Doug Paul, D.O. FACOS Medical Director, Trauma Services Kettering Health Network
|
|
|
- Marion Tate
- 5 years ago
- Views:
Transcription

1 Doug Paul, D.O. FACOS Medical Director, Trauma Services Kettering Health Network
2 A paradigm shift (or revolutionary science) is, a change in the basic assumptions, or paradigms, within the ruling theory of science. A paradigm is what members of a scientific community, and they alone, share" The Structure of Scientific Revolutions (1962) (The Essential Tension, 1977).
3 The Problem 4 million ICU admissions / year in USA 80-90% survive ICU 50% unable to return to previous work > 1 year Cognitive, psychological & physically disabling side effects 78% ICU survivors cognitive impairment Hopkins & Jackson, Neurorehabilitation 2012;31 PTSD at discharge (44%), 5 (25%) and 8 (24%) years later Psychosom Med 2008;70
 Increased healthcare costs (Leslie et al.")
4 Problem Identification Increased length of stay on the ventilator, ICU, hospital Associated with aspiration, VAP, hospital acquired pressure ulcers, DVT (Seeling, Heymann & Spies, 2009) Increased mortality at six months and one year (Lat et al. 2009) Increased healthcare costs (Leslie et al. 2008) Acute brain dysfunction that has lasting effects on cognitive abilities (Balas et al. 2012)
5 The Problem Survivors suffer as a result of processes acquired or accelerated by ICU stay. These symptoms typically arise from two common and often unrecognized conditions that have a significant impact on the quality and quantity of life following critical illness: ICU delirium and ICU-acquired weakness and their chronic sequelae
6 The Problem Health care today harms too frequently and routinely fails to deliver potential benefits Crossing the Quality Chasm: A New Health System for 21 st Century-2001
7 Risk Factors: ICUAD & ICUAW Severity of Illness Sepsis Dementia Time on Vent Sedation /NM blockade Immobility
8 Relationship between ICU-acquired delirium and weakness in a patient with sepsis. Vasilevskis E E et al. Chest 2010;138: by American College of Chest Physicians
9 The Answer = ABCDEF ABCDEF implementation independently reduces: HLOS & Delirium incidence Increase return to independent functioning Needham DM,. Arch Phys Med Rehabil. 2010;914: Schweickert WD,. Lancet. 2009; :
10 ABCDEF ABCDEF is a multicomponent process that is intentionally interdependent and designed to: (1) improve collaboration among clinical team members (2) standardize care processes (3) break the cycle of over sedation and prolonged ventilation, which appear causative to delirium and weakness
 Complex Bundle Difficult to Implement and")
11 ABCDEF BUNDLE Minimal Expense Interdisciplinary (not multidisciplinary) Complex Bundle Difficult to Implement and Therefore: Poorly Executed
12 ABCDEF Assess and Manage Pain Both Spontaneous Awakening and Breathing Trial- Coordinated Careful Selection of Analgesic and Sedative Delirium Assessment, Prevention and Management Early Mobility Family Engagement/Involvement Barr et al Critical Care Medicine 41(1),
13 The Problem = ICU Providers!! 40% use SAT (60% don t) 31-42% use SBT (58% don t) 33% use delirium assessment tool (67% don t) 50% use sedation monitoring scale (50% don t) Patel RPS, Gambrell MB, Speroff TP, et al. Crit Care Med. 2009;373:
14 OUTCOMES 2000 Extubation Survival OUTCOMES 2014 Extubation Survival Functionality Cognitive Mobility
15 ABCDEF Analgesia First Approach Definition of Pain The International Association for the Study of Pain defines pain as an: unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage. Barr et al Critical Care Medicine 41(1),

16 Pain in the Critically Ill Many critically ill patients experience pain during hospitalization in the critical care unit. More than 30% have significant pain at rest. More than 50% have significant pain during routine care such as turning, endotracheal suctioning and wound care. Untreated pain can result in negative consequences including multisystem complications. Chanques et al Anesthesiology 107(5): Puntillo et al Am J Crit Care. 10 (4):

17 Pain Assessment The patient s self report is the gold standard for pain assessment. This self report can be given by speaking, nodding, or pointing. The 0-10 numerical rating scale is the most valid tool when the patient can self report. Barr et al Critical Care Medicine 41(1),

18 Avoid the use of Vital Signs as primary assessment for pain Vital signs should be considered cues to begin further pain assessment; but should never be used as the sole indicator of pain. Barr et al Critical Care Medicine 41(1),
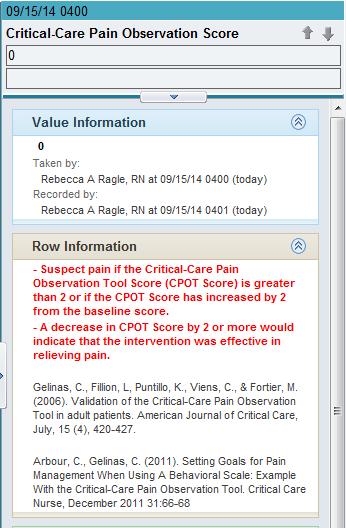
19 CPOT Measures presence or absence of pain Does not measure severity or intensity CPOT of 2 or greater indicates presence of pain Measurement of CPOT after intervention for pain decreases by at least 2 = may be associated with effectiveness of pain management interventions

20 Critical Care Pain Observation Tool (CPOT)

21 Analgesia First! Inter-related Assess using validated tools Lack of treatment of pain can result in many complications including delirium Treat pain first Preemptive
22 Preemptive Analgesia Patients undergoing painful procedures should have preemptive analgesia (analgesia given before the procedure begins) Non-pharmacologic interventions should also be used to help alleviate pain (such as positioning, heat/cold, relaxation or music) Barr et al Critical Care Medicine 41(1),

23 ABCDEF Awakening-SAT
24 Vent Wean / Liberation 70% Simple Weaning OK on 1 st attempt When is the first attempt 20% Difficult Weaning: 7-14 days 10% Prolonged Weaning
25 Daily Interruption of Sedatives 128 patients Intervention group = Sedatives interrupted until awake Control group = Sedatives interrupted at discretion of the clinicians
26 Kaplan Meier Analysis of the Length of Stay in the Intensive Care Unit (ICU), According to Study Group. Kress JP et al. N Engl J Med 2000;342:
27 Continuous infusions of sedative drugs in the intensive care unit may: prolong duration of mechanical ventilation, prolong the ICULOS and the HLOS Impede daily neurologic examinations increase the need for tests to assess alterations in mental status N Engl J Med May 18;342(20):
28 Daily interruption of sedative infusions in critically ill patients undergoing mechanical ventilation Days Mechanical Ventilation 4.9 (I) vs. 7.3 (C) P=0.004 ICULOS (days) 6.4 (I) vs. 9.9 (C) P= o.02 CONCLUSIONS: In patients who are receiving mechanical ventilation, daily interruption of sedative-drug infusions decreases the duration of mechanical ventilation and the length of stay in the intensive care unit. N Engl J Med May 18;342(20):1471-7
29 SAT Not Used Around World Canada 40% get SATs (273 physicians in 2005) U.S. 40% get SATs ( ) Germany 34% get SATs (214 ICUs in 2006) France 40-50% deeply sedated with 90% on continuous infusion (44 ICUs in 2005) UK 28% use sedation breaks, 82% use midazolam when on > 24 hours Brazil 32% get SATs (1,015 MDs in 2008) Mehta S, CCM 2006;34: Devlin J, CCM 2006;34: Payen JF, Anesthes 2007;106: Tanios M, Proc Am Thorac Soc 2005;2:A793.Martin J and Spies C, Crit Care 2007;11:R124Ramaswamy S, Intens Care Med (ESICM 2009)Salluh J, J Crit Care 2009
30 JAMA 2007 MENDS Precedex vs. Ativan Precedex 4 days Less Coma & Delirium Better 28 day Survival (83% vs. 73%)
31 JAMA 2009 SEDCOM Precedex vs. Versed Precedex 23% Less delirium 3 days less mechanical ventilation
32 Sedation Assessment RASS Richmond Agitation-Sedation Scale SAS Riker Sedation Assessment Scale Both SAS and RASS led to similar rates of delirium assessment using the CAM-ICU. Chest. Jul 2012; 142(1):


33 Richmond Agitation Sedation Scale (RASS)
34 PAD Guidelines 2013 Light Sedation vs. Deep Sedation Earlier extubation (2.2 vs. 7.7 days) Improved Hospital survival Improved 180 day survival Lower PTSD scores

35 Spontaneous awakening trial Collaboration between nursing and respiratory therapy when doing SAT and SBT Tough love Pain Controlled? Home meds reconciled?

