BRAIN. Tumor byproducts. Autonomic nerves. Somatic nerves. Host immune cells. Cytokines
|
|
|
- Cameron Fox
- 6 years ago
- Views:
Transcription
1 Patient s Problems Pain (80%) Fatigue (90%) Weight Loss (80%) Lack of Appetite (80%) Nausea, Vomiting (90%) Anxiety (25%) Shortness of Breath (50%) Confusion-Agitation (80%)
2 Tumor Mass Tumor Function Somatic nerves Autonomic nerves Tumor byproducts Host immune cells Cytokines BRAIN Fatigue Delirium Pain Depression Anxiety sedation PC Assessment
3 Delirium Global brain failure The way most of us here will die
4 A Big Problem Frequent neuro-psychiatric complication Distressing to patients and caregivers Associated with poor prognosis Negative impact on Symptom expression Interventions (e.g. counseling) Communication Decision making
5 Delirium Confusion (time, space, recent memory) Hallucinations tactile! Delusions Agitation Disinhibition: symptoms or emotions!!

6
7 2 MAJOR DISORDERS OF COGNITION DELIRIUM AND DEMENTIA DELIRIUM: - Usually acute in onset - Relatively brief in duration - Fluctuating level of consciousness - Can be reversible DEMENTIA: - Intellectual deterioration of protracted & usually irreversible nature - Delirium reported to be most common OMS in Cancer PTS
8 Differential diagnosis Dementia (easy from history) Sedation (opioids) Obstructive sleep apnea (Reddy 2008) Depression (60% delirium referrals) Anxiety/ manic episode Akathisia
9 Dementia/ nursing home Delirium due to multiple causes!!!: MI, fracture, UTI, urinary retention Frequent mixed syndromes: delirium + dementia+ depression+ pain.
10 Tumor byproducts and host cytokines OPIOIDS and other drugs (psych!!) Metabolic N a, Ca, Creat Chemo Delirium Sepsis Dehydration CNS Involvement
11 COGNITIVE FAILURE IN CANCER PATIENTS 71 PATIENTS APPROACHED 67 CONSENTED 13 (19%) MMSE <24/30 54 (81%) MMSE 24/30 8/13 (62%)* DROP OUT BEFORE STUDY COMPLETED 6/54 (11%)* DROP OUT BEFORE STUDY COMPLETED * p,0.01, χ 2 Test Bruera et al, Lancet, 1993
12 Cognitive Failure (CF) Prospective study, 61 consecutive admissions to PCU CF determined by MMSE* CF present in 16/47 (83%) before death 22/66 (33%) improved with or without treatment Physician and nurse missed 15/66 (23%) and 13/66 (20%) of episodes of CF *Mini Mental State Questionnaire Bruera et al. J Pain Symptom Manage 1993
13
14
15 Terminal Delirium Memorial Delirium Assessment Scale Avg MDAS (alive) Avg MDAS (dead) Average MDAS score Days from death
16
17 Delirium 85% cancer pts before death Multicausal 80% of brain is GABA Disinhibition: expression of symptoms and emotions
18

19 Delgado-Guay MO, Yennurajalingam S, Bruera E. JPSM 2008; 36(4): 444
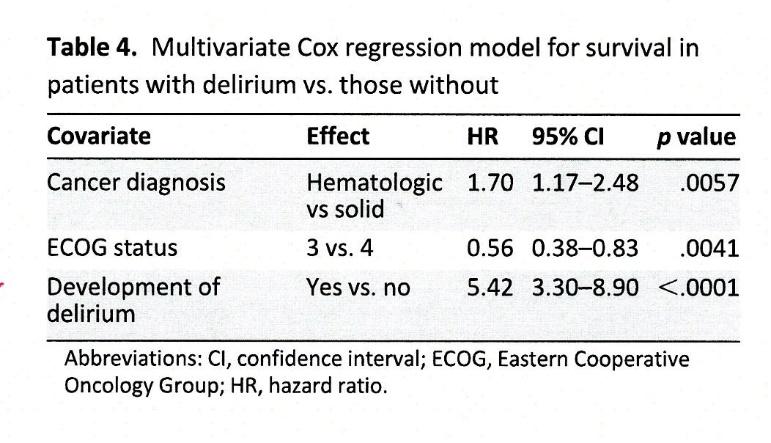
20 Hematological CA consults more delirium( Fadul, JPM 2008) 125 consecutive hematol: 51 delirium (41%) 125 consecutive solid: 20 delirium ( 16%, p<0.001) Median interval consult/ death: Hematol 13 days; solid 46 days (p=001) Hematol <pain &>sedation Similar symptom distress score
21 ICU Pall care consults (Delgado-Guay M, Cancer 2009) 88/ 1607 Pall care consults were ICU (5%) 71/88 pts had delirium ( 81%) 31/71 pts delirium resolved ( 44%) 37/88 consults d/c home (42%) 12/ 35 ICU- PCU transfers d/c home (34%)
22 Frequency and outcome of delirium among cancer patients admitted to the PCU. De La Cruz M et al. The oncologist /556 (58%) consecutive admissions had delirium ( MDAS score >7/30) 229(71%) delirium upon admission(41% of admissions) and 94 (29% after admission) 26% of delirium episodes reversed Overall survival of delirium pts shorter Delirium AFTER admission to PCU: lower reversal and worse survival!!
23
24
25 Occurrence and Reversibility of Delirium Prospective study, admissions to PCU 44/104 (42%) delirium on admission 71/104 (68%) delirium at some stage 46 of 52 who died (88%) had terminal delirium 46 of 94 episodes, (49%) reversible Reversibility associated with psychoactive medication Patients with delirium had poorer survival than controls Lawlor et al. Arch Intern Med, 2000

26 Terminal Delirium Predictors Prospective study of 104 APCU patients 71 (68%) had delirium: 44 on admission, 27 during admission Lawlor et al. Arch Intern Med 2000
27 Delirium among advanced cancer patients assessed at the emergency center ( Elsayem A et al, Cancer 2016) 22/243 patients prospectively assessed had delirium (CAM +)with median MDAS 14/30 Delirium was mild in 18 ( 82%) of patients MD detected delirium in 13/22 cases (59%) No association with age, but association with PS ED great place to make early diagnosis of delirium!
