Compliant EM Coding and Documentation Outpatient Coding
|
|
|
- Martin Willis
- 6 years ago
- Views:
Transcription



1 Compliant EM Coding and Documentation Outpatient Coding Steve Adams, MCS, COC, CPC, CPMA, CPC-I, PCS, FCS, COA

2
3 Incident To & Shared Visits E and M Coding for: - New Office Visits - Established Office Visits - Consultation Visits Preventive Services - Tobacco - Home Health - AWV Discussion Points
4 Incident To & Shared Visit
5 Incident To Billing (office) Four standard criteria: 1.Physician must be in office 2.Must be an established patient 3.Must not change anything from previous plan of care 4.Doctor should see patient every 3 rd or 4 th visit (shows active participation)
6 Shared Visits (hospital) Two standard criteria: 1.NPP sees patient and documents note 2.MD sees patient and documents mini hx, exam and MDM on same date
7 E&M Coding
8 Code Selection Medical necessity of a service is the overarching criterion for payment in addition to the individual requirements of a CPT code. It would not be medically necessary or appropriate to bill a higher level of evaluation and management service when a lower level of service is warranted. The volume of documentation should not be the primary influence upon which a specific level of service is billed. Documentation should support the level of service reported. The service should be documented during, or as soon as practicable after it is provided in order to maintain an accurate medical record.
9 Office Outpatient Services
10 Outpatient Visit New Requires All Three Key Elements

11 Q1. Which of the following statements is most compliant with CMS documentation? point system review normal 2. See HPI for ROS 3. ROS positive for SOB, all other systems reviewed were negative 4. All of the above 0% 0% 0% 0%
12 New Patients Think: No treatment Short term meds, OTC, minor surgery Long term meds, major surgery Sick enough to admit / major surgery with risks / extensive data Also check grid to make sure you document correct history and examination!!


13 Initial Visits New Outpatient Peer Data Dr. Gotcha 45% 54% 27% 31% 22% 1% 4% 5% 6% 6%
14 New/Consultation Patient Visits (3 out of 3) Code Minutes History Examination Decision-Making CC 1HPI Problem Focused Problem Focused 1995 (1) 1997 (1 check) Straightforward Diagnosis Minimal Data Minimal or None Risk Minimal CC 1 HPI 1 ROS Exp. Problem Focused Exp. Problem Focused 1995 (2 7) 1997 (6 checks) Straightforward Diagnosis Minimal Data Minimal or None Risk Minimal Detailed CC 4 HPI or status of 3 chronic conditions 2 ROS Medical or Family or Social History Detailed 1995 (4-7 need 4x4) 1997 (12 checks) Low Diagnosis Limited Data Limited Risk Low OTC, Short-term Meds, Minor Surgery Comprehensive CC 4 HPI or status of 3 chronic conditions 10 ROS Medical, Family, Social History Comprehensive 1995 (8) 1997 (2 checks from 9 areas); or 1997(all checks in border & 1 check in others) Moderate Diagnosis Multiple Data Moderate Risk Moderate Long term Rx or Major Surgery Comprehensive CC 4 HPI or status of 3 chronic conditions 10 ROS Medical, Family, Social History Comprehensive 1995 (8) 1997 (2 checks from 9 areas); or 1997(all checks in border & 1 check in others) High Diagnosis Extensive Data Extensive Risk High
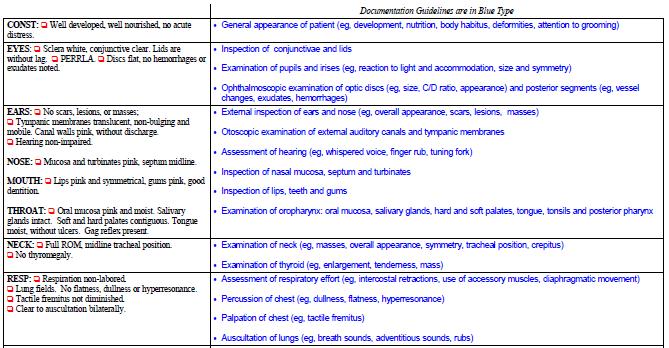
15 1995 Comprehensive (8) 1. Const: Vital signs listed above. Well developed, well nourished and in no acute distress. Alert and oriented X s 3. No mood disorders noted, calm affect. 2. Eyes: Sclera white, conjunctiva clear, lids are without lag. PERRLA. Pupils and irises are equal and round without defect. 3. ENT: TMs intact and clear, normal canals, grossly normal hearing. Oropharanx clear and moist without erythema. Gums pink, good dentition. 4. Lymph/Neck: No masses, thyromegaly, or abnormal cervical notes. No bruit. Tracheal midline. 5. Cardio: RRR, Normal S1, S2 w/o murmurs, rubs or gallops. Skin warm and dry. No peripheral edema. 6. Respiratory: Chest symmetrical, respirations non-labored. No dullness or flatness. Clear bilaterally to auscultation, non-tender to palpitation. 7. Musculo: No deformity or scoliosis noted. No frank gait disturbance noted. No cyanosis or edema. Pulses normal in all 4 extremities. No atrophy or abnormal movements. Appropriate muscle strength bilaterally. 8. Neurologic: No focal deficits, cranial nerves II-XII grossly intact with normal sensation, reflexes, coordination, muscle strength and tone. 9. GI/Abdomen: Soft, non tender, non distended, no hepatosplemomegaly, normal bowel sounds, no masses noted.
16 What Doesn t Count (8) Head Neck Thyroid Abdomen Extremities Back Under the 1995 Guidelines CMS and the AMA want you to examine ORGAN SYSTEMS and not body areas with regard to any code with the number (8) in the exam criteria
17 Expanded vs. Extended The difference is not the number of systems examined. Two to seven systems are required for both examinations. The difference is the detail in which the examined systems are described.
18 1995 Detailed 4-7 (4x4) 1. Const: Vital signs listed above. Well developed, well nourished and in no acute distress. Alert and oriented X s 3. No mood disorders noted, calm affect. 2. Eyes: Sclera white, conjunctiva clear, lids are without lag. PERRLA. Pupils and irises are equal and round without defect. 3. ENT: TMs intact and clear, normal canals, grossly normal hearing. Oropharanx clear and moist without erythema. Gums pink, good dentition. 4. Lymph/Neck: No masses, thyromegaly, or abnormal cervical notes. No bruit. Tracheal midline. 5. Cardio: RRR, Normal S1, S2 w/o murmurs, rubs or gallops. Skin warm and dry. No peripheral edema. 6. Respiratory: Chest symmetrical, respirations non-labored. No dullness or flatness. Clear bilaterally to auscultation, non-tender to palpitation. 7. Musculo: No deformity or scoliosis noted. No frank gait disturbance noted. No cyanosis or edema. Pulses normal in all 4 extremities. No atrophy or abnormal movements. Appropriate muscle strength bilaterally. 8. Neurologic: No focal deficits, cranial nerves II-XII grossly intact with normal sensation, reflexes, coordination, muscle strength and tone. 9. GI/Abdomen: Soft, non tender, non distended, no hepatosplemomegaly, normal bowel sounds, no masses noted.
19 1997 Bullet Guidelines Allow you to document systems and areas, however you have to be very specific about what you document about those systems and areas. Most EMRs are based on the 1997 guidelines but are not compliant
20 Multi-System


21 Single System
22 What To Do I ll have a copy of those guidelines posted on my web site and I ll give you a link on medicalofficeblog.com Make sure that you are only getting credit for what the government says you get credit for documenting. THIS IS A CRITICAL COMPONENT OF YOUR EMR COMPLIANCE
23 New Patients Think: No treatment Short term meds, OTC, minor surgery Long term meds, major surgery Sick enough to admit / major surgery with risks / extensive data Also check grid to make sure you document correct history and examination!!

24 Q2. A new patient is someone not seen by you or a member of the same group, same specialty, within the last? 0% A. New problem new patient 0% 0% 0% B. Two years C. New practice new patient D. Three years 10
25 Outpatient Visit Established Patient Requires Two of Three Key Elements

26 Q3. When billing for a based on a counseling driven encounter, what is the minimum amount of time you are required to spend face-to-face with the patient? A. 17 minutes B. 25 minutes C. 45 minutes D. 40 minutes 0% 0% 0% 0% A. B. C. D. 10
27 Established Patients Think: One stable condition Two stable or one unstable problem 99214: - 3 chronic stable on meds - 2 unstable on meds - 1 stable and one unstable on meds Sick enough to admit/extensive dx with risk or data Also check grid to make sure you document correct history and examination or counseling time!!