36 Spontaneous Awakening Trial-BOTH groups getting patient targeted sedation
37 ABCDEF Breathing-SBT


38 Two Decades of Progress
39 The Length of Time from Initiating Weaning to Extubation in the Four Groups. Esteban A et al. N Engl J Med 1995;332:
40 Successful 2 Hr SBT (Ely) (Now 30 minutes) RR < 35 SATS > 90 HR < 140 BP, HR Stability (<20% change) No Anxiety, Diaphoresis
41 Kaplan Meier Analysis of the Duration of Mechanical Ventilation after a Successful Screening Test. Ely EW et al. N Engl J Med1996;335:
42 SBT Weaning Protocol a) Improvement or resolution of the underlying disease process that precipitated need for mechanical ventilation. b) PaO 2 > 60 mm Hg on PEEP/FiO 2 Requirements of < 8 cm H 2 O and FiO 2 < c) Stable oxygenation: PEEP/FiO 2 requirements not increased in the past 24 hrs d) No use of neuromuscular blocking agents; no evidence of persistent blockade. e) ph > 7.30 f) Consistent patient-triggered breaths at baseline A/C settings. If not, minute ventilation by 50% and observe for 2 min
43 THE LANCET Girard TD, et al. Lancet 2008;371:126-34
44 ABC Trial Objectives To determine the efficacy and safety of a protocol combining daily interruption of sedatives and spontaneous breathing trials (SBTs) Measured Outcomes Ventilator-free days ICU and hospital length of stay Survival Duration of coma and delirium Long-term neuropsychological outcomes
45 Awakening and Breathing Controlled Trial (ABC) Paired SAT with SBT 336 MV patients, Randomly assigned Intervention - SAT + SBT (168 pts.) Control Usual Sedation + daily SBT (167 pts.)
46 Awakening and Breathing Controlled Trial SAT + SBT Reduced Hospital Stay by 4 days Reduced Mortality by 14%
47 One-year survival analysis of the Awakening and Breathing Controlled Trial Survival was 14% higher at 1 year among the intervention group(sat coordinated with SBT) vs. the control group (usual care plus SBT) by American College of Chest Physicians Vasilevskis E E et al. Chest 2010;138:

48 Spontaneous Breathing Trial


49 ABCDEF Careful Selection of Analgesics & Sedative
50 A, Data from Pandharipande et al10 indicate that lorazepam dose in the preceding 24 h is an independent predictor for transitioning to delirium in the ICU. Vasilevskis E E et al. Chest 2010;138: by American College of Chest Physicians
51 2013 PAD Sedation Guidelines Benzodiazepines avoided Midazolam & Lorazepam Analgesia first sedation (Analgosedation) More vent free days Shorter ICU & Hospital days More agitated delirium days


52 ABCDEF Delirium Monitoring


53 Temporary alteration in cognition characterized by inattention and disorganized thinking Hyperactive Hypoactive Mixed 75% of ICU patients Morandi, Int Rev Psych 2009; 21

54 Question How often do you or your ICU team document in the medical record the level of delirium or agitation? Always Sometimes Never

.")
55 Delirium Assessment and Management Identifying patients at risk for developing delirium is the first step in prevention. Assessment for delirium should be done once a shift in all critically ill patients using the Confusion Assessment Method-ICU (CAM-ICU). AACN Practice Alert: Delirium Assessment and Management. 2011
56 Delirium Measurement Assess multiple times daily using: CAM-ICU Confusion Assessment Method for ICU ICDSC Intensive Care Delirium Screening Checklist

57 CAM-ICU 2010 by American College of Chest Physicians Vasilevskis E E et al. Chest 2010;138:

58 ABCDEF Early Mobility



59 Mobility is Medicine! The following are health benefits of physical activity: Improves blood sugar homeostasis Enhances cardiovascular function Decreases chronic inflammation Regulates hormone levels Preserves musculoskeletal and neuromuscular integrity Decreases depression and improves cognition

60 ICUAW Disabling weakness 50% of ICU survivors of sepsis, MOF or prolonged mechanical ventilation due to: Inflammatory & metabolic changes Prolonged best rest
61 ICUAW Axonal Polyneuropathy/ Myopathy present in 65% of Patients in ICU for 7 days

62 Comparison of Representative Case and Control Diaphragm-Biopsy Specimens with Respect to Fiber Size. Levine S et al. N Engl J Med 2008;358:

63 Early PT & OT Ventilated Pts. Lancet 2009 PT/OT Control Independent at discharge 59% 35% Delirium Days Vent Free Days (out of 28)

64 Early Mobilization Protocol in Mechanically Ventilated Patients 24% improvement (1.7-fold better) return to independent functional status at discharge

65 ABCDEF is an ICU-acquired delirium and weakness mitigation strategy. Vasilevskis E E et al. Chest 2010;138: by American College of Chest Physicians

66 ABCDEF Family Engagement and Empowerment

67 Family Involvement in Bedside Rounds
68 Implementation ABCDE 2011 Grant Medical Center Trauma Service Columbus Ohio Goals: Time on Vent by 0.5 to 1.0 days Decrease HLOS & ICULOS Improved Survival
69 SAT/SBT Lessons Learned Failures Not done at a consistent time Staff did not understand SAT Varied physician practice Incorrect restart of medications Poor documentation by RN Poor communication at shift change
70 SAT/SBT Lessons Learned Communication with Respiratory therapy Physician understanding of SAT/SBT Sedation minimization not done appropriately prior to SAT/SBT
71 SAT/SBT Process Improvement Timing of SAT/SBT Communication RT, Physician, Nurses Sedation Minimization Educations for all involved Ownership and daily oversight by ICU leadership
72 Daily Evaluation / Huddle SAT done? If not WHY not? SAT passed? If not WHY not? SBT done? If not WHY not? Pt. + SAT/SBT not extubated? WHY not?
73 Electronic Medical Record Include prompts or links to support critical thinking
74 Build medication orders with appropriate ranges and sedation targets
75 Electronic Medical Record Build reports that capture assessment and interventions so readily viewed by all team members Build assessments that limits errors CAM- ICU build

76 Sustaining practice. Creating organization memory Knowledge reservoirs Create passion Virani, Lemieux-Charles, Davis, & Berta. (2009).

77
78 Conclusions: ABCDEF Protocol Reduces ICU and HLOS Reduces Ventilator days Improves In hospital and 128 day survival Improves cognitive and performance function status at 1 year
79 The Problem = ICU Providers!! 40% use SAT (60% don t) 31-42% use SBT (58% don t) 33% use delirium assessment tool (67% don t) 50% use sedation monitoring scale (50% don t) Patel RPS, Gambrell MB, Speroff TP, et al. Delirium and sedation in the intensive care unit: survey of behaviors and attitudes of 1384 healthcare professionals. Crit Care Med. 2009;373:

