Review July Page 1 of 36. Title of Guideline. Contact Names and Job Title (authors) Directorate & Speciality
|
|
|
- Rodger Greene
- 6 years ago
- Views:
Transcription
1 Title of Guideline Contact Names and Job Title (authors) Directorate & Speciality Date of submission 06/07/2017 Date on which guideline must be reviewed Explicit definition of patient group to which it applies (e.g. inclusion and exclusion criteria, diagnosis) Abstract Key Words Insertion and management of tracheostomies within Adult Critical Care Dr Martin Beed, Consultant in Intensive Care Medicine & Anaesthesia, NUH Dr Allan Howatson, Consultant in Intensive Care Medicine & Anaesthesia, NUH Clinical Support Adult Critical Care Review July 2022 Applies to all adult patients requiring tracheostomy insertion during, or prior to Critical Care admission. Excludes: All paediatric cases All cases where immediate tracheostomy insertion is required for the first time as part of resuscitation for an obstructed airway All cases where tracheostomy insertion is required as part of a surgical procedure not requiring Critical Care This guideline describes the procedures associated with the initial insertion of planned percutaneous and surgical tracheostomies in critically ill patients. Also described are guidelines associated with the ongoing care and management of such patients. Tracheostomy; Percutaneous tracheostomy; Adult critical care Evidence base of the guideline: Peer reviewed by: NUH critical care consultants; Critical Care Governance; Tracheostomy working group; Evidence base: (1-5) 3 well designed non-experimental descriptive studies (i.e. comparative / correlation and case studies) 4 expert committee reports or opinions and / or clinical experiences of respected authorities 5 recommended best practise based on the clinical experience of the guideline developer Consultation Process Target audience All intensive care consultants Senior ICU nursing staff Critical Care Governance Cardiac anaesthetists; Thoracic and upper GI surgery; ENT / Maxillo-facial surgery; CCOT Medical and nursing staff all adult critical care areas This guideline has been registered with the trust. However, clinical guidelines are guidelines only. The interpretation and application of clinical guidelines will remain the responsibility of the individual clinician. If in doubt contact a senior colleague or expert. Caution is advised when using guidelines after the review date. Page 1 of 36
2 Contents Introduction 3 Exclusions (what this guideline does not cover) 4 Indications 4 Contra-indications 5 Hazards / cautions 6 Guidelines for tracheostomy insertion 7 Consent 7 Preparation for insertion 8 Tracheostomy insertion procedure 8 Types of tracheostomy tubes available 10 Post-procedure investigations and documentation 12 Continuing care of patients with tracheostomies on critical care 13 Suture removal and tracheostomy changes 13 Managing patients with tracheostomies whilst within critical care 13 Managing complications of tracheostomies 14 Weaning whilst within critical care 17 Planned tracheostomy changes and decannulation 17 Swallowing assessments 18 Discharge from ICU 19 Provisions for audit 19 References 20 Appendix One Tracheostomy patient and relatives information leaflet 21 Appendix Two Adult Critical Care Percutaneous Tracheostomy Insertion Record (includes pre-printed consent 4) 22 Appendix Three Summary of different tracheostomy tubes available within NUH Appendix Four Emergency tracheostomy management patent upper airway Emergency laryngectomy management Appendix Five Equality impact assessment Page 2 of 36
3 NOTTINGHAM UNIVERSITY HOSPITALS NHS TRUST CRITICAL CARE GUIDELINES Guidance for the insertion and subsequent medical management of tracheostomies in adult patients requiring intensive care or highdependency care Introduction: A tracheostomy, or tracheal stoma, is a connection between the tracheal lumen and the anterior neck. However, it is frequently used to describe a tube inserted directly into the trachea through which the patient can breathe or be mechanically ventilated. A small surgical procedure is required in order to insert this tube. The surgical procedure itself may involve a percutaneous or open surgical approach. Tracheostomies are usually temporary, and are often used in patients requiring critical care for a variety of reasons (see below). This document contains guidelines developed using evidence concerning best practice or, where this does not exist, a locally agreed consensus of opinion. The aim of these guidelines is to address the following areas: Basic standards associated with the insertion of a tracheostomy Documentation required to be completed associated with the initial surgical procedure Choice of initial tracheostomy tube Initial and subsequent management of the tracheostomy whilst the patient is managed within critical care These guidelines are not intended as instructions on how to perform a tracheostomy, and only give limited guidance as to when to consider a surgical rather than percutaneous technique. It is expected that the decision to proceed to tracheostomy will be taken by senior clinicians only, and that the procedure will be performed by trained operators, or under their immediate/direct supervision. Page 3 of 36
4 Where reference is made to Critical Care Consultants in this guide it includes Cardiac Intensive Care Anaesthetists. Exclusion This protocol does not cover the emergency insertion of tracheostomies for upper airway obstruction. In these cases the primary aim is to secure an adequate airway as soon as possible and request specialist help if it is not already present. Where appropriate the subsequent management of patients who have undergone emergency tracheostomy insertion should be broadly the same as other ICU/HDU patients with tracheostomies. This protocol does not cover the insertion of mini-tracheostomies, which are used to aid suctioning and are not a definitive airway. This protocol is intended to apply predominantly to critically ill patients and does not cover all the aspects of tracheostomy insertion and management that may be required as elective processes in the subspecialist areas of ENT surgery and Maxillo-facial surgery (for example the management of permanent tracheostomies in laryngectomy patients). Indications for use The elective insertion of a tracheostomy may be required in a patient managed on ICU/HDU for a number of reasons: In order to protect an airway at risk To facilitate weaning from a ventilator and weaning from sedation To improve respiratory dynamics To facilitate tracheal suction To allow ongoing respiratory support both on and after ICU/HDU Additionally patients may require a tracheostomy as part of a planned surgical procedure. Page 4 of 36
5 The ongoing care of patients with tracheostomies should take into account the following: The airway should remain as secure as possible The tracheostomy tube should be as clean as possible Care should be taken to avoid introducing infection via the tracheostomy The tracheostomy stoma should be kept as clean as possible Care should be taken not to damage any associated tissue (for example grafts or flaps around the neck) Weaning with the eventual aim of removing the tracheostomy should be undertaken where appropriate (see separate guideline) Contra-Indications There are no absolute contra-indications to the insertion of a tracheostomy except for refusal by a mentally competent adult patient. Relative contra-indications include: Patients in whom the anatomical or disease-related changes my make the siting of a tracheostomy technically difficult (such as patients who have had previous tracheal or neck surgery or who have a goitre) Patients requiring high oxygen concentration or high ventilator pressures Patients who are severely cardiovascularly unstable Patients with raised intra-cranial pressure Patients who have clotting abnormalities (including thrombocytopaenia) Patients who are at increased risk of tissue infection or breakdown following tracheostomy insertion (for example patients who have mediastinitis or who have had recent neck burns) Recent surgery in an anatomically close area (for example high oesophagectomy, carotid endarterectomy, or anterior spinal surgery) Patients with cervical spine injuries or instability In most of the above situations the procedure may be delayed until the patient s condition(s) has improved / been corrected. Any delay must be balanced against the potential disadvantages of delaying tracheostomy. A surgical technique may be the technique of choice in some of the above situations, depending upon the experience of the operator. Page 5 of 36
6 Hazards / Cautions Patients with tracheostomies are at risk of the following At insertion: Bleeding Airway damage / loss of airway Damage to surrounding structures (including the oesophagus resulting in a fistula) Pneumothorax Surgical emphysema After insertion: Late-onset bleeding (i.e. through erosion into a major vessel which may be fatal) Infection of stoma site Tracheostomy cuff leaks Loss of airway (tracheostomy coughed out / pulled out / dislodged; or at tracheostomy change) The following may also occur, but are also a risk associated with endotracheal tubes Tracheal ulceration / granulomas and/or stenosis (can become evident very late) Aspiration Blocked tube (e.g. from blood and/or dried secretions) Ventilator-associated pneumonia NB although tube dislodgement can be associated with tracheostomies and endotracheal tubes, tracheostomy insertion may be associated with the formation of a false-passage making re-siting of tubes potentially more hazardous Although rare many of the above risks have the potential to result in the death of the patient. Page 6 of 36
