Determination of Death by Brain Death Criteria in Adults Page 1 of 10. All attending physicians certified to determine brain death.
|
|
|
- Roger O’Brien’
- 6 years ago
- Views:
Transcription
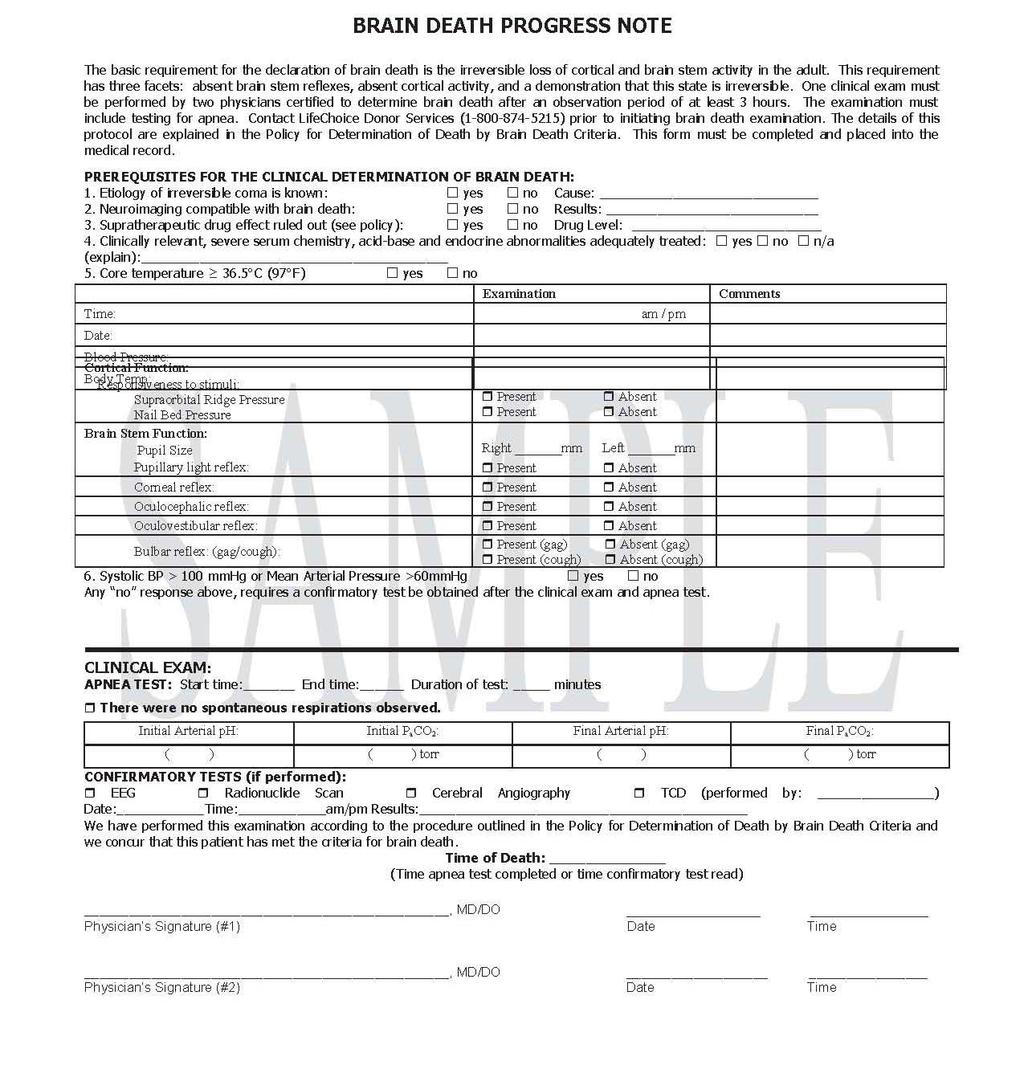
1 Page 1 of 10 Scope: All attending physicians certified to determine brain death. Statutory Background Uniform Determination of Death Act (Adopted in various forms in most states including Connecticut) An individual who has sustained either (1) irreversible cessation of circulatory and respiratory functions, or (2) irreversible cessation of all functions of the entire brain, including the brain stem is dead. A determination of death must be made in accordance with accepted medial standards. Connecticut Determination of Death Statutes Section 19a-504a (b) (Continuation or removal of life support system. Determination of death.) For purposes of making a determination concerning the continuation or removal of any life support system in a general hospital licensed under section 19a-491, an individual who has sustained either (1) irreversible cessation of circulatory and respiratory functions, or (2) irreversible cessation of all functions of the entire brain, including the brain stem, is dead. A determination of death must be made in accordance with accepted medical standards. Section 19a-289m (i) (Rights and responsibilities of a procurement organization. Donee's rights. Procedures for removing or transplanting donated body parts) Neither the physician who attends the decedent at death nor the physician who determines the time of the decedent's death may participate in the procedures for removing or transplanting a part from the decedent. Standard for Determination of Death For the purpose of these criteria, an individual is dead after a defined, irreversible brain insult results in cessation of all brain function, including the brain stem.
2 Page 2 of 10 Definitions: For the purposes of this policy, an attending physician certified to determine brain death as required by the Medical Staff shall be defined as a Board Eligible/Certified Neurologist, Intensivist, Anesthesiologist, Surgeon or Neurosurgeon on the Medical Staff certified as qualified for these determinations by their departments/divisions. Residents/Fellows in the above disciplines, certified as qualified for brain death determinations by their departments/divisions may also participate as defined below. Policy: For the purposes of this policy, adult is defined as all patients aged 18 years and older. For the purposes of this policy, the functions of the entire brain that are relevant to the determination of death are those that are clinically ascertainable. Confirmation by laboratory tests described herein is performed at the discretion of the clinician and is not required. A. General Determination of death hereunder requires a written documentation of the findings of one examination by at least two physicians qualified for brain death determinations (one of whom must be an attending physician and one who may be a resident/fellow) with documentation of the appropriate supporting medical data in the patient s chart. The Brain Death Progress Note form (#571120) shall be completed for documentation of the examination and placed in the chart. In the event death is being determined for purposes of anatomical donations, physicians participating in the removal or transplant procedure must exempt themselves from death determination in these instances. B. Timing of Examination An observation period of at least three hours is required prior to initiating the formal examination for the determination of brain death. Because cardiovascular instability often occurs following brain death, formal examination should begin as soon as possible after the three hour observation period has passed. The observation period may be decreased to a minimum of one hour if, in the opinion of the physicians performing the formal examination for the determination of brain death, the cause of the patient s brain injury is non-survivable and/or neuroimaging is consistent with brain death. This observation period will begin after documentation in the medical record of a neurologic examination performed by an MD, RN and/or Advanced Practitioner revealing the absence of cortical and brain stem function. Page 3 of 10
3 The examination must include the following: Absence of motor responsiveness to painful stimuli Spinally mediated motor responsiveness does not represent the presence of cortical or brain stem function Absence of bilateral pupillary light reflex; Absence of bilateral corneal reflex; Absence of bulbar reflex (cough and gag reflexes); Absence of spontaneous breaths C. Confirmatory Testing Confirmatory tests (see E. 3.) are not required unless any of the following conditions apply or other anatomic abnormalities exist, which preclude a complete evaluation. The following conditions may interfere with the clinical diagnosis of brain death: Severe cardio or respiratory instability; Severe facial trauma; Pre-existing pupillary abnormalities; Supratherapeutic dosages of any sedative drugs, or drugs with CNS effects or ability to affect respiratory drive or function such as aminoglycosides, tricyclic antidepressants, anticholinergics, antiepileptic drugs, chemotherapeutic agents, or neuromuscular blocking agents (see Complicating Conditions A); Sleep apnea or severe pulmonary disease resulting in chronic retention of CO2; Less than 24-hours from a hypoxic/anoxic event causing suspected neurologic condition D. Documentation The standardized Brain Death Progress Note form shall be completed and placed in the medical record to document the performance and results of the examination. The forms are available in each Intensive Care Unit. A sample of this form is provided in the Appendix. E. Examination for the Determination of Death by Brain Death Criteria The following criteria must be met: 1. CESSATION OF ALL FUNCTIONS OF THE ENTIRE BRAIN WHEN THE CAUSE OF THE INSULT IS KNOWN AND IS IRREVERSIBLE. THE EVALUATION MUST DEMONSTRATE FINDINGS OF 1a AND 1b: a. CEREBRAL FUNCTIONS ARE ABSENT: There is cerebral unreceptivity and unresponsiveness as evidenced by total unresponsiveness to environmental stimuli. There will be no spontaneous movement and no cerebral motor response to noxious stimuli applied to the supraorbital ridge and nail beds of all four extremities.