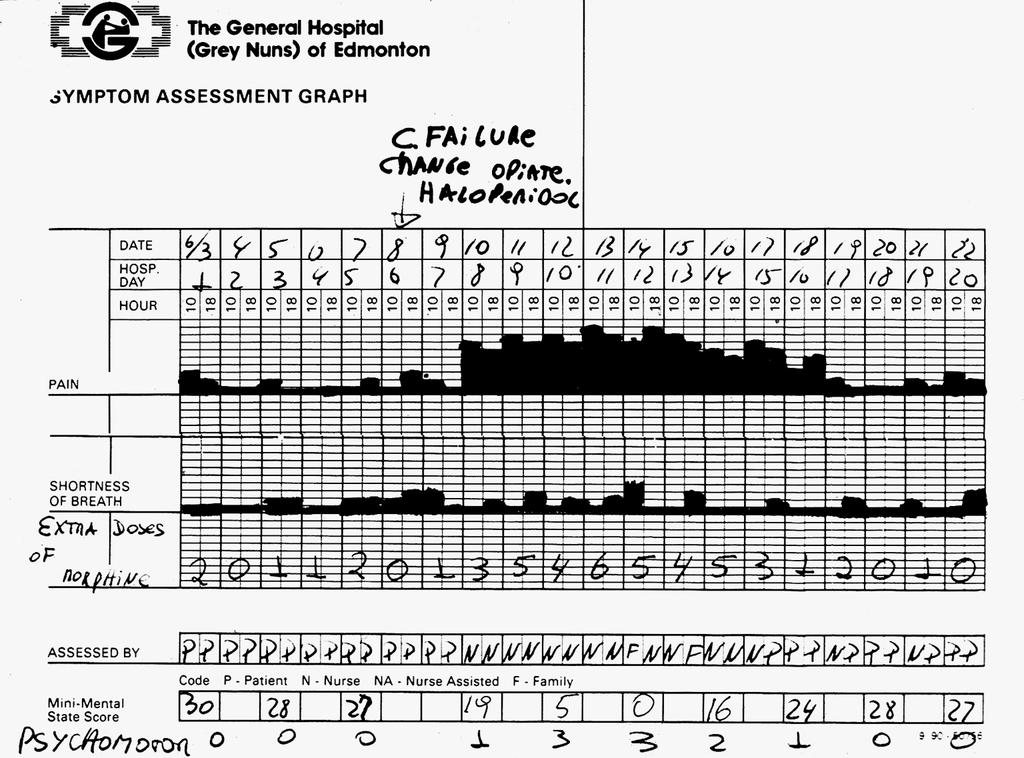
28
29
30 Delirium Recall ( Bruera E et al, Cancer 2009) 99 Patients with Complete resolution < 72hs before HYPO 20% ; HYPER 13%; MIXED 67% 250 Contributing Factors 73/99 Patients (74%) Remembered DELIRIUM!!!! 59/73 Recall expressed distress (81%); vs. 11/26 No Recall (42%); p = 0.01
31
32 Delirium: Bedside Babel
33 Settings Post-operative Delirium Different Settings, Different Patients Medical-surgical units Critical care Cancer Patients Old vs. young Non-cancer vs. cancer Reversible vs. terminal delirium
34 Delirium management Treat reversible causes Drugs Infection Metabolic causes Structural causes Palliation Non-pharmacologic measures Pharmacologic measures Neuroleptics haloperidol, chlorpromazine, olanzapine, risperidone, quetiapine Benzodiazepines?!? Dexmedetomidine
35 Opioid induced neurotoxicity (OIN) severe sedation cognitive failure hallucinosis/delirium myoclonus/grand mal seizures hyperalgesia/allodynia

36 O.I.N. Diagnosis Cognitive Failure Myoclonus Hyperalgesia Tactile hallucinations History Of: High opioid dose Prolonged time Borderline cognition Decreased glomerular filtration
37 Risk Factors for OIN High opioid dose Prolonged opioid exposure Pre-existing borderline cognition/delirium Dehydration Renal failure Other psychoactive drugs Opioids with mixed agonist/antagonist activity
38 Which drug to choose? 1. Delirium/ Opioid induced neurotoxicity: All opioids can cause it. Opioid rotation works by eliminating the offending drug.
39 Opioid Rotation Retrospective Study of 80 Rotations for OIN in PCU Symptoms of OIN improved in 58/80 (73% p<0.01) Pain control improved significantly 4.4 ± 2.3 to 3.6 ± 2.0 p<0.04) Dose was significantly lower than that thought to be equianalgesic 477 ± 1535 vs. 366 ± 593 (p<0.04) De Stoutz et al. J Pain Symptom Manage; 1995
40 16 years later Recognized syndrome Rotation fully established for management Translational research: multiple sub- mu, EAA/ NMDA, active opioid metabolites- all 3!! Methadone (better pain, decreased OIN, less cost, billions saved)- orphan drug (all patented ones funding professors to hit it )

41
42 Delirium management 1. Screening/ early (or late) diagnosis 2. Look for reversible causes 3. Pharmacological treatment 4. Environmental control 5. Bedside nurse/ referring MD education 6. Family education/ counseling
43 MDAS Memorial Delirium Assessment Scale ITEM 1 REDUCED LEVEL OF CONSICIOUSNESS (AWARENESS): 0: none 1: mild 2: moderate 3: severe ITEM 2 DISORIENTATION: 0: none 1: mild 2: moderate 3: severe ITEM 3 SHORT-TERM MEMORY IMPAIRMENT: 0: none 1: mild 2: moderate 3: severe ITEM 4 IMPAIRED DIGIT SPAN: 0: none 1: mild 2: moderate 3: severe ITEM 5 REDUCED ABILITY TO MAINTAIN AND SHIFT ATTENTION 0: none 1: mild 2: moderate 3: severe
44 MDAS Memorial Delirium Assessment Scale ITEM 6 DISORGANIZED THINKING 0: none 1: mild 2: moderate 3: severe ITEM 7 PERCEPTUAL DISTURBANCE: 0: none 1: mild 2: moderate 3: severe ITEM 8 DELUSIONS: 0: none 1: mild 2: moderate 3: severe ITEM 9 DECREASED OR INCREASED PSYCHOMOTOR ACTIVITY: 0: none 1: mild 2: moderate 3: severe ITEM 10 SLEEP-WAKE CYCLE DISTURBANCE (DISORDER OR AROUSAL): 0: none 1: mild 2: moderate 3: severe TOTAL
45 Other tools CAM DRS DSM TN criteria interview
46 The purpose of drug treatment of delirium 1. Drugs are unable to reverse delirium 2. Eliminate hyperactive features ( delusions, hallucinations, psychomotor agitation) 3. Sedation when other measures fail

47 Delirium Different Settings, Different Patients Candy et al. Cochrane Database 2012
48 Haloperidol Onset: min; dose mg, half life 18 hs, metabolized and into urine. Time to peak: oral 2-6hs; IM 20 min DPM blocker Extrapyramidal ( less in autonomic neuropathy?), tardive diskynesia, NMS Q-T prolongation, more IV
49 Pharmacological Management Haloperidol IV/ SC/ PO. Dose:???. loading (up to 5 mg/ dose q1h) and maintenance regular (2mg q 6h, etc) and breakthrough (q1-2h) Wide dose, less extrapyramidal in cancer (autonomic?)
50 Should every cancer patient with delirium be on regular haloperidol? Hyperactive and mixed YES In cancer 80 % are MIXED In PURE hypo no evidence, prn needed in case of change to mixed
51 Shin, HS et al. Frequency and outcome of neuroleptic rotation in patients with advanced cancer. Cancer Res treat /266 consecutive PCU admissions (63%) delirium treated with haloperidol 1 st line 128 (77%) only haloperidol (71% discharged alive) 39 (23%) required neuroleptic rotation (41% discharged alive) Median (IQR) H dose: 5 (3-7) mg/day
52 Then benzo story Most common drugs!!! Breitbart RCT worsened delirium Add to haloperidol en severe agitation (VS change to chlorpromazine, methotrimeprazine)- on a temporary basis Palliative sedation
53 Environment control 1. Excessive or NO light 2. Loud noises ( TV, sitter on cell phone) 3. Stimulation ( visitors, consultants, family) 4. Large clock/ calendar 5. Familiar objects, sounds smells 6. Do not ask for consent/ debate
54 Bedside RN/ referring MD Diagnosis ( frequently made by PC team) Need to search for reversible causes MAJOR med changes needed!! Disinhibition!! patient in a lot of pain, decision making NOT always opioid-induced, haloperidol best drug ( no, not akathisia, running from taxpayers with AIG bonus pay) Bedside RN support!! ( distress) mainly with education and good patient/ family care!!
55 Family Global brain dysfunction (blood products, poor quality fuel) Very common and poor prognosis Disinhibition of symptoms and emotions Environmental control Expressive/ supportive counseling!!! High distress
56 COUNSELING 1. Patient Brief conversations Avoid Confrontation Avoid stimulation (hyperactivity) Reassurance: familiar objects, people and sounds 2. Family Monitor behavior regularly Explain the mechanism of delirium Reassure regarding physical suffering Major cause of conflict!! 3. Staff Difference between pain and agitated delirium Aggressive behavior by patient Family distress and dissatisfaction Importance of consistent behavior! team approach!
