Cigna Care Designation and Physician Quality and Cost-Efficiency Displays 2016 Methodologies Whitepaper
|
|
|
- Julia Lane
- 6 years ago
- Views:
Transcription
1 Cigna Care Designation and Physician Quality and Cost-Efficiency Displays 2016 Methodologies Whitepaper For Health Care Professionals February 2016 Introduction... 2 Cigna Physician Quality and Cost-Efficiency Display Principles... 2 Cigna Care Designation and Physician Quality and Cost-Efficiency Displays Overview... 3 Specialty Assessed for Cigna Care Designation and Physician Quality and Cost-Efficiency Displays... 6 Quality Evaluation... 6 Evidence Based Medicine (EBM) Assessment Process... 8 Cost-Efficiency Evaluation and 2016 Outlier Methodology Assigning the Cigna Care Designation (2015 and 2016 CCD Inclusion Methodology) Buffer Zone Methodology Collaborative Accountable Care Pathway to Achieving Cigna Care Designation Data Sources Additional Information and Data Limitations Process to Display Strategic Alliances Information Feedback Process Physician Process to Correct Errors, Request Reconsideration, or Appeal How to Register Complaints and 2016 Physician Evaluation Methodology Changes Appendices Appendix 1: 2015 and 2016 Cigna Care Designation Market Information Appendix 2: 2015 and 2016 Quality and Cost-Efficiency Display Markets Appendix 3: EBM Rules Used for the 2015 and 2016 Physician Evaluation Appendix 4: Appeals Process for Colorado Health Care Professionals Abbreviations List THN Cigna. Some content provided under license. 1
2 Introduction We evaluate physician quality and cost-efficiency information by using a methodology consistent with national standards and incorporating physician feedback. Using this information, we are able to provide our customers and clients with relevant consumer-oriented information through the physician quality and cost- efficiency displays and the Cigna Care designation (CCD) program. The purpose of this document is to provide an overview of our Physician Quality and Cost-Efficiency Displays Program, explain the methodology used to measure individual physicians and medical groups for quality and costefficiency results, and provide details regarding the physician quality and cost-efficiency display information used. Cigna Physician Quality and Cost-Efficiency Display Principles We believe that our customers and employers have a right to know information regarding the quality and costeffectiveness of physicians. We follow three key principles when providing our physician quality and costeffectiveness information to customers, clients, and physicians: 1. Standardized performance measures using the most comprehensive data set available We use nationally recognized measures derived from those endorsed by the Forum (NQF), Ambulatory Care Quality Alliance (AQA), Healthcare Effectiveness Data Information Set (HEDIS 1 ), or those developed by national physician organizations such as the American Medical Association (AMA). 2. Responsible use of the information The displays reflect a partial assessment of quality and cost-efficiency based on our claims data, and should not be the sole basis for decision-making (as such measures have a risk of error). Cigna customers are encouraged to consider all relevant factors and to consult with their treating physician when selecting a physician for care. In general, the health care professionals in Cigna's networks are independent practitioners; they are not employees or agents of Cigna. Treatment decisions are made exclusively by the treating physician and the patient. Cigna provides its customers with helpful information to allow them to make informed decisions. The quality and cost-efficiency markers used in evaluating physicians for Cigna Care designation are intended for that purpose only. Cigna does not guarantee the quality or cost-efficiency of the actual services provided by network physicians - even those physicians that qualify for the Cigna Care designation. 3. Collaboration and Improvement Enablement We are committed to providing information and solutions that can support access to quality health care. A detailed description of our methodology, information about the summary metrics, and ongoing data to help improve performance is available to physicians and physician groups. We also continue to have ongoing discussions with key physician organizations, ranging from national associations to large physician groups, who provide input for future design changes. Frequency of Reviews The methodology for determining the Cigna Care designation and physician quality and cost-efficiency displays is subject to change annually as tools and industry standards evolve and physician feedback is obtained. The assessment review period for Cigna Care designation and quality and cost-effectiveness displays for 2015 and 2016 is January 1, 2012 through December 31, This review includes claims data from Cigna Managed Care and PPO plans. The current 2015 Cigna Care designation and physician quality and cost-efficiency displays in the directory will remain in effect through December 31, HEDIS is a registered trademark of the National Committee for Quality Assurance (NCQA). THN Cigna. Some content provided under license. 2
3 External Certification Cigna earned Physician and Hospital Quality Certification for the fourth time in July The NCQA Physician and Hospital Quality (PHQ) certification program evaluates how well health plans measure and report the quality and cost of physicians and hospitals. NCQA Physician Quality Certification Standards meet New York state requirements implemented in November 2007 concerning physician performance measurement, reporting, and tiering programs. Cigna Care Designation and Physician Quality and Cost-Efficiency Displays Overview There are two components of the Cigna Care designation and Physician Quality and Cost-Efficiency Displays programs, each of which is explained in more detail in the following sections of this document: 1. Quality evaluation and display: Physicians are evaluated on a number of criteria that we believe are markers of physician practice quality. The results of this evaluation are displayed in mycigna.com, our online health care professional directory that is available to Cigna customers. Results of selected quality markers (e.g., evidence based medicine (EBM) rule adherence and NCQA Physician Recognition) are used to qualify physicians and physician groups for Cigna Care designation. 2. Cost-efficiency evaluation and display: Individual physicians and physician groups are evaluated for their cost-efficiency using an industry-standard methodology (i.e., Episode Treatment Groups) that determines the average cost of treating an episode of care for a variety of medical conditions and surgical procedures. We then compare those episode costs to those of other physicians and medical groups of the same specialty in the same geographical market. The results of this evaluation are displayed in our online health care professional directory using one, two or three stars, with three stars being the highest rating (i.e., the most cost-efficient). Cigna Care designation: Cigna Care designation is assigned to individual participating physicians and physician groups based on Cigna's cost-efficiency and quality criteria. If an individual physician or physician group does not meet the Cigna Care designation criteria and the physician or physician group participates in a Cigna Collaborative Accountable Care (CAC), they may receive Cigna Care designation if they meet certain cost and quality thresholds (see pages for more details). Cost efficiency and quality evaluations provide individual physicians and physician groups that are ranked in the top 40% for quality and the top 40% for cost-efficiency compared to all physicians and physician groups of the same group specialty type in the same geographic market with the Cigna Care designation. In the absence of a sufficient number of cost episodes to evaluate cost-efficiency, physicians and physician groups that rank in the top 34% for quality compared to groups of the same specialty in their market also receive the Cigna Care designation. In the absence of a sufficient number of quality opportunities to evaluate quality, physicians and physician groups that rank in the top 34% for cost compared to groups of the same specialty in their market also receive the Cigna Care designation (see page 11 for more information regarding assigning CCD based on cost and quality). They are identified with a Symbol ( ) and Cigna Care Designation in the online health care professional directory on Cigna.com and mycigna.com. (Please see the sample healthcare professional directory display on page 5.) Cigna Care designation benefit design: The Cigna Care designation is a benefit-plan design option offered to organizations sponsoring group health benefit plans. Available in 73 service areas, the designation distinguishes physicians in 21 specialties (3 primary care + 18 other specialties) who participate in our network, based on their meeting the above referenced quality and cost-efficiency criteria. THN Cigna. Some content provided under license. 3
4 The Cigna Care benefit design, which is intended to encourage Cigna customers covered by these plans to consider using a Cigna Care designated physician, affords a lower co-payment or coinsurance for services provided by a designated physician than if the individual were to select a participating, non-designated physician. Overall physician reimbursement is unchanged. Geographical markets that the Cigna Care designation benefit plan is offered in 2015 and 2016 were defined by our Network Contracting and Market Medical Executive teams. The zip code of a physician s primary office address is used to align a physician with a given market. The physician s primary specialty and geographic market is then used to determine the physician peer group for comparison of quality and cost-efficiency outcomes. Please see Appendix 1 for a list of markets, the volume of physicians reviewed, and the percent of physicians reviewed in each market that are Cigna Care designated, effective January 1, Physician Cost-Efficiency Displays Information regarding the physician s cost-effectiveness performance is displayed only on mycigna.com, the secure website for Cigna customers. The displays are available in 73 markets for the 21 specialty types assessed for Cigna Care designation, including the 18 specialty types assessed for the Cigna Care designation, and three primary care physician (PCP) specialty types (,, and ). Cost-efficiency stars are used to communicate cost-efficiency performance. Three stars for cost- efficiency represent the top 34% of physicians or physician groups when compared to other physicians and physician groups of the same group specialty type within the geographic market. Two stars represent physicians or physician groups in the middle 33% for cost-efficiency. Physician groups that are in the lower 33% for costefficiency receive one star. Cost-Efficiency Symbols Results in top category for cost-efficiency measures Results in middle category for cost-efficiency Results in the low category for cost-efficiency Please see Appendix 2 for the geographical markets and volume of physicians reviewed for physician quality and cost-efficiency displays, beginning January 1, THN Cigna. Some content provided under license. 4
5 Sample: Online health care professional directory displays (mycigna.com) Denotes physician with Cigna Care designation Quality and cost-efficiency recognitions THN Cigna. Some content provided under license. 5