80 Don t be a Problem - Be a Solver Institute ABCDEF protocol Create a paradigm shift at your institution



81 Thank You!!!!!
82 Questions???
ICU Liberation for the Pharmacist. A. Kendall Gross, PharmD, BCPS, BCCCP Critical Care Pharmacist UCSF Medical Center
 ICU Liberation for the Pharmacist A. Kendall Gross, PharmD, BCPS, BCCCP Critical Care Pharmacist UCSF Medical Center Disclosure No conflicts of interest to disclose Objectives o Outline the elements of
ICU Liberation for the Pharmacist A. Kendall Gross, PharmD, BCPS, BCCCP Critical Care Pharmacist UCSF Medical Center Disclosure No conflicts of interest to disclose Objectives o Outline the elements of
Interaction between Sedation and Weaning: How to Balance Them? Guillermo Castorena MD Fundacion Clinica Medica Sur Mexico
 Interaction between Sedation and Weaning: How to Balance Them? Guillermo Castorena MD Fundacion Clinica Medica Sur Mexico Balance is not that easy! Weaning Weaning is the liberation of a patient from
Interaction between Sedation and Weaning: How to Balance Them? Guillermo Castorena MD Fundacion Clinica Medica Sur Mexico Balance is not that easy! Weaning Weaning is the liberation of a patient from
Managing Delirium: The best way to achieve clarity (of mind) Tim Walsh. Professor of Critical Care, Edinburgh University
 Tim Walsh. Professor of Critical Care, Edinburgh University") Managing Delirium: The best way to achieve clarity (of mind) Tim Walsh Professor of Critical Care, Edinburgh University Lecture Plan: a route to clarity What is delirium? Why is delirium important? Step
Managing Delirium: The best way to achieve clarity (of mind) Tim Walsh Professor of Critical Care, Edinburgh University Lecture Plan: a route to clarity What is delirium? Why is delirium important? Step
ICU LIBERATION: IMPLEMENTING THE ABCDEF BUNDLE AND IMPROVING THE LIVES OF ICU PATIENTS
 ICU LIBERATION: IMPLEMENTING THE ABCDEF BUNDLE AND IMPROVING THE LIVES OF ICU PATIENTS J. MATTHEW ALDRICH, MD ASSOCIATE CLINICAL PROFESSOR OF ANESTHESIA AND PERIOPERATIVE CARE UNIVERSITY OF CALIFORNIA
ICU LIBERATION: IMPLEMENTING THE ABCDEF BUNDLE AND IMPROVING THE LIVES OF ICU PATIENTS J. MATTHEW ALDRICH, MD ASSOCIATE CLINICAL PROFESSOR OF ANESTHESIA AND PERIOPERATIVE CARE UNIVERSITY OF CALIFORNIA
Critical Care Strategic Clinical Network Provincial ICU Delirium Framework
 Pain assessed and documentation using validated tool (CPOT and NRS) Assess and document q4h and prn 100% of patients assessed for pain and documented q4h A: Assess, Prevent & Manage Pain Self Reporting
Pain assessed and documentation using validated tool (CPOT and NRS) Assess and document q4h and prn 100% of patients assessed for pain and documented q4h A: Assess, Prevent & Manage Pain Self Reporting
KICU Spontaneous Awakening Trial (SAT) Questionnaire
 Questionnaire") KICU Spontaneous Awakening Trial (SAT) Questionnaire Please select your best answer(s): 1. What is your professional role? 1 Staff Nurse 2 Nurse Manager 3 Nurse Educator 4 Physician 5 Medical Director
KICU Spontaneous Awakening Trial (SAT) Questionnaire Please select your best answer(s): 1. What is your professional role? 1 Staff Nurse 2 Nurse Manager 3 Nurse Educator 4 Physician 5 Medical Director
Kendiss Olafson MD FRCPC MPH Section of Critical Care University of Manitoba
 Kendiss Olafson MD FRCPC MPH Section of Critical Care University of Manitoba Outline Sedation in ICU Purpose/Goals Common Drugs Sedation delivery strategies Mobility in the ICU Weakness with critical illness
Kendiss Olafson MD FRCPC MPH Section of Critical Care University of Manitoba Outline Sedation in ICU Purpose/Goals Common Drugs Sedation delivery strategies Mobility in the ICU Weakness with critical illness
Overview of Presentation. Delirium Definition. Assessing & Managing ICU Delirium: What is the Evidence?
 Assessing & Managing ICU Delirium: What is the Evidence? Dale Needham, MD, PhD Professor Pulmonary & Critical Care Medicine, and Physical Medicine & Rehabilitation Medical Director, Critical Care Physical
Assessing & Managing ICU Delirium: What is the Evidence? Dale Needham, MD, PhD Professor Pulmonary & Critical Care Medicine, and Physical Medicine & Rehabilitation Medical Director, Critical Care Physical
Ventilator-Associated Event Prevention: Innovations
 Ventilator-Associated Event Prevention: Innovations Michael J. Apostolakos, MD Professor of Medicine Director, Adult Critical Care University of Rochester Mobility/Sedation in the ICU Old teaching: Keep
Ventilator-Associated Event Prevention: Innovations Michael J. Apostolakos, MD Professor of Medicine Director, Adult Critical Care University of Rochester Mobility/Sedation in the ICU Old teaching: Keep
Sedation and delirium- drugs and clinical management
 Sedation and delirium- drugs and clinical management Shannon S. Carson, MD Associate Professor and Chief Division of Pulmonary and Critical Care Medicine University of North Carolina Probability of transitioning
Sedation and delirium- drugs and clinical management Shannon S. Carson, MD Associate Professor and Chief Division of Pulmonary and Critical Care Medicine University of North Carolina Probability of transitioning
Sedation of the Critically Ill Patient
 Buffalo theory of sedation It s a well known fact that a herd of buffalo can only move as fast as the slowest buffalo. And when the herd is hunted, it s the slowest and weakest ones at the back that are
Buffalo theory of sedation It s a well known fact that a herd of buffalo can only move as fast as the slowest buffalo. And when the herd is hunted, it s the slowest and weakest ones at the back that are
Executive Sponsorship of Delirium Initiatives Lessons from ICU Liberation
 Executive Sponsorship of Delirium Initiatives Lessons from ICU Liberation J. Matthew Aldrich, MD Co-Chair, SCCM ICU Liberation Committee Associate Professor Medical Director, Critical Care Medicine UCSF
Executive Sponsorship of Delirium Initiatives Lessons from ICU Liberation J. Matthew Aldrich, MD Co-Chair, SCCM ICU Liberation Committee Associate Professor Medical Director, Critical Care Medicine UCSF
9/28/2016. Sedation Strategies in the ICU. Outline. ICU sedation. Recent clinical practice guidelines Top 10 myths A practical approach
 Sedation Strategies in the ICU UW Medicine EMS and Trauma Conference Seattle, Washington September 26 th, 2016 C. Terri Hough, MD MSc Associate Professor of Medicine Division of Pulmonary and Critical
Sedation Strategies in the ICU UW Medicine EMS and Trauma Conference Seattle, Washington September 26 th, 2016 C. Terri Hough, MD MSc Associate Professor of Medicine Division of Pulmonary and Critical
Disclosure. Hospira Pharmaceuticals. Unrestricted research funding Honoraria for CME education administered via France Foundation
 Disclosure Hospira Pharmaceuticals Unrestricted research funding Honoraria for CME education administered via France Foundation Economics in Sedation: Responsible Use of the ICU Budget John W. Devlin,
Disclosure Hospira Pharmaceuticals Unrestricted research funding Honoraria for CME education administered via France Foundation Economics in Sedation: Responsible Use of the ICU Budget John W. Devlin,
DELIRIUM IN ICU: Prevention and Management. Milind Baldi
 DELIRIUM IN ICU: Prevention and Management Milind Baldi Contents Introduction Risk factors Assessment Prevention Management Introduction Delirium is a syndrome characterized by acute cerebral dysfunction
DELIRIUM IN ICU: Prevention and Management Milind Baldi Contents Introduction Risk factors Assessment Prevention Management Introduction Delirium is a syndrome characterized by acute cerebral dysfunction
KEY REFERENCES Laying the foundation for D of ABCDEF bundle
 KEY REFERENCES Laying the foundation for D of ABCDEF bundle Ely E. JAMA. 2001;286:2703-2710 (CAM-ICU) Bergeron N. Intensive Care Med. 2001;27:859-864 (ICDSC) Dubois M. Intensive Care Med. 2001;27:1297-1304
KEY REFERENCES Laying the foundation for D of ABCDEF bundle Ely E. JAMA. 2001;286:2703-2710 (CAM-ICU) Bergeron N. Intensive Care Med. 2001;27:859-864 (ICDSC) Dubois M. Intensive Care Med. 2001;27:1297-1304
Liberation from Mechanical Ventilation in Critically Ill Adults
