DEPRESCRIBING IN THE ELDERLY
|
|
|
- Arron Sutton
- 6 years ago
- Views:
Transcription
 B R U Y È R E C O N T I N U I N G C A R")
1 DEPRESCRIBING IN THE ELDERLY G E R I A T R I C S R E F R E S H E R D A Y W E D N E S D A Y, A P R I L 5 TH, V É R O N I Q U E F R E N C H M E R K L E Y, M D, C C F P ( C O E ) B R U Y È R E C O N T I N U I N G C A R E
2 DISCLOSURES I have no conflicts of interest to declare.
3 ACKNOWLEDGEMENTS Many thanks to Dr. Barbara Farrell for her pioneering work in this field, for her input on this presentation, and for sharing her expertise and enthusiasm with us every day in the Geriatric Day Hospital at Bruyère Continuing Care.
4 DEPRESCRIBING ( The planned and supervised process of dose reduction or stopping of medication that may be causing harm or no longer be of benefit. The goal of deprescribing is to reduce medication burden and harm, while maintaining or improving quality of life. Deprescribing is part of good prescribing backing off when doses are too high, or stopping medications that are no longer needed.
5 LEARNING OBJECTIVES 1. Identify factors that motivate deprescribing. 2. Work through a case that illustrates the development of a deprescribing plan. 3. Review simple strategies that can help to make deprescribing changes stick. 4. List key resources for future reference.
6 SYSTEM FACTORS DRIVING DEPRESCRIBING Rising medication costs (CIHI 2008; 6 provinces) One billion from publicly funded programs (17.4% of health care spending) Increased health care utilization Adverse drug events account for 10-17% of elderly patient hospital admissions; as many as 75% are preventable > 1 in 9 ER visits due to drug-related adverse events Those with adverse drug reactions incur more health services
7 DEPRESCRIBING TRIGGERS FOR HEALTH CARE PROVIDERS Identification of high-risk medications Beers criteria, STOPP/START criteria Medications contributing to geriatric syndromes such as cognitive impairment, falls etc. Prescribing cascades Multiple medications (sometimes > 25)
8 PATIENT MOTIVATORS FOR ENGAGING IN DEPRESCRIBING Feeling frustrated about taking too many pills and still not feeling well Seeing their health and well-being priorities acknowledged Having the opportunity to discuss the HCP s concerns about their medications Feeling empowered to participate in setting the deprescribing agenda going forward
9 CHALLENGES: MULTIMORBIDITY AND POLYPHARMACY Prevalence of chronic illness increases with age: 65-69: men 35%, women 45% 80 yrs +: men 53%, women 70% As comorbidities accumulate, management becomes more challenging: Guideline Gridlock One comorbidity can increase the risk of another e.g. dementia and delirium More specialists involved = competing priorities and risk for miscommunication Patient s priorities often lost

10 CHALLENGES: NON-ADHERENCE Intentional: Too many! Why bother? Nonintentional: Too complex! Forgets.
11 THE CASE OF MRS. A. 84 yr old widow, living alone Severe knee pain limiting mobility Often confused, unable to get out of bed 3 falls in the last year Doesn t want to go out anymore Children think she should no longer be living alone Referred to the Geriatric Day Hospital by her family physician
12 MRS. A. S MEDICATION LIST In dosette: Not in dosette: Ibuprofen 400mg twice daily ASA 81mg daily Lorazepam 1mg at bedtime Dimenhydrinate 50mg at bedtime Warfarin daily as directed Lakota capsules four times daily Metoprolol 50mg twice daily Dextromethorphan syrup at bedtime Ramipril 5mg daily Furosemide 40mg twice daily Atorvastatin 40mg daily Lansoprazole 30mg daily Oxybutynin XL 10mg daily Vitamin B mcg daily Slow-K (potassium) daily Calcium/Vitamin D twice daily
13 IDENTIFYING MEDS TO BE TARGETED Explicit approaches Screening criteria such as Beers, STOPP/START Many limitations: Do not capture all drug-related problems and prescribing cascades May inadvertently identify a useful medication as potentially inappropriate Have limited evidence for reducing morbidity, ADR s, ER visits, mortality Are not patient-specific Implicit approaches Assess each medication for indication, effectiveness, safety, compliance Always ask: Could this be caused by a drug?
14 MRS. A. S MEDICATION HISTORY 10 years ago 3-5 years ago Atrial fibrillation metoprolol and warfarin Husband died - lorazepam Knee pain ibuprofen Hypertension ramipril Cough dextromethorphan Hypertension amlodipine Daughter told her to take ASA for hypertension 2 years ago Ankle swelling furosemide Potassium low potassium Nausea dimenhydrinate, then lansoprazole (taking ibuprofen) B12 levels low B12 supplement Knee pain Lakota Nocturia oxybutynin Osteopenia calcium/vitamin D
15 MRS. A S PRESCRIBING WEB ramipril Need for CV protection Cough ASA dextromethorphan Increased blood pressure ibuprofen Need for GI prophylaxis amlodipine Heartburn lansoprazole Ankle swelling Incontinence oxybutynin furosemide Incontinence Decreased vitamin absorption Low potassium dimenhydrinate Incontinence Incontinence Vitamin B12 potassium Nausea lorazepam
16 MRS. A S DRUG-RELATED PROBLEMS (*NOT CAUGHT BY SCREENING) 1. high risk of bleeding secondary to combination of warfarin, ASA, ibuprofen and Lakota (has easy bruising and some gum bleeding) 2. states no longer having benefit from ibuprofen for knee pain; may be contributing to her hypertension and bleeding risk with warfarin; patient willing to try regular acetaminophen instead* 3. high blood pressure may improve with stopping ibuprofen, in which case (and in order to minimize orthostatic hypotension and ankle swelling), she may no longer need amlodipine* 4. if ankle swelling improves with stopping amlodipine, consider tapering furosemide (which may also help with OH)* 5. if we taper furosemide, try to stop potassium (at risk of hyperkalemia because of ramipril)* 6. once ibuprofen, ASA and Lakota stopped, will not likely require ongoing lansoprazole as she does not describe a history of either heartburn or ulcer* 7. cough may be due to ramipril and her use of dextromethorphan is likely contributing to confusion and falls* 8. high dose and frequent use of dimenhydrinate may be contributing to fatigue and fall risk* 9. periodic nausea may be due to potassium* 10. urinary urgency and incontinence may be contributed to by high dose of furosemide and by taking the furosemide in the evening* 11. dry mouth may improve with a lower dose of oxybutynin* 12. risk of falls and morning fatigue are likely contributed to by lorazepam
