Management of HMB in women with haematological disease and other medical disorders. Rezan A Kadir The Royal Free Foundation Trust IfWH, UCL
|
|
|
- Scarlett Knight
- 5 years ago
- Views:
Transcription



1 Management of HMB in women with haematological disease and other medical disorders Rezan A Kadir The Royal Free Foundation Trust IfWH, UCL
2 HMB - Systemic causes FIGO Classification - PALM-COEIN COEIN- Non Structural Coagulopathy Ovulatory Dysfunction Endometrial Iatrogenic Not yet classified Systemic conditions Inherited bleeding disorders VWD Carriers of haemophilia Inherited Platelet abnormalities Rare coagulation factor defects Acquired Bleeding disorders Immune thrombocytopenia Anticoagulant therapy Other medical disorders Endocrine abnormalities Chronic disorders
3 HMB - Other medical disorders Chronic conditions Possible mechanisms Renal failure Liver failure Diabetes Thyroid abnormalities Adrenal abnormalities Blood malignancies Coagulopathy Impaired Clotting factor production Thrombocytopenia, impaired platelet function Anticaogulant therapy HPO axis - direct effect or secondary to medications Oestrogen metabolism Chemotherapy, steroids, other medications

4 Von Willebrand Disease - VWD

5 VWF mediated platelet aggregation Fibrin formation Vasoconstriction Tissue regeneration Hemostasis in menstruation INADEQUATE and/or OVER- INDUCTION COMPENSATION Platelet adhesion Platelet aggregation PG induced platelet inhibition Fibrinolysis Vasodilatation platelets platelets GP 1b Endothelial cells VWF platelets Increased menstrual blood loss HMB Subendothelium Collagen

6 PBAC score - higher in affected women p = Excessive bleeding at Menarche
7 Breakthrough bleeding IMB and PCB Iron deficiency anaemia Early hysterectomy
8 HMB and Bleeding Disorders VWD in women with HMB Overall = 13% (C.I %) 131/998 European studies Edlund 1996 Kadir 1998 Woo 2001 Krause 2000 Total 18% N. American studies Kouides 2000 Hambleton 2000 G-Gruen 2001 Dilley 2001 Philip 2003 Total 10% Other studies Baindur 2000 Ekiaby Shanker et al 2004
9 HMB and Bleeding Disorders Platelet function defect 50% 45% 40% 35% 30% 25% 20% 15% 10% Platelet aggregation and/or release defect Agonists Platelet agg./rel. defect to multiple agonists Platelet agg./rel. defect to ristocetin at 1 ng/ml Platelet agg./rel. defect with one non-risotcetin 5% 0% VWD others Platelet dysfunction Miller CH et al 2007

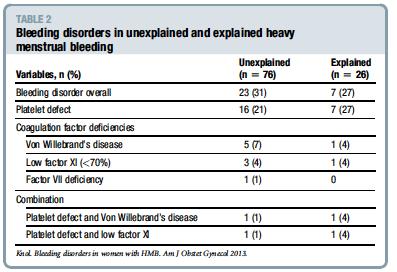
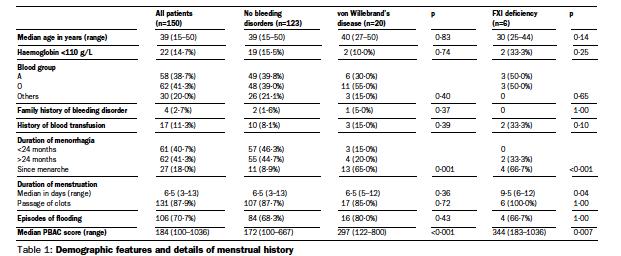
10 102 women with HMB
11
12

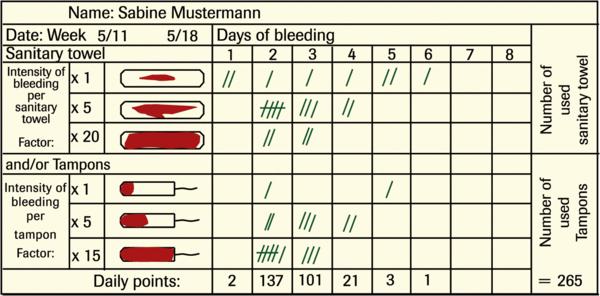
13 Pictorial blood assessment chart (PBAC)
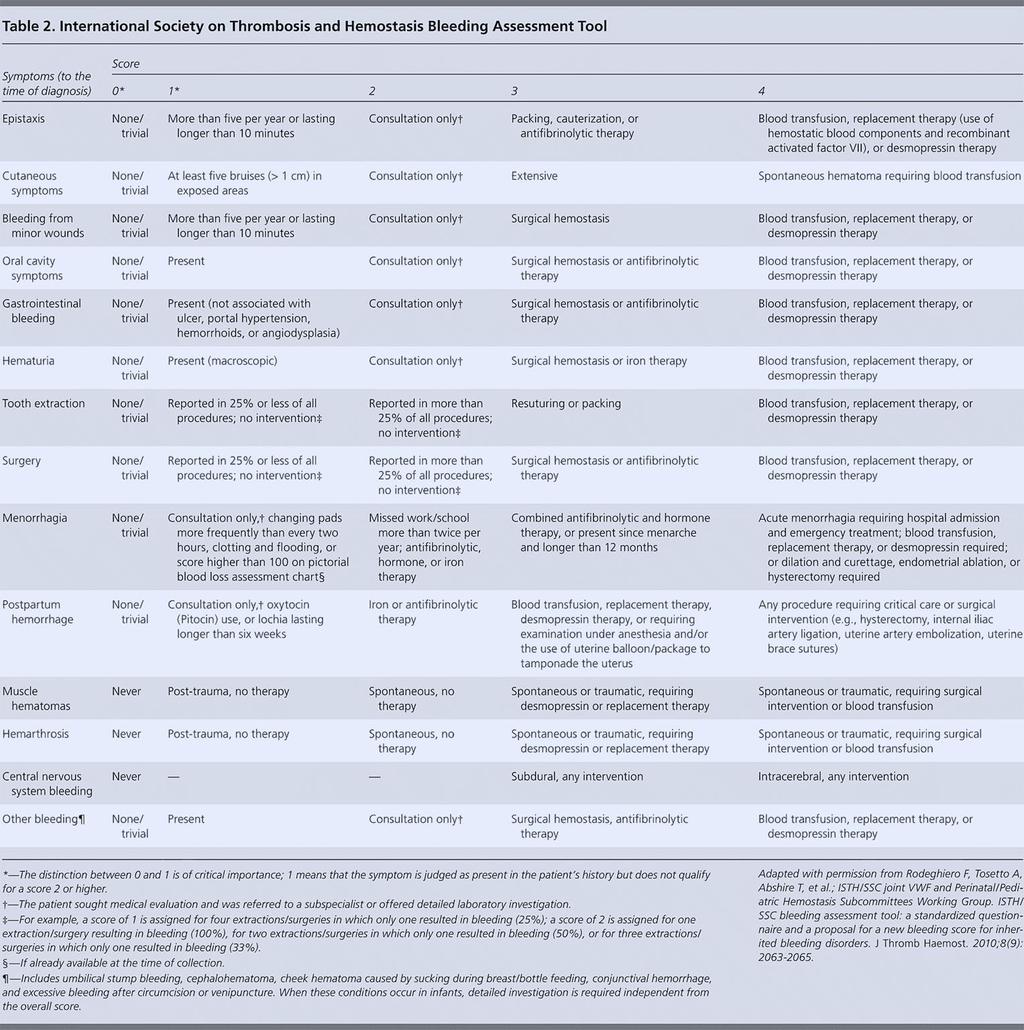
14 Condensed MCMDM-1 VWD Bleeding Questionnaire Epistaxis -- No or trivial ( 5 per year) > 5 per year or more than 10 Consultation only Packing or cauterization or antifibrinolytic Blood transfusion or replacement therapy or desmopressin Cutaneous -- No or trivial ( 1 cm) > 1 cm and no trauma Consultation only Bleeding from minor wounds -- No or trivial ( 5 per year) > 5 per year or more than 5 Consultation only Surgical hemostasis Blood transfusion or replacement therapy or desmopressin Oral cavity -- No Referred, no consultation Consultation only Surgical hemostasis or antifibrinolytic Blood transfusion or replacement therapy or desmopressin Gastrointestinal bleeding -- No Associated with ulcer, portal hypertension, hemorrhoids, angiodysplasia Spontaneous Surgical hemostasis, blood transfusion, replacement therapy, desmopressin, antifibrinolytic -- Tooth extraction No bleeding in at least 2 extractions None done or no bleeding in 1 extraction Reported, no consultation Consultation only Resuturing or packing Blood transfusion or replacement therapy or desmopressin Surgery No bleeding in at least 2 surgeries None done or no bleeding in 1 surgery Reported, no consultation Consultation only Surgical hemostasis or antifibrinolytic Blood transfusion or replacement therapy or desmopressin Menorrhagia -- No Consultation only Antifibrinolytics, oral contraceptive pill use Dilation & curettage, iron therapy, ablation Blood transfusion or replacement therapy or desmopressin or hysterectomy Postpartum hemorrhage No bleeding in at least 2 deliveries None done or no bleeding in 1 delivery Consultation only Dilation & curettage, iron therapy, antifibrinolytics Blood transfusion or replacement therapy or desmopressin Hysterectomy Muscle hematomas -- Never Post trauma, no therapy Spontaneous, no therapy Spontaneous or traumatic, requiring desmopressin or replacement therapy Hemarthrosis -- Never Post trauma, no therapy Spontaneous, no therapy Spontaneous or traumatic, requiring desmopressin or replacement therapy Spontaneous or traumatic, requiring surgical intervention or blood transfusion Spontaneous or traumatic, requiring surgical intervention or blood transfusion Central nervous system bleeding -- Never Subdural, any intervention Intracerebral, any intervention
15
16 HMB - Haemostatic assessment Heavy menstrual bleeding since menarche Recurrent ovulation bleeding Not responding to medical treatment Or HMB + One of the following bleeding Significant or recurrent postpartum haemorrhage Surgery-related bleeding Bleeding associated with dental work Two or more of the following conditions: Bruising, epistaxis, gum bleeding Family history of bleeding disorder Or BS 5
17 HMB - Haemostatic assessment Diagnostic approach FBC and Ferritin level PT, APTT FVIII, VWF:Ag, VWF:Ricof, VWF:CB Platelet function tests Further testing - If high suspicion for Bleeding disorder - or FH of specific BD

18 HMB - Haemostatic assessment Diagnostic approach VWF FVIII variation Physical activity, stress Effect of female hormones Collaboration Haemotology team Hormonal therapy? mask Dx Day of the cycle, use of OC pill, HRT noted Borderline levels repeat test Day 1-5 of the cycle Variation Mandalaki et al 1980, Blomback et al 1992, Kadir et al 1999, Miller et al 2002