 Liberation from Mechanical Ventilation in Critically Ill Adults 2017 ACCP/ATS Clinical Practice Guidelines Timothy D. Girard, MD, MSCI Clinical Research, Investigation, and Systems Modeling of Acute Illness
Liberation from Mechanical Ventilation in Critically Ill Adults 2017 ACCP/ATS Clinical Practice Guidelines Timothy D. Girard, MD, MSCI Clinical Research, Investigation, and Systems Modeling of Acute Illness
ABCDEF Bundle Breakout
 ABCDEF Bundle Breakout Andrew Masica, MD, MSCI VP, Chief Clinical Effectiveness Officer Baylor Scott & White Health andrew.masica@bswhealth.org Disclosures/Funding Support Grant R18-HS021459 from the Agency
ABCDEF Bundle Breakout Andrew Masica, MD, MSCI VP, Chief Clinical Effectiveness Officer Baylor Scott & White Health andrew.masica@bswhealth.org Disclosures/Funding Support Grant R18-HS021459 from the Agency
ABCs of ICU Delirium Marian Maxwell, Pharm.D., BCCCP January 6, 2018
 ABCs of ICU Delirium Marian Maxwell, Pharm.D., BCCCP January 6, 2018 Disclosures I do not have any financial/non-financial relationships to disclose. Learning Objectives Define delirium and discuss the
ABCs of ICU Delirium Marian Maxwell, Pharm.D., BCCCP January 6, 2018 Disclosures I do not have any financial/non-financial relationships to disclose. Learning Objectives Define delirium and discuss the
Pain, Agitation & Delirium (2013) Immobility & Sleep (2018) Catherine Jones Practice Educator GICU October 2018
 Immobility & Sleep (2018) Catherine Jones Practice Educator GICU October 2018") Pain, Agitation & Delirium (2013) Immobility & Sleep (2018) Catherine Jones Practice Educator GICU October 2018 1 Plan for session Why Pain Agitation & Delirium are important considerations in critical
Pain, Agitation & Delirium (2013) Immobility & Sleep (2018) Catherine Jones Practice Educator GICU October 2018 1 Plan for session Why Pain Agitation & Delirium are important considerations in critical
Improving the Management of Pain, Agitation, and Delirium (PAD) in the Intensive Care Unit: Translating Evidence Into Practice
 in the Intensive Care Unit: Translating Evidence Into Practice") Improving the Management of Pain, Agitation, and Delirium (PAD) in the Intensive Care Unit: Translating Evidence Into Practice Christine M. Groth, Pharm.D., BCCCP NYS Partnership for Patients September
Improving the Management of Pain, Agitation, and Delirium (PAD) in the Intensive Care Unit: Translating Evidence Into Practice Christine M. Groth, Pharm.D., BCCCP NYS Partnership for Patients September
Do benzos, opioids, or strong anticholinergics cause delirium? Lisa Burry
 Do benzos, opioids, or strong anticholinergics cause delirium? Lisa Burry Delirium in the ICU Occurs in up to 85% of MICU/SICU MV patients 20-50% of lower severity ICU patients develop delirium Hypoactive
Do benzos, opioids, or strong anticholinergics cause delirium? Lisa Burry Delirium in the ICU Occurs in up to 85% of MICU/SICU MV patients 20-50% of lower severity ICU patients develop delirium Hypoactive
Can Goal Directed Sedation Improve Outcomes?
 Can Goal Directed Sedation Improve Outcomes? Yahya SHEHABI, FANZCA, FCICM, EMBA Professor and Program Director Critical care Monash Health and Monash University - Melbourne School of Medicine, University
Can Goal Directed Sedation Improve Outcomes? Yahya SHEHABI, FANZCA, FCICM, EMBA Professor and Program Director Critical care Monash Health and Monash University - Melbourne School of Medicine, University
Sedation Hold/Interruption and Weaning Protocol ( Wake-up and Breathe )
") PROTOCOL Sedation Hold/Interruption and Weaning Protocol ( Wake-up and Breathe ) Page 1 of 6 Scope: Population: Outcome: Critical care clinicians and providers. All ICU patients intubated or mechanically
PROTOCOL Sedation Hold/Interruption and Weaning Protocol ( Wake-up and Breathe ) Page 1 of 6 Scope: Population: Outcome: Critical care clinicians and providers. All ICU patients intubated or mechanically
Sarah V. Cogle, PharmD, BCCCP Assistant Clinical Professor Auburn University Harrison School of Pharmacy Auburn, AL ALSHP Annual Clinical Meeting
 Sarah V. Cogle, PharmD, BCCCP Assistant Clinical Professor Auburn University Harrison School of Pharmacy Auburn, AL ALSHP Annual Clinical Meeting 2018 I have no actual or potential conflict of interest
Sarah V. Cogle, PharmD, BCCCP Assistant Clinical Professor Auburn University Harrison School of Pharmacy Auburn, AL ALSHP Annual Clinical Meeting 2018 I have no actual or potential conflict of interest
MARIA KOBYLECKY RN, MScN, CNCC JEANENE LUCKHART BSc, Grad Dip PT CELINA ROGERS RRT SUZANNE WATTS BHSc PT
 MARIA KOBYLECKY RN, MScN, CNCC JEANENE LUCKHART BSc, Grad Dip PT CELINA ROGERS RRT SUZANNE WATTS BHSc PT Objectives Understand some of the detrimental effects of critical illness, prolonged bed rest and
MARIA KOBYLECKY RN, MScN, CNCC JEANENE LUCKHART BSc, Grad Dip PT CELINA ROGERS RRT SUZANNE WATTS BHSc PT Objectives Understand some of the detrimental effects of critical illness, prolonged bed rest and
ICU Delirium and sedation: understanding their role in long-term patient outcomes. Yoanna Skrobik MD FRCP(c)
") ICU Delirium and sedation: understanding their role in long-term patient outcomes Yoanna Skrobik MD FRCP(c) Conflicts of interest Member, SCCM Pain, Agitation and Delirium guidelines writing committee
ICU Delirium and sedation: understanding their role in long-term patient outcomes Yoanna Skrobik MD FRCP(c) Conflicts of interest Member, SCCM Pain, Agitation and Delirium guidelines writing committee
Sedation and Delirium Questions
 Sedation and Delirium Questions TLC Curriculum William J. Ehlenbach, MD MSc Assistant Professor of Medicine Pulmonary & Critical Care Medicine Question 1 Deep sedation in ventilated critically patients
Sedation and Delirium Questions TLC Curriculum William J. Ehlenbach, MD MSc Assistant Professor of Medicine Pulmonary & Critical Care Medicine Question 1 Deep sedation in ventilated critically patients
ANALGESIA AND SEDATION IN MECHANICAL VENTILATION
 ANALGESIA AND SEDATION IN MECHANICAL VENTILATION Erik Stoltenberg, MD Abbott Northwestern Hospital February 27, 2018 DISCLOSURE Nothing to disclose AllinaHealthSystem 1 OBJECTIVE To apply knowledge of
ANALGESIA AND SEDATION IN MECHANICAL VENTILATION Erik Stoltenberg, MD Abbott Northwestern Hospital February 27, 2018 DISCLOSURE Nothing to disclose AllinaHealthSystem 1 OBJECTIVE To apply knowledge of
Conducting Delirium Research
 Optimizing Clinical Trials When Conducting Research Research funding: Disclosure NHLBI, NIA, AstraZeneca John W. Devlin, PharmD, FCCP, FCCM, Professor of Pharmacy, Northeastern University Scientific Staff,
Optimizing Clinical Trials When Conducting Research Research funding: Disclosure NHLBI, NIA, AstraZeneca John W. Devlin, PharmD, FCCP, FCCM, Professor of Pharmacy, Northeastern University Scientific Staff,
Delirium in the ICU: Prevention and Treatment. Delirium Defined Officially. Delirium: Really Defined. S. Andrew Josephson, MD
 Delirium in the ICU: Prevention and Treatment S. Andrew Josephson, MD Director, Neurohospitalist Service Medical Director, Inpatient Neurology June 2, 2011 Delirium Defined Officially (DSM-IV-TR) criteria
Delirium in the ICU: Prevention and Treatment S. Andrew Josephson, MD Director, Neurohospitalist Service Medical Director, Inpatient Neurology June 2, 2011 Delirium Defined Officially (DSM-IV-TR) criteria
EFFECT OF ABCDE BUNDLE IMPLEMENTATION DELIRIUM IN INTENSIVE CARE UNIT PATIENTS ON PREVALENCE OF. Delirium Assessment. 1.0 Hour
 Delirium Assessment EFFECT OF ABCDE BUNDLE IMPLEMENTATION ON PREVALENCE OF DELIRIUM IN INTENSIVE CARE UNIT PATIENTS By Mandy Bounds, RN, MSN, CCRN, Stacey Kram, RN-BC, DNP, PCCN, CCRN, Karen Gabel Speroni,
Delirium Assessment EFFECT OF ABCDE BUNDLE IMPLEMENTATION ON PREVALENCE OF DELIRIUM IN INTENSIVE CARE UNIT PATIENTS By Mandy Bounds, RN, MSN, CCRN, Stacey Kram, RN-BC, DNP, PCCN, CCRN, Karen Gabel Speroni,
+ Change in baseline mental status, inattention, and either disorganized thinking or altered level of consciousness. Delirium. Disclosure.
 47 th Annual Meeting August 2-4, 2013 Orlando, FL Identification, Prevention and Treatment of Delirium: The Role of the Health System Pharmacist Jennifer Cortes, PharmD, BCPS Medical ICU Clinical Pharmacy
