatedly, until you get really good at each one. If you aren t good at Feeling Empathy, you could do about ten Feeling Empathy responses in a row with the help of a colleague. This would take about ten minutes, and you d get pretty good at acknowledging anger and other negative feelings, if that was one of your blind spots. However, when you get negative feedback, you might get upset, thinking that you "failed," or you might tell yourself that you are no good, or that you SHOULD have done better, or that you will be judged or rejected by other group members. If you want to learn how to minimize those kinds of reactions, you can use the Daily Mood Log, starting with the Event and Emotions, just as you would use with a patient. Then you can record these Negative Thoughts (NTs) using short sentences. Number them and indicate how strongly you believe each one in the Percent Belief column. Then see if you can pinpoint some of the distortions in your thoughts. Here are a few examples of the kinds of distortions you may discover:
2 Page 2 The Ten Distortions that Make it Difficult to Use the Five Secrets of Effective Communication Effectively 1. All-or-Nothing Thinking. You tell yourself that if you re not awesome when using the Five Secrets, you ve failed completely. Shades of gray do not exist. This has also been called the fixed vs. growth model of learning. 2. Overgeneralization. You overgeneralize from some specific problem (such as needing to do more work on the Disarming Technique) to your entire "self," telling yourself that you re "a failure. You are beat up on your self, rather than focusing on the specific skill you need to learn and practice. 3. Mental Filter. You selectively focus on all your errors and shortcomings and overlook your strengths as well as what you are learning. 4. Discounting the Positive. You discount your own capacity to learn and grow through repeated practice. You may also discount the tremendous value of learning from your mistakes and failures. And you may discount your skills, thinking they don t count because you screwed up or made errors in a practice exercise, or during a therapy session with a patient or problematic interaction with a friend of loved one. 5. Jumping to Conclusions. You jump to conclusions not supported by facts. Fortune-Telling. You may predict endless failure and defeat, thinking you will never learn and or develop good therapy skills. You may also tell yourself that when you do a role-play you will blow it completely (Allor-Nothing Thinking, Fortune Telling) and look like a fool (Mind-Reading, Overgeneralization, Labeling, Fortune Telling.) During a conflict with a challenging patient or loved one, you tell yourself that he or she will never change. Then may feel hopeless, frustrated, or overwhelmed. Mind-Reading. You may be thinking that your colleagues and teachers are judging you, or looking down on you, or disliking you when you screw up in a role play exercise or if you ask a foolish question. 6. Magnification and Minimization. You may Magnify your errors, failures, or shortcomings, or Minimize your own strengths. 7. Should Statements. You use shoulds, shouldn ts, musts, ought tos, and have tos. Self-Directed Should Statements. You may be telling yourself, "I should be better at this, or I shouldn t have made that mistake again. Other-Directed Should Statements. You may be telling yourself that your patients or loved ones shouldn t be so unreasonable or critical, or that they should appreciate your efforts, or that they should be more motivated, or that they shouldn t insist on constant venting. 8. Labeling and Mislabeling. You may think of yourself or someone else as a loser, a failure, or inept or unlovable, or a bad father (or mother or teacher or therapist.) 9. Emotional Reasoning. You reason from how you feel to how you are. So if you feel inadequate, inferior, hopeless, or ashamed, so you may conclude that you really are inadequate, inferior, hopeless, or bad. Blame Self-Blame. You may use up your energy beating up on yourself instead of figuring out how to improve in the specific area where you are weak, or where you need to grow. Other Blame. You feel like a victim and tell yourself that the other person is entirely to blame for the problems in your relationship. You may tell yourself that people should be more tactful and respectful, or shouldn t think and feel the way they do. You may tell yourself that your patients, students or children shouldn t be so resistant, needy, lazy or argumentative and that they should take more initiative and should be more willing to work on solving their problems with the wonderful tools you are offering them.
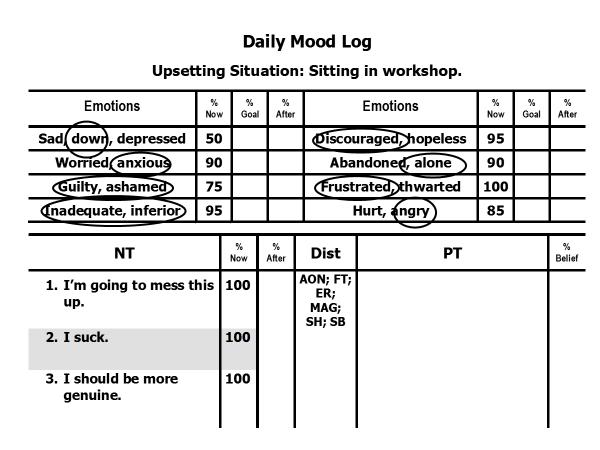
3 Page 3 Underneath those distorted thoughts you will frequently find a number of familiar Self- Defeating Beliefs, such as Perfectionism, the Approval or Achievement Addictions, or Entitlement or Submissiveness, to name just a few. Working on the inner solution gives you the chance to grow significantly when learning the Five Secrets. You may need to spend time on both the inner and outer solutions to do good clinical work, because if you are busy beating up on yourself and feeling anxious, ashamed, defensive, frustrated, or resentful, it makes it harder to respond to the other person with warmth, and harder to use any of the Five Secrets skillfully. Everything I have said is so obvious and basic that I may sound rather ridiculous in writing this. Still, I am convinced that the personal work is (the inner solution) is absolutely necessary if you hope to develop excellent Five Secrets skills, and it will make your learning more fun as well. The problem is almost never our failures, but rather the shame we feel because of our distorted thoughts about our failures. In fact, someone once said that your greatest therapeutic failures are actually your greatest successes in disguise. Do you grasp what that means? If not, ask in group. Once you ve pinpointed your own NTs and identified the distortions in them, you can take one of your NTs and put it in a Recovery Circle. Then you can select ten to fifteen or more techniques to challenge that thought. Of course, you will want to do your own Paradoxical Agenda Setting first. What do your negative thoughts and feelings show about you that is positive and awesome? And what are some advantages or benefits of your negative thoughts and feelings? Working on the Inner Solution can help you with the Outer solution, and may also show you how to help many of your patients who struggle with similar self-doubts. You can find an example of how to set up your Daily Mood Log on pages 5 and 6. This was a man who was upset during a workshop because he kept making errors when he was trying to learn the five Secrets. See if you can identify one or more cognitive distortions in each of his Negative Thoughts, and record them in the Distortions column using abbreviations, as I have done for his first Negative Thoughts. Then see if you can write down a Positive Thought (PT) for each NT that will have two characteristics: David 1. The PT is 100% true. 2. It drastically reduces the belief in the NT.