19 HMB - Haemostatic assessment FBC and Ferritin assessment Iron deficiency (ID) /Low Ferritin predicts Clinical severity of HMB Low ferritin - predict 60% of MBL>80ml Underlying bleeding disorders HMB and ID odd ratio 3.3 Jayasinghe et al 2005, Warner et al 2004 Medical management of ID/IDA Improve PF - May reduce MBL Reduce the need for BT in HMB Reduce peri-operative BT 370 women prior Hysterectomy Iron therapy - BT reduced 22.7% to 1% Akay et al 2007, Sheth&Das 2002

20 HMB - Therapeutic options Options - haemostatic, hormonal and surgical Choice - age, fertility wishes, underlying cause, severity and type of bleeding disorder, side effect profile and availability of the treatment Women with bleeding disorders - often require combination therapy
21 LNG-IUS (Mirena IUS) Most effective treatment for HMB Most effective reversible contraceptive 5 years Other Possible Health Benefits Menstrual pain &PMS Endometrial hyperplasia Endometriosis, adenomyosis, fibroid Suitable for women with Bleeding disorders Thrombotic disorders
22 LNG-IUS (Mirena IUS) HMB in women with bleeding disorders Follow up - 3 years 45% - amenorrhea Improved QoL Kingman et al 2004, Chi et al 2007
23 Other hormonal contraceptives Combined Hormonal Contraception (Oral, Transdermal, vaginal rings) Effective Contraception Good cycle control Control menstrual pain and PMS Inhibit ovulation - prevent ovulation bleeding Extended use - reduce menstrual episodes with no complications Progesterone only contraceptives Progesterone only contraceptives pill (POP) - Desogestrel Amenorrhoea in up to 20% - can be used when OCP is contraindicated Depot medroxyprogesterone acetate (DMPA) - amenorrhoea 50% But significant irregular bleeding in women with bleeding disorders
24 Other hormonal therapies Cyclical progestagens 63% and 78% reduction in MBL during 1 st and 3 rd cycle Discontinuation - 78% - hormonal SE GnRH analogue with/without add-back therapy Amenorrhea - but menopausal symptoms Long-term - significant SE - Osteoporosis Last option in severe BD - with add-back therapy - GT and BSS
25 Haemostatic agent (Tranexamic acid - DDAVP) 116 women TA and DDAVP Improved HRQOL Combination of TA+DDAVP Improve efficacy Shorter duration and smaller dose DDAVP Reduce adverse effects Discontinuation TA 4, DDAVP 6 (1 hyponatremia) Edlund et al 2003, Kouides et al 2009
26 Haemostatic agent - Factor Replacement Menstrual related bleeding Factor Replacement 10% Chi et al 2010
27 HMB - Surgical Management Hysterectomy - Pelvic pathology, unresponsive to other therapies Appropriate haemostatic assessment and haemostaic cover No VWD n=1,357,588 VWD n=545 P value Thrombosis 0.20% Infection 0.38% 0.73% Transfusion 2.13% 7.34% <0.001 Bleeding 0.86% 2.75% <0.001 Wound compl. 0.15% 0.37% Length of stay 3.49 days Cost $13,225 $19,584 <0.001 Died 0.13% 0.18% James et al 2009, data from the NIS
28 HMB - Endometrial Ablation Women with coagulopathy not responding to medical treatments Uterus 10/52, fibroids < 3 cm PBAC Scores Pre Ablation Post Ablation P value Mean Median <0.01 Increased Hb, Ferritin Improved QOL El-Nashar et al 2007 Huq et al 2013
29 HMB - Oral anticoagulant Vitamin K antagonists 90 menstruating women - after starting VKA 71% reported HMB - 30% required treatment Sjalander et al % - PBAC score >100 VKA therapy - 53 women - 70% reported change - 50% increase MBL - 30% - referral to gynaecologist None - major bleeding Yaq et al 2011


30 Direct Oral Anti-Coagulants (DOACs) Initiation TF VIIa VII X IX Propagation Direct Factor Xa inhibition Rivaroxaban Apixaban Edoxaban Betrixaban Darexaban Xa IIa IXa II Thrombin Prothrombin Direct Factor IIa inhibition Dabigatran etexilate Clot formation Fibrinogen Fibrin Adapted from Spyropoulos AC. Expert Opin Investig Drugs 2007;16:
31 HMB - Direct Oral Anti-Coagulant Meta-analysis of 8 RCTs on DOACs for VTE patients Difference between men and women No difference in the primary efficacy outcome of recurrent VTE Men had less major bleeding compared to women [RR 0.79, 95% CI , p=0.03] Alotaibi et al DOACs women 57 women reported - 72 vaginal bleeding HMB - 6 (8%) Major bleed - 4 in Rivaroxaban Jan Beyer-Westendorf et al 2016
32 Menstrual bleeding - DOACs Study Cases Major findings Ferreira; Br J Haematol 2016 De Crem; Thromb Res 2015 Bryk; Vascul Pharmacol Kline; Patient Prefer Adherence Godin; Vascul Pharmacol Women rivaroxaban 52 women rivaroxaban vs 52 women VKA 76 women rivaroxaban vs. 45 women VKA 113 women with rivaroxaban therapy 139 women (96 rivaroxaban vs. 43 apixaban) HMB in 26 (20%); mean age 38,7 years Increase in MB duration more frequent with rivaroxaban vs. VKA; also interventions more frequent Increase of MB intensity more frequent with rivaroxaban vs. VKA (41% vs 18%); also interventions more frequent high rate of menorrhagia after starting rivaroxaban (15% of women); hysterectomy in one patient 24 (25%) HMB with rivaroxaban (9 women discontinued rivaroxaban) 4 (9.3%) HMB with apixaban (1 woman discontinued apixaban)
33 HMB - Women on anticoagulant therapy Prior assessment and counselling Menstrual history Use of other medication that may exacerbate HMB Check for ID/IDA Advice - report any change in menstrual loss Those affected with heavy bleeding on on treatment Assess severity of bleeding Exclude pelvic pathology Dresden series - 18% had anatomical abnormality (fibroid, polyp), with worse bleeding in such women Jan Beyer-Westendorf et al 2016
34 Management of HMB - Anticoagulant therapy Anticoagulant management Reduce / split does or omit during heavy menstrual days or change type Alternative anticoagulant therapy Hormonal therapy Mirena IUS - thrombotic risk? - benefit outweigh the risk 17 women- Reduction MBL reported in 59% and amenorrhea in 23% CHC - Controversial WHO 2015 guideline - CHC - confers an unacceptable health risk ISTH SSC- CHC or HRT until they discontinue anticoagulant therapy ENJM 2010
 as a timedependent variable to VTE incidence densities on and off hormonal therapy were 3.7%/year and 4.7%/year (adjusted HR, 0.56; 95% CI 0.23-1.39), respectively VTE incidence densities 3.")