47 th Annual Meeting August 2-4, 2013 Orlando, FL Identification, Prevention and Treatment of Delirium: The Role of the Health System Pharmacist Jennifer Cortes, PharmD, BCPS Medical ICU Clinical Pharmacy
CUSP 4 MVP-VAP Patient Care Bundle
 Spontaneous Awakening and Spontaneous Breathing Trials, Literature Synopsis CUSP 4 MVP-VAP Patient Care Bundle Spontaneous awakening trials (SAT) and spontaneous breathing trials (SBT) reduce the length
Spontaneous Awakening and Spontaneous Breathing Trials, Literature Synopsis CUSP 4 MVP-VAP Patient Care Bundle Spontaneous awakening trials (SAT) and spontaneous breathing trials (SBT) reduce the length
Putting the Pieces of the Puzzle Together: A Journey through ABCDEF
 Putting the Pieces of the Puzzle Together: A Journey through ABCDEF Kristy Colford RN,BSN, CCRN Clinical Nurse Educator Avera McKennan Intensive Care Kristy Colford- Have No Disclosures ZOOM in & ZOOM
Putting the Pieces of the Puzzle Together: A Journey through ABCDEF Kristy Colford RN,BSN, CCRN Clinical Nurse Educator Avera McKennan Intensive Care Kristy Colford- Have No Disclosures ZOOM in & ZOOM
DIAGRAM OF THE PRESENTATION. Post ICU Rehabilitation. Effective strategies in ICU. During two last decades
 1 1st European Conference on Weaning & Rehabilitation in Critically ill Patients INTERNATIONAL EARLY MOBILISATION NETWORK Post ICU Rehabilitation Serafeim N. Nanas Professor of Critical Care Medicine Evaggelismos
1 1st European Conference on Weaning & Rehabilitation in Critically ill Patients INTERNATIONAL EARLY MOBILISATION NETWORK Post ICU Rehabilitation Serafeim N. Nanas Professor of Critical Care Medicine Evaggelismos
Supplementary appendix
 Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Page VJ, Casarin A, Ely EW, et al. Evaluation
Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Page VJ, Casarin A, Ely EW, et al. Evaluation
ICU Liberation ABCDEF Bundle Implementation: Focus on Delirium
 ICU Liberation ABCDEF Bundle Implementation: Focus on Delirium Diane Byrum MSN RN CCRN-K CCNS FCCM Quality Implementation Consultant Innovative Solutions For Healthcare Education, LLC Oak Island, NC ICU
ICU Liberation ABCDEF Bundle Implementation: Focus on Delirium Diane Byrum MSN RN CCRN-K CCNS FCCM Quality Implementation Consultant Innovative Solutions For Healthcare Education, LLC Oak Island, NC ICU
KEY REFERENCES laying the foundation for A of ABCDEF bundle
 KEY REFERENCES laying the foundation for A of ABCDEF bundle Puntillo K. Am J Crit Care (Response Procedural Pain) 2001;10:238-251 Payen J. Crit Care Med (Behavioral Pain Scale) 2001;29:2258-2263 Gelinas
KEY REFERENCES laying the foundation for A of ABCDEF bundle Puntillo K. Am J Crit Care (Response Procedural Pain) 2001;10:238-251 Payen J. Crit Care Med (Behavioral Pain Scale) 2001;29:2258-2263 Gelinas
PHYSICIAN'S ORDERS Mark in for desired orders. If is blank, order is inactive. VENTILATOR SEDATION / ANALGESIC / DELIRIUM ORDER
 Nursing Daily awakenings PHYSICIAN'S ORDERS Mark in for desired orders. If is blank, order is inactive. VENTILATOR SEDATION / ANALGESIC / DELIRIUM ORDER Do not perform daily awakenings: Rationale: Daily
Nursing Daily awakenings PHYSICIAN'S ORDERS Mark in for desired orders. If is blank, order is inactive. VENTILATOR SEDATION / ANALGESIC / DELIRIUM ORDER Do not perform daily awakenings: Rationale: Daily
What are Appropriate End-points for Delirium Prevention/Treatment Studies
 What are Appropriate End-points for Delirium Prevention/Treatment Studies Pratik Pandharipande, MD, MSCI Professor of Anesthesiology and Surgery Department of Anesthesiology Vanderbilt University School
What are Appropriate End-points for Delirium Prevention/Treatment Studies Pratik Pandharipande, MD, MSCI Professor of Anesthesiology and Surgery Department of Anesthesiology Vanderbilt University School
7/6/ ANNUAL MEETING BRINGING THE ABC(DEF) S TO THE ICU ICU TRIAD DISCLOSURE ICU TRIAD SEDATION AND ANALGESIA OBJECTIVES
 S TO THE ICU ICU TRIAD DISCLOSURE ICU TRIAD SEDATION AND ANALGESIA OBJECTIVES") ICU TRIAD BRINGING THE ABC(DEF) S TO THE ICU GINA RIGGI, PHARMD, BCPS, BCCCP CLINICAL HOSPITAL PHARMACIST- TRAUMA INTENSIVE CARE UNIT JACKSON MEMORIAL HOSPITAL MIAMI, FLORIDA Figure 1. Reade M and Finfer
ICU TRIAD BRINGING THE ABC(DEF) S TO THE ICU GINA RIGGI, PHARMD, BCPS, BCCCP CLINICAL HOSPITAL PHARMACIST- TRAUMA INTENSIVE CARE UNIT JACKSON MEMORIAL HOSPITAL MIAMI, FLORIDA Figure 1. Reade M and Finfer
Clinical Practice Guidelines for the Management of Pain, Agitation, and Delirium in Adult Patients
 Clinical Practice Guidelines for the Management of Pain, Agitation, and Delirium in Adult Patients in the Intensive Care Unit January 2013 Volume 41 Number 1 Society of Critical Care Medicine 本檔僅供內部教學使用檔案內所使用之照片之版權仍屬於原期刊公開使用時,
Clinical Practice Guidelines for the Management of Pain, Agitation, and Delirium in Adult Patients in the Intensive Care Unit January 2013 Volume 41 Number 1 Society of Critical Care Medicine 本檔僅供內部教學使用檔案內所使用之照片之版權仍屬於原期刊公開使用時,
Fighting the Fog A Collaborative Approach to Decreasing ICU Delirium
 Fighting the Fog A Collaborative Approach to Decreasing ICU Delirium Kimberly Scherr NP Jennifer Barker RN Misericordia Hospital ICU Edmonton, AB CACCN Dynamics Sept 21, 2014 Delirium Delirium is an acute
Fighting the Fog A Collaborative Approach to Decreasing ICU Delirium Kimberly Scherr NP Jennifer Barker RN Misericordia Hospital ICU Edmonton, AB CACCN Dynamics Sept 21, 2014 Delirium Delirium is an acute
Start Walking: Improving Outcomes through Use of an Early Progressive Mobility Program. Theresa Murray MSN,RN, CCRN,CCNS Samantha Lichti BSN, RN
 Start Walking: Improving Outcomes through Use of an Early Progressive Mobility Program Theresa Murray MSN,RN, CCRN,CCNS Samantha Lichti BSN, RN Challenge, Journey, Evolution Everest is 29, 035 ft. 5 ½
Start Walking: Improving Outcomes through Use of an Early Progressive Mobility Program Theresa Murray MSN,RN, CCRN,CCNS Samantha Lichti BSN, RN Challenge, Journey, Evolution Everest is 29, 035 ft. 5 ½
Sedation in The ICU: The Biological Cost of the Depression of Consciousness
 Sedation in The ICU: The Biological Cost of the Depression of Consciousness Michael Ramsay MD FRCA Chairman Department of Anesthesia Baylor University Medical Center Professor Texas A&M University Clinical
Sedation in The ICU: The Biological Cost of the Depression of Consciousness Michael Ramsay MD FRCA Chairman Department of Anesthesia Baylor University Medical Center Professor Texas A&M University Clinical
Optimize vent weaning and SBT outcomes. Identify underlying causes for SBT failures. Role SBT and weaning protocol have in respiratory care
 Optimize vent weaning and SBT outcomes Identify underlying causes for SBT failures Role SBT and weaning protocol have in respiratory care Lower risk of developing complications Lower risk of VAP, other
Optimize vent weaning and SBT outcomes Identify underlying causes for SBT failures Role SBT and weaning protocol have in respiratory care Lower risk of developing complications Lower risk of VAP, other
Delirium Screening and Prevention. Faculty Disclosures. Objectives 5/13/2014. I have nothing to disclose
 Delirium Screening and Prevention Kathleen Puntillo RN, PhD, FAAN, FCCM Professor Emeritus School of Nursing, UCSF Faculty Disclosures I have nothing to disclose Objectives Discuss prevalence, risk factors
Delirium Screening and Prevention Kathleen Puntillo RN, PhD, FAAN, FCCM Professor Emeritus School of Nursing, UCSF Faculty Disclosures I have nothing to disclose Objectives Discuss prevalence, risk factors
Management of Delirium in the ICU. Yahya Shehabi
 Management of Delirium in the ICU Yahya Shehabi Hello! Doctor, your patient is CAM + ve Good morning Dr, Am one of the RC, Just examined Mr XXX he is CAM +ve Positive what? Sir replied RC: I meant he is
Management of Delirium in the ICU Yahya Shehabi Hello! Doctor, your patient is CAM + ve Good morning Dr, Am one of the RC, Just examined Mr XXX he is CAM +ve Positive what? Sir replied RC: I meant he is
NYSPFP HIIN: VAE/Delirium Prevention. Operationalizing the Pain, Agitation and Delirium Assessments
 NYSPFP HIIN: VAE/Delirium Prevention Operationalizing the Pain, Agitation and Delirium Assessments March 28, 2017 1 Agenda Topic Welcome and Introductions A Guide for Success: Implementing the Confusion