6 Specialty Assessed for Cigna Care Designation and Physician Quality and Cost-Efficiency Displays We assess 21 physician specialty types including primary care, as identified in the following table. A physician may only be assigned one specialty, tax identification number (TIN), and geographical market for Cigna Care designation or physician quality and cost-efficiency displays. The physician s primary specialty, as listed in the Cigna Central Provider File, is used to establish the specialty to evaluate physicians with multiple specialties. Assessed Specialty Allergy and Immunology Cardiology Cardio-Thoracic Surgery Dermatology Ear, Nose and Throat Endocrinology Gastroenterology General Surgery Hematology and Oncology* Nephrology Neurology Neurosurgery Obstetrics and Gynecology Ophthalmology Orthopedics and Surgery Pulmonary Rheumatology Urology *Does not include Radiation Oncology Participating physicians in the 21 specialty types reviewed for the Cigna Care designation account for over 90% of primary and specialty care and 85% of total medical and pharmaceutical spending based on our claims data. Quality Evaluation Information relative to specific quality criteria met by a physician is displayed in the online health care professional directory on both the public and secure websites at Cigna.com and mycigna.com. We use five quality indicators to review participating physicians in the 21 specialty types. Each physician qualifying for a specific quality indicator is identified in our online healthcare professional directory. 1. National Committee for Quality Assurance (NCQA) Physician Recognition The NCQA recognition in our online directory is given to physicians who have received recognition in any of the six NCQA Physician Recognition Programs: back pain, diabetes, heart/stroke, physician practice connections, and patient-centered medical home 2011 (two versions). Effective January 1, 2015, Cigna began recognizing the additional physician recognition - the NCQA Patient Centered Specialty Practice Program - as a quality indicator for reviewing participating physicians in the 21 specialty types. The verbiage below reflects the display of the quality recognitions in the online directory. NCQA Diabetes Physician Recognition Program (DRP) - identifies primary care physicians, endocrinologists, and diabetes specialists who provide care to people with diabetes. This program assesses key measures specific to diabetes care, such as monitoring and management of blood pressure, cholesterol and glucose levels, patient satisfaction, and other important measures. NCQA Heart/Stroke Physician Recognition Program (HSRP) - identifies doctors who provide quality care to people with heart disease or a history of strokes. This program assesses key measures specific to heart disease and stroke care, such as blood pressure and cholesterol level control, smoking status and advice or treatment for quitting, patient satisfaction, and other important measures. NCQA Physician Practice Connections (PPC) - assesses the systematic use of information in doctors' practices to improve the quality of care. This program recognizes physicians who consistently keep their patients well informed about their health, who are actively engaged in improving their patients' health over time, and who successfully use technology and other tools to prevent medical errors. NCQA Back Pain Recognition Program (BPRP) - recognizes physicians and chiropractors who deliver superior care to their patients suffering from low back pain. The program assesses the diagnosis process, treatment, and advice focused on helping patients return to normal activities. THN Cigna. Some content provided under license. 6
7 NCQA Physician Practice Connections - Patient-Centered Medical Home TM (PCMH - 2 versions) - recognizes doctors that effectively manage their patient's care by coordinating with other doctors, specialists, and family members to deliver a holistic, or comprehensive, patient treatment. NCQA Patient Centered Specialty Practice (PCSP) recognizes practices that have demonstrated commitment to patient-centered care and clinical quality through streamlined referral processes and care coordination with referring clinicians, timely patient and caregiver-focused care management, and continuous clinical quality improvement. Additional information about these programs is available on the NCQA website ( > Programs > Recognition). 2. Group Board Certification Group board certification criteria, based on American Board of Medical Specialties & American Osteopathic Association certification information, determine if care provided by a group is predominantly provided by board certified physicians. This standard is met if: either 80% of physicians within a group are board certified and provide 50% of the care, or at least 80% of the care is provided by board certified physicians, OR for practices/groups with 4 or fewer physicians, either 65% of physicians within a group are board certified and provide 50% of the care, or at least 65% of the care is provided by board certified physicians 3. Adherence to Evidence-Based Medicine (EBM) Rules The quality of physician care is evaluated using a claims-based assessment based on 99 EBM rules derived from rules endorsed by the Forum (NQF), Ambulatory Care Quality Alliance (AQA), Healthcare Effectiveness Data Information Set (HEDIS), or developed by physician organizations. These rules span 48 diseases and preventive care conditions (see Appendix 3), and are potentially applicable to the care provided by physicians in 20 specialty types. For a list of the specialty types that are covered by evidencebased medicine rules, please see the Specialty Covered by Evidence Based Medicine Rules chart below. 4. American Board of Process Improvement Module Completion (ABIM-PIM) We recognize physicians who have completed one or more American Board of Practice Improvement modules (ABIM PIM) as part of the ABIM Maintenance of Certification program. Certification/recertification must be achieved every two years. The ABIM-PIM recognition will no longer be displayed after December 31, Evidence-Based Medicine (EBM) Assessment Process Evidence-based medicine rules that we currently use are applicable to 20 primary care and non-primary care specialties. Currently there are no evidence based medicine rules applicable to dermatology. Overall, approximately 15% of physicians in the specialties noted below (including Dermatology) are associated with groups that do not have sufficient volume to assess adherence to the EBM rules however, they have sufficient volume to assess cost-efficiency. Similarly, 4,226 or almost 1% of physicians are associated with groups that do not have sufficient volume to assess cost-efficiency and therefore are assessed based on adherence with the EBM rules alone. THN Cigna. Some content provided under license. 7
8 Evidence Based Medicine (EBM) Assessment Process Specialty Covered by Evidence Based Medicine Rules Allergy and Immunology Cardiology Cardiothoracic Surgery Endocrinology Gastroenterology General Surgery Hematology and Oncology Nephrology Neurology Neurosurgery Obstetrics and Gynecology (OB/GYN) Ophthalmology Orthopedics and Surgery Otolaryngology (ENT) Pulmonary Rheumatology Urology The EBM assessment component of the Cigna Care Designation program for 2015 and 2016 involves assessment of compliance with a total of 99 EBM rules (see Appendix 3) for the medical conditions displayed in the following table: Disease and Preventive Care Conditions Covered By Evidence Based Medicine Rules Adenoidectomy Adolescent Well-Care Asthma Atrial Fibrillation Attention Deficit Hyperactivity Disorder (ADHD) Breast Cancer I & II Bronchitis (Acute) Cardiac Surgery Cerebral Vascular Accident Cervical Dysplasia Children and Adolescents' Access to Primary Care Practitioners Children s Access to Primary Care Practitioners Chlamydia Screening Cholesterol Management Chronic Kidney Disease Chronic Obstructive Pulmonary Disease Congestive Heart Failure Colon Cancer -II Depression Medication Management Diabetes COPD Exacerbation, Pharmacotherapy Management Comprehensive Ischemic Vascular Disease Care Coronary Artery Disease Epilepsy Hepatitis C Hypertension Inflammatory Bowel Disease Knee Replacement Low Back Pain Migraine Multiple Sclerosis Obesity and Overweight Osteoporosis Otitis Externa (Acute) Pharyngitis Otitis Media Pneumonia (Community Acquires Bacterial) Persistence of Beta Blocker Treatment After MI Pregnancy Management Prenatal Care Prostate Cancer I & II Rheumatoid Arthritis Rheumatoid Arthritis, Drug Therapy Sickle Cell Anemia Sinusitis Tonsillectomy Tympanostomy Upper Respiratory Infection THN Cigna. Some content provided under license. 8
9 Definitions used in the following methodology description: 1. Physician specialty type: any one of the 21 specialty types listed in the table of Assessed Specialty found on page 6 of this white paper 2. Group specialty type: any one of the 21specialty types listed in the table of Assessed Specialty found on p. of this white paper if the medical group is comprised of physicians all of the same specialty, or in the case of mixed specialty groups, one of the following mixed specialty group designations: multispecialty medical group (mixture of multiple non-pcp specialists), mixed specialty medical group (mixture of PCPs and non-pcp specialists), primary care medical group (mixture of PCP specialists) 3. Specialty category: primary care specialties (FP, IM, PD) or non-primary care specialties (the 18 other specialties assessed for CCD) We determine the extent to which an individual physician or physician group complies with evidence-based medicine rules according to the following conventions: Determining peer or market EBM rule adherence for each geographic market: In order for an EBM rule to be included for review at the geographic market level for a physician or physician group, there must be at least 20 opportunities for the rule within the specialty category (primary care or nonprimary care specialties) and market for the most recent two-year data review period. For 2015 and 2016 displays and Cigna Care designation, that period is January 1, 2012 December 31, 2013 The average adherence rate for each EBM rule is calculated for the specialty category (primary care or nonprimary care specialties) for each geographic market to derive the peer/market average result. Determining individual physician or group practice EBM rule adherence: Opportunities and successes for each eligible EBM rule are aligned to the appropriate individual physician (using the visit requirements outlined below and relevant specialty type category). Visit Requirements: A physician is considered responsible for adherence to the EBM rule if the following conditions are met: o The EBM rule is relevant to the physician s specialty (see Appendix 3). For example, the Cervical Dysplasia EBM rule is relevant to OB/GYN,, and, but it is not relevant to other specialties. o There have been at least two office visit encounters for an individual with Cigna coverage during the claim review period. o At least one of the office visit encounters occurred in the last 12 months of the claim review period. Note: 19 of our EBM measures require only one office visit encounter in the last 12 months of the claim review period. These measures are identified by an asterisk [*] in Appendix 3. Individual physicians are aligned to medical groups (practices), and EBM rule opportunities, successes, and expected successes are then summed to obtain medical group totals. A Quality Index for the medical group is calculated by dividing the physician s or physician group s number of actual EBM rule adherence successes by the physician s or physician group s number of expected EBM rule adherence successes. Expected EBM rule adherence successes are derived by applying the geographic market average EBM rule adherence success rates to that physician medical group s particular rule mix opportunities. THN Cigna. Some content provided under license. 9
10 A 90% confidence interval around the Quality Index is determined, allowing EBM quality performance to be measured with a strong degree of certainty. The lower bound of the 90% confidence interval for a particular physician or physician group is defined as the Adjusted Quality Index for that physician medical group. Physician groups that meet the Cigna group board-certification criteria have 30 or more total EBM ruleadherence opportunities, and have at least 50% of their treatment episodes (used in the physician s or medical group s cost-efficiency (ETG) analysis) attributed to the physician specialty types that are assessed for EBM rule adherence, and are assessed and ranked using the Adjusted Quality Index score. Physicians or physician groups with an Adjusted Quality Index score in the best 34% of their medical group specialty type and geographic market are placed in the best category for EBM rule adherence. Physicians or physician groups that have results in approximately the lowest 2.5%, for the medical group specialty types in the market where there are at least 20 medical groups of that medical group specialty type in the market, are placed in the bottom category. The remainder is in the middle category. A threshold is set for each market and for each medical group specialty type within a market. These thresholds are determined by specific market considerations such as geography, specialty volume, access to specialty care and contract requirements. Thresholds range from approximately 30% - 70%. The use of threshold adjustments allow for individual market factors to be taken into account; however, it is important to note that when such market-specific threshold adjustments are made, all other physician medical groups in that market with the same medical group specialty type that meets the revised market threshold value, will then be deemed to have met the quality requirement for Cigna Care designation. We do not risk adjust EBM (quality) measures because the EBM rules have explicit definitions for both the numerator and the denominator of each measure. The denominator explicitly defines the population that is at risk; thus, risk adjustment is incorporated into the definition of the measure. Cost-Efficiency Evaluation We use Episode Treatment Group (ETG) methodology, an industry standard, available through OPTUM to evaluate the cost-efficiency of individual physicians and medical groups. The methodology incorporates case-mix and severity adjustment, and claims are clustered into over 500 different episodes of care. Additional information about the OPTUMInsight Episode Treatment Groups, including a complete listing of the ETGs, is available at Using the ETG methodology, we can determine how a physician medical group s cost-efficiency compares to other physician medical groups of the same group specialty type (primary care physician group, single-specialty group, mixed specialty group, or multi-specialty group) in the same geographic market. For example, in the case of single-specialty primary care medical groups, the medical group s cost-efficiency performance is compared to the performance of other single-specialty primary care medical groups in the same market (i.e., FP medical groups are compared to other FP medical groups, IM medical groups are compared to other IM medical groups, and PD medical groups are compared to other PD medical groups). A physician or physician group s performance is a result of its fee schedule, utilization patterns and referral patterns (e.g., use of hospitals and other facilities). ETG Assessment Requirements: There must be at least 10 occurrences of a specific ETG (e.g., incorporating episode severity and treatment level, co-morbidity, complications, or the presence of Rx benefits) within the geographic market and specific physician specialty type in order to determine the market average cost for that ETG, and thus include it in the market s analysis. THN Cigna. Some content provided under license. 10