28 Established Visits Established Outpatient Peer Data Dr. Gotcha 45% 43% 41% 36% 18% 5% 1% 4% 5% 1%
29 Established Patient Visits (2 out of 3) N/A N/A N/A N/A CC 1HPI Problem Focused Problem Focused 1995 (1) 1997 (1 check) Straightforward Diagnosis Minimal 1 Data Minimal or None 1 Risk Minimal 1 1 stable problem CC 1 HPI 1 ROS Exp. Problem Focused Exp. Problem Focused 1995 (2 7) 1997 (6 checks) Low Diagnosis Limited 2 Data Limited 2 Risk Low 2 2 stable problems 1 unstable problem Detailed CC 4 HPI or status of 3 chronic conditions 2 ROS Medical or Family or Social History Detailed 1995 (4-7 need 4x4) 1997 (12 checks) Moderate Diagnosis Multiple 3 Data Moderate 3 Risk Moderate 3 3 stable problems on meds 1 stable and 1 unstable on meds 2 unstable problems on meds New problem requiring major surg Comprehensive CC 4 HPI or status of 3 chronic conditions 10 ROS Medical, Family, Social History Comprehensive 1995 (8) 1997 (2 checks from 9 areas); or 1997(all checks in border & 1 check in others) High Diagnosis Extensive 4 Data Extensive 4 Risk High 4 Very sick patient with extensive data review and high risk
30 Counseling Dominated 3 standard criteria for time: 1. Total Face-to-Face time of provider 2. That more than 50% was counseling 3. Topics you discussed If the level of care is being based on time spent with the patient for counseling/coordination of care documentation should support the time for the visit and the documentation must support in sufficient detail the nature of the counseling
31 Signature Requirements Make sure you properly SIGN all your notes, orders, test results; all documentation that supports a claim in the patient chart should have the provider s signature. If the provider is initialing this documentation he/she must also print their name by the initials or circle the typed name on an office form. This lets the reviewer clearly see that who documented the medical record.
32 Established Patients Think: One stable condition Two stable or one unstable problem 99214: - 3 chronic stable on meds - 2 unstable on meds - 1 stable and one unstable on meds Sick enough to admit/extensive dx with risk or data Also check grid to make sure you document correct history and examination or counseling time!!
33 Consultation Visits
34 Q4. Which of the following codes should be used when seeing a new Medicare patient in your office for the first time moderate complexity consultation? 0% A % 0% 0% B C D
35 Outpatient Visit Consults Requires All Three Key Elements
36 New/Consultation Patient Visits (3 out of 3) Code Minutes History Examination Decision-Making CC 1HPI Problem Focused Problem Focused 1995 (1) 1997 (1 check) Straightforward Diagnosis Minimal Data Minimal or None Risk Minimal CC 1 HPI 1 ROS Exp. Problem Focused Exp. Problem Focused 1995 (2 7) 1997 (6 checks) Straightforward Diagnosis Minimal Data Minimal or None Risk Minimal Detailed CC 4 HPI or status of 3 chronic conditions 2 ROS Medical or Family or Social History Detailed 1995 (4-7 need 4x4) 1997 (12 checks) Low Diagnosis Limited Data Limited Risk Low OTC, Short-term Meds, Minor Surgery Comprehensive CC 4 HPI or status of 3 chronic conditions 10 ROS Medical, Family, Social History Comprehensive 1995 (8) 1997 (2 checks from 9 areas); or 1997(all checks in border & 1 check in others) Moderate Diagnosis Multiple Data Moderate Risk Moderate Long term Rx or Major Surgery Comprehensive CC 4 HPI or status of 3 chronic conditions 10 ROS Medical, Family, Social History Comprehensive 1995 (8) 1997 (2 checks from 9 areas); or 1997(all checks in border & 1 check in others) High Diagnosis Extensive Data Extensive Risk High
37 Preventive Medicine Services
38 Q5. G0436 (Tobacco cessation counseling) is billable in what place of service (8 times per year, per patient)? A. Office B. Hospital C. Nursing Home D. All above 0% 0% 0% 0% A. B. C. D. 10
39 Tobacco Cessation Codes The CPT Codes: 99406: Smoking and tobacco cessation counseling; intermediate, greater than 3 minutes, up to 10 minutes, 99407: Smoking and tobacco cessation counseling; intensive, greater than 10 minutes, The Diagnosis Codes Medical dx of the patient at the time of the visit the tobacco is affecting If used with E/M, don t forget modifier 25
40 New Tobacco Cessation Codes The HCPCS Codes: G0436: Smoking and tobacco cessation counseling visit for the asymptomatic patient; intermediate, greater than 3 minutes, up to 10 minutes, G0437: Smoking and tobacco cessation counseling visit for the asymptomatic patient; intensive, greater than 10 minutes, The Diagnosis Codes ICD-9 code (non-dependent tobacco use disorder), or ICD-9 code V15.82 (history of tobacco use).
41 Home Health Certification The HCPCs Codes: G0179 Re-certification for Medicare-covered home health under a plan of care, including contacts with home health agency and review of reports of patient status required by physician to affirm plan of care G Certification for Medicare-covered home health under a plan of care, including contacts with home health agency and review of reports of patient status required by physician to affirm plan of care
42 New AWV Codes G0438 (Annual wellness visit; includes a personalized prevention plan of service (PPPS), first visit); and G0439 (Annual wellness visit; includes a personalized prevention plan of service (PPPS),subsequent visit). We note that practitioners furnishing a preventive medicine E/M service that does not meet the requirements for the IPPE or the AWV would continue to report one of the preventive medicine E/M services CPT codes in the range of through as appropriate to the patient's circumstances, and these codes continue to be noncovered by Medicare."
43 1. Health Risk Assessment AWV - Initial 2. Establishment of an individual's medical and family history. 3. Establishment of a list of current providers and suppliers that are regularly involved in providing medical care to the individual. 4. Measurement of an individual's height, weight, body mass index (or waist circumference, if appropriate), blood pressure, and other routine measurements as deemed appropriate, based on the individual's medical and family history. 5. Detection of any cognitive impairment that the individual may have. 6. Review of the individual's potential (risk factors) for depression, Review of the individual's functional ability and level of safety, based on direct observation. 7. Review of the individual's functional ability and level of safety, based on direct observation 8. Establishment of the following: ++ A written screening schedule, such as a checklist, for the next 5 to 10 years ++ A list of risk factors and conditions for which primary, secondary or tertiary interventions are recommended. 9. Furnishing of personalized health advice to the individual and a referral, as appropriate Any other element determined appropriate through the National Coverage Determination process.
44 1. Health Risk Assessment AWV - Subsequent 2. An update of the individual's medical and family history. 3. An update of the list of current providers and suppliers that are regularly involved in providing medical care to the individual, as that list was developed for the first AWV providing personalized prevention plan services. 4. Measurement of an individual's weight (or waist circumference), blood pressure, and other routine measurements as deemed appropriate, based on the individual's medical and family history. 5. Detection of any cognitive impairment, as that term is defined in this section, that the individual may have. 6. An update to both of the following: ++ The written screening schedule for the individual as that schedule was developed at the first AWV providing personalized prevention plan services. CMS-1503-FC The list of risk factors and conditions for which primary, secondary or tertiary interventions are recommended or are underway for the individual as that list was developed at the first AWV providing personalized prevention plan services. 7. Furnishing of personalized health advice to the individual and a referral, as appropriate, to health education or preventive counseling services or programs as that advice and related services are defined in paragraph (a) of this section. 8. Any other element determined through the NCD process.
45 Breast / Pelvic Exam The HCPCS Code: G0101 Pelvic and Breast Exam The Diagnosis Codes V72.31 Routine gynecological exam V76.47 Screening for neoplasm of the vagina V76.49 Screening of woman without a cervix V76.2 Screening for neoplasm of cervix V15.89* - Every Year Presenting health hazards
46 Obtain Pap Smear The HCPCS Code: Q Obtaining screen pap smear The Diagnosis Codes V72.31 Routine gynecological exam V76.47 Screening for neoplasm of the vagina V76.49 Screening of woman without a cervix V76.2 Screening for neoplasm of cervix V15.89* - Every Year Presenting health hazards
47 Incident To & Shared Visits E and M Coding for: - New Office Visits - Established Office Visits - Consultation Visits Preventive Services - Tobacco - Home Health - AWV Discussion Points

48 Evaluation Please take < 90 seconds to evaluate this session. Time permitting, speaker will take questions following evaluation. Responses are not displayed and are important in maintaining high quality education.
