Rapid Response Teams. January 17, Safe Table Webinar
|
|
|
- Carol Parsons
- 5 years ago
- Views:
Transcription


1 Rapid Response Teams January 17, 2017 Safe Table Webinar



2 Christin Gordanier, MSN, RN, Inpatient Nursing Director at Virginia Mason Medical Center in Seattle, Washington. Alice Ferguson, BSN, RN, Project Manager for Sepsis and RRT at Virginia Mason Medical Center in Seattle, Washington. Ryan Hosken, MBA, RN, Director of Quality and Performance Improvement, Patient Safety, Phone: , 2

3 3 Partnership for Patients Alaska, Oregon, Washington: Learning With Others
4 Partnership for Patients 20% reduction in all-cause harm 12% reduction readmissions By September,
5 Eleven Topics 1. Adverse drug events (ADE), opioid, anticoagulation, and glycemic management 2. Central line-associated blood stream infections (CLABSI) 1 3. Catheter-associated urinary tract infections (CAUTI) 1 4. Clostridium difficile (C. diff), including Antibiotic Stewardship 1 5. Falls 6. Pressure Ulcers 1 7. Sepsis and Septic Shock 1 8. Surgical Site Infections (SSI) 1 9. Venous thromboembolism (VTE) Ventilator-Associated Events (VAE), to include Infection-related Ventilator-Associated Complication (IVAC) and Ventilator-Associated Condition (VAC) Readmissions 1 1 Linked to payment through CMS Value Based Purchasing
6 Measuring Results Comparison: Total number of Code Blue calls (as reference for RRT calls) Outcome Numerator: Number of calls to the RRT that month Denominator: Total number of discharges for same time period Process Number of hospitals where RRTs are in place Exclusions: Stillbirths, deaths in ED Sample 1: 14 RRT calls in one month (December 1, 2016 through December 31, 2016) with 420 discharges (per 1000) in the same time period. 14 divided by.420 = Sample 2: 10 RRT calls in one month (December 1, 2016 through December 31, 2016) with 150 discharges (per 1000) in the same time period. 10 divided by.150 =

7 Rapid Response at Virginia Mason Empowering Nurses, Improving Outcomes Christin Gordanier, RN MN, Inpatient Nursing Director Alice Ferguson, RN BSN, RN Project Manager
8 Objectives Empowering nursing to identify and respond to changes in patient condition improves outcomes Look upstream for improvement opportunities Care protocols decrease variation and time to treatment
9 Rapid Response-Vision Decrease Morbidity and Mortality by: Providing early assessment and intervention Facilitating transfers to higher level of care Supporting staff development through education 9
10 Rapid Response-Key Points Key Points: Available for all hospitalized patients 24 hours per day No patients are ineligible for a Rapid Response Good, patient-focused process that needed improvement 10
 who had a full compliment of patients 11")
11 Rapid Response-Baseline Before Improvement 4 RRT calls per day (~120 per month) 44 minutes per call Many responders, including a hospitalist, (along with two residents) who had a full compliment of patients 11


12 Rapid Response-Baseline RRT Outcomes Transferred to a Higher Level of Care 51% Stabilized 49% 12

13 A New Approach Two-pronged approach Improving upstream care of patients Improving Rapid Response process Primary methods Multidisciplinary quality improvement Nurse empowerment 13
14 How Nurse Empowerment Works at Virginia Mason Increasing patient acuity 14
15 Nurse Empowerment Increasing patient acuity 15
16 Nurse Empowerment Increasing patient acuity 16
")
17 Upstream Approach Three major groups of work Intake Huddle Getting the patient into the right bed the first time Watch List Extra eyes on high risk patients Early Recognition and Treatment of Sepsis (ED and hospital) 17
 by a multidisciplinary team The huddle takes less than 5 minutes and focuses on getting the patient to the right")
18 Intake Huddle The Right Level of Care Every Time Designed in an improvement event that targeted early transfers (within 24 hours of admission) to Critical Care (CCU) Patients with unclear trajectories are flagged and reviewed upon arrival in the Emergency Department (ED) by a multidisciplinary team The huddle takes less than 5 minutes and focuses on getting the patient to the right level of care in a timely manner 18


19 Watch List Operationalizing the nurse s sixth sense Is anyone else seeing what I m seeing?
20 Watch List-Before
21 Watch List-After
22 Watch List-After Patient seen by CCU RN and RT within 45 minutes Provider aware of RN concerns Multidisciplinary team comes to the patient BEFORE an RRT is needed
23 Watch List Case Example Elderly Patient with gradual increase in work of breathing Admitted for UTI Allergic to albuterol Primary RN placed patient on Watch List Notified provider of concerns CCU RN and RT assessed patient with primary RN and provider Plan was developed for symptom management 23
24 Rapid Response-Baseline Post RRT Outcomes/Diagnoses Stroke Activation STEMI Sepsis Bundle Code 4 24

25 Sepsis Power Hour: Nurse Leads RN Work: < 30mins Identify Sepsis Check Lactate within 10 min Check Blood Cultures Start 500cc fluid bolus MD Work: < 60mins Confirm Sepsis Start Antibiotics Complete 2L fluid bolus Pharmacy Work: Prioritize Antibiotics Dose and Prepare STAT Hand-Deliver to patient s location 25

26 Don t Wait Initiate! Sepsis Power Hour Huddle Card There was a sepsis Power Hour called on our unit on 4/02 at 13:33. The patient met criteria with elevated T and HR. Lactic acid was 1.48 and the patient received antibiotics Great Catch!!! What information led me to initiate the Power Hour? What went well? Don t Wait Initiate! What could have gone better? What (if anything) would I do different next time? Sepsis Power Hour
27 Sepsis Case Example Suspected sepsis in patient with tachycardia and fever Immunocompromised Admitted for fever of unknown origin Primary RN initiated the Sepsis Power Hour Fluid Bolus, Blood Cultures, Lactate Patient found to have a lactate of 3.58 Provider ordered additional fluid resuscitation and antibiotics Patient diagnosed with pneumonia 27
28 Power Hour Data (n=375) 100% Element and Bundle Compliance 90% 92% Power Hour Baseline 80% 60% 48% 40% 36% 20% 0% Bolus Lactate
29 Rapid Response Process-Before 29
30 Rapid Response Process-Before Six initial responders Waiting! Waiting! Waiting! Repeating work! Repeating work! 30
31 Where we were Waiting! Waiting! Waiting! Repeating work! Repeating work! 31
32 Where We Were Waiting! Waiting! Waiting! Repeating work! Repeating work! 32
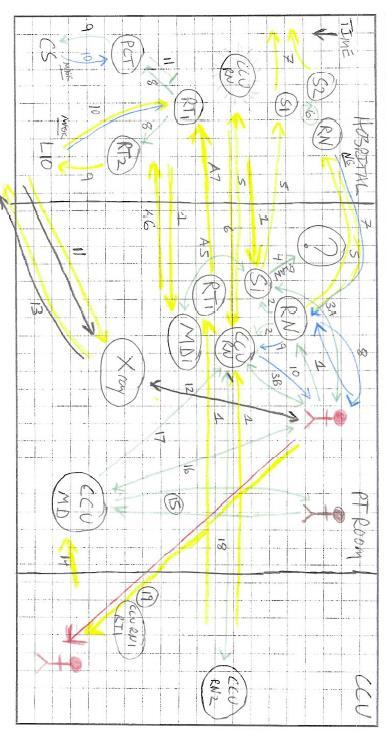
33 Chaos! 33