4 Page 4 of 10 Purely spinal reflexes, such as the deep tendon reflexes and the triple flexion response may be maintained. Decorticate or decerebrate posturing, indicative of diencephalic and/or brain stem function exclude the patient from a declaration of brain death. The following clinical observations are compatible with the diagnosis of brain death and should not be misinterpreted as evidence for brain stem function: Spontaneous movements of limbs due to spinal reflexes Respiratory-like movements (shoulder elevation and adduction, back arching, intercostals expansion without significant tidal volumes); Sweating, blushing, tachycardia Normal blood pressure without pharmacologic support or sudden increases in blood pressure Absence of diabetes insipidus Deep tendon reflexes; superficial abdominal reflexes; triple flexion response Babinski reflex b. BRAIN STEM FUNCTIONS ARE ABSENT: Pupillary light, corneal, oculocephalic, oculovestibular, oropharyngeal and respiratory (apnea) reflexes should be tested. When any one of these reflexes (excluding oculocephalic) cannot be adequately assessed, because of anatomical deformity or cardio/respiratory instability, a confirmatory test is required. The reason for the inability to perform any portion of the exam must be documented on the progress note form. i) Pupils The pupils will be fixed and greater than or equal to 4mm in diameter and will not respond to sharp changes of light intensity. A magnifying glass may be useful if response is uncertain. Both direct and consensual pupillary response will be absent. Mydriatic agents can confound the pupillary exam. If there is a possibility of pupillary effect by prior mydriatic agent administration, then a confirmatory test must be obtained. ii) Corneal Reflex The corneal reflexes will be absent. The eyes will be checked for both direct and consensual blink responses. An effort will be made to ascertain the patient s status as either a contact wearer or the recipient of previous eye surgery, which might blunt the response to the corneal reflex test. If known or suspected corneal abnormalities would preclude proper exam, then the criteria for confirmatory testing would apply. iii) Oropharyngeal (Bulbar) Reflex No cough, gag or response to endotracheal suctioning will be present. Page 5 of 10
5 iv) Oculocephalic Reflex The response to the oculocephalic (doll s eyes) maneuver is absent. This test will be done only after suitable x-ray examination of the cervical spine in the injured patient indicates no apparent fracture(s) or instability. The test is performed by observing the eyes while quickly turning the head to both sides. The absence of the oculocephalic reflex will be indicated by the eyes remaining in a fixed position with head movement. v) Oculovestibular Reflex Oculovestibular (caloric) response will not be present. The procedure will be to place the patient s head of bed at 30 degrees and to instill 50cc ice water in the ear after otoscopic inspection has insured that the external auditory canal is patent, that the stimulus can reach the tympanum, and that the tympanum is intact. The test will be performed on both sides with the lapse of at least 5 minutes between the deliveries of stimuli. Conjugate eye deviation towards the stimulus during at least a minute of observation should not be present. vi) Apnea Test Spontaneous respiration will be absent. The procedure for documenting apnea in the patient will be performed by the physicians and Respiratory Care Practitioner as follows: Patient s body temperature should be greater than or equal to 36.5 o C (97 o F) and serum potassium within normal limits. Draw an arterial blood sample to ensure that PaCO2 is between 3250mmHg and that the ph is between If the blood gas shows that these values are not within these ranges, make necessary ventilator adjustments and/or administer NaHCO3 and repeat arterial blood gas sample. The Respiratory Care Practitioner will set up the equipment and calculate the goal EtCO2 per the Apnea Test Procedure outlined in the Respiratory Care Department Procedure Manual. When the above conditions have been met, begin the flow of Carbogen (3% CO2 and 97% O2), adjust the ventilator to SIMV mode with a rate of 4 breaths per minute, the sensitivity on the ventilator to Psens of 2 or greater and a pressure support of 5 cmh2o or greater to aid in the detection of spontaneous respiratory efforts. Monitor the increase in EtCO2 while observing the patient and ventilator screen for spontaneous respiratory efforts. The IMV rate may be decreased gradually by 1 breath/minute if the EtCO2 has not increased incrementally or is not likely to reach the calculated EtCO2 goal within 10 minutes. Draw an arterial blood sample when the calculated target EtCO2 is reached. Return the patient to previous ventilator settings and discontinue the flow of Carbogen.
6 Page 6 of 10 The Apnea Test is terminated: 1. When the EtCO2 goal is reached and the arterial blood gas is drawn; 2. If there is a significant change in heart rate, blood pressure, cardiac rhythm or O2 saturation, indicating an unstable or critical situation. An arterial blood gas should be drawn prior to returning the patient to the previous ventilator settings. Confirmation of Apnea: If the pco2 is greater than or equal to 60mmHg or there is an increase of 20mmHg or greater in the normal baseline pco2 and there were no spontaneous respiratory efforts detected by the observers or mechanical ventilator, apnea is confirmed. 2. IRREVERSIBILITY IS RECOGNIZED WHEN EVALUATION DISCLOSES FINDINGS OF 2a AND 2b AND 2c: A. THE CAUSE OF COMA IS ESTABLISHED AND IS SUFFICIENT TO ACCOUNT FOR THE LOSS OF BRAIN FUNCTIONS AND Most difficulties with the determination of death on the basis of neurologic criteria have resulted from inadequate attention to this basic diagnostic prerequisite. In addition to a careful clinical examination and investigation of history, relevant knowledge of causation may be acquired by computed tomographic scan, measurement of core temperature, drug screening, EEG, angiography, or other procedures. B. THE POSSIBILITY OF RECOVERY OF ANY BRAIN FUNCTIONS IS EXCLUDED, AND The most important reversible conditions are sedation, hypothermia, neuromuscular blockade and shock (vide infra). A determination that blood flow to the brain is absent can be used to demonstrate a sufficient and irreversible condition. C. THE CESSATION OF BRAIN FUNCTIONS PERSISTS FOR A MINIMUM OF 1 TO 3 HOURS OF OBSERVATION WITH OR WITHOUT A TRIAL OF THERAPY. Even when coma is known to have started at an earlier time, the absence of brain functions must be established at the initiation of the observation period (See B: Timing of Examination) 3. Confirmatory tests include (in decreasing order of sensitivity): cerebral angiogram, electroencephalography, transcranial Doppler ultrasonography (TCD) and radionuclide brain flow study. Page 7 of 10
7 Tests of Blood Flow Complete cessation of circulation to the normothermic adult brain for more than 10 minutes is incompatible with survival of brain tissue. Documentation of this circulatory failure is therefore evidence of death of the entire brain. Four-vessel intracranial angiography is confirmatory for diagnosing cessation of circulation to the entire brain (both cerebrum and posterior fossa) but entails substantial practical difficulties and risks. Tests are available that assess circulation only in the cerebral hemispheres, namely radioisotope cerebral angiography. Without complicating conditions, absent cerebral blood flow as measured by these tests, in conjunction with the clinical determination of cessation of all brain function is diagnostic of death. For TCD s, one of two patterns must be observed: a) absence of diastolic flows or reverberating flow indicating high vascular resistance associated with greatly increased intracranial pressure; b) small systolic peaks in early systole. Lack of TCD signal cannot be interpreted as confirmatory of brain death as 10% of patient may not have temporal insonation windows. Test of Electrical Activity Electrocerebral silence verified irreversible loss of cortical functions, except in patients with drug intoxication or hypothermia. (Important technical details are provided in, American Electroencephalographic Society, Guidelines in EEG 1980, section 4: Minimum Technical Standards for EEG Recording in Suspected Cerebral Death, pp.19-24, Atlanta, 1980). When joined with the clinical findings of absent brain stem functions, electrocerebral silence confirms the diagnosis. The absence of evoked potentials is not a criterion of brain death. The examiner may elect to use short latency evoked potentials to ascertain that brain activity is present. 4. Complicating Conditions Drug and Metabolic Intoxication Drug intoxication is the most serious problem in the determination of death, especially when multiple drugs are used. Cessation of brain functions caused by sedative and anesthetic drugs, such as barbiturates, benzodiazepines, meprobamate, methaqualone, and trichloroethylene, may be completely reversible even though they produce clinical cessation of brain functions and electrocerebral silence. The presence of a supratherapeutic CNS-depressant drug effect should be excluded by history, drug screen, calculation of clearance using 5 times the drug s half-life (assuming normal hepatic and renal function), or, if available, drug plasma levels within or below the therapeutic range. If the particular drug is not known but high suspicion persists, the patient should be observed for 48-hours to determine whether a change in brain stem reflexes occurs;
8 Page 8 of 10 if no change is observed, a confirmatory test should be performed. A period of observation Longer than 48-hours may be necessary if renal or hepatic function is severely impaired. Prior use of hypothermia may also delay drug metabolism. The legal alcohol limit for driving (blood alcohol content 0.08%) is a practical threshold below which an examination to determine brain death could reasonably proceed. Toxicology consult service is available if there are questions regarding intoxicants. Total paralysis may cause unresponsiveness, areflexia, and apnea that closely simulate death. Exposure to drugs such as neuromuscular blocking agents or aminoglycoside antibiotics, and diseases like myasthenia gravis are usually apparent by careful review of the history. Prolonged paralysis after use of succinylcholine chloride and related drugs requires evaluation for pseudocolinesterase deficiency. If there is any question, low-dose atropine stimulation, electromyogram, peripheral nerve stimulation, EEG, tests of intracranial circulation, or extended observation, as indicated, will make the diagnosis clear. In drug-induced coma, EEG activity may return or persist while the patient remains unresponsive, and therefore the EEG may be an important evaluation along with extended observation. If barbiturates are used to control intracranial pressure, and, in the event that the barbiturate level can be documented to be less than or equal to 10mg/mL, the above guidelines may be used to establish brain death on a clinical basis. Barbiturate level of greater than 10mg/mL precludes the declaration of brain death. Some severe illnesses (e.g. hepatic encephalopathy, hyperosmolar coma, and preterminal uremia) can cause deep coma. Before irreversible cessation of brain functions can be determined, clinically relevant severe metabolic abnormalities (serum chemistry, acid-base, endocrine) should be considered and, if possible, corrected. Confirmatory tests or circulation or EEG may be necessary. Hypothermia Criteria for reliable recognition of death are not available in the presence of hypothermia (below 32oC core temperature [90oF]). However, minimal body temperature required for the apnea test procedure is 36.5oC (97oF). The patient may need to be warmed to achieve this temperature in order to perform the apnea test. The variables of cerebral circulation in hypothermic patients are not sufficiently well studied to know whether tests of absent or diminished circulation are confirmatory.