49 The overall performance of the speaker: 1. Poor 2. Fair 3. Average 4. Good 5. Excellent 0% 0% 0% 0% 0%
50 How well were the learning objectives met? 1. Poor 2. Fair 3. Average 4. Good 5. Excellent 0% 0% 0% 0% 0% Poor Fair Average Good Excellent 10
51 Did speaker present a balanced view of therapeutic options? 1. Yes 2. No 3. N/A 0% 0% 0% Yes No N/A 10
52 How useful will this session be in your practice? 1. Poor 2. Fair 3. Average 4. Good 5. Excellent 0% 0% 0% 0% 0% Poor Fair Average Good Excellent 10


53 As a result of this program, do you intend to change your patient care? 1. Yes 2. No 0% 0% Yes No 10
54 Thank you!
55 Questions?
56 Any Questions Direct: E-Fax: Web: Facebook: facebook.com/kingofcoders
Agenda. Medicare G codes Initial Preventive Physical Examination (IPPE) Annual Wellness Visit (AWV) Preventive Services
 Annual Wellness Visit (AWV) Preventive Services") Medicare G Codes Agenda Medicare G codes Initial Preventive Physical Examination (IPPE) Annual Wellness Visit (AWV) Preventive Services Initial Preventative Physical Examination (IPPE) Components of the
Medicare G Codes Agenda Medicare G codes Initial Preventive Physical Examination (IPPE) Annual Wellness Visit (AWV) Preventive Services Initial Preventative Physical Examination (IPPE) Components of the
How to Code Correctly for E/M Services (1997 Guidelines)
") How to Code Correctly for E/M Services (1997 Guidelines) Phillip Ward, DPM CPT Editorial Board Advisor for Foot and Ankle Former CPT Assistant Editorial Board Member Past President, APMA General Principles
How to Code Correctly for E/M Services (1997 Guidelines) Phillip Ward, DPM CPT Editorial Board Advisor for Foot and Ankle Former CPT Assistant Editorial Board Member Past President, APMA General Principles
2/21/
 Medical Billing Made Easy Presents Optimizing Office Visits for Preventive Services Beginning now www.kareo.com Today s Program Introduction Presentation: Betsy Nicoletti, M.S., CPC Kareo Special Offer:
Medical Billing Made Easy Presents Optimizing Office Visits for Preventive Services Beginning now www.kareo.com Today s Program Introduction Presentation: Betsy Nicoletti, M.S., CPC Kareo Special Offer:
8/3/2011. Presented by: Brenda Edwards, CPC, CPMA, CPC I, CEMC AAPCCA Board of Directors. Documentation. Results ? 2
 Presented by: Brenda Edwards, CPC, CPMA, CPC I, CEMC AAPCCA Board of Directors 1 Documentation Auditing Results? 2 1 HANDWRITTEN Legibility Personalized DICTATED Concise Personalized Timely? EMR Lengthy,
Presented by: Brenda Edwards, CPC, CPMA, CPC I, CEMC AAPCCA Board of Directors 1 Documentation Auditing Results? 2 1 HANDWRITTEN Legibility Personalized DICTATED Concise Personalized Timely? EMR Lengthy,
Practical Approaches to Medical Necessity
 Practical Approaches to Medical Necessity CAROLYN AVERY, CPC, CEMC CAROLYN AVERY & ASSOCIATES, PC ROBERT OSSOFF DMD, MD, CHC ASSISTANT VICE CHANCELLOR FOR COMPLIANCE &CORPORATE INTEGRITY VANDERBILT MEDICAL
Practical Approaches to Medical Necessity CAROLYN AVERY, CPC, CEMC CAROLYN AVERY & ASSOCIATES, PC ROBERT OSSOFF DMD, MD, CHC ASSISTANT VICE CHANCELLOR FOR COMPLIANCE &CORPORATE INTEGRITY VANDERBILT MEDICAL
Slide 1. Slide 2 The Scream by Edvard Munch, Slide 3
 1 Jan DiSantostefano, MS, NP SAS Institute, Inc. Cary, NC Jdisantostefano@nc.rr.com November, 2011 2 The Scream by Edvard Munch, 1893 2 3 1893 - in France by a physician, Jacques Bertillion. Bertillon
1 Jan DiSantostefano, MS, NP SAS Institute, Inc. Cary, NC Jdisantostefano@nc.rr.com November, 2011 2 The Scream by Edvard Munch, 1893 2 3 1893 - in France by a physician, Jacques Bertillion. Bertillon
Practical E/M Audit Form: Initial Outpatient Visit (p.1)
") Patient: Name: Chart #: Date of visit: / / Reviewed by: Date of review: / / Practical E/M Audit Form: Initial Outpatient Visit (p.1) Medical History Review Select the level corresponding to lowest of the
Patient: Name: Chart #: Date of visit: / / Reviewed by: Date of review: / / Practical E/M Audit Form: Initial Outpatient Visit (p.1) Medical History Review Select the level corresponding to lowest of the
Welcome to Medicare: Exam Overview
 Welcome to Medicare: Exam Overview June 8, 2016 Agenda Opening Remarks Housekeeping Polling Questions Presentations Polling Questions Q&A Closing Remarks 2 Introduction to the atom Alliance Multi-state
Welcome to Medicare: Exam Overview June 8, 2016 Agenda Opening Remarks Housekeeping Polling Questions Presentations Polling Questions Q&A Closing Remarks 2 Introduction to the atom Alliance Multi-state
Evaluating an Apparent Unprovoked First Seizure in Adults
 Evaluating an Apparent Unprovoked First Seizure in Adults Case Presentation A 52 year old woman is brought to the emergency room after a witnessed seizure. She was shopping at the local mall when she was
Evaluating an Apparent Unprovoked First Seizure in Adults Case Presentation A 52 year old woman is brought to the emergency room after a witnessed seizure. She was shopping at the local mall when she was
PCCSS, LLP Pulmonary, Critical Care & Sleep Specialists
 NAME: AGE: DOB: DATE: REQUESTING PHYSICIAN: NOTE: Please help us find out about you by filling out the Patient side of this form on pages 1 3. If you don t know the answer to one of the questions, ask
NAME: AGE: DOB: DATE: REQUESTING PHYSICIAN: NOTE: Please help us find out about you by filling out the Patient side of this form on pages 1 3. If you don t know the answer to one of the questions, ask
Patient to complete this information
 Patient to complete this information Patient s Name Birth date Today s date Referring Physician Primary Care Physician Age Occupation Retired, how long? Prior operations Medications Type Date Name Dose
Patient to complete this information Patient s Name Birth date Today s date Referring Physician Primary Care Physician Age Occupation Retired, how long? Prior operations Medications Type Date Name Dose
Logo Placement *######*
 INPATIENT ADMITTING HISTORY AND PHYSICAL Page 1 of 8 Date of Service / / Time of Service : AM PM CHIEF COMPLAINT(S): HISTORY UNOBTAINABLE -- Patient was admitted UNACCOMPANIED, and no history could be
INPATIENT ADMITTING HISTORY AND PHYSICAL Page 1 of 8 Date of Service / / Time of Service : AM PM CHIEF COMPLAINT(S): HISTORY UNOBTAINABLE -- Patient was admitted UNACCOMPANIED, and no history could be
H&P Checklist (Inpatient) Evaluator: Subject: Program:
 Evaluator: Subject: Program:") H&P Checklist (Inpatient) Evaluator: Subject: Program: PROFESSIONALISM 1) Introduces self/role and preceptor Did 2) Verbal and non-verbal language demonstrates respect for patient & family. Did 3) Respects
H&P Checklist (Inpatient) Evaluator: Subject: Program: PROFESSIONALISM 1) Introduces self/role and preceptor Did 2) Verbal and non-verbal language demonstrates respect for patient & family. Did 3) Respects
Note for Jane Doe on 7/22/05 - Chart 5407
 Note for Jane Doe on 7/22/05 - Chart 5407 Chief Complaint: This 31 year old female presents today with abdominal pain. Duration: Condition has existed for one month. Modifying Factors: Patient indicates
Note for Jane Doe on 7/22/05 - Chart 5407 Chief Complaint: This 31 year old female presents today with abdominal pain. Duration: Condition has existed for one month. Modifying Factors: Patient indicates
Are You Sure You Can Bill Preventive Services? Disclaimer
 Are You Sure You Can Bill Preventive Services? AAPC Regional Conference Chicago, Illinoisi October 2012 1 Disclaimer The information in this presentation was current at the time the presentation was complied
Are You Sure You Can Bill Preventive Services? AAPC Regional Conference Chicago, Illinoisi October 2012 1 Disclaimer The information in this presentation was current at the time the presentation was complied
Physical Examination Reporting Form
 Building Trades National Medical Screening Program Physical Examination Reporting Form Name: Date: P1. Vital Signs Height: BP: / Weight: lbs. #2 nd BP:* / Arm: L R Cuff Size:** Regular Large Ped Pulse:
Building Trades National Medical Screening Program Physical Examination Reporting Form Name: Date: P1. Vital Signs Height: BP: / Weight: lbs. #2 nd BP:* / Arm: L R Cuff Size:** Regular Large Ped Pulse:
Compliance Department ELEMENTS OF GENITOURINARY EXAMINATION 11/2010