35 No increase of VTE recurrence risk from COC during OAC 1888 women aged < 60 years included in EINSTEIN DVT/PE Cox regression models with hormonal therapy (on vs. off) as a timedependent variable to VTE incidence densities on and off hormonal therapy were 3.7%/year and 4.7%/year (adjusted HR, 0.56; 95% CI ), respectively VTE incidence densities 3.7%/year for estrogen-containing and 3.8%/year for progestin-only therapy Blood 2016;127(11):
36 Management of HMB - Anticoagulant therapy Cyclical Progesterone - therapeutic dose WHO collaborative study - odd ratio for VTE 5.92 GPRD women - odd ratio 5.3 GPRD nested case control study of 134 women with a VTE event and HMB - adjusted OR Norethisterone Vs medroxyprogesterone acetate Sundstrom et al 2009
37 Management of HMB - Anticoagulant therapy Non Hormonal therapies Tranexamic acid - No increase in thrombotic risk Mefanamic acid (NSAIDs) Improve menstrual symptoms But increased bleeding risk GPRD - increased VTE risk - OR 5.54 ( ) Sundstrom et al 2009
38 Management of HMB - Anticoagulant therapy Surgical treatment Endometrial ablation - women require long-term anticoagulant therapy and completed their family Cohen et al 2017 El-Nashar et al 2007
39 Conclusions HMB is a common gynaecological problem has a significant health impact and adversely affect women QOL Women with bleeding disorders and those on anticoagulant therapy are at a higher risk of HMB Close collaboration between Gynaecology and haematology teams is essential for provision of quality care There are several therapeutic options - an individualised approach is important to provide the women the best option Further research is required especially in better understanding the local factors within the endometrium for development of future therapeutic options and for precision medicine approach for management
40

41 Thank you
42
43 n= 105 patients Referred for HMB 62% diagnosed with BD - 36% had Platelet Storage Pool Deficiency Vo K et al. Haemophilia (2012)

44 100 women with AUB 30% abnormal thyroid function Hypothyroid - HMB and prolonged menses Hyperthyroid - oligomenorrhea 50 women with AUB - 44% Thyroid dysfunction

45 VWD - bleeding symptoms in women

46 VWD - bleeding symptoms in women HMB in girls/women with mild/moderate VWD Initial bleeding symptom 53% of women The only bleeding symptom for a long time Kadir et al haemophilia 1999 Ragni et al haemophilia 1999
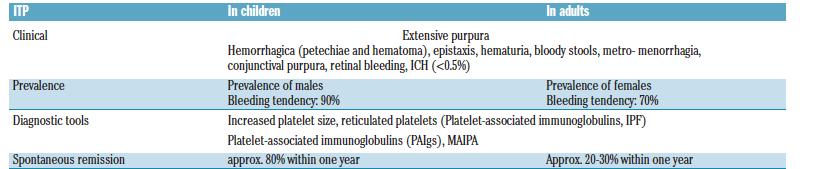
47 Immune thrombocytopenia - ITP
Controversies in the Diagnosis of Type 1 VWD. Paula James MD, FRCPC ISLH Honolulu, Hawaii Friday, May 5, 2017
 Controversies in the Diagnosis of Type 1 VWD Paula James MD, FRCPC ISLH Honolulu, Hawaii Friday, May 5, 2017 Disclosures for Paula James Research Support/P.I. Employee Consultant Major Stockholder Speakers
Controversies in the Diagnosis of Type 1 VWD Paula James MD, FRCPC ISLH Honolulu, Hawaii Friday, May 5, 2017 Disclosures for Paula James Research Support/P.I. Employee Consultant Major Stockholder Speakers
GUIDELINES. for the diagnosis and management of von Willebrand disease (VWD)
") GUIDELINES for the diagnosis and management of von Willebrand disease (VWD) The Canadian Hemophilia Society (CHS) is committed to improve the health and quality of life of all people with inherited bleeding
GUIDELINES for the diagnosis and management of von Willebrand disease (VWD) The Canadian Hemophilia Society (CHS) is committed to improve the health and quality of life of all people with inherited bleeding
Dysfunctional Uterine Bleeding
 Long term effects of PCOS Dysfunctional Uterine Bleeding Dr. Arulmozhi Ramarajan Church of South India Hospital, Bangalore Abnormal uterine bleeding Affects health-related QOL Causes social embarrasment
Long term effects of PCOS Dysfunctional Uterine Bleeding Dr. Arulmozhi Ramarajan Church of South India Hospital, Bangalore Abnormal uterine bleeding Affects health-related QOL Causes social embarrasment
BLEEDING. Introduction. Starship Children s Health Clinical Guideline. Introduction Bleeding Questionnaire. Scoring Key References
 te: The electronic version of this guideline is the version currently in use. Any printed version can Introduction Bleeding Questionnaire Scoring Key References Introduction This bleeding questionnaire
te: The electronic version of this guideline is the version currently in use. Any printed version can Introduction Bleeding Questionnaire Scoring Key References Introduction This bleeding questionnaire
Menstrual Disorders & Ambulatory Gynaecology
 Menstrual Disorders & Ambulatory Gynaecology Mr. Nagui Lewis Aziz M B, CH B, FRCOG Consultant Gynaecologist The Royal Oldham Hospital 01/09/2018 Heavy menstrual bleeding (HMB ) is a common problem responsible
Menstrual Disorders & Ambulatory Gynaecology Mr. Nagui Lewis Aziz M B, CH B, FRCOG Consultant Gynaecologist The Royal Oldham Hospital 01/09/2018 Heavy menstrual bleeding (HMB ) is a common problem responsible
Heavy Menstrual Bleeding. Mr Nick Nicholas MD FRCOG Grad Dip Law. Consultant Gynaecologist
 Heavy Menstrual Bleeding Mr Nick Nicholas MD FRCOG Grad Dip Law. Consultant Gynaecologist Why is HMB so important? 1:20 women aged 30-49 consult their GP with HMB Once referred to gynaecologist, surgical
Heavy Menstrual Bleeding Mr Nick Nicholas MD FRCOG Grad Dip Law. Consultant Gynaecologist Why is HMB so important? 1:20 women aged 30-49 consult their GP with HMB Once referred to gynaecologist, surgical
Healthcare Education Research
 Healthcare Education Research Heavy menstrual bleeding: investigation, diagnosis & management An update for health professionals Assessment of heavy menstrual bleeding in primary care Dr Amanda Newman
Healthcare Education Research Heavy menstrual bleeding: investigation, diagnosis & management An update for health professionals Assessment of heavy menstrual bleeding in primary care Dr Amanda Newman
Dr. Nancy Van Eyk Associate Professor, Dalhousie University Chief of Gynaecology, IWK Health Centre
 Dr. Nancy Van Eyk Associate Professor, Dalhousie University Chief of Gynaecology, IWK Health Centre AUB Outline Terminology Classification/Etiology Assessment Treatment Referral to Gynaecology U c pt 4
Dr. Nancy Van Eyk Associate Professor, Dalhousie University Chief of Gynaecology, IWK Health Centre AUB Outline Terminology Classification/Etiology Assessment Treatment Referral to Gynaecology U c pt 4
Frequency of menses. Duration of menses 3 days to 7 days. Flow/amount of menses Average blood loss with menstruation is 60-80cc.
 Frequency of menses 24 days (0.5%) to 35 days (0.9%) Age 25, 40% are between 25 and 28 days Age 25-35, 60% are between 25 and 28 days Teens and women over 40 s cycles may be longer apart Duration of menses
Frequency of menses 24 days (0.5%) to 35 days (0.9%) Age 25, 40% are between 25 and 28 days Age 25-35, 60% are between 25 and 28 days Teens and women over 40 s cycles may be longer apart Duration of menses
Abnormal Uterine Bleeding: Evaluation of Premenopausal Women. Vanessa Jacoby, MD, MAS Assistant Professor Ob, Gyn, & Reproductive Sciences UCSF
 Abnormal Uterine Bleeding: Evaluation of Premenopausal Women Vanessa Jacoby, MD, MAS Assistant Professor Ob, Gyn, & Reproductive Sciences UCSF Objectives Define normal and abnormal uterine bleeding Review
Abnormal Uterine Bleeding: Evaluation of Premenopausal Women Vanessa Jacoby, MD, MAS Assistant Professor Ob, Gyn, & Reproductive Sciences UCSF Objectives Define normal and abnormal uterine bleeding Review
Abnormal uterine bleeding:
 Primary Care Women s Health Forum 16th June 2010 Abnormal uterine bleeding: The University Of Birmingham T Justin Clark MD (Hons), MRCOG Consultant Obstetrician and Gynaecologist Birmingham Women s Hospital
Primary Care Women s Health Forum 16th June 2010 Abnormal uterine bleeding: The University Of Birmingham T Justin Clark MD (Hons), MRCOG Consultant Obstetrician and Gynaecologist Birmingham Women s Hospital
Hemostasis. PHYSIOLOGICAL BLOOD CLOTTING IN RESPONSE TO INJURY OR LEAK no disclosures
 Hemostasis PHYSIOLOGICAL BLOOD CLOTTING IN RESPONSE TO INJURY OR LEAK no disclosures Disorders of Hemostasis - Hemophilia - von Willebrand Disease HEMOPHILIA A defect in the thrombin propagation phase
Hemostasis PHYSIOLOGICAL BLOOD CLOTTING IN RESPONSE TO INJURY OR LEAK no disclosures Disorders of Hemostasis - Hemophilia - von Willebrand Disease HEMOPHILIA A defect in the thrombin propagation phase
Medical treatment for uterine fibroids
 Medical treatment for uterine fibroids Prof Mary Ann Lumsden Prof of Gynaecology and Medical Education University of Glasgow Senior Vice President RCOG Conflict of Interest Chair, Guideline development
Medical treatment for uterine fibroids Prof Mary Ann Lumsden Prof of Gynaecology and Medical Education University of Glasgow Senior Vice President RCOG Conflict of Interest Chair, Guideline development
Easy bruising vs Coagulopathy
 Easy bruising vs Coagulopathy Sept. 19, 2015 Lakehead Summer School Chris Hillis, MD MSc FRCPC hillis@hhsc.ca @HemeHillis Aim & Objectives Aim: To increase comfort in detecting non-pathologic bleeding
Easy bruising vs Coagulopathy Sept. 19, 2015 Lakehead Summer School Chris Hillis, MD MSc FRCPC hillis@hhsc.ca @HemeHillis Aim & Objectives Aim: To increase comfort in detecting non-pathologic bleeding
Pediatric Bleeding Questionnaire (PBQ)
") Date Patient Number Patient Name Gender Male Female Age DOB (dd/mm/yy) Ethnic Background of: Father Mother Presenting complaint of bleeding or bruising today? Ever been diagnosed with a bleeding disorder?
