Brain Death Examination Importance and Pitfalls. Dr. Reshi Professor of Neurology/Neurosurgery University of Minnesota
|
|
|
- Olivia Manning
- 5 years ago
- Views:
Transcription
1 Brain Death Examination Importance and Pitfalls Dr. Reshi Professor of Neurology/Neurosurgery University of Minnesota
2 Conflict No Conflicts to report Will not discuss off label use of any medication.
3 Presentation Objectives To present the key findings of the update of the 1995 American Academy of Neurology (AAN) guideline 1 To present evidence-based recommendations for Brain Death Examination Identify areas for improvement
4 So why should we worry about Brain Death? 1) Reduce cost of healthcare. 2) Recovery of coma is very unrealistic. 3) We need organs for donation. 4) All of the Above. 5) None of the above.
5 Public Poll 98% of respondents had heard of brain death, but only one-third (33.7%) believed that a person who had been declared brain dead was legally dead. Furthermore, 28.1% thought brain-dead people can hear, and only 40.4% classified someone who is brain dead as dead. Rather, 43.3% characterized persons who are brain dead as good as dead, and 16.0% stated that they are alive doctors would deliberately remove a patient s organs, before the patient had died, whereas others believed that life-saving medical care would be withheld so that patients could become eligible for organ donation.(newton, et al.) Newton JD. How does the general public view posthumous organ donation? A meta-synthesis of the qualitative literature. BMC Public Health 2011;11:
6 It Matters: We got to get this right. Because one mistake undermines the trust. Confirms the perceived conflict of interest. Robs many organ recipient s of possible life. Robs the family and friends of a proper grieving.
7 Brain Death: History 1968 Harvard Ad hoc committee published paper on irreversible coma These Criteria got adopted into Brain Death Criteria around 1970 s by different states. In 1981 a Presidential commission issued Defining Death: Medical, Legal, and ethical issues Report used to adopt Uniform Determination of Death Act by 39 States. AAN came up with recommendations in 1995 to examine patients for Brain Death. Revised in 2010.
8 Definition The President s Commission report on guidelines for the determination of death 2 culminated in a proposal for a legal definition that led to the Uniform Determination of Death Act (UDDA). The act reads: An individual who has sustained either 1) irreversible cessation of circulatory and respiratory functions, or 2) irreversible cessation of all functions of the entire brain, including the brain stem, is dead. A determination of death must be made with accepted medical standards. 3
9 Why should I trust the process 1. Are there patients who fulfill the clinical criteria of brain death who recover brain function? 2. Are complex motor movements that falsely suggest retained brain function sometimes observed in brain death?
10 AAN Study MEDLINE and EMBASE January 1996 to May 2009 A secondary bibliography search of all full-text articles Relevant, fully published, peer-reviewed articles Search terms included the MeSH term brain death and the text words brain death, irreversible coma, and apnea test.
11 Literature Review 367 abstracts Exclusion criteria: - Articles that studied patients younger than 18 years - Articles that confirmed prior observations - Review articles, bioethical reviews, articles without description of a brain death examination - Articles with questionable practices or describing rarely used ancillary technology 38 articles
12 Analysis of Evidence Question 1: Are there patients who fulfill the clinical criteria of brain death who recover brain function?
13 Conclusion/Recommendation Conclusion: In adults, recovery of neurologic function has not been reported after the clinical diagnosis of brain death has been established using the criteria given in the 1995 AAN practice parameter. Recommendation: The criteria for the determination of brain death given in the 1995 AAN practice parameter have not been invalidated by published reports of neurological recovery in patients who fulfill these criteria (Level U).
14 Analysis of Evidence Question 2: Are complex motor movements that falsely suggest retained brain function sometimes observed in brain death?
15 Conclusion/Recommendation Conclusion: For some patients diagnosed as brain dead, complex, nonbrain-mediated spontaneous movements can falsely suggest retained brain function. Additionally, ventilator autocycling may falsely suggest patient-initiated breathing. Recommendation: Complex spontaneous motor movements and false-positive triggering of the ventilator may occur in patients who are brain dead (Level C).