 Compliance Department ELEMENTS OF GENITOURINARY EXAMINATION 11/2010 Elements of Examination Constitutional Measurement of any three of the following seven vital signs: 1) sitting or standing blood pressure,
Compliance Department ELEMENTS OF GENITOURINARY EXAMINATION 11/2010 Elements of Examination Constitutional Measurement of any three of the following seven vital signs: 1) sitting or standing blood pressure,
Evaluation and Management (E/M) Training. Module 12
 Training. Module 12") Evaluation and Management (E/M) Training Module 12 AMA Disclaimer CPT copyright 2011 American Medical Association. All rights reserved. Fee schedules, relative value units, conversion factors and/or related
Evaluation and Management (E/M) Training Module 12 AMA Disclaimer CPT copyright 2011 American Medical Association. All rights reserved. Fee schedules, relative value units, conversion factors and/or related
Fundamental E&M for Primary Care Risk Adjustment 2010
 2-hr Fundamental E&M for Primary Care Risk Adjustment 2010 E/M Relevance to Diagnosis Coding Presented by: Liz Jeremia Market Consultant Toni Toone, CPC, CPMA Sr. Provider Training & Development Consultant
2-hr Fundamental E&M for Primary Care Risk Adjustment 2010 E/M Relevance to Diagnosis Coding Presented by: Liz Jeremia Market Consultant Toni Toone, CPC, CPMA Sr. Provider Training & Development Consultant
A Strategic Approach to HCCs and Risk Adjustment Kathryn DeVault, MSL, RHIA, CCS, CCS-P, FAHIMA
 A Strategic Approach to HCCs and Risk Adjustment Kathryn DeVault, MSL, RHIA, CCS, CCS-P, FAHIMA Objectives Identify the impact of HCC coding in the Medicare Advantage (MA) program Define documentation
A Strategic Approach to HCCs and Risk Adjustment Kathryn DeVault, MSL, RHIA, CCS, CCS-P, FAHIMA Objectives Identify the impact of HCC coding in the Medicare Advantage (MA) program Define documentation
Note for Jane Doe on 02/10/ Chart 3642
 Note for Jane Doe on 02/10/2005 - Chart 3642 Consultation was requested by Dr. Smith Chief Complaint (1/1): This 31 year old Caucasian female presents today for evaluation of chest pain. Chest pains HPI:
Note for Jane Doe on 02/10/2005 - Chart 3642 Consultation was requested by Dr. Smith Chief Complaint (1/1): This 31 year old Caucasian female presents today for evaluation of chest pain. Chest pains HPI:
CODING and RVU s: What AHLTA Can Do For You (and what it can t)! Edited 2015 from USAFP Conference March 2007 Mark Stackle, MD
! Edited 2015 from USAFP Conference March 2007 Mark Stackle, MD") CODING and RVU s: What AHLTA Can Do For You (and what it can t)! Edited 2015 from USAFP Conference March 2007 Mark Stackle, MD Coding Basics The Dry Stuff Evaluation and Management Coding 2/3 areas for
CODING and RVU s: What AHLTA Can Do For You (and what it can t)! Edited 2015 from USAFP Conference March 2007 Mark Stackle, MD Coding Basics The Dry Stuff Evaluation and Management Coding 2/3 areas for
Supporting Documents Case Studies
 Supporting Documents Case Studies ONA Presentation/Case Studies 1 CASE STUDY #1 CC: Right Breast Lump History of Present Illness: 41 yr old G3P0 with an LMP of 08/01/2017 who presents today to discuss
Supporting Documents Case Studies ONA Presentation/Case Studies 1 CASE STUDY #1 CC: Right Breast Lump History of Present Illness: 41 yr old G3P0 with an LMP of 08/01/2017 who presents today to discuss
Intensive Behavioral Therapy for Obesity Guidelines
 Health First Technologies Inc. dba Renua Medical 777 E. William Street, Suite 210 Carson City, NV 89701 877-885-1258 775-546-6156 E-fax www.renuamedical.com Intensive Behavioral Therapy for Obesity Guidelines
Health First Technologies Inc. dba Renua Medical 777 E. William Street, Suite 210 Carson City, NV 89701 877-885-1258 775-546-6156 E-fax www.renuamedical.com Intensive Behavioral Therapy for Obesity Guidelines
Counseling to Prevent Tobacco Use
 News Flash Vaccination is the Best Protection Against the Flu. This year, the Centers for Disease Control and Prevention (CDC) is encouraging everyone 6 months of age and older to get vaccinated against
News Flash Vaccination is the Best Protection Against the Flu. This year, the Centers for Disease Control and Prevention (CDC) is encouraging everyone 6 months of age and older to get vaccinated against
Charting Smarter, not Longer: Basic Concepts in Outpatient Coding
 Charting Smarter, not Longer: Basic Concepts in Outpatient Coding Workshop WA01 SGIM 29 th Annual Meeting April 27, 2006 Sponsored by the SGIM Clinical Practice Task Force (CPTF) Faculty: Jeannine Engel,
Charting Smarter, not Longer: Basic Concepts in Outpatient Coding Workshop WA01 SGIM 29 th Annual Meeting April 27, 2006 Sponsored by the SGIM Clinical Practice Task Force (CPTF) Faculty: Jeannine Engel,
HIV/AIDS Care: The Service (CPT) Code Evaluation and Management Series 1
 Code Evaluation and Management Series 1") HIV/AIDS Care: The Service (CPT) Code Evaluation and Management Series 1 Prepared By: Stacey L. Murphy, MPA, RHIA, CPC AHIMA Approved ICD-10-CM/ICD-10-CM Trainer Learning Outcomes Explain the importance
HIV/AIDS Care: The Service (CPT) Code Evaluation and Management Series 1 Prepared By: Stacey L. Murphy, MPA, RHIA, CPC AHIMA Approved ICD-10-CM/ICD-10-CM Trainer Learning Outcomes Explain the importance
OUTPATIENT SUMMARY LIST. Social / Family HX. Additional Information: USE A SECOND SHEET IF NECESSARY DO NOT WRITE ON BACK OF FORM.
 Washington Institute of Surgery, LLC. 2311 M Street, N.W. Suite 501, Washington, DC 20037. Tel: (202) 775 9375 Fax: (202) 776 9088 Web: www.washingtoninstituteofsurgery.com OUTPATIENT SUMMARY LIST MR #:
Washington Institute of Surgery, LLC. 2311 M Street, N.W. Suite 501, Washington, DC 20037. Tel: (202) 775 9375 Fax: (202) 776 9088 Web: www.washingtoninstituteofsurgery.com OUTPATIENT SUMMARY LIST MR #:
Evaluation and Management Coding Advisor
 Evaluation and Management Coding Advisor 2016 Contents Chapter 1: Introduction... 1 Origin And Development Of Evaluation And Management Codes... 1 Physician or Other Qualified Health Care Professional...
Evaluation and Management Coding Advisor 2016 Contents Chapter 1: Introduction... 1 Origin And Development Of Evaluation And Management Codes... 1 Physician or Other Qualified Health Care Professional...
04/11/2014. Retina Coding and Reimbursement 101. Financial Disclosure. Chief Complaint
 Retina Coding and Reimbursement 101 William T. Koch, COA, COE, CPC Administrative Director Director of Billing Operations The Retina Institute St. Louis, Missouri Advisory Boards Allergan Genentech Regeneron
Retina Coding and Reimbursement 101 William T. Koch, COA, COE, CPC Administrative Director Director of Billing Operations The Retina Institute St. Louis, Missouri Advisory Boards Allergan Genentech Regeneron
Compliance Department ELEMENTS OF EAR, NOSE AND THROAT EXAMINATION 11/2010
 Compliance Department ELEMENTS OF EAR, NOSE AND THROAT EXAMINATION 11/2010 System/ Body Area Constitutional Measurement of any three of the following seven vital signs: 1) sitting or standing blood pressure,
Compliance Department ELEMENTS OF EAR, NOSE AND THROAT EXAMINATION 11/2010 System/ Body Area Constitutional Measurement of any three of the following seven vital signs: 1) sitting or standing blood pressure,
John Sanchez, D.O. August 18, 2013
 John Sanchez, D.O. August 18, 2013 Ø Coding Caps Ø Relevance to Clinical Practice Ø Current Guidelines 1995 (organ systems) 1997 (bullets) Ø Definitions ICD- 9 CPT E/M ( 99 _ ) Ø Who Should Determine the
John Sanchez, D.O. August 18, 2013 Ø Coding Caps Ø Relevance to Clinical Practice Ø Current Guidelines 1995 (organ systems) 1997 (bullets) Ø Definitions ICD- 9 CPT E/M ( 99 _ ) Ø Who Should Determine the
Med 536 Communicating About Prognosis Workshop. Case 2
 Med 536 Communicating About Prognosis Workshop Case 2 ID / CC: 33 year-old man with intracranial hemorrhage History of the Presenting Illness 33 year-old man with a prior history of melanoma of the neck
Med 536 Communicating About Prognosis Workshop Case 2 ID / CC: 33 year-old man with intracranial hemorrhage History of the Presenting Illness 33 year-old man with a prior history of melanoma of the neck
Reporting Mammograms for Medicare Patients Coding these preventive procedures depends on the payer.
