Arizona Chapter AACE Paul D. Miller, M.D.
|
|
|
- Kelly Thornton
- 5 years ago
- Views:
Transcription
1 Arizona Chapter AACE Paul D. Miller, M.D. Management of fractures in CKD and atypical subtrochanteric femur fractures September 2018
2 Paul D. Miller, M.D. Disclosures: Amgen (Consultant, Advisory Board, grants) Radius Health (Advisory Board, grants) Alexion (consultant, grants) Regeneron (consultant, grants) Merck and Co (consultant, grants) Eli Lilly and Co (Advisory board, grants, consultant) National Bone Health Alliance (scientific advisory board and research grants) EQUITY : NONE
3 Fracture Risk is Very High In Stage 5 KD ~ 50 % prevalence of fractures ~ 50% excess mortality as compared to age-matched controls without stage 5 CKD Fractures occur ~ 10 years earlier than age-matched, BMD matched patients without CKD Hip fractures risk 17X higher than age-matched patients without stage 5 CKD Leinau L and Perazella MA. Sem Dialysis 19: 75-79, 2006 Bliue D, et al. JAMA 301: , 2009
4 Mortality is Much Higher Following Hip Fracture in ESRD Patients than Age- Matched Controls 1 year mortality after hip fracture in stage 5D CKD: 60% 1 year mortality after hip fracture in age-matched controls: 15% female 30% male Leinau L and Perazella MA. Sem Dialysis 19: 75-79, Bliue D, et al. JAMA 301: , 2009
5 It s Just Not ESRD All stages of CKD have higher fracture risk than aged-matched persons without CKD
6 Studies of Fracture Risk Associated with Age-Related Reductions in GFR Author N Kidney Function Dukas 1 5,481 GFR: <65 ml/min Hip 1.57* ( ) Ensrud 2 9,704 Tiered GFR 60 ml/min ml/min <45 ml/min OR for Fracture (95% Confidence Interval) Vertebral 1.31* ( ) Hip ( ) 2.32 ( ) Radial 1.79* ( ) Fried 3 4,699 Tiered Cystatin-C <0.92 mg/l mg/l mg/l 1.22 mg/l Men at Hip ( ) 0.80 ( ) 1.25 ( ) Women at Hip ( ) 1.49 ( ) 1.66 ( ) Nickolas 4 6,270 GFR: <60 ml/min Hip 2.12 ( ) *P<0.01; P for trend <0.05 Mild to moderate kidney impairment is associated with an approximate doubling in OR of all fractures as compared to agematched people with normal kidney function 1.Dukas L et al. Osteoporos Int. 2005;16: Ensrud KE et al. Arch Intern Med. 2007;167: Fried LF et al. J Am Soc Nephrol. 2007;18: Nickolas TL et al. J Am Soc Nephrol. 2006;17:3223.
7 Elevated PTH Phosphorus and pyrophosphate retention Elevated FGF 23 Chronic metabolic acidosis Sarcopenia

8 Regulation of Serum Phosphorus The Interactions Between the Parathyroid Glands, Kidneys, Bone and Systemic Vasculature: Miller PD, Sprague S and Shane E Am J Kid Dis 2014 PTH Serum P Ca Absorption P Absorption 1,25 D GFR PTH 1,25 D PTH P Reabsorption SCLEROSTIN Ca and P Osteoclast FGF 23 1,25 D FGF 23 P Reabsorption FGF 23 Osteocyt e Osteoblast FGF 23 PTH PTH Osteoblast Activity
9 Fractures In Chronic Kidney Disease 1. Hyperparathyroidism 2. Adynamic bone disease 3. Osteomalacia 4. Post-transplantation 5. Osteoporosis Atsumi K, et al Am J Kidney Dis 1999; 33(2): Gupta A, et al. Journal of Bone and Mineral Research 12(Suppl. 1):S274. Stehman-Breen CO, et al. Kidney Int 2000; 58(5): Fried LF et al J Am Soc Nephrol 2007; 18: Coco M and Rush H. Am J Kid Dis 2000; 36 (6): Nickolas TL et al. Kid Internat 2008; 74(6):
10 2 Bone Diseases to Avoid turning bone turnover down Osteomalacia Adynamic bone disease




11 Von Kossa, H&E Stain for Calcium and Osteoid: Osteomalacia Thick Trabeculae Increased Osteoid A 25X B 100X Unstained, Fluorescent for Tetracycline Von Kossa, H&E Stain, Fluorescent for Osteoid Peri-osteocytic Osteoid No label Osteoid Diffuse label Single label C 100X D 100X Courtesy of PD Miller
12 Osteomalacia: always has a cause Severe 25 OHD deficiency (< 8 ng/ml). Chronic hypophosphatemia Vitamin D resistant rickets Renal tubular acidosis Oncogenic osteomalacia TIO: (low serum PO⁴, elevated FGF 23, low, 1, 25 D, phosphaturia)
13 Biochemical Tests to Screen for Etiologies of Osteomalacia 25D 1,25D Serum and urine phosphorus Electrolytes, arterial blood gases, urine ph FGF 23 Elevated BSAP
14 Elevated BSAP Excludes adynamic bone disease (unless there has been a recent fracture)
15 Elevated BSAP (DDX) 1.Severe primary hyperparathyroidism 2. Hyperthyroidism 3. Metastatic cancer in bone 4. Paget s disease of bone 5. Recent large bone fracture 6. Osteomalacia 7. Severe (< 8-10 ng/ml) vitamin D deficiency 7. Space travel 8. Immobilization 9. Treatment with anabolics (teriparatide) 10. Treatment with strontium ranelate (Europe) 11. Future: treatment with PTHrp analogues, anti-sclerostin 12. High bone turnover osteoporosis
16 Adynamic Bone Disease Absence of single tetracycline labels
17 Renal Adynamic Bone Disease

18 Normal Double Tetracycline Labels
19 PTH and BSAP combining the best of both worlds 1. PTH extremes ( < 100 pg/ml) or (> 600pg/ml) high specificity for adynamic/ofc. 2. Bone specific alkaline phosphatase ( < 20 IU/L) has a high PPV (80%) for low bone turnover. 3.BSAP correlate with PTH values in stage 5D CKD: both are increased on bone biopsy in established high bone turnover. 4. Combining the lower quartile BSAP and PTH < have a high PPV (90%) for adynamic bone disease. Garrett G et al CJASN 2013 Couttenye C et al Nephrol Dialysis Transpl 2009
20 Bone Biopsy in CKD 1. Is the gold standard for diagnosis of renal bone disease and for defining the bone turnover activity. 2. Require double tetracycline labeling for quantitative bone histomorphometry 3. Is safe and has very low morbidity (including post-op pain) in experienced operators 4. Is especially important before bone turnover is turned down

21 Courtesy of Dr. Elliott Schwartz

22 Renal Adynamic Bone Disease Courtesy of Dr. Paul Miller
23 Therapies for osteoporosis: USA Hormone therapy Raloxifene Bisphosphonates Alendronate Risedronate Ibandronate Zoledronate Calcitonin Teriparatide Denosumab (anti-rank ligand antibody) Abaloparatide
24 Treatment of Osteoporosis in CKD 1. Stage 1-3 CKD: Treatment does not differ as in patients with PMO since clinical trials randomized patients down to GFR of 30 ml/min 2. Stage 4 CKD: Management dependent on considerations for off-label use: Post-hoc analysis show efficacy and safety through 3 years of risedronate, alendronate and raloxifene and denosumab down to egfr of 15 ml/min for 2-3 years. Teriparatide to egfr of Stage 5/5D CKD: No data- off-label consideration for fracturing patients, e.g. very high risk with established osteoporosis. Miller PD. Chronic kidney disease and the skeleton. Bone Res (2):
25 Bisphosphonates in CKD
26 US/European Labeling States: Oral bisphosphonates are not recommended in patients with creatinine clearance < 30 (35) ml/min: (Stage 4-5 CKD) Zoledronic acid contraindicated at GFR < 35 ml/min
27 FDA Label 1. Randomization excluded patients with elevated baseline serum creatinine (< 1.5/<2.4). 2. egfr exclusion criteria added by HORIZON and FREEDOM. 2. Renal (glomerulosclerosis or ATN) seen in case reports with IV bisphosphonates. 3. Bone retention probably greater with reduced GFR since bisphosphonates are cleared by the kidney (both filtration and tubular secretion) Miller PD, Jamal SA, Evenepoel P, Eastell R, Boonen S. Renal safety in patients treated with bisphosphonates for osteoporosis: a review. J Bone Miner Res. 2013;28(10):
28 Mean (±SE) Change From Baseline in Calculated Creatinine Clearance (ml/min) Mean Changes in Calculated Creatinine Clearance From Baseline Over Time Horizon: Zolendronate 5mg/yr vs Placebo Placebo ZOL 5 mg Last Visit ZOL n = PBO n = Black D et al NEJM 2007
29 Managing Renal Risk with ZOL 1. Faster infusion time and greater risk of ARF suggests renal damage might be due to the Cmax rather than the AUC. 2. Slower infusion rate (30 minutes) suggested (opinion) in Stage 3 CKD (egfr ml/min). 3. Patients should be well hydrated, off diuretics for several days, and avoid NSAIDs for several days before infusion. 4. Off-label use in stage 4-5 CKD in established osteoporosis - suggest even slower infusion rate (60 minutes). Miller PD. Cleve Clin J Med. 2009;76: ; Miller PD. Semin Dial. 2007;20: Miller PD. Semin Nephrol. 2009;29: Miller PD. BONE 2011 Miller PD et al JBMR 2013
30 Percent (%) of Patients Vertebral Fracture Risk Reduction With Risedronate 32% (14,46%) P=0.001 Control 45% (31,57% P<0.001 Mild Moderate Severe Baseline Renal Impairment 56% (11,78%) P=0.021 Miller PD et al JBMR 2005
31 Fracture Risk with Alendronate by Estimated GFR (egfr) Site egfr All Women (n=6459) Clinical Fractures Severely reduced Moderately reduced or normal Odds Ratio (95% Confidence Interval) 0.78 (0.51 to 1.2) 0.81 (0.70 to 0.94) P-value for Interaction 0.90 Spine Fractures Severely Reduced Moderately reduced or normal 0.72 (0.31 to 1.7) 0.50 (0.32 to 0.76) 0.44 Jamal S et at JBMR 2007
 N1 3691 3702 33 31 1309 1332 1952 1924 394 413 All 15 29 ml/min 7.0 2.9 30 59 ml/min 7.0 1.8 60 89 ml/min 8.1 3.1 90 ml/min N = number of randomized subjects.")