4 Page 4
5 Page 5
6 Common Five Secrets Therapist Errors Page 1 Common Five Secrets Therapist Errors By Jill Levitt PhD and David D. Burns, MD* This table will provide you with an understanding of errors that nearly all therapists make when first trying to learn the five Secrets of Effective Communication. Reading and studying this table with not improve your ability to use the Five Secrets. This can ONLY be achieved through frequent practice with feedback from colleagues. That s because most of these errors such as defensiveness when criticized seem to be hard-wired into our neurologic system. Many, or perhaps most, of these errors arise from the emotional responses of therapists to conflict or criticism or failure. These responses tend to cluster in two patterns. The first pattern is I m no good. This involves anxiety and shame, and results from intense self-criticism. The second patter is You re not good. These responses typically involve should statements and blame directed toward the patient. Overcoming these two patterns may require you to do your own work on a personal Daily Mood Log. You may need some help from your therapist, a trusted colleague, or your training group. There s an incredibly useful practice technique that will help you master the Five Secrets. In training exercises, we ve noticed that different therapists tend to have difficulty with one or another of the Five Secrets. For example, the hardest technique for me (DB) to master was the Disarming Technique, because I naturally tend to have an argumentative tendency. So it was difficult, at first, to see the truth in criticisms I thought were exaggerated or unfair or off-base. I ve seen therapists who ve had extreme difficulties with Thought Empathy, or Feeling Empathy, or I Feel Statements, or any of these techniques. As a first step, see if you can identify your blind spot when you practice with the Five Secrets. You may have trouble with more than one of the techniques, but you can focus on learning them one at a time. Let s say you notice that over and over again you tend to do poorly on Feeling Empathy. You can set up what I call the Zen Exercise, for lack of a better name. Get a copy of my Feeling Words Chart, and hold it in your hand. Then ask one or more colleagues to attack you, using only one or two sentences. For example, they might say, You re not helping me. This therapy is a waste of time! Your job is to respond ONLY with Feeling Empathy. You can use a formula such as, I can imagine you might be feeling X, Y, and Z, where X, Y, and Z are words you ve selected from the Feeling Words chart. For example, you might say something like this: Wow, I can imagine you might be feeling discouraged, disappointed, frustrated, and perhaps even a bit angry with me. It will probably sound artificial, because you re only allowed to use ONE technique. Ask your colleagues if you got it right and did a good job. If you didn t, ask them what you missed and try again. If you did a good job, ask them to attack you again and again. After ten or fifteen iterations, you ll be really good at the technique that you found the most difficult! It only takes about ten minutes or so. Learning to use the Five Secrets requires lots of hard work and practice. The good news is that the process of learning and overcoming your own defensiveness can transform not only your clinical work with patients, but also your personal and professional relationships as well. Another fun way to integrate five secrets practice into your life is to pick one day of the week and designate it the day for the Disarming Technique, or I Feel Statements or whichever secret you need to work on. If Monday is disarming day, try to disarm anything that comes your way. You can disarm people in the grocery store, or your family members, or your patients, or the person who cuts you off in traffic (e.g., You re right, I WAS driving kind of slowly, and you re in a hurry! ) Copyright 2015 by Jill Levitt PhD and David D. Burns, MD
7 Common Five Secrets Therapist Errors Page 2 Technique Common Therapist Errors When Trying To Use this Technique Emotional Barriers to Using this Technique Skillfully The Disarming Technique Thought Empathy Feeling Empathy You can t see the truth in what patient is saying because you want to be right, or because you ve been trained to see the patient s criticism as transference or a distortion based on his or her diagnosis. You don t disarm at all (skipping this step) but instead, simply paraphrase what the patient is saying. You use disarming in words only, saying something patronizing, like I can see why you might feel that way. This is a subtle putdown that implies that the patient is wrong. You use the Disarming Technique in a half-hearted way, without seeing the full truth in what the patient is saying. Skillful disarming is usually emphatic, saying things like: "you are absolutely right," or "this makes a lot of sense", or "I have to agree with you on this." You tend to leave out the most important parts of what the patient is saying because you didn t jot the patient s comments down, or because you want the most threatening comments to go away. When you paraphrase the patient s words, you put your own spin on them, instead of using the patient s exact words. You add more on, or make an interpretation, based on your training or school of therapy. You may do this because you want to appear smart, or because you think you re enhancing what the patient says when, in fact, your interpretation is off-base. You paraphrase in a robotic, formulaic way, without I Feel Statements, so your response sounds like a gimmick or a formula. You forget to acknowledge the patient s anger, especially his or her anger with you. This error is almost universal and almost impossible to overcome without considerable determination and practice. Pride / shame--we want to avoid the death of the ego. Defensiveness--Our professional identity may be threatened by the patient s criticism, which implies we are not competent, or sufficiently caring, etc. Fear we think that something bad will happen (escalation, lawsuit, gossip) if we agree with a patient who is angry and critical of us. Anger we label the patient as the enemy, or bad, or unfair, or irrational, and want to get back at him or her. Competition we are afraid we ll seem unprofessional or weak if we give in. Power you feel you must put limits on your patient s criticisms, or counter them, or else you ll reinforce the patient s negative behaviors and the aggressive statements will spiral out of control. Anxiety you feel so anxious and panicky when the patient criticizes you that you concentrate on what you re going to say next. As a result, by the time the patient finishes, you have almost no idea what he or she said, and respond at right angles. This irritates the patient because it s clear you weren t listening, and the problem escalates. Emotophobia this is the fear of negative emotions in general. Conflict Phobia / Anger Phobia this is the fear of anger and conflict. Copyright 2015 by Jill Levitt PhD and David D. Burns, MD
8 Common Five Secrets Therapist Errors Page 3 Inquiry I Feel Statements You say "you must be feeling X, Y, and Z" instead of saying, "I wonder if you might be feeling X, Y, and Z" This sounds like an accusation and may put the patient on the defensive. In addition, you may not be reading the patient s emotions correctly. You minimize the patient s emotions. For example, you might say, "you seem a little bit irritated at person X" instead of "it sounds like you might be feeling furious with person X." But this has to be balanced with the next consideration. You accuse the patient of being angry ( You re clear angry with me ), instead of softening the anger and making it acceptable, as in: Given what you just said, I wouldn t be a bit surprised if you re feeling a bit annoyed or even angry with me, and for good reason. Can you tell me more about how you are feeling? In this case, the four softeners make it easier for the patient to own up to the anger: 1. if you re feeling; 2. a bit; 3. annoyed or even angry: 4. and for good reason. You forget to acknowledge the tender feelings (such as feeling hurt, lonely, sad, lonely, rejected, put down, and so forth) that are nearly always associated with harsh, negative feelings such as anger. You ask questions that lead to problem-solving or helping. For example, you might say, How can I help you more? This is not inquiry, because the patient is not your supervisor and does not know what you should be doing differently. Asking how you could do better is also a form of therapist conflict phobia, because you re trying to make nice, rather than asking about the patient s negative and potentially upsetting feelings about you. Inquiry is encouraging patients to tell you more about how they think and feel, as well as the problems you re not helping them with. You don t express your feelings. Instead, you make a comment about the patient that begins with I feel that you... Examples might be, "I feel that you re not listening, or I feel like you re There are, in general, only two types of feelings that therapists cannot deal with: your own feelings and your patients feelings. However, few therapists are aware of this, and wrongly believe they are good at dealing with feelings. For more information, see the emotional barriers to I Feel Statements below. Codependency you cannot resist the compulsive need to jump in and help. Conflict Phobia / Anger Phobia you are afraid of the patient s negative feelings, so you want to divert the conversation to something that is nicer and more positive. Anxiety you feel threatened by the patient s criticisms because they trigger your own self-criticisms and feelings of inadequacy. You avoid talking about your negative feelings because you ve been trained never to reveal your feelings to your patients. Copyright 2015 by Jill Levitt PhD and David D. Burns, MD
9 Common Five Secrets Therapist Errors Page 4 Stroking wrong. These You Statements involve blaming or criticizing the patient instead of expressing your feelings. You express your feelings in an overly dramatic or self-effacing way that makes the patient feel pity for you. For example, you might say, "Yes, my wife also accuses me of not listening, and she just filed for divorce. I hear this from my other patients, too. In fact, most of them have dropped out of therapy. PLEASE don t leave me! Your comment does not sound genuine. For example, after a severe criticism, you may say, Oh, I m so happy you shared that with me, when in fact you re not feeling at all happy. You re actually feeling defensive, annoyed, anxious, frustrated, and on the spot! Your attempt at a compliment sounds formulaic: "Good for you for coming in here today!" Your comment sounds phony and self-serving: Or I m so glad you told me the therapy has been a waste of time. You re becoming more assertive, just as I ve been teaching you to do. Your comment is non-specific: You are a great person or you are a wonderful patient. This compliment is more specific: I admire how thoughtful you are of your family members, and how hard you work to keep them happy. Your comment does not sound genuine: It was very brave of you to tell me that my comments often sound phony (when it did not take courage at all, and you still sound phony!) You avoid talking about your negative feelings because you ve made the subconscious and automatic judgment that you shouldn t be feeling the way you do. In other words, you think you shouldn t be feeling angry, or anxious, or ashamed. You are convinced that these feelings are inappropriate, or unprofessional, or wrong. You may also be convinced that others would judge you if they knew you felt this way. This emotional censoring happens so quickly and automatically that most therapists simply don t notice they re hiding and suppressing their feelings. Anger / frustration. When you get angry with anyone, including a patient, there s a tendency to think about that person in a globally negative way, so you can t think of anything positive to say about him or her. Love / hate dichotomy. Most humans, including most therapists, act as if there was an all-or-nothing split between positive vs. negative emotions. So if you re angry with someone, it means you can t simultaneously have positive feelings for that person. Defensiveness. You feel hurt by the patient s comments and feel an overwhelming urge to defend yourself. Copyright 2015 by Jill Levitt PhD and David D. Burns, MD
Helping Your Asperger s Adult-Child to Eliminate Thinking Errors
 Helping Your Asperger s Adult-Child to Eliminate Thinking Errors Many people with Asperger s (AS) and High-Functioning Autism (HFA) experience thinking errors, largely due to a phenomenon called mind-blindness.
