Sedation in The ICU: The Biological Cost of the Depression of Consciousness
|
|
|
- Abel Sherman
- 6 years ago
- Views:
Transcription




1 Sedation in The ICU: The Biological Cost of the Depression of Consciousness Michael Ramsay MD FRCA Chairman Department of Anesthesia Baylor University Medical Center Professor Texas A&M University Clinical Professor UT Southwestern Medical School President Baylor Research Institute Dallas Texas Cognition
2 Speaker Disclosure I have received research grants from Masimo Corp.
3 Postoperative cognitive impairment at extremes of life and with critical illness in response to depth of sedation and anesthesia Sedation Depth under Spinal Anesthesia and Survival in Elderly Patients Undergoing Hip Fracture Repair. Brown CH et al. Anesth Analg 2014; 118: Presence of EEG burst suppression in sedated critically ill patients is associated with increased mortality. Watson PL et al. Crit Care Med 2008;36: Long-term differences in language and cognitive function after childhood exposure to anesthesia. al. Pediatrics 2012;130:e Ing C et

4 Pediatrics 136; July 2015

5

6
7

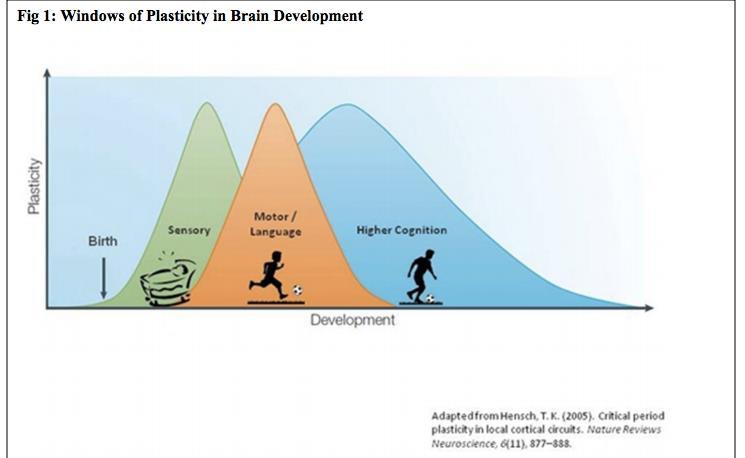
8 Anne E. Takesian*, Takao K. Hensch*,{, Prog Brain Res 2013;207:3-34
9
10
11 Long-Term Cognitive Impairment after Critical Illness Pandharipande et al. N Engl J Med 2013; 369: Patients in medical and surgical ICUs are at a high risk for long-term cognitive impairment. A longer duration of delirium in the hospital was associated with worse global cognition and executive function scores at 3 months (40%)(P=0.001) and 12 months (34%)(P=0.004) 40% equivalent to TBI 26% equivalent to mild Alzheimer s
12 Causes of Neurologic Failure Trauma/Increasing ICP Circulatory shock Hypoxemia/Hypoperfusion/Vasospasm Infection Systemic inflammation Metabolic and endocrine imbalances Pharmacologic agents;?benzodiazepines

13 Acute Brain Dysfunction During Critical Illness Result of Inflammation Causing Endothelial Dysfunction Hughes et al Anesthesiology 2013; 118:631-9
14 Petty TL. Suspended Life or Extending Death? Chest 1998;114:360 But what I see these days are sedated patients, lying without motion, appearing to be dead, except for the monitors that tell me otherwise.. By being awake and alert they could interact with family.feel human sustain the zest for living which is a requirement for survival
15 One Year Outcomes in Survivors of ARDS Herridge et al. NEMJ 2003;348: Functional limitations 1 year later Most patients have muscle wasting and weakness. Neurocognitive impairments. Hopkins & Brett. Cur Opin Crit Care 2005;11:369 Depression and memory dysfunction increased in ARDS survivors. Chest 2009;135:678
16 Over Sedation in ICU Excessive sustained alteration in consciousness Prolonged time on mechanical ventilation Increased ventilator associated pneumonia Increased prolonged muscular weakness Annals of Intensive Care 2013, 3:24
17 Consciousness No consciousness meter Consciousness: I can see, hear, smell and spatially perceive objects Awareness of surroundings, time, orientation. How can you measure it?
18 Ramsay Sedation Scale 1 Anxious and agitated or restless or both 2 Cooperative, oriented, and tranquil 3 Responding to commands only 4 Asleep, brisk response to stimuli* 5 Asleep, sluggish response to stimuli* 6 Asleep, no response to stimuli* * light glabellar tap Ramsay, et al. Brit Med J. 1974;2(920):
19
20 Richmond Agitation Sedation Scale (RASS) Score State + 4 Combative + 3 Very agitated + 2 Agitated + 1 Restless 0 Alert and calm -1 Drowsy eye contact > 10 sec -2 Light sedation eye contact < 10 sec -3 Moderate sedation no eye contact -4 Deep sedation physical stimulation -5 Unarousable no response even with physical Verbal Stimulus Physical Stimulus Ely EW, et al. JAMA. 2003;289: Sessler CN, et al. Am J Respir Crit Care Med. 2002;166(10):

21 Critical Care Medicine 2013; 41:
22 Pain and Analgesia Pain is common in ICU patients Assessment should be routine (+1B) These are the most valid and reliable tools if patient unable to self-report: The Behavioral Pain Scale (BPS) (B) Critical Care Observation Tool (CPOT) (B)
23 Treatment of Pain Multimodal Pharmacological & non-pharmacological (music, massage, sleep) Opioids 1 st line for non-neuropathic pain All available IV opioids titrated to similar pain intensity endpoints equally effective Use non-opioids to limit side effects of opioids NSAIDs acetominophen, ibuprofen renal/liver function, risk bleed??? Dexmedetomidine reduce need for opioids Neuropathic Pain: Enteral gabapentin or carbamazepine in addition to IV opioids Consider regional LA +/- opioids Check coagulation Clear neuraxial spine Monitor volume status carefully
24 Agitation & Sedation Monitor for depth of sedation Use protocols for monitoring, reassess regularly Richmond agitation sedation scale (RASS) & Sedation-Agitation Scale (SAS) most valid & reliable scales for assessing quality & Depth of Sedation: Recommend objective measures of brain function (BIS, Sedline (PSI), SE, AEP, & NI) as 1 method to monitor Depth of Sedation in comatose and/or paralyzed patients. Monitor EEG for non-convulsive seizure activity
25 Sedation Controlled lighter sedation better than deeper sedation unless clinically contraindicated Maintain cognitive function Shorter length mechanical ventilation, LOS in ICU and hospital
26 Delirium Routinely monitor for delirium Confusion Assessment Method in the ICU (CAM- ICU ) Intensive Care Delirium Screening Checklist (ICDSC) most valid & reliable delirium monitoring tools Quick & reliable
27 DELIRIUM Prevention & Early mobilization as able Treatment No clear cut pharmacological agent or protocol appears to prevent delirium Haloperidol, atypical antipsychotics, DO NOT appear to prevent delirium Dexmedetomidine and atypical antipsychotics may shorten the duration of delirium No evidence of efficacy for haloperidol BZ use may be a risk factor for delirium Conflicting data on risk of various opioids
28 Strategy Whole-body rehabilitation Animation with a highly coordinated, multidisciplinary team implementing: Co-operative sedation Spontaneous breathing trials Good Analgesia Physical and occupational therapy RESULTS IN: Superior functional and cognitive patient outcomes WD Schweickert, MC Pohlman, AS Pohlman et al LANCET 2009;373:
29 Daily Wake-up Study: Clinical Outcomes Mechanical ventilation duration (days) Wake-up Group 4.9 ( ) Standard of Care Group 7.3 ( ) ICU LOS (days) 6.4 ( ) 9.9 ( ) *P=.004. P=.02 Adapted from Kress et al. N Engl J Med. 2000;342:1474.