32 Percent Incidence at Month 36 Incidence of New Vertebral Fracture Through Month 36 by Baseline CrCl * 2.3 Placebo (N=3906) DMAb (N=3902) N All ml/min ml/min ml/min ml/min N = number of randomized subjects. N1 = number of randomized subjects with an evaluation during the time period of interest. There were no subjects with a CrCl < 15 ml/min. *P < 0.05 * * * Jamal S et JBMR 2012
33 Effect of Renal Function on Changes in PINP Concentrations with Teriparatide PINP (3 months) Median Change from Baseline [ng/ml] ((25th, 75th percentiles) * * * * * * Placebo TPTD20 TPTD40 * P<0.05 from Placebo Normal (> 80 ml/min) Mild Impairment (50-79 ml/min) Moderate Impairment (30-49 ml/min) Miller P, et al. Osteopor Int 2007

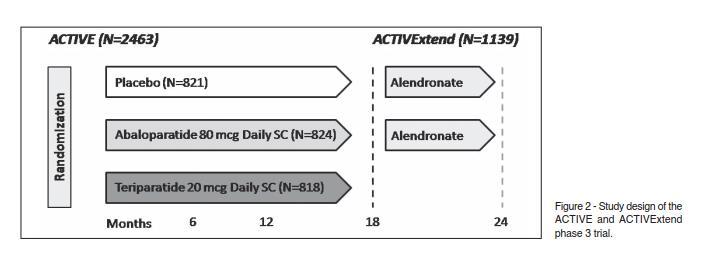
34 Active Trial
35 BTM s of TPTD and Abaloparatide
36 Time to Event of Non-vertebral Fractures

37 Adverse Events

38 X-rays of Stress Fractures Later mid-shaft Femur Stress fracture with beaking Courtesy of Dr. Paul Miller
39 X-ray 3 Days later after Diagnosis of Stress Fractures Completed sub-trochanteric femur fracture Courtesy of Dr. Paul Miller
40 Case 24 yo healthy recent Colorado College graduate, healthy, pre-menopausal woman. No Hx of eating disorder, weight change in past 5 years Runs ~2 miles/day Jogging in Denver City Park had sharp pain right thigh. Went to a local Denver hospital and had x-rays that showed a stress fracture and sent home. 3 days later while walking at work heard a snap and fell to the ground with right femur at ~30 degree angle
41 Atypical Subtrochanteric Femur Fracture ASSOCIATIONS 1. Long term bisphosphonate exposure 2. Chronic glucocorticoids 3. Chronic protein pump inhibitors 4. Hypophosphatasia 5. Cathepsin K inhibitior defeciency 6. Young healthy premenopausal women (? Elevated sclerostin) 7. Diabetes Mellitus Shane E et al. ASBMR Working Group JBMR 2015
42 Teriparatide in Atypical Subtrochanteric Femur Fractures The BAFFETT Study Responses to Treatment With Teriparatide in Patients With Atypical Femur Fractures Previously Treated With Bisphosphonates Nelson B Watts, Deborah Aggers, Edward F McCarthy, Tina Savage, Stephanie Martinez, Rachel Patterson, Erin Carrithers, and Paul D Miller Mercy Health Osteoporosis and Bone Health Services, Cincinnati, OH, USA 2Colorado Center for Bone Research at Centura Health, Lakewood, CO, USA 3Department of Orthopedic Pathology, Johns Hopkins University School of Medicine, Baltimore, MD, Watts N et al. JBMR 2016
43 Conclusions Patients with Stage 1-3 CKD should be diagnosed and managed as patients with normal GFR In stage 4-5 CKD the DDX in patients that fracture could be one or more of a heterogeneous group of metabolic bone disease that requires different therapeutic approaches. The 2 most important renal related metabolic bone diseases that must be R/O before turning bone turnover down are adynamic and osteomalacia bone disease ASFF have heterogeneous conditions associated with their presentation-not all due to bisphosphonates
44 Thank You Arizona AACE For the invitation Paul D. Miller, M.D.
AACE ANNUAL MEETING. Osteoporois and Fractures across the 5 stages of Chronic Kidney Disease. Boston, Mass Paul D. Miller, M.
 AACE ANNUAL MEETING Osteoporois and Fractures across the 5 stages of Chronic Kidney Disease Boston, Mass 2018 Paul D. Miller, M.D Medical Director Paul D. Miller, M.D. Disclosures: Amgen (Consultant, Advisory
AACE ANNUAL MEETING Osteoporois and Fractures across the 5 stages of Chronic Kidney Disease Boston, Mass 2018 Paul D. Miller, M.D Medical Director Paul D. Miller, M.D. Disclosures: Amgen (Consultant, Advisory
Osteoporosis and Chronic Kidney Disease: Diagnosis and Treatment Recommendations
 Osteoporosis and Chronic Kidney Disease: Diagnosis and Treatment Recommendations Nancy E. Lane, MD Director, Center for Musculoskeletal Health Endowed Professor of Medicine and Rheumatology University
Osteoporosis and Chronic Kidney Disease: Diagnosis and Treatment Recommendations Nancy E. Lane, MD Director, Center for Musculoskeletal Health Endowed Professor of Medicine and Rheumatology University
Disclosures. Endocrine Fellows Forum 2016 Atlanta, Georgia 9/29/2016. Osteoporosis Across the Spectrum of Chronic Kidney Disease Paul D. Miller, M.D.