17 STRATEGIC (DE)PRESCRIBING FOR MRS. A. Start with medications with: - Risk of harm with no known benefit - Unclear/no indication - Indication but unknown/minimal benefit - Little chance of ADWE - Benefit but side effect or safety issues ***involve the patient in choosing where to start Adapt guidelines for the frail elderly E.g. appropriate BP targets Use combination pills when possible Reduce medication-taking frequency Aim for daily or bid dosing if possible
18 MRS. A. S GDH INTERVENTIONS Stop ASA and Lakota Decrease dimenhydrinate Week 1 Week 2 Document BP target Switch ibuprofen to acetaminophen Physio and exercise Stop B12 Begin amlodipine taper Begin lansoprazole taper Week 3
19 MRS. A. S GDH INTERVENTIONS Stop amlodipine Increase acetaminophen dose Start lorazepam taper Provide sleep hygiene education Week 4 Week 5 Switch acetaminophen to small dose hydromorphone Taper ramipril Start furosemide taper Add lactulose Stop ramipril Stop furosemide Stop potassium Taper oxybutynin Week 6
20 MRS. A. S GDH INTERVENTIONS Stop dextromethorphan and dimenhydrinate Review and advise re: salt and calcium intake Start HCTZ Continue lorazepam taper Week 7 Week 8 Stop oxybutynin Stop lorazepam Change lansoprazole to prn Provide heartburn management education Change metoprolol to bisoprolol Combine calcium and vitamin D Stop lansoprazole Week 9
21 AFTER A 10-WEEK GDH ADMISSION: Mrs. A s medications Hydromorphone 0.5mg q12h Hydrochlorothiazide 12.5mg daily Bisoprolol 2.5mg daily Warfarin as directed Caltrate Select with vitamin D twice daily Lactulose 15ml daily Mrs. A s life Knee pain improved Getting out of house now Urgency and nocturia better (up 1-2 x/night) Sleep improved (to bed 10pm, up about 7am) Meal times normal (8, 12, 6) Bruising/gum bleeding gone No heartburn, nausea, cough or swollen ankles
22 STRATEGIES TO HELP DEPRESCRIBING STICK Involve the patient/family in decisions and monitoring Be up front about how long ADWE s can last Work with team members to trial non-drug approaches Follow up and document progress Communicate clearly with other involved HCP s o Especially the community pharmacist Use a variety of educational media o Verbal, written handouts, medication logs to organize info Empower patients to avoid future problems

23 HELPING DEPRESCRIBING STICK : THE SPEEDIMEMO
24 HELPING DEPRESCRIBING STICK : A DIFFERENT RX
25

26 NEW ONLINE MODULE DEPRESCRIBING
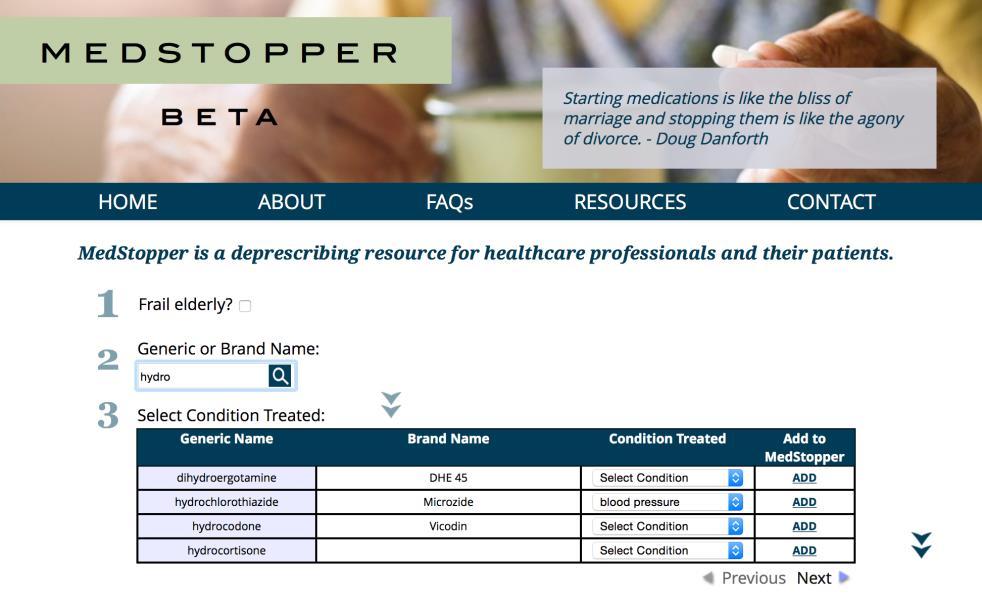
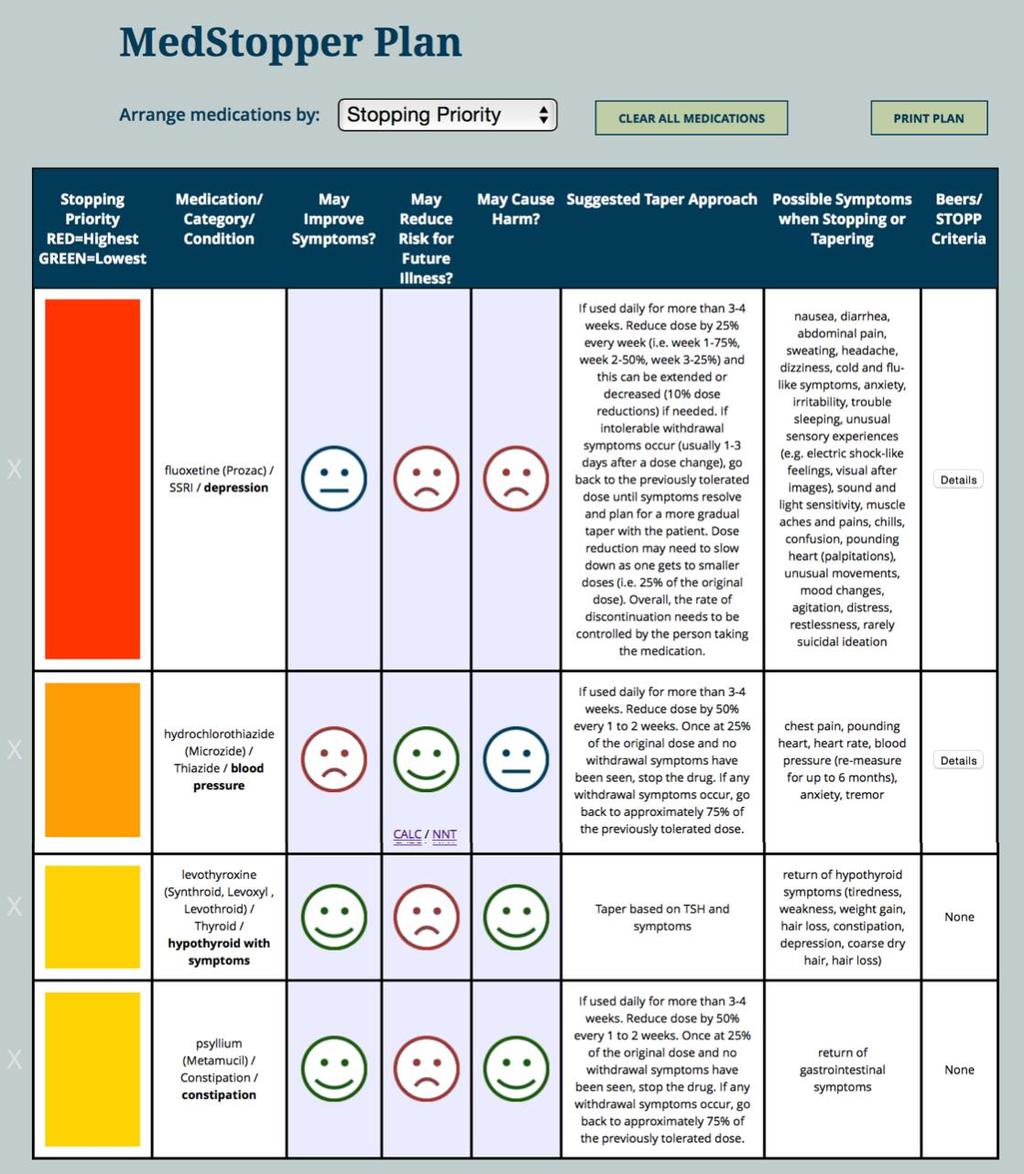
27 MEDSTOPPER medstopper.com
28
Polypharmacy and Polymorbid Patients: Practical Tips and Tricks
 Polypharmacy and Polymorbid Patients: Practical Tips and Tricks November 2, 2013 Faculty/Presenter Disclosure Faculty: Chris Fan-Lun, BScPhm, ACPR, CGP Pharmacist - Geriatric Medicine Clinical Practice
Polypharmacy and Polymorbid Patients: Practical Tips and Tricks November 2, 2013 Faculty/Presenter Disclosure Faculty: Chris Fan-Lun, BScPhm, ACPR, CGP Pharmacist - Geriatric Medicine Clinical Practice
Managing Polypharmacy in the Elderly March 21, Barbara Farrell BScPhm, PharmD, FCSHP Pharmacist, Bruyère Geriatric Day Hospital
 Managing Polypharmacy in the Elderly March 21, 2012 Barbara Farrell BScPhm, PharmD, FCSHP Pharmacist, Bruyère Geriatric Day Hospital Objectives Participants will be able to: Describe the impact of polypharmacy
Managing Polypharmacy in the Elderly March 21, 2012 Barbara Farrell BScPhm, PharmD, FCSHP Pharmacist, Bruyère Geriatric Day Hospital Objectives Participants will be able to: Describe the impact of polypharmacy
Deconstructing Polypharmacy. Alan B. Douglass, M.D. Director
 Deconstructing Polypharmacy Alan B. Douglass, M.D. Director Recognize this patient? Mrs. Brown- 82 years young Active Medical Problems Hypertension Hyperlipidemia Type 2 Diabetes Peripheral edema Osteoarthritis
Deconstructing Polypharmacy Alan B. Douglass, M.D. Director Recognize this patient? Mrs. Brown- 82 years young Active Medical Problems Hypertension Hyperlipidemia Type 2 Diabetes Peripheral edema Osteoarthritis
A C A D E M I C D E TA I L I N G C H O O S I N G W I S E LY C O N F E R E N C E O C T 2 1, PA M M C L E A N - V E Y S E Y B S C P H A R M D R
 PPI DEPRESCRIBING Canadian Deprescribing Network (CaDeN) goals are to: Reduce harm by raising awareness and cutting risky prescriptions for seniors by 50% by 2020. Promote health by ensuring access to
PPI DEPRESCRIBING Canadian Deprescribing Network (CaDeN) goals are to: Reduce harm by raising awareness and cutting risky prescriptions for seniors by 50% by 2020. Promote health by ensuring access to
BLCS 1-Clinical Overview. Dr. Chris Rauscher Clinical Lead Shared Care Polypharmacy Risk Reduction Initiative
 BLCS 1-Clinical Overview Dr. Chris Rauscher Clinical Lead Shared Care Polypharmacy Risk Reduction Initiative Fraser Health Guide To Person-Centered Medication Decisions Factors to Consider When Systematically
BLCS 1-Clinical Overview Dr. Chris Rauscher Clinical Lead Shared Care Polypharmacy Risk Reduction Initiative Fraser Health Guide To Person-Centered Medication Decisions Factors to Consider When Systematically
Polypharmacy and the Older Adult. Leslie Baker, PharmD, BCGP Umanga Sharma, MD
 Polypharmacy and the Older Adult Leslie Baker, PharmD, BCGP Umanga Sharma, MD Objectives Identify what polypharmacy is Identify factors leading to polypharmacy Discuss consequences of polypharmacy Identify
Polypharmacy and the Older Adult Leslie Baker, PharmD, BCGP Umanga Sharma, MD Objectives Identify what polypharmacy is Identify factors leading to polypharmacy Discuss consequences of polypharmacy Identify
Reviewing Medicines in at risk patients care homes
 Reviewing Medicines in at risk patients care homes Clinical Medication Reviews by Pharmacists in Collaboration with GP Surgeries across Brighton and Hove CCG Liz Butterfield FRPharmS 19th April 2016 NICE:
Reviewing Medicines in at risk patients care homes Clinical Medication Reviews by Pharmacists in Collaboration with GP Surgeries across Brighton and Hove CCG Liz Butterfield FRPharmS 19th April 2016 NICE:
Polypharmacy & De-prescribing In Older Adults