34 What we did Refining the RRT Process June 2015 week-long improvement event Multidisciplinary team Executive sponsorship 34
35 Rapid Response Process-After 35
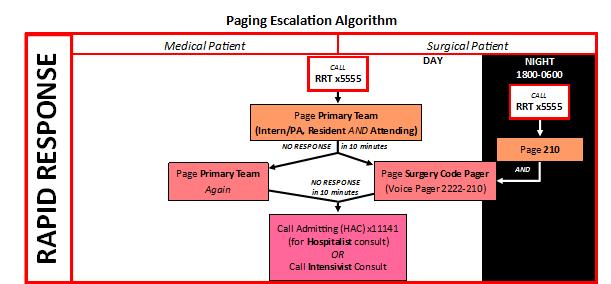
36 Rapid Response Process-After Three initial responders CCU RN leads Treatment begins via the RRT Nurse Initiated Protocol BEFORE provider arrival Hospitalist only comes if additional support needed Primary Providers respond because they know the patient best 36
37 Communication 37
38 RRT Protocol Development Data-driven Evidence-based Separate protocol for stroke to facilitate timely treatment Multi-disciplinary development Multi-disciplinary approval REASON FOR RRT ACTIVATION 14% 34% Hypotension/ Tachycardia Chest Pain 24% SOB 22% 6% AMS Other 38

39 RRT Protocol-EHR Orderset 39
40 RRT Protocol-Clinical Algorithm 40
41 RRT Case Example RRT called for Elderly Patient with Acute Tachypnea Multiple co-morbidities CCU RN initiated the RRT Protocol Oxygen, fluid bolus, albuterol, ABG, and Chest X-Ray Patient found to have pneumonia Provider ordered antibiotics and placed patient on BiPAP 41
42 RRT Case Example RRT called for Post-Operative Patient with hypotension and tachycardia Otherwise healthy CCU RN initiated the RRT Protocol Oxygen, fluid bolus Patient found to be volume depleted Provider ordered additional fluid resuscitation 42
43 RRT Protocol-Clinical Algorithm 43
44 Rapid Response-Baseline Post RRT Outcomes/Diagnoses Stroke Activation STEMI Sepsis Bundle Code 4 44

45 Stroke Protocol-EHR orderset 45

46 Stroke Protocol-Clinical Algorithm 46

47 Don t Wait Time is Brain! 47



48 Stroke Protocol-Data Code Stroke Outcomes 3/1/ /1/ % 36% New or Worsening Stroke New non-stroke neuro diagnosis Ruled out 22% 48
49 Stroke Case-Example Elderly patient with new confusion and a positive FAST exam Admitted for urosepsis CCU RN initiated the Code Stroke Protocol CT scan completed Stroke Team activated Patient found to have a right sided infarct Received IV TPA in 27 minutes 49

50 Implementation Making the Work Happen Education Feedback Detailed data-tracking Sharing successes Drills 50


51 In-House Code Stroke Drill 51
 25 minutes per call No increase in the number of Code Blues")
52 Outcomes 2016 Data After Improvement 1 RRT call per day (~35 per month) 25 minutes per call No increase in the number of Code Blues 52





53 Outcomes RRT Outcomes RRT OUTCOMES-2016 Stabilized with RRT Interventions, 49% Stabilized with RRT Interventio ns, 67% Stabilized Transferred to a Higher Level of Care
54 Reduction in RRTs 180 RRTs and Code Blues (outside CCU) 03/ / Number of RRTs Number of Code Blues (outside CCU)