7 Guidelines for tracheostomy insertion Consent Where possible appropriate consent should be obtained from the patient prior to the initial procedure to insert a tracheostomy, and prior to any sedation and analgesia required to facilitate insertion. Exceptions to this include: Life-threatening airway obstruction requiring a tracheostomy, and where it is appropriate to resuscitate the patient using this procedure Where the patient is incapable of consent (the usual situation within critical care) Where consent is not possible, and the procedure is elective in nature, it is considered best practice to discuss the procedure with the patient s relatives or advocates, where possible gaining their assent to the procedure An information sheet is available for patients and/or their relatives and this may be used in addition to verbal discussions where appropriate For the insertion of percutaneous tracheostomies it is recommended that a pre-printed consent form is used (included within the Tracheostomy Insertion Booklet) which outlines the risks and benefits associated with the procedure (see appendix one). If this is not used it is recommended that the following lifethreatening risks are included in any discussion: Death Loss of the airway Damage to the airway Haemorrhage in or around the airway (early and late) Infection Pneumothorax For the insertion of surgical tracheostomies surgical consent should take place according to the current best-practice standards applied by the surgical team involved. It is envisaged that a similar discussion of risks and benefits should take place. A sample information leaflet for patients or their relatives can be found in Appendix One The consent form for the insertion of percutaneous tracheostomies in patients who are incapable of consent, which allows for discussion with relatives, is now found within the Adult Critical Care Percutaneous Tracheostomy Insertion Record and can be found in Appendix Two. Page 7 of 36
8 Preparation for insertion Patients should be assessed prior to insertion of tracheostomy to ensure that it is safe to proceed. Assessment should include: Confirmation that anatomy is favourable to the tracheostomy technique proposed by the operator Identification / correction of any coagulopathy Ensuring that a blood sample has been sent for group-and-save (cross-matched blood should be available where there is a higher-than-normal risk of haemorrhage) Confirmation that the patient s cardiovascular and respiratory systems are stable enough to tolerate the procedure. In most situations this would mean an inspired oxygen concentration of 60% and a positive-end-expiratory-pressure of less than 10 cmh 2 O If the patient is eating and drinking they should be starved according to hospital guidelines (6 hours solids, 2 hours clear fluids); if the patient is NG fed then feeding should be discontinued and the NG tube aspirated prior to the procedure Planning for discontinuation and restarting insulin infusion (if being used) Tracheostomy insertion procedure The technique used for tracheostomy insertion will depend upon the experience of the operator. The majority of tracheostomies inserted in critical care will be percutaneous and will be inserted by the critical care clinician. Surgical techniques may be preferred where there are anatomical considerations which increase the risk associated with percutaneous techniques. Where a percutaneous technique is performed the insertion technique should be comparable to the guidelines for insertion as described in the Intensive Care Society guidelines Standards for the care of adult patients with a temporary tracheostomy pages Page 8 of 36
9 In general percutaneous techniques should be performed By consultants in intensive care (or other related disciplines) who have been trained in the technique, or by senior intensive care trainees under immediate, close-proximity supervision With a minimum of two physicians present, one performing the procedure and one available to monitor and support the patient With a minimum of one critical care nurse present Within normal working hours, or day-time working hours if performed over the weekend After the application of anaesthesia and analgesia, as well as neuromuscular blockade With the patient receiving 100% inspired oxygen with mandatory ventilation. With fibre-optic bronchoscopic guidance The following equipment should be available regardless of insertion technique (all available on the standardised critical care resus trolleys the resus trolley in the Cardiac Intensive Care Unit differs slightly from those in CCD, AICU and E12 but the contents are similar): Immediately available Standard resuscitation equipment Full monitoring, including capnography Airway equipment, including laryngoscope and a range of different sized endo-tracheal tubes A range of cuffed non-fenestrated tracheostomy tubes with inner tubes (minimum size 7, 8 and 9) A size 8* adjustable flange tracheostomy Available with only minimal delay A range of sizes of other tracheostomy tubes (adjustable flange and standard) Surgical diathermy Difficult airway equipment *Sizes refer to Jackson Sizes, or internal diameter in mm (without inner-tubes), according to manufacturer Page 9 of 36
10 A sample checklist for the assessment of patients prior to the insertion of a percutaneous tracheostomy can be found within the Adult Critical Care Percutaneous Tracheostomy Insertion Record (Appendix Two) Initial tracheostomy tube at insertion Should be non-fenestrated Where possible should be of size 8 or above in order to facilitate bronchoscopy and have an integral inner-tube Should be sutured in place with Ethilon (or similar) suture Where a long-stitch to the wall of the trachea is used to hold open a tracheal flap it should be of a different suture material, or identified as different in some way Should also be fixed with tracheostomy tapes, except where there has been recent neck-flap surgery (or any other anatomical complication) Should have an absorbent dressing between the tracheostomy flanges and skin, unless there is a surgical indication not to Where possible patients going from critical care to theatres for a tracheostomy should be sent with the appropriate tracheostomy tube to be inserted Types of critical care tracheostomy tubes available within Nottingham University Hospitals Descriptions of the types of tracheostomy tubes commonly found within critical care areas can be found in Appendix Three Different types of tracheostomy tubes are currently being evaluated within Nottingham University Hospitals and within the Mid-Trent Critical Care Network. Should any change in the range of tracheostomy tubes available within Critical Care be required, these guidelines will be updated appropriately and an education and training package will be implemented. Other types of tracheostomy tubes may be used in other specialist areas, for example ENT or Maxillo-facial wards. Occasionally patients with these tracheostomies in may require critical care nursing. If you are unfamiliar with the type of tracheostomy tube and how to manage it please discuss this with any of the following (whichever is most appropriate in the circumstances) Page 10 of 36
11 ENT ward senior nursing staff Critical care outreach staff Intensive care consultants ENT / Maxillo-facial surgical consultants ENT and Critical Care wards have their own supply of tracheostomies. Page 11 of 36
12 Post-procedure investigations and documentation A post-procedure chest X-ray is may be requested, and should be considered mandatory if there have been any difficulty and/or complications during or after insertion Documentation of the procedure should follow standard surgical guidelines and be on the Adult Critical Care Trachesotomy Insertion Booklet (see appendix three), but should include as a minimum: Date and time Name and grade of operator, assistant(s), and anaesthetist or bronchoscopist Description of procedure Drugs given Description of any complications Details of tracheostomy tube inserted Any post-operative instructions NB Where a tracheostomy is inserted because of a blocked or narrowed airway above the tracheostomy site this should be clearly documented at the time of insertion and on any discharge documentation Page 12 of 36
13 Continuing care of patients with tracheostomies within critical care Standard tracheostomy care whilst within critical care should continue as detailed in guidelines concerned with the nursing care for, and weaning management of, patients with tracheostomies. Suture removal and tracheostomy changes Sutures holding tracheostomies in place should be removed on day 5 post insertion unless there is a documented medical reason for them to stay in situ Where a long-stitch to the wall of the trachea is used it should be removed as per the instructions of the surgeon responsible Non-fenestrated tracheostomies may be exchanged for fenestrated tracheostomies at day 14 (or later) after insertion. This may take place in a general ward environment by appropriately trained individuals Where possible no tracheostomy should be exchanged before day 14* *Elective ENT tracheostomies may occasionally require changing at earlier than 14 days and in such cases ENT will be involved in any decision-making process Managing patients with tracheostomies whilst within critical care The ongoing management, care and weaning of patients with tracheostomies is covered in detail by the hospital Tracheostomy Management Protocol (separate document). The following equipment should be immediately available for all patients with a tracheostomy in situ, regardless of which ward they are managed on (i.e. including ICU): Standard resuscitation equipment, including Self-inflating bag and mask Oxygen with face-masks (non-rebreathing type) and tracheostomy masks Working suction and suction catheters Intubation equipment (including Bougie) and a range of endotracheal tubes Laryngeal mask airway device Dilating tracheostomy forceps Spare tracheostomy inner-tube appropriate for tracheostomy in place (i.e. dedicated to the patient and their tracheostomy) Page 13 of 36
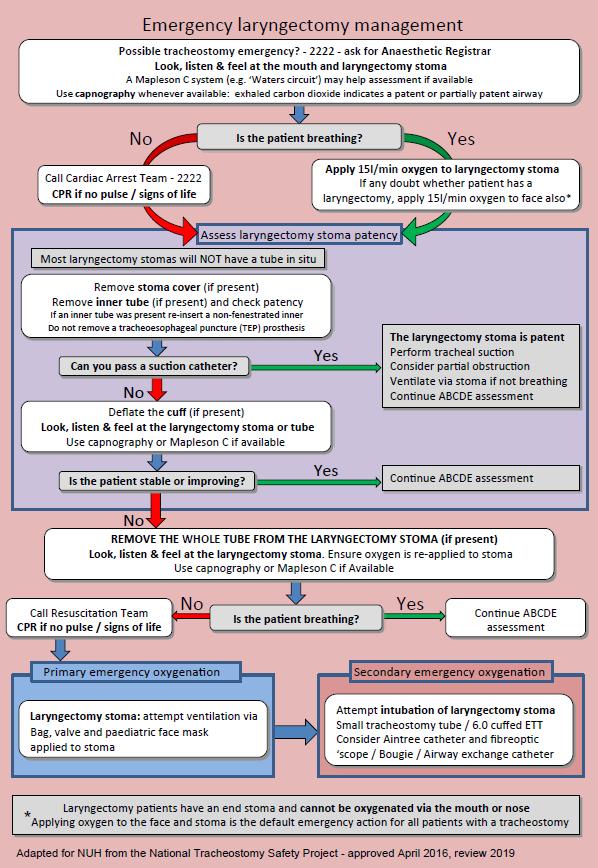
14 Managing complications of tracheostomies Complications may occur with tracheostomies at any time, but are more likely in the time immediately following insertion or during mechanical ventilation on the ICU. Potential complications include: Obstruction of inner tube Dislodged tracheostomy Complete loss of airway Airway haemorrhage Persistent tracheostomy cuff leak Management of emergencies in ward patients should be managed according to the following guidelines, performing in sequence as required Airway obstruction / breathing difficulties: The National Tracheostomy Safety Project algorithms (as modified for NUH) should be followed see Emergency tracheostomy management patent upper airway and Emergency laryngectomy management in Appendix Four. These algorithms should be by every bed space in patients with a tracheostomy and are also available on the trust intranet and guidelines app. The Tracheostomy Passport also contains the Emergency tracheostomy management patent upper airway algorithm. 1. Apply oxygen to the nose/mouth and tracheostomy 2. Remove inner tube and suction patient 3. Call ICU / Anaesthesia / Outreach 4. If at any time the patient is in-extremis (i.e. profoundly low oxygen saturations / cyanosis / new unconsciousness / severe bradycardia or tachycardia) call arrest team AND ICU doctors and follow the emergency algorithms 2222 Major airway haemorrhage causing airway obstruction: Page 14 of 36