11 The peer or market average for each specific ETG is established for each market and physician specialty type. To reduce variation within cost-efficiency results, several ETGs are excluded from the assessment process, including routine immunizations and other inoculations, transplants, and ETGs with low volume or wide cost variation. Episodes with a severity level of four (the highest severity level assigned by the OPTUMInsight ETG software), are also excluded from analysis, for most conditions. Example: For the Nashville market during the data analysis period, 15 occurrences of ETG XX (with the same severity, treatment level, co-morbidity, complications, and presence of pharmacy benefits) are attributed to family physicians. The average cost of ETG XX for family physicians in the Nashville market is established by computing the numerical average of the cost of all 15 occurrences of this ETG subject to the application of outlier trimming methodology outlined in the following section. This process is replicated for each ETG with at least 10 occurrences in the Nashville market for a given physician specialty type in order to determine the market cost average for each ETG that is eligible for evaluation in the market. ETG Assessment Process: Individual physician medical groups must have at least 30 total episodes of care during the review period in order to be reviewed for cost-efficiency. In order for an episode to be attributed to a physician (responsible physician), two criteria must be met: (1) the physician must be responsible for more costs for medical or surgical management services than any other physician providing care for the episode, and (2) the medical or surgical management costs for the physician must be at least 30% of the total episode medical or surgical management costs. If these two criteria are not met, the episode is excluded from analysis. While only the costs associated with physicians provision of management services are used to attribute the episode to a particular physician, total costs (physician management costs + all ancillary costs (e.g., lab, X-ray, hospital, ambulatory surgery, physical therapy, etc.) are used to characterize the total cost of the episode. The actual cost of an episode of care for each physician group and for the physicians within that group is compared to the market average cost of an episode of care, which is derived using their unique mix of ETGs and the peer averages. The sum of all actual ETG episode costs for a medical group divided by the sum of all corresponding ETG episode market average costs is the medical group s Performance Index. Example: The ABC Physician Group consisting of three family physicians in the Nashville market has five episodes of care belonging to two unique ETGs (ETG1 and ETG2) that are attributable to the group. For the sake of simplicity, disregard for the purpose of this example the requirement that the physician or physician group must have a minimum of 30 attributable episodes in order to be reviewed for cost- efficiency. Average episode costs for ETG1 and ETG2 have been established for all other primary care physicians or groups practicing in the Nashville market. Three episodes of ETG1 are attributable to the ABC Physician Group and two episodes of ETG2 are attributable to the ABC Physician Group. THN Cigna. Some content provided under license. 11
12 In the table below, the physician group s cost per episode is displayed for each of the three occurrences of ETG1 and for each of the two occurrences of ETG2, along with the market average cost for an episode for ETG1 and ETG2 for all family physicians in the Nashville Market. Actual Episode Cost Market Average Cost ETG ETG ETG ETG 2 15,000 19,000 ETG 2 18,000 19,000 Average 8,000 9,700 Performance Index = 8,000/9,700 = Dividing the average cost of all episodes of care attributable to the physician group by the average of all market average episode costs for the ETGs on which the physician group s cost-efficiency performance is being evaluated yields a Performance Index (PI) of The PI for the medical group can be interpreted as Medical Group ABC is 17.5% more cost-efficient than other family medicine physician medical groups in the Nashville market. A 90% Confidence Interval around the Performance Index is used to determine a range of performance within which the medical group s true performance would fall with a high level of confidence. The upper bound of the confidence interval is defined as the Adjusted Performance Index and is used to compare cost-efficiency performance among physician medical groups. The upper bound of the 90% confidence interval is used in order to ensure that the medical group s performance is at least as good as or better than the upper bound threshold. A threshold is set for each market and for each medical group specialty type within a market. These thresholds are determined by specific market considerations such as geography, specialty volume, access to specialty care and contract requirements. Thresholds range from approximately 30% - 70%. The use of threshold adjustments allows for individual market factors to be taken into account; however, it is important to note that when such market-specific threshold adjustments are made, all other physician medical groups in that market of the same medical group specialty type that also meet the revised market threshold value, will then be deemed to have met the cost-efficiency requirement for Cigna Care designation. Physician groups in the same medical group specialty type that meet Cigna board certification criteria and Cigna minimum volume of 30 episodes of care are ranked using the (cost-efficiency) Adjusted Performance Index score. Those groups with an Adjusted Performance Index score in the top 40% of their respective medical group specialty type and market are placed in the top category for cost-efficiency and consequently meet the cost-efficiency component requirement for Cigna Care designation (provided they score in the top 40% for quality). To qualify for CCD based on cost alone, medical groups must score in the top 34% of their respective medical group specialty type and market.) 2015 and 2016 Outlier Methodology In order to portray physicians cost-efficiency performance in the most accurate manner, the cost-efficiency evaluation includes a methodology to account for episodes that are outliers. Outliers are episodes that are substantially different from the market expected amounts. High cost episodes (ETGs) that are greater than 1.5 times the market specialty averages are reduced to 1.5 times the market specialty average. Low cost outlier episodes are determined by the OPTUM software or are episodes of less than $25.00 and are excluded from the evaluation. THN Cigna. Some content provided under license. 12
13 Level of Evaluation (Unit of Analysis) While we review participating physicians at the individual level, the majority of assessments are performed at the physician group or practice, or group tax identification number level. Individual physicians who are not part of a group are assessed if volume criteria are met. This approach provides robust data for evaluation and is consistent with the assumption that: Patients with Cigna-administered coverage often chose a group rather than a specific physician within the group, and; Patients with Cigna-administered coverage who initially choose a specific physician frequently receive care by another physician within the practice or group. Assigning the Cigna Care Designation (2015 and 2016 CCD Inclusion Methodology) In order to receive the Cigna Care designation, a physician must qualify on the basis of both medical group specialty quality and cost-efficiency OR be ranked in the top 34% for quality or cost-efficiency of an eligible medical group specialty within his/her geographic market for cost-efficiency. The details of the Cigna Care Designation assignment logic are outlined below and are displayed in the diagram on page 14. To be considered for Cigna Care Designation, physicians must be MDs and/or DOs in one of 18 non- primary care specialties or one of three primary care specialties. Note: Cigna performs its evaluations at the group level. Some groups include geriatric physicians, nurse practitioners, and physician assistants who deliver primary care services as part of the group. In such cases, geriatric physicians, nurse practitioners, and physician assistants will be considered for Cigna Care designation as part of the group. Physicians must meet a board certification requirement. For medical groups, this standard is met if: o either 80% of physicians within a group are board certified and provide 50% of the care, or at least 80% of the care is provided by board certified physicians, OR o for practices/groups with 4 or less physicians, either 65% of physicians within a group are board certified and provide 50% of the care, or at least 65% of the care is provided by board certified physicians The physician practice must have at least 30 evidence-based medicine (EBM) opportunities during the data collection period and at least 50% of the total care provided by the practice must be provided by physicians for whom there are applicable EBM rules. A Quality Index and Adjusted Quality Index are calculated for each practice. Physician practices are assigned to one of three quality categories based on the Adjusted Quality Index: top 34% of practices in the market for the practice s group specialty type; bottom 2.5% of practices in the market for the practice group specialty type; middle 2.5% to 66% of practices in the market for the practice s group specialty type. Practices in the Top 34% of Practices for Quality Based on EBM Assessment: If the Adjusted Quality Index for the practice is in the top 34% of all physician practices in the geographic market of the same physician group specialty type OR if the group has 50% or more of their physicians recognized in one of the six NCQA recognition programs, the practice meets the CCD quality requirement and is then evaluated on its cost-efficiency. THN Cigna. Some content provided under license. 13
14 The practice must have at least 30 episodes available for ETG assessment during the data collection period. A practice Performance Index and a practice Adjusted Performance Index are calculated. If the practice Adjusted Performance Index shows the practice is in the top 40% of all practices of the same group specialty type in the geographic market, the practice is awarded Cigna Care designation. Practices in the Middle Category (2.5% - 66%) for Quality Based on EBM Assessment: If the Adjusted Quality Index for the practice is in the middle category (2.5% - 66%) of all physician practices in the geographic market of the same specialty physician group specialty type, the practice is evaluated to determine if it is in the top 34% of all practices for cost-efficiency. The practice must have at least 30 episodes available for ETG assessment during the data collection period. A practice Performance Index and a practice Adjusted Performance Index are calculated. If the practice Adjusted Performance Index shows the practice is in the top 34% of all practices of the same group specialty type in the geographic market, the practice is awarded Cigna Care designation. Practices in the Bottom 2.5% for Quality Based on EBM Assessment: If the Adjusted Quality Index for the practice is in the bottom 2.5% of all physician practices in the geographic market of the same physician group specialty type, the practice, if it is a medical group, is excluded from Cigna Care designation. Note: Practices are only assigned to the bottom 2.5% in quality performance if there are at least 20 or more quality ranked groups in a specific geographic market. Practices Having Insufficient Volume to Assess Quality Based on EBM Assessment: If the practice has an insufficient volume of EBM opportunities (less than 30) in order to be assessed for quality based on EBM rule adherence, the practice is assessed to determine if it has at least 30 episodes eligible for ETG assessment. If it meets the 30-episode criterion and the calculated practice Adjusted Performance Index is in the top 34% of all practices of the same physician group specialty type in the geographic market, the practice is awarded Cigna Care designation. If the practice has an insufficient volume of EBM opportunities in order to be assessed for quality based on EBM rule adherence, the practice is assessed to determine if it has at least 30 episodes eligible for ETG assessment. If it meets the 30-episode criterion and the calculated Practice Adjusted Performance Index is NOT in the top 34% of all practices of the same group specialty type in the geographic market, the practice is excluded from Cigna Care designation. Practices Having Insufficient Volume to Assess Cost Based on ETG Assessment: If the practice has an insufficient volume of ETG opportunities (less than 30) for cost profiling but has a sufficient number of EBM opportunities (at least 30) for quality profiling or meets the NCQA recognition criterion, the practice is eligible for CCD designation through a quality-only pathway. If the Adjusted Quality Index of the practice places it within the top 34% of practices of the same group specialty type in the same geographic market, the practice is awarded Cigna Care designation. THN Cigna. Some content provided under license. 14