55 Questions and Comments? WSHA Contact: Ryan Hosken/ // The analyses upon which this publication is based were performed under Contract Number HHSM C entitled "Hospital Engagement Network 2.0 sponsored by the Centers for Medicare & Medicaid Services, Department of Health and Human Se rvices. 55
Measure Applications Partnership. Hospital Workgroup In-Person Meeting Follow- Up Call
 Measure Applications Partnership Hospital Workgroup In-Person Meeting Follow- Up Call December 21, 2016 Feedback on Current Measure Sets for IQR, HACs, Readmissions, and VBP 2 Previously Identified Crosscutting
Measure Applications Partnership Hospital Workgroup In-Person Meeting Follow- Up Call December 21, 2016 Feedback on Current Measure Sets for IQR, HACs, Readmissions, and VBP 2 Previously Identified Crosscutting
Quality & Hospital Acquired Conditions
 Quality & Hospital Acquired Conditions Rebecca Armbruster, DO, MS, FACOI Medical Director Resource Management Patricia Heys, BS Director of Infection Prevention & Control Sally Hinkle, DNP, MPA, RN Director
Quality & Hospital Acquired Conditions Rebecca Armbruster, DO, MS, FACOI Medical Director Resource Management Patricia Heys, BS Director of Infection Prevention & Control Sally Hinkle, DNP, MPA, RN Director
Using Big Data to Prevent Infections
 Using Big Data to Prevent Infections A thought paper by Scalable Health Big Data Analytics Reduces Infections in Hospitals Healthcare Associated Infections (HAIs) are developed while patients are receiving
Using Big Data to Prevent Infections A thought paper by Scalable Health Big Data Analytics Reduces Infections in Hospitals Healthcare Associated Infections (HAIs) are developed while patients are receiving
CMS Hospital Inpatient Quality Reporting (IQR) Program Measures for the FY 2019 Payment Update
 Program Measures for the FY 2019 Payment Update") CMS Inpatient Quality Reporting (IQR) Program Measures for the Update Measures Required to Meet IQR Program APU Requirements NHSN Submission CAUTI National Healthcare Safety Network (NHSN) Catheter-Associated
CMS Inpatient Quality Reporting (IQR) Program Measures for the Update Measures Required to Meet IQR Program APU Requirements NHSN Submission CAUTI National Healthcare Safety Network (NHSN) Catheter-Associated
CMS Hospital Inpatient Quality Reporting (IQR) Program Measures for the FY 2020 Payment Update
 Program Measures for the FY 2020 Payment Update") CMS Inpatient Quality Reporting (IQR) Program Measures for the Payment Update Measures Required to Meet IQR Program APU Requirements Healthcare-Associated Infection on CAUTI National Healthcare Safety
CMS Inpatient Quality Reporting (IQR) Program Measures for the Payment Update Measures Required to Meet IQR Program APU Requirements Healthcare-Associated Infection on CAUTI National Healthcare Safety
Nancy Hailpern, Director, Regulatory Affairs K Street, NW, Suite 1000 Washington, DC 20005
 Summary of Infection Prevention Issues in the Centers for Medicare & Medicaid Services (CMS) FY 2014 Inpatient Prospective Payment System (IPPS) Final Rule Hospital Readmissions Reduction Program-Fiscal
Summary of Infection Prevention Issues in the Centers for Medicare & Medicaid Services (CMS) FY 2014 Inpatient Prospective Payment System (IPPS) Final Rule Hospital Readmissions Reduction Program-Fiscal
AMI Talking Points. Provide appropriate treatment to Acute MI patients with these core measures:
 AMI Provide appropriate treatment to Acute MI patients with these core measures: Aspirin received within 24 hours of arrival or contraindication documented Primary PCI Received Within 90 Minutes of Hospital
AMI Provide appropriate treatment to Acute MI patients with these core measures: Aspirin received within 24 hours of arrival or contraindication documented Primary PCI Received Within 90 Minutes of Hospital
2016 Hospital Measures
 2016 Hospital Measures Vicki Tang Olson, Stratis Health Statewide Quality Reporting and Measurement System (SQRMS) Annual Forum June 22, 2015 Objectives Share the process used for 2016 hospital measures
2016 Hospital Measures Vicki Tang Olson, Stratis Health Statewide Quality Reporting and Measurement System (SQRMS) Annual Forum June 22, 2015 Objectives Share the process used for 2016 hospital measures
COOK COUNTY HEALTH Meaningful Metrics
 COOK COUNTY HEALTH Meaningful Metrics 2018-2019 Ronald Wyatt MD MHA January 18, 2019 2 Meaningful Measures 3 Meaningful Measures Framework Meaningful Measure Areas Achieve: High quality healthcare Meaningful
COOK COUNTY HEALTH Meaningful Metrics 2018-2019 Ronald Wyatt MD MHA January 18, 2019 2 Meaningful Measures 3 Meaningful Measures Framework Meaningful Measure Areas Achieve: High quality healthcare Meaningful
SEP-1 CHALLENGING CASES WITH DR. TOWNSEND
 UW MEDICINE PATIENTS ARE FIRST SEP-1 CHALLENGING CASES WITH DR. TOWNSEND AMADAE AREVALO RN, MSN, CCRN KATIE MEHRING RN, BSN, CCDS AMANDA SIGALA, RN, BSN, MPH, CPHQ JUNE 12, 2018 OBJECTIVES 1. Summarize
UW MEDICINE PATIENTS ARE FIRST SEP-1 CHALLENGING CASES WITH DR. TOWNSEND AMADAE AREVALO RN, MSN, CCRN KATIE MEHRING RN, BSN, CCDS AMANDA SIGALA, RN, BSN, MPH, CPHQ JUNE 12, 2018 OBJECTIVES 1. Summarize
Preventing Sepsis: A Community Based Approach. NYS Senior Action Council December 13, 2016 Eve Bankert MT (ASCP)
") Preventing Sepsis: A Community Based Approach NYS Senior Action Council December 13, 2016 Eve Bankert MT (ASCP) What is Sepsis? Sepsis is a life threatening condition that arises when the body s response
Preventing Sepsis: A Community Based Approach NYS Senior Action Council December 13, 2016 Eve Bankert MT (ASCP) What is Sepsis? Sepsis is a life threatening condition that arises when the body s response
PIN BENCHMARKING DATA DEFINITIONS DICTIONARY
 CORE MEASURES PIN BENCHMARKING DATA DEFINITIONS DICTIONARY 1 Total number of CAH acute care patient admissions. Report all CAH acute care only patient admissions for the quarter. Exclude CAH swing bed,
CORE MEASURES PIN BENCHMARKING DATA DEFINITIONS DICTIONARY 1 Total number of CAH acute care patient admissions. Report all CAH acute care only patient admissions for the quarter. Exclude CAH swing bed,
CMS Hospital IQR Program Measure Comparison Tables FY 2018 (CY 2016) Measures Required to Meet Hospital IQR APU Requirements NHSN Submission
 Measures Required to Meet Hospital IQR APU Requirements NHSN Submission") CMS IQR Program Measure Comparison Tables (CY 2016) NHSN Submission CLABSI Central Line-Associated Bloodstream Infection (CLABSI) Required NHSN CAUTI Catheter-Associated Urinary Tract Infection (CAUTI)
CMS IQR Program Measure Comparison Tables (CY 2016) NHSN Submission CLABSI Central Line-Associated Bloodstream Infection (CLABSI) Required NHSN CAUTI Catheter-Associated Urinary Tract Infection (CAUTI)
Saving Lives: Focusing on Severe Sepsis and Septic Shock
 Saving Lives: Focusing on Severe Sepsis and Septic Shock Deborah Cameron, RN, CPHQ Paul Pratt, RN Glenn Russ, RN Providence Little Company of Mary Medical Center San Pedro January 18, 2011 Objectives 1.
Saving Lives: Focusing on Severe Sepsis and Septic Shock Deborah Cameron, RN, CPHQ Paul Pratt, RN Glenn Russ, RN Providence Little Company of Mary Medical Center San Pedro January 18, 2011 Objectives 1.
Appendix G Explanation/Clarification Summary
 Appendix G Explanation/Clarification Summary Summary of Changes for Recommendations Alignment of measures with VBP by fiscal year Measures and service dates were adjusted to be consistent with the FY2016
Appendix G Explanation/Clarification Summary Summary of Changes for Recommendations Alignment of measures with VBP by fiscal year Measures and service dates were adjusted to be consistent with the FY2016
Target: STROKE. The Team-Based Approached
 Target: STROKE The Team-Based Approached November 19, 2013 Tuesday 1300 1400 Thank you for joining today s webinar, the presentation will begin shortly. A special thank you to Cornerstone Therapeutics
