Palliative Care Workforce Service Review
|
|
|
- Brittany Benson
- 5 years ago
- Views:
Transcription
1 Palliative Care Workforce Service Review Page 1 of 36
2 Table of Contents Page Executive Summary 3 Recommendations 5 1. Introduction 6 2. Population trends and Palliative Care needs 6 3. Palliative Care Services in New Zealand Palliative Care Workforce Vision and Model for Palliative Care Vision Managed Clinical Networks Palliative Care Managed Care Clinical Networks: Regions Network Structure and Organisation Integrated Model of Palliative Care for Networks Pilot Palliative Care Managed Clinical Network Education/Training Board Summary of Key Points Recommendations 29 Appendix 1: Review Members 31 Appendix 2: Definition of Palliative Care 32 Appendix 3: Definition of Palliative Care Workforce 33 Appendix 4: Role Delineation Model 34 Page 2 of 36
3 Executive Summary Palliative care in New Zealand is provided in a variety of settings including community, hospitals, residential care and hospices. The majority of people with cancer will require palliative care but an increasing number of people with chronic diseases also require and benefit from palliative care and often require it for a longer duration than people with cancer. Specialist palliative care services are essential in providing expert clinical care and advice for people with complex symptoms requiring palliation. Non-specialist services particularly primary care; community health nursing and residential care are also essential in the provision of palliative care. The aim of the Palliative Care Workforce Service Review was to develop a vision and model of palliative care service and workforce for 2020 in a context of increasing demand and limited funding. The review was informed by literature; palliative care service and workforce data; population and forecasting data; patient experience in palliative care and also innovations that are occurring in palliative care services in New Zealand. The review identified the following: Palliative Care Need The demand for palliative care services, and thus workforce, will increase slowly over the next ten years but thereafter will increase more rapidly in line with the ageing population The bulk of the aging population will be European The number of deaths and palliative patients will nearly double by 2061 The number of people requiring palliative care will increase by nearly 25% over the next 15 years and will be just over double that by Palliative Care Services There are gaps in palliative care service provision particularly in 24 hour care in the home, bereavement counselling, community and primary care and rural palliative care There are a variety of palliative care models utilised by services and differing levels of regional governance Page 3 of 36
4 Palliative Care Workforce and Training There is a large variation in workforce numbers amongst regions. The number of FTEs (medical and nursing) per 1,000 patients varies between 20.7 per 1,000 patients (Upper South Island) to 42.2 per 1,000 (Central region) with the average being 27.9 per 1,000 patients There are a number of palliative care workforce issues that need to be addressed including an aging workforce; recruitment and retention of palliative care medicine specialists; a shortage of general practitioners with an interest in palliative care; a shortage of nurses with specialist palliative care skills; confusion over advanced nursing practice in specialist palliative care across clinical settings; and a need to define and develop the role of allied health professionals within the multidisciplinary team There is a need to develop and rationalise training for both palliative care specialist and non-specialist health professionals. Vision and Model The review identified that the next ten years will provide time to plan for palliative care services and workforce to ensure the vision from this review is achieved. This vision is to ensure that all people receive effective palliative care from a qualified and competent interdisciplinary team. The vision would be achieved through developing a set of eight regional palliative care managed clinical networks that would link locally, regionally and nationally that are mandated by the Ministry and DHBs. These regional networks would use an integrated model of palliative care that enables most people with palliative care needs to be cared for in the community by primary care and district nursing professionals but have access to effective specialist palliative care services for those that require them. Each network would have a governance and clinical team that would be selected from providers within the region to manage the network and would include a DHB representative. The funding of leadership positions including the director of palliative care and primary care lead and administration of the network would be essential for the success of the network. It is expected that the regional palliative care networks would lead to more effective and efficient palliative care services. This would be enabled through regional planning, development and management of palliative care services and workforce. More importantly, it would enable networks to ensure that all people within the network would receive effective palliative care services in a timely manner no matter where they live. Page 4 of 36
5 In developing the networks it would be essential to develop and fund the primary care sector over and above their core funding as the demand for community palliative care will be substantial in the future years. A demonstration pilot that is evaluated through action research could inform the development of the other seven palliative care managed clinical networks. It would be important to ensure that this pilot is set up in a region where there is support from a palliative care clinical champion. MidCentral, Lower South island and Counties Manukau were suggested as regions for the pilot (s). A useful complement to the palliative care regional networks would be the development of an Interdisciplinary Education/Training Board that links with Health Workforce New Zealand (HWNZ) whose task would be to prioritise and progress palliative care education and training needs. Recommendations 1. That HWNZ funds a demonstration pilot managed clinical network in palliative care that is evaluated through action research to inform the development of palliative care managed clinical networks nationwide. This pilot should include funding for the director of palliative care, primary care lead and administration. 2. That the demonstration pilot is piloted in regions order of priority: MidCentral, Lower South Island and Counties Manukau. 3. That the palliative care managed clinical network develops a funding model for primary care services to provide community palliative care. 4. That HWNZ requests that the Ministry s Cancer Programme Team consider the development of eight managed clinical networks that are linked nationally to manage palliative care in New Zealand as part of their work on palliative care models of service delivery. 5. That HWNZ work with the Ministry s nursing team to undertake a national project outlining the service definition and utilisation of advanced nursing roles (nurse practitioner and clinical nurse specialist) within palliative care including the development of accredited training programmes within palliative care managed clinical network regions. 6. That HWNZ requests the Ministry cancer team to develop the role of allied health professionals within the multidisciplinary team within their national work programme on models of palliative care, the role delineation model and the specialist palliative care service provisions. 7. That HWNZ sets up an Interdisciplinary Education/Training Board that links with HWNZ to prioritise and progress the palliative care workforce requirements. Page 5 of 36
6 1. Introduction The aim of the Palliative Care Workforce Service Review was to develop: A vision of the palliative care service and workforce for 2020 A model of care for the palliative care workforce that is patientcentred, team based and builds in primary care where appropriate. The review was to be done in the context of increasing demand for palliative care services and limited funding. A review team was put together for the review (Appendix 1) that was to be completed within a sixteen-week period. The review was finished in February 2011 and was informed by literature; palliative care service and workforce data 1, population and forecasting data 2, patient experience in palliative care, and also innovations that are occurring in palliative care services in New Zealand. 2. Population Trends and Palliative Care Need This section provides the context for considering future palliative care need and thus services and workforce. The graphs and tables are taken from the forecasting and modelling work done by HWNZ that accompanies this report 3. Aging population Figure 1 shows that there is a steady increase in the elderly population between 2011 and 2061 but that the increase is much more rapid after Table one shows that the number of people aged 65+ years is projected to increase by approximately 2.6 times over the next five decades to reach just over 1.4 million in 2061 (an increase of 885,000 or 160%). Figure 2 (p.8) highlights that the bulk of the aging population in 2026 will be European. 1 Ministry of Health, Gap Analysis of Specialist Palliative Care in New Zealand, Providing a national overview of hospice and hospital-based services, Ministry of Health, Health Workforce New Zealand, New Zealand Palliative Care Demand and Workforce Projections , Ministry of Health, 2011, Unpublished report. 3 Ibid Page 6 of 36
 4,316,000 553,000 28,900 36.5 13% 6.7 2011 4,425,000 586,000 30,000 36.8 13% 6.8 2021 4,818,000 812,000 34,800 38.1 17% 7.")
7 Figure 1: Projected Population Aged 65+, Table 1: Projected Total Population, Aged 65+, Deaths and Characteristics, 2009(Base)-2061 Year Total Population Population Age 65+ Deaths Median Age* Proportion of population Aged 65+ Deaths per 1000 population 2009 (base) 4,316, ,000 28, % ,425, ,000 30, % ,818, ,000 34, % ,149,000 1,072,000 41, % ,402,000 1,232,000 49, % ,597,000 1,312,000 55, % ,755,000 1,438,000 57, % 10.0 Change Number increase 1,439, ,000 28, Percentage growth 33% 160% 100% 19% - - Average annual growth 0.55% 1.85% 1.34% 0.34% - - * Median age that divides the population, with half being older and the other half younger than this age. Page 7 of 36
.")
.")
