DEPRESCRIBING. Phil St John CSIM Workshop
|
|
|
- Alberta Townsend
- 5 years ago
- Views:
Transcription
1 DEPRESCRIBING Phil St John CSIM Workshop
2 Conflict of Interest Disclosure Consultant for: none Speaker for: none Received grant/research support from: CIHR, MHRC, Riverview Foundation Received honoraria from: Co-chair Longterm care formulary, Winnipeg Regional Health Authority
3 JAMA Editorial, March 19, 1910

4 JAMA, 1937
5
6 KEY POINTS Life is complicated Need to enumerate problems, set goals of treatments, set acceptable trade offs and target therapy Need to understand the patient and family goals
7 Functional status and frailty should be considered in treatment decisions Start low, go slow, and be patient Can dither and change course in some cases, not in others
8 OLDER PEOPLE Are very heterogeneous Highly unpredictable drug effects On average, have more things wrong with them Have more doctors On average, have higher fat/water ratios Generally, longer half-life of lipophilic drugs On average, have lower renal function Generally value functional status more than life extension Have been on medications for longer On average, live less long
9 ALL PEOPLE Generally don t like side-effects Generally like symptomatic benefits Don t adhere to their medications Adhere better to simple regimens Don t always tell the complete truth Have friends and families Read the newspapers and/or internet Should know what we are thinking
10 DEFINITIONS Polypharmacy depends on setting initially four or more Risk Factors Polyproblems Polydoctors Age Gender Low Social Position
11 deprescribing is the cessation of long-term therapy, supervised by a clinician.
12 Clin Geriatr Med 28 (2012)
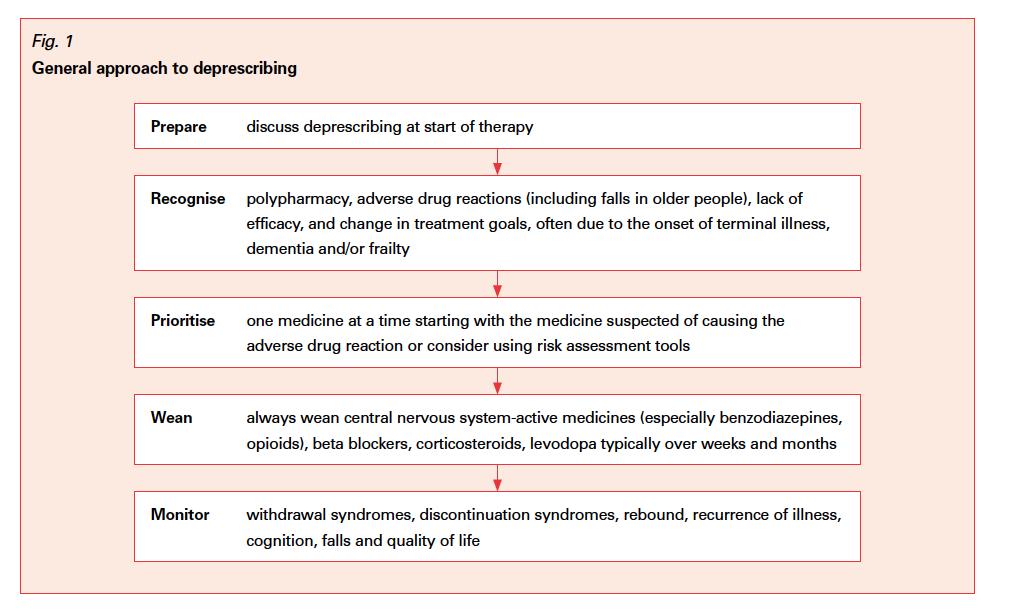
13 A GENERAL APPROACH Enumerate the problems in all domains Set goals and a plan for them Prioritize and balance Understand patient and family goals Determine the Global approach
14 Get an accurate and up to date medication list Find out how they got there Determine if and how they are taking them Determine risks and benefits Set up a treatment plan May involve starting new meds May involve stopping and or/tapering Should know the guidelines, but not always follow them all the time in all people
15 Should look things up Should take our time Tapering off (Start low, go slow in reverse) A process not an event Collaborative approach Family Friends Pharmacists Nursing Other physicians But should know who is in charge
16
17 Mrs S 93 year old Assisted Living resident Previous IADL and some ADL dependence Past History of falls, fractured hip, macular degeneration, cataracts, IHD (CABG), CVA, falls, atrial fibrillation, hypertension, CHF (normal systolic fcn), renal insufficiency, osteoporosis, vascular dementia, urinary incontinence Fall with hip fracture Transferred for rehab
18 MEDS Metoprolol 75 mg BID Ramipril 5 mg BID ISDN 15 mg TID ASA 325 mg daily Plavix 75 mg daily Lasix 80 mg daily Amlodipine 5 mg daily Donepezil 10 mg daily Ciprofloxacin 500 mg po daily Omeprazole 20 mg daily Tylenol 3 PRN Morphine prn Fentanyl patch 50 mcg daily Gabapentin 100 mg tid Oyxbutinin 5 mg bid Risperidone 1 mg BID Alendronate 70 mg weekly Vitamin D 400 units daily Zoplicone 7.5 mg QHS LMWH should she go back on warfarin?
19 CAN WE FIX THIS? Which medications are inappropriate? Which medications can be stopped? Which medications must be tapered? Which medications directly antagonize each other? Should she be on any other medications? Are the doses correct?

20
21
22
23
24 QUESTIONS Did she have a UTI? What happened two days after she was admitted to non-teaching medicine? When did her peripheral oedema start? Why? Why was she itchy? How would you go about medication reduction?
25 What is a prescribing cascade?
26 PRESCRIBING CASCADE DRUG 1 Adverse drug effect - misinterpreted as a new medical condition DRUG 2 Adverse drug effect misinterpreted as a new medical condition Slide 26
27 COMMON CASCADES Anticholinergics and cholinergics NSAIDS and antihypertensives Ca antagonists and diuretics Antipsychotics and antiparkinson agents
28
29 CASE 3 90 year old man Retired bombardier Living independently in a house in the community Previous history hypertension, osteoarthritis and poor sleep Fell and complained of pain in his back Admitted to family medicine
30 Meds HCT 12.5 mg daily Tylenol plain prn Diazepam 10 mg at HS
31 Admitted to family medicine with L1 fracture Started on heparin S/Q, Vitamin D, Calcium, Calcitonin, Tylenol 975 mg po tid, and Morphine 2.5 mg Q1H for breakthrough Attempted to taper his Valium to 7.5 mg every night
32 Paged at 10, 11, 12 and 1h Started back on original dose Fell and fractured hip three days later Transferred to teaching hospital with ortho
33 Added zopliclone Is this safer?
34 Transferred to Geriatrics Osteoporosis work-up unremarkable What would you do?
35 Agreed to taper zopiclone Attempted diazepam does reduction to 7.5 mg daily Paged hourly from 10 to 1 Restarted
36 Fell 8 days later and fractured two ribs

37 Bush Vows To Wipe Out Prescription- Drug Addiction Among Seniors
38 Pooled odds ratios in relation to not using benzodiazepines in studies aimed at withdrawal from these drugs at post-intervention.a. Gould R L et al. BJP 2014;204: by The Royal College of Psychiatrists
39 Conclusions Supervised benzodiazepine withdrawal augmented with psychotherapy should be considered in older people, although pragmatic reasons may necessitate consideration of other strategies such as medication review.
40 From: Meta-analysis of the Impact of 9 Medication Classes on Falls in Elderly Persons Arch Intern Med. 2009;169(21): doi: /archinternmed Figure Legend: Medications and falls: meta analysis results. Odds ratios and 95% credible intervals or 95% confidence intervals on a logarithmic scale for individual or pooled study data for each class of medication. Outcome is occurrence of at least 1 fall. NSAIDs indicates nonsteroidal anti-inflammatory drugs. Date of download: 9/24/2014 Copyright 2014 American Medical Association. All rights reserved.