30 Girard TD, et al. ABC Trial The Lancet 2008; Daily Awakening Sedation combined with Spontaneous Breathing Trial Adding Respiratory Therapy to Sedation Team duration of MV; ICU & Hosp LOS; Improved 1 year mortality 30
31 ICU SEDATION TEAM RN Patient MD
32 ICU SEDATION TEAM RN Patient MD RPh
33 ICU SEDATION TEAM RN RT Patient RPh MD
34 ICU SEDATION TEAM RN PT/OT RPh Patient RT MD

35
36 The Animated ICU Minimize neuromuscular blockade Sedation strategies to avoid accumulation and prolonged effects Early physical therapy Reduce/avoid opiates Dexmedetomidine allows interactive safe comfortable care in many patients
37 Analgosedation Patients should be in the COMFORT ZONE Analgesia with cognitive sedation Protect the brain and the mind Aim for early extubation, mobilization and conversation ANALGOSEDATION without coma or delirium
38 Cognitive ICU

39
40
41 The Effect of a Positive Affect In severe illness a positive affect is related to survival in a dose-response pattern. Positive affect can be considered a resource for medium-term survival Scherer & Hermann-Lingen. Gen Hosp Psych 2009;31:8-13
42 Baylor Sedation Strategies Comfort, Calm and Co-operative: Dexmedetomidine mcgs/kg.h plus low dose fentanyl. Titrate to RSS 2-3 Moderate Sedation: Propofol up to 50 mcgs/kg/min. Titrate to RSS 3-4. Plus fentanyl Deep Sedation: Fentanyl and midazolam infusion and SedLine Root monitoring and titrate to RSS 5-6
43 Pitfall of Pulse Oximetry The pulse oximeter is a LATE detector of respiratory depression if supplemental oxygen is being administered

44 Fu ES, Downs JB, Schweiger JW, et al. Supplemental oxygen impairs detection of hypoventilation by pulse oximetry. Chest Nov; 126(5):
45 35 yr old Liver Transplant ph 6.86 pco2 148 po2 202 HCO3 25 Recipient Patient 8 hours postop in ICU, sitting in chair with nasal cannula O 2 at 3l/min. RN in room documenting on computer Rounded on patient and RN says she is doing well O 2 sat 98% I found her unresponsive and RR 4. O2 Sat 98% 45
46
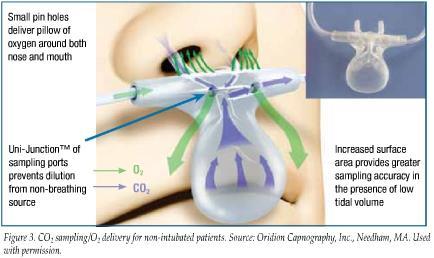
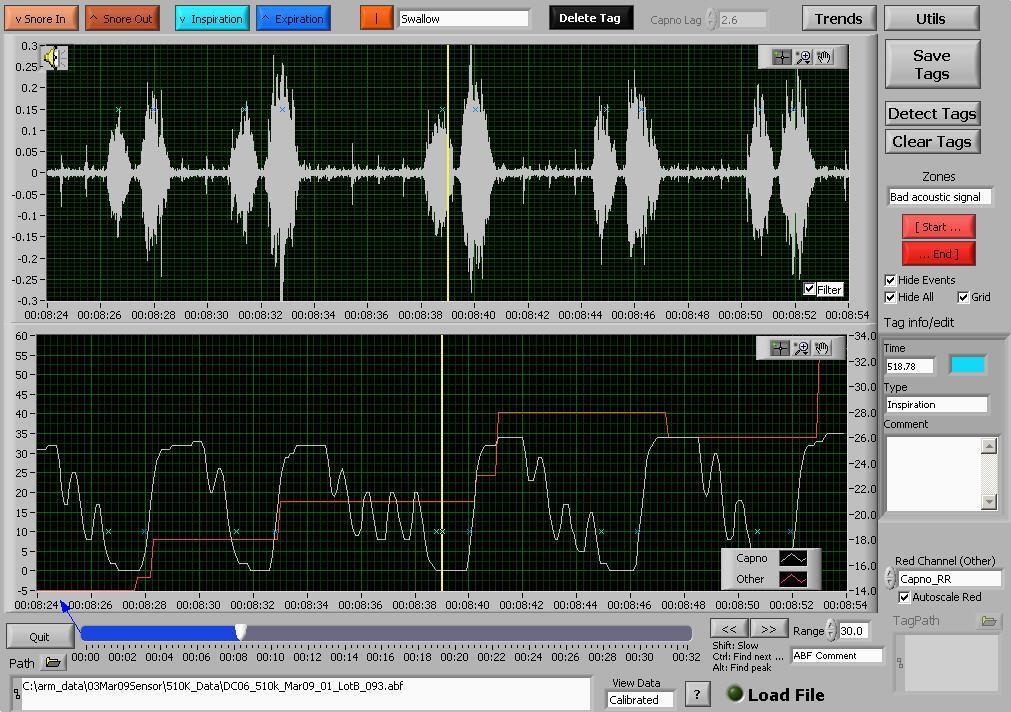
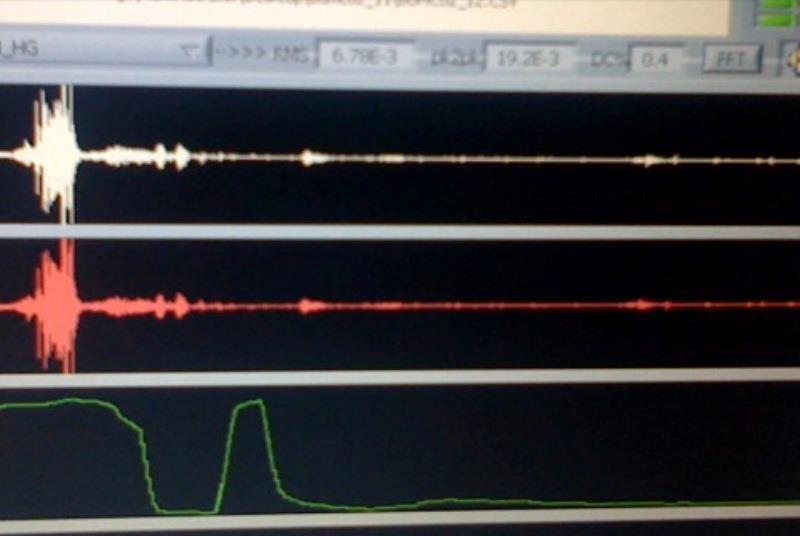
47 Current Respiration Rate Methods Physical assessment (intermittent) Transthoracic impedance (continuous) Requires monitor and ECG electrodes As chest expands impedance changes Respiration rate measured from cyclical changes in impedance Cannot differentiate PARADOXICAL breathing with no air movement Capnography (continuous) Direct monitoring of the inhaled and exhaled concentration or partial pressure of CO2 using sensor mask or nasal cannula Respiration rate measured by CO2 waveform analysis Shape of waveform can provide additional information Hypoventilation may result in LOW EtCO2 because of poor alveolar exchange
48 Human Observation Intermittent Cannot be audited Should assess: Respiratory Rate; Pattern; Depth; Quality Difficult to distinguish CO2 narcosis from natural sleep
49 Transthoracic Impedance Plethysmography The changing air volumes in the lungs alter thoracic impedance. Continuous monitor of respiratory rate Historically has been limited in detecting obstructed breathing Newer technology is more sensitive and more accurate and measues TV, MV and RR. Voscopoulos et al. Anesth Analg 2013;117:91 100)
50 Airflow Sensors Sensors can detect airflow as expired air is warmer more humid and contains carbon dioxide. Temperature: Real-time infrared thermography. In the neonate respiration was monitored based on a 0.3 degree C to 0.5 degree C temperature difference between inspiration and expiration. Abbas et al. Biomed Eng Online 2011:10:93. Humidity: A miniature optical humidity sensor is placed on a face mask and measures water vapor of exhaled air. Mathew et al. Biomed Opt Express 2012;3:3325
51 Photoplethysmography Derived Respiratory Rate RR oxi Continuous monitoring of respiratory rate, SpO2 and pulse rate. Derives respiratory rate from the variability in baseline of the plethysmogram The pleth variability index can predict fluid responsiveness in the mechanically ventilated patient Sensitive to movement artifacts and vasoconstriction Obstructed airflow affects pleth signal does this affect rate calculation?
52 Capnography Capnography measures ventilation and provides a graphical waveform available for interpretation
53
 may help clinicians assess respiratory status and help determine treatment options")
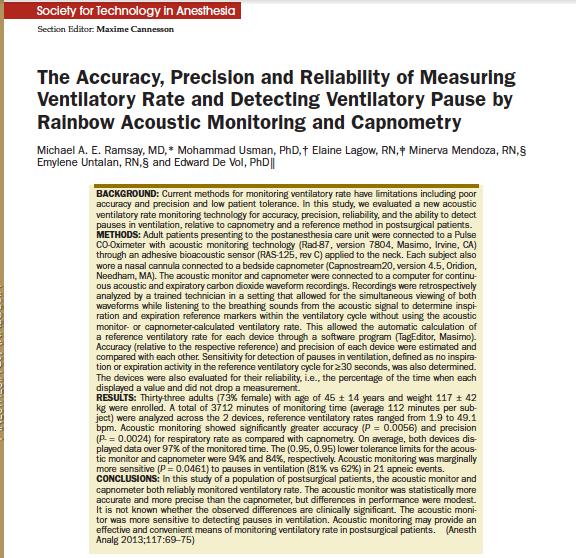
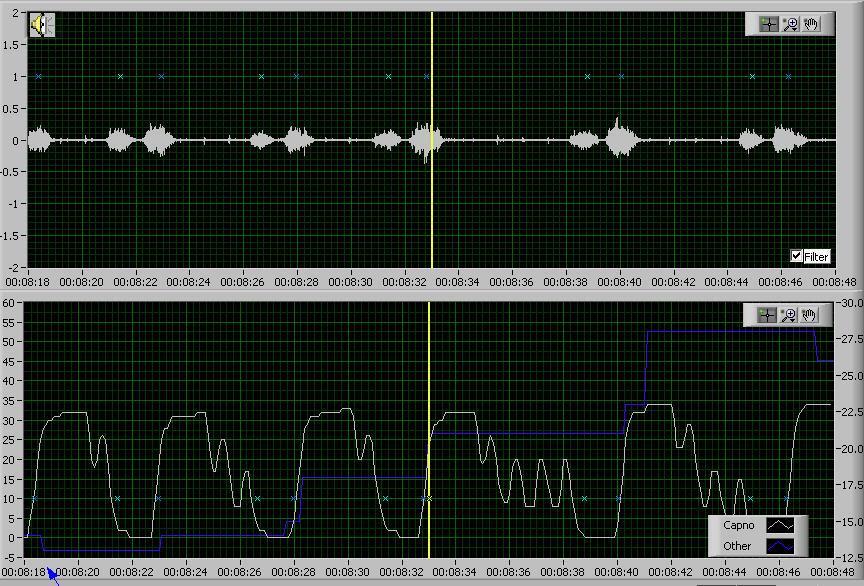
54 Acoustic Respiration Rate (RRa) Accurate > Easy-to-Use > Patient-Tolerant When used with other clinical variables, first-ever continuous and noninvasive monitoring of acoustic respiration rate (RRa) may help clinicians assess respiratory status and help determine treatment options
