Absent: Director Layla P. Suleiman Gonzalez, PhD, JD (1)
|
|
|
- Ella Parks
- 5 years ago
- Views:
Transcription
1 Minutes of the meeting of the Quality and Patient Safety Committee of the Board of Directors of the Cook County Health and Hospitals System held Friday, January 18, 2019 at the hour of 10:00 A.M. at 1950 W. Polk Street, in Conference Room 5301, Chicago, Illinois. I. Attendance/Call to Order Chair Gugenheim called the meeting to order. Present: Chair Ada Mary Gugenheim and Director Mary Driscoll, RN, MPH (2) Board Chair M. Hill Hammock (ex-officio) and Directors Heather M. Prendergast, MD, MS, MPH and Mary B. Richardson-Lowry Telephonically Present: Karen Kim, MD and Patricia Merryweather (Non-Director Members) Patrick T. Driscoll, Jr. (Non-Director Member) Absent: Director Layla P. Suleiman Gonzalez, PhD, JD (1) Additional attendees and/or presenters were: Debra Carey Deputy Chief Executive Officer, Operations Trevor Lewis, MD John H. Stroger, Jr. Hospital of Cook County Kent Ray Associate General Counsel Deborah Santana Secretary to the Board John Jay Shannon, MD Chief Executive Officer Ronald Wyatt, MD Chief Quality Officer II. Public Speakers Chair Gugenheim asked the Secretary to call upon the registered public speakers. The Secretary called upon the following registered public speaker: 1. George Blakemore Concerned Citizen III. Report from Chief Quality Officer A. Regulatory and Accreditation Updates B. Metrics (Attachment #1) Dr. Ronald Wyatt, Chief Quality Officer, provided an overview of the metrics. The Committee reviewed and discussed the information. IV. Action Items A. Approve appointments and reappointments of Stroger Hospital Department Chair(s) and Division Chair(s) There were no appointments/reappointments presented for the Committee s consideration. Page 1 of 54
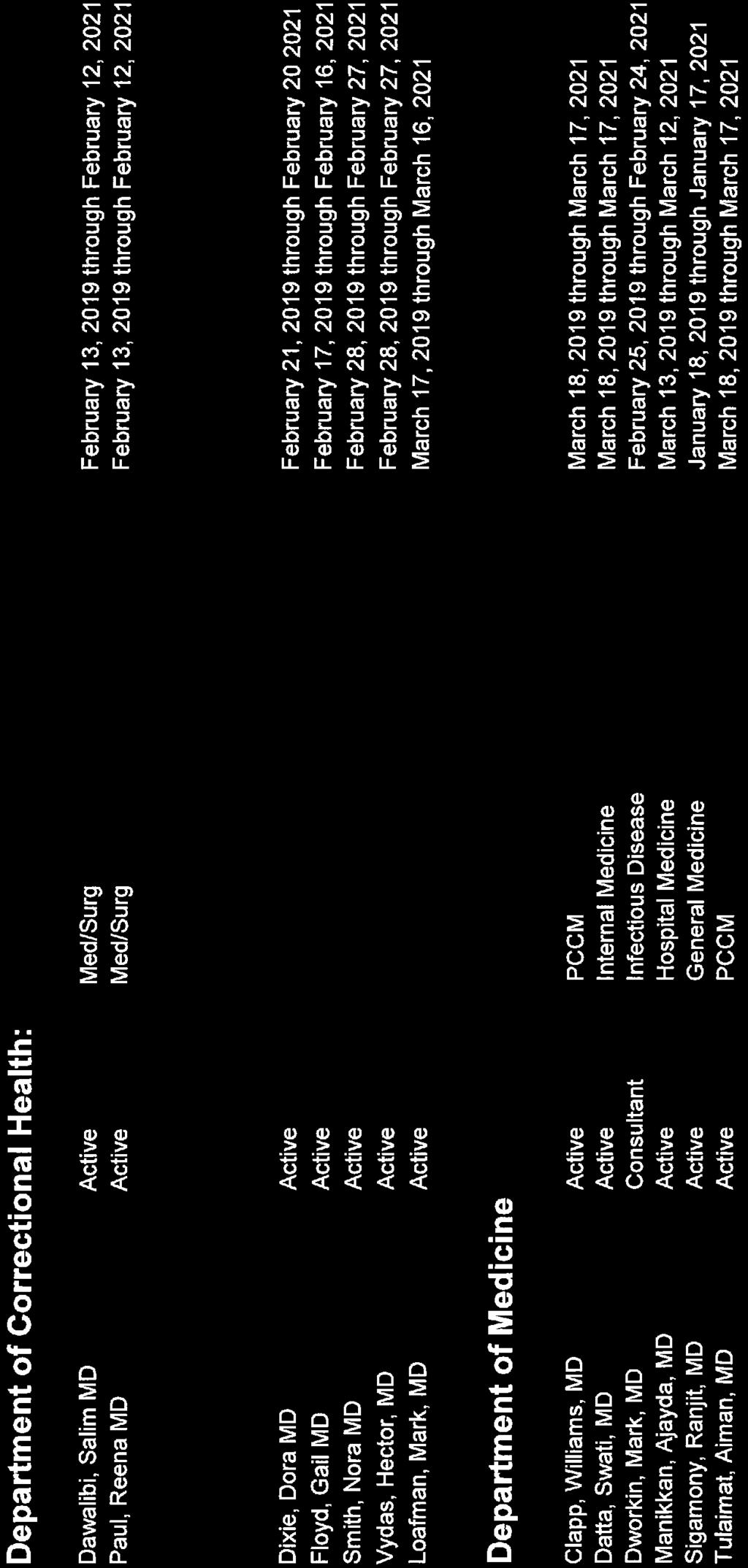
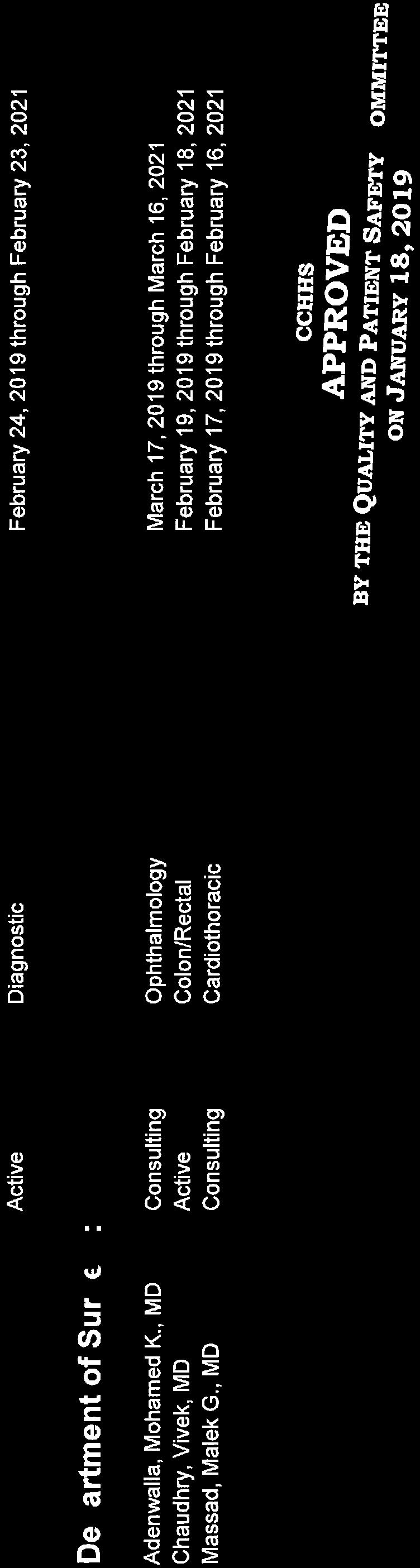
2 Minutes of the Meeting of the Quality and Patient Safety Committee Friday, January 18, 2019 Page 2 IV. Action Items (continued) B. Executive Medical Staff (EMS) Committees of Provident Hospital of Cook County and John H. Stroger, Jr. Hospital of Cook County i. Receive reports from EMS Presidents ii. Approve Medical Staff Appointments/Reappointments/Changes (Attachment #2) Dr. Trevor Lewis, President of the EMS of John H. Stroger, Jr. Hospital of Cook County, presented the medical staff appointments/reappointments/changes for the Committee s consideration. He reminded the Committee that the annual meeting of the Medical Staff will be held on January 22 nd at 4:00 P.M. Dr. Valerie Hansbrough, President of the EMS of Provident Hospital of Cook County, was unable to attend the meeting. Director Driscoll, seconded by Chair Gugenheim, moved to approve the Medical Staff Appointments/Re-appointments/Changes for John H. Stroger, Jr. Hospital of Cook County. THE MOTION CARRIED UNANIMOUSLY. Director Driscoll, seconded by Chair Gugenheim, moved to approve the Medical Staff Appointments/Re-appointments/Changes for Provident Hospital of Cook County. THE MOTION CARRIED UNANIMOUSLY. C. Minutes of the Quality and Patient Safety Committee Meeting, December 14, 2018 Director Driscoll, seconded by Chair Gugenheim, moved to accept the Minutes of the Quality and Patient Safety Committee Meeting of December 14, THE MOTION CARRIED UNANIMOUSLY. D. Any items listed under Sections IV and VI V. Recommendations, Discussion / Information Item A. Strategic planning discussion: Quality Measures (Attachment #3) Dr. Wyatt provided an overview of the presentation, which included information on the following subjects: Definition of Health Care Quality Meaningful Measures Framework, Goals and Objectives Most Critical Measures Areas Aim: Promote Effective Prevention and Treatment of Chronic Disease Centers for Medicare and Medicaid Services (CMS) Star Ratings Measures and Data Star Quality Action Plan Star Quality Steering Committee CMS Measure Focused Finding Workgroup Proposed Structure Next Steps Page 2 of 54
3 V. Recommendations, Discussion / Information Item A. Strategic planning discussion: Quality Measures (continued) Minutes of the Meeting of the Quality and Patient Safety Committee Friday, January 18, 2019 Page 3 During the review of the measures and data, Board Chair Hammock recommended that the column in the data charts that show the comparison to national mean should instead reflect whether Stroger Hospital s results are better or otherwise than the national mean, rather than above or below. Following the discussion, Board Chair Hammock observed that this is a great programmatic approach; however, he did not hear a lot about financial impact. He thinks the organization has to be realistic in the following two (2) ways: 1) each initiative needs to have a candid cost benefit review; and 2) in cooperation with the Chief Financial Officer, the administration should determine a sum of money that could be used to fund key initiatives, and get that on the budget prospect for the year. VI. Closed Meeting Items A. Medical Staff Appointments/Re-appointments/Changes B. Claims, Litigation and Quality and Patient Safety Matters C. Matters protected under the federal Patient Safety and Quality Improvement Act of 2005 and the Health Insurance Portability and Accountability Act of 1996 The Committee did not recess into a closed meeting. VII. Adjourn As the agenda was exhausted, Chair Gugenheim declared the meeting ADJOURNED. Respectfully submitted, Quality and Patient Safety Committee of the Board of Directors of the Cook County Health and Hospitals System Attest: XXXXXXXXXXXXXXXXXXXXXX Ada Mary Gugenheim, Chair XXXXXXXXXXXXXXXXXXXXXX Deborah Santana, Secretary Requests/follow-up: Request: A request was made regarding the column in the strategic planning presentation data charts that show the comparison to national mean - they should instead reflect whether Stroger Hospital s results are better or otherwise than the national mean, rather than above or below. Page 3 Page 3 of 54
4 Cook County Health and Hospitals System Quality and Patient Safety Committee Meeting Friday, January 18, 2019 ATTACHMENT #1 Page 4 of 54
5 QPS Quality Dashboard January 18, 2019 Page 5 of 54