9 Page 9 of 10 Hypothermia can mimic brain death by ordinary clinical criteria and can protect against neurologic damage due to hypoxia. Further complications arise since hypothermia also usually precedes and follows death. If these complicating factors make it unclear whether an individual is alive, the only available measure to resolve this issue is to restore normothermia. Hypothermia is not a common cause of difficulty in the determination of death. Shock Physician should also be particularly cautious in applying neurologic criteria to determine death in patients in shock because the reduction in cerebral circulation can render clinical examination and laboratory tests unreliable. The systolic blood pressure shall be 100mmHg or greater or the mean arterial blood pressure shall be 60mmHg or greater; pressure less than this level shall be indicative of shock and should be treated prior to initiating testing for brain death. Key Words Search: Brain Death, Apnea Test Reference: Wijdicks FM et al. Evidence-based guideline update: Determining brain death in adults: Report of the Quality Standards Subcommittee of the American Academy of Neurology. Neurology 2010; 74:
10
Hospital of the University of Pennsylvania POLICY MANUAL
 Page 1 of 8 KEY WORDS: Brain Death Coma # 1-6-11 Procedures Following Patient Death # 1-6-13 Organ Donation and Anatomical Donation and Pennsylvania s Anatomical Gift Act #1-6-17 Withholding and Withdrawing
Page 1 of 8 KEY WORDS: Brain Death Coma # 1-6-11 Procedures Following Patient Death # 1-6-13 Organ Donation and Anatomical Donation and Pennsylvania s Anatomical Gift Act #1-6-17 Withholding and Withdrawing
DETERMINATION OF NEUROLOGIC DEATH IN ADULTS AND CHILDREN April 2010
 Chicago, Illinois PAGE: 1 of 7 DETERMINATION OF NEUROLOGIC DEATH IN ADULTS AND CHILDREN April 2010 Key Content Expert: Medical Center Ethics Committee in consultation with Chiefs of Service for Neurology
Chicago, Illinois PAGE: 1 of 7 DETERMINATION OF NEUROLOGIC DEATH IN ADULTS AND CHILDREN April 2010 Key Content Expert: Medical Center Ethics Committee in consultation with Chiefs of Service for Neurology
GUIDELINES: The following guidelines for determining brain death in adults are accepted practice parameters of the American Academy of Neurology 1
 Page 1 of 5 PURPOSE: The purpose of this policy is to provide licensed staff and medical personnel with a guideline to determine when a patient on a ventilator demonstrates clinical brain death. POLICY
Page 1 of 5 PURPOSE: The purpose of this policy is to provide licensed staff and medical personnel with a guideline to determine when a patient on a ventilator demonstrates clinical brain death. POLICY
YALE-NEW HAVEN HOSPITAL CLINICAL ADMINISTRATIVE POLICY & PROCEDURE MANUAL
 YALE-NEW HAVEN HOSPITAL CLINICAL ADMINISTRATIVE POLICY & PROCEDURE MANUAL Administrative Policy Title: Brain Death, Guidelines Determination of Death by Neurological Criteria in the Pediatric Patient Manual
YALE-NEW HAVEN HOSPITAL CLINICAL ADMINISTRATIVE POLICY & PROCEDURE MANUAL Administrative Policy Title: Brain Death, Guidelines Determination of Death by Neurological Criteria in the Pediatric Patient Manual
Sample Guidelines for the Determination of Death: Including Death by Neurologic Criteria
 Sample Guidelines for the Determination of Death: Including Death by Neurologic Criteria A. SUBJECT: Guidelines for the Determination of Death: Including Death by Neurologic Criteria B. POLICY: The Medical
Sample Guidelines for the Determination of Death: Including Death by Neurologic Criteria A. SUBJECT: Guidelines for the Determination of Death: Including Death by Neurologic Criteria B. POLICY: The Medical
Determination of Death
 Policy Legal Standard UTMB physicians will determine death in accordance with this policy which is based on Texas law and the practice parameters recommended by the American Academy of Neurology for adults
Policy Legal Standard UTMB physicians will determine death in accordance with this policy which is based on Texas law and the practice parameters recommended by the American Academy of Neurology for adults
Brain Death Determination: Outline. Definition. Brain Death Determination. Brain Death Determination. No conflict of interest
 No conflict of interest : Outline Definition Definition Confounding factors Clinical examination Apnea test Confirmatory testing Communicating the diagnosis Ethical issues Brain death remains the preferred
No conflict of interest : Outline Definition Definition Confounding factors Clinical examination Apnea test Confirmatory testing Communicating the diagnosis Ethical issues Brain death remains the preferred
Policy No: Title: Determination of Death by Brain Criteria Department: PATIENT CARE. Originated: May 1992
 Title: Determination of Death by Brain Criteria Department: PATIENT CARE Policy No: Page 1 of 6 Revised: April 2009 Previous revisions: 9/96, 7/99, 7/07 Reviewed: August 2010 Originated: May 1992 I. POLICY:
Title: Determination of Death by Brain Criteria Department: PATIENT CARE Policy No: Page 1 of 6 Revised: April 2009 Previous revisions: 9/96, 7/99, 7/07 Reviewed: August 2010 Originated: May 1992 I. POLICY:
Neurological Determination of Death Adult
 Approved by: Vice President and Chief Medical Officer Neurological Determination of Death Adult Corporate Policy & Procedures Manual Number: VII-B-400 Date Approved June 9, 2015 Next Review (3 years from
Approved by: Vice President and Chief Medical Officer Neurological Determination of Death Adult Corporate Policy & Procedures Manual Number: VII-B-400 Date Approved June 9, 2015 Next Review (3 years from
Name Signature Date IRB & Ethics Committee Dr. Ejaz A. Khan Chairman IRB & EC Dr. Shoukat Matabddin
 Prepared by Reviewed By Name Signature Date IRB & Ethics Committee Dr. Ejaz A. Khan Chairman IRB & EC Dr. Shoukat Matabddin Dr. M. Salim Khan Medical Director Approved by Dr. Manzoor H Qazi Chief Executive
Prepared by Reviewed By Name Signature Date IRB & Ethics Committee Dr. Ejaz A. Khan Chairman IRB & EC Dr. Shoukat Matabddin Dr. M. Salim Khan Medical Director Approved by Dr. Manzoor H Qazi Chief Executive
PROPOSED REVISIONS OF ISMA BRAIN DEATH GUIDELINES
 RESOLUTION 17-04 Introduced by: Action: PROPOSED REVISIONS OF ISMA BRAIN DEATH GUIDELINES Emil Weber, MD Adopted as Amended RESOLVED, that ISMA adopt updated brain death guidelines for adults and children,
RESOLUTION 17-04 Introduced by: Action: PROPOSED REVISIONS OF ISMA BRAIN DEATH GUIDELINES Emil Weber, MD Adopted as Amended RESOLVED, that ISMA adopt updated brain death guidelines for adults and children,
The Determination of Brain Death. James Zisfein, M.D. Chief, Division of Neurology Lincoln Medical Center, Bronx, NY
 The Determination of Brain Death James Zisfein, M.D. Chief, Division of Neurology Lincoln Medical Center, Bronx, NY James.Zisfein@nychhc.org The early history of brain death Until recently, death was determined
The Determination of Brain Death James Zisfein, M.D. Chief, Division of Neurology Lincoln Medical Center, Bronx, NY James.Zisfein@nychhc.org The early history of brain death Until recently, death was determined
Declaring Brain Death. Ali Salim, MD Professor of Surgery Chief, Division of Trauma, Burns, Surgical Critical Care, and Emergency General Surgery
 Declaring Brain Death Ali Salim, MD Professor of Surgery Chief, Division of Trauma, Burns, Surgical Critical Care, and Emergency General Surgery Disclosures I have nothing to disclose Why should we know
Declaring Brain Death Ali Salim, MD Professor of Surgery Chief, Division of Trauma, Burns, Surgical Critical Care, and Emergency General Surgery Disclosures I have nothing to disclose Why should we know
Brain Death Its History (and Some Controversies ) Eelco F.M. Wijdicks, MD, PhD Division of Critical Care Neurology Mayo College of Medicine
 Eelco F.M. Wijdicks, MD, PhD Division of Critical Care Neurology Mayo College of Medicine") Brain Death Its History (and Some Controversies ) Eelco F.M. Wijdicks, MD, PhD Division of Critical Care Neurology Mayo College of Medicine 2016 MFMER 3583421-1 Brain Death or 2016 MFMER 3583421-2 Where