 Endocrine Fellows Forum 2016 Atlanta, Georgia Osteoporosis Across the Spectrum of Chronic Kidney Disease Paul D. Miller, M.D. Disclosures 1. Research Grants: Alexion, Amgen, Lilly, Merck, Novartis, Radius
Endocrine Fellows Forum 2016 Atlanta, Georgia Osteoporosis Across the Spectrum of Chronic Kidney Disease Paul D. Miller, M.D. Disclosures 1. Research Grants: Alexion, Amgen, Lilly, Merck, Novartis, Radius
Metabolic Bone Disease Related to Chronic Kidney Disease
 Metabolic Bone Disease Related to Chronic Kidney Disease Deborah Sellmeyer, MD Director, Johns Hopkins Metabolic Bone Center Dept of Medicine, Division of Endocrinology Disclosure DSMB member for denosumab
Metabolic Bone Disease Related to Chronic Kidney Disease Deborah Sellmeyer, MD Director, Johns Hopkins Metabolic Bone Center Dept of Medicine, Division of Endocrinology Disclosure DSMB member for denosumab
CKD-MBD CKD mineral bone disorder
 CKD Renal bone disease Dr Mike Stone University Hospital Llandough Affects 5 10 % of population Increasingly common Ageing, diabetes, undetected hypertension Associated with: Cardiovascular disease Premature
CKD Renal bone disease Dr Mike Stone University Hospital Llandough Affects 5 10 % of population Increasingly common Ageing, diabetes, undetected hypertension Associated with: Cardiovascular disease Premature
Update on Osteoporosis 2016
 WELCOME! Update on Osteoporosis 2016 Jennifer J. Kelly, D.O., F.A.C.E. Associate Professor of Medicine Division of Endocrinology, Diabetes and Metabolism Upstate Medical University Director of the Clinical
WELCOME! Update on Osteoporosis 2016 Jennifer J. Kelly, D.O., F.A.C.E. Associate Professor of Medicine Division of Endocrinology, Diabetes and Metabolism Upstate Medical University Director of the Clinical
An Update on Osteoporosis Treatments
 An Update on Osteoporosis Treatments Dr Mike Stone University Hospital Llandough Treatments for osteoporosis Calcium and vitamin D HRT Raloxifene Etidronate Alendronate Risedronate Ibandronate (oral and
An Update on Osteoporosis Treatments Dr Mike Stone University Hospital Llandough Treatments for osteoporosis Calcium and vitamin D HRT Raloxifene Etidronate Alendronate Risedronate Ibandronate (oral and
Forteo (teriparatide) Prior Authorization Program Summary
 Prior Authorization Program Summary") Forteo (teriparatide) Prior Authorization Program Summary FDA APPROVED INDICATIONS DOSAGE 1 FDA Indication 1 : Forteo (teriparatide) is indicated for: the treatment of postmenopausal women with osteoporosis
Forteo (teriparatide) Prior Authorization Program Summary FDA APPROVED INDICATIONS DOSAGE 1 FDA Indication 1 : Forteo (teriparatide) is indicated for: the treatment of postmenopausal women with osteoporosis
Osteoporosis Treatment Overview. Colton Larson RFUMS October 26, 2018
 Osteoporosis Treatment Overview Colton Larson RFUMS October 26, 2018 Burden of Disease Most common bone disease 9.9 million Americans + 43.1 million Americans have low bone mineral density (BMD) Stealthy
Osteoporosis Treatment Overview Colton Larson RFUMS October 26, 2018 Burden of Disease Most common bone disease 9.9 million Americans + 43.1 million Americans have low bone mineral density (BMD) Stealthy
Clinician s Guide to Prevention and Treatment of Osteoporosis
 Clinician s Guide to Prevention and Treatment of Osteoporosis Published: 15 August 2014 committee of the National Osteoporosis Foundation (NOF) Tipawan khiemsontia,md outline Basic pathophysiology screening
Clinician s Guide to Prevention and Treatment of Osteoporosis Published: 15 August 2014 committee of the National Osteoporosis Foundation (NOF) Tipawan khiemsontia,md outline Basic pathophysiology screening
AACE. Orlando Drug Holidays. Disclosures. Advisory boards: Alexion, Amgen, Lilly, Merck, Radius Health
 AACE Orlando 2016 Drug Holidays Disclosures Advisory boards: Alexion, Amgen, Lilly, Merck, Radius Health Scientific grants: Alexion, Amgen, Immunodiagnostics, Lilly, Merck, Regeneron, Radius Health, Roche
AACE Orlando 2016 Drug Holidays Disclosures Advisory boards: Alexion, Amgen, Lilly, Merck, Radius Health Scientific grants: Alexion, Amgen, Immunodiagnostics, Lilly, Merck, Regeneron, Radius Health, Roche
Kristen M. Nebel, DO PENN/ LGHP Geriatrics. Temple Family Medicine Review
 Kristen M. Nebel, DO PENN/ LGHP Geriatrics 10/3/17 Temple Family Medicine Review OBJECTIVES Define Revised 2017 American College of Physician Recommendations Screening, Prevention and Treatment Application
Kristen M. Nebel, DO PENN/ LGHP Geriatrics 10/3/17 Temple Family Medicine Review OBJECTIVES Define Revised 2017 American College of Physician Recommendations Screening, Prevention and Treatment Application
Annual Rheumatology & Therapeutics Review for Organizations & Societies
 Annual Rheumatology & Therapeutics Review for Organizations & Societies Biochemical Markers of Bone Turnover: Definitions and Recommendations for Monitoring Therapy Learning Objectives for Biochemical
Annual Rheumatology & Therapeutics Review for Organizations & Societies Biochemical Markers of Bone Turnover: Definitions and Recommendations for Monitoring Therapy Learning Objectives for Biochemical
Chronic kidney disease and the skeleton
 OPEN Citation: Bone Research (2014) 2, 14044; doi:10.1038/boneres.2014.44 ß 2014 Sichuan University All rights reserved 2095-4700/14 www.nature.com/boneres REVIEW ARTICLE Paul D Miller Fractures across
OPEN Citation: Bone Research (2014) 2, 14044; doi:10.1038/boneres.2014.44 ß 2014 Sichuan University All rights reserved 2095-4700/14 www.nature.com/boneres REVIEW ARTICLE Paul D Miller Fractures across
Assessment and Treatment of Osteoporosis Professor T.Masud
 Assessment and Treatment of Osteoporosis Professor T.Masud Nottingham University Hospitals NHS Trust University of Nottingham University of Derby University of Southern Denmark What is Osteoporosis? Osteoporosis
Assessment and Treatment of Osteoporosis Professor T.Masud Nottingham University Hospitals NHS Trust University of Nottingham University of Derby University of Southern Denmark What is Osteoporosis? Osteoporosis
Bone Disorders in CKD
 Osteoporosis in Dialysis Patients Challenges in Management David M. Klachko MD FACP Professor Emeritus of Medicine University of Missouri-Columbia Bone Disorders in CKD PTH-mediated high-turnover (osteitis
Osteoporosis in Dialysis Patients Challenges in Management David M. Klachko MD FACP Professor Emeritus of Medicine University of Missouri-Columbia Bone Disorders in CKD PTH-mediated high-turnover (osteitis
Drug Intervals (Holidays) with Oral Bisphosphonates
 with Oral Bisphosphonates") Drug Intervals (Holidays) with Oral Bisphosphonates Rizwan Rajak Consultant Rheumatologist & Lead for Osteoporosis GP Postgraduate Meeting April 2018 Contents Case presentation Pathway for Bisphosphonate
Drug Intervals (Holidays) with Oral Bisphosphonates Rizwan Rajak Consultant Rheumatologist & Lead for Osteoporosis GP Postgraduate Meeting April 2018 Contents Case presentation Pathway for Bisphosphonate
Osteoporosis Management
 Osteoporosis Management Lisa Voss PA C, CCD Laura Frontiero NP C, CCD Kaiser Healthy Bones Program San Diego Disclosures: Nothing to disclose www.zazzle.com 1 Overview How to diagnose Osteoporosis FRAX
Osteoporosis Management Lisa Voss PA C, CCD Laura Frontiero NP C, CCD Kaiser Healthy Bones Program San Diego Disclosures: Nothing to disclose www.zazzle.com 1 Overview How to diagnose Osteoporosis FRAX
Chapter 5: Evaluation and treatment of kidney transplant bone disease Kidney International (2009) 76 (Suppl 113), S100 S110; doi: /ki.2009.
