Integrating Transgender Health Care Into Our Medical Culture
|
|
|
- Darrell Bryant
- 5 years ago
- Views:
Transcription
1 Integrating Transgender Health Care Into Our Medical Culture JOHN F. RANDOLPH, JR., MD DIVISION OF REPRODUCTIVE ENDOCRINOLOGY AND INFERTILITY DEPARTMENT OF OBSTETRICS AND GYNECOLOGY UNIVERSITY OF MICHIGAN HEALTH SYSTEM OCTOBER 27, 2016
2 Disclosures None I have been a member of the University of Michigan Comprehensive Gender Services Program since it was formed in 1994.
3 How do you care for a population of which you were unaware and for which you have received no training? You don t, so patients can t find care. You try, but your setting and care do not meet patients needs, so they don t return and may not get care. You really try, so your patients teach you what they need. You learn how to care for them optimally, and they get high quality long term care.
4 Objectives Extend cultural competence to clinical competence. Let s talk about gender dysphoria. Health issues for transpeople. What is the role of an obstetrician-gynecologist? Transgender medical therapy: the basics. What needs to happen next? A vision of transcare in the future.
5 Translanguage Transgender (trans): A term for people whose gender identity, expression or behavior is different from those typically associated with their assigned sex at birth. Cisgender (cis): A term for people whose gender identity, expression or behavior matches those typically associated with their assigned sex at birth. Gender non-conforming: A term for individuals whose gender expression is different from societal expectations related to gender. Gender dysphoria in adult (DSM-5): A noticeable incongruence between the gender the patient believes they are, and what society perceives them to be. (ICD 10: F64.0) Gender identity disorder (DSM-4): Do not use; replace it in the Problem List.
6
7 Etiology of Gender Dysphoria Unknown, but generally agreed now to be inborn. Earliest theories argued for a psychosocial disorder or failure of optimal parent-child interactions. Origins of initial care recommendations. Biological theories postulate early prenatal exposure to incongruent sex steroids. Not well supported by DSD experience. Scattered evidence for differences in hypothalamic nuclei. Uncertain cause. Gender Dysphoria is not a lifestyle choice!
8 Prevalence of Gender dysphoria DSM-5: % for adult natal males and % for adult natal females. Halley Crissman, M.D., HO 2: Approximately 1 in 189 U.S. adults identify as transgender. Secondary analysis of data from 20 states and territories in the 2014 Behavioral Risk Factor Surveillance System. 151,456 asked Do you consider yourself to be transgender? Transgender individuals made up 0.53% and were more likely to be nonwhite, below the poverty line, and less likely to attend college. Transgender prevalence and demographics: a household probability sample of United States adults, 2014 currently under revision for AJPH. New Zealand teens: 1.2 %.
9 Sobering numbers US population January 1, 2016 (projected): 322,762,018. US transgender population January 1, 2016 (Crissman projected): 1,710,661. Require lifetime care. ~51% could desire a hysterectomy: 872,437. US transgender population of year olds January 1, 2016 (7% estimate): 119,746. Potential initial presentation for care. NP visits for gender care UM Ob-Gyn FY 16: 142. Primarily to initiate hormone therapy. Some requesting surgery. Some with gynecologic concerns.
10 Changing insurance climate May, 2014: Medicare no longer considers gender surgery as experimental and will cover it. May 13, 2016: HHS finalizes Section 1557 of the Affordable Care Act Prohibiting denial of health care or health coverage based on an individual s sex, including discrimination based on pregnancy, gender identity, and sex stereotyping. June 2, 2016: VA proposes to provide coverage for gender surgery. June 30, 2016: DoD Service members with a diagnosis from a military medical provider indicating that gender transition is medically necessary will be provided medical care and treatment for the diagnosed medical condition.
11 Financial access to gender health care is changing Lack of coverage has been the primary impediment to both hormone therapy and gender surgery. Increasing numbers of health plans cover all services. Cost is minimal to date due to relatively low numbers. It is unclear how the ACA ruling will be interpreted by the courts. It may be mandated that all plans cover all services offered to other patients for recognized medical conditions.
12 The legal climate is changing June, 2010: U.S. State Department policy issues passports that reflect a person s current gender. A previous passport or certification from a physician confirming that he or she has had appropriate clinical treatment for gender transition. Can then change Social Security gender status. Gender marker determined by states. Varies widely. March 10, 2016: Michigan Secretary of State revises the rule requiring gender confirming surgery to change drivers license gender designation. Passport, birth certificate or court order is needed. Gender identity is not a protected class under Michigan s anti-discrimination law. Elliott-Larsen Civil Rights Act Employment and housing are not protected.
13 Demand for transgender health care services will continue to increase Increasing social acceptance. Varies widely. Increasing economic access. Increasing legal access. A major limiting factor is a lack of available high quality care.
14 Health issues for transpeople 2011 National Transgender Discrimination Survey: 6450 transgender and gender non-conforming study participants Barriers to care: 19% reported being refused medical care due to their transgender or gender non-conforming status. 28% were subjected to harassment in medical settings. 2% were victims of violence in the doctor s office. 50% reported having to teach their medical providers about transgender care. Despite barriers, 62% had accessed hormone therapy. Disparities: Greater than 4 times the national average of HIV infection (2.6% vs. 0.6%). 26% use or have used alcohol and drugs to cope with discrimination. 41% reported attempting suicide compared to 1.6% of the general population. 57% faced some rejection by their family. Family rejection significantly increased rates of homelessness, incarceration, sex work, HIV, suicide attempts, smoking, and use of drugs and alcohol.
15 Health care needs for transpeople Routine health care Screening. Breast and cervix/uterus/ovaries in transmen. Breast and prostate in transwomen. STI in a traditionally high risk population. All other needs, with cultural competence. Mental health care High rate of need. Uncertain intersection of gender dysphoria and other mental health conditions. Trained professionals.
16 Health care wants for transpeople Hormonal transition to the gender of identity. Transwomen: estrogen, anti-androgen. Transmen: testosterone. Surgery. Gender confirming/affirming. NOT sex reassignment surgery (SRS)! Transmen: bilateral mastectomies/hysterectomy/bso/vaginectomy/phalloplasty/scrotoplasty. Transwomen: orchiectomy/penectomy/vulvo-vaginoplasty. Identity enhancing. Facial feminization/tracheochondroplasty/body contouring/implants. Vocal cord. Hair transplants.
17 More health care wants for transpeople Reproductive options. Gamete cryopreservation/art. Counseling on recovery of reproductive capacity. Contraception/STI prevention. Cosmetic options. Electrolysis/ laser for unwanted terminal hair. Counseling in make-up and hair care. Behavior modification. Vocal coaching for pitch and speech patterns. Gender specific patterns of dress and action.
18 Standards of care for transpeople WPATH. Incorporated in 1979 as the Harry Benjamin International Gender Dysphoria Association, changed to World Professional Association for Transgender Health in th version of Standards of Care (SOC) published in Mission to promote evidence based care, education, research, advocacy, public policy, and respect in transgender health. Fenway Center, Boston. The Medical Care of Transgender Persons, UCSF Center of Excellence for Transgender Health. Primary Care Protocol, 2011.
19 What is the role of an obstetriciangynecologist in the care of transpeople? Women s Health consultants. Remember, the need is for lifelong health care. Screening recommendations/provision. STI and cervix: same care as anyone with a vagina and cervix. May not use and/or want either: use a Pederson or pediatric speculum. Ask about sexual behaviors and concerns. Discuss contraception. Breasts: same care as anyone who has breasts, spontaneously or medically induced. Risk with long term hormone use, estrogen or testosterone, is unknown. Uncertain recommendations after mastectomies; concern is occurrence, not recurrence. Estrogen use will (probably) be lifelong. Prostate: same care as anyone who has a prostate. Unknown effect on cancer risk with long term estrogen use.
20 What is the role of an obstetriciangynecologist in the care of transpeople? Gynecologists. Abnormal bleeding in transmen with a uterus. Any bleeding is a concern, but usually explained by hormone use. Work-up if modifying the use doesn t resolve it. Long term risk of cancer with androgen use is unknown. Care of a neovagina/neovulva. Frequently, the initial surgery was done elsewhere. Graft sloughing/incisional breakdown are not uncommon. Need for long term dilation; strictures are the most common problem. Postop neoclitoral/labial pain or hypersensitivity may require revision. HPV surveillance?
21 Medical Care of Transpeople Hormones and hormone therapy Sex steroids Goals Risks Options Surgery Other issues
22 Sex steroids Androgens Testosterone and derivatives Androstenedione Precursor only Dihydrotestosterone (DHT) Potent metabolite of T in skin Not used clinically Synthetics
23 Sex steroids Estrogens Estradiol and derivatives Most potent Estrone Estriol Conjugated equine (CEE) Synthetic
24 Testosterone Where does it come from?: gonads and adrenal glands What does it do?: Spermatogenesis Muscle density and mass Bone density and length, cartilage growth Libido Male secondary sex characteristics organs, voice, hair, growth
25 Testosterone The primary androgen. How much does it take to make things happen?: Men have ten-fold higher T levels than women. Adult Male: ng/ml. Adult Female: 0.10 to 0.90 ng/ml. Slightly elevated levels can cause acne and hirsutism.