57 Conclusions Delirium will develop in more than 80% of palliative care patients It is s source of distress and conflict It is severely underdiagnosed by HCPs The best management is to eliminate precipitating factors Haloperidol remains the main drug Communication/ education is a major intervention
Delirium. Assessment and Management
 Delirium Assessment and Management Goals and Objectives Participants will: 1. be able to recognize and diagnose the syndrome of delirium. 2. understand the causes of delirium. 3. become knowledgeable about
Delirium Assessment and Management Goals and Objectives Participants will: 1. be able to recognize and diagnose the syndrome of delirium. 2. understand the causes of delirium. 3. become knowledgeable about
Delirium. A Plan to Reduce Use of Restraints. David Wensel DO, FAAHPM Medical Director Midland Care
 Delirium A Plan to Reduce Use of Restraints David Wensel DO, FAAHPM Medical Director Midland Care Objectives Define delirium Describe pathophysiology of delirium Understand most common etiologies Define
Delirium A Plan to Reduce Use of Restraints David Wensel DO, FAAHPM Medical Director Midland Care Objectives Define delirium Describe pathophysiology of delirium Understand most common etiologies Define
Delirium in Cancer: Psychopharmacologic Management
 Delirium in Cancer: Psychopharmacologic Management William Breitbart, MD Professor and Chief, Psychiatry Service Memorial Sloan-Kettering Cancer Center New York, New York Delirium in Patients with Cancer
Delirium in Cancer: Psychopharmacologic Management William Breitbart, MD Professor and Chief, Psychiatry Service Memorial Sloan-Kettering Cancer Center New York, New York Delirium in Patients with Cancer
Delirium. Approach. Symptom Update Masterclass:
 Symptom Update Masterclass: Delirium Jason Boland Senior Clinical Lecturer and Honorary Consultant in Palliative Medicine Wolfson Centre for Palliative Care Research Hull York Medical School University
Symptom Update Masterclass: Delirium Jason Boland Senior Clinical Lecturer and Honorary Consultant in Palliative Medicine Wolfson Centre for Palliative Care Research Hull York Medical School University
Delirium. Dr. Lesley Wiesenfeld. Deputy Psychiatrist in Chief, Mount Sinai Hospital. Dr. Carole Cohen
 Delirium Dr. Lesley Wiesenfeld Deputy Psychiatrist in Chief, Mount Sinai Hospital Dr. Carole Cohen Department of Psychiatry, University of Toronto and Sunnybrook Health Sciences Centre Case Study Mrs B
Delirium Dr. Lesley Wiesenfeld Deputy Psychiatrist in Chief, Mount Sinai Hospital Dr. Carole Cohen Department of Psychiatry, University of Toronto and Sunnybrook Health Sciences Centre Case Study Mrs B
Learning Objectives. Delirium. Delirium. Delirium. Terminal Restlessness 3/28/2016
 Terminal Restlessness Dr. Christopher Churchill St. Cloud VA Health Care System EC&R Service Line Director & Medical Director Hospice & Palliative Care March 31, 2016 Learning Objectives Different Terminology
Terminal Restlessness Dr. Christopher Churchill St. Cloud VA Health Care System EC&R Service Line Director & Medical Director Hospice & Palliative Care March 31, 2016 Learning Objectives Different Terminology
OPIOID- INDUCED NEUROTOXICITY*
 OPIOID- INDUCED NEUROTOXICITY* Sriram Yennu MD, MS, FAAHPM Palliative Care, Rehabilitation and Integrative Medicine U.T. M.D. Anderson Cancer Center *Slide Deck courtesy Dept PRIM MDACC PATIENT #1: MRS
OPIOID- INDUCED NEUROTOXICITY* Sriram Yennu MD, MS, FAAHPM Palliative Care, Rehabilitation and Integrative Medicine U.T. M.D. Anderson Cancer Center *Slide Deck courtesy Dept PRIM MDACC PATIENT #1: MRS
g Prevention, Diagnosis, and Management in Palliative Care
 8/3/2012 Improving p g Prevention, Diagnosis, g and Management in Palliative Care MN Rural Palliative Care Networking Group Quarterly Education Session June 27,2012 Sandra W. Gordon-Kolb, MD, MMM, CPE
8/3/2012 Improving p g Prevention, Diagnosis, g and Management in Palliative Care MN Rural Palliative Care Networking Group Quarterly Education Session June 27,2012 Sandra W. Gordon-Kolb, MD, MMM, CPE
Delirium. A Geriatric Syndrome. Jonathan McCaleb, MD, CMD, HMDC UNSOM, Assistant Professor of Medicine Geriatrics / Hospice & Palliative Medicine
 Delirium A Geriatric Syndrome Jonathan McCaleb, MD, CMD, HMDC UNSOM, Assistant Professor of Medicine Geriatrics / Hospice & Palliative Medicine Introduction Common Serious Unrecognized: a medical emergency
Delirium A Geriatric Syndrome Jonathan McCaleb, MD, CMD, HMDC UNSOM, Assistant Professor of Medicine Geriatrics / Hospice & Palliative Medicine Introduction Common Serious Unrecognized: a medical emergency
Symptom Management Pocket Guides: DELIRIUM
 Symptom Management Pocket Guides: DELIRIUM August 2010 DELIRIUM Page Considerations. 1 Assessment 2 Diagnosis. 3 Non-Pharmacological treatment 3 Pharmacological treatment. 5 Mild Delirium... 6 Moderate
Symptom Management Pocket Guides: DELIRIUM August 2010 DELIRIUM Page Considerations. 1 Assessment 2 Diagnosis. 3 Non-Pharmacological treatment 3 Pharmacological treatment. 5 Mild Delirium... 6 Moderate
Delirium. Delirium. Delirium Etiology and Pathophysiology. Fall 2018
 Three most common cognitive problems in adults 1. (acute confusion) 2. Dementia 3. Depression These problems often occur together Can you think of common stimuli for each? 1 1 State of temporary but acute
Three most common cognitive problems in adults 1. (acute confusion) 2. Dementia 3. Depression These problems often occur together Can you think of common stimuli for each? 1 1 State of temporary but acute
Management of Delirium in Hospice Patients
 Presentation Objectives Management of Delirium in Hospice Patients Lynn Williams, BSPharm Clinical Pharmacist Hospice Pharmacy Solutions Identify the clinical features of delirium Understand the underlying
Presentation Objectives Management of Delirium in Hospice Patients Lynn Williams, BSPharm Clinical Pharmacist Hospice Pharmacy Solutions Identify the clinical features of delirium Understand the underlying
Confusion in the acute setting Dr Susan Shenkin
 Confusion in the acute setting Dr Susan Shenkin Susan.Shenkin@ed.ac.uk 4 th International Conference, Society for Acute Medicine, Edinburgh 7-8 October 2010 Summary Confusion is not a diagnosis Main differentials
Confusion in the acute setting Dr Susan Shenkin Susan.Shenkin@ed.ac.uk 4 th International Conference, Society for Acute Medicine, Edinburgh 7-8 October 2010 Summary Confusion is not a diagnosis Main differentials
Palliative Care and Delirium. Ambereen K. Mehta, MD MPH Assistant Professor Division of General Medicine, Geriatrics, and Palliative Care
 Palliative Care and Delirium Ambereen K. Mehta, MD MPH Assistant Professor Division of General Medicine, Geriatrics, and Palliative Care Disclosures I have no personal or professional financial relationships
Palliative Care and Delirium Ambereen K. Mehta, MD MPH Assistant Professor Division of General Medicine, Geriatrics, and Palliative Care Disclosures I have no personal or professional financial relationships
Delirium in Hospital Care
 Delirium in Hospital Care Dr John Puxty 1 Learning Objectives By the end of the workshop participants will be able to: Appreciate the main diagnostic criteria for delirium. Describe common risk factors,