55
56
57
58 Snore Out
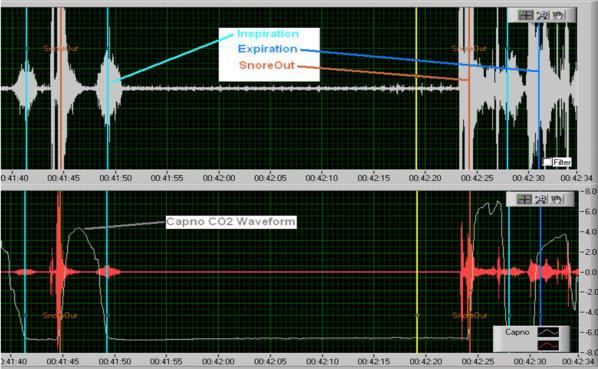
59 Snore Out
60
61 Breathing is Good!

62 Thanks for your attention
Respiratory Rate. Disclosure: Research grants and honoraria from Masimo Corp
 Respiratory Rate Acoustic Monitoring Michael Ramsay MD Chairman, Department of Anesthesia Baylor University Medical Center President, Baylor Research Institute Professor, Texas A&M Health Science Center
Respiratory Rate Acoustic Monitoring Michael Ramsay MD Chairman, Department of Anesthesia Baylor University Medical Center President, Baylor Research Institute Professor, Texas A&M Health Science Center
Monitoring the Brain
 Cognition Monitoring the Brain Michael Ramsay MD FRCA Chairman Department of Anesthesia Baylor University Medical Center President Baylor Research Institute Dallas Texas Speaker Disclosure I have received
Cognition Monitoring the Brain Michael Ramsay MD FRCA Chairman Department of Anesthesia Baylor University Medical Center President Baylor Research Institute Dallas Texas Speaker Disclosure I have received
Sedation and delirium- drugs and clinical management
 Sedation and delirium- drugs and clinical management Shannon S. Carson, MD Associate Professor and Chief Division of Pulmonary and Critical Care Medicine University of North Carolina Probability of transitioning
Sedation and delirium- drugs and clinical management Shannon S. Carson, MD Associate Professor and Chief Division of Pulmonary and Critical Care Medicine University of North Carolina Probability of transitioning
ICU Liberation for the Pharmacist. A. Kendall Gross, PharmD, BCPS, BCCCP Critical Care Pharmacist UCSF Medical Center
 ICU Liberation for the Pharmacist A. Kendall Gross, PharmD, BCPS, BCCCP Critical Care Pharmacist UCSF Medical Center Disclosure No conflicts of interest to disclose Objectives o Outline the elements of
ICU Liberation for the Pharmacist A. Kendall Gross, PharmD, BCPS, BCCCP Critical Care Pharmacist UCSF Medical Center Disclosure No conflicts of interest to disclose Objectives o Outline the elements of
Ventilator-Associated Event Prevention: Innovations
 Ventilator-Associated Event Prevention: Innovations Michael J. Apostolakos, MD Professor of Medicine Director, Adult Critical Care University of Rochester Mobility/Sedation in the ICU Old teaching: Keep
Ventilator-Associated Event Prevention: Innovations Michael J. Apostolakos, MD Professor of Medicine Director, Adult Critical Care University of Rochester Mobility/Sedation in the ICU Old teaching: Keep
Interaction between Sedation and Weaning: How to Balance Them? Guillermo Castorena MD Fundacion Clinica Medica Sur Mexico
 Interaction between Sedation and Weaning: How to Balance Them? Guillermo Castorena MD Fundacion Clinica Medica Sur Mexico Balance is not that easy! Weaning Weaning is the liberation of a patient from
Interaction between Sedation and Weaning: How to Balance Them? Guillermo Castorena MD Fundacion Clinica Medica Sur Mexico Balance is not that easy! Weaning Weaning is the liberation of a patient from
Managing Delirium: The best way to achieve clarity (of mind) Tim Walsh. Professor of Critical Care, Edinburgh University
 Tim Walsh. Professor of Critical Care, Edinburgh University") Managing Delirium: The best way to achieve clarity (of mind) Tim Walsh Professor of Critical Care, Edinburgh University Lecture Plan: a route to clarity What is delirium? Why is delirium important? Step
Managing Delirium: The best way to achieve clarity (of mind) Tim Walsh Professor of Critical Care, Edinburgh University Lecture Plan: a route to clarity What is delirium? Why is delirium important? Step
DELIRIUM IN ICU: Prevention and Management. Milind Baldi
 DELIRIUM IN ICU: Prevention and Management Milind Baldi Contents Introduction Risk factors Assessment Prevention Management Introduction Delirium is a syndrome characterized by acute cerebral dysfunction
DELIRIUM IN ICU: Prevention and Management Milind Baldi Contents Introduction Risk factors Assessment Prevention Management Introduction Delirium is a syndrome characterized by acute cerebral dysfunction
Pain, Agitation & Delirium (2013) Immobility & Sleep (2018) Catherine Jones Practice Educator GICU October 2018
 Immobility & Sleep (2018) Catherine Jones Practice Educator GICU October 2018") Pain, Agitation & Delirium (2013) Immobility & Sleep (2018) Catherine Jones Practice Educator GICU October 2018 1 Plan for session Why Pain Agitation & Delirium are important considerations in critical
Pain, Agitation & Delirium (2013) Immobility & Sleep (2018) Catherine Jones Practice Educator GICU October 2018 1 Plan for session Why Pain Agitation & Delirium are important considerations in critical
Pain Module. Opioid-RelatedRespiratory Depression (ORRD)
") Pain Module Opioid-RelatedRespiratory Depression (ORRD) Characteristics of patients who are at higher risk for Opioid- Related Respiratory Depression (ORRD) Sleep apnea or sleep disorder diagnosis : typically
Pain Module Opioid-RelatedRespiratory Depression (ORRD) Characteristics of patients who are at higher risk for Opioid- Related Respiratory Depression (ORRD) Sleep apnea or sleep disorder diagnosis : typically
Biological cost of the depression of consciousness
 312 ARTYKUŁ POGLĄDOWY/REVIEW PAPER Otrzymano/Submitted: 25.09.2013. Zaakceptowano/Accepted: 30.09.2013 Akademia Medycyny Biological cost of the depression of consciousness Michael A. E. Ramsay Chairman,
312 ARTYKUŁ POGLĄDOWY/REVIEW PAPER Otrzymano/Submitted: 25.09.2013. Zaakceptowano/Accepted: 30.09.2013 Akademia Medycyny Biological cost of the depression of consciousness Michael A. E. Ramsay Chairman,
Collaborative Regional Benchmarking Group (North of England, North Yorkshire & Humber and West Yorkshire)
") Best Practice Guidance Sedation These recommendations are bound by the current evidence and best practice at the time of writing and so will be subject to change as further developments are made in this
Best Practice Guidance Sedation These recommendations are bound by the current evidence and best practice at the time of writing and so will be subject to change as further developments are made in this
Sedation Hold/Interruption and Weaning Protocol ( Wake-up and Breathe )
") PROTOCOL Sedation Hold/Interruption and Weaning Protocol ( Wake-up and Breathe ) Page 1 of 6 Scope: Population: Outcome: Critical care clinicians and providers. All ICU patients intubated or mechanically
PROTOCOL Sedation Hold/Interruption and Weaning Protocol ( Wake-up and Breathe ) Page 1 of 6 Scope: Population: Outcome: Critical care clinicians and providers. All ICU patients intubated or mechanically
PHYSICIAN'S ORDERS Mark in for desired orders. If is blank, order is inactive. VENTILATOR SEDATION / ANALGESIC / DELIRIUM ORDER
 Nursing Daily awakenings PHYSICIAN'S ORDERS Mark in for desired orders. If is blank, order is inactive. VENTILATOR SEDATION / ANALGESIC / DELIRIUM ORDER Do not perform daily awakenings: Rationale: Daily
Nursing Daily awakenings PHYSICIAN'S ORDERS Mark in for desired orders. If is blank, order is inactive. VENTILATOR SEDATION / ANALGESIC / DELIRIUM ORDER Do not perform daily awakenings: Rationale: Daily
SEDATION / ANALGESIA for Brain Failure Patient INASNACC
 SEDATION / ANALGESIA for Brain Failure Patient INASNACC Neuroendocrinological metabolic responses to surgical or traumatic injury Endocrine : increase in ACTH, cortisol, ADH, GH, glucagon, renin, aldosteron,
SEDATION / ANALGESIA for Brain Failure Patient INASNACC Neuroendocrinological metabolic responses to surgical or traumatic injury Endocrine : increase in ACTH, cortisol, ADH, GH, glucagon, renin, aldosteron,