Target: STROKE The Team-Based Approached November 19, 2013 Tuesday 1300 1400 Thank you for joining today s webinar, the presentation will begin shortly. A special thank you to Cornerstone Therapeutics
NYSDOH Sepsis Q&A Session from February 2018 Data Abstraction Meetings Table of Content
 NYSDOH Sepsis Q&A Session from February 2018 Data Abstraction Meetings Table of Content Adherence variables Q: within 3 hours of the start datetime. How can we document that monotherapy was started before
NYSDOH Sepsis Q&A Session from February 2018 Data Abstraction Meetings Table of Content Adherence variables Q: within 3 hours of the start datetime. How can we document that monotherapy was started before
Inpatient Quality Reporting Program
 SEP-1 Early Management Bundle, Severe Sepsis/Septic Shock Part II Questions and Answers Moderator: Candace Jackson, RN Inpatient Quality Reporting (IQR) Program Lead Hospital Inpatient Value, Incentives,
SEP-1 Early Management Bundle, Severe Sepsis/Septic Shock Part II Questions and Answers Moderator: Candace Jackson, RN Inpatient Quality Reporting (IQR) Program Lead Hospital Inpatient Value, Incentives,
Inpatient Quality Reporting Program
 SEP-1 Early Management Bundle, Severe Sepsis/Septic Shock Part III: Measure updates and Abstraction Guidance Questions and Answers Moderator: Candace Jackson, RN Inpatient Quality Reporting (IQR) Program
SEP-1 Early Management Bundle, Severe Sepsis/Septic Shock Part III: Measure updates and Abstraction Guidance Questions and Answers Moderator: Candace Jackson, RN Inpatient Quality Reporting (IQR) Program
SEPSIS: GETTING STARTED
 SEPSIS: GETTING STARTED Ohio Sepsis Initiative July 15, 2015 SEPSIS INCIDENCE Definition: the number of severe sepsis or septic shock encounters using the following ICD-9 codes (995.91 Sepsis, 995.92 severe
SEPSIS: GETTING STARTED Ohio Sepsis Initiative July 15, 2015 SEPSIS INCIDENCE Definition: the number of severe sepsis or septic shock encounters using the following ICD-9 codes (995.91 Sepsis, 995.92 severe
SURVIVING SEPSIS: Early Management Saves Lives
 SURVIVING SEPSIS: Early Management Saves Lives Pat Posa RN, BSN, MSA System Performance Improvement Leader St. Joseph Mercy Health System Ann Arbor, MI Patricia.posa@stjoeshealth.org Objectives a. Understand
SURVIVING SEPSIS: Early Management Saves Lives Pat Posa RN, BSN, MSA System Performance Improvement Leader St. Joseph Mercy Health System Ann Arbor, MI Patricia.posa@stjoeshealth.org Objectives a. Understand
End-Stage Renal Disease Quality Incentive Program (ESRD QIP) Status Type NQF Measure Title
 Status Type NQF Measure Title") End-Stage Renal Disease Quality Incentive Program (ESRD QIP) Status Type NQF Measure Title NQF Status ID Implemented Outcome 1454 Proportion of patients with hypercalcemia 0256 Vascular Access Type Catheter
End-Stage Renal Disease Quality Incentive Program (ESRD QIP) Status Type NQF Measure Title NQF Status ID Implemented Outcome 1454 Proportion of patients with hypercalcemia 0256 Vascular Access Type Catheter
John Park, MD Assistant Professor of Medicine
 John Park, MD Assistant Professor of Medicine Faculty photo will be placed here park.john@mayo.edu 2015 MFMER 3543652-1 Sepsis Out with the Old, In with the New Mayo School of Continuous Professional Development
John Park, MD Assistant Professor of Medicine Faculty photo will be placed here park.john@mayo.edu 2015 MFMER 3543652-1 Sepsis Out with the Old, In with the New Mayo School of Continuous Professional Development
4. Which survey program does your facility use to get your program designated by the state?
 TRAUMA SURVEY Please complete one survey for each TCD designation you have in your facility. There would be a maximum of three surveys completed if your facility was designated as a trauma, stroke and
TRAUMA SURVEY Please complete one survey for each TCD designation you have in your facility. There would be a maximum of three surveys completed if your facility was designated as a trauma, stroke and
Sepsis 3 & Early Identification. Disclosures. Objectives 9/19/2016. David Carlbom, MD Medical Director, HMC Sepsis Program
 Sepsis 3 & Early Identification David Carlbom, MD Medical Director, HMC Sepsis Program Disclosures I have no relevant financial relationships with a commercial interest and will not discuss off-label use
Sepsis 3 & Early Identification David Carlbom, MD Medical Director, HMC Sepsis Program Disclosures I have no relevant financial relationships with a commercial interest and will not discuss off-label use
Wait, is this sepsis?
 Wait, is this sepsis? Reconciling Disparate Sepsis Definitions LAURA QUINNAN, M.D. NWH SEPSIS COMMITTEE CO-CHAIR, CHIEF OF MEDICINE AND MEDICAL DIRECTOR OF HOSPITALIST TEAM Goals Describe Sepsis-3 definitions
Wait, is this sepsis? Reconciling Disparate Sepsis Definitions LAURA QUINNAN, M.D. NWH SEPSIS COMMITTEE CO-CHAIR, CHIEF OF MEDICINE AND MEDICAL DIRECTOR OF HOSPITALIST TEAM Goals Describe Sepsis-3 definitions
Great Lakes Partners for Patients: Hospital Improvement Innovation Network - Encyclopedia of Measures Frequently Asked Questions
 Great Lakes Partners for Patients: Hospital Improvement Innovation Network - Encyclopedia of Measures Frequently Asked Questions Contents Great Lakes Partners for Patients: Hospital Improvement Innovation
Great Lakes Partners for Patients: Hospital Improvement Innovation Network - Encyclopedia of Measures Frequently Asked Questions Contents Great Lakes Partners for Patients: Hospital Improvement Innovation
FY X Time (48 hrs for cardiac surgery) SCIP-Inf-4 Cardiac Surgery Patients With Controlled 6 A.M. Postoperative Blood
 SCIP-Inf-4 Cardiac Surgery Patients With Controlled 6 A.M. Postoperative Blood") Valuebased 2013 Hospital Measure Summary Data Collection for Inpatient Quality Reporting FY2015 and Outpatient Reporting CY2014 January 2013 Key: = Required by both CMS and State of Minnesota = Required
Valuebased 2013 Hospital Measure Summary Data Collection for Inpatient Quality Reporting FY2015 and Outpatient Reporting CY2014 January 2013 Key: = Required by both CMS and State of Minnesota = Required
Sepsis Early Recognition and Management. Therese Hughes, PhD, MPA, RN
 Sepsis Early Recognition and Management Therese Hughes, PhD, MPA, RN 1 Sepsis a Deadly Progression Affects millions around the world each year, killing one in four Contributes to approximately 50% of all
Sepsis Early Recognition and Management Therese Hughes, PhD, MPA, RN 1 Sepsis a Deadly Progression Affects millions around the world each year, killing one in four Contributes to approximately 50% of all
Sepsis Story At Intermountain Healthcare Intensive Medicine Clinical Program
 Sepsis Story At Intermountain Healthcare 2004-2012 Intensive Medicine Clinical Program The International Surviving Sepsis Campaign Was Organized In 2002 During The ESICM International Meeting In Barcelona,
Sepsis Story At Intermountain Healthcare 2004-2012 Intensive Medicine Clinical Program The International Surviving Sepsis Campaign Was Organized In 2002 During The ESICM International Meeting In Barcelona,
MHA Keystone Center. MICAH QN Meeting May 18, 2018
 MHA Keystone Center MICAH QN Meeting May 18, 2018 Agenda ADEs due to Opioids measure Sepsis measures a) Post-Operative Sepsis (PSI-13) b) Sepsis Mortality Rate Falls with Injury measure Person & Family
MHA Keystone Center MICAH QN Meeting May 18, 2018 Agenda ADEs due to Opioids measure Sepsis measures a) Post-Operative Sepsis (PSI-13) b) Sepsis Mortality Rate Falls with Injury measure Person & Family
The Centers for Medicare & Medicaid Services (CMS) Acute Care Hospital Fiscal Year (FY) 2018 Quality Improvement Program Measures
 Acute Care Hospital Fiscal Year (FY) 2018 Quality Improvement Program Measures") ID M easure Name NQF # H os pital M easurement Period H os pital H os pital Value-Bas ed Purchas ing M easurement Period H os pital H ealth Record (EH R) Incentive M easurement Period H os pital H os pital-