Delirium in Hospital Care Dr John Puxty 1 Learning Objectives By the end of the workshop participants will be able to: Appreciate the main diagnostic criteria for delirium. Describe common risk factors,
Delirium in the Elderly
 Delirium in the Elderly ELITE 2017 Liza Genao, MD Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity Very much under-recognized
Delirium in the Elderly ELITE 2017 Liza Genao, MD Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity Very much under-recognized
5 older patients become delirious every minute
 Management of Delirium: Nonpharmacologic and Pharmacologic Approaches Sharon K. Inouye, M.D., M.P.H. Professor of Medicine Beth Israel Deaconess Medical Center Harvard Medical School Milton and Shirley
Management of Delirium: Nonpharmacologic and Pharmacologic Approaches Sharon K. Inouye, M.D., M.P.H. Professor of Medicine Beth Israel Deaconess Medical Center Harvard Medical School Milton and Shirley
Delirium in the ICU: Prevention and Treatment. Delirium Defined Officially. Delirium: Really Defined. S. Andrew Josephson, MD
 Delirium in the ICU: Prevention and Treatment S. Andrew Josephson, MD Director, Neurohospitalist Service Medical Director, Inpatient Neurology June 2, 2011 Delirium Defined Officially (DSM-IV-TR) criteria
Delirium in the ICU: Prevention and Treatment S. Andrew Josephson, MD Director, Neurohospitalist Service Medical Director, Inpatient Neurology June 2, 2011 Delirium Defined Officially (DSM-IV-TR) criteria
Delirium in the Elderly
 Delirium in the Elderly ELITE 2015 Mamata Yanamadala M.B.B.S, MS Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity
Delirium in the Elderly ELITE 2015 Mamata Yanamadala M.B.B.S, MS Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity
Delirium. Dr. John Puxty
 Delirium Dr. John Puxty Learning Objectives By the end of the workshop participants will be able to: Appreciate the main diagnostic criteria for delirium. Describe common risk factors, causes and main
Delirium Dr. John Puxty Learning Objectives By the end of the workshop participants will be able to: Appreciate the main diagnostic criteria for delirium. Describe common risk factors, causes and main
DELIRIUM IN ICU: Prevention and Management. Milind Baldi
 DELIRIUM IN ICU: Prevention and Management Milind Baldi Contents Introduction Risk factors Assessment Prevention Management Introduction Delirium is a syndrome characterized by acute cerebral dysfunction
DELIRIUM IN ICU: Prevention and Management Milind Baldi Contents Introduction Risk factors Assessment Prevention Management Introduction Delirium is a syndrome characterized by acute cerebral dysfunction
Tim Hiebert - MD MSc FRCPC General Internist/Palliative Care Winnipeg Regional Health Authority
 Tim Hiebert - MD MSc FRCPC General Internist/Palliative Care Winnipeg Regional Health Authority Conflicts of Interest: None 1. Identify key features that suggest the End-of-Life 2. Review of Common End-of-life
Tim Hiebert - MD MSc FRCPC General Internist/Palliative Care Winnipeg Regional Health Authority Conflicts of Interest: None 1. Identify key features that suggest the End-of-Life 2. Review of Common End-of-life
Acute cognitive failure and delirium: screening
 Acute cognitive failure and delirium: screening instruments for research and clinical practice Augusto Caraceni Director Palliative Care, Pain therapy and rehabilitation Fondazione IRCCS National Cancer
Acute cognitive failure and delirium: screening instruments for research and clinical practice Augusto Caraceni Director Palliative Care, Pain therapy and rehabilitation Fondazione IRCCS National Cancer
DELIRIUM DR S A R A H A B D E L A T I S A S DR H I L A R Y W O L F E N D A L E S T 4
 DELIRIUM DR S A R A H A B D E L A T I S A S DR H I L A R Y W O L F E N D A L E S T 4 AIMS Define delirium Identify: Different types of delirium Risk factors Preventable causes Screening tools Management
DELIRIUM DR S A R A H A B D E L A T I S A S DR H I L A R Y W O L F E N D A L E S T 4 AIMS Define delirium Identify: Different types of delirium Risk factors Preventable causes Screening tools Management
Delirium in Palliative care. Presentation to Volunteers 2016 David Falk
 Delirium in Palliative care Presentation to Volunteers 2016 David Falk Delirium What is delirium? Case Study - Delirium 60+ year old PQ presents to hospice very somnolent. She was admitted with her adult
Delirium in Palliative care Presentation to Volunteers 2016 David Falk Delirium What is delirium? Case Study - Delirium 60+ year old PQ presents to hospice very somnolent. She was admitted with her adult
The last days of life in hospital and at home
 The last days of life in hospital and at home Beaumont Multi-disciplinary Palliative Care Study Day 28/9/2017 Dr Sarah McLean Consultant in Palliative Medicine St Francis Hospice Beaumont Hospital Overview
The last days of life in hospital and at home Beaumont Multi-disciplinary Palliative Care Study Day 28/9/2017 Dr Sarah McLean Consultant in Palliative Medicine St Francis Hospice Beaumont Hospital Overview
Interprofessional Webinar Series
 Interprofessional Webinar Series Assessment and Management of Delirium Pauline Lesage, MD, LLM Physician Educator MJHS Institute for Innovation in Palliative Care Disclosure Slide Pauline Lesage, MD, LLM,
Interprofessional Webinar Series Assessment and Management of Delirium Pauline Lesage, MD, LLM Physician Educator MJHS Institute for Innovation in Palliative Care Disclosure Slide Pauline Lesage, MD, LLM,
Delirium in Critical Care. Recognition, Management, Research tasters. Dr Valerie Page Watford General Hospital
 Delirium in Critical Care. Recognition, Management, Research tasters Dr Valerie Page Watford General Hospital What does it look like? Diagnosing delirium CAM-ICU CAM-ICU Feature 1: Acute onset of mental
Delirium in Critical Care. Recognition, Management, Research tasters Dr Valerie Page Watford General Hospital What does it look like? Diagnosing delirium CAM-ICU CAM-ICU Feature 1: Acute onset of mental
Objectives. Symptom Management in the Frail Elderly Population. Disclosures. Symptom Management: Pain 12/05/2014
 Objectives Symptom Management in the Frail Elderly Population Dr. Katie Marchington, MD, CCFP Palliative Care Physician Toronto Western Hospital Kensington Hospice To reflect on why we should identify
Objectives Symptom Management in the Frail Elderly Population Dr. Katie Marchington, MD, CCFP Palliative Care Physician Toronto Western Hospital Kensington Hospice To reflect on why we should identify
譫妄症 (Delirium) Objectives. Epidemiology. Delirium. DSM-5 Diagnostic Criteria. Prognosis 台大醫院老年醫學部陳人豪 2016/8/28
 Objectives. Epidemiology. Delirium. DSM-5 Diagnostic Criteria. Prognosis 台大醫院老年醫學部陳人豪 2016/8/28") 譫妄症 (Delirium) 台大醫院老年醫學部陳人豪 2016/8/28 Objectives Delirium Epidemiology Etiology Diagnosis Evaluation and Management Postoperative delirium Delirium (and acute problematic behavior) in the longterm care
譫妄症 (Delirium) 台大醫院老年醫學部陳人豪 2016/8/28 Objectives Delirium Epidemiology Etiology Diagnosis Evaluation and Management Postoperative delirium Delirium (and acute problematic behavior) in the longterm care
NIH Public Access Author Manuscript Cancer. Author manuscript; available in PMC 2009 September 28.
 NIH Public Access Author Manuscript Published in final edited form as: Cancer. 2009 May 1; 115(9): 2004 2012. doi:10.1002/cncr.24215. The impact of delirium and recall on the level of distress in patients
NIH Public Access Author Manuscript Published in final edited form as: Cancer. 2009 May 1; 115(9): 2004 2012. doi:10.1002/cncr.24215. The impact of delirium and recall on the level of distress in patients
Charles Bernick, MD, MPH Cleveland Clinic Lou Ruvo Center for Brain Health June 2, 2018
 Charles Bernick, MD, MPH Cleveland Clinic Lou Ruvo Center for Brain Health June 2, 2018 Delirium common Prolongs hospitalization Worsens dementia ( if you survive) Increased risk of institutionalization
Charles Bernick, MD, MPH Cleveland Clinic Lou Ruvo Center for Brain Health June 2, 2018 Delirium common Prolongs hospitalization Worsens dementia ( if you survive) Increased risk of institutionalization
Canadian Practices for the Treatment of Delirium. Lisa Burry, BScPharm, PharmD
 Canadian Practices for the Treatment of Delirium Lisa Burry, BScPharm, PharmD Disclosures & Acknowledgements Conflicts of interest: None Acknowledgements: our patients and the clinical staff that supported
Canadian Practices for the Treatment of Delirium Lisa Burry, BScPharm, PharmD Disclosures & Acknowledgements Conflicts of interest: None Acknowledgements: our patients and the clinical staff that supported
Update - Delirium in Elders
 Update - Delirium in Elders Impact Recognition Prevention, and Management Michael J. Lichtenstein, MD F. Carter Pannill, Jr. Professor of Medicine Chief, Division of Geriatrics, Gerontology and Palliative
Update - Delirium in Elders Impact Recognition Prevention, and Management Michael J. Lichtenstein, MD F. Carter Pannill, Jr. Professor of Medicine Chief, Division of Geriatrics, Gerontology and Palliative
Delirium in the hospitalized patient
 Delirium in the hospitalized patient Jennifer A. Tarin, M.D. Department of Hospital Medicine Geriatric Health Safety Chair Colorado Permanente Medical Group UCLA Reynolds Scholar Delirium Preventing delirium
Delirium in the hospitalized patient Jennifer A. Tarin, M.D. Department of Hospital Medicine Geriatric Health Safety Chair Colorado Permanente Medical Group UCLA Reynolds Scholar Delirium Preventing delirium
Delirium. Geriatric Giants Lecture Series Divisions of Geriatric Medicine and Care of the Elderly University of Alberta
 Delirium Geriatric Giants Lecture Series Divisions of Geriatric Medicine and Care of the Elderly University of Alberta Overview A. Delirium - the nature of the beast B. Significance of delirium C. An approach
Delirium Geriatric Giants Lecture Series Divisions of Geriatric Medicine and Care of the Elderly University of Alberta Overview A. Delirium - the nature of the beast B. Significance of delirium C. An approach
Delirium in Palliative Care. Case Studies 2015
 Delirium in Palliative Care Case Studies 2015 Case 1 - Alex 35 yo M with metastatic melanoma Decreased LOC, unilateral hearing loss and bilateral vision loss, back pain, lower extremity weakness,? confusion/hallucinations
Delirium in Palliative Care Case Studies 2015 Case 1 - Alex 35 yo M with metastatic melanoma Decreased LOC, unilateral hearing loss and bilateral vision loss, back pain, lower extremity weakness,? confusion/hallucinations
Delirium. Quick reference guide. Issue date: July Diagnosis, prevention and management
 Issue date: July 2010 Delirium Diagnosis, prevention and management Developed by the National Clinical Guideline Centre for Acute and Chronic Conditions About this booklet This is a quick reference guide
Issue date: July 2010 Delirium Diagnosis, prevention and management Developed by the National Clinical Guideline Centre for Acute and Chronic Conditions About this booklet This is a quick reference guide
Delirium. Delirium is characterized by an acute onset (hours or days) and fluctuating course of deterioration in mental functioning.
 and fluctuating course of deterioration in mental functioning.") Delirium Delirium is characterized by an acute onset (hours or days) and fluctuating course of deterioration in mental functioning. DELIRIUM IS A MEDICAL EMERGENCY! Delirium: Hallmark Features Inattention-
Delirium Delirium is characterized by an acute onset (hours or days) and fluctuating course of deterioration in mental functioning. DELIRIUM IS A MEDICAL EMERGENCY! Delirium: Hallmark Features Inattention-
Cognitive Effects of Opioid Therapy. Cognitive Function. Prevalence. Delirium (DSM IV) Significance of Cognitive Effects
 Significance of Cognitive Effects") Cognitive Effects of Opioid Therapy Jeannine M. Brant RN, MS, AOCN St.Vincent Healthcare Billings, MT Cognitive Function! Brain s acquisition! Information system Processing Storage Retrieval! Includes:
Cognitive Effects of Opioid Therapy Jeannine M. Brant RN, MS, AOCN St.Vincent Healthcare Billings, MT Cognitive Function! Brain s acquisition! Information system Processing Storage Retrieval! Includes:
For more information about how to cite these materials visit
 Author(s): Rachel Glick, M.D., 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Noncommercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
Author(s): Rachel Glick, M.D., 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Noncommercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
Agitation Predictors in Acute Traumatic Brain Injury
 Agitation Predictors in Acute Traumatic Brain Injury Dr Jehane H Dagher, MD, BScPT, FRCPC, FABPMR Physiatre Chef de Programme Trauma Cranio-Cerebral Professeure agrégée - Physiatrie Universite de Montreal
Agitation Predictors in Acute Traumatic Brain Injury Dr Jehane H Dagher, MD, BScPT, FRCPC, FABPMR Physiatre Chef de Programme Trauma Cranio-Cerebral Professeure agrégée - Physiatrie Universite de Montreal
Decreasing Delirium Resolution Times for the Elderly: An Interprofessional Approach
 Decreasing Delirium Resolution Times for the Elderly: An Interprofessional Approach Featuring: Felice Rogers Evans BSN RN BC Ty Breiter MSN RN CNL Tampa General Hospital NICHE exemplar hospital Three time
Decreasing Delirium Resolution Times for the Elderly: An Interprofessional Approach Featuring: Felice Rogers Evans BSN RN BC Ty Breiter MSN RN CNL Tampa General Hospital NICHE exemplar hospital Three time
Test your Knowledge: Recognizing Delirium
 The Ottawa Hospital Name: Unit: Profession: RN RPN PT OT SW Other Note: Each question has only one correct answer. 1. If a patient is identified as being at high risk for developing delirium, his/her mental
The Ottawa Hospital Name: Unit: Profession: RN RPN PT OT SW Other Note: Each question has only one correct answer. 1. If a patient is identified as being at high risk for developing delirium, his/her mental
Sarah V. Cogle, PharmD, BCCCP Assistant Clinical Professor Auburn University Harrison School of Pharmacy Auburn, AL ALSHP Annual Clinical Meeting
 Sarah V. Cogle, PharmD, BCCCP Assistant Clinical Professor Auburn University Harrison School of Pharmacy Auburn, AL ALSHP Annual Clinical Meeting 2018 I have no actual or potential conflict of interest
Sarah V. Cogle, PharmD, BCCCP Assistant Clinical Professor Auburn University Harrison School of Pharmacy Auburn, AL ALSHP Annual Clinical Meeting 2018 I have no actual or potential conflict of interest
Delirium assessment and management. Dr Kim Jeffs Northern Health
 Delirium assessment and management Dr Kim Jeffs Northern Health What do you need to know? Epidemiology How big is the problem? Who is at risk? Assessment Tools for diagnosis Prevention Evidence base Management
Delirium assessment and management Dr Kim Jeffs Northern Health What do you need to know? Epidemiology How big is the problem? Who is at risk? Assessment Tools for diagnosis Prevention Evidence base Management
Jacinta Lucke Resident Emergency Medicine PHD Gerontology & Geriatrics
 Jacinta Lucke Resident Emergency Medicine PHD Gerontology & Geriatrics TAKE HOME MESSAGE When managing confusion in older patients: Routinely screen for impaired cognition Patients with impaired cognition
Jacinta Lucke Resident Emergency Medicine PHD Gerontology & Geriatrics TAKE HOME MESSAGE When managing confusion in older patients: Routinely screen for impaired cognition Patients with impaired cognition
DELIRIUM. Approach and Management
 DELIRIUM Approach and Management By Dr. K.S. Jacob, Professor of Psychiatry and Dr. Anju Kuruvilla, Professor of Psychiatry, Christian Medical College, Vellore. Based on a chapter in the book Psychiatric
DELIRIUM Approach and Management By Dr. K.S. Jacob, Professor of Psychiatry and Dr. Anju Kuruvilla, Professor of Psychiatry, Christian Medical College, Vellore. Based on a chapter in the book Psychiatric
4/3/2018. Management of Acute Pain Crises. Five Mistakes I ve made and why you shouldn t
 Management of Acute Pain Crises Maggie O Connor, M.D. Retired Palliative Care Physician Hope is not the conviction that something will turn out well, but the certainty that something makes sense, regardless
Management of Acute Pain Crises Maggie O Connor, M.D. Retired Palliative Care Physician Hope is not the conviction that something will turn out well, but the certainty that something makes sense, regardless
Objectives. Delirium in the Elderly Patient. Disclosure. Arizona Geriatrics Society Fall Symposium 2010
 Delirium in the Elderly Patient Sandra Jacobson, MD Banner Sun Health Research Institute Arizona Geriatrics Society Fall Symposium 2010 Disclosure Dr. Jacobson has disclosed that she does not have any
Delirium in the Elderly Patient Sandra Jacobson, MD Banner Sun Health Research Institute Arizona Geriatrics Society Fall Symposium 2010 Disclosure Dr. Jacobson has disclosed that she does not have any
DIAH MUSTIKA HW SpS,KIC Intensive Care Unit of Emergency Department Naval Hospital dr RAMELAN, Surabaya
 DIAH MUSTIKA HW SpS,KIC Intensive Care Unit of Emergency Department Naval Hospital dr RAMELAN, Surabaya Encephalopathy is a common complication of systemic illness or direct brain injury. Acute confusional
DIAH MUSTIKA HW SpS,KIC Intensive Care Unit of Emergency Department Naval Hospital dr RAMELAN, Surabaya Encephalopathy is a common complication of systemic illness or direct brain injury. Acute confusional
Evidence-Based Treatment of Delirium in Patients With Cancer William Breitbart and Yesne Alici
 Published Ahead of Print on March 12, 2012 as 10.1200/JCO.2011.39.8784 The latest version is at http://jco.ascopubs.org/cgi/doi/10.1200/jco.2011.39.8784 JOURNAL OF CLINICAL ONCOLOGY R E V I E W A R T I
Published Ahead of Print on March 12, 2012 as 10.1200/JCO.2011.39.8784 The latest version is at http://jco.ascopubs.org/cgi/doi/10.1200/jco.2011.39.8784 JOURNAL OF CLINICAL ONCOLOGY R E V I E W A R T I
The Agitated. Older Patient: old. What To Do? Michelle Gibson, MD, CCFP Presented at Brockville General Hospital Rounds, May 2003
 Focus on CME at Queen s University Focus on CME at Queen s University The Agitated The Older Patient: What To Do? Michelle Gibson, MD, CCFP Presented at Brockville General Hospital Rounds, May 2003 Both
Focus on CME at Queen s University Focus on CME at Queen s University The Agitated The Older Patient: What To Do? Michelle Gibson, MD, CCFP Presented at Brockville General Hospital Rounds, May 2003 Both
HHS Public Access Author manuscript Curr Opin Support Palliat Care. Author manuscript; available in PMC 2017 December 01.