8 Figure 2: Ethnic Population Age Pyramids, 2006 and 2026 Deaths The number of deaths provides the context for considering palliative care need/demand. Figure 3 shows that 71% of deaths occurred to people aged 70 and over and nearly half of the deaths are in the age group (49%). Figure 4 shows that as with the aging population, the number of deaths increases steadily between 2010 to 2025 but thereafter increases rapidly until 2045 and then start to slow down. This is mainly due to the effect of aging baby boomers (those born during ). Figure 3: Proportion of Deaths by Age, June % 0 1% % % 40s 50s % % % 60s % 80s % 70s % Page 8 of 36
9 Figure 4: Projected Annual Deaths and Change, Deaths 60,000 Change Deaths Annual Change 1,800 50,000 1,500 40,000 1,200 30, , , Palliative Care Need/Demand The number of potential palliative care patients is based on the workforce model developed by HWNZ (figure 5). This model is based on evidence 4, expert opinion and tested against current numbers of palliative patients in New Zealand. This was also discussed with the New Zealand Palliative Care Council who is doing work on palliative care need 5. The model assumes that 90% of people with cancer and 40% of people with chronic disease would require some level of palliative care: Figure 6 (p. 11) shows that from just over half (55%) of the people that died would have required prior palliative care. It also shows that the number of deaths is projected to increase by 96% during and a similar increase in palliative care patients Figure 7 shows that from 2010 to 2026 there is approximately a 24% increase in palliative care patients Figure 8 illustrates the regional variation in the numbers of palliative 4 Rosenwax R, McNamara, Blackmore A, Holman C, Estimating the size of a potential palliative care population, The University of Western Australia; Palliative Medicine 2005, 19: It is acknowledge that when the Palliative Care Council s final report on the needs analysis is completed it will continue to inform the development of palliative care services and its workforce into the future along with the HWNZ Workforce Demand and Projections report. Page 9 of 36
10 care patients, which is mainly due to different population size and age structure within these regions. Figure 5: Model for Estimating Palliative Care Patients Cancer deaths 30% 90% Projected Deaths Non-cancer deaths 70% 40% Projected palliative care patients Figure 6: Projected Deaths and Palliative Care Patients, Deaths ,500 57,700 Palliative Care Patients ` 16,225 31, ,000 20,000 30,000 40,000 50,000 60,000 70,000 Figure 7: Projected Deaths and Palliative Care Patients Deaths ,295 36,381 Palliative Care Patients ,112 20, ,000 10,000 15,000 20,000 25,000 30,000 35,000 40,000 Page 10 of 36
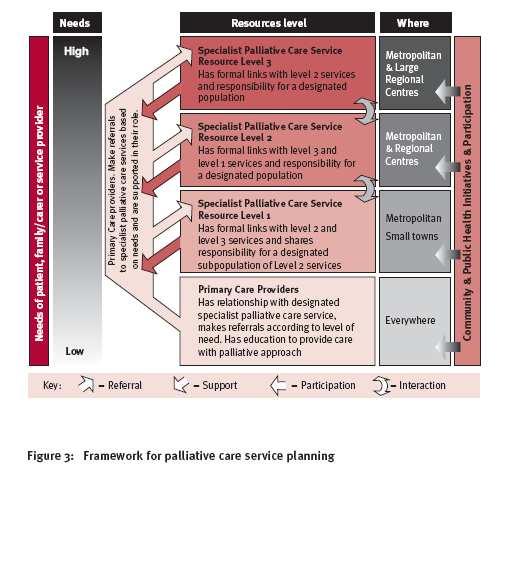
11 Figure 8: Projected Palliative Care Patients by Region Northland & Waitemata 2. Auckland 3. Counties Manukau 4. Waikato & Bay of Plenty 5. Mid-Central 6. Central 7. Upper South Island 8. Lower South Island ,000 1,500 2,000 2,500 3,000 3,500 4,000 Note: the regions in figure 8 are those based on the regions proposed for the palliative care managed clinical networks outlined in section Palliative Care Services in New Zealand Palliative care in New Zealand is provided in a variety of settings including community, hospitals, residential care and hospices (see appendix 2 for a definition of palliative care). The majority of people with cancer will require palliative care but an increasing number of people with chronic diseases also require and benefit from palliative care and often require it for a longer duration than people with cancer 67. Specialist palliative care services are essential in providing expert clinical care and advice for people with complex symptoms requiring palliation. Non-specialist services particularly primary care, community health nursing and residential care is also essential in the provision of palliative care (see appendix 3 for more information on specialist and non-specialist palliative care providers). The provision of palliative care can make a huge difference to the quality of life of people that are at the end of their life. The three patient scenarios below highlight this. 6 Ministry of Health, The New Zealand Palliative Care Strategy, Ministry of Health, Commonwealth of Australia, Supporting Australians to Live Well at the End of Life, Commonwealth of Australia Page 11 of 36
12 Scenario 1 Aroha is 64 years of age and lives in rural NZ close to her ancestral roots. Aroha has: No GP No partner as he left her last year Two children living in Australia. Aroha has been diagnosed with metastatic colon cancer and has 3 months to live. Her symptoms of pain, nausea, weight loss and fear are overwhelming her life at present and she has no desire to go to the regional hospital or hospice which are both 2 hours drive from home. A neighbour is her main support who visits daily and offers meals. Aroha has become more withdrawn in the past 3 weeks. Aroha could benefit from palliative care. She does not need to go to the hospice or hospital for palliative care she could receive palliative care in her home, which would significantly improve her quality of life. If Aroha had care from a primary care team (possibly an Iwi provider) that is linked to a specialist palliative care service (mainly a hospice) the team could assess her palliative care needs in her home and gain specialist advice when it is needed. Specialist advice is likely to be that some simple medication could offer her control of her symptoms and enable her to be more comfortable at the end of her life. Scenario 2 Jim is 72 years of age, a previous heavy smoker with chronic obstructive airways disease who is on home oxygen. Jim lives in the city centre with his wife Mary who suffers from rheumatoid arthritis. They have been married for 52 years and have no children. They receive home help that has recently been cut to 1.5 hours per week. During the past year Jim has had 13 admissions to the emergency department some of which have resulted in 7-10 day ward admissions for broncho-pulmonary infections. During these admissions the panic that accompanies Jim s respiratory distress has often been noted. Although Jim has been in hospital a number of times he has not been referred to palliative care services. When Jim has difficulties he has no option but to go the emergency department for help. However, the hospital does not have a palliative care team and has a poor awareness of the palliative care needs for people with chronic disease. The coordination between hospital, hospice and residential care is very poor. The burden of palliative care lies with the general practitioner who has tried unsuccessfully to refer Jim to palliative care services. Jim could benefit from palliative care. Patients like Jim experience a rapid improvement in quality of life, thus reducing the need to go to the emergency department in times of distress. Palliative care could result in Jim spending more time in his chosen place of care with greater comfort and a more cohesive team of health professionals caring for him. Page 12 of 36
13 Scenario 3: Letter from a family whose mum received palliative care I cannot thank you enough for the care and attention that mum received during the time that she was being cared for by the hospice. She loved you all and especially Vicky who was her assigned palliative care nurse. We, as a family, have reflected on the elements of care, which has led this sad time to actually be healing and indeed at times happy! I well remember the shock and indeed anger when our surgeon said there was nothing else to be done for mum but the palliative care nurse at the hospital was able to give us some hope and encouraged mum to go to the hospice for a few days. Well the team was brilliant and could not be faulted. Mum was a new woman in just 2 days and was able to come back home with dad. She did so want to be back in her home and see the paddocks from the bed in the lounge. At home, the district nurses where great and nothing was too much trouble. Vicky was always there to make sure mum s care and medication were sorted. I didn t think we would see Dr. Evans again because he is so busy but when mum needed him he came straight away. It seemed that everyone knew what was happening to mum, even the pharmacist who delivered mum s medication to her house. Mum was clear she wanted to die at home but did worry about the process of dying as we all did. Dad did not want to speak about it and thought that we should just send Mum to hospital if there was a crisis. Vicky came to the rescue again and gave us all reassurance about what happens when someone is dying. Mum died at home surrounded by love and was free of pain. Please thanks Vicky for calling in after the funeral, I think we will be OK but we will come back to the memorial service at hospice when we are ready. Please accept this small donation for Hospice and once again our thanks to you all for supporting us through this time with such love and care, yours sincerely, Claire. Palliative Care Service Issues The above scenarios highlight how people could and can benefit from palliative care. However, they also highlight that palliative care may not be available even though a person may need it. The Ministry of Health and the Palliative Care Workforce Review Team have identified a number of service and workforce issues that need to be addressed in developing a model of palliative care to ensure its availability to all who need it 89. The palliative care service issues are outlined below (see section 4 for workforce issues). 8 Ministry of Health, Gap Analysis of Specialist Palliative Care in New Zealand, Providing a national overview of hospice and hospital-based services, Ministry of Health Palliative Care Workforce Service Review Team Page 13 of 36
14 There are major gaps in palliative care service provision There is an increasing demand for palliative care services There is a lack of 24 hour palliative care in the home that results in unnecessary hospital admissions There are increasing referrals and increasing demand for hospital palliative care services due to an under-resourced community palliative care service There are limited palliative care services in many rural areas Apart from a few places in New Zealand (e.g. MidCentral DHB), palliative care provided by primary care professionals is not funded (over their core funding) and therefore not consistently available or accessible There are major gaps in bereavement support There are different models of palliative care There is limited regional governance of palliative care services 4. Palliative Care Workforce This section provides information on the current and projected palliative care workforce, and workforce and training issues. Table 2 below provides the numbers of medical, nursing and allied health staff in the palliative care professional workforce based on a survey by the Ministry of Health in It is important to note that this survey also identified that there were a number of gaps in the workforce that were not quantified in the report. 10 Ministry of Health, Gap Analysis of Specialist Palliative Care in New Zealand, Providing a national overview of hospice and hospital-based services, Ministry of Health, Page 14 of 36
15 Table 2: Palliative Care Workforce by Occupation, 2007/2008 financial year Hospice Hospital Hospice+Hospital Occupation Head Head Head FTEs Counts FTEs Counts FTEs Counts Medical Specialist MOSS Registrar GP with special interest Other medical Total Medical Nurses Nurse Practitioner Clinical Nurse Specialist Registered Nurse Enrolled & Other Nurse Total Nurses Allied Health Physiotherapist Social Worker Pharmacist Occupational Therapy Dietician Other Allied Health Total Allied Total PC Workforce FTEs: Full-Time Equivalent employees. Source: Gap Analysis Survey, year ended June 2008 Figure 9 (p.16) shows that at the time of the Ministry of Health survey 11, nurses formed the highest proportion of palliative care staff (376, 81%). Table 3 illustrates the large variation in workforce numbers between regions 12. The number of FTEs per 1000 patients varies between 20.7 per 1,000 (Upper South Island) to 42.2 per 1,000 (Central Region) with the average being 27.9 per 1, Ibid 12 Note that the regions referred to are those outlined in Section 5 as part of the review team s proposed regional palliative care managed clinical networks. Page 15 of 36
16 Figure 9: Palliative Care Workforce by Occupation (FTEs & % share) Medical, 60, 13% Allied Health, 30, 6% Nurses, 376, 81% Table 3: Workforce and Patients Ratios, 2008 (Medical and Nursing FTEs per 1000 Patients) PC Networks Patients (1) Medical FTEs Medical FTEs per 1000 Patients Nursing FTEs Nursing FTEs per 1000 Patients Total FTEs per 1000 Patients 1. Northland & Waitemata 2, Auckland 1, Counties Manukau 1, Waikato & Bay of Plenty 2, Mid-Central 2, Central 1, Upper South Island 2, Lower South Island 1, New Zealand 15, (1) Patient numbers are estimated from death numbers, assuming 30% being cancer and 70% non-cancer deaths; and 90% of cancer and 40% of non-cancer deaths required some prior palliative care. Page 16 of 36