41
42
43
44
45
46

47 Undercover Cop Never Knew Selling Drugs Was Such Hard Work MARCH 5, 2003 ISSUE 39 08
48 Mr O 87 year old man, living in nursing home Relocated to rehab unit when NH evacuated Previous history HBP DM2 IHD stents and CABG CHF class III - IV Arrest with ICD PVD
49 Falls OA Osteoporosis Prostate Cancer with retention and foley Macular Degeneration CRF Vascular Dementia Dependent in BADLs Aggressive and violent behaviour Atrial fibrillation
50 MEDS Metoprolol 50 mg po BID Warfarin Clopidogrel 75 mg daily ASA 81 mg daily Glyburide 5 mg daily ISDN 15 mg tid Tylenol prn Finasteride Ditropan 5 mg bid Flomax 0.4 mg daily Lasix 80 mg po BID Donepezil 5 mg daily Risperidone 5 mg BID
51 What medications are working in the opposite direction? Would you streamline meds? How would you go about this?
52 COMMON DRUG-DRUG INTERACTIONS Combination ACE inhibitor + diuretic ACE inhibitor + potassium Antiarrhythmic + diuretic Benzodiazepine + antidepressant, antipsychotic, or benzodiazepine Calcium channel blocker + diuretic or nitrate Risk Hypotension, hyperkalemia Hyperkalemia Electrolyte imbalance, arrhythmias Confusion, sedation, falls Hypotension Digitalis + diuretic Arrhythmias Slide 52
53 Selected High-Risk Drugs Copyright restrictions may apply. Steinman, M. A. et al. JAMA 2010;304:
54 COMMON DRUG-DISEASE INTERACTIONS Obesity alters VD of lipophilic drugs Ascites alters VD of hydrophilic drugs Dementia may sensitivity, induce paradoxical reactions to drugs with CNS or anticholinergic activity Renal or hepatic impairment may impair detoxification and excretion of drugs
55 BEFORE PRESCRIBING A NEW DRUG, CONSIDER: Is this medication necessary? What are the therapeutic end points? Do the benefits outweigh the risks? Is it used to treat effects of another drug? Could 1 drug be used to treat 2 conditions? Could it interact with diseases, other drugs? Does patient know what it s for, how to take it, and what ADEs to look for? Slide 55
56 PRINCIPLES OF DRUG REVIEW Ask patient to bring in all medications (prescribed, OTC, supplements) for review LOOK AT THEIR MEDS LOOK AT AIDES DPIN Ask about side effects and screen for drug and disease interactions Look for duplicate therapies or pharmacologic effect Eliminate unnecessary medications and simplify dosing regimens Get collateral family, other doctors, pharmacist
57 NONADHERENCE May be as high as 50% among older patients May result from clinician s failure to consider patient s financial, cognitive, functional status May result from patient s beliefs and understanding of drugs and diseases Slide 57
58 CONCLUSIONS This is a complicated area Need to think less about polypharmacy and more about appropriateness
Deconstructing Polypharmacy. Alan B. Douglass, M.D. Director
 Deconstructing Polypharmacy Alan B. Douglass, M.D. Director Recognize this patient? Mrs. Brown- 82 years young Active Medical Problems Hypertension Hyperlipidemia Type 2 Diabetes Peripheral edema Osteoarthritis
Deconstructing Polypharmacy Alan B. Douglass, M.D. Director Recognize this patient? Mrs. Brown- 82 years young Active Medical Problems Hypertension Hyperlipidemia Type 2 Diabetes Peripheral edema Osteoarthritis
A Primer on Safe Prescribing to the Elderly. Dr. John Puxty
 A Primer on Safe Prescribing to the Elderly Dr. John Puxty Learning Objectives Describe an approach to safe prescribing for older patients. Appreciate the significance and causes of Polypharmacy. Identify
A Primer on Safe Prescribing to the Elderly Dr. John Puxty Learning Objectives Describe an approach to safe prescribing for older patients. Appreciate the significance and causes of Polypharmacy. Identify
Medication Reviews within Care Homes. Catherine Armstrong
 Medication Reviews within Care Homes Catherine Armstrong What is a Medication Review? A structured, critical examination of a patient s medicines with the objective of reaching an agreement with the patient
Medication Reviews within Care Homes Catherine Armstrong What is a Medication Review? A structured, critical examination of a patient s medicines with the objective of reaching an agreement with the patient
If a bad thing is happening to a patient, a drug did it until proven otherwise
 Dr Vicki s First Rule of Geriatrics Deprescribing in the Elderly Victoria Braund MD, FACP, CMD Director, Division of Geriatrics NorthShore University HealthSystem Medical Director, Brandel Health & Rehab
Dr Vicki s First Rule of Geriatrics Deprescribing in the Elderly Victoria Braund MD, FACP, CMD Director, Division of Geriatrics NorthShore University HealthSystem Medical Director, Brandel Health & Rehab
Polypharmacy & De-prescribing In Older Adults
 Polypharmacy & De-prescribing In Older Adults Maryland Association of Osteopathic Physicians Annual Meeting September 15, 2018 Elizabeth Phung, DO Lead Clinical Associate Physician Beacham Center for Geriatric
Polypharmacy & De-prescribing In Older Adults Maryland Association of Osteopathic Physicians Annual Meeting September 15, 2018 Elizabeth Phung, DO Lead Clinical Associate Physician Beacham Center for Geriatric
Presented by: Ontario s Geriatric Steering Committee
 Polypharmacy: A Medication Management Opportunity Chris Fan-Lun, BScPhm, ACPR, CGP Clinical Practice Leader, Dept. of Pharmacy Services Mount Sinai Hospital, Sinai Health system Learning Objectives Provide
Polypharmacy: A Medication Management Opportunity Chris Fan-Lun, BScPhm, ACPR, CGP Clinical Practice Leader, Dept. of Pharmacy Services Mount Sinai Hospital, Sinai Health system Learning Objectives Provide
POLYPHARMACY IN OLDER ADULTS AND BEERS CRITERIA UPDATE
 POLYPHARMACY IN OLDER ADULTS AND BEERS CRITERIA UPDATE Jeannie Kim Lee, PharmD, BCPS, CGP Clinical Pharmacy Director College of Pharmacy The University of Arizona Learning Objectives: State the risks of
POLYPHARMACY IN OLDER ADULTS AND BEERS CRITERIA UPDATE Jeannie Kim Lee, PharmD, BCPS, CGP Clinical Pharmacy Director College of Pharmacy The University of Arizona Learning Objectives: State the risks of
Pharmaceutical Care for Geriatrics
 Continuing Professional Pharmacy Development Program Pharmaceutical Care for Geriatrics Presented by: Alla El-Awaisi; MPharm, MRPharmS, MSc Event Organizer: Dr. Nadir Kheir; PhD Disclaimer: PRESENTING
Continuing Professional Pharmacy Development Program Pharmaceutical Care for Geriatrics Presented by: Alla El-Awaisi; MPharm, MRPharmS, MSc Event Organizer: Dr. Nadir Kheir; PhD Disclaimer: PRESENTING
DEPRESCRIBING IN THE ELDERLY
 DEPRESCRIBING IN THE ELDERLY G E R I A T R I C S R E F R E S H E R D A Y W E D N E S D A Y, A P R I L 5 TH, 2 0 1 7 V É R O N I Q U E F R E N C H M E R K L E Y, M D, C C F P ( C O E ) B R U Y È R E C O
DEPRESCRIBING IN THE ELDERLY G E R I A T R I C S R E F R E S H E R D A Y W E D N E S D A Y, A P R I L 5 TH, 2 0 1 7 V É R O N I Q U E F R E N C H M E R K L E Y, M D, C C F P ( C O E ) B R U Y È R E C O
PRESCRIBING IN THE ELDERLY. CARE HOME PHARMACY TEAM Bhavini Shah, Eleesha Pentiah & Puja Vyas
 PRESCRIBING IN THE ELDERLY CARE HOME PHARMACY TEAM Bhavini Shah, Eleesha Pentiah & Puja Vyas LEARNING OUTCOMES Medicines Optimisation The effects of aging on health and medicines. Polypharmacy Acute Kidney
PRESCRIBING IN THE ELDERLY CARE HOME PHARMACY TEAM Bhavini Shah, Eleesha Pentiah & Puja Vyas LEARNING OUTCOMES Medicines Optimisation The effects of aging on health and medicines. Polypharmacy Acute Kidney