Brain Death Its History (and Some Controversies ) Eelco F.M. Wijdicks, MD, PhD Division of Critical Care Neurology Mayo College of Medicine 2016 MFMER 3583421-1 Brain Death or 2016 MFMER 3583421-2 Where
Last printed 9/15/2016 9:51 AM. Departmental/Patient Care Page 1 of 6. Origination Date: 6/18/2014. Grady Memorial Hospital Brain Death Policy
 Last printed 9/15/2016 9:51 AM Departmental/Patient Care Page 1 of 6 Grady Memorial Hospital Brain Death Policy Origination Date: 6/18/2014 Revision Date: 2/2/2015 I. POLICY STATEMENT: Mission statement:
Last printed 9/15/2016 9:51 AM Departmental/Patient Care Page 1 of 6 Grady Memorial Hospital Brain Death Policy Origination Date: 6/18/2014 Revision Date: 2/2/2015 I. POLICY STATEMENT: Mission statement:
Clinical Report Guidelines for the Determination of Brain Death in Infants and Children: An Update of the 1987 Task Force Recommendations
 Guidance for the Clinician in Rendering Pediatric Care Clinical Report Guidelines for the Determination of Brain Death in Infants and Children: An Update of the 1987 Task Force Recommendations abstract
Guidance for the Clinician in Rendering Pediatric Care Clinical Report Guidelines for the Determination of Brain Death in Infants and Children: An Update of the 1987 Task Force Recommendations abstract
Ethical Challenges With Documenting Brain Death
 Ethical Challenges With Documenting Brain Death William Reitsma, BSN, CPTC Consultant AOPO Accreditation Surveyor 2015 Doug Miller Symposium Wisconsin Dells, Wisconsin When are You Dead? History of Brain
Ethical Challenges With Documenting Brain Death William Reitsma, BSN, CPTC Consultant AOPO Accreditation Surveyor 2015 Doug Miller Symposium Wisconsin Dells, Wisconsin When are You Dead? History of Brain
NEW YORK CITY HEALTH AND HOSPITALS CORPORATION CORPORATE BRAIN DEATH POLICY
 NEW YORK CITY HEALTH AND HOSPITALS CORPORATION CORPORATE BRAIN DEATH POLICY PURPOSE: To describe the guidelines, procedure, and documentation requirements for: Initiation of a brain death evaluation, Determination
NEW YORK CITY HEALTH AND HOSPITALS CORPORATION CORPORATE BRAIN DEATH POLICY PURPOSE: To describe the guidelines, procedure, and documentation requirements for: Initiation of a brain death evaluation, Determination
CLINICAL GUIDELINE Pages 5 NTC Policy #4
 I. PURPOSE: To provide guidelines for the recording of Electrocerebral Silence Electroencephalography in accordance with the American Clinical Neurophysiology Society (ACNS) guidelines. To provide supportive
I. PURPOSE: To provide guidelines for the recording of Electrocerebral Silence Electroencephalography in accordance with the American Clinical Neurophysiology Society (ACNS) guidelines. To provide supportive
Diagnosis and Declaration of Death: A Dilemma
 Review Article Print ISSN: 2321-6379 Online ISSN: 2321-595X DOI: 10.17354/ijss/2016/392 Diagnosis and Declaration of Death: A Dilemma Niranjan Kumar Verma 1, Ashutosh Ranjan 2, Alok Kumar Singh 3 1 Professor
Review Article Print ISSN: 2321-6379 Online ISSN: 2321-595X DOI: 10.17354/ijss/2016/392 Diagnosis and Declaration of Death: A Dilemma Niranjan Kumar Verma 1, Ashutosh Ranjan 2, Alok Kumar Singh 3 1 Professor
Brain Death Examination Importance and Pitfalls. Dr. Reshi Professor of Neurology/Neurosurgery University of Minnesota
 Brain Death Examination Importance and Pitfalls Dr. Reshi Professor of Neurology/Neurosurgery University of Minnesota Conflict No Conflicts to report Will not discuss off label use of any medication. Presentation
Brain Death Examination Importance and Pitfalls Dr. Reshi Professor of Neurology/Neurosurgery University of Minnesota Conflict No Conflicts to report Will not discuss off label use of any medication. Presentation
GUIDELINE for the diagnosis and confirmation of death within Adult Critical Care
 Guideline for the diagnosis and confirmation of death within adult critical care 1. Introduction Death occurs when there is permanent loss of capacity for consciousness and loss of all brainstem functions.
Guideline for the diagnosis and confirmation of death within adult critical care 1. Introduction Death occurs when there is permanent loss of capacity for consciousness and loss of all brainstem functions.
Ancillary Testing in Death
 Ancillary Testing in Death MICHAËL CHASSÉ, MD, PHD, FRCPC ASSISTANT PROFESSOR, DEPARTMENT OF ANESTHESIOLOGY AND CRITICAL CARE, UNIVERSITÉ LAVAL INTENSIVIST, DEPARTMENT OF ANESTHESIOLOGY, DIVISION OF CRITICAL
Ancillary Testing in Death MICHAËL CHASSÉ, MD, PHD, FRCPC ASSISTANT PROFESSOR, DEPARTMENT OF ANESTHESIOLOGY AND CRITICAL CARE, UNIVERSITÉ LAVAL INTENSIVIST, DEPARTMENT OF ANESTHESIOLOGY, DIVISION OF CRITICAL
Alex Manara Regional Clinical Lead in Organ Donation South West Region Frenchay Hospital, Bristol
 Alex Manara Regional Clinical Lead in Organ Donation South West Region Frenchay Hospital, Bristol Diagnosis of Death Masterclass 2. Increased diagnosis of brain stem death 3. Increased donation after cardiac
Alex Manara Regional Clinical Lead in Organ Donation South West Region Frenchay Hospital, Bristol Diagnosis of Death Masterclass 2. Increased diagnosis of brain stem death 3. Increased donation after cardiac
Babak Tamizi Far MD. Assistant professor of internal medicine Al-zahra hospital, Isfahan university of medical sciences
 Babak Tamizi Far MD. Assistant professor of internal medicine Al-zahra hospital, Isfahan university of medical sciences ٢ Level of consciousness is depressed Stuporous patients respond only to repeated
Babak Tamizi Far MD. Assistant professor of internal medicine Al-zahra hospital, Isfahan university of medical sciences ٢ Level of consciousness is depressed Stuporous patients respond only to repeated
Experiences as a Donation Support Physician. Dead or not Dead? Are the following statements consistent with neurological
 Experiences as a Donation Support Physician Dead or not Dead? Are the following statements consistent with neurological determination of death (dead)? or not (not dead)? With thanks to Drs. Alex Manara,
Experiences as a Donation Support Physician Dead or not Dead? Are the following statements consistent with neurological determination of death (dead)? or not (not dead)? With thanks to Drs. Alex Manara,
BRAIN DEATH S34 (1) Brain Death
 Brain Death") BRAIN DEATH S34 (1) Brain Death Last updated: September 5, 2017 CRITERIA FOR BRAIN DEATH... 1 APNEA TEST (S. APNEA CHALLENGE)... 4 ANCILLARY STUDIES... 5 CARE OF ORGAN DONOR... 7 ORGAN DONATION AFTER CARDIAC
BRAIN DEATH S34 (1) Brain Death Last updated: September 5, 2017 CRITERIA FOR BRAIN DEATH... 1 APNEA TEST (S. APNEA CHALLENGE)... 4 ANCILLARY STUDIES... 5 CARE OF ORGAN DONOR... 7 ORGAN DONATION AFTER CARDIAC
PRACTICE GUIDELINE. DEFINITIONS: Mild head injury: Glasgow Coma Scale* (GCS) score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8
 score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8") PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
뇌사의진단과진단을위한보조적검사 서울아산병원신경과. The Diagnosis and Ancillary Tests of Brain Death. Kim, Cheon-Sik
 대한임상검사학회지 : 36 권제 1 호, 64-68, 2004 뇌사의진단과진단을위한보조적검사 김천식 The Diagnosis and Ancillary Tests of Brain Death Kim, Cheon-Sik Department of Clinical Neurosciences, Asan Medical Center Brain death is defined
대한임상검사학회지 : 36 권제 1 호, 64-68, 2004 뇌사의진단과진단을위한보조적검사 김천식 The Diagnosis and Ancillary Tests of Brain Death Kim, Cheon-Sik Department of Clinical Neurosciences, Asan Medical Center Brain death is defined
Med 536 Communicating About Prognosis Workshop. Case 2
 Med 536 Communicating About Prognosis Workshop Case 2 ID / CC: 33 year-old man with intracranial hemorrhage History of the Presenting Illness 33 year-old man with a prior history of melanoma of the neck
Med 536 Communicating About Prognosis Workshop Case 2 ID / CC: 33 year-old man with intracranial hemorrhage History of the Presenting Illness 33 year-old man with a prior history of melanoma of the neck
Take A Breath: Pulmonary Management of the Organ Donor. Whitni Noyes, RN, CPTC Midwest Transplant Network
 Take A Breath: Pulmonary Management of the Organ Donor Whitni Noyes, RN, CPTC Midwest Transplant Network Objectives Recognize MTN referral criteria. Be familiar with the apnea test for brain death pronouncement.