 Reporting Mammograms for Medicare Patients Coding these preventive procedures depends on the payer. By Barbara Aubry, RN, CPC, CPMA, CHCQM, FABQAURP For 2017, the American Medical Association (AMA) deleted
Reporting Mammograms for Medicare Patients Coding these preventive procedures depends on the payer. By Barbara Aubry, RN, CPC, CPMA, CHCQM, FABQAURP For 2017, the American Medical Association (AMA) deleted
04/06/2015. Documentation Do s and Don ts In The Retina Practice. Financial Disclosure. Documentation Dos and Don ts
 Documentation Do s and Don ts In The Retina Practice William T. Koch, COA, COE, CPC Administrative Director Director of Billing Operations The Retina Institute St. Louis, Missouri Advisory Boards Allergan
Documentation Do s and Don ts In The Retina Practice William T. Koch, COA, COE, CPC Administrative Director Director of Billing Operations The Retina Institute St. Louis, Missouri Advisory Boards Allergan
Appendix I: E/M CodeBuilder
 Appendix I: E/M CodeBuilder For use with CMS 1997 Documentation Guidelines for Evaluation & Management Coding, which is located on the Student Companion Web Site at www.cengagebrain.com. CMS also published
Appendix I: E/M CodeBuilder For use with CMS 1997 Documentation Guidelines for Evaluation & Management Coding, which is located on the Student Companion Web Site at www.cengagebrain.com. CMS also published
Medicare Medicare Annual Well Visits. CHUG October 23, 2011
 Medicare 2011 Medicare Annual Well Visits CHUG October 23, 2011 Background/Disclaimers 60 % of my clinical work is Geriatrics 40% Medical Informatics No conflict of interests I do not work for CMS Agenda
Medicare 2011 Medicare Annual Well Visits CHUG October 23, 2011 Background/Disclaimers 60 % of my clinical work is Geriatrics 40% Medical Informatics No conflict of interests I do not work for CMS Agenda
10/17/2013. Billing and Coding in Long Term Care: Keeping the Wolves at Bay. Disclosure
 Billing and Coding in Long Term Care: Keeping the Wolves at Bay Maine Medical Directors Association Annual Conference October 11, 2013 Alva S Baker, MD, CMD-R Disclosure Dr. Baker has indicated that he
Billing and Coding in Long Term Care: Keeping the Wolves at Bay Maine Medical Directors Association Annual Conference October 11, 2013 Alva S Baker, MD, CMD-R Disclosure Dr. Baker has indicated that he
COMPREHENSIVE PAIN MANAGEMENT NEW PATIENT INTAKE FORM ( )
") 1 13660 N 94th Dr., Suite C-4 Peoria, AZ 85381-4841 phone (623) 266-1722 fax (623) 266-1746 COMPREHENSIVE PAIN MANAGEMENT NEW PATIENT INTAKE FORM (Please Print) Last Name: Middle: First: Home Phone: DOB:
1 13660 N 94th Dr., Suite C-4 Peoria, AZ 85381-4841 phone (623) 266-1722 fax (623) 266-1746 COMPREHENSIVE PAIN MANAGEMENT NEW PATIENT INTAKE FORM (Please Print) Last Name: Middle: First: Home Phone: DOB:
Medicare Preventive Services and Screenings
 Welcome to PMI s Webinar Presentation Brought to you by: pmimd.com Meet the Presenter Linda D'Spain, CMPE, CMC, CMIS, CMOM, CMCO On the topic: Medicare Preventive Services and Screenings Welcome to s Webinar
Welcome to PMI s Webinar Presentation Brought to you by: pmimd.com Meet the Presenter Linda D'Spain, CMPE, CMC, CMIS, CMOM, CMCO On the topic: Medicare Preventive Services and Screenings Welcome to s Webinar
DUKEMedicine. SMITH, JAMES MRN: D DOB: 2/6/1993, Sex: M Adm: 2/15/2016, D/C: 2/15/2016
 History Chief Complaint Patient presents with Motor Vehicle Crash HPI James Smith is a 23 y.o. male here today for evaluation of injuries sustained today in a MVA. He was a restrained driver of a car struck
History Chief Complaint Patient presents with Motor Vehicle Crash HPI James Smith is a 23 y.o. male here today for evaluation of injuries sustained today in a MVA. He was a restrained driver of a car struck
2015 Behavioral Medicine Resident Chart Documentation. Laura Sullivan, MSW, CPC Compliance Auditor
 2015 Behavioral Medicine Resident Chart Documentation Laura Sullivan, MSW, CPC Compliance Auditor 1 Legal Stuff The information provided here is being provided by a nonlawyer and should not be construed
2015 Behavioral Medicine Resident Chart Documentation Laura Sullivan, MSW, CPC Compliance Auditor 1 Legal Stuff The information provided here is being provided by a nonlawyer and should not be construed
ChiroCredit.com / OnlineCE.com presents Documentation 101 Part 5 of 10 Instructor: Paul Sherman, DC
 Online Continuing Education Courses www.onlinece.com www.chirocredit.com ChiroCredit.com / OnlineCE.com presents Documentation 101 Part 5 of 10 Instructor: Paul Sherman, DC Important Notice: This download
Online Continuing Education Courses www.onlinece.com www.chirocredit.com ChiroCredit.com / OnlineCE.com presents Documentation 101 Part 5 of 10 Instructor: Paul Sherman, DC Important Notice: This download
EPSDT. EPSDT-Acute Visit & Well Visit EPSDT Documentation. Acute Visit & Well Visit L. Chana Spearmon, MD, FAAP Neighborhood Health Pediatrics
 EPSDT Acute Visit & Well Visit L. Chana Spearmon, MD, FAAP Neighborhood Health Pediatrics EPSDT Documentation Comprehensive Health and Developmental History Screenings for Vision/Hearing Developmental
EPSDT Acute Visit & Well Visit L. Chana Spearmon, MD, FAAP Neighborhood Health Pediatrics EPSDT Documentation Comprehensive Health and Developmental History Screenings for Vision/Hearing Developmental
2016 Behavioral Medicine Resident Chart Documentation. Laura Sullivan, MSW, CPC Compliance Auditor
 2016 Behavioral Medicine Resident Chart Documentation Laura Sullivan, MSW, CPC Compliance Auditor 1 Legal Stuff The information provided here is being provided by a nonlawyer and should not be construed
2016 Behavioral Medicine Resident Chart Documentation Laura Sullivan, MSW, CPC Compliance Auditor 1 Legal Stuff The information provided here is being provided by a nonlawyer and should not be construed
Patient Care Report Guidelines
 A rrival on scene / Scene assessment C omplaint H istory A. Position of patient B. Impression of patient C. Does the patient acknowledge your presence D. Any significant characteristics of the scene A.
A rrival on scene / Scene assessment C omplaint H istory A. Position of patient B. Impression of patient C. Does the patient acknowledge your presence D. Any significant characteristics of the scene A.
History Data Panel. Case 030 Preg Trauma. Presenting Complaint Altered mental status s/p MVC. Person Giving Information EMS
 History Data Panel Presenting Complaint Altered mental status s/p MVC Person Giving Information EMS History of Present Illness 28 year old woman, 35 weeks pregnant per report of her husband the passenger.
History Data Panel Presenting Complaint Altered mental status s/p MVC Person Giving Information EMS History of Present Illness 28 year old woman, 35 weeks pregnant per report of her husband the passenger.
CONSULTATION REFRESHER
 060310 BLAST CONSULTATION REFRESHER We have had many requests from clients recently asking how to correctly code Medicare consultations utilizing the new CMS requirements. Attached is a mini refresher
060310 BLAST CONSULTATION REFRESHER We have had many requests from clients recently asking how to correctly code Medicare consultations utilizing the new CMS requirements. Attached is a mini refresher
UBMD Internal Medicine
 UBMD Internal Medicine Clinical Documentation Example Established Outpatient Visit - 99215 Pat Kisiel-Neunder, Compliance Administrator Email: pkisieln@buffalo.edu Regulations The following information
UBMD Internal Medicine Clinical Documentation Example Established Outpatient Visit - 99215 Pat Kisiel-Neunder, Compliance Administrator Email: pkisieln@buffalo.edu Regulations The following information
REASON FOR REFERRAL Referred for blisters and rash of mucous membranes and skin.