 Polypharmacy & De-prescribing In Older Adults Maryland Association of Osteopathic Physicians Annual Meeting September 15, 2018 Elizabeth Phung, DO Lead Clinical Associate Physician Beacham Center for Geriatric
Polypharmacy & De-prescribing In Older Adults Maryland Association of Osteopathic Physicians Annual Meeting September 15, 2018 Elizabeth Phung, DO Lead Clinical Associate Physician Beacham Center for Geriatric
TOP 5 DRUGS.. TO AVOID IN THE ELDERLY
 TOP 5 DRUGS.. TO AVOID IN THE ELDERLY Debbie Kwan, BScPhm., MSc., FCSHP Canadian Geriatrics Society, April 20, 2013 Disclosure of Potential for Conflict of Interest: Financial Disclosure: None Mar 26,
TOP 5 DRUGS.. TO AVOID IN THE ELDERLY Debbie Kwan, BScPhm., MSc., FCSHP Canadian Geriatrics Society, April 20, 2013 Disclosure of Potential for Conflict of Interest: Financial Disclosure: None Mar 26,
PRESCRIBING IN THE ELDERLY. CARE HOME PHARMACY TEAM Bhavini Shah, Eleesha Pentiah & Puja Vyas
 PRESCRIBING IN THE ELDERLY CARE HOME PHARMACY TEAM Bhavini Shah, Eleesha Pentiah & Puja Vyas LEARNING OUTCOMES Medicines Optimisation The effects of aging on health and medicines. Polypharmacy Acute Kidney
PRESCRIBING IN THE ELDERLY CARE HOME PHARMACY TEAM Bhavini Shah, Eleesha Pentiah & Puja Vyas LEARNING OUTCOMES Medicines Optimisation The effects of aging on health and medicines. Polypharmacy Acute Kidney
Appropriate prescribing and deprescribing for older people getting it right. Alan Davis Northland District Health Board
 Appropriate prescribing and deprescribing for older people getting it right Alan Davis Northland District Health Board Unused returns Potentially inappropriate medication use in the elderly 15% of older
Appropriate prescribing and deprescribing for older people getting it right Alan Davis Northland District Health Board Unused returns Potentially inappropriate medication use in the elderly 15% of older
Preventing Medication Related Falls
 A Team Approach to Deprescribing and Preventing Medication Related Falls Wednesday, February 13 th 2019 Pam Howell THIS WEBINAR IS BEING RECORDED. THE SLIDE DECK AND RECORDING WILL BE EMAILED AFTER THE
A Team Approach to Deprescribing and Preventing Medication Related Falls Wednesday, February 13 th 2019 Pam Howell THIS WEBINAR IS BEING RECORDED. THE SLIDE DECK AND RECORDING WILL BE EMAILED AFTER THE
Travel Health Conference. April 27, 2018 Jamie Falk, BScPharm, PharmD
 Travel Health Conference April 27, 2018 Jamie Falk, BScPharm, PharmD Presenter: Jamie Falk Drug interactions in travelers with chronic conditions I have no conflicts to disclose By attending this session
Travel Health Conference April 27, 2018 Jamie Falk, BScPharm, PharmD Presenter: Jamie Falk Drug interactions in travelers with chronic conditions I have no conflicts to disclose By attending this session
< = > less is more. De-diagnosing De-prescribing Non-testing
 < = > less is more De-diagnosing De-prescribing Non-testing Who says? Overdiagnosis Polypharmacy False positives Too much medicine Risk aversion $$$ Sources Prof David Le Couteur, Clin Pharm and Aged Care
< = > less is more De-diagnosing De-prescribing Non-testing Who says? Overdiagnosis Polypharmacy False positives Too much medicine Risk aversion $$$ Sources Prof David Le Couteur, Clin Pharm and Aged Care
START, STOPP, Beers Oh My! Navigating the World of Geriatric Pharmacy
 START, STOPP, Beers Oh My! Navigating the World of Geriatric Pharmacy Jessica DiLeo, PharmD Kate Murphy, PharmD OBJECTIVES Identify pharmacodynamic and pharmacokinetic parameters that may influence treatment
START, STOPP, Beers Oh My! Navigating the World of Geriatric Pharmacy Jessica DiLeo, PharmD Kate Murphy, PharmD OBJECTIVES Identify pharmacodynamic and pharmacokinetic parameters that may influence treatment
Transitions of Care & Medication Reconciliation Ashley King, PharmD, BCGP Clinical Pharmacist LECOM Health March 2018
 Transitions of Care & Medication Reconciliation Ashley King, PharmD, BCGP Clinical Pharmacist LECOM Health March 2018 Objectives Identify when to complete medication reconciliation Understand the importance
Transitions of Care & Medication Reconciliation Ashley King, PharmD, BCGP Clinical Pharmacist LECOM Health March 2018 Objectives Identify when to complete medication reconciliation Understand the importance
Geriatric Pharmacology
 Geriatric Pharmacology Janice Scheufler R.Ph.,PharmD, FASCP Clinical Pharmacist Hospice of the Western Reserve Objectives List three risk factors for adverse drug events in the elderly Discuss two physiological
Geriatric Pharmacology Janice Scheufler R.Ph.,PharmD, FASCP Clinical Pharmacist Hospice of the Western Reserve Objectives List three risk factors for adverse drug events in the elderly Discuss two physiological
If a bad thing is happening to a patient, a drug did it until proven otherwise
 Dr Vicki s First Rule of Geriatrics Deprescribing in the Elderly Victoria Braund MD, FACP, CMD Director, Division of Geriatrics NorthShore University HealthSystem Medical Director, Brandel Health & Rehab
Dr Vicki s First Rule of Geriatrics Deprescribing in the Elderly Victoria Braund MD, FACP, CMD Director, Division of Geriatrics NorthShore University HealthSystem Medical Director, Brandel Health & Rehab
Katee Kindler, PharmD, BCACP
 Speaker Introduction Katee Kindler, PharmD, BCACP Current Practice: Clinical Pharmacy Specialist Ambulatory Care, St. Vincent Indianapolis Assistant Professor of Pharmacy Practice, Manchester University,
Speaker Introduction Katee Kindler, PharmD, BCACP Current Practice: Clinical Pharmacy Specialist Ambulatory Care, St. Vincent Indianapolis Assistant Professor of Pharmacy Practice, Manchester University,
Black holes taped on floor Redirection Music and activities Yellow straps across the door Remind other residents to use call bell when she comes in
 Intrusive Wandering Case study........................................... A 97 year old woman with dementia lives in a mixed 23 bed LTC unit. She is independently mobile in her wheelchair and goes in and
Intrusive Wandering Case study........................................... A 97 year old woman with dementia lives in a mixed 23 bed LTC unit. She is independently mobile in her wheelchair and goes in and
Frailty: what s it all about?