 76 (Suppl 113), S100 S110; doi: /ki.2009.") http://www.kidney-international.org & 2009 KDIGO Chapter 5: Evaluation and treatment of kidney transplant bone disease ; doi:10.1038/ki.2009.193 Grade for strength of recommendation a Strength Wording
http://www.kidney-international.org & 2009 KDIGO Chapter 5: Evaluation and treatment of kidney transplant bone disease ; doi:10.1038/ki.2009.193 Grade for strength of recommendation a Strength Wording
Current and Emerging Strategies for Osteoporosis
 Current and Emerging Strategies for Osteoporosis I have nothing to disclose. Anne Schafer, MD Assistant Professor of Medicine Division of Endocrinology & Metabolism December 12, 2014 Outline Osteoporosis
Current and Emerging Strategies for Osteoporosis I have nothing to disclose. Anne Schafer, MD Assistant Professor of Medicine Division of Endocrinology & Metabolism December 12, 2014 Outline Osteoporosis
Current Issues in Osteoporosis
 Current Issues in Osteoporosis California AACE 18TH Annual Meeting & Symposium Marina del Rey, CA September 15, 2018 Michael R. McClung, MD, FACP,FACE Director, Oregon Osteoporosis Center Portland, Oregon,
Current Issues in Osteoporosis California AACE 18TH Annual Meeting & Symposium Marina del Rey, CA September 15, 2018 Michael R. McClung, MD, FACP,FACE Director, Oregon Osteoporosis Center Portland, Oregon,
Advanced medicine conference. Monday 20 Tuesday 21 June 2016
 Advanced medicine conference Monday 20 Tuesday 21 June 2016 Osteoporosis: recent advances in risk assessment and management Juliet Compston Emeritus Professor of Bone Medicine Cambridge Biomedical Campus
Advanced medicine conference Monday 20 Tuesday 21 June 2016 Osteoporosis: recent advances in risk assessment and management Juliet Compston Emeritus Professor of Bone Medicine Cambridge Biomedical Campus
Osteoporosis Update. Greg Summers Consultant Rheumatologist
 Osteoporosis Update Greg Summers Consultant Rheumatologist DEFINITION OSTEOPOROSIS is LOW BONE MASS (& micro-architectural deterioration) causing AN INCREASED RISK OF FRACTURE 23 years 82 years 23 y/o
Osteoporosis Update Greg Summers Consultant Rheumatologist DEFINITION OSTEOPOROSIS is LOW BONE MASS (& micro-architectural deterioration) causing AN INCREASED RISK OF FRACTURE 23 years 82 years 23 y/o
Differentiating Pharmacological Therapies for Osteoporosis
 Differentiating Pharmacological Therapies for Osteoporosis Socrates E Papapoulos Department of Endocrinology & Metabolic Diseases Leiden University Medical Center The Netherlands Competing interests: consulting/speaking
Differentiating Pharmacological Therapies for Osteoporosis Socrates E Papapoulos Department of Endocrinology & Metabolic Diseases Leiden University Medical Center The Netherlands Competing interests: consulting/speaking
Osteoporosis: current treatment and future prospects. Juliet Compston Professor Emeritus of Bone Medicine Cambridge Biomedical Campus
 Osteoporosis: current treatment and future prospects Juliet Compston Professor Emeritus of Bone Medicine Cambridge Biomedical Campus Disclosures Consultancy and speaking fees for Gilead, related to development
Osteoporosis: current treatment and future prospects Juliet Compston Professor Emeritus of Bone Medicine Cambridge Biomedical Campus Disclosures Consultancy and speaking fees for Gilead, related to development
Fracture=Bone Attack:
 Fracture=Bone Attack: Linking Hip Fractures to Osteoporosis Care Angela M. Cheung, MD, PhD, FRCPC Professor of Medicine, University of Toronto Potential Conflicts of Interests Industry Grants (to UHN)
Fracture=Bone Attack: Linking Hip Fractures to Osteoporosis Care Angela M. Cheung, MD, PhD, FRCPC Professor of Medicine, University of Toronto Potential Conflicts of Interests Industry Grants (to UHN)
CASE 1 WHY IS IT IMPORTANT TO TREAT? FACTS CONCERNS
 4:30-5:15pm Ask the Expert: Osteoporosis SPEAKERS Silvina Levis, MD OSTEOPOROSIS - FACTS 1:3 older women and 1:5 older men will have a fragility fracture after age 50 After 3 years of treatment, depending
4:30-5:15pm Ask the Expert: Osteoporosis SPEAKERS Silvina Levis, MD OSTEOPOROSIS - FACTS 1:3 older women and 1:5 older men will have a fragility fracture after age 50 After 3 years of treatment, depending
TREATING OSTEOPOROSIS IN 2018: WHAT'S OLD, WHAT'S NEW, WHAT'S UNPROVEN AND WHAT'S TRUE. Nelson B. Watts, MD
 TREATING OSTEOPOROSIS IN 2018: WHAT'S OLD, WHAT'S NEW, WHAT'S UNPROVEN AND WHAT'S TRUE Nelson B. Watts, MD OSTEOPOROSIS AND BONE HEALTH SERVICES CINCINNATI, OHIO Honoraria: Amgen, Radius, Shire Consulting
TREATING OSTEOPOROSIS IN 2018: WHAT'S OLD, WHAT'S NEW, WHAT'S UNPROVEN AND WHAT'S TRUE Nelson B. Watts, MD OSTEOPOROSIS AND BONE HEALTH SERVICES CINCINNATI, OHIO Honoraria: Amgen, Radius, Shire Consulting
2017 Santa Fe Bone Symposium McClung
 217 Santa Fe Bone Symposium Insights into the Use of Anti-remodeling and Anabolic Agents for Osteoporosis Developing a Long-term Management Plan Michael R., MD, FACP Oregon Osteoporosis Center Portland,
217 Santa Fe Bone Symposium Insights into the Use of Anti-remodeling and Anabolic Agents for Osteoporosis Developing a Long-term Management Plan Michael R., MD, FACP Oregon Osteoporosis Center Portland,
How to treat osteoporosis With what and for how long?
 How to treat osteoporosis With what and for how long? Professor Neil Gittoes Consultant Endocrinologist & Honorary Professor Where will we be going? Drug therapies Current Indications Contraindications/unmet
How to treat osteoporosis With what and for how long? Professor Neil Gittoes Consultant Endocrinologist & Honorary Professor Where will we be going? Drug therapies Current Indications Contraindications/unmet
Osteoporosis 2017 Breaking News. Julie L. Carkin, MD The Seattle Arthritis Clinic
 Osteoporosis 2017 Breaking News Julie L. Carkin, MD The Seattle Arthritis Clinic 1 Yes, Hopefully & No Anabolic Teriparatide Abaloparatide Romosozumab blosozumab Anti-catabolic Bisphosphonates Denosumab
Osteoporosis 2017 Breaking News Julie L. Carkin, MD The Seattle Arthritis Clinic 1 Yes, Hopefully & No Anabolic Teriparatide Abaloparatide Romosozumab blosozumab Anti-catabolic Bisphosphonates Denosumab
11/4/2018. Osteoporosis Update. ACP Oregon Chapter November 9 th, 2018 Sarah Hopkins Providence Medical Group Endocrinology East. No disclosures.
 Osteoporosis Update ACP Oregon Chapter November 9 th, 2018 Sarah Hopkins Providence Medical Group Endocrinology East No disclosures. 1 Goals Review screening recommendations and workup of secondary causes
Osteoporosis Update ACP Oregon Chapter November 9 th, 2018 Sarah Hopkins Providence Medical Group Endocrinology East No disclosures. 1 Goals Review screening recommendations and workup of secondary causes
TREATMENT OF OSTEOPOROSIS HOLIDAYS OR NO HOLIDAYS? Nelson B. Watts, MD OSTEOPOROSIS AND BONE HEALTH SERVICES CINCINNATI, OHIO
 TREATMENT OF OSTEOPOROSIS HOLIDAYS OR NO HOLIDAYS? Nelson B. Watts, MD OSTEOPOROSIS AND BONE HEALTH SERVICES CINCINNATI, OHIO DISCLOSURES Honoraria: Amgen, Merck, Shire Consulting : AbbVie, Amgen, Merck,
TREATMENT OF OSTEOPOROSIS HOLIDAYS OR NO HOLIDAYS? Nelson B. Watts, MD OSTEOPOROSIS AND BONE HEALTH SERVICES CINCINNATI, OHIO DISCLOSURES Honoraria: Amgen, Merck, Shire Consulting : AbbVie, Amgen, Merck,
Updates in Osteoporosis. I have no conflicts of interest. What Would You Do? Mrs. C. What s New in Osteoporosis. Page 1
 Updates in Osteoporosis Jeffrey A. Tice, MD Associate Professor of Medicine Division of General Internal Medicine, University of California, San Francisco I have no conflicts of interest What s New in
Updates in Osteoporosis Jeffrey A. Tice, MD Associate Professor of Medicine Division of General Internal Medicine, University of California, San Francisco I have no conflicts of interest What s New in
Posttransplant Bone Disease. Budapest 2007
 Posttransplant Bone Disease Budapest 2007 Post-transplant bone disease 7 10 % of kidney transplanted patients develope a fracture. The risk is higher in postmenopausal female transplanted patients. Diabetic,
Posttransplant Bone Disease Budapest 2007 Post-transplant bone disease 7 10 % of kidney transplanted patients develope a fracture. The risk is higher in postmenopausal female transplanted patients. Diabetic,
AN OVERVIEW of TREATMENT: WHO and WHEN to TREAT
 AN OVERVIEW of TREATMENT: WHO and WHEN to TREAT Dolores Shoback, MD Professor of Medicine, UCSF San Francisco VA Medical Center July 16, 21 ~ QUESTIONS ~ Who should receive therapy to prevent fractures?
