Delirium and cognitive impairment in the perioperative
|
|
|
- Easter Ball
- 5 years ago
- Views:
Transcription
1 Delirium and cognitive impairment in the perioperative period Richard Sztramko Assistant Professor, McMaster University Divisions of Geriatrics and General Internal Medicine
2 Disclosures Chief Medical Officer - Reliq Health Technologies Director - Virtual Ward Medicine Corp Director - Apollo Healthcare Technologies
3 Objectives Demonstrate an understanding of the morbidity and mortality associated with acute delirium Describe key bedside tests to diagnose delirium Integrate evidence-based and evidence-informed management principles of peri-operative delirium into clinical practice Describe principles for dealing with cognitively impaired individuals in the peri-operative period
4 What is delirium? Acute confusional state characterized by: Fluctuation Inattention Depressed level of consciousness Disorganized thinking Perceptual disturbances - hallucinations/illusions Emotional dysregulation - anxiety/paranoia/depression/apathy
5 What is delirium? Not better explained by pre-existing cognitive impairment - dementa/abi etc Usually explained by a general medical condition, medication, status post-op Delirium = ATN of the brain - weak brain/weak insult - strong brain/strong insult
6 Pathophysiology Inflammation Stress and related hormonal imbalances Neurotransmitter abnormalities
7 Clinical Causes DIMSUS Drugs - OTC, intoxication, withdrawal Infection - systemic Metabolic - liver, kidneys, 02/c02, lytes, tsh, glucose, acidosis Structural - blood, tumor, pus, vascular insults***, inflammation, Urinary Retention Fecal Impaction/Constipation Pain, sleep debt, change in environment, restraints
8 Risk Factors Age Dementia Previous delirium Medical comorbidities Polypharmacy Frailty


9 Incidence of delirium
10 Morbidity/Mortality $164 billion in health care costs in US annually Increased risk of: Falls Functional Decline Dementia (30% of delirium cases display cog. 6 months) Prolonged hospital stay Institutionalization Estimated 30-40% of delirium cases are preventable
11 Delirium Prediction Poor cognitive performance before surgery Low hemoglobin levels Low albumin levels Cerebrovascular disease Increased CRP Prior delirium No one validated score, but many multi-variate regressions studies to identify RF s Hard to operationalize aside from picking out RFs at baseline
12 Diagnosis at the bedside Inattention: Not following commands/conversation Serial 7 s/world backwards/months/days backwards Digit Span - normal 6 forward, 4 backwards Somnolent/tired/withdrawn A person should be able to have a reasonable conversation with you - even if they are tired/in pain, if they can t there s something wrong
13 Diagnosis at the bedside Inattention: Mini-Mental State Examination MoCA Not created for the purpose of screening for delirium If a sudden drop in performance, than it supports a diagnosis Ensure that if the patient is delirious, a score isn t permanently reflected in their medical record
14 Diagnosis at the bedside Confusion Assessment Method (CAM) 1.Acute onset and Fluctuant 2.Inattention 3.Altered level of consciousness 4.Disorganized thought 1 AND 2 plus 3 OR 4 Long form is very onerous - 8 pages, 3D Cam is more pragmatic

15 Diagnosis at the bedside ity 95%, Specificity 95% - works in demented/non-demented pat

16 Diagnosis at the bedside Marcantonio et al Annal Int Med.
17 Prevention Modifiable Variables for Intervention: Orientation protocols Cognitive stimulation Facilitating sleep Early mobilization/minimizing restraints Visual/hearing aids Monitoring for offending medications Managing pain Bowel and bladder management
18 Prevention Prototypic - Hospital Elder Life Program - Delirium Prevention Trial - Inouye et al. NEJM 2004 Hydration/Nutrition Sleep Cognitive stimulation Mobility Vision/Hearing
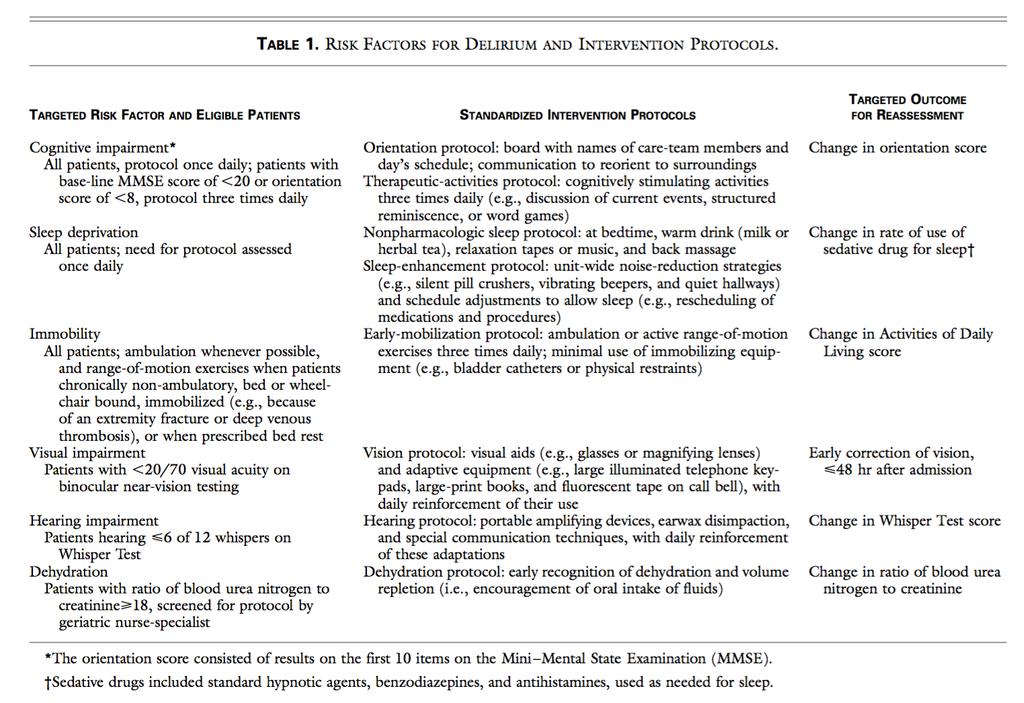

19 Prevention
20 Figures Prevention
21 Prevention Incident Delirium
22 Prevention Incident Falls
 Rockwood")
23 Prevention Pre-printed orders (PPOs) Rockwood
 Rockwood")
24 Prevention Pre-printed orders (PPOs) Rockwood
25 Prevention Preoperative Geriatrics Consultation 10 specific modules of recommendations No more than 5 recommendations at one time No more than 3 recommendations subsequently Focused on many of the non-pharmacological strategies already discussed
26 Prevention RR 0.64 Delirium RR 0.40 Severe Delirium
27 Non-pharmacologic Prevention Non-pharmacologic strategies are extremely effective (pooled 0.45 OR, or RR 0.60 in a very high quality RCT) Standardized protocols are the common theme, not necessarily the practitioners - but experience helps
28 Pharmacologic Prevention
29 Prevention Antipsychotics Theory to prevent or quiet down altered neurotransmission before it gets started

30 Prevention
31 Prevention

32 Prevention
33 Antipsychotics Prevention (OFF LABEL) No guidelines to suggest prophylaxis with antipsychotics No predictive model practically used to identify high risk people and treat accordingly Fairly robust signal to noise ratio, but generally reserved for treatment, not for prevention Perhaps in the future
34 Prevention Antipsychotics No impact on length of stay No impact on severity of delirium No differences in adverse events One study suggests risk of 18% is the risk level below which treatment may not be beneficial
35 Prevention
36 Prevention (OFF LABEL) Melatonin Mixed evidence Much lower rate of side effects/well tolerated No guidelines to suggest its use at this time Explaining risks/benefits to patients and let them decide
37 Prevention Cholinesterase Inhibitors Gabapentin
38 Treatment Step 1 - find and treat an underlying cause or causes (DIMSUS) Step 2 - regulate sleep Step 3 - regulate agitation Step 4 - modify all other variables outlined in non-pharmacologic prevention
39 Treatment Step 1 - find and treat an underlying cause or causes (DIMSUS) - you all know what do do Don t forget the PVR or AXR!