 Frailty: what s it all about? What is frailty? 1. an inevitable consequence of aging 2. A state due to multiple long term conditions 3. A condition in which the person becomes fragile 4. A state associated
Frailty: what s it all about? What is frailty? 1. an inevitable consequence of aging 2. A state due to multiple long term conditions 3. A condition in which the person becomes fragile 4. A state associated
Case #3 Clinician. Past Medical History: hypertension, hypercholesterolemia, arthritis, seasonal allergies, remote history of stroke
 Case #3 Clinician Be the clinician taking a best possible medication history Use the space below to document your best possible medication history You are going to see patient Frank Ribello Reason for
Case #3 Clinician Be the clinician taking a best possible medication history Use the space below to document your best possible medication history You are going to see patient Frank Ribello Reason for
Taking the harm out of Polypharmacy Step by step. Karen Reid and Claire Stein Lead Integrated Care Pharmacist NHS Lothian
 Taking the harm out of Polypharmacy Step by step Karen Reid and Claire Stein Lead Integrated Care Pharmacist NHS Lothian Presentation: Polypharmacy Overview of the 2015 guidelines The Seven Steps Application
Taking the harm out of Polypharmacy Step by step Karen Reid and Claire Stein Lead Integrated Care Pharmacist NHS Lothian Presentation: Polypharmacy Overview of the 2015 guidelines The Seven Steps Application
Meds and Falls: Keep in Step with your Meds
 Meds and Falls: Keep in Step with your Meds Donna Bartlett PharmD, CGP, RPh Associate Professor-Pharmacy Practice MCPHS University Clinical Pharmacist-MCPHS University- Pharmacy Outreach Program donna.bartlett@mcphs.edu
Meds and Falls: Keep in Step with your Meds Donna Bartlett PharmD, CGP, RPh Associate Professor-Pharmacy Practice MCPHS University Clinical Pharmacist-MCPHS University- Pharmacy Outreach Program donna.bartlett@mcphs.edu
Polypharmacy. Polypharmacy. Suboptimal Prescribing in Older Adults. Kenneth Schmader, MD Professor of Medicine-Geriatrics
 Polypharmacy Kenneth Schmader, MD Professor of Medicine-Geriatrics Polypharmacy Definition Causes Consequences Prevention/management Suboptimal Prescribing in Older Adults Overuse Polypharmacy Underuse
Polypharmacy Kenneth Schmader, MD Professor of Medicine-Geriatrics Polypharmacy Definition Causes Consequences Prevention/management Suboptimal Prescribing in Older Adults Overuse Polypharmacy Underuse
Geriatric Pharmacology. Kwi Bulow, M.D. Clinical Professor of Medicine Director, Academic Geriatric Resource Center
 Geriatric Pharmacology Kwi Bulow, M.D. Clinical Professor of Medicine Director, Academic Geriatric Resource Center Silver Tsunami 2010: 40 million (13%) 2030: 72 million (20%) Baby Boomers (1946-1964)
Geriatric Pharmacology Kwi Bulow, M.D. Clinical Professor of Medicine Director, Academic Geriatric Resource Center Silver Tsunami 2010: 40 million (13%) 2030: 72 million (20%) Baby Boomers (1946-1964)
1/21/2016 UPDATE ON THE AMERICAN GERIATRICS SOCIETY 2015 BEERS CRITERIA DISCLOSURE OBJECTIVES AGING GOALS BEERS CRITERIA
 UPDATE ON THE AMERICAN GERIATRICS SOCIETY 2015 BEERS CRITERIA DISCLOSURE I have no financial conflict of interest to disclose. Lacey Charbonneau, Pharm.D. PGY-1 Community Practice Resident Baptist Medical
UPDATE ON THE AMERICAN GERIATRICS SOCIETY 2015 BEERS CRITERIA DISCLOSURE I have no financial conflict of interest to disclose. Lacey Charbonneau, Pharm.D. PGY-1 Community Practice Resident Baptist Medical
Deprescribing Unnecessary Medications: A Four-Part Process
 Deprescribing Unnecessary Medications: A Four-Part Process Scott Endsley, MD Fam Pract Manag. 2018;25(3):28-32. Abstract and Introduction Introduction www.medscape.com Ms. Horatio is a 76-year-old patient
Deprescribing Unnecessary Medications: A Four-Part Process Scott Endsley, MD Fam Pract Manag. 2018;25(3):28-32. Abstract and Introduction Introduction www.medscape.com Ms. Horatio is a 76-year-old patient
Medication rationalization in patients with advanced medical illness
 Medication rationalization in patients with advanced medical illness Kiran Battu, BScPhm, RPh Sandra Porter, BScPhm, RPh Rachel Whitty, BScPhm, RPh, ACPR James Downar, MDCM, MHSc, FRCPC CHPC September
Medication rationalization in patients with advanced medical illness Kiran Battu, BScPhm, RPh Sandra Porter, BScPhm, RPh Rachel Whitty, BScPhm, RPh, ACPR James Downar, MDCM, MHSc, FRCPC CHPC September
Adjusting and Withdrawing Medications in the Elderly
 Adjusting and Withdrawing Medications in the Elderly Louise Mallet, B.Sc.Pharm., Pharm.D., CGP Professor in Clinical Pharmacy, Faculty of Pharmacy, University of Montreal Clinical Pharmacist in Geriatrics,
Adjusting and Withdrawing Medications in the Elderly Louise Mallet, B.Sc.Pharm., Pharm.D., CGP Professor in Clinical Pharmacy, Faculty of Pharmacy, University of Montreal Clinical Pharmacist in Geriatrics,
Polypharmacy. A CPPE distance learning programme
 A CPPE distance learning programme DLP 177 January 2016 Contents About CPPE distance learning programmes About this learning programme Glossary of key terms v vii ix Contents Section 1 The problem with
A CPPE distance learning programme DLP 177 January 2016 Contents About CPPE distance learning programmes About this learning programme Glossary of key terms v vii ix Contents Section 1 The problem with
A Geriatrician s Perspective on Successful Aging. Ariel Green, MD, MPH Assistant Professor of Medicine
 A Geriatrician s Perspective on Successful Aging Ariel Green, MD, MPH Assistant Professor of Medicine 1 Disclosures Johns Hopkins Clinical Research Scholars Program American College of Cardiology Foundation
A Geriatrician s Perspective on Successful Aging Ariel Green, MD, MPH Assistant Professor of Medicine 1 Disclosures Johns Hopkins Clinical Research Scholars Program American College of Cardiology Foundation
Prescribing Drugs to the Elderly
 Answers to your questions from University of Toronto experts Prescribing Drugs to the Elderly Can drugs do more harm than good? M.A. is a 90-year-old man living at home. He has dementia and due to wandering
Answers to your questions from University of Toronto experts Prescribing Drugs to the Elderly Can drugs do more harm than good? M.A. is a 90-year-old man living at home. He has dementia and due to wandering
The Geriatrician in the Trauma Service. Trauma Quality Improvement Program (TQIP) Annual Scientific Meeting and Training 2013
 Annual Scientific Meeting and Training 2013") The Geriatrician in the Trauma Service Trauma Quality Improvement Program (TQIP) Annual Scientific Meeting and Training 2013 Challenges of the Geriatric Trauma Patient Challenges of the Geriatric Patient
The Geriatrician in the Trauma Service Trauma Quality Improvement Program (TQIP) Annual Scientific Meeting and Training 2013 Challenges of the Geriatric Trauma Patient Challenges of the Geriatric Patient
Losartan and swollen ankles
 Losartan and swollen ankles Search Losartan Potassium and Hydrochlorothiazide official prescribing information for healthcare professionals. Includes: indications, dosage, adverse reactions. Q: I am a
Losartan and swollen ankles Search Losartan Potassium and Hydrochlorothiazide official prescribing information for healthcare professionals. Includes: indications, dosage, adverse reactions. Q: I am a
Medication Reviews within Care Homes. Catherine Armstrong
 Medication Reviews within Care Homes Catherine Armstrong What is a Medication Review? A structured, critical examination of a patient s medicines with the objective of reaching an agreement with the patient
Medication Reviews within Care Homes Catherine Armstrong What is a Medication Review? A structured, critical examination of a patient s medicines with the objective of reaching an agreement with the patient
Special thanks to the EJC Foundation for their support of Sanford Center Geriatric Specialty Clinic
 Special thanks to the EJC Foundation for their support of Sanford Center Geriatric Specialty Clinic Sanford Center for Aging 775-784-4744 med.unr.edu/aging Diabetes Management Series: From Selfmanagement