15 1. Apply oxygen to the nose/mouth and tracheostomy 2. Call arrest team AND ICU doctors Attempt to suction excess blood Page 15 of 36
16 For all other minor problems (including minor dislodgement, and persistent tracheostomy cuff leak) check that airway is not compromised and contact Critical Care Outreach or ICU doctors. In ICU the above guidelines also apply with the following alterations: In ventilated patients oxygen fraction should be increased to 100% Where haemorrhage is present a member of staff should immediately be detailed to find out the most recent coagulation results and relay this information to the ICU doctor In any case that is not minor the ICU consultant should be informed In any case that is not minor a member of staff should be detailed to obtain a bronchoscope and light-source from the nearest available store Page 16 of 36
17 Weaning whilst within critical care Weaning patients with tracheostomies whilst on intensive care will be done according to the ICU ventilation and weaning guidelines (separate document), and Tracheostomy Weaning Guidelines (separate document) Please note that this may involve periods of cuff deflation or a Passey-Muir valve (also known as a one-way valve, or phonate / speaking valve) at the discretion of the senior ICU nursing or medical staff, or following involvement of Critical Care Outreach. Passey-Muir valves (also known as a one-way valve, or phonate / speaking valve) must ONLY BE USED WITH FENESTRATED TRACHEOSTOMIES. They must not be used with non-fenestrated tracheostomy tubes (see appendix four). Planned tracheostomy changes and decannulation Planned tracheostomy changes (i.e. not done as an emergency) Tracheostomies inserted in ICU patients should not normally be changed for the first 14 days after the initial tracheostomy Any changes must be approved by an ICU consultant (or where appropriate ENT / Maxillo-facial consultants) The change must only be done by an appropriately trained individual. Such individuals may include: ICU consultants, ENT / Maxillo-facial consultants, many senior ICU trainees and anaesthetic trainees, many members of Critical Care Outreach (who have their own training guidelines) Decannulation (i.e. complete removal of the tracheostomy, not done as an emergency) can occur at any time once the patient is appropriately weaned but only if approved by an ICU consultant, ENT / Maxillo-facial consultant or appropriately trained member of CCOT. Following decannulation a patient may suffer complications including airway obstruction. Patient monitoring, including oxygen saturation monitoring should continue for at least 30 minutes after decannulation. Page 17 of 36
18 Equipment that must be immediately available on the ward at the time of a planned tracheostomy change or at the time of decannulation includes: Standard Self-inflating bag and mask resuscitation Oxygen with face-masks (non-rebreathing type) and equipment, including tracheostomy masks Working suction and suction catheters Intubation equipment (including Bougie) and a range of endotracheal tubes Laryngeal mask airway device Dilating tracheostomy forceps Spare tracheostomy inner-tube appropriate for tracheostomy Swallowing assessments Patients with tracheostomies often have impaired swallowing reflexes and can still aspirate oral contents into the lungs even with a cuffed tracheostomy tube. Patients with tracheostomies should be kept nil-by-mouth unless an appropriate member of staff has performed a swallowing assessment. Examples of staff who can safely perform tracheostomy swallow assessment include: Speech and language therapists Appropriately trained critical care outreach staff Even after a successful swallow assessment there is still the possibility that a patient s swallow reflex may deteriorate. If aspiration is suspected the patient should again be kept nil-by-mouth until a further swallow assessment can take place. NB: while patients may be able to safely swallow with a tracheostomy tube in situ they will require close supervision. This may be possible in a critical care environment but not on general wards due to staffing ratios. If in doubt keep patients nil-by-mouth and request a Speech and Language Therapist assessment. Page 18 of 36
19 Discharge from ICU At time of discharge from ICU a record should be made in any discharge summary of the type of tracheostomy (i.e. fenestrated or non-fenestrated, and with or without inner-tube), as well as the date of insertion and any relevant instructions (for example where sutures are still in situ). The ongoing management, care and weaning of patients with tracheostomies is covered in detail by the hospital Tracheostomy Management Protocol (separate document) and should be documented within the Tracheostomy Passport Where a tracheostomy is inserted because of a blocked or narrowed airway above the tracheostomy site this should be clearly documented at the time of insertion and on any discharge documentation Provisions for audit Percutaneous tracheostomy procedures and outcomes are subject to regular audit. Page 19 of 36
20 References: Mackenzie S, Murphy P, Bodenham A, et al Standards for the care of adult patients with a temporary tracheostomy Intensive Care Society 2009 Fikkers BG, van Veen JA, Kooloos JG, et al Emphysema and Pneumothorax After Percutaneous Tracheostomy Case Reports and an Anatomic Study Chest 2004; 125: Eggert SM, Jerwood C Percutaneous tracheostomy Brit J Anaesth CEPD Reviews 2003; 3(5): Beiderlinden M, Karl Walz M, Sander A, et al Complications of bronchoscopically guided percutaneous dilational tracheostomy: beyond the learning curve Intensive Care Med 2002; 28:59 62 Krishnan K, Elliot SC, Mallick A The current practice of tracheostomy in the United Kingdom: a postal survey Anaesthesia 2005; 60: Hinerman R, Alvarez F, Keller CA Outcome of bedside percutaneous tracheostomy with bronchoscopic guidance Intensive Care Med 2000; 226: Pothermann W, Tonner PH, Schulte am Esch J. Percutaneous dilatational tracheostomy: risks and benefits Intensive Care Med 1997; 23: MPS Guide to Consent in the UK Medical Protection Society 2008 Good practice in consent - Achieving the NHS Plan commitment to patientcentred consent practice NHS Executive 2001 MPS Guide to Medical Records Medical Protection Society 2008 Page 20 of 36
21 Appendix One Page 21 of 36
22 Page 22 of 36
23 Page 23 of 36
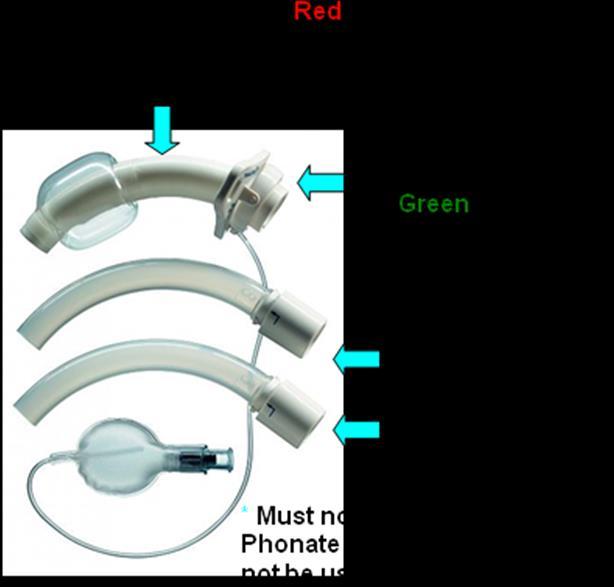
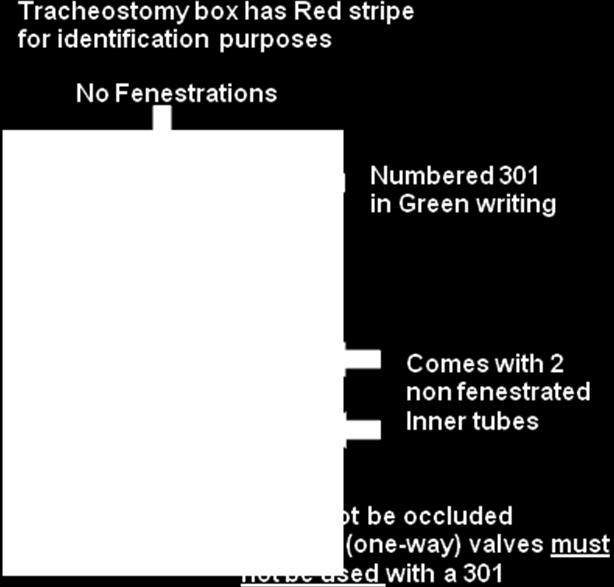
24 Appendix Two Document NUH03501N to be included here Appendix Three (Addendum: Different types of tracheostomy tubes are currently being evaluated within Nottingham University Hospitals and within the Mid-Trent Critical Care Network. Should any change in the range of tracheostomy tubes available within Critical Care be required, this guideline will be updated appropriately and an education and training package will be implemented.) Kapitex Tracoe 301 (and inner tubes) The Tracoe 301 is standard percutaneous and surgical tracheostomy inserted in critical care patients. It has an inner tube and is nonfenestrated and cannot be used with one-way (phonate) valves. Size 8 will be the most common size inserted, though some patients may require a larger or smaller size. 24
25 25
 where there is unlikely to be a need for immediate postoperative ventilation.")

26 Kapitex Tracoe 302 (and inner tubes) The Tracoe 302 may also be used in critical care patients but will not normally be used as the first tracheostomy tube (i.e. it should not be the very first tube inserted when the tracheostomy is performed unless there are exceptional circumstances). Tracoe 302s may be inserted by maxilla-facial / ENT surgeons (even at first-insertion) where there is unlikely to be a need for immediate postoperative ventilation. The Tracoe 302 may also be inserted into patients who require extra assistance during the weaning phase (i.e. they already have a 301 in place and this is swapped for a 302) this should not normally within the first 14 days following first-insertion. The outer tracheostomy of a 302 is fenestrated and it has two inner tubes that can be used with it, one is fenestrated whilst the other is not. One-way (phonate) valves may be used with Tracoe 302s (but not 301s). This should only be done under the guidance of critical care outreach staff. 26

27 Portex Uniperc adjustable flange tube (and inner tubes) The Portex Uniperc adjustable flange is a flexible tube that may be used in patients with abnormal anatomy. It is not fenestrated and has inner tubes that should be used. It is suitable for first-insertion in critical care patients instead f the Tracoe 301. Where the Tracoe 301 cannot be inserted at the time of initial tracheostomy in ICU patients because of difficult anatomy (i.e. lots of subcutaneous neck tissue) the Portex Uniperc adjustable flange tracheostomy may be inserted instead. As an adjustable flange tracheostomy the tube should be carefully positioned at tracheostomy and a note made of the distances markings on the tube at the level of the skin. Care should be taken not to allow the tube to move inwards or outwards from this point unless ICU, ENT or Maxillofacial consultants direct such a repositioning. 27

28 Moore tube (and inner tubes) The Moore tube is a flexible soft tube that may be used in patients with abnormal anatomy. It will not be used as the first-insertion percutaneous tracheostomy and is unlikely to be used as the first-insertion surgical tracheostomy except in exceptional circumstances. Its main use will be in the weaning phase of patients with difficult anatomy (i.e. in patients who have another tracheostomy in place it may occasionally be swapped for a Moore tube at the discretion of ICU, ENT or Maxillo-facial consultants). Because it is flexible it may not be suitable for patients at risk of gross swelling around the tracheostomy site. It is not fenestrated or cuffed but has inner tubes. 28
 but have no cuff.")