Geriatric Pharmacology. Kwi Bulow, M.D. Clinical Professor of Medicine Director, Academic Geriatric Resource Center
 Geriatric Pharmacology Kwi Bulow, M.D. Clinical Professor of Medicine Director, Academic Geriatric Resource Center Silver Tsunami 2010: 40 million (13%) 2030: 72 million (20%) Baby Boomers (1946-1964)
Geriatric Pharmacology Kwi Bulow, M.D. Clinical Professor of Medicine Director, Academic Geriatric Resource Center Silver Tsunami 2010: 40 million (13%) 2030: 72 million (20%) Baby Boomers (1946-1964)
Deprescribing Unnecessary Medications: A Four-Part Process
 Deprescribing Unnecessary Medications: A Four-Part Process Scott Endsley, MD Fam Pract Manag. 2018;25(3):28-32. Abstract and Introduction Introduction www.medscape.com Ms. Horatio is a 76-year-old patient
Deprescribing Unnecessary Medications: A Four-Part Process Scott Endsley, MD Fam Pract Manag. 2018;25(3):28-32. Abstract and Introduction Introduction www.medscape.com Ms. Horatio is a 76-year-old patient
OBJECTIVES. Key issues in geriatric pharmacology. Effects of age on pharmacokinetics and pharmacodynamics
 PHARMACOTHERAPY 1 OBJECTIVES 2 Know and understand: Key issues in geriatric pharmacology Effects of age on pharmacokinetics and pharmacodynamics Risk factors for adverse drug events for older patients
PHARMACOTHERAPY 1 OBJECTIVES 2 Know and understand: Key issues in geriatric pharmacology Effects of age on pharmacokinetics and pharmacodynamics Risk factors for adverse drug events for older patients
COMMON DRUG RELATED PROBLEMS SEEN IN PACE AND MECHANISMS TO MITIGATE RISK
 COMMON DRUG RELATED PROBLEMS SEEN IN PACE AND MECHANISMS TO MITIGATE RISK Robert L Alesiani, PharmD, CGP Chief Pharmacotherapy Officer CareKinesis, Inc. (a Tabula Rasa Healthcare Company) 2 3 4 5 Pharmacogenomics
COMMON DRUG RELATED PROBLEMS SEEN IN PACE AND MECHANISMS TO MITIGATE RISK Robert L Alesiani, PharmD, CGP Chief Pharmacotherapy Officer CareKinesis, Inc. (a Tabula Rasa Healthcare Company) 2 3 4 5 Pharmacogenomics
PHARMACOTHERAPY IN THE OLDER PERSON NAMIRAH JAMSHED M.B;B.S ASSOCIATE PROFESSOR UTSW MEDICAL CENTER DALLAS
 1 PHARMACOTHERAPY IN THE OLDER PERSON NAMIRAH JAMSHED M.B;B.S ASSOCIATE PROFESSOR UTSW MEDICAL CENTER DALLAS OBJECTIVES 2 Know and understand: Key issues in geriatric pharmacology Effects of age on pharmacokinetics
1 PHARMACOTHERAPY IN THE OLDER PERSON NAMIRAH JAMSHED M.B;B.S ASSOCIATE PROFESSOR UTSW MEDICAL CENTER DALLAS OBJECTIVES 2 Know and understand: Key issues in geriatric pharmacology Effects of age on pharmacokinetics
1/21/2016 UPDATE ON THE AMERICAN GERIATRICS SOCIETY 2015 BEERS CRITERIA DISCLOSURE OBJECTIVES AGING GOALS BEERS CRITERIA
 UPDATE ON THE AMERICAN GERIATRICS SOCIETY 2015 BEERS CRITERIA DISCLOSURE I have no financial conflict of interest to disclose. Lacey Charbonneau, Pharm.D. PGY-1 Community Practice Resident Baptist Medical
UPDATE ON THE AMERICAN GERIATRICS SOCIETY 2015 BEERS CRITERIA DISCLOSURE I have no financial conflict of interest to disclose. Lacey Charbonneau, Pharm.D. PGY-1 Community Practice Resident Baptist Medical
Transitions of Care & Medication Reconciliation Ashley King, PharmD, BCGP Clinical Pharmacist LECOM Health March 2018
 Transitions of Care & Medication Reconciliation Ashley King, PharmD, BCGP Clinical Pharmacist LECOM Health March 2018 Objectives Identify when to complete medication reconciliation Understand the importance
Transitions of Care & Medication Reconciliation Ashley King, PharmD, BCGP Clinical Pharmacist LECOM Health March 2018 Objectives Identify when to complete medication reconciliation Understand the importance
Polypharmacy and Deprescribing for Older People
 Polypharmacy and Deprescribing for Older People Sarah Hilmer Head of Department, Clinical Pharmacology and Senior Staff Specialist Aged Care, RNSH Conjoint Professor of Geriatric Pharmacology, Sydney University
Polypharmacy and Deprescribing for Older People Sarah Hilmer Head of Department, Clinical Pharmacology and Senior Staff Specialist Aged Care, RNSH Conjoint Professor of Geriatric Pharmacology, Sydney University
Maximizing Medication Safety UNIVERSITY OF HAWAII AUGUST 31, 2016
 Maximizing Medication Safety UNIVERSITY OF HAWAII AUGUST 31, 2016 Adverse Drug Events (ADE s) RISK FACTORS FOR Adverse Drug Events (ADEs) 6 or more concurrent chronic conditions 12 or more doses of drugs/day
Maximizing Medication Safety UNIVERSITY OF HAWAII AUGUST 31, 2016 Adverse Drug Events (ADE s) RISK FACTORS FOR Adverse Drug Events (ADEs) 6 or more concurrent chronic conditions 12 or more doses of drugs/day
Transforming Care for the Elderly
 Transforming Care for the Elderly Session 2: Engaging Pharmacists & Interdisciplinary Care Teams to Improve Prescribing of Antipsychotics & to Reduce Polypharmacy January 11, 2017 3 @cfhi_fcass Welcome
Transforming Care for the Elderly Session 2: Engaging Pharmacists & Interdisciplinary Care Teams to Improve Prescribing of Antipsychotics & to Reduce Polypharmacy January 11, 2017 3 @cfhi_fcass Welcome
MEDICATION APPROPRIATENESS FOR THE AGING POPULATION. Building Partnerships for Successful Aging
 MEDICATION APPROPRIATENESS FOR THE AGING POPULATION Building Partnerships for Successful Aging Learning objectives Appreciate complexities involved in making appropriate clinical decisions in older adults
MEDICATION APPROPRIATENESS FOR THE AGING POPULATION Building Partnerships for Successful Aging Learning objectives Appreciate complexities involved in making appropriate clinical decisions in older adults
START, STOPP, Beers Oh My! Navigating the World of Geriatric Pharmacy
 START, STOPP, Beers Oh My! Navigating the World of Geriatric Pharmacy Jessica DiLeo, PharmD Kate Murphy, PharmD OBJECTIVES Identify pharmacodynamic and pharmacokinetic parameters that may influence treatment
START, STOPP, Beers Oh My! Navigating the World of Geriatric Pharmacy Jessica DiLeo, PharmD Kate Murphy, PharmD OBJECTIVES Identify pharmacodynamic and pharmacokinetic parameters that may influence treatment
Objectives. Case Ruby. 1- Warfarin. 1- Warfarin. Warfarin discontinuation 8/13/ DRUGS TO STOP GIVING HOSPICE PATIENTS
 Objectives 10 DRUGS TO STOP GIVING HOSPICE PATIENTS Richard E. Allen MD, MPH Hospice Medical Director Family Medicine Residency Director Salt Lake City, Utah 2 Recognize 10 commonly prescribed medications
Objectives 10 DRUGS TO STOP GIVING HOSPICE PATIENTS Richard E. Allen MD, MPH Hospice Medical Director Family Medicine Residency Director Salt Lake City, Utah 2 Recognize 10 commonly prescribed medications
Polypharmacy and Polymorbid Patients: Practical Tips and Tricks
 Polypharmacy and Polymorbid Patients: Practical Tips and Tricks November 2, 2013 Faculty/Presenter Disclosure Faculty: Chris Fan-Lun, BScPhm, ACPR, CGP Pharmacist - Geriatric Medicine Clinical Practice
Polypharmacy and Polymorbid Patients: Practical Tips and Tricks November 2, 2013 Faculty/Presenter Disclosure Faculty: Chris Fan-Lun, BScPhm, ACPR, CGP Pharmacist - Geriatric Medicine Clinical Practice
Mucky Meds: A (practical) approach the nightmare med list. Michelle Gibson, MD, CCFP (COE), FCFP and Erin Beattie, MD, CCFP
 approach the nightmare med list. Michelle Gibson, MD, CCFP (COE), FCFP and Erin Beattie, MD, CCFP") Mucky Meds: A (practical) approach the nightmare med list Michelle Gibson, MD, CCFP (COE), FCFP and Erin Beattie, MD, CCFP Faculty/Presenter Disclosure Faculty: Michelle Gibson Relationships with financial