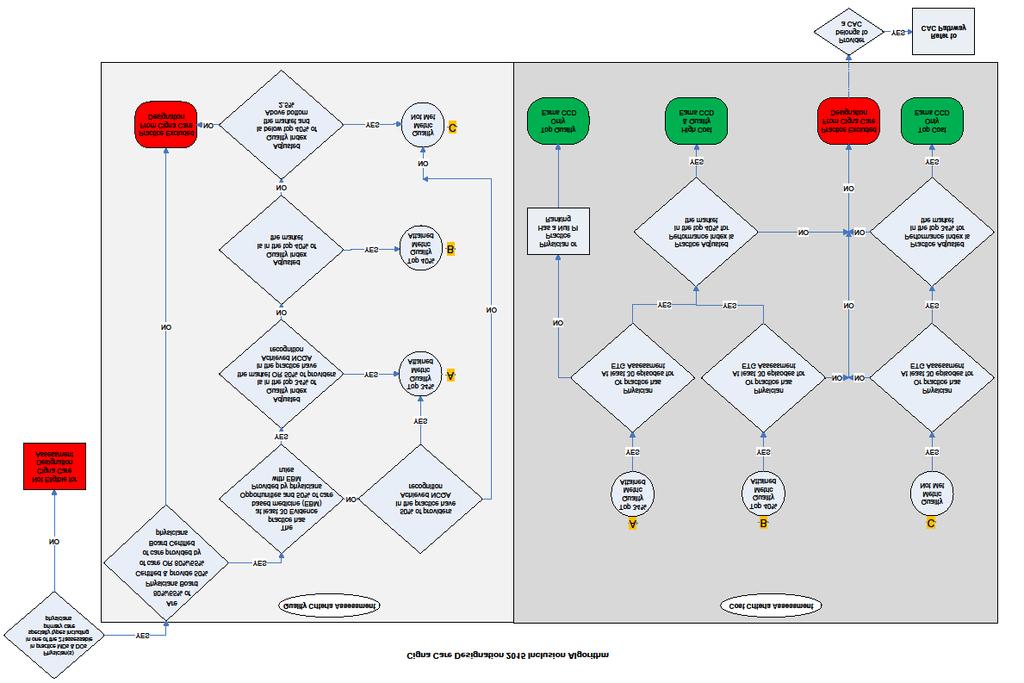
15 15
16 Buffer Zone Methodology Variation in physician group or physician group performance (e.g., positive or negative, substantial, or minimal) is inevitable and expected in an annual review process due to various factors (e.g., changes to physician group makeup, external market factors, and practice pattern modifications). A buffer zone methodology addresses small-scale variation for physician groups or physician groups whose Cigna Care designation changes from the previous review cycle. A practice may maintain its Cigna Care designation status if the group was designated during the prior cycle, is within 3% of the current year's quality AND cost criteria, OR is within 3% of the cost index when the group does not meet cost and quality criteria. The selected physician group must meet certain standard Cigna Care designation criteria to achieve the 2015 and 2016 buffer zone designation. The standard criteria applied includes meeting the physician group Board Certification criteria, the Board Certified physicians must be responsible for at least 50% of the group episodes, the group must have at least 30 episodes, and the group must not be in the bottom 2.5 market percentile for EBM quality performance in a market with greater than 20 groups within the specialty category in the market. Collaborative Accountable Care Pathway to Achieving Cigna Care Designation CAC to CCD Pathway Cigna has teamed up with selected physician groups in order to help them achieve the triple aim of improving quality, improving cost-effectiveness and improving the patient experience of care. This is called the Cigna Collaborative Accountable Care (CAC) model. Cigna's approach builds upon the foundation of Accountable Care Organizations (ACOs) and Patient Centered Medical Home (PCMH) models by recognizing physicians affiliated with the CACs that demonstrate improvement in medical delivery and clinical outcomes and achieve improvement in reducing the cost of care. Cigna's approach is to work with physicians to provide them with resource support and data that can help them deliver optimal care. This support can include data about ER visits, hospitalizations, potential gaps in care, medication compliance, etc., which the physician might not otherwise have access to, and which can support the physician in optimal management of care delivery across multiple settings. This support can also focus on chronically ill patients by working with nurses who are part of the group practice, to provide them with information and tools to help them manage these patients and coordinate case management and educational support when needed. Cigna's CAC model is designed for collaboration with large physician groups that may or may not include specialists. These groups must meet volume thresholds for physicians and Cigna customers, as well as other minimum criteria. The groups enter into a contract with Cigna in which they agree to be evaluated based on quality and cost criteria that are unique to the CAC model. The 2015 profiles will remain in effect until December 31, Physicians and physician groups are first assessed by applying the standard CCD pathway to determine inclusion. If the physicians and physician groups were unable to achieve designation through the standard CCD pathway described previously in this white paper but they are affiliated with the CAC, then the CAC pathway inclusion criteria may be applied next to determine if they can be designated. The CAC achieving a Total Medical Cost Performance Index of less than or equal to 1.03 AND a CAC Quality Index of greater than or equal to 0.99 will be assigned the Cigna Care designation. Specialists that are affiliated with a CAC that meet the CCD criteria for inclusion and the markets determine the specialists are to be included with the CAC; the specialists will be assigned designation. THN Cigna. Some content provided under license. 16
17 To be considered for Cigna Care designation, CAC physicians must be MDs and/or DOs in one of three primary care specialties or one of 18 non-primary care specialties. Note: Cigna performs its evaluations at the group level. Some groups include geriatric physicians, nurse practitioners, and physician assistants who deliver primary care services as part of the group. In such cases, geriatric physicians, nurse practitioners, and physician assistants will be considered for Cigna Care designation as part of the group. Quality Assessment The CAC must have at least 30 evidence-based medicine (EBM) opportunities during the data collection period. A Quality Index is calculated for each CAC based on adherence to Evidence Based Medicine (EBM) measures. If the CAC s Quality Index is 0.99 or better, the quality requirement is met. Cost-Efficiency Assessment To contract with Cigna as a CAC, a minimum volume of Cigna customers is required so there is sufficient volume for cost evaluation. Based on 2014 data, this results in episode counts ranging from 8,600 to 131,000 episodes per group, per year. Total Medical Cost (TMC) is used to evaluate cost-efficiency for CAC arrangements. A Total Medical Cost Performance Index (PI) is calculated. If the group's TMC Performance Index is 1.03 or less, the practice meets the CCD cost requirement for CCD. The Quality Index and Total Medical Cost Index are calculated as follows: Quality Index The Quality Index is calculated based on adherence to Evidence Based Medicine (EBM) standards, and EBM rules for CACs are the same as those described for primary care specialties in the section titled "Evidence-Based Medicine (EBM) Assessment Process" which appears on pages 7-10 of this paper. Determining CAC EBM rule adherence: Opportunities and successes for each eligible EBM rule are aligned to the appropriate individual physician (using the visit requirements outlined below and relevant specialty type category). Visit Requirements - A physician is considered responsible for adherence to the EBM rule if the following conditions are met: The EBM rule is relevant to the physician s primary care specialty (see Appendix 3). For example, the Cervical Dysplasia EBM rule is relevant to OB/GYN,, and, but it is not relevant to other specialties. There have been at least two office visit encounters for a Cigna customer At least one of the office visit encounters occurred in the last 12 months of the claim review period. Note: Nineteen of our EBM measures require only one office visit encounter in the last 12 months of the claim review period. These measures are identified by an asterisk [*] in Appendix 3. Individual physicians are aligned to the CAC, and EBM rule opportunities, successes, and expected successes are then summed to obtain CAC totals. A Quality Index for the CAC is calculated by dividing the number of actual EBM rule adherence successes for the CAC by number of expected EBM rule adherence successes. Expected EBM rule adherence successes are derived by applying the geographic market average EBM rule adherence success rates from primary care groups in the market. Total Medical Cost Index The Total Medical Cost index reflects all medical costs for Cigna customers who are aligned to PCPs in the CAC, excluding pharmacy and non-pcp behavioral health costs. THN Cigna. Some content provided under license. 17
18 For the CAC model, Cigna maintains a roster of all Cigna customers who are patients of the CAC. Patients are aligned to a specific PCP if they have had at least one visit in the prior 12 months. If no visit is found, the look back period is 24 months and the patient is aligned to the PCP with the most recent visits. When there are no visits to PCPs in 24 months, then the same search is conducted for Nurse Practitioners, Physicians Assistants and OB/GYN physicians in the group. If a patient was seen by more than one primary care practitioner in the CAC, the patient is aligned to the practitioner with the most visits. Once the aligned patients and practitioners are identified, the Total Medical Cost is calculated as follows: Capture all claims expenses (excluding pharmacy expense) for patients who are aligned to the CAC PCPs for the 12-month reporting period. Pharmacy costs today are not included in TMC calculation. Calculate member months for all aligned patients of the CAC and the market. Calculate an Episode Risk score using Episode Risk Grouper (ERG) software for both the market and the CAC. Additional information about the OPTUMInsight Episode Risk Grouper software is available at Calculate total medical cost for all aligned patients of the CAC. Outliers are identified and outlier claim expense is capped at $100,000. Calculate per Patient per Month (PPPM) expenses for both the market and the CAC practice. (PPPM is calculated by dividing the total medical cost by member months). Adjust the CAC PPPM to consider to ERG risk score for patients of the CAC. Divide the final risk adjusted CAC PPPM score by the market PPPM score to create the TMC performance index. When the CAC adjusted expense is the same as the market, the result will be 1.0. A TMC Performance Index of less than 1.0 reflects that claim expenses are lower than the market average and a TMC performance index of greater than 1.0 reflects that claim expenses are higher than the market average. Buffer Zone Methodology Variation in CAC performance (e.g., positive or negative, substantial, or minimal) is inevitable and expected in an annual review process due to various factors (e.g., changes to physician group makeup, external market factors, and practice pattern modifications). A buffer zone or grandfathering methodology addresses variation for physician groups or physician groups whose Cigna Care designation changes from the previous review cycle. A CAC may maintain its Cigna Care designation status if the CAC was in during the prior cycle. NOTE: Individual markets may adjust the grandfathering criteria for CACs at the market level, in order to exclude from grandfathering those CACs with large-scale variation in results from the prior year. Adjustments are made at the market level and are applied to all CACs in the market. Collaborative Accountable Care (CAC) Review Process The evaluation methodology is applied annually (and quarterly as needed) to all existing CAC arrangements and to new CACs that become effective. CACs that do not meet criteria can be re-evaluated using quarterly data, through our reconsideration process. If the quality and performance indexes improve and are meeting the market criteria for inclusion during two consecutive quarters, the CAC will be given Cigna Care Designation status. THN Cigna. Some content provided under license. 18

19 Since CACs can earn CCD status on a quarterly basis, Cigna reserves the right to remove the CCD status if the CAC demonstrates significant decline in performance below the required criteria in four consecutive quarters, or if the CAC discontinues it collaborative agreement with Cigna and does not meet the standard CCD criteria. A re-evaluation occurs annually where grandfathering may be applied. As noted above, individual markets may adjust the grandfathering criteria at the market level. When adjustments are made at the market level, they are applied to all CACs in the market. THN Cigna. Some content provided under license. 19
2019 QUALITY, COST EFFICIENCY, AND CIGNA CARE DESIGNATION METHODOLOGY
 2019 QUALITY, COST EFFICIENCY, AND CIGNA CARE DESIGNATION METHODOLOGY For physicians and physician groups June 2018 Table of contents Introduction... 3 Cigna quality and cost-efficiency display principles...
2019 QUALITY, COST EFFICIENCY, AND CIGNA CARE DESIGNATION METHODOLOGY For physicians and physician groups June 2018 Table of contents Introduction... 3 Cigna quality and cost-efficiency display principles...