Helping Your Asperger s Adult-Child to Eliminate Thinking Errors Many people with Asperger s (AS) and High-Functioning Autism (HFA) experience thinking errors, largely due to a phenomenon called mind-blindness.
15 Common Cognitive Distortions
 15 Common Cognitive Distortions By JOHN M. GROHOL, PSY.D. July 2, 2009 http://psychcentral.com/lib/2009/15-common-cognitive-distortions/ What s a cognitive distortion and why do so many people have them?
15 Common Cognitive Distortions By JOHN M. GROHOL, PSY.D. July 2, 2009 http://psychcentral.com/lib/2009/15-common-cognitive-distortions/ What s a cognitive distortion and why do so many people have them?
When Panic Attacks / Burns Evolution of Psychotherapy / 12/15/17
 When Panic Attacks High-Speed, Drug-Free Treatment with TEAM-CBT David D. Burns, M.D. Emeritus Adjunct Clinical Professor of Psychiatry and Behavioral Sciences, Stanford Medical School 1 Four Powerful
When Panic Attacks High-Speed, Drug-Free Treatment with TEAM-CBT David D. Burns, M.D. Emeritus Adjunct Clinical Professor of Psychiatry and Behavioral Sciences, Stanford Medical School 1 Four Powerful
Overview of cognitive work in CBT
 Overview of cognitive work in CBT Underlying assumptions: Cognitive Behavioral Therapy How an individual interprets life events plays a role in determining how he or she responds to those events (Beck,
Overview of cognitive work in CBT Underlying assumptions: Cognitive Behavioral Therapy How an individual interprets life events plays a role in determining how he or she responds to those events (Beck,
Problem Situation Form for Parents
 Problem Situation Form for Parents Please complete a form for each situation you notice causes your child social anxiety. 1. WHAT WAS THE SITUATION? Please describe what happened. Provide enough information
Problem Situation Form for Parents Please complete a form for each situation you notice causes your child social anxiety. 1. WHAT WAS THE SITUATION? Please describe what happened. Provide enough information
The Therapist s Craft Advanced Empathy Training. TEAM Therapy. Empathy Training / Burns. Copyright 2013 by David Burns, M.D.
 The Therapist s Craft Advanced Empathy Training David D. Burns, M.D. Adjunct Clinical Professor of Psychiatry and Behavioral Sciences, Stanford Medical School 1 TEAM Therapy T = Testing E = Empathy A =
The Therapist s Craft Advanced Empathy Training David D. Burns, M.D. Adjunct Clinical Professor of Psychiatry and Behavioral Sciences, Stanford Medical School 1 TEAM Therapy T = Testing E = Empathy A =
The Therapist s Craft Overcoming Therapeutic Resistance. TEAM Therapy. Overcoming Resistance / Burns. Copyright 2013 by David Burns, M.D.
 The Therapist s Craft Overcoming Therapeutic Resistance David D. Burns, M.D. Adjunct Clinical Professor of Psychiatry and Behavioral Sciences, Stanford Medical School 1 TEAM Therapy T = Testing E = Empathy
The Therapist s Craft Overcoming Therapeutic Resistance David D. Burns, M.D. Adjunct Clinical Professor of Psychiatry and Behavioral Sciences, Stanford Medical School 1 TEAM Therapy T = Testing E = Empathy
COGNITIVE DISTORTIONS
 COGNITIVE DISTORTIONS Cognitive distortions are simply ways that Impostor Syndrome convinces us to believe things that aren t really true. These are inaccurate thought patterns that reinforce our negative
COGNITIVE DISTORTIONS Cognitive distortions are simply ways that Impostor Syndrome convinces us to believe things that aren t really true. These are inaccurate thought patterns that reinforce our negative
Chapter 1. Dysfunctional Behavioral Cycles
 Chapter 1. Dysfunctional Behavioral Cycles For most people, the things they do their behavior are predictable. We can pretty much guess what someone is going to do in a similar situation in the future
Chapter 1. Dysfunctional Behavioral Cycles For most people, the things they do their behavior are predictable. We can pretty much guess what someone is going to do in a similar situation in the future
Take new look emotions we see as negative may be our best friends (opposite to the script!)
") Tony Robbins - emotions Take new look emotions we see as negative may be our best friends (opposite to the script!) How do people deal? 1. They avoid them try not to feel them. a. Rejection 2. I ll endure
Tony Robbins - emotions Take new look emotions we see as negative may be our best friends (opposite to the script!) How do people deal? 1. They avoid them try not to feel them. a. Rejection 2. I ll endure
Step 2 Challenging negative thoughts "Weeding"
 Managing Automatic Negative Thoughts (ANTs) Step 1 Identifying negative thoughts "ANTs" Step 2 Challenging negative thoughts "Weeding" Step 3 Planting positive thoughts 'Potting" Step1 Identifying Your
Managing Automatic Negative Thoughts (ANTs) Step 1 Identifying negative thoughts "ANTs" Step 2 Challenging negative thoughts "Weeding" Step 3 Planting positive thoughts 'Potting" Step1 Identifying Your
From the scenario below please identify the situation, thoughts, and emotions/feelings.
 Introduction to Mental Gremlins: Example From the scenario below please identify the situation, thoughts, and emotions/feelings. Bob has been working for Big Corporation for 12 years and has his annual
Introduction to Mental Gremlins: Example From the scenario below please identify the situation, thoughts, and emotions/feelings. Bob has been working for Big Corporation for 12 years and has his annual
Look to see if they can focus on compassionate attention, compassionate thinking and compassionate behaviour. This is how the person brings their
 Compassionate Letter Writing Therapist Notes The idea behind compassionate mind letter writing is to help people engage with their problems with a focus on understanding and warmth. We want to try to bring
Compassionate Letter Writing Therapist Notes The idea behind compassionate mind letter writing is to help people engage with their problems with a focus on understanding and warmth. We want to try to bring
Assertive Communication
 Assertive Communication Listed below are some of the key features of the three main communication styles: Passive Aggressive Assertive Apologetic You statements I statements Overly soft or tentative voice
Assertive Communication Listed below are some of the key features of the three main communication styles: Passive Aggressive Assertive Apologetic You statements I statements Overly soft or tentative voice
Nonjudgmentally and Cognitive Therapy
 Nonjudgmentally and Cognitive Therapy See, but don t evaluate. Take a nonjudgmental stance. Just the facts. Focus on the what, not the good or bad, the terrible or wonderful, the should or should not.
Nonjudgmentally and Cognitive Therapy See, but don t evaluate. Take a nonjudgmental stance. Just the facts. Focus on the what, not the good or bad, the terrible or wonderful, the should or should not.