29 Tracoe 303 and 304 uncuffed tubes (and inner tubes) In some situations Tracoe 303 or Tracoe 304 tubes may be used. These are similar to 301 and 302 tubes (previously mentioned) but have no cuff. Because they have no cuffs they are not suitable for first-insertion tracheostomy tubes in patients who are likely to require ventilation, except in exceptional circumstances. They may be used at the discretion of ICU, ENT or Maxillo-facial consultants. 29

30 Portex Blue-line adjustable flange tube (has NO inner tube) Portex adjustable flange tracheostomy tubes are single lumen tubes (i.e. they have no inner tube) that may be used in critical care patients in exceptional circumstances. They are not fenestrated. As an adjustable flange tracheostomy the tube should be carefully positioned at tracheostomy and a note made of the distances markings on the tube at the level of the skin. Care should be taken not to allow the tube to move inwards or outwards from this point unless ICU, ENT or Maxillofacial consultants direct such a repositioning. Patients with single-lumen tubes in should only be nursed in specialist ward areas (ICU, HDU, ENT wards). 30
31 The above tracheostomy tubes are those most likely to be used in critically ill patients. The subspecialist areas of ENT surgery and Maxillo-facial surgery (for example tracheostomy management in laryngectomy patients) may use different tubes for which separate guidelines are available. Newer versions of the above tubes may become available at a later date and may include separate suction ports for subglottic secretion drainage. These guidelines will be updated if and when such tracheostomies become widely used in critical care patients. 31
32 Comparison of tubes (all measurements are in mm) Size Length Inner tube Outer tube outer diameter Comments inner diameter (at neck) Tracoe Un-fenestrated First-line ICU tracheostomy Tracoe Fenestrated Portex Uniperc 7 adjustable Un-fenestrated adjustable flange 8 adjustable adjustable adjustable 10 unavailable Moore tube Un-fenestrated No cuff Tracoe No cuff Tracoe Un-fenestrated No cuff Portex blue-line adjustable flange adjustable Un-fenestrated 8 adjustable No inner tube 9 adjustable adjustable

33 Appendix Four 33
34 34
35 Appendix Five Equality Impact Assessment Report 1. Name of Policy or Service Response to external best practice policy 2. Responsible Manager Owen Bennett (Clinical Quality, Risk and Safety Manager) 3. Name of person Completing EIA Dr Allan Howatson (Consultant in Intensive Care and Anaesthesia) 4. Date EIA Completed 28/06/ Description and Aims of Policy/Service This clinical guideline has been written to inform adult critical care staff of how to safely manage critically ill patients requiring a tracheostomy. 6. Brief Summary of Research and Relevant Data There is no research or relevant data at the present time. 7. Methods and Outcome of Consultation Consultations have been carried out with the following: Adult critical care consultants and senior nurses Comments from the above consultations have been received and incorporated where appropriate. 8. Results of Initial Screening or Full Equality Impact Assessment: Equality Group Age Assessment of Impact No Impact Identified 35
36 Gender Race Sexual Orientation Religion or belief Disability Dignity and Human Rights Working Patterns Social Deprivation No Impact Identified No Impact Identified No Impact Identified No Impact Identified No Impact Identified No Impact Identified No Impact Identified No Impact Identified 9. Decisions and/or Recommendations (including supporting rationale) From the information contained in the procedure, and following the initial screening, it is my decision that a full assessment is not required at the present time. 10. Equality Action Plan (if required) N/A 11. Monitoring and Review Arrangements 36
Tracheostomy and laryngectomy airway emergencies: an overview for medical and nursing staff
 2013 Medical Journal Tracheostomy and laryngectomy airway emergencies: an overview for medical and nursing staff Steven Lobaz 1 and Paul Bush 2 1 ST6 and 2 Consultant Department of Anaesthesia and Intensive
2013 Medical Journal Tracheostomy and laryngectomy airway emergencies: an overview for medical and nursing staff Steven Lobaz 1 and Paul Bush 2 1 ST6 and 2 Consultant Department of Anaesthesia and Intensive
Foundations of Critical Care Nursing Course. Tracheostomy Workbook
 Foundations of Critical Care Nursing Course Tracheostomy Workbook 1 Key Reference: Dawson D (2014) Essential principles:trachepstomy care in the adult patient, Nursing in Critical Care, Vol 19, 2 p.63-72.
Foundations of Critical Care Nursing Course Tracheostomy Workbook 1 Key Reference: Dawson D (2014) Essential principles:trachepstomy care in the adult patient, Nursing in Critical Care, Vol 19, 2 p.63-72.
Emergency)tracheostomy)management)/)Patent)upper)airway)
tracheostomy)management)/)Patent)upper)airway)") Emergency)tracheostomy)management)/)Patent)upper)airway) Call,for,airway,expert,help,,Look,,listen,&,feel,at,the,mouth,and,tracheostomy) A)Mapleson)C)system)(e.g.) Waters)circuit ))may)help)assessment)if)available)
Emergency)tracheostomy)management)/)Patent)upper)airway) Call,for,airway,expert,help,,Look,,listen,&,feel,at,the,mouth,and,tracheostomy) A)Mapleson)C)system)(e.g.) Waters)circuit ))may)help)assessment)if)available)
Competency 1: General principles and equipment required to safely manage a patient with a tracheostomy tube.
 Competency 1: General principles and equipment required to safely manage a patient with a tracheostomy tube. Trainee Name: ------------------------------------------------------------- Title: ---------------------------------------------------------------
Competency 1: General principles and equipment required to safely manage a patient with a tracheostomy tube. Trainee Name: ------------------------------------------------------------- Title: ---------------------------------------------------------------
Changing tracheostomy tubes
 Changing tracheostomy tubes Changing the tracheostomy tube should be a multidisciplinary decision. The first change should always be performed or supervised by a suitably trained member of the medical
Changing tracheostomy tubes Changing the tracheostomy tube should be a multidisciplinary decision. The first change should always be performed or supervised by a suitably trained member of the medical
Disclosures. Learning Objectives. Coeditor/author. Associate Science Editor, American Heart Association
 Tracheotomy Challenges for airway specialists Elizabeth H. Sinz, MD Professor of Anesthesiology & Neurosurgery Associate Dean for Clinical Simulation Disclosures Coeditor/author Associate Science Editor,
Tracheotomy Challenges for airway specialists Elizabeth H. Sinz, MD Professor of Anesthesiology & Neurosurgery Associate Dean for Clinical Simulation Disclosures Coeditor/author Associate Science Editor,
Tracheostomy. Hope Building Neurosurgery
 Tracheostomy Hope Building Neurosurgery 0161 206 5055 All Rights Reserved 2017. Document for issue as handout. Unique Identifier: CS36(17). Review date: November 2019 What is a tracheostomy? A tracheostomy
Tracheostomy Hope Building Neurosurgery 0161 206 5055 All Rights Reserved 2017. Document for issue as handout. Unique Identifier: CS36(17). Review date: November 2019 What is a tracheostomy? A tracheostomy
Tracheostomy management Kate Regan MRCP FRCA Katharine Hunt FRCA
 Kate Regan MRCP FRCA Katharine Hunt FRCA The use of tracheostomy has increased over recent years. Traditionally, it was confined to the emergency management of upper airway obstruction; more recently,
Kate Regan MRCP FRCA Katharine Hunt FRCA The use of tracheostomy has increased over recent years. Traditionally, it was confined to the emergency management of upper airway obstruction; more recently,
Tracheostomy. Information for patients and relatives
 Tracheostomy Information for patients and relatives page 2 What is a tracheostomy? A tracheostomy is a small hole (stoma) made at the front of the neck, which goes into the trachea (windpipe). A tube called
Tracheostomy Information for patients and relatives page 2 What is a tracheostomy? A tracheostomy is a small hole (stoma) made at the front of the neck, which goes into the trachea (windpipe). A tube called
Title of Guideline (must include the word Guideline (not protocol, policy, procedure etc)
") Title of Guideline (must include the word Guideline (not protocol, policy, procedure etc) Contact Name and Job Title (author) Guideline on the management of excessive coumarin anticoagulation in adults
Title of Guideline (must include the word Guideline (not protocol, policy, procedure etc) Contact Name and Job Title (author) Guideline on the management of excessive coumarin anticoagulation in adults
TRACHEOSTOMY EMERGENCIES
 TRACHEOSTOMY EMERGENCIES MODULE: AIRWAY TARGET: ALL ANAESTHETISTS, INTENSIVISTS, ED & ACUTE PHYSICIANS, FOUNDATION DOCTORS BACKGROUND: Around 16% of ICU patients may have a tracheostomy. Life- threatening
TRACHEOSTOMY EMERGENCIES MODULE: AIRWAY TARGET: ALL ANAESTHETISTS, INTENSIVISTS, ED & ACUTE PHYSICIANS, FOUNDATION DOCTORS BACKGROUND: Around 16% of ICU patients may have a tracheostomy. Life- threatening
All bedside percutaneously placed tracheostomies
 Page 1 of 5 Scope: All bedside percutaneously placed tracheostomies Population: All ICU personnel Outcomes: To standardize and outline the steps necessary to safely perform a percutaneous tracheostomy
Page 1 of 5 Scope: All bedside percutaneously placed tracheostomies Population: All ICU personnel Outcomes: To standardize and outline the steps necessary to safely perform a percutaneous tracheostomy
CARING FOR THE TRACHEOSTOMISED PATIENT: WHAT TO LOOK OUT FOR
 CARING FOR THE TRACHEOSTOMISED PATIENT: WHAT TO LOOK OUT FOR DR MOHD NAZRI ALI Anaesthesiologist & Intensivist HRPZ II, Kota Bharu, Kelantan Tracheostomy The Enabling Disability Tracheostomy Are becoming
CARING FOR THE TRACHEOSTOMISED PATIENT: WHAT TO LOOK OUT FOR DR MOHD NAZRI ALI Anaesthesiologist & Intensivist HRPZ II, Kota Bharu, Kelantan Tracheostomy The Enabling Disability Tracheostomy Are becoming
Rota-Trach Double Lumen Tracheostomy Tube VITALTEC
 Rota-Trach Double Lumen Tracheostomy Tube VITALTEC Contents INTRODUCTION HISTORY REVIEW ANATOMY & PHYSIOLOGY OPERATIVE PROCEDURE THE RANGE OF TRACHEOSTOMY TUBES ROTA-TRACH TRACHEOSTOMY TUBE INTRODUCTION
Rota-Trach Double Lumen Tracheostomy Tube VITALTEC Contents INTRODUCTION HISTORY REVIEW ANATOMY & PHYSIOLOGY OPERATIVE PROCEDURE THE RANGE OF TRACHEOSTOMY TUBES ROTA-TRACH TRACHEOSTOMY TUBE INTRODUCTION
Clearing the air.. How to assist and rescue neck breathing patients. Presented by: Don Hall MCD, CCC/SLP Sarah Markel RRT, MHA
 Clearing the air.. How to assist and rescue neck breathing patients Presented by: Don Hall MCD, CCC/SLP Sarah Markel RRT, MHA Learning Objectives Define common terms identified with total (laryngectomy)
Clearing the air.. How to assist and rescue neck breathing patients Presented by: Don Hall MCD, CCC/SLP Sarah Markel RRT, MHA Learning Objectives Define common terms identified with total (laryngectomy)
Other methods for maintaining the airway (not definitive airway as still unprotected):
:") Page 56 Where anaesthetic skills and drugs are available, endotracheal intubation is the preferred method of securing a definitive airway. This technique comprises: rapid sequence induction of anaesthesia
Page 56 Where anaesthetic skills and drugs are available, endotracheal intubation is the preferred method of securing a definitive airway. This technique comprises: rapid sequence induction of anaesthesia
Information resource for the safer management of patients with tracheostomies and laryngectomies