17 Figure 10 illustrates the model for projecting the palliative care workforce 13. Figure 11 shows the projected increase to This is based on the 2008 workforce data, projected deaths and palliative care patients. 14 There is an additional 105 FTEs needed by 2026 with 94 (86%) of those being in nursing. This does not include the number of allied health professionals. Figure 10: Model for Projecting Palliative Care Workforce Projected palliative care patients Medical FTEs/Patients ratios Projected Medical FTEs X & = & Nursing FTEs/Patients ratios Projected Nursing FTEs Figure 11: Projected Palliative Care Workforce Increase FTEs Medical Nurse Total Medical Nurse Total Medical Nurse Total Hospice Hospital Hospice & Hospital Palliative Care Workforce and Training Issues 13 Health Workforce New Zealand, New Zealand Palliative Care Demand and Workforce Projections , Ministry of Health, 2011, Unpublished report. 14 Ministry of Health, Gap Analysis of Specialist Palliative Care in New Zealand. Providing a national overview of hospice and hospital-based services, Ministry of Health, Page 17 of 36
18 The Ministry of Health survey identified a number of workforce and training issues in their review 15. The review team identified some further issues and both are outlined in the boxes below. Palliative Care Workforce There is an urgent need for palliative care workforce development The palliative care workforce is aging There is a shortage of trained palliative care staff in rural areas There is a variation in qualifications of staff employed in palliative care There is a lack of cultural diversity in the palliative care workforce Volunteers are sometimes needed to fill gaps in the professional workforce Professional isolation and maintenance of clinical competency is an issue Nurses There is a shortage of nurses with specialist palliative care skills - pay parity with hospitals is an issue for some hospices There is confusion in the sector about the roles and functions of advanced nursing roles within palliative care such as clinical nurse specialists and nurse practitioners There is a major workload in palliative care for community/district nurses/aged residential nurses and care assistants and the model of care between district nursing and hospice nursing is not consistent throughout the country Doctors The recruitment and retention of palliative care medicine specialists in urban and provincial areas is a major issue There is a shortage of GPs with an interest in training in palliative care There are only a few GP champions for palliative care 15 Ministry of Health, Gap Analysis of Specialist Palliative Care in New Zealand, Providing a national overview of hospice and hospital-based services, Ministry of Health 2009 Page 18 of 36
19 Allied Health Hospices vary in the employment of allied health staff (e.g. social workers, psychotherapists, physiotherapists and pharmacists not all hospices employ these staff who are mainly based in a DHB allied health pool and not always available for palliative care Allied health professionals are commonly part of the palliative care multidisciplinary team in other countries (e.g. United Kingdom) but are not always in New Zealand16 The role of allied health professionals within the multidisciplinary team needs to be defined and developed for New Zealand. Palliative Care Training There is a need to develop and rationalise palliative care education/training Undergraduate programmes currently do not have sufficient palliative care content which is essential to ensure that all health professionals achieve the skills and knowledge to deliver a palliative care approach to care There are not enough doctors training to become palliative care medicine specialists The education/training pathway for nurses to develop the skills required to work in specialist palliative care and practice roles is unclear Allied health professionals currently do not have access to funded training places in palliative care There is an insufficient focus on training programmes for non-specialist palliative care staff GPs do not have access to funded diploma training places in palliative care, and yet are required to provide palliative care in the community Over a third of people die in rest homes yet health assistants do not have access to funded palliative care certificate places The nursing workforce in residential care is not supported to develop their skills in palliative care. 16 Greensmith C, Allied health professionals in palliative care, Unpublished paper prepared for the Palliative care workforce service review, November 2010 Page 19 of 36
20 Implications of Workforce Data In developing palliative care services and workforce to meet future need, it is important to take into consideration the current workforce gaps; the increase in workforce that will be required to meet future demand; and the above workforce and training issues. 5. Vision and Model for Palliative Care The review team took the following into consideration in the development of the vision and model of palliative care: Aging population and increasing numbers of people that will require palliative care Current palliative care services Current workforce and training issues Increase required in the palliative care workforce The effective use of palliative care services and workforce. The challenge for the review team was to: 1. Develop a vision and model of how palliative care services could be provided more efficiently and effectively 2. Identify how specialist and non-specialist palliative care workforce could be better and more innovatively deployed within palliative care 3. Develop a method of prioritising palliative care training needs. 5.1 Vision The vision for palliative care service and workforce is: The consumer will receive effective palliative care from a qualified and competent interdisciplinary team This vision for palliative care services will be realized through the development of eight regional palliative care managed clinical networks that will link locally, regionally and nationally Page 20 of 36
21 5.2 Managed Clinical Networks The review team identified that the answer to meeting the palliative care needs of New Zealand was through regional managed clinical networks (MCNs). This would enable networks to plan and deliver services based on their region s needs as well as link nationally to create a leadership infrastructure. The review team s decision was informed by the literature and experience of managed clinical networks Managed clinical networks are intended to be patient centred and have been defined as...linked groups of health professionals and organisations from primary, secondary and tertiary care working in a coordinated manner, unconstrained by existing professional and organisational boundaries to ensure equitable provision of high quality effective (national) health services MCNs have been developed for a wide range of conditions including neurology, vascular services, coronary heart disease, stroke, diabetes, palliative care, epilepsy, multiple sclerosis, and cleft lip and palate. MCNs can also be developed in relation to service functions e.g. (emergency, pathology, critical care) 22. It is suggested that MCNs stimulate creativity and innovation by creating an environment where multidisciplinary teams, consumers and organisations come together to plan for the network. This includes the ability of the Network to be more dynamic and flexible in responding to the needs of clients and changing the way that services are delivered to meet these needs. MCNs can also address their workforce issues by making better use of scarce specialist expertise, utilising staff more efficiently, developing more innovative roles and ways of work thus preventing duplication of effort and resources. The type of Network and the geographical range of the Network need to be developed based on the best interests of patients 23. MCNs are currently part of government policy and require a mandate from the government and DHBs to operate. They can be formed locally (DHB), 17 McKinlay E, McBain L, Evaluation of the Palliative Care Partnership: a New Zealand solution to the provision of integrated palliative care, NZMJ, 12 October Australian Government Cancer Australia, CanNET Information Bulletin No 1. The managed clinical networks model February Palliative Care Australia, A Guide to Palliative Care Service Development, May Scottish Executive Health Department NHS Circular: HDL (2002) Lambie L. Managed Clinical Networks: Unpublished paper prepared for the review team. Ministry of Health unpublished, October Ibid 23 Scottish Executive Health Department NHS Circular: HDL (2002) 69. Page 21 of 36
22 regionally, or nationally Palliative Care Managed Care Clinical Networks: Regions The map on the next page (figure 12) illustrates where the eight palliative care managed clinical networks would be situated. The regions were chosen based on demographics, geography, DHB boundaries (see table 4), existing provider relationships and size (around 400,000 a level for effective workforce and service management). Figure 13 below shows the size of the population of each of the networks. The average population size is 546,000, with the Lower South Island being the smallest network (300,346) and the Upper South Island being the largest (734, 426). Interestingly the Upper South Island is also the network with the least FTEs per 1,000 patients (20.7 per 1,000 patients) (see table 3, p.17). Figure 12: Palliative Care Regions 24 HR : Government Policy on the development of clinical networks. Page 22 of 36
23 Table 4: DHBs within Regional Palliative Care Networks Palliative Care Managed Clinical Networks 1. Northland & Waitemata Northland DHB Constituent District Health Boards Waitamata DHB 2. Auckland Auckland DHB 3. Counties Manukau Counties Manukau DHB 4. Waikato & Bay of Plenty Waikato DHB Lakes DHB Bay of Plenty DHB 5. Mid-Central Tairawhiti DHB Taranaki DHB Hawke's Bay DHB Whanganui DHB MidCentral DHB 6. Central Hutt Valley DHB Capital & Coast DHB Wairarapa DHB 7. Upper South Island Nelson Marlborough DHB West Coast DHB Canterbury DHB South Canterbury DHB 8. Lower South Island Southern DHB Figure 13: Population by Palliative Care Network Region, (people and % share) 2010 Upper South Is., 734,426, 17% Lower South Is., 300,346, 7% Northland & Waitemata, 697,240, 16% Auckland, 451,821, 10% Central, 473,942, 11% M id-central, 541,322, 12% Waikato & Bay of Plenty, 677,887, 16% Counties M anukau, 493,203, 11% Page 23 of 36
24 5.2.2 Network Structure and Organisation A governance team and a clinical management team will manage the networks. Their functions are outlined in the boxes below. Governance Team The Governance Team will provide the overall leadership for the network and link with other palliative care networks regionally and nationally. The team will include: Director of palliative care A representative of DHB Funding and Planning Primary care lead Secondary care lead Hospice lead Aged care lead Consumer/community representative There will need to be funding for positions including the director of palliative care, primary care lead and administration of the network. Network leads will be chosen for their leadership skills and experience in the sector. Responsibilities Create the structure and develop the organisation of the network Identify the need/demand for palliative care services within the region. Note that data is available for regions as a basis for undertaking the needs analysis25 Undertake strategic planning for all specialist and non-specialist palliative care services and workforce Develop 24-hour (7 days a week) systems for after hour home support Support a business model to support the relevant palliative care services of the region Manage change e.g. service change Develop and connect IT systems within the networks- locally, regionally and nationally Support the development and funding of research into NZ relevant aspects of palliative care Develop linkages with tertiary education providers 25 Health Workforce New Zealand, New Zealand Palliative Care Demand and Workforce Projections , Ministry of Health, 2011, Unpublished report. Page 24 of 36
25 Clinical Management Team The clinical management team will provide the clinical leadership for the sector. The team is made up of clinical leaders from the various organisations within the network. This is aimed at avoiding duplication of work and efficient use of workforce. The team includes: Director of Palliative Care Palliative care medicine specialist Nurse Practitioner Primary care professional Allied health professional Aged care professional Responsibilities Clinical governance and leadership Quality and service improvement including 24 hour cover Advance care planning Development of the interdisciplinary team including advanced nursing roles and allied health staff11 Workforce innovation and deployment Education/Training Developing and implementing a model of bereavement support Research Development of resources Integrated Model of Palliative Care for Networks Networks will use an integrated model of care for the provision of palliative care (figure 14). This model builds on the role delineation model (see appendix 4). It also builds on the evidence that educated and remunerated primary care teams supported by specialist palliative care can successfully care for the majority of palliative care need in their region. This is a model that the review team believes has potential to be adopted more widely throughout the country Stewart B, Allan S, Keane B, Marshall B, Ayling J, Luxford T, Palliative Care Partnership a successful model of primary/secondary integration, the New Zealand Medical Journal, Vol 119, No 1242, ISSN, McKinlay E, McBain L, Evaluation of the Palliative Care Partnership: A New Zealand solution to the provision of integrated palliative care, The New Zealand Medical Journal, Vol 120, No 1263, ISSN, Page 25 of 36
 palliative care professionals, particularly primary care and district nursing and that some people will require specialist palliative care.")