Why Is It That Men Can t Say What They Mean, Or Do What They Say? - An In Depth Explanation
 Why Is It That Men Can t Say What They Mean, Or Do What They Say? - An In Depth Explanation It s that moment where you feel as though a man sounds downright hypocritical, dishonest, inconsiderate, deceptive,
Why Is It That Men Can t Say What They Mean, Or Do What They Say? - An In Depth Explanation It s that moment where you feel as though a man sounds downright hypocritical, dishonest, inconsiderate, deceptive,
How to Help Your Patients Overcome Anxiety with Mindfulness
 How to Help Your Patients Overcome Anxiety with Mindfulness Video 5 - Transcript - pg. 1 How to Help Your Patients Overcome Anxiety with Mindfulness How to Work with the Roots of Anxiety with Ron Siegel,
How to Help Your Patients Overcome Anxiety with Mindfulness Video 5 - Transcript - pg. 1 How to Help Your Patients Overcome Anxiety with Mindfulness How to Work with the Roots of Anxiety with Ron Siegel,
Addressing What s Missing From Our Conversations about Resilience: The Role of Cognitive Biases
 Addressing What s Missing From Our Conversations about Resilience: The Role of Cognitive Biases April 7, 9:15-11:15 Association of Pediatric Program Directors (APPD) 2017 Alyssa Bogetz, MSW Albina Gogo,
Addressing What s Missing From Our Conversations about Resilience: The Role of Cognitive Biases April 7, 9:15-11:15 Association of Pediatric Program Directors (APPD) 2017 Alyssa Bogetz, MSW Albina Gogo,
MALE LIBIDO- EBOOKLET
 MALE LIBIDO- EBOOKLET Hi there, Thank you for ordering this Native Remedies ebooklet! ebooklets are modified from consultations with real people and cover some of the most frequently dealt with problems
MALE LIBIDO- EBOOKLET Hi there, Thank you for ordering this Native Remedies ebooklet! ebooklets are modified from consultations with real people and cover some of the most frequently dealt with problems
ADDITIONAL CASEWORK STRATEGIES
 ADDITIONAL CASEWORK STRATEGIES A. STRATEGIES TO EXPLORE MOTIVATION THE MIRACLE QUESTION The Miracle Question can be used to elicit clients goals and needs for his/her family. Asking this question begins
ADDITIONAL CASEWORK STRATEGIES A. STRATEGIES TO EXPLORE MOTIVATION THE MIRACLE QUESTION The Miracle Question can be used to elicit clients goals and needs for his/her family. Asking this question begins
The Cognitive Model Adapted from Cognitive Therapy by Judith S. Beck
 The Cognitive Model Adapted from Cognitive Therapy by Judith S. Beck Automatic Thoughts The Cognitive Model is based on the idea that our emotions and behaviors are influenced by our perceptions of events.
The Cognitive Model Adapted from Cognitive Therapy by Judith S. Beck Automatic Thoughts The Cognitive Model is based on the idea that our emotions and behaviors are influenced by our perceptions of events.
Overcoming Subconscious Resistances
 Overcoming Subconscious Resistances You ve previously learned that to become anxiety-free you want to overcome your subconscious resistance. This is important because as long as the subconscious mind the
Overcoming Subconscious Resistances You ve previously learned that to become anxiety-free you want to overcome your subconscious resistance. This is important because as long as the subconscious mind the
Section 4 - Dealing with Anxious Thinking
 Section 4 - Dealing with Anxious Thinking How do we challenge our unhelpful thoughts? Anxiety may decrease if we closely examine how realistic and true our unhelpful/negative thoughts are. We may find
Section 4 - Dealing with Anxious Thinking How do we challenge our unhelpful thoughts? Anxiety may decrease if we closely examine how realistic and true our unhelpful/negative thoughts are. We may find
Difficult Conversations
 Difficult Conversations Corban Sanchez Academic Advisor NACADA Conference 2011 Douglas Stone, Bruce Patton, and Sheila Heen of the Harvard Negotiation Project Moving Toward a Learning Conversation Normal
Difficult Conversations Corban Sanchez Academic Advisor NACADA Conference 2011 Douglas Stone, Bruce Patton, and Sheila Heen of the Harvard Negotiation Project Moving Toward a Learning Conversation Normal
Managing Your Emotions
 Managing Your Emotions I love to ask What s your story? (pause) You immediately had an answer to that question, right? HOW you responded in your mind is very telling. What I want to talk about in this
Managing Your Emotions I love to ask What s your story? (pause) You immediately had an answer to that question, right? HOW you responded in your mind is very telling. What I want to talk about in this
Building Emotional Self-Awareness
 Building Emotional Self-Awareness Definition Notes Emotional Self-Awareness is the ability to recognize and accurately label your own feelings. Emotions express themselves through three channels physically,
Building Emotional Self-Awareness Definition Notes Emotional Self-Awareness is the ability to recognize and accurately label your own feelings. Emotions express themselves through three channels physically,
Understanding Emotional TRIGGER. What are triggers?
 What are triggers? We all have emotional triggers. Perhaps someone makes an off-hand comment about how you look, your new project at work, how you seem a little tired lately, or a comment about someone
What are triggers? We all have emotional triggers. Perhaps someone makes an off-hand comment about how you look, your new project at work, how you seem a little tired lately, or a comment about someone
Culminating Portfolio Readings Mind over Mood - Getting Psyched for Learning 1. Section 1 - Getting Psyched for Learning
 Culminating Portfolio Readings Mind over Mood - Getting Psyched for Learning 1 Section 1 - Getting Psyched for Learning This section will show us strategies, methods, and skills that have been shown to
Culminating Portfolio Readings Mind over Mood - Getting Psyched for Learning 1 Section 1 - Getting Psyched for Learning This section will show us strategies, methods, and skills that have been shown to
STAR-CENTER PUBLICATIONS. Services for Teens at Risk
 STAR-CENTER PUBLICATIONS Services for Teens at Risk Teen Handbook on Depression Services for Teens at Risk (STAR-Center) Western Psychiatric Institute and Clinic (412)864-3346 All Rights Reserved - 2018
STAR-CENTER PUBLICATIONS Services for Teens at Risk Teen Handbook on Depression Services for Teens at Risk (STAR-Center) Western Psychiatric Institute and Clinic (412)864-3346 All Rights Reserved - 2018
Functional Analytic Psychotherapy Basic Principles. Clinically Relevant Behavior (CRB)
") Functional Analytic Psychotherapy Basic Principles Clinically Relevant Behavior (CRB) CRB1: In-session instances of daily-life problems CRB2: In-session instances of daily-life improvements CRB3: Client
Functional Analytic Psychotherapy Basic Principles Clinically Relevant Behavior (CRB) CRB1: In-session instances of daily-life problems CRB2: In-session instances of daily-life improvements CRB3: Client
TWO WAYS OF THINKING ABOUT A RELATIONSHIP ISSUE
 TWO WAYS OF THINKING ABOUT A RELATIONSHIP ISSUE Here are two different ways of thinking about a relationship issue. Take a mild issue (4 on a scale of 10 in intensity) and view it through these two different
TWO WAYS OF THINKING ABOUT A RELATIONSHIP ISSUE Here are two different ways of thinking about a relationship issue. Take a mild issue (4 on a scale of 10 in intensity) and view it through these two different
Why Is Mommy Like She Is?
 Why Is Mommy Like She Is? A Book For Kids About PTSD Deployment Edition Patience H. C. Mason Patience Press High Springs, Florida PP Patience Press 2010 by Patience Mason All rights reserved. No part of
Why Is Mommy Like She Is? A Book For Kids About PTSD Deployment Edition Patience H. C. Mason Patience Press High Springs, Florida PP Patience Press 2010 by Patience Mason All rights reserved. No part of
Depression. Most of the time, people manage to deal with these feelings and get past them with a little time and care.