Mucky Meds: A (practical) approach the nightmare med list Michelle Gibson, MD, CCFP (COE), FCFP and Erin Beattie, MD, CCFP Faculty/Presenter Disclosure Faculty: Michelle Gibson Relationships with financial
Preventing Falls in Older Adults A Matter of Safety
 Preventing Falls in Older Adults A Matter of Safety Roger Tam, BSc. Pharm. Wal-Mart Clinical Designated Pharmacist Falls Prevention Pharmacist Specialist NCCHC-Pre/Post Test Educator Q.U.I.T Educator Overview
Preventing Falls in Older Adults A Matter of Safety Roger Tam, BSc. Pharm. Wal-Mart Clinical Designated Pharmacist Falls Prevention Pharmacist Specialist NCCHC-Pre/Post Test Educator Q.U.I.T Educator Overview
< = > less is more. De-diagnosing De-prescribing Non-testing
 < = > less is more De-diagnosing De-prescribing Non-testing Who says? Overdiagnosis Polypharmacy False positives Too much medicine Risk aversion $$$ Sources Prof David Le Couteur, Clin Pharm and Aged Care
< = > less is more De-diagnosing De-prescribing Non-testing Who says? Overdiagnosis Polypharmacy False positives Too much medicine Risk aversion $$$ Sources Prof David Le Couteur, Clin Pharm and Aged Care
Medicines in Older People- Some of the Key Issues
 Medicines in Older People- Some of the Key Issues Associate Professor Vasi Naganathan Sydney Medical School Consultant Geriatrician, Centre for Education and Research on Ageing Concord Hospital, Sydney,
Medicines in Older People- Some of the Key Issues Associate Professor Vasi Naganathan Sydney Medical School Consultant Geriatrician, Centre for Education and Research on Ageing Concord Hospital, Sydney,
Prescribing appropriately. May 2016
 Prescribing appropriately May 2016 Prescribing process Prescribing process Patient problem Core knowledge Decision to prescribe Medicines Choice Modification Habit Formulation Dose Frequency Preferred
Prescribing appropriately May 2016 Prescribing process Prescribing process Patient problem Core knowledge Decision to prescribe Medicines Choice Modification Habit Formulation Dose Frequency Preferred
GERIATRICS 101. Victoria L. Braund, MD, FACP, CMD. Director, Division of Geriatrics, NorthShore Medical Director, Symphony of Evanston
 GERIATRICS 101 Victoria L. Braund, MD, FACP, CMD Director, Division of Geriatrics, NorthShore Medical Director, Symphony of Evanston LET S REVIEW Medicare Hospice Pain mgmt. Bowel business Delirium Sleep
GERIATRICS 101 Victoria L. Braund, MD, FACP, CMD Director, Division of Geriatrics, NorthShore Medical Director, Symphony of Evanston LET S REVIEW Medicare Hospice Pain mgmt. Bowel business Delirium Sleep
AGS Annual Meeting May Sponsored by the Polypharmacy Special Interest Group and the Pharmacists Section
 AGS Annual Meeting May 2010 Sponsored by the Polypharmacy Special Interest Group and the Pharmacists Section No financial conflicts of interest Sponsored by the Polypharmacy Special Interest Group Thanks
AGS Annual Meeting May 2010 Sponsored by the Polypharmacy Special Interest Group and the Pharmacists Section No financial conflicts of interest Sponsored by the Polypharmacy Special Interest Group Thanks
From MCI to Dementia DR YU- MIN LIN GERIATRICIAN AUG 2018
 From MCI to Dementia DR YU- MIN LIN GERIATRICIAN AUG 2018 Overview What is dementia? Common causes Normal cognitive decline Abnormal decline and mild cognitive impairment How do we manage dementia Can
From MCI to Dementia DR YU- MIN LIN GERIATRICIAN AUG 2018 Overview What is dementia? Common causes Normal cognitive decline Abnormal decline and mild cognitive impairment How do we manage dementia Can
Pharmacology in the Elderly
 Pharmacology in the Elderly James Hardy Geriatrician, Royal North Shore Hospital A recent consultation Aspirin Clopidogrel Warfarin Coloxyl with senna Clearlax Methotrexate Paracetamol Pantoprazole Cholecalciferol
Pharmacology in the Elderly James Hardy Geriatrician, Royal North Shore Hospital A recent consultation Aspirin Clopidogrel Warfarin Coloxyl with senna Clearlax Methotrexate Paracetamol Pantoprazole Cholecalciferol
Meds and Falls: Keep in Step with your Meds
 Meds and Falls: Keep in Step with your Meds Donna Bartlett PharmD, CGP, RPh Associate Professor-Pharmacy Practice MCPHS University Clinical Pharmacist-MCPHS University- Pharmacy Outreach Program donna.bartlett@mcphs.edu
Meds and Falls: Keep in Step with your Meds Donna Bartlett PharmD, CGP, RPh Associate Professor-Pharmacy Practice MCPHS University Clinical Pharmacist-MCPHS University- Pharmacy Outreach Program donna.bartlett@mcphs.edu
Deprescribing in CKD patients: Is less more? Speaker: Dr. Judith G. Marin, PharmD
 2016 Deprescribing in CKD patients: Is less more? Speaker: Dr. Judith G. Marin, PharmD Case Mr. Kid Ney is a 75 y/o patient who has been on dialysis for the last 4 years (PD, then HD). PMHx: HTN, DM,
2016 Deprescribing in CKD patients: Is less more? Speaker: Dr. Judith G. Marin, PharmD Case Mr. Kid Ney is a 75 y/o patient who has been on dialysis for the last 4 years (PD, then HD). PMHx: HTN, DM,
Polypharmacy. Polypharmacy. Suboptimal Prescribing in Older Adults. Kenneth Schmader, MD Professor of Medicine-Geriatrics
 Polypharmacy Kenneth Schmader, MD Professor of Medicine-Geriatrics Polypharmacy Definition Causes Consequences Prevention/management Suboptimal Prescribing in Older Adults Overuse Polypharmacy Underuse
Polypharmacy Kenneth Schmader, MD Professor of Medicine-Geriatrics Polypharmacy Definition Causes Consequences Prevention/management Suboptimal Prescribing in Older Adults Overuse Polypharmacy Underuse
Polypharmacy and the Older Adult. Leslie Baker, PharmD, BCGP Umanga Sharma, MD
 Polypharmacy and the Older Adult Leslie Baker, PharmD, BCGP Umanga Sharma, MD Objectives Identify what polypharmacy is Identify factors leading to polypharmacy Discuss consequences of polypharmacy Identify
Polypharmacy and the Older Adult Leslie Baker, PharmD, BCGP Umanga Sharma, MD Objectives Identify what polypharmacy is Identify factors leading to polypharmacy Discuss consequences of polypharmacy Identify
Management of DM in Older Adults: It s not all about sugar! Who needs treatment for DM? Peggy Odegard, Pharm.D., BCPS, CDE
 Management of DM in Older Adults: It s not all about sugar! Peggy Odegard, Pharm.D., BCPS, CDE Who needs treatment for DM? 87 year old, frail male with moderately severe dementia living in NH with persistent
Management of DM in Older Adults: It s not all about sugar! Peggy Odegard, Pharm.D., BCPS, CDE Who needs treatment for DM? 87 year old, frail male with moderately severe dementia living in NH with persistent
Katee Kindler, PharmD, BCACP
 Speaker Introduction Katee Kindler, PharmD, BCACP Current Practice: Clinical Pharmacy Specialist Ambulatory Care, St. Vincent Indianapolis Assistant Professor of Pharmacy Practice, Manchester University,
Speaker Introduction Katee Kindler, PharmD, BCACP Current Practice: Clinical Pharmacy Specialist Ambulatory Care, St. Vincent Indianapolis Assistant Professor of Pharmacy Practice, Manchester University,
Evidence-Based Clinical Practice Guideline for Deprescribing Cholinesterase Inhibitors and Memantine in People with Dementia
 Evidence-Based Clinical Practice Guideline for Deprescribing Cholinesterase Inhibitors and Memantine in People with Dementia ADI 2018, Chicago FACULTY OF MEDICINE Dr Emily Reeve NHMRC Cognitive Decline