NYSPFP HIIN: VAE/Delirium Prevention Operationalizing the Pain, Agitation and Delirium Assessments March 28, 2017 1 Agenda Topic Welcome and Introductions A Guide for Success: Implementing the Confusion
Implementation of a Delirium Screening Tool in a Pediatric Intensive Care Unit
 Implementation of a Delirium Screening Tool in a Pediatric Intensive Care Unit BY: ABBY WACHHOLTZ, BSN, RN, PEDIATRIC ACUTE CARE DNP STUDENT Disclosures I have no disclosures. 1 Objectives 1. Recognize
Implementation of a Delirium Screening Tool in a Pediatric Intensive Care Unit BY: ABBY WACHHOLTZ, BSN, RN, PEDIATRIC ACUTE CARE DNP STUDENT Disclosures I have no disclosures. 1 Objectives 1. Recognize
Summary of Delirium Clinical Practice Guideline Recommendations Post Operative
 Summary of Delirium Clinical Practice Guideline Recommendations Post Operative Intensive Care Unit Clinical Practice Guideline for Postoperative Clinical Practice Guidelines for the Delirium in Older Adults;
Summary of Delirium Clinical Practice Guideline Recommendations Post Operative Intensive Care Unit Clinical Practice Guideline for Postoperative Clinical Practice Guidelines for the Delirium in Older Adults;
Delirium in the hospitalized patient
 Delirium in the hospitalized patient Jennifer A. Tarin, M.D. Department of Hospital Medicine Geriatric Health Safety Chair Colorado Permanente Medical Group UCLA Reynolds Scholar Delirium Preventing delirium
Delirium in the hospitalized patient Jennifer A. Tarin, M.D. Department of Hospital Medicine Geriatric Health Safety Chair Colorado Permanente Medical Group UCLA Reynolds Scholar Delirium Preventing delirium
Management of pain, agitation, and delirium in critically ill patients
 REVIEW ARTICLE Management of pain, agitation, and delirium in critically ill patients Pratik P. Pandharipande 1,2, Mayur B. Patel 2,3, Juliana Barr 4 1 Division of Critical Care, Department of Anesthesiology,
REVIEW ARTICLE Management of pain, agitation, and delirium in critically ill patients Pratik P. Pandharipande 1,2, Mayur B. Patel 2,3, Juliana Barr 4 1 Division of Critical Care, Department of Anesthesiology,
Delirium Screening and Prevention Faculty Disclosures
 Delirium Screening and Prevention Faculty Disclosures I have nothing to disclose Kathleen Puntillo RN, PhD, FAAN, FCCM Professor Emeritus School of Nursing, UCSF Objectives Discuss prevalence, risk factors
Delirium Screening and Prevention Faculty Disclosures I have nothing to disclose Kathleen Puntillo RN, PhD, FAAN, FCCM Professor Emeritus School of Nursing, UCSF Objectives Discuss prevalence, risk factors
NYSPFP HIIN: VAE/Delirium Prevention. Operationalizing Prevention Strategies in the ICU
 NYSPFP HIIN: VAE/Delirium Prevention Operationalizing Prevention Strategies in the ICU 1 Agenda Time Topic Speakers 9:00 a.m.-9:10 a.m. Welcome & Introductions NYSPFP Staff 9:10 a.m.-10:40 am Why Prevent
NYSPFP HIIN: VAE/Delirium Prevention Operationalizing Prevention Strategies in the ICU 1 Agenda Time Topic Speakers 9:00 a.m.-9:10 a.m. Welcome & Introductions NYSPFP Staff 9:10 a.m.-10:40 am Why Prevent
PREVENTING VENTILATORASSOCIATED EVENTS >>> >>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>> 2018 UPDATE
 2018 UPDATE PREVENTING VENTILATORASSOCIATED EVENTS >>> PREVENTING VENTILATOR-ASSOCIATED EVENTS CHANGE PACKAGE ii >>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>> ACKNOWLEDGEMENTS The analyses upon
2018 UPDATE PREVENTING VENTILATORASSOCIATED EVENTS >>> PREVENTING VENTILATOR-ASSOCIATED EVENTS CHANGE PACKAGE ii >>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>> ACKNOWLEDGEMENTS The analyses upon
ICU Delirium in Infants & Children: Cause for Concern or False Alarm. Objectives
 ICU Delirium in Infants & Children: Cause for Concern or False Alarm Peter (Pete) N. Johnson, Pharm.D., BCPS, BCPPS, FPPAG Associate Professor of Pharmacy Practice University of Oklahoma College of Pharmacy
ICU Delirium in Infants & Children: Cause for Concern or False Alarm Peter (Pete) N. Johnson, Pharm.D., BCPS, BCPPS, FPPAG Associate Professor of Pharmacy Practice University of Oklahoma College of Pharmacy
Sleep in the ICU: helped by drugs? Yoanna Skrobik MD FRCP(c) MSc.
 MSc.") Sleep in the ICU: helped by drugs? Yoanna Skrobik MD FRCP(c) MSc. Conflicts of interest Member, SCCM Pain, Agitation and Delirium guidelines writing committee Vice-chair, SCCM Pain, Agitation, Delirium,
Sleep in the ICU: helped by drugs? Yoanna Skrobik MD FRCP(c) MSc. Conflicts of interest Member, SCCM Pain, Agitation and Delirium guidelines writing committee Vice-chair, SCCM Pain, Agitation, Delirium,
ICU Early Mobilization at UCSF
 ICU Early Mobilization at UCSF Critical Care Medicine & Trauma Conference San Francisco, CA June 5, 2010 Presented by Heidi Engel, PT, DPT Heidi.Engel@ucsfmedctr.org Can We Do Better? Herridge MS. Mobile,
ICU Early Mobilization at UCSF Critical Care Medicine & Trauma Conference San Francisco, CA June 5, 2010 Presented by Heidi Engel, PT, DPT Heidi.Engel@ucsfmedctr.org Can We Do Better? Herridge MS. Mobile,
Juliana Barr, MD, FCCM
 Juliana Barr, MD, FCCM Staff Anesthesiologist and Intensivist, VA Palo Alto Health Care System Associate Professor, Anesthesiology, Perioperative, and Pain Medicine Stanford University School of Medicine
Juliana Barr, MD, FCCM Staff Anesthesiologist and Intensivist, VA Palo Alto Health Care System Associate Professor, Anesthesiology, Perioperative, and Pain Medicine Stanford University School of Medicine
Implementing the 2013 PAD Guidelines
 1 of 20 8/11/2013 10:25 PM www.medscape.com Implementing the 2013 PAD Guidelines Top Ten Points to Consider Brenda T. Pun, MSN, RN, ACNP, Michele C. Balas, PhD, RN, APRN-NP, CCRN, Judy Davidson, DNP, RN,
1 of 20 8/11/2013 10:25 PM www.medscape.com Implementing the 2013 PAD Guidelines Top Ten Points to Consider Brenda T. Pun, MSN, RN, ACNP, Michele C. Balas, PhD, RN, APRN-NP, CCRN, Judy Davidson, DNP, RN,
Preventing Delirium in the IntensiveCareUnit
 Preventing Delirium in the IntensiveCareUnit Nathan E. Brummel, MD a,b,c, *, Timothy D. Girard, MD, MSCI a,b,c,d KEYWORDS Delirium Intensive care unit Prevention Sedation KEY POINTS Delirium in the intensive
Preventing Delirium in the IntensiveCareUnit Nathan E. Brummel, MD a,b,c, *, Timothy D. Girard, MD, MSCI a,b,c,d KEYWORDS Delirium Intensive care unit Prevention Sedation KEY POINTS Delirium in the intensive
What About All Those Critical Lines? Lines, catheters and drains can be accommodated, secured EVD line stationary bike
 What About All Those Critical Lines? Lines, catheters and drains can be accommodated, secured EVD line stationary bike What About All Those Critical Lines?. Patient lines and drains can be accommodated
What About All Those Critical Lines? Lines, catheters and drains can be accommodated, secured EVD line stationary bike What About All Those Critical Lines?. Patient lines and drains can be accommodated
1. Screening to identify SBT candidates
 Karen E. A. Burns MD, FRCPC, MSc (Epid) Associate Professor, Clinician Scientist St. Michael s Hospital, Toronto, Canada burnsk@smh.ca Review evidence supporting: 1. Screening to identify SBT candidates
Karen E. A. Burns MD, FRCPC, MSc (Epid) Associate Professor, Clinician Scientist St. Michael s Hospital, Toronto, Canada burnsk@smh.ca Review evidence supporting: 1. Screening to identify SBT candidates
Strategies for Enhancing Sepsis Survivorship
 Strategies for Enhancing Sepsis Survivorship Hallie Prescott, MD, MSc Ohio Hospital Association August 16, 2016 Disclosures I have no relevant financial conflicts of interest Key Funding NIH/NIGMS American
Strategies for Enhancing Sepsis Survivorship Hallie Prescott, MD, MSc Ohio Hospital Association August 16, 2016 Disclosures I have no relevant financial conflicts of interest Key Funding NIH/NIGMS American
POST-INTUBATION ANALGESIA AND SEDATION. August 2012 J Pelletier
 POST-INTUBATION ANALGESIA AND SEDATION August 2012 J Pelletier Intubated patients experience pain and anxiety Mechanical ventilation, endotracheal tube Blood draws, positioning, suctioning Surgical procedures,
POST-INTUBATION ANALGESIA AND SEDATION August 2012 J Pelletier Intubated patients experience pain and anxiety Mechanical ventilation, endotracheal tube Blood draws, positioning, suctioning Surgical procedures,