The BlueCompare SM Physician Designation Program
 The BlueCompare SM Physician Designation Program Continuing escalation of health care costs has driven premiums and medical expenses to higher and higher levels each year, motivating employers and consumers
The BlueCompare SM Physician Designation Program Continuing escalation of health care costs has driven premiums and medical expenses to higher and higher levels each year, motivating employers and consumers
Anthem Blue Precision Quality Designation Methodology Summary 2017
 This document outlines Anthem s Blue Precision methodology for measuring Physician Quality. Anthem has physician quality transparency programs for physicians practicing in the following specialties: Allergy/Immunology,
This document outlines Anthem s Blue Precision methodology for measuring Physician Quality. Anthem has physician quality transparency programs for physicians practicing in the following specialties: Allergy/Immunology,
UnitedHealth Premium Physician Designation Program Episode Treatment Groups (ETG ) Description and Specialty
 Description and Specialty") UnitedHealth Premium Physician Designation Program Episode Treatment Groups (ETG ) Description and Specialty 666700 Acne Family Medicine, Internal Medicine, Pediatrics 438300 Acute Bronchitis Allergy,
UnitedHealth Premium Physician Designation Program Episode Treatment Groups (ETG ) Description and Specialty 666700 Acne Family Medicine, Internal Medicine, Pediatrics 438300 Acute Bronchitis Allergy,
TN Bundled Payment Initiative: Overview of Episode Risk Adjustment
 TN Bundled Payment Initiative: Overview of Episode Risk Adjustment United Healthcare, April 2014 The State of Tennessee has implemented an episode-based approach to reimburse providers for the care delivered
TN Bundled Payment Initiative: Overview of Episode Risk Adjustment United Healthcare, April 2014 The State of Tennessee has implemented an episode-based approach to reimburse providers for the care delivered
Highmark s Physician Pay for Performance Program
 Highmark s Physician Pay for Performance Program Pay for Performance Summit February 20, 2013 Julie A. Hobson R.N., B.S.N. Manager Provider Engagement, Performance and Partnership Highmark Inc. Overview
Highmark s Physician Pay for Performance Program Pay for Performance Summit February 20, 2013 Julie A. Hobson R.N., B.S.N. Manager Provider Engagement, Performance and Partnership Highmark Inc. Overview
Trends in Health Plan Design: High Performance Networks. John Bertko, F.S.A., MAAA Vice President and Chief Actuary Humana Inc July 28, 2005
 Trends in Health Plan Design: High Performance Networks John Bertko, F.S.A., MAAA Vice President and Chief Actuary Humana Inc July 28, 2005 1 Overview What is a High Performance Network (HPN) Tighter network
Trends in Health Plan Design: High Performance Networks John Bertko, F.S.A., MAAA Vice President and Chief Actuary Humana Inc July 28, 2005 1 Overview What is a High Performance Network (HPN) Tighter network
TENNCARE Bundled Payment Initiative: Description of Bundle Risk Adjustment for Wave 4 Episodes
 TENNCARE Bundled Payment Initiative: Description of Bundle Risk Adjustment for Wave 4 Episodes Attention deficit hyperactivity disorder (ADHD); Opposition defiance disorder (ODD); Coronary artery bypass
TENNCARE Bundled Payment Initiative: Description of Bundle Risk Adjustment for Wave 4 Episodes Attention deficit hyperactivity disorder (ADHD); Opposition defiance disorder (ODD); Coronary artery bypass
NCQA Health Insurance Plan Ratings Methodology October 2014
 NCQA Health Insurance Plan Ratings Methodology October 2014 REVISION CHART Date Published December 2013 April 2014 October 2014 Description Draft version Final version Updated measure list with 50% rule
NCQA Health Insurance Plan Ratings Methodology October 2014 REVISION CHART Date Published December 2013 April 2014 October 2014 Description Draft version Final version Updated measure list with 50% rule
Impact of WRVU Changes. Allowed Charges (Millions)
") Key Financial and Operational s from the Proposed 2018 PFS Rule: The 2018 Physician Fee Schedule (PFS) proposed rule was made available on July 13, 2018. A detailed summary of the rule will be available
Key Financial and Operational s from the Proposed 2018 PFS Rule: The 2018 Physician Fee Schedule (PFS) proposed rule was made available on July 13, 2018. A detailed summary of the rule will be available
What Does Walt Disney Have To Do With Heath Care: The Importance of Quality, Reliability, and Engaged Physicians
 What Does Walt Disney Have To Do With Heath Care: The Importance of Quality, Reliability, and Engaged Physicians Scott Hines, MD Chief Quality Officer Crystal Run Healthcare October 22, 2015 Learning Objectives
What Does Walt Disney Have To Do With Heath Care: The Importance of Quality, Reliability, and Engaged Physicians Scott Hines, MD Chief Quality Officer Crystal Run Healthcare October 22, 2015 Learning Objectives
MEASURING CARE QUALITY
 MEASURING CARE QUALITY Region December 2013 For Clinical Effectiveness of Care Measures of Performance From: Healthcare Effectiveness Data and Information Set (HEDIS ) HEDIS is a set of standardized performance
MEASURING CARE QUALITY Region December 2013 For Clinical Effectiveness of Care Measures of Performance From: Healthcare Effectiveness Data and Information Set (HEDIS ) HEDIS is a set of standardized performance
Affordability AMGA - MIPS Webinar
 Affordability AMGA - MIPS Webinar Beth Averbeck, MD Senior Medical Director Primary Care, HealthPartners Consumer-governed, non-profit HealthPartners Medical Group Primary Care: 500,000 patients 29 locations
Affordability AMGA - MIPS Webinar Beth Averbeck, MD Senior Medical Director Primary Care, HealthPartners Consumer-governed, non-profit HealthPartners Medical Group Primary Care: 500,000 patients 29 locations
TN Bundled Payment Initiative: Overview of Episode Risk Adjustment
 TN Bundled Payment Initiative: Overview of Episode Risk Adjustment Amerigroup, April 2014 The State of Tennessee has implemented an episode-based approach to reimburse providers for the care delivered
TN Bundled Payment Initiative: Overview of Episode Risk Adjustment Amerigroup, April 2014 The State of Tennessee has implemented an episode-based approach to reimburse providers for the care delivered
Letter to the AMGA Board of Directors...1 Introduction...3
 Table of Contents Letter to the AMGA Board of Directors...1 Introduction...3 Section I: Executive Summary Survey at a Glance...6 Participant Profile...10 Survey Methodology...18 How to Use This Report...21
Table of Contents Letter to the AMGA Board of Directors...1 Introduction...3 Section I: Executive Summary Survey at a Glance...6 Participant Profile...10 Survey Methodology...18 How to Use This Report...21
Combining Risk Adjustment and HEDIS to Improve Quality of Care. Colleen Gianatasio, CPC, CPC-P, CPMA, CPC-I, CRC
 Combining Risk Adjustment and HEDIS to Improve Quality of Care Colleen Gianatasio, CPC, CPC-P, CPMA, CPC-I, CRC Agenda Improving primary care in today s health care environment Risk adjustment basics (using
Combining Risk Adjustment and HEDIS to Improve Quality of Care Colleen Gianatasio, CPC, CPC-P, CPMA, CPC-I, CRC Agenda Improving primary care in today s health care environment Risk adjustment basics (using
UnitedHealth Premium Program Case-mix Adjusted Benchmarks with Severity or Risk Adjustment
 UnitedHealth Premium Program Case-mix Adjusted Benchmarks with Severity or Risk Adjustment Resources u Phone: 866-270-5588 u u Website: UHCprovider.com/Premium Mail: UnitedHealthcare - UnitedHealth Premium
UnitedHealth Premium Program Case-mix Adjusted Benchmarks with Severity or Risk Adjustment Resources u Phone: 866-270-5588 u u Website: UHCprovider.com/Premium Mail: UnitedHealthcare - UnitedHealth Premium
TENNCARE Bundled Payment Initiative: Description of Bundle Risk Adjustment for Wave 3 Episodes
 TENNCARE Bundled Payment Initiative: Description of Bundle Risk Adjustment for Wave 3 Episodes Respiratory Infection (RI); Pneumonia (PNA); Inpatient Urinary Tract Infection (UTI-I; Outpatient Urinary
TENNCARE Bundled Payment Initiative: Description of Bundle Risk Adjustment for Wave 3 Episodes Respiratory Infection (RI); Pneumonia (PNA); Inpatient Urinary Tract Infection (UTI-I; Outpatient Urinary
2018 MIPS Reporting Family Medicine
 2018 MIPS Reporting Family Medicine Quality Reporting Requirements: Report on 6 quality measures or a specialty measure set Include at least ONE outcome or high-priority measure Report on patients of All-Payers
2018 MIPS Reporting Family Medicine Quality Reporting Requirements: Report on 6 quality measures or a specialty measure set Include at least ONE outcome or high-priority measure Report on patients of All-Payers
HEDIS/CAHPS 101 August 13, 2012 Minnesota Measurement and Reporting Workgroup
 HEDIS/CAHPS 101 Minnesota Measurement and Reporting Workgroup MNsure s Accessibility & Equal Opportunity (AEO) office can provide this information in accessible formats for individuals with disabilities.
HEDIS/CAHPS 101 Minnesota Measurement and Reporting Workgroup MNsure s Accessibility & Equal Opportunity (AEO) office can provide this information in accessible formats for individuals with disabilities.
Letter to the AMGA Board of Directors... 1 Introduction... 3
 Table of Contents Letter to the AMGA Board of Directors... 1 Introduction... 3 Section I: Executive Summary Survey at a Glance... 6 Participant Profile... 10 Survey Methodology... 19 How to Use This Report...
Table of Contents Letter to the AMGA Board of Directors... 1 Introduction... 3 Section I: Executive Summary Survey at a Glance... 6 Participant Profile... 10 Survey Methodology... 19 How to Use This Report...
Supplementary Online Content
 Supplementary Online Content Friedberg MW, Rosenthal MB, Werner RM, Volpp KG, Schneider EC. Effects of a medical home and shared savings intervention on quality and utilization of care. Published online
Supplementary Online Content Friedberg MW, Rosenthal MB, Werner RM, Volpp KG, Schneider EC. Effects of a medical home and shared savings intervention on quality and utilization of care. Published online
Letter to the AMGA Board of Directors...1 Introduction...3
 Table of Contents Letter to the AMGA Board of Directors...1 Introduction...3 Section I: Executive Summary Survey at a Glance...6 Participant Profile...10 Survey Methodology...18 How to Use This Report...21
Table of Contents Letter to the AMGA Board of Directors...1 Introduction...3 Section I: Executive Summary Survey at a Glance...6 Participant Profile...10 Survey Methodology...18 How to Use This Report...21
TENNCARE Bundled Payment Initiative: Description of Bundle Risk Adjustment for Wave 5 Episodes
 TENNCARE Bundled Payment Initiative: Description of Bundle Risk Adjustment for Wave 5 Episodes Mastectomy, Breast Cancer Medical Oncology, Breast Biopsy, Tonsillectomy, Otitis media, Anxiety, Non-emergent
TENNCARE Bundled Payment Initiative: Description of Bundle Risk Adjustment for Wave 5 Episodes Mastectomy, Breast Cancer Medical Oncology, Breast Biopsy, Tonsillectomy, Otitis media, Anxiety, Non-emergent
Arkansas Blue Cross and Blue Shield (ABCBS) Patient Centered Medical Home (PCMH) Specifications Manual
 Patient Centered Medical Home (PCMH) Specifications Manual") Arkansas Blue Cross and Blue Shield (ABCBS) Patient Centered Medical Home (PCMH) Specifications Manual 2017 This document is a guide to the 2017 Arkansas Blue Cross and Blue Shield Patient-Centered Medical
Arkansas Blue Cross and Blue Shield (ABCBS) Patient Centered Medical Home (PCMH) Specifications Manual 2017 This document is a guide to the 2017 Arkansas Blue Cross and Blue Shield Patient-Centered Medical
2017 Chronic Respiratory. Program Evaluation. Our mission is to improve the health and quality of life of our members
 2017 Chronic Respiratory Program Evaluation Our mission is to improve the health and quality of life of our members 2017 Chronic Respiratory Program Evaluation Program Title: Chronic Respiratory Program
2017 Chronic Respiratory Program Evaluation Our mission is to improve the health and quality of life of our members 2017 Chronic Respiratory Program Evaluation Program Title: Chronic Respiratory Program
Letter to the AMGA Board of Directors... 1 Introduction... 3
 Table of Contents Letter to the AMGA Board of Directors... 1 Introduction... 3 Section I: Executive Summary Survey at a Glance... 6 Participant Profile... 10 Survey Methodology... 19 How to Use This Report...
Table of Contents Letter to the AMGA Board of Directors... 1 Introduction... 3 Section I: Executive Summary Survey at a Glance... 6 Participant Profile... 10 Survey Methodology... 19 How to Use This Report...