Evidence-Based Clinical Practice Guideline for Deprescribing Cholinesterase Inhibitors and Memantine in People with Dementia ADI 2018, Chicago FACULTY OF MEDICINE Dr Emily Reeve NHMRC Cognitive Decline
STOPP and START criteria October 2011
 # START and STOPP are newer criteria to identify potentially inappropriate medications in elderly, including drug drug and drug disease interactions, drugs which increase risk of falls and drugs which
# START and STOPP are newer criteria to identify potentially inappropriate medications in elderly, including drug drug and drug disease interactions, drugs which increase risk of falls and drugs which
Geriatric Pharmacology
 Geriatric Pharmacology Janice Scheufler R.Ph.,PharmD, FASCP Clinical Pharmacist Hospice of the Western Reserve Objectives List three risk factors for adverse drug events in the elderly Discuss two physiological
Geriatric Pharmacology Janice Scheufler R.Ph.,PharmD, FASCP Clinical Pharmacist Hospice of the Western Reserve Objectives List three risk factors for adverse drug events in the elderly Discuss two physiological
Early Intervention the Key to Geriatric Assessment: Geriatric Assessment Outreach Teams
 Early Intervention the Key to Geriatric Assessment: Geriatric Assessment Outreach Teams Regional Geriatric Program of Eastern Ontario Outpatient Clinics Geriatric Rehabilitation Unit Community Referrals
Early Intervention the Key to Geriatric Assessment: Geriatric Assessment Outreach Teams Regional Geriatric Program of Eastern Ontario Outpatient Clinics Geriatric Rehabilitation Unit Community Referrals
Geri-PARDY! (2015 Beers Criteria) Pharmacology Edition
 Pharmacology Edition") Geri-PARDY! Pharmacology Edition (2015 Beers Criteria) Aurelio Muyot, MD, AGSF, FACP Assistant Professor College of Osteopathic Medicine Touro University Nevada Objectives Review the 2015 Beers Criteria
Geri-PARDY! Pharmacology Edition (2015 Beers Criteria) Aurelio Muyot, MD, AGSF, FACP Assistant Professor College of Osteopathic Medicine Touro University Nevada Objectives Review the 2015 Beers Criteria
A C A D E M I C D E TA I L I N G C H O O S I N G W I S E LY C O N F E R E N C E O C T 2 1, PA M M C L E A N - V E Y S E Y B S C P H A R M D R
 PPI DEPRESCRIBING Canadian Deprescribing Network (CaDeN) goals are to: Reduce harm by raising awareness and cutting risky prescriptions for seniors by 50% by 2020. Promote health by ensuring access to
PPI DEPRESCRIBING Canadian Deprescribing Network (CaDeN) goals are to: Reduce harm by raising awareness and cutting risky prescriptions for seniors by 50% by 2020. Promote health by ensuring access to
Great Low Cost in SNF-NF Jabbar Fazeli, MD Maine Medical Directors Association
 Great Care @ Low Cost in SNF-NF Jabbar Fazeli, MD Maine Medical Directors Association Principles Best interest of the patient (SNF) and resident (NF) comes first. Lowest cost to achieve the same care.
Great Care @ Low Cost in SNF-NF Jabbar Fazeli, MD Maine Medical Directors Association Principles Best interest of the patient (SNF) and resident (NF) comes first. Lowest cost to achieve the same care.
How to prescribe The elderly. Andi Shirtcliffe Pharmacist
 How to prescribe The elderly Andi Shirtcliffe Pharmacist Psycho geriatric long stay hospital Rest home Generalist in a specialist setting Workshop outline Step through how I perform a medicine review Cases
How to prescribe The elderly Andi Shirtcliffe Pharmacist Psycho geriatric long stay hospital Rest home Generalist in a specialist setting Workshop outline Step through how I perform a medicine review Cases
Renee Flores, MD Division of Geriatrics & Palliative Medicine Department of Internal Medicine
 Renee Flores, MD Division of Geriatrics & Palliative Medicine Department of Internal Medicine Define AMS and delirium Describe how to recognize and diagnose delirium Identify the predisposing or precipitating
Renee Flores, MD Division of Geriatrics & Palliative Medicine Department of Internal Medicine Define AMS and delirium Describe how to recognize and diagnose delirium Identify the predisposing or precipitating
STOPP START Toolkit Supporting Medication Review in the Older Person
 STOPP START Toolkit Supporting Medication Review in the Older Person STOPP: Screening Tool of Older People s potentially inappropriate Prescriptions START: Screening Tool to Alert doctors to Right (appropriate,
STOPP START Toolkit Supporting Medication Review in the Older Person STOPP: Screening Tool of Older People s potentially inappropriate Prescriptions START: Screening Tool to Alert doctors to Right (appropriate,
Thank You to Our Sponsors: Evaluations & CE Credits. Featured Speakers. Conflict of Interest & Disclosure Statements 10/18/2016
 Thank You to Our Sponsors: University at Albany School of Public Health NYS Department of Health Conflict of Interest & Disclosure Statements The planners and presenters do not have any financial arrangements
Thank You to Our Sponsors: University at Albany School of Public Health NYS Department of Health Conflict of Interest & Disclosure Statements The planners and presenters do not have any financial arrangements
Delirium. Assessment and Management
 Delirium Assessment and Management Goals and Objectives Participants will: 1. be able to recognize and diagnose the syndrome of delirium. 2. understand the causes of delirium. 3. become knowledgeable about
Delirium Assessment and Management Goals and Objectives Participants will: 1. be able to recognize and diagnose the syndrome of delirium. 2. understand the causes of delirium. 3. become knowledgeable about
Medication Use in Older Adults
 Medication Use in Older Adults F. Michael Gloth, III, MD, AGSF, FACP, CMD Clinical Professor Department of Geriatrics, Florida State University College of Medicine Associate Professor of Medicine Division
Medication Use in Older Adults F. Michael Gloth, III, MD, AGSF, FACP, CMD Clinical Professor Department of Geriatrics, Florida State University College of Medicine Associate Professor of Medicine Division
Intelligent Polypharmacy. Professor Colin P Bradley Department of General Practice University College Cork
 Intelligent Polypharmacy Professor Colin P Bradley Department of General Practice University College Cork Polypharmacy No standard definition 2005 review the use of medications that are not clinically
Intelligent Polypharmacy Professor Colin P Bradley Department of General Practice University College Cork Polypharmacy No standard definition 2005 review the use of medications that are not clinically
Anthony J. Caprio, MD, CMD, AGSF 1
 Objectives 1) Discuss the dangers of polypharmacy 2) Review potentially inappropriate medications for older adults Doc, I think I am taking too many medications! 3) Develop strategies for prioritizing
Objectives 1) Discuss the dangers of polypharmacy 2) Review potentially inappropriate medications for older adults Doc, I think I am taking too many medications! 3) Develop strategies for prioritizing
Prescribing Drugs to the Elderly
 Answers to your questions from University of Toronto experts Prescribing Drugs to the Elderly Can drugs do more harm than good? M.A. is a 90-year-old man living at home. He has dementia and due to wandering
Answers to your questions from University of Toronto experts Prescribing Drugs to the Elderly Can drugs do more harm than good? M.A. is a 90-year-old man living at home. He has dementia and due to wandering