Special thanks to the EJC Foundation for their support of Sanford Center Geriatric Specialty Clinic Sanford Center for Aging 775-784-4744 med.unr.edu/aging Diabetes Management Series: From Selfmanagement
Demystifying the Complex Patient
 Demystifying the Complex Patient Jay Reaume, BSc, BScPhm, RPh, CDE Suzanne Singh, BScPhm, ACPR, PharmD, RPh May 30, 2015 Disclosures Jay Reaume No conflicts of interest to disclose Suzanne Singh No conflicts
Demystifying the Complex Patient Jay Reaume, BSc, BScPhm, RPh, CDE Suzanne Singh, BScPhm, ACPR, PharmD, RPh May 30, 2015 Disclosures Jay Reaume No conflicts of interest to disclose Suzanne Singh No conflicts
Family Medicine for English language students of Medical University of Lodz. Seminar 12. Elderly care. Przemysław Kardas MD PhD
 Family Medicine for English language students of Medical University of Lodz Seminar 12 Elderly care Przemysław Kardas MD PhD Europe is facing demographic challenge 2014 2080 2 3 Old vs young: major differences
Family Medicine for English language students of Medical University of Lodz Seminar 12 Elderly care Przemysław Kardas MD PhD Europe is facing demographic challenge 2014 2080 2 3 Old vs young: major differences
Warfarin PATIENT EDUCATION
 Warfarin PATIENT EDUCATION Information for patients taking warfarin Read this booklet to learn: What warfarin is and why you are taking it What blood tests you need to use warfarin safely How other medicines
Warfarin PATIENT EDUCATION Information for patients taking warfarin Read this booklet to learn: What warfarin is and why you are taking it What blood tests you need to use warfarin safely How other medicines
Disclosure. The elderly at risk: reducing medications safely to meet life s changes. Relevant financial relationships.
 The elderly at risk: reducing medications safely to meet life s changes Barbara Farrell BScPhm, PharmD, FCSHP European Society of Hospital Pharmacists Conference March 2017 Disclosure Relevant financial
The elderly at risk: reducing medications safely to meet life s changes Barbara Farrell BScPhm, PharmD, FCSHP European Society of Hospital Pharmacists Conference March 2017 Disclosure Relevant financial
Optimising prescribing in primary care in the face of multimorbidity and polypharmacy
 University of Dundee School of Medicine Optimising prescribing in primary care in the face of multimorbidity and polypharmacy Bruce Guthrie Professor of Primary Care Medicine, University of Dundee NICE
University of Dundee School of Medicine Optimising prescribing in primary care in the face of multimorbidity and polypharmacy Bruce Guthrie Professor of Primary Care Medicine, University of Dundee NICE
Alzheimer s Disease: Mary s Journey Through the Health-care System
 April 2009 Interdisciplinary Case Conference This Case revolves around a 72 year old, recently widowed, woman named Mary who is beginning to experience changes in her daily routine. While the potential
April 2009 Interdisciplinary Case Conference This Case revolves around a 72 year old, recently widowed, woman named Mary who is beginning to experience changes in her daily routine. While the potential
Let it go! Rationalising medicines for patients with life limiting illness
 Let it go! Rationalising medicines for patients with life limiting illness Inga Andrew Senior Clinical Pharmacist Northumbria Healthcare Trust E-mail: inga_andrew@northumbria-healthcare.nhs.uk Welcome
Let it go! Rationalising medicines for patients with life limiting illness Inga Andrew Senior Clinical Pharmacist Northumbria Healthcare Trust E-mail: inga_andrew@northumbria-healthcare.nhs.uk Welcome
Danielle Pierotti RN, PhD, AOCN, CHPN Chief Nurse/Director of Clinical Practice HCI Hospice. with you at every step
 Danielle Pierotti RN, PhD, AOCN, CHPN Chief Nurse/Director of Clinical Practice HCI Hospice Objectives Review current policy and environmental issues influencing medication choices at end of life Discuss
Danielle Pierotti RN, PhD, AOCN, CHPN Chief Nurse/Director of Clinical Practice HCI Hospice Objectives Review current policy and environmental issues influencing medication choices at end of life Discuss
Sample. Fractured Hip Post-Operative Orders. Legend < Mandatory fields o Optional fields. Height Allergies: List or o Up to date in electronic system
 Legend Mandatory fields o Optional fields Height Allergies: List or o Up to date in electronic system cm Weight Diagnosis kg Date (yyyy-mon-dd) Time (hh:mm) Anticipated Date Of Discharge (ADOD) o Greater
Legend Mandatory fields o Optional fields Height Allergies: List or o Up to date in electronic system cm Weight Diagnosis kg Date (yyyy-mon-dd) Time (hh:mm) Anticipated Date Of Discharge (ADOD) o Greater
Prescribing in the Elderly. Dr Alison Macrae and Dr Debbie Vest GPST2 Drs in Psychiatry
 Prescribing in the Elderly Dr Alison Macrae and Dr Debbie Vest GPST2 Drs in Psychiatry 24 th September 2014 Objectives Understand the significance of polypharmacy in the elderly Become familiar with the
Prescribing in the Elderly Dr Alison Macrae and Dr Debbie Vest GPST2 Drs in Psychiatry 24 th September 2014 Objectives Understand the significance of polypharmacy in the elderly Become familiar with the
Hypertension Management Controversies in the Elderly Patient
 Hypertension Management Controversies in the Elderly Patient Juan Bowen, MD Geriatric Update for the Primary Care Provider November 17, 2016 2016 MFMER slide-1 Disclosure No financial relationships No
Hypertension Management Controversies in the Elderly Patient Juan Bowen, MD Geriatric Update for the Primary Care Provider November 17, 2016 2016 MFMER slide-1 Disclosure No financial relationships No
Presented by: Ontario s Geriatric Steering Committee
 Polypharmacy: A Medication Management Opportunity Chris Fan-Lun, BScPhm, ACPR, CGP Clinical Practice Leader, Dept. of Pharmacy Services Mount Sinai Hospital, Sinai Health system Learning Objectives Provide
Polypharmacy: A Medication Management Opportunity Chris Fan-Lun, BScPhm, ACPR, CGP Clinical Practice Leader, Dept. of Pharmacy Services Mount Sinai Hospital, Sinai Health system Learning Objectives Provide
About ISMP Canada. Analysis Outputs: Safety Bulletins. Less is More: An Introduction to Deprescribing. canada.org
 Less is More: An Introduction to Deprescribing Lindsay Yoo, BSc, BScPhm, RPh, CDE, CGP, PharmD Medication Safety Analyst, ISMP Canada About ISMP Canada The Institute for Safe Medication Practices Canada
Less is More: An Introduction to Deprescribing Lindsay Yoo, BSc, BScPhm, RPh, CDE, CGP, PharmD Medication Safety Analyst, ISMP Canada About ISMP Canada The Institute for Safe Medication Practices Canada
Doreen Wan-Chow-Wah, MD, FRCPC Assistant Professor, Division of Geriatric Medicine, Department of Medicine McGill University Health Center Associate
 Doreen Wan-Chow-Wah, MD, FRCPC Assistant Professor, Division of Geriatric Medicine, Department of Medicine McGill University Health Center Associate member, Department of Oncology McGill University Medical
Doreen Wan-Chow-Wah, MD, FRCPC Assistant Professor, Division of Geriatric Medicine, Department of Medicine McGill University Health Center Associate member, Department of Oncology McGill University Medical
Fall Risk Assessment and Management. Elizabeth A. Phelan, MD, MS Assistant Professor, Medicine/Gerontology October 24, 2007
 Fall Risk Assessment and Management Elizabeth A. Phelan, MD, MS Assistant Professor, Medicine/Gerontology October 24, 2007 Slide 2 OBJECTIVES Know and understand: The importance of falls by older persons
Fall Risk Assessment and Management Elizabeth A. Phelan, MD, MS Assistant Professor, Medicine/Gerontology October 24, 2007 Slide 2 OBJECTIVES Know and understand: The importance of falls by older persons
Disclosure and Acknowledgements
 Greetings from Penn Nursing SOHN 37 TH ANNUAL CONGRESS AND NURSING SYMPOSIUM POLYPHARMACY AND OLDER ADULTS: HIGH RISK MEDS, TOO MANY MEDS, AND TOO FEW MEDS Sarah H. Kagan PhD, RN University of Pennsylvania,