Utility of Social Networks For Physicians and Life Sciences Companies. January 2011
 Utility of Social Networks For Physicians and Life Sciences Companies January 2011 What is Sermo? Largest online physician community 117,000+ members (1 in 5 practicing US physicians) All physicians are
Utility of Social Networks For Physicians and Life Sciences Companies January 2011 What is Sermo? Largest online physician community 117,000+ members (1 in 5 practicing US physicians) All physicians are
UnitedHealth Premium Designation Program Case-mix Adjusted Benchmarks with Severity or Risk Adjustment
 UnitedHealth Premium Designation Program Case-mix Adjusted Benchmarks with Severity or Risk Adjustment Resources u Phone: 866-270-5588 u u u Website: UnitedHealthcareOnline.com > Quick Links > UnitedHealth
UnitedHealth Premium Designation Program Case-mix Adjusted Benchmarks with Severity or Risk Adjustment Resources u Phone: 866-270-5588 u u u Website: UnitedHealthcareOnline.com > Quick Links > UnitedHealth
Premium Specialty: Pediatrics
 Premium Specialty: Pediatrics Credentialed Specialties include: Adolescent Medicine, Pediatric Adolescent, and Pediatrics This document is designed to be used in conjunction with the UnitedHealth Premium
Premium Specialty: Pediatrics Credentialed Specialties include: Adolescent Medicine, Pediatric Adolescent, and Pediatrics This document is designed to be used in conjunction with the UnitedHealth Premium
Aexcel. Specialist Designation in Aetna Performance Network. Methodology Guide
 Aexcel Specialist Designation in Aetna Performance Network Methodology Guide Aexcel 2009 TABLE OF CONTENTS Background on Aexcel Performance Networks... 3 Clinical Performance Evaluation Process... 8 General
Aexcel Specialist Designation in Aetna Performance Network Methodology Guide Aexcel 2009 TABLE OF CONTENTS Background on Aexcel Performance Networks... 3 Clinical Performance Evaluation Process... 8 General
CFO Council. Physician Compensation Trends. Survey Challenges
 CFO Council Physician Compensation Trends 1 Survey Challenges Many healthcare organizations use surveys in their compensation plans. Some to set specific targets and benchmarks and others to determine
CFO Council Physician Compensation Trends 1 Survey Challenges Many healthcare organizations use surveys in their compensation plans. Some to set specific targets and benchmarks and others to determine
MEASURING CARE QUALITY
 MEASURING CARE QUALITY Region November 2016 For Clinical Effectiveness of Care Measures of Performance From: Healthcare Effectiveness Data and Information Set (HEDIS ) HEDIS is a set of standardized performance
MEASURING CARE QUALITY Region November 2016 For Clinical Effectiveness of Care Measures of Performance From: Healthcare Effectiveness Data and Information Set (HEDIS ) HEDIS is a set of standardized performance
Boosting the Value of Lab Testing: How HEDIS Uses Lab
 Boosting the Value of Lab Testing: How HEDIS Uses Lab Cindy Ottone, MHA Director HEDIS Policy All materials 2009, National Committee for Quality Assurance Overview What is NCQA and HEDIS? How are measures
Boosting the Value of Lab Testing: How HEDIS Uses Lab Cindy Ottone, MHA Director HEDIS Policy All materials 2009, National Committee for Quality Assurance Overview What is NCQA and HEDIS? How are measures
NORTH CAROLINA STATE HEALTH PLAN FOR TEACHERS AND STATE EMPLOYEES
 NORTH CAROLINA STATE HEALTH PLAN FOR TEACHERS AND STATE EMPLOYEES Using Clinical Risk Groups to Focus Board Strategic Initiatives July 26, 2013 Copyright 2013 by The Segal Group, Inc., parent of The Segal
NORTH CAROLINA STATE HEALTH PLAN FOR TEACHERS AND STATE EMPLOYEES Using Clinical Risk Groups to Focus Board Strategic Initiatives July 26, 2013 Copyright 2013 by The Segal Group, Inc., parent of The Segal
Commercial Business Measurement Period Handbook-Medical Cost Target Model For Enhanced Personal Health Care Measurement Period beginning: 01/1/17
 Commercial Business Measurement Period Handbook-Medical Cost Target Model For Enhanced Personal Health Care Measurement Period beginning: 01/1/17 CBMCT Version 010117 V3 Introduction: Welcome to your Commercial
Commercial Business Measurement Period Handbook-Medical Cost Target Model For Enhanced Personal Health Care Measurement Period beginning: 01/1/17 CBMCT Version 010117 V3 Introduction: Welcome to your Commercial
Provider Perspective of Quality Measurement
 Provider Perspective of Quality Measurement The American Medical Group Association supports its members in enhancing population health and care for patients through integrated systems of care Improve
Provider Perspective of Quality Measurement The American Medical Group Association supports its members in enhancing population health and care for patients through integrated systems of care Improve
Physician Profile. Revised For January 1, 2005 December 31, 2007
 Physician Profile Revised For January 1, 2005 December 31, 2007 Contents Physician Profile Overview... 3 Sub-specialty Definitions... 4 Cost of Care... 5 Definitions... 5 Notes... 5 Cost Comparison Report
Physician Profile Revised For January 1, 2005 December 31, 2007 Contents Physician Profile Overview... 3 Sub-specialty Definitions... 4 Cost of Care... 5 Definitions... 5 Notes... 5 Cost Comparison Report
TENNCARE Bundled Payment Initiative: Description of Bundle Risk Adjustment for Wave 8 Episodes
 TENNCARE Bundled Payment Initiative: Description of Bundle Risk Adjustment for Wave 8 Episodes Acute Seizure, Syncope, Acute Gastroenteritis, Pediatric Pneumonia, Bronchiolitis, Colposcopy, Hysterectomy,
TENNCARE Bundled Payment Initiative: Description of Bundle Risk Adjustment for Wave 8 Episodes Acute Seizure, Syncope, Acute Gastroenteritis, Pediatric Pneumonia, Bronchiolitis, Colposcopy, Hysterectomy,
SUMMARY TABLE OF MEASURES, PRODUCT LINES AND CHANGES
 Summary Table of Measures, Product Lines and Changes 1 SUMMARY TABLE OF MEASURES, PRODUCT LINES AND CHANGES General Guidelines for Data Collection and Reporting Guidelines for Calculations and Sampling
Summary Table of Measures, Product Lines and Changes 1 SUMMARY TABLE OF MEASURES, PRODUCT LINES AND CHANGES General Guidelines for Data Collection and Reporting Guidelines for Calculations and Sampling
Table 1 ABMS MEMBER BOARDS APPROVED GENERAL CERTIFICATES
 Table 1 ABMS MEMBER BOARDS APPROVED GENERAL CERTIFICATES A general certificate is the first certification awarded by a Member Board to candidates who meet the requirements for board certification in a
Table 1 ABMS MEMBER BOARDS APPROVED GENERAL CERTIFICATES A general certificate is the first certification awarded by a Member Board to candidates who meet the requirements for board certification in a
Consultant Services to Kansas Family Physicians
 Consultant Services to Kansas Family Physicians The purpose of this study is to track the use of consultants. An e-mail survey was sent to 114 Kansas family physicians The survey was launched on 11/25/2009
Consultant Services to Kansas Family Physicians The purpose of this study is to track the use of consultants. An e-mail survey was sent to 114 Kansas family physicians The survey was launched on 11/25/2009
Preferred Care Partners. HEDIS Technical Standards
 Preferred Care Partners HEDIS Technical Standards 1 HEDIS What is HEDIS HEDIS Overview Adults HEDIS Overview Pediatrics HEDIS is a registered trademark of the National Committee for Quality Assurance 2
Preferred Care Partners HEDIS Technical Standards 1 HEDIS What is HEDIS HEDIS Overview Adults HEDIS Overview Pediatrics HEDIS is a registered trademark of the National Committee for Quality Assurance 2
Integration of Specialty Care into ACOs: Considering JMAP and Beyond
 Integration of Specialty Care into ACOs: Considering JMAP and Beyond The Seventh National Accountable Care Organization Summit Scott A. Berkowitz MD MBA Senior Medical Director, Accountable Care, Johns
Integration of Specialty Care into ACOs: Considering JMAP and Beyond The Seventh National Accountable Care Organization Summit Scott A. Berkowitz MD MBA Senior Medical Director, Accountable Care, Johns
Bridges to Excellence Chronic Obstructive Pulmonary Disease Care Recognition Program Guide
 Bridges to Excellence Chronic Obstructive Pulmonary Disease Care Recognition Program Guide Altarum Bridges to Excellence 3520 Green Court, Suite 300 Ann Arbor, MI 48105 bte@altarum.org www.bridgestoexcellence.org
Bridges to Excellence Chronic Obstructive Pulmonary Disease Care Recognition Program Guide Altarum Bridges to Excellence 3520 Green Court, Suite 300 Ann Arbor, MI 48105 bte@altarum.org www.bridgestoexcellence.org
TENNCARE Bundled Payment Initiative: Description of Bundle Risk Adjustment for Wave 2 Episodes
 TENNCARE Bundled Payment Initiative: Description of Bundle Risk Adjustment for Wave 2 Episodes Acute COPD exacerbation (COPD); Screening and surveillance colonoscopy (COL); and Outpatient and non-acute
TENNCARE Bundled Payment Initiative: Description of Bundle Risk Adjustment for Wave 2 Episodes Acute COPD exacerbation (COPD); Screening and surveillance colonoscopy (COL); and Outpatient and non-acute
CLINICAL PROCESS IMPROVEMENT INITIATIVE (CPII) EFFICIENCY REPORT EXPLANATION January 4, 2016
 EFFICIENCY REPORT EXPLANATION January 4, 2016") CLINICAL PROCESS IMPROVEMENT INITIATIVE (CPII) EFFICIENCY REPORT EXPLANATION January 4, 2016 WHAT IS AN EPISODE OF CARE? An episode of care is a grouping of a patient s health care claims for a unique
CLINICAL PROCESS IMPROVEMENT INITIATIVE (CPII) EFFICIENCY REPORT EXPLANATION January 4, 2016 WHAT IS AN EPISODE OF CARE? An episode of care is a grouping of a patient s health care claims for a unique
Member-centered cancer care In Georgia
 Quality health plans & benefits Healthier living Financial well-being Intelligent solutions Member-centered cancer care In Georgia Ira Klein, MD, MBA, FACP GASCO Annual Meeting September 5, 2015 > One
Quality health plans & benefits Healthier living Financial well-being Intelligent solutions Member-centered cancer care In Georgia Ira Klein, MD, MBA, FACP GASCO Annual Meeting September 5, 2015 > One
Advances in Alignment, Measurement, and Performance MY 2017 Results Highlights
 Advances in Alignment, Measurement, and Performance MY 2017 Results Highlights Align. Measure. Perform. (AMP) Programs Launched in 2003, VBP4P is a statewide performance improvement program and one of
Advances in Alignment, Measurement, and Performance MY 2017 Results Highlights Align. Measure. Perform. (AMP) Programs Launched in 2003, VBP4P is a statewide performance improvement program and one of
Academic Year Accreditation Council for Graduate Medical Education. Data Resource Book
 Academic Year 29-2 Accreditation Council for Graduate Medical Education Data Resource Book We improve health care by assessing and advancing the quality of resident physicians education through accreditation
Academic Year 29-2 Accreditation Council for Graduate Medical Education Data Resource Book We improve health care by assessing and advancing the quality of resident physicians education through accreditation
Meaningful Use Overview
 Eligibility Providers may be eligible for incentives from either Medicare or Medicaid, but not both. In addition, providers may not be hospital based. Medicare: A Medicare Eligible Professional (EP) is
Eligibility Providers may be eligible for incentives from either Medicare or Medicaid, but not both. In addition, providers may not be hospital based. Medicare: A Medicare Eligible Professional (EP) is
LCD L B-type Natriuretic Peptide (BNP) Assays
 Assays") LCD L30559 - B-type Natriuretic Peptide (BNP) Assays Contractor Information Contractor Name: Novitas Solutions, Inc. Contractor Number(s): 12501, 12502, 12101, 12102, 12201, 12202, 12301, 12302, 12401,
LCD L30559 - B-type Natriuretic Peptide (BNP) Assays Contractor Information Contractor Name: Novitas Solutions, Inc. Contractor Number(s): 12501, 12502, 12101, 12102, 12201, 12202, 12301, 12302, 12401,
proposed set to a required subset of 3 to 5 measures based on the availability of electronic
 CMS-0033-P 143 proposed set to a required subset of 3 to 5 measures based on the availability of electronic measure specifications and comments received. We propose to require for 2011 and 2012 that EP's
CMS-0033-P 143 proposed set to a required subset of 3 to 5 measures based on the availability of electronic measure specifications and comments received. We propose to require for 2011 and 2012 that EP's
Commercial Business Measurement Period Handbook For Patient-Centered Primary Care
 Commercial Business Measurement Period Handbook For Patient-Centered Primary Care Measurement Period beginning: 07/01/16 CB Version 070116 V1 Introduction: Welcome to your Commercial Business Measurement
Commercial Business Measurement Period Handbook For Patient-Centered Primary Care Measurement Period beginning: 07/01/16 CB Version 070116 V1 Introduction: Welcome to your Commercial Business Measurement