26 Estradiol Where: gonads, fat, muscle What does it do?: Menstrual cycle, endometrium Bone, skin, hair, GI, lungs Clotting factors Lipids Female secondary sex characteristics Breast, vaginal growth, fat distribution
27 Estradiol The primary estrogen. How much does it take to make things happen?: Harder to estimate: women cycle! Adult male: 6-44 pg/ml Adult female: early follicular pg/ml; late follicular pg/ml; midcycle pg/ml; luteal phase pg/ml; postmenopausal <20 pg/ml. Ballpark mid-range: pg/ml.
28 Two Primary goals of hormone therapy Induce the desired secondary sex characteristics ( Minipuberty ), a direct effect of the administered hormone. Women: breast growth, body composition. Men: voice deepening, terminal facial and body hair, body composition. Cause regression of already induced characteristics, an indirect effect through suppression of the pituitary hormones that drive the gonads (FSH/LH). Men: Amenorrhea, fat mass, some breast tissue. Women: facial and body terminal hair, muscle mass, gonads, spontaneous erections. Unnecessary after gonadectomy.
29 Adjunct goal of hormone therapy Do no harm. Short term: Several studies of overall risk. Long term: Few data on long term risks. Patients don t consider hormones an elective option.
30 TABLE 1a. Effects and Expected Time Course of Masculinizing Hormones a Expected Expected maximum Effect onset b effect b Skin oiliness/acne 1 6 months 1 2 years Facial/body hair Growth 3 6 months 3 5 years Scalp hair loss >12 months c Variable Increased muscle mass/strength 6 12 months 2 5 years d Body fat Redistribution 3 6 months 2 5 years Cessation of Menses 2 6 months n/a Clitoral Enlargement 3 6 months 1 2 years Vaginal atrophy 3 6 months 1 2 years Deepened voice 3 12 months 1 2 years a Adapted with permission from Hembree et al. (2009). Copyright 2009, The Endocrine Society. b Estimates represent published and unpublished clinical observations. c Highly dependent on age and inheritance; may be minimal. d Significantly dependent on amount of exercise.
31 TABLE 1b. Effects and Expected Time Course of Feminizing Hormones a Effect Expected onset b effect b Expected maximum Body fat redistribution 3 6 months 2 5 years Decreased muscle mass/strength 3 6 months 1 2 years c Softening of skin/decreased oiliness 3 6 months Unknown Decreased libido 1 3 months 1 2 years Decreased spontaneous erections 1 3 months 3 6 months Male sexual dysfunction Variable Variable Breast growth 3 6 months 2 3 years Decreased testicular volume 3 6 months 2 3 years Decreased sperm production Variable Variable Thinning/slowed growth of body facial hair 6 12 months > 3 years d Male pattern baldness No regrowth, 1 2 years loss stops 1 3 months a Adapted with permission from Hembree et al. (2009). Copyright 2009, The Endocrine Society. b Estimates represent published and unpublished clinical observations. c Significantly dependent on amount of exercise. d Complete removal of male facial and body hair requires electrolysis, laser treatment, or both.
32 TABLE 2. Risks Associated with Hormone Therapy Risk level Feminizing hormones Masculinizing hormones Likely increased risk Venous thromboembolic disease a Polycythemia Gallstones Weight gain Elevated liver enzymes Acne Weight gain Androgenic alopecia (balding) Hypertriglyceridemia Sleep apnea Likely increased risk with presence of additional risk factors b Cardiovascular disease Possible increased risk Hypertension Elevated liver enzymes Hyperprolactinemia or prolactinoma Hyperlipidemia Possible increased risk with presence of additional risk factors b Type 2 diabetes a Destabilization of certain psychiatric disorders c Cardiovascular disease Hypertension Type 2 diabetes No increased risk or inconclusive Breast cancer Loss of bone density Breast cancer Cervical cancer Ovarian cancer Uterine cancer Note. Bolded items are clinically significant. a Risk is greater with oral estrogen administration than with transdermal estrogen administration. b Additional risk factors include age. c Includes bipolar, schizoaffective, and other disorders that may include manic or psychotic symptoms. This adverse event appears to be associated with higher doses or supraphysiologic blood levels of testosterone.
33 Hormone Therapy Quagmire There are no scientifically valid data to serve as the basis for hormonal augmentation regimens. This is not evidence-based medicine. Hormones will be administered for unapproved indications. WPATH: Letter of recommendation from a qualified mental health professional.
34 Assessment of Response to Hormone Therapy Short term: Suppression of serum levels of the principal endogenous gonadal hormone. Long term: Development of biological effects of the administered hormones, and suppression of the manifestations of the endogenous gonadal hormones.
35 Hormone Therapy in Transwomen Initial and principal therapy: Estrogens If adequate suppression of testicular function is not achieved, consider adjunctive therapy, using: Anti-androgens GnRH agonists
36 Estrogen Therapy in Transwomen Dosage is typically 6-8 times that used in menopausal hormone therapy (reduced after orchiectomy, if GCS is performed). Oral preparations, twice daily most commonly. Avoid oral preparations of unknown bioavailability. Non-oral options are increasingly requested, and may become the option of choice to minimize risk.
37 Preferred Estrogen Therapy in Transwomen Estradiol (micronized) (e.g. Estrace) 4-8 mg/day p.o. Conjugated estrogens USP (e.g. Premarin) 5-10 mg/day p.o. Transdermal patches More expensive One-three 0.1 mg patches at a time Decreased thromboembolic risk Intramuscular depo-estradiol (e.g. Delestrogen) 5 mg weekly Buccal micronized estradiol Dose is half of oral dose No good studies, but theoretically same safety profile as transdermal
38 Adjunctive Hormonal Therapy in Transwomen Anti-androgens: Spironolactone 100 mg/2x a day p.o. Finasteride 1-5 mg/day p.o. Other 5 α reductase inhibitors Cyproterone acetate (FDA denied approval in the U.S.) Progestins: Requests for breast growth Medroxyprogesterone (e.g. Provera) 5-10 mg/day p.o. Micronized progesterone mg/day p.o.
39 Surveillance of Hormone Therapy in Tranwomen Baseline, 2, 6, 12 months, then annually Serum estradiol & testosterone E pg/ml; T< 0.9 ng/ml. Blood pressure Electrolytes Per standard guidelines Mammograms Prostate
40 Hormone Therapy in Transmen Initial and principal therapy: Testosterone If adequate suppression of ovarian function is not achieved, consider adjunctive therapy, using: Anti-estrogen GnRH agonist
41 Testosterone Therapy in Transmen Dosage is typically 2-4 times that used as hormone replacement in male hypogonadism (reduced after oophorectomy, if GCS performed). Intramuscular administration is the standard. Depot testosterone esters (cypionate or enanthate) mg IM q 1-3 weeks
42 Testosterone Therapy in Transmen Other routes: Transdermal gel Steadier levels More expensive Avoid contact with others Transdermal patch (inconvenient & costly) Oral fluoxymesterone (Halotestin) (not recommended: frequent adverse effects at high dosages)
43 Adjunctive Hormonal Therapy in Transmen Anti-estrogens (infrequently used) Aromatase inhibitors (testosterone to estradiol): anastrozole, letrozole Estrogen receptor antagonists: tamoxiphene, toremifene, raloxifene
44 Surveillance of Hormone Therapy in Transmen Baseline, 2, 6, 12 months, then annually Serum testosterone & estradiol T in the mid-normal male range; E2 <50 pg/ml. Hemoglobin/hematocrit Liver function tests Baseline, annually Serum lipid profile Per standard guidelines Gyn screening
45 Adjunct Hormone Therapy in adolescents Inhibition of pituitary gonadotropins & thus gonadal steroidogenesis Goserelin subcutaneous implant q 3-4 weeks Leuprolide acetate depot suspension IM q 4 weeks Nafarelin nasal spray
46 Street-based hormone therapy Easy to get Internet Friends Many regimens Usually oral or transdermal. Oral androgens are most concerning. Frequently underdosed or overdosed. No screening for risks or monitoring for safety.
47 Bio-identical hormones Natural compounds of varying potency. Frequently don t achieve levels to suppress the endogenous gonads. Frequently associated with a lab to monitor levels: expensive. No evidence that they are safer or more effective than approved compounds.
48 Gender Confirming Surgery (GCS) Irreversible and final. Recommendation by an appropriate counselor. WPATH: Two letters, one by an independent psychologist/psychiatrist. Financial obstacles must be overcome. Multidisciplinary surgeon teams. May need several sessions of surgery.
49 Gender Confirming Surgery WPATH Readiness Criteria Demonstrable progress in consolidating the evolving gender identity. Demonstrable progress in dealing with work, family, and interpersonal issues resulting in a significantly better state of mental health. Tolerating hormonal therapy and maintaining good health. May become a prerequisite for insurance coverage.
50 Gender Confirming Surgery Male-to-Female Genital GCS Orchiectomy Vaginoplasty/clitoroplasty/labiaplasty Inversion of penile/scrotal skin Penectomy and pedicled rectosigmoid transplant; or Penectomy and free skin graft to line a neovagina



51 Penile inversion vaginoplasty 1. Incise penis and scrotum, remove testes. 2. Denude penile shaft. 3. Remove erectile tissue, preserving the urethra and neurovascular bundle and glans. 4. Create neovagina by inverting penile skin, shortening urethra, and trimming glans to form a clitoris. Form scrotal skin into labia.