40 Treatment (OFF LABEL) Step 2 - sleep regulation Mild - Melatonin 3 mg po qhs - regular, increased to 6 mg Moderate - night time quetiapine 12.5 mg - 25 mg - regular, loxapine 5 mg-10 mg SC ohs Severe - sundowning and 2100 doses of quetipine and loxapine
41 Treatment (OFF LABEL) Step 3 - regulate agitation Haldol 0.5 mg IM/IV q30 minutes If more than 3 mg is required, consider alternative diagnosis and call psych Risperidone mg po bid, titrate up to 0.5 mg po bid
42 Treatment Step 4 - modify all other factors HELP to see if available, volunteers or pastoral care if no HELP program dc restraints, foley catheters if possible, sometimes it s not Up to chair tid for meals if non-mobile or decreased exercise tolerance Orthostatic vitals Regular laxatives OT - glasses/hearing aids/gait aids at bedside PT - involvement for mobility Counsel family on reorientation strategies and value of having them at the bedside
43 Cognitively Impaired Highest risk for delirium Call family/caregivers and ask about their baseline cognition/function Place a high priority on non-pharmacologic strategies - family to take shifts, call family in the middle of the night Discuss strategies with nurses
44 Cognitively Impaired Parkinson s Disease 38% rate of neuroleptic sensitivity Dementia with Lewy Bodies 50% rate of neuroleptic sensitivity Avoid Haldol, Risperidone, Loxapine - call a Geriatric Psychiatrist or Geriatrician for these patients as reactions can be permanent
45 Thank you! Questions and Discussion
Delirium in the Elderly
 Delirium in the Elderly ELITE 2017 Liza Genao, MD Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity Very much under-recognized
Delirium in the Elderly ELITE 2017 Liza Genao, MD Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity Very much under-recognized
Delirium in the Elderly
 Delirium in the Elderly ELITE 2015 Mamata Yanamadala M.B.B.S, MS Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity
Delirium in the Elderly ELITE 2015 Mamata Yanamadala M.B.B.S, MS Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity
Delirium. Dr. Lesley Wiesenfeld. Deputy Psychiatrist in Chief, Mount Sinai Hospital. Dr. Carole Cohen
 Delirium Dr. Lesley Wiesenfeld Deputy Psychiatrist in Chief, Mount Sinai Hospital Dr. Carole Cohen Department of Psychiatry, University of Toronto and Sunnybrook Health Sciences Centre Case Study Mrs B
Delirium Dr. Lesley Wiesenfeld Deputy Psychiatrist in Chief, Mount Sinai Hospital Dr. Carole Cohen Department of Psychiatry, University of Toronto and Sunnybrook Health Sciences Centre Case Study Mrs B
Update - Delirium in Elders
 Update - Delirium in Elders Impact Recognition Prevention, and Management Michael J. Lichtenstein, MD F. Carter Pannill, Jr. Professor of Medicine Chief, Division of Geriatrics, Gerontology and Palliative
Update - Delirium in Elders Impact Recognition Prevention, and Management Michael J. Lichtenstein, MD F. Carter Pannill, Jr. Professor of Medicine Chief, Division of Geriatrics, Gerontology and Palliative
Delirium. Dr. John Puxty
 Delirium Dr. John Puxty Learning Objectives By the end of the workshop participants will be able to: Appreciate the main diagnostic criteria for delirium. Describe common risk factors, causes and main
Delirium Dr. John Puxty Learning Objectives By the end of the workshop participants will be able to: Appreciate the main diagnostic criteria for delirium. Describe common risk factors, causes and main
Delirium in Hospital Care
 Delirium in Hospital Care Dr John Puxty 1 Learning Objectives By the end of the workshop participants will be able to: Appreciate the main diagnostic criteria for delirium. Describe common risk factors,
Delirium in Hospital Care Dr John Puxty 1 Learning Objectives By the end of the workshop participants will be able to: Appreciate the main diagnostic criteria for delirium. Describe common risk factors,
DELIRIUM. Sabitha Rajan, MD, MSc, FHM Scott &White Healthcare Texas A&M Health Science Center School of Medicine
 DELIRIUM Sabitha Rajan, MD, MSc, FHM Scott &White Healthcare Texas A&M Health Science Center School of Medicine Disclosure Milliman Care Guidelines - Editor Objectives Define delirium Epidemiology Diagnose
DELIRIUM Sabitha Rajan, MD, MSc, FHM Scott &White Healthcare Texas A&M Health Science Center School of Medicine Disclosure Milliman Care Guidelines - Editor Objectives Define delirium Epidemiology Diagnose
Delirium in Older Persons: An Investigative Journey
 Delirium in Older Persons: An Investigative Journey Sharon K. Inouye, M.D., M.P.H. Professor of Medicine Beth Israel Deaconess Medical Center Harvard Medical School Milton and Shirley F. Levy Family Chair
Delirium in Older Persons: An Investigative Journey Sharon K. Inouye, M.D., M.P.H. Professor of Medicine Beth Israel Deaconess Medical Center Harvard Medical School Milton and Shirley F. Levy Family Chair
Delirium in the ICU: Prevention and Treatment. Delirium Defined Officially. Delirium: Really Defined. S. Andrew Josephson, MD
 Delirium in the ICU: Prevention and Treatment S. Andrew Josephson, MD Director, Neurohospitalist Service Medical Director, Inpatient Neurology June 2, 2011 Delirium Defined Officially (DSM-IV-TR) criteria
Delirium in the ICU: Prevention and Treatment S. Andrew Josephson, MD Director, Neurohospitalist Service Medical Director, Inpatient Neurology June 2, 2011 Delirium Defined Officially (DSM-IV-TR) criteria
Do you know. Assessment of Delirium. What is Delirium? Which syndrome occurs more commonly in elderly populations? a. Delirium b.