Deprescribing with Confidence Dr Sanjay Suman MD FRCP
 Deprescribing with Confidence Dr Sanjay Suman MD FRCP Clinical Director Elderly Care and Stroke Medway NHS Foundation Trust Kent 45% of all medications prescribed for 65 years 1 1. Wynne et al Maturitas
Deprescribing with Confidence Dr Sanjay Suman MD FRCP Clinical Director Elderly Care and Stroke Medway NHS Foundation Trust Kent 45% of all medications prescribed for 65 years 1 1. Wynne et al Maturitas
Condition/Procedure Measure Compliance Criteria Reference Attribution Method
 Premium Specialty: Cardiology Credentialed Specialties include: Cardiac Diagnostic, Cardiology, Cardiovascular Disease, Clinical Cardiac Electrophysiology, and Interventional Cardiology This document is
Premium Specialty: Cardiology Credentialed Specialties include: Cardiac Diagnostic, Cardiology, Cardiovascular Disease, Clinical Cardiac Electrophysiology, and Interventional Cardiology This document is
TOP 5 DRUGS.. TO AVOID IN THE ELDERLY
 TOP 5 DRUGS.. TO AVOID IN THE ELDERLY Debbie Kwan, BScPhm., MSc., FCSHP Canadian Geriatrics Society, April 20, 2013 Disclosure of Potential for Conflict of Interest: Financial Disclosure: None Mar 26,
TOP 5 DRUGS.. TO AVOID IN THE ELDERLY Debbie Kwan, BScPhm., MSc., FCSHP Canadian Geriatrics Society, April 20, 2013 Disclosure of Potential for Conflict of Interest: Financial Disclosure: None Mar 26,
Cover images courtesy of jk1991 at FreeDigitalPhotos.net Infographics courtesy of SIMPATHY consortium
 If using any content from this document, please acknowledge the Scottish Government Polypharmacy Model of Care Group, 2018. When referencing this document, please use the following format: Scottish Government
If using any content from this document, please acknowledge the Scottish Government Polypharmacy Model of Care Group, 2018. When referencing this document, please use the following format: Scottish Government
The Failing Heart in Primary Care
 The Failing Heart in Primary Care Hamid Ikram How fares the Heart Failure Epidemic? 4357 patients, 57% women, mean age 74 years HFSA 2010 Practice Guideline (3.1) Heart Failure Prevention A careful and
The Failing Heart in Primary Care Hamid Ikram How fares the Heart Failure Epidemic? 4357 patients, 57% women, mean age 74 years HFSA 2010 Practice Guideline (3.1) Heart Failure Prevention A careful and
Polypharmacy. A CPPE distance learning programme
 A CPPE distance learning programme DLP 177 January 2016 Contents About CPPE distance learning programmes About this learning programme Glossary of key terms v vii ix Contents Section 1 The problem with
A CPPE distance learning programme DLP 177 January 2016 Contents About CPPE distance learning programmes About this learning programme Glossary of key terms v vii ix Contents Section 1 The problem with
Chronic heart failure: management of chronic heart failure in adults in primary and secondary care (partial update)
") Chronic heart failure: management of chronic heart failure in adults in primary and secondary care (partial update) NICE guideline Apendix C The algorithms Draft for consultation, January 2010 Chronic
Chronic heart failure: management of chronic heart failure in adults in primary and secondary care (partial update) NICE guideline Apendix C The algorithms Draft for consultation, January 2010 Chronic
HA CONVENTION Effectiveness of Pharmacist-led Frail Elderly Medication Service in Acute Geriatric Ward
 Effectiveness of Pharmacist-led Frail Elderly Medication Service in Acute Geriatric Ward HA CONVENTION 2017 Candis Chang Pharmacist Department of Pharmacy Ruttonjee and Tang Shiu Kin Hospitals Background
Effectiveness of Pharmacist-led Frail Elderly Medication Service in Acute Geriatric Ward HA CONVENTION 2017 Candis Chang Pharmacist Department of Pharmacy Ruttonjee and Tang Shiu Kin Hospitals Background
Iatrogenic Delirium. Heather Carey, PharmD, BCPP Clinical Psychiatric Pharmacist University Hospitals Richmond Medical Center
 Iatrogenic Delirium Heather Carey, PharmD, BCPP Clinical Psychiatric Pharmacist University Hospitals Richmond Medical Center Objectives Discuss proposed mechanisms of medication induced delirium Identify
Iatrogenic Delirium Heather Carey, PharmD, BCPP Clinical Psychiatric Pharmacist University Hospitals Richmond Medical Center Objectives Discuss proposed mechanisms of medication induced delirium Identify
De-prescribing in Older Adults. Wael Hamade, MD, FAAFP 04/08/2016
 De-prescribing in Older Adults Wael Hamade, MD, FAAFP 04/08/2016 DISCLOSURES None of the faculty, planners, speakers, providers nor CME committee has any relevant financial relationships with commercial
De-prescribing in Older Adults Wael Hamade, MD, FAAFP 04/08/2016 DISCLOSURES None of the faculty, planners, speakers, providers nor CME committee has any relevant financial relationships with commercial
A Geriatrician s Perspective on Successful Aging. Ariel Green, MD, MPH Assistant Professor of Medicine
 A Geriatrician s Perspective on Successful Aging Ariel Green, MD, MPH Assistant Professor of Medicine 1 Disclosures Johns Hopkins Clinical Research Scholars Program American College of Cardiology Foundation
A Geriatrician s Perspective on Successful Aging Ariel Green, MD, MPH Assistant Professor of Medicine 1 Disclosures Johns Hopkins Clinical Research Scholars Program American College of Cardiology Foundation
Doreen Wan-Chow-Wah, MD, FRCPC Assistant Professor, Division of Geriatric Medicine, Department of Medicine McGill University Health Center Associate
 Doreen Wan-Chow-Wah, MD, FRCPC Assistant Professor, Division of Geriatric Medicine, Department of Medicine McGill University Health Center Associate member, Department of Oncology McGill University Medical
Doreen Wan-Chow-Wah, MD, FRCPC Assistant Professor, Division of Geriatric Medicine, Department of Medicine McGill University Health Center Associate member, Department of Oncology McGill University Medical
Canadian Guideline for Opioids for Chronic Non-Cancer Pain. Speaker Disclosure. Objectives. Canadian Guideline for Opioids for Chronic Non-Cancer Pain
 Canadian Guideline for Opioids for Chronic Non-Cancer Pain John Fraser Community Hospital Program New Glasgow November 1, 2017 This speaker has been asked to disclose to the audience any involvement with
Canadian Guideline for Opioids for Chronic Non-Cancer Pain John Fraser Community Hospital Program New Glasgow November 1, 2017 This speaker has been asked to disclose to the audience any involvement with
Optimising prescribing in primary care in the face of multimorbidity and polypharmacy
 University of Dundee School of Medicine Optimising prescribing in primary care in the face of multimorbidity and polypharmacy Bruce Guthrie Professor of Primary Care Medicine, University of Dundee NICE
University of Dundee School of Medicine Optimising prescribing in primary care in the face of multimorbidity and polypharmacy Bruce Guthrie Professor of Primary Care Medicine, University of Dundee NICE
Taking the harm out of Polypharmacy Step by step. Karen Reid and Claire Stein Lead Integrated Care Pharmacist NHS Lothian
 Taking the harm out of Polypharmacy Step by step Karen Reid and Claire Stein Lead Integrated Care Pharmacist NHS Lothian Presentation: Polypharmacy Overview of the 2015 guidelines The Seven Steps Application
Taking the harm out of Polypharmacy Step by step Karen Reid and Claire Stein Lead Integrated Care Pharmacist NHS Lothian Presentation: Polypharmacy Overview of the 2015 guidelines The Seven Steps Application
Safe Prescribing in Dementia
 Safe Prescribing in Dementia Dr Daniel Harwood Consultant Psychiatrist and Clinical Director, London Strategic Clinical Network Gurdeep Kaur Major Rapid Access Team Senior Pharmacist, Camden CNWL NHS Trust
Safe Prescribing in Dementia Dr Daniel Harwood Consultant Psychiatrist and Clinical Director, London Strategic Clinical Network Gurdeep Kaur Major Rapid Access Team Senior Pharmacist, Camden CNWL NHS Trust
Antipsychotic Medications
 TRAIL: Team Review of EVIDENCE REVIEW & RECOMMENDATIONS FOR LTC Behavioural and psychological symptoms of dementia (BPSD) refer to the non-cognitive symptoms of disturbed perception, thought content, mood
TRAIL: Team Review of EVIDENCE REVIEW & RECOMMENDATIONS FOR LTC Behavioural and psychological symptoms of dementia (BPSD) refer to the non-cognitive symptoms of disturbed perception, thought content, mood
4/27/2015. Cardiac Events #1 cause of postoperative complications/ mortality- CHF, complete heart block, MI,
 Not intended for medical clearance Identify, document, and evaluate health conditions Medication Management Stratify Risks Optimize conditions within context of surgical illness Recommend measures that
Not intended for medical clearance Identify, document, and evaluate health conditions Medication Management Stratify Risks Optimize conditions within context of surgical illness Recommend measures that
Appropriate prescribing and deprescribing for older people getting it right. Alan Davis Northland District Health Board
 Appropriate prescribing and deprescribing for older people getting it right Alan Davis Northland District Health Board Unused returns Potentially inappropriate medication use in the elderly 15% of older
Appropriate prescribing and deprescribing for older people getting it right Alan Davis Northland District Health Board Unused returns Potentially inappropriate medication use in the elderly 15% of older
Polypharmacy: What the Nurse Practitioner Should Know Audrey M. Stevenson PhD, MPH, MSN, FNP-BC Las Vegas 2017
 Polypharmacy: What the Nurse Practitioner Should Know Audrey M. Stevenson PhD, MPH, MSN, FNP-BC Las Vegas 2017 Disclosure I have no current affiliation or financial arrangement with any grantor or commercial
Polypharmacy: What the Nurse Practitioner Should Know Audrey M. Stevenson PhD, MPH, MSN, FNP-BC Las Vegas 2017 Disclosure I have no current affiliation or financial arrangement with any grantor or commercial
Prescribing in the Elderly. Dr Alison Macrae and Dr Debbie Vest GPST2 Drs in Psychiatry
 Prescribing in the Elderly Dr Alison Macrae and Dr Debbie Vest GPST2 Drs in Psychiatry 24 th September 2014 Objectives Understand the significance of polypharmacy in the elderly Become familiar with the
Prescribing in the Elderly Dr Alison Macrae and Dr Debbie Vest GPST2 Drs in Psychiatry 24 th September 2014 Objectives Understand the significance of polypharmacy in the elderly Become familiar with the
Polypharmacy in the Elderly
 Polypharmacy in the Elderly Or How Scotland invented the Modern World Sir William Ferguson Anderson 1914-2001 Became the first Professor of Geriatrics in the world when he was appointed to the David Cargill
Polypharmacy in the Elderly Or How Scotland invented the Modern World Sir William Ferguson Anderson 1914-2001 Became the first Professor of Geriatrics in the world when he was appointed to the David Cargill
Polypharmacy: What the Nurse Practitioner Should Know Audrey M. Stevenson PhD, MPH, MSN, FNP-BC Nashville, TN 2017
 What is Polypharmacy Polypharmacy: What the Nurse Practitioner Should Know Audrey M. Stevenson PhD, MPH, MSN, FNP-BC Nashville, TN 2017 The use of multiple medications simultaneously Rx OTC Herbal Disclosure
What is Polypharmacy Polypharmacy: What the Nurse Practitioner Should Know Audrey M. Stevenson PhD, MPH, MSN, FNP-BC Nashville, TN 2017 The use of multiple medications simultaneously Rx OTC Herbal Disclosure
ROAD TO UNDERSTANDING POLYPHARMACY. Lt Col PHIL L. SAMPLES BS Phr, Pharm. D., BCNSP
 ROAD TO UNDERSTANDING POLYPHARMACY Lt Col PHIL L. SAMPLES BS Phr, Pharm. D., BCNSP Definition occurs when: 1. a medical regimen includes at least one unnecessary medication 2. Medications have not been
ROAD TO UNDERSTANDING POLYPHARMACY Lt Col PHIL L. SAMPLES BS Phr, Pharm. D., BCNSP Definition occurs when: 1. a medical regimen includes at least one unnecessary medication 2. Medications have not been
POLICY DOCUMENT. Pharmacy MMG/MPG. Approved By and Date Medicines Management roup March March 2016
 POLICY DOCUMENT Document Title High dose and combination antipsychotic guidance Reference Number n/a Policy Type Prescribing and Treatment Guideline Electronic File/Location Clinical Resources/Pharmacy/Prescribing
POLICY DOCUMENT Document Title High dose and combination antipsychotic guidance Reference Number n/a Policy Type Prescribing and Treatment Guideline Electronic File/Location Clinical Resources/Pharmacy/Prescribing
Demystifying the Complex Patient
 Demystifying the Complex Patient Jay Reaume, BSc, BScPhm, RPh, CDE Suzanne Singh, BScPhm, ACPR, PharmD, RPh May 30, 2015 Disclosures Jay Reaume No conflicts of interest to disclose Suzanne Singh No conflicts
Demystifying the Complex Patient Jay Reaume, BSc, BScPhm, RPh, CDE Suzanne Singh, BScPhm, ACPR, PharmD, RPh May 30, 2015 Disclosures Jay Reaume No conflicts of interest to disclose Suzanne Singh No conflicts
POLYPHARMACY. A practical approach to deprescribing in care homes. Care Home Pharmacy Team. Herts Valleys Clinical Commissioning Group
 POLYPHARMACY A practical approach to deprescribing in care homes. Care Home Pharmacy Team Herts Valleys Clinical Commissioning Group Neeta Gulhane Specialist Pharmaceutical Advisor Care Homes The Care
POLYPHARMACY A practical approach to deprescribing in care homes. Care Home Pharmacy Team Herts Valleys Clinical Commissioning Group Neeta Gulhane Specialist Pharmaceutical Advisor Care Homes The Care
Pitfalls in Pharmacotherapy of Geriatrics
 Pitfalls in Pharmacotherapy of Geriatrics DR Ali M. Alyami (M Pharm., PhD) Case Study An 85 year old female with a history of atrial fibrillation, stroke, dementia, and hypertension, who is receiving chronic
Pitfalls in Pharmacotherapy of Geriatrics DR Ali M. Alyami (M Pharm., PhD) Case Study An 85 year old female with a history of atrial fibrillation, stroke, dementia, and hypertension, who is receiving chronic
Fall Prevention and hip protectors
 Presenter Disclosure Information Edgar Pierluissi Division of Geriatrics Edgar Pierluissi, MD Medical Director, Acute Care for Elders Unit, San Francisco General Hospital and Trauma Center Fall Prevention
Presenter Disclosure Information Edgar Pierluissi Division of Geriatrics Edgar Pierluissi, MD Medical Director, Acute Care for Elders Unit, San Francisco General Hospital and Trauma Center Fall Prevention
Update in Geriatrics: Choosing Wisely Primum Non Nocere
 Joseph G. Ouslander, M.D. Professor of Clinical Biomedical Science Senior Associate Dean for Geriatric Programs Chair, Department of Integrated Medical Science Charles E. Schmidt College of Medicine Professor