6 Illinois Avg. National Avg Page 6 of 54 2
7 Page 7 of 54 3
8 Page 8 of 54 4
9 Page 9 of 54 5

10 Page 10 of 54 6
11 SIR (Standardized Infection Ratio) is a summary measure which compares the actual number of Healthcare Associated Infections (HAI) in a facility with the baseline data for standard population. SIR > 1.0 indicates more HAIs were observed than predicted, conversely SIR of < 1.0 indicates that fewer HAIs were observed than predicted. Page 11 of 54 7
12 Page 12 of 54 8
13 Page 13 of 54 9
14 Page 14 of 54 10
15 Cook County Health and Hospitals System Quality and Patient Safety Committee Meeting Friday, January 18, 2019 ATTACHMENT #2 Page 15 of 54


16 Page 16 of 54

17 Page 17 of 54

18 Page 18 of 54

19 Page 19 of 54

20 Page 20 of 54


21 Page 21 of 54



22 Page 22 of 54

23 Page 23 of 54
24 Cook County Health and Hospitals System Quality and Patient Safety Committee Meeting Friday, January 18, 2019 ATTACHMENT #3 Page 24 of 54
25 COOK COUNTY HEALTH Meaningful Metrics Ronald Wyatt MD MHA January 18, 2019 Page 25 of 54
26 Page 26 of 54 2

27 Meaningful Measures Page 27 of 54 3
28 Meaningful Measures Framework Meaningful Measure Areas Achieve: High quality healthcare Meaningful outcomes for patients Criteria meaningful for patients and actionable for providers Draws on measure work by: Health Care Payment Learning and Action Network National Quality Forum High Impact Outcomes National Academies of Medicine IOM Vital Signs Core Metrics Includes perspectives from experts and external stakeholders: Core Quality Measures Collaborative Agency for Healthcare Research and Quality Quality Measures Page 28 of 54 4

29 Meaningful Measures Page 29 of 54 Source: CMS 5

30 Meaningful Measures Goals Page 30 of 54 6
31 Meaningful Measures Objectives Page 31 of 54 Source: AHIMA/CMS 7

32 The Most Critical Measures Areas Page 32 of 54 Source: AHIMA/CMS 8

33 Aim: Promote Effective Prevention and Treatment of Chronic Disease Page 33 of 54 Source: CMS 9

34 CMS STAR RATINGS Page 34 of 54 10

35 Page 35 of 54 HVBP=Hospital Value-Based Purchasing Source: CMS 11

36 Measure Group Score Results and Weights for the Overall Hospital Quality Star Rating JOHN H STROGER JR HOSPITAL Page 36 of 54 12
37 Mortality Measure ID Measure Name Stroger Result on Hospital Compare National Mean Comparison to National Mean MORT-30-AMI Myocardial Infarction 11.9% 13.2% Better MORT-30-COPD Chronic Lung Disease 7.7% 8.4% Better MORT-30-HF Heart Failure 10.8% 11.8% Better MORT-30-PN Pneumonia 13.4% 15.9% Better MORT-30-STK Stroke 12.8% 14.3% Better PSI-4-SURG-COMP Death Rate Among Surgical Inpatients with Serious Treatable Complications Worse MORT-30-CABG Coronary Artery Bypass Graft (CABG) 30-Day Mortality Rate N/A 3.2% -- Page 37 of 54 13
38 Measure ID Measure Name Stroger Safety of Care Result on Hospital Compare HAI-1 HAI-2 HAI-3 HAI-4 Safety of Care Central Line Associated Blood Stream Infection Catheter Associated Urinary Tract Infection Surgical Site Infection from Colon Surgery (SSI-colon) Surgical Site Infection from Abdominal Hysterectomy (SSIabdominal hysterectomy) National Mean Comparison to National Mean Worse Better Better Worse HAI-5 MRSA Bacteremia Better HAI-6 Clostridium difficile (C.difficile) Better COMP-HIP-KNEE PSI-90 Hospital-Level Risk- Standardized Complication Rate (RSCR) Following Elective Primary Total Hip Arthroplasty (THA) and Total Knee Arthroplasty (TKA)¹ Patient Safety and Adverse Events Composite Page 38 of 54 N/A Worse 14
39 Readmissions Measure ID Measure Name Stroger Result on Hospital Compare National Mean Comparison To National Mean EDAC -30-AMI Myocardial Infarction Worse READM-30-COPD Chronic Lung Disease 20.4% 19.6% Worse EDAC-30-HF Heart Failure Better EDAC-30-PN Pneumonia Worse READM-30-STK Stroke 11.7% 11.9% Same READM-30-HOSP Hospital-wide, all cause 16.9% 15.3% Worse OP-32 Facility Seven-Day Risk- Standardized Hospital Visit Rate after Outpatient Colonoscopy Page 39 of % 14.8% Worse *Excess days in acute care 15
40 Patient Experience Measure ID Measure Name Stroger Measure Result on Hospital Compare National Mean of Scores Comparison To National Mean H-CLEAN-HOSP Cleanliness of Hospital Worse H-COMP1 Nurse Communication Worse H-COMP-2 Physician Communication Same H-COMP-3 H-COMP-5 Responsiveness of Hospital Staff Communication about Medicines Worse Worse H-COMP-6 Discharge Information Worse H-HSP-RATING Overall Hospital Rating Worse H-QUIET-HOSP Quietness Of Hospital Environment Worse H-COMP-7 Care Transitions Worse H-RECMND Willingness To Recommend Hospital Page 40 of Worse 16
41 Efficient Use of Medical Imaging Measure ID Measure Name Stroger Measure Result on Hospital Compare (%) National Mean (%) Comparison to National Mean OP-8 MRI Lumbar Spine for Low Back Pain Worse OP-10 Abdomen CT Use of Contrast Worse OP-11 Thorax CT Use of Contrast Better OP-13 Pre-operative Cardiac Imaging Better OP-14 Simultaneous Use of Brain Computed N/A Tomography (CT) and Sinus CT 3 1 Indicator is use of contrast and non-contrast imaging during the same study 2 Imaging which is not indicated Page in 41 low of 54 risk patients 3- Performance category not assigned due to not meeting the minimum measure threshold 17
42 Timeliness of Care Measure ID Measure Name Stroger Measure Result on Hospital Compare (min) National Mean (min) Comparison to National Mean ED-1b Median Time from ED Arrival to ED Departure for Admitted ED Patients Worse ED-2b Admit Decision Time to ED Departure Time for Admitted Patients Worse OP-1 Median Time to Fibrinolysis TFH TFH OP-2 Fibrinolytic Therapy Received Within 30 Minutes of Emergency Department Arrival TFH TFH OP-3b Median Time to Transfer to Another Facility for Acute Coronary Intervention N/A OP-5 Median Time to ECG N/A OP-18b/ED-3 Median Time from ED Arrival to ED Departure for Discharged ED Patients Worse OP-20 Door to Diagnostic Evaluation by a Qualified Medical Professional Worse OP-21 ED-Median Time to Pain Management for Long Bone Fracture Better 1: Too Few Hospitals to Count Page 42 of 54 18
43 Effectiveness of Care Measure ID Measure Name Stroger Measure Result on Hospital Compare National Mean Comparison to National Mean IMM-2 Influenza Immunization 65% 91% Better OP-4 Aspirin on Arrival N/A 95% ---- IMM-3/OP-27 Healthcare Personnel Influenza Vaccination 94% 87% Better OP-22 ED-Patient Left Without Being Seen 5% 2% Worse OP-23 OP-29 OP-30 OP-33 PC-01 ED-Head CT or MRI Scan Results for Acute Ischemic Stroke or Hemorrhagic Stroke who Received Head CT or MRI Scan Interpretation Within 45 Minutes of Arrival Endoscopy/Polyp Surveillance: Appropriate Follow-up Interval for Normal Colonoscopy in Average Risk Patients Endoscopy/Polyp Surveillance: Colonoscopy Interval for Patients with a History of Adenomatous Polyps Avoidance of Inappropriate Use External Beam Radiotherapy for Bone Metastases Elective Delivery Prior to 39 Completed Weeks Gestation: Percentage of Babies Electively Delivered Prior to 39 Completed Weeks Gestation N/A 74% % 87% Worse 100% 91% Better N/A 86% % 2% Better SEP-1 Severe Sepsis and Septic Shock 68% 51% Worse VTE-6 Hospital Acquired Potentially-Preventable Venous Thromboembolism Page 43 of 54 2% 3% Better 19
44 Measure Group Scores Summary Measure Group Number of Measures within Each Group Number of Measures for Stroger Stroger Measure Group Score National Group Score Comparison to National Average Mortality Same Readmission Worse Safety of Care Worse Patient Experience Worse Efficient Use of Medical Imaging Same Timeliness of Care Worse Effectiveness of Care Worse Page 44 of 54 20