 Page 1 of 5 TeensHealth.org A safe, private place to get doctor-approved information on health, emotions, and life. Depression Lately Lindsay hasn't felt like herself. Her friends have noticed it. Kia
Page 1 of 5 TeensHealth.org A safe, private place to get doctor-approved information on health, emotions, and life. Depression Lately Lindsay hasn't felt like herself. Her friends have noticed it. Kia
How to Work with the Patterns That Sustain Depression
 How to Work with the Patterns That Sustain Depression Module 5.2 - Transcript - pg. 1 How to Work with the Patterns That Sustain Depression How the Grieving Mind Fights Depression with Marsha Linehan,
How to Work with the Patterns That Sustain Depression Module 5.2 - Transcript - pg. 1 How to Work with the Patterns That Sustain Depression How the Grieving Mind Fights Depression with Marsha Linehan,
Homework Tracking Notes
 Homework Tracking Food & activity records online (myfitnesspal) Meditation practice days this week Food, activity & mood journal (paper) Specific food or eating behavior goal: Specific activity /fun goal:
Homework Tracking Food & activity records online (myfitnesspal) Meditation practice days this week Food, activity & mood journal (paper) Specific food or eating behavior goal: Specific activity /fun goal:
Step Five. Admitted to ourselves and another human being the exact nature of our wrongs.
 Step Five Admitted to ourselves and another human being the exact nature of our wrongs. Our Basic Text tells us that Step Five is not simply a reading of Step Four. Yet we know that reading our Fourth
Step Five Admitted to ourselves and another human being the exact nature of our wrongs. Our Basic Text tells us that Step Five is not simply a reading of Step Four. Yet we know that reading our Fourth
Workbook 3 Being assertive Dr. Chris Williams
 Workbook 3 Being assertive Dr. Chris Williams From: Overcoming Depression: A Five Areas Approach. Chris Williams, Arnold Publishers (2002) 2 Section 1: Introduction. In this workbook you will: Find out
Workbook 3 Being assertive Dr. Chris Williams From: Overcoming Depression: A Five Areas Approach. Chris Williams, Arnold Publishers (2002) 2 Section 1: Introduction. In this workbook you will: Find out
Overcoming Perfectionism
 Overcoming Perfectionism Perfectionism is a behavioural pattern that is created with an intent to protect you. But this need to be perfect around people causes you to be stiff, rigid and inflexible. And
Overcoming Perfectionism Perfectionism is a behavioural pattern that is created with an intent to protect you. But this need to be perfect around people causes you to be stiff, rigid and inflexible. And
What is stress? Stress is an emotional/ bodily reaction to
 The Basics What is stress? What are some causes of stress? Stress is an emotional/ bodily reaction to a physical, psychological or emotional demand We all display stress in different ways Some stress is
The Basics What is stress? What are some causes of stress? Stress is an emotional/ bodily reaction to a physical, psychological or emotional demand We all display stress in different ways Some stress is
Depression: Dealing with unhelpful thoughts
 Depression: Dealing with unhelpful thoughts Macquarie University Counselling Service, Campus Wellbeing Level 2 Lincoln Building C8A 9850 7497 counselling@mq.edu.au http://www.campuslife.mq.edu.au/campus-wellbeing/counselling
Depression: Dealing with unhelpful thoughts Macquarie University Counselling Service, Campus Wellbeing Level 2 Lincoln Building C8A 9850 7497 counselling@mq.edu.au http://www.campuslife.mq.edu.au/campus-wellbeing/counselling
CHANGING NEGATIVE THOUGHTS COURSE NOTES
 Module 3: Think Differently WiredForHappy.com CHANGING NEGATIVE THOUGHTS COURSE NOTES Learning to change negative thoughts is a crucial skill on your journey to emotional wellness. In this module, you
Module 3: Think Differently WiredForHappy.com CHANGING NEGATIVE THOUGHTS COURSE NOTES Learning to change negative thoughts is a crucial skill on your journey to emotional wellness. In this module, you
Test Anxiety. New Perspective Counseling Services Dr. Elyse Deleski, LMFT
 Test Anxiety New Perspective Counseling Services Dr. Elyse Deleski, LMFT What is Test Anxiety? Excessive worry about the test. Fear of being evaluated. A sick feeling you get when you are about to take
Test Anxiety New Perspective Counseling Services Dr. Elyse Deleski, LMFT What is Test Anxiety? Excessive worry about the test. Fear of being evaluated. A sick feeling you get when you are about to take
Motivational Interviewing
 Motivational Interviewing By: Tonia Stott, PhD What is Motivational Interviewing? A client-centered, directive method for enhancing intrinsic motivation to change by exploring and resolving ambivalence
Motivational Interviewing By: Tonia Stott, PhD What is Motivational Interviewing? A client-centered, directive method for enhancing intrinsic motivation to change by exploring and resolving ambivalence
Psychotherapy. A Cognitive Approach. Mark J. Berber, MD
 Mark J. Berber, MD Dr. Mark Berber has written an excellent brief approach to psychotherapy. If you use Dr. Berber s booklet you can appreciably help yourself with your thinking and feeling problems...and
Mark J. Berber, MD Dr. Mark Berber has written an excellent brief approach to psychotherapy. If you use Dr. Berber s booklet you can appreciably help yourself with your thinking and feeling problems...and
Goldsmith. Marshall. FEEDFORWARD Coaching For Your Future. Coaching For Your Future. MMIX ChartHouse Learning. All Rights Reserved. What Is It?
 FOR PREVIEW ONLY Marshall Goldsmith Table of Contents.............................................. 2 Get 360 Feedback...3 Pick a Behavior...4 Respond.......................................... 4 Involve...6
FOR PREVIEW ONLY Marshall Goldsmith Table of Contents.............................................. 2 Get 360 Feedback...3 Pick a Behavior...4 Respond.......................................... 4 Involve...6
Step One for Gamblers
 Step One for Gamblers We admitted we were powerless over gambling that our lives had become unmanageable. Gamblers Anonymous (GA) (1989b, p. 38) Before beginning this exercise, please read Step One in
Step One for Gamblers We admitted we were powerless over gambling that our lives had become unmanageable. Gamblers Anonymous (GA) (1989b, p. 38) Before beginning this exercise, please read Step One in
THERAPEUTIC COMMUNICATION CLINICAL ASSIGNMENT STUDY ACTIVITY FOR EGO DEFENSE MECHANISMS
 NUR2712C a. Displacement b. Reaction formation c. Splitting d. Regression e. Sublimation f. Rationalization g. Projection h. Suppression i. Identification j. Compensation k. Minimization l. Intellectualization
NUR2712C a. Displacement b. Reaction formation c. Splitting d. Regression e. Sublimation f. Rationalization g. Projection h. Suppression i. Identification j. Compensation k. Minimization l. Intellectualization
FIGURE 1-The Cognitive Model. Core belief. I m incompetent. Intermediate belief. If I don t understand something perfectly, then I m dumb
 FIGURE 1-The Cognitive Model Core belief I m incompetent Intermediate belief If I don t understand something perfectly, then I m dumb Situation Automatic thoughts Reactions Reading this book This is too
FIGURE 1-The Cognitive Model Core belief I m incompetent Intermediate belief If I don t understand something perfectly, then I m dumb Situation Automatic thoughts Reactions Reading this book This is too
Choosing Life: Empowerment, Action, Results! CLEAR Menu Sessions. Substance Use Risk 2: What Are My External Drug and Alcohol Triggers?
 Choosing Life: Empowerment, Action, Results! CLEAR Menu Sessions Substance Use Risk 2: What Are My External Drug and Alcohol Triggers? This page intentionally left blank. What Are My External Drug and
Choosing Life: Empowerment, Action, Results! CLEAR Menu Sessions Substance Use Risk 2: What Are My External Drug and Alcohol Triggers? This page intentionally left blank. What Are My External Drug and
The Power of Feedback
 The Power of Feedback 35 Principles for Turning Feedback from Others into Personal and Professional Change By Joseph R. Folkman The Big Idea The process of review and feedback is common in most organizations.