Disclosures. Implementation of the ABCDEF Bundle: Reducing Patient Injury. Sage Products Speaker Bureau & Consultant Hill-Rom Eloquest Healthcare
 Implementation of the ABCDEF Bundle: Reducing Patient Injury Kathleen M. Vollman MSN, RN, CCNS, FCCM, FAAN Clinical Nurse Specialist / Educator / Consultant ADVANCING NURSING kvollman@comcast.net Northville
Implementation of the ABCDEF Bundle: Reducing Patient Injury Kathleen M. Vollman MSN, RN, CCNS, FCCM, FAAN Clinical Nurse Specialist / Educator / Consultant ADVANCING NURSING kvollman@comcast.net Northville
What you need to know about Delirium in ICU. Dr Valerie Page Watford General Hospital
 What you need to know about Delirium in ICU Dr Valerie Page Watford General Hospital Delirium and outcome 40 year old ARDS ICU survivor college graduate I have been out of hospital and trying to get on
What you need to know about Delirium in ICU Dr Valerie Page Watford General Hospital Delirium and outcome 40 year old ARDS ICU survivor college graduate I have been out of hospital and trying to get on
CRITICALLY APPRAISED PAPER (CAP)
") CRITICALLY APPRAISED PAPER (CAP) Schweickert, W. D., Pohlman, M. C., Pohlman, A. S., Nigos, C., Pawlik, A. J., Esbrook, C. L., Kress, J.P. (2009). Early physical and occupational therapy in mechanically
CRITICALLY APPRAISED PAPER (CAP) Schweickert, W. D., Pohlman, M. C., Pohlman, A. S., Nigos, C., Pawlik, A. J., Esbrook, C. L., Kress, J.P. (2009). Early physical and occupational therapy in mechanically
ICU Rehabilitation: Current Issues Changing the ICU Paradigm: Role of Early Mobilization
 ICU Rehabilitation: Current Issues Changing the ICU Paradigm: Role of Early Mobilization Carolyn L. Rochester, M.D. Yale University School of Medicine VA Connecticut Healthcare System August 29, 2015 WFSICCM,
ICU Rehabilitation: Current Issues Changing the ICU Paradigm: Role of Early Mobilization Carolyn L. Rochester, M.D. Yale University School of Medicine VA Connecticut Healthcare System August 29, 2015 WFSICCM,
Wake up and Breathe: A journey in quality improvement and unintended benefits
 Wake up and Breathe: A journey in quality improvement and unintended benefits Jeffrey Singh MD FRCPC MSc Toronto Western Hospital Interdepartmental Division of Critical Care University of Toronto Disclosures
Wake up and Breathe: A journey in quality improvement and unintended benefits Jeffrey Singh MD FRCPC MSc Toronto Western Hospital Interdepartmental Division of Critical Care University of Toronto Disclosures
Canadian Practices for the Treatment of Delirium. Lisa Burry, BScPharm, PharmD
 Canadian Practices for the Treatment of Delirium Lisa Burry, BScPharm, PharmD Disclosures & Acknowledgements Conflicts of interest: None Acknowledgements: our patients and the clinical staff that supported
Canadian Practices for the Treatment of Delirium Lisa Burry, BScPharm, PharmD Disclosures & Acknowledgements Conflicts of interest: None Acknowledgements: our patients and the clinical staff that supported
The Pharmacist s Role in Implementing the New Pain, Agitation, and Delirium Guidelines in the Critical Care Setting
 The Pharmacist s Role in Implementing the New Pain, Agitation, and Delirium Guidelines in the Critical Care Setting Presented as a Breakfast Symposium and Live Webcast at the 47 th ASHP Midyear Clinical
The Pharmacist s Role in Implementing the New Pain, Agitation, and Delirium Guidelines in the Critical Care Setting Presented as a Breakfast Symposium and Live Webcast at the 47 th ASHP Midyear Clinical
Curr Opin Anesthesiol 24: ß 2011 Wolters Kluwer Health Lippincott Williams & Wilkins
 The complex interplay between delirium, sedation, and early mobility during critical illness: applications in the trauma unit Arna Banerjee a, Timothy D. Girard b,c and Pratik Pandharipande d a Department
The complex interplay between delirium, sedation, and early mobility during critical illness: applications in the trauma unit Arna Banerjee a, Timothy D. Girard b,c and Pratik Pandharipande d a Department
Changes in Breathing Variables During a 30-Minute Spontaneous Breathing Trial
 Changes in Breathing Variables During a 30-Minute Spontaneous Breathing Trial Juan B Figueroa-Casas MD, Sean M Connery MSc, and Ricardo Montoya RRT BACKGROUND: Spontaneous breathing trials (SBTs) are increasingly
Changes in Breathing Variables During a 30-Minute Spontaneous Breathing Trial Juan B Figueroa-Casas MD, Sean M Connery MSc, and Ricardo Montoya RRT BACKGROUND: Spontaneous breathing trials (SBTs) are increasingly
Effectiveness and Safety of the Awakening and Breathing Coordination, Delirium Monitoring/ Management, and Early Exercise/Mobility Bundle*
 Feature Articles Effectiveness and Safety of the Awakening and Breathing Coordination, Delirium Monitoring/ Management, and Early Exercise/Mobility Bundle* Michele C. Balas, PhD, RN, APRN-NP, CCRN 1 ;
Feature Articles Effectiveness and Safety of the Awakening and Breathing Coordination, Delirium Monitoring/ Management, and Early Exercise/Mobility Bundle* Michele C. Balas, PhD, RN, APRN-NP, CCRN 1 ;
Early Rehabilitation in the ICU: Do We Still Need Chest Physiotherapy?
 Early Rehabilitation in the ICU: Do We Still Need Chest Physiotherapy? Michelle Kho, PT, PhD Assistant Professor, School of Rehabilitation Science, McMaster University Adjunct Assistant Professor, Department
Early Rehabilitation in the ICU: Do We Still Need Chest Physiotherapy? Michelle Kho, PT, PhD Assistant Professor, School of Rehabilitation Science, McMaster University Adjunct Assistant Professor, Department
From the Department of Pharmacy (JM, CAF) and Department of Pulmonary and Critical
 and Department of Pulmonary and Critical") PrintClose Impact of a clinical pharmacist-enforced intensive care unit sedation protocol on duration of mechanical ventilation and hospital stay * Author(s): Marshall, John PharmD; Finn, Christine A.
PrintClose Impact of a clinical pharmacist-enforced intensive care unit sedation protocol on duration of mechanical ventilation and hospital stay * Author(s): Marshall, John PharmD; Finn, Christine A.
Dexmedetomidine: the various roles and utilization strategies. Julie Belfer, PharmD September 2014
 Dexmedetomidine: the various roles and utilization strategies Julie Belfer, PharmD September 2014 Disclosure No disclosures concerning possible financial or personal relationships with commercial entities
Dexmedetomidine: the various roles and utilization strategies Julie Belfer, PharmD September 2014 Disclosure No disclosures concerning possible financial or personal relationships with commercial entities
Delirium Screening: The next nurse sensitive indicator?
 Delirium Screening: The next nurse sensitive indicator? Sharon Gunn, MSN, MA, RN, ACNS-BC, CCRN Clinical Nurse Specialist Critical Care Baylor University Medical Center Dallas, TX Objectives Recognize
Delirium Screening: The next nurse sensitive indicator? Sharon Gunn, MSN, MA, RN, ACNS-BC, CCRN Clinical Nurse Specialist Critical Care Baylor University Medical Center Dallas, TX Objectives Recognize
Collaborative Regional Benchmarking Group (North of England, North Yorkshire & Humber and West Yorkshire)
") Best Practice Guidance Sedation These recommendations are bound by the current evidence and best practice at the time of writing and so will be subject to change as further developments are made in this
Best Practice Guidance Sedation These recommendations are bound by the current evidence and best practice at the time of writing and so will be subject to change as further developments are made in this
NIH Public Access Author Manuscript Crit Care Med. Author manuscript; available in PMC 2015 December 01.
 NIH Public Access Author Manuscript Published in final edited form as: Crit Care Med. 2014 December ; 42(12): e791 e795. doi:10.1097/ccm.0000000000000660. Effectiveness of Implementing a Wake up and Breathe
NIH Public Access Author Manuscript Published in final edited form as: Crit Care Med. 2014 December ; 42(12): e791 e795. doi:10.1097/ccm.0000000000000660. Effectiveness of Implementing a Wake up and Breathe
Early Goal Directed Sedation In Critically Ill Patients
 Early Goal Directed Sedation In Critically Ill Patients Yahya Shehabi, FCICM, FANZCA, EMBA Professor, Intensive Care Medicine Clinical School of Medicine, University New South Wales School of Epidemiology