AN OVERVIEW of TREATMENT: WHO and WHEN to TREAT Dolores Shoback, MD Professor of Medicine, UCSF San Francisco VA Medical Center July 16, 21 ~ QUESTIONS ~ Who should receive therapy to prevent fractures?
Osteoporosis in Men Professor Peter R Ebeling
 Osteoporosis in Men MD FRACP Head, Department of Medicine, School for Clinical Sciences Monash Health Translation Precinct Monash University, Clayton, Victoria 1 MonashHealth Potential Conflicts Departmental
Osteoporosis in Men MD FRACP Head, Department of Medicine, School for Clinical Sciences Monash Health Translation Precinct Monash University, Clayton, Victoria 1 MonashHealth Potential Conflicts Departmental
CKD-Mineral Bone Disorder (MBD) Pathogenesis of Metabolic Bone Disease. Grants: NIH, Abbott, Amgen, OPKO, Shire
 Pathogenesis of Metabolic Bone Disease. Grants: NIH, Abbott, Amgen, OPKO, Shire") Pathogenesis of Metabolic Bone Disease Stuart M. Sprague, D.O. Chief, Division of Nephrology and Hypertension Professor of Medicine NorthShore University HealthSystem University of Chicago Pritzker School
Pathogenesis of Metabolic Bone Disease Stuart M. Sprague, D.O. Chief, Division of Nephrology and Hypertension Professor of Medicine NorthShore University HealthSystem University of Chicago Pritzker School
Upcoming Agents for Osteoporosis
 Upcoming Agents for Osteoporosis May 5, 2017 Michael R. McClung, MD, FACP Director, Oregon Osteoporosis Center Portland, Oregon, USA Professorial Fellow, Institute of Health and Ageing Australian Catholic
Upcoming Agents for Osteoporosis May 5, 2017 Michael R. McClung, MD, FACP Director, Oregon Osteoporosis Center Portland, Oregon, USA Professorial Fellow, Institute of Health and Ageing Australian Catholic
7/5/2016. We need drugs that. Disclosures. New Osteoporosis Treatments. What we have today. Maintain or promote bone formation
 New Osteoporosis Treatments Disclosures Mary L. Bouxsein, PhD Department of Orthopedic Surgery Harvard Medical School, Boston, MA Advisory Board: Research funding: Merck, Eli Lilly, Radius Merck, Amgen
New Osteoporosis Treatments Disclosures Mary L. Bouxsein, PhD Department of Orthopedic Surgery Harvard Medical School, Boston, MA Advisory Board: Research funding: Merck, Eli Lilly, Radius Merck, Amgen
Persistent post transplant hyperparathyroidism. Shiva Seyrafian IUMS-97/10/18-8/1/2019
 Persistent post transplant hyperparathyroidism Shiva Seyrafian IUMS-97/10/18-8/1/2019 normal weight =18-160 mg In HPT= 500-1000 mg 2 Epidemiology Mild 2 nd hyperparathyroidism (HPT) resolve after renal
Persistent post transplant hyperparathyroidism Shiva Seyrafian IUMS-97/10/18-8/1/2019 normal weight =18-160 mg In HPT= 500-1000 mg 2 Epidemiology Mild 2 nd hyperparathyroidism (HPT) resolve after renal
Treatment of Osteoporosis: IHFD 6 th March 2015
 Treatment of Osteoporosis: IHFD 6 th March 2015 Dr. John J. Carey, MB, MS, FACR, FRCPI, CCD. Consultant Physician Galway University Hospitals Associate Professor in Medicine, NUIG, Galway Vice-President
Treatment of Osteoporosis: IHFD 6 th March 2015 Dr. John J. Carey, MB, MS, FACR, FRCPI, CCD. Consultant Physician Galway University Hospitals Associate Professor in Medicine, NUIG, Galway Vice-President
Chau Nguyen, D.O. Rheumatologist Clinical Assistant Professor of Internal Medicine at Western University of Health Sciences
 Chau Nguyen, D.O Rheumatologist Clinical Assistant Professor of Internal Medicine at Western University of Health Sciences I do not have any relationship with the manufacturer of any commercial products
Chau Nguyen, D.O Rheumatologist Clinical Assistant Professor of Internal Medicine at Western University of Health Sciences I do not have any relationship with the manufacturer of any commercial products
Osteoporosis/Fracture Prevention
 Osteoporosis/Fracture Prevention NATIONAL GUIDELINE SUMMARY This guideline was developed using an evidence-based methodology by the KP National Osteoporosis/Fracture Prevention Guideline Development Team
Osteoporosis/Fracture Prevention NATIONAL GUIDELINE SUMMARY This guideline was developed using an evidence-based methodology by the KP National Osteoporosis/Fracture Prevention Guideline Development Team
A Review of Bone Health Issues in Oncology
 A Review of Bone Health Issues in Oncology David L. Kendler MD FRCPC CCD Professor of Medicine (Endocrinology) University of British Columbia Vancouver Canada Disclosures David Kendler has received research
A Review of Bone Health Issues in Oncology David L. Kendler MD FRCPC CCD Professor of Medicine (Endocrinology) University of British Columbia Vancouver Canada Disclosures David Kendler has received research
Page 1. Updates in Osteoporosis. I have no conflicts of interest. What is osteoporosis? What s New in Osteoporosis
 Updates in Osteoporosis Jeffrey A. Tice, MD Professor of Medicine Division of General Internal Medicine, University of California, San Francisco I have no conflicts of interest What s New in Osteoporosis
Updates in Osteoporosis Jeffrey A. Tice, MD Professor of Medicine Division of General Internal Medicine, University of California, San Francisco I have no conflicts of interest What s New in Osteoporosis
Osteoporosis: An Overview. Carolyn J. Crandall, MD, MS
 Osteoporosis: An Overview Carolyn J. Crandall, MD, MS Osteoporosis: An Overview Carolyn J. Crandall, MD, MS Professor of Medicine David Geffen School of Medicine at UCLA Objectives Review osteoporosis
Osteoporosis: An Overview Carolyn J. Crandall, MD, MS Osteoporosis: An Overview Carolyn J. Crandall, MD, MS Professor of Medicine David Geffen School of Medicine at UCLA Objectives Review osteoporosis
Ramzi Vareldzis, MD Avanelle Jack, MD Dept of Internal Medicine Section of Nephrology and Hypertension LSU Health New Orleans September 13, 2016
 Ramzi Vareldzis, MD Avanelle Jack, MD Dept of Internal Medicine Section of Nephrology and Hypertension LSU Health New Orleans September 13, 2016 1 MBD + CKD in Elderly patients Our focus for today: CKD
Ramzi Vareldzis, MD Avanelle Jack, MD Dept of Internal Medicine Section of Nephrology and Hypertension LSU Health New Orleans September 13, 2016 1 MBD + CKD in Elderly patients Our focus for today: CKD
Management of mineral and bone disorders in renal transplant recipients
 Nephrology 22, Suppl. 2 (2017) 65 69 Management of mineral and bone disorders in renal transplant recipients MATTHEW J DAMASIEWICZ 1,3 and PETER R EBELING 2,3,4 Departments of 1 Nephrology, and 2 Endocrinology,