2012 Chronic Respiratory. Program Evaluation. Our mission is to improve the health and quality of life of our members
 2012 Chronic Respiratory Program Evaluation Our mission is to improve the health and quality of life of our members 2012 Chronic Respiratory Program Evaluation Program Title: Chronic Respiratory Program
2012 Chronic Respiratory Program Evaluation Our mission is to improve the health and quality of life of our members 2012 Chronic Respiratory Program Evaluation Program Title: Chronic Respiratory Program
Quality measures a for measurement year 2016
 Quality measures a for measurement year 2016 Measure Description Eligible members Childhood immunizations b Adolescent immunizations b Children who turned 2 during the measurement and who were identified
Quality measures a for measurement year 2016 Measure Description Eligible members Childhood immunizations b Adolescent immunizations b Children who turned 2 during the measurement and who were identified
2017 Medicare Physician Fee Schedule Proposed Rule Summary
 2017 Medicare Physician Fee Schedule Proposed Rule Summary On July 7, 2016, the Centers for Medicare and Medicaid Services (CMS) released the proposed Medicare Physician Fee Schedule (MPFS) for 2017. The
2017 Medicare Physician Fee Schedule Proposed Rule Summary On July 7, 2016, the Centers for Medicare and Medicaid Services (CMS) released the proposed Medicare Physician Fee Schedule (MPFS) for 2017. The
Capital Health Plan CMS Star Ratings Strategies for Improvement
 Capital Health Plan CMS Star Ratings Strategies for Improvement ESTRELLITA REDMON, MD, MBA MEDICAL DIRECTOR The Ultimate Goal Outline Current 5 Star Plans CHP History Importance of Ratings Part C and Part
Capital Health Plan CMS Star Ratings Strategies for Improvement ESTRELLITA REDMON, MD, MBA MEDICAL DIRECTOR The Ultimate Goal Outline Current 5 Star Plans CHP History Importance of Ratings Part C and Part
HEALTHCARE REFORM. September 2012
 HEALTHCARE REFORM Accountable Care Organizations: ACOs 101 September 2012 The enclosed slides are intended to provide you with a general overview of accountable care organizations (ACOs), created within
HEALTHCARE REFORM Accountable Care Organizations: ACOs 101 September 2012 The enclosed slides are intended to provide you with a general overview of accountable care organizations (ACOs), created within
Commercial Business Medical Cost Target
 Commercial Business Medical Cost Target Measurement Period Handbook For Enhanced Personal Health Care Measurement Period beginning: April 1, 2018 CBMCT 040118 V3 Introduction Welcome to your Commercial
Commercial Business Medical Cost Target Measurement Period Handbook For Enhanced Personal Health Care Measurement Period beginning: April 1, 2018 CBMCT 040118 V3 Introduction Welcome to your Commercial
B&T Format. New Measures. Better health care. Better choices. Better health.
 1100 13th Street NW, Third Floor Washington, DC 20005 phone 202.955.3500 fax 202.955.3599 www.ncqa.org TO: Interested Organizations FROM: Patrick Dahill, Assistant Vice President, Policy DATE: August 13,
1100 13th Street NW, Third Floor Washington, DC 20005 phone 202.955.3500 fax 202.955.3599 www.ncqa.org TO: Interested Organizations FROM: Patrick Dahill, Assistant Vice President, Policy DATE: August 13,
Helen Burstin, MD, MPH, FACP Executive Vice President & CEO Council of Medical Specialty Societies. November 28, 2017 ECRI Annual Conference
 Helen Burstin, MD, MPH, FACP Executive Vice President & CEO Council of Medical Specialty Societies November 28, 2017 ECRI Annual Conference I have no disclosures American Academy of Allergy, Asthma & Immunology
Helen Burstin, MD, MPH, FACP Executive Vice President & CEO Council of Medical Specialty Societies November 28, 2017 ECRI Annual Conference I have no disclosures American Academy of Allergy, Asthma & Immunology
PCMH 2018 Enrollment and Update August 25, 2017
 PCMH 2018 Enrollment and Update August 25, 2017 Enrollment Requirements Anne Santifer HealthCare Innovations Department of Human Services 2018 Enrollment Requirements A physician practice that is enrolled
PCMH 2018 Enrollment and Update August 25, 2017 Enrollment Requirements Anne Santifer HealthCare Innovations Department of Human Services 2018 Enrollment Requirements A physician practice that is enrolled
Bridges to Excellence Coronary Artery Disease Care Recognition Program Guide
 Bridges to Excellence Coronary Artery Disease Care Recognition Program Guide Altarum Bridges to Excellence 3520 Green Court, Suite 300 Ann Arbor, MI 48105 bte@altarum.org www.bridgestoexcellence.org Rev:
Bridges to Excellence Coronary Artery Disease Care Recognition Program Guide Altarum Bridges to Excellence 3520 Green Court, Suite 300 Ann Arbor, MI 48105 bte@altarum.org www.bridgestoexcellence.org Rev:
OCHSNER PHYSICIAN PARTNERS. PQRS Measures by Specialty (FINAL)
") OCHSNER PHYSICIAN PARTNERS PQRS Measures by Specialty (FINAL) Allergy and Immunology 2. Asthma: Pharmacologic Therapy for Persistent Asthma - Ambulatory Care Setting (PQRS 53) 3. Patients aged 18 years
OCHSNER PHYSICIAN PARTNERS PQRS Measures by Specialty (FINAL) Allergy and Immunology 2. Asthma: Pharmacologic Therapy for Persistent Asthma - Ambulatory Care Setting (PQRS 53) 3. Patients aged 18 years
B&T Format. New Measures. 2 CAHPS is a registered trademark of the Agency for Healthcare Research and Quality (AHRQ).
.") TO: Interested Organizations FROM: Patrick Dahill, Assistant Vice President, Policy DATE: February 4, 2018 RE: 2018 Accreditation Benchmarks and Thresholds This document reports national benchmarks and
TO: Interested Organizations FROM: Patrick Dahill, Assistant Vice President, Policy DATE: February 4, 2018 RE: 2018 Accreditation Benchmarks and Thresholds This document reports national benchmarks and
NCQA Health Insurance Plan Ratings Methodology March 2018
 00 3th Street NW, Third Floor Washington, DC 20005 phone 202.955.3500 fax 202.955.3599 www.ncqa.org NCQA Health Insurance Plan Ratings Methodology March 208 Better health care. Better choices. Better health.
00 3th Street NW, Third Floor Washington, DC 20005 phone 202.955.3500 fax 202.955.3599 www.ncqa.org NCQA Health Insurance Plan Ratings Methodology March 208 Better health care. Better choices. Better health.
Ministry of Children and Youth Services. Follow-up to VFM Section 3.01, 2013 Annual Report RECOMMENDATION STATUS OVERVIEW
 Chapter 4 Section 4.01 Ministry of Children and Youth Services Autism Services and Supports for Children Follow-up to VFM Section 3.01, 2013 Annual Report RECOMMENDATION STATUS OVERVIEW # of Status of
Chapter 4 Section 4.01 Ministry of Children and Youth Services Autism Services and Supports for Children Follow-up to VFM Section 3.01, 2013 Annual Report RECOMMENDATION STATUS OVERVIEW # of Status of
Symmetry Episode Treatment Groups
 Symmetry Episode Treatment Groups Measuring health care with meaningful episodes of care Identifying clinical episodes of illness and the services involved in their diagnosis, management, and treatment
Symmetry Episode Treatment Groups Measuring health care with meaningful episodes of care Identifying clinical episodes of illness and the services involved in their diagnosis, management, and treatment
B&T Format. New Measures. Better health care. Better choices. Better health.
 1100 13th Street NW, Third Floor Washington, DC 20005 phone 202.955.3500 fax 202.955.3599 www.ncqa.org TO: Interested Organizations FROM: Patrick Dahill, Assistant Vice President, Policy DATE: February
1100 13th Street NW, Third Floor Washington, DC 20005 phone 202.955.3500 fax 202.955.3599 www.ncqa.org TO: Interested Organizations FROM: Patrick Dahill, Assistant Vice President, Policy DATE: February
Scott Hines, MD Co-Chief Clinical Transformation Officer Crystal Run Healthcare AMGA IQL Conference September 26, 2013
 Scott Hines, MD Co-Chief Clinical Transformation Officer Crystal Run Healthcare AMGA IQL Conference September 26, 2013 Learning Objectives Understand the process of variation reduction Understand that
Scott Hines, MD Co-Chief Clinical Transformation Officer Crystal Run Healthcare AMGA IQL Conference September 26, 2013 Learning Objectives Understand the process of variation reduction Understand that
Reducing Practice Variation To Increase Value. Scott Hines, MD Chief Quality Officer Crystal Run Healthcare June 20, 20127
 Reducing Practice Variation To Increase Value Scott Hines, MD Chief Quality Officer Crystal Run Healthcare June 20, 20127 Learning Objectives Understand the process of variation reduction Understand that
Reducing Practice Variation To Increase Value Scott Hines, MD Chief Quality Officer Crystal Run Healthcare June 20, 20127 Learning Objectives Understand the process of variation reduction Understand that
Health outcomes improve and costs are lower when care is consistent with evidence-based treatments. Optum Symmetry EBM Connect
 Denit Optum audist Symmetry aut eostisciam EBM Connect nime Health care organizations recognize the need to measure and improve health care quality. According to a 2013 report from the U.S. Department
Denit Optum audist Symmetry aut eostisciam EBM Connect nime Health care organizations recognize the need to measure and improve health care quality. According to a 2013 report from the U.S. Department
EHR SOFTWARE COMPARISON
 EHR SOFTWARE COMPARISON C M CONVERTED MEDIA WHY NOT CREATE YOUR OWN COMPARISON? With our free comparison engine you can build your own side-by-side comparison of leading EHR solutions. Narrow down your
EHR SOFTWARE COMPARISON C M CONVERTED MEDIA WHY NOT CREATE YOUR OWN COMPARISON? With our free comparison engine you can build your own side-by-side comparison of leading EHR solutions. Narrow down your
Diagnostics for the early detection and prevention of colon cancer. Fourth-Quarter 2014 Earnings Call February 24, 2015
 Diagnostics for the early detection and prevention of colon cancer Fourth-Quarter 2014 Earnings Call February 24, 2015 Safe Harbor Statement Certain statements made in this presentation contain forward-looking
Diagnostics for the early detection and prevention of colon cancer Fourth-Quarter 2014 Earnings Call February 24, 2015 Safe Harbor Statement Certain statements made in this presentation contain forward-looking
Extraordinary service, far from ordinary
 Signature Services Premier International Health Extraordinary service, far from ordinary Why Choose Lenox Hill Hospital International Health? Lenox Hill Hospital is the care destination of choice for more
Signature Services Premier International Health Extraordinary service, far from ordinary Why Choose Lenox Hill Hospital International Health? Lenox Hill Hospital is the care destination of choice for more
UT Health Physicians. Carlos A. Rosende, M.D., F.A.C.S. Executive Vice Dean for Clinical Affairs Executive Director, UT Health Physicians
 UT Health Physicians Carlos A. Rosende, M.D., F.A.C.S. Executive Vice Dean for Clinical Affairs Executive Director, UT Health Physicians UT Medicine UT Health Physicians Our New Name UT Health San Antonio
UT Health Physicians Carlos A. Rosende, M.D., F.A.C.S. Executive Vice Dean for Clinical Affairs Executive Director, UT Health Physicians UT Medicine UT Health Physicians Our New Name UT Health San Antonio
QUALITY IMPROVEMENT Section 9
 Quality Improvement Program The Plan s Quality Improvement Program serves to improve the health of its members through emphasis on health maintenance, education, diagnostic testing and treatment. The Quality
Quality Improvement Program The Plan s Quality Improvement Program serves to improve the health of its members through emphasis on health maintenance, education, diagnostic testing and treatment. The Quality
Consensus Core Set: ACO and PCMH / Primary Care Measures Version 1.0
 Consensus Core Set: ACO and PCMH / Primary Care s 0018 Controlling High Blood Pressure patients 18 to 85 years of age who had a diagnosis of hypertension (HTN) and whose blood pressure (BP) was adequately
Consensus Core Set: ACO and PCMH / Primary Care s 0018 Controlling High Blood Pressure patients 18 to 85 years of age who had a diagnosis of hypertension (HTN) and whose blood pressure (BP) was adequately
2017 HEDIS Measures. PREVENTIVE SCREENING 2017 Measure Quality Indicator
 PREVENTIVE SCREENING Childhood Immunization Children who turn 2 during the Adolescent Immunization Adolescents who turn 13 during the Lead Screening Children who turn 2 during the Breast Cancer Screening
PREVENTIVE SCREENING Childhood Immunization Children who turn 2 during the Adolescent Immunization Adolescents who turn 13 during the Lead Screening Children who turn 2 during the Breast Cancer Screening
NATIONAL HEALTH POLICY FORUM
 NATIONAL HEALTH POLICY FORUM UTILIZATION PATTERNS IN ADVANCED IMAGING: THE RADIOLOGY BENEFIT MANAGEMENT EXPERIENCE Susan Nedza, MD, MBA, FACEP Chief Medical Officer AIM Specialty Health / WellPoint, Inc.