Date Patient Number Patient Name Gender Male Female Age DOB (dd/mm/yy) Ethnic Background of: Father Mother Presenting complaint of bleeding or bruising today? Ever been diagnosed with a bleeding disorder?
Topics. Periods Menopause & HRT Contraception Vulva problems
 Girls stuff Topics Periods Menopause & HRT Contraception Vulva problems Menorrhagia Excessive menstrual loss occurring with regular or irregular cycles Ovulatory Anovulatory Usual blood loss 30-40ml per
Girls stuff Topics Periods Menopause & HRT Contraception Vulva problems Menorrhagia Excessive menstrual loss occurring with regular or irregular cycles Ovulatory Anovulatory Usual blood loss 30-40ml per
Chapter 100 Gynecologic Disorders
 Chapter 100 Gynecologic Disorders Episode Overview: 1. Describe the presentation and RF for Adnexal torsion 2. List the imaging findings of adnexal torsion (US vs CT) 3. What is the management of adnexal
Chapter 100 Gynecologic Disorders Episode Overview: 1. Describe the presentation and RF for Adnexal torsion 2. List the imaging findings of adnexal torsion (US vs CT) 3. What is the management of adnexal
Conflicts 10/5/2016. Abnormal Uterine Bleeding. Objectives Review diagnosis and updated nomenclature. Management options for acute and chronic AUB.
 Abnormal Uterine Bleeding Barbara L. Keller, MD JD Naval Hospital Oak Harbor OB/GYN Physician Conflicts I have no conflicts or financial interests to disclose. Objectives Review diagnosis and updated nomenclature.
Abnormal Uterine Bleeding Barbara L. Keller, MD JD Naval Hospital Oak Harbor OB/GYN Physician Conflicts I have no conflicts or financial interests to disclose. Objectives Review diagnosis and updated nomenclature.
Cynthia Morris DO, FACOOG, FACOS Medical Director, Women s Wellness Center Fayette County Memorial Hospital
 Cynthia Morris DO, FACOOG, FACOS Medical Director, Women s Wellness Center Fayette County Memorial Hospital Touchdown to CME Eighth District Academy of Osteopathic Medicine & Surgery October 8. 2017 Goals
Cynthia Morris DO, FACOOG, FACOS Medical Director, Women s Wellness Center Fayette County Memorial Hospital Touchdown to CME Eighth District Academy of Osteopathic Medicine & Surgery October 8. 2017 Goals
Approach to bleeding disorders &treatment. by RAJESH.N General medicine post graduate
 Approach to bleeding disorders &treatment by RAJESH.N General medicine post graduate 2 Approach to a patient of bleeding diathesis 1. Clinical evaluation: History, Clinical features 2. Laboratory approach:
Approach to bleeding disorders &treatment by RAJESH.N General medicine post graduate 2 Approach to a patient of bleeding diathesis 1. Clinical evaluation: History, Clinical features 2. Laboratory approach:
Elaina Sexton, MD, MSc Obstetrics and Gynecology St. Vincent s Hospital. Objectives
 Elaina Sexton, MD, MSc Obstetrics and Gynecology St. Vincent s Hospital Objectives Definition of normal menstrual cycle and abnormal uterine bleeding (AUB) Evaluation of AUB Medical options for AUB Surgical
Elaina Sexton, MD, MSc Obstetrics and Gynecology St. Vincent s Hospital Objectives Definition of normal menstrual cycle and abnormal uterine bleeding (AUB) Evaluation of AUB Medical options for AUB Surgical
ROLE OF LOW MOLECULAR WEIGHT HEPARIN IN THE AGE OF DIRECT ORAL ANTICOAGULANTS
 ROLE OF LOW MOLECULAR WEIGHT HEPARIN IN THE AGE OF DIRECT ORAL ANTICOAGULANTS Chee Yen Lin Consultant Haematologist NCIS Haematology National University Hospital Singapore Nomenclature direct oral anticoagulant
ROLE OF LOW MOLECULAR WEIGHT HEPARIN IN THE AGE OF DIRECT ORAL ANTICOAGULANTS Chee Yen Lin Consultant Haematologist NCIS Haematology National University Hospital Singapore Nomenclature direct oral anticoagulant
ANEMIA AND HEAVY MENSTRUAL BLEEDING
 ANEMIA AND HEAVY MENSTRUAL BLEEDING MENAKA PAI, BSC, MSC, MD, FRCPC Associate Professor, Dept Of Medicine, McMaster University Associate Member, Dept Of Pathology & Molecular Medicine, McMaster University
ANEMIA AND HEAVY MENSTRUAL BLEEDING MENAKA PAI, BSC, MSC, MD, FRCPC Associate Professor, Dept Of Medicine, McMaster University Associate Member, Dept Of Pathology & Molecular Medicine, McMaster University
Update on Medical and Surgical Therapy Sara Jane Pieper, MD Chair, Gynecology Development Team
 ABNORMAL UTERINE BLEEDING Update on Medical and Surgical Therapy Sara Jane Pieper, MD Chair, Gynecology Development Team Goals Review appropriate medical therapies for abnormal uterine bleeding Review
ABNORMAL UTERINE BLEEDING Update on Medical and Surgical Therapy Sara Jane Pieper, MD Chair, Gynecology Development Team Goals Review appropriate medical therapies for abnormal uterine bleeding Review
Investigating HMB- an evidence based approach
 BSGE Meeting: Contemporary management of heavy menstrual bleeding (HMB) in primary and secondary care: (7 th December 2018, RCOG) Investigating HMB- an evidence based approach T. Justin Clark MB ChB, MD(Hons),
BSGE Meeting: Contemporary management of heavy menstrual bleeding (HMB) in primary and secondary care: (7 th December 2018, RCOG) Investigating HMB- an evidence based approach T. Justin Clark MB ChB, MD(Hons),
Treatment of Heavy Menstrual Bleeding: Ludkin (Nurse Hysteroscopist, Bradford Royal Infirmary) & M Rogers (Advanced
 & M Rogers (Advanced") Treatment of Heavy Menstrual Bleeding: Nov 14 th 2013- Authors: Prof Sian Jones (Gynaecologist, Bradford Royal Infirmary, H Ludkin (Nurse Hysteroscopist, Bradford Royal Infirmary) & M Rogers (Advanced
Treatment of Heavy Menstrual Bleeding: Nov 14 th 2013- Authors: Prof Sian Jones (Gynaecologist, Bradford Royal Infirmary, H Ludkin (Nurse Hysteroscopist, Bradford Royal Infirmary) & M Rogers (Advanced
TREATMENT & MANAGEMENT OF VON WILLEBRAND DISEASE
 TREATMENT & MANAGEMENT OF VON WILLEBRAND DISEASE Dr Susan Russell Director HTC Sydney Children s Hospital, Randwick HFA Meeting 2015 What is von Willebrand Factor? VWF is a large multimeric protein Two
TREATMENT & MANAGEMENT OF VON WILLEBRAND DISEASE Dr Susan Russell Director HTC Sydney Children s Hospital, Randwick HFA Meeting 2015 What is von Willebrand Factor? VWF is a large multimeric protein Two
PALM-COEIN: Your AUB Counseling Guide
 PALM-COEIN: Your AUB Counseling Guide 10 million+ Treat the cause, not the symptom In the U.S, more than 10 million women between the ages of 35 and 49 are affected by AUB 1 Diagnosis Cause Structural
PALM-COEIN: Your AUB Counseling Guide 10 million+ Treat the cause, not the symptom In the U.S, more than 10 million women between the ages of 35 and 49 are affected by AUB 1 Diagnosis Cause Structural
Cancer Associated Thrombosis An update.
 Cancer Associated Thrombosis An update. Simon Noble Marie Curie Professor of Supportive and Palliative Medicine Marie Curie Palliative Care Research Centre Cardiff University The coagulation pathway LIQUID
Cancer Associated Thrombosis An update. Simon Noble Marie Curie Professor of Supportive and Palliative Medicine Marie Curie Palliative Care Research Centre Cardiff University The coagulation pathway LIQUID
Current approaches to managing heavy menstrual bleeding
 Drug review Heavy menstrual bleeding Current approaches to managing heavy menstrual bleeding Jasmine Tay BM BS, Shruti Mohan MRCOG and Jenny Higham FRCOG SPL The choice of drug treatment for heavy menstrual
Drug review Heavy menstrual bleeding Current approaches to managing heavy menstrual bleeding Jasmine Tay BM BS, Shruti Mohan MRCOG and Jenny Higham FRCOG SPL The choice of drug treatment for heavy menstrual
Dysfunctional Uterine Bleeding (DUB) OB/GYN Hospital of Fudan University Weiwei Feng, MD,Ph D Tel:
 OB/GYN Hospital of Fudan University Weiwei Feng, MD,Ph D Tel:") Dysfunctional Uterine Bleeding (DUB) OB/GYN Hospital of Fudan University Weiwei Feng, MD,Ph D Email: wfeng7347@aliyun.com Tel: 13918551061 2014-8-20 Contents DUB: definition, mechanism of normal menses,
Dysfunctional Uterine Bleeding (DUB) OB/GYN Hospital of Fudan University Weiwei Feng, MD,Ph D Email: wfeng7347@aliyun.com Tel: 13918551061 2014-8-20 Contents DUB: definition, mechanism of normal menses,
Heavy Menstrual Bleeding (HMB) Dysmenorrhoea / Endometriosis Endometrial Hyperplasia HRT
 Dysmenorrhoea / Endometriosis Endometrial Hyperplasia HRT") Heavy Menstrual Bleeding (HMB) Dysmenorrhoea / Endometriosis Endometrial Hyperplasia HRT Janesh Gupta Professor of Obstetrics and Gynaecology Birmingham Women s Hospital Heavy Menstrual Bleeding (HMB)
Heavy Menstrual Bleeding (HMB) Dysmenorrhoea / Endometriosis Endometrial Hyperplasia HRT Janesh Gupta Professor of Obstetrics and Gynaecology Birmingham Women s Hospital Heavy Menstrual Bleeding (HMB)
The 6 th Scientific Meeting of the Asia Pacific Menopause Federation
 Abnormal uterine bleeding in the perimenopause Perimenopausal menstrual problems are among the most common causes for family practitioner and specialist referral. Often it is due to the hormone changes
Abnormal uterine bleeding in the perimenopause Perimenopausal menstrual problems are among the most common causes for family practitioner and specialist referral. Often it is due to the hormone changes
Guidelines for Shared Care Centres and Community Staff
 Reference: CG1410 Written by: Dr Jeanette Payne Peer reviewer Dr Jenny Welch Approved: February 2016 Approved by D&TC: 8th January 2016 Review Due: February 2019 Intended Audience This document contains
Reference: CG1410 Written by: Dr Jeanette Payne Peer reviewer Dr Jenny Welch Approved: February 2016 Approved by D&TC: 8th January 2016 Review Due: February 2019 Intended Audience This document contains
An Overview of Non Vitamin-K Antagonist Oral Anticoagulants. Helen Williams Consultant Pharmacist for CV Disease South London
 An Overview of Non Vitamin-K Antagonist Oral Anticoagulants Helen Williams Consultant Pharmacist for CV Disease South London Contents Drugs and drug classes Licensed indications and NICE recommendations
An Overview of Non Vitamin-K Antagonist Oral Anticoagulants Helen Williams Consultant Pharmacist for CV Disease South London Contents Drugs and drug classes Licensed indications and NICE recommendations
Appendix 3 PCC Warfarin Reversal
 Appendix 3 PCC Warfarin Reversal Reversal of Warfarin and Analogues 1. Principle of Procedure Guidelines for the Reversal of Oral-anticoagulation in the Event of Life Threatening Haemorrhage Prothrombin
Appendix 3 PCC Warfarin Reversal Reversal of Warfarin and Analogues 1. Principle of Procedure Guidelines for the Reversal of Oral-anticoagulation in the Event of Life Threatening Haemorrhage Prothrombin
New oral anticoagulants and Palliative Care.
 New oral anticoagulants and Palliative Care. Simon Noble Marie Curie Professor of Supportive and Palliative Medicine Marie Curie Palliative Care Research Centre Cardiff University The coagulation pathway
New oral anticoagulants and Palliative Care. Simon Noble Marie Curie Professor of Supportive and Palliative Medicine Marie Curie Palliative Care Research Centre Cardiff University The coagulation pathway
Management of Challenging Bleeding: Patients with Coagulopathy
 Management of Challenging Bleeding: Patients with Coagulopathy Joanne E Joseph Department of Haematology, SydPath St Vincent s Hospital University of NSW Sydney First and foremost.. It helps to know which
Management of Challenging Bleeding: Patients with Coagulopathy Joanne E Joseph Department of Haematology, SydPath St Vincent s Hospital University of NSW Sydney First and foremost.. It helps to know which
Von Willebrand Disease: Management and Complications. Mike Makris Sheffield, UK
 Von Willebrand Disease: Management and Complications Mike Makris Sheffield, UK Disclosures for Mike Makris Research Support/P.I. Employee Consultant Major Stockholder Speakers Bureau Honoraria Scientific
Von Willebrand Disease: Management and Complications Mike Makris Sheffield, UK Disclosures for Mike Makris Research Support/P.I. Employee Consultant Major Stockholder Speakers Bureau Honoraria Scientific
Original Article ABSTRACT
 Original Article Effectiveness and safety of Levonorgestrel Releasing Intrauterine System in treatment of menorrhagia secondary to oral anticoagulations and chronic liver disease Abeera Choudry, Ayesha
Original Article Effectiveness and safety of Levonorgestrel Releasing Intrauterine System in treatment of menorrhagia secondary to oral anticoagulations and chronic liver disease Abeera Choudry, Ayesha
Gayatrri Anipindi *, Vani I. Original Research Article. Abstract
 Original Research Article Role of levonorgestrel releasing intrauterine device in management of heavy menstrual bleeding: A safe and effective option for all PALM COEIN variants Gayatrri Anipindi *, Vani
Original Research Article Role of levonorgestrel releasing intrauterine device in management of heavy menstrual bleeding: A safe and effective option for all PALM COEIN variants Gayatrri Anipindi *, Vani
5/5/2010 FINANCIAL DISCLOSURE. Abnormal Uterine Bleeding. Is This A Problem? About me % of visits to gynecologist
 Abnormal Uterine FINANCIAL DISCLOSURE I HAVE NO FINANCIAL INTEREST IN ANY OF THE PRODUCTS MENTIONED IN MY PRESENTATION Bryan K. Rone, M.D. University of Kentucky Obstetrics and Gynecology May 5, 2010 About
Abnormal Uterine FINANCIAL DISCLOSURE I HAVE NO FINANCIAL INTEREST IN ANY OF THE PRODUCTS MENTIONED IN MY PRESENTATION Bryan K. Rone, M.D. University of Kentucky Obstetrics and Gynecology May 5, 2010 About
Bleeding Disorders. Dr. Mazen Fawzi Done by Saja M. Al-Neaumy Noor A Mohammad Noor A Joseph Joseph
 Bleeding Disorders Dr. Mazen Fawzi Done by Saja M. Al-Neaumy Noor A Mohammad Noor A Joseph Joseph Normal hemostasis The normal hemostatic response involves interactions among: The blood vessel wall (endothelium)
Bleeding Disorders Dr. Mazen Fawzi Done by Saja M. Al-Neaumy Noor A Mohammad Noor A Joseph Joseph Normal hemostasis The normal hemostatic response involves interactions among: The blood vessel wall (endothelium)
Excessive menstrual blood loss
 Ian Chilcott Excessive menstrual blood loss >80mls - That interferes with physical, emotional, social and material quality of life 1 in 20 women aged 30 to 49 years consult their GP each year with menorrhagia
Ian Chilcott Excessive menstrual blood loss >80mls - That interferes with physical, emotional, social and material quality of life 1 in 20 women aged 30 to 49 years consult their GP each year with menorrhagia
Prothrombin Complex Concentrate- Octaplex. Octaplex
 Prothrombin Complex Concentrate- Concentrated Factors Prothrombin Complex Concentrate (PCC) 3- factor (factor II, IX, X) 4-factor (factors II, VII, IX, X) Activated 4-factor (factors II, VIIa, IX, X) Coagulation
Prothrombin Complex Concentrate- Concentrated Factors Prothrombin Complex Concentrate (PCC) 3- factor (factor II, IX, X) 4-factor (factors II, VII, IX, X) Activated 4-factor (factors II, VIIa, IX, X) Coagulation
Dr. MUBARAK ABDELRAHMAN MD PEDIATRICS AND CHILD HEALTH Assistant Professor FACULTY OF MEDICINE -JAZAN
 Dr. MUBARAK ABDELRAHMAN MD PEDIATRICS AND CHILD HEALTH Assistant Professor FACULTY OF MEDICINE -JAZAN The student should be able:» To identify the mechanism of homeostasis and the role of vessels, platelets
Dr. MUBARAK ABDELRAHMAN MD PEDIATRICS AND CHILD HEALTH Assistant Professor FACULTY OF MEDICINE -JAZAN The student should be able:» To identify the mechanism of homeostasis and the role of vessels, platelets
of AUB DISCLOSURES 10/29/2018
 of AUB DR. DEBRA GIERUT MD DEPARTMENT OF OBSTETRICS AND GYNECOLOGY KAISER PERMANENTE, ORANGE COUNTY DISCLOSURES I have no financial disclosures Lisa Samerdyke, the Director of National Accounts for Hologic
of AUB DR. DEBRA GIERUT MD DEPARTMENT OF OBSTETRICS AND GYNECOLOGY KAISER PERMANENTE, ORANGE COUNTY DISCLOSURES I have no financial disclosures Lisa Samerdyke, the Director of National Accounts for Hologic
Platelet Disorders. By : Saja Al-Oran
 Platelet Disorders By : Saja Al-Oran Introduction The platelet arise from the fragmentation of the cytoplasm of megakaryocyte in the bone marrow. circulate in the blood as disc-shaped anucleate particles
Platelet Disorders By : Saja Al-Oran Introduction The platelet arise from the fragmentation of the cytoplasm of megakaryocyte in the bone marrow. circulate in the blood as disc-shaped anucleate particles
Vani Lingam Consultant Obstetrician and Gynaecologist Queens Hospital Burton NHS Trust 13 th June
 Vani Lingam Consultant Obstetrician and Gynaecologist Queens Hospital Burton NHS Trust 13 th June Definition of normal menstruation Cycle Length Cycle predictability Duration Volume of blood flow Cycle
Vani Lingam Consultant Obstetrician and Gynaecologist Queens Hospital Burton NHS Trust 13 th June Definition of normal menstruation Cycle Length Cycle predictability Duration Volume of blood flow Cycle
GUIDELINES FOR MANAGEMENT OF BLEEDING AND EXCESSIVE ANTICOAGULATION WITH ORAL ANTICOAGULANTS
 GUIDELINES FOR MANAGEMENT OF BLEEDING AND EXCESSIVE ANTICOAGULATION WITH ORAL ANTICOAGULANTS This guideline covers the management of patients being treated with Vitamin K antagonists (VKA): Warfarin Acenocoumarol
GUIDELINES FOR MANAGEMENT OF BLEEDING AND EXCESSIVE ANTICOAGULATION WITH ORAL ANTICOAGULANTS This guideline covers the management of patients being treated with Vitamin K antagonists (VKA): Warfarin Acenocoumarol
Abnormal Uterine Bleeding Case Studies
 Case Study 1 Abnormal Uterine Bleeding Case Studies Abigail, a 24 year old female, presents to your office complaining that her menstrual cycles have become a problem. They are now lasting 6 7 days instead
Case Study 1 Abnormal Uterine Bleeding Case Studies Abigail, a 24 year old female, presents to your office complaining that her menstrual cycles have become a problem. They are now lasting 6 7 days instead
John Davidson Consultant in Intensive Care Medicine Freeman Hospital, Newcastle upon Tyne
 John Davidson Consultant in Intensive Care Medicine Freeman Hospital, Newcastle upon Tyne Overview of coagulation Testing coagulation Coagulopathy in ICU Incidence Causes Evaluation Management Coagulation
John Davidson Consultant in Intensive Care Medicine Freeman Hospital, Newcastle upon Tyne Overview of coagulation Testing coagulation Coagulopathy in ICU Incidence Causes Evaluation Management Coagulation
Management of Abnormal Uterine Bleeding. Julie Strickland MD, MPH University of Missouri Kansas City Department of Obstetrics and Gynecology
 Management of Abnormal Uterine Bleeding Julie Strickland MD, MPH University of Missouri Kansas City Department of Obstetrics and Gynecology AUB Abnormal uterine bleeding (AUB): fairly broad term referring
Management of Abnormal Uterine Bleeding Julie Strickland MD, MPH University of Missouri Kansas City Department of Obstetrics and Gynecology AUB Abnormal uterine bleeding (AUB): fairly broad term referring
Thrombosis and Women s Health Risk factors, contraceptive pill, HRT and your doctor
 Thrombosis and Women s Health Risk factors, contraceptive pill, HRT and your doctor Dr Matthew Fay GP Principal The Willows Medical Practice- Queensbury GPwSI and Co-Founder Westcliffe Cardiology Service
Thrombosis and Women s Health Risk factors, contraceptive pill, HRT and your doctor Dr Matthew Fay GP Principal The Willows Medical Practice- Queensbury GPwSI and Co-Founder Westcliffe Cardiology Service
Introduction to von Willebrand Disease Mary Lesh RN, MS, CPNP
 Introduction to von Willebrand Disease Mary Lesh RN, MS, CPNP OVERVIEW Von Willebrand Disease (VWD) is the most common hereditary bleeding disorder in humans, with an estimated prevalence ranging upward
Introduction to von Willebrand Disease Mary Lesh RN, MS, CPNP OVERVIEW Von Willebrand Disease (VWD) is the most common hereditary bleeding disorder in humans, with an estimated prevalence ranging upward
Debate: New Generation Anti-Coagulation Agents are a Better Choice than Warfarin in the Management of AF
 Debate: New Generation Anti-Coagulation Agents are a Better Choice than Warfarin in the Management of AF Bradley P. Knight, MD Director of Cardiac Electrophysiology Bluhm Cardiovascular Institute Northwestern
Debate: New Generation Anti-Coagulation Agents are a Better Choice than Warfarin in the Management of AF Bradley P. Knight, MD Director of Cardiac Electrophysiology Bluhm Cardiovascular Institute Northwestern
What s New in Adolescent Contraception?
 What s New in Adolescent Contraception? Abby Furukawa, MD Legacy Medical Group Portland Obstetrics and Gynecology April 29, 2017 Objectives Provide an update on contraception options for the adolescent
What s New in Adolescent Contraception? Abby Furukawa, MD Legacy Medical Group Portland Obstetrics and Gynecology April 29, 2017 Objectives Provide an update on contraception options for the adolescent
BLEEDING DISORDERS Simple complement:
 BLEEDING DISORDERS Simple complement: 1. Select the statement that describe the thrombocytopenia definition: A. Marked decrease of the Von Willebrandt factor B. Absence of antihemophilic factor A C. Disorder
BLEEDING DISORDERS Simple complement: 1. Select the statement that describe the thrombocytopenia definition: A. Marked decrease of the Von Willebrandt factor B. Absence of antihemophilic factor A C. Disorder
UKMEC SUMMARY TABLE HORMONAL AND INTRAUTERINE CONTRACEPTION
 SUMMARY TABLE SUMMARY TABLE HORMONAL AND INTRAUTERINE CONTRACEPTION Cu-IUD = Copper-bearing intrauterine device; LNG-IUS = Levonorgestrel-releasing intrauterine system; IMP = Progestogen-only implant;
SUMMARY TABLE SUMMARY TABLE HORMONAL AND INTRAUTERINE CONTRACEPTION Cu-IUD = Copper-bearing intrauterine device; LNG-IUS = Levonorgestrel-releasing intrauterine system; IMP = Progestogen-only implant;
Bleeding disorders. Hemostatic failure: Inappropriate and excessive bleeding either spontaneous or in response to injury.
 1 Bleeding disorders Objectives: 1. Discuss briefly the physiology of hemostasis. 2. Define the mechanisms of thrombocytopenia and the relative bleeding risk at any given platelet count. 3. Be able to
1 Bleeding disorders Objectives: 1. Discuss briefly the physiology of hemostasis. 2. Define the mechanisms of thrombocytopenia and the relative bleeding risk at any given platelet count. 3. Be able to
 Non-contraceptive Uses of the Levonorgestrel Intrauterine Device Elena Gates, MD http://www.mirena-us.com/pvs1/pri/whatisframe.html Progestin levels with LNG- IUS Lower plasma levels Mirena 150-200 pg/ml
Non-contraceptive Uses of the Levonorgestrel Intrauterine Device Elena Gates, MD http://www.mirena-us.com/pvs1/pri/whatisframe.html Progestin levels with LNG- IUS Lower plasma levels Mirena 150-200 pg/ml
Medical Management of Fibroids Esmya. Dr Paula Briggs Consultant in Sexual and Reproductive Health
 Medical Management of Fibroids Esmya Dr Paula Briggs Consultant in Sexual and Reproductive Health Treatment options for Uterine Fibroids ESMYA Selective Uterine Artery Embolisation Fibroid ablation (hysteroscopic
Medical Management of Fibroids Esmya Dr Paula Briggs Consultant in Sexual and Reproductive Health Treatment options for Uterine Fibroids ESMYA Selective Uterine Artery Embolisation Fibroid ablation (hysteroscopic
Primary Care Gynaecology Guidelines: HEAVY REGULAR MENSTRUAL BLEEDING
 Primary Care Guidelines: HEAVY REGULAR MENSTRUAL BLEEDING
Primary Care Guidelines: HEAVY REGULAR MENSTRUAL BLEEDING
Dr Mary Birdsall. Fertility Associates Auckland
 Dr Mary Birdsall Fertility Associates Auckland Period Problems Mary Birdsall Medical Director Fertility Associates Auckland Period Problems Basic Physiology No Periods Irregular Periods Heavy Periods
Dr Mary Birdsall Fertility Associates Auckland Period Problems Mary Birdsall Medical Director Fertility Associates Auckland Period Problems Basic Physiology No Periods Irregular Periods Heavy Periods
DOAC and NOAC are terms for a novel class of directly acting oral anticoagulant drugs including Rivaroxaban, Apixaban, Edoxaban, and Dabigatran.
 Guideline for Patients on Direct Oral Anticoagulant Therapy Requiring Urgent Surgery for Hip Fracture Trust Ref:C10/2017 1. Introduction This guideline is for the clinical management of patients on direct
Guideline for Patients on Direct Oral Anticoagulant Therapy Requiring Urgent Surgery for Hip Fracture Trust Ref:C10/2017 1. Introduction This guideline is for the clinical management of patients on direct
GUIDELINE: ASSESSMENT OF BRUISING & BLEEDING IN CHILDREN. All children in whom there is concern regarding bruising / bleeding
 GUIDELINE: ASSESSMENT OF BRUISING & BLEEDING IN CHILDREN Reference: Bruising / Bleeding / NAI Version No: 1 Applicable to All children in whom there is concern regarding bruising / bleeding Classification
GUIDELINE: ASSESSMENT OF BRUISING & BLEEDING IN CHILDREN Reference: Bruising / Bleeding / NAI Version No: 1 Applicable to All children in whom there is concern regarding bruising / bleeding Classification
Guidance for management of bleeding in patients taking the new oral anticoagulant drugs: rivaroxaban, dabigatran or apixaban
 Guidance for management of bleeding in patients taking the new oral anticoagulant drugs: rivaroxaban, dabigatran or apixaban Purpose The aim of this guidance is to outline the management of patients presenting
Guidance for management of bleeding in patients taking the new oral anticoagulant drugs: rivaroxaban, dabigatran or apixaban Purpose The aim of this guidance is to outline the management of patients presenting
Moneli Golara Consultant Obstetrician and Gynaecologist Barnet Hospital Royal Free NHS Trust
 Moneli Golara Consultant Obstetrician and Gynaecologist Barnet Hospital Royal Free NHS Trust Endometriosis one of the most common conditions requiring treatment Growth of endometrial like tissue outside
Moneli Golara Consultant Obstetrician and Gynaecologist Barnet Hospital Royal Free NHS Trust Endometriosis one of the most common conditions requiring treatment Growth of endometrial like tissue outside
Heavy menstrual bleeding: assessment and management
 Heavy menstrual bleeding: assessment and management NICE guideline Draft for consultation, August 0 This guideline covers assessing and treating heavy menstrual bleeding. It aims to help healthcare professionals
Heavy menstrual bleeding: assessment and management NICE guideline Draft for consultation, August 0 This guideline covers assessing and treating heavy menstrual bleeding. It aims to help healthcare professionals
Emergency Management of Patients on Direct Oral Anticoagulants (DOACs)
") Emergency Management of Patients on Direct Oral Anticoagulants (DOACs) Dr Tina Biss Consultant Haematologist Newcastle upon Tyne Hospitals NHS Foundation Trust NE RTC Annual Education Symposium 11 th October
Emergency Management of Patients on Direct Oral Anticoagulants (DOACs) Dr Tina Biss Consultant Haematologist Newcastle upon Tyne Hospitals NHS Foundation Trust NE RTC Annual Education Symposium 11 th October
Menopause management NICE Implementation
 Menopause management NICE Implementation Dr Paula Briggs Consultant in Sexual & Reproductive Health Southport and Ormskirk NHS Hospital Trust Why a NICE guideline (NG 23) Media reports about HRT have not
Menopause management NICE Implementation Dr Paula Briggs Consultant in Sexual & Reproductive Health Southport and Ormskirk NHS Hospital Trust Why a NICE guideline (NG 23) Media reports about HRT have not
Mr Doug Barclay Gynaecologist Ascot Central Women s Clinic Auckland. Mr Simon Edmonds Gynaecologist Middlemore Hospital Auckland
 Mr Doug Barclay Gynaecologist Ascot Central Women s Clinic Auckland Mr Simon Edmonds Gynaecologist Middlemore Hospital Auckland 16:30-17:25 WS #69: Practical Mirena Insertion and Pipelle Endometrial Sampling
Mr Doug Barclay Gynaecologist Ascot Central Women s Clinic Auckland Mr Simon Edmonds Gynaecologist Middlemore Hospital Auckland 16:30-17:25 WS #69: Practical Mirena Insertion and Pipelle Endometrial Sampling
Haemostasis, thrombosis risk and hormone replacement therapy
 Haemostasis, thrombosis risk and hormone replacement therapy Serge Motte Brussels 13.05.17 - MY TALK TODAY The coagulation cascade and its regulation Effects of hormone replacement therapy on haemostasis
Haemostasis, thrombosis risk and hormone replacement therapy Serge Motte Brussels 13.05.17 - MY TALK TODAY The coagulation cascade and its regulation Effects of hormone replacement therapy on haemostasis
von Willebrand Disease
 von Willebrand Disease Jeremy Robertson Paediatric Haematologist Royal Children s s Hospital & Pathology Queensland Foglo,, April 1924: the journey begins Oskar and Augusta sail to Helsinki... ...to o
von Willebrand Disease Jeremy Robertson Paediatric Haematologist Royal Children s s Hospital & Pathology Queensland Foglo,, April 1924: the journey begins Oskar and Augusta sail to Helsinki... ...to o
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE. Health and social care directorate. Quality standards and indicators.
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Health and social care directorate Quality standards and indicators Briefing paper Quality standard topic: Heavy menstrual bleeding Output: Prioritised
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Health and social care directorate Quality standards and indicators Briefing paper Quality standard topic: Heavy menstrual bleeding Output: Prioritised
Dysmenorrhoea Gynaecology د.شيماءعبداالميرالجميلي. Aetiology of secondary dysmenorrhea
 30-11-2014 Gynaecology Dysmenorrhoea د.شيماءعبداالميرالجميلي Dysmenorrhoea is defined as painful menstruation. It is experienced by 45 95 per cent of women of reproductive age.primary Spasmodic Dysmenorrhea
30-11-2014 Gynaecology Dysmenorrhoea د.شيماءعبداالميرالجميلي Dysmenorrhoea is defined as painful menstruation. It is experienced by 45 95 per cent of women of reproductive age.primary Spasmodic Dysmenorrhea
THROMBOTIC DISORDERS: The Final Frontier
 THROMBOTIC DISORDERS: The Final Frontier Jeffrey I. Weitz, MD, FRCP(C), FACP Professor of Medicine and Biochemistry McMaster University Canada Research Chair in Thrombosis Heart & Stroke Foundation/ J.F.
THROMBOTIC DISORDERS: The Final Frontier Jeffrey I. Weitz, MD, FRCP(C), FACP Professor of Medicine and Biochemistry McMaster University Canada Research Chair in Thrombosis Heart & Stroke Foundation/ J.F.
Coagulation Disorders. Dr. Muhammad Shamim Assistant Professor, BMU
 Coagulation Disorders Dr. Muhammad Shamim Assistant Professor, BMU 1 Introduction Local Vs. General Hematoma & Joint bleed Coagulation Skin/Mucosal Petechiae & Purpura PLT wound / surgical bleeding Immediate
Coagulation Disorders Dr. Muhammad Shamim Assistant Professor, BMU 1 Introduction Local Vs. General Hematoma & Joint bleed Coagulation Skin/Mucosal Petechiae & Purpura PLT wound / surgical bleeding Immediate
World Health Organization Medical Eligibility for Contraceptive Use. Connie Kraus, PharmD, BCACP Professor (CHS) Director Office of Global Health
 Director Office of Global Health") World Health Organization Medical Eligibility for Contraceptive Use Connie Kraus, PharmD, BCACP Professor (CHS) Director Office of Global Health Objectives After this session, learners should be able to:
World Health Organization Medical Eligibility for Contraceptive Use Connie Kraus, PharmD, BCACP Professor (CHS) Director Office of Global Health Objectives After this session, learners should be able to:
Meiqiu Lu and Xin Yang *
 Lu and Yang BMC Women's Health (2018) 18:45 https://doi.org/10.1186/s12905-018-0533-0 CASE REPORT Open Access Levonorgestrel-releasing intrauterine system for treatment of heavy menstrual bleeding in adolescents
Lu and Yang BMC Women's Health (2018) 18:45 https://doi.org/10.1186/s12905-018-0533-0 CASE REPORT Open Access Levonorgestrel-releasing intrauterine system for treatment of heavy menstrual bleeding in adolescents
Clinical issues which drug for which patient
 Anticoagulants - a matter of heart! Towards a bright future? Clinical issues which drug for which patient Sabine Eichinger Dept. of Medicine I Medical University of Vienna/Austria Conflicts of interest
Anticoagulants - a matter of heart! Towards a bright future? Clinical issues which drug for which patient Sabine Eichinger Dept. of Medicine I Medical University of Vienna/Austria Conflicts of interest
Sysmex Educational Enhancement and Development No
 SEED Coagulation Sysmex Educational Enhancement and Development No 2 2016 An approach to the bleeding patient The purpose of this newsletter is to provide an overview of the approach to the bleeding patient
SEED Coagulation Sysmex Educational Enhancement and Development No 2 2016 An approach to the bleeding patient The purpose of this newsletter is to provide an overview of the approach to the bleeding patient
3/19/2012. What is the indication for anticoagulation? Has the patient previously been on warfarin? If so, what % of the time was the INR therapeutic?
 Abigail E. Miller, PharmD, BCPS Clinical Specialist, Cardiology University of North Carolina Hospitals I have no personal financial relationships with the manufacturers of the products to disclose. Boehringer
Abigail E. Miller, PharmD, BCPS Clinical Specialist, Cardiology University of North Carolina Hospitals I have no personal financial relationships with the manufacturers of the products to disclose. Boehringer
Mabel Labrada, MD Miami VA Medical Center
 Mabel Labrada, MD Miami VA Medical Center *1-Treatment for acute DVT with underlying malignancy is for 3 months. *2-Treatment of provoked acute proximal DVT can be stopped after 3months of treatment and
Mabel Labrada, MD Miami VA Medical Center *1-Treatment for acute DVT with underlying malignancy is for 3 months. *2-Treatment of provoked acute proximal DVT can be stopped after 3months of treatment and
Modern Management of Fibroids
 Modern Management of Fibroids Mr Narendra Pisal The Portland Hospital Fibroids Very common 20-40% of all women Up to 80% of black women by 50y Most fibroids are asymptomatic 50% will have significant symptoms
Modern Management of Fibroids Mr Narendra Pisal The Portland Hospital Fibroids Very common 20-40% of all women Up to 80% of black women by 50y Most fibroids are asymptomatic 50% will have significant symptoms
MANAGEMENT OF COAGULOPATHY AFTER TRAUMA OR MAJOR SURGERY
 MANAGEMENT OF COAGULOPATHY AFTER TRAUMA OR MAJOR SURGERY 19th ANNUAL CONTROVERSIES AND PROBLEMS IN SURGERY Thabo Mothabeng General Surgery: 1 Military Hospital HH Stone et al. Ann Surg. May 1983; 197(5):
MANAGEMENT OF COAGULOPATHY AFTER TRAUMA OR MAJOR SURGERY 19th ANNUAL CONTROVERSIES AND PROBLEMS IN SURGERY Thabo Mothabeng General Surgery: 1 Military Hospital HH Stone et al. Ann Surg. May 1983; 197(5):
COLLEGE OF OBSTETRICIANS AND GYNAECOLOGISTS, SINGAPORE 2006
 COLLEGE OF OBSTETRICIANS AND GYNAECOLOGISTS, SINGAPORE 2006 CONSENSUS STATEMENT ON THE MANAGEMENT AND EVALUATION OF MENORRHAGIA (INCLUDING MANAGEMENT OF FIBROIDS) Introduction Menorrhagia is defined as
COLLEGE OF OBSTETRICIANS AND GYNAECOLOGISTS, SINGAPORE 2006 CONSENSUS STATEMENT ON THE MANAGEMENT AND EVALUATION OF MENORRHAGIA (INCLUDING MANAGEMENT OF FIBROIDS) Introduction Menorrhagia is defined as
Contraception: Common Problems Faced in Office Practice. Jane S. Sillman, MD Brigham and Women s Hospital
 Contraception: Common Problems Faced in Office Practice Jane S. Sillman, MD Brigham and Women s Hospital Disclosures I have no conflicts of interest Contraception: Common Problems How to discuss contraception
Contraception: Common Problems Faced in Office Practice Jane S. Sillman, MD Brigham and Women s Hospital Disclosures I have no conflicts of interest Contraception: Common Problems How to discuss contraception
Gynecologic Decision Making Based on Sonographic Findings
 Gynecologic Decision Making Based on Sonographic Findings Mindy Goldman, MD Department of Obstetrics & Gynecology & Vickie A. Feldstein, MD Department of Radiology University of California, San Francisco
Gynecologic Decision Making Based on Sonographic Findings Mindy Goldman, MD Department of Obstetrics & Gynecology & Vickie A. Feldstein, MD Department of Radiology University of California, San Francisco
HEME 10 Bleeding Disorders
 HEME 10 Bleeding Disorders When injury occurs, three mechanisms occur Blood vessels Primary hemostasis Secondary hemostasis Diseases of the blood vessels Platelet disorders Thrombocytopenia Functional
HEME 10 Bleeding Disorders When injury occurs, three mechanisms occur Blood vessels Primary hemostasis Secondary hemostasis Diseases of the blood vessels Platelet disorders Thrombocytopenia Functional
Consensus Statement for Management of Anticoagulants and Antiplatelet drugs in Patients with Hip Fracture
 Consensus Statement for Management of Anticoagulants and Antiplatelet drugs in Patients with Hip Fracture Patients with hip fractures should be operated on within 36 hours of presentation wherever possible.
Consensus Statement for Management of Anticoagulants and Antiplatelet drugs in Patients with Hip Fracture Patients with hip fractures should be operated on within 36 hours of presentation wherever possible.
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Abdominal myomectomy in leiomyoma management, 77 Abnormal uterine bleeding (AUB) described, 103 105 normal menstrual bleeding vs., 104
Index Note: Page numbers of article titles are in boldface type. A Abdominal myomectomy in leiomyoma management, 77 Abnormal uterine bleeding (AUB) described, 103 105 normal menstrual bleeding vs., 104
Menorrhagia Update. Simon Edmonds Middlemore Hospital Ascot Central Women s Clinic Auckland
 Menorrhagia Update Simon Edmonds Middlemore Hospital Ascot Central Women s Clinic Auckland What is it? Subjective Excessive blood loss at time of menstruation flooding heavy clots Objective > 80mls volume
Menorrhagia Update Simon Edmonds Middlemore Hospital Ascot Central Women s Clinic Auckland What is it? Subjective Excessive blood loss at time of menstruation flooding heavy clots Objective > 80mls volume
Contraception and gynecological pathologies
 1 Contraception and gynecological pathologies 18 years old, 2 CMI normal First menstruation at 14 years old Irregular (every 2/3 months), painful + She does not need contraception She is worried about
1 Contraception and gynecological pathologies 18 years old, 2 CMI normal First menstruation at 14 years old Irregular (every 2/3 months), painful + She does not need contraception She is worried about
What are InherIted platelet FunCtIon disorders?
 What are InherIted platelet FunCtIon disorders? Published by the World Federation of Hemophilia (WFH) World Federation of Hemophilia, 2010 This publication was developed by the WFH and reviewed by Dr.
What are InherIted platelet FunCtIon disorders? Published by the World Federation of Hemophilia (WFH) World Federation of Hemophilia, 2010 This publication was developed by the WFH and reviewed by Dr.
1. Ng M et a l. Global, regional, and national prevalence of overweight and obesity in children and adults during : A systematic analysis
 1 2 3 1. Ng M et a l. Global, regional, and national prevalence of overweight and obesity in children and adults during 1980 2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet
1 2 3 1. Ng M et a l. Global, regional, and national prevalence of overweight and obesity in children and adults during 1980 2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet
General approach to the investigation of haemostasis. Jan Gert Nel Dept. of Haematology University of Pretoria 2013
 General approach to the investigation of haemostasis Jan Gert Nel Dept. of Haematology University of Pretoria 2013 Clinical reasons to investigate haemostasis Investigating a clinically suspected bleeding
General approach to the investigation of haemostasis Jan Gert Nel Dept. of Haematology University of Pretoria 2013 Clinical reasons to investigate haemostasis Investigating a clinically suspected bleeding
Dr. Rai Muhammad Asghar Associate Professor Head of Pediatric Department Rawalpindi Medical College
 Dr. Rai Muhammad Asghar Associate Professor Head of Pediatric Department Rawalpindi Medical College AN APPROACH TO BLEEDING DISORDERS NORMAL HEMOSTASIS After injury, 3 processes halt bleeding Vasoconstriction
Dr. Rai Muhammad Asghar Associate Professor Head of Pediatric Department Rawalpindi Medical College AN APPROACH TO BLEEDING DISORDERS NORMAL HEMOSTASIS After injury, 3 processes halt bleeding Vasoconstriction
New Oral Anticoagulant Drugs in the Prevention of DVT
 New Oral Anticoagulant Drugs in the Prevention of DVT Targets for Anticoagulants ORAL DIRECT VKAs inhibit the hepatic synthesis of several coagulation factors Rivaroxaban Apixaban Edoxaban Betrixaban X
New Oral Anticoagulant Drugs in the Prevention of DVT Targets for Anticoagulants ORAL DIRECT VKAs inhibit the hepatic synthesis of several coagulation factors Rivaroxaban Apixaban Edoxaban Betrixaban X
Abnormal Uterine Bleeding. Richard Dover Specialist gynaecologist
 Abnormal Uterine Bleeding Richard Dover Specialist gynaecologist A pragmatic guide. Wide topic range What s not coming up Precocious puberty Menorrhagia well maybe just a little Topics Adolescents IMB
Abnormal Uterine Bleeding Richard Dover Specialist gynaecologist A pragmatic guide. Wide topic range What s not coming up Precocious puberty Menorrhagia well maybe just a little Topics Adolescents IMB