52 Penile inversion vaginoplasty
53 Cosmetic GCS Gender Confirming Surgery Male-to-Female Augmentation mammoplasty After achieving stable breast growth Optional procedures to assist feminization: Reduction thyroid chondroplasty Suction lipoplasty/lipofilling Rhinoplasty Facial bone reduction, face-lift, blepharoplasty Pectoral/gluteal implants Vocal cord reconstruction
54 Gender Confirming Surgery Male-to-Female Post-op problems Graft failure Vaginal stenosis Maintenance requires use of dilators/stents or regular intercourse. Cosmetic appearance Hypersensitivity of reconstructed clitoris/vulva Anorgasmia
55 Genital GCS Gender Confirming Surgery Female-to-Male Hysterectomy +/- salpingo-oophorectomy Usually laparoscopic Vaginectomy Phalloplasty Free vascular graft/urethroplasty Flap Metoidioplasty Scrotoplasty with testicular implants Cosmetic GCS Reduction mammoplasty

56 Phalloplasty techniques Both require subsequent scrotoplasty and testicular implants using labial skin. Erections will require placement of an erectile device.

57 Free forearm flap phalloplasty

58 Metoidioplasty 1. Incise mucosa around urethral meatus and clitoral shaft. 2. Cut suspensory ligament. 3. Create an elongated urethra from vaginal/labial mucosa. 4. Attach neourethra to ventral shaft, and cover with mucosa. 5. Create a neoscrotum from vaginal mucosa, place implants.
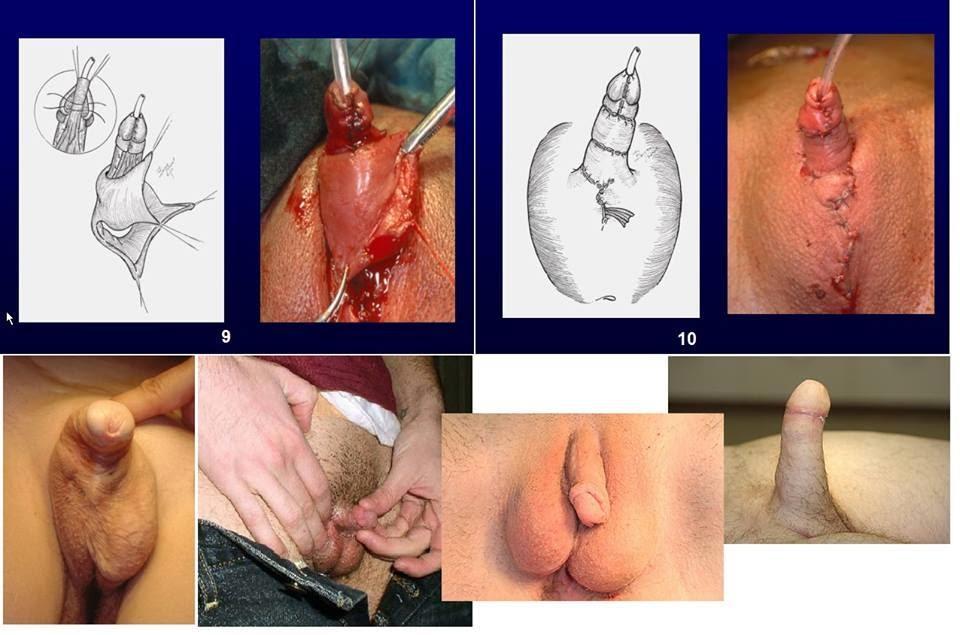
59 Metoidioplasty
60 Gender Confirming Surgery Female-to-Male Post-op problems Urethral strictures/fistulas Graft failure Pain Scarring at the graft donor site
61 Gender Confirming Surgery Post-Operative Care Reduce hormone therapy: suppression of gonadal function is no longer needed. Stop adjunctive medications. Continue counseling. Once completely healed, establish maintenance surveillance. Good primary care!
62 Gender Confirming Surgery Fertility Concerns Hormone therapy suppresses gonadal function and fertility. Returns with cessation of therapy. Does not automatically cause gonadal failure. Gonadectomy precludes genetic reproduction. Sperm can be frozen and stored, but must be collected off of hormones. Egg freezing is now available, but requires stimulation and retrieval, and is expensive.
63 Adjunctive therapies Ambisexual hair Hair biology Becomes terminal (thick, dark) at T levels above the female range. Chin, neck, upper back, midline chest and upper abdomen. Has a 3-5 year growth cycle. Scalp hair With genetic predisposition, will lose follicles in a male pattern with T.
64 Adjunctive therapies Ambisexual hair Hair induction Providing male levels of T will induce terminal growth in those areas. Density is determined by family. Takes as long as the hair cycle. Scalp hair Providing male levels of T will induce follicle loss in susceptible men.
65 Adjunctive therapies Hair removal Temporary Shaving, plucking, depilatories, bleaches. Semi-permanent: laser Wavelength targeted to the pigment in hair follicles. Faster, fewer sessions, less painful. Permanent: electrolysis Hot needle inserted down a hair follicle to destroy the papillae.
66 Adjunctive therapies Hair removal Unless T is blocked or removed, or all susceptible follicles are destroyed, terminal hair will return. Must maintain therapy if T or follicles are still present. Uncertain regrowth of follicles. Combination of T blocker or gonadectomy and laser/electrolysis provides the fastest cosmetic result.
67 Adjunctive therapies Vocal Vocal cords lengthen with T. longer lower pitch. Will not ever shorten, even with T removal. Speech therapy can train women to speak in their upper range. Speech therapy can instruct in genderspecific speech patterns. Voice feminization surgery.
68 Adjunctive therapies Restrictive Chest binding Tight, hot, restrictive of movement No known health consequences Genital tucking Uncomfortable Unclear effect on fertility
69 Transgender Clinical Care Education Risk assessment Informed decision making Appropriate therapy with appropriate monitoring Well considered surgery with experienced surgeons Good primary care
70 Transgender health care: What needs to happen next? Cultural competence All health care systems. Starting to happen. Clinical competence Integrated into ALL training programs at all levels. Medical school. Residency: Family Medicine, Internal Medicine, Pediatrics, Obstetrics and Gynecology. Post-residency. Must be part of each curriculum. Standard content. Assessment of competence.
71 A vision of transgender healthcare Early recognition Childhood (or earlier?). in the future Gender identity is ascertained, not assigned. Early treatment Puberty determined by identity, not genitals. Age-appropriate induction by the hormones of identity. Surgery when appropriate, and desired. At adulthood? Reproductive capacity preserved, if desired. Lifelong maintenance by competent providers.
72 Observations/musings/insights I have yet to see a patient start hormones and have major emotional problems. It s hard to be patient. Health insurance is the biggest current impediment to care, but access to competent clinical care will become so in the near future. Once hormonal/surgical changes have stabilized, patients frequently move on.
73 OBGYN Diversity, Equity, and Inclusion Initiative
Hormone Therapy Overview for the Behavioral Health Provider. Julie Thompson, PA Fenway Health
 Hormone Therapy Overview for the Behavioral Health Provider Julie Thompson, PA Fenway Health Continuing Medical Education Disclosure Program Faculty: Julie Thompson, PA Current Position: Physician s Assistant,
Hormone Therapy Overview for the Behavioral Health Provider Julie Thompson, PA Fenway Health Continuing Medical Education Disclosure Program Faculty: Julie Thompson, PA Current Position: Physician s Assistant,
Transgender Medicine beyond the guidelines.
 Transgender Medicine beyond the guidelines. Rachel Hopkins, MD Assistant Professor of Medicine SUNY Upstate Medical University Division of Endocrinology and Metabolism Overview Definitions and history
Transgender Medicine beyond the guidelines. Rachel Hopkins, MD Assistant Professor of Medicine SUNY Upstate Medical University Division of Endocrinology and Metabolism Overview Definitions and history
MEDICAL POLICY No R1 GENDER REASSIGNMENT SURGERY
 GENDER REASSIGNMENT SURGERY Effective Date: January 1, 2017* Review Dates: 8/15, 8/16, 11/16 Date Of Origin: August 12, 2015 Status: Current *Note: For fully funded commercial (individual or group), this
GENDER REASSIGNMENT SURGERY Effective Date: January 1, 2017* Review Dates: 8/15, 8/16, 11/16 Date Of Origin: August 12, 2015 Status: Current *Note: For fully funded commercial (individual or group), this
What to Know a 21 st Century Approach to Transgender Medical Care
 What to Know a 21 st Century Approach to Transgender Medical Care Joshua Safer, MD Transgender Medicine Research Group Center for Transgender Medicine and Surgery Patient / Mental Health Provider Gatekeeper
What to Know a 21 st Century Approach to Transgender Medical Care Joshua Safer, MD Transgender Medicine Research Group Center for Transgender Medicine and Surgery Patient / Mental Health Provider Gatekeeper
Harold Husovsky, MD. Associate Professor of General Medicine at SUNY Health Science Center
 Harold Husovsky, MD Associate Professor of General Medicine at SUNY Health Science Center Care of the Transgendered Syracuse University, 1/09/07 Goals Introductions Definitions Statistics Evaluation Treatments
Harold Husovsky, MD Associate Professor of General Medicine at SUNY Health Science Center Care of the Transgendered Syracuse University, 1/09/07 Goals Introductions Definitions Statistics Evaluation Treatments
HEALTH CARE FOR TRANSGENDER PERSONS
 HEALTH CARE FOR TRANSGENDER PERSONS Tim Cavanaugh, MD Medical Director for the Trans Health Program Fenway Health 1 TRANSGENDER refers to a person who is born with the genetic traits of one gender but
HEALTH CARE FOR TRANSGENDER PERSONS Tim Cavanaugh, MD Medical Director for the Trans Health Program Fenway Health 1 TRANSGENDER refers to a person who is born with the genetic traits of one gender but
Patient education for transgender masculinizing hormone therapy
 Date name DOB Patient education for transgender masculinizing hormone therapy o Some transsexual, transgender, and gender non-conforming people choose to take hormone therapy to treat gender dysphoria
Date name DOB Patient education for transgender masculinizing hormone therapy o Some transsexual, transgender, and gender non-conforming people choose to take hormone therapy to treat gender dysphoria
Values Accountability Integrity Service Excellence Innovation Collaboration
 n05586 Transgender and Gender Dysphoria /Gender Incongruence Services Values Accountability Integrity Service Excellence Innovation Collaboration Abstract Purpose: Network Health Plan/Network Health Insurance
n05586 Transgender and Gender Dysphoria /Gender Incongruence Services Values Accountability Integrity Service Excellence Innovation Collaboration Abstract Purpose: Network Health Plan/Network Health Insurance
Disclosures. Endocrine Care of the Transgender Patient. Objectives. Start where you are. Use what you have. Do what you can. Vocabulary.