ID M easure Name NQF # H os pital M easurement Period H os pital H os pital Value-Bas ed Purchas ing M easurement Period H os pital H ealth Record (EH R) Incentive M easurement Period H os pital H os pital-
2016 Sepsis Update: Pearls, Pitfalls, and Core Measure Quicksand
 2016 Sepsis Update: Pearls, Pitfalls, and Core Measure Quicksand Jack Perkins, MD FACEP, FAAEM, FACP Assistant Professor of Emergency and Internal Medicine Virginia Tech Carilion School of Medicine Why
2016 Sepsis Update: Pearls, Pitfalls, and Core Measure Quicksand Jack Perkins, MD FACEP, FAAEM, FACP Assistant Professor of Emergency and Internal Medicine Virginia Tech Carilion School of Medicine Why
CMS Measures - Fiscal Year 2019
 ID Me asure Name NQF # Value- (VBP) - (HACRP) (HRRP) ID Me asure Name NQF # Value- (VBP) - (HACRP) (HRRP) CMS s - Fiscal Year 2019 ID Name NQF # The Centers for Medicare & Medicaid Services (CMS) Improvement
ID Me asure Name NQF # Value- (VBP) - (HACRP) (HRRP) ID Me asure Name NQF # Value- (VBP) - (HACRP) (HRRP) CMS s - Fiscal Year 2019 ID Name NQF # The Centers for Medicare & Medicaid Services (CMS) Improvement
Staging Sepsis for the Emergency Department: Physician
 Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
SCORES FOR 4 TH QUARTER, RD QUARTER, 2014
 SCORES FOR 4 TH QUARTER, 2013 3 RD QUARTER, 2014 PATIENT SATISFACTION SCORES (HCAHPS): 4 STARS OUT OF 5 (ONLY 4 AREA ACUTE CARE HOSPITALS RECEIVED A 4-STAR RATING. NONE ACHIEVED 5-STARS). STRUCTURAL MEASURES:
SCORES FOR 4 TH QUARTER, 2013 3 RD QUARTER, 2014 PATIENT SATISFACTION SCORES (HCAHPS): 4 STARS OUT OF 5 (ONLY 4 AREA ACUTE CARE HOSPITALS RECEIVED A 4-STAR RATING. NONE ACHIEVED 5-STARS). STRUCTURAL MEASURES:
Troubleshooting Audio
 Welcome Audio for this event is available via ReadyTalk Internet streaming. No telephone line is required. Computer speakers or headphones are necessary to listen to streaming audio. Limited dial-in lines
Welcome Audio for this event is available via ReadyTalk Internet streaming. No telephone line is required. Computer speakers or headphones are necessary to listen to streaming audio. Limited dial-in lines
McHenry Western Lake County EMS System CE for Paramedics, EMT-B and PHRN s Sepsis Patients. November/December 2017
 McHenry Western Lake County EMS System CE for Paramedics, EMT-B and PHRN s Sepsis Patients November/December 2017 This month we are going to take a look at the patient with Sepsis. Webster s defines septic
McHenry Western Lake County EMS System CE for Paramedics, EMT-B and PHRN s Sepsis Patients November/December 2017 This month we are going to take a look at the patient with Sepsis. Webster s defines septic
Chasing Zero Infections Coaching Call No Catheter = No CAUTI: Reducing Catheter Utilization Feb. 13, 2018
 Chasing Zero Infections Coaching Call No Catheter = No CAUTI: Reducing Catheter Utilization Feb. 13, 2018 Agenda Welcome & FHA Mission to Care HIIN Trends and Progress: CAUTI and Device Utilization Cheryl
Chasing Zero Infections Coaching Call No Catheter = No CAUTI: Reducing Catheter Utilization Feb. 13, 2018 Agenda Welcome & FHA Mission to Care HIIN Trends and Progress: CAUTI and Device Utilization Cheryl
50198 Federal Register / Vol. 75, No. 157 / Monday, August 16, 2010 / Rules and Regulations
 50198 Federal Register / Vol. 75, No. 157 / Monday, August 16, 2010 / Rules and Regulations mstockstill on DSKH9S0YB1PROD with RULES2 VerDate Mar2010 17:02 Aug 13, 2010 Jkt 220001 PO 00000 Frm 00158
50198 Federal Register / Vol. 75, No. 157 / Monday, August 16, 2010 / Rules and Regulations mstockstill on DSKH9S0YB1PROD with RULES2 VerDate Mar2010 17:02 Aug 13, 2010 Jkt 220001 PO 00000 Frm 00158
Sepsis! Dr Eric Van Den Bergh Consultant in Emergency Medicine 2015
 Sepsis! Dr Eric Van Den Bergh Consultant in Emergency Medicine 2015 Annual UK Mortality Sepsis Stroke Heart attack COPD Lung cancer COPD Heart attack Stroke Sepsis Lung cancer 0 10000 20000 30000 40000
Sepsis! Dr Eric Van Den Bergh Consultant in Emergency Medicine 2015 Annual UK Mortality Sepsis Stroke Heart attack COPD Lung cancer COPD Heart attack Stroke Sepsis Lung cancer 0 10000 20000 30000 40000
Welcome and Instructions
 Welcome and Instructions For audio, join by telephone at 877-594-8353, participant code 56350822# Your line is OPEN. Please do not use the hold feature on your phone but do mute your line by dialing *6.
Welcome and Instructions For audio, join by telephone at 877-594-8353, participant code 56350822# Your line is OPEN. Please do not use the hold feature on your phone but do mute your line by dialing *6.
Core Measures SEPSIS UPDATES
 Patricia Walker, RN-BC, BSN Evidence Based Practice Manager Quality Management Services UCLA Health System, Ronald Reagan Medical Center Core Measures SEPSIS UPDATES Severe Sepsis and Septic Shock Based
Patricia Walker, RN-BC, BSN Evidence Based Practice Manager Quality Management Services UCLA Health System, Ronald Reagan Medical Center Core Measures SEPSIS UPDATES Severe Sepsis and Septic Shock Based
Medicare Value Based Purchasing Andrew B. Wheeler Vice President of Federal Finance
 Medicare Value Based Purchasing - 101 Andrew B. Wheeler Vice President of Federal Finance What is Medicare s VBP System? Incentive program to improve outcomes, safety, patient satisfaction, and efficiency
Medicare Value Based Purchasing - 101 Andrew B. Wheeler Vice President of Federal Finance What is Medicare s VBP System? Incentive program to improve outcomes, safety, patient satisfaction, and efficiency
Stratis Health
 2017 Hospital Measure Summary Minnesota Statewide Quality eporting & Measurement System (SQMS) and FY2019 for Center for Medicare & Medicaid Services (CMS) Contents Key... 1 Chart Abstracted Measures...
2017 Hospital Measure Summary Minnesota Statewide Quality eporting & Measurement System (SQMS) and FY2019 for Center for Medicare & Medicaid Services (CMS) Contents Key... 1 Chart Abstracted Measures...
PHYSIOLOGY AND MANAGEMENT OF THE SEPTIC PATIENT
 PHYSIOLOGY AND MANAGEMENT OF THE SEPTIC PATIENT Melanie Sanchez, RN, MSNE, OCN, CCRN Clinical Nurse III City of Hope National Medical Center HOW THE EXPERTS TREAT HEMATOLOGIC MALIGNANCIES LAS VEGAS, NV
PHYSIOLOGY AND MANAGEMENT OF THE SEPTIC PATIENT Melanie Sanchez, RN, MSNE, OCN, CCRN Clinical Nurse III City of Hope National Medical Center HOW THE EXPERTS TREAT HEMATOLOGIC MALIGNANCIES LAS VEGAS, NV
Statit pimd Client Panel. Guy March, Product Lead, Midas+ Statit
 Statit pimd Client Panel Guy March, Product Lead, Midas+ Statit Statit pimd/ppr Statit Software Started ~25 years ago Currently serving 650 hospitals Guy March Working with Statit QC products for over
Statit pimd Client Panel Guy March, Product Lead, Midas+ Statit Statit pimd/ppr Statit Software Started ~25 years ago Currently serving 650 hospitals Guy March Working with Statit QC products for over
LINKS OF INTEREST DISCLOSURE
 LINKS OF INTEREST DISCLOSURE Name of the speaker: Sarah L. Krein I have no link of interest. www.sf2h.net 7, 8 et 9 juin 2017 And what about getting rid of catheter-associated urinary tract infections?
LINKS OF INTEREST DISCLOSURE Name of the speaker: Sarah L. Krein I have no link of interest. www.sf2h.net 7, 8 et 9 juin 2017 And what about getting rid of catheter-associated urinary tract infections?
Knowledge to Practice; Applying New Skills
 Knowledge to Practice; Applying New Skills Linda R. Greene, RN, BS, MPS,CIC UR Highland Hospital Rochester, NY linda_greene@urmc.rochester.edu Kim M. Delahanty, RN, BSN, PHN,MBA/HCM,CIC UCSD Health System
Knowledge to Practice; Applying New Skills Linda R. Greene, RN, BS, MPS,CIC UR Highland Hospital Rochester, NY linda_greene@urmc.rochester.edu Kim M. Delahanty, RN, BSN, PHN,MBA/HCM,CIC UCSD Health System
C E R T I FI C AT I O N. Benchmarking Performance in HFAP-certified Primary Stroke Centers