 Information resource for the safer management of patients with tracheostomies and laryngectomies Draft guidance for review November 2010 2 Introduction This guide is a resource to help promote and facilitate
Information resource for the safer management of patients with tracheostomies and laryngectomies Draft guidance for review November 2010 2 Introduction This guide is a resource to help promote and facilitate
*gurgle* *snore* *slaver* Tracheostomy Emergencies with Trachy Tracey Helen Lyall ACCP LUHT 03/06/2016
 *gurgle* *snore* *slaver* Tracheostomy Emergencies with Trachy Tracey Helen Lyall ACCP LUHT 03/06/2016 Learning objectives Describe the difference in anatomy between a tracheotomy and a laryngectomy Understand
*gurgle* *snore* *slaver* Tracheostomy Emergencies with Trachy Tracey Helen Lyall ACCP LUHT 03/06/2016 Learning objectives Describe the difference in anatomy between a tracheotomy and a laryngectomy Understand
Oral care & swallowing
 Oral care & swallowing Oral care is important as it has a role to play in preventing healthcare associated infections. Dental plaque and the oropharynx can become colonized by bacteria and a biofilm can
Oral care & swallowing Oral care is important as it has a role to play in preventing healthcare associated infections. Dental plaque and the oropharynx can become colonized by bacteria and a biofilm can
Policies and Procedures. I.D. Number: 1154
 Policies and Procedures Title: TRACHEOSTOMY TUBE CHANGE - PEDIATRIC I.D. Number: 1154 Authorization: [X ] SHR Nursing Practice Committee Source: Nursing Date Effective: October 2008 Date Revised: March
Policies and Procedures Title: TRACHEOSTOMY TUBE CHANGE - PEDIATRIC I.D. Number: 1154 Authorization: [X ] SHR Nursing Practice Committee Source: Nursing Date Effective: October 2008 Date Revised: March
Translaryngeal tracheostomy
 Translaryngeal tracheostomy Issued: August 2013 NICE interventional procedure guidance 462 guidance.nice.org.uk/ipg462 NICE has accredited the process used by the NICE Interventional Procedures Programme
Translaryngeal tracheostomy Issued: August 2013 NICE interventional procedure guidance 462 guidance.nice.org.uk/ipg462 NICE has accredited the process used by the NICE Interventional Procedures Programme
Safer Tracheostomy Care Course
 Patients Name: Samira Patel Patients Age / DOB: 65 year old female on a general ward Major Medical Problem Blocked tracheostomy tube Learning Goal Medical Early recognition of respiratory distress Understanding
Patients Name: Samira Patel Patients Age / DOB: 65 year old female on a general ward Major Medical Problem Blocked tracheostomy tube Learning Goal Medical Early recognition of respiratory distress Understanding
Tracheostomy Sim Course
 Patients Name: Robert Smith Patients Age / DOB: 45 year old gentleman on medical ward Major Medical Problem Displaced tracheostomy tube Learning Goal Medical Early recognition of displaced tracheostomy
Patients Name: Robert Smith Patients Age / DOB: 45 year old gentleman on medical ward Major Medical Problem Displaced tracheostomy tube Learning Goal Medical Early recognition of displaced tracheostomy
Tracheostomy management
 BJA Education, 15 (3): 149 153 (2015) doi: 10.1093/bjaceaccp/mku008 Advance Access Publication Date: 25 April 2014 Matrix reference 1C02, 2A01, 3A01 Tracheostomy management Katharine Hunt MBBS FRCA 1,
BJA Education, 15 (3): 149 153 (2015) doi: 10.1093/bjaceaccp/mku008 Advance Access Publication Date: 25 April 2014 Matrix reference 1C02, 2A01, 3A01 Tracheostomy management Katharine Hunt MBBS FRCA 1,
Full Range of Tracheostomy Solutions
 Full Range of Tracheostomy Solutions Every Breath Counts Choices by Setting Throughout the hospital or home Smiths Medical tracheostomy tubes are designed for performance ER The Portex Cricothyroidotomy
Full Range of Tracheostomy Solutions Every Breath Counts Choices by Setting Throughout the hospital or home Smiths Medical tracheostomy tubes are designed for performance ER The Portex Cricothyroidotomy
Kapitex Healthcare. making things clearer for tracheostomy patients
 Kapitex Healthcare making things clearer for tracheostomy patients preface In publishing this booklet, Kapitex Healthcare Ltd hopes to provide information and understanding for both the patient and carer
Kapitex Healthcare making things clearer for tracheostomy patients preface In publishing this booklet, Kapitex Healthcare Ltd hopes to provide information and understanding for both the patient and carer
Tracheostomy discharge information. Information for community nurses, patients and carers
 Tracheostomy discharge information Information for community nurses, patients and carers What is a tracheostomy? A tracheostomy is a surgical incision (cut) through the neck tissues into the trachea leaving
Tracheostomy discharge information Information for community nurses, patients and carers What is a tracheostomy? A tracheostomy is a surgical incision (cut) through the neck tissues into the trachea leaving
TRACHEOSTOMY 186 INTENSIVE CARE
 186 INTENSIVE CARE Table 7.4 Indications for tracheostomy Upper-airway obstruction Prolonged mechanical ventilation To facilitate bronchopulmonary toilet To maintain and protect the airway use of oral
186 INTENSIVE CARE Table 7.4 Indications for tracheostomy Upper-airway obstruction Prolonged mechanical ventilation To facilitate bronchopulmonary toilet To maintain and protect the airway use of oral
Tracheostomy: Procedures, Timing and Tubes
 TRACHEOSTOMY: PROCEDURES, TIMING AND TUBES Gail M. Sudderth RRT Clinical Specialist Passy-Muir Inc. gsudderth@passy-muir.com (949) 833-8255 Objectives Explain how the timing of the tracheotomy and tube
TRACHEOSTOMY: PROCEDURES, TIMING AND TUBES Gail M. Sudderth RRT Clinical Specialist Passy-Muir Inc. gsudderth@passy-muir.com (949) 833-8255 Objectives Explain how the timing of the tracheotomy and tube
Policy x.xxx. Issued: Artificial Airways and Airway Care. ABC Home Medical Company Policy & Procedure Manual. A. Tracheostomy Tubes ( trach tubes)
") A. Tracheostomy Tubes ( trach tubes) A tracheotomy is a surgical procedure whereby an opening is cut into the trachea of the patient for the purpose of inserting a tube (trach tube). The trach tube allows
A. Tracheostomy Tubes ( trach tubes) A tracheotomy is a surgical procedure whereby an opening is cut into the trachea of the patient for the purpose of inserting a tube (trach tube). The trach tube allows
The essential principles of tracheostomy care
 The essential principles of tracheostomy care Deborah Dawson Consultant Nurse Critical Care Excellence in specialist and community healthcare Key publications https://www.stgeorges.nhs.uk/gps-andclinicians/clinical-resources/tracheostomyguidelines/
The essential principles of tracheostomy care Deborah Dawson Consultant Nurse Critical Care Excellence in specialist and community healthcare Key publications https://www.stgeorges.nhs.uk/gps-andclinicians/clinical-resources/tracheostomyguidelines/
Major complications of airway management in the United Kingdom
 The Royal College of Anaesthetists The Difficult Airway Society 4th National Audit Project of The Royal College of Anaesthetists and The Difficult Airway Society Major complications of airway management
The Royal College of Anaesthetists The Difficult Airway Society 4th National Audit Project of The Royal College of Anaesthetists and The Difficult Airway Society Major complications of airway management
Having a Bronchoscopy
 Having a Bronchoscopy Department of Respiratory Medicine 2 Patient Information This leaflet will help you and your family to understand more about bronchoscopy. Please read it and ask any questions you
Having a Bronchoscopy Department of Respiratory Medicine 2 Patient Information This leaflet will help you and your family to understand more about bronchoscopy. Please read it and ask any questions you
Section 4.1 Paediatric Tracheostomy Introduction
 Bite- sized training from the GTC Section 4.1 Paediatric Tracheostomy Introduction This is one of a series of bite- sized chunks of educational material developed by the Global Tracheostomy Collaborative.
Bite- sized training from the GTC Section 4.1 Paediatric Tracheostomy Introduction This is one of a series of bite- sized chunks of educational material developed by the Global Tracheostomy Collaborative.
(ix) Difficult & Failed Intubation Queen Charlotte s Hospital
 Difficult & Failed Intubation Queen Charlotte s Hospital") (ix) Difficult & Failed Intubation Queen Charlotte s Hospital Pre-operative Assessment Clinical assessment of airway and risk of difficult intubation: (can be performed in a matter of seconds): 1. Mouth
(ix) Difficult & Failed Intubation Queen Charlotte s Hospital Pre-operative Assessment Clinical assessment of airway and risk of difficult intubation: (can be performed in a matter of seconds): 1. Mouth
COMMUNICATION. Communication and Swallowing post Tracheostomy. Role of SLT. Impact of Tracheostomy. Normal Speech. Facilitating Communication
 Communication and Swallowing post Tracheostomy. Role of SLT 1. 2. 3. Management of communication needs. Management of swallowing issues. Working with the multidisciplinary team to facilitate weaning. Impact
Communication and Swallowing post Tracheostomy. Role of SLT 1. 2. 3. Management of communication needs. Management of swallowing issues. Working with the multidisciplinary team to facilitate weaning. Impact
Airway complications on the general medical unit after prolonged ICU admission
 Airway complications on the general medical unit after prolonged ICU admission Palash Kar Discipline of Acute Care Medicine, University of Adelaide Intensive Care Unit, Royal Adelaide Hospital, Adelaide,
Airway complications on the general medical unit after prolonged ICU admission Palash Kar Discipline of Acute Care Medicine, University of Adelaide Intensive Care Unit, Royal Adelaide Hospital, Adelaide,
28 th September Author Jeremy Gilbert Bariatric Nurse Specialist
 POLICY FOR SELF ADMINISTRATION OF CONTINUOUS POSITIVE AIRWAY PRESSURE BY COMPETENT PATIENTS COMING IN FOR METABOLIC AND OBESITY SURGERY (BARIATRIC SURGERY) TO PENDENNIS WARD 28 th September 2014 Author
POLICY FOR SELF ADMINISTRATION OF CONTINUOUS POSITIVE AIRWAY PRESSURE BY COMPETENT PATIENTS COMING IN FOR METABOLIC AND OBESITY SURGERY (BARIATRIC SURGERY) TO PENDENNIS WARD 28 th September 2014 Author
National Hospital for Neurology and Neurosurgery
 National Hospital for Neurology and Neurosurgery Venous sinus stents (for the treatment of venous sinus stenosis and idiopathic intracranial hypertension) Lysholm Department of Neuroradiology If you would
National Hospital for Neurology and Neurosurgery Venous sinus stents (for the treatment of venous sinus stenosis and idiopathic intracranial hypertension) Lysholm Department of Neuroradiology If you would
DOWNLOAD OR READ : TRACHEOSTOMY MANAGEMENT PDF EBOOK EPUB MOBI
 DOWNLOAD OR READ : TRACHEOSTOMY MANAGEMENT PDF EBOOK EPUB MOBI Page 1 Page 2 tracheostomy management tracheostomy management pdf tracheostomy management Tracheostomy is a common procedure in intensive
DOWNLOAD OR READ : TRACHEOSTOMY MANAGEMENT PDF EBOOK EPUB MOBI Page 1 Page 2 tracheostomy management tracheostomy management pdf tracheostomy management Tracheostomy is a common procedure in intensive
Collaborative Regional Benchmarking Group (North of England, North Yorkshire & Humber and West Yorkshire)
") Collaborative Regional Benchmarking Group (North of England, North Yorkshire & Humber and West Yorkshire) Best Practice Guidance Endo Tracheal Tube Care These recommendations are based on the current evidence
Collaborative Regional Benchmarking Group (North of England, North Yorkshire & Humber and West Yorkshire) Best Practice Guidance Endo Tracheal Tube Care These recommendations are based on the current evidence
TRACHEOSTOMY CARE. Tracheostomy- Surgically created hole that extends from the neck skin into the windpipe or trachea.