The Power of Feedback 35 Principles for Turning Feedback from Others into Personal and Professional Change By Joseph R. Folkman The Big Idea The process of review and feedback is common in most organizations.
Reframing I can t do it
 Chapter 23 Reframing I can t do it A Practical Exercise We are upset not by things but the view we take of them Epictetus Saturday afternoon. Reframing distressing thoughts is a practice that helps you
Chapter 23 Reframing I can t do it A Practical Exercise We are upset not by things but the view we take of them Epictetus Saturday afternoon. Reframing distressing thoughts is a practice that helps you
Managing Negative or Unhelpful Thoughts
 Managing Negative or Unhelpful Thoughts In Cognitive Behavioural Therapy, we give particular focus to the pattern, force, frequency and content of negative or unhelpful thinking. Thoughts play a key role
Managing Negative or Unhelpful Thoughts In Cognitive Behavioural Therapy, we give particular focus to the pattern, force, frequency and content of negative or unhelpful thinking. Thoughts play a key role
CBT Self-Help Module 1. How to Identify Automatic Thoughts, Evaluate Their Distortions, and Begin to Challenge Them
 CBT Self-Help Module 1 How to Identify Automatic Thoughts, Evaluate Their Distortions, and Begin to Challenge Them The essence of cognitive behavioral therapy (CBT) is to: Identify patterns of thinking
CBT Self-Help Module 1 How to Identify Automatic Thoughts, Evaluate Their Distortions, and Begin to Challenge Them The essence of cognitive behavioral therapy (CBT) is to: Identify patterns of thinking
ME Project Handouts Weeks 1-6
 ME Project Handouts Weeks 1-6 Note: This document is formatted so that the two-page handouts are double-side. In order to print this document correctly, please make sure that your printer is set to print
ME Project Handouts Weeks 1-6 Note: This document is formatted so that the two-page handouts are double-side. In order to print this document correctly, please make sure that your printer is set to print
QUESTIONS ANSWERED BY
 Module 16 QUESTIONS ANSWERED BY BERNIE SIEGEL, MD 2 Q How do our thoughts and beliefs affect the health of our bodies? A You can t separate thoughts and beliefs from your body. What you think and what
Module 16 QUESTIONS ANSWERED BY BERNIE SIEGEL, MD 2 Q How do our thoughts and beliefs affect the health of our bodies? A You can t separate thoughts and beliefs from your body. What you think and what
Introduction to TEAM-CBT: Is High Speed Treatment Really Possible? Why TEAM-CBT? British CoBalT Trial. Copyright 2017 by David Burns, M.D.
 Introduction to TEAM-CBT: Is High Speed Treatment Really Possible? David D. Burns, M.D. Adjunct Clinical Professor of Psychiatry and Behavioral Sciences, Stanford Medical School 1 Why TEAM-CBT? Attempt
Introduction to TEAM-CBT: Is High Speed Treatment Really Possible? David D. Burns, M.D. Adjunct Clinical Professor of Psychiatry and Behavioral Sciences, Stanford Medical School 1 Why TEAM-CBT? Attempt
Here are a few ideas to help you cope and get through this learning period:
 Coping with Diabetes When you have diabetes you may feel unwell and have to deal with the fact that you have a life long disease. You also have to learn about taking care of yourself. You play an active
Coping with Diabetes When you have diabetes you may feel unwell and have to deal with the fact that you have a life long disease. You also have to learn about taking care of yourself. You play an active
Paul Figueroa. Washington Municipal Clerks Association ANNUAL CONFERENCE. Workplace Bullying: Solutions and Prevention. for
 Workplace Bullying: Solutions and Prevention for Washington Municipal Clerks Association ANNUAL CONFERENCE Paul@PeaceEnforcement.com 206-650-5364 Peace Enforcement LLC Bullying described: Why people do
Workplace Bullying: Solutions and Prevention for Washington Municipal Clerks Association ANNUAL CONFERENCE Paul@PeaceEnforcement.com 206-650-5364 Peace Enforcement LLC Bullying described: Why people do
Ingredients of Difficult Conversations
 Ingredients of Difficult Conversations Differing Perceptions In most difficult conversations, there are different perceptions of the same reality. I think I'm right and the person with whom I disagree
Ingredients of Difficult Conversations Differing Perceptions In most difficult conversations, there are different perceptions of the same reality. I think I'm right and the person with whom I disagree
How to Reduce Test Anxiety
 How to Reduce Test Anxiety To reduce math test anxiety, you need to understand both the relaxation response and how negative self-talk undermines your abilities. Relaxation Techniques The relaxation response
How to Reduce Test Anxiety To reduce math test anxiety, you need to understand both the relaxation response and how negative self-talk undermines your abilities. Relaxation Techniques The relaxation response
The University of Manchester Library. My Learning Essentials. Now or never? Understanding the procrastination cycle CHEAT SHEET.
 The University of Manchester Library My Learning Essentials Now or never? Understanding the procrastination cycle CHEAT SHEET @mlemanchester https://www.escholar.manchester.ac.uk/learning-objects/mle/counselling/
The University of Manchester Library My Learning Essentials Now or never? Understanding the procrastination cycle CHEAT SHEET @mlemanchester https://www.escholar.manchester.ac.uk/learning-objects/mle/counselling/
Guidelines for Working with People Affected by Trauma
 Guidelines for Working with People Affected by Trauma Guidelines For Working with People Affected by Trauma Strengths-Based Perspective Focusing on strengths instead of weaknesses is a basic tenant of
Guidelines for Working with People Affected by Trauma Guidelines For Working with People Affected by Trauma Strengths-Based Perspective Focusing on strengths instead of weaknesses is a basic tenant of
Family Connections Validation Skills
 Page 24 Definition of validation What Is Validation? (Fruzzetti) Identifying and communicating your understanding of what the other person is saying or feeling in a CLEAR way Communicate what you understand
Page 24 Definition of validation What Is Validation? (Fruzzetti) Identifying and communicating your understanding of what the other person is saying or feeling in a CLEAR way Communicate what you understand
COGNITIVE DISTORTIONS AND PERCEPTION HOW THINKING IMPACTS BEHAVIOR
 COGNITIVE DISTORTIONS AND PERCEPTION HOW THINKING IMPACTS BEHAVIOR WHAT DOES THIS MEAN TO YOU? OBJECTIVES THREE PRINCIPLES OF CBT. CORE BELIEFS AND IMPACT ON BEHAVIOR. DEFINE COGNITIVE DISTORTIONS. HISTORY
COGNITIVE DISTORTIONS AND PERCEPTION HOW THINKING IMPACTS BEHAVIOR WHAT DOES THIS MEAN TO YOU? OBJECTIVES THREE PRINCIPLES OF CBT. CORE BELIEFS AND IMPACT ON BEHAVIOR. DEFINE COGNITIVE DISTORTIONS. HISTORY
Learn how to more effectively communicate with others. This will be a fun and informative workshop! Sponsored by
 Assertiveness Training Learn how to more effectively communicate with others. This will be a fun and informative workshop! Sponsored by Lack of Assertiveness Examples Allowing others to coerce you into
Assertiveness Training Learn how to more effectively communicate with others. This will be a fun and informative workshop! Sponsored by Lack of Assertiveness Examples Allowing others to coerce you into
The Wellbeing Course. Resource: Mental Skills. The Wellbeing Course was written by Professor Nick Titov and Dr Blake Dear
 The Wellbeing Course Resource: Mental Skills The Wellbeing Course was written by Professor Nick Titov and Dr Blake Dear About Mental Skills This resource introduces three mental skills which people find
The Wellbeing Course Resource: Mental Skills The Wellbeing Course was written by Professor Nick Titov and Dr Blake Dear About Mental Skills This resource introduces three mental skills which people find
Feeling Great High-Speed Cognitive Therapy. Why TEAM-CBT? Disappointing Results with Outcome Studies. Copyright 2018 by David Burns, M.D.