45 Outpatient Measurements Page 45 of 54 21

46 Safety and Quality Balanced Scorecard Population Health Efficiency Access HEDIS Medical Home Network Connect Patient Experience Willingness to recommend Communication Cleanliness Equity Continual Readiness TJC IDPH CMS Safety and Performance Improvement Mortality Readmissions Venous Thromboembolism Falls Pressure Ulcers Hospital Acquired Infections Diabetes mellitus type 2 Page 46 of 54 22
47 QUALITY ACTION PLAN Debra Carey, MS, FACHE Deputy CEO, Operations January 18, 2019 Page 47 of 54
48 Quality Action Plan Steering Committee Care Processes Mortality Patient Experience Readmissions Documentation and Coding Priority Measures Focus Workgroups Activities/Principles/High Reliability Across All Settings Inpatient, Ambulatory, Corrections Page 48 of 54 24
49 QUALITY STEERING COMMITTEE Provides oversight for organizational success and drives accountability Recommended MEMBERS: COOs(5), CQO, CMO, CNO, CFO, CLINICAL CHAIRS (3-4) PRIORITIZE SPECIFIC MEASURES IN EACH DOMAIN FOR FOCUS WORKGROUP IDENTIFY MD/RN/ADMIN LEAD FOR FOCUS WORKGROUP APPROVES CHARTER FOR EACH FOCUS WORKGROUP DESIGNATES THE REPORTING TOOL TO BE USED BY WORKGROUPS Page 49 of 54 25
50 Quality Measure Focused Finding Workgroup Led by MD, RN, Administrator Facilitated by MD, RN, Administrator Participants will be selected OR Existing Committee(s) may be used Engage functional areas as required Charter Defines Scope of Work Corrective Actions Identified Metrics / Measures Identified Timeline Developed Completes Reporting Tool Page 50 of 54 26
51 Quality Measure Focused Finding Workgroup Led by MD, RN, Administrator WORKGROUP APPROACH Use PDSA Methodology Balanced Scorecards w/ Reliable Data Uniform Process Across System WORKGROUP TASKS Review / Change Policies Change Process / Practices Train Staff Track Progress for Measures of Success Page 51 of 54 27
52 Proposed Structure QPS EMS HQUIPS Quality Steering Committee Patient Experience Readmissions Mortality Care Processes Documentation and Coding Page 52 of 54 28
53 NEXT STEPS STEERING COMMITTEE TEAMS NAMED BY JANUARY 29, 2019 FIRST MEETINGS WEEK OF FEBRUARY 4, 2019 ASSESS NEED FOR PROJECT MANAGEMENT SUPPORT ASSESS DATA NEEDS AND DATA SOURCES Page 53 of 54 29

54 Questions Page 54 of 54 30
COOK COUNTY HEALTH Meaningful Metrics
 COOK COUNTY HEALTH Meaningful Metrics 2018-2019 Ronald Wyatt MD MHA January 18, 2019 2 Meaningful Measures 3 Meaningful Measures Framework Meaningful Measure Areas Achieve: High quality healthcare Meaningful
COOK COUNTY HEALTH Meaningful Metrics 2018-2019 Ronald Wyatt MD MHA January 18, 2019 2 Meaningful Measures 3 Meaningful Measures Framework Meaningful Measure Areas Achieve: High quality healthcare Meaningful
End-Stage Renal Disease Quality Incentive Program (ESRD QIP) Status Type NQF Measure Title
 Status Type NQF Measure Title") End-Stage Renal Disease Quality Incentive Program (ESRD QIP) Status Type NQF Measure Title NQF Status ID Implemented Outcome 1454 Proportion of patients with hypercalcemia 0256 Vascular Access Type Catheter
End-Stage Renal Disease Quality Incentive Program (ESRD QIP) Status Type NQF Measure Title NQF Status ID Implemented Outcome 1454 Proportion of patients with hypercalcemia 0256 Vascular Access Type Catheter
CMS Hospital Inpatient Quality Reporting (IQR) Program Measures for the FY 2019 Payment Update
 Program Measures for the FY 2019 Payment Update") CMS Inpatient Quality Reporting (IQR) Program Measures for the Update Measures Required to Meet IQR Program APU Requirements NHSN Submission CAUTI National Healthcare Safety Network (NHSN) Catheter-Associated
CMS Inpatient Quality Reporting (IQR) Program Measures for the Update Measures Required to Meet IQR Program APU Requirements NHSN Submission CAUTI National Healthcare Safety Network (NHSN) Catheter-Associated
CMS Hospital IQR Program Measure Comparison Tables FY 2018 (CY 2016) Measures Required to Meet Hospital IQR APU Requirements NHSN Submission
 Measures Required to Meet Hospital IQR APU Requirements NHSN Submission") CMS IQR Program Measure Comparison Tables (CY 2016) NHSN Submission CLABSI Central Line-Associated Bloodstream Infection (CLABSI) Required NHSN CAUTI Catheter-Associated Urinary Tract Infection (CAUTI)
CMS IQR Program Measure Comparison Tables (CY 2016) NHSN Submission CLABSI Central Line-Associated Bloodstream Infection (CLABSI) Required NHSN CAUTI Catheter-Associated Urinary Tract Infection (CAUTI)
CMS Hospital Inpatient Quality Reporting (IQR) Program Measures for the FY 2020 Payment Update
 Program Measures for the FY 2020 Payment Update") CMS Inpatient Quality Reporting (IQR) Program Measures for the Payment Update Measures Required to Meet IQR Program APU Requirements Healthcare-Associated Infection on CAUTI National Healthcare Safety
CMS Inpatient Quality Reporting (IQR) Program Measures for the Payment Update Measures Required to Meet IQR Program APU Requirements Healthcare-Associated Infection on CAUTI National Healthcare Safety
CMS Measures - Fiscal Year 2019
 ID Me asure Name NQF # Value- (VBP) - (HACRP) (HRRP) ID Me asure Name NQF # Value- (VBP) - (HACRP) (HRRP) CMS s - Fiscal Year 2019 ID Name NQF # The Centers for Medicare & Medicaid Services (CMS) Improvement
ID Me asure Name NQF # Value- (VBP) - (HACRP) (HRRP) ID Me asure Name NQF # Value- (VBP) - (HACRP) (HRRP) CMS s - Fiscal Year 2019 ID Name NQF # The Centers for Medicare & Medicaid Services (CMS) Improvement
SCORES FOR 4 TH QUARTER, RD QUARTER, 2014
 SCORES FOR 4 TH QUARTER, 2013 3 RD QUARTER, 2014 PATIENT SATISFACTION SCORES (HCAHPS): 4 STARS OUT OF 5 (ONLY 4 AREA ACUTE CARE HOSPITALS RECEIVED A 4-STAR RATING. NONE ACHIEVED 5-STARS). STRUCTURAL MEASURES:
SCORES FOR 4 TH QUARTER, 2013 3 RD QUARTER, 2014 PATIENT SATISFACTION SCORES (HCAHPS): 4 STARS OUT OF 5 (ONLY 4 AREA ACUTE CARE HOSPITALS RECEIVED A 4-STAR RATING. NONE ACHIEVED 5-STARS). STRUCTURAL MEASURES:
The Centers for Medicare & Medicaid Services (CMS) Acute Care Hospital Fiscal Year (FY) 2018 Quality Improvement Program Measures
 Acute Care Hospital Fiscal Year (FY) 2018 Quality Improvement Program Measures") ID M easure Name NQF # H os pital M easurement Period H os pital H os pital Value-Bas ed Purchas ing M easurement Period H os pital H ealth Record (EH R) Incentive M easurement Period H os pital H os pital-
ID M easure Name NQF # H os pital M easurement Period H os pital H os pital Value-Bas ed Purchas ing M easurement Period H os pital H ealth Record (EH R) Incentive M easurement Period H os pital H os pital-
Measure Applications Partnership. Hospital Workgroup In-Person Meeting Follow- Up Call
 Measure Applications Partnership Hospital Workgroup In-Person Meeting Follow- Up Call December 21, 2016 Feedback on Current Measure Sets for IQR, HACs, Readmissions, and VBP 2 Previously Identified Crosscutting
Measure Applications Partnership Hospital Workgroup In-Person Meeting Follow- Up Call December 21, 2016 Feedback on Current Measure Sets for IQR, HACs, Readmissions, and VBP 2 Previously Identified Crosscutting
Core = Core required measures for all CAH nationally r = Required by State of Minnesota X = Additional for MBQIP
 Key: 2016 Hospital Measure Summary Minnesota Statewide Quality eporting and Measurement System (SQMS) and FY2018 for Center for Medicare and Medicaid Services () January 2016 = equired by Core = Core required
Key: 2016 Hospital Measure Summary Minnesota Statewide Quality eporting and Measurement System (SQMS) and FY2018 for Center for Medicare and Medicaid Services () January 2016 = equired by Core = Core required
FY X Time (48 hrs for cardiac surgery) SCIP-Inf-4 Cardiac Surgery Patients With Controlled 6 A.M. Postoperative Blood
 SCIP-Inf-4 Cardiac Surgery Patients With Controlled 6 A.M. Postoperative Blood") Valuebased 2013 Hospital Measure Summary Data Collection for Inpatient Quality Reporting FY2015 and Outpatient Reporting CY2014 January 2013 Key: = Required by both CMS and State of Minnesota = Required
Valuebased 2013 Hospital Measure Summary Data Collection for Inpatient Quality Reporting FY2015 and Outpatient Reporting CY2014 January 2013 Key: = Required by both CMS and State of Minnesota = Required
Stratis Health
 2017 Hospital Measure Summary Minnesota Statewide Quality eporting & Measurement System (SQMS) and FY2019 for Center for Medicare & Medicaid Services (CMS) Contents Key... 1 Chart Abstracted Measures...
2017 Hospital Measure Summary Minnesota Statewide Quality eporting & Measurement System (SQMS) and FY2019 for Center for Medicare & Medicaid Services (CMS) Contents Key... 1 Chart Abstracted Measures...
UCLA Health System Apr - Jun 2013 (Q2)
") Denom Observed VBP Standard VBP Benchmark Denom Observed VBP Standard VBP Benchmark N Percent x/n N Percent x/n Value Based Purchasing-Clinical Process of Care Measures (%) SCIP-Inf-9 Urinary catheter
Denom Observed VBP Standard VBP Benchmark Denom Observed VBP Standard VBP Benchmark N Percent x/n N Percent x/n Value Based Purchasing-Clinical Process of Care Measures (%) SCIP-Inf-9 Urinary catheter
SUNY Downstate Medical Center/University Hospital Oct - Dec 2013 (Q4)
") Value Based Purchasing-Clinical Process of Care Measures Denom Observed VBP VBP Benchmark Standard Denom Observed VBP VBP Benchmark Standard N Percent x/n N Percent x/n SCIP-Inf-9 Urinary catheter removed
Value Based Purchasing-Clinical Process of Care Measures Denom Observed VBP VBP Benchmark Standard Denom Observed VBP VBP Benchmark Standard N Percent x/n N Percent x/n SCIP-Inf-9 Urinary catheter removed
2016 Hospital Measures
 2016 Hospital Measures Vicki Tang Olson, Stratis Health Statewide Quality Reporting and Measurement System (SQRMS) Annual Forum June 22, 2015 Objectives Share the process used for 2016 hospital measures
2016 Hospital Measures Vicki Tang Olson, Stratis Health Statewide Quality Reporting and Measurement System (SQRMS) Annual Forum June 22, 2015 Objectives Share the process used for 2016 hospital measures
Performance Measure. Inpatient Clinical Process of Care Measures
 Acute Myocardial Infarction (AMI) 's Maryland Hospital Performance Evaluation System: Inpatient s Quality Based Reimbursement () Measures Highlighted in Green (02/27/2014) Inpatient Clinical Process of
Acute Myocardial Infarction (AMI) 's Maryland Hospital Performance Evaluation System: Inpatient s Quality Based Reimbursement () Measures Highlighted in Green (02/27/2014) Inpatient Clinical Process of
Hospital OQR Quality Measures and Timelines for CY 2015 and Subsequent Payment Determinations
 OQR Quality Measures and Timelines for CY 2015 and Subsequent Payment Determinations Data collection, implementation, and public reporting information for each measure are detailed by measure set in the
OQR Quality Measures and Timelines for CY 2015 and Subsequent Payment Determinations Data collection, implementation, and public reporting information for each measure are detailed by measure set in the
Appendix G Explanation/Clarification Summary
 Appendix G Explanation/Clarification Summary Summary of Changes for Recommendations Alignment of measures with VBP by fiscal year Measures and service dates were adjusted to be consistent with the FY2016
Appendix G Explanation/Clarification Summary Summary of Changes for Recommendations Alignment of measures with VBP by fiscal year Measures and service dates were adjusted to be consistent with the FY2016
Medicare Value Based Purchasing Andrew B. Wheeler Vice President of Federal Finance
 Medicare Value Based Purchasing - 101 Andrew B. Wheeler Vice President of Federal Finance What is Medicare s VBP System? Incentive program to improve outcomes, safety, patient satisfaction, and efficiency
Medicare Value Based Purchasing - 101 Andrew B. Wheeler Vice President of Federal Finance What is Medicare s VBP System? Incentive program to improve outcomes, safety, patient satisfaction, and efficiency
Mandatory Elements of Healthcare Reform Walter Coleman. healthcare consulting
 Mandatory Elements of Healthcare Reform Walter Coleman 1 Agenda ACA Mandatory Elements of Reform Value Based Purchasing Readmission Reduction Program Hospital Acquired Conditions Best practices to analyze
Mandatory Elements of Healthcare Reform Walter Coleman 1 Agenda ACA Mandatory Elements of Reform Value Based Purchasing Readmission Reduction Program Hospital Acquired Conditions Best practices to analyze
Specifications Manual Update: Hospital Outpatient Quality Reporting (OQR) Program
 Program") Specifications Manual Update: Hospital Outpatient Quality Reporting (OQR) Program Melissa Thompson, RN, BSN Specifications Manual Lead Hospital OQR Program Support Contractor January 23, 2019 Featuring:
Specifications Manual Update: Hospital Outpatient Quality Reporting (OQR) Program Melissa Thompson, RN, BSN Specifications Manual Lead Hospital OQR Program Support Contractor January 23, 2019 Featuring:
Nancy Hailpern, Director, Regulatory Affairs K Street, NW, Suite 1000 Washington, DC 20005
 Summary of Infection Prevention Issues in the Centers for Medicare & Medicaid Services (CMS) FY 2014 Inpatient Prospective Payment System (IPPS) Final Rule Hospital Readmissions Reduction Program-Fiscal
Summary of Infection Prevention Issues in the Centers for Medicare & Medicaid Services (CMS) FY 2014 Inpatient Prospective Payment System (IPPS) Final Rule Hospital Readmissions Reduction Program-Fiscal
50198 Federal Register / Vol. 75, No. 157 / Monday, August 16, 2010 / Rules and Regulations
 50198 Federal Register / Vol. 75, No. 157 / Monday, August 16, 2010 / Rules and Regulations mstockstill on DSKH9S0YB1PROD with RULES2 VerDate Mar2010 17:02 Aug 13, 2010 Jkt 220001 PO 00000 Frm 00158
50198 Federal Register / Vol. 75, No. 157 / Monday, August 16, 2010 / Rules and Regulations mstockstill on DSKH9S0YB1PROD with RULES2 VerDate Mar2010 17:02 Aug 13, 2010 Jkt 220001 PO 00000 Frm 00158
Table of Contents. Claims Based Measures Calculated by CMS (Outpatient) Imaging Efficiency Page 10
 Imaging Efficiency Page 10") Current Proposed Quality Measures Table of Contents Inpatient Measures Collected Submitted by Hospital Acute Myocardial Infarction/Emergency Department Page2 Immunization/Heart Failure/Pneumonia/Stroke
Current Proposed Quality Measures Table of Contents Inpatient Measures Collected Submitted by Hospital Acute Myocardial Infarction/Emergency Department Page2 Immunization/Heart Failure/Pneumonia/Stroke
Hospital Outpatient Quality Reporting. Benchmarks and Trends. Fourth Quarter 2013 through Fourth Quarter 2014
 Hospital Outpatient Quality Reporting s and Trends Fourth Quarter through Fourth Quarter Hospital Outpatient Quality Reporting (Hospital OQR) Acute Myocardial Infarction (AMI), Surgery, and Stroke Data
Hospital Outpatient Quality Reporting s and Trends Fourth Quarter through Fourth Quarter Hospital Outpatient Quality Reporting (Hospital OQR) Acute Myocardial Infarction (AMI), Surgery, and Stroke Data
Table of Contents. Current and Proposed CMS Quality Measures for Reporting in 2017 through 2023 Revised 8/8/2017
 Table of Contents Current and Proposed CMS Quality Measures Inpatient Measures Collected and Submitted by Hospital AMI/ED/IMM/Pneumonia/Sepsis/Stroke Page 2 Surgical Care Improvement/VTE/Perinatal Care/Pediatric
Table of Contents Current and Proposed CMS Quality Measures Inpatient Measures Collected and Submitted by Hospital AMI/ED/IMM/Pneumonia/Sepsis/Stroke Page 2 Surgical Care Improvement/VTE/Perinatal Care/Pediatric
In Pursuit of Excellence: The CheckPoint Journey
 Focus On Quality... In Pursuit of Excellence: The CheckPoint Journey Charles Shabino, MD; Dana Richardson, RN, MHA Abstract In March 2004, the Wisconsin Hospital Association launched CheckPoint sm (www.wicheckpoint.org)
Focus On Quality... In Pursuit of Excellence: The CheckPoint Journey Charles Shabino, MD; Dana Richardson, RN, MHA Abstract In March 2004, the Wisconsin Hospital Association launched CheckPoint sm (www.wicheckpoint.org)
Medicare Hospital Acquired Conditions Reduction Program Andrew B. Wheeler Vice President of Federal Finance
 Medicare Hospital Acquired Conditions Reduction Program - 201 Andrew B. Wheeler Vice President of Federal Finance Value-Based Hospital Acquired Purchasing Conditions FFY 2018 FFY -2016 2020 AHRQ Claims
Medicare Hospital Acquired Conditions Reduction Program - 201 Andrew B. Wheeler Vice President of Federal Finance Value-Based Hospital Acquired Purchasing Conditions FFY 2018 FFY -2016 2020 AHRQ Claims
Troubleshooting Audio
 Welcome! Audio for this event is available via ReadyTalk Internet Streaming. No telephone line is required. Computer speakers or headphones are necessary to listen to streaming audio. Limited dial-in lines
Welcome! Audio for this event is available via ReadyTalk Internet Streaming. No telephone line is required. Computer speakers or headphones are necessary to listen to streaming audio. Limited dial-in lines
Table of Contents. Current and Proposed CMS Quality Measures for Reporting in 2017 through 2023 Revised 5/4/2017
 Table of Contents Current and Proposed CMS Quality Measures for Reporting in 2017 through 2023 Inpatient Measures Collected and Submitted by Hospital AMI/ED/IMM/Pneumonia/Sepsis/Stroke Page 2 Surgical
Table of Contents Current and Proposed CMS Quality Measures for Reporting in 2017 through 2023 Inpatient Measures Collected and Submitted by Hospital AMI/ED/IMM/Pneumonia/Sepsis/Stroke Page 2 Surgical
A Physician Leader s Role In Becoming A High Performing Health System
 A Physician Leader s Role In Becoming A High Performing Health System Byron C. Scott, MD, MBA Associate Chief Medical Officer, Truven Health Analytics Truven Health Analytics Inc. All Rights Reserved.
A Physician Leader s Role In Becoming A High Performing Health System Byron C. Scott, MD, MBA Associate Chief Medical Officer, Truven Health Analytics Truven Health Analytics Inc. All Rights Reserved.
2016 AMC Quality and Accountability Performance Scorecard Vidant Medical Center. Overall Rank. Overall Score 63.4% Efficiency 7.
 2016 AMC Quality and Accountability Performance Scorecard Vidant Medical Center Star Rating Mortality 12.66% of 25% Domain Performance Overall Rank 27 Overall Score 63.4% Equity 5.00% of 5% Efficiency
2016 AMC Quality and Accountability Performance Scorecard Vidant Medical Center Star Rating Mortality 12.66% of 25% Domain Performance Overall Rank 27 Overall Score 63.4% Equity 5.00% of 5% Efficiency
The table below includes the quality measures an ACO is required to submit to CMS as a participant in an MSSP Track 3 ACO
 The table below includes the quality measures an ACO is required to submit to CMS as a participant in an MSSP Track 3 ACO ACO-1 ACO-2 Getting Timely Care, Appointments, and Information How Well Your Providers
The table below includes the quality measures an ACO is required to submit to CMS as a participant in an MSSP Track 3 ACO ACO-1 ACO-2 Getting Timely Care, Appointments, and Information How Well Your Providers
Quality & Hospital Acquired Conditions
 Quality & Hospital Acquired Conditions Rebecca Armbruster, DO, MS, FACOI Medical Director Resource Management Patricia Heys, BS Director of Infection Prevention & Control Sally Hinkle, DNP, MPA, RN Director
Quality & Hospital Acquired Conditions Rebecca Armbruster, DO, MS, FACOI Medical Director Resource Management Patricia Heys, BS Director of Infection Prevention & Control Sally Hinkle, DNP, MPA, RN Director
State of the State: Hospital Performance in Pennsylvania September 2012
 State of the State: Hospital Performance in Pennsylvania September 2012 Measuring Progress in PA Hospital Performance: Process Measures 1 PA Hospital Performance: Process Measures We examined the latest
State of the State: Hospital Performance in Pennsylvania September 2012 Measuring Progress in PA Hospital Performance: Process Measures 1 PA Hospital Performance: Process Measures We examined the latest
Surgical Care, Pneumonia, Immunizations and Emergency Department Core Measures
 Surgical Care, Pneumonia, Immunizations and Emergency Department Core Measures Audrey Paulman, MD, MMM Principal Clinical Coordinator & Jackie Trojan, RN, BSN Quality Improvement Advisor This material
Surgical Care, Pneumonia, Immunizations and Emergency Department Core Measures Audrey Paulman, MD, MMM Principal Clinical Coordinator & Jackie Trojan, RN, BSN Quality Improvement Advisor This material
NEW JERSEY 2011 HOSPITAL PERFORMANCE REPORT TECHNICAL REPORT: METHODOLOGY RECOMMENDED CARE (PROCESS OF CARE) MEASURES
 MEASURES") NEW JERSEY 2011 HOSPITAL PERFORMANCE REPORT TECHNICAL REPORT: METHODOLOGY RECOMMENDED CARE (PROCESS OF CARE) MEASURES New Jersey Department of Health and Senior Services Health Care Quality Assessment
NEW JERSEY 2011 HOSPITAL PERFORMANCE REPORT TECHNICAL REPORT: METHODOLOGY RECOMMENDED CARE (PROCESS OF CARE) MEASURES New Jersey Department of Health and Senior Services Health Care Quality Assessment
Hospital Compare Quality Measures: 2011 National and Tennessee Results for Critical Access Hospitals
 March 2013 Hospital Compare Quality Measures: 2011 National and Results for Critical Access Michelle Casey, MS, Peiyin Hung, MSPH, Maeve McClellan, BS, Ira Moscovice, PhD, University of Minnesota Rural
March 2013 Hospital Compare Quality Measures: 2011 National and Results for Critical Access Michelle Casey, MS, Peiyin Hung, MSPH, Maeve McClellan, BS, Ira Moscovice, PhD, University of Minnesota Rural
Aligning for Ambulatory Clinical Excellence at Providence St. Joseph Health
 Aligning for Ambulatory Clinical Excellence at Providence St. Joseph Health Trista Johnson, PhD Chris Dale, MD MPH Andrea Ramirez VP, Ambulatory Quality and Clinical Services-Providence St Joseph Chief
Aligning for Ambulatory Clinical Excellence at Providence St. Joseph Health Trista Johnson, PhD Chris Dale, MD MPH Andrea Ramirez VP, Ambulatory Quality and Clinical Services-Providence St Joseph Chief
This Core Measure Report shows performance to date. CAVEAT: Data collection is still in progress for the current and immediate past quarter!
 This Core Measure Report shows performance to date. CAVEAT: Data collection is still in progress for the current and immediate past quarter! AMI-1 -- Aspirin at Arrival 9 8 7 6 5 4 3 2 1 AMI-2 -- Aspirin
This Core Measure Report shows performance to date. CAVEAT: Data collection is still in progress for the current and immediate past quarter! AMI-1 -- Aspirin at Arrival 9 8 7 6 5 4 3 2 1 AMI-2 -- Aspirin
PfP Quality Metrics: Readmissions, Value-Based Purchasing and Beyond
 PfP Quality Metrics: Readmissions, Value-Based Purchasing and Beyond Presented to ASHNHA Alaska Partnership for Patients Advisory Group February 4, 2015 Gloria Kupferman Readmissions Calculation methods
PfP Quality Metrics: Readmissions, Value-Based Purchasing and Beyond Presented to ASHNHA Alaska Partnership for Patients Advisory Group February 4, 2015 Gloria Kupferman Readmissions Calculation methods
NEW JERSEY 2012 HOSPITAL PERFORMANCE REPORT TECHNICAL REPORT: METHODOLOGY RECOMMENDED CARE (PROCESS OF CARE) MEASURES
 MEASURES") NEW JERSEY 2012 HOSPITAL PERFORMANCE REPORT TECHNICAL REPORT: METHODOLOGY RECOMMENDED CARE (PROCESS OF CARE) MEASURES New Jersey Department of Health Health Care Quality Assessment June 2013 NEW JERSEY
NEW JERSEY 2012 HOSPITAL PERFORMANCE REPORT TECHNICAL REPORT: METHODOLOGY RECOMMENDED CARE (PROCESS OF CARE) MEASURES New Jersey Department of Health Health Care Quality Assessment June 2013 NEW JERSEY
Reports delivery. MICAHQN Reports Schedule 5/15/ Q17 Core Measures and 1Q18 MBQIP Data. May 18, Joshua Salander, MBA, PMP Consultant
 /1/21 Q1 Core Measures and 1Q1 MBQIP Data May 1, 21 Joshua Salander, MBA, PMP Consultant Reports delivery Updated Q1 reports were sent via email on May 1, 21 Quarterly Reports Quarterly Trend Charts Please
/1/21 Q1 Core Measures and 1Q1 MBQIP Data May 1, 21 Joshua Salander, MBA, PMP Consultant Reports delivery Updated Q1 reports were sent via email on May 1, 21 Quarterly Reports Quarterly Trend Charts Please
4Q17 Core Measures and 2Q18 MBQIP Data
 4Q17 Core Measures and 2Q18 MBQIP Data August 17, 2018 Joshua Salander, MBA, PMP Consultant Reports delivery 4Q17 reports were sent via email on August 12, 2018 Quarterly Reports Quarterly Trend Charts
4Q17 Core Measures and 2Q18 MBQIP Data August 17, 2018 Joshua Salander, MBA, PMP Consultant Reports delivery 4Q17 reports were sent via email on August 12, 2018 Quarterly Reports Quarterly Trend Charts
Table 1. Proposed Measures for Use in Establishing Quality Performance Standards that ACOs Must Meet for Shared Savings
 CMS-1345-P 174 Table 1. Proposed Measures for Use in Establishing Quality Performance Standards that ACOs Must Meet for Shared Savings AIM: Better Care for Individuals 1. Patient/Care Giver Experience
CMS-1345-P 174 Table 1. Proposed Measures for Use in Establishing Quality Performance Standards that ACOs Must Meet for Shared Savings AIM: Better Care for Individuals 1. Patient/Care Giver Experience
HQID Hospital Performance Update & Analysis of Quality, Cost and Mortality Trends Fact Sheet
 HQID Hospital Performance Update & Analysis of Quality, Cost and Mortality Trends Fact Sheet I.) Performance of Hospitals in the Hospital Quality Incentive Demonstration over 15 Quarters* (pages 2-5) Launched
HQID Hospital Performance Update & Analysis of Quality, Cost and Mortality Trends Fact Sheet I.) Performance of Hospitals in the Hospital Quality Incentive Demonstration over 15 Quarters* (pages 2-5) Launched
Quality Reporting for CAHs and Rural PPS Hospitals: The Potential Impact of Composite Measures
 UpperMidwest Rural Health Research Center www.uppermidwestrhrc.org July 202 Policy Brief Quality Reporting for CAHs and Rural PPS Hospitals: The Potential Impact of Composite Measures Michelle Casey MS,
UpperMidwest Rural Health Research Center www.uppermidwestrhrc.org July 202 Policy Brief Quality Reporting for CAHs and Rural PPS Hospitals: The Potential Impact of Composite Measures Michelle Casey MS,
Rapid Response Teams. January 17, Safe Table Webinar
 Rapid Response Teams January 17, 2017 Safe Table Webinar Christin Gordanier, MSN, RN, Inpatient Nursing Director at Virginia Mason Medical Center in Seattle, Washington. Alice Ferguson, BSN, RN, Project
Rapid Response Teams January 17, 2017 Safe Table Webinar Christin Gordanier, MSN, RN, Inpatient Nursing Director at Virginia Mason Medical Center in Seattle, Washington. Alice Ferguson, BSN, RN, Project
Improving Quality of Care for Medicare Patients: Accountable Care Organizations
 DEPARTMENT OF HEALTH & HUMAN SERVICES Centers for Medicare & Medicaid Services Room 352-G 200 Independence Avenue, SW Washington, DC 20201 Office of Media Affairs MEDICARE FACT SHEET FOR IMMEDIATE RELEASE
DEPARTMENT OF HEALTH & HUMAN SERVICES Centers for Medicare & Medicaid Services Room 352-G 200 Independence Avenue, SW Washington, DC 20201 Office of Media Affairs MEDICARE FACT SHEET FOR IMMEDIATE RELEASE
Final Recommendation for Updating the Quality Based Reimbursement Program
 Final Recommendation for Updating the Quality Based Reimbursement Program for FY 2018 October 14, 2015 Health Services Cost Review Commission 4160 Patterson Avenue Baltimore, Maryland 21215 (410) 764 2605
Final Recommendation for Updating the Quality Based Reimbursement Program for FY 2018 October 14, 2015 Health Services Cost Review Commission 4160 Patterson Avenue Baltimore, Maryland 21215 (410) 764 2605
America s Hospitals: Improving Quality and Safety
 America s Hospitals: Improving Quality and Safety The Joint Commission s Annual Report 2014 Top Performer on Key Quality Measures America s Hospitals: Improving Quality and Safety The Joint Commission
America s Hospitals: Improving Quality and Safety The Joint Commission s Annual Report 2014 Top Performer on Key Quality Measures America s Hospitals: Improving Quality and Safety The Joint Commission
Standards of excellence
 The Accreditation Canada Stroke Distinction program was launched in March 2010 to offer a rigorous and highly specialized process above and beyond the requirements of Qmentum. The comprehensive Stroke
The Accreditation Canada Stroke Distinction program was launched in March 2010 to offer a rigorous and highly specialized process above and beyond the requirements of Qmentum. The comprehensive Stroke
What ASMBS Members Need to Know About: New Medicare Payment Policy Governing Bariatric Surgery and Hospital Acquired Conditions (HACs)
") What ASMBS Members Need to Know About: New Medicare Payment Policy Governing Bariatric Surgery and Hospital Acquired Conditions (HACs) Robin Blackstone, MD, FACS, FASMBS Beginning October 1, 2008, Medicare
What ASMBS Members Need to Know About: New Medicare Payment Policy Governing Bariatric Surgery and Hospital Acquired Conditions (HACs) Robin Blackstone, MD, FACS, FASMBS Beginning October 1, 2008, Medicare
Objectives 1/10/2013. Hospital Outpatient Quality Reporting Specifications Manual Updates January 1, 2013
 Hospital Outpatient Quality Reporting Specifications Manual Updates January 1, 2013 Wanda Johnson, OFMQ Casey Thompson, OFMQ Kari Johnston, OFMQ Hospital Outpatient Quality Reporting Program Announcements
Hospital Outpatient Quality Reporting Specifications Manual Updates January 1, 2013 Wanda Johnson, OFMQ Casey Thompson, OFMQ Kari Johnston, OFMQ Hospital Outpatient Quality Reporting Program Announcements
2015 PQRS Registry. Source Measure Title Measure Description CITIUS1
 1 CQ-IQ covers 65 CMS defined measures that Eligible Providers (EPs) have to report on to assess quality of care provided to the patients. Version Supported: PQRS Registry 2015 65 measures Reporting Period:
1 CQ-IQ covers 65 CMS defined measures that Eligible Providers (EPs) have to report on to assess quality of care provided to the patients. Version Supported: PQRS Registry 2015 65 measures Reporting Period:
NATIONAL QUALITY FORUM
 Cardiovascular and Diabetes Task Force Summary of In-Person Meeting #2 An in-person meeting of the Measure Applications Partnership (MAP) Cardiovascular and Diabetes Task Force was held on Tuesday, July
Cardiovascular and Diabetes Task Force Summary of In-Person Meeting #2 An in-person meeting of the Measure Applications Partnership (MAP) Cardiovascular and Diabetes Task Force was held on Tuesday, July
JAWDA Quarterly Waiting Time Guidelines for (Specialized and General Hospitals)
") JAWDA Waiting Time Guidelines for (Specialized and General Hospitals) January 2019 Page 1 of 22 Table of Contents Executive Summary... 3 About this Guidance... 4 Performance Indicators... 5 APPENDIX -
JAWDA Waiting Time Guidelines for (Specialized and General Hospitals) January 2019 Page 1 of 22 Table of Contents Executive Summary... 3 About this Guidance... 4 Performance Indicators... 5 APPENDIX -
PPS Exempt Cancer Hospital Quality Reporting (PCHQR) Program Relationship Matrix of Program Measures by Years and Quarters
 Program Relationship Matrix of Program Measures by Years and Quarters") PPS Exempt Cancer Quality (PCHQR) Relationship Matrix of Measures by and This reference document for PCHQR participants provides the following: Specific measures with their National Quality Forum (NQF)
PPS Exempt Cancer Quality (PCHQR) Relationship Matrix of Measures by and This reference document for PCHQR participants provides the following: Specific measures with their National Quality Forum (NQF)
CAH Participation and Quality Measure Results for Hospital Compare 2007 Discharges and Trends: National and North Carolina Results
 January 2009 CAH Participation and Quality Measure Results for Hospital Compare Discharges and - Trends: and Results Michelle Casey, MS 1, Michele Burlew, MS 2, Ira Moscovice, PhD 1 1 University of Minnesota
January 2009 CAH Participation and Quality Measure Results for Hospital Compare Discharges and - Trends: and Results Michelle Casey, MS 1, Michele Burlew, MS 2, Ira Moscovice, PhD 1 1 University of Minnesota
HEART FAILURE QUALITY IMPROVEMENT. American Heart Association Shawni Smith Regional Director, Quality & Systems Improvement
 HEART FAILURE QUALITY IMPROVEMENT American Heart Association Shawni Smith Regional Director, Quality & Systems Improvement 1 DISCLOSURES NONE 2 3 WHY IS THIS IMPORTANT? WHY? Heart Failure Currently, an
HEART FAILURE QUALITY IMPROVEMENT American Heart Association Shawni Smith Regional Director, Quality & Systems Improvement 1 DISCLOSURES NONE 2 3 WHY IS THIS IMPORTANT? WHY? Heart Failure Currently, an
Infectious Diseases-HAI Idaho Department of Health and Welfare, Division of Public Health Boise, Idaho. Assignment Description
 Infectious Diseases-HAI Idaho Department of Health and Welfare, Division of Public Health Boise, Idaho Assignment Description The Fellow s assignments will primarily focus on projects within the HAI and
Infectious Diseases-HAI Idaho Department of Health and Welfare, Division of Public Health Boise, Idaho Assignment Description The Fellow s assignments will primarily focus on projects within the HAI and
Appendix 1: Supplementary tables [posted as supplied by author]
![Appendix 1: Supplementary tables [posted as supplied by author]](/thumbs/81/83505567.jpg "Appendix 1: Supplementary tables [posted as supplied by author]") Appendix 1: Supplementary tables [posted as supplied by author] Table A. International Classification of Diseases, Ninth Revision, Clinical Modification Codes Used to Define Heart Failure, Acute Myocardial
Appendix 1: Supplementary tables [posted as supplied by author] Table A. International Classification of Diseases, Ninth Revision, Clinical Modification Codes Used to Define Heart Failure, Acute Myocardial
PPS Exempt Cancer Hospital Quality Reporting (PCHQR) Program Relationship Matrix of Program Measures by Years and Quarters
 Program Relationship Matrix of Program Measures by Years and Quarters") PPS Exempt Cancer Quality (PCHQR) Relationship Matrix of Measures by and This reference document for PCHQR participants provides the following: Specific measures with their National Quality Forum (NQF)
PPS Exempt Cancer Quality (PCHQR) Relationship Matrix of Measures by and This reference document for PCHQR participants provides the following: Specific measures with their National Quality Forum (NQF)
Troubleshooting Audio
 Welcome Audio for this event is available via ReadyTalk Internet streaming. No telephone line is required. Computer speakers or headphones are necessary to listen to streaming audio. Limited dial-in lines
Welcome Audio for this event is available via ReadyTalk Internet streaming. No telephone line is required. Computer speakers or headphones are necessary to listen to streaming audio. Limited dial-in lines
H-SAA AMENDING AGREEMENT B E T W E E N: TORONTO CENTRAL LOCAL HEALTH INTEGRATION NETWORK (the LHIN ) AND. SINAI HEALTH SYSTEM (the Hospital )
 AND. SINAI HEALTH SYSTEM (the Hospital )") H-SAA AMENDING AGREEMENT THIS AMENDING AGREEMENT (the Agreement ) is made as of the 1 st day of April, 2016 B E T W E E N: TORONTO CENTRAL LOCAL HEALTH INTEGRATION NETWORK (the LHIN ) AND SINAI HEALTH
H-SAA AMENDING AGREEMENT THIS AMENDING AGREEMENT (the Agreement ) is made as of the 1 st day of April, 2016 B E T W E E N: TORONTO CENTRAL LOCAL HEALTH INTEGRATION NETWORK (the LHIN ) AND SINAI HEALTH
2014 Clinical Quality Measures: Changes for the Medicaid EHR Incentive Program. Tracy McDonald Medicaid EHR Incentive Program Coordinator
 2014 Clinical Quality Measures: Changes for the Medicaid EHR Incentive Program Tracy McDonald Medicaid EHR Incentive Program Coordinator Agenda Why are Clinical Quality Measures important? Clinical Quality
2014 Clinical Quality Measures: Changes for the Medicaid EHR Incentive Program Tracy McDonald Medicaid EHR Incentive Program Coordinator Agenda Why are Clinical Quality Measures important? Clinical Quality
THE NATIONAL QUALITY FORUM
 THE NATIONAL QUALITY FORUM National Voluntary Consensus Standards for Patient Outcomes Table of Measures Submitted-Phase 1 As of March 5, 2010 Note: This information is for personal and noncommercial use
THE NATIONAL QUALITY FORUM National Voluntary Consensus Standards for Patient Outcomes Table of Measures Submitted-Phase 1 As of March 5, 2010 Note: This information is for personal and noncommercial use
INPATIENT REIMBURSEMENT PROSPECTUS
 2018 CARDIOVASCULAR SERVICE LINE INPATIENT REIMBURSEMENT PROSPECTUS Increasing financial risk to U.S. health care providers, including physicians and hospitals, has been centered on outcomes-based modifiers
2018 CARDIOVASCULAR SERVICE LINE INPATIENT REIMBURSEMENT PROSPECTUS Increasing financial risk to U.S. health care providers, including physicians and hospitals, has been centered on outcomes-based modifiers
AMCP Webinar Series. Exchanges and Qualified Health Plans: How your voice can shape the future of quality reporting 14 January 2014.
 AMCP Webinar Series Exchanges and Qualified Health Plans: How your voice can shape the future of quality reporting 14 January 2014 Speaker Mitzi Wasik, Pharm.D., BCPS Director, Pharmacy Medicare Programs
AMCP Webinar Series Exchanges and Qualified Health Plans: How your voice can shape the future of quality reporting 14 January 2014 Speaker Mitzi Wasik, Pharm.D., BCPS Director, Pharmacy Medicare Programs
MEMORANDUM. Vincent J. Mastracco Jr., Acting Chair William P. Kanto Jr., M.D. The Hon. Lewis F. Payne
 July 9, 2010 MEMORANDUM TO: The Medical Center Operating Board: Vincent J. Mastracco Jr., Acting Chair William P. Kanto Jr., M.D. The Hon. Lewis F. Payne Constance R. Kincheloe Randl L. Shure Randy J.
July 9, 2010 MEMORANDUM TO: The Medical Center Operating Board: Vincent J. Mastracco Jr., Acting Chair William P. Kanto Jr., M.D. The Hon. Lewis F. Payne Constance R. Kincheloe Randl L. Shure Randy J.
Introduction and Purpose
 Proceedings Illinois Oral Health Summit September 11, 2001 Illinois Response to the Surgeon General s Report on Introduction and Purpose The landmark Illinois Oral Health Summit convened on September 11,
Proceedings Illinois Oral Health Summit September 11, 2001 Illinois Response to the Surgeon General s Report on Introduction and Purpose The landmark Illinois Oral Health Summit convened on September 11,
C E R T I FI C AT I O N. Benchmarking Performance in HFAP-certified Primary Stroke Centers
 PRIMARY STROKE C E R T I FI C AT I O N Benchmarking Performance in HFAP-certified Primary Stroke Centers HFAP s mission is to advance high quality patient care and safety through objective application
PRIMARY STROKE C E R T I FI C AT I O N Benchmarking Performance in HFAP-certified Primary Stroke Centers HFAP s mission is to advance high quality patient care and safety through objective application
TRUST BOARD SUBMISSION TEMPLATE MEETING Trust Board - Public Ref No. 6.1
 TRUST BOARD SUBMISSION TEMPLATE MEETING Trust Board - Public Ref No. 6.1 DIRECTOR Interim Director of Planning, Performance and Informatics Date 4 th October 2018 Trust Performance Report Purpose Corporate
TRUST BOARD SUBMISSION TEMPLATE MEETING Trust Board - Public Ref No. 6.1 DIRECTOR Interim Director of Planning, Performance and Informatics Date 4 th October 2018 Trust Performance Report Purpose Corporate
Operational Performance. SaTH Overall Performance
 Balanced Scorecard Summary 3 Operational Performance inance Previous This Year to Date Previous This Year to Date Number Number Number Number Number Green 16 17 17 Green 7 7 0 Amber 4 3 3 Amber 0 1 0 Red
Balanced Scorecard Summary 3 Operational Performance inance Previous This Year to Date Previous This Year to Date Number Number Number Number Number Green 16 17 17 Green 7 7 0 Amber 4 3 3 Amber 0 1 0 Red
NHS Outcomes Framework: at-a-glance
 April 2016 NHS Outcomes Framework: at-a-glance List of outcomes and indicators in the NHS Outcomes Framework for 2016-17 Domain 1: Preventing people from dying prematurely 1a Potential years of life lost
April 2016 NHS Outcomes Framework: at-a-glance List of outcomes and indicators in the NHS Outcomes Framework for 2016-17 Domain 1: Preventing people from dying prematurely 1a Potential years of life lost
e-module Centers for Medicaid and Medicare (CMS) Core Measures
 Core Measures") Centers for Medicaid and Medicare (CMS) Core Measures 1 Purpose The purpose of this e-learning module is to provide education for health care providers on Core Measures. This module is not all inclusive,
Centers for Medicaid and Medicare (CMS) Core Measures 1 Purpose The purpose of this e-learning module is to provide education for health care providers on Core Measures. This module is not all inclusive,
Technical Appendix for Outcome Measures
 Study Overview Technical Appendix for Outcome Measures This is a report on data used, and analyses done, by MPA Healthcare Solutions (MPA, formerly Michael Pine and Associates) for Consumers CHECKBOOK/Center
Study Overview Technical Appendix for Outcome Measures This is a report on data used, and analyses done, by MPA Healthcare Solutions (MPA, formerly Michael Pine and Associates) for Consumers CHECKBOOK/Center
2012 Core Measures. Acute Myocardial Infarction (AMI)
") 2012 Core Measures Acute Myocardial Infarction (AMI) Aspirin at Arrival Aspirin Prescribed at Discharge Angiotensin converting enzyme inhibitor (ACEI) or angiotensin receptor blocker (ARB) for left ventricular
2012 Core Measures Acute Myocardial Infarction (AMI) Aspirin at Arrival Aspirin Prescribed at Discharge Angiotensin converting enzyme inhibitor (ACEI) or angiotensin receptor blocker (ARB) for left ventricular
Evolution of Heart Failure Disease Management at a Large VA Medical Center. Richard S. Schofield MD, FACC North Florida/South Georgia VHS
 Evolution of Heart Failure Disease Management at a Large VA Medical Center Richard S. Schofield MD, FACC North Florida/South Georgia VHS Disclosures None 2 1,000,000 Increasing VA Burden: Outpatient Encounters
Evolution of Heart Failure Disease Management at a Large VA Medical Center Richard S. Schofield MD, FACC North Florida/South Georgia VHS Disclosures None 2 1,000,000 Increasing VA Burden: Outpatient Encounters
Non-QPP Measures 3 AQUA12. 6 AQUA15 Stones: Urinalysis documented 30 days before
 Non-QPP Measures 1 Measure ID Measure Title Definition Type Domain AQUA3 (inverse) Cryptorchidism: Inappropriate use of scrotal/groin ultrasound on boys Percentage of patients (boys) =< 18 years of age
Non-QPP Measures 1 Measure ID Measure Title Definition Type Domain AQUA3 (inverse) Cryptorchidism: Inappropriate use of scrotal/groin ultrasound on boys Percentage of patients (boys) =< 18 years of age
State of the State: Hospital Performance in Pennsylvania August 2010
 State of the State: Hospital Performance in Pennsylvania August 2010 Measuring Progress in PA Hospital Performance: Process Measures Quality Measures Analysis We reviewed the latest year-over-year changes
State of the State: Hospital Performance in Pennsylvania August 2010 Measuring Progress in PA Hospital Performance: Process Measures Quality Measures Analysis We reviewed the latest year-over-year changes
Quality Committee Core Measures Report AMI. Acute Myocardial Infarction
 AMI 2011 Acute Myocardial Infarction ASPIRIN AT ARRIVAL: A higher number is better. This measure shows the percentage of heart attack patients who receive aspirin within 24 hrs of arrival at hospital.
AMI 2011 Acute Myocardial Infarction ASPIRIN AT ARRIVAL: A higher number is better. This measure shows the percentage of heart attack patients who receive aspirin within 24 hrs of arrival at hospital.
convey the clinical quality measure's title, number, owner/developer and contact
 CMS-0033-P 153 convey the clinical quality measure's title, number, owner/developer and contact information, and a link to existing electronic specifications where applicable. TABLE 20: Proposed Clinical
CMS-0033-P 153 convey the clinical quality measure's title, number, owner/developer and contact information, and a link to existing electronic specifications where applicable. TABLE 20: Proposed Clinical
Troubleshooting Audio
 Welcome! Audio for this event is available via ReadyTalk Internet streaming. No telephone line is required. Computer speakers or headphones are necessary to listen to streaming audio. Limited dial-in lines
Welcome! Audio for this event is available via ReadyTalk Internet streaming. No telephone line is required. Computer speakers or headphones are necessary to listen to streaming audio. Limited dial-in lines
proposed set to a required subset of 3 to 5 measures based on the availability of electronic
 CMS-0033-P 143 proposed set to a required subset of 3 to 5 measures based on the availability of electronic measure specifications and comments received. We propose to require for 2011 and 2012 that EP's
CMS-0033-P 143 proposed set to a required subset of 3 to 5 measures based on the availability of electronic measure specifications and comments received. We propose to require for 2011 and 2012 that EP's
Using Big Data to Prevent Infections
 Using Big Data to Prevent Infections A thought paper by Scalable Health Big Data Analytics Reduces Infections in Hospitals Healthcare Associated Infections (HAIs) are developed while patients are receiving
Using Big Data to Prevent Infections A thought paper by Scalable Health Big Data Analytics Reduces Infections in Hospitals Healthcare Associated Infections (HAIs) are developed while patients are receiving
Hospital Sector
 Hospital Sector Schedule A: Funding Allocation Target Intended Purpose or Use of Funding Estimated 1 Funding Allocation FUNDING SUMMARY Global Funding (LHIN Allocation) Health System Funding Reform (HSFR)
Hospital Sector Schedule A: Funding Allocation Target Intended Purpose or Use of Funding Estimated 1 Funding Allocation FUNDING SUMMARY Global Funding (LHIN Allocation) Health System Funding Reform (HSFR)
QUALITY IMPROVEMENT Section 9
 Quality Improvement Program The Plan s Quality Improvement Program serves to improve the health of its members through emphasis on health maintenance, education, diagnostic testing and treatment. The Quality
Quality Improvement Program The Plan s Quality Improvement Program serves to improve the health of its members through emphasis on health maintenance, education, diagnostic testing and treatment. The Quality
August 29, Dear Dr. Berwick:
 August 29, 2011 Donald Berwick, MD Administrator Centers for Medicare & Medicaid Services U.S. Department of Health and Human Services 200 Independence Avenue, SW Room 445-G Washington, DC 20201 Re: Proposed
August 29, 2011 Donald Berwick, MD Administrator Centers for Medicare & Medicaid Services U.S. Department of Health and Human Services 200 Independence Avenue, SW Room 445-G Washington, DC 20201 Re: Proposed
The Future of Cardiac Care: Managing Our Patients Together
 The Future of Cardiac Care: Managing Our Patients Together Charles R. Caldwell, MD, FACC Disclosures: iheartdoc,inc. Telemedicine 1 MACRA Medicare Access and CHIP Reauthorization Act of 2015 Repealed the
The Future of Cardiac Care: Managing Our Patients Together Charles R. Caldwell, MD, FACC Disclosures: iheartdoc,inc. Telemedicine 1 MACRA Medicare Access and CHIP Reauthorization Act of 2015 Repealed the
Clinical Integration Quality Measures
 Clinical Integration Quality Measures Valley Integrated Care Network (VIPN) is physician-driven, with physicians determining which quality measures will be used to improve overall quality of care. Purpose:
Clinical Integration Quality Measures Valley Integrated Care Network (VIPN) is physician-driven, with physicians determining which quality measures will be used to improve overall quality of care. Purpose:
Improving Prevention and Control of Infection Quarter 2 Report: April 2009 September 2009
 Improving Prevention and Control of Infection Quarter 2 Report: April 2009 September 2009 1. Introduction This Quarter 2 updates the Health Board on infection prevention and control issues within the BCUHB.
Improving Prevention and Control of Infection Quarter 2 Report: April 2009 September 2009 1. Introduction This Quarter 2 updates the Health Board on infection prevention and control issues within the BCUHB.
A Pause in the Availability of Risk Adjusted National Benchmarks for AHRQ Indicators and an Alternative Measurement Approach
 A Pause in the Availability of Risk Adjusted National Benchmarks for AHRQ Indicators and an Alternative Measurement Approach Joseph Greenway, MPH Director of the Center for Health Information Analysis
A Pause in the Availability of Risk Adjusted National Benchmarks for AHRQ Indicators and an Alternative Measurement Approach Joseph Greenway, MPH Director of the Center for Health Information Analysis
PIN BENCHMARKING DATA DEFINITIONS DICTIONARY
 CORE MEASURES PIN BENCHMARKING DATA DEFINITIONS DICTIONARY 1 Total number of CAH acute care patient admissions. Report all CAH acute care only patient admissions for the quarter. Exclude CAH swing bed,
CORE MEASURES PIN BENCHMARKING DATA DEFINITIONS DICTIONARY 1 Total number of CAH acute care patient admissions. Report all CAH acute care only patient admissions for the quarter. Exclude CAH swing bed,
Our Commitment to Quality and Patient Safety Core Measures
 Calvert Memorial Hospital is committed to our community, with a focus on patient-centered care. High quality and safe patient care is not our goal, it is our priority. That means delivering the best possible
Calvert Memorial Hospital is committed to our community, with a focus on patient-centered care. High quality and safe patient care is not our goal, it is our priority. That means delivering the best possible
Quality Payment Program: A Closer Look at the Proposed Rule for Year 3
 Quality Payment Program: A Closer Look at the Proposed Rule for Year 3 Sandy Swallow and Michelle Brunsen August 21, 2018 1 This material was prepared by Telligen, the Medicare Quality Innovation Network
Quality Payment Program: A Closer Look at the Proposed Rule for Year 3 Sandy Swallow and Michelle Brunsen August 21, 2018 1 This material was prepared by Telligen, the Medicare Quality Innovation Network
Fifth Annual National ACO Summit
 Fifth Annual National ACO Summit June 18 20, 2014 Follow us on Twitter at @ACO_LN and use #ACOsummit The Engelberg Center for Health Care Reform at Brookings The Dartmouth Institute Track One: Performance
Fifth Annual National ACO Summit June 18 20, 2014 Follow us on Twitter at @ACO_LN and use #ACOsummit The Engelberg Center for Health Care Reform at Brookings The Dartmouth Institute Track One: Performance
QIOs: Partners for Quality Improvement Under the Medicare Drug Benefit
 QIOs: Partners for Quality Improvement Under the Medicare Drug Benefit Presentation to The 2 nd Annual National Medicare Prescription Drug Congress David Schulke Executive Vice President The American Health
QIOs: Partners for Quality Improvement Under the Medicare Drug Benefit Presentation to The 2 nd Annual National Medicare Prescription Drug Congress David Schulke Executive Vice President The American Health
NQF-ENDORSED VOLUNTARY CONSENSUS STANDARD FOR HOSPITAL CARE. Measure Information Form Collected For: CMS Outcome Measures (Claims Based)
") Last Updated: Version 4.3 NQF-ENDORSED VOLUNTARY CONSENSUS STANDARD FOR HOSPITAL CARE Measure Information Form Collected For: CMS Outcome Measures (Claims Based) Measure Set: CMS Readmission Measures Set
Last Updated: Version 4.3 NQF-ENDORSED VOLUNTARY CONSENSUS STANDARD FOR HOSPITAL CARE Measure Information Form Collected For: CMS Outcome Measures (Claims Based) Measure Set: CMS Readmission Measures Set
CARDIOLOGY IMAGING PROGRAM
 CARDIOLOGY IMAGING PROGRAM TABLE OF CONTENTS. OVERVIEW............................................................................................. 618..... MEMBERS........... EXEMPT.......... FROM.......
CARDIOLOGY IMAGING PROGRAM TABLE OF CONTENTS. OVERVIEW............................................................................................. 618..... MEMBERS........... EXEMPT.......... FROM.......