26 Figure 14: Integrated Model of Palliative Care HPCT = Hospital Palliative Care Team The integrated care model assumes that: Most people with palliative care needs will be cared for in the community by non-specialist (generalist) palliative care professionals, particularly primary care and district nursing and that some people will require specialist palliative care. An Advance Care Pathway for end of life care (e.g. Gold Standards Framework 28 ) that will incorporate a NZ advance care planning tool (under development by the Advance Care Planning Cooperative) will be used in the community which will enable more people to remain in their homes at the end of life Patients who require it will move between non-specialist and specialist palliative care. All non-specialist palliative care staff will have expertise in the palliative care approach and that specialist staff in palliative care settings will have specialist palliative care training/education Community palliative care (including primary care and palliative care in residential care) is a universal right and is available free to palliative care patients There will be a collaborative approach amongst all organisations and professionals Page 26 of 36
27 5.2.4 Pilot Palliative Care Managed Clinical Network The review team recommended that a demonstration pilot that is evaluated through action research should be set up to inform the development of the regional networks. These networks should be set up where there are existing champions. The suggested pilot regions for palliative care managed clinical networks are outlined in the table below in order of priority. Network Characteristics Mid-Central Mixed urban/rural population Inequities of access Sizeable Maori population Two hospices One Hospital Palliative Care Team Lower South Island Large geographical area to service Range of population Cancer network in operation Two hospices One Hospital Palliative Care Team Training university Counties Manukau Predominantly urban Inequities of access Large Maori and Pacific population Two hospices One Hospital Palliative Care Team 6. Education/Training Board With the large number of palliative care education/training issues that need to be addressed the review team developed the idea of having a Palliative Care Interdisciplinary Education/Training Board that would complement the regional palliative care managed clinical networks. The review team s vision is that this training board would be linked with HWNZ and would be tasked with prioritizing and progressing the palliative care workforce s training needs. The box below identifies the immediate priorities that would be addressed by such a training board. Page 27 of 36
28 Priorities of the Palliative Care Interdisciplinary Education/Training Board 1. C oordinate a review the palliative care content in all undergraduate and post-graduate health education programmes 2. R eview the education/training of the interdisciplinary team 3. A ssist in the development of accredited training sites for nurses to develop advance palliative care nursing skills 4. E nsure access to a variety of training/upskilling programmes in palliative care for non-specialist (generalist) palliative care staff including e-learning programmes 5. I ntroduce funded places for general practitioners to complete the Clinical Diploma in Palliative Medicine developed by the Royal Australasian College of Physicians (RACP) 6. I ncrease the capacity of palliative care specialist medical training within New Zealand 7. R eview the ARRMOS (Auckland regional resident medical officers service) model in conjunction with PaMTraCC (Palliative Medicine Training Coordination Committee) within the NZ branch of the Royal Australasian College of Physicians, for wider use within New Zealand 8. A ssist in identifying education and training needs and scope of practice of 7. Summary of key points Key Points 1. The demand for palliative care services, and thus workforce, will increase slowly over the next ten years but thereafter will increase more rapidly in line with the ageing population 2. The next ten years will provide time to plan for palliative care services and workforce to ensure they will meet population need Page 28 of 36
29 3. The development and funding of the primary care sector will be essential to meet the future increasing demand for community palliative care 4. As well as future demand there is a need to address the current gaps in palliative care service provision, workforce and training 5. There is a need to define and develop the roles of nurses and allied health professionals within the multidisciplinary team 6. A set of eight palliative care managed clinical networks could enable services to come together to integrate services and ensure that all people who need palliative care receive it. These networks would use an integrated model of palliative care 7. A demonstration pilot that is evaluated through action research could inform the development of the other palliative care managed clinical networks. Potential places where they are likely to be successful include MidCentral, Lower South Island and Counties Manukau. This pilot will need to include funding for the Director in Palliative Care, the Primary Care Lead and administration 8. An Interdisciplinary Education/Training Board would be a useful structure to prioritise and progress palliative care education and training needs. 8. Recommendations Palliative Care Managed Clinical Networks 1. That HWNZ funds a demonstration pilot managed clinical network in palliative care that is evaluated through action research to inform the development of palliative care managed clinical networks nationwide. This pilot should include funding for the director of palliative care, primary care lead and administration. 2. That the demonstration pilot is piloted in regions order of priority: MidCentral, Lower South Island and Counties Manukau. 3. That the palliative care managed clinical network develops a funding model for primary care services to provide community palliative care. 4. That HWNZ requests that the Ministry s Cancer programme team Page 29 of 36
30 consider the development of eight managed clinical networks that are linked nationally to manage palliative care in New Zealand as part of their work on palliative care models of service delivery. Development of the Multidisciplinary Team 5. That HWNZ work with the Ministry s nursing team to undertake a national project outlining the service definition and utilisation of advanced nursing practice roles (nurse practitioner and clinical nurse specialist) within palliative care including the development of accredited training programmes within palliative care managed clinical network regions. 6. That HWNZ requests the Ministry cancer team to develop the role of allied health professionals within the multidisciplinary team within their national work programme on models of palliative care, the role delineation model and the specialist palliative care service provisions. Interdisciplinary Training/Education Board 7. That HWNZ sets up an Interdisciplinary Education/Training Board that links with HWNZ to prioritise and progress the palliative care workforce requirements. Page 30 of 36
31 Appendix 1: Review members Members of the Review Team Name Simon Allan Profession Director of Palliative Care Senior advisor palliative care, Ministry of Health Chair of the Review Team Jackie Robinson Nurse Practitioner in palliative care Clare Randall Hospice manager/pharmacist Clare Greensmith Patient and family/whānau support services/ Psychotherapist Suzanne Brocx Rod MacLeod Bruce Stewart Deborah Peters Northland palliative care specialist nurse educator/advisor Palliative care medicine specialist and academic General practitioner Consumer Laura Lambie Michael Batson Mike Chan Project manager of the review HWNZ senior policy analyst HWNZ senior analyst Page 31 of 36
32 Appendix 2: Definition of palliative care Palliative care: World Health Organisation Definition (2002) Palliative care is an approach that improves the quality of life of patients and their families facing the problems associated with life-threatening illness, through the prevention and relief of suffering by means of early identification and impeccable assessment and treatment of pain and other problems, physical, psychosocial and spiritual. Palliative care: Provides relief from pain and other distressing symptoms Affirms life and regards dying as a normal process Intends neither to hasten nor postpone death Integrates the psychological and spiritual aspects of patients care Offers a support system to help patients live as actively as possible until death Offers a support system to help the family cope during the patient s illness and in their own bereavement Uses a team approach to address the needs of patients and their families, including bereavement counselling, if indicated Will enhance quality of life, and may also positively influence the course of illness Palliative Care: New Zealand Definition (2007) The New Zealand definition of Palliative Care is: Care for people of all ages with a life-limiting illness which aims to: 1. Optimise an individual s quality of life until death by addressing the person s physical, psychosocial, spiritual and cultural needs. 2. Support the individual s family, whānau, and other caregivers where needed, through the illness and after death. Palliative care is provided according to an individual s need, and may be suitable whether death is days, weeks, months or occasionally even years away. It may be suitable sometimes when treatments are being given aimed at improving quantity of life. It should be available wherever the person may be. It should be provided by all heath care professionals, supported where necessary, by specialist palliative care services. Palliative care should be provided in such a way as to meet the unique needs of individuals from particular communities or groups. These include Maori, children and young people, immigrants, refugees, and those in isolated communities. Page 32 of 36
33 Appendix 3: Definition of palliative care workforce Current palliative care Workforce The current palliative care workforce is divided into two categories: Specialist palliative care health professionals Non-Specialist (Generalist) palliative care health professionals The following description is adapted from a gap analysis of specialist palliative care services undertaken by the Ministry of Health 29. Specialist palliative care workforce Specialist palliative care is palliative care provided by those who have undergone specific training and/or accreditation in palliative care or medicine, and who are working in the context of an expert interdisciplinary team of palliative care health professionals. Specialist palliative care can be provided by hospices (community), hospital-based palliative care services, or paediatric specialist palliative care teams. Specialist palliative care health professionals can include: 1. Palliative care medicine specialists 2. Nurse practitioners 3. Palliative care nurse specialists 4. Registered nurses 5. Social workers 6. Counsellors 7. Grief and loss health professionals 8. Physiotherapists 9. Occupational Therapists 10. Spiritual/Pastoral support Specialist palliative care practice builds on the palliative care provided by generalist providers and reflects a higher level of expertise in complex symptom management, spiritual support, psychosocial support, cultural support, and grief and loss support. Specialist palliative care provision works in two ways. 1. It works directly by providing direct management and support to people, their families and whānau where complex palliative care need exceeds the resources of the generalist provider. The involvement of specialist palliative care with any person and their 29 Ministry of Health, Gap Analysis of Specialist Palliative Care in New Zealand, Providing a national overview of hospice and hospital-based services, Ministry of Health, Page 33 of 36
34 family and whānau can be continuous or episodic depending on their assessed changing need. Complex need in this context is defined as a level of need that exceeds the resources of the generalist team: this may apply in any of the domains of care physical, psychosocial, spiritual or cultural, for example. 2. It works indirectly by providing advice, support, education and training to other health professionals and volunteers to support their generalist provision of palliative care. Non-Specialist (Generalist) palliative care workforce Non-Specialist (Generalist) palliative care is palliative care provided for those affected by life-limiting illness as an integral part of standard clinical practice by any health care professional that is not part of a specialist palliative care team. It is provided in the community by primary care teams (including general practitioners and practice nurses), Māori and Pacific health providers, allied health teams, district nurses, residential care staff, community support services, and community paediatric teams. It is provided in hospitals by general adult and paediatric medical and surgical teams, as well as disease specific teams including oncology, respiratory, renal, intensive care and cardiac teams. Some of these generalist providers, such as general practice teams, will have ongoing contact with a family throughout and following illness. Others, such as district nurses and hospital teams, will have episodic contact, depending on the needs of the person and their family and whānau. Providers of generalist palliative care will have defined links with specialist palliative care team(s) for the purposes of support and advice, or in order to refer people with complex needs. They will also have access to palliative care education and learning to support their practice. Appendix 4: Role Delineation Model References: Palliative Care Australia, Standards for providing quality palliative care for all Australians, May 2005 Palliative Care Australia, A Guide to Palliative Care Service Development, May 2005 This model was used to inform the development of the integrated care model outlined in this report. Page 34 of 36

35 Page 35 of 36

36 Page 36 of 36
New Zealand Palliative Care: A Working Definition.
 New Zealand Palliative Care: A Working Definition. 1. Preamble The NZ Palliative Care Strategy (2001) aims to set in place a systematic and informed approach to the provision and funding of palliative
New Zealand Palliative Care: A Working Definition. 1. Preamble The NZ Palliative Care Strategy (2001) aims to set in place a systematic and informed approach to the provision and funding of palliative
BSA New Zealand Hawkes Bay District Health Board Coverage Report
 BSA New Zealand Hawkes Bay District Health Board Coverage Report For the period ending 31 December 2016 Citation: Ministry of Health. February 2017. BSA New Zealand District Health Board Coverage Report:
BSA New Zealand Hawkes Bay District Health Board Coverage Report For the period ending 31 December 2016 Citation: Ministry of Health. February 2017. BSA New Zealand District Health Board Coverage Report:
Ministry of Health. Refresh of rheumatic fever prevention plans: Guiding information for high incidence District Health Boards June 2015
 Ministry of Health Refresh of rheumatic fever prevention plans: Guiding information for high incidence District Health Boards June 2015 Contents Introduction... 1 Guidance for update of Rheumatic Fever
Ministry of Health Refresh of rheumatic fever prevention plans: Guiding information for high incidence District Health Boards June 2015 Contents Introduction... 1 Guidance for update of Rheumatic Fever
Diabetic Retinal Screening, Grading, Monitoring and Referral Guidance. Objective
 Diabetic Retinal Screening, Grading, Monitoring and Referral Guidance. Objective The Diabetic Retinal Grading, Monitoring and Referral Guidance 2015 updates all previous guidelines And outlines the key
Diabetic Retinal Screening, Grading, Monitoring and Referral Guidance. Objective The Diabetic Retinal Grading, Monitoring and Referral Guidance 2015 updates all previous guidelines And outlines the key
Palliative & End of Life Care Plan
 Palliative & End of Life Care Plan 2018-2023 Contents 1. Palliative Care Definition Page 1 2. Our Vision Page 2 3. Key Aims Page 2 4. Planned Actions Page 3-5 5. Priorities Page 6-7 6. Appendix 1 HSCP
Palliative & End of Life Care Plan 2018-2023 Contents 1. Palliative Care Definition Page 1 2. Our Vision Page 2 3. Key Aims Page 2 4. Planned Actions Page 3-5 5. Priorities Page 6-7 6. Appendix 1 HSCP
Kidney Transplant Activity New Zealand
 Kidney Transplant Activity New Zealand 2016 Calendar Year Author: Nick Cross, Clinical Director Dale Gommans, Analyst National Renal Transplant Service Data Collection Data is provided directly to the
Kidney Transplant Activity New Zealand 2016 Calendar Year Author: Nick Cross, Clinical Director Dale Gommans, Analyst National Renal Transplant Service Data Collection Data is provided directly to the
Kidney Transplant Activity New Zealand
 Kidney Transplant Activity New Zealand 2017 Calendar Year Author: Nick Cross, Clinical Director National Renal Transplant Service Date: 13 March 2018 Data Collection Data is provided directly to the National
Kidney Transplant Activity New Zealand 2017 Calendar Year Author: Nick Cross, Clinical Director National Renal Transplant Service Date: 13 March 2018 Data Collection Data is provided directly to the National
Suicide Facts. Deaths and intentional self-harm hospitalisations
 Suicide Facts Deaths and intentional self-harm hospitalisations 2012 Citation: Ministry of Health. 2015. Suicide Facts: Deaths and intentional self-harm hospitalisations 2012. Wellington: Ministry of Health.
Suicide Facts Deaths and intentional self-harm hospitalisations 2012 Citation: Ministry of Health. 2015. Suicide Facts: Deaths and intentional self-harm hospitalisations 2012. Wellington: Ministry of Health.
Tobacco Trends 2007 A brief update on monitoring indicators
 Tobacco Trends 2007 A brief update on monitoring indicators Citation: Ministry of Health. 2008. Tobacco Trends 2007: A brief update on monitoring indicators. Wellington: Ministry of Health. Published in
Tobacco Trends 2007 A brief update on monitoring indicators Citation: Ministry of Health. 2008. Tobacco Trends 2007: A brief update on monitoring indicators. Wellington: Ministry of Health. Published in
Bay of Plenty Adult Palliative Care Service Plan
 Bay of Plenty Adult Palliative Care Service Plan 2011-2016 Author: Sharon Hardaker, Midland Cancer Network Last Updated: 3 June 2012 Document Name: Bay of Plenty Adult Palliative Care Service Plan Version:
Bay of Plenty Adult Palliative Care Service Plan 2011-2016 Author: Sharon Hardaker, Midland Cancer Network Last Updated: 3 June 2012 Document Name: Bay of Plenty Adult Palliative Care Service Plan Version:
Universal Newborn Hearing Screening and Early Intervention Programme (UNHSEIP) Monitoring Report
 Monitoring Report") Universal ewborn Hearing Screening and Early Intervention Programme (UHSEIP) Monitoring Report January to December 2015 Released 2016 health.govt.nz Copyright The copyright owner of this publication is
Universal ewborn Hearing Screening and Early Intervention Programme (UHSEIP) Monitoring Report January to December 2015 Released 2016 health.govt.nz Copyright The copyright owner of this publication is
Resource and Capability Framework for Integrated Adult Palliative Care Services in New Zealand Consultation document
 Resource and Capability Framework for Integrated Adult Palliative Care Services in New Zealand Consultation document Citation: Ministry of Health. 2012. Resource and Capability Framework for Integrated
Resource and Capability Framework for Integrated Adult Palliative Care Services in New Zealand Consultation document Citation: Ministry of Health. 2012. Resource and Capability Framework for Integrated
Case studies: palliative care in Vital Signs 2014: The State of Safety and Quality in Australian Health Care
 University of Wollongong Research Online Australian Health Services Research Institute Faculty of Business 2014 Case studies: palliative care in Vital Signs 2014: The State of Safety and Quality in Australian
University of Wollongong Research Online Australian Health Services Research Institute Faculty of Business 2014 Case studies: palliative care in Vital Signs 2014: The State of Safety and Quality in Australian
Dr Alasdair Patrick. Dr Nagham Al-Mozany. 9:45-10:10 Where Are We Up To With Bowel Cancer Screening?
 Dr Alasdair Patrick Gastroenterologist and General Physician Middlemore Hospital Auckland Dr Nagham Al-Mozany Colorectal Surgeon Auckland City Hospital Clinical Senior Lecturer University of Auckland 9:45-10:10
Dr Alasdair Patrick Gastroenterologist and General Physician Middlemore Hospital Auckland Dr Nagham Al-Mozany Colorectal Surgeon Auckland City Hospital Clinical Senior Lecturer University of Auckland 9:45-10:10
Palliative care services and home and community care services inquiry
 3 August 20120 Mr Peter Dowling MP Chair, Health and Community Services Committee Parliament House George Street Brisbane QLD 4000 Email: hcsc@parliament.qld.gov.au Dear Mr Dowling, Palliative care services
3 August 20120 Mr Peter Dowling MP Chair, Health and Community Services Committee Parliament House George Street Brisbane QLD 4000 Email: hcsc@parliament.qld.gov.au Dear Mr Dowling, Palliative care services
HERTS VALLEYS CCG PALLIATIVE AND END OF LIFE CARE STRATEGY FOR ADULTS AND CHILDREN
 HERTS VALLEYS CCG PALLIATIVE AND END OF LIFE CARE STRATEGY FOR ADULTS AND CHILDREN 2016-2021 1 1. Introduction Herts Valleys Palliative and End of Life Care Strategy is guided by the End of Life Care Strategic
HERTS VALLEYS CCG PALLIATIVE AND END OF LIFE CARE STRATEGY FOR ADULTS AND CHILDREN 2016-2021 1 1. Introduction Herts Valleys Palliative and End of Life Care Strategy is guided by the End of Life Care Strategic
JOB DESCRIPTION DIRECTOR OF PALLIATIVE CARE
 JOB DESCRIPTION DIRECTOR OF PALLIATIVE CARE Reporting to: The Chief Executive Employment Status: Permanent FTE 1.0 Direct Reports: Hospice Medical Team Education Research Quality Improvement Date Prepared:
JOB DESCRIPTION DIRECTOR OF PALLIATIVE CARE Reporting to: The Chief Executive Employment Status: Permanent FTE 1.0 Direct Reports: Hospice Medical Team Education Research Quality Improvement Date Prepared:
National Cancer Programme. Work Plan 2015/16
 National Cancer Programme Work Plan 2015/16 Citation: Ministry of Health. 2015. National Cancer Programme: Work plan 2015/16. Wellington: Ministry of Health. Published in October 2015 by the Ministry of
National Cancer Programme Work Plan 2015/16 Citation: Ministry of Health. 2015. National Cancer Programme: Work plan 2015/16. Wellington: Ministry of Health. Published in October 2015 by the Ministry of
Ministry of Health and Long-Term Care. Palliative Care. Follow-Up on VFM Section 3.08, 2014 Annual Report RECOMMENDATION STATUS OVERVIEW
 Chapter 1 Section 1.08 Ministry of Health and Long-Term Care Palliative Care Follow-Up on VFM Section 3.08, 2014 Annual Report RECOMMENDATION STATUS OVERVIEW # of Status of Actions Recommended Actions
Chapter 1 Section 1.08 Ministry of Health and Long-Term Care Palliative Care Follow-Up on VFM Section 3.08, 2014 Annual Report RECOMMENDATION STATUS OVERVIEW # of Status of Actions Recommended Actions
Resource and Capability Framework for Integrated Adult Palliative Care Services in New Zealand
 Resource and Capability Framework for Integrated Adult Palliative Care Services in New Zealand Citation: Ministry of Health. 2012. Resource and Capability Framework for Integrated Adult Palliative Care
Resource and Capability Framework for Integrated Adult Palliative Care Services in New Zealand Citation: Ministry of Health. 2012. Resource and Capability Framework for Integrated Adult Palliative Care
Deaths in New Zealand and the Need for Palliative Care
 Clinical Stream Deaths in New Zealand and the Need for Palliative Care Professor Heather McLeod Deaths in New Zealand and the Need for Palliative Care National Rural Health Conference Rotorua, March 2015
Clinical Stream Deaths in New Zealand and the Need for Palliative Care Professor Heather McLeod Deaths in New Zealand and the Need for Palliative Care National Rural Health Conference Rotorua, March 2015
Judy Li Nick Chen The Quit Group
 Redemption of Nicotine Replacement Therapy (NRT) Quit Cards distributed through the Quitline, January June 2007 Judy Li Nick Chen The Quit Group July 2008 1 EXECUTIVE SUMMARY Aims 1. To give an indication
Redemption of Nicotine Replacement Therapy (NRT) Quit Cards distributed through the Quitline, January June 2007 Judy Li Nick Chen The Quit Group July 2008 1 EXECUTIVE SUMMARY Aims 1. To give an indication
Health of Older People Strategy
 Health of Older People Strategy Health Sector Action to 2010 to Support Positive Ageing Draft for Consultation Hon Ruth Dyson Associate Minister of Health and Minister for Disability Issues September 2001
Health of Older People Strategy Health Sector Action to 2010 to Support Positive Ageing Draft for Consultation Hon Ruth Dyson Associate Minister of Health and Minister for Disability Issues September 2001
PERTUSSIS REPORT. November 2013
 PERTUSSIS REPORT Data contained within this monthly report is based on information recorded on EpiSurv by public health service staff as at 12 December 213. Changes made to EpiSurv data after this date
PERTUSSIS REPORT Data contained within this monthly report is based on information recorded on EpiSurv by public health service staff as at 12 December 213. Changes made to EpiSurv data after this date
Laboratory Surveillance of Chlamydia and Gonorrhoea in New Zealand. October to December 2010
 ISSN 1176-7316 Laboratory Surveillance of Chlamydia and Gonorrhoea in New Zealand October to December 2010 Prepared as part of a Ministry of Health contract for scientific services by Health Intelligence
ISSN 1176-7316 Laboratory Surveillance of Chlamydia and Gonorrhoea in New Zealand October to December 2010 Prepared as part of a Ministry of Health contract for scientific services by Health Intelligence
Effectiveness of the Get Checked diabetes programme
 Effectiveness of the Get Checked diabetes programme This is an independent report published under section 21 of the Public Audit Act 2001. September 2010 ISBN 978-0-478-32675-8 (online) 2 Contents Auditor-General
Effectiveness of the Get Checked diabetes programme This is an independent report published under section 21 of the Public Audit Act 2001. September 2010 ISBN 978-0-478-32675-8 (online) 2 Contents Auditor-General
The New Zealand Palliative Care Strategy
 The New Zealand Palliative Care Strategy Discussion Document i Published in July 2000 by the Ministry of Health PO Box 5013, Wellington, New Zealand ISBN 0-478-23961-0 (Booklet) ISBN 0-478-23962-9 (Internet)
The New Zealand Palliative Care Strategy Discussion Document i Published in July 2000 by the Ministry of Health PO Box 5013, Wellington, New Zealand ISBN 0-478-23961-0 (Booklet) ISBN 0-478-23962-9 (Internet)
COVER SHEET. Accessed from Copyright 2003 Australasian Medical Publishing Company
 COVER SHEET Cairns, Will and Yates, Patsy (2003) Education and training in palliative care. Medical Journal of Australia 179:S26-S28. - reproduced with permission. Accessed from http://eprints.qut.edu.au
COVER SHEET Cairns, Will and Yates, Patsy (2003) Education and training in palliative care. Medical Journal of Australia 179:S26-S28. - reproduced with permission. Accessed from http://eprints.qut.edu.au
Tairawhiti Palliative Care Review
 APPENDIX 8 Tairawhiti Palliative Care Review Prepared for the Tairawhiti District Health Board Brenda Hall 29/05/2012 2 All people who are dying and their family/whanau who could benefit from palliative
APPENDIX 8 Tairawhiti Palliative Care Review Prepared for the Tairawhiti District Health Board Brenda Hall 29/05/2012 2 All people who are dying and their family/whanau who could benefit from palliative