 Disclosures Endocrine Care of the Transgender Patient Kathryn Tierney, MSN, APRN, FNP-BC Medical Director, Middlesex Hospital Transgender Medicine Program Middlesex Multispecialty Group Division of Endocrinology
Disclosures Endocrine Care of the Transgender Patient Kathryn Tierney, MSN, APRN, FNP-BC Medical Director, Middlesex Hospital Transgender Medicine Program Middlesex Multispecialty Group Division of Endocrinology
Prescribing Guidelines
 Porterbrook Clinic Sheffield Gender Identity Clinic Michael Carlisle Centre 75 Osborne Road Sheffield S11 9BF Version V10 22-01-18 Tel: 0114 271 6671 Fax: 0114 271 8693 Email: Porterbrook@shsc.nhs.uk Website:
Porterbrook Clinic Sheffield Gender Identity Clinic Michael Carlisle Centre 75 Osborne Road Sheffield S11 9BF Version V10 22-01-18 Tel: 0114 271 6671 Fax: 0114 271 8693 Email: Porterbrook@shsc.nhs.uk Website:
Fertility Issues for Transgender Persons. Timothy Cavanaugh, MD Fenway Health
 Fertility Issues for Transgender Persons Timothy Cavanaugh, MD Fenway Health Transgender refers to a person who is born with the genetic traits of one gender but has the internalized identity of another
Fertility Issues for Transgender Persons Timothy Cavanaugh, MD Fenway Health Transgender refers to a person who is born with the genetic traits of one gender but has the internalized identity of another
Client Information for Informed Consent FEMINIZING MEDICATIONS FOR TRANSGENDER CLIENTS
 Client Information for Informed Consent FEMINIZING MEDICATIONS FOR TRANSGENDER CLIENTS Before using medications to transition and feminize, you need to know the possible advantages, disadvantages and risks
Client Information for Informed Consent FEMINIZING MEDICATIONS FOR TRANSGENDER CLIENTS Before using medications to transition and feminize, you need to know the possible advantages, disadvantages and risks
HEALTH: Presented by: Alsean R. Bryant, Pharm.D., AAHIVP AIDS Healthcare Foundation
 HEALTH: Presented by: Alsean R. Bryant, Pharm.D., AAHIVP AIDS Healthcare Foundation 1 The presenter has no actual or potential conflict of interest in relation to this presentation program. 2 Pharmacists:
HEALTH: Presented by: Alsean R. Bryant, Pharm.D., AAHIVP AIDS Healthcare Foundation 1 The presenter has no actual or potential conflict of interest in relation to this presentation program. 2 Pharmacists:
There are four areas where you can expect changes to occur as your hormone therapy progresses.
 You are considering taking testosterone, so you should learn about some of the risks, expectations, long term considerations, and medications associated with medical transition. If is very important to
You are considering taking testosterone, so you should learn about some of the risks, expectations, long term considerations, and medications associated with medical transition. If is very important to
Division: Medical Management Department: Utilization Management
 Retired Date: Page 1 of 1 1. POLICY DESCRIPTION: Gender Reassignment Surgery 2. RESPONSIBLE PARTIES: Medical Management Administration, Utilization Management, Integrated Care Management, Pharmacy, Claims
Retired Date: Page 1 of 1 1. POLICY DESCRIPTION: Gender Reassignment Surgery 2. RESPONSIBLE PARTIES: Medical Management Administration, Utilization Management, Integrated Care Management, Pharmacy, Claims
GUIDELINES FOR THE USE OF FEMINISING HORMONE THERAPY IN GENDER DYSPHORIA. Information for Primary Care December 2015 (Review Date June 2016)
") GUIDELINES FOR THE USE OF FEMINISING HORMONE THERAPY IN GENDER DYSPHORIA Information for Primary Care December 2015 (Review Date June 2016) Further information on this guideline can be obtained from: Claire
GUIDELINES FOR THE USE OF FEMINISING HORMONE THERAPY IN GENDER DYSPHORIA Information for Primary Care December 2015 (Review Date June 2016) Further information on this guideline can be obtained from: Claire
Transgender Medical Benefits
 Transgender Medical Benefits The following Transgender Medical Benefits are based on the Standards of Care published by the World Professional Association for Transgender Health (WPATH). All transgender
Transgender Medical Benefits The following Transgender Medical Benefits are based on the Standards of Care published by the World Professional Association for Transgender Health (WPATH). All transgender
Patient education for transgender feminizing hormone therapy
 Date name DOB Patient education for transgender feminizing hormone therapy o Some transsexual, transgender, and gender non-conforming people choose to take hormone therapy to treat gender dysphoria and
Date name DOB Patient education for transgender feminizing hormone therapy o Some transsexual, transgender, and gender non-conforming people choose to take hormone therapy to treat gender dysphoria and
10/07/18. Conflict of interest statement
 Care: principles, best practices in Europe and how reproductive/sexual health care providers might contribute Petra De Sutter University Hospital Gent Conflict of interest statement My department occasionally
Care: principles, best practices in Europe and how reproductive/sexual health care providers might contribute Petra De Sutter University Hospital Gent Conflict of interest statement My department occasionally
North of Tyne and Gateshead Area Prescribing Committee GUIDELINES FOR THE USE OF FEMINISING HORMONE THERAPY IN GENDER DYSPHORIA
 North of Tyne and Gateshead Area Prescribing Committee GUIDELINES FOR THE USE OF FEMINISING HORMONE THERAPY IN GENDER DYSPHORIA Information for Primary Care July 2014 (Minor update November 2014) (Review
North of Tyne and Gateshead Area Prescribing Committee GUIDELINES FOR THE USE OF FEMINISING HORMONE THERAPY IN GENDER DYSPHORIA Information for Primary Care July 2014 (Minor update November 2014) (Review
Horizon BCBSNJ Uniform Medical Policy Manual Policy Number: 115 Effective Date: 01/01/2017
 Horizon BCBSNJ Uniform Medical Policy Manual Section: Surgery Policy Number: 115 Effective Date: 01/01/2017 Original Policy Date: 05/25/2010 Last Review Date: 05/10/2016 Date Published to Web: 06/23/2010
Horizon BCBSNJ Uniform Medical Policy Manual Section: Surgery Policy Number: 115 Effective Date: 01/01/2017 Original Policy Date: 05/25/2010 Last Review Date: 05/10/2016 Date Published to Web: 06/23/2010
INFORMED CONSENT FOR FEMINIZING HORMONE THERAPY
 INFORMED CONSENT FOR FEMINIZING HORMONE THERAPY The use of hormone therapy for gender transition/affirmation is based on many years of experience treating trans persons. Research on hormone therapy is
INFORMED CONSENT FOR FEMINIZING HORMONE THERAPY The use of hormone therapy for gender transition/affirmation is based on many years of experience treating trans persons. Research on hormone therapy is
Transgender: A broad spectrum of individuals who transiently or persistently identify with a gender different from their natal gender.
 POLICY TITLE: Gender Reassignment Surgery POLICY STATEMENT: Gender reassignment surgery is one treatment option for extreme cases of Gender Dysphoria Disorder. Gender dysphoria disorder (formerly termed
POLICY TITLE: Gender Reassignment Surgery POLICY STATEMENT: Gender reassignment surgery is one treatment option for extreme cases of Gender Dysphoria Disorder. Gender dysphoria disorder (formerly termed
Please note that this should only be used for feedback and comments specifically related to this particular medical policy.
 E-Mail Us Close Please note that this email should only be used for feedback and comments specifically related to this particular medical policy. Horizon BCBSNJ Uniform Medical Policy Manual Section: Surgery
E-Mail Us Close Please note that this email should only be used for feedback and comments specifically related to this particular medical policy. Horizon BCBSNJ Uniform Medical Policy Manual Section: Surgery
8/17/2015. Objectives. Disclosures
 NPANY Annual Conference Niagara Falls, NY October 2015 Laura Markwick, DNP, FNP C Associate Professor Wegmans School of Nursing St Joh Fisher College Objectives The learner will gain an understanding of
NPANY Annual Conference Niagara Falls, NY October 2015 Laura Markwick, DNP, FNP C Associate Professor Wegmans School of Nursing St Joh Fisher College Objectives The learner will gain an understanding of
Gender Health Center, Hormone Clinic th St #201 Sacramento, CA 95817
 MTF Clinical Approach and Protocols Gender Health Center, Hormone Clinic Sacramento, CA Katherine Gardner, MD Revised 11/6/2015 Name and Pronouns: Preferred names and pronouns are used at all times when
MTF Clinical Approach and Protocols Gender Health Center, Hormone Clinic Sacramento, CA Katherine Gardner, MD Revised 11/6/2015 Name and Pronouns: Preferred names and pronouns are used at all times when
All service users will benefit from having the information on these forms. The consent forms may be read in conjunction with the NHS booklet
 INFORMED CONSENT FORMS The following forms are intended to protect both service users and clinicians by ensuring that proper information has been given to service users, and that this is fully understood,
INFORMED CONSENT FORMS The following forms are intended to protect both service users and clinicians by ensuring that proper information has been given to service users, and that this is fully understood,
There are four areas where you can expect changes to occur as your hormone therapy progresses. 1) Physical
 Physical") You are considering taking feminizing hormones, so you should learn about some of the risks, expectations, long term considerations, and medications associated with medical transition. It is very important
You are considering taking feminizing hormones, so you should learn about some of the risks, expectations, long term considerations, and medications associated with medical transition. It is very important
GENder Education and Care Interdisciplinary Support (GENECIS) Feminizing Medications for Patients with Gender Dysphoria
 Feminizing Medications for Patients with Gender Dysphoria") GENder Education and Care Interdisciplinary Support (GENECIS) Feminizing Medications for Patients with Gender Dysphoria Patient Information and Informed Consent and Assent for Minors Before using medications
GENder Education and Care Interdisciplinary Support (GENECIS) Feminizing Medications for Patients with Gender Dysphoria Patient Information and Informed Consent and Assent for Minors Before using medications
Medical Necessity Guidelines: Transgender Surgical Procedures
 Medical Necessity Guidelines: Transgender Surgical Procedures Effective: September 13, 2017 Clinical Documentation and Prior Authorization Required Applies to: Coverage Guideline, No Prior Authorization
Medical Necessity Guidelines: Transgender Surgical Procedures Effective: September 13, 2017 Clinical Documentation and Prior Authorization Required Applies to: Coverage Guideline, No Prior Authorization
Guidelines for the Clinical Care of Persons with Gender Dysphoria
 Guidelines for the Clinical Care of Persons with Gender Dysphoria Friday, May 27, 2016 2:15 5:00 PM 25 th Annual Scientific and Clinical Congress American Association of Clinical Endocrinologist Orlando,
Guidelines for the Clinical Care of Persons with Gender Dysphoria Friday, May 27, 2016 2:15 5:00 PM 25 th Annual Scientific and Clinical Congress American Association of Clinical Endocrinologist Orlando,
Transgender Medicine: Essentials for the Primary Care Provider BENJAMIN J. BOH, DO, MS
 Transgender Medicine: Essentials for the Primary Care Provider BENJAMIN J. BOH, DO, MS ASSISTANT PROFESSOR OF MEDICINE SECTION OF ENDOCRINOLOGY GEISEL SCHOOL OF MEDICINE AT DARTMOUTH Disclosure I will
Transgender Medicine: Essentials for the Primary Care Provider BENJAMIN J. BOH, DO, MS ASSISTANT PROFESSOR OF MEDICINE SECTION OF ENDOCRINOLOGY GEISEL SCHOOL OF MEDICINE AT DARTMOUTH Disclosure I will
Endocrinology and the Transgender Patient
 Endocrinology and the Transgender Patient Matthew Leinung MD Professor of Medicine Albany Medical College This project is supported by the Health Resources and Services Administration (HRSA) of the U.S.
Endocrinology and the Transgender Patient Matthew Leinung MD Professor of Medicine Albany Medical College This project is supported by the Health Resources and Services Administration (HRSA) of the U.S.
A Guide to Hormone Therapy for Trans People available at
 INFORMED CONSENT FORMS The following forms are intended to protect both service users and clinicians by ensuring that proper information has been given to service users, and that this is fully understood,
INFORMED CONSENT FORMS The following forms are intended to protect both service users and clinicians by ensuring that proper information has been given to service users, and that this is fully understood,
Coding... 4 Benefit Application... 6 Description of Services... 7 Clinical Evidence... 8
 Title: TABLE OF CONTENTS Product Variations.... 1 Policy Statement.... 1 Related Policies.... 3 Policy Guidelines..... 3 Coding.... 4 Benefit Application........ 6 Description of Services..... 7 Clinical
Title: TABLE OF CONTENTS Product Variations.... 1 Policy Statement.... 1 Related Policies.... 3 Policy Guidelines..... 3 Coding.... 4 Benefit Application........ 6 Description of Services..... 7 Clinical
Care for Transgender Patient: Providing Competent and Compassionate Care During a Time of Transition
 Care for Transgender Patient: Providing Competent and Compassionate Care During a Time of Transition Jessica Francis, MD Assistant Professor Department of Obstetrics and Gynecology Froedtert and the Medical
Care for Transgender Patient: Providing Competent and Compassionate Care During a Time of Transition Jessica Francis, MD Assistant Professor Department of Obstetrics and Gynecology Froedtert and the Medical
Information About Hormonal Treatment for Trans women
 Information About Hormonal Treatment for Trans women Leighton J Seal PhD FRCP Consultant Endocrinologist, Gender Identity Clinic, (Charing Cross) West London Mental Health NHS Trust 12/12/2016 1 Introduction...
Information About Hormonal Treatment for Trans women Leighton J Seal PhD FRCP Consultant Endocrinologist, Gender Identity Clinic, (Charing Cross) West London Mental Health NHS Trust 12/12/2016 1 Introduction...
Reproductive System. Testes. Accessory reproductive organs. gametogenesis hormones. Reproductive tract & Glands
 Reproductive System Testes gametogenesis hormones Accessory reproductive organs Reproductive tract & Glands transport gametes provide nourishment for gametes Hormonal regulation in men Hypothalamus - puberty
Reproductive System Testes gametogenesis hormones Accessory reproductive organs Reproductive tract & Glands transport gametes provide nourishment for gametes Hormonal regulation in men Hypothalamus - puberty
A Guide to Masculinizing Hormones Gender Affirming Care
 Patient and Family Education A Guide to Masculinizing Hormones Gender Affirming Care Hormone therapy is an option that can help transgender people feel more comfortable in their bodies. Like other medical
Patient and Family Education A Guide to Masculinizing Hormones Gender Affirming Care Hormone therapy is an option that can help transgender people feel more comfortable in their bodies. Like other medical
Information About Hormonal Treatment for Trans men
 Information About Hormonal Treatment for Trans men Leighton J Seal PhD FRCP Consultant Endocrinologist, Gender Identity Clinic, (Charing Cross) West London Mental Health NHS Trust 12/12/2016 Introduction...
Information About Hormonal Treatment for Trans men Leighton J Seal PhD FRCP Consultant Endocrinologist, Gender Identity Clinic, (Charing Cross) West London Mental Health NHS Trust 12/12/2016 Introduction...
Medical Policy. Transgender Reassignment Surgery. Policy Number: Policy History
 Policy Number: 1069 Policy History Approve Date: 06/01/2018 Effective Date: 06/01/2018 Preauthorization All Plans Benefit plans vary in coverage and some plans may not provide coverage for certain service(s)
Policy Number: 1069 Policy History Approve Date: 06/01/2018 Effective Date: 06/01/2018 Preauthorization All Plans Benefit plans vary in coverage and some plans may not provide coverage for certain service(s)
NHS MEDICAL POLICY. Transgender Surgical Procedures Procedure
 Effective Date: 12/13/2017 NHS MEDICAL POLICY Transgender Surgical Procedures Procedure 2017-003 Transgender surgical procedures may be indicated when ALL of the following are present: 1 The member is
Effective Date: 12/13/2017 NHS MEDICAL POLICY Transgender Surgical Procedures Procedure 2017-003 Transgender surgical procedures may be indicated when ALL of the following are present: 1 The member is
CITY AND COUNTY OF SAN FRANCISCO
 CITY AND COUNTY OF SAN FRANCISCO Department of Public Health Transgender Health Services 50 Lech Walesa Street San Francisco, CA 94102 Telephone: (415) 355-7498 FAX: (415) 355-7407 transgenderhealthservices@sfdph.org
CITY AND COUNTY OF SAN FRANCISCO Department of Public Health Transgender Health Services 50 Lech Walesa Street San Francisco, CA 94102 Telephone: (415) 355-7498 FAX: (415) 355-7407 transgenderhealthservices@sfdph.org
Corporate Medical Policy
 Corporate Medical Policy Gender Confirmation Surgery and Hormone Therapy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: gender_confirmation_surgery_and_hormone_therapy 7/2011 5/2018
Corporate Medical Policy Gender Confirmation Surgery and Hormone Therapy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: gender_confirmation_surgery_and_hormone_therapy 7/2011 5/2018
State of California, California Health and Human Services Agency, Department of Managed Health Care 2013:
 This policy has been developed through review of medical literature, consideration of medical necessity, generally accepted medical practice standards, and approved by the IEHP Pharmacy and Therapeutics
This policy has been developed through review of medical literature, consideration of medical necessity, generally accepted medical practice standards, and approved by the IEHP Pharmacy and Therapeutics
Transgender Sexual Health. Dr Tara Suchak CliniQ / 56 Dean Street
 Transgender Sexual Health Dr Tara Suchak CliniQ / 56 Dean Street Contents Introduction to Transgender Issues Introduction to CliniQ Trans Men Trans Women The Future.. https://cliniq.org.uk Every Wednesday
Transgender Sexual Health Dr Tara Suchak CliniQ / 56 Dean Street Contents Introduction to Transgender Issues Introduction to CliniQ Trans Men Trans Women The Future.. https://cliniq.org.uk Every Wednesday
Sexual dysfunction of chronic kidney disease. Razieh salehian.md psychiatrist
 Sexual dysfunction of chronic kidney disease Razieh salehian.md psychiatrist Disturbances in sexual function are a common feature of chronic renal failure. Sexual dysfunction is inversely associated with
Sexual dysfunction of chronic kidney disease Razieh salehian.md psychiatrist Disturbances in sexual function are a common feature of chronic renal failure. Sexual dysfunction is inversely associated with
Jamie Feldman M.D., Ph.D. Dept. of Family Medicine/Program in Human Sexuality University of Minnesota
 Jamie Feldman M.D., Ph.D. Dept. of Family Medicine/Program in Human Sexuality University of Minnesota University of Illinois, Urbana-Champaign Urbana, IL February 9, 2016 } MSP from 1984-1993 PhD in Anthropology
Jamie Feldman M.D., Ph.D. Dept. of Family Medicine/Program in Human Sexuality University of Minnesota University of Illinois, Urbana-Champaign Urbana, IL February 9, 2016 } MSP from 1984-1993 PhD in Anthropology
Guidelines for the Clinical Care of Persons with Gender Dysphoria
 Guidelines for the Clinical Care of Persons with Gender Dysphoria Friday, May 27, 2016 2:15 5:00 PM 25 th Annual Scientific and Clinical Congress American Association of Clinical Endocrinologist Orlando,
Guidelines for the Clinical Care of Persons with Gender Dysphoria Friday, May 27, 2016 2:15 5:00 PM 25 th Annual Scientific and Clinical Congress American Association of Clinical Endocrinologist Orlando,
12/13/2017. Important references for PCOS. Polycystic Ovarian Syndrome (PCOS) for the Family Physician. 35 year old obese woman
 for the Family Physician. 35 year old obese woman") Polycystic Ovarian Syndrome (PCOS) for the Family Physician Barbara S. Apgar MD, MS Professor or Family Medicine University of Michigan Ann Arbor, Michigan Important references for PCOS Endocrine Society
Polycystic Ovarian Syndrome (PCOS) for the Family Physician Barbara S. Apgar MD, MS Professor or Family Medicine University of Michigan Ann Arbor, Michigan Important references for PCOS Endocrine Society
TESTOSTERONE DEFINITION
 DEFINITION A hormone that is a hydroxyl steroid ketone (C19H28O2) produced especially by the testes or made synthetically and that is responsible for inducing and maintaining male secondary sex characteristics.
DEFINITION A hormone that is a hydroxyl steroid ketone (C19H28O2) produced especially by the testes or made synthetically and that is responsible for inducing and maintaining male secondary sex characteristics.
Pharmacy Policy. Adult transgender hormonal therapy may be approved when all of the following criteria are met:
 Pharmacy Policy Class: Transgender Hormonal Treatment for Adults Line of Business: Medi-Cal Effective date: February 15, 2017 Revision date: February 15, 2017 This policy has been developed through review
Pharmacy Policy Class: Transgender Hormonal Treatment for Adults Line of Business: Medi-Cal Effective date: February 15, 2017 Revision date: February 15, 2017 This policy has been developed through review
TRANSGENDER HEALTHCARE Barry Zevin, MD Conrad Wenzel, MSW
 TRANSGENDER HEALTHCARE Barry Zevin, MD Conrad Wenzel, MSW Disclosures Dr. Zevin is an employee of the San Francisco Department of Public Health There are no other relevant financial or personal relationships
TRANSGENDER HEALTHCARE Barry Zevin, MD Conrad Wenzel, MSW Disclosures Dr. Zevin is an employee of the San Francisco Department of Public Health There are no other relevant financial or personal relationships
Case Studies in Primary care
 Case Studies in Primary care Holistic care of Transgender and Gender-nonconforming People Katy Kropf DO Ohio University Heritage College of Osteopathic medicine pronouns she/her/hers kropf@ohio.edu My
Case Studies in Primary care Holistic care of Transgender and Gender-nonconforming People Katy Kropf DO Ohio University Heritage College of Osteopathic medicine pronouns she/her/hers kropf@ohio.edu My
Trust Women Seattle Client Information for Informed Consent MASCULIZING MEDICATIONS FOR TRANSGENDER CLIENTS
 Client Information for Informed Consent MASCULIZING MEDICATIONS FOR TRANSGENDER CLIENTS Before using medications to transition and Masculinize, you need to know the possible advantages, disadvantages and
Client Information for Informed Consent MASCULIZING MEDICATIONS FOR TRANSGENDER CLIENTS Before using medications to transition and Masculinize, you need to know the possible advantages, disadvantages and
MODULE 1 F E M I N I Z I N G
 MODULE 1 F E M I N I Z I N G MODULE 1 MEDICAL TRANSITION - FEMINIZING Objectives: Describe the basic science underpinning feminizing gender hormonal transition List the pharmacologic options including
MODULE 1 F E M I N I Z I N G MODULE 1 MEDICAL TRANSITION - FEMINIZING Objectives: Describe the basic science underpinning feminizing gender hormonal transition List the pharmacologic options including
Medi-Cal, Healthy Workers, Healthy Kids
 Disclaimer: Criteria may change as the state and Medi-Cal update current regulations for transgender services Department Owner: Lines of Business Affected: Utilization Management Medi-Cal, Healthy Workers,
Disclaimer: Criteria may change as the state and Medi-Cal update current regulations for transgender services Department Owner: Lines of Business Affected: Utilization Management Medi-Cal, Healthy Workers,
Department of Pediatrics
 Page 1 of 5 What is testosterone? Consent Form: MASCULINIZING MEDICATIONS You want to take testosterone to masculinize your body. Before taking it, there are several things you need to know about. They
Page 1 of 5 What is testosterone? Consent Form: MASCULINIZING MEDICATIONS You want to take testosterone to masculinize your body. Before taking it, there are several things you need to know about. They
Gender Identity Services
 Gender Identity Services www.sandyford.org 2 Contents Welcome to Sandyford....... 4 The Gender Identity Clinic...... 4 Treatment Options for Transsexual Women Male to Female (MTF)........ 6 Treatment Options
Gender Identity Services www.sandyford.org 2 Contents Welcome to Sandyford....... 4 The Gender Identity Clinic...... 4 Treatment Options for Transsexual Women Male to Female (MTF)........ 6 Treatment Options
Transgender Populations
 Treating HIV in Transgender Patients: A Clinical Update Tonia Poteat, PhD, MPH, PA-C Physician Assistant, JHMI Assistant Professor, JHSPH 18 November 2016 Transgender Populations Transgender (trans): people
Treating HIV in Transgender Patients: A Clinical Update Tonia Poteat, PhD, MPH, PA-C Physician Assistant, JHMI Assistant Professor, JHSPH 18 November 2016 Transgender Populations Transgender (trans): people
Hormonal Control of Human Reproduction
 Hormonal Control of Human Reproduction Bởi: OpenStaxCollege The human male and female reproductive cycles are controlled by the interaction of hormones from the hypothalamus and anterior pituitary with
Hormonal Control of Human Reproduction Bởi: OpenStaxCollege The human male and female reproductive cycles are controlled by the interaction of hormones from the hypothalamus and anterior pituitary with
Providing Primary Care for Gender-Diverse Clients. Seaway Valley Community Health Centre June 30 th, 2016 Jennifer Douek, Jordan Zaitzow
 Providing Primary Care for Gender-Diverse Clients Seaway Valley Community Health Centre June 30 th, 2016 Jennifer Douek, Jordan Zaitzow Introductions Jennifer Douek, MD Jordan Zaitzow, MSW Faculty / Presenter
Providing Primary Care for Gender-Diverse Clients Seaway Valley Community Health Centre June 30 th, 2016 Jennifer Douek, Jordan Zaitzow Introductions Jennifer Douek, MD Jordan Zaitzow, MSW Faculty / Presenter
Therapeutic Cohort Results
 Patient: PAGE LOVE DOB: January 11, 1983 Sex: F MRN: 1232704193 Order Number: J9020008 Completed: July 08, 2016 Received: July 02, 2016 Collected: July 01, 2016 Aum Healing Center Sarika Arora MD 332 Newbury
Patient: PAGE LOVE DOB: January 11, 1983 Sex: F MRN: 1232704193 Order Number: J9020008 Completed: July 08, 2016 Received: July 02, 2016 Collected: July 01, 2016 Aum Healing Center Sarika Arora MD 332 Newbury
Hypogonadism 4/27/2018. Male Hypogonadism -- Definition. Epidemiology. Objectives HYPOGONADISM. Men with Hypogonadism. 95% untreated.
 Male Hypogonadism -- Definition - Low T, Low Testosterone Hypogonadism -...a clinical syndrome that results from failure of the testes to produce physiological concentrations of testosterone due to pathology
Male Hypogonadism -- Definition - Low T, Low Testosterone Hypogonadism -...a clinical syndrome that results from failure of the testes to produce physiological concentrations of testosterone due to pathology
Information on Feminizing Medications
 201 Plageman Building 108 SW Memorial Place Corvallis, Oregon 97331 P 541-737-9355 F 541-737-9694 studenthealth@oregonstate.edu Information on Feminizing Medications Persons in the male-to-female spectrum
201 Plageman Building 108 SW Memorial Place Corvallis, Oregon 97331 P 541-737-9355 F 541-737-9694 studenthealth@oregonstate.edu Information on Feminizing Medications Persons in the male-to-female spectrum
Outline. Male Reproductive System Testes and Sperm Hormonal Regulation
 Outline Male Reproductive System Testes and Sperm Hormonal Regulation Female Reproductive System Genital Tract Hormonal Levels Uterine Cycle Fertilization and Pregnancy Control of Reproduction Infertility
Outline Male Reproductive System Testes and Sperm Hormonal Regulation Female Reproductive System Genital Tract Hormonal Levels Uterine Cycle Fertilization and Pregnancy Control of Reproduction Infertility
Information on Testosterone Therapy
 Information on Testosterone Therapy 201 Plageman Building 108 SW Memorial Place Corvallis, Oregon 97331 P 541-737-9355 F 541-737-9694 studenthealth@oregonstate.edu Persons in the female-to-male spectrum
Information on Testosterone Therapy 201 Plageman Building 108 SW Memorial Place Corvallis, Oregon 97331 P 541-737-9355 F 541-737-9694 studenthealth@oregonstate.edu Persons in the female-to-male spectrum
A Guide to Feminizing Hormones Gender Affirming Care
 Patient and Family Education A Guide to Feminizing Hormones Gender Affirming Care Hormone therapy is an option that can help transgender people feel more comfortable in their bodies. Like other medical
Patient and Family Education A Guide to Feminizing Hormones Gender Affirming Care Hormone therapy is an option that can help transgender people feel more comfortable in their bodies. Like other medical
Male Hypogonadism. Types and causes of hypogonadism. What is male hypogonadism? Symptoms. Testosterone production. Patient Information.
 Patient Information English 31 Male Hypogonadism The underlined terms are listed in the glossary. What is male hypogonadism? Male hypogonadism means the testicles do not produce enough of the male sex
Patient Information English 31 Male Hypogonadism The underlined terms are listed in the glossary. What is male hypogonadism? Male hypogonadism means the testicles do not produce enough of the male sex
CLIENT INFORMATION and INFORMED CONSENT TESTOSTERONE THERAPY
 CLIENT INFORMATION and INFORMED CONSENT TESTOSTERONE THERAPY This form explains the use of testosterone for someone who wishes to become more masculine as part of a gender transitioning process. Testosterone
CLIENT INFORMATION and INFORMED CONSENT TESTOSTERONE THERAPY This form explains the use of testosterone for someone who wishes to become more masculine as part of a gender transitioning process. Testosterone
Transgender Health Cases from the Transgender and Intersex Specialty Care Clinic
 Transgender Health Cases from the Transgender and Intersex Specialty Care Clinic Caroline Davidge-Pitts, MD Todd B Nippoldt, MD Department of Endocrinology, Diabetes, Nutrition Mayo Clinic, Rochester 2017
Transgender Health Cases from the Transgender and Intersex Specialty Care Clinic Caroline Davidge-Pitts, MD Todd B Nippoldt, MD Department of Endocrinology, Diabetes, Nutrition Mayo Clinic, Rochester 2017
Endocrine Treatment of Gender-Dysphoric/ Gender-Incongruent Persons: An Endocrine Society Clinical Practice Guideline. Education Module June, 2017
 Endocrine Treatment of Gender-Dysphoric/ Gender-Incongruent Persons: An Endocrine Society Clinical Practice Guideline Education Module June, 2017 Introduction Wylie C. Hembree, MD Associate Attending Physician
Endocrine Treatment of Gender-Dysphoric/ Gender-Incongruent Persons: An Endocrine Society Clinical Practice Guideline Education Module June, 2017 Introduction Wylie C. Hembree, MD Associate Attending Physician
Biology of Reproduction-Biol 326
 Biology of Reproduction-Biol 326 READ ALL INSTRUCTIONS CAREFULLY. ANSWER ALL THE QUESTIONS ON THE ANSWER SHEET. THE ANSWER ON THE ANSWER SHEET IS YOUR OFFICIAL ANSWER REGARDLESS OF WHAT YOU MARK ON THE
Biology of Reproduction-Biol 326 READ ALL INSTRUCTIONS CAREFULLY. ANSWER ALL THE QUESTIONS ON THE ANSWER SHEET. THE ANSWER ON THE ANSWER SHEET IS YOUR OFFICIAL ANSWER REGARDLESS OF WHAT YOU MARK ON THE
Informed Consent Form for Feminizing Medications
 Student Health Services Oregon State University, 201 Plageman Building, Corvallis, Oregon 97331-8567 Tel 541-737-9355 General Fax 541-737-4530 Medical Fax 541-737-9665 http://studenthealth.oregonstate.edu/
Student Health Services Oregon State University, 201 Plageman Building, Corvallis, Oregon 97331-8567 Tel 541-737-9355 General Fax 541-737-4530 Medical Fax 541-737-9665 http://studenthealth.oregonstate.edu/
Therapeutic Cohort Results
 Patient: SAMPLE PATIENT DOB: Sex: MRN: Menopause Plus - Salivary Profile Therapeutic Cohort Results Hormone Average Result QUINTILE DISTRIBUTION 1st 2nd 3rd 4th 5th Therapeutic Range* Estradiol (E2) 8.7
Patient: SAMPLE PATIENT DOB: Sex: MRN: Menopause Plus - Salivary Profile Therapeutic Cohort Results Hormone Average Result QUINTILE DISTRIBUTION 1st 2nd 3rd 4th 5th Therapeutic Range* Estradiol (E2) 8.7
DISCLOSURES LEARNING OBJECTIVES. 21st Century Strategies: Transgender Hormone Care. Patient/PCP. Medical model
 21st Century Strategies: Transgender Hormone Care DISCLOSURES Joshua Safer, MD Center for Transgender Medicine and Surgery No conflicts of interest Just about the entire talk is "off label" LEARNING OBJECTIVES
21st Century Strategies: Transgender Hormone Care DISCLOSURES Joshua Safer, MD Center for Transgender Medicine and Surgery No conflicts of interest Just about the entire talk is "off label" LEARNING OBJECTIVES
Treatment of hirsutism with a gonadotropin-releasing hormone agonist and estrogen replacement therapy*
 Gynecology-endocrinology FERTILITY AND STERILITY Copyright 1994 The American Fertility Society Printed on acid-free paper in U S. A. Treatment of hirsutism with a gonadotropin-releasing hormone agonist
Gynecology-endocrinology FERTILITY AND STERILITY Copyright 1994 The American Fertility Society Printed on acid-free paper in U S. A. Treatment of hirsutism with a gonadotropin-releasing hormone agonist
THE YEAR IN REVIEW: SURGERY. Marta Bizic Faculty of Medicine, University of Belgrade, Serbia Belgrade Center for Genital Reconstructive Surgery
 THE YEAR IN REVIEW: SURGERY Marta Bizic Faculty of Medicine, University of Belgrade, Serbia Belgrade Center for Genital Reconstructive Surgery Conflict of interest I have no potential conflict of interest
THE YEAR IN REVIEW: SURGERY Marta Bizic Faculty of Medicine, University of Belgrade, Serbia Belgrade Center for Genital Reconstructive Surgery Conflict of interest I have no potential conflict of interest
Prof.Dr. Nabil Lymon Head of Internal Medicine Department
 By Prof.Dr. Nabil Lymon Head of Internal Medicine Department Definitions: Hirsutism: Is the presence of terminal hair in androgendependent sites where hair does not normally grow in women. This hair growth
By Prof.Dr. Nabil Lymon Head of Internal Medicine Department Definitions: Hirsutism: Is the presence of terminal hair in androgendependent sites where hair does not normally grow in women. This hair growth
Symptom Management. Fertility and You
 Symptom Management Fertility and You Table of Contents 3 Will cancer impact my ability to have children? 4 How do I talk to my children about preserving their fertility during cancer treatment? 5 What
Symptom Management Fertility and You Table of Contents 3 Will cancer impact my ability to have children? 4 How do I talk to my children about preserving their fertility during cancer treatment? 5 What
FLASH CARDS. Kalat s Book Chapter 11 Alphabetical
 FLASH CARDS www.biologicalpsych.com Kalat s Book Chapter 11 Alphabetical alpha-fetoprotein alpha-fetoprotein Alpha-Fetal Protein (AFP) or alpha-1- fetoprotein. During a prenatal sensitive period, estradiol
FLASH CARDS www.biologicalpsych.com Kalat s Book Chapter 11 Alphabetical alpha-fetoprotein alpha-fetoprotein Alpha-Fetal Protein (AFP) or alpha-1- fetoprotein. During a prenatal sensitive period, estradiol
Hormone Replacement Therapy For Men Consultation Information
 Hormone Replacement Therapy For Men Consultation Information www.urologyaustin.com Biological Aging and Hormones As we age, a natural degeneration and aging of organs causes the levels of our hormones
Hormone Replacement Therapy For Men Consultation Information www.urologyaustin.com Biological Aging and Hormones As we age, a natural degeneration and aging of organs causes the levels of our hormones
Arti Barnes MD MPH Tuesday AM series ENCOMPASSING THE MARGINALIZED: CARE FOR THE TRANSGENDER COMMUNITY
 Arti Barnes MD MPH Tuesday AM series 9-29-2015 ENCOMPASSING THE MARGINALIZED: CARE FOR THE TRANSGENDER COMMUNITY Disclosures None Objectives Increase awareness of HIV and STD epidemiology among Transgenders
Arti Barnes MD MPH Tuesday AM series 9-29-2015 ENCOMPASSING THE MARGINALIZED: CARE FOR THE TRANSGENDER COMMUNITY Disclosures None Objectives Increase awareness of HIV and STD epidemiology among Transgenders
Transgender. Transgender Health and HIV. Transgender Terminology. Gender Identity & Sexual Orientation 12/8/17
 Transgender Transgender Health and HIV Madeline B. Deutsch, MD, MPH Associate Professor of Clinical Family & Community Medicine Director, UCSF Transgender Care Center of Excellence for Transgender Health
Transgender Transgender Health and HIV Madeline B. Deutsch, MD, MPH Associate Professor of Clinical Family & Community Medicine Director, UCSF Transgender Care Center of Excellence for Transgender Health
Caring for Trans and Gender Diverse Clients in BC: A Primary Care Toolkit
 March 2017 Caring for Trans and Gender Diverse Clients in BC: A Primary Care Toolkit Version 1.0 Contents Table of Contents...i Acknowledgment and Disclaimer...ii Introduction... 1 Gender affirming health
March 2017 Caring for Trans and Gender Diverse Clients in BC: A Primary Care Toolkit Version 1.0 Contents Table of Contents...i Acknowledgment and Disclaimer...ii Introduction... 1 Gender affirming health
One Day Hormone Check
 One Day Hormone Check DOB: Sex: F MRN: Order Number: Completed: Received: Collected: Salivary Hormone Results Estradiol pmol/l >3330.0 Testosterone pmol/l
One Day Hormone Check DOB: Sex: F MRN: Order Number: Completed: Received: Collected: Salivary Hormone Results Estradiol pmol/l >3330.0 Testosterone pmol/l
Transgender Services Corporate Medical Policy
 Transgender Services Corporate Medical Policy File name: Transgender Services File Code: UM.SURG.06 Origination: 5/30/2011 Last Review: 06/2017 Next Review: 06/2018 Effective Date: 09/01/2017 Policy Coding
Transgender Services Corporate Medical Policy File name: Transgender Services File Code: UM.SURG.06 Origination: 5/30/2011 Last Review: 06/2017 Next Review: 06/2018 Effective Date: 09/01/2017 Policy Coding
Why do I need any hormone replacement? What is Menopause? What symptoms are treated by estrogen Injections?
 1 Why do I need any hormone replacement? Women need replacement if they desire to: Delay the symptoms of aging Reverse depression and anxiety Regain libido Preserve skin and muscle tone Look younger Increase
1 Why do I need any hormone replacement? Women need replacement if they desire to: Delay the symptoms of aging Reverse depression and anxiety Regain libido Preserve skin and muscle tone Look younger Increase
Disclosures. Overview: How did I get Here? Pfizer Safe Medical Designs (SMD) MLM Medicus, LLC. Current Concepts in Caring for Transgender Patients
 MLM Medicus, LLC. Current Concepts in Caring for Transgender Patients") Disclosures Pfizer Safe Medical Designs (SMD) MLM Medicus, LLC Current Concepts in Caring for Transgender Patients No financial relationships relevant to this presentation to disclose UCSF Controversies
Disclosures Pfizer Safe Medical Designs (SMD) MLM Medicus, LLC Current Concepts in Caring for Transgender Patients No financial relationships relevant to this presentation to disclose UCSF Controversies
When testes make no testosterone: Identifying a rare cause of 46, XY female phenotype in adulthood
 When testes make no testosterone: Identifying a rare cause of 46, XY female phenotype in adulthood Gardner DG, Shoback D. Greenspan's Basic & Clinical Endocrinology, 10e; 2017 Sira Korpaisarn, MD Endocrinology
When testes make no testosterone: Identifying a rare cause of 46, XY female phenotype in adulthood Gardner DG, Shoback D. Greenspan's Basic & Clinical Endocrinology, 10e; 2017 Sira Korpaisarn, MD Endocrinology
Reproductive Health and Pituitary Disease
 Reproductive Health and Pituitary Disease Janet F. McLaren, MD Assistant Professor Division of Reproductive Endocrinology and Infertility Department of Obstetrics and Gynecology jmclaren@uabmc.edu Objectives
Reproductive Health and Pituitary Disease Janet F. McLaren, MD Assistant Professor Division of Reproductive Endocrinology and Infertility Department of Obstetrics and Gynecology jmclaren@uabmc.edu Objectives
Polycystic Ovary Syndrome HEATHER BURKS, MD OU PHYSICIANS REPRODUCTIVE MEDICINE SEPTEMBER 21, 2018
 Polycystic Ovary Syndrome HEATHER BURKS, MD OU PHYSICIANS REPRODUCTIVE MEDICINE SEPTEMBER 21, 2018 Learning Objectives At the conclusion of this lecture, learners should: 1) Know the various diagnostic
Polycystic Ovary Syndrome HEATHER BURKS, MD OU PHYSICIANS REPRODUCTIVE MEDICINE SEPTEMBER 21, 2018 Learning Objectives At the conclusion of this lecture, learners should: 1) Know the various diagnostic
Cancer and Fertility Ashley Munchel, MD Assistant Professor of Pediatrics University of Maryland Medical Center
 Cancer and Fertility Ashley Munchel, MD Assistant Professor of Pediatrics University of Maryland Medical Center Trends in Pediatric Cancer Incidence Rates by Site, Ages Birth to 19 Years, 1975 to 2010.
Cancer and Fertility Ashley Munchel, MD Assistant Professor of Pediatrics University of Maryland Medical Center Trends in Pediatric Cancer Incidence Rates by Site, Ages Birth to 19 Years, 1975 to 2010.
MULTIPLE CHOICE. Choose the one alternative that best completes the statement or answers the question.
 MULTIPLE CHOICE. Choose the one alternative that best completes the statement or answers the question. 1) Which of the following hormones controls the release of anterior pituitary gonadotropins? A) LH
MULTIPLE CHOICE. Choose the one alternative that best completes the statement or answers the question. 1) Which of the following hormones controls the release of anterior pituitary gonadotropins? A) LH
Index. urologic.theclinics.com. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Acquired hypogonadism, prevalence of, 165 167 primary, 165 secondary, 167 Adipose tissue, as an organ, 240 241 Adrenal hyperplasia, congenital,
Note: Page numbers of article titles are in boldface type. A Acquired hypogonadism, prevalence of, 165 167 primary, 165 secondary, 167 Adipose tissue, as an organ, 240 241 Adrenal hyperplasia, congenital,
What is PCOS? PCOS THE CONQUER PCOS E-BOOK. You'll be amazed when you read this...
 PCOS What is PCOS? You'll be amazed when you read this... What is PCOS?. Who is at risk? How to get tested? What are the complications. Is there a cure? What are the right ways to eat? What lifestyle changes
PCOS What is PCOS? You'll be amazed when you read this... What is PCOS?. Who is at risk? How to get tested? What are the complications. Is there a cure? What are the right ways to eat? What lifestyle changes
patient education Fact Sheet
 patient education Fact Sheet PFS007: BRCA1 and BRCA2 Mutations OCTOBER 2017 BRCA1 and BRCA2 Mutations Cancer is caused by several different factors. A few types of cancer run in families. These types are
patient education Fact Sheet PFS007: BRCA1 and BRCA2 Mutations OCTOBER 2017 BRCA1 and BRCA2 Mutations Cancer is caused by several different factors. A few types of cancer run in families. These types are
What to do about infertility?
 What to do about infertility? Dr. M.A. Fischer Section Head, Division of Urology, Department of Surgery Assistant Clinical Professor, Department of Obstetrics and Gynecology Hamilton Health Sciences, Hamilton,
What to do about infertility? Dr. M.A. Fischer Section Head, Division of Urology, Department of Surgery Assistant Clinical Professor, Department of Obstetrics and Gynecology Hamilton Health Sciences, Hamilton,