 Report 1 Listen to the audio to fill in the blanks. Name: DERMATOLOGY CONSULTATION REPORT REASON FOR REFERRAL Referred for blisters and rash of mucous membranes and skin. HISTORY OF PRESENT ILLNESS Rash
Report 1 Listen to the audio to fill in the blanks. Name: DERMATOLOGY CONSULTATION REPORT REASON FOR REFERRAL Referred for blisters and rash of mucous membranes and skin. HISTORY OF PRESENT ILLNESS Rash
Medicare & Dual Options. 1. Every page of the EMR document must include: a. Member Name b. Patient Identifiers (i.e. Date of Birth) c.
 c.") Medicare & SUBMITTING PROGRESS NOTES OR EMR You may use your own progress notes or Electronic Medical Record (EMR) to document the annual comprehensive examination. The EMR must include the elements indicated
Medicare & SUBMITTING PROGRESS NOTES OR EMR You may use your own progress notes or Electronic Medical Record (EMR) to document the annual comprehensive examination. The EMR must include the elements indicated
Program Script. Nursing Assessment The Head-to-Toe Assessment
 Program Script Nursing Assessment The Head-to-Toe Assessment This document comprises the complete script for this program including chapter titles. This is provided to instructors to enhance the educational
Program Script Nursing Assessment The Head-to-Toe Assessment This document comprises the complete script for this program including chapter titles. This is provided to instructors to enhance the educational
Evaluation and Management Services
 Advanced E/M Auditing Evaluation and Management Services Disclaimer area Evaluation and Management Services History Exam Medical Decision Making Select the E/M Code Subjective portion of the visit where
Advanced E/M Auditing Evaluation and Management Services Disclaimer area Evaluation and Management Services History Exam Medical Decision Making Select the E/M Code Subjective portion of the visit where
Evaluation & Mangement ( E & M) Visits Adapted from 1997 CMS Guidance Using Single Organ System
 Visits Adapted from 1997 CMS Guidance Using Single Organ System") 5/7/15 University of Rochester Center for Health & Behavioral Training 1 Evaluation & Mangement ( E & M) Visits Adapted from 1997 CMS Guidance Using Single Organ System New Patient Office Visit [Patient
5/7/15 University of Rochester Center for Health & Behavioral Training 1 Evaluation & Mangement ( E & M) Visits Adapted from 1997 CMS Guidance Using Single Organ System New Patient Office Visit [Patient
A PROVIDER S GUIDE TO PREVENTIVE HEALTH SERVICES FOR YOUR PATIENTS
 ConnectiCare, together with the Centers for Medicare & Medicaid Services, encourages the use of preventive health services. For certain basic preventive health services, ConnectiCare Medicare Plan beneficiaries
ConnectiCare, together with the Centers for Medicare & Medicaid Services, encourages the use of preventive health services. For certain basic preventive health services, ConnectiCare Medicare Plan beneficiaries
PUFF THE MAGIC DRAGON
 PUFF THE MAGIC DRAGON AN UNUSUAL CASE OF A PUFFY FACE MA ACP Annual Scientific Meeting Gurbir Gill, M.D., PGY-3 (Associate) George M. Abraham, MD, MPH, FACP Department of Medicine, Saint Vincent Hospital,
PUFF THE MAGIC DRAGON AN UNUSUAL CASE OF A PUFFY FACE MA ACP Annual Scientific Meeting Gurbir Gill, M.D., PGY-3 (Associate) George M. Abraham, MD, MPH, FACP Department of Medicine, Saint Vincent Hospital,
Documentation Dissection
 History of Present Illness: Documentation Dissection The patient is a 50-year-old male c/o symptoms for past 4 months 1, severe 2 bloating and stomach cramps, some nausea, vomiting, diarrhea. In last 3
History of Present Illness: Documentation Dissection The patient is a 50-year-old male c/o symptoms for past 4 months 1, severe 2 bloating and stomach cramps, some nausea, vomiting, diarrhea. In last 3
E/M for Orthopaedics
 E/M for Orthopaedics Julie A. Leu, CPC, CPMA, CPC-I 2009-2011 NAB Member, Region 7 1 Objectives Review of Evaluation and Management Guidelines Comparison of the 1995 and 1997 Exam Guidelines Reporting
E/M for Orthopaedics Julie A. Leu, CPC, CPMA, CPC-I 2009-2011 NAB Member, Region 7 1 Objectives Review of Evaluation and Management Guidelines Comparison of the 1995 and 1997 Exam Guidelines Reporting
Welcome to: Coding Scenarios for STD Clinic Visits. We will begin in a few minutes. There will be no sound until the webinar starts.
 Welcome to: Coding Scenarios for STD Clinic Visits We will begin in a few minutes. There will be no sound until the webinar starts. Welcome to: Coding Scenarios for STD Clinic Visits You are using audio
Welcome to: Coding Scenarios for STD Clinic Visits We will begin in a few minutes. There will be no sound until the webinar starts. Welcome to: Coding Scenarios for STD Clinic Visits You are using audio
Medicare Well Patient Visits
 Last First MI Type of Wellness Exam: Medicare Part B Eligibility Date: Vital signs: IPPE Welcome to Medicare Select G0402, G0403, G0404 or G0405 (1 time during first 12 months on Medicare) Medicare Well
Last First MI Type of Wellness Exam: Medicare Part B Eligibility Date: Vital signs: IPPE Welcome to Medicare Select G0402, G0403, G0404 or G0405 (1 time during first 12 months on Medicare) Medicare Well
Rural STEMI System of Care Success. Nicole Huber, PA-C Cumberland Healthcare Emergency Department
 Rural STEMI System of Care Success Nicole Huber, PA-C Cumberland Healthcare Emergency Department DISCLOSURES I HAVE NO ACTUAL OR POTENTIAL CONFLICT OF INTEREST IN RELATION TO THIS PRESENTATION Ideal Process
Rural STEMI System of Care Success Nicole Huber, PA-C Cumberland Healthcare Emergency Department DISCLOSURES I HAVE NO ACTUAL OR POTENTIAL CONFLICT OF INTEREST IN RELATION TO THIS PRESENTATION Ideal Process
Coders Are Unstoppable!! Are You Sure You Can Bill Preventive Services? Presented by Pat Champion, CPC, CPC-I
 Coders Are Unstoppable!! Are You Sure You Can Bill Preventive Services? Presented by Pat Champion, CPC, CPC-I 1 Let s Take a Look Review Initial Preventive Physical Examination (IPPE) Understand the difference
Coders Are Unstoppable!! Are You Sure You Can Bill Preventive Services? Presented by Pat Champion, CPC, CPC-I 1 Let s Take a Look Review Initial Preventive Physical Examination (IPPE) Understand the difference
Date of Admission: [DATE]. Date of Discharge:
![Date of Admission: [DATE]. Date of Discharge:](/thumbs/74/71277118.jpg "Date of Admission: [DATE]. Date of Discharge:") Date of Admission: [DATE]. Date of Discharge: History of Present Illness: Mr. [NAME] AKA [NAME] is a 31-year-old male who presents to the [PLACE] Trauma Surgery Service as a moderate trauma on [DATE] following
Date of Admission: [DATE]. Date of Discharge: History of Present Illness: Mr. [NAME] AKA [NAME] is a 31-year-old male who presents to the [PLACE] Trauma Surgery Service as a moderate trauma on [DATE] following
A PROVIDER S GUIDE TO PREVENTIVE HEALTH SERVICES FOR YOUR PATIENTS
 ConnectiCare, together with the Centers for Medicare & Medicaid Services, encourages the use of preventive health services. For certain basic preventive health services, ConnectiCare Medicare Plan beneficiaries
ConnectiCare, together with the Centers for Medicare & Medicaid Services, encourages the use of preventive health services. For certain basic preventive health services, ConnectiCare Medicare Plan beneficiaries
GENERAL MULTI-SYSTEM EXAMINATION WORKSHEET
 GENERAL MULTI-SYSTEM EXAMINATION WORKSHEET HPI ROS PFSH History Location Timing Allergic/Imm Eyes Musc/Sk el Past History Documentation of history of Problem Pertinent ROS = Related System Expanded General
GENERAL MULTI-SYSTEM EXAMINATION WORKSHEET HPI ROS PFSH History Location Timing Allergic/Imm Eyes Musc/Sk el Past History Documentation of history of Problem Pertinent ROS = Related System Expanded General
E & M Chart Audit for the Allergy Practice
 E & M Chart Audit for the Allergy Practice Teresa Thompson, CPC, CCC TM Consulting, Inc. P O Box 267 Carlsborg, WA 98324 360-683-8293 Physician Documentation Verification that the coding is appropriate
E & M Chart Audit for the Allergy Practice Teresa Thompson, CPC, CCC TM Consulting, Inc. P O Box 267 Carlsborg, WA 98324 360-683-8293 Physician Documentation Verification that the coding is appropriate