NATIONAL HEALTH POLICY FORUM UTILIZATION PATTERNS IN ADVANCED IMAGING: THE RADIOLOGY BENEFIT MANAGEMENT EXPERIENCE Susan Nedza, MD, MBA, FACEP Chief Medical Officer AIM Specialty Health / WellPoint, Inc.
Submission of Webicina.com for the Social Innovation Tournament
 Submission of Webicina.com for the Social Innovation Tournament Webicina LLC Bertalan Mesko, MD Twitter.com/Berci info@webicina.com Skype: ncurse How does Webicina serve the public? Webicina.com curates
Submission of Webicina.com for the Social Innovation Tournament Webicina LLC Bertalan Mesko, MD Twitter.com/Berci info@webicina.com Skype: ncurse How does Webicina serve the public? Webicina.com curates
Drug Coverage for EpiPens to Change July 1
 Drug Coverage for EpiPens to Change July 1 Epinephrine auto-injector pens (e.g., EpiPen and Adrenaclick ) have seen recent cost increases, now with a price tag of more than $600 for each prescription.
Drug Coverage for EpiPens to Change July 1 Epinephrine auto-injector pens (e.g., EpiPen and Adrenaclick ) have seen recent cost increases, now with a price tag of more than $600 for each prescription.
Patient-Centered Medical Home
 2017 Primary Care Commercial and QUEST Integration January 2017 HMSA Patient-Centered Medical Home Getting Started and Ongoing Management P R O G R A M G U I D E An Independent Licensee of the Blue Cross
2017 Primary Care Commercial and QUEST Integration January 2017 HMSA Patient-Centered Medical Home Getting Started and Ongoing Management P R O G R A M G U I D E An Independent Licensee of the Blue Cross
2018 P4P Overview 0518.PR.P.PP.1 6/18
 2018 P4P Overview Agenda MHS Pay For Performance (P4P) Ambetter P4P Program Secure Web Reporting Question and Answer What You Will Learn 1. Measure Overviews & Specifications 2. Documentation Requirements
2018 P4P Overview Agenda MHS Pay For Performance (P4P) Ambetter P4P Program Secure Web Reporting Question and Answer What You Will Learn 1. Measure Overviews & Specifications 2. Documentation Requirements
Jan Feb Mar Apr May Jun Jul Aug Sep X X X X X X X. Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov X X X X X X X X X X X X X
 Primary Prevention Breast Cancer Prevention Member: Mammography reminder letters to female members ages 51.5-74 who are overdue to get a mammogram Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Providers:
Primary Prevention Breast Cancer Prevention Member: Mammography reminder letters to female members ages 51.5-74 who are overdue to get a mammogram Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Providers:
Achieving Quality and Value in Chronic Care Management
 The Burden of Chronic Disease One of the greatest burdens on the US healthcare system is the rapidly growing rate of chronic disease. These statistics illustrate the scope of the problem: Nearly half of
The Burden of Chronic Disease One of the greatest burdens on the US healthcare system is the rapidly growing rate of chronic disease. These statistics illustrate the scope of the problem: Nearly half of
How pharmacy and retail health can support health and wellness. Nancy Gagliano Chief Medical Officer, MC September, 2014
 How pharmacy and retail health can support health and wellness Nancy Gagliano Chief Medical Officer, MC September, 2014 2 An important decision for public health Current Health Care Challenges The State
How pharmacy and retail health can support health and wellness Nancy Gagliano Chief Medical Officer, MC September, 2014 2 An important decision for public health Current Health Care Challenges The State
Precyse University ICD-10 Education Tracks
 Precyse University ICD-10 Education Tracks The following information will help you understand the Precyse University ICD-10 Educational Tracks. Each impacted population requires specific education to prepare
Precyse University ICD-10 Education Tracks The following information will help you understand the Precyse University ICD-10 Educational Tracks. Each impacted population requires specific education to prepare
M4 Coursework Information
 M4 Coursework Information This guide is intended to assist students in selecting and scheduling courses based upon their specialty of interest. Contents ANESTHESIOLOGY... 1 DERMATOLOGY... 2 EMERGENCY MEDICINE...
M4 Coursework Information This guide is intended to assist students in selecting and scheduling courses based upon their specialty of interest. Contents ANESTHESIOLOGY... 1 DERMATOLOGY... 2 EMERGENCY MEDICINE...
Across The Chasm: The Transition From Volume To Value
 Across The Chasm: The Transition From Volume To Value Joseph Bisordi, MD, Executive Vice President & CMO Ochsner Health System Our Mission is to Serve, Heal, Lead, Educate, and Innovate $1.6 Revenue ($B)
Across The Chasm: The Transition From Volume To Value Joseph Bisordi, MD, Executive Vice President & CMO Ochsner Health System Our Mission is to Serve, Heal, Lead, Educate, and Innovate $1.6 Revenue ($B)
ETG Analyzer Report. Your Practice # Episodes. Mkt Share Mkt Volume WHIO Dermatology 575 Acne 746 $508 1,698 $
 ETG Analyzer Report Practice: Practice Group: Badger County Severity: Level 1 Payers: Commercial Episode Types: Complete Claims: Full Claims Outliers: No Outliers DMV6 Created: April 1, 2010 March 31,
ETG Analyzer Report Practice: Practice Group: Badger County Severity: Level 1 Payers: Commercial Episode Types: Complete Claims: Full Claims Outliers: No Outliers DMV6 Created: April 1, 2010 March 31,
Long-stay patients methodology Published by NHS England and NHS Improvement
 Long-stay patients methodology Published by NHS England and NHS Improvement July 2018 1 Document Title: Long-stay patients methodology Version number: 1.0 First published: 9 July 2018 Updated: Prepared
Long-stay patients methodology Published by NHS England and NHS Improvement July 2018 1 Document Title: Long-stay patients methodology Version number: 1.0 First published: 9 July 2018 Updated: Prepared
The Choosing Wisely Project. Disclosures. Learning Objectives 3/18/2014. Marie Gilbert, PA C, DFAAPA
 The Choosing Wisely Project Marie Gilbert, PA C, DFAAPA Disclosures This speaker has no commercial relationships to disclose. Learning Objectives List the five "Choosing Wisely" program items for Otolaryngology.
The Choosing Wisely Project Marie Gilbert, PA C, DFAAPA Disclosures This speaker has no commercial relationships to disclose. Learning Objectives List the five "Choosing Wisely" program items for Otolaryngology.
Understanding Hierarchical Condition Categories (HCC)
") Understanding Hierarchical Condition Categories (HCC) How hierarchical condition category coding will impact your practice and how you can use these codes to increase quality, improve the patient experience,
Understanding Hierarchical Condition Categories (HCC) How hierarchical condition category coding will impact your practice and how you can use these codes to increase quality, improve the patient experience,
Bridges to Excellence Asthma Care Recognition Program Guide for Patients 5 years of age and older
 Bridges to Excellence Asthma Care Recognition Program Guide for Patients 5 years of age and older Altarum Bridges to Excellence 3520 Green Court, Suite 300 Ann Arbor, MI 48105 bte@altarum.org www.bridgestoexcellence.org
Bridges to Excellence Asthma Care Recognition Program Guide for Patients 5 years of age and older Altarum Bridges to Excellence 3520 Green Court, Suite 300 Ann Arbor, MI 48105 bte@altarum.org www.bridgestoexcellence.org
Now iknow SM : Frequently Asked Questions
 Now iknow SM : Frequently Asked Questions Overview Beginning December 2013, Harvard Pilgrim in partnership with Castlight Health, a leader in health care transparency will introduce a new online health
Now iknow SM : Frequently Asked Questions Overview Beginning December 2013, Harvard Pilgrim in partnership with Castlight Health, a leader in health care transparency will introduce a new online health
Commercial Business Medical Cost Target
 Commercial Business Medical Cost Target Measurement Period Handbook For Enhanced Personal Health Care Measurement Period beginning: April 1, 2018 CBMCT 040118 V1 Introduction Welcome to your Commercial
Commercial Business Medical Cost Target Measurement Period Handbook For Enhanced Personal Health Care Measurement Period beginning: April 1, 2018 CBMCT 040118 V1 Introduction Welcome to your Commercial
Quality Care Plus 2015 Primary Care Physician Incentive Program. Now includes Medicare patients!
 Quality Care Plus 2015 Primary Care Physician Incentive Program Now includes Medicare patients! Health Partners Plans (HPP) would like to express our appreciation for the invaluable role our primary care
Quality Care Plus 2015 Primary Care Physician Incentive Program Now includes Medicare patients! Health Partners Plans (HPP) would like to express our appreciation for the invaluable role our primary care
2015 Healthy Heart. Program Evaluation. Our mission is to improve the health and quality of life of our members
 2015 Healthy Heart Program Evaluation Our mission is to improve the health and quality of life of our members 2015 Healthy Heart Program Evaluation Program Title: Healthy Heart Program Evaluation Period:
2015 Healthy Heart Program Evaluation Our mission is to improve the health and quality of life of our members 2015 Healthy Heart Program Evaluation Program Title: Healthy Heart Program Evaluation Period: