If you would like bypass the presentation for the summary, right click on your mouse and go to slide # 138. Enjoy
|
|
|
- Clare Cecilia Sullivan
- 5 years ago
- Views:
Transcription
1 Welcome This is an online version of a presentation given by Dr Keith Merritt. Its purpose is to give a balanced review of the risks, benefits and alternative treatments for the changes and symptoms of female menopause. We hope you find it helpful.
2 If you would like bypass the presentation for the summary, right click on your mouse and go to slide # 138. Enjoy
3 Depression, Hot Flashes, Insomnia Are there safe treatment options for symptomatic midlife women?
4 The Basics
5 Common Abbreviations HRT- Hormone Replacement Therapy CHD- Coronary Heart Disease HERS- Heart Estrogen/Progesterone Replacement Study WHI- Women s Health Initiative (Study) mcgm- micrograms
6 Common Terms Premarin- - a mixture of estrogens isolated from the urine of pregnant mares. The most well studied estrogen HRT Provera- - a synthetic progesterone. Again, the most well studied progesterone HRT Estradiol- - the form of estrogen that actually acts in the body. All types of estrogen HRT are eventually converted to this by the body before they act on the body s estrogen receptors.
7 Common Terms DVT- - deep vein thrombosis -a blood clot forming in a deep vein Thromboembolism- - a blood clot either forming in or breaking free from a clot in a deep vein and flowing to an artery in the lungs
8 What is Menopause?
9 Menopause is A natural transition The end of fertility A loss of estrogen production by the ovaries A change in the estrogen dependant parts of a woman s body
10 Menopause is Not A disease An estrogen deficient state that requires replacement to prevent illness
11 Postmenopausal When there has been no menstrual flow for one year
12 What is a Hormone? A chemical messenger -Secreted by one body part -Directs the function of other body parts
13 Hormones Affected by Menopause Estrogen Progesterone Testosterone
14 Estrogen The hormone whose loss at menopause is most associated with the symptoms of menopause Symptoms are caused more by blood level fluctuations than by the actual levels Body changes of menopause are due to the actual levels Majority is made by the ovaries Some is produced by conversion of male type hormones, made by the ovary and adrenal gland, to weak estrogens by the body s fatty tissue
15 Progesterone Produced by the ovaries during each monthly cycle after the egg is released Purpose is to work with estrogen to provide a healthy lining in the uterus for implantation of a fertilized egg Replacement may help some menopausal symptoms Not given as part of hormone replacement in women who have had a hysterectomy Required as part of hormone replacement regimen in women with a uterus to prevent the estrogen replacement from causing cancer of the uterine lining (endometrial cancer)
16 Testosterone Responsible for a woman s libido 50% is made by the ovaries Blood levels peak each month with ovulation Ovarian production typically continues until age 65 years May or may not be an issue in those who have their ovaries surgically removed
17 The Ovary
18 Analogous to a man s testicle Contain around 1 million eggs at birth During fertile years a small number of eggs are recruited each month for ovulation One dominant egg is then released each month In the late 30 s, there is a very large increase in number of eggs recruited for each cycle Eggs are depleted in the early 50 s- menopause
19
20 The ovary is driven by the brain Glands in the brain produce hormones that direct hormone secretion by the ovary Ovarian hormones then feedback and mediate the brains hormone secretions The hypothalamus, the part of the brain that controls both body temperature and most hormone secretions, is affected by changes in ovarian hormone levels
21 Ovarian hormones act on the uterus over a 28 day cycle During the first half of the cycle, the ovary produces estrogen which thickens the lining of the uterus (endometrium) An egg is released around mid-cycle After an egg is released, the ovary makes both estrogen and progesterone Progesterone organizes the thickened lining in preparation for a fertilized egg to implant
22 If the uterine lining is exposed to estrogen without any progesterone exposure for a prolonged period of time it may develop endometrial hyperplasia (uncontrolled growth) which can in time progress to cancer- the reason all abnormal bleeding requires a biopsy
23 Historical Views of HRT 1930 s- expensive miracle 1960 s- critical to remaining feminine 1970 s- endometrial cancer scare 1980 s- hormones keep your bones strong 1990 s- hormones prevent heart attacks 2000 s- hormones will kill you Perhaps a more balanced, informed view
24 2014 Common View During menopause, I have only two options 1- Stay off hormones and want to die 2- Take hormones and die
25 Makes one feel a bit like a squirrel caught in the middle of the road
26 History of Hormone Replacement
27 1930 s- estrogen therapy began -isolated originally from the urine of pregnant women -later pregnant mares were, and continue to be, used for conjugated estrogens (premarin) 1960 s- rapid expansion of use
28 Feminine Forever - Dr Robert Wilson 1966 best seller Nationwide lecture tour menopause is completely preventable every woman alive today has the option to remain feminine forever
29 Dr Robert Wilson Financed by a major pharmaceutical company (guess what they made)
30 Women s Health Advocates 1950 s- began raising safety questions 1970 s- linked to endometrial cancer -reason why pro(gesterone) is in prempro
31 Women and the Crisis in Sex Hormones 1977 bestseller -Barbara Seaman Raised questions about risk of HRT -Breast cancer, blood clots, stroke Warned against over-promotion
32 But One book was no match for a multimillion dollar drug industry
33 Decades that followed Drug companies pushed & doctors prescribed increasing numbers of hormones for broad range of ailments and conditions associated with aging
34 FDA Approved Uses Initially only for treatment of symptoms -not disease prevention approved for osteoporosis prevention concluded- evidence did not support use for CHD prevention
35 But then, who really cares what the FDA thinks?
36 Seriously Who really cares what the FDA thinks?
37 Against a backdrop of multiple small, poor quality studies with conflicting results, hormones became the most widely prescribed drugs in the world
38 1980 s & 1990 s Widespread belief within medical community that postmenopausal women absolutely needed hormones to prevent heart attacks
39 The momentum behind this belief was the observation that very few women had heart attacks until after menopause. After menopause they then rapidly began approaching the rates of heart attacks in men.
40 Well designed trial HERS Trial Intention was to show that HRT reduced heart attacks in women with known coronary heart disease
41 1998- HERS Trial Result Women with heart disease who took hormones had no change in risk Critics of study countered that the study did not apply to healthy women Results did not impact hormone use
42 Well designed trial WHI Trial Intended to show that HRT reduced risk of developing coronary heart disease in healthy postmenopausal women
43 2002- WHI Trial Results Hormone use increased risk of -breast cancer -heart attack -stroke -blood clots
44
45 Symptoms of Menopause
46 Vasomotor Instability Hot Flashes Night Sweats Insomnia
47 Vasomotor instability (hot flashes) is caused by a malfunction of the bodies thermostat. This thermostat is located in the hypothalamus- - a small part of the mammalian brain layer that controls multiple critical body functions. The hypothalamus monitors the body s core temperature and will alter blood flow to the skin to either conserve heat or radiate heat off.
48 The hypothalamus will allow a certain range in core body temperature without intervening. When estrogen levels are not stable, the hypothalamus allows a much smaller rise in core temperature before it acts by increasing blood flow to the skin. This creates the flash and sweating followed by chills as the core body temperature then drops.
49 Prevalence of Hot Flashes Fertile Meno 70's % Flash
50 Non-HRT Treatment of Hot Flashes Effexor XR- low dose effective in 70% Other SSRI antidepressants- effective Clonidine- effective in 40% Neurontin- effective in 40% Lifestyle alterations
51 Lifestyle Alterations Hot shower before bedtime- depletes flashes Loose clothing Avoid -hot drinks -alcohol -spicy foods
52 Other Causes of Hot Flashes Hyperthyroidism Malignancy Infection Drug therapies Alcohol Emotional distress
53 Mood Instability
54 Common- easy irritability & depression May have rapid swings in mood Estrogen replacement very effective Common to see women on antidepressants without HRT with little relief
55 Vaginal Atrophy Loss of caliber and depth Dryness Loss of lubrication Loss of sensation Irritation Itching
56 All vaginal tissues, including the skin lining the vagina, and the surrounding support tissues require estrogen to remain healthy. With the loss of estrogen at menopause, all of these tissues thin, weaken and become more fragile. Blood flow and sensation are diminished.
57 The result is often prolapse of pelvic organs, urinary incontinence, pain with intercourse, decreased sensation during intercourse, dryness, frequent bladder infections, itching and irritation. These changes can either be prevented or stabilized and reversed by simply applying a small amount of estrogen into the vagina two times each week.

58
59 Vaginal Atrophy and Estrogen Compared to direct application into vagina -systemic estrogen(ex- pills) gives only 25% as much benefit Low dose systemic estrogen (pills) may not have any impact on the vagina
60 Types of Vaginal Estrogen All have similar efficacy - creams, pills, rings Choices -Estring, Phadia -Femring- (provides systemic estrogen) -Vagifem -Creams- Premarin & Estrace
61 Vaginal Estrogen Creams Applied 2 times each week into the vagina Can be a little messy but very effective & cheaper -one $150 prescription is enough for one year May adjust dose- recommended 0.5 gm- provides -Premarin- 30 mcgm of conjugate estrogens or -Estrace- 50 mcgm of estradiol
62 Vagifem Vaginal tablet inserted 2 times each week 25 mcgm estradiol per dose Minimal increase in systemic levels Less messy & lower dose than creams More expensive than creams
63 Estring (Phadia) Lowest dosing option for vaginal estrogen Flexible silastic ring self-inserted every 3 months Expensive 6-9 mcgm estradiol released daily -1/10 of amount produced in menstrual cycle -only 1/10 of this is absorbed systemically
64 Femring Provides both local & systemic estrogen 50 & 100 mcgm per day Not recommended for women needing only vaginal estrogen Requires progesterone if uterus is present
65 Systemic Absorption of Vaginal Estrogen Depends on degree of atrophy -higher when more atrophic -minimal when atrophy is reversed No systemic progesterone is needed except when Femring is used However, sufficient to reduce bone loss in study using 7.5 mcgm/day vaginal ring
66 Alternative Treatments Continued sexual activity -includes masturbation -helps preserve vaginal elasticity & pliability -related to increased androgens & gonadotropins Water soluble lubricants aiding intercourse Astroglide K-Y lubricant
67 Alternative Treatments Replens Must be used on regular basis Binds to vaginal epithelium Slowly releases purified water Not for use on an as needed basis before intercourse Does not slow or reverse vaginal atrophy
68 Alternative Treatments Vitamin E vaginal suppositories Vitamin E with coconut oil vaginal suppositories Both are over the counter and can provide non-hormonal relief of dryness and itching
69 Other Clinical Symptoms of Menopause helped by HRT Irregular bleeding Joint pain Breast pain Skin changes Menstrual Migraines Loss of balance Sexual dysfunction
70 Clinical Risks of Menopause Fractures Cardiovascular disease Incontinence & prolapse
71 Fractures
72 Common Fractures Vertebral compression fractures Wrist fractures Hip fractures -most serious -20% mortality within 1st year -Only 20% of survivors return to previous levels of activity
73 Annual Hip Fractures per 10,000 Women, 1953 Annual Hip Fractures per 10,000 women 1983
74 Prevalence is Increasing Population is now less active Less sun exposure -Vitamin D deficiency now common Less dairy consumption Critical to build as much bone density as possible before menopause with exercise, calcium & vitamin D
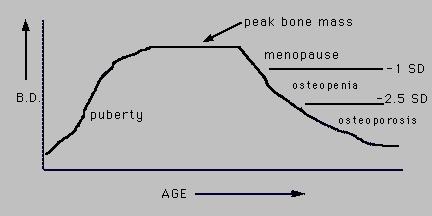
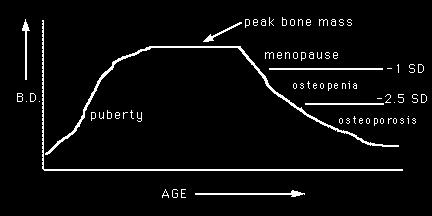
75
76 Hormone replacement will slow loss of bone density after menopause and will reduce fracture risk
77
78 HRT Reduces Hip Fractures
79 Clinical Risk Factors for Fracture Advancing age Previous fracture Glucocorticoid therapy Parental history of hip fracture Low body weight Current cigarette smoking Excessive alcohol consumption Rheumatoid arthritis Secondary osteoporosis (eg, hypogonadism or premature menopause, malabsorption, chronic liver disease, inflammatory bowel disease)
80 Drug Therapy Recommended for Vertebral compression fractures Total hip bone density T-score below -2.5 Bone diseases with high resorption
81 Non-HRT Fracture Prevention Exercise- very, very important -no copay -reduces hip fracture risk by 40% Calcium mg/day Sunlight- vitamin D (free!) -deficiency is very common Stop smoking!!!! Bisphosphonates SERMS
82 Bisphosphonates Didronel Aredia Fosamax Actonel Boniva Zometa, Reclast
83 Bisphosphonates To be effective must have normal blood levels of Calcium Vitamin D
84 Bisphosphonates Clinically significant reduction in hip fractures only in those women with vertebral fractures No additional benefit beyond 5 years of use No fracture data supports use for preventing fracture in those without osteoporosis
85 Bisphosphonate Fracture Reduction A group of postmenopausal women were treated with a bisphosphonate for 3 years. Hip fracture rates were then compared to similar group that was not treated In those with no prior vertebral fracture 2.9% per year vs 3.2% per year Prior vertebral fracture 4.5% per year vs 6.1% per year
86 Bisphosphonate Fracture Reduction That is Using these very expensive drugs with known side effects provided only a very small benefit
87 SERMS Selective Estrogen Receptor Modulators -ex.- Raloxifen Improves bone density -but, provides no hip fracture risk reduction Increases blood clot risk but not CHD risk Decreases breast cancer risk Worsens hot flashes and vaginal atrophy Expensive
88 Risks of HRT
89 Heart Attack


90 Or, How to rearrange the Deck Chairs
91 There was an epidemic increase in US cardiac deaths in the past century that began long before HRT was introduced This increase is thought to have been due to a dramatic decrease in physical labor and a radical decline in quality of diet
92 US Cardiac Deaths/Million
93 How much cardiac risk does HRT add?
94 Lets look at the data HERS -Heart and Estrogen/progestin Replacement Study WHI -Women s Health Initiative
95 To understand the results of HRT trials we must understand the concept of Hazard Ratio
96 Hazard Ratio (HR) HR= 1.5= 50% increase in relative risk Must not confuse with absolute risk
97 For Example Suppose: in 1000 people not taking HRT 2 have a heart attack Compare to: in 1000 people taking HRT 3 have a heart attack HR=3/2= 1.5 or In those taking hormones the Relative risk of a heart attack= 50%
98 However Absolute risk of hormones causing a heart attack is only 1/1000= 0.1%, yet Relative Risk makes for a better headline
99 HERS Large, well designed clinical trial 7 years 2763 postmenopausal with heart disease Avg age- 67 years Premarin + provera
100 HERS Result Premarin + Provera had no impact on heart attack risk in Older postmenopausal women with Documented heart disease
101 Women s Health Initiative (WHI) Series of well designed clinical trials Healthy postmenopausal women yo (Avg- 63 yo) Two of these trials were HRT studies 1) Premarin + Provera (uterus present) 2) Premarin only (hysterectomy)
102 WHI: Premarin + Provera 16,608 women -8,506 on premarin + provera -8,102 on a placebo pill Planned to run 8 years Stopped at 5 years -increased breast cancer risk
103 Heart Attack Risk HR= 1.29= 29% increase in relative risk Premarin + Provera group (8506 women) -162 heart attacks over 5 years Placebo group (8102 women) -125 heart attacks over 5 years
104 Or
105 In 10,000 Women on Premarin + provera 37 will have a heart attack each year 7 are caused by premarin + provera 30 are caused by lifestyle & diet The absolute risk of premarin+provera causing a heart attack is 0.07%/yr
106 WHI: Premarin only 10,739 healthy postmenopausal women Ages yo Stopped after 7 years due to increased stroke risk No impact on heart attack risk
107 Suggests that Provera (progesterone) may be the cause of increased heart attack risk
108 Just how healthy were the WHI participants? 50% were smokers 34% were obese No valid dietary or lifestyle intervention
109 Average age of women in WHI- 63 years Average age of menopause- 51 years
110 Now We know that the risk of heart disease in women rises rapidly after menopause
111 And Most women seek hormone replacement in early menopause when they are having symptoms and before significant heart disease is established
112 So How valid is applying data from an older population that is not having symptoms to a younger population that is having symptoms and has less heart disease risk
113 Timing Hypothesis The age that postmenopausal hormones are started may be extremely important in determining the impact of hormones on heart disease risk
114 Timing Hypothesis Second look at WHI by age groups Women who start HRT earlier appear to actually have lower heart attack risk when they take hormones
115 Hazard Ratio Heart Attacks Per 10,000 per-yrs yo yo yo
116 KEEPS Trail Kronos Early Estrogen Prevention Study In progress To determine impact of early HRT
117 Factors not affecting heart attack risk with HRT in the WHI Study Obesity High blood pressure Aspirin therapy Smoking Diabetes Statin use Family history C reactive protein
118 Breast Cancer
119 WHI- Premarin + Provera HR= 1.26= 26% relative risk breast ca In 10,000 women on Premarin + Provera 38 will develop breast cancer each year 8 are due to premarin + provera 30 are due to other factors Absolute Risk- 0.08%/yr
120 However Increased risk was not seen until 4 years of premarin + provera use Risk declined when Premarin + Provera was stopped Risk continued to increase if Premarin + Provera was not stopped after four years
121 WHI- Premarin only HR= 0.77= relative risk decrease= = -23% In 10,000 women on premarin only 28 will develop breast cancer each year vs 32 per year in placebo group
122 Again, suggesting Provera (progesterone) and not premarin (estrogen) may be the problem
123 Best to avoid HRT in breast cancer survivors
124 Risk in Breast Cancer Survivors HABITS Trial 442 women randomized- HRT vs placebo Stopped at four years due to increased risk of recurrent breast cancer Total cancer incidence over four years 39 out of 221 subjects in hormone group 17 out of 221 subjects in placebo group
125 Stroke
126 WHI Stroke Risk Relative Risks Premarin + Provera= 41% Premarin= 39% In 10,000 women, each year, strokes for HRT vs placebo Premarin + Provera- 31 vs 24 strokes Premarin only- 38 vs 25 strokes
127 WHI Stroke Risk Absolute risk in yo group- 0
128 Do not use HRT if history of ischemic stroke -stroke caused by a blood clot -does not apply to stroke due to a ruptured blood vessel

129 WHI HRT Stroke Risk was not affected by Hypertension Documented cardiovascular disease Smoking Diabetes Biomarkers of inflammation Statin or aspirin use
130 Thromboembolism (DVT & Pulmonary embolism)
131 WHI Thromboembolism Risk (DVT, Pulmonary Embolus) In 10,000 women, yearly events for HRT vs Placebo Premarin + Provera 34 vs 16 For Premarin only group- risk was smaller and was significant only for DVT s
132 WHI Thromboembolism Risk (DVT, Pulmonary Embolus) Risk increased by Increased age Obesity Leiden V mutation HR- 6.7 Risk not affected by Smoking Aspirin Statins Other genetic clotting disorders
133 HAZARD RATIOS (HR) IN MAJOR TRIALS Clinical event HERS (E+P) WHI (E+P) WHI (E only) CHD events Stroke Pulmonary embolism Breast cancer Colon cancer Hip fracture Death
134 WHI Bottom Line Overall the risk for any adverse event being caused by hormone replacement is extremely low.
135 WHI Participant Website Extended discussions and information posted by WHI Study
136 WHI Premarin + Provera Extra Events/10,000 women/year 8 more breast cancers 6 more heart attacks 8 more strokes 8 more pulmonary emboli 6 fewer colon cancers 5 fewer hip fractures
137 WHI Premarin only Extra Events/10,000 women/year 12 more strokes No impact on colon cancer risk -does provera protect the colon? No impact on heart attack risk -decreased risk in yo? Decreased breast cancer risk?
138 Summing It All Up In the final analysis, HRT most likely does not either increase or decrease longevity -any increased risk is very, very small HRT does improve quality of life for symptomatic women around the time of menopause There is no firm data yet for the most pertinent issue- what is the impact of HRT on women just entering menopause? -currently being investigated by the KEEPS trial
139 Summing It All Up When discussing risk the most important questions are -Has there been a hysterectomy- i.e.- is progesterone needed? -What is the patient s age? -Is there a history of either breast cancer or stroke? -Is there a genetic risk of breast cancer? -Is there a Leiden Factor V mutation? -What symptoms are being treated and will alternative treatments be effective?
140 Summing It All Up In those needing estrogen + progesterone (have uterus) -yearly absolute risks of heart attack, breast cancer and stroke are each less than 1/1000 -yearly absolute risk of thromboembolism is 1.8/1000 -breast cancer risk is not increased until after 4 years of HRT- the risk then recedes if HRT is stopped -In women with known heart disease HRT does not increase the risk of another heart attack -Colon cancer and hip fracture risks are slightly lower
141 Summing It All Up In those needing only estrogen (prior hysterectomy) -Yearly absolute risks of stroke or thromboembolism are less than 1/1000 -Heart disease risk is not increased and may actually be decreased especially in women starting HRT early -There is no increased pulmonary embolus risk -Breast cancer risk is not increased (may actually be decreased) -Fracture risk is slightly decreased -No impact on colon cancer risk
142 Summing It All Up For women beyond the symptomatic years of menopause, the only real benefits of adding HRT is for a very small decrease in fracture risk and for treatment or prevention of vaginal atrophy -vaginal estrogen is adequate for both and for vaginal health is superior to systemic HRT
143 Summing It All Up Topical estrogen may be safer and may decrease total body fat and increase total body lean tissue -mostly theory with no firm data If taking drugs that may interact with liver metabolism of estrogen, better to use a topical estrogen Prometrium, a progesterone that is the same as that produced by your body, may be safer than synthetic -again, mostly theory with no firm data

144 A Reasonable Strategy If symptomatic with menopause begin systemic HRT as soon as possible provided there is no history of -stroke due to blood clot -breast cancer or breast cancer gene (BRCA) -pulmonary embolus or deep vein thrombosis If uterus is still present taper off systemic HRT and start vaginal estrogen before four years -if prior hysterectomy may continue systemic estrogen Consider Effexor XR if cannot take HRT
145 So if I do need or choose to use something What are my options?
146 Types of Systemic Hormone Replacement Estrogen, progesterone, testosterone Pills Patch Other topical- creams, emulsions, sprays Vaginal Rings Herbal & phytoestrogens Bioidenticals
147 Types of Estrogen Conjugated equine estrogen Conjugated synthetic estrogen 17-B estradiol Esterified estradiol Ethinyl estradiol (birth control pills)
148 Type of Estrogen may have an impact on CHD Risk WHI & HERS trials- conjugated estrogen Estrogen in Prevention of Atherosclerosis Trial (EPAT)- Estradiol (not premarin) -surrogate CHD marker improved Adding a progesterone may negate benefit
149 Transdermal Estrogen may be safer for secondary CHD prevention Improved markers of heart disease Less impact on clotting than oral However, no firm evidence far so
150 Effects of Progestins Synthetic progestins negate improved lipid effects of estrogen -However, prometrium does not. Prometrium is a natural progesterone Increase serum markers of inflammation
151 Oral Estrogen Quickly metabolized by the liver Has an effect on the liver -Increases proteins made by the liver -Increases HDL cholesterol & triglycerides Increases clearance of certain drugs -seizure medicines, thyroid replacement Increases gallstone risk
152 Oral Estrogens All preparations have similar efficacy All are either absorbed as or converted to estrone sulfate. The body then slowly converts to estradiol which is the from acting on estrogen receptors. Unproven but suspected that risk may vary with the type of estrogen preparation
153 Cardiovascular effects of Oral Estrogen Improved lipid profile -except for increased triglycerides Improved endothelial function -however, seen only in healthy younger women Possible improved insulin sensitivity Decreased clotting factors- fibrinogen, Factor VII, and antithrombin III (important anti-clot factor) Increased vascular inflammatory markers
154 Oral Estrogens- Equivalents Sulfocongugated estrogens mg Esterified estrogens mg Micronized estradiol- 1.0 mg Ethinyl estradiol mg Transdermal17B-estradiol 0.05 mg
155 Low Dose Estrogen 0.3 mg congugated estrogen 0.5 mg micronized estradiol Ultralow dose 0.25 mg micronized estradiol mg transdermal
156 Ultra Low Dose Estrogen Reduces bone loss May not control vasomotor symptoms May not prevent vaginal atrophy
157 Topical Estrogens Less impact on liver related items -Liver proteins -cholesterol -gallstone risk Possible -reduction in body fat -increase in lean body tissue
158 Topical Estrogens Patches, gels, emulsions, sprays All provide 17B-Estradiol Allow variable dosing Femring (vaginal ring) is also form of topical estrogen for systemic dosing All are more expensive than pills Beware of bioidenticals -Premarin gel is not absorbed through the skin -most forms of progesterone gel are not well absorbed through the skin
159 Topical Estrogens Gels, emulsions and sprays -daily application Patches -either once or twice weekly application Vaginal ring -placed by patient every three months -excellent option if vaginal atrophy is also an issue
160 Progesterones Provera (medroxyprogesterone acetate) -most commonly prescribed progestin -used in most of studies Testosterone derivatives -used in birth control pills & Mirena IUD -may have mild testosterone effect
161 Progesterones Prometrium -micronized natural progesterone -less well studied -less negative impact on serum lipids -reasonable alternative -vaginal application may be coming
162 Progesterones Drospirenone -newer -used in birth control pills -derived from sprironolactone -anti-testosterone effect -debatable effect on electrolytes -favorable impact on lipids
163 Progesterones Mirena IUD -excellent birth control -endometrial protection: off label use -not a safe alternative with breast cancer
164 Testosterone Efficacy and safety data are very limited No clear criteria for deficiency Supplements can have side effects -hair growth and acne -Decreases HDL (the good cholesterol)
165 Testosterone Pills, patches, creams, implants One small study shows sexual benefit Controls of hot flashes in difficult cases Improved sense of well being Improved mental function- data very weak Improved bone density- increased estrogen? Use with caution- risk vs benefit unclear
166 Clearest Indications for Testosterone Supplementation Adrenal failure Premature ovarian failure Surgical removal of ovaries Pituitary failure
167 Medical Conditions to consider when prescribing HRT Anticonvulsants- increase hormone clearance Thyroid and glucocorticoid replacement -increased dosing may be needed Alcohol- increases estrogen levels 3x End stage renal disease requires lower dosing
168 Phytoestrogens Naturally occurring compounds in fruits and vegetables Act by varying degrees on estrogen receptors Three main types -isoflavons- greatest effect -coumestans -lignans- weakest
169 Phytoestrogens Isoflavons -soy, chickpeas & lentils Coumestans -sprouts- legume, clover, alfalfa Lignans -flaxseed, grains, fruit, lentils, vegetables
170 Little to no evidence of benefit for Hot flashes General health Bone mineral density- conflicting data Breast cancer-?antiestrogen at high dose
171 Herbal Medicines Evidence of any benefit debated Safety concerns legitimate -manufacturers are not required to report adverse events Unregulated - huge potential variation in quality Play strongly into placebo effect

172
173 Dr Tierraona Low Dog DrLowDog.com Respected bridge between traditional and alternative medicine Herbalist and Family Physician Evidenced based medicine University of New Mexico Menopause strongly open to placebo
174 Bioidentical Hormones No evidence of safety or efficacy Require frequent testing Very expensive Unregulated (but not for long) Quality varies Variable absorption
175 Bioidentical Hormones The appeal of paying more for less -quality -benefit A clever way to make money on novelty and public distrust Plays strongly into placebo effect
176 HRT Drug List
177 ORAL ESTRADIOL* -Estrace (Warner Chilcot) -Gynodiol (Fielding) 0.5, 1, 2 mg 0.5, 1, 1.5, 2 mg ORAL ESTERIFIED ESTROGEN* -Menest (Monarch) -Ogen (Pharmacia) -Ortho-Est (Women First Healthcare) ORAL CONJUGATED EQUINE ESTROGEN* -Premarin (Wyeth-Ayerst) ORAL CONJUGATED SYNTHETIC ESTROGENS* -Cenestin (Elan) 0.3, 0.625, 1.25, 2.5 mg 0.75, 1.5, 3 mg estropipate (equivalent to 0.625, 1.25, 2.5 mg conjugated equine estrogen) 0.75, 1.5 mg estropipate (equivalent to 0.625, 1.25 mg conjugated equine estrogen) 0.3, 0.45, 0.625, 0.9, 1.25 mg 0.3, 0.45, 0.625, 0.9, 1.25 mg -Enjuvia (Elan) 0.625, 1.25 mg
178 ORAL ESTROGEN-PROGESTIN COMBINATIONS Prempro (Wyeth-Ayerst) Prefest (Duramed) Activella (Novo Nordisk) FemHRT (Warner Chilcot) Angeliq (Berlex) 0.3 mg CEE/1.5 mg medroxyprogesterone, 0.45/1.5 mg, 0.625/2.5 mg, 0.625/5 mg 1 mg estradiol/0.9 mg norgestimate 1 mg estradiol/0.5 mg norethindrone acetate 5 mcg ethinyl estradiol/1 mg norethindrone acetate 1 mg estradiol/0.5 mg drosperinone
179 ORAL ESTROGEN-TESTOSTERONE COMBINATIONS* Estratest (Solvay) Estratest HS (Solvay) Syntest DS (Breckenridge) Syntest HS (Breckenridge) 1.25 esterified estrogen/2.5 mg methyltestosterone mg esterified estrogen/1.25 mg methyltestosterone 1.25 mg esterified estrogen/2.5 mg methyltestosterone 0.25 mg esterified estrogen/1.25 mg methyltestosterone
180 ESTRADIOL PATCHES* Alora (Watson) Climara (Berlax) 0.025, 0.05, 0.075, 0.1 mg/d 0.025, 0.05, 0.06, 0.075, 0.1 mg/d Esclim (Women First) 0.025, , 0.05, 0.075, 0.1 mg/d Estraderm (Novartis) 0.05, 0.1 mg/d Vivelle (Novartis) 0.025, , 0.05, 0.075, 0.1 mg/d Menostar (Bayer) mg/d
181 ESTROGEN-PROGESTIN PATCH Combi-Patch (Novartis) 0.05 mg estradiol/0.14 mg norethindrone, 0.05 mg/0.25 mg Climara Pro (Berlex) mg estradiol/0.015 mg levonorgestrel
182 GEL* EstroGel (Solvay) EMULSION* Estrasorb (Novavox) Divigel (Upsher-Smith) Elestrin (Kenwood) TOPICAL SPRAY* EvaMist (KV Pharmaceutical) 0.75 mg estradiol per pump mg estradiol/pouch 0.25, 0.5, 1 mg estradiol/pouch 0.52 mg estradiol/pump 1.5 mg estradiol/spray
183 INTRAVAGINAL RINGS* Femring (Warner- Chilcott) 0.05 & 0.10 mg estradiol/day over 3 months
184 VAGINAL ESTROGEN PREPERATIONS FOR GENITOURINARY ATROPHY (inadequate dose to relieve vasomotor symptoms) VAGINAL RING Estring (Pharmacia) VAGINAL TABLET Vagifem (Novo Nordisk) mg estradiol/day, released over 3 months mg estradiol/tablet VAGINAL CREAM Estrace (Warner-Chilcot) 0.1 mg estradiol/gram Premarin (Wyeth-Ayerst) mg equine conjugated estrogen/gram Back to Acacia Ob/Gyn Website
Menopause. Medicines To Help You
 Medicines To Help You Menopause Use this guide to help you talk to your doctor, pharmacist, or nurse about your hormone medicines. The guide lists all of the FDA-approved products now available to treat
Medicines To Help You Menopause Use this guide to help you talk to your doctor, pharmacist, or nurse about your hormone medicines. The guide lists all of the FDA-approved products now available to treat
Appendix: Reference Table of HT Brand Names
 Appendix: Reference Table of HT Brand Names This is a full reference table in alphabetical order, of Brand Name drugs used in HT. It is the basis for prescription advice throughout this handbook. Drug
Appendix: Reference Table of HT Brand Names This is a full reference table in alphabetical order, of Brand Name drugs used in HT. It is the basis for prescription advice throughout this handbook. Drug
Learning Objectives. Peri menopause. Menopause Overview. Recommendation grading categories
 Learning Objectives Identify common symptoms of the menopause transition Understand the risks and benefits of hormone replacement therapy (HRT) Be able to choose an appropriate hormone replacement regimen
Learning Objectives Identify common symptoms of the menopause transition Understand the risks and benefits of hormone replacement therapy (HRT) Be able to choose an appropriate hormone replacement regimen
Hormone Products for Postmenopausal Use in the United States and Canada
 Hormone Products for Postmenopausal Use in the United States and Canada Copyright The North American Menopause Society October 25, 2011 Table 1. Oral ET products for postmenopausal use in the United States
Hormone Products for Postmenopausal Use in the United States and Canada Copyright The North American Menopause Society October 25, 2011 Table 1. Oral ET products for postmenopausal use in the United States
Deciding whether or not to use Hormone Therapy (HT) is a big decision and should be
 is a big decision and should be") Deciding whether or not to use Hormone Therapy (HT) is a big decision and should be made with input from your healthcare provider. After the decision has been made to take HT, many women don t realize
Deciding whether or not to use Hormone Therapy (HT) is a big decision and should be made with input from your healthcare provider. After the decision has been made to take HT, many women don t realize
OB/GYN Update: Menopausal Management What Does The Evidence Show? Rebecca Levy-Gantt D.O. PremierObGyn Napa Inc.
 OB/GYN Update: Menopausal Management What Does The Evidence Show? Rebecca Levy-Gantt D.O. PremierObGyn Napa Inc. Napa, California IMPORTANT SAFETY INFORMATION ABOUT EVAMIST: WARNING: ENDOMETRIAL CANCER,
OB/GYN Update: Menopausal Management What Does The Evidence Show? Rebecca Levy-Gantt D.O. PremierObGyn Napa Inc. Napa, California IMPORTANT SAFETY INFORMATION ABOUT EVAMIST: WARNING: ENDOMETRIAL CANCER,
Menopausal Symptoms. Hormone Therapy Products Available in Canada for the Treatment of. Physician Desk Reference - 3rd Edition
 Hormone Therapy Products Available in Canada for the Treatment of Menopausal Symptoms Physician Desk Reference - 3rd Edition A clinical resource provided to you by: The Society of Obstetricians and Gynaecologists
Hormone Therapy Products Available in Canada for the Treatment of Menopausal Symptoms Physician Desk Reference - 3rd Edition A clinical resource provided to you by: The Society of Obstetricians and Gynaecologists
BioIdentical Hormone Replacement Therapy for Women
 BioIdentical Hormone Replacement Therapy for Women Bio-Identical Hormones are manufactured hormone products from soy or yam. They are changed in a laboratory so that the hormones produced are identical
BioIdentical Hormone Replacement Therapy for Women Bio-Identical Hormones are manufactured hormone products from soy or yam. They are changed in a laboratory so that the hormones produced are identical
HRT in Perimenopausal Women. Dr. Rubina Yasmin Asst. Prof. Medicine Dhaka Dental College
 HRT in Perimenopausal Women Dr. Rubina Yasmin Asst. Prof. Medicine Dhaka Dental College 1 This is the Change But the CHANGE is not a disease 2 Introduction With a marked increase in longevity, women now
HRT in Perimenopausal Women Dr. Rubina Yasmin Asst. Prof. Medicine Dhaka Dental College 1 This is the Change But the CHANGE is not a disease 2 Introduction With a marked increase in longevity, women now
Disclosures. Objec7ves 9/9/15. What Exactly are bio- iden7cal hormones and what should I tell my pa7ents? Christy Blanco, DNP, RN, WHNP- BC.
 What Exactly are bio- iden7cal hormones and what should I tell my pa7ents? Christy Blanco, DNP, RN, WHNP- BC Disclosures None Objec7ves Discuss terminology of bio- iden7cal, synthe7c and natural hormones.
What Exactly are bio- iden7cal hormones and what should I tell my pa7ents? Christy Blanco, DNP, RN, WHNP- BC Disclosures None Objec7ves Discuss terminology of bio- iden7cal, synthe7c and natural hormones.
Women s Health: Managing Menopause. Jane S. Sillman, MD Assistant Professor of Medicine Harvard Medical School
 Women s Health: Managing Menopause Jane S. Sillman, MD Assistant Professor of Medicine Harvard Medical School Disclosures I have no conflicts of interest. Learning Objectives 1. Apply strategies to help
Women s Health: Managing Menopause Jane S. Sillman, MD Assistant Professor of Medicine Harvard Medical School Disclosures I have no conflicts of interest. Learning Objectives 1. Apply strategies to help
Menopausal Management: What Has Changed?
 Menopausal Management: What Has Changed? Julia V. Johnson, M.D. Professor and Chair, OB/GYN University of Massachusetts Medical School UMass Memorial Medical Center Conflicts of Interest None Learning
Menopausal Management: What Has Changed? Julia V. Johnson, M.D. Professor and Chair, OB/GYN University of Massachusetts Medical School UMass Memorial Medical Center Conflicts of Interest None Learning
HOW TO MAKE SENSE OF MENOPAUSE. by Steven. F. Hotze, M.D.
 HOW TO MAKE SENSE OF MENOPAUSE by Steven. F. Hotze, M.D. INTRODUCTION Dr. Hotze is founder of Hotze Health & Wellness Center and author of the book Hormones, Health, and Happiness. He has enabled thousands
HOW TO MAKE SENSE OF MENOPAUSE by Steven. F. Hotze, M.D. INTRODUCTION Dr. Hotze is founder of Hotze Health & Wellness Center and author of the book Hormones, Health, and Happiness. He has enabled thousands
Ohio Northern University HealthWise. Authors: Alexis Dolin, Andrew Duska, Hannah Lamb, Eric Miller, Pharm D Candidates 2018 May 2018
 Women s Health Authors: Alexis Dolin, Andrew Duska, Hannah Lamb, Eric Miller, Pharm D Candidates 2018 May 2018 Let Your Body Empower You! National Women s Health Week Polycystic Ovary Syndrome Page 2 Breast
Women s Health Authors: Alexis Dolin, Andrew Duska, Hannah Lamb, Eric Miller, Pharm D Candidates 2018 May 2018 Let Your Body Empower You! National Women s Health Week Polycystic Ovary Syndrome Page 2 Breast
HORMONES AND YOUR HEALTH Charlie Tucker Pharm. D
 HORMONES AND YOUR HEALTH Charlie Tucker Pharm. D All of the hormones in your body are designed to work together. This is God s plan. Therefore, if one is altered, or deficient, it will affect the actions
HORMONES AND YOUR HEALTH Charlie Tucker Pharm. D All of the hormones in your body are designed to work together. This is God s plan. Therefore, if one is altered, or deficient, it will affect the actions
Managing menopause in Primary Care and recent advances in HRT
 Managing menopause in Primary Care and recent advances in HRT Raj Saha, MD, DMRT, FRCOG Consultant Gynaecologist Heart of England NHS Foundation Trust rajsaha1@yahoo.co.uk Content of today s talk Aims
Managing menopause in Primary Care and recent advances in HRT Raj Saha, MD, DMRT, FRCOG Consultant Gynaecologist Heart of England NHS Foundation Trust rajsaha1@yahoo.co.uk Content of today s talk Aims
OVERVIEW OF MENOPAUSE
 OVERVIEW OF MENOPAUSE Nicole Budrys, MD, MPH Reproductive Endocrinology Michigan Center for Fertility and Women s Health Presented at SEMCME March 13,2019 Objectives Define menopause Etiology of menopause
OVERVIEW OF MENOPAUSE Nicole Budrys, MD, MPH Reproductive Endocrinology Michigan Center for Fertility and Women s Health Presented at SEMCME March 13,2019 Objectives Define menopause Etiology of menopause
Menopause Symptoms and Management: After Breast Cancer
 Menopause Symptoms and Management: After Breast Cancer An Educational Webinar for Patients and their Caregivers Wen Shen, MD, MPH Division of Gynecologic Specialties July 27, 2018 1 Disclosure I have a
Menopause Symptoms and Management: After Breast Cancer An Educational Webinar for Patients and their Caregivers Wen Shen, MD, MPH Division of Gynecologic Specialties July 27, 2018 1 Disclosure I have a
2017 Position Statement of Hormone Therapy of NAMS: overview SHELAGH LARSON, MS, RNC WHNP, NCMP ACCLAIM, JPS HEALTH NETWORK
 2017 Position Statement of Hormone Therapy of NAMS: overview SHELAGH LARSON, MS, RNC WHNP, NCMP ACCLAIM, JPS HEALTH NETWORK WHI the only large, long-term RCT of HT in women aged 50 to 79 years, Drug trail
2017 Position Statement of Hormone Therapy of NAMS: overview SHELAGH LARSON, MS, RNC WHNP, NCMP ACCLAIM, JPS HEALTH NETWORK WHI the only large, long-term RCT of HT in women aged 50 to 79 years, Drug trail
Managing menopause in Primary Care and recent advances in HRT
 Managing menopause in Primary Care and recent advances in HRT Raj Saha, MD, DMRT, FRCOG PG Cert. Advanced Gynaecology Endoscopy Consultant Gynaecologist Heart of England NHS Foundation Trust Spire Parkway
Managing menopause in Primary Care and recent advances in HRT Raj Saha, MD, DMRT, FRCOG PG Cert. Advanced Gynaecology Endoscopy Consultant Gynaecologist Heart of England NHS Foundation Trust Spire Parkway
Hormone Treatments and the Risk of Breast Cancer
 Cornell University Program on Breast Cancer and Environmental Risk Factors in New York State (BCERF) Updated July 2002 Hormone Treatments and the Risk of Breast Cancer 1) Hormone Treatment After Menopause
Cornell University Program on Breast Cancer and Environmental Risk Factors in New York State (BCERF) Updated July 2002 Hormone Treatments and the Risk of Breast Cancer 1) Hormone Treatment After Menopause
WHI Estrogen--Progestin vs. Placebo (Women with intact uterus)
") HORMONE REPLACEMENT THERAPY In the historical period it was commonly held that estrogen had two principal benefits to postmenopausal women: 1) To alleviate the constitutional symptoms related to the climacteric
HORMONE REPLACEMENT THERAPY In the historical period it was commonly held that estrogen had two principal benefits to postmenopausal women: 1) To alleviate the constitutional symptoms related to the climacteric
presents with Ken Sekine, MD
 presents Pioneering Technologies For Pellet Hormone Therapy Lifestyle Based Medicine A Primer for Clinicians with Ken Sekine, MD Dr. Sekine is a board certified OB-GYN who has been in private practice
presents Pioneering Technologies For Pellet Hormone Therapy Lifestyle Based Medicine A Primer for Clinicians with Ken Sekine, MD Dr. Sekine is a board certified OB-GYN who has been in private practice
UPDATE: Women s Health Issues
 UPDATE: Women s Health Issues Renee B. Alexis, MD, MBA, MPH, FACOG Associate Professor Department of OBGYN Kiran C. Patel College of Osteopathic Medicine Disclosure of Conflicts of Interest I have no financial
UPDATE: Women s Health Issues Renee B. Alexis, MD, MBA, MPH, FACOG Associate Professor Department of OBGYN Kiran C. Patel College of Osteopathic Medicine Disclosure of Conflicts of Interest I have no financial
Benton Franklin County Medical Society 31st Annual CME Seminar
 Management of Current HT/ET and SERM Recommendations Benton Franklin County Medical Society 31st Annual CME Seminar February 21, 2015 Kennewick, Washington Spokane steoporosis Dr. Lynn Kohlmeier Lynn Kohlmeier,
Management of Current HT/ET and SERM Recommendations Benton Franklin County Medical Society 31st Annual CME Seminar February 21, 2015 Kennewick, Washington Spokane steoporosis Dr. Lynn Kohlmeier Lynn Kohlmeier,
The Estrogen Question
 The Estrogen Question Hormone Therapy still offers the best relief for menopausal symptoms. Is it right for you? When 49-year-old Lee Ann Dodson heard the news that the Women's Health Initiative (WHI)
The Estrogen Question Hormone Therapy still offers the best relief for menopausal symptoms. Is it right for you? When 49-year-old Lee Ann Dodson heard the news that the Women's Health Initiative (WHI)
Menopause and HIV. Together, we can change the course of the HIV epidemic one woman at a time.
 Menopause and HIV Together, we can change the course of the HIV epidemic one woman at a time. #onewomanatatime #thewellproject What Is Menopause? Menopause: Point in time when a woman's menstrual periods
Menopause and HIV Together, we can change the course of the HIV epidemic one woman at a time. #onewomanatatime #thewellproject What Is Menopause? Menopause: Point in time when a woman's menstrual periods
Arizona Natural Medicine, L.L.C W. Ray Road, Suite 1, Chandler, AZ
 MENOPAUSE: THE ROAD TO HARMONY by Dr. Sarv Varta Khalsa, N.M.D. Have you been feeling like your emotions are out of control lately? Do you feel irritable one minute, snapping impatiently at your family
MENOPAUSE: THE ROAD TO HARMONY by Dr. Sarv Varta Khalsa, N.M.D. Have you been feeling like your emotions are out of control lately? Do you feel irritable one minute, snapping impatiently at your family
Flashpoint: Regulating Your Body s Temperature. Presented by: Shari M. Lawson, MD MBA Date Presented: November 1,
 Flashpoint: Regulating Your Body s Temperature Presented by: Shari M. Lawson, MD MBA Date Presented: November 1, 2014 1 Disclosures None 2 Objectives Today s discussion will cover How body temperature
Flashpoint: Regulating Your Body s Temperature Presented by: Shari M. Lawson, MD MBA Date Presented: November 1, 2014 1 Disclosures None 2 Objectives Today s discussion will cover How body temperature
Women s Health Initiative (WHI) Study How July 2002 changed menopausal management and what the study really says. Robert P.
 Study How July 2002 changed menopausal management and what the study really says. Robert P.") 3400-A Old Milton Pkwy Ste 360 Alpharetta GA 30005 770.475.0077 georgiahormones.com Women s Health Initiative (WHI) Study How July 2002 changed menopausal management and what the study really says. Robert
3400-A Old Milton Pkwy Ste 360 Alpharetta GA 30005 770.475.0077 georgiahormones.com Women s Health Initiative (WHI) Study How July 2002 changed menopausal management and what the study really says. Robert
By J. Jayasutha Lecturer Department of Pharmacy Practice SRM College of Pharmacy SRM University
 By J. Jayasutha Lecturer Department of Pharmacy Practice SRM College of Pharmacy SRM University Cessation of menstruation as a result of the aging process of or surgical removal of the ovaries; change
By J. Jayasutha Lecturer Department of Pharmacy Practice SRM College of Pharmacy SRM University Cessation of menstruation as a result of the aging process of or surgical removal of the ovaries; change
Estrogens and progestogens
 Estrogens and progestogens Estradiol and Progesterone hormones produced by the gonads are necessary for: conception embryonic maturation development of primary and secondary sexual characteristics at puberty.
Estrogens and progestogens Estradiol and Progesterone hormones produced by the gonads are necessary for: conception embryonic maturation development of primary and secondary sexual characteristics at puberty.
Menopausal Symptoms The Who: Hot flashes are reported by as many as 75% of perimenopausal women in the U.S.
 Menopausal Hormone Therapy: The Who, What, Where, When and Why Laurie Birkholz, MD, NCMP Knowledge of Clinical Trials Regarding Hormone Therapy and Likelihood of Prescribing Hormone Objective: The aim
Menopausal Hormone Therapy: The Who, What, Where, When and Why Laurie Birkholz, MD, NCMP Knowledge of Clinical Trials Regarding Hormone Therapy and Likelihood of Prescribing Hormone Objective: The aim
Drug Class Review on Hormone Therapy for Postmenopausal Women or Women in the Menopausal Transition Stage
 Drug Class Review on Hormone Therapy for Postmenopausal Women or Women in the Menopausal Transition Stage Final Report Update 3 October 2007 Original Report Date: February 2003 Update 1 Report Date: November
Drug Class Review on Hormone Therapy for Postmenopausal Women or Women in the Menopausal Transition Stage Final Report Update 3 October 2007 Original Report Date: February 2003 Update 1 Report Date: November
Menopause management NICE Implementation
 Menopause management NICE Implementation Dr Paula Briggs Consultant in Sexual & Reproductive Health Southport and Ormskirk NHS Hospital Trust Why a NICE guideline (NG 23) Media reports about HRT have not
Menopause management NICE Implementation Dr Paula Briggs Consultant in Sexual & Reproductive Health Southport and Ormskirk NHS Hospital Trust Why a NICE guideline (NG 23) Media reports about HRT have not
Female Patient Questionnaire & History
 !! Female Patient Questionnaire & History Name: Today s Date: (Last) (First) (Middle) Date of Birth: Age: Weight: Occupation: Home Address: City: State: Zip: Home Phone: Cell Phone: Work: E-Mail Address:
!! Female Patient Questionnaire & History Name: Today s Date: (Last) (First) (Middle) Date of Birth: Age: Weight: Occupation: Home Address: City: State: Zip: Home Phone: Cell Phone: Work: E-Mail Address:
Hormone Replacement Therapy For Men Consultation Information
 Hormone Replacement Therapy For Men Consultation Information www.urologyaustin.com Biological Aging and Hormones As we age, a natural degeneration and aging of organs causes the levels of our hormones
Hormone Replacement Therapy For Men Consultation Information www.urologyaustin.com Biological Aging and Hormones As we age, a natural degeneration and aging of organs causes the levels of our hormones
Female Patient Questionnaire & History
 Female Patient Questionnaire & History Name: (Last) (First) (Middle) Today s Date: Home Phone: Cell Phone: Work: E-Mail Address: Primary Care Physician s Name: May we contact you via E-Mail? ( ) YES (
Female Patient Questionnaire & History Name: (Last) (First) (Middle) Today s Date: Home Phone: Cell Phone: Work: E-Mail Address: Primary Care Physician s Name: May we contact you via E-Mail? ( ) YES (
22/09/2014. Menopause Management. Menopause. Menopause symptoms
 Menopause Management Dr Sonia Davison Jean Hailes for Women s Health Menopause Time of last menstrual period - average age 51 Premature Menopause: occurs before age 40 Perimenopause (menopause transition):
Menopause Management Dr Sonia Davison Jean Hailes for Women s Health Menopause Time of last menstrual period - average age 51 Premature Menopause: occurs before age 40 Perimenopause (menopause transition):
 Apples & Oranges Synthetic vs. Bio-Identical Studied Under the Nation s Greats in Hormone Therapy! Salt Lake City Dr. Neal Rouzier Orlando Dr. Sangeeta Pati Naples Dr. Daved Rosensweet And finally Dallas
Apples & Oranges Synthetic vs. Bio-Identical Studied Under the Nation s Greats in Hormone Therapy! Salt Lake City Dr. Neal Rouzier Orlando Dr. Sangeeta Pati Naples Dr. Daved Rosensweet And finally Dallas
Why do I need any hormone replacement? What is Menopause? What symptoms are treated by estrogen Injections?
 1 Why do I need any hormone replacement? Women need replacement if they desire to: Delay the symptoms of aging Reverse depression and anxiety Regain libido Preserve skin and muscle tone Look younger Increase
1 Why do I need any hormone replacement? Women need replacement if they desire to: Delay the symptoms of aging Reverse depression and anxiety Regain libido Preserve skin and muscle tone Look younger Increase
Hormone Replacement Therapy For Women
 Hormone Replacement Therapy For Women Consultation Information www.urologyaustin.com Biological Aging and Hormones As we age, a natural degeneration and aging of organs causes the levels of our hormones
Hormone Replacement Therapy For Women Consultation Information www.urologyaustin.com Biological Aging and Hormones As we age, a natural degeneration and aging of organs causes the levels of our hormones
Hormonal Control of Human Reproduction
 Hormonal Control of Human Reproduction Bởi: OpenStaxCollege The human male and female reproductive cycles are controlled by the interaction of hormones from the hypothalamus and anterior pituitary with
Hormonal Control of Human Reproduction Bởi: OpenStaxCollege The human male and female reproductive cycles are controlled by the interaction of hormones from the hypothalamus and anterior pituitary with
Management of Menopausal Symptoms
 Management of Menopausal Symptoms Tammie Koehler DO, FACOG 1 Menopause Permanent cessation of menstruation that occurs after the loss of ovarian activity Determined to have occurred after 1 full year of
Management of Menopausal Symptoms Tammie Koehler DO, FACOG 1 Menopause Permanent cessation of menstruation that occurs after the loss of ovarian activity Determined to have occurred after 1 full year of
A Practitioner s Toolkit for the Management of the Menopause
 Medicine, Nursing and Health Sciences A Practitioner s Toolkit for the Management of the Menopause Developed by the Women s Health Research Program School of Public Health and Preventive Medicine Monash
Medicine, Nursing and Health Sciences A Practitioner s Toolkit for the Management of the Menopause Developed by the Women s Health Research Program School of Public Health and Preventive Medicine Monash
Data Shows Reduction in Frequency and Severity in Hot Flashes in as Early as 14 Days
 Newly Published Menopause Study: Bioidentical and FDA Approved Divigel (estradiol gel) 0.1 Percent Safe and Effective Treatment for Moderate to Severe Hot Flashes Associated with Menopause Data Shows Reduction
Newly Published Menopause Study: Bioidentical and FDA Approved Divigel (estradiol gel) 0.1 Percent Safe and Effective Treatment for Moderate to Severe Hot Flashes Associated with Menopause Data Shows Reduction
INSURANCE DISCLAIMER
 INSURANCE DISCLAIMER Preventative medicine and bio- identical hormone replacement is a unique practice and is considered a form of alternative medicine. Even though the physicians and nurses are board
INSURANCE DISCLAIMER Preventative medicine and bio- identical hormone replacement is a unique practice and is considered a form of alternative medicine. Even though the physicians and nurses are board
Page 1
 Osteoporosis Osteoporosis is a condition characterised by weakened bones that fracture easily. After menopause many women are at risk of developing osteoporosis. Peak bone mass is usually reached during
Osteoporosis Osteoporosis is a condition characterised by weakened bones that fracture easily. After menopause many women are at risk of developing osteoporosis. Peak bone mass is usually reached during
COPING A newsletter from COPN December 23, 2010 Remember: You can live well with osteoporosis!
 COPING A newsletter from COPN December 23, 2010 Remember: You can live well with osteoporosis! SEASONS GREETINGS! This issue of COPING draws to a close our series of articles on the 2010 Clinical Practice
COPING A newsletter from COPN December 23, 2010 Remember: You can live well with osteoporosis! SEASONS GREETINGS! This issue of COPING draws to a close our series of articles on the 2010 Clinical Practice
Menopause & HRT. Rosie & Alex. Image:
 Menopause & HRT Rosie & Alex Image: http://www.keepcalm-o-matic.co.uk/ Menopause The permanent cessation of menstruation for 12 months When does it happen? Average age 51 Image: Nature Medicine - 12, 612-613
Menopause & HRT Rosie & Alex Image: http://www.keepcalm-o-matic.co.uk/ Menopause The permanent cessation of menstruation for 12 months When does it happen? Average age 51 Image: Nature Medicine - 12, 612-613
Post-menopausal hormone replacement therapy. Evan Klass, MD May 17, 2018
 Post-menopausal hormone replacement therapy Evan Klass, MD May 17, 2018 Are we really still talking about this? Are we really still talking about this? 1960-1975- estrogen prescriptions doubled. Pharma
Post-menopausal hormone replacement therapy Evan Klass, MD May 17, 2018 Are we really still talking about this? Are we really still talking about this? 1960-1975- estrogen prescriptions doubled. Pharma
Summary of the risk management plan (RMP) for Duavive (conjugated oestrogens / bazedoxifene)
 for Duavive (conjugated oestrogens / bazedoxifene)") EMA/679870/2014 Summary of the risk management plan (RMP) for Duavive (conjugated oestrogens / bazedoxifene) This is a summary of the risk management plan (RMP) for Duavive, which details the measures
EMA/679870/2014 Summary of the risk management plan (RMP) for Duavive (conjugated oestrogens / bazedoxifene) This is a summary of the risk management plan (RMP) for Duavive, which details the measures
Hormone Restoration and Support
 Hormone Restoration and Support As a doctor with a strong interest in functional medicine, I strive to help my patients to achieve optimal health in the best ways I know how. This encompasses a combined,
Hormone Restoration and Support As a doctor with a strong interest in functional medicine, I strive to help my patients to achieve optimal health in the best ways I know how. This encompasses a combined,
Difference between vagifem and yuvafem
 Difference between vagifem and yuvafem Generally, when estrogen is prescribed for a postmenopausal woman with a uterus, a progestin should also be considered to reduce the risk of endometrial cancer. Estrogen-alone
Difference between vagifem and yuvafem Generally, when estrogen is prescribed for a postmenopausal woman with a uterus, a progestin should also be considered to reduce the risk of endometrial cancer. Estrogen-alone
What's New in Menopause Management
 Annual Review of Family Medicine December 10, 2015 San Francisco, CA What's New in Menopause Management Michael Policar, MD, MPH Clinical Professor of Ob, Gyn, and Repro Sciences UCSF School of Medicine
Annual Review of Family Medicine December 10, 2015 San Francisco, CA What's New in Menopause Management Michael Policar, MD, MPH Clinical Professor of Ob, Gyn, and Repro Sciences UCSF School of Medicine
Ms. Y. Outline. Updates of SERMs and Estrogen
 Ms. Y Updates of SERMs and Estrogen Steven R. Cummings, MD, FACP San Francisco Coordinating Center CPMC Research Institute and UCSF Support from Lilly, Pfizer, Berlex 55 y.o. woman with mild hypertension
Ms. Y Updates of SERMs and Estrogen Steven R. Cummings, MD, FACP San Francisco Coordinating Center CPMC Research Institute and UCSF Support from Lilly, Pfizer, Berlex 55 y.o. woman with mild hypertension
Female New Patient Package
 Female New Patient Package The contents of this package are your first step to restore your vitality. Please take time to read this carefully and answer all the questions as completely as possible. Thank
Female New Patient Package The contents of this package are your first step to restore your vitality. Please take time to read this carefully and answer all the questions as completely as possible. Thank
Topic 24: Estrogens and Female Reproductive Drugs
 Topic 24: Estrogens and Female Reproductive Drugs I. Contraceptives A. Estrogen-Progestin Contraceptives Note all of these drugs contain one estrogen (listed first) and one progestin Drug to know: ethinyl
Topic 24: Estrogens and Female Reproductive Drugs I. Contraceptives A. Estrogen-Progestin Contraceptives Note all of these drugs contain one estrogen (listed first) and one progestin Drug to know: ethinyl
11/15/2017. Update on HRT. Highgate Private Hospital (Barnet Hospital) Women s Health. Menopause
 Women s Health. Menopause") Update on HRT Miss Moneli Golara Consultant Obstetrician and Gynaecologist MBBS, FRCOG Highgate Private Hospital (Barnet Hospital) E: lauren@medicaladministration.co.uk Women s Health Life expectancy of
Update on HRT Miss Moneli Golara Consultant Obstetrician and Gynaecologist MBBS, FRCOG Highgate Private Hospital (Barnet Hospital) E: lauren@medicaladministration.co.uk Women s Health Life expectancy of
Kathryn M. Rexrode, MD, MPH. Assistant Professor. Division of Preventive Medicine Brigham and Women s s Hospital Harvard Medical School
 Update: Hormones and Cardiovascular Disease in Women Kathryn M. Rexrode, MD, MPH Assistant Professor Division of Preventive Medicine Brigham and Women s s Hospital Harvard Medical School Overview Review
Update: Hormones and Cardiovascular Disease in Women Kathryn M. Rexrode, MD, MPH Assistant Professor Division of Preventive Medicine Brigham and Women s s Hospital Harvard Medical School Overview Review
For Immediate Release
 Media Contact The Reilly Group 773.348.3800 For Immediate Release DIVIGEL (ESTRADIOL GEL) 0.1% IS ONE OF A NEWER GENERATION OF BIOIDENTICAL ESTROGENS THAT IS FDA APPROVED FOR RELIEF OF HOT FLASHES, INCLUDING
Media Contact The Reilly Group 773.348.3800 For Immediate Release DIVIGEL (ESTRADIOL GEL) 0.1% IS ONE OF A NEWER GENERATION OF BIOIDENTICAL ESTROGENS THAT IS FDA APPROVED FOR RELIEF OF HOT FLASHES, INCLUDING
North American Menopause Society (NAMS)
") North American Menopause Society (NAMS) 2012 Hormone Therapy Position Statement Cynthia B. Evans, MD Assistant Professor-Clinical Department of Obstetrics and Gynecology The Ohio State University College
North American Menopause Society (NAMS) 2012 Hormone Therapy Position Statement Cynthia B. Evans, MD Assistant Professor-Clinical Department of Obstetrics and Gynecology The Ohio State University College
Endocrine Steroids 2. Signal transduction 3. Prostaglandins
 Endocrine - 2 1. Steroids 2. Signal transduction 3. Prostaglandins Estrogen Menopause (pause in the menes) ["change of life" at about 50] - lack of estrogen. (Some hysterectomy or ovarian cancer surgeries
Endocrine - 2 1. Steroids 2. Signal transduction 3. Prostaglandins Estrogen Menopause (pause in the menes) ["change of life" at about 50] - lack of estrogen. (Some hysterectomy or ovarian cancer surgeries
Patient education for transgender feminizing hormone therapy
 Date name DOB Patient education for transgender feminizing hormone therapy o Some transsexual, transgender, and gender non-conforming people choose to take hormone therapy to treat gender dysphoria and
Date name DOB Patient education for transgender feminizing hormone therapy o Some transsexual, transgender, and gender non-conforming people choose to take hormone therapy to treat gender dysphoria and
Female New Patient Questionnaire
 Patient Demographics First Name: Middle: Last Name: Home Phone: Cell Phone: Email: Address: SSN: City: State: Zip: Age: Date of Birth: Referred by: OBGYN: Occupation: Primary Care Physician: Marital Status:
Patient Demographics First Name: Middle: Last Name: Home Phone: Cell Phone: Email: Address: SSN: City: State: Zip: Age: Date of Birth: Referred by: OBGYN: Occupation: Primary Care Physician: Marital Status:
Female New Patient Package
 Female New Patient Package The contents of this package are your first step to restore your vitality. Please take time to read this carefully and answer all the questions as completely as possible. Thank
Female New Patient Package The contents of this package are your first step to restore your vitality. Please take time to read this carefully and answer all the questions as completely as possible. Thank
This information can be found by going to Hot Flashes
 Winsor Pilates - Official Site Reach physical and mental health while sculpting your... www.winsorpilates.com ML Speakers Group -Women's Health Today Book an exciting speaker to make your event special.
Winsor Pilates - Official Site Reach physical and mental health while sculpting your... www.winsorpilates.com ML Speakers Group -Women's Health Today Book an exciting speaker to make your event special.
HRT & Menopause Where Do We Stand Now?
 HRT & Menopause Where Do We Stand Now? Mrs. SY Hussain Consultant Gynaecologist The Holly Private Hospital Spire Roding Hospital The Wellington Hospital Discussion Points Discuss Recommendations made by
HRT & Menopause Where Do We Stand Now? Mrs. SY Hussain Consultant Gynaecologist The Holly Private Hospital Spire Roding Hospital The Wellington Hospital Discussion Points Discuss Recommendations made by
HORMONE REPLACEMENT THERAPY-UPDATE KHALED SAKHEL, MD FACOG FACS FAIUM ASSOCIATE PROFESSOR EASTERN VIRGINIA MEDICAL SCHOOL
 HORMONE REPLACEMENT THERAPY-UPDATE KHALED SAKHEL, MD FACOG FACS FAIUM ASSOCIATE PROFESSOR EASTERN VIRGINIA MEDICAL SCHOOL INTRODUCTION NORMAL WOMEN HAVE MENOPAUSE AT A MEAN AGE OF 51 YEARS, WITH 95 PERCENT
HORMONE REPLACEMENT THERAPY-UPDATE KHALED SAKHEL, MD FACOG FACS FAIUM ASSOCIATE PROFESSOR EASTERN VIRGINIA MEDICAL SCHOOL INTRODUCTION NORMAL WOMEN HAVE MENOPAUSE AT A MEAN AGE OF 51 YEARS, WITH 95 PERCENT
Bioidentical Hormone Replacement Therapy For Men and Women
 Bioidentical Hormone Replacement Therapy For Men and Women Welcome to our Aesthetic Medicine practice where we will be introducing our clients to bioidentical hormone replacement. The simplest definition
Bioidentical Hormone Replacement Therapy For Men and Women Welcome to our Aesthetic Medicine practice where we will be introducing our clients to bioidentical hormone replacement. The simplest definition
MENOPAUSE. I have no disclosures 10/11/18 OBJECTIVES WHAT S NEW? WHAT S SAFE?
 MENOPAUSE WHAT S NEW? WHAT S SAFE? I have no disclosures Sara Whetstone, MD, MHS OBJECTIVES To describe risks of HT by age and menopause onset To recommend specific HT regimen for women who undergo early
MENOPAUSE WHAT S NEW? WHAT S SAFE? I have no disclosures Sara Whetstone, MD, MHS OBJECTIVES To describe risks of HT by age and menopause onset To recommend specific HT regimen for women who undergo early
SERMS, Hormone Therapy and Calcitonin
 SERMS, Hormone Therapy and Calcitonin Tiffany Kim, MD Clinical Fellow VA Advanced Women s Health UCSF Endocrinology and Metabolism I have nothing to disclose Thanks to Clifford Rosen and Steven Cummings
SERMS, Hormone Therapy and Calcitonin Tiffany Kim, MD Clinical Fellow VA Advanced Women s Health UCSF Endocrinology and Metabolism I have nothing to disclose Thanks to Clifford Rosen and Steven Cummings
Pearls for Menopause Management: I m ready: now what?
 Pearls for Menopause Management: I m ready: now what? Friday November 13, 2015 Susan Goldstein MD CCFP FCFP NCMP Assistant Professor Department of Family and Community Medicine University of Toronto Menarche
Pearls for Menopause Management: I m ready: now what? Friday November 13, 2015 Susan Goldstein MD CCFP FCFP NCMP Assistant Professor Department of Family and Community Medicine University of Toronto Menarche
The Physical and Emotional Toll of Hormone Imbalance for Women. Sally Brooks
 The Physical and Emotional Toll of Hormone Imbalance for Women Sally Brooks 2 A hormone imbalance happens when your body produces too much or too few hormones needed for optimal health. When that happens,
The Physical and Emotional Toll of Hormone Imbalance for Women Sally Brooks 2 A hormone imbalance happens when your body produces too much or too few hormones needed for optimal health. When that happens,
Menopause - a summary of management
 Page 1 of 5 Menopause - a summary of management Original article by: May Su Resources Menopause treatment algorithm The Jean Hales Foundation for women's heath. Menopause, a treatment algorithm. (Australian
Page 1 of 5 Menopause - a summary of management Original article by: May Su Resources Menopause treatment algorithm The Jean Hales Foundation for women's heath. Menopause, a treatment algorithm. (Australian
WHAT IS THE MOST IMPORTANT INFORMATION I SHOULD KNOW ABOUT OGEN (AN ESTROGEN HORMONE)?
?") PATIENT INFORMATION (Updated July 2006) OGEN estropipate tablets, USP Read this PATIENT INFORMATION before you start taking OGEN and read what you get each time you refill OGEN. There may be new information.
PATIENT INFORMATION (Updated July 2006) OGEN estropipate tablets, USP Read this PATIENT INFORMATION before you start taking OGEN and read what you get each time you refill OGEN. There may be new information.
HORMONE THERAPY A BALANCED VIEW?? Prof Greta Dreyer
 HORMONE THERAPY A BALANCED VIEW?? Prof Greta Dreyer -- PART 1 -- Definitions HRT hormone replacement therapy HT genome therapy ERT estrogen replacement therapy ET estrogen EPT estrogen progesterone therapy
HORMONE THERAPY A BALANCED VIEW?? Prof Greta Dreyer -- PART 1 -- Definitions HRT hormone replacement therapy HT genome therapy ERT estrogen replacement therapy ET estrogen EPT estrogen progesterone therapy
HRT. Responding to questions about. The Women s Health Initiative (WHI) is a large, CME Workshop. associated with combined
 is a large, CME Workshop. associated with combined") CME Workshop Responding to questions about HRT By Margaret Burnett, MD, BA(Hon), MA, CCFP, FRCPC The Women s Health Initiative (WHI) is a large, prospective, placebo-controlled trial sponsored by the National
CME Workshop Responding to questions about HRT By Margaret Burnett, MD, BA(Hon), MA, CCFP, FRCPC The Women s Health Initiative (WHI) is a large, prospective, placebo-controlled trial sponsored by the National
MENOPAUSE - WHAT TO EXPECT CONCLUSION WEB LINKS
 NOTES CONCLUSION The average Canadian woman can expect to live to 80 years of age or older. This means you may live more than one-third of your life after menopause. Knowing what to expect and how to care
NOTES CONCLUSION The average Canadian woman can expect to live to 80 years of age or older. This means you may live more than one-third of your life after menopause. Knowing what to expect and how to care
Current Topics in Hormone Replacement Therapy
 Current Topics in Hormone Replacement Therapy Corey R. Babb, D.O., FACOOG, IF, NCMP Clinical Assistant Professor of Obstetrics and Gynecology Director of the Oklahoma State University Center for Women
Current Topics in Hormone Replacement Therapy Corey R. Babb, D.O., FACOOG, IF, NCMP Clinical Assistant Professor of Obstetrics and Gynecology Director of the Oklahoma State University Center for Women
INFORMED CONSENT FOR FEMINIZING HORMONE THERAPY
 INFORMED CONSENT FOR FEMINIZING HORMONE THERAPY The use of hormone therapy for gender transition/affirmation is based on many years of experience treating trans persons. Research on hormone therapy is
INFORMED CONSENT FOR FEMINIZING HORMONE THERAPY The use of hormone therapy for gender transition/affirmation is based on many years of experience treating trans persons. Research on hormone therapy is
Summary of the risk management plan (RMP) for Senshio (ospemifene)
 for Senshio (ospemifene)") EMA/736568/2014 Summary of the risk management plan (RMP) for Senshio (ospemifene) This is a summary of the risk management plan (RMP) for Senshio, which details the measures to be taken in order to ensure
EMA/736568/2014 Summary of the risk management plan (RMP) for Senshio (ospemifene) This is a summary of the risk management plan (RMP) for Senshio, which details the measures to be taken in order to ensure
Reproductive System. Testes. Accessory reproductive organs. gametogenesis hormones. Reproductive tract & Glands
 Reproductive System Testes gametogenesis hormones Accessory reproductive organs Reproductive tract & Glands transport gametes provide nourishment for gametes Hormonal regulation in men Hypothalamus - puberty
Reproductive System Testes gametogenesis hormones Accessory reproductive organs Reproductive tract & Glands transport gametes provide nourishment for gametes Hormonal regulation in men Hypothalamus - puberty
Navigating the Change: Leading Patients Through Menopause
 4:30pm - 5:30pm: Breakout 5 - Women s Health Option A: Navigating the Change: Leading Patients Through Menopause ACPE UAN 0107-0000-10-025-L01-P 0.1 CEU/1.0 Hr. Activity Type: Application-Based Program
4:30pm - 5:30pm: Breakout 5 - Women s Health Option A: Navigating the Change: Leading Patients Through Menopause ACPE UAN 0107-0000-10-025-L01-P 0.1 CEU/1.0 Hr. Activity Type: Application-Based Program
Inside. Stop Living in Fear! Take Steps to Prevent Breast Cancer. This Issue
 S Stop Living in Fear! Take Steps to Prevent Breast Cancer BREAST CANCER RISK FACTORS Family history of mother or sister with breast cancer Menstruation before age 12 Menopause after age 50 First child
S Stop Living in Fear! Take Steps to Prevent Breast Cancer BREAST CANCER RISK FACTORS Family history of mother or sister with breast cancer Menstruation before age 12 Menopause after age 50 First child
Dr. Jack Monaco Safe Solutions for Menopause
 Dr. Jack Monaco Safe Solutions for Menopause The following is taken from The Future of Health Now interview conducted by Ann Wixon with menopause and hormone expert, Dr. Jack Monaco. We have compiled the
Dr. Jack Monaco Safe Solutions for Menopause The following is taken from The Future of Health Now interview conducted by Ann Wixon with menopause and hormone expert, Dr. Jack Monaco. We have compiled the
Thrombosis and Women s Health Risk factors, contraceptive pill, HRT and your doctor
 Thrombosis and Women s Health Risk factors, contraceptive pill, HRT and your doctor Dr Matthew Fay GP Principal The Willows Medical Practice- Queensbury GPwSI and Co-Founder Westcliffe Cardiology Service
Thrombosis and Women s Health Risk factors, contraceptive pill, HRT and your doctor Dr Matthew Fay GP Principal The Willows Medical Practice- Queensbury GPwSI and Co-Founder Westcliffe Cardiology Service
Progesterone. What is progesterone? Important information. Before taking this medicine
 Progesterone Generic Name: progesterone (proe JESS te rone) Brand Names: First Progesterone MC10, Menopause Formula Progesterone, Prometrium What is progesterone? Progesterone is a female hormone important
Progesterone Generic Name: progesterone (proe JESS te rone) Brand Names: First Progesterone MC10, Menopause Formula Progesterone, Prometrium What is progesterone? Progesterone is a female hormone important
There are four areas where you can expect changes to occur as your hormone therapy progresses.
 You are considering taking testosterone, so you should learn about some of the risks, expectations, long term considerations, and medications associated with medical transition. If is very important to
You are considering taking testosterone, so you should learn about some of the risks, expectations, long term considerations, and medications associated with medical transition. If is very important to
CASE 4- Toy et al. CASE FILES: Obstetrics & Gynecology
 CASE 4- Toy et al. CASE FILES: Obstetrics & Gynecology A 49-year-old woman complains of irregular menses over the past 6 months, feelings of inadequacy, vaginal dryness, difficulty sleeping, and episodes
CASE 4- Toy et al. CASE FILES: Obstetrics & Gynecology A 49-year-old woman complains of irregular menses over the past 6 months, feelings of inadequacy, vaginal dryness, difficulty sleeping, and episodes
Menopause and HRT. John Smiddy and Alistair Ledsam
 Menopause and HRT John Smiddy and Alistair Ledsam Menopause The cessation of menstruation Diagnosed retrospectively after 1 year of amenorrhoea Average age 51 in the UK Normal physiology - Menstruation
Menopause and HRT John Smiddy and Alistair Ledsam Menopause The cessation of menstruation Diagnosed retrospectively after 1 year of amenorrhoea Average age 51 in the UK Normal physiology - Menstruation
Hormone Replacement Therapy (HRT) Benefits & Risks - The Facts
 Benefits & Risks - The Facts") Hormone Replacement Therapy (HRT) Benefits & Risks - The Facts HRT is a prescription only treatment that replaces some of the lost oestrogen and progesterone hormones which occur during menopause. It can
Hormone Replacement Therapy (HRT) Benefits & Risks - The Facts HRT is a prescription only treatment that replaces some of the lost oestrogen and progesterone hormones which occur during menopause. It can
What is the menopause?
 Information for you Alternatives to hormone replacement therapy for symptoms of the menopause Published in December 2011 This information is for you if you are considering alternatives to hormone replacement
Information for you Alternatives to hormone replacement therapy for symptoms of the menopause Published in December 2011 This information is for you if you are considering alternatives to hormone replacement
THE SAFETY CHECK LIST BEFORE STARTING HT
 THE SAFETY CHECK LIST BEFORE STARTING HT This safety checklist was designed by the Endocrine Society in 2015 to minimize the chance of giving hormone therapy to women who may be negatively affected by
THE SAFETY CHECK LIST BEFORE STARTING HT This safety checklist was designed by the Endocrine Society in 2015 to minimize the chance of giving hormone therapy to women who may be negatively affected by
Management of Menopausal Symptoms in Patients with Breast Cancer. Mike Dixon Edinburgh Breast Unit
 Management of Menopausal Symptoms in Patients with Breast Cancer Mike Dixon Edinburgh Breast Unit Menopausal symptoms have a major impact on Quality of Life Variety of Symptoms associated with the Menopause
Management of Menopausal Symptoms in Patients with Breast Cancer Mike Dixon Edinburgh Breast Unit Menopausal symptoms have a major impact on Quality of Life Variety of Symptoms associated with the Menopause
There are four areas where you can expect changes to occur as your hormone therapy progresses. 1) Physical
 Physical") You are considering taking feminizing hormones, so you should learn about some of the risks, expectations, long term considerations, and medications associated with medical transition. It is very important
You are considering taking feminizing hormones, so you should learn about some of the risks, expectations, long term considerations, and medications associated with medical transition. It is very important
1/11/2017. Disclosure Statement. Describe the most common medical issues associated with peri-menopause and menopause. Case study:
 The Pharmacological Management of Peri-Menopause and Menopause Debora Bear, FNP, MSN, MPH University Of New Mexico Hospital Hormones and other Treatments Gwen Iffil, Stepmber 29, 19 to vember 14, 2016
The Pharmacological Management of Peri-Menopause and Menopause Debora Bear, FNP, MSN, MPH University Of New Mexico Hospital Hormones and other Treatments Gwen Iffil, Stepmber 29, 19 to vember 14, 2016
The Study of Tamoxifen and Raloxifene (STAR): Questions and Answers. Key Points
: Questions and Answers. Key Points") CANCER FACTS N a t i o n a l C a n c e r I n s t i t u t e N a t i o n a l I n s t i t u t e s o f H e a l t h D e p a r t m e n t o f H e a l t h a n d H u m a n S e r v i c e s The Study of Tamoxifen
CANCER FACTS N a t i o n a l C a n c e r I n s t i t u t e N a t i o n a l I n s t i t u t e s o f H e a l t h D e p a r t m e n t o f H e a l t h a n d H u m a n S e r v i c e s The Study of Tamoxifen