Nephrology 22, Suppl. 2 (2017) 65 69 Management of mineral and bone disorders in renal transplant recipients MATTHEW J DAMASIEWICZ 1,3 and PETER R EBELING 2,3,4 Departments of 1 Nephrology, and 2 Endocrinology,
Controversies in Osteoporosis Management
 Controversies in Osteoporosis Management 2018 Northwest Rheumatism Society Meeting Portland, OR April 28, 2018 Michael R. McClung, MD, FACP Director, Oregon Osteoporosis Center Portland, Oregon, USA Institute
Controversies in Osteoporosis Management 2018 Northwest Rheumatism Society Meeting Portland, OR April 28, 2018 Michael R. McClung, MD, FACP Director, Oregon Osteoporosis Center Portland, Oregon, USA Institute
Outline. Osteoporosis Definition DXA* Osteoporosis is Common. Brittle bones: Pitfalls in the evaluation and management of osteoporosis
 Brittle bones: Pitfalls in the evaluation and management of osteoporosis Sri Harsha Tella, MD CCD Department of Internal Medicine Division of Endocrinology, Diabetes and Metabolism University of South
Brittle bones: Pitfalls in the evaluation and management of osteoporosis Sri Harsha Tella, MD CCD Department of Internal Medicine Division of Endocrinology, Diabetes and Metabolism University of South
Osteoporosis Agents Drug Class Prior Authorization Protocol
 Osteoporosis Agents Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed through review of
Osteoporosis Agents Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed through review of
Monitoring Osteoporosis Therapy
 Monitoring Osteoporosis Therapy SUZANNE MORIN DEPT OF MEDICINE, DIVISION OF GENERAL INTERNAL MEDICINE, MUHC CENTRE FOR OUTCOMES RESEARCH AND EVALUATION, RI MUHC November 2017 Conflict of Interest Disclosures
Monitoring Osteoporosis Therapy SUZANNE MORIN DEPT OF MEDICINE, DIVISION OF GENERAL INTERNAL MEDICINE, MUHC CENTRE FOR OUTCOMES RESEARCH AND EVALUATION, RI MUHC November 2017 Conflict of Interest Disclosures
Updates in Osteoporosis
 Updates in Osteoporosis Jeffrey A. Tice, MD Associate Professor of Medicine Division of General Internal Medicine, University of California, San Francisco I have no conflicts of interest What s New in
Updates in Osteoporosis Jeffrey A. Tice, MD Associate Professor of Medicine Division of General Internal Medicine, University of California, San Francisco I have no conflicts of interest What s New in
Osteoporosis: How to Manage Long- Term Use of Bisphosphonates AKA Now What? David E Feinstein, DO, CCD November 15 th, 2017
 Osteoporosis: How to Manage Long- Term Use of Bisphosphonates AKA Now What? David E Feinstein, DO, CCD November 15 th, 2017 Introduction A fracture due to OP occurs every 3 seconds around the world. 1
Osteoporosis: How to Manage Long- Term Use of Bisphosphonates AKA Now What? David E Feinstein, DO, CCD November 15 th, 2017 Introduction A fracture due to OP occurs every 3 seconds around the world. 1
Bone Disease after Kidney Transplantation
 Bone Disease after Kidney Transplantation BTS March 2018 Dr Arif Khwaja PhD, FRCP Sheffield Kidney Institute Clinical case 47 year old female FSGS DBD 2007 egfr 25mls/min. Sirolimus, Azathioprine and prednisolone
Bone Disease after Kidney Transplantation BTS March 2018 Dr Arif Khwaja PhD, FRCP Sheffield Kidney Institute Clinical case 47 year old female FSGS DBD 2007 egfr 25mls/min. Sirolimus, Azathioprine and prednisolone
From Fragile to Firm. Monika Starosta MD. Advocate Medical Group
 From Fragile to Firm Monika Starosta MD Advocate Medical Group Bone Remodeling 10% remodeled each year Calcium homoeostasis Maintain Mechanical strength Replace Osteocytes Release Growth Factors Bone remodeling
From Fragile to Firm Monika Starosta MD Advocate Medical Group Bone Remodeling 10% remodeled each year Calcium homoeostasis Maintain Mechanical strength Replace Osteocytes Release Growth Factors Bone remodeling
Download slides:
 Download slides: https://www.tinyurl.com/m67zcnn https://tinyurl.com/kazchbn OSTEOPOROSIS REVIEW AND UPDATE Boca Raton Regional Hospital Internal Medicine Conference 2017 Benjamin Wang, M.D., FRCPC Division
Download slides: https://www.tinyurl.com/m67zcnn https://tinyurl.com/kazchbn OSTEOPOROSIS REVIEW AND UPDATE Boca Raton Regional Hospital Internal Medicine Conference 2017 Benjamin Wang, M.D., FRCPC Division
Osteoporosis update. Dr. Claire Vandevelde Consultant Rheumatologist, LTHT
 Osteoporosis update Dr. Claire Vandevelde Consultant Rheumatologist, LTHT Outline Background BMD Tools for assessing fracture risk Case study Denosumab Treatment breaks BMD BMD predicts fracture risk but
Osteoporosis update Dr. Claire Vandevelde Consultant Rheumatologist, LTHT Outline Background BMD Tools for assessing fracture risk Case study Denosumab Treatment breaks BMD BMD predicts fracture risk but
New Therapeutic Directions: Osteoanabolic and Antiresorptive Therapy in Combination Therapy and in Sequence
 New Therapeutic Directions: Osteoanabolic and Antiresorptive Therapy in Combination Therapy and in Sequence John P. Bilezikian, MD, PhD(hon), MACE Silberberg Professor of Medicine Vice-Chair for International
New Therapeutic Directions: Osteoanabolic and Antiresorptive Therapy in Combination Therapy and in Sequence John P. Bilezikian, MD, PhD(hon), MACE Silberberg Professor of Medicine Vice-Chair for International
Bone strength is proportional to bone mass, measured with DXA. Bone turnover markers indicate the status of bone quality.
 Bone strength is proportional to bone mass, measured with DXA Bone quality depend on bone architecture, rate of bone turnover, quality of bone matrix. Bone turnover markers indicate the status of bone
Bone strength is proportional to bone mass, measured with DXA Bone quality depend on bone architecture, rate of bone turnover, quality of bone matrix. Bone turnover markers indicate the status of bone
Osteoporosis Update. Case 2. Case 1: Monday morning, 8:15
 Osteoporosis Update Laura E. Ryan, MD Assistant Director for Special Programs Center for Women s Health Clinical Assistant Professor of Medicine Division of Endocrinology, Diabetes and Metabolism The Ohio
Osteoporosis Update Laura E. Ryan, MD Assistant Director for Special Programs Center for Women s Health Clinical Assistant Professor of Medicine Division of Endocrinology, Diabetes and Metabolism The Ohio
What is Osteoporosis?
 What is Osteoporosis? 2000 NIH Definition A skeletal disorder characterized by compromised bone strength predisposing a person to an increased risk of fracture. Bone strength reflects the integration of
What is Osteoporosis? 2000 NIH Definition A skeletal disorder characterized by compromised bone strength predisposing a person to an increased risk of fracture. Bone strength reflects the integration of
Agents that Affect Bone & Mineral Homeostasis
 Agents that Affect Bone & Mineral Homeostasis 1 Agents that Affect Bone & Mineral Homeostasis Calcium and phosphate are the major mineral constituents of bone. They are also two of the most important minerals
Agents that Affect Bone & Mineral Homeostasis 1 Agents that Affect Bone & Mineral Homeostasis Calcium and phosphate are the major mineral constituents of bone. They are also two of the most important minerals
Osteoporosis Medications: A Case-Based Discussion. Laila S. Tabatabai, MD August 5, 2017
 Osteoporosis Medications: A Case-Based Discussion Laila S. Tabatabai, MD August 5, 2017 Disclosures Eli Lilly Radius Objectives Determine which patients with low bone density require treatment, along with
Osteoporosis Medications: A Case-Based Discussion Laila S. Tabatabai, MD August 5, 2017 Disclosures Eli Lilly Radius Objectives Determine which patients with low bone density require treatment, along with
OSTEOPOROSIS IN MEN. Nelson B. Watts, MD OSTEOPOROSIS AND BONE HEALTH SERVICES CINCINNATI, OHIO
 OSTEOPOROSIS IN MEN Nelson B. Watts, MD OSTEOPOROSIS AND BONE HEALTH SERVICES CINCINNATI, OHIO DISCLOSURES Speakers Bureau: Amgen, Radius Consultant: Abbvie, Amgen, Janssen, Radius, Sanofi Watts NB et
OSTEOPOROSIS IN MEN Nelson B. Watts, MD OSTEOPOROSIS AND BONE HEALTH SERVICES CINCINNATI, OHIO DISCLOSURES Speakers Bureau: Amgen, Radius Consultant: Abbvie, Amgen, Janssen, Radius, Sanofi Watts NB et
Parathyroid Hormone Analogs
 Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.36 Subject: Parathyroid Hormone Analogs Page: 1 of 6 Last Review Date: September 15, 2017 Parathyroid
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.36 Subject: Parathyroid Hormone Analogs Page: 1 of 6 Last Review Date: September 15, 2017 Parathyroid
Pharmacy Management Drug Policy
 SUBJECT: - Forteo (teriparatide), Prolia (denosumab), Tymlos (abaloparatide) POLICY NUMBER: Pharmacy-35 EFFECTIVE DATE: 9/07 LAST REVIEW DATE: 9/29/2017 If the member s subscriber contract excludes coverage
SUBJECT: - Forteo (teriparatide), Prolia (denosumab), Tymlos (abaloparatide) POLICY NUMBER: Pharmacy-35 EFFECTIVE DATE: 9/07 LAST REVIEW DATE: 9/29/2017 If the member s subscriber contract excludes coverage
SpongeBone Menopants*
 SpongeBone Menopants* Adam Fershko, MD, FACP Kettering Health Network *Postmenopausal Osteoporosis Objectives O Epidemiology O Clinical significance O Pathophysiology O Screening and Diagnosis O Treatment
SpongeBone Menopants* Adam Fershko, MD, FACP Kettering Health Network *Postmenopausal Osteoporosis Objectives O Epidemiology O Clinical significance O Pathophysiology O Screening and Diagnosis O Treatment
ACP Colorado-Evidence Based Management of Osteoporosis
 ACP Colorado-Evidence Based Management of Osteoporosis Micol S. Rothman, MD Associate Professor of Medicine and Radiology Clinical Director Metabolic Bone Program University of Colorado School of Medicine
ACP Colorado-Evidence Based Management of Osteoporosis Micol S. Rothman, MD Associate Professor of Medicine and Radiology Clinical Director Metabolic Bone Program University of Colorado School of Medicine
Renata Caudarella. Fondazione Ettore Sansavini per la Ricerca Scientifica (Health Science Foundation ) - GVM Care & Research
 - GVM Care & Research") Renata Caudarella Fondazione Ettore Sansavini per la Ricerca Scientifica (Health Science Foundation ) - GVM Care & Research Introduc/on During the past two decades, many randomized controlled trials (RCTs)
Renata Caudarella Fondazione Ettore Sansavini per la Ricerca Scientifica (Health Science Foundation ) - GVM Care & Research Introduc/on During the past two decades, many randomized controlled trials (RCTs)
HRT and Risedronate Combined Anabolic and Antiresorptive Therapy
 Optimizing Combined and Sequential Osteoanabolic and Antiresorptive Therapy Benjamin Leder, M.D. Endocrine Unit Massachusetts General Hospital Boston, MA Antiresorptive and Osteoanabolic Therapies Increase
Optimizing Combined and Sequential Osteoanabolic and Antiresorptive Therapy Benjamin Leder, M.D. Endocrine Unit Massachusetts General Hospital Boston, MA Antiresorptive and Osteoanabolic Therapies Increase
Page 1. Diagnosis and Treatment of Osteoporosis: What s New and Controversial in 2018? What s New in Osteoporosis
 Diagnosis and Treatment of Osteoporosis: What s New and Controversial in 2018? Douglas C. Bauer, MD Professor of Medicine and Epidemiology & Biostatistics University of California, San Francisco What s
Diagnosis and Treatment of Osteoporosis: What s New and Controversial in 2018? Douglas C. Bauer, MD Professor of Medicine and Epidemiology & Biostatistics University of California, San Francisco What s
NAMS Practice Pearl. Use of Drug Holidays in Women Taking Bisphosphonates. Released April 1, 2013
 NAMS Practice Pearl Use of Drug Holidays in Women Taking Bisphosphonates Released April 1, 2013 Dima L. Diab, MD 1, and Nelson B. Watts, MD 2 ( 1 Cincinnati VA Medical Center, Cincinnati, OH, 2 Mercy Health
NAMS Practice Pearl Use of Drug Holidays in Women Taking Bisphosphonates Released April 1, 2013 Dima L. Diab, MD 1, and Nelson B. Watts, MD 2 ( 1 Cincinnati VA Medical Center, Cincinnati, OH, 2 Mercy Health
Diagnosis and Treatment of Osteoporosis: What s New and Controversial in ? What s New in Osteoporosis
 Diagnosis and Treatment of Osteoporosis: What s New and Controversial in 2018-19? What s New in Osteoporosis The crisis in treatment and compliance Douglas C. Bauer, MD Professor of Medicine and Epidemiology
Diagnosis and Treatment of Osteoporosis: What s New and Controversial in 2018-19? What s New in Osteoporosis The crisis in treatment and compliance Douglas C. Bauer, MD Professor of Medicine and Epidemiology
Management of postmenopausal osteoporosis
 Management of postmenopausal osteoporosis Yeap SS, Hew FL, Chan SP, on behalf of the Malaysian Osteoporosis Society Committee Working Group for the Clinical Guidance on the Management of Osteoporosis,
Management of postmenopausal osteoporosis Yeap SS, Hew FL, Chan SP, on behalf of the Malaysian Osteoporosis Society Committee Working Group for the Clinical Guidance on the Management of Osteoporosis,
The Role of the Laboratory in Metabolic Bone Disease
 The Role of the Laboratory in Metabolic Bone Disease Howard Morris PhD, FAACB, FFSc(RCPA) President, IFCC Professor of Medical Sciences, University of South Australia, Clinical Scientist, SA Pathology
The Role of the Laboratory in Metabolic Bone Disease Howard Morris PhD, FAACB, FFSc(RCPA) President, IFCC Professor of Medical Sciences, University of South Australia, Clinical Scientist, SA Pathology
Osteoporosis: A Tale of 3 Task Forces!
 Osteoporosis: A Tale of 3 Task Forces! Robert A. Adler, MD McGuire Veterans Affairs Medical Center Virginia Commonwealth University Richmond, Virginia, USA Disclosures The opinions are those of the speaker
Osteoporosis: A Tale of 3 Task Forces! Robert A. Adler, MD McGuire Veterans Affairs Medical Center Virginia Commonwealth University Richmond, Virginia, USA Disclosures The opinions are those of the speaker
Division of Nephrology, Bone and Mineral Metabolism
 Osteoporosis and fractures Measurement of bone density Diagnosis of osteoporosis Bone biopsy Newer therapies and challenges Osteoporosis: Definition Normal Bone Osteoporotic Bone NIH Definition:..A skeletal
Osteoporosis and fractures Measurement of bone density Diagnosis of osteoporosis Bone biopsy Newer therapies and challenges Osteoporosis: Definition Normal Bone Osteoporotic Bone NIH Definition:..A skeletal
Secondary Hyperparathyroidism: Where are we now?
 Secondary Hyperparathyroidism: Where are we now? Dylan M. Barth, Pharm.D. PGY-1 Pharmacy Resident Mayo Clinic 2017 MFMER slide-1 Objectives Identify risk factors for the development of complications caused
Secondary Hyperparathyroidism: Where are we now? Dylan M. Barth, Pharm.D. PGY-1 Pharmacy Resident Mayo Clinic 2017 MFMER slide-1 Objectives Identify risk factors for the development of complications caused
A KL/R / AN A K/O / P O G G
 Outline and New Treatments on the Horizon Steven R. Cummings, MD CPMC and UCSF San Francisco Coordinating Center Support from Lilly and Amgen New treatments, new mechanisms of action Cathepsin K inhibition
Outline and New Treatments on the Horizon Steven R. Cummings, MD CPMC and UCSF San Francisco Coordinating Center Support from Lilly and Amgen New treatments, new mechanisms of action Cathepsin K inhibition
Do We Do Too Many Parathyroidectomies in Dialysis? Sagar Nigwekar MD, MMSc Massachusetts General Hospital
 Do We Do Too Many Parathyroidectomies in Dialysis? Sagar Nigwekar MD, MMSc Massachusetts General Hospital E-mail: snigwekar@mgh.harvard.edu March 13, 2017 Disclosures statement: Consultant: Allena, Becker
Do We Do Too Many Parathyroidectomies in Dialysis? Sagar Nigwekar MD, MMSc Massachusetts General Hospital E-mail: snigwekar@mgh.harvard.edu March 13, 2017 Disclosures statement: Consultant: Allena, Becker
Therapeutic Updates in the Prevention and Treatment of Osteoporosis
 Therapeutic Updates in the Prevention and Treatment of Osteoporosis 2013 Fall Managed Care Forum Las Vegas November 15, 2013 Steven T Harris MD FACP Clinical Professor of Medicine University of California,
Therapeutic Updates in the Prevention and Treatment of Osteoporosis 2013 Fall Managed Care Forum Las Vegas November 15, 2013 Steven T Harris MD FACP Clinical Professor of Medicine University of California,
Hot Topics in Osteoporosis and Fracture Prevention
 Hot Topics in Osteoporosis and Fracture Prevention Sid Feldman, MD CCFP (COE) FCFP Sandra Kim, MD, FRCPC November 15, 2018 Family Medicine Forum, Toronto Faculty/Presenter Disclosure Faculty: Sid Feldman
Hot Topics in Osteoporosis and Fracture Prevention Sid Feldman, MD CCFP (COE) FCFP Sandra Kim, MD, FRCPC November 15, 2018 Family Medicine Forum, Toronto Faculty/Presenter Disclosure Faculty: Sid Feldman
Refracture Prevention The Role of Primary Care
 MonashHealth Refracture Prevention The Role of Primary Care Professor Peter R Ebeling AO MBBS MD FRACP Head, Department of Medicine School for Clinical Sciences Monash Health Translation Precinct Monash
MonashHealth Refracture Prevention The Role of Primary Care Professor Peter R Ebeling AO MBBS MD FRACP Head, Department of Medicine School for Clinical Sciences Monash Health Translation Precinct Monash
AACE. Osteoporosis Treatment: Then and Now
 AACE 25 th Annual Scientific and Clinical Congress Osteoporosis Treatment: Then and Now Orlando, FL May 28, 2016 Michael R. McClung, MD Oregon Osteoporosis Center Portland, Oregon, USA Disclosures I am
AACE 25 th Annual Scientific and Clinical Congress Osteoporosis Treatment: Then and Now Orlando, FL May 28, 2016 Michael R. McClung, MD Oregon Osteoporosis Center Portland, Oregon, USA Disclosures I am
Parathyroid Hormone Analog for Osteoporosis Prior Authorization with Quantity Limit Criteria Program Summary
 Parathyroid Hormone Analog for Osteoporosis Prior Authorization with Quantity Limit Criteria Program Summary This prior authorization program applies to Commercial, NetResults A series, NetResults F series
Parathyroid Hormone Analog for Osteoporosis Prior Authorization with Quantity Limit Criteria Program Summary This prior authorization program applies to Commercial, NetResults A series, NetResults F series
Page 1. New Developments in Osteoporosis. What s New in Osteoporosis
 New Developments in Osteoporosis Eliseo J. Pérez-Stable MD Professor of Medicine Division of General Internal Medicine Department of Medicine July 4, 2013 Declaration of full disclosure: No conflict of
New Developments in Osteoporosis Eliseo J. Pérez-Stable MD Professor of Medicine Division of General Internal Medicine Department of Medicine July 4, 2013 Declaration of full disclosure: No conflict of
Page 1. Current and Emerging Strategies What s New in Osteoporosis. Osteoporosis. What is Osteoporosis? Traditional Risk Factors for Fracture
 Current and Emerging Strategies for Osteoporosis What s New in Osteoporosis Risk stratification Douglas C. Bauer, MD University of California, San Francisco Under recognition and poor compliance New potential
Current and Emerging Strategies for Osteoporosis What s New in Osteoporosis Risk stratification Douglas C. Bauer, MD University of California, San Francisco Under recognition and poor compliance New potential
Management of Osteoporosis in Chronic Kidney Disease
 doi: 10.2169/internalmedicine.8618-16 Intern Med Advance Publication http://internmed.jp REVIEW ARTICLE Management of Osteoporosis in Chronic Kidney Disease Kosaku Nitta 1, Aiji Yajima 1 and Ken Tsuchiya
doi: 10.2169/internalmedicine.8618-16 Intern Med Advance Publication http://internmed.jp REVIEW ARTICLE Management of Osteoporosis in Chronic Kidney Disease Kosaku Nitta 1, Aiji Yajima 1 and Ken Tsuchiya
Annual Rheumatology & Therapeutics Review for Organizations & Societies
 Annual Rheumatology & Therapeutics Review for Organizations & Societies Osteoporosis in Men: An Update on the Epidemiology, Clinical Evaluation Current Treatments and Treatments in Development Learning
Annual Rheumatology & Therapeutics Review for Organizations & Societies Osteoporosis in Men: An Update on the Epidemiology, Clinical Evaluation Current Treatments and Treatments in Development Learning
Overview. Bone Biology Osteoporosis Osteomalacia Paget s Disease Cases. People Centred Positive Compassion Excellence
 Overview Osteoporosis and Metabolic Bone Disease Dr Chandini Rao Consultant Rheumatologist Bone Biology Osteoporosis Osteomalacia Paget s Disease Cases Bone Biology Osteoporosis Increased bone remodelling
Overview Osteoporosis and Metabolic Bone Disease Dr Chandini Rao Consultant Rheumatologist Bone Biology Osteoporosis Osteomalacia Paget s Disease Cases Bone Biology Osteoporosis Increased bone remodelling
Long-term Osteoporosis Therapy What To Do After 5 Years?
 Long-term Osteoporosis Therapy What To Do After 5 Years? Developing a Long-term Management Plan North American Menopause Society Philadelphia, PA October 11, 2017 Michael R. McClung, MD, FACP Institute
Long-term Osteoporosis Therapy What To Do After 5 Years? Developing a Long-term Management Plan North American Menopause Society Philadelphia, PA October 11, 2017 Michael R. McClung, MD, FACP Institute
Skeletal Manifestations
 Skeletal Manifestations of Metabolic Bone Disease Mishaela R. Rubin, MD February 21, 2008 The Three Ages of Women Gustav Klimt 1905 1 Lecture Outline Osteoporosis epidemiology diagnosis secondary causes
Skeletal Manifestations of Metabolic Bone Disease Mishaela R. Rubin, MD February 21, 2008 The Three Ages of Women Gustav Klimt 1905 1 Lecture Outline Osteoporosis epidemiology diagnosis secondary causes
THE GROWING GAP IN OSTEOPOROSIS TREATMENT
 THE GROWING GAP IN OSTEOPOROSIS TREATMENT Sundeep Khosla, M.D. Mayo Clinic, Rochester, MN DISCLOSURES SUNDEEP KHOSLA, M.D. NONE 1 OVERALL CONCLUSIONS There has been remarkable progress in our understanding
THE GROWING GAP IN OSTEOPOROSIS TREATMENT Sundeep Khosla, M.D. Mayo Clinic, Rochester, MN DISCLOSURES SUNDEEP KHOSLA, M.D. NONE 1 OVERALL CONCLUSIONS There has been remarkable progress in our understanding
Drugs Affecting Bone. Rosa McCarty PhD. Department of Pharmacology & Therapeutics
 Drugs Affecting Bone Rosa McCarty PhD Department of Pharmacology & Therapeutics rmccarty@unimelb.edu.au Objectives At the end of this lecture you should have gained: An understanding of bone metabolism
Drugs Affecting Bone Rosa McCarty PhD Department of Pharmacology & Therapeutics rmccarty@unimelb.edu.au Objectives At the end of this lecture you should have gained: An understanding of bone metabolism
Pharmacy Management Drug Policy
 SUBJECT: - Forteo (teriparatide), Prolia (denosumab), Tymlos (abaloparatide), Boniva injection (Ibandronate) POLICY NUMBER: Pharmacy-35 EFFECTIVE DATE: 9/07 LAST REVIEW DATE: 10/15/2018 If the member s
SUBJECT: - Forteo (teriparatide), Prolia (denosumab), Tymlos (abaloparatide), Boniva injection (Ibandronate) POLICY NUMBER: Pharmacy-35 EFFECTIVE DATE: 9/07 LAST REVIEW DATE: 10/15/2018 If the member s
Calcium Nephrolithiasis and Bone Health. Noah S. Schenkman, MD
 Calcium Nephrolithiasis and Bone Health Noah S. Schenkman, MD Associate Professor of Urology and Residency Program Director, University of Virginia Health System; Charlottesville, Virginia Objectives:
Calcium Nephrolithiasis and Bone Health Noah S. Schenkman, MD Associate Professor of Urology and Residency Program Director, University of Virginia Health System; Charlottesville, Virginia Objectives:
Task Force Co-Chairs. Members
 Managing Osteoporosis Patients After Long-Term Bisphosphonate Treatment Report of a Task Force* of the American Society for Bone and Mineral Research Robert A. Adler, MD Task Force Co-Chairs Ghada El-Hajj
Managing Osteoporosis Patients After Long-Term Bisphosphonate Treatment Report of a Task Force* of the American Society for Bone and Mineral Research Robert A. Adler, MD Task Force Co-Chairs Ghada El-Hajj