Take A Breath: Pulmonary Management of the Organ Donor Whitni Noyes, RN, CPTC Midwest Transplant Network Objectives Recognize MTN referral criteria. Be familiar with the apnea test for brain death pronouncement.
Practice variability in brain death determination A call to action
 Practice variability in brain death determination A call to action Claire N. Shappell, BA Jeffrey I. Frank, MD Khalil Husari, MD Matthew Sanchez, BS Fernando Goldenberg, MD Agnieszka Ardelt, MD, PhD Correspondence
Practice variability in brain death determination A call to action Claire N. Shappell, BA Jeffrey I. Frank, MD Khalil Husari, MD Matthew Sanchez, BS Fernando Goldenberg, MD Agnieszka Ardelt, MD, PhD Correspondence
BRAIN DEATH. Frequently Asked Questions 04for the General Public
 BRAIN DEATH Frequently Asked Questions 04for the General Public Neurocritical Care Society BRAIN DEATH FAQ s FOR THE GENERAL PUBLIC NEUROCRITICAL CARE SOCIETY 1. Q: Why was this FAQ created? A: Several
BRAIN DEATH Frequently Asked Questions 04for the General Public Neurocritical Care Society BRAIN DEATH FAQ s FOR THE GENERAL PUBLIC NEUROCRITICAL CARE SOCIETY 1. Q: Why was this FAQ created? A: Several
Committee on Organ Donor Intervention Research
 National Academics of Science, Engineering, Medicine Committee on Organ Donor Intervention Research Galen V. Henderson, MD Director, Neurocritical Care Brigham and Women s Hospital Harvard Medical School
National Academics of Science, Engineering, Medicine Committee on Organ Donor Intervention Research Galen V. Henderson, MD Director, Neurocritical Care Brigham and Women s Hospital Harvard Medical School
TCD evaluation is used in several countries as a confirmatory test to assess CBF arrest
 ! BRAIN DEATH IS THE IRREVERSIBLE LOSS OF FUNCTION OF THE ENTIRE BRAIN INCLUDING THE BRAIN STEM Conventional Confirmatory Tests: EEG, CEREBRAL AGF, BRAIN SCINTIGRAPHY LOGISTICAL PROBLEMS TCD evaluation
! BRAIN DEATH IS THE IRREVERSIBLE LOSS OF FUNCTION OF THE ENTIRE BRAIN INCLUDING THE BRAIN STEM Conventional Confirmatory Tests: EEG, CEREBRAL AGF, BRAIN SCINTIGRAPHY LOGISTICAL PROBLEMS TCD evaluation
Neurologic Determination of Death. Ian Ball FRCPC Regional Medical Lead for Organ Donation October 26, 2015
 Neurologic Determination of Death Ian Ball FRCPC Regional Medical Lead for Organ Donation October 26, 2015 Format Definition of Brain Death Historical Perspectives International consistency / inconsistency
Neurologic Determination of Death Ian Ball FRCPC Regional Medical Lead for Organ Donation October 26, 2015 Format Definition of Brain Death Historical Perspectives International consistency / inconsistency
Brain Death* CARY SUTER, M.D.
 Brain Death* CARY SUTER, M.D. Professor and Chairman, Department of Neurology, Medical College of Virginia, Health Sciences Division of Virginia Commonwealth University, Richmond, Virginia Until recently
Brain Death* CARY SUTER, M.D. Professor and Chairman, Department of Neurology, Medical College of Virginia, Health Sciences Division of Virginia Commonwealth University, Richmond, Virginia Until recently
UNIVERSITY OF TENNESSEE HOSPITAL 1924 Alcoa Highway * Knoxville, TN (865) LABEL
 LABEL") 1003 UNIVERSITY OF TENNESSEE HOSPITAL 1924 Alcoa Highway * Knoxville, TN 37920 (865) 544-9000 LABEL Knoxville Neurology Clinic Orders and Progress tes : NAME: MED REC#: PHYSICIAN: DATE: DATE PHYSICIAN'S
1003 UNIVERSITY OF TENNESSEE HOSPITAL 1924 Alcoa Highway * Knoxville, TN 37920 (865) 544-9000 LABEL Knoxville Neurology Clinic Orders and Progress tes : NAME: MED REC#: PHYSICIAN: DATE: DATE PHYSICIAN'S
Post Cardiac Arrest Care 2015 American Heart Association Guideline Update for CPR and Emergency Cardiovascular Care
 Post Cardiac Arrest Care 2015 American Heart Association Guideline Update for CPR and Emergency Cardiovascular Care รศ.ดร.พญ.ต นหยง พ พานเมฆาภรณ ภาคว ชาว ส ญญ ว ทยา คณะแพทยศาสตร มหาว ทยาล ยเช ยงใหม System
Post Cardiac Arrest Care 2015 American Heart Association Guideline Update for CPR and Emergency Cardiovascular Care รศ.ดร.พญ.ต นหยง พ พานเมฆาภรณ ภาคว ชาว ส ญญ ว ทยา คณะแพทยศาสตร มหาว ทยาล ยเช ยงใหม System
Deceased donor. Solid organ transplantation
 Deceased donor Solid organ transplantation Deceased donor donation process 1. Potential donor detection 2. Brain death diagnosis 3. Donor management 4. Organ allocation 5. Organ retrieval Brain death Irreversible
Deceased donor Solid organ transplantation Deceased donor donation process 1. Potential donor detection 2. Brain death diagnosis 3. Donor management 4. Organ allocation 5. Organ retrieval Brain death Irreversible
Bilaga 4 till rapport 1 (17)
") Bilaga 4 Tabeller, beskrivning av studier Bilaga 4 till rapport 1 (17) Bilddiagnostik vid misstanke om total hjärninfarkt en systematisk litteraturöversikt, rapport 282 (2018) SBU Statens beredning för
Bilaga 4 Tabeller, beskrivning av studier Bilaga 4 till rapport 1 (17) Bilddiagnostik vid misstanke om total hjärninfarkt en systematisk litteraturöversikt, rapport 282 (2018) SBU Statens beredning för
Legal Determination of Brain Death
 Research and Reviews Legal Determination of Brain Death JMAJ 54(6): 363 367, 2011 Yoshihiro NATORI* 1 Abstract Revisions to the Organ Transplant Act have made it possible for the organs of a brain-dead
Research and Reviews Legal Determination of Brain Death JMAJ 54(6): 363 367, 2011 Yoshihiro NATORI* 1 Abstract Revisions to the Organ Transplant Act have made it possible for the organs of a brain-dead
Michigan Pediatric Cardiac Protocols. Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS
 Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS Pediatric Asystole Section 4-1 Pediatric Bradycardia Section 4-2 Pediatric Cardiac Arrest General Section 4-3 Pediatric Narrow Complex Tachycardia
Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS Pediatric Asystole Section 4-1 Pediatric Bradycardia Section 4-2 Pediatric Cardiac Arrest General Section 4-3 Pediatric Narrow Complex Tachycardia
Variability of brain death determination guidelines in leading US neurologic institutions
 Variability of brain death determination guidelines in leading US neurologic institutions David M. Greer, MD, MA Panayiotis N. Varelas, MD, PhD Shamael Haque, DO, MPH Eelco F.M. Wijdicks, MD, PhD Address
Variability of brain death determination guidelines in leading US neurologic institutions David M. Greer, MD, MA Panayiotis N. Varelas, MD, PhD Shamael Haque, DO, MPH Eelco F.M. Wijdicks, MD, PhD Address
Neurocritical Care Basics. Tapan Kavi, MD Christina Fox, RN
 Neurocritical Care Basics Tapan Kavi, MD Christina Fox, RN GOAL 1: DON T LET THE PATIENT DIE Not unique ACLS, ATLS, ENLS, other strategies common to all emergency medical care ABCs MORE not less important
Neurocritical Care Basics Tapan Kavi, MD Christina Fox, RN GOAL 1: DON T LET THE PATIENT DIE Not unique ACLS, ATLS, ENLS, other strategies common to all emergency medical care ABCs MORE not less important