Sedation and Delirium Questions
 Sedation and Delirium Questions TLC Curriculum William J. Ehlenbach, MD MSc Assistant Professor of Medicine Pulmonary & Critical Care Medicine Question 1 Deep sedation in ventilated critically patients
Sedation and Delirium Questions TLC Curriculum William J. Ehlenbach, MD MSc Assistant Professor of Medicine Pulmonary & Critical Care Medicine Question 1 Deep sedation in ventilated critically patients
ICU LIBERATION: IMPLEMENTING THE ABCDEF BUNDLE AND IMPROVING THE LIVES OF ICU PATIENTS
 ICU LIBERATION: IMPLEMENTING THE ABCDEF BUNDLE AND IMPROVING THE LIVES OF ICU PATIENTS J. MATTHEW ALDRICH, MD ASSOCIATE CLINICAL PROFESSOR OF ANESTHESIA AND PERIOPERATIVE CARE UNIVERSITY OF CALIFORNIA
ICU LIBERATION: IMPLEMENTING THE ABCDEF BUNDLE AND IMPROVING THE LIVES OF ICU PATIENTS J. MATTHEW ALDRICH, MD ASSOCIATE CLINICAL PROFESSOR OF ANESTHESIA AND PERIOPERATIVE CARE UNIVERSITY OF CALIFORNIA
Sedation of the Critically Ill Patient
 Buffalo theory of sedation It s a well known fact that a herd of buffalo can only move as fast as the slowest buffalo. And when the herd is hunted, it s the slowest and weakest ones at the back that are
Buffalo theory of sedation It s a well known fact that a herd of buffalo can only move as fast as the slowest buffalo. And when the herd is hunted, it s the slowest and weakest ones at the back that are
Sedation and Analgesia in the Critically Ill
 12th Congress of the World Federation of Societies of Intensive and Critical Care Medicine August 29 (Sat.) September 1 (Tue.), 2015 COEX, Seoul, Korea ONE STEP FURTHER: THE PURSUIT OF EXCELLENCE IN CRITICAL
12th Congress of the World Federation of Societies of Intensive and Critical Care Medicine August 29 (Sat.) September 1 (Tue.), 2015 COEX, Seoul, Korea ONE STEP FURTHER: THE PURSUIT OF EXCELLENCE IN CRITICAL
Doug Paul, D.O. FACOS Medical Director, Trauma Services Kettering Health Network
 Doug Paul, D.O. FACOS Medical Director, Trauma Services Kettering Health Network A paradigm shift (or revolutionary science) is, a change in the basic assumptions, or paradigms, within the ruling theory
Doug Paul, D.O. FACOS Medical Director, Trauma Services Kettering Health Network A paradigm shift (or revolutionary science) is, a change in the basic assumptions, or paradigms, within the ruling theory
Overview of Presentation. Delirium Definition. Assessing & Managing ICU Delirium: What is the Evidence?
 Assessing & Managing ICU Delirium: What is the Evidence? Dale Needham, MD, PhD Professor Pulmonary & Critical Care Medicine, and Physical Medicine & Rehabilitation Medical Director, Critical Care Physical
Assessing & Managing ICU Delirium: What is the Evidence? Dale Needham, MD, PhD Professor Pulmonary & Critical Care Medicine, and Physical Medicine & Rehabilitation Medical Director, Critical Care Physical
Capnography. Capnography. Oxygenation. Pulmonary Physiology 4/15/2018. non invasive monitor for ventilation. Edward C. Adlesic, DMD.
 Capnography Edward C. Adlesic, DMD University of Pittsburgh School of Dental Medicine 2018 North Carolina Program Capnography non invasive monitor for ventilation measures end tidal CO2 early detection
Capnography Edward C. Adlesic, DMD University of Pittsburgh School of Dental Medicine 2018 North Carolina Program Capnography non invasive monitor for ventilation measures end tidal CO2 early detection
9/28/2016. Sedation Strategies in the ICU. Outline. ICU sedation. Recent clinical practice guidelines Top 10 myths A practical approach
 Sedation Strategies in the ICU UW Medicine EMS and Trauma Conference Seattle, Washington September 26 th, 2016 C. Terri Hough, MD MSc Associate Professor of Medicine Division of Pulmonary and Critical
Sedation Strategies in the ICU UW Medicine EMS and Trauma Conference Seattle, Washington September 26 th, 2016 C. Terri Hough, MD MSc Associate Professor of Medicine Division of Pulmonary and Critical
Supplementary appendix
 Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Page VJ, Casarin A, Ely EW, et al. Evaluation
Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Page VJ, Casarin A, Ely EW, et al. Evaluation
Disclosure. Hospira Pharmaceuticals. Unrestricted research funding Honoraria for CME education administered via France Foundation
 Disclosure Hospira Pharmaceuticals Unrestricted research funding Honoraria for CME education administered via France Foundation Economics in Sedation: Responsible Use of the ICU Budget John W. Devlin,
Disclosure Hospira Pharmaceuticals Unrestricted research funding Honoraria for CME education administered via France Foundation Economics in Sedation: Responsible Use of the ICU Budget John W. Devlin,
Critical Care Strategic Clinical Network Provincial ICU Delirium Framework
 Pain assessed and documentation using validated tool (CPOT and NRS) Assess and document q4h and prn 100% of patients assessed for pain and documented q4h A: Assess, Prevent & Manage Pain Self Reporting
Pain assessed and documentation using validated tool (CPOT and NRS) Assess and document q4h and prn 100% of patients assessed for pain and documented q4h A: Assess, Prevent & Manage Pain Self Reporting
KEY REFERENCES Laying the foundation for D of ABCDEF bundle
 KEY REFERENCES Laying the foundation for D of ABCDEF bundle Ely E. JAMA. 2001;286:2703-2710 (CAM-ICU) Bergeron N. Intensive Care Med. 2001;27:859-864 (ICDSC) Dubois M. Intensive Care Med. 2001;27:1297-1304
KEY REFERENCES Laying the foundation for D of ABCDEF bundle Ely E. JAMA. 2001;286:2703-2710 (CAM-ICU) Bergeron N. Intensive Care Med. 2001;27:859-864 (ICDSC) Dubois M. Intensive Care Med. 2001;27:1297-1304
Clinical Practice Guidelines for the Management of Pain, Agitation, and Delirium in Adult Patients
 Clinical Practice Guidelines for the Management of Pain, Agitation, and Delirium in Adult Patients in the Intensive Care Unit January 2013 Volume 41 Number 1 Society of Critical Care Medicine 本檔僅供內部教學使用檔案內所使用之照片之版權仍屬於原期刊公開使用時,
Clinical Practice Guidelines for the Management of Pain, Agitation, and Delirium in Adult Patients in the Intensive Care Unit January 2013 Volume 41 Number 1 Society of Critical Care Medicine 本檔僅供內部教學使用檔案內所使用之照片之版權仍屬於原期刊公開使用時,
Spontaneous Breathing Trial and Mechanical Ventilation Weaning Process
 Page 1 of 5 ASSESSMENT INTERVENTION Patient receiving mechanical ventilation Baseline ventilatory mode/ settings RT and RN to assess criteria 1 for SBT Does patient meet criteria? RT to initiate SBT Does
Page 1 of 5 ASSESSMENT INTERVENTION Patient receiving mechanical ventilation Baseline ventilatory mode/ settings RT and RN to assess criteria 1 for SBT Does patient meet criteria? RT to initiate SBT Does
Can Goal Directed Sedation Improve Outcomes?
 Can Goal Directed Sedation Improve Outcomes? Yahya SHEHABI, FANZCA, FCICM, EMBA Professor and Program Director Critical care Monash Health and Monash University - Melbourne School of Medicine, University
Can Goal Directed Sedation Improve Outcomes? Yahya SHEHABI, FANZCA, FCICM, EMBA Professor and Program Director Critical care Monash Health and Monash University - Melbourne School of Medicine, University
Capnography 101. James A Temple BA, NRP, CCP
 Capnography 101 James A Temple BA, NRP, CCP Expected Outcomes 1. Gain a working knowledge of the physiology and science behind End-Tidal CO2. 2.Relate End-Tidal CO2 to ventilation, perfusion, and metabolism.
Capnography 101 James A Temple BA, NRP, CCP Expected Outcomes 1. Gain a working knowledge of the physiology and science behind End-Tidal CO2. 2.Relate End-Tidal CO2 to ventilation, perfusion, and metabolism.