Greetings from Penn Nursing SOHN 37 TH ANNUAL CONGRESS AND NURSING SYMPOSIUM POLYPHARMACY AND OLDER ADULTS: HIGH RISK MEDS, TOO MANY MEDS, AND TOO FEW MEDS Sarah H. Kagan PhD, RN University of Pennsylvania,
The Use, Misuse and Abuse of Alcohol, and Psychoactive Drugs among Older Persons
 The Use, Misuse and Abuse of Alcohol, and Psychoactive Drugs among Older Persons Alison A. Moore, MD, MPH Division of Geriatric Medicine David Geffen School of Medicine at UCLA Drinking in Older Adults:
The Use, Misuse and Abuse of Alcohol, and Psychoactive Drugs among Older Persons Alison A. Moore, MD, MPH Division of Geriatric Medicine David Geffen School of Medicine at UCLA Drinking in Older Adults:
Strategies to manage medication related falls in older people
 Strategies to manage medication related falls in older people ALLEN R. HUANG, MDCM, FRCPC RGPEO Refresher Day, April 5, 2017 www.ottawahospital.on.ca Affiliated with Affilié à DISCLOSURES I have no conflict
Strategies to manage medication related falls in older people ALLEN R. HUANG, MDCM, FRCPC RGPEO Refresher Day, April 5, 2017 www.ottawahospital.on.ca Affiliated with Affilié à DISCLOSURES I have no conflict
Mucky Meds: A (practical) approach the nightmare med list. Michelle Gibson, MD, CCFP (COE), FCFP and Erin Beattie, MD, CCFP
 approach the nightmare med list. Michelle Gibson, MD, CCFP (COE), FCFP and Erin Beattie, MD, CCFP") Mucky Meds: A (practical) approach the nightmare med list Michelle Gibson, MD, CCFP (COE), FCFP and Erin Beattie, MD, CCFP Faculty/Presenter Disclosure Faculty: Michelle Gibson Relationships with financial
Mucky Meds: A (practical) approach the nightmare med list Michelle Gibson, MD, CCFP (COE), FCFP and Erin Beattie, MD, CCFP Faculty/Presenter Disclosure Faculty: Michelle Gibson Relationships with financial
Dr Narender Goel MD (Internal Medicine and Nephrology) Financial Disclosure: None, Conflict of Interest: None
 Financial Disclosure: None, Conflict of Interest: None") Dr Narender Goel MD (Internal Medicine and Nephrology) drnarendergoel@gmail.com Financial Disclosure: None, Conflict of Interest: None 12 th December 2013, New York Visit us at: http://kidneyscience.info/
Dr Narender Goel MD (Internal Medicine and Nephrology) drnarendergoel@gmail.com Financial Disclosure: None, Conflict of Interest: None 12 th December 2013, New York Visit us at: http://kidneyscience.info/
Geri-PARDY! (2015 Beers Criteria) Pharmacology Edition
 Pharmacology Edition") Geri-PARDY! Pharmacology Edition (2015 Beers Criteria) Aurelio Muyot, MD, AGSF, FACP Assistant Professor College of Osteopathic Medicine Touro University Nevada Objectives Review the 2015 Beers Criteria
Geri-PARDY! Pharmacology Edition (2015 Beers Criteria) Aurelio Muyot, MD, AGSF, FACP Assistant Professor College of Osteopathic Medicine Touro University Nevada Objectives Review the 2015 Beers Criteria
For the Patient: LUAVPEM
 For the Patient: LUAVPEM Other Names: Second-Line Treatment Of Advanced Non- Small Cell Lung Cancer (NSCLC) With Pemetrexed LU = LUng AV = AdVanced PEM = PEMetrexed ABOUT THIS MEDICATION What is this drug
For the Patient: LUAVPEM Other Names: Second-Line Treatment Of Advanced Non- Small Cell Lung Cancer (NSCLC) With Pemetrexed LU = LUng AV = AdVanced PEM = PEMetrexed ABOUT THIS MEDICATION What is this drug
Medicines optimisation for older people with disabilities
 Medicines optimisation for older people with disabilities Riddhika Joshi Care of older people and stroke pharmacist Objectives Medicines Optimisation Examples Identifying patients PREVENT Targeting patients
Medicines optimisation for older people with disabilities Riddhika Joshi Care of older people and stroke pharmacist Objectives Medicines Optimisation Examples Identifying patients PREVENT Targeting patients
Home MURs for vulnerable older people
 8 This module is also online at pharmacymagazine.co.uk CPD MODULE module 258 Home MURs for vulnerable older people Contributing author: Lelly Oboh, consultant pharmacist, care of older people WORKING IN
8 This module is also online at pharmacymagazine.co.uk CPD MODULE module 258 Home MURs for vulnerable older people Contributing author: Lelly Oboh, consultant pharmacist, care of older people WORKING IN
POLYPHARMACY. A practical approach to deprescribing in care homes. Care Home Pharmacy Team. Herts Valleys Clinical Commissioning Group
 POLYPHARMACY A practical approach to deprescribing in care homes. Care Home Pharmacy Team Herts Valleys Clinical Commissioning Group Neeta Gulhane Specialist Pharmaceutical Advisor Care Homes The Care
POLYPHARMACY A practical approach to deprescribing in care homes. Care Home Pharmacy Team Herts Valleys Clinical Commissioning Group Neeta Gulhane Specialist Pharmaceutical Advisor Care Homes The Care
Polypharmacy, Medication Nihilism, and the art of de-prescribing
 Polypharmacy, Medication Nihilism, and the art of de-prescribing Temple Family Practice Review Course Leon S. Kraybill, MD, CMD Geriatrics, Lancaster General Hospital Physicians Division Chief, LGH Division
Polypharmacy, Medication Nihilism, and the art of de-prescribing Temple Family Practice Review Course Leon S. Kraybill, MD, CMD Geriatrics, Lancaster General Hospital Physicians Division Chief, LGH Division
DEPRESCRIBING. Phil St John CSIM Workshop
 DEPRESCRIBING Phil St John CSIM Workshop Conflict of Interest Disclosure Consultant for: none Speaker for: none Received grant/research support from: CIHR, MHRC, Riverview Foundation Received honoraria
DEPRESCRIBING Phil St John CSIM Workshop Conflict of Interest Disclosure Consultant for: none Speaker for: none Received grant/research support from: CIHR, MHRC, Riverview Foundation Received honoraria
Thank You to Our Sponsors: Evaluations & CE Credits. Featured Speakers. Conflict of Interest & Disclosure Statements 10/18/2016
 Thank You to Our Sponsors: University at Albany School of Public Health NYS Department of Health Conflict of Interest & Disclosure Statements The planners and presenters do not have any financial arrangements
Thank You to Our Sponsors: University at Albany School of Public Health NYS Department of Health Conflict of Interest & Disclosure Statements The planners and presenters do not have any financial arrangements
For the Patient: Everolimus tablets Other names: AFINITOR
 For the Patient: Everolimus tablets Other names: AFINITOR Everolimus (e'' ver oh' li mus) is a drug that is used to treat some types of cancer. It is a tablet that you take by mouth. Tell your doctor if
For the Patient: Everolimus tablets Other names: AFINITOR Everolimus (e'' ver oh' li mus) is a drug that is used to treat some types of cancer. It is a tablet that you take by mouth. Tell your doctor if
HA CONVENTION Effectiveness of Pharmacist-led Frail Elderly Medication Service in Acute Geriatric Ward
 Effectiveness of Pharmacist-led Frail Elderly Medication Service in Acute Geriatric Ward HA CONVENTION 2017 Candis Chang Pharmacist Department of Pharmacy Ruttonjee and Tang Shiu Kin Hospitals Background
Effectiveness of Pharmacist-led Frail Elderly Medication Service in Acute Geriatric Ward HA CONVENTION 2017 Candis Chang Pharmacist Department of Pharmacy Ruttonjee and Tang Shiu Kin Hospitals Background
Hypertension diagnosis (see detail document) Diabetic. Target less than 130/80mmHg
 Diabetic. Target less than 130/80mmHg") Hypertension diagnosis (see detail document) Non-diabetic Diabetic Very elderly (older than 80 years) Target less than 140/90mmHg Target less than 130/80mmHg Consider SBP target less than 150mmHg Non-diabetic
Hypertension diagnosis (see detail document) Non-diabetic Diabetic Very elderly (older than 80 years) Target less than 140/90mmHg Target less than 130/80mmHg Consider SBP target less than 150mmHg Non-diabetic
Polypharmacy in the Elderly
 Polypharmacy in the Elderly Physiotherapy Alberta Conference September 24 th 2016 Lesley Charles Associate Professor and Program Director Division of Care of the Elderly Department of Family Medicine,
Polypharmacy in the Elderly Physiotherapy Alberta Conference September 24 th 2016 Lesley Charles Associate Professor and Program Director Division of Care of the Elderly Department of Family Medicine,