 PRIMARY STROKE C E R T I FI C AT I O N Benchmarking Performance in HFAP-certified Primary Stroke Centers HFAP s mission is to advance high quality patient care and safety through objective application
PRIMARY STROKE C E R T I FI C AT I O N Benchmarking Performance in HFAP-certified Primary Stroke Centers HFAP s mission is to advance high quality patient care and safety through objective application
Great Lakes Partners for Patients: Hospital Improvement Innovation Network - Encyclopedia of Measures Frequently Asked Questions
 Great Lakes Partners for Patients: Hospital Improvement Innovation Network - Encyclopedia of Measures Frequently Asked Questions Contents Great Lakes Partners for Patients: Hospital Improvement Innovation
Great Lakes Partners for Patients: Hospital Improvement Innovation Network - Encyclopedia of Measures Frequently Asked Questions Contents Great Lakes Partners for Patients: Hospital Improvement Innovation
Our Commitment to Quality and Patient Safety Core Measures
 Calvert Memorial Hospital is committed to our community, with a focus on patient-centered care. High quality and safe patient care is not our goal, it is our priority. That means delivering the best possible
Calvert Memorial Hospital is committed to our community, with a focus on patient-centered care. High quality and safe patient care is not our goal, it is our priority. That means delivering the best possible
Patient Safety Safe Table Webcast: Sepsis (Part III and IV) December 17, 2014
 December 17, 2014") Patient Safety Safe Table Webcast: Sepsis (Part III and IV) December 17, 2014 Presenters Mark Blaney, RN Regional Nurse Educator CHI Franciscan Health Karen Lautermilch Director, Quality & Performance
Patient Safety Safe Table Webcast: Sepsis (Part III and IV) December 17, 2014 Presenters Mark Blaney, RN Regional Nurse Educator CHI Franciscan Health Karen Lautermilch Director, Quality & Performance
Great Lakes Partners for Patients: Hospital Improvement Innovation Network - Encyclopedia of Measures Frequently Asked Questions
 Great Lakes Partners for Patients: Hospital Improvement Innovation Network - Encyclopedia of Measures Frequently Asked Questions Contents Great Lakes Partners for Patients: Hospital Improvement Innovation
Great Lakes Partners for Patients: Hospital Improvement Innovation Network - Encyclopedia of Measures Frequently Asked Questions Contents Great Lakes Partners for Patients: Hospital Improvement Innovation
Troubleshooting Audio
 Welcome Audio for this event is available via ReadyTalk Internet streaming. No telephone line is required. Computer speakers or headphones are necessary to listen to streaming audio. Limited dial-in lines
Welcome Audio for this event is available via ReadyTalk Internet streaming. No telephone line is required. Computer speakers or headphones are necessary to listen to streaming audio. Limited dial-in lines
Standards of excellence
 The Accreditation Canada Stroke Distinction program was launched in March 2010 to offer a rigorous and highly specialized process above and beyond the requirements of Qmentum. The comprehensive Stroke
The Accreditation Canada Stroke Distinction program was launched in March 2010 to offer a rigorous and highly specialized process above and beyond the requirements of Qmentum. The comprehensive Stroke
Hospital Transition Management. Barbara Wood, BSN, MBA
 Hospital Transition Management Barbara Wood, BSN, MBA Director, Embedded Care Management Programs OBJECTIVES Improve health care quality for our patients by streamlining care transitions Reduce avoidable
Hospital Transition Management Barbara Wood, BSN, MBA Director, Embedded Care Management Programs OBJECTIVES Improve health care quality for our patients by streamlining care transitions Reduce avoidable
Improving Quality of Care for Medicare Patients: Accountable Care Organizations
 DEPARTMENT OF HEALTH & HUMAN SERVICES Centers for Medicare & Medicaid Services Room 352-G 200 Independence Avenue, SW Washington, DC 20201 Office of Media Affairs MEDICARE FACT SHEET FOR IMMEDIATE RELEASE
DEPARTMENT OF HEALTH & HUMAN SERVICES Centers for Medicare & Medicaid Services Room 352-G 200 Independence Avenue, SW Washington, DC 20201 Office of Media Affairs MEDICARE FACT SHEET FOR IMMEDIATE RELEASE
Evolutions in Geriatric Fracture Care Preparing for the Silver Tsunami
 Evolutions in Geriatric Fracture Care Preparing for the Silver Tsunami James Holstine, DO Medical Director for the Joint Replacement Center, Geriatric Fracture Center, Orthopedic Surgeon PeaceHealth Whatcom
Evolutions in Geriatric Fracture Care Preparing for the Silver Tsunami James Holstine, DO Medical Director for the Joint Replacement Center, Geriatric Fracture Center, Orthopedic Surgeon PeaceHealth Whatcom
Sepsis Awareness and Education
 Sepsis Awareness and Education Meets the updated New York State Department of Health (NYSDOH) requirements for Infection Control and Barrier Precautions coursework Element VII: Sepsis Awareness and Education
Sepsis Awareness and Education Meets the updated New York State Department of Health (NYSDOH) requirements for Infection Control and Barrier Precautions coursework Element VII: Sepsis Awareness and Education
SUCCESS IN SEPSIS MORTALITY REDUCTION. Maryanne Whitney RN MSN CNS Improvement Advisor, Cynosure Health HRET HEN AK Webinar
 SUCCESS IN SEPSIS MORTALITY REDUCTION Maryanne Whitney RN MSN CNS Improvement Advisor, Cynosure Health HRET HEN AK Webinar Got Sepsis? Now What?- Alerts & Bundles Maryanne Whitney RN, MS, CNS Improvement
SUCCESS IN SEPSIS MORTALITY REDUCTION Maryanne Whitney RN MSN CNS Improvement Advisor, Cynosure Health HRET HEN AK Webinar Got Sepsis? Now What?- Alerts & Bundles Maryanne Whitney RN, MS, CNS Improvement
Sepsis. Reliability- can we achieve Dr Ron Daniels
 Sepsis. Reliability- can we achieve it? @SepsisUK Dr Ron Daniels Chief Executive, Global Sepsis Alliance Fellow: NHS Improvement Faculty Chief Executive: United Kingdom Sepsis Trust & Chair, UK SSC RRAILS
Sepsis. Reliability- can we achieve it? @SepsisUK Dr Ron Daniels Chief Executive, Global Sepsis Alliance Fellow: NHS Improvement Faculty Chief Executive: United Kingdom Sepsis Trust & Chair, UK SSC RRAILS
convey the clinical quality measure's title, number, owner/developer and contact
 CMS-0033-P 153 convey the clinical quality measure's title, number, owner/developer and contact information, and a link to existing electronic specifications where applicable. TABLE 20: Proposed Clinical
CMS-0033-P 153 convey the clinical quality measure's title, number, owner/developer and contact information, and a link to existing electronic specifications where applicable. TABLE 20: Proposed Clinical
IDENTIFYING SEPSIS IN THE PREHOSPITAL SETTING
 IDENTIFYING SEPSIS IN THE PREHOSPITAL SETTING Christopher Hunter, MD, PhD, FACEP Director, Health Services Department Associate Medical Director, Orange County EMS System Medical Director, Orlando Health
IDENTIFYING SEPSIS IN THE PREHOSPITAL SETTING Christopher Hunter, MD, PhD, FACEP Director, Health Services Department Associate Medical Director, Orange County EMS System Medical Director, Orlando Health
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv
 Rv") ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv.8.18.18 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) SUDDEN PROGRESSIVE FORM OF ACUTE RESPIRATORY FAILURE ALVEOLAR CAPILLARY MEMBRANE BECOMES DAMAGED AND MORE
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv.8.18.18 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) SUDDEN PROGRESSIVE FORM OF ACUTE RESPIRATORY FAILURE ALVEOLAR CAPILLARY MEMBRANE BECOMES DAMAGED AND MORE
Moving from VAP to VAC
 Moving from VAP to VAC Cindy Munro, PhD, RN, ANP-BC, FAANP, FAAN Associate Dean of Research and Innovation Professor College of Nursing Conflict of interest: No relationships with pharmaceutical companies,
Moving from VAP to VAC Cindy Munro, PhD, RN, ANP-BC, FAANP, FAAN Associate Dean of Research and Innovation Professor College of Nursing Conflict of interest: No relationships with pharmaceutical companies,
Sepsis 3.0: The Impact on Quality Improvement Programs
 Sepsis 3.0: The Impact on Quality Improvement Programs Mitchell M. Levy MD, MCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care Warren Alpert Medical School of Brown University
Sepsis 3.0: The Impact on Quality Improvement Programs Mitchell M. Levy MD, MCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care Warren Alpert Medical School of Brown University
Performance Measure. Inpatient Clinical Process of Care Measures
 Acute Myocardial Infarction (AMI) 's Maryland Hospital Performance Evaluation System: Inpatient s Quality Based Reimbursement () Measures Highlighted in Green (02/27/2014) Inpatient Clinical Process of
Acute Myocardial Infarction (AMI) 's Maryland Hospital Performance Evaluation System: Inpatient s Quality Based Reimbursement () Measures Highlighted in Green (02/27/2014) Inpatient Clinical Process of
Inpatient Quality Reporting (IQR) Program
 Program") The Clinician Perspective on Sepsis Care: Early Management Bundle for Severe Sepsis/Septic Shock Questions & Answers Moderator Candace Jackson, RN Project Lead, Hospital Inpatient Quality Reporting (IQR)
The Clinician Perspective on Sepsis Care: Early Management Bundle for Severe Sepsis/Septic Shock Questions & Answers Moderator Candace Jackson, RN Project Lead, Hospital Inpatient Quality Reporting (IQR)
Troubleshooting Audio
 Welcome! Audio for this event is available via ReadyTalk Internet Streaming. No telephone line is required. Computer speakers or headphones are necessary to listen to streaming audio. Limited dial-in lines
Welcome! Audio for this event is available via ReadyTalk Internet Streaming. No telephone line is required. Computer speakers or headphones are necessary to listen to streaming audio. Limited dial-in lines
Diagnosis: Allergies:
 Patient Name: Diagnosis: Allergies: ICU Sepsis Version 5 1/11/17 This order set must be used with an admission order set if patient not already admitted. Nursing Orders Verify that cultures have been obtained
Patient Name: Diagnosis: Allergies: ICU Sepsis Version 5 1/11/17 This order set must be used with an admission order set if patient not already admitted. Nursing Orders Verify that cultures have been obtained
Publicly Reported Quality Measures
 Publicly Reported Quality Measures Five-Star Quality Rating System As part of the initiative to add five-star quality ratings to its Compare Web sites, the Centers for Medicare & Medicaid Services (CMS)
Publicly Reported Quality Measures Five-Star Quality Rating System As part of the initiative to add five-star quality ratings to its Compare Web sites, the Centers for Medicare & Medicaid Services (CMS)
Quality Data on Core Measures
 Quality Data on Core Measures The Centers for Medicare and Medicaid (CMS) have developed several measurements to reflect the quality of care in hospitals. They include pneumonia, surgical care, heart failure
Quality Data on Core Measures The Centers for Medicare and Medicaid (CMS) have developed several measurements to reflect the quality of care in hospitals. They include pneumonia, surgical care, heart failure
Sepsis Update: Early Identification and Management
 Sepsis Update: Early Identification and Management Q&A From the Live Webinar Presenter: Tom Ahrens, RN, PhD, FAAN Live webinar: Thursday, May 09, 2013 The AACN Critical Care Webinar Series is not only
Sepsis Update: Early Identification and Management Q&A From the Live Webinar Presenter: Tom Ahrens, RN, PhD, FAAN Live webinar: Thursday, May 09, 2013 The AACN Critical Care Webinar Series is not only
2016 AMC Quality and Accountability Performance Scorecard Vidant Medical Center. Overall Rank. Overall Score 63.4% Efficiency 7.
 2016 AMC Quality and Accountability Performance Scorecard Vidant Medical Center Star Rating Mortality 12.66% of 25% Domain Performance Overall Rank 27 Overall Score 63.4% Equity 5.00% of 5% Efficiency
2016 AMC Quality and Accountability Performance Scorecard Vidant Medical Center Star Rating Mortality 12.66% of 25% Domain Performance Overall Rank 27 Overall Score 63.4% Equity 5.00% of 5% Efficiency
Primary Stroke Center Quality & Performance Measures
 Primary Stroke Center Quality & Performance Measures This section of the manual contains information related to the quality performance of Primary Stroke Centers. Brain Attack Coalition Definitions Recognition
Primary Stroke Center Quality & Performance Measures This section of the manual contains information related to the quality performance of Primary Stroke Centers. Brain Attack Coalition Definitions Recognition
Objectives. Medicare Spending per Beneficiary: Analyzing MSPB Data to Identify Primary Drivers
 Medicare Spending per Beneficiary: Analyzing MSPB Data to Identify Primary Drivers August 22, 2017 Objectives Understand the basics of the hospital specific MSPB data files and reports Review the factors
Medicare Spending per Beneficiary: Analyzing MSPB Data to Identify Primary Drivers August 22, 2017 Objectives Understand the basics of the hospital specific MSPB data files and reports Review the factors
Q1 Contact Information
 Q1 Contact Information Answered: 7 Skipped: 0 ANSWER CHOICES Hospital Name of Person Completing Survey Email RESPONSES 100.00% 7 100.00% 7 100.00% 7 # HOSPITAL DATE 1 Saint Luke's Hospital of Kansas City
Q1 Contact Information Answered: 7 Skipped: 0 ANSWER CHOICES Hospital Name of Person Completing Survey Email RESPONSES 100.00% 7 100.00% 7 100.00% 7 # HOSPITAL DATE 1 Saint Luke's Hospital of Kansas City
4/1/2014 ICD-10 CM/PCS. Benefits to ICD-10. Fewer queries and/or requests for additional clarification. Fewer denials based on medical necessity
 Clinical Documentation and ICD-10 Presented by: Altegra Health 1 ICD-10 CM/PCS ICD-10 will be the official HIPAA-transaction set to communicate all patient conditions and all inpatient treatments, beginning
Clinical Documentation and ICD-10 Presented by: Altegra Health 1 ICD-10 CM/PCS ICD-10 will be the official HIPAA-transaction set to communicate all patient conditions and all inpatient treatments, beginning
Mandatory Elements of Healthcare Reform Walter Coleman. healthcare consulting
 Mandatory Elements of Healthcare Reform Walter Coleman 1 Agenda ACA Mandatory Elements of Reform Value Based Purchasing Readmission Reduction Program Hospital Acquired Conditions Best practices to analyze
Mandatory Elements of Healthcare Reform Walter Coleman 1 Agenda ACA Mandatory Elements of Reform Value Based Purchasing Readmission Reduction Program Hospital Acquired Conditions Best practices to analyze
Troubleshooting Audio
 Welcome! Audio for this event is available via ReadyTalk Internet Streaming. No telephone line is required. Computer speakers or headphones are necessary to listen to streaming audio. Limited dial-in lines
Welcome! Audio for this event is available via ReadyTalk Internet Streaming. No telephone line is required. Computer speakers or headphones are necessary to listen to streaming audio. Limited dial-in lines
No conflicts of interest
 Robert M. Rodriguez, MD FAAEM Clinical Professor of Medicine and Emergency Medicine, UCSF No conflicts of interest Major Points Most ICU patients start in ED Chain of critical care starting in field and
Robert M. Rodriguez, MD FAAEM Clinical Professor of Medicine and Emergency Medicine, UCSF No conflicts of interest Major Points Most ICU patients start in ED Chain of critical care starting in field and
Frank Sebat, MD - June 29, 2006
 Types of Shock Hypovolemic Shock Low blood volume decreasing cardiac output. AN INTEGRATED SYSTEM OF CARE FOR PATIENTS AT RISK SHOCK TEAM and RAPID RESPONSE TEAM Septic or Distributive Shock Decrease in