 Assessment of Delirium Marianne McCarthy, PhD, GNP, PMHNP Arizona State University College of Nursing and Health Innovation What is Delirium? Delirium is a common clinical syndrome characterized by: Inattention
Assessment of Delirium Marianne McCarthy, PhD, GNP, PMHNP Arizona State University College of Nursing and Health Innovation What is Delirium? Delirium is a common clinical syndrome characterized by: Inattention
Perioperative Care of Older Adults
 Perioperative Care of Older Adults SARAH A. WINGFIELD, MD AND THOMAS O. DALTON, MD UNIVERSITY OF TEXAS SOUTHWESTERN MEDICAL CENTER DIVISION OF GERIATRIC MEDICINE We have no disclosures. Objectives -Recognize
Perioperative Care of Older Adults SARAH A. WINGFIELD, MD AND THOMAS O. DALTON, MD UNIVERSITY OF TEXAS SOUTHWESTERN MEDICAL CENTER DIVISION OF GERIATRIC MEDICINE We have no disclosures. Objectives -Recognize
Perioperative Care of Older Adults
 Perioperative Care of Older Adults SARAH A. WINGFIELD, MD AND THOMAS O. DALTON, MD UNIVERSITY OF TEXAS SOUTHWESTERN MEDICAL CENTER DIVISION OF GERIATRIC MEDICINE We have no disclosures. Objectives -Recognize
Perioperative Care of Older Adults SARAH A. WINGFIELD, MD AND THOMAS O. DALTON, MD UNIVERSITY OF TEXAS SOUTHWESTERN MEDICAL CENTER DIVISION OF GERIATRIC MEDICINE We have no disclosures. Objectives -Recognize
Delirium Pilot Project
 CCU Nurses: Delirium Pilot Project Our unit has been selected to develop and implement a delirium assessment and intervention program. We are beginning Phase 1 with education and assessing for our baseline
CCU Nurses: Delirium Pilot Project Our unit has been selected to develop and implement a delirium assessment and intervention program. We are beginning Phase 1 with education and assessing for our baseline
Delirium assessment and management. Dr Kim Jeffs Northern Health
 Delirium assessment and management Dr Kim Jeffs Northern Health What do you need to know? Epidemiology How big is the problem? Who is at risk? Assessment Tools for diagnosis Prevention Evidence base Management
Delirium assessment and management Dr Kim Jeffs Northern Health What do you need to know? Epidemiology How big is the problem? Who is at risk? Assessment Tools for diagnosis Prevention Evidence base Management
Geriatric Grand Rounds
 Geriatric Grand Rounds Prevalence and Risk Factors of Delirium in Older Patients Admitted to a Community Based Acute Care Hospital Tuesday, October 27, 2009 12:00 noon Dr. Bill Black Auditorium Glenrose
Geriatric Grand Rounds Prevalence and Risk Factors of Delirium in Older Patients Admitted to a Community Based Acute Care Hospital Tuesday, October 27, 2009 12:00 noon Dr. Bill Black Auditorium Glenrose
5 older patients become delirious every minute
 Management of Delirium: Nonpharmacologic and Pharmacologic Approaches Sharon K. Inouye, M.D., M.P.H. Professor of Medicine Beth Israel Deaconess Medical Center Harvard Medical School Milton and Shirley
Management of Delirium: Nonpharmacologic and Pharmacologic Approaches Sharon K. Inouye, M.D., M.P.H. Professor of Medicine Beth Israel Deaconess Medical Center Harvard Medical School Milton and Shirley
The Agitated. Older Patient: old. What To Do? Michelle Gibson, MD, CCFP Presented at Brockville General Hospital Rounds, May 2003
 Focus on CME at Queen s University Focus on CME at Queen s University The Agitated The Older Patient: What To Do? Michelle Gibson, MD, CCFP Presented at Brockville General Hospital Rounds, May 2003 Both
Focus on CME at Queen s University Focus on CME at Queen s University The Agitated The Older Patient: What To Do? Michelle Gibson, MD, CCFP Presented at Brockville General Hospital Rounds, May 2003 Both
Delirium in Older Persons
 Objectives Delirium in Older Persons ELITE 2018 Liza Isabel Genao, MD Division of Geriatrics Describe rate, cost, complications of delirium Effectively diagnose the syndrome Describe multicomponent model
Objectives Delirium in Older Persons ELITE 2018 Liza Isabel Genao, MD Division of Geriatrics Describe rate, cost, complications of delirium Effectively diagnose the syndrome Describe multicomponent model
How to prevent delirium in nursing home. Dr. Sophie ALLEPAERTS Geriatric department CHU-Liège Belgium
 How to prevent delirium in nursing home Dr. Sophie ALLEPAERTS Geriatric department CHU-Liège Belgium 1 CONFLICT OF INTEREST DISCLOSURE I have no potential conflict of interest to report 2 Outline 1. Introduction
How to prevent delirium in nursing home Dr. Sophie ALLEPAERTS Geriatric department CHU-Liège Belgium 1 CONFLICT OF INTEREST DISCLOSURE I have no potential conflict of interest to report 2 Outline 1. Introduction
Summary of Delirium Clinical Practice Guideline Recommendations Post Operative
 Summary of Delirium Clinical Practice Guideline Recommendations Post Operative Intensive Care Unit Clinical Practice Guideline for Postoperative Clinical Practice Guidelines for the Delirium in Older Adults;
Summary of Delirium Clinical Practice Guideline Recommendations Post Operative Intensive Care Unit Clinical Practice Guideline for Postoperative Clinical Practice Guidelines for the Delirium in Older Adults;
Delirium. Approach. Symptom Update Masterclass:
 Symptom Update Masterclass: Delirium Jason Boland Senior Clinical Lecturer and Honorary Consultant in Palliative Medicine Wolfson Centre for Palliative Care Research Hull York Medical School University
Symptom Update Masterclass: Delirium Jason Boland Senior Clinical Lecturer and Honorary Consultant in Palliative Medicine Wolfson Centre for Palliative Care Research Hull York Medical School University
Delirium in the hospitalized patient
 Delirium in the hospitalized patient Jennifer A. Tarin, M.D. Department of Hospital Medicine Geriatric Health Safety Chair Colorado Permanente Medical Group UCLA Reynolds Scholar Delirium Preventing delirium
Delirium in the hospitalized patient Jennifer A. Tarin, M.D. Department of Hospital Medicine Geriatric Health Safety Chair Colorado Permanente Medical Group UCLA Reynolds Scholar Delirium Preventing delirium
9/19/2018. Common Medical Issues and Management in the Geriatric Trauma Patient. Disclosures. Objectives. I have no financial disclosures
 Common Medical Issues and Management in the Geriatric Trauma Patient 2018 UW Medicine EMS & Trauma Conference September 17, 2018 Joe C. Huang, M.D. Clinical Instructor Medical Director, Geriatrics-Palliative
Common Medical Issues and Management in the Geriatric Trauma Patient 2018 UW Medicine EMS & Trauma Conference September 17, 2018 Joe C. Huang, M.D. Clinical Instructor Medical Director, Geriatrics-Palliative
Delirium. Delirium. Delirium Etiology and Pathophysiology. Fall 2018
 Three most common cognitive problems in adults 1. (acute confusion) 2. Dementia 3. Depression These problems often occur together Can you think of common stimuli for each? 1 1 State of temporary but acute
Three most common cognitive problems in adults 1. (acute confusion) 2. Dementia 3. Depression These problems often occur together Can you think of common stimuli for each? 1 1 State of temporary but acute
Delirium. Geriatric Giants Lecture Series Divisions of Geriatric Medicine and Care of the Elderly University of Alberta
 Delirium Geriatric Giants Lecture Series Divisions of Geriatric Medicine and Care of the Elderly University of Alberta Overview A. Delirium - the nature of the beast B. Significance of delirium C. An approach
Delirium Geriatric Giants Lecture Series Divisions of Geriatric Medicine and Care of the Elderly University of Alberta Overview A. Delirium - the nature of the beast B. Significance of delirium C. An approach
Delirium and Dementia. Summary
 Delirium and Dementia Paul Kettl, M.D., M.H.A. Summary DELIRIUM Acute brain failure Identify cause (meds, infection) Treat sx Poor prognostic sign DEMENTIA Chronic brain failure AD most common cause Often
Delirium and Dementia Paul Kettl, M.D., M.H.A. Summary DELIRIUM Acute brain failure Identify cause (meds, infection) Treat sx Poor prognostic sign DEMENTIA Chronic brain failure AD most common cause Often
Delirium Assessment. February 24, Susan Schumacher, MS, APRN-BC
 Delirium Assessment February 24, 2016 Susan Schumacher, MS, APRN-BC Objectives Define delirium Differentiate delirium from dementia Identify predisposing and precipitating factors leading to delirium.