Joseph G. Ouslander, M.D. Professor of Clinical Biomedical Science Senior Associate Dean for Geriatric Programs Chair, Department of Integrated Medical Science Charles E. Schmidt College of Medicine Professor
Reviewing Medicines in at risk patients care homes
 Reviewing Medicines in at risk patients care homes Clinical Medication Reviews by Pharmacists in Collaboration with GP Surgeries across Brighton and Hove CCG Liz Butterfield FRPharmS 19th April 2016 NICE:
Reviewing Medicines in at risk patients care homes Clinical Medication Reviews by Pharmacists in Collaboration with GP Surgeries across Brighton and Hove CCG Liz Butterfield FRPharmS 19th April 2016 NICE:
NURSING HOME MEDICINE UPDATE
 NURSING HOME MEDICINE UPDATE - 2018 Bryan Primary Care Conference, Spring 2018 DISCLOSURES No financial disclosures I will mention non-fda approved use of medications OBJECTIVES 1. Review the new CMS rules
NURSING HOME MEDICINE UPDATE - 2018 Bryan Primary Care Conference, Spring 2018 DISCLOSURES No financial disclosures I will mention non-fda approved use of medications OBJECTIVES 1. Review the new CMS rules
DRUG THERAPY CHOICES FOR THE DEMENTED PATIENT Past, Present and Future
 DRUG THERAPY CHOICES FOR THE DEMENTED PATIENT Past, Present and Future Daniel S. Sitar Professor Emeritus University of Manitoba Email: Daniel.Sitar@umanitoba.ca March 6, 2018 INTRODUCTION EPIDEMIOLOGY
DRUG THERAPY CHOICES FOR THE DEMENTED PATIENT Past, Present and Future Daniel S. Sitar Professor Emeritus University of Manitoba Email: Daniel.Sitar@umanitoba.ca March 6, 2018 INTRODUCTION EPIDEMIOLOGY
2016 Update in Geriatrics Elizabeth Eckstrom, MD, MPH Oregon Health & Science University Oregon Geriatrics Society October 7, 2016
 2016 Update in Geriatrics Elizabeth Eckstrom, MD, MPH Oregon Health & Science University Oregon Geriatrics Society October 7, 2016 I have no conflicts of interest Photos thanks to Google images This year
2016 Update in Geriatrics Elizabeth Eckstrom, MD, MPH Oregon Health & Science University Oregon Geriatrics Society October 7, 2016 I have no conflicts of interest Photos thanks to Google images This year
Interprofessional Outpatient Clinic Polypharmacy Management. Objectives
 Interprofessional Outpatient Clinic Polypharmacy Management Brett Hoffecker, MD University of Kansas School of Medicine Wichita Family Medicine Residency Program at Via Christi April 10th, 2015 Objectives
Interprofessional Outpatient Clinic Polypharmacy Management Brett Hoffecker, MD University of Kansas School of Medicine Wichita Family Medicine Residency Program at Via Christi April 10th, 2015 Objectives
Western University of Health Sciences, College of Pharmacy is accredited by the Accreditation Council for Pharmacy Education as a provider of
 Western University of Health Sciences, College of Pharmacy is accredited by the Accreditation Council for Pharmacy Education as a provider of continuing pharmacy education. Topic UAN# Target Audience A
Western University of Health Sciences, College of Pharmacy is accredited by the Accreditation Council for Pharmacy Education as a provider of continuing pharmacy education. Topic UAN# Target Audience A
Bulletin Independent prescribing information for NHS Wales
 Bulletin Independent prescribing information for NHS Wales July 2016 Optimising medicines use in care homes There are currently over 22 000 resident places in older adult care homes in Wales. 1 An ageing
Bulletin Independent prescribing information for NHS Wales July 2016 Optimising medicines use in care homes There are currently over 22 000 resident places in older adult care homes in Wales. 1 An ageing
Can PK and Modelling Help?
 Safeguarding public health Can PK and Modelling Help? Terry Shepard Pharmacokinetics Assessor, Statistics Unit MHRA, London EMA Workshop: Ensuring safe and effective medicines for an ageing population
Safeguarding public health Can PK and Modelling Help? Terry Shepard Pharmacokinetics Assessor, Statistics Unit MHRA, London EMA Workshop: Ensuring safe and effective medicines for an ageing population
Using the ASCP-NCOA Falls Risk Reduction Toolkit Part 1: A Companion to CDC's STEADI Toolkit
 Using the ASCP-NCOA Falls Risk Reduction Toolkit Part 1: A Companion to CDC's STEADI Toolkit Target Audience: Pharmacists ACPE#: 0202-9999-18-056-L01-P Activity Type: Application-based Disclosures Kathleen
Using the ASCP-NCOA Falls Risk Reduction Toolkit Part 1: A Companion to CDC's STEADI Toolkit Target Audience: Pharmacists ACPE#: 0202-9999-18-056-L01-P Activity Type: Application-based Disclosures Kathleen
About ISMP Canada. Analysis Outputs: Safety Bulletins. Less is More: An Introduction to Deprescribing. canada.org
 Less is More: An Introduction to Deprescribing Lindsay Yoo, BSc, BScPhm, RPh, CDE, CGP, PharmD Medication Safety Analyst, ISMP Canada About ISMP Canada The Institute for Safe Medication Practices Canada
Less is More: An Introduction to Deprescribing Lindsay Yoo, BSc, BScPhm, RPh, CDE, CGP, PharmD Medication Safety Analyst, ISMP Canada About ISMP Canada The Institute for Safe Medication Practices Canada
Disclosures. Learning Objectives. Hypertension: a sprint to the finish Ontario Pharmacists Association 1
 Disclosures I have no current or past relationships with commercial entities I have received a speaker s fee from the Ontario Pharmacists Association for this learning activity Laura Tsang PharmD Sunnybrook
Disclosures I have no current or past relationships with commercial entities I have received a speaker s fee from the Ontario Pharmacists Association for this learning activity Laura Tsang PharmD Sunnybrook
 20.9 15.4 3.1 0.1 0.2 0.2 0.3 0.4 0.6 0.9 1.5 2.2 9.6 6.1 7.3 4.2 1900 1910 1920 1930 1940 1950 1960 1970 1980 1990 2000 2010 2020 2030 2040 2050 All Ages Age 65+ Age 85+ Female 50.9% Male 49.1% Female
20.9 15.4 3.1 0.1 0.2 0.2 0.3 0.4 0.6 0.9 1.5 2.2 9.6 6.1 7.3 4.2 1900 1910 1920 1930 1940 1950 1960 1970 1980 1990 2000 2010 2020 2030 2040 2050 All Ages Age 65+ Age 85+ Female 50.9% Male 49.1% Female
Rational prescribing in the older adult. Assoc Prof Craig Whitehead
 Rational prescribing in the older adult Assoc Prof Craig Whitehead Introduction Physioloical ageing and frailty Medication risks in older adults Drug Burden Anticholinergic and sedative drug burden Cascade
Rational prescribing in the older adult Assoc Prof Craig Whitehead Introduction Physioloical ageing and frailty Medication risks in older adults Drug Burden Anticholinergic and sedative drug burden Cascade
Adjusting and Withdrawing Medications in the Elderly
 Adjusting and Withdrawing Medications in the Elderly Louise Mallet, B.Sc.Pharm., Pharm.D., CGP Professor in Clinical Pharmacy, Faculty of Pharmacy, University of Montreal Clinical Pharmacist in Geriatrics,
Adjusting and Withdrawing Medications in the Elderly Louise Mallet, B.Sc.Pharm., Pharm.D., CGP Professor in Clinical Pharmacy, Faculty of Pharmacy, University of Montreal Clinical Pharmacist in Geriatrics,
Chapter 01 Introduction
 Chapter 01 Introduction Defining the Elderly There is no universally accepted age cut-off defining elderly. This reflects the fact that chronological age itself is less important than biological events
Chapter 01 Introduction Defining the Elderly There is no universally accepted age cut-off defining elderly. This reflects the fact that chronological age itself is less important than biological events