Sarah V. Cogle, PharmD, BCCCP Assistant Clinical Professor Auburn University Harrison School of Pharmacy Auburn, AL ALSHP Annual Clinical Meeting
 Sarah V. Cogle, PharmD, BCCCP Assistant Clinical Professor Auburn University Harrison School of Pharmacy Auburn, AL ALSHP Annual Clinical Meeting 2018 I have no actual or potential conflict of interest
Sarah V. Cogle, PharmD, BCCCP Assistant Clinical Professor Auburn University Harrison School of Pharmacy Auburn, AL ALSHP Annual Clinical Meeting 2018 I have no actual or potential conflict of interest
Capnography: The Most Vital Sign
 Capnography: The Most Vital Sign Mike McEvoy, PhD, NRP, RN, CCRN Cardiac Surgical ICU RN & Chair Resuscitation Committee Albany Medical Center EMS Coordinator Saratoga County, NY www.mikemcevoy.com CO
Capnography: The Most Vital Sign Mike McEvoy, PhD, NRP, RN, CCRN Cardiac Surgical ICU RN & Chair Resuscitation Committee Albany Medical Center EMS Coordinator Saratoga County, NY www.mikemcevoy.com CO
ICU Delirium and sedation: understanding their role in long-term patient outcomes. Yoanna Skrobik MD FRCP(c)
") ICU Delirium and sedation: understanding their role in long-term patient outcomes Yoanna Skrobik MD FRCP(c) Conflicts of interest Member, SCCM Pain, Agitation and Delirium guidelines writing committee
ICU Delirium and sedation: understanding their role in long-term patient outcomes Yoanna Skrobik MD FRCP(c) Conflicts of interest Member, SCCM Pain, Agitation and Delirium guidelines writing committee
Kendiss Olafson MD FRCPC MPH Section of Critical Care University of Manitoba
 Kendiss Olafson MD FRCPC MPH Section of Critical Care University of Manitoba Outline Sedation in ICU Purpose/Goals Common Drugs Sedation delivery strategies Mobility in the ICU Weakness with critical illness
Kendiss Olafson MD FRCPC MPH Section of Critical Care University of Manitoba Outline Sedation in ICU Purpose/Goals Common Drugs Sedation delivery strategies Mobility in the ICU Weakness with critical illness
Appendix D An unresponsive patient with shallow, gasping breaths at a rate of six per minute requires:
 Answer Key Appendix D-2 1. An unresponsive patient with shallow, gasping breaths at a rate of six per minute requires: a. oxygen given via nasal cannula b. immediate transport to a medical facility c.
Answer Key Appendix D-2 1. An unresponsive patient with shallow, gasping breaths at a rate of six per minute requires: a. oxygen given via nasal cannula b. immediate transport to a medical facility c.
End Tidal CO2 Not All Its Cracked Up To Be The Limitations of PETCO2 In Sedation Analgesia
 End Tidal CO2 Not All Its Cracked Up To Be The Limitations of PETCO2 In Sedation Analgesia Tidal Volume Noninvasive monitoring of ventilation and exhaled carbon dioxide of a patient End Tidal CO2 Produces
End Tidal CO2 Not All Its Cracked Up To Be The Limitations of PETCO2 In Sedation Analgesia Tidal Volume Noninvasive monitoring of ventilation and exhaled carbon dioxide of a patient End Tidal CO2 Produces
PHYSICIAN COMPETENCY FOR ADULT DEEP SEDATION (Ages 14 and older)
") Name Score PHYSICIAN COMPETENCY FOR ADULT DEEP SEDATION (Ages 14 and older) 1. Pre-procedure evaluation for moderate sedation should involve all of the following EXCEPT: a) Airway Exam b) Anesthetic history
Name Score PHYSICIAN COMPETENCY FOR ADULT DEEP SEDATION (Ages 14 and older) 1. Pre-procedure evaluation for moderate sedation should involve all of the following EXCEPT: a) Airway Exam b) Anesthetic history
ABCs of ICU Delirium Marian Maxwell, Pharm.D., BCCCP January 6, 2018
 ABCs of ICU Delirium Marian Maxwell, Pharm.D., BCCCP January 6, 2018 Disclosures I do not have any financial/non-financial relationships to disclose. Learning Objectives Define delirium and discuss the
ABCs of ICU Delirium Marian Maxwell, Pharm.D., BCCCP January 6, 2018 Disclosures I do not have any financial/non-financial relationships to disclose. Learning Objectives Define delirium and discuss the
Capnography Connections Guide
 Capnography Connections Guide Patient Monitoring Contents I Section 1: Capnography Introduction...1 I Section 2: Capnography & PCA...3 I Section 3: Capnography & Critical Care...7 I Section 4: Capnography
Capnography Connections Guide Patient Monitoring Contents I Section 1: Capnography Introduction...1 I Section 2: Capnography & PCA...3 I Section 3: Capnography & Critical Care...7 I Section 4: Capnography
Summary of Delirium Clinical Practice Guideline Recommendations Post Operative
 Summary of Delirium Clinical Practice Guideline Recommendations Post Operative Intensive Care Unit Clinical Practice Guideline for Postoperative Clinical Practice Guidelines for the Delirium in Older Adults;
Summary of Delirium Clinical Practice Guideline Recommendations Post Operative Intensive Care Unit Clinical Practice Guideline for Postoperative Clinical Practice Guidelines for the Delirium in Older Adults;
Pain & Sedation Management in PICU. Marut Chantra, M.D.
 Pain & Sedation Management in PICU Marut Chantra, M.D. Pain Diseases Trauma Procedures Rogers Textbook of Pediatric Intensive Care, 5 th ed, 2015 Emotional Distress Separation from parents Unfamiliar
Pain & Sedation Management in PICU Marut Chantra, M.D. Pain Diseases Trauma Procedures Rogers Textbook of Pediatric Intensive Care, 5 th ed, 2015 Emotional Distress Separation from parents Unfamiliar
Conflict of Interest. Patient Case. Objectives. The Balancing Act. Why We Need Sedation
 Agitation in the ICU Have we swung the pendulum too far from benzodiazepines? Conflict of Interest The author of this presentation has no conflicts of interest to disclose Nina Vadiei, PharmD PGY1 Pharmacy
Agitation in the ICU Have we swung the pendulum too far from benzodiazepines? Conflict of Interest The author of this presentation has no conflicts of interest to disclose Nina Vadiei, PharmD PGY1 Pharmacy
ICU Delirium in Infants & Children: Cause for Concern or False Alarm. Objectives
 ICU Delirium in Infants & Children: Cause for Concern or False Alarm Peter (Pete) N. Johnson, Pharm.D., BCPS, BCPPS, FPPAG Associate Professor of Pharmacy Practice University of Oklahoma College of Pharmacy
ICU Delirium in Infants & Children: Cause for Concern or False Alarm Peter (Pete) N. Johnson, Pharm.D., BCPS, BCPPS, FPPAG Associate Professor of Pharmacy Practice University of Oklahoma College of Pharmacy
Critical Care Pharmacological Management of Delirium
 Critical Care Pharmacological Management of Delirium Policy Title: in the Critical Care Unit Executive Summary: This policy provides guidance Pharmacological Management of delirium in the Critical Care
Critical Care Pharmacological Management of Delirium Policy Title: in the Critical Care Unit Executive Summary: This policy provides guidance Pharmacological Management of delirium in the Critical Care
Identification of patients at risk for Opioid-Induced Respiratory Depression
 Identification of patients at risk for Opioid-Induced Respiratory Depression 2015 Objectives: Discuss the significance of Opioid Induced Respiratory depression (OIRD) Review the patient characteristics/risk
Identification of patients at risk for Opioid-Induced Respiratory Depression 2015 Objectives: Discuss the significance of Opioid Induced Respiratory depression (OIRD) Review the patient characteristics/risk
Adult Procedural Sedation A Training Program for Providers
 Adult Procedural Sedation A Training Program for Providers Adult Procedural Sedation by the Non-Anesthesiologist Guidelines for adult procedural sedation promote safe and effective medical practice: Many
Adult Procedural Sedation A Training Program for Providers Adult Procedural Sedation by the Non-Anesthesiologist Guidelines for adult procedural sedation promote safe and effective medical practice: Many
BIS Brain Monitoring for Critical Care
 BIS Brain Monitoring for Critical Care The Bispectral Index (BIS ) is a processed EEG parameter that provides a direct measure of the effects of sedatives on the brain. The BIS monitoring value is represented
BIS Brain Monitoring for Critical Care The Bispectral Index (BIS ) is a processed EEG parameter that provides a direct measure of the effects of sedatives on the brain. The BIS monitoring value is represented
Responding to The Joint Commission Alert on Safe Use of Opioids in Hospitals
 Responding to The Joint Commission Alert on Safe Use of Opioids in Hospitals Suzanne A Nesbit, PharmD, CPE Clinical Pharmacy Specialist, Pain Management The Johns Hopkins Hospital Objectives and Disclosures
Responding to The Joint Commission Alert on Safe Use of Opioids in Hospitals Suzanne A Nesbit, PharmD, CPE Clinical Pharmacy Specialist, Pain Management The Johns Hopkins Hospital Objectives and Disclosures
Foundation in Critical Care Nursing. Airway / Respiratory / Workbook
 Foundation in Critical Care Nursing Airway / Respiratory / Workbook Airway Anatomy: Please label the following: Tongue Larynx Epiglottis Pharynx Trachea Vertebrae Oesophagus Where is the ET (endotracheal)
Foundation in Critical Care Nursing Airway / Respiratory / Workbook Airway Anatomy: Please label the following: Tongue Larynx Epiglottis Pharynx Trachea Vertebrae Oesophagus Where is the ET (endotracheal)
Interesting Capnography Cases
 Interesting Capnography Cases Mike McEvoy, PhD, NRP, RN, CCRN Cardiac Surgical ICU RN & Chair Resuscitation Committee Albany Medical Center EMS Coordinator Saratoga County, NY www.mikemcevoy.com Outline
Interesting Capnography Cases Mike McEvoy, PhD, NRP, RN, CCRN Cardiac Surgical ICU RN & Chair Resuscitation Committee Albany Medical Center EMS Coordinator Saratoga County, NY www.mikemcevoy.com Outline
Transcutaneous CO2 Monitoring: Alerting the Anesthesia Provider to Impending Respiratory Depression
 Transcutaneous CO2 Monitoring: Alerting the Anesthesia Provider to Impending Respiratory Depression JEANETTE R BAUCHAT, MD, MS ASSOCIATE PROFESSOR OF ANESTHESIOLOGY DIVISION CHIEF, OBSTETRIC ANESTHESIOLOGY
Transcutaneous CO2 Monitoring: Alerting the Anesthesia Provider to Impending Respiratory Depression JEANETTE R BAUCHAT, MD, MS ASSOCIATE PROFESSOR OF ANESTHESIOLOGY DIVISION CHIEF, OBSTETRIC ANESTHESIOLOGY
3/30/12. Luke J. Gasowski BS, BSRT, NREMT-P, FP-C, CCP-C, RRT-NPS
 Luke J. Gasowski BS, BSRT, NREMT-P, FP-C, CCP-C, RRT-NPS 1) Define and describe ETCO 2 2) Explain methods of measuring ETCO 2 3) Describe various clinical applications of ETCO 2 4) Describe the relationship
Luke J. Gasowski BS, BSRT, NREMT-P, FP-C, CCP-C, RRT-NPS 1) Define and describe ETCO 2 2) Explain methods of measuring ETCO 2 3) Describe various clinical applications of ETCO 2 4) Describe the relationship
Sleep in the ICU: helped by drugs? Yoanna Skrobik MD FRCP(c) MSc.