 Neuroleptics in the Management of Delirium in Patients with Advanced Cancer David Hui, MD, MSc, Rony Dev, MD and Eduardo Bruera, MD Department of Palliative Care and Rehabilitation Medicine, MD Anderson
Neuroleptics in the Management of Delirium in Patients with Advanced Cancer David Hui, MD, MSc, Rony Dev, MD and Eduardo Bruera, MD Department of Palliative Care and Rehabilitation Medicine, MD Anderson
Managing Delirium: The best way to achieve clarity (of mind) Tim Walsh. Professor of Critical Care, Edinburgh University
 Tim Walsh. Professor of Critical Care, Edinburgh University") Managing Delirium: The best way to achieve clarity (of mind) Tim Walsh Professor of Critical Care, Edinburgh University Lecture Plan: a route to clarity What is delirium? Why is delirium important? Step
Managing Delirium: The best way to achieve clarity (of mind) Tim Walsh Professor of Critical Care, Edinburgh University Lecture Plan: a route to clarity What is delirium? Why is delirium important? Step
Critical Care Pharmacological Management of Delirium
 Critical Care Pharmacological Management of Delirium Policy Title: in the Critical Care Unit Executive Summary: This policy provides guidance Pharmacological Management of delirium in the Critical Care
Critical Care Pharmacological Management of Delirium Policy Title: in the Critical Care Unit Executive Summary: This policy provides guidance Pharmacological Management of delirium in the Critical Care
Delirium, Depression and Dementia
 Delirium, Depression and Dementia Martha Watson, MS, APRN, GCNS Some material included in this presentation is adapted from: NICHE (2009). Geriatric Resource Nurse Core Curriculum [Power Point presentation].
Delirium, Depression and Dementia Martha Watson, MS, APRN, GCNS Some material included in this presentation is adapted from: NICHE (2009). Geriatric Resource Nurse Core Curriculum [Power Point presentation].
Delirium and Dementia. Summary
 Delirium and Dementia Paul Kettl, M.D., M.H.A. Summary DELIRIUM Acute brain failure Identify cause (meds, infection) Treat sx Poor prognostic sign DEMENTIA Chronic brain failure AD most common cause Often
Delirium and Dementia Paul Kettl, M.D., M.H.A. Summary DELIRIUM Acute brain failure Identify cause (meds, infection) Treat sx Poor prognostic sign DEMENTIA Chronic brain failure AD most common cause Often
Acute vs. Maintenance
 Acute vs. Maintenance The objective of rapid and effective management of acute agitation, confusion and decompensation is to minimize the morbidities of the post acute or chronic course, and thus reduce
Acute vs. Maintenance The objective of rapid and effective management of acute agitation, confusion and decompensation is to minimize the morbidities of the post acute or chronic course, and thus reduce
Geriatrics and Cancer Care
 Geriatrics and Cancer Care Roger Wong, BMSc, MD, FRCPC, FACP Postgraduate Dean of Medical Education Clinical Professor, Division of Geriatric Medicine UBC Faculty of Medicine Disclosure No competing interests
Geriatrics and Cancer Care Roger Wong, BMSc, MD, FRCPC, FACP Postgraduate Dean of Medical Education Clinical Professor, Division of Geriatric Medicine UBC Faculty of Medicine Disclosure No competing interests
BEHAVIORAL PROBLEMS IN DEMENTIA
 BEHAVIORAL PROBLEMS IN DEMENTIA CLINICAL FEATURES Particularly as dementia progresses, psychiatric symptoms may develop that resemble discrete mental disorders such as depression or mania The course and
BEHAVIORAL PROBLEMS IN DEMENTIA CLINICAL FEATURES Particularly as dementia progresses, psychiatric symptoms may develop that resemble discrete mental disorders such as depression or mania The course and
Delirium Prevention: The State-of-the-Art & Implications to Improve Care in our State
 Delirium Prevention: The State-of-the-Art & Implications to Improve Care in our State Jonny Macias, MD & Michael Malone, MD Aurora Health Care/ University of Wisconsin School of Medicine & Public Health
Delirium Prevention: The State-of-the-Art & Implications to Improve Care in our State Jonny Macias, MD & Michael Malone, MD Aurora Health Care/ University of Wisconsin School of Medicine & Public Health
Cognitive Status. Read each question below to the patient. Score one point for each correct response.