Form for the Diagnosis of Death using Neurological Criteria in Children >2 months to <18 years {full guidance version}
 This form is consistent with and should be used in conjunction with, the AoMRC (2008) A Code of Practice for the Diagnosis and Confirmation of Death 1 and has been endorsed for use by the following institutions:
This form is consistent with and should be used in conjunction with, the AoMRC (2008) A Code of Practice for the Diagnosis and Confirmation of Death 1 and has been endorsed for use by the following institutions:
Neurological Prognosis after Cardiac Arrest Guideline
 Neurological Prognosis after Cardiac Arrest Guideline I. Associated Guidelines and Appendices 1. Therapeutic Hypothermia after Cardiac Arrest 2. Hypothermia after Cardiac Arrest Algorithm II. Rationale
Neurological Prognosis after Cardiac Arrest Guideline I. Associated Guidelines and Appendices 1. Therapeutic Hypothermia after Cardiac Arrest 2. Hypothermia after Cardiac Arrest Algorithm II. Rationale
First Person Consent Uniform Anatomical Gift Act of 1968
 Andrew Wilson, Medicolegal Death Investigator Not-for-profit Organ Procurement Organization (OPO) & Tissue Recovery Agency Regulated by Centers for Medicaid and Medicare Services (CMS) and FDA Offices
Andrew Wilson, Medicolegal Death Investigator Not-for-profit Organ Procurement Organization (OPO) & Tissue Recovery Agency Regulated by Centers for Medicaid and Medicare Services (CMS) and FDA Offices
How to Diagnose Brainstem Death. Akhmad Imron Dept./SMF Bedah Saraf FK.Unpad/RSHS
 How to Diagnose Brainstem Death Akhmad Imron Dept./SMF Bedah Saraf FK.Unpad/RSHS RSUP Dr. Hasan Sadikin Bandung Jalan Pasteur No. 38 Bandung telephone.62-022-2034953/57 Fax.62-022-2032216 Diagnosis of
How to Diagnose Brainstem Death Akhmad Imron Dept./SMF Bedah Saraf FK.Unpad/RSHS RSUP Dr. Hasan Sadikin Bandung Jalan Pasteur No. 38 Bandung telephone.62-022-2034953/57 Fax.62-022-2032216 Diagnosis of
Waiting for a Kidney. Objectives
 Waiting for a Kidney Department of Urologic Sciences Grand Rounds William Gourlay Christopher Nguan April 25, 2007 Objectives 1. review the waiting times for deceased-donor kidney transplants in BC and
Waiting for a Kidney Department of Urologic Sciences Grand Rounds William Gourlay Christopher Nguan April 25, 2007 Objectives 1. review the waiting times for deceased-donor kidney transplants in BC and
Med 536 Communicating About Prognosis Workshop. Case 1
 Med 536 Communicating About Prognosis Workshop Case 1 ID / CC: 39 year-old woman status-post motor-vehicle collision History of the Presenting Illness Previously healthy 39 year-old woman was found in
Med 536 Communicating About Prognosis Workshop Case 1 ID / CC: 39 year-old woman status-post motor-vehicle collision History of the Presenting Illness Previously healthy 39 year-old woman was found in
Pronouncing brain death Contemporary practice and safety of the apnea test
 Pronouncing brain death Contemporary practice and safety of the apnea test Eelco F.M. Wijdicks, MD, PhD Alejandro A. Rabinstein, MD Edward M. Manno, MD John D. Atkinson, MD Address correspondence and reprint
Pronouncing brain death Contemporary practice and safety of the apnea test Eelco F.M. Wijdicks, MD, PhD Alejandro A. Rabinstein, MD Edward M. Manno, MD John D. Atkinson, MD Address correspondence and reprint
Hypothermia in Neonates with HIE TARA JENDZIO, DNP(C), RN, RNC-NIC
, RN, RNC-NIC") Hypothermia in Neonates with HIE TARA JENDZIO, DNP(C), RN, RNC-NIC Objectives 1. Define Hypoxic-Ischemic Encephalopathy (HIE) 2. Identify the criteria used to determine if an infant qualifies for therapeutic
Hypothermia in Neonates with HIE TARA JENDZIO, DNP(C), RN, RNC-NIC Objectives 1. Define Hypoxic-Ischemic Encephalopathy (HIE) 2. Identify the criteria used to determine if an infant qualifies for therapeutic
Brain Death and Disorders of Consciousness. John Banja, PhD Center for Ethics Emory University
 Brain Death and Disorders of Consciousness John Banja, PhD Center for Ethics Emory University jbanja@emory.edu Five kinds of catastrophic neurological injury Minimal Responsiveness Persistent Vegetative
Brain Death and Disorders of Consciousness John Banja, PhD Center for Ethics Emory University jbanja@emory.edu Five kinds of catastrophic neurological injury Minimal Responsiveness Persistent Vegetative
Ethical Dilemmas Brain Death and Overdose. Disclosures
 Ethical Dilemmas Brain Death and Overdose Ross W. Sullivan MD Director Toxicology Consultation Service Medical Toxicology Fellowship Director Assistant Professor Emergency Medicine SUNY Upstate Hospital,
Ethical Dilemmas Brain Death and Overdose Ross W. Sullivan MD Director Toxicology Consultation Service Medical Toxicology Fellowship Director Assistant Professor Emergency Medicine SUNY Upstate Hospital,
Pulse normal; brain dead
 Page 1 of 5 w w w. h a a r e t z. c o m Last update - 03:03 25/09/2007 Pulse normal; brain dead By Avinoam Reches There is no more difficult moment in medicine than when a doctor is required to inform
Page 1 of 5 w w w. h a a r e t z. c o m Last update - 03:03 25/09/2007 Pulse normal; brain dead By Avinoam Reches There is no more difficult moment in medicine than when a doctor is required to inform
Case 1. Case 5/30/2013. Traumatic Brain Injury : Review, Update, and Controversies
 Case 1 Traumatic Brain Injury : Review, Update, and Controversies Shirley I. Stiver MD, PhD 32 year old male s/p high speed MVA Difficult extrication Intubated at scene Case BP 75 systolic / palp GCS 3
Case 1 Traumatic Brain Injury : Review, Update, and Controversies Shirley I. Stiver MD, PhD 32 year old male s/p high speed MVA Difficult extrication Intubated at scene Case BP 75 systolic / palp GCS 3
IOM at University of. Training for physicians. art of IOM. neurologic. injury during surgery. surgery on by IOM. that rate is.
 Topics covered: Overview of science and art of IOM IOM at University of Michigan Hospital and Health Systems What is the purpose of Intraoperative monitoring? Training for physicians Overview of science
Topics covered: Overview of science and art of IOM IOM at University of Michigan Hospital and Health Systems What is the purpose of Intraoperative monitoring? Training for physicians Overview of science
THE ANZICS STATEMENT ON DEATH AND ORGAN DONATION
 Australian and New Zealand Intensive Care Society (ANZICS) ACN 057 619 986 THE ANZICS STATEMENT ON DEATH AND ORGAN DONATION Edition 3.2 2013 2 Australian and New Zealand Intensive Care Society 2013. ACN
Australian and New Zealand Intensive Care Society (ANZICS) ACN 057 619 986 THE ANZICS STATEMENT ON DEATH AND ORGAN DONATION Edition 3.2 2013 2 Australian and New Zealand Intensive Care Society 2013. ACN
Legal Issues at the End of Life: Who Decides?
 Legal Issues at the End of Life: Who Decides? Dan Larriviere, MD, JD University of Virginia Schools of Law and Medicine Chair, American Academy of Neurology Ethics, Law and Humanities Committee My Perspective
Legal Issues at the End of Life: Who Decides? Dan Larriviere, MD, JD University of Virginia Schools of Law and Medicine Chair, American Academy of Neurology Ethics, Law and Humanities Committee My Perspective
NEONATAL HYPOXIC-ISCHAEMIC ENCEPHALOPATHY (HIE) & COOLING THERAPY
 & COOLING THERAPY") Background NEONATAL HYPOXIC-ISCHAEMIC ENCEPHALOPATHY (HIE) & COOLING THERAPY A perinatal hypoxic-ischaemic insult may present with varying degrees of neonatal encephalopathy, neurological disorder and
Background NEONATAL HYPOXIC-ISCHAEMIC ENCEPHALOPATHY (HIE) & COOLING THERAPY A perinatal hypoxic-ischaemic insult may present with varying degrees of neonatal encephalopathy, neurological disorder and
Saving Lives & Restoring Health Through Organ and Tissue Donation On-line Module
 Saving Lives & Restoring Health Through Organ and Tissue Donation On-line Module 1 N3 Who is New Jersey Organ and Tissue Sharing Network? Organ Procurement Organization (OPO) Private, Non-profit Service
Saving Lives & Restoring Health Through Organ and Tissue Donation On-line Module 1 N3 Who is New Jersey Organ and Tissue Sharing Network? Organ Procurement Organization (OPO) Private, Non-profit Service
10. Severe traumatic brain injury also see flow chart Appendix 5
 10. Severe traumatic brain injury also see flow chart Appendix 5 Introduction Severe traumatic brain injury (TBI) is the leading cause of death in children in the UK, accounting for 15% of deaths in 1-15
10. Severe traumatic brain injury also see flow chart Appendix 5 Introduction Severe traumatic brain injury (TBI) is the leading cause of death in children in the UK, accounting for 15% of deaths in 1-15
THE ANZICS STATEMENT ON DEATH AND ORGAN DONATION
 Australian and New Zealand Intensive Care Society (ANZICS) ACN 057 619 986 THE ANZICS STATEMENT ON DEATH AND ORGAN DONATION Third Edition 2008 Australian and New Zealand Intensive Care Society 2008. ACN
Australian and New Zealand Intensive Care Society (ANZICS) ACN 057 619 986 THE ANZICS STATEMENT ON DEATH AND ORGAN DONATION Third Edition 2008 Australian and New Zealand Intensive Care Society 2008. ACN
Administrative Policies and Procedures. Originating Venue: Provision of Care, Treatment and Services Policy No.: PC 2916
 Administrative Policies and Procedures Originating Venue: Provision of Care, Treatment and Services Policy No.: PC 2916 Title: Sedation Cross Reference: Date Issued: 05/09 Date Reviewed: 04/11 Date: Revised:
Administrative Policies and Procedures Originating Venue: Provision of Care, Treatment and Services Policy No.: PC 2916 Title: Sedation Cross Reference: Date Issued: 05/09 Date Reviewed: 04/11 Date: Revised:
Pediatric emergencies (SHOCK & COMA) Dr Mubarak Abdelrahman Assistant Professor Jazan University
 Dr Mubarak Abdelrahman Assistant Professor Jazan University") Pediatric emergencies (SHOCK & COMA) Dr Mubarak Abdelrahman Assistant Professor Jazan University SHOCK Definition: Shock is a syndrome = inability to provide sufficient oxygenated blood to tissues. Oxygen
Pediatric emergencies (SHOCK & COMA) Dr Mubarak Abdelrahman Assistant Professor Jazan University SHOCK Definition: Shock is a syndrome = inability to provide sufficient oxygenated blood to tissues. Oxygen
Pediatric Advanced Life Support
 Pediatric Advanced Life Support Pediatric Chain of Survival Berg M D et al. Circulation 2010;122:S862-S875 Prevention Early cardiopulmonary resuscitation (CPR) Prompt access to the emergency response system
Pediatric Advanced Life Support Pediatric Chain of Survival Berg M D et al. Circulation 2010;122:S862-S875 Prevention Early cardiopulmonary resuscitation (CPR) Prompt access to the emergency response system
Michigan Pediatric Cardiac Protocols. Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS
 Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS Pediatric Asystole Section 4-1 Pediatric Bradycardia Section 4-2 Pediatric Cardiac Arrest General Section 4-3 Pediatric Narrow Complex Tachycardia
Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS Pediatric Asystole Section 4-1 Pediatric Bradycardia Section 4-2 Pediatric Cardiac Arrest General Section 4-3 Pediatric Narrow Complex Tachycardia
APPENDIX VI HFOV Quick Guide
 APPENDIX VI HFOV Quick Guide Overall goal: Maintain PH in the target range at the minimum tidal volume. This is achieved by favoring higher frequencies over lower P (amplitude). This goal is also promoted
APPENDIX VI HFOV Quick Guide Overall goal: Maintain PH in the target range at the minimum tidal volume. This is achieved by favoring higher frequencies over lower P (amplitude). This goal is also promoted
Addendum D. Procedural Sedation Test MERCY MEDICAL CENTER- SIOUX CITY. Procedural Sedation Questions
 Addendum D. Procedural Sedation Test MERCY MEDICAL CENTER- SIOUX CITY Procedural Sedation Questions Individuals applying for moderate sedation privileges must achieve a score of 80%. PRACTITIONER NAME
Addendum D. Procedural Sedation Test MERCY MEDICAL CENTER- SIOUX CITY Procedural Sedation Questions Individuals applying for moderate sedation privileges must achieve a score of 80%. PRACTITIONER NAME
SARASOTA MEMORIAL HOSPITAL NURSING DEPARTMENT POLICY
 PS1006 SARASOTA MEMORIAL HOSPITAL NURSING DEPARTMENT POLICY TITLE: MONITORING NEUROMUSCULAR BLOCKADE IN THE CRITICAL CARE Job Title of Reviewer: Director, ICU EFFECTIVE DATE: REVISED DATE: POLICY TYPE:
PS1006 SARASOTA MEMORIAL HOSPITAL NURSING DEPARTMENT POLICY TITLE: MONITORING NEUROMUSCULAR BLOCKADE IN THE CRITICAL CARE Job Title of Reviewer: Director, ICU EFFECTIVE DATE: REVISED DATE: POLICY TYPE:
The NJ Sharing Network Organ and Tissue Donation as an End of Life option for Families
 The NJ Sharing Network Organ and Tissue Donation as an End of Life option for Families NJ Sharing Network Private non-profit service organization Federal designation to provide recovery services State
The NJ Sharing Network Organ and Tissue Donation as an End of Life option for Families NJ Sharing Network Private non-profit service organization Federal designation to provide recovery services State
Basic Standards for Fellowship Training in Sleep Medicine
 Basic Standards for Fellowship Training in Sleep Medicine American Osteopathic Association and American College of Osteopathic Neurologists and Psychiatrists and American College of Osteopathic Internists
Basic Standards for Fellowship Training in Sleep Medicine American Osteopathic Association and American College of Osteopathic Neurologists and Psychiatrists and American College of Osteopathic Internists
LOSS OF CONSCIOUSNESS & ASSESSMENT. Sheba Medical Center Acute Medicine Department MATTHEW WRIGHT
 LOSS OF CONSCIOUSNESS & ASSESSMENT Sheba Medical Center Acute Medicine Department MATTHEW WRIGHT OUTLINE Causes Head Injury Clinical Features Complications Rapid Assessment Glasgow Coma Scale Classification
LOSS OF CONSCIOUSNESS & ASSESSMENT Sheba Medical Center Acute Medicine Department MATTHEW WRIGHT OUTLINE Causes Head Injury Clinical Features Complications Rapid Assessment Glasgow Coma Scale Classification
Bilaga 3 till rapport 1 (5)
") Bilaga 3 till rapport 1 (5) som stöd för diagnosen total hjärninfarkt hos barn yngre än två år en systematisk litteraturöversikt, rapport 290 (2018) Bilaga 3 Tabell, beskrivning av studier SBU Statens
Bilaga 3 till rapport 1 (5) som stöd för diagnosen total hjärninfarkt hos barn yngre än två år en systematisk litteraturöversikt, rapport 290 (2018) Bilaga 3 Tabell, beskrivning av studier SBU Statens
Pediatric Cardiac Arrest General
 Date: November 15, 2012 Page 1 of 5 Pediatric Cardiac Arrest General This protocol should be followed for all pediatric cardiac arrests. If an arrest is of a known traumatic origin refer to the Dead on
Date: November 15, 2012 Page 1 of 5 Pediatric Cardiac Arrest General This protocol should be followed for all pediatric cardiac arrests. If an arrest is of a known traumatic origin refer to the Dead on
PEDIATRIC NEUROLOGY CLINICAL PRIVILEGES
 Name: Page 1 Initial Appointment Reappointment All new applicants must meet the following requirements as approved by the governing body effective: 04/02/2014. Applicant: Check off the Requested box for
Name: Page 1 Initial Appointment Reappointment All new applicants must meet the following requirements as approved by the governing body effective: 04/02/2014. Applicant: Check off the Requested box for
ABCDE HOW TO RECOGNISE AND TREAT THE SERIOUSLY ILL CHILD
 ABCDE HOW TO RECOGNISE AND TREAT THE SERIOUSLY ILL CHILD A B C D E Possible Problems Airway obstruction Partial or complete Foreign body Secretions/blood/vomit Infection Swelling e.g. anaphylaxis trauma
ABCDE HOW TO RECOGNISE AND TREAT THE SERIOUSLY ILL CHILD A B C D E Possible Problems Airway obstruction Partial or complete Foreign body Secretions/blood/vomit Infection Swelling e.g. anaphylaxis trauma
Introduction. Clinical diagnosis of brain death. DOI: /tpa.46.54
 94 Invited Author DOI: 10.4274/tpa.46.54 Brain death in children Burak Tatl, Bar fl Ekici stanbul University Medical Faculty, Department of Pediatrics Division of Pediatric Neurology, stanbul, Turkey Summary
94 Invited Author DOI: 10.4274/tpa.46.54 Brain death in children Burak Tatl, Bar fl Ekici stanbul University Medical Faculty, Department of Pediatrics Division of Pediatric Neurology, stanbul, Turkey Summary
Retraction Retracted: Clinical Brain Death with False Positive Radionuclide Cerebral Perfusion Scans
 Hindawi Publishing Corporation Volume 2016, Article ID 2057806, 1 page http://dx.doi.org/10.1155/2016/2057806 Retraction Retracted: Clinical Brain Death with False Positive Radionuclide Cerebral Perfusion
Hindawi Publishing Corporation Volume 2016, Article ID 2057806, 1 page http://dx.doi.org/10.1155/2016/2057806 Retraction Retracted: Clinical Brain Death with False Positive Radionuclide Cerebral Perfusion
Understanding Neurological Death
 Understanding Neurological Death Special thanks to Trillium Gift Of Life Network s Donor Family Advisory Council, whose dedication and commitment never fail to profoundly move us all. Understanding Neurological
Understanding Neurological Death Special thanks to Trillium Gift Of Life Network s Donor Family Advisory Council, whose dedication and commitment never fail to profoundly move us all. Understanding Neurological
ASPIRUS WAUSAU HOSPITAL, INC. Passion for excellence. Compassion for people. SUBJECT: END TIDAL CARBON DIOXIDE MONITORING (CAPNOGRAPHY)
") Passion for excellence. Compassion for people. P&P REF : NEW 7-2011 ONBASE POLICY ID: 13363 REPLACES: POLICY STATUS : FINAL DOCUMENT TYPE: Policy EFFECTIVE DATE: 4/15/2014 PROPOSED BY: Respiratory Therapy
Passion for excellence. Compassion for people. P&P REF : NEW 7-2011 ONBASE POLICY ID: 13363 REPLACES: POLICY STATUS : FINAL DOCUMENT TYPE: Policy EFFECTIVE DATE: 4/15/2014 PROPOSED BY: Respiratory Therapy
61.10 Dental anesthesia certification.
 61.10 Dental anesthesia certification. a. *Definitions. For purposes of this section, the following definitions shall apply: 1. Acceptable accrediting body means an accrediting body which is accepted by
61.10 Dental anesthesia certification. a. *Definitions. For purposes of this section, the following definitions shall apply: 1. Acceptable accrediting body means an accrediting body which is accepted by
Traumatic Brain Injury
 Traumatic Brain Injury Mark J. Harris M.D. Associate Professor University of Utah Salt Lake City USA Overview In US HI responsible for 33% trauma deaths. Closed HI 80% Missile / Penetrating HI 20% Glasgow
Traumatic Brain Injury Mark J. Harris M.D. Associate Professor University of Utah Salt Lake City USA Overview In US HI responsible for 33% trauma deaths. Closed HI 80% Missile / Penetrating HI 20% Glasgow
Medical Policy Manual
 Medical Policy Manual Policy Number: 0013 Effective Date: Reviewed Date: Next Review: August 2019 CLINICAL BACKGROUND INTRAOPERATIVE NEUROMONITORING BACKGROUND Intraoperative neurophysiologic monitoring
Medical Policy Manual Policy Number: 0013 Effective Date: Reviewed Date: Next Review: August 2019 CLINICAL BACKGROUND INTRAOPERATIVE NEUROMONITORING BACKGROUND Intraoperative neurophysiologic monitoring
Subhairline EEG Part II - Encephalopathy
 Subhairline EEG Part II - Encephalopathy Teneille Gofton September 2013 Objectives To review the subhairline EEG changes seen with encephalopathy To discuss specific EEG findings in encephalopathy To outline
Subhairline EEG Part II - Encephalopathy Teneille Gofton September 2013 Objectives To review the subhairline EEG changes seen with encephalopathy To discuss specific EEG findings in encephalopathy To outline
COMA & INTENSIVE CARE
 COMA & INTENSIVE CARE Jozef Firment, MD. PhD., Judita Capkova, MD. PhD. Department of Anaesthesiology & Intensive Care Medicine Šafárik University Faculty of Medicine, Košice Coma Is a state of unarousable
COMA & INTENSIVE CARE Jozef Firment, MD. PhD., Judita Capkova, MD. PhD. Department of Anaesthesiology & Intensive Care Medicine Šafárik University Faculty of Medicine, Košice Coma Is a state of unarousable
Neurological Prognostication After Cardiac Arrest Murad Talahma, M.D. Neurocritical Care Ochsner Medical Center
 Neurological Prognostication After Cardiac Arrest Murad Talahma, M.D. Neurocritical Care Ochsner Medical Center Financial Disclosure None 1 Introduction Each year, 356,000 Americans are treated by EMS
Neurological Prognostication After Cardiac Arrest Murad Talahma, M.D. Neurocritical Care Ochsner Medical Center Financial Disclosure None 1 Introduction Each year, 356,000 Americans are treated by EMS
Capnography Connections Guide
 Capnography Connections Guide Patient Monitoring Contents I Section 1: Capnography Introduction...1 I Section 2: Capnography & PCA...3 I Section 3: Capnography & Critical Care...7 I Section 4: Capnography
Capnography Connections Guide Patient Monitoring Contents I Section 1: Capnography Introduction...1 I Section 2: Capnography & PCA...3 I Section 3: Capnography & Critical Care...7 I Section 4: Capnography
Lecture Notes. Chapter 2: Introduction to Respiratory Failure
 Lecture Notes Chapter 2: Introduction to Respiratory Failure Objectives Define respiratory failure, ventilatory failure, and oxygenation failure List the causes of respiratory failure Describe the effects
Lecture Notes Chapter 2: Introduction to Respiratory Failure Objectives Define respiratory failure, ventilatory failure, and oxygenation failure List the causes of respiratory failure Describe the effects
PHYSICIAN COMPETENCY FOR ADULT DEEP SEDATION (Ages 14 and older)
") Name Score PHYSICIAN COMPETENCY FOR ADULT DEEP SEDATION (Ages 14 and older) 1. Pre-procedure evaluation for moderate sedation should involve all of the following EXCEPT: a) Airway Exam b) Anesthetic history
Name Score PHYSICIAN COMPETENCY FOR ADULT DEEP SEDATION (Ages 14 and older) 1. Pre-procedure evaluation for moderate sedation should involve all of the following EXCEPT: a) Airway Exam b) Anesthetic history
Sample Case Study. The patient was a 77-year-old female who arrived to the emergency room on
 Sample Case Study The patient was a 77-year-old female who arrived to the emergency room on February 25 th with a chief complaint of shortness of breath and a deteriorating pulmonary status along with
Sample Case Study The patient was a 77-year-old female who arrived to the emergency room on February 25 th with a chief complaint of shortness of breath and a deteriorating pulmonary status along with
FOR REPRESENTATIVE EDUCATION
 Neuromuscular Blockade in the ICU NIMBEX Indication 1 NIMBEX (cisatracurium besylate) is indicated as an adjunct to general anesthesia to facilitate tracheal intubation in adults and in pediatric patients
Neuromuscular Blockade in the ICU NIMBEX Indication 1 NIMBEX (cisatracurium besylate) is indicated as an adjunct to general anesthesia to facilitate tracheal intubation in adults and in pediatric patients
Examination Approach. Examination Approach. Case 1: Mental Status. The Neurological Exam In the ICU: High Yield Techniques 5/8/2015
 The Neurological Exam In the ICU: High Yield Techniques Examination Approach Two types of neurologic examinations 1. Screening Examination 2. Testing Hypotheses Select high-yield tests and techniques S.
The Neurological Exam In the ICU: High Yield Techniques Examination Approach Two types of neurologic examinations 1. Screening Examination 2. Testing Hypotheses Select high-yield tests and techniques S.
Post-Arrest Care: Beyond Hypothermia
 Post-Arrest Care: Beyond Hypothermia Damon Scales MD PhD Department of Critical Care Medicine Sunnybrook Health Sciences Centre University of Toronto Disclosures CIHR Physicians Services Incorporated Main
Post-Arrest Care: Beyond Hypothermia Damon Scales MD PhD Department of Critical Care Medicine Sunnybrook Health Sciences Centre University of Toronto Disclosures CIHR Physicians Services Incorporated Main
Chronic Brain-Dead Patients Who Exhibit Lazarus Sign
 CASE REPORT Korean J Neurotrauma 2017;13(2):153-157 pissn 2234-8999 / eissn 2288-2243 https://doi.org/10.13004/kjnt.2017.13.2.153 Chronic Brain-Dead Patients Who Exhibit Lazarus Sign Department of Neurosurgery,
CASE REPORT Korean J Neurotrauma 2017;13(2):153-157 pissn 2234-8999 / eissn 2288-2243 https://doi.org/10.13004/kjnt.2017.13.2.153 Chronic Brain-Dead Patients Who Exhibit Lazarus Sign Department of Neurosurgery,
INCREASED INTRACRANIAL PRESSURE
 INCREASED INTRACRANIAL PRESSURE Sheba Medical Center, Acute Medicine Department Irene Frantzis P-Year student SGUL 2013 Normal Values Normal intracranial volume: 1700 ml Volume of brain: 1200-1400 ml CSF:
INCREASED INTRACRANIAL PRESSURE Sheba Medical Center, Acute Medicine Department Irene Frantzis P-Year student SGUL 2013 Normal Values Normal intracranial volume: 1700 ml Volume of brain: 1200-1400 ml CSF:
ITLS Pediatric Provider Course Basic Pre-Test
 ITLS Pediatric Provider Course Basic Pre-Test 1. You arrive at the scene of a motor vehicle collision and are directed to evaluate a child who was in one of the vehicles. The patient appears to be a child
ITLS Pediatric Provider Course Basic Pre-Test 1. You arrive at the scene of a motor vehicle collision and are directed to evaluate a child who was in one of the vehicles. The patient appears to be a child
Head injuries. Severity of head injuries
 Head injuries ED Teaching day 23 rd October Severity of head injuries Minor GCS 14-15 Must not have any of the following: Amnesia 10min Neurological sign or symptom Skull fracture (clinically or radiologically)
Head injuries ED Teaching day 23 rd October Severity of head injuries Minor GCS 14-15 Must not have any of the following: Amnesia 10min Neurological sign or symptom Skull fracture (clinically or radiologically)
NEUROLOGY CLERKSHIP CORE CURRICULUM GUIDELINES
 NEUROLOGY CLERKSHIP CORE CURRICULUM GUIDELINES Endorsed by the following organizations - October 2000: American Academy of Neurology Association of University Professors of Neurology American Neurological
NEUROLOGY CLERKSHIP CORE CURRICULUM GUIDELINES Endorsed by the following organizations - October 2000: American Academy of Neurology Association of University Professors of Neurology American Neurological