 MSc.") Sleep in the ICU: helped by drugs? Yoanna Skrobik MD FRCP(c) MSc. Conflicts of interest Member, SCCM Pain, Agitation and Delirium guidelines writing committee Vice-chair, SCCM Pain, Agitation, Delirium,
Sleep in the ICU: helped by drugs? Yoanna Skrobik MD FRCP(c) MSc. Conflicts of interest Member, SCCM Pain, Agitation and Delirium guidelines writing committee Vice-chair, SCCM Pain, Agitation, Delirium,
HOSPITAL PROCEDURE Collaborative Practice Committee
 Title: Capnography (ETC0 2 ) Monitoring Code: CPC-2012AUG-1.C.35 HOSPITAL PROCEDURE Collaborative Practice Committee Title of Responsible Party: Director of Medical-Surgical Services Origination Date:
Title: Capnography (ETC0 2 ) Monitoring Code: CPC-2012AUG-1.C.35 HOSPITAL PROCEDURE Collaborative Practice Committee Title of Responsible Party: Director of Medical-Surgical Services Origination Date:
Julie Zimmerman, MSN, RN, CCRN Clinical Nurse Specialist
 Julie Zimmerman, MSN, RN, CCRN Clinical Nurse Specialist Objectives Define capnography vs. end tidal CO2 (EtCO 2 ) Identify what normal vs. abnormal EtCO2 values mean and what to do Understand when to
Julie Zimmerman, MSN, RN, CCRN Clinical Nurse Specialist Objectives Define capnography vs. end tidal CO2 (EtCO 2 ) Identify what normal vs. abnormal EtCO2 values mean and what to do Understand when to
+ Change in baseline mental status, inattention, and either disorganized thinking or altered level of consciousness. Delirium. Disclosure.
 47 th Annual Meeting August 2-4, 2013 Orlando, FL Identification, Prevention and Treatment of Delirium: The Role of the Health System Pharmacist Jennifer Cortes, PharmD, BCPS Medical ICU Clinical Pharmacy
47 th Annual Meeting August 2-4, 2013 Orlando, FL Identification, Prevention and Treatment of Delirium: The Role of the Health System Pharmacist Jennifer Cortes, PharmD, BCPS Medical ICU Clinical Pharmacy
Conducting Delirium Research
 Optimizing Clinical Trials When Conducting Research Research funding: Disclosure NHLBI, NIA, AstraZeneca John W. Devlin, PharmD, FCCP, FCCM, Professor of Pharmacy, Northeastern University Scientific Staff,
Optimizing Clinical Trials When Conducting Research Research funding: Disclosure NHLBI, NIA, AstraZeneca John W. Devlin, PharmD, FCCP, FCCM, Professor of Pharmacy, Northeastern University Scientific Staff,
Anesthesia Monitoring. D. J. McMahon rev cewood
 Anesthesia Monitoring D. J. McMahon 150114 rev cewood 2018-01-19 Key Points Anesthesia Monitoring: - Understand the difference between guidelines & standards - ASA monitoring Standard I states that an
Anesthesia Monitoring D. J. McMahon 150114 rev cewood 2018-01-19 Key Points Anesthesia Monitoring: - Understand the difference between guidelines & standards - ASA monitoring Standard I states that an
Delirium in Critical Care. Recognition, Management, Research tasters. Dr Valerie Page Watford General Hospital
 Delirium in Critical Care. Recognition, Management, Research tasters Dr Valerie Page Watford General Hospital What does it look like? Diagnosing delirium CAM-ICU CAM-ICU Feature 1: Acute onset of mental
Delirium in Critical Care. Recognition, Management, Research tasters Dr Valerie Page Watford General Hospital What does it look like? Diagnosing delirium CAM-ICU CAM-ICU Feature 1: Acute onset of mental
CRITICALLY APPRAISED PAPER (CAP)
") CRITICALLY APPRAISED PAPER (CAP) Schweickert, W. D., Pohlman, M. C., Pohlman, A. S., Nigos, C., Pawlik, A. J., Esbrook, C. L., Kress, J.P. (2009). Early physical and occupational therapy in mechanically
CRITICALLY APPRAISED PAPER (CAP) Schweickert, W. D., Pohlman, M. C., Pohlman, A. S., Nigos, C., Pawlik, A. J., Esbrook, C. L., Kress, J.P. (2009). Early physical and occupational therapy in mechanically
Respiratory Depression and Considerations for Monitoring Following Ophthalmologic Surgery
 Respiratory Depression and Considerations for Monitoring Following Ophthalmologic Surgery Athir Morad, M.D. Division of Neurocritical care Departments of Anesthesiology/ Critical Care Medicine and Neurology
Respiratory Depression and Considerations for Monitoring Following Ophthalmologic Surgery Athir Morad, M.D. Division of Neurocritical care Departments of Anesthesiology/ Critical Care Medicine and Neurology
How it Works. CO 2 is the smoke from the flames of metabolism 10/21/18. -Ray Fowler, MD. Metabolism creates ETC0 2 for excretion
 CO 2 is the smoke from the flames of metabolism -Ray Fowler, MD How it Works Metabolism creates ETC0 2 for excretion ETC02 and Oxygen are exchanged at the alveolar level in the lungs with each breath.
CO 2 is the smoke from the flames of metabolism -Ray Fowler, MD How it Works Metabolism creates ETC0 2 for excretion ETC02 and Oxygen are exchanged at the alveolar level in the lungs with each breath.