National Palliative Care Strategy 2017 Draft 2.1. Draft AUGUST 2017 DRAFT 2.1 PREPARED FOR DEPARTMENT OF HEALTH
 National Palliative Care Strategy 2017 2.1 AUGUST 2017 DRAFT 2.1 PREPARED FOR DEPARTMENT OF HEALTH To receive this document in an accessible format phone 02 8233 9909, using the National Relay Service
National Palliative Care Strategy 2017 2.1 AUGUST 2017 DRAFT 2.1 PREPARED FOR DEPARTMENT OF HEALTH To receive this document in an accessible format phone 02 8233 9909, using the National Relay Service
What is palliative care? What is palliative care? Dr Claire L Hookey
 What is palliative care? What is palliative care? Dr Claire L Hookey Palliative Care an approach that improves the quality of life of patients and their families facing the problems associated with life-threatening
What is palliative care? What is palliative care? Dr Claire L Hookey Palliative Care an approach that improves the quality of life of patients and their families facing the problems associated with life-threatening
Palliative Care Bereavement Support Guidelines. Clinical Psychologist,
 Palliative Care Bereavement Support Guidelines Bridget Marshall CNS, Arohanui Hospice Maria Berrett Clinical Psychologist, Massey Health Psychology Services Outline Background MidCentral Palliative Care
Palliative Care Bereavement Support Guidelines Bridget Marshall CNS, Arohanui Hospice Maria Berrett Clinical Psychologist, Massey Health Psychology Services Outline Background MidCentral Palliative Care
Dialysis and Transplantation Audit
 New Zealand Dialysis and Transplantation Audit and A summary report of activity for New Zealand nephrology services Dr Suetonia Palmer On behalf of the National Renal Advisory Board NRAB Standard and Audits
New Zealand Dialysis and Transplantation Audit and A summary report of activity for New Zealand nephrology services Dr Suetonia Palmer On behalf of the National Renal Advisory Board NRAB Standard and Audits
Dr Chris Jackson. Consultant Medical Oncologist Southern Blood and Cancer Service (SDHB) University of Otago
 University of Otago") Dr Chris Jackson Consultant Medical Oncologist Southern Blood and Cancer Service (SDHB) University of Otago 14:50-15:15 Priorities for Cancer Care in NZ - The Cancer Society's View Priorities for Cancer
Dr Chris Jackson Consultant Medical Oncologist Southern Blood and Cancer Service (SDHB) University of Otago 14:50-15:15 Priorities for Cancer Care in NZ - The Cancer Society's View Priorities for Cancer
Palliative Care Action Plan
 Palliative Care Action Plan Citation: Ministry of Health. 2017.. Wellington: Ministry of Health. Published in March 2017 by the Ministry of Health PO Box 5013, Wellington 6145, New Zealand ISBN 978-1-98-850234-2
Palliative Care Action Plan Citation: Ministry of Health. 2017.. Wellington: Ministry of Health. Published in March 2017 by the Ministry of Health PO Box 5013, Wellington 6145, New Zealand ISBN 978-1-98-850234-2
Scoping exercise to inform the development of an education strategy for Children s Hospices Across Scotland (CHAS) SUMMARY DOCUMENT
 SUMMARY DOCUMENT") School of Health and Social Care Scoping exercise to inform the development of an education strategy for Children s Hospices Across Scotland (CHAS) SUMMARY DOCUMENT Background Children s palliative care
School of Health and Social Care Scoping exercise to inform the development of an education strategy for Children s Hospices Across Scotland (CHAS) SUMMARY DOCUMENT Background Children s palliative care
The Vision. The Objectives
 The Vision Older people participate to their fullest ability in decisions about their health and wellbeing and in family, whānau and community life. They are supported in this by co-ordinated and responsive
The Vision Older people participate to their fullest ability in decisions about their health and wellbeing and in family, whānau and community life. They are supported in this by co-ordinated and responsive
Palliative and end of life care for older people: the options.
 Palliative and end of life care for older people: the options. Chris Murphy Project Leader Hospice New Zealand August 2017 This presentation will explore: Strategies and guidelines that guide palliative
Palliative and end of life care for older people: the options. Chris Murphy Project Leader Hospice New Zealand August 2017 This presentation will explore: Strategies and guidelines that guide palliative
National Cancer Programme. Work Plan 2014/15
 National Cancer Programme Work Plan 2014/15 Citation: Ministry of Health. 2014. National Cancer Programme: Work Plan 2014/15. Wellington: Ministry of Health. Published in December 2014 by the Ministry
National Cancer Programme Work Plan 2014/15 Citation: Ministry of Health. 2014. National Cancer Programme: Work Plan 2014/15. Wellington: Ministry of Health. Published in December 2014 by the Ministry
Primary Health Networks Greater Choice for At Home Palliative Care
 Primary Health Networks Greater Choice for At Home Palliative Care Brisbane South PHN When submitting the Greater Choice for At Home Palliative Care Activity Work Plan 2017-2018 to 2019-2020 to the Department
Primary Health Networks Greater Choice for At Home Palliative Care Brisbane South PHN When submitting the Greater Choice for At Home Palliative Care Activity Work Plan 2017-2018 to 2019-2020 to the Department
Community and Hospital Surveillance
 6SSN 2324-497 Community and Hospital Surveillance ILI, SARI, Influenza and Respiratory Pathogens 217 Influenza Season, Week 3, ending 3 July 217 SUMMARY Influenza-like illness (ILI) consultation rates
6SSN 2324-497 Community and Hospital Surveillance ILI, SARI, Influenza and Respiratory Pathogens 217 Influenza Season, Week 3, ending 3 July 217 SUMMARY Influenza-like illness (ILI) consultation rates
Midland Region All Boards Development Days. Midland Cancer Network. 15, 16 October, 2015
 Midland Region All Boards Development Days Midland Cancer Network 15, 16 October, 2015 NZ cancer incidence 1948-2011 Source: NZ Cancer 0.0 50.0 100.0 150.0 200.0 250.0 300.0 350.0 400.0 0 5000 10000 15000
Midland Region All Boards Development Days Midland Cancer Network 15, 16 October, 2015 NZ cancer incidence 1948-2011 Source: NZ Cancer 0.0 50.0 100.0 150.0 200.0 250.0 300.0 350.0 400.0 0 5000 10000 15000
Dudley End of Life and Palliative Care Strategy Implementation Plan 2017
 Dudley End of Life and Palliative Care Strategy Implementation Plan 2017 End of Life and Palliative Care Strategy 2017 1 Contents Page What is a strategy plan? 3 Terminology 3 Demographics 3 Definitions
Dudley End of Life and Palliative Care Strategy Implementation Plan 2017 End of Life and Palliative Care Strategy 2017 1 Contents Page What is a strategy plan? 3 Terminology 3 Demographics 3 Definitions
Palliative Care in Regional and Rural Australia
 Palliative Care in Regional and Rural Australia Jane Phillips Funded by Australian Government Department of Health and Ageing National Rural Palliative Care Program 2004-06 Rural Palliative Care Project
Palliative Care in Regional and Rural Australia Jane Phillips Funded by Australian Government Department of Health and Ageing National Rural Palliative Care Program 2004-06 Rural Palliative Care Project
Published in January 2012 by: The Palliative Care Council of New Zealand, Hospice New Zealand & the Ministry of Health
 The Palliative Care Glossary was prepared by: Wayne Naylor Senior Analyst Palliative Care Council of New Zealand Acknowledgements Mary Schumacher - CEO, Hospice New Zealand; Dr Kate Grundy - Chair, Palliative
The Palliative Care Glossary was prepared by: Wayne Naylor Senior Analyst Palliative Care Council of New Zealand Acknowledgements Mary Schumacher - CEO, Hospice New Zealand; Dr Kate Grundy - Chair, Palliative
PART one. The Palliative Care Spectrum: Providing Care Across Settings
 PART one The Palliative Care Spectrum: Providing Care Across Settings Chapter 1 An Introduction to Palliative Pharmacy Care Jennifer M. Strickland To palliate means to alleviate. Palliative care, as the
PART one The Palliative Care Spectrum: Providing Care Across Settings Chapter 1 An Introduction to Palliative Pharmacy Care Jennifer M. Strickland To palliate means to alleviate. Palliative care, as the
Renal Service Plan for the Midland Region
 Renal Service Plan for the Midland Region Part Two Recommendations Options and Opportunities Prepared by: Jan Barber, Midland Regional Service Planner Date: December 2004 Acknowledgements: A number of
Renal Service Plan for the Midland Region Part Two Recommendations Options and Opportunities Prepared by: Jan Barber, Midland Regional Service Planner Date: December 2004 Acknowledgements: A number of
Yukon Palliative Care Framework
 Yukon Palliative Care Framework Contents Executive Summary...2 Introduction...3 Principles of the Framework...6 Continuum of Integrated Services...7 Supporting Care Providers...8 Best Practice Service
Yukon Palliative Care Framework Contents Executive Summary...2 Introduction...3 Principles of the Framework...6 Continuum of Integrated Services...7 Supporting Care Providers...8 Best Practice Service
POSITION DESCRIPTION Grade 4 Physiotherapist Physiotherapy Department
 POSITION DESCRIPTION Grade 4 Physiotherapist Physiotherapy Department Date revised: June 2015 POSITION: AWARD/AGREEMENT: Grade 4 Physiotherapists Health Professionals (Public Sector Victoria) CLASSIFICATION
POSITION DESCRIPTION Grade 4 Physiotherapist Physiotherapy Department Date revised: June 2015 POSITION: AWARD/AGREEMENT: Grade 4 Physiotherapists Health Professionals (Public Sector Victoria) CLASSIFICATION
Palliative care: Pharmacist challenges and Opportunities
 Palliative care: Pharmacist challenges and Opportunities Palliative care medicine was officially recognized as a specialty in Lebanon 28 June 2013 Ministry of Public Health issued decree number 1/1048
Palliative care: Pharmacist challenges and Opportunities Palliative care medicine was officially recognized as a specialty in Lebanon 28 June 2013 Ministry of Public Health issued decree number 1/1048
This specification should be read in conjunction with the Rotherham Hospice overall contract and schedules.