 Diagnosis of dementia or delirium Cognitive Status Six Item Screener Read to the patient: I have a few questions I would like to ask you. First, I am going to name three objects. After I have said all
Diagnosis of dementia or delirium Cognitive Status Six Item Screener Read to the patient: I have a few questions I would like to ask you. First, I am going to name three objects. After I have said all
Cognitive disorders. Dr S. Mashaphu Department of Psychiatry
 Cognitive disorders Dr S. Mashaphu Department of Psychiatry Delirium Syndrome characterised by: Disturbance of consciousness Impaired attention Change in cognition Develops over hours-days Fluctuates during
Cognitive disorders Dr S. Mashaphu Department of Psychiatry Delirium Syndrome characterised by: Disturbance of consciousness Impaired attention Change in cognition Develops over hours-days Fluctuates during
Delirium Screening Tools: Just- In- Time Education and Evaluation Using the EMR
 Delirium Screening Tools: Just- In- Time Education and Evaluation Using the EMR Implementation of an EMR based protocol for detection of delirium in elderly Medical and palliative care patients Parul Goyal,
Delirium Screening Tools: Just- In- Time Education and Evaluation Using the EMR Implementation of an EMR based protocol for detection of delirium in elderly Medical and palliative care patients Parul Goyal,
nicheprogram.org 16th Annual NICHE Conference Forging New Paths and Partnerships 1
 Improving Patient Outcomes in Geriatric Post-Operative Orthopedic Patients: Translating Research into Practice Tripping into The CAM Presented by: Diana LaBumbard, RN, MSN, ACNP/GNP-BC, CWOCN Denise Williams,
Improving Patient Outcomes in Geriatric Post-Operative Orthopedic Patients: Translating Research into Practice Tripping into The CAM Presented by: Diana LaBumbard, RN, MSN, ACNP/GNP-BC, CWOCN Denise Williams,
AACN PCCN Review. Behavioral
 AACN PCCN Review Behavioral Presenter: Carol A. Rauen, RN, MS, CCNS, CCRN, PCCN, CEN Independent Clinical Nurse Specialist & Education Consultant rauen.carol104@gmail.com 0 Behavioral I. INTRODUCTION PCCN
AACN PCCN Review Behavioral Presenter: Carol A. Rauen, RN, MS, CCNS, CCRN, PCCN, CEN Independent Clinical Nurse Specialist & Education Consultant rauen.carol104@gmail.com 0 Behavioral I. INTRODUCTION PCCN
Care of Patient with Delirium
 Care of Patient with Delirium Introduction Delirium is an alteration in consciousness involving confusion and other changes in cognitive ability that has a brief duration. 1 Patients specifically at risk
Care of Patient with Delirium Introduction Delirium is an alteration in consciousness involving confusion and other changes in cognitive ability that has a brief duration. 1 Patients specifically at risk
Delirium: A Condition of All Ages. Delirium, also known as acute confusional state, Definition. Epidemiology
 Focus on CME at the University of Calgary : A Condition of All Ages While delirium can strike at any age, physicians need to be particularly watchful for it in elderly patients, so that a search for the
Focus on CME at the University of Calgary : A Condition of All Ages While delirium can strike at any age, physicians need to be particularly watchful for it in elderly patients, so that a search for the
Waterloo Wellington (WW) Symptom Management Guideline for the End of Life (EOL) Medication Order Set for Long Term Care (LTC)
 Symptom Management Guideline for the End of Life (EOL) Medication Order Set for Long Term Care (LTC)") Waterloo Wellington (WW) Symptom Management Guideline for the End of Life (EOL) Medication Order Set for Long Term Care (LTC) May 2018 THE WATERLOO WELLINGTON SYMPTOM MANAGEMENT GUIDELINE FOR THE END OF
Waterloo Wellington (WW) Symptom Management Guideline for the End of Life (EOL) Medication Order Set for Long Term Care (LTC) May 2018 THE WATERLOO WELLINGTON SYMPTOM MANAGEMENT GUIDELINE FOR THE END OF
Drug induced delirium
 Drug induced delirium Knut Erik Hovda, MD, PhD, FACMT, FEAPCCT The Norwegian CBRNe Centre of Medicine Department of Acute Medicine Oslo University hospital Content 1. Introduction 2. Risk factors 3. Prevalence
Drug induced delirium Knut Erik Hovda, MD, PhD, FACMT, FEAPCCT The Norwegian CBRNe Centre of Medicine Department of Acute Medicine Oslo University hospital Content 1. Introduction 2. Risk factors 3. Prevalence
Delirium and cognitive impairment in the perioperative
 Delirium and cognitive impairment in the perioperative period Richard Sztramko Assistant Professor, McMaster University Divisions of Geriatrics and General Internal Medicine Disclosures Chief Medical Officer
Delirium and cognitive impairment in the perioperative period Richard Sztramko Assistant Professor, McMaster University Divisions of Geriatrics and General Internal Medicine Disclosures Chief Medical Officer
Pain management. Coleman Palliative Care Conference: February 2016 Josh Baru MD Stacie Levine MD
 Pain management Coleman Palliative Care Conference: February 2016 Josh Baru MD Stacie Levine MD Case #1 61 yo man with history of Stage 3 colon cancer, s/p resection and adjuvant chemotherapy with FOLFOX
Pain management Coleman Palliative Care Conference: February 2016 Josh Baru MD Stacie Levine MD Case #1 61 yo man with history of Stage 3 colon cancer, s/p resection and adjuvant chemotherapy with FOLFOX
DELIRIUM. Sabitha Rajan, MD, MSc, FHM Scott &White Healthcare Texas A&M Health Science Center School of Medicine
 DELIRIUM Sabitha Rajan, MD, MSc, FHM Scott &White Healthcare Texas A&M Health Science Center School of Medicine Disclosure Milliman Care Guidelines - Editor Objectives Define delirium Epidemiology Diagnose
DELIRIUM Sabitha Rajan, MD, MSc, FHM Scott &White Healthcare Texas A&M Health Science Center School of Medicine Disclosure Milliman Care Guidelines - Editor Objectives Define delirium Epidemiology Diagnose
Delirium Information for patients and relatives. Delirium is common Delirium is treatable Relatives can stay to help us
 Delirium Information for patients and relatives Delirium is common Delirium is treatable Relatives can stay to help us What is delirium? Delirium is caused by a disturbance of brain function. It is used
Delirium Information for patients and relatives Delirium is common Delirium is treatable Relatives can stay to help us What is delirium? Delirium is caused by a disturbance of brain function. It is used
Strategies to minimize delirium for hip fracture patients
 Strategies to minimize delirium for hip fracture patients Stephen L Kates, M.D. Professor and Chairman Department Date of Orthopaedic Surgery Delirium incidence Up to 61% of hip fracture patients get delirium
Strategies to minimize delirium for hip fracture patients Stephen L Kates, M.D. Professor and Chairman Department Date of Orthopaedic Surgery Delirium incidence Up to 61% of hip fracture patients get delirium
Delirium in Older Persons
 Objectives Delirium in Older Persons ELITE 2018 Liza Isabel Genao, MD Division of Geriatrics Describe rate, cost, complications of delirium Effectively diagnose the syndrome Describe multicomponent model
Objectives Delirium in Older Persons ELITE 2018 Liza Isabel Genao, MD Division of Geriatrics Describe rate, cost, complications of delirium Effectively diagnose the syndrome Describe multicomponent model
Care of the dying in End Stage Kidney Disease (ESKD) - Conservative. Elizabeth Josland Renal Supportive Care CNC St George Hospital
 - Conservative. Elizabeth Josland Renal Supportive Care CNC St George Hospital") Care of the dying in End Stage Kidney Disease (ESKD) - Conservative Elizabeth Josland Renal Supportive Care CNC St George Hospital Introduction What does conservative management look like? How does the
Care of the dying in End Stage Kidney Disease (ESKD) - Conservative Elizabeth Josland Renal Supportive Care CNC St George Hospital Introduction What does conservative management look like? How does the
Acute vs. Maintenance
 Acute vs. Maintenance The objective of rapid and effective management of acute agitation, confusion and decompensation is to minimize the morbidities of the post acute or chronic course, and thus reduce
Acute vs. Maintenance The objective of rapid and effective management of acute agitation, confusion and decompensation is to minimize the morbidities of the post acute or chronic course, and thus reduce
Acute vs. Maintenance
 Acute vs. Maintenance The objective of rapid and effective management of acute agitation, confusion and decompensation is to minimize the morbidities of the post acute or chronic course, and thus reduce
Acute vs. Maintenance The objective of rapid and effective management of acute agitation, confusion and decompensation is to minimize the morbidities of the post acute or chronic course, and thus reduce
PRESCRIBING PRACTICE IN DELIRIUM. John Warburton Critical Care Pharmacist
 PRESCRIBING PRACTICE IN DELIRIUM John Warburton Critical Care Pharmacist Learning outcomes Modifiable medication risk factors for delirium An appreciation of contributing factors modifiable with medicines
PRESCRIBING PRACTICE IN DELIRIUM John Warburton Critical Care Pharmacist Learning outcomes Modifiable medication risk factors for delirium An appreciation of contributing factors modifiable with medicines
Behavior Management in Children with Cancer
 Behavior Management in Children with Cancer Anna (Nina) Muriel, MD, MPH Chief, Division of Pediatric Psychosocial Oncology Department of Psychosocial Oncology and Palliative Care Behavior matters Behavior
Behavior Management in Children with Cancer Anna (Nina) Muriel, MD, MPH Chief, Division of Pediatric Psychosocial Oncology Department of Psychosocial Oncology and Palliative Care Behavior matters Behavior
Summary of Delirium Clinical Practice Guideline Recommendations Post Operative
 Summary of Delirium Clinical Practice Guideline Recommendations Post Operative Intensive Care Unit Clinical Practice Guideline for Postoperative Clinical Practice Guidelines for the Delirium in Older Adults;
Summary of Delirium Clinical Practice Guideline Recommendations Post Operative Intensive Care Unit Clinical Practice Guideline for Postoperative Clinical Practice Guidelines for the Delirium in Older Adults;
Management of Severe Agitation
 Management of Severe Agitation Key Points 1. The management of the severely agitated or violent patient embraces psychological, physical and pharmacological approaches. 2. Psychological methods focus on
Management of Severe Agitation Key Points 1. The management of the severely agitated or violent patient embraces psychological, physical and pharmacological approaches. 2. Psychological methods focus on
Critical Care Pharmacological Management of Delirium
 Critical Care Pharmacological Management of Delirium Policy Title: in the Critical Care Unit Executive Summary: This policy provides guidance Pharmacological Management of delirium in the Critical Care
Critical Care Pharmacological Management of Delirium Policy Title: in the Critical Care Unit Executive Summary: This policy provides guidance Pharmacological Management of delirium in the Critical Care
Improving the quality of care of patients with delirium
 Improving the quality of care of patients with delirium Alasdair MacLullich MRCP(UK), PhD Professor of Geriatric Medicine University of Edinburgh Scotland How are we doing now? We are doing badly. Difficult
Improving the quality of care of patients with delirium Alasdair MacLullich MRCP(UK), PhD Professor of Geriatric Medicine University of Edinburgh Scotland How are we doing now? We are doing badly. Difficult
Delirium Pilot Project
 CCU Nurses: Delirium Pilot Project Our unit has been selected to develop and implement a delirium assessment and intervention program. We are beginning Phase 1 with education and assessing for our baseline
CCU Nurses: Delirium Pilot Project Our unit has been selected to develop and implement a delirium assessment and intervention program. We are beginning Phase 1 with education and assessing for our baseline
Delirium Assessment. February 24, Susan Schumacher, MS, APRN-BC
 Delirium Assessment February 24, 2016 Susan Schumacher, MS, APRN-BC Objectives Define delirium Differentiate delirium from dementia Identify predisposing and precipitating factors leading to delirium.