Hypertension (JNC-8)
") Hypertension (JNC-8) Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! The 8 th Joint
Hypertension (JNC-8) Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! The 8 th Joint
Ketorolac injection. Supportive care
 Supportive care Ketorolac injection Supportive care: specialist medicines This leaflet provides information on a medicine called ketorolac which is used to treat pain that is difficult to control. It is
Supportive care Ketorolac injection Supportive care: specialist medicines This leaflet provides information on a medicine called ketorolac which is used to treat pain that is difficult to control. It is
Review of Current Literature 4/2/18 POLYPHARMACY IN ASSISTED LIVING EVIDENCE BASED APPROACH
 POLYPHARMACY IN ASSISTED LIVING A Evidence Based Approach to Management of Medication Regimen Complexity By Burton Korer, MSN, RN-BC, CPHQ EVIDENCE BASED APPROACH Evidence-based practice (EBP) is the conscientious
POLYPHARMACY IN ASSISTED LIVING A Evidence Based Approach to Management of Medication Regimen Complexity By Burton Korer, MSN, RN-BC, CPHQ EVIDENCE BASED APPROACH Evidence-based practice (EBP) is the conscientious
Residents Who Don t Sleep
 Residents Who Don t Sleep Case study........................................... An 86 yr. old woman has diagnoses of Alzheimer s disease, congestive heart failure, constipation, depression, hypertension
Residents Who Don t Sleep Case study........................................... An 86 yr. old woman has diagnoses of Alzheimer s disease, congestive heart failure, constipation, depression, hypertension
Deprescribing in CKD patients: Is less more? Speaker: Dr. Judith G. Marin, PharmD
 2016 Deprescribing in CKD patients: Is less more? Speaker: Dr. Judith G. Marin, PharmD Case Mr. Kid Ney is a 75 y/o patient who has been on dialysis for the last 4 years (PD, then HD). PMHx: HTN, DM,
2016 Deprescribing in CKD patients: Is less more? Speaker: Dr. Judith G. Marin, PharmD Case Mr. Kid Ney is a 75 y/o patient who has been on dialysis for the last 4 years (PD, then HD). PMHx: HTN, DM,
Alternatives to Physical Restraints
 Alternatives to Physical Restraints Case study. A 78 yr. old resident has a history of dementia (possibly Korsakoff s), chronic atrial fibrillation, CHF, COPD, frequent chest infections, obesity, heavy
Alternatives to Physical Restraints Case study. A 78 yr. old resident has a history of dementia (possibly Korsakoff s), chronic atrial fibrillation, CHF, COPD, frequent chest infections, obesity, heavy
Deprescribing with Confidence Dr Sanjay Suman MD FRCP
 Deprescribing with Confidence Dr Sanjay Suman MD FRCP Clinical Director Elderly Care and Stroke Medway NHS Foundation Trust Kent 45% of all medications prescribed for 65 years 1 1. Wynne et al Maturitas
Deprescribing with Confidence Dr Sanjay Suman MD FRCP Clinical Director Elderly Care and Stroke Medway NHS Foundation Trust Kent 45% of all medications prescribed for 65 years 1 1. Wynne et al Maturitas
Polypharmacy in the Elderly
 Polypharmacy in the Elderly Or How Scotland invented the Modern World Sir William Ferguson Anderson 1914-2001 Became the first Professor of Geriatrics in the world when he was appointed to the David Cargill
Polypharmacy in the Elderly Or How Scotland invented the Modern World Sir William Ferguson Anderson 1914-2001 Became the first Professor of Geriatrics in the world when he was appointed to the David Cargill
Early Intervention the Key to Geriatric Assessment: Geriatric Assessment Outreach Teams
 Early Intervention the Key to Geriatric Assessment: Geriatric Assessment Outreach Teams Regional Geriatric Program of Eastern Ontario Outpatient Clinics Geriatric Rehabilitation Unit Community Referrals
Early Intervention the Key to Geriatric Assessment: Geriatric Assessment Outreach Teams Regional Geriatric Program of Eastern Ontario Outpatient Clinics Geriatric Rehabilitation Unit Community Referrals
For the Patient: Mitoxantrone Other names:
 For the Patient: Mitoxantrone Other names: Mitoxantrone (mite-oh-zan-trone) is a drug that is used to treat many types of cancer. It is a blue liquid that is injected into a vein. Tell your doctor if you
For the Patient: Mitoxantrone Other names: Mitoxantrone (mite-oh-zan-trone) is a drug that is used to treat many types of cancer. It is a blue liquid that is injected into a vein. Tell your doctor if you
Polypharmacy and Elders. Leslie Baker, Pharm. D., RPh, CGP Sanford Center for Aging
 Polypharmacy and Elders Leslie Baker, Pharm. D., RPh, CGP Sanford Center for Aging Prescription Medication Use In Elders 1 13% of the US population is age 65+ Age 65 years 13% Age 65+ account for 34% of
Polypharmacy and Elders Leslie Baker, Pharm. D., RPh, CGP Sanford Center for Aging Prescription Medication Use In Elders 1 13% of the US population is age 65+ Age 65 years 13% Age 65+ account for 34% of
Specialist palliative care for patients with heart failure. Dr Katie Taylor Consultant in Palliative Medicine
 Specialist palliative care for patients with heart failure Dr Katie Taylor Consultant in Palliative Medicine Objectives Identify which patients to refer to hospice Review symptom management Think about
Specialist palliative care for patients with heart failure Dr Katie Taylor Consultant in Palliative Medicine Objectives Identify which patients to refer to hospice Review symptom management Think about
From MCI to Dementia DR YU- MIN LIN GERIATRICIAN AUG 2018
 From MCI to Dementia DR YU- MIN LIN GERIATRICIAN AUG 2018 Overview What is dementia? Common causes Normal cognitive decline Abnormal decline and mild cognitive impairment How do we manage dementia Can
From MCI to Dementia DR YU- MIN LIN GERIATRICIAN AUG 2018 Overview What is dementia? Common causes Normal cognitive decline Abnormal decline and mild cognitive impairment How do we manage dementia Can
Le politerapie complesse: l'arte del deprescribing. Andrea Corsonello IRCCS INRCA - Cosenza
 Le politerapie complesse: l'arte del deprescribing Andrea Corsonello IRCCS INRCA - Cosenza Archibald Leman Cochrane (12 January 1909 18 June 1988) was a Scottish doctor noted for his book Effectiveness
Le politerapie complesse: l'arte del deprescribing Andrea Corsonello IRCCS INRCA - Cosenza Archibald Leman Cochrane (12 January 1909 18 June 1988) was a Scottish doctor noted for his book Effectiveness
Less is More: Introduction to Deprescribing
 Less is More: Introduction to Deprescribing 7th Annual Pharmaceutical Care Conference Muscat, Oman Feb 23, 2017 Lindsay Yoo, BSc, BScPhm, RPh, CDE, CGP, PharmD Medication Safety Analyst, ISMP Canada About
Less is More: Introduction to Deprescribing 7th Annual Pharmaceutical Care Conference Muscat, Oman Feb 23, 2017 Lindsay Yoo, BSc, BScPhm, RPh, CDE, CGP, PharmD Medication Safety Analyst, ISMP Canada About
Medication Use in Older Adults
 Medication Use in Older Adults F. Michael Gloth, III, MD, AGSF, FACP, CMD Clinical Professor Department of Geriatrics, Florida State University College of Medicine Associate Professor of Medicine Division
Medication Use in Older Adults F. Michael Gloth, III, MD, AGSF, FACP, CMD Clinical Professor Department of Geriatrics, Florida State University College of Medicine Associate Professor of Medicine Division
AGS Annual Meeting May Sponsored by the Polypharmacy Special Interest Group and the Pharmacists Section
 AGS Annual Meeting May 2010 Sponsored by the Polypharmacy Special Interest Group and the Pharmacists Section No financial conflicts of interest Sponsored by the Polypharmacy Special Interest Group Thanks
AGS Annual Meeting May 2010 Sponsored by the Polypharmacy Special Interest Group and the Pharmacists Section No financial conflicts of interest Sponsored by the Polypharmacy Special Interest Group Thanks
5AB Dysrhythmia Interpretation and Management 2016
 5AB Dysrhythmia Interpretation and Management 2016 How to complete your biennial ECG review: A website has been created that contains the basic review information. Use this as a reference during your review.