 Care Pathway/Service Commissioner Lead Provider Lead Period Applicability of Module E (Acute Services Requirements) Rotherham Palliative Medicine Service Gail Palmer Fiona Hendry 1 April 2011 31 March
Care Pathway/Service Commissioner Lead Provider Lead Period Applicability of Module E (Acute Services Requirements) Rotherham Palliative Medicine Service Gail Palmer Fiona Hendry 1 April 2011 31 March
What You Need To Know About Palliative Care. Natalie Wu Moy, LCSW, MSPA RUHS Medical Center Hospital Social Services Director
 What You Need To Know About Palliative Care Natalie Wu Moy, LCSW, MSPA RUHS Medical Center Hospital Social Services Director None of the faculty, planners, speakers, providers, nor CME committee members
What You Need To Know About Palliative Care Natalie Wu Moy, LCSW, MSPA RUHS Medical Center Hospital Social Services Director None of the faculty, planners, speakers, providers, nor CME committee members
Kent Joint Commissioning Action Plan For Adults with Autism and or ADHD (2017 / 2021)
") Easy Read Kent Joint Commissioning Action Plan For Adults with Autism and or ADHD (2017 / 2021) Action Plan The plan was developed to address the needs identified from the Kent Autism Strategy and Joint
Easy Read Kent Joint Commissioning Action Plan For Adults with Autism and or ADHD (2017 / 2021) Action Plan The plan was developed to address the needs identified from the Kent Autism Strategy and Joint
Primary Health Networks
 Primary Health Networks Drug and Alcohol Treatment Activity Work Plan 2016-17 to 2018-19 Drug and Alcohol Treatment Budget Murray PHN When submitting this Activity Work Plan 2016-2018 to the Department
Primary Health Networks Drug and Alcohol Treatment Activity Work Plan 2016-17 to 2018-19 Drug and Alcohol Treatment Budget Murray PHN When submitting this Activity Work Plan 2016-2018 to the Department
SOLIHULL BEREAVEMENT COUNSELLING SERVICE (SBCS)
") SOLIHULL BEREAVEMENT COUNSELLING SERVICE (SBCS) REVIEW AND DEVELOPMENT PLAN 2013 2016 1 EXECUTIVE SUMMARY Solihull Bereavement Counselling Service (SBCS) is a charity which provides specialist bereavement
SOLIHULL BEREAVEMENT COUNSELLING SERVICE (SBCS) REVIEW AND DEVELOPMENT PLAN 2013 2016 1 EXECUTIVE SUMMARY Solihull Bereavement Counselling Service (SBCS) is a charity which provides specialist bereavement
The National Council for Palliative Care Awards 2017 Judges Profiles
 The National Council for Palliative Care Awards 2017 Judges Profiles Alison Penny Coordinator, Childhood Bereavement Network Alison coordinates the Childhood Bereavement Network (CBN) and provides project
The National Council for Palliative Care Awards 2017 Judges Profiles Alison Penny Coordinator, Childhood Bereavement Network Alison coordinates the Childhood Bereavement Network (CBN) and provides project
Palliative Medicine Specialist
 Date XXXXXXX Job Title : Palliative Medicine Specialist Department : Palliative Care Services, Medicine & Health of Older People Services Location : Hibiscus Hospice will be the primary location and there
Date XXXXXXX Job Title : Palliative Medicine Specialist Department : Palliative Care Services, Medicine & Health of Older People Services Location : Hibiscus Hospice will be the primary location and there
Improving the Lives of People with Dementia
 Improving the Lives of People with Dementia Released August 2014 www.health.govt.nz Introduction Good health is essential for the social and economic wellbeing of New Zealanders. As the population of older
Improving the Lives of People with Dementia Released August 2014 www.health.govt.nz Introduction Good health is essential for the social and economic wellbeing of New Zealanders. As the population of older
POSITION DESCRIPTION. Clinical Psychologist Critical Care Complex
 POSITION DESCRIPTION Clinical Psychologist Critical Care Complex Date Produced/Reviewed: 18 April 2011 Position Holder's Name:... Position Holder's Signature:... Manager/Supervisor's Name:... Manager/Supervisor's
POSITION DESCRIPTION Clinical Psychologist Critical Care Complex Date Produced/Reviewed: 18 April 2011 Position Holder's Name:... Position Holder's Signature:... Manager/Supervisor's Name:... Manager/Supervisor's
Psychotherapist/Child Psychotherapist Marinoto CAMHS
 Date: March 2017 Job Title : Allied health- Psychotherapist/ Child Psychotherapist Department : Marinoto Location : North Shore/ Waitakere Reporting To : Team Manager Direct Reports : No Functional Relationships
Date: March 2017 Job Title : Allied health- Psychotherapist/ Child Psychotherapist Department : Marinoto Location : North Shore/ Waitakere Reporting To : Team Manager Direct Reports : No Functional Relationships
MidCentral District Health Board Rheumatic Fever Prevention Plan. October 2013
 MidCentral District Health Board Rheumatic Fever Prevention Plan October 2013 Contents Section 1: Introduction... 3 1.1 Executive summary... 3 1.2 Purpose... 5 Section 2: Overview of acute rheumatic fever
MidCentral District Health Board Rheumatic Fever Prevention Plan October 2013 Contents Section 1: Introduction... 3 1.1 Executive summary... 3 1.2 Purpose... 5 Section 2: Overview of acute rheumatic fever
Bereavement support in Scotland. A report by Sue Ryder and Hospice UK October 2018
 Bereavement support in Scotland A report by Sue Ryder and Hospice UK October 2018 2 Introduction Modest estimates put the number of people bereaved each year in Scotland at over 230,000. 1 A crucial component
Bereavement support in Scotland A report by Sue Ryder and Hospice UK October 2018 2 Introduction Modest estimates put the number of people bereaved each year in Scotland at over 230,000. 1 A crucial component
Promoting Excellence: A framework for all health and social services staff working with people with Dementia, their families and carers
 Promoting Excellence: A framework for all health and social services staff working with people with Dementia, their families and carers Mapped to the NHS Knowledge and Skills Framework () Background and
Promoting Excellence: A framework for all health and social services staff working with people with Dementia, their families and carers Mapped to the NHS Knowledge and Skills Framework () Background and
Supporting information for the Report on National Gynaecological Oncology Service Provision Models
 Discussion document Supporting information for the Report on National Gynaecological Oncology Service Provision Models Sub Group of the National Gynaecological Cancer Working Group 26 November 2013 For
Discussion document Supporting information for the Report on National Gynaecological Oncology Service Provision Models Sub Group of the National Gynaecological Cancer Working Group 26 November 2013 For
DEPARTMENT OF EDUCATION WESTERN AUSTRALIA JOB DESCRIPTION FORM THIS POSITION REPORTING RELATIONSHIPS
 School Education Act 1999 Group: Region: DEPARTMENT OF EDUCATION WESTERN AUSTRALIA JOB DESCRIPTION FORM Schools Salaries/Agreement/Award Teachers (Public Sector Primary and Secondary) Award 1993; The School
School Education Act 1999 Group: Region: DEPARTMENT OF EDUCATION WESTERN AUSTRALIA JOB DESCRIPTION FORM Schools Salaries/Agreement/Award Teachers (Public Sector Primary and Secondary) Award 1993; The School
World Cancer Congress, August 2012, Montreal, Canada
 World Cancer Congress, August 2012, Montreal, Canada Palliative Care and Health Systems Strengthening in Africa Fatia Kiyange Director of Programs African Palliative Care Association Kampala, Uganda The
World Cancer Congress, August 2012, Montreal, Canada Palliative Care and Health Systems Strengthening in Africa Fatia Kiyange Director of Programs African Palliative Care Association Kampala, Uganda The
Invasive Pneumococcal Disease Quarterly Report
 Invasive Pneumococcal Disease Quarterly Report April June 2018 Prepared as part of a Ministry of Health contract for scientific services by Liza Lopez Helen Heffernan July 2018 Acknowledgements This report
Invasive Pneumococcal Disease Quarterly Report April June 2018 Prepared as part of a Ministry of Health contract for scientific services by Liza Lopez Helen Heffernan July 2018 Acknowledgements This report
Palliative Care Standards & Models
 Palliative Care Standards & Models Ian Anderson Continuing Education Program in End-of of-life Care End-of of-life Care! 222,000 Canadians die each year! 75% die in institutions! 90% want to die at home
Palliative Care Standards & Models Ian Anderson Continuing Education Program in End-of of-life Care End-of of-life Care! 222,000 Canadians die each year! 75% die in institutions! 90% want to die at home
Primary Health Networks
 Primary Health Networks Drug and Alcohol Treatment Activity Work Plan 2016-17 to 2018-19 Hunter New England & Central Coast Please note: This Activity Work Plan was developed in response to the HNECC PHN
Primary Health Networks Drug and Alcohol Treatment Activity Work Plan 2016-17 to 2018-19 Hunter New England & Central Coast Please note: This Activity Work Plan was developed in response to the HNECC PHN
REGIONAL DIFFERENCES IN HF SERVICE DEMAND AND DELIVERY
 REGIONAL DIFFERENCES IN HF SERVICE DEMAND AND DELIVERY Raewyn Fisher, Waikato Hospital On behalf of Midland Cardiac Network (With thanks to Population Health data analysts) Cardiac Network Plans (Midland)
REGIONAL DIFFERENCES IN HF SERVICE DEMAND AND DELIVERY Raewyn Fisher, Waikato Hospital On behalf of Midland Cardiac Network (With thanks to Population Health data analysts) Cardiac Network Plans (Midland)
Discussion Document - National Health and Social Care Workforce Plan
 Discussion Document - National Health and Social Care Workforce Plan Are you responding as an individual or organisation? Organisation Full name or organisation s name British Dental Association Phone
Discussion Document - National Health and Social Care Workforce Plan Are you responding as an individual or organisation? Organisation Full name or organisation s name British Dental Association Phone
PART A: BACKGROUND TO CLINICAL GUIDELINES PROJECT
 Development Supported by the Ministry of Health (2015) PAEDIATRIC PALLIATIVE CARE IN NEW ZEALAND: CLINICAL GUIDELINES FOR END-OF-LIFE CARE PART A: BACKGROUND TO CLINICAL GUIDELINES PROJECT PART A: BACKGROUND
Development Supported by the Ministry of Health (2015) PAEDIATRIC PALLIATIVE CARE IN NEW ZEALAND: CLINICAL GUIDELINES FOR END-OF-LIFE CARE PART A: BACKGROUND TO CLINICAL GUIDELINES PROJECT PART A: BACKGROUND
NZ Organised Stroke Rehabilitation Service Specifications (in-patient and community)
") NZ Organised Stroke Rehabilitation Service Specifications (in-patient and community) Prepared by the National Stroke Network to outline minimum and strongly recommended standards for DHBs. Date: December
NZ Organised Stroke Rehabilitation Service Specifications (in-patient and community) Prepared by the National Stroke Network to outline minimum and strongly recommended standards for DHBs. Date: December
New Zealand Nephrology Activity Report 2014
 New Zealand Nephrology Activity Report Care Processes and Treatment Targets Key findings about care for people with end-stage kidney disease treated with dialysis or kidney transplantation in New Zealand
New Zealand Nephrology Activity Report Care Processes and Treatment Targets Key findings about care for people with end-stage kidney disease treated with dialysis or kidney transplantation in New Zealand
There For You. Your Compassionate Guide. World-Class Hospice Care Since 1979
 There For You Your Compassionate Guide World-Class Hospice Care Since 1979 What Is Hospice? Hospice is a type of care designed to provide support during an advanced illness. Hospice care focuses on comfort
There For You Your Compassionate Guide World-Class Hospice Care Since 1979 What Is Hospice? Hospice is a type of care designed to provide support during an advanced illness. Hospice care focuses on comfort
The Way Ahead Our Three Year Strategic Plan EVERY MOMENT MATTERS
 The Way Ahead Our Three Year Strategic Plan 2017-2020 EVERY MOMENT MATTERS Every moment matters - that s what our logo says right next to our name John Taylor Hospice and for us the two are inseparable.