Delirium Assessment February 24, 2016 Susan Schumacher, MS, APRN-BC Objectives Define delirium Differentiate delirium from dementia Identify predisposing and precipitating factors leading to delirium.
Addressing Difficult Behaviors in Dementia
 Addressing Difficult Behaviors in Dementia GEORGE SCHOEPHOERSTER, MD GERIATRICIAN GENEVIVE/CENTRACARE CLINIC Objectives By the end of the session, you will be able to: 1) Explain the role of pain management
Addressing Difficult Behaviors in Dementia GEORGE SCHOEPHOERSTER, MD GERIATRICIAN GENEVIVE/CENTRACARE CLINIC Objectives By the end of the session, you will be able to: 1) Explain the role of pain management
ICU Delirium: Recognition, Management and Long-Term Outcomes
 ICU Delirium: Recognition, Management and Long-Term Outcomes Sandy Staveski RN, PhD, CPNP-AC/PC, CNS Assistant Professor, Nurse Scientist Cincinnati Children s Hospital Medical Center Research in Patient
ICU Delirium: Recognition, Management and Long-Term Outcomes Sandy Staveski RN, PhD, CPNP-AC/PC, CNS Assistant Professor, Nurse Scientist Cincinnati Children s Hospital Medical Center Research in Patient
Delirium and Nausea. Delirium - definition. Delirium Incidence. Predisposing Risk Factors for Delirium. Impact. Delirium Types 10/14/2016
 Delirium - definition Delirium and Nausea Etiologically non-specific global cerebral dysfunction associated with changes in LOC, attention, thinking, perception, memory, psychomotor behavior, emotion and
Delirium - definition Delirium and Nausea Etiologically non-specific global cerebral dysfunction associated with changes in LOC, attention, thinking, perception, memory, psychomotor behavior, emotion and
Psychiatric and Behavioral Symptoms in Alzheimer s and Other Dementias. Aaron H. Kaufman, MD
 Psychiatric and Behavioral Symptoms in Alzheimer s and Other Dementias Aaron H. Kaufman, MD Psychiatric and Behavioral Symptoms in Alzheimer s and Other Dementias Aaron H. Kaufman, M.D. Health Sciences
Psychiatric and Behavioral Symptoms in Alzheimer s and Other Dementias Aaron H. Kaufman, MD Psychiatric and Behavioral Symptoms in Alzheimer s and Other Dementias Aaron H. Kaufman, M.D. Health Sciences
AGED SPECIFIC ASSESSMENT TOOLS. Anna Ciotta Senior Clinical Neuropsychologist Peninsula Mental Health Services
 AGED SPECIFIC ASSESSMENT TOOLS Anna Ciotta Senior Clinical Neuropsychologist Peninsula Mental Health Services Issues in assessing the Elderly Association between biological, psychological, social and cultural
AGED SPECIFIC ASSESSMENT TOOLS Anna Ciotta Senior Clinical Neuropsychologist Peninsula Mental Health Services Issues in assessing the Elderly Association between biological, psychological, social and cultural
Delirium in the Emergency Department. Emergency Medicine Rounds April 14, 2015 Paul R. Vanhoutte
 Delirium in the Emergency Department Emergency Medicine Rounds April 14, 2015 Paul R. Vanhoutte Goals of Rounds: Review Definition Management An Understanding What is important is to spread confusion,
Delirium in the Emergency Department Emergency Medicine Rounds April 14, 2015 Paul R. Vanhoutte Goals of Rounds: Review Definition Management An Understanding What is important is to spread confusion,
Table 1: 1. : Summary y of the selection criteria.
 Table 1: 1 : Summary y of the selection criteria. Exclusion criteria: a. Timing (Jan 2000 and March 2016) b. e of the following uses: procedural sedation for surgical procedures, as part of burn care,
Table 1: 1 : Summary y of the selection criteria. Exclusion criteria: a. Timing (Jan 2000 and March 2016) b. e of the following uses: procedural sedation for surgical procedures, as part of burn care,
End of Life with Dementia Sue Quist RN, CHPN
 End of Life with Dementia Sue Quist RN, CHPN Objectives: Describe the Medicare hospice benefit and services. Discuss the Medicare admission criteria for hospice patients with dementia due to Alzheimer
End of Life with Dementia Sue Quist RN, CHPN Objectives: Describe the Medicare hospice benefit and services. Discuss the Medicare admission criteria for hospice patients with dementia due to Alzheimer
Geriatric Alterations Associated with Neurological Conditions
 Geriatric Alterations Associated with Neurological Conditions I have no conflicts of interest. Julie Bronson The Older Adult According to the World Health Organization Africa 50-55 or 50-65 United Nations
Geriatric Alterations Associated with Neurological Conditions I have no conflicts of interest. Julie Bronson The Older Adult According to the World Health Organization Africa 50-55 or 50-65 United Nations
Fighting the Fog A Collaborative Approach to Decreasing ICU Delirium
 Fighting the Fog A Collaborative Approach to Decreasing ICU Delirium Kimberly Scherr NP Jennifer Barker RN Misericordia Hospital ICU Edmonton, AB CACCN Dynamics Sept 21, 2014 Delirium Delirium is an acute
Fighting the Fog A Collaborative Approach to Decreasing ICU Delirium Kimberly Scherr NP Jennifer Barker RN Misericordia Hospital ICU Edmonton, AB CACCN Dynamics Sept 21, 2014 Delirium Delirium is an acute
Memory Matters Service Dementia, Depression and Delerium Cancer Awareness Toolkit Evaluation Event
 Cumbria Partnership NHS Foundation Trust Memory Matters Service Dementia, Depression and Delerium Cancer Awareness Toolkit Evaluation Event Andrew Milburn Occupational Therapy Clinical Lead, Dementia Pathways
Cumbria Partnership NHS Foundation Trust Memory Matters Service Dementia, Depression and Delerium Cancer Awareness Toolkit Evaluation Event Andrew Milburn Occupational Therapy Clinical Lead, Dementia Pathways
Conducting Delirium Research
 Optimizing Clinical Trials When Conducting Research Research funding: Disclosure NHLBI, NIA, AstraZeneca John W. Devlin, PharmD, FCCP, FCCM, Professor of Pharmacy, Northeastern University Scientific Staff,
Optimizing Clinical Trials When Conducting Research Research funding: Disclosure NHLBI, NIA, AstraZeneca John W. Devlin, PharmD, FCCP, FCCM, Professor of Pharmacy, Northeastern University Scientific Staff,