Delirium Assessment February 24, 2016 Susan Schumacher, MS, APRN-BC Objectives Define delirium Differentiate delirium from dementia Identify predisposing and precipitating factors leading to delirium.
Delirium Assessment and management in relation to falls risk in hospital
 Delirium Assessment and management in relation to falls risk in hospital A house call - Mrs JM 95-year-old lady Normally cognitively intact Multiple medical problems, including falls Housebound, mobile
Delirium Assessment and management in relation to falls risk in hospital A house call - Mrs JM 95-year-old lady Normally cognitively intact Multiple medical problems, including falls Housebound, mobile
Delirium Prevention: The State-of-the-Art & Implications to Improve Care in our State
 Delirium Prevention: The State-of-the-Art & Implications to Improve Care in our State Jonny Macias, MD & Michael Malone, MD Aurora Health Care/ University of Wisconsin School of Medicine & Public Health
Delirium Prevention: The State-of-the-Art & Implications to Improve Care in our State Jonny Macias, MD & Michael Malone, MD Aurora Health Care/ University of Wisconsin School of Medicine & Public Health
Renee Flores, MD Division of Geriatrics & Palliative Medicine Department of Internal Medicine
 Renee Flores, MD Division of Geriatrics & Palliative Medicine Department of Internal Medicine Define AMS and delirium Describe how to recognize and diagnose delirium Identify the predisposing or precipitating
Renee Flores, MD Division of Geriatrics & Palliative Medicine Department of Internal Medicine Define AMS and delirium Describe how to recognize and diagnose delirium Identify the predisposing or precipitating
Learning Objectives. Delirium. Delirium. Delirium. Terminal Restlessness 3/28/2016
 Terminal Restlessness Dr. Christopher Churchill St. Cloud VA Health Care System EC&R Service Line Director & Medical Director Hospice & Palliative Care March 31, 2016 Learning Objectives Different Terminology
Terminal Restlessness Dr. Christopher Churchill St. Cloud VA Health Care System EC&R Service Line Director & Medical Director Hospice & Palliative Care March 31, 2016 Learning Objectives Different Terminology
Geriatrics and Cancer Care
 Geriatrics and Cancer Care Roger Wong, BMSc, MD, FRCPC, FACP Postgraduate Dean of Medical Education Clinical Professor, Division of Geriatric Medicine UBC Faculty of Medicine Disclosure No competing interests
Geriatrics and Cancer Care Roger Wong, BMSc, MD, FRCPC, FACP Postgraduate Dean of Medical Education Clinical Professor, Division of Geriatric Medicine UBC Faculty of Medicine Disclosure No competing interests
Why Target Delirium for Surgical Quality Improvement?
 Why Target Delirium for Surgical Quality Improvement? Tom Robinson MD FACS thomas.robinson@ucdenver.edu July 22, 2018 Disclosures Tom Robinson has no disclosures. Who Cares About the Brain? Acute Organ
Why Target Delirium for Surgical Quality Improvement? Tom Robinson MD FACS thomas.robinson@ucdenver.edu July 22, 2018 Disclosures Tom Robinson has no disclosures. Who Cares About the Brain? Acute Organ
Confusion in the acute setting Dr Susan Shenkin
 Confusion in the acute setting Dr Susan Shenkin Susan.Shenkin@ed.ac.uk 4 th International Conference, Society for Acute Medicine, Edinburgh 7-8 October 2010 Summary Confusion is not a diagnosis Main differentials
Confusion in the acute setting Dr Susan Shenkin Susan.Shenkin@ed.ac.uk 4 th International Conference, Society for Acute Medicine, Edinburgh 7-8 October 2010 Summary Confusion is not a diagnosis Main differentials
Guidelines for Management and Prevention of Delirium In Geriatric Trauma Patients
 Guidelines for Management and Prevention of Delirium In Geriatric Trauma Patients Objectives: Provide a guideline for recognizing and managing delirium in geriatric trauma patients. Provide a template
Guidelines for Management and Prevention of Delirium In Geriatric Trauma Patients Objectives: Provide a guideline for recognizing and managing delirium in geriatric trauma patients. Provide a template
Cognitive Status. Read each question below to the patient. Score one point for each correct response.
 Diagnosis of dementia or delirium Cognitive Status Six Item Screener Read to the patient: I have a few questions I would like to ask you. First, I am going to name three objects. After I have said all
Diagnosis of dementia or delirium Cognitive Status Six Item Screener Read to the patient: I have a few questions I would like to ask you. First, I am going to name three objects. After I have said all
Delirium. A Plan to Reduce Use of Restraints. David Wensel DO, FAAHPM Medical Director Midland Care
 Delirium A Plan to Reduce Use of Restraints David Wensel DO, FAAHPM Medical Director Midland Care Objectives Define delirium Describe pathophysiology of delirium Understand most common etiologies Define
Delirium A Plan to Reduce Use of Restraints David Wensel DO, FAAHPM Medical Director Midland Care Objectives Define delirium Describe pathophysiology of delirium Understand most common etiologies Define
A17/B17: Delirium Can Be Deadly: Save Lives With a Standardized Approach to Delirium IHI 25th Annual National Forum, December 10, 2013
 A17/B17: Delirium Can Be Deadly: Save Lives With a Standardized Approach to Delirium IHI 25th Annual National Forum, December 10, 2013 Clay Angel, MD, Hospital Medicine; Chief of Continuum/SNF Kristen
A17/B17: Delirium Can Be Deadly: Save Lives With a Standardized Approach to Delirium IHI 25th Annual National Forum, December 10, 2013 Clay Angel, MD, Hospital Medicine; Chief of Continuum/SNF Kristen
Critical themes in Ageing - Delirium
 Critical themes in Ageing - Delirium Peteris Darzins BMBS PhD FRACP FRCPC Professor of Geriatric Medicine, Monash University, and Executive Clinical Director of Aged Medicine, Eastern Health Penelope Casey
Critical themes in Ageing - Delirium Peteris Darzins BMBS PhD FRACP FRCPC Professor of Geriatric Medicine, Monash University, and Executive Clinical Director of Aged Medicine, Eastern Health Penelope Casey
5 older patients become. What is delirium? (Acute confusional state) Where We ve Been and
 Where We ve Been and") Update on Delirium: Where We ve Been and Where We re Going Sharon K. Inouye, M.D., M.P.H. M PH Professor of Medicine Beth Israel Deaconess Medical Center Harvard Medical School Milton and Shirley F. Levy