 Feeling Great High-Speed Cognitive Therapy David D. Burns, M.D. Adjunct Clinical Professor of Psychiatry and Behavioral Sciences, Stanford Medical School 1 Why TEAM-CBT? Attempt to improve therapy outcomes
Feeling Great High-Speed Cognitive Therapy David D. Burns, M.D. Adjunct Clinical Professor of Psychiatry and Behavioral Sciences, Stanford Medical School 1 Why TEAM-CBT? Attempt to improve therapy outcomes
Adapted from information provided at kidshealth.org
 Emma's mum first noticed the cuts when Emma was doing the dishes one night. Emma told her mum that their cat had scratched her. Her mum seemed surprised that the cat had been so rough, but she didn't think
Emma's mum first noticed the cuts when Emma was doing the dishes one night. Emma told her mum that their cat had scratched her. Her mum seemed surprised that the cat had been so rough, but she didn't think
Secrets to Leading with Assertiveness. Participant Manual
 Secrets to Leading with Assertiveness Participant Manual Copyright 2017 Dale Carnegie & Associates, Inc. 290 Motor Parkway Hauppauge, New York 11788 All rights reserved. Except as permitted under the U.S.
Secrets to Leading with Assertiveness Participant Manual Copyright 2017 Dale Carnegie & Associates, Inc. 290 Motor Parkway Hauppauge, New York 11788 All rights reserved. Except as permitted under the U.S.
12 hours. Your body has eliminates all excess carbon monoxide and your blood oxygen levels become normal.
 Balance March 2018 What happens after the last cigarette? You know that smoking is one of the leading causes of preventable deaths but the process of quitting seems too daunting. After all, you ve tried
Balance March 2018 What happens after the last cigarette? You know that smoking is one of the leading causes of preventable deaths but the process of quitting seems too daunting. After all, you ve tried
Self-harm Workshop. Gemma Fieldsend
 Self-harm Workshop Gemma Fieldsend Don t give up you are not alone it s important to not feel alone Self-harm Self-harm is a common coping mechanism for young people who turn to it as quickly as other
Self-harm Workshop Gemma Fieldsend Don t give up you are not alone it s important to not feel alone Self-harm Self-harm is a common coping mechanism for young people who turn to it as quickly as other
The Psychotherapy File
 The Psychotherapy File An Aid to Understanding Ourselves Better Published April 2000 V.04.00 Association for Cognitive Analytic Therapy 3rd Floor, South Wing, Division of Academic Psychiatry enquiries@acat.org.uk
The Psychotherapy File An Aid to Understanding Ourselves Better Published April 2000 V.04.00 Association for Cognitive Analytic Therapy 3rd Floor, South Wing, Division of Academic Psychiatry enquiries@acat.org.uk
Grief After Suicide. Grief After Suicide. Things to Know about Suicide
 Grief After Suicide Grief After Suicide Your grief after a suicide may feel quite different than the grief you have felt after other kinds of losses. Usually the death of someone from suicide has a much
Grief After Suicide Grief After Suicide Your grief after a suicide may feel quite different than the grief you have felt after other kinds of losses. Usually the death of someone from suicide has a much
Agenda. Challenging Issues in CBT: Handling the Difficult Patient. Readings. Readings. Specifying the Difficulty. Specifying the Difficulty
 Agenda Challenging Issues in CBT: Handling the Difficult Patient Judith S. Beck, PhD President, Beck Institute for Cognitive Therapy and Research Bala Cynwyd, Pennsylvania Clinical Associate Professor
Agenda Challenging Issues in CBT: Handling the Difficult Patient Judith S. Beck, PhD President, Beck Institute for Cognitive Therapy and Research Bala Cynwyd, Pennsylvania Clinical Associate Professor
For young people living with someone s excessive drinking, drug use or addiction
 Taking the Lid Off For young people living with someone s excessive drinking, drug use or addiction When your mum, dad, or other family member has been drinking or using drugs, do they: Embarrass you?
Taking the Lid Off For young people living with someone s excessive drinking, drug use or addiction When your mum, dad, or other family member has been drinking or using drugs, do they: Embarrass you?
Leadership Beyond Reason
 1-Values... 2 2-Thoughts... 2 Cognitive Style... 2 Orientation to Reality... 2 Holding Opposing Thoughts... 2 Adapting to New Realities... 2 Intuition... 2 Creativity... 3 Cognitive Distortions... 3 Observe
1-Values... 2 2-Thoughts... 2 Cognitive Style... 2 Orientation to Reality... 2 Holding Opposing Thoughts... 2 Adapting to New Realities... 2 Intuition... 2 Creativity... 3 Cognitive Distortions... 3 Observe
CAUSING OTHERS TO WANT YOUR LEADERSHIP
 CAUSING OTHERS TO WANT YOUR LEADERSHIP...for Administrators 2nd edition ROBERT L. DEBRUYN AUTHOR OF THE MASTER TEACHER Table of ConTenTs INTRODUCTION...vii Part one You and PeoPle ChaPter 1. What LeaDershIP
CAUSING OTHERS TO WANT YOUR LEADERSHIP...for Administrators 2nd edition ROBERT L. DEBRUYN AUTHOR OF THE MASTER TEACHER Table of ConTenTs INTRODUCTION...vii Part one You and PeoPle ChaPter 1. What LeaDershIP
We admitted that we were powerless over alcohol that our lives had become unmanageable.
 Step One We admitted that we were powerless over alcohol that our lives had become unmanageable. Alcoholics Anonymous (AA) (2001, p. 59) Before beginning this exercise, please read Step One in Twelve Steps
Step One We admitted that we were powerless over alcohol that our lives had become unmanageable. Alcoholics Anonymous (AA) (2001, p. 59) Before beginning this exercise, please read Step One in Twelve Steps
Dealing with Difficult People Personality Disordered Psychopaths. Anna Salter
 Dealing with Difficult People Personality Disordered Psychopaths Anna Salter Current Zeitgeist Good Lives Model Primary Goods People seek primary goods Primary Goods Experiences, states of mind, activities
Dealing with Difficult People Personality Disordered Psychopaths Anna Salter Current Zeitgeist Good Lives Model Primary Goods People seek primary goods Primary Goods Experiences, states of mind, activities
We admitted that we were powerless over alcohol that our lives had become unmanageable. Alcoholics Anonymous (AA) (2001, p. 59)
 (2001, p. 59)") Step One 22 istockphoto.com/qingwa We admitted that we were powerless over alcohol that our lives had become unmanageable. Alcoholics Anonymous (AA) (2001, p. 59) Before beginning this exercise, please
Step One 22 istockphoto.com/qingwa We admitted that we were powerless over alcohol that our lives had become unmanageable. Alcoholics Anonymous (AA) (2001, p. 59) Before beginning this exercise, please
Stories of depression
 Stories of depression Does this sound like you? D E P A R T M E N T O F H E A L T H A N D H U M A N S E R V I C E S P U B L I C H E A L T H S E R V I C E N A T I O N A L I N S T I T U T E S O F H E A L
Stories of depression Does this sound like you? D E P A R T M E N T O F H E A L T H A N D H U M A N S E R V I C E S P U B L I C H E A L T H S E R V I C E N A T I O N A L I N S T I T U T E S O F H E A L
Motivational Strategies for Challenging Situations
 Motivational Strategies for Challenging Situations Mandy Fauble, PhD, LCSW Executive Director, Safe Harbor Behavioral Health of UPMC Hamot James, Wyler, MA, CPRP Scenario When I talked to her about my
Motivational Strategies for Challenging Situations Mandy Fauble, PhD, LCSW Executive Director, Safe Harbor Behavioral Health of UPMC Hamot James, Wyler, MA, CPRP Scenario When I talked to her about my
How to Help Your Patients Overcome Anxiety with Mindfulness
 How to Help Your Patients Overcome Anxiety with Mindfulness Video 7 - Transcript - pg. 1 How to Help Your Patients Overcome Anxiety with Mindfulness How to Teach Clients to Self-Soothe with Ron Siegel,
How to Help Your Patients Overcome Anxiety with Mindfulness Video 7 - Transcript - pg. 1 How to Help Your Patients Overcome Anxiety with Mindfulness How to Teach Clients to Self-Soothe with Ron Siegel,
AN INFORMATION BOOKLET FOR YOUNG PEOPLE WHO SELF HARM & THOSE WHO CARE FOR THEM
 SeLf- HaRM AN INFORMATION BOOKLET FOR YOUNG PEOPLE WHO SELF HARM & THOSE WHO CARE FOR THEM SELF HARM // An Information Booklet 4 SELF HARM An Information Booklet For Young People Who Self Harm And Those
SeLf- HaRM AN INFORMATION BOOKLET FOR YOUNG PEOPLE WHO SELF HARM & THOSE WHO CARE FOR THEM SELF HARM // An Information Booklet 4 SELF HARM An Information Booklet For Young People Who Self Harm And Those
Practical Skills for Working with Clients Who Are Angry
 Practical Skills for Working with Clients Who Are Angry - Video 9 Hanson, PhD and Z. Segal, PhD - Transcript - pg. 1 Practical Skills for Working with Clients Who Are Angry Two Ways to Work with a Passive-Aggressive
Practical Skills for Working with Clients Who Are Angry - Video 9 Hanson, PhD and Z. Segal, PhD - Transcript - pg. 1 Practical Skills for Working with Clients Who Are Angry Two Ways to Work with a Passive-Aggressive
Step One. We admitted we were powerless over our addictions and compulsions --that our lives had become unmanageable.