Sedation Guidelines for Air Ambulance Transfer of Psychiatric Patients
 Sedation Guidelines for Air Ambulance Transfer of Psychiatric Patients 1 Determine transfer risks as per BC Ambulance Risk Stratification Tool 2 Determine required sedation level accordingly: RASS Level
Sedation Guidelines for Air Ambulance Transfer of Psychiatric Patients 1 Determine transfer risks as per BC Ambulance Risk Stratification Tool 2 Determine required sedation level accordingly: RASS Level
Optimal sedation and management of anxiety in patients undergoing endobronchial ultrasound (EBUS)
") Optimal sedation and management of anxiety in patients undergoing endobronchial ultrasound (EBUS) Georgios Dadoudis Anesthesiologist ICU DIRECTOR INTERBALKAN MEDICAL CENTER Optimal performance requires:
Optimal sedation and management of anxiety in patients undergoing endobronchial ultrasound (EBUS) Georgios Dadoudis Anesthesiologist ICU DIRECTOR INTERBALKAN MEDICAL CENTER Optimal performance requires:
Capnography: The Most Vital of Vital Signs. Tom Ahrens, PhD, RN, FAAN Research Scientist, Barnes-Jewish Hospital, St. Louis, MO May, 2017
 Capnography: The Most Vital of Vital Signs Tom Ahrens, PhD, RN, FAAN Research Scientist, Barnes-Jewish Hospital, St. Louis, MO May, 2017 Assessing Ventilation and Blood Flow with Capnography Capnography
Capnography: The Most Vital of Vital Signs Tom Ahrens, PhD, RN, FAAN Research Scientist, Barnes-Jewish Hospital, St. Louis, MO May, 2017 Assessing Ventilation and Blood Flow with Capnography Capnography
Ventilator-Associated Pneumonia Prevention Bundle 2010 Revised Edition (JSICM-VAP Bundle)
") 1 Ventilator-Associated Pneumonia Prevention Bundle 2010 Revised Edition (JSICM-VAP Bundle) Committee on ICU Evaluation Japanese Society of Intensive Care Medicine 2 I. Ensuring hand hygiene Hand washing
1 Ventilator-Associated Pneumonia Prevention Bundle 2010 Revised Edition (JSICM-VAP Bundle) Committee on ICU Evaluation Japanese Society of Intensive Care Medicine 2 I. Ensuring hand hygiene Hand washing
PHYSICIAN PROCEDURAL SEDATION AND ANALGESIA QUIZ
 PHYSICIAN PROCEDURAL SEDATION AND ANALGESIA QUIZ 1. Which of the following statements are TRUE? (Select ALL that apply) o Sedative/analgesic drugs should be given in small, incremental doses that are titrated
PHYSICIAN PROCEDURAL SEDATION AND ANALGESIA QUIZ 1. Which of the following statements are TRUE? (Select ALL that apply) o Sedative/analgesic drugs should be given in small, incremental doses that are titrated
ANALGESIA AND SEDATION IN MECHANICAL VENTILATION
 ANALGESIA AND SEDATION IN MECHANICAL VENTILATION Erik Stoltenberg, MD Abbott Northwestern Hospital February 27, 2018 DISCLOSURE Nothing to disclose AllinaHealthSystem 1 OBJECTIVE To apply knowledge of
ANALGESIA AND SEDATION IN MECHANICAL VENTILATION Erik Stoltenberg, MD Abbott Northwestern Hospital February 27, 2018 DISCLOSURE Nothing to disclose AllinaHealthSystem 1 OBJECTIVE To apply knowledge of
Administrative Policies and Procedures. Originating Venue: Provision of Care, Treatment and Services Policy No.: PC 2916
 Administrative Policies and Procedures Originating Venue: Provision of Care, Treatment and Services Policy No.: PC 2916 Title: Sedation Cross Reference: Date Issued: 05/09 Date Reviewed: 04/11 Date: Revised:
Administrative Policies and Procedures Originating Venue: Provision of Care, Treatment and Services Policy No.: PC 2916 Title: Sedation Cross Reference: Date Issued: 05/09 Date Reviewed: 04/11 Date: Revised:
New approaches of sedation in critically ill patients.
 New approaches of sedation in critically ill patients. Jean Mantz, MD, PhD Professor and Chair, Department of Anesthesia and Critical Care F- Paris Val de Seine University Hospitals Univ Paris Diderot,
New approaches of sedation in critically ill patients. Jean Mantz, MD, PhD Professor and Chair, Department of Anesthesia and Critical Care F- Paris Val de Seine University Hospitals Univ Paris Diderot,
Jennifer Mando-Vandrick, PharmD, BCPS Clinical Pharmacist, Emergency Department Director, PGY2 Critical Care Pharmacy Residency Duke University
 Jennifer Mando-Vandrick, PharmD, BCPS Clinical Pharmacist, Emergency Department Director, PGY2 Critical Care Pharmacy Residency Duke University Hospital Objectives Review pertinent pharmacotherapy common
Jennifer Mando-Vandrick, PharmD, BCPS Clinical Pharmacist, Emergency Department Director, PGY2 Critical Care Pharmacy Residency Duke University Hospital Objectives Review pertinent pharmacotherapy common
Pharmacological methods of behaviour management
 Pharmacological methods of behaviour management Pharmacological methods CONCIOUS SEDATION?? Sedation is the use of a mild sedative (calming drug) to manage special needs or anxiety while a child receives
Pharmacological methods of behaviour management Pharmacological methods CONCIOUS SEDATION?? Sedation is the use of a mild sedative (calming drug) to manage special needs or anxiety while a child receives
Critical Care Pharmacological Management of Delirium
 Critical Care Pharmacological Management of Delirium Policy Title: in the Critical Care Unit Executive Summary: This policy provides guidance Pharmacological Management of delirium in the Critical Care
Critical Care Pharmacological Management of Delirium Policy Title: in the Critical Care Unit Executive Summary: This policy provides guidance Pharmacological Management of delirium in the Critical Care
Optimize vent weaning and SBT outcomes. Identify underlying causes for SBT failures. Role SBT and weaning protocol have in respiratory care
 Optimize vent weaning and SBT outcomes Identify underlying causes for SBT failures Role SBT and weaning protocol have in respiratory care Lower risk of developing complications Lower risk of VAP, other
Optimize vent weaning and SBT outcomes Identify underlying causes for SBT failures Role SBT and weaning protocol have in respiratory care Lower risk of developing complications Lower risk of VAP, other
SARASOTA MEMORIAL HOSPITAL NURSING DEPARTMENT POLICY
 PS1006 SARASOTA MEMORIAL HOSPITAL NURSING DEPARTMENT TITLE: PROPOFOL SEDATION PROTOCOL Job Title of Reviewer: Director, ICU :#: EFFECTIVE DATE: REVISED DATE: TYPE: 1/95 8/06, 5/09 DEPARTMENTAL INTERDEPARTMENTAL
PS1006 SARASOTA MEMORIAL HOSPITAL NURSING DEPARTMENT TITLE: PROPOFOL SEDATION PROTOCOL Job Title of Reviewer: Director, ICU :#: EFFECTIVE DATE: REVISED DATE: TYPE: 1/95 8/06, 5/09 DEPARTMENTAL INTERDEPARTMENTAL
North Wales Critical Care Network
 North Wales Critical Care Network SEDATION GUIDELINES FOR ADULTS IN CRITICAL CARE Approved 6.9.12 1 Sedation guidelines for intensive care Betsi Cadwaladr University Health Board (Adapted from guidelines
North Wales Critical Care Network SEDATION GUIDELINES FOR ADULTS IN CRITICAL CARE Approved 6.9.12 1 Sedation guidelines for intensive care Betsi Cadwaladr University Health Board (Adapted from guidelines
NON INVASIVE LIFE SAVERS. Non Invasive Ventilation (NIV)
") Table 1. NIV: Mechanisms Of Action Decreases work of breathing Increases functional residual capacity Recruits collapsed alveoli Improves respiratory gas exchange Reverses hypoventilation Maintains upper
Table 1. NIV: Mechanisms Of Action Decreases work of breathing Increases functional residual capacity Recruits collapsed alveoli Improves respiratory gas exchange Reverses hypoventilation Maintains upper
Keywords: Dexmedetomidine, fentanyl, tympanoplasty, monitored anaesthesia care. INTRODUCTION:
 13 Original article A COMPARATIVE OBSERVATIONAL STUDY BETWEEN DEXMEDETOMIDINE V/S COMBINATION OF MIDAZOLAM- FENTANYL FOR TYMPANOPLASTY SURGERY UNDER MONITORED ANESTHESIA CARE Dr. Parul Pachotiya (Professor
13 Original article A COMPARATIVE OBSERVATIONAL STUDY BETWEEN DEXMEDETOMIDINE V/S COMBINATION OF MIDAZOLAM- FENTANYL FOR TYMPANOPLASTY SURGERY UNDER MONITORED ANESTHESIA CARE Dr. Parul Pachotiya (Professor
DIAGRAM OF THE PRESENTATION. Post ICU Rehabilitation. Effective strategies in ICU. During two last decades
 1 1st European Conference on Weaning & Rehabilitation in Critically ill Patients INTERNATIONAL EARLY MOBILISATION NETWORK Post ICU Rehabilitation Serafeim N. Nanas Professor of Critical Care Medicine Evaggelismos
1 1st European Conference on Weaning & Rehabilitation in Critically ill Patients INTERNATIONAL EARLY MOBILISATION NETWORK Post ICU Rehabilitation Serafeim N. Nanas Professor of Critical Care Medicine Evaggelismos
Prepared by : Bayan Kaddourah RN,MHM. GICU Clinical Instructor
 Mechanical Ventilation Prepared by : Bayan Kaddourah RN,MHM. GICU Clinical Instructor 1 Definition Is a supportive therapy to facilitate gas exchange. Most ventilatory support requires an artificial airway.
Mechanical Ventilation Prepared by : Bayan Kaddourah RN,MHM. GICU Clinical Instructor 1 Definition Is a supportive therapy to facilitate gas exchange. Most ventilatory support requires an artificial airway.