The Way Ahead Our Three Year Strategic Plan 2017-2020 EVERY MOMENT MATTERS Every moment matters - that s what our logo says right next to our name John Taylor Hospice and for us the two are inseparable.
Invasive Pneumococcal Disease Quarterly Report
 Invasive Pneumococcal Disease Quarterly Report January March 2018 Prepared as part of a Ministry of Health contract for scientific services by Rebekah Roos Helen Heffernan June 2018 Acknowledgements This
Invasive Pneumococcal Disease Quarterly Report January March 2018 Prepared as part of a Ministry of Health contract for scientific services by Rebekah Roos Helen Heffernan June 2018 Acknowledgements This
What is Palliative Care? DEFINITIONS PALLIATIVE CARE. Palliative & End of Life Care Services N E Lincs 28/09/2017 1
 What is Palliative Care? 1 DEFINITIONS Palliative Care: is the active holistic care of patients with advanced progressive illness. The goal of palliative care is achievement of the best quality of life
What is Palliative Care? 1 DEFINITIONS Palliative Care: is the active holistic care of patients with advanced progressive illness. The goal of palliative care is achievement of the best quality of life
Updated Activity Work Plan : Drug and Alcohol Treatment
 Web Version HPRM DOC/17/1043 Updated Activity Work Plan 2016-2019: Drug and Alcohol Treatment This Drug and Alcohol Treatment Activity Work Plan template has the following parts: 1. The updated strategic
Web Version HPRM DOC/17/1043 Updated Activity Work Plan 2016-2019: Drug and Alcohol Treatment This Drug and Alcohol Treatment Activity Work Plan template has the following parts: 1. The updated strategic
Helplines and local mental health services
 Helplines and local mental health services FEBRUARY 2018 Tēnā koe In this resource you will find a directory of helplines and local mental health service contact details. To help connect people with their
Helplines and local mental health services FEBRUARY 2018 Tēnā koe In this resource you will find a directory of helplines and local mental health service contact details. To help connect people with their
Coordination of palliative care in community settings. Summary report
 Coordination of palliative care in community settings Summary report This resource may also be made available on request in the following formats: 0131 314 5300 nhs.healthscotland-alternativeformats@nhs.net
Coordination of palliative care in community settings Summary report This resource may also be made available on request in the following formats: 0131 314 5300 nhs.healthscotland-alternativeformats@nhs.net
Adult mental health and addiction consumer and peer workforce survey of Vote Health funded services
 Adult mental health and addiction consumer and peer workforce 2014 survey of Vote Health funded services Contents Introduction... 3 Existing workforce information... 3 The 2014 More than numbers organisation
Adult mental health and addiction consumer and peer workforce 2014 survey of Vote Health funded services Contents Introduction... 3 Existing workforce information... 3 The 2014 More than numbers organisation
Recognition of Skills and Training Q. Does the Greens support direct referrals to selected medical specialist services?
 22 September 2014 Colleen Hartland, MLC 75 Victoria Street SEDDON VIC 3011 Dear Ms Hartland, The Australian Physiotherapy Association represents more than 4,100 Victorian physiotherapists and over 16,500
22 September 2014 Colleen Hartland, MLC 75 Victoria Street SEDDON VIC 3011 Dear Ms Hartland, The Australian Physiotherapy Association represents more than 4,100 Victorian physiotherapists and over 16,500
Revitalising the National HPV Immunisation Programme. with agreed outcomes from the August 2014 workshop
 Revitalising the National HPV Immunisation Programme with agreed outcomes from the August 2014 workshop Citation: Ministry of Health. 2015. Revitalising the National HPV Immunisation Programme with Agreed
Revitalising the National HPV Immunisation Programme with agreed outcomes from the August 2014 workshop Citation: Ministry of Health. 2015. Revitalising the National HPV Immunisation Programme with Agreed
Guest Editorial for Virtual Issue on Supportive and Palliative Care in Health and Social Care in the Community
 Guest Editorial for Virtual Issue on Supportive and Palliative Care in Health and Social Care in the Community How can communities be better supported to provide palliative care? Merryn Gott PhD, MA (Oxon),
Guest Editorial for Virtual Issue on Supportive and Palliative Care in Health and Social Care in the Community How can communities be better supported to provide palliative care? Merryn Gott PhD, MA (Oxon),
EMU A NEW MODEL OF EMERGENCY CARE FOR THE FRAIL & ELDERLY
 EMU A NEW MODEL OF EMERGENCY CARE FOR THE FRAIL & ELDERLY Geriatrics, General practice, Emergency medicine, Interface medicine SUMMARY An integrated, community emergency service specifically designed for
EMU A NEW MODEL OF EMERGENCY CARE FOR THE FRAIL & ELDERLY Geriatrics, General practice, Emergency medicine, Interface medicine SUMMARY An integrated, community emergency service specifically designed for
Position Description Counsellor/ Psychosocial Team leader
 We get it. Just when life should be full of possibilities, cancer crashes into a young person s world and shatters everything. CanTeen is the game changer. CanTeen is a national support organisation for
We get it. Just when life should be full of possibilities, cancer crashes into a young person s world and shatters everything. CanTeen is the game changer. CanTeen is a national support organisation for
PERINATAL PALLIATIVE CARE SUPPORTING FAMILIES AS THEY PREPARE TO WELCOME THEIR BABY AND TO SAY GOOD-BYE
 PERINATAL PALLIATIVE CARE SUPPORTING FAMILIES AS THEY PREPARE TO WELCOME THEIR BABY AND TO SAY GOOD-BYE Kathy Cromwell CT, MSW, LCSW Director, Hinds Hospice Angel Babies HINDS HOSPICE ANGEL BABIES Our
PERINATAL PALLIATIVE CARE SUPPORTING FAMILIES AS THEY PREPARE TO WELCOME THEIR BABY AND TO SAY GOOD-BYE Kathy Cromwell CT, MSW, LCSW Director, Hinds Hospice Angel Babies HINDS HOSPICE ANGEL BABIES Our
Bringing prostate cancer education to regional and rural Australian communities
 Bringing prostate cancer education to regional and rural Australian communities Julie Sykes 1, Lisa Fodero 2, Nick Brook 3, Rachel Jenkin 4 1 Prostate Cancer Foundation of Australia; 2 Health Consult;
Bringing prostate cancer education to regional and rural Australian communities Julie Sykes 1, Lisa Fodero 2, Nick Brook 3, Rachel Jenkin 4 1 Prostate Cancer Foundation of Australia; 2 Health Consult;
Consultation on Legislative Options for Assisted Dying
 Consultation on Legislative Options for Assisted Dying A submission to the External Panel by the Canadian Hospice Palliative Care Association October 9, 2015 Sharon Baxter Executive Director Sbaxter@bruyere.org
Consultation on Legislative Options for Assisted Dying A submission to the External Panel by the Canadian Hospice Palliative Care Association October 9, 2015 Sharon Baxter Executive Director Sbaxter@bruyere.org
POSITION DESCRIPTION
 POSITION DETAILS: POSITION DESCRIPTION TITLE: Mental Health Smoke Free Coordinator REPORTS TO: Nurse Director Mental Health & Addiction Directorate LOCATION: Across the Directorate AUTHORISED BY: Nurse
POSITION DETAILS: POSITION DESCRIPTION TITLE: Mental Health Smoke Free Coordinator REPORTS TO: Nurse Director Mental Health & Addiction Directorate LOCATION: Across the Directorate AUTHORISED BY: Nurse
Palliative and End of Life Care in Scotland: The Case For a Cohesive Approach
 Palliative and End of Life Care in Scotland: The Case For a Cohesive Approach Membership Dr Patricia Cantley, Consultant in Elderly Medicine, NHS Lothian Dr Fiona Downs, Consultant in Palliative Care,
Palliative and End of Life Care in Scotland: The Case For a Cohesive Approach Membership Dr Patricia Cantley, Consultant in Elderly Medicine, NHS Lothian Dr Fiona Downs, Consultant in Palliative Care,
Workforce Assessment Report DHB Audiology (Reo Ataata) Workforce 2018
 Workforce 2018") Prepared by: Strategic Workforce Services Workforce Assessment Report DHB Audiology (Reo Ataata) Workforce 2018 Strategic Workforce Services - DHB Audiology (Reo Ataata) Workforce Copyright C/- Central
Prepared by: Strategic Workforce Services Workforce Assessment Report DHB Audiology (Reo Ataata) Workforce 2018 Strategic Workforce Services - DHB Audiology (Reo Ataata) Workforce Copyright C/- Central
Strategic Plan
 Strategic Plan 2018 2022 Pallative Care Victoria Palliative Care Victoria Palliative Care Victoria is the peak body for palliative care and end of life care. Established in 1981, we are an incorporated
Strategic Plan 2018 2022 Pallative Care Victoria Palliative Care Victoria Palliative Care Victoria is the peak body for palliative care and end of life care. Established in 1981, we are an incorporated
Background. Yet, as a nation, we find it hard to talk about and harder still to help people dealing with a bereavement.
 A better grief 2 A better grief Background We all experience bereavement and grief at some stage in our lives. Seventy-two per cent of us have been bereaved at least once in the last five years, according
A better grief 2 A better grief Background We all experience bereavement and grief at some stage in our lives. Seventy-two per cent of us have been bereaved at least once in the last five years, according
National Year 10 ASH Snapshot Survey, : Trends in Tobacco Use by Students Aged Years
 National Year 10 ASH Snapshot Survey, 1999-2009: Trends in Tobacco Use by Students Aged 14-15 Years Janine Paynter On behalf of Action on Smoking and Health, Health Sponsorship Council and the Ministry
National Year 10 ASH Snapshot Survey, 1999-2009: Trends in Tobacco Use by Students Aged 14-15 Years Janine Paynter On behalf of Action on Smoking and Health, Health Sponsorship Council and the Ministry
Cancer Control Council Evaluation and Monitoring Framework
 Cancer Control Council Evaluation and Monitoring Framework Table of contents 1. Purpose...1 2. Background...1 3. Clarification of key tasks...2 4. International evaluation and monitoring frameworks...3
Cancer Control Council Evaluation and Monitoring Framework Table of contents 1. Purpose...1 2. Background...1 3. Clarification of key tasks...2 4. International evaluation and monitoring frameworks...3
Arts therapy changes to systems through alternative health and wellness program
 POSTER 22 Arts therapy changes to systems through alternative health and wellness program Jennifer Stirling 1 1 Maryborough District Health Services, Vic Introduction Maryborough District Health Service
POSTER 22 Arts therapy changes to systems through alternative health and wellness program Jennifer Stirling 1 1 Maryborough District Health Services, Vic Introduction Maryborough District Health Service
Palliative Care. Working towards the future of quality palliative care for all
 Palliative Care Working towards the future of quality palliative care for all FEBRUARY 2019 Recommended citation Palliative Care Australia 2018, Palliative Care 2030 working towards the future of quality
Palliative Care Working towards the future of quality palliative care for all FEBRUARY 2019 Recommended citation Palliative Care Australia 2018, Palliative Care 2030 working towards the future of quality