 Step One We admitted we were powerless over our addictions and compulsions --that our lives had become unmanageable. I know that nothing good lives in me, that is, in my sinful nature. For I have the desire
Step One We admitted we were powerless over our addictions and compulsions --that our lives had become unmanageable. I know that nothing good lives in me, that is, in my sinful nature. For I have the desire
CONCEPTS GUIDE. Improving Personal Effectiveness With Versatility
 CONCEPTS GUIDE Improving Personal Effectiveness With Versatility TABLE OF CONTENTS PAGE Introduction...1 The SOCIAL STYLE MODEL TM...1 Where Did Your Style Come From?...1 SOCIAL STYLE and Versatility Work...
CONCEPTS GUIDE Improving Personal Effectiveness With Versatility TABLE OF CONTENTS PAGE Introduction...1 The SOCIAL STYLE MODEL TM...1 Where Did Your Style Come From?...1 SOCIAL STYLE and Versatility Work...
Why does someone develop bipolar disorder?
 Bipolar Disorder Do you go through intense moods? Do you feel very happy and energized some days, and very sad and depressed on other days? Do these moods last for a week or more? Do your mood changes
Bipolar Disorder Do you go through intense moods? Do you feel very happy and energized some days, and very sad and depressed on other days? Do these moods last for a week or more? Do your mood changes
Reframing Perspectives
 Page 1 Reframing Perspectives Reframing is an essential part of the coaching process as it helps others to see things differently and, as a result, come to different, more empowering conclusions or feelings
Page 1 Reframing Perspectives Reframing is an essential part of the coaching process as it helps others to see things differently and, as a result, come to different, more empowering conclusions or feelings
REASON FOR REFLECTING
 Reflecting Skills Paraphrase and Reflection of Feeling REASON FOR REFLECTING Reflecting is a verbal way of communicating empathy A form of feedback that enables the client to confirm or correct the impression
Reflecting Skills Paraphrase and Reflection of Feeling REASON FOR REFLECTING Reflecting is a verbal way of communicating empathy A form of feedback that enables the client to confirm or correct the impression
#1. What is SAD and how will we resolve it?
 SCS Workbook I highly recommend using this workbook and writing everything down as it will deepen your results. The act of writing it down (typing is fine too) makes everything go into your subconscious
SCS Workbook I highly recommend using this workbook and writing everything down as it will deepen your results. The act of writing it down (typing is fine too) makes everything go into your subconscious
Anger. The causes of our anger and how we deal with it will often be heavily influenced by our upbringing and cultural background.
 Anger What is anger? Anger is a natural human emotion we all feel angry at some point and this is healthy, as anger is a natural response to many events that can happen in life, like being attacked, insulted,
Anger What is anger? Anger is a natural human emotion we all feel angry at some point and this is healthy, as anger is a natural response to many events that can happen in life, like being attacked, insulted,
My Creativity 1. Do I tend to do things in the accepted way or am I more creative? HDIFAT? 2. HDIF when my creative juices are flowing?
 Dialogue Questions Choose the questions that most appropriately fit for your situation or relationship. Some questions can be adapted or modified depending on whether you are journaling as an individual
Dialogue Questions Choose the questions that most appropriately fit for your situation or relationship. Some questions can be adapted or modified depending on whether you are journaling as an individual
Jack Grave All rights reserved. Page 1
 Page 1 Never Worry About Premature Ejaculation Again Hey, I m Jack Grave, author of and today is a great day! Through some great fortune you ve stumbled upon the knowledge that can transform your sex life.
Page 1 Never Worry About Premature Ejaculation Again Hey, I m Jack Grave, author of and today is a great day! Through some great fortune you ve stumbled upon the knowledge that can transform your sex life.
Interviewer: Tell us about the workshops you taught on Self-Determination.
 INTERVIEW WITH JAMIE POPE This is an edited translation of an interview by Jelica Nuccio on August 26, 2011. Jelica began by explaining the project (a curriculum for SSPs, and for Deaf-Blind people regarding
INTERVIEW WITH JAMIE POPE This is an edited translation of an interview by Jelica Nuccio on August 26, 2011. Jelica began by explaining the project (a curriculum for SSPs, and for Deaf-Blind people regarding
EMOTION CARDS. Introduction and Ideas. How Do You Use These Cards?
 Introduction and Ideas A significant part of helping kids to deal with their emotions (Jump In! Stand Strong! Rise Up!) is helping them to develop a robust feelings vocabulary. That is why we are excited
Introduction and Ideas A significant part of helping kids to deal with their emotions (Jump In! Stand Strong! Rise Up!) is helping them to develop a robust feelings vocabulary. That is why we are excited
Coach on Call. Letting Go of Stress. A healthier life is on the line for you! How Does Stress Affect Me?
 Coach on Call How Does Stress Affect Me? Over time, stress can affect the way you feel, think, and act. You need some time when you are free of stress. You need ways to get relief from stress. Without
Coach on Call How Does Stress Affect Me? Over time, stress can affect the way you feel, think, and act. You need some time when you are free of stress. You need ways to get relief from stress. Without
Self-confidence can increase or decrease according to the context (situation, time, people) we are in.
 we are in.") Self Confidence 1 SELF-CONFIDENCE Self-confidence can be described as one's trust in his/her own thoughts, feelings and learning ability. Self-confident people can evaluate their experience in a correct
Self Confidence 1 SELF-CONFIDENCE Self-confidence can be described as one's trust in his/her own thoughts, feelings and learning ability. Self-confident people can evaluate their experience in a correct
FEARBUSTER EXERCISES
 FEARBUSTER EXERCISES Welcome to Module Five: Wheel of Fear Video One: Wheel of Fear Review Fearbuster Exercise: Fear Drawing Video 5.1 Fearbuster Exercise: Integration Questions Video 5.1 Please write
FEARBUSTER EXERCISES Welcome to Module Five: Wheel of Fear Video One: Wheel of Fear Review Fearbuster Exercise: Fear Drawing Video 5.1 Fearbuster Exercise: Integration Questions Video 5.1 Please write