Fighting the Fog A Collaborative Approach to Decreasing ICU Delirium
 Fighting the Fog A Collaborative Approach to Decreasing ICU Delirium Kimberly Scherr NP Jennifer Barker RN Misericordia Hospital ICU Edmonton, AB CACCN Dynamics Sept 21, 2014 Delirium Delirium is an acute
Fighting the Fog A Collaborative Approach to Decreasing ICU Delirium Kimberly Scherr NP Jennifer Barker RN Misericordia Hospital ICU Edmonton, AB CACCN Dynamics Sept 21, 2014 Delirium Delirium is an acute
Conflict of Interest Disclosure
 Monitoring for Opioid Induced Respiratory Depression: Paradigm Shift from Threshold Monitoring to Trend Monitoring Carla R. Jungquist, ANP BC, PhD Assistant Professor University at Buffalo J. Paul Curry,
Monitoring for Opioid Induced Respiratory Depression: Paradigm Shift from Threshold Monitoring to Trend Monitoring Carla R. Jungquist, ANP BC, PhD Assistant Professor University at Buffalo J. Paul Curry,
Pediatric Sedation Pocket Reference
 Pediatric Sedation Pocket Reference No part of this publication may be reproduced, stored in a retrieval system, or transmitted, in any form or by any means, electronic, mechanical, photocopy, recording,
Pediatric Sedation Pocket Reference No part of this publication may be reproduced, stored in a retrieval system, or transmitted, in any form or by any means, electronic, mechanical, photocopy, recording,
Executive Sponsorship of Delirium Initiatives Lessons from ICU Liberation
 Executive Sponsorship of Delirium Initiatives Lessons from ICU Liberation J. Matthew Aldrich, MD Co-Chair, SCCM ICU Liberation Committee Associate Professor Medical Director, Critical Care Medicine UCSF
Executive Sponsorship of Delirium Initiatives Lessons from ICU Liberation J. Matthew Aldrich, MD Co-Chair, SCCM ICU Liberation Committee Associate Professor Medical Director, Critical Care Medicine UCSF
Liberation from Mechanical Ventilation in Critically Ill Adults
 Liberation from Mechanical Ventilation in Critically Ill Adults 2017 ACCP/ATS Clinical Practice Guidelines Timothy D. Girard, MD, MSCI Clinical Research, Investigation, and Systems Modeling of Acute Illness
Liberation from Mechanical Ventilation in Critically Ill Adults 2017 ACCP/ATS Clinical Practice Guidelines Timothy D. Girard, MD, MSCI Clinical Research, Investigation, and Systems Modeling of Acute Illness
Monitoring Patients for Respiratory Depression: outside of the ICU. James D. Harrell, RCP San Diego Patient Safety Council November 14, 2014
 Monitoring Patients for Respiratory Depression: outside of the ICU James D. Harrell, RCP San Diego Patient Safety Council November 14, 2014 1 What is the San Diego Patient Safety Council? SDPSC consists
Monitoring Patients for Respiratory Depression: outside of the ICU James D. Harrell, RCP San Diego Patient Safety Council November 14, 2014 1 What is the San Diego Patient Safety Council? SDPSC consists
Dr Alireza Yarahmadi and Dr Arvind Perathur Mercy Medical Center - Winter Retreat Des Moines February 2012
 Dr Alireza Yarahmadi and Dr Arvind Perathur Mercy Medical Center - Winter Retreat Des Moines February 2012 Why screen of OSA prior to surgery? What factors increase the risk? When due to anticipate problems?
Dr Alireza Yarahmadi and Dr Arvind Perathur Mercy Medical Center - Winter Retreat Des Moines February 2012 Why screen of OSA prior to surgery? What factors increase the risk? When due to anticipate problems?
What are Appropriate End-points for Delirium Prevention/Treatment Studies
 What are Appropriate End-points for Delirium Prevention/Treatment Studies Pratik Pandharipande, MD, MSCI Professor of Anesthesiology and Surgery Department of Anesthesiology Vanderbilt University School
What are Appropriate End-points for Delirium Prevention/Treatment Studies Pratik Pandharipande, MD, MSCI Professor of Anesthesiology and Surgery Department of Anesthesiology Vanderbilt University School
I. Subject. Moderate Sedation
 I. Subject II. III. Moderate Sedation Purpose To establish criteria for the monitoring and management of patients receiving moderate throughout the hospital Definitions A. Definitions of three levels of
I. Subject II. III. Moderate Sedation Purpose To establish criteria for the monitoring and management of patients receiving moderate throughout the hospital Definitions A. Definitions of three levels of
REFERENCE GUIDE USING THE BISPECTRAL INDEX (BIS ) MONITORING SYSTEM FOR CRITICAL CARE
 MONITORING SYSTEM FOR CRITICAL CARE") REFERENCE GUIDE USING THE BISPECTRAL INDEX (BIS ) MONITORING SYSTEM FOR CRITICAL CARE WHAT IS THE BIS MONITORING SYSTEM? The BIS brain monitoring system generates a processed EEG parameter that provides
REFERENCE GUIDE USING THE BISPECTRAL INDEX (BIS ) MONITORING SYSTEM FOR CRITICAL CARE WHAT IS THE BIS MONITORING SYSTEM? The BIS brain monitoring system generates a processed EEG parameter that provides
POST-INTUBATION ANALGESIA AND SEDATION. August 2012 J Pelletier
 POST-INTUBATION ANALGESIA AND SEDATION August 2012 J Pelletier Intubated patients experience pain and anxiety Mechanical ventilation, endotracheal tube Blood draws, positioning, suctioning Surgical procedures,
POST-INTUBATION ANALGESIA AND SEDATION August 2012 J Pelletier Intubated patients experience pain and anxiety Mechanical ventilation, endotracheal tube Blood draws, positioning, suctioning Surgical procedures,
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Acetaminophen, for geriatric surgical patients, 569 570 Acute kidney injury, critical care issues in geriatric patients with, 555 556
Index Note: Page numbers of article titles are in boldface type. A Acetaminophen, for geriatric surgical patients, 569 570 Acute kidney injury, critical care issues in geriatric patients with, 555 556
Identification and Treatment of the Patient with Sleep Related Hypoventilation
 Identification and Treatment of the Patient with Sleep Related Hypoventilation Hillary Loomis-King, MD Pulmonary and Critical Care of NW MI Munson Sleep Disorders Center X Conflict of Interest Disclosures
Identification and Treatment of the Patient with Sleep Related Hypoventilation Hillary Loomis-King, MD Pulmonary and Critical Care of NW MI Munson Sleep Disorders Center X Conflict of Interest Disclosures
ICU Liberation ABCDEF Bundle Implementation: Focus on Delirium
 ICU Liberation ABCDEF Bundle Implementation: Focus on Delirium Diane Byrum MSN RN CCRN-K CCNS FCCM Quality Implementation Consultant Innovative Solutions For Healthcare Education, LLC Oak Island, NC ICU
ICU Liberation ABCDEF Bundle Implementation: Focus on Delirium Diane Byrum MSN RN CCRN-K CCNS FCCM Quality Implementation Consultant Innovative Solutions For Healthcare Education, LLC Oak Island, NC ICU
Detecting Adverse Respiratory Effects of Anesthetics and Opioid Analgesics in the Postoperative Period
 2014 Rocky Mountain Space Grant Consortium 1 Detecting Adverse Respiratory Effects of Anesthetics and Opioid Analgesics in the Postoperative Period Sean Ermer, B.S., Lara Brewer, Ph.D, and Joseph Orr,
2014 Rocky Mountain Space Grant Consortium 1 Detecting Adverse Respiratory Effects of Anesthetics and Opioid Analgesics in the Postoperative Period Sean Ermer, B.S., Lara Brewer, Ph.D, and Joseph Orr,
Emergency Department Guideline. Procedural Sedation and Analgesia Policy for the Registered Nurse
 Emergency Department Guideline Purpose: To ensure safe, consistent patient monitoring and documentation standards when procedure related sedation and analgesia is indicated. Definitions: Minimal Sedation
Emergency Department Guideline Purpose: To ensure safe, consistent patient monitoring and documentation standards when procedure related sedation and analgesia is indicated. Definitions: Minimal Sedation
Overview. Introduction. Opioids and Respiratory Monitoring Technology WHITE PAPER
 WHITE PAPER Opioids and Respiratory Monitoring Technology JW Beard, MD, MBA Overview Opioids play a central role in postoperative multimodal analgesic therapy but are considered high-alert medications
WHITE PAPER Opioids and Respiratory Monitoring Technology JW Beard, MD, MBA Overview Opioids play a central role in postoperative multimodal analgesic therapy but are considered high-alert medications
Pediatric Dental Sedation
 Pediatric Dental Sedation L. Stephen Long, MD Pediatric Anesthesiologist Children s Dental Anesthesia Group UCSF Benioff Children s Hospital Oakland Part 1: Pediatric Airways and Lungs 1 Three questions:
Pediatric Dental Sedation L. Stephen Long, MD Pediatric Anesthesiologist Children s Dental Anesthesia Group UCSF Benioff Children s Hospital Oakland Part 1: Pediatric Airways and Lungs 1 Three questions:
Sleep Apnea and ifficulty in Extubation. Jean Louis BOURGAIN May 15, 2016
 Sleep Apnea and ifficulty in Extubation Jean Louis BOURGAIN May 15, 2016 Introduction Repetitive collapse of the upper airway > sleep fragmentation, > hypoxemia, hypercapnia, > marked variations in intrathoracic
Sleep Apnea and ifficulty in Extubation Jean Louis BOURGAIN May 15, 2016 Introduction Repetitive collapse of the upper airway > sleep fragmentation, > hypoxemia, hypercapnia, > marked variations in intrathoracic