Types of Shock Hypovolemic Shock Low blood volume decreasing cardiac output. AN INTEGRATED SYSTEM OF CARE FOR PATIENTS AT RISK SHOCK TEAM and RAPID RESPONSE TEAM Septic or Distributive Shock Decrease in
The research questions are presented in priority order, and are further elaborated with lay summaries and three-part questions where applicable.
 Top 30 Emergency Medicine Research Priorities 23 January 2017 The rankings were established by consensus at the final prioritisation workshop run by the James Lind Alliance Emergency Medicine Priority
Top 30 Emergency Medicine Research Priorities 23 January 2017 The rankings were established by consensus at the final prioritisation workshop run by the James Lind Alliance Emergency Medicine Priority
Infection Control: Meeting the Challenge
 22nd Annual Midas+ User Symposium June 2 5, 2013 Tucson, Arizona Infection Control: Meeting the Challenge Wednesday, June 5, 2:30 pm The data demands placed on Infection Control departments have significantly
22nd Annual Midas+ User Symposium June 2 5, 2013 Tucson, Arizona Infection Control: Meeting the Challenge Wednesday, June 5, 2:30 pm The data demands placed on Infection Control departments have significantly
Documenting in the World of ICD-10 Capturing all your CCs and MCCs Crystal Coen, RN, MSN, FNP-BC NPSS Asheville, NC
 Documenting in the World of ICD-10 Capturing all your CCs and MCCs Crystal Coen, RN, MSN, FNP-BC 2017 NPSS Asheville, NC Objectives Understand the importance of documenting to the highest specificity Understand
Documenting in the World of ICD-10 Capturing all your CCs and MCCs Crystal Coen, RN, MSN, FNP-BC 2017 NPSS Asheville, NC Objectives Understand the importance of documenting to the highest specificity Understand
Hospital Inpatient Quality Reporting (IQR) Program
 Program") SEP-1 Early Management Bundle, Severe Sepsis/Septic Shock: v5.4 Measure Updates Presentation Transcript Speakers Noel Albritton, RN, BS Lead Solutions Specialist Hospital Inpatient and Outpatient Process
SEP-1 Early Management Bundle, Severe Sepsis/Septic Shock: v5.4 Measure Updates Presentation Transcript Speakers Noel Albritton, RN, BS Lead Solutions Specialist Hospital Inpatient and Outpatient Process
R-SCAN: Engaging Clinicians in Value-based Care
 R-SCAN: Engaging Clinicians in Value-based Care Nancy Fredericks, MBA R-SCAN Director rscan.org What is R-SCAN? A collaborative between referring clinicians and radiologists to improve patient care R-SCAN
R-SCAN: Engaging Clinicians in Value-based Care Nancy Fredericks, MBA R-SCAN Director rscan.org What is R-SCAN? A collaborative between referring clinicians and radiologists to improve patient care R-SCAN
2016 Report Card Gwen Neilsen Anderson Rehabilitation Center Inpatient Rehabilitation Unit. stlukesonline.org
 2016 Report Card Gwen Neilsen Anderson Rehabilitation Center Inpatient Rehabilitation Unit stlukesonline.org Why the Gwen Neilsen Anderson Rehabilitation Center? The Gwen Neilsen Anderson Rehabilitation
2016 Report Card Gwen Neilsen Anderson Rehabilitation Center Inpatient Rehabilitation Unit stlukesonline.org Why the Gwen Neilsen Anderson Rehabilitation Center? The Gwen Neilsen Anderson Rehabilitation
CEDR 2018 QCDR Measures for CMS 2018 MIPS Performance Year Reporting
 ACEP19 Emergency Department Utilization of CT for Minor Blunt Head Trauma for Aged 18 Years and Older Percentage of visits for aged 18 years and older who presented with a minor blunt head trauma who had
ACEP19 Emergency Department Utilization of CT for Minor Blunt Head Trauma for Aged 18 Years and Older Percentage of visits for aged 18 years and older who presented with a minor blunt head trauma who had
Written 01/09/17 Rewritten 3/29/17 for Interior Regional EMS Symposium
 Written 01/09/17 Rewritten 3/29/17 for Interior Regional EMS Symposium MARIA E. MANDICH MD Fairbanks Memorial Hospital Emergency Department Attending Physician Interior Region EMS Council Medical Director
Written 01/09/17 Rewritten 3/29/17 for Interior Regional EMS Symposium MARIA E. MANDICH MD Fairbanks Memorial Hospital Emergency Department Attending Physician Interior Region EMS Council Medical Director
Do Specialized Units Improve Outcomes?
 Do Specialized Units Improve Outcomes? Gordon D. Rubenfeld, MD MSc Professor of Medicine, University of Toronto Chief, Program in Trauma, Emergency, and Critical Care Sunnybrook Health Sciences Centre
Do Specialized Units Improve Outcomes? Gordon D. Rubenfeld, MD MSc Professor of Medicine, University of Toronto Chief, Program in Trauma, Emergency, and Critical Care Sunnybrook Health Sciences Centre
SEPSIS: IT ALL BEGINS WITH INFECTION. Theresa Posani, MS, RN, ACNS-BC, CCRN M/S CNS/Sepsis Coordinator Texas Health Harris Methodist Ft.
 SEPSIS: IT ALL BEGINS WITH INFECTION Theresa Posani, MS, RN, ACNS-BC, CCRN M/S CNS/Sepsis Coordinator Texas Health Harris Methodist Ft. Worth 1 2 3 OBJECTIVES Review the new Sepsis 3 definitions of sepsis
SEPSIS: IT ALL BEGINS WITH INFECTION Theresa Posani, MS, RN, ACNS-BC, CCRN M/S CNS/Sepsis Coordinator Texas Health Harris Methodist Ft. Worth 1 2 3 OBJECTIVES Review the new Sepsis 3 definitions of sepsis
UCLA Health System Apr - Jun 2013 (Q2)
") Denom Observed VBP Standard VBP Benchmark Denom Observed VBP Standard VBP Benchmark N Percent x/n N Percent x/n Value Based Purchasing-Clinical Process of Care Measures (%) SCIP-Inf-9 Urinary catheter
Denom Observed VBP Standard VBP Benchmark Denom Observed VBP Standard VBP Benchmark N Percent x/n N Percent x/n Value Based Purchasing-Clinical Process of Care Measures (%) SCIP-Inf-9 Urinary catheter
Inpatient Quality Reporting (IQR) Program
 Program") Hypotension Inpatient Quality Reporting (IQR) Program SEP-1 Early Management Bundle, Severe Sepsis/ Septic Shock: v5.1 Measure Updates Questions and Answers Moderator: Candace Jackson, RN Project Lead,
Hypotension Inpatient Quality Reporting (IQR) Program SEP-1 Early Management Bundle, Severe Sepsis/ Septic Shock: v5.1 Measure Updates Questions and Answers Moderator: Candace Jackson, RN Project Lead,
Core = Core required measures for all CAH nationally r = Required by State of Minnesota X = Additional for MBQIP
 Key: 2016 Hospital Measure Summary Minnesota Statewide Quality eporting and Measurement System (SQMS) and FY2018 for Center for Medicare and Medicaid Services () January 2016 = equired by Core = Core required
Key: 2016 Hospital Measure Summary Minnesota Statewide Quality eporting and Measurement System (SQMS) and FY2018 for Center for Medicare and Medicaid Services () January 2016 = equired by Core = Core required
Bedside assessment of fluid status
 Bedside assessment of fluid status 2nd AKI Academy October 18 th 2014 David Treacher Guy s & St Thomas NHS Trust Assessing the circulation - the 3 key questions v Is my patient adequately filled? v What
Bedside assessment of fluid status 2nd AKI Academy October 18 th 2014 David Treacher Guy s & St Thomas NHS Trust Assessing the circulation - the 3 key questions v Is my patient adequately filled? v What
Physician's Core Measure Pocket Guide AMI
 Physician's Core Measure Pocket Guide Core Measure Hotline: Ext. 4448 http://centegramedsource.com Indicator: AMI AMI VER. 9/2018 MUST document WHY no ASA unless there is documentation of contraindication
Physician's Core Measure Pocket Guide Core Measure Hotline: Ext. 4448 http://centegramedsource.com Indicator: AMI AMI VER. 9/2018 MUST document WHY no ASA unless there is documentation of contraindication
Sepsis. Patient Information
 Sepsis Patient Information This leaflet aims to answer your questions about what the Sepsis is. It will explain the signs and symptoms of sepsis, treatment of sepsis and information about what Brighton
Sepsis Patient Information This leaflet aims to answer your questions about what the Sepsis is. It will explain the signs and symptoms of sepsis, treatment of sepsis and information about what Brighton