Early Goal Directed Sedation In Critically Ill Patients Yahya Shehabi, FCICM, FANZCA, EMBA Professor, Intensive Care Medicine Clinical School of Medicine, University New South Wales School of Epidemiology
Preventing Postoperative Cognitive Decline in the Elderly
 Preventing Postoperative Cognitive Decline in the Elderly Alex Bekker, M.D., Ph.D Professor and Chair Department of Anesthesiology Rutgers New Jersey Medical School "My brain, that's my second favorite
Preventing Postoperative Cognitive Decline in the Elderly Alex Bekker, M.D., Ph.D Professor and Chair Department of Anesthesiology Rutgers New Jersey Medical School "My brain, that's my second favorite
Early Physical Rehabilitation in the ICU and Ventilator Liberation
 Early Physical Rehabilitation in the ICU and Ventilator Liberation 本檔僅供內部教學使用檔案內所使用之照片之版權仍屬於原期刊公開使用時, 須獲得原期刊之同意授權 Respiratory Care 2012 Oct Vol 57 No 10 Pedro A Mendez-Tellez MD and Dale M Needham MD PhD
Early Physical Rehabilitation in the ICU and Ventilator Liberation 本檔僅供內部教學使用檔案內所使用之照片之版權仍屬於原期刊公開使用時, 須獲得原期刊之同意授權 Respiratory Care 2012 Oct Vol 57 No 10 Pedro A Mendez-Tellez MD and Dale M Needham MD PhD
Delirium and ICU Liberation: Impact on Survival and Survivorship
 Delirium and ICU Liberation: Impact on Survival and Survivorship E. Wesley Ely, MD, MPH Professor of Medicine and Critical Care Vanderbilt University, Nashville, TN VA TN Valley Health Care System GRECC
Delirium and ICU Liberation: Impact on Survival and Survivorship E. Wesley Ely, MD, MPH Professor of Medicine and Critical Care Vanderbilt University, Nashville, TN VA TN Valley Health Care System GRECC
Management of delirium in mechanically ventilated patients. Advances in Critical Care Medicine King Hussein Cancer Center
 Management of delirium in mechanically ventilated patients Advances in Critical Care Medicine King Hussein Cancer Center Introduction Outline: Prevalence of delirium in ICU Why it is important to screen
Management of delirium in mechanically ventilated patients Advances in Critical Care Medicine King Hussein Cancer Center Introduction Outline: Prevalence of delirium in ICU Why it is important to screen
Naeem Ali, MD Medical Director. The Ohio State University Wexner Medical Center
 Update in Critical Care, 2012: Teamwork in the ICU Naeem Ali, MD Medical Director Medical Intensive Care Unit The Ohio State University Wexner Medical Center 1 Many developments in Critical Care Emergence
Update in Critical Care, 2012: Teamwork in the ICU Naeem Ali, MD Medical Director Medical Intensive Care Unit The Ohio State University Wexner Medical Center 1 Many developments in Critical Care Emergence
Jennifer Mando-Vandrick, PharmD, BCPS Clinical Pharmacist, Emergency Department Director, PGY2 Critical Care Pharmacy Residency Duke University
 Jennifer Mando-Vandrick, PharmD, BCPS Clinical Pharmacist, Emergency Department Director, PGY2 Critical Care Pharmacy Residency Duke University Hospital Objectives Review pertinent pharmacotherapy common
Jennifer Mando-Vandrick, PharmD, BCPS Clinical Pharmacist, Emergency Department Director, PGY2 Critical Care Pharmacy Residency Duke University Hospital Objectives Review pertinent pharmacotherapy common
Monday, October 17 3:45 p.m. 5:45 p.m. Convention Center: Spirit of Pittsburgh Ballroom A
 Critical Care PRN and Society of Critical Care Medicine Focus Session Sedation and Delirium in the ICU: Update on the Status of the 2011 SCCM Guidelines Activity No. 0217-0000-11-079-L01-P (Application-Based
Critical Care PRN and Society of Critical Care Medicine Focus Session Sedation and Delirium in the ICU: Update on the Status of the 2011 SCCM Guidelines Activity No. 0217-0000-11-079-L01-P (Application-Based
Effectiveness and Safety of the Awakening and Breathing Coordination, Delirium
 Online Data Supplement Effectiveness and Safety of the Awakening and Breathing Coordination, Delirium Monitoring/Management, and Early Exercise/Mobility (ABCDE) Bundle Authors-Michele C. Balas, Eduard
Online Data Supplement Effectiveness and Safety of the Awakening and Breathing Coordination, Delirium Monitoring/Management, and Early Exercise/Mobility (ABCDE) Bundle Authors-Michele C. Balas, Eduard
Difficult weaning from mechanical ventilation
 Difficult weaning from mechanical ventilation Paolo Biban, MD Director, Neonatal and Paediatric Intensive Care Unit Division of Paediatrics, Major City Hospital Azienda Ospedaliera Universitaria Integrata
Difficult weaning from mechanical ventilation Paolo Biban, MD Director, Neonatal and Paediatric Intensive Care Unit Division of Paediatrics, Major City Hospital Azienda Ospedaliera Universitaria Integrata
Update in Critical Care Medicine
 Update in Critical Care Medicine Michael A. Gropper, MD, PhD Professor and Executive Vice Chair Department of Anesthesia and Perioperative Care Director, Critical Care Medicine UCSF Disclosure None Update
Update in Critical Care Medicine Michael A. Gropper, MD, PhD Professor and Executive Vice Chair Department of Anesthesia and Perioperative Care Director, Critical Care Medicine UCSF Disclosure None Update
Crit Vent Bundle for Mechanical Ventilation (337) [337] Physician - Also, enter Critical Care Admission Orders
![Crit Vent Bundle for Mechanical Ventilation (337) [337] Physician - Also, enter Critical Care Admission Orders](/thumbs/83/87321224.jpg "Crit Vent Bundle for Mechanical Ventilation (337) [337] Physician - Also, enter Critical Care Admission Orders") Crit Vent Bundle for Mechanical Ventilation (337) [337] Physician - Also, enter Critical Care Admission Orders Initial Vent Settings (Single Response) [6360] If no previous orders and no choice made by
Crit Vent Bundle for Mechanical Ventilation (337) [337] Physician - Also, enter Critical Care Admission Orders Initial Vent Settings (Single Response) [6360] If no previous orders and no choice made by
PHYSICIAN SIGNATURE DATE TIME DRUG ALLERGIES WT: KG
 Available ONLY at: BMC-B BMC-D BMC-N BMC-S Intubation Phase Notify Therapy for STAT intubation SUB Rapid Sequence Induction(SUB)* ***The above subphase is available at the end of the powerplan under the
Available ONLY at: BMC-B BMC-D BMC-N BMC-S Intubation Phase Notify Therapy for STAT intubation SUB Rapid Sequence Induction(SUB)* ***The above subphase is available at the end of the powerplan under the
ANWICU knowledge
 ANWICU knowledge www.anwicu.org.uk This presentation is provided by ANWICU We are a collaborative association of ICUs in the North West of England. Permission to provide this presentation has been granted
ANWICU knowledge www.anwicu.org.uk This presentation is provided by ANWICU We are a collaborative association of ICUs in the North West of England. Permission to provide this presentation has been granted
ICU Updates: Delirium in Hospitalized Patients
 ICU Updates: Delirium in Hospitalized Patients James A. Frank, MD Associate Professor Pulmonary and Critical Care UCSF Dept. of Medicine Director, MICU San Francisco VAMC Recognizing and preventing delirium
ICU Updates: Delirium in Hospitalized Patients James A. Frank, MD Associate Professor Pulmonary and Critical Care UCSF Dept. of Medicine Director, MICU San Francisco VAMC Recognizing and preventing delirium
9/15/2017. Conflict of Interest. Coordinating Spontaneous Breathing and Spontaneous Awakening* Overly Conservative Weaning Practices
 Conflict of Interest Coordinating Spontaneous Breathing and Spontaneous Awakening* Richard H Kallet MS RRT FAARC, FCCM Respiratory Care Services Dept of Anesthesia & Perioperative Care University of California,
Conflict of Interest Coordinating Spontaneous Breathing and Spontaneous Awakening* Richard H Kallet MS RRT FAARC, FCCM Respiratory Care Services Dept of Anesthesia & Perioperative Care University of California,
The Journal of Thoracic and Cardiovascular Surgery
 Accepted Manuscript Mechanical ventilation: a toxic asset David Bichell, M.D. PII: S0022-5223(18)33152-0 DOI: https://doi.org/10.1016/j.jtcvs.2018.11.039 Reference: YMTC 13799 To appear in: The Journal
Accepted Manuscript Mechanical ventilation: a toxic asset David Bichell, M.D. PII: S0022-5223(18)33152-0 DOI: https://doi.org/10.1016/j.jtcvs.2018.11.039 Reference: YMTC 13799 To appear in: The Journal