 1 TRACHEOSTOMY CARE Definitions: Trachea-Windpipe Tracheostomy- Surgically created hole that extends from the neck skin into the windpipe or trachea. Outer Cannula- The outer part of a trach tube. Usually
1 TRACHEOSTOMY CARE Definitions: Trachea-Windpipe Tracheostomy- Surgically created hole that extends from the neck skin into the windpipe or trachea. Outer Cannula- The outer part of a trach tube. Usually
Tracheostomy Guidelines for NHS Wales
 Tracheostomy Guidelines for NHS Wales Prepared by the All Wales Tracheostomy Advisory Group, chaired by Duncan Ingrams, Assistant Medical Director ABUHB. 1 Introduction April 2018 Formulating one set of
Tracheostomy Guidelines for NHS Wales Prepared by the All Wales Tracheostomy Advisory Group, chaired by Duncan Ingrams, Assistant Medical Director ABUHB. 1 Introduction April 2018 Formulating one set of
Tracheostomy. Intensive Care Unit Patient Information Leaflet
 Tracheostomy Intensive Care Unit Patient Information Leaflet Introduction This leaflet is for patients having a tracheostomy and their relatives. It gives information on the procedure, and its benefits
Tracheostomy Intensive Care Unit Patient Information Leaflet Introduction This leaflet is for patients having a tracheostomy and their relatives. It gives information on the procedure, and its benefits
Long-gap Oesophageal Atresia
 Long-gap Atresia A guide for parents Nate (6 weeks old) Atresia Research Association Are there different types of OA? There are four main types of oesophageal atresia with or without TOF. These include
Long-gap Atresia A guide for parents Nate (6 weeks old) Atresia Research Association Are there different types of OA? There are four main types of oesophageal atresia with or without TOF. These include
Original Article Percutaneous dilational tracheostomy: An initial experience in community based teaching hospital
 Kathmandu University Medical Journal (2006), Vol. 4, No. 3, Issue 15, 275-280 Original Article Percutaneous dilational tracheostomy: An initial experience in community based teaching hospital Joshi S 1,
Kathmandu University Medical Journal (2006), Vol. 4, No. 3, Issue 15, 275-280 Original Article Percutaneous dilational tracheostomy: An initial experience in community based teaching hospital Joshi S 1,
Flexible bronchoscopy
 National Cancer Institute (unknown photographer) Turnberg Building Respiratory Medicine 0161 206 4575 Page 1 of 6 G18041101W. Design Services, Salford Royal NHS Foundation Trust, All Rights Reserved 2018.
National Cancer Institute (unknown photographer) Turnberg Building Respiratory Medicine 0161 206 4575 Page 1 of 6 G18041101W. Design Services, Salford Royal NHS Foundation Trust, All Rights Reserved 2018.
Welcome to the Specialized Medical Services respiratory training webinar series!
 Welcome to the Specialized Medical Services respiratory training webinar series! SMS is your LTC facility single source for oxygen, medical equipment, respiratory care services and supplies nationwide.
Welcome to the Specialized Medical Services respiratory training webinar series! SMS is your LTC facility single source for oxygen, medical equipment, respiratory care services and supplies nationwide.
Day care adenotonsillectomy in sleep apnoea
 Day care adenotonsillectomy in sleep apnoea Title of Guideline (must include the word Guideline (not protocol, policy, procedure etc) Day care adenotonsillectomy in presence of sleep apnoea 1a 2a 2b Contact
Day care adenotonsillectomy in sleep apnoea Title of Guideline (must include the word Guideline (not protocol, policy, procedure etc) Day care adenotonsillectomy in presence of sleep apnoea 1a 2a 2b Contact
8/8/2013. Disclaimer. Tracheostomy Care in the Home. Polling Question 1. Upper Airway and Respiratory System
 Disclaimer Appendix 3 Declaration of Vested Interest Form Name of presenter: Heather Murgatroyd RRT RPSGT Name of employer: DeVilbiss Healthcare Tracheostomy Care in the Home Heather Murgatroyd, RRT, RPSGT
Disclaimer Appendix 3 Declaration of Vested Interest Form Name of presenter: Heather Murgatroyd RRT RPSGT Name of employer: DeVilbiss Healthcare Tracheostomy Care in the Home Heather Murgatroyd, RRT, RPSGT
Airway Management in the ICU
 Airway Management in the ICU New developments in management of epistaxis. April 28, 2008 Methods of airway control Non surgical BIPAP CPAP Mask ventilation Laryngeal Mask Intubation Surgical Cricothyrotomy
Airway Management in the ICU New developments in management of epistaxis. April 28, 2008 Methods of airway control Non surgical BIPAP CPAP Mask ventilation Laryngeal Mask Intubation Surgical Cricothyrotomy
TRACHEOSTOMY. Tracheostomy means creation an artificial opening in the trachea with tracheostomy tube insertion
 TRACHEOSTOMY Definition Tracheostomy means creation an artificial opening in the trachea with tracheostomy tube insertion Indications for tracheostomy 1-upper airway obstruction with stridor, air hunger,
TRACHEOSTOMY Definition Tracheostomy means creation an artificial opening in the trachea with tracheostomy tube insertion Indications for tracheostomy 1-upper airway obstruction with stridor, air hunger,
Anatomy and Physiology. The airways can be divided in to parts namely: The upper airway. The lower airway.
 Airway management Anatomy and Physiology The airways can be divided in to parts namely: The upper airway. The lower airway. Non-instrumental airway management Head Tilt and Chin Lift Jaw Thrust Advanced
Airway management Anatomy and Physiology The airways can be divided in to parts namely: The upper airway. The lower airway. Non-instrumental airway management Head Tilt and Chin Lift Jaw Thrust Advanced
Translaryngeal Tracheostomy - TLT Fantoni Method
 Translaryngeal Tracheostomy - TLT Fantoni Method Fantoni A., Ripamonti D., Lesmo A. About the Authors Fantoni Antonio Chief Emeritus of Department of Anaesthesia and Intensive Care - San Carlo Borromeo
Translaryngeal Tracheostomy - TLT Fantoni Method Fantoni A., Ripamonti D., Lesmo A. About the Authors Fantoni Antonio Chief Emeritus of Department of Anaesthesia and Intensive Care - San Carlo Borromeo
AIRWAY MANAGEMENT SOLUTIONS
 KAPITEX HEALTHCARE - SPECIALIST KNOWLEDGE, SUPPORT AND CARE AIRWAY MANAGEMENT SOLUTIONS Specialist tracheostomy management solutions you can trust Kapitex - Adding Quality of Life to Airway Management
KAPITEX HEALTHCARE - SPECIALIST KNOWLEDGE, SUPPORT AND CARE AIRWAY MANAGEMENT SOLUTIONS Specialist tracheostomy management solutions you can trust Kapitex - Adding Quality of Life to Airway Management
Your anaesthetic for heart surgery
 Your anaesthetic for heart surgery Information for patients and carers First Edition 2018 www.rcoa.ac.uk/patientinfo This leaflet gives you information about your anaesthetic for adult heart (cardiac)
Your anaesthetic for heart surgery Information for patients and carers First Edition 2018 www.rcoa.ac.uk/patientinfo This leaflet gives you information about your anaesthetic for adult heart (cardiac)
A CRITICALLY ILL CHILD PRESENTING AT AN ACUTE TRUST- A CLINICAL AND ETHICAL CHALLENGE
 A CRITICALLY ILL CHILD PRESENTING AT AN ACUTE TRUST- A CLINICAL AND ETHICAL CHALLENGE DR SRIKANTH UPPUGONDURI CONSULTANT ANAESTHESTIST NEW CROSS HOSPITAL CALL FROM PAEDIATRIC TEAM CALL FROM PAEDIATRIC
A CRITICALLY ILL CHILD PRESENTING AT AN ACUTE TRUST- A CLINICAL AND ETHICAL CHALLENGE DR SRIKANTH UPPUGONDURI CONSULTANT ANAESTHESTIST NEW CROSS HOSPITAL CALL FROM PAEDIATRIC TEAM CALL FROM PAEDIATRIC
Flow-diverting stents (in the Treatment of intracranial aneurysms)
") National Hospital for Neurology and Neurosurgery Flow-diverting stents (in the Treatment of intracranial aneurysms) Lysholm Department of Neuroradiology If you would like this document in another language
National Hospital for Neurology and Neurosurgery Flow-diverting stents (in the Treatment of intracranial aneurysms) Lysholm Department of Neuroradiology If you would like this document in another language
Weaning guidelines for Spinal Cord Injured patients in Critical Care Units
 RISCI Respiratory Information for Spinal Cord Injury UK Weaning guidelines for Spinal Cord Injured patients in Critical Care Units Introduction It is an unfortunate fact that Spinal Cord Injury Centres
RISCI Respiratory Information for Spinal Cord Injury UK Weaning guidelines for Spinal Cord Injured patients in Critical Care Units Introduction It is an unfortunate fact that Spinal Cord Injury Centres
Title of Guideline (must include the word Guideline (not. Guidelines. Contact Name and Job Title (author)
") Title of Guideline (must include the word Guideline (not protocol, policy, procedure etc) Contact Name and Job Title (author) Directorate & Speciality Date of submission Date on which guideline must be
Title of Guideline (must include the word Guideline (not protocol, policy, procedure etc) Contact Name and Job Title (author) Directorate & Speciality Date of submission Date on which guideline must be
DOCUMENT CONTROL PAGE
 DOCUMENT CONTROL PAGE Title Title: UNDERGOING SPINAL DEFORMITY SURGERY Version: 2 Reference Number: Supersedes Supersedes: all other versions Description of Amendment(s): Revision of analgesia requirements
DOCUMENT CONTROL PAGE Title Title: UNDERGOING SPINAL DEFORMITY SURGERY Version: 2 Reference Number: Supersedes Supersedes: all other versions Description of Amendment(s): Revision of analgesia requirements
Basic Airway Management
 Basic Airway Management Dr. Madhurita Singh, Assoc. Professor, Dept. of Critical Care, CMC Vellore. This is the first module in a series on management of airway and ventilation in critically ill patients.
Basic Airway Management Dr. Madhurita Singh, Assoc. Professor, Dept. of Critical Care, CMC Vellore. This is the first module in a series on management of airway and ventilation in critically ill patients.
SECTION 1: INCLUSION, EXCLUSION & RANDOMISATION INFORMATION
 SECTION 1: INCLUSION, EXCLUSION & RANDOMISATION INFORMATION DEMOGRAPHIC INFORMATION Given name Family name Date of birth Consent date Gender Female Male Date of surgery INCLUSION & EXCLUSION CRITERIA YES
SECTION 1: INCLUSION, EXCLUSION & RANDOMISATION INFORMATION DEMOGRAPHIC INFORMATION Given name Family name Date of birth Consent date Gender Female Male Date of surgery INCLUSION & EXCLUSION CRITERIA YES
Laparoscopic partial removal of the kidney
 Laparoscopic partial removal of the kidney Department of Urology 2 Patient Information What evidence is this information based on? This booklet includes advice from consensus panels, the British Association
Laparoscopic partial removal of the kidney Department of Urology 2 Patient Information What evidence is this information based on? This booklet includes advice from consensus panels, the British Association
Surgical Care at the District Hospital. EMERGENCY & ESSENTIAL SURGICAL CARE
 Surgical Care at the District Hospital 1 14 Practical Anesthesia Key Points 2 14.1 General Anesthesia Have a clear plan before starting anesthesia Never use an unfamiliar anesthetic technique in an emergency
Surgical Care at the District Hospital 1 14 Practical Anesthesia Key Points 2 14.1 General Anesthesia Have a clear plan before starting anesthesia Never use an unfamiliar anesthetic technique in an emergency
Epidural Infusions for Pain Relief Including Discharge Advice
 Royal Manchester Children s Hospital Epidural Infusions for Pain Relief Including Discharge Advice Children s Pain Team- Information For Parents and Carers This leaflet aims to provide information for
Royal Manchester Children s Hospital Epidural Infusions for Pain Relief Including Discharge Advice Children s Pain Team- Information For Parents and Carers This leaflet aims to provide information for
AIRWAY MANAGEMENT AND VENTILATION
 AIRWAY MANAGEMENT AND VENTILATION D1 AIRWAY MANAGEMENT AND VENTILATION Basic airway management and ventilation The laryngeal mask airway and Combitube Advanced techniques of airway management D2 Basic
AIRWAY MANAGEMENT AND VENTILATION D1 AIRWAY MANAGEMENT AND VENTILATION Basic airway management and ventilation The laryngeal mask airway and Combitube Advanced techniques of airway management D2 Basic
Percutaneous nephrolithotomy (PCNL)
") PLEASE PRINT WHOLE FORM DOUBLE SIDED ON YELLOW PAPER Patient Information to be retained by patient affix patient label What does this procedure involve? The breakdown and removal of kidney stones using
PLEASE PRINT WHOLE FORM DOUBLE SIDED ON YELLOW PAPER Patient Information to be retained by patient affix patient label What does this procedure involve? The breakdown and removal of kidney stones using
INDEPENDENT LUNG VENTILATION
 INDEPENDENT LUNG VENTILATION Giuseppe A. Marraro, MD Director Anaesthesia and Intensive Care Department Paediatric Intensive Care Unit Fatebenefratelli and Ophthalmiatric Hospital Milan, Italy gmarraro@picu.it
INDEPENDENT LUNG VENTILATION Giuseppe A. Marraro, MD Director Anaesthesia and Intensive Care Department Paediatric Intensive Care Unit Fatebenefratelli and Ophthalmiatric Hospital Milan, Italy gmarraro@picu.it
PEMSS PROTOCOLS INVASIVE PROCEDURES
 PEMSS PROTOCOLS INVASIVE PROCEDURES Panhandle Emergency Medical Services System SURGICAL AND NEEDLE CRICOTHYROTOMY Inability to intubate is the primary indication for creating an artificial airway. Care
PEMSS PROTOCOLS INVASIVE PROCEDURES Panhandle Emergency Medical Services System SURGICAL AND NEEDLE CRICOTHYROTOMY Inability to intubate is the primary indication for creating an artificial airway. Care
P01. Title of Guideline (must include the word Guideline (not protocol, policy, procedure etc) P01 Guideline for Peak flow recording
 P01 Guideline for Peak flow recording") Title of Guideline (must include the word Guideline (not protocol, policy, procedure etc) Contact Name and Job Title (author) Directorate & Speciality Guideline for Peak flow recording Caroline Youle,
Title of Guideline (must include the word Guideline (not protocol, policy, procedure etc) Contact Name and Job Title (author) Directorate & Speciality Guideline for Peak flow recording Caroline Youle,
Audit on Tracheostomies Performed at the General Intensive Care Unitt Kuala Lumpur Hospital
 ORIGINAL ARTICLE Audit on Tracheostomies Performed at the General Intensive Care Unitt Kuala Lumpur Hospital A S Rao, FANZCA, L Mansor, FRCA, K Inbasegaran, FANZCA Department of Anaesthesia and Intensive
ORIGINAL ARTICLE Audit on Tracheostomies Performed at the General Intensive Care Unitt Kuala Lumpur Hospital A S Rao, FANZCA, L Mansor, FRCA, K Inbasegaran, FANZCA Department of Anaesthesia and Intensive
Transcatheter Aortic Valve Implantation Procedure (TAVI)
") Page 1 of 5 Procedure (TAVI) Introduction Aortic stenosis (AS) is a common heart valve problem associated with heart failure and death. Surgical valve repair or replacement is recommended if AS patients
Page 1 of 5 Procedure (TAVI) Introduction Aortic stenosis (AS) is a common heart valve problem associated with heart failure and death. Surgical valve repair or replacement is recommended if AS patients
Competency Title: Continuous Positive Airway Pressure
 Competency Title: Continuous Positive Airway Pressure Trainee Name: ------------------------------------------------------------- Title: ---------------------------------------------------------------
Competency Title: Continuous Positive Airway Pressure Trainee Name: ------------------------------------------------------------- Title: ---------------------------------------------------------------
Pacemaker and AV Node Ablation Patient Information
 Melbourne Heart Rhythm Pacemaker and AV Node Ablation Patient Information The Heart The heart is a pump responsible for maintaining blood supply to the body. It has four chambers. The two upper chambers
Melbourne Heart Rhythm Pacemaker and AV Node Ablation Patient Information The Heart The heart is a pump responsible for maintaining blood supply to the body. It has four chambers. The two upper chambers
COBIS Management of airway burns and inhalation injury PAEDIATRIC
 COBIS Management of airway burns and inhalation injury PAEDIATRIC 1 A multidisciplinary team should provide the management of the child with inhalation injury. Childhood inhalation injury mandates transfer
COBIS Management of airway burns and inhalation injury PAEDIATRIC 1 A multidisciplinary team should provide the management of the child with inhalation injury. Childhood inhalation injury mandates transfer
H: Respiratory Care. Saskatchewan Association of Licensed Practical Nurses, Competency Profile for LPNs, 3rd Ed. 79
 H: Respiratory Care Saskatchewan Association of Licensed Practical Nurses, Competency Profile for LPNs, 3rd Ed. 79 Competency: H-1 Airway Management H-1-1 H-1-2 H-1-3 H-1-4 H-1-5 Demonstrate knowledge
H: Respiratory Care Saskatchewan Association of Licensed Practical Nurses, Competency Profile for LPNs, 3rd Ed. 79 Competency: H-1 Airway Management H-1-1 H-1-2 H-1-3 H-1-4 H-1-5 Demonstrate knowledge
Interfacility Protocol Protocol Title:
 Interfacility Protocol Protocol Title: Mechanical Ventilator Monitoring & Management Original Adoption Date: 05/2009 Past Protocol Updates 05/2009, 12/2013 Date of Most Recent Update: March 23, 2015 Medical
Interfacility Protocol Protocol Title: Mechanical Ventilator Monitoring & Management Original Adoption Date: 05/2009 Past Protocol Updates 05/2009, 12/2013 Date of Most Recent Update: March 23, 2015 Medical
2010 National Audit of Dementia (Care in General Hospitals) North West London Hospitals NHS Trust
 North West London Hospitals NHS Trust") Royal College of Psychiatrists 2010 National Audit of Dementia (Care in General Hospitals) Organisational checklist results and commentary for: rth West London Hospitals NHS Trust The 2010 national audit
Royal College of Psychiatrists 2010 National Audit of Dementia (Care in General Hospitals) Organisational checklist results and commentary for: rth West London Hospitals NHS Trust The 2010 national audit
Self- Assessment. Self- assessment checklist
 Self- Assessment Peer Review Self- assessment checklist (Based on RCA guidelines for the provision of anaesthetic services 2004, RCA/AA Guide for Departments of Anaesthesia 2002, NSF for children Standard
Self- Assessment Peer Review Self- assessment checklist (Based on RCA guidelines for the provision of anaesthetic services 2004, RCA/AA Guide for Departments of Anaesthesia 2002, NSF for children Standard
Feasibility of Percutaneous Dilatational Tracheostomy with a Light Source in the Surgical Intensive Care Unit
 Acute and Critical Care 2018 May 33(2):89-94 / ISSN 2586-6052 (Print) ㆍ ISSN 2586-6060 (Online) Original Article Feasibility of Percutaneous Dilatational Tracheostomy with a Light Source in the Surgical
Acute and Critical Care 2018 May 33(2):89-94 / ISSN 2586-6052 (Print) ㆍ ISSN 2586-6060 (Online) Original Article Feasibility of Percutaneous Dilatational Tracheostomy with a Light Source in the Surgical
Neonatal Airway Disorders, Treatments, and Outcomes. Steven Goudy, MD Pediatric Otolaryngology Emory University Medical Center
 Neonatal Airway Disorders, Treatments, and Outcomes Steven Goudy, MD Pediatric Otolaryngology Emory University Medical Center Disclosure I have nothing to disclose Neonatal and Pediatric Tracheostomy Tracheostomy
Neonatal Airway Disorders, Treatments, and Outcomes Steven Goudy, MD Pediatric Otolaryngology Emory University Medical Center Disclosure I have nothing to disclose Neonatal and Pediatric Tracheostomy Tracheostomy
Risky Extubation. Andy Higgs. Warrington Hospitals Cheshire UK
 Andy Higgs Warrington Hospitals Cheshire UK Declaration COOKMEDICAL Extubation plan DAS guideline Airway Exchange Catheters # 11 CAEC post maxillo-facial surgery Used as intubation stylets Airway Exchange
Andy Higgs Warrington Hospitals Cheshire UK Declaration COOKMEDICAL Extubation plan DAS guideline Airway Exchange Catheters # 11 CAEC post maxillo-facial surgery Used as intubation stylets Airway Exchange
ASPIRATION DURING ANAESTHESIA
 ASPIRATION DURING ANAESTHESIA MODULE: CRITICAL INCIDENTS TARGET: ALL ANAESTHETISTS BACKGROUND: Passive regurgitation or vomiting can occur during the pre-, peri- or post- operative period risking aspiration
ASPIRATION DURING ANAESTHESIA MODULE: CRITICAL INCIDENTS TARGET: ALL ANAESTHETISTS BACKGROUND: Passive regurgitation or vomiting can occur during the pre-, peri- or post- operative period risking aspiration
Can't Intubate, Can't oxygenate (CICO) The new terminology What is the Military Experience What is the Civilian Experience What is your role.
 The new terminology What is the Military Experience What is the Civilian Experience What is your role.") Disclaimer The views in the presentation are the author's, and do not reflect the views of the Department of Defence I am a full time Australian Defence Force Procedural Specialist (Anaesthetist) Can't
Disclaimer The views in the presentation are the author's, and do not reflect the views of the Department of Defence I am a full time Australian Defence Force Procedural Specialist (Anaesthetist) Can't
How do you use a bougie as an airway adjunct for endotracheal intubation?
 Ruth Bird, MBBCh -Specialist Registrar: Anaesthesia & Paediatric Trauma Fellow Daniel Nevin, MBBCh -Consultant in Anaesthesia & Pre-Hospital Care The Royal London Hospital London s Air Ambulance (HEMS)
Ruth Bird, MBBCh -Specialist Registrar: Anaesthesia & Paediatric Trauma Fellow Daniel Nevin, MBBCh -Consultant in Anaesthesia & Pre-Hospital Care The Royal London Hospital London s Air Ambulance (HEMS)
Department of Vascular Surgery Femoral to Femoral or Iliac to Femoral Crossover Bypass Graft
 Department of Vascular Surgery Femoral to Femoral or Iliac to Femoral Crossover Bypass Graft Why do you need this operation? You need this operation because you have either pain in your legs or a leg ulcer
Department of Vascular Surgery Femoral to Femoral or Iliac to Femoral Crossover Bypass Graft Why do you need this operation? You need this operation because you have either pain in your legs or a leg ulcer
Tumescent Liposuction
 Standards & Guidelines October 2015 v5 Serving the public by guiding the medical profession Revision date: October 2015 v5 Approval date: September 1999 Originating Committee: Advisory Committee on Non-Hospital
Standards & Guidelines October 2015 v5 Serving the public by guiding the medical profession Revision date: October 2015 v5 Approval date: September 1999 Originating Committee: Advisory Committee on Non-Hospital
2010 National Audit of Dementia (Care in General Hospitals) Chelsea and Westminster Hospital NHS Foundation Trust
 Chelsea and Westminster Hospital NHS Foundation Trust") Royal College of Psychiatrists 2010 National Audit of Dementia (Care in General Hospitals) Organisational checklist results and commentary for: NHS Foundation Trust The 2010 national audit of dementia
Royal College of Psychiatrists 2010 National Audit of Dementia (Care in General Hospitals) Organisational checklist results and commentary for: NHS Foundation Trust The 2010 national audit of dementia
If you have any further questions, please speak to a doctor or nurse caring for you.
 Surgical Removal of a Paraganglioma of the Temporal Bone This leaflet explains more about surgery for the removal of a paraganglioma of the temporal bone, including the benefits, risks and any alternatives
Surgical Removal of a Paraganglioma of the Temporal Bone This leaflet explains more about surgery for the removal of a paraganglioma of the temporal bone, including the benefits, risks and any alternatives
Advanced Airway Management. University of Colorado Medical School Rural Track
 Advanced Airway Management University of Colorado Medical School Rural Track Advanced Airway Management Basic Airway Management Airway Suctioning Oxygen Delivery Methods Laryngeal Mask Airway ET Intubation
Advanced Airway Management University of Colorado Medical School Rural Track Advanced Airway Management Basic Airway Management Airway Suctioning Oxygen Delivery Methods Laryngeal Mask Airway ET Intubation
PERCUTANEOUS NEPHROLITHOTOMY
 PERCUTANEOUS NEPHROLITHOTOMY AN INFORMATION LEAFLET Written by: Department of Urology May 2011 Stockport Tel: 0161 419 5698 Website: www.stockport.nhs.uk Tameside Tel: 0161 922 6696/6698 Website: www.tameside.nhs.uk
PERCUTANEOUS NEPHROLITHOTOMY AN INFORMATION LEAFLET Written by: Department of Urology May 2011 Stockport Tel: 0161 419 5698 Website: www.stockport.nhs.uk Tameside Tel: 0161 922 6696/6698 Website: www.tameside.nhs.uk
Non-invasive Ventilation protocol For COPD
 NHS LANARKSHIRE MONKLANDS HOSPITAL Non-invasive Ventilation protocol For COPD April 2017 S Baird Review Date: Oct 2019 Approved by Medical Directorate Indications for Non-Invasive Ventilation (NIV) NIV
NHS LANARKSHIRE MONKLANDS HOSPITAL Non-invasive Ventilation protocol For COPD April 2017 S Baird Review Date: Oct 2019 Approved by Medical Directorate Indications for Non-Invasive Ventilation (NIV) NIV
LESSON ASSIGNMENT. After completing this lesson, you should be able to:
 LESSON ASSIGNMENT LESSON 3 Cricothyroidotomy LESSON ASSIGNMENT Paragraphs 3-1 through 3-7. LESSON OBJECTIVES After completing this lesson, you should be able to: 3-1. Define cricothyroidotomy. 3-2. Identify
LESSON ASSIGNMENT LESSON 3 Cricothyroidotomy LESSON ASSIGNMENT Paragraphs 3-1 through 3-7. LESSON OBJECTIVES After completing this lesson, you should be able to: 3-1. Define cricothyroidotomy. 3-2. Identify
Clinical Guideline for Intravenous Opioids for Adults in Recovery Areas The Recovery Protocol
 Clinical Guideline for Intravenous Opioids for Adults in Recovery Areas The Recovery Protocol 1. Aim/Purpose of this Guideline 1.1. To Provide safe and efficient administration of Opioids in Recovery.
Clinical Guideline for Intravenous Opioids for Adults in Recovery Areas The Recovery Protocol 1. Aim/Purpose of this Guideline 1.1. To Provide safe and efficient administration of Opioids in Recovery.
Inserting a percutaneous biliary drain and biliary stent (a tube to drain bile)
") Patient information - Radiology Unit Tel 0118 322 7991 Inserting a percutaneous biliary drain and biliary stent (a tube to drain bile) Introduction This leaflet tells you about the procedures known as
Patient information - Radiology Unit Tel 0118 322 7991 Inserting a percutaneous biliary drain and biliary stent (a tube to drain bile) Introduction This leaflet tells you about the procedures known as
1.3. A Registration standard for conscious sedation has been adopted by the Dental Board of Australia.
 Policy Statement 6.17 Conscious Sedation in Dentistry 1 (Including the ADA Recommended Guidelines for Conscious Sedation in Dentistry and Guidelines for the Administration of Nitrous Oxide Inhalation Sedation
Policy Statement 6.17 Conscious Sedation in Dentistry 1 (Including the ADA Recommended Guidelines for Conscious Sedation in Dentistry and Guidelines for the Administration of Nitrous Oxide Inhalation Sedation
Needle biopsy of lung or pleura (lining of the lung) (guided by ultrasound or CT scanner)
 (guided by ultrasound or CT scanner)") Needle biopsy of lung or pleura (guided by ultrasound or CT scanner) Turnberg Building Respiratory Medicine 0161 206 4039 Page 1 of 6 Document for issue as handout. Unique Identifier: MED23(18). Review
Needle biopsy of lung or pleura (guided by ultrasound or CT scanner) Turnberg Building Respiratory Medicine 0161 206 4039 Page 1 of 6 Document for issue as handout. Unique Identifier: MED23(18). Review
Clinical Guidelines for Tracheostomy Care. On behalf of the Tracheostomy Care Group, South Tees Hospitals NHS FT. June 2017 Tracheostomy Care Group 1
 June 2017 On behalf of the Tracheostomy Care Group, South Tees Hospitals NHS FT June 2017 Tracheostomy Care Group 1 TABLE OF CONTENTS 1. INTRODUCTION... 4 Key Issues... 5 Tracheostomy Care Group at South
June 2017 On behalf of the Tracheostomy Care Group, South Tees Hospitals NHS FT June 2017 Tracheostomy Care Group 1 TABLE OF CONTENTS 1. INTRODUCTION... 4 Key Issues... 5 Tracheostomy Care Group at South
Having a PEG tube inserted
 Having a PEG tube inserted This information leaflet is for patients who are having a PEG (Percutaneous Endoscopic Gastrostomy) tube inserted. It explains what is involved, what to expect and what significant
Having a PEG tube inserted This information leaflet is for patients who are having a PEG (Percutaneous Endoscopic Gastrostomy) tube inserted. It explains what is involved, what to expect and what significant