Preventative and Immunization Brochure
 Preventative Immunization Brochure Table Of Contents 2016 Medicare Advantage Preventative Visits Guidelines... 1 Preventative Visits... 3 Common Preventive Services s*... 5 Additional Services Provided
Preventative Immunization Brochure Table Of Contents 2016 Medicare Advantage Preventative Visits Guidelines... 1 Preventative Visits... 3 Common Preventive Services s*... 5 Additional Services Provided
Documentation Dissection
 Documentation Dissection 07/07/20xx Phone call to patient post discharge: Discharged from medical center 7/5/20xx 1 dx dehydration (&HH orders) 1. I spoke with patient s niece who states she is out with
Documentation Dissection 07/07/20xx Phone call to patient post discharge: Discharged from medical center 7/5/20xx 1 dx dehydration (&HH orders) 1. I spoke with patient s niece who states she is out with
Reassessment: Neuroimaging in the Emergency Patient Presenting with Seizure
 Reassessment: Neuroimaging in the Emergency Patient Presenting with Seizure This evidence-based report provides clinicians with information to identify which seizure patients in the emergency department
Reassessment: Neuroimaging in the Emergency Patient Presenting with Seizure This evidence-based report provides clinicians with information to identify which seizure patients in the emergency department
CLINICAL SKILLS ASSESSMENT
 Office of Medical Education (412) 648-8714 Fax: (412) 383-7477 www.omed.pitt.edu CLINICAL SKILLS ASSESSMENT Information for Medical Students Prepared by the Performance Based Assessment Task Force University
Office of Medical Education (412) 648-8714 Fax: (412) 383-7477 www.omed.pitt.edu CLINICAL SKILLS ASSESSMENT Information for Medical Students Prepared by the Performance Based Assessment Task Force University
2013 UPDATE ON PREVENTION & SCREENING IN THE ELDERLY West Virginia Geriatrics Society October 3, 2013
 2013 UPDATE ON PREVENTION & SCREENING IN THE ELDERLY West Virginia Geriatrics Society October 3, 2013 Joy Pelfrey, RN, MSN, FNP, NEA-BC Director of Senior Service Line Objective Providers will understand
2013 UPDATE ON PREVENTION & SCREENING IN THE ELDERLY West Virginia Geriatrics Society October 3, 2013 Joy Pelfrey, RN, MSN, FNP, NEA-BC Director of Senior Service Line Objective Providers will understand
The Third-Party Reimbursement Process for Orthotics
 The Third-Party Reimbursement Process for Orthotics When the foot hits the ground, everything changes. We know that over 90% of the population suffers with overpronation of their feet. Implementing Foot
The Third-Party Reimbursement Process for Orthotics When the foot hits the ground, everything changes. We know that over 90% of the population suffers with overpronation of their feet. Implementing Foot
HUSKY Health Benefits and Prior Authorization Requirements Grid* Behavioral Health Partnership Effective: January 1, 2012
 Behavioral Health Health and Behavior Assessments (CPT 96150-96155) When Performed by Psychologists Mental Health Inpatient 100% covered under medical benefit for members with diagnoses outside the range
Behavioral Health Health and Behavior Assessments (CPT 96150-96155) When Performed by Psychologists Mental Health Inpatient 100% covered under medical benefit for members with diagnoses outside the range
Describe how chief complaint developed in a chronologic and organized manner. Address why the patient is seeking attention at this time
 B. Guide to the Comprehensive Adult H&P Write Up (Adapted from D Bynum MD, C Colford MD, D McNeely MD, University of North Carolina at Chapel Hill, North Carolina) Chief Complaint Source & Reliability
B. Guide to the Comprehensive Adult H&P Write Up (Adapted from D Bynum MD, C Colford MD, D McNeely MD, University of North Carolina at Chapel Hill, North Carolina) Chief Complaint Source & Reliability
SMALL GROUP DISCUSSION
 MHD II, Seesion II Student Copy - Page 1 SMALL GROUP DISCUSSION MHD II Session II JANUARY 15, 2014 Recent Review highlighting disease process in Case 2: Fasano A, Catassi, C. NEJM 2012; 367: 2419-26 STUDENT
MHD II, Seesion II Student Copy - Page 1 SMALL GROUP DISCUSSION MHD II Session II JANUARY 15, 2014 Recent Review highlighting disease process in Case 2: Fasano A, Catassi, C. NEJM 2012; 367: 2419-26 STUDENT
Evaluation and Management (E/M) Training. Module 9
 Training. Module 9") Evaluation and Management (E/M) Training Module 9 AMA Disclaimer CPT copyright 2011 American Medical Association. All rights reserved. Fee schedules, relative value units, conversion factors and/or related
Evaluation and Management (E/M) Training Module 9 AMA Disclaimer CPT copyright 2011 American Medical Association. All rights reserved. Fee schedules, relative value units, conversion factors and/or related
This section includes billing guidelines and treatment information for alternative care providers including:
 Alternative care Alternative care overview This section includes billing guidelines and treatment information for alternative care providers including: Acupuncturists/East Asian Medicine Practitioners
Alternative care Alternative care overview This section includes billing guidelines and treatment information for alternative care providers including: Acupuncturists/East Asian Medicine Practitioners
Discuss the Process for PQRS Reporting. Explain How Often Therapists Should Report
 2016 Define PQRS Explain Who Should Participate Discuss the Process for PQRS Reporting Explain How Often Therapists Should Report Physician Quality Reporting System A quality reporting system for Medicare
2016 Define PQRS Explain Who Should Participate Discuss the Process for PQRS Reporting Explain How Often Therapists Should Report Physician Quality Reporting System A quality reporting system for Medicare
10/20/2015. Valerie Ballard, DNP Women s Health Nurse Practitioner
 S.Storm - Dementia Valerie Ballard, DNP Women s Health Nurse Practitioner A WELL VISIT IS PART OF A JOURNEY TO WELLNESS AND HEALTH FOR OUR PATIENTS. As a provider, take the opportunity to listen, teach
S.Storm - Dementia Valerie Ballard, DNP Women s Health Nurse Practitioner A WELL VISIT IS PART OF A JOURNEY TO WELLNESS AND HEALTH FOR OUR PATIENTS. As a provider, take the opportunity to listen, teach
BCCCNP NEW PROGRAM FORMS WEBINAR. January 8, 2019 E.J. Siegl, Program Director Breast and Cervical Cancer Control Navigation Program
 BCCCNP NEW PROGRAM FORMS WEBINAR January 8, 2019 E.J. Siegl, Program Director Breast and Cervical Cancer Control Navigation Program NEW GRANT CHANGE IN FOCUS New Clinical Data Requirements by CDC for BCCCNP
BCCCNP NEW PROGRAM FORMS WEBINAR January 8, 2019 E.J. Siegl, Program Director Breast and Cervical Cancer Control Navigation Program NEW GRANT CHANGE IN FOCUS New Clinical Data Requirements by CDC for BCCCNP
Coding for the Contraceptive Implant and IUDs
 LARC Quick Coding Guide 2018 UPDATE Coding for the Contraceptive Implant and IUDs CORRECT CODING can result in more appropriate compensation for services and devices. To help practices receive appropriate
LARC Quick Coding Guide 2018 UPDATE Coding for the Contraceptive Implant and IUDs CORRECT CODING can result in more appropriate compensation for services and devices. To help practices receive appropriate
Lumify. Lumify reimbursement guide {D DOCX / 1
 Lumify Lumify reimbursement guide {D0672917.DOCX / 1 {D0672917.DOCX / 1 } Contents Overview 4 How claims are paid 4 Documentation requirements 5 Billing codes for ultrasound: Non-hospital setting 6 Billing
Lumify Lumify reimbursement guide {D0672917.DOCX / 1 {D0672917.DOCX / 1 } Contents Overview 4 How claims are paid 4 Documentation requirements 5 Billing codes for ultrasound: Non-hospital setting 6 Billing
CASE-BASED SMALL GROUP DISCUSSION MHD II SESSION VI
 MHD II, Session VI, Student Copy Page 1 CASE-BASED SMALL GROUP DISCUSSION MHD II SESSION VI Wednesday, MARCH 26, 2014 STUDENT COPY MHD II, Session VI, Student Copy Page 2 CASE 1 History: A 57-year-old
MHD II, Session VI, Student Copy Page 1 CASE-BASED SMALL GROUP DISCUSSION MHD II SESSION VI Wednesday, MARCH 26, 2014 STUDENT COPY MHD II, Session VI, Student Copy Page 2 CASE 1 History: A 57-year-old
Compliance Institute 2003
 Compliance Institute 2003 The Fundamentals of Coding for Non-Coders and Potential Compliance Issues Related to Coding Activities April 29, 2003 Robert A. Pelaia, JD, CPC Associate General Counsel Director
Compliance Institute 2003 The Fundamentals of Coding for Non-Coders and Potential Compliance Issues Related to Coding Activities April 29, 2003 Robert A. Pelaia, JD, CPC Associate General Counsel Director
DATA BASE SAMPLE: PHYSICAL EXAMINATION WITH ALL NORMAL FINDINGS
 DATA BASE SAMPLE: PHYSICAL EXAMINATION WITH ALL NORMAL FINDINGS GENERAL APPEARANCE: (include general mental status) 45 y/o female who is awake and alert and who appears healthy and looks her stated age
DATA BASE SAMPLE: PHYSICAL EXAMINATION WITH ALL NORMAL FINDINGS GENERAL APPEARANCE: (include general mental status) 45 y/o female who is awake and alert and who appears healthy and looks her stated age
Tobacco Use: Screening & Cessation Intervention
 Tobacco Use: Screening and Cessation Intervention MSSP ACO Measure Tobacco Use: Screening & Cessation Intervention Domain: Preventive Care and Screening ACO 17 PREV- 10 PQRS - 226 NQF 0028 Measure Steward:
Tobacco Use: Screening and Cessation Intervention MSSP ACO Measure Tobacco Use: Screening & Cessation Intervention Domain: Preventive Care and Screening ACO 17 PREV- 10 PQRS - 226 NQF 0028 Measure Steward:
ADULT WELLNESS VISIT & WELL WOMAN EXAM
 *This timeframe is the average amount of time most patients spend with the Medical Assistant and Provider, complete any ordered testing in the office (e.g. lab, x-ray, EKG, spirometry, etc.) and check-out
*This timeframe is the average amount of time most patients spend with the Medical Assistant and Provider, complete any ordered testing in the office (e.g. lab, x-ray, EKG, spirometry, etc.) and check-out
MARYWOOD UNIVERSITY PHYSICIAN ASSISTANT PROGRAM HISTORY, PHYSICAL, ASSESSMENT AND PLAN
 MARYWOOD UNIVERSITY PHYSICIAN ASSISTANT PROGRAM HISTORY, PHYSICAL, ASSESSMENT AND PLAN PA: PRECEPTOR: MARYWOOD STAFF: PATIENT ID: AGE: SEX: DATE: Chief Complaint: History of Present Illness: 1 Medications:
MARYWOOD UNIVERSITY PHYSICIAN ASSISTANT PROGRAM HISTORY, PHYSICAL, ASSESSMENT AND PLAN PA: PRECEPTOR: MARYWOOD STAFF: PATIENT ID: AGE: SEX: DATE: Chief Complaint: History of Present Illness: 1 Medications:
Physician s Compliance Guide
 Physician s Compliance Guide Updates to this guide will be posted on the Optum website and can be found at: http://www.optumcoding.com/product/updates/2013pcg/pcg13 Please use the following password to
Physician s Compliance Guide Updates to this guide will be posted on the Optum website and can be found at: http://www.optumcoding.com/product/updates/2013pcg/pcg13 Please use the following password to
CODING REVIEW FOR ACCESS2MD PROVIDERS
 CODING REVIEW FOR ACCESS2MD PROVIDERS May 27, 2015 Tricia Stanley, DNP, RN, ANP-BC, FNP-BC TYPES OF CODES CPT What was done during the visit Two Types CPT Evaluation and Management ICD Why it was done
CODING REVIEW FOR ACCESS2MD PROVIDERS May 27, 2015 Tricia Stanley, DNP, RN, ANP-BC, FNP-BC TYPES OF CODES CPT What was done during the visit Two Types CPT Evaluation and Management ICD Why it was done
Cancer Rehabilitation New Patient Intake Form
 _ I. Personal Information Date of Birth Age: Home Address: Home Phone: Cell Phone: Office Phone: Fax: E-Mail: II. Chief Complaint Please describe the major problem that brings you in today: Who referred
_ I. Personal Information Date of Birth Age: Home Address: Home Phone: Cell Phone: Office Phone: Fax: E-Mail: II. Chief Complaint Please describe the major problem that brings you in today: Who referred
Inspire Medical Systems. Hospital Billing Guide
 Inspire Medical Systems Hospital Billing Guide Inspire Medical Systems Hospital Billing Guide This Hospital Billing Guide was developed to help centers correctly bill for Inspire Upper Airway Stimulation
Inspire Medical Systems Hospital Billing Guide Inspire Medical Systems Hospital Billing Guide This Hospital Billing Guide was developed to help centers correctly bill for Inspire Upper Airway Stimulation
Documentation Guidelines for Evaluation and Management Services
 Documentation Guidelines for Evaluation and Management Services American College of Emergency Physicians November 5, 1997 1 HCFA ANNOUNCES SIX MONTH EXTENSION OF GRACE PERIOD ON DOCUMENTATION GUIDELINES
Documentation Guidelines for Evaluation and Management Services American College of Emergency Physicians November 5, 1997 1 HCFA ANNOUNCES SIX MONTH EXTENSION OF GRACE PERIOD ON DOCUMENTATION GUIDELINES
UF NEUROLOGY HISTORY AND PHYSICAL GUIDELINES
 UF NEUROLOGY HISTORY AND PHYSICAL GUIDELINES HISTORY Chief Complaint A maximally succinct statement of the patient age, handedness, gender, main problem, and its duration (e.g. 56 year old right-handed
UF NEUROLOGY HISTORY AND PHYSICAL GUIDELINES HISTORY Chief Complaint A maximally succinct statement of the patient age, handedness, gender, main problem, and its duration (e.g. 56 year old right-handed
A Guide to Billing Mammograms, PAP Tests, Pelvic Exams and Colon Cancer Screenings. Medicare Preventive Services: Women s Health
 A Guide to Billing Mammograms, PAP Tests, Pelvic Exams and Colon Cancer Screenings Medicare Preventive Services: Women s Health For additional free Medicare education and training opportunities, including
A Guide to Billing Mammograms, PAP Tests, Pelvic Exams and Colon Cancer Screenings Medicare Preventive Services: Women s Health For additional free Medicare education and training opportunities, including
Please print clearly; illegible forms will delay your receiving credit/verification: City State ZIP. Yes No
 PARTICIPANT INFORMATION Please print clearly; illegible forms will delay your receiving credit/verification: First Name MI Last Name Address 1 Address 2 City State ZIP Country Daytime Telephone Fax E-mail
PARTICIPANT INFORMATION Please print clearly; illegible forms will delay your receiving credit/verification: First Name MI Last Name Address 1 Address 2 City State ZIP Country Daytime Telephone Fax E-mail
Med 536 Communicating About Prognosis Workshop. Case 1
 Med 536 Communicating About Prognosis Workshop Case 1 ID / CC: 39 year-old woman status-post motor-vehicle collision History of the Presenting Illness Previously healthy 39 year-old woman was found in
Med 536 Communicating About Prognosis Workshop Case 1 ID / CC: 39 year-old woman status-post motor-vehicle collision History of the Presenting Illness Previously healthy 39 year-old woman was found in
CPT Code Changes for 2013 Frequently Asked Questions Last Updated 12/2/2012
 1. Why are CPT codes changing? CPT Code Changes for 2013 Frequently Asked Questions Last Updated 12/2/2012 CPT code changes occur every year. The Current Procedural Terminology, or CPT, code set is maintained
1. Why are CPT codes changing? CPT Code Changes for 2013 Frequently Asked Questions Last Updated 12/2/2012 CPT code changes occur every year. The Current Procedural Terminology, or CPT, code set is maintained
History. History and Physical Exam of the Pediatric Patient. History of Present Illness. Chief Complaint. Past Medical History. Past Medical History
 History History and Physical Exam of the Pediatric Patient Colleen A. Kraft, M.D., FAAP Richmond Pediatric Associates, Inc. Source Who is giving the history? Is this the patient s primary caretaker? 1
History History and Physical Exam of the Pediatric Patient Colleen A. Kraft, M.D., FAAP Richmond Pediatric Associates, Inc. Source Who is giving the history? Is this the patient s primary caretaker? 1
Evaluation and Management Services
 DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Medicare & Medicaid Services Open a Text-Only Version Evaluation and Management Services ICN 006764 August 2017 A review of this product in August 2017
DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Medicare & Medicaid Services Open a Text-Only Version Evaluation and Management Services ICN 006764 August 2017 A review of this product in August 2017