5AB Dysrhythmia Interpretation and Management 2016 How to complete your biennial ECG review: A website has been created that contains the basic review information. Use this as a reference during your review.
Wednesday September 20 th CMT Regional Study Day. Dr Colin Mason, Consultant DME, Addenbrooke s Hospital
 Wednesday September 20 th CMT Regional Study Day Dr Colin Mason, Consultant DME, Addenbrooke s Hospital Develop a structured approach to a patient presenting with a fall Risk stratify who can go home and
Wednesday September 20 th CMT Regional Study Day Dr Colin Mason, Consultant DME, Addenbrooke s Hospital Develop a structured approach to a patient presenting with a fall Risk stratify who can go home and
Selecting the right patient for medication reviews
 Selecting the right patient for medication reviews Prof dr Petra Denig, Clinical Pharmacy & Pharmacology, University Medical Center Groningen, the Netherlands 2 Who is in need of medication review: can
Selecting the right patient for medication reviews Prof dr Petra Denig, Clinical Pharmacy & Pharmacology, University Medical Center Groningen, the Netherlands 2 Who is in need of medication review: can
Frailty. Nicholas Butler MD, MBA Department of Family Medicine University of Iowa
 Frailty Nicholas Butler MD, MBA Department of Family Medicine University of Iowa Doris 84 yo female who comes into your clinic with her daughter. She complains of feeling increasingly fatigued and just
Frailty Nicholas Butler MD, MBA Department of Family Medicine University of Iowa Doris 84 yo female who comes into your clinic with her daughter. She complains of feeling increasingly fatigued and just
For the Patient: Olaparib tablets Other names: LYNPARZA
 For the Patient: Olaparib tablets Other names: LYNPARZA Olaparib (oh lap' a rib) is a drug that is used to treat some types of cancer. It is a tablet that you take by mouth. Tell your doctor if you have
For the Patient: Olaparib tablets Other names: LYNPARZA Olaparib (oh lap' a rib) is a drug that is used to treat some types of cancer. It is a tablet that you take by mouth. Tell your doctor if you have
Featured Topic: Weight Loss Fiber, Grape Seed Extract, and Ginger (6 slides)
") Featured Topic: Weight Loss Fiber, Grape Seed Extract, and Ginger (6 slides) America s Obesity Problem 1/3 of children ages 6-19 are overweight or obese 70% of American adults are overweight or obese,
Featured Topic: Weight Loss Fiber, Grape Seed Extract, and Ginger (6 slides) America s Obesity Problem 1/3 of children ages 6-19 are overweight or obese 70% of American adults are overweight or obese,
Case Study #1 GUIDING PRINCIPLES FOR THE CARE OF OLDER ADULTS WITH MULTIMORBIDITY
 Case Study #1 GUIDING PRINCIPLES FOR THE CARE OF OLDER ADULTS WITH MULTIMORBIDITY Panel Moderator & Panelists: Edward Perrin, MD Banner icare Scott Bolhack, MD, MBA Sandra Brownstein, PharmD Paige Hector,
Case Study #1 GUIDING PRINCIPLES FOR THE CARE OF OLDER ADULTS WITH MULTIMORBIDITY Panel Moderator & Panelists: Edward Perrin, MD Banner icare Scott Bolhack, MD, MBA Sandra Brownstein, PharmD Paige Hector,
Evidence-Based Clinical Practice Guideline for Deprescribing Cholinesterase Inhibitors and Memantine in People with Dementia
 Evidence-Based Clinical Practice Guideline for Deprescribing Cholinesterase Inhibitors and Memantine in People with Dementia ADI 2018, Chicago FACULTY OF MEDICINE Dr Emily Reeve NHMRC Cognitive Decline
Evidence-Based Clinical Practice Guideline for Deprescribing Cholinesterase Inhibitors and Memantine in People with Dementia ADI 2018, Chicago FACULTY OF MEDICINE Dr Emily Reeve NHMRC Cognitive Decline
Transforming Care for the Elderly
 Transforming Care for the Elderly Session 2: Engaging Pharmacists & Interdisciplinary Care Teams to Improve Prescribing of Antipsychotics & to Reduce Polypharmacy January 11, 2017 3 @cfhi_fcass Welcome
Transforming Care for the Elderly Session 2: Engaging Pharmacists & Interdisciplinary Care Teams to Improve Prescribing of Antipsychotics & to Reduce Polypharmacy January 11, 2017 3 @cfhi_fcass Welcome
Amal AL-Anazi, BSc.(Pharm) Medication Safety Officer In Eastern Region
 Medication Safety Officer In Eastern Region") Risks Of Polypharmacy Amal AL-Anazi, BSc.(Pharm) Medication Safety Officer In Eastern Region What is Polypharmacy? Polypharmacy means many drugs. In practice, polypharmacy refers to the use of more medication
Risks Of Polypharmacy Amal AL-Anazi, BSc.(Pharm) Medication Safety Officer In Eastern Region What is Polypharmacy? Polypharmacy means many drugs. In practice, polypharmacy refers to the use of more medication
For the Patient: Bendamustine Other names: TREANDA
 For the Patient: Bendamustine Other names: TREANDA Bendamustine (ben'' da mus' teen) is a drug that is used to treat some types of cancer (lymphoma). It is a clear liquid that is injected into a vein.
For the Patient: Bendamustine Other names: TREANDA Bendamustine (ben'' da mus' teen) is a drug that is used to treat some types of cancer (lymphoma). It is a clear liquid that is injected into a vein.
Supplemental materials for:
 Supplemental materials for: Wallis KA, Andrews A, Henderson M. Swimming against the tide: primary care physicians views on deprescribing in everyday practice. Ann Fam Med. 2017;15(4):341-346. General Practice
Supplemental materials for: Wallis KA, Andrews A, Henderson M. Swimming against the tide: primary care physicians views on deprescribing in everyday practice. Ann Fam Med. 2017;15(4):341-346. General Practice
Road Blocks in Non-Cancer Palliative Care Obstacles observed from outpatient non-cancer palliative practice.
 Road Blocks in Non-Cancer Palliative Care Obstacles observed from outpatient non-cancer palliative practice. 25th Annual Palliative Education and Research Days, West Edmonton Mall. Edmonton. 2014 Amanda
Road Blocks in Non-Cancer Palliative Care Obstacles observed from outpatient non-cancer palliative practice. 25th Annual Palliative Education and Research Days, West Edmonton Mall. Edmonton. 2014 Amanda