Update on Delirium: Where We ve Been and Where We re Going Sharon K. Inouye, M.D., M.P.H. M PH Professor of Medicine Beth Israel Deaconess Medical Center Harvard Medical School Milton and Shirley F. Levy
Delirium. A Geriatric Syndrome. Jonathan McCaleb, MD, CMD, HMDC UNSOM, Assistant Professor of Medicine Geriatrics / Hospice & Palliative Medicine
 Delirium A Geriatric Syndrome Jonathan McCaleb, MD, CMD, HMDC UNSOM, Assistant Professor of Medicine Geriatrics / Hospice & Palliative Medicine Introduction Common Serious Unrecognized: a medical emergency
Delirium A Geriatric Syndrome Jonathan McCaleb, MD, CMD, HMDC UNSOM, Assistant Professor of Medicine Geriatrics / Hospice & Palliative Medicine Introduction Common Serious Unrecognized: a medical emergency
Chapter 01 Introduction
 Chapter 01 Introduction Defining the Elderly There is no universally accepted age cut-off defining elderly. This reflects the fact that chronological age itself is less important than biological events
Chapter 01 Introduction Defining the Elderly There is no universally accepted age cut-off defining elderly. This reflects the fact that chronological age itself is less important than biological events
nicheprogram.org 16th Annual NICHE Conference Forging New Paths and Partnerships 1
 Improving Patient Outcomes in Geriatric Post-Operative Orthopedic Patients: Translating Research into Practice Tripping into The CAM Presented by: Diana LaBumbard, RN, MSN, ACNP/GNP-BC, CWOCN Denise Williams,
Improving Patient Outcomes in Geriatric Post-Operative Orthopedic Patients: Translating Research into Practice Tripping into The CAM Presented by: Diana LaBumbard, RN, MSN, ACNP/GNP-BC, CWOCN Denise Williams,
Improving the quality of care of patients with delirium
 Improving the quality of care of patients with delirium Alasdair MacLullich MRCP(UK), PhD Professor of Geriatric Medicine University of Edinburgh Scotland How are we doing now? We are doing badly. Difficult
Improving the quality of care of patients with delirium Alasdair MacLullich MRCP(UK), PhD Professor of Geriatric Medicine University of Edinburgh Scotland How are we doing now? We are doing badly. Difficult
Delirium Screening Tools: Just- In- Time Education and Evaluation Using the EMR
 Delirium Screening Tools: Just- In- Time Education and Evaluation Using the EMR Implementation of an EMR based protocol for detection of delirium in elderly Medical and palliative care patients Parul Goyal,
Delirium Screening Tools: Just- In- Time Education and Evaluation Using the EMR Implementation of an EMR based protocol for detection of delirium in elderly Medical and palliative care patients Parul Goyal,
譫妄症 (Delirium) Objectives. Epidemiology. Delirium. DSM-5 Diagnostic Criteria. Prognosis 台大醫院老年醫學部陳人豪 2016/8/28
 Objectives. Epidemiology. Delirium. DSM-5 Diagnostic Criteria. Prognosis 台大醫院老年醫學部陳人豪 2016/8/28") 譫妄症 (Delirium) 台大醫院老年醫學部陳人豪 2016/8/28 Objectives Delirium Epidemiology Etiology Diagnosis Evaluation and Management Postoperative delirium Delirium (and acute problematic behavior) in the longterm care
譫妄症 (Delirium) 台大醫院老年醫學部陳人豪 2016/8/28 Objectives Delirium Epidemiology Etiology Diagnosis Evaluation and Management Postoperative delirium Delirium (and acute problematic behavior) in the longterm care
Strategies to minimize delirium for hip fracture patients
 Strategies to minimize delirium for hip fracture patients Stephen L Kates, M.D. Professor and Chairman Department Date of Orthopaedic Surgery Delirium incidence Up to 61% of hip fracture patients get delirium
Strategies to minimize delirium for hip fracture patients Stephen L Kates, M.D. Professor and Chairman Department Date of Orthopaedic Surgery Delirium incidence Up to 61% of hip fracture patients get delirium
David A Scott Lis Evered. Department of Anaesthesia and Acute Pain Medicine St Vincent s Hospital, Melbourne University of Melbourne
 David A Scott Lis Evered Department of Anaesthesia and Acute Pain Medicine St Vincent s Hospital, Melbourne University of Melbourne This talk will include live polling so please be sure to have the meeting
David A Scott Lis Evered Department of Anaesthesia and Acute Pain Medicine St Vincent s Hospital, Melbourne University of Melbourne This talk will include live polling so please be sure to have the meeting
Palliative Care and Delirium. Ambereen K. Mehta, MD MPH Assistant Professor Division of General Medicine, Geriatrics, and Palliative Care
 Palliative Care and Delirium Ambereen K. Mehta, MD MPH Assistant Professor Division of General Medicine, Geriatrics, and Palliative Care Disclosures I have no personal or professional financial relationships
Palliative Care and Delirium Ambereen K. Mehta, MD MPH Assistant Professor Division of General Medicine, Geriatrics, and Palliative Care Disclosures I have no personal or professional financial relationships
QuickTime and a DV - NTSC decompressor are needed to see this picture.
 QuickTime and a DV - NTSC decompressor are needed to see this picture. Case Presentation (Actual Case) 66 y/o Female c/o Hip Pain Fell, but no pre-fall symptoms Did not hit head or have LOC PMHx: DM, ESRD,
QuickTime and a DV - NTSC decompressor are needed to see this picture. Case Presentation (Actual Case) 66 y/o Female c/o Hip Pain Fell, but no pre-fall symptoms Did not hit head or have LOC PMHx: DM, ESRD,
Delirium Screening: The next nurse sensitive indicator?
 Delirium Screening: The next nurse sensitive indicator? Sharon Gunn, MSN, MA, RN, ACNS-BC, CCRN Clinical Nurse Specialist Critical Care Baylor University Medical Center Dallas, TX Objectives Recognize
Delirium Screening: The next nurse sensitive indicator? Sharon Gunn, MSN, MA, RN, ACNS-BC, CCRN Clinical Nurse Specialist Critical Care Baylor University Medical Center Dallas, TX Objectives Recognize
Geriatric Screening in Five Minutes or Less: Skills Stations
 Geriatric Screening in Five Minutes or Less: Skills Stations Charlotte A. Paolini, D. O., CMD June 14, 2014 (Special thanks to Sarah Hallen, M.D., for allowing the use of her materials for this presentation.)
Geriatric Screening in Five Minutes or Less: Skills Stations Charlotte A. Paolini, D. O., CMD June 14, 2014 (Special thanks to Sarah Hallen, M.D., for allowing the use of her materials for this presentation.)
Charles Bernick, MD, MPH Cleveland Clinic Lou Ruvo Center for Brain Health June 2, 2018
 Charles Bernick, MD, MPH Cleveland Clinic Lou Ruvo Center for Brain Health June 2, 2018 Delirium common Prolongs hospitalization Worsens dementia ( if you survive) Increased risk of institutionalization
Charles Bernick, MD, MPH Cleveland Clinic Lou Ruvo Center for Brain Health June 2, 2018 Delirium common Prolongs hospitalization Worsens dementia ( if you survive) Increased risk of institutionalization
Delirium in the Elderly
 Delirium in the Elderly Jeffrey M. Burock, MD Division Director/ Psychiatry / Miriam Hospital Clinical Assistant Professor Warren Alpert School Of Medicine Learning Objectives Identify the symptoms of
Delirium in the Elderly Jeffrey M. Burock, MD Division Director/ Psychiatry / Miriam Hospital Clinical Assistant Professor Warren Alpert School Of Medicine Learning Objectives Identify the symptoms of
Delirium. Quick reference guide. Issue date: July Diagnosis, prevention and management
 Issue date: July 2010 Delirium Diagnosis, prevention and management Developed by the National Clinical Guideline Centre for Acute and Chronic Conditions About this booklet This is a quick reference guide
Issue date: July 2010 Delirium Diagnosis, prevention and management Developed by the National Clinical Guideline Centre for Acute and Chronic Conditions About this booklet This is a quick reference guide
Delirium. Assessment and Management
 Delirium Assessment and Management Goals and Objectives Participants will: 1. be able to recognize and diagnose the syndrome of delirium. 2. understand the causes of delirium. 3. become knowledgeable about
Delirium Assessment and Management Goals and Objectives Participants will: 1. be able to recognize and diagnose the syndrome of delirium. 2. understand the causes of delirium. 3. become knowledgeable about
Management of Delirium in the ICU. Yahya Shehabi
 Management of Delirium in the ICU Yahya Shehabi Hello! Doctor, your patient is CAM + ve Good morning Dr, Am one of the RC, Just examined Mr XXX he is CAM +ve Positive what? Sir replied RC: I meant he is
Management of Delirium in the ICU Yahya Shehabi Hello! Doctor, your patient is CAM + ve Good morning Dr, Am one of the RC, Just examined Mr XXX he is CAM +ve Positive what? Sir replied RC: I meant he is
Jacinta Lucke Resident Emergency Medicine PHD Gerontology & Geriatrics
 Jacinta Lucke Resident Emergency Medicine PHD Gerontology & Geriatrics TAKE HOME MESSAGE When managing confusion in older patients: Routinely screen for impaired cognition Patients with impaired cognition
Jacinta Lucke Resident Emergency Medicine PHD Gerontology & Geriatrics TAKE HOME MESSAGE When managing confusion in older patients: Routinely screen for impaired cognition Patients with impaired cognition
Aging Research Day March 8, 2012
 Aging Research Day March 8, 2012 Heidi R. Wierman, MD Mane Medical Center Division Director, Geriatrics Assistant Professor, Tufts School of Medicine Overview 1.Brief Delirium Review 2.Describe HELP function
Aging Research Day March 8, 2012 Heidi R. Wierman, MD Mane Medical Center Division Director, Geriatrics Assistant Professor, Tufts School of Medicine Overview 1.Brief Delirium Review 2.Describe HELP function
Delirium: A Condition of All Ages. Delirium, also known as acute confusional state, Definition. Epidemiology
 Focus on CME at the University of Calgary : A Condition of All Ages While delirium can strike at any age, physicians need to be particularly watchful for it in elderly patients, so that a search for the
Focus on CME at the University of Calgary : A Condition of All Ages While delirium can strike at any age, physicians need to be particularly watchful for it in elderly patients, so that a search for the
Delirium and Dementia
 Delirium and Dementia Elder Friendly Care in Acute Care Seniors Health Strategic Clinical Network Acute Care Stress Blender Poor Poor sleep At-Risk Older Adult TREAT CAUSE immediately & aggressively. Increased
Delirium and Dementia Elder Friendly Care in Acute Care Seniors Health Strategic Clinical Network Acute Care Stress Blender Poor Poor sleep At-Risk Older Adult TREAT CAUSE immediately & aggressively. Increased
Improving Delirium Management: Mapping Out One Unit s Journey. Geriatrics Institute June 27, 2013
 Improving Delirium Management: Mapping Out One Unit s Journey Geriatrics Institute June 27, 2013 Rebecca Ramsden, NP Mary Ann Hamelin, CNS Susanne Loay, RN Objectives Background RNAO Best Practice Guideline
Improving Delirium Management: Mapping Out One Unit s Journey Geriatrics Institute June 27, 2013 Rebecca Ramsden, NP Mary Ann Hamelin, CNS Susanne Loay, RN Objectives Background RNAO Best Practice Guideline
Causes of Transient Incontinence. Geriatrics: Urinary Incontinence, Dementia, and Delirium. Classification of Established Incontinence
 Causes of Transient Geriatrics: Urinary, Dementia, and Delirium Carla Zeilmann, PharmD, BCPS St. Louis College of Pharmacy Therapeutics 3 Fall 2003 D delirium I infection A atrophic urethritis and vaginitis
Causes of Transient Geriatrics: Urinary, Dementia, and Delirium Carla Zeilmann, PharmD, BCPS St. Louis College of Pharmacy Therapeutics 3 Fall 2003 D delirium I infection A atrophic urethritis and vaginitis
Addressing Difficult Behaviors in Dementia
 Addressing Difficult Behaviors in Dementia GEORGE SCHOEPHOERSTER, MD GERIATRICIAN GENEVIVE/CENTRACARE CLINIC Objectives By the end of the session, you will be able to: 1) Explain the role of pain management
Addressing Difficult Behaviors in Dementia GEORGE SCHOEPHOERSTER, MD GERIATRICIAN GENEVIVE/CENTRACARE CLINIC Objectives By the end of the session, you will be able to: 1) Explain the role of pain management
Test your Knowledge: Recognizing Delirium
 The Ottawa Hospital Name: Unit: Profession: RN RPN PT OT SW Other Note: Each question has only one correct answer. 1. If a patient is identified as being at high risk for developing delirium, his/her mental
The Ottawa Hospital Name: Unit: Profession: RN RPN PT OT SW Other Note: Each question has only one correct answer. 1. If a patient is identified as being at high risk for developing delirium, his/her mental
Objectives. Delirium in the Elderly Patient. Disclosure. Arizona Geriatrics Society Fall Symposium 2010
 Delirium in the Elderly Patient Sandra Jacobson, MD Banner Sun Health Research Institute Arizona Geriatrics Society Fall Symposium 2010 Disclosure Dr. Jacobson has disclosed that she does not have any
Delirium in the Elderly Patient Sandra Jacobson, MD Banner Sun Health Research Institute Arizona Geriatrics Society Fall Symposium 2010 Disclosure Dr. Jacobson has disclosed that she does not have any
Delirium clinical and research challenges
 Delirium clinical and research challenges Daniel Davis Senior Clinical Researcher Consultant in Geriatric Medicine University College London London Memory Assessment Network 4 th May 2016 Overview Core
Delirium clinical and research challenges Daniel Davis Senior Clinical Researcher Consultant in Geriatric Medicine University College London London Memory Assessment Network 4 th May 2016 Overview Core
Falls Prevention Best Practice
 Falls Prevention Best Practice Prepared by Denise Tomassini Falls Prevention A case study : Mr Tony Topples ISLHD Clinical Quality Manager Clinical Governance Unit November 2011 Falls Prevention Best Practice
Falls Prevention Best Practice Prepared by Denise Tomassini Falls Prevention A case study : Mr Tony Topples ISLHD Clinical Quality Manager Clinical Governance Unit November 2011 Falls Prevention Best Practice
DISCLAIMER: ECHO Nevada emphasizes patient privacy and asks participants to not share ANY Protected Health Information during ECHO clinics.
 DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
Decreasing Delirium Resolution Times for the Elderly: An Interprofessional Approach
 Decreasing Delirium Resolution Times for the Elderly: An Interprofessional Approach Featuring: Felice Rogers Evans BSN RN BC Ty Breiter MSN RN CNL Tampa General Hospital NICHE exemplar hospital Three time
Decreasing Delirium Resolution Times for the Elderly: An Interprofessional Approach Featuring: Felice Rogers Evans BSN RN BC Ty Breiter MSN RN CNL Tampa General Hospital NICHE exemplar hospital Three time
GERIATRIC MENTAL HEALTH AND MEDICATION TREATMENT
 Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences GERIATRIC MENTAL HEALTH AND MEDICATION TREATMENT RUTH KOHEN ASSOCIATE PROFESSOR UW DEPARTMENT OF PSYCHIATRY 5-4-2017
Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences GERIATRIC MENTAL HEALTH AND MEDICATION TREATMENT RUTH KOHEN ASSOCIATE PROFESSOR UW DEPARTMENT OF PSYCHIATRY 5-4-2017
DELIRIUM DR S A R A H A B D E L A T I S A S DR H I L A R Y W O L F E N D A L E S T 4
 DELIRIUM DR S A R A H A B D E L A T I S A S DR H I L A R Y W O L F E N D A L E S T 4 AIMS Define delirium Identify: Different types of delirium Risk factors Preventable causes Screening tools Management
DELIRIUM DR S A R A H A B D E L A T I S A S DR H I L A R Y W O L F E N D A L E S T 4 AIMS Define delirium Identify: Different types of delirium Risk factors Preventable causes Screening tools Management
Delirium in the Emergency Department. Emergency Medicine Rounds April 14, 2015 Paul R. Vanhoutte
 Delirium in the Emergency Department Emergency Medicine Rounds April 14, 2015 Paul R. Vanhoutte Goals of Rounds: Review Definition Management An Understanding What is important is to spread confusion,
Delirium in the Emergency Department Emergency Medicine Rounds April 14, 2015 Paul R. Vanhoutte Goals of Rounds: Review Definition Management An Understanding What is important is to spread confusion,
H.E.L.P. ing Elder Trauma Patients Avoid Delirium and Functional Decline
 H.E.L.P. ing Elder Trauma Patients Avoid Delirium and Functional Decline Montreal ITC 2014 Sept. 26 Joann Creager, CNS Geriatrics, Manager, MUHC Elder Friendly Hospital Presentation Overview 1. Elder patient
H.E.L.P. ing Elder Trauma Patients Avoid Delirium and Functional Decline Montreal ITC 2014 Sept. 26 Joann Creager, CNS Geriatrics, Manager, MUHC Elder Friendly Hospital Presentation Overview 1. Elder patient
BRAIN. Tumor byproducts. Autonomic nerves. Somatic nerves. Host immune cells. Cytokines
 Patient s Problems Pain (80%) Fatigue (90%) Weight Loss (80%) Lack of Appetite (80%) Nausea, Vomiting (90%) Anxiety (25%) Shortness of Breath (50%) Confusion-Agitation (80%) Tumor Mass Tumor Function Somatic
Patient s Problems Pain (80%) Fatigue (90%) Weight Loss (80%) Lack of Appetite (80%) Nausea, Vomiting (90%) Anxiety (25%) Shortness of Breath (50%) Confusion-Agitation (80%) Tumor Mass Tumor Function Somatic
Managing Delirium: The best way to achieve clarity (of mind) Tim Walsh. Professor of Critical Care, Edinburgh University
 Tim Walsh. Professor of Critical Care, Edinburgh University") Managing Delirium: The best way to achieve clarity (of mind) Tim Walsh Professor of Critical Care, Edinburgh University Lecture Plan: a route to clarity What is delirium? Why is delirium important? Step
Managing Delirium: The best way to achieve clarity (of mind) Tim Walsh Professor of Critical Care, Edinburgh University Lecture Plan: a route to clarity What is delirium? Why is delirium important? Step
POST STROKE DELIRIUM. Dr Janet Ballantyne
 POST STROKE DELIRIUM Dr Janet Ballantyne Delirium de: away from/off lira: ridge between ploughed farrows/tracks off the tracks Acute confusional state Acute brain syndrome Acute brain failure Metabolic
POST STROKE DELIRIUM Dr Janet Ballantyne Delirium de: away from/off lira: ridge between ploughed farrows/tracks off the tracks Acute confusional state Acute brain syndrome Acute brain failure Metabolic
The triad of inpatient harm
 Delirium in hospital: Identification, prevention and management Dr Jonathan Treml Consultant Geriatrician Queen Elizabeth Hospital Birmingham, UK With thanks to Dr Thomas Jackson for some of the slides
Delirium in hospital: Identification, prevention and management Dr Jonathan Treml Consultant Geriatrician Queen Elizabeth Hospital Birmingham, UK With thanks to Dr Thomas Jackson for some of the slides
DELIRIUM. J. Sukanya 28.Jun.12
 DELIRIUM J. Sukanya 28.Jun.12 Outline Why? What? How? What s next? Delirium Introduction Delirium An acute decline in attention and cognition The most frequent neuropsychiatric syndrome A common, life-threatening,
DELIRIUM J. Sukanya 28.Jun.12 Outline Why? What? How? What s next? Delirium Introduction Delirium An acute decline in attention and cognition The most frequent neuropsychiatric syndrome A common, life-threatening,
Delirium Superimposed on Dementia: What Do We Know and What Can We Do? Delirium Superimposed on MY MESSAGES TODAY
 Delirium Superimposed on Dementia: What Do We Know and What Can We Do? Donna Fick, RN, PhD, FGSA, FAAN¹, 2 Distinguished Professor Director Hartford Center of Geriatric Nursing Excellence Editor, Journal
Delirium Superimposed on Dementia: What Do We Know and What Can We Do? Donna Fick, RN, PhD, FGSA, FAAN¹, 2 Distinguished Professor Director Hartford Center of Geriatric Nursing Excellence Editor, Journal
Geriatric Alterations Associated with Neurological Conditions
 Geriatric Alterations Associated with Neurological Conditions I have no conflicts of interest. Julie Bronson The Older Adult According to the World Health Organization Africa 50-55 or 50-65 United Nations
Geriatric Alterations Associated with Neurological Conditions I have no conflicts of interest. Julie Bronson The Older Adult According to the World Health Organization Africa 50-55 or 50-65 United Nations
Drug induced delirium
 Drug induced delirium Knut Erik Hovda, MD, PhD, FACMT, FEAPCCT The Norwegian CBRNe Centre of Medicine Department of Acute Medicine Oslo University hospital Content 1. Introduction 2. Risk factors 3. Prevalence
Drug induced delirium Knut Erik Hovda, MD, PhD, FACMT, FEAPCCT The Norwegian CBRNe Centre of Medicine Department of Acute Medicine Oslo University hospital Content 1. Introduction 2. Risk factors 3. Prevalence
Delirium, The Geriatrics Ward Challenge
 American Journal of Pharmacology and Pharmacotherapeutics Research Article Delirium, The Geriatrics Ward Challenge Pardo Pastor Ricardo Fernandes 1, Rafaela Veríssimo 2 and António Agripino Oliveira 3*
American Journal of Pharmacology and Pharmacotherapeutics Research Article Delirium, The Geriatrics Ward Challenge Pardo Pastor Ricardo Fernandes 1, Rafaela Veríssimo 2 and António Agripino Oliveira 3*
Management of delirium in mechanically ventilated patients. Advances in Critical Care Medicine King Hussein Cancer Center
 Management of delirium in mechanically ventilated patients Advances in Critical Care Medicine King Hussein Cancer Center Introduction Outline: Prevalence of delirium in ICU Why it is important to screen
Management of delirium in mechanically ventilated patients Advances in Critical Care Medicine King Hussein Cancer Center Introduction Outline: Prevalence of delirium in ICU Why it is important to screen
g Prevention, Diagnosis, and Management in Palliative Care
 8/3/2012 Improving p g Prevention, Diagnosis, g and Management in Palliative Care MN Rural Palliative Care Networking Group Quarterly Education Session June 27,2012 Sandra W. Gordon-Kolb, MD, MMM, CPE
8/3/2012 Improving p g Prevention, Diagnosis, g and Management in Palliative Care MN Rural Palliative Care Networking Group Quarterly Education Session June 27,2012 Sandra W. Gordon-Kolb, MD, MMM, CPE
Symptom Management Pocket Guides: DELIRIUM
 Symptom Management Pocket Guides: DELIRIUM August 2010 DELIRIUM Page Considerations. 1 Assessment 2 Diagnosis. 3 Non-Pharmacological treatment 3 Pharmacological treatment. 5 Mild Delirium... 6 Moderate
Symptom Management Pocket Guides: DELIRIUM August 2010 DELIRIUM Page Considerations. 1 Assessment 2 Diagnosis. 3 Non-Pharmacological treatment 3 Pharmacological treatment. 5 Mild Delirium... 6 Moderate
Delirium. Delirium is characterized by an acute onset (hours or days) and fluctuating course of deterioration in mental functioning.
 and fluctuating course of deterioration in mental functioning.") Delirium Delirium is characterized by an acute onset (hours or days) and fluctuating course of deterioration in mental functioning. DELIRIUM IS A MEDICAL EMERGENCY! Delirium: Hallmark Features Inattention-
Delirium Delirium is characterized by an acute onset (hours or days) and fluctuating course of deterioration in mental functioning. DELIRIUM IS A MEDICAL EMERGENCY! Delirium: Hallmark Features Inattention-
Management of Delirium in the Elderly Patients: A Review of Evidence
 Review Article imedpub Journals http://journals.imedpub.com Journal of Drug Abuse 2471-853X DOI: 10.21767/2471-853X.10006 Abstract Management of Delirium in the Elderly Patients: A Review of Evidence Delirium
Review Article imedpub Journals http://journals.imedpub.com Journal of Drug Abuse 2471-853X DOI: 10.21767/2471-853X.10006 Abstract Management of Delirium in the Elderly Patients: A Review of Evidence Delirium
ICU Delirium in Infants & Children: Cause for Concern or False Alarm. Objectives
 ICU Delirium in Infants & Children: Cause for Concern or False Alarm Peter (Pete) N. Johnson, Pharm.D., BCPS, BCPPS, FPPAG Associate Professor of Pharmacy Practice University of Oklahoma College of Pharmacy
ICU Delirium in Infants & Children: Cause for Concern or False Alarm Peter (Pete) N. Johnson, Pharm.D., BCPS, BCPPS, FPPAG Associate Professor of Pharmacy Practice University of Oklahoma College of Pharmacy
DELIRIUM. Approach and Management
 DELIRIUM Approach and Management By Dr. K.S. Jacob, Professor of Psychiatry and Dr. Anju Kuruvilla, Professor of Psychiatry, Christian Medical College, Vellore. Based on a chapter in the book Psychiatric
DELIRIUM Approach and Management By Dr. K.S. Jacob, Professor of Psychiatry and Dr. Anju Kuruvilla, Professor of Psychiatry, Christian Medical College, Vellore. Based on a chapter in the book Psychiatric
Disentangling Delirium and Dementia
 Disentangling Delirium and Dementia Sharon K. Inouye, M.D., M.P.H. Professor of Medicine Beth Israel Deaconess Medical Center Harvard Medical School Milton and Shirley F. Levy Family Chair Director, Aging
Disentangling Delirium and Dementia Sharon K. Inouye, M.D., M.P.H. Professor of Medicine Beth Israel Deaconess Medical Center Harvard Medical School Milton and Shirley F. Levy Family Chair Director, Aging
Care of older people in surgery (COPS)
") Care of older people in surgery (COPS) Who, what, and does it make a difference Professor Jacqueline Close Geriatrician - POWH Clinical Director Falls, Balance and Injury Research Centre Early Mobilisation
Care of older people in surgery (COPS) Who, what, and does it make a difference Professor Jacqueline Close Geriatrician - POWH Clinical Director Falls, Balance and Injury Research Centre Early Mobilisation
Dementia. Aetiology, pathophysiology and the role of neuropsychological testing. Dr Sheng Ling Low Geriatrician
 Dementia Aetiology, pathophysiology and the role of neuropsychological testing Dr Sheng Ling Low Geriatrician Topics to cover Why is dementia important What is dementia Differentiate between dementia,
Dementia Aetiology, pathophysiology and the role of neuropsychological testing Dr Sheng Ling Low Geriatrician Topics to cover Why is dementia important What is dementia Differentiate between dementia,
Prevention of Delirium in Dementia
 Prevention of Delirium in Dementia Appropriate Use of Antipsychotics Project Seniors Health Strategic Clinical Network (SCN) In collaboration with Addiction & Mental Health SCN Introduce your team/family
Prevention of Delirium in Dementia Appropriate Use of Antipsychotics Project Seniors Health Strategic Clinical Network (SCN) In collaboration with Addiction & Mental Health SCN Introduce your team/family
Summary of funded Dementia Research Projects
 Summary of funded Dementia Research Projects Health Services and Delivery Research (HS&DR) Programme: HS&DR 11/2000/05 The detection and management of pain in patients with dementia in acute care settings:
Summary of funded Dementia Research Projects Health Services and Delivery Research (HS&DR) Programme: HS&DR 11/2000/05 The detection and management of pain in patients with dementia in acute care settings:
Disclosures. Post operative Delirium. Set up audience participation. Delirium Definitions. Incidence of Delirium
 Post operative Delirium Disclosures IP for monitoring technology licensed to Medtronic Ken Brady, MD Pediatrics, Anesthesia, Critical Care Texas Children s Hospital Baylor College of Medicine Set up audience
Post operative Delirium Disclosures IP for monitoring technology licensed to Medtronic Ken Brady, MD Pediatrics, Anesthesia, Critical Care Texas Children s Hospital Baylor College of Medicine Set up audience
For more information about how to cite these materials visit
 Author(s): Rachel Glick, M.D., 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Noncommercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
Author(s): Rachel Glick, M.D., 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Noncommercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
Delirium and dementia: The best of friends, the worst of enemies David Meagher
 Delirium and dementia: The best of friends, the worst of enemies David Meagher Professor of Psychiatry, UL Graduate-Entry Medical School Two Sumo Wrestlers Two great heavyweights Generalised Cognitive
Delirium and dementia: The best of friends, the worst of enemies David Meagher Professor of Psychiatry, UL Graduate-Entry Medical School Two Sumo Wrestlers Two great heavyweights Generalised Cognitive
Update in Geriatrics. Muriel Rainfray Department of Gerontology CHU Bordeaux
 Update in Geriatrics Muriel Rainfray Department of Gerontology CHU Bordeaux What s new about frailty? The frailty phenotype and the frailty index : different instruments for different purposes Matteo Cesari
Update in Geriatrics Muriel Rainfray Department of Gerontology CHU Bordeaux What s new about frailty? The frailty phenotype and the frailty index : different instruments for different purposes Matteo Cesari
Memory Matters Service Dementia, Depression and Delerium Cancer Awareness Toolkit Evaluation Event
 Cumbria Partnership NHS Foundation Trust Memory Matters Service Dementia, Depression and Delerium Cancer Awareness Toolkit Evaluation Event Andrew Milburn Occupational Therapy Clinical Lead, Dementia Pathways
Cumbria Partnership NHS Foundation Trust Memory Matters Service Dementia, Depression and Delerium Cancer Awareness Toolkit Evaluation Event Andrew Milburn Occupational Therapy Clinical Lead, Dementia Pathways