16 Clinical Context Much of the framework necessary for the development of accepted medical standards for the declaration of brain death is based on straightforward principles. These principles can be derived from the definition of brain death provided by the UDDA.
17 Process Overview 1. Patient in coma 2. Evidence of Injury: Irreversible, Catastrophic whole brain injury on imaging 3. No obvious metabolic cause, medication or intoxicant to explain this. 4. Neurological Exam No Brain stem or cerebral function 5. Apnea testing 6. Ancillary testing (if Needed)
18 Practical Guidance for Determining Brain Death. First Condition Coma. Patients must lack all evidence of responsiveness. o Eye opening or eye movement to noxious stimuli is absent. Noxious stimuli should not produce a motor response other than spinally mediated reflexes. Evidence of Catastrophic Irreversible Whole Brain Injury Absence of ALL brainstem reflexes.
19 Practical Guidance for Determining Brain Death, cont. 1. The clinical evaluation (PREREQUISETES). Establish IRREVERSIBLE and proximate cause of coma. The cause of coma can usually be established by history, examination, neuroimaging, and laboratory tests. Rule out CNS-depressant Drug effect. Drug screen. 5 times the drug s half-life, or drug plasma levels below the therapeutic range. Prior use of hypothermia may delay drug metabolism. Neuromuscular blocking agents (this can be defined by the presence of a train of four twitches with maximal ulnar nerve stimulation). There should be no severe electrolyte, acid-base, or endocrine disturbance (defined by severe acidosis or laboratory values markedly deviated from the norm). Rule out other metabolic reasons for Coma, e.g. Hepatic coma, Sepsis etc.
20 What Happens Next Treatment team makes plans for further examination Nursing staff can inform Organ Donation Agency to evaluate the patient in the background No contact with family at this point. Federal and state law requires the physician to contact an organ procurement organization following determination of brain death. 4,5
21 Practical Guidance for Determining Brain Death, cont. Achieve normal core temperature. In most patients, a warming blanket is needed to raise the body temperature and maintain a normal or near-normal temperature (>36 C). After the initial equilibration of arterial carbon dioxide with mixed central venous carbon dioxide the PaCO 2 rises steeply, but then more slowly when the body metabolism raises PaCO 2.To avoid delaying an increase in PaCO 2, normal or near-normal core temperature is preferred during the apnea test. Achieve normal systolic blood pressure. Hypotension from loss of peripheral vascular tone or hypovolemia (diabetes insipidus) is common; vasopressors or vasopressin are often required. Neurologic examination is usually reliable with a systolic blood pressure 100 mm Hg.
22 Practical Guidance for Determining Brain Death, cont. Perform First neurologic examination Comatose patient, irreversible cause established, other causes of coma ruled out ---- PROCEED with Neurological examination. Legally, all physicians are allowed to determine brain death in most US states. Neurologists, neurosurgeons, and intensive care specialists may have specialized expertise. physicians making a determination of brain death be have demonstrated competence in this complex examination. Brain death statutes in the US do differ by state and institution. Some US state or hospital guidelines require the examiner to have certain expertise.
23 Practical Guidance for Determining Brain Death, cont. 2. The clinical evaluation (neurologic assessment). Coma. Patients must lack all evidence of responsiveness. o Eye opening or eye movement to noxious stimuli is absent. Noxious stimuli should not produce a motor response other than spinally mediated reflexes. Absence of brainstem reflexes. Absence of pupillary response to a bright light is documented in both eyes. o Usually the pupils are fixed in a midsize or dilated position (4 9 mm). Constricted pupils suggest the possibility of drug intoxication. When uncertainty exists a magnifying glass should be used.
24 Practical Guidance for Determining Brain Death, cont. Absence of ocular movements using oculocephalic testing o Once the integrity of the cervical spine is ensured, the head is briskly rotated horizontally and vertically. There should be no movement of the eyes relative to head movement. - Absence oculovestibular reflex --- Cold Caloric Testing. o The oculovestibular reflex is tested by irrigating each ear with ice water (caloric testing) after the patency of the external auditory canal is confirmed. o The head is elevated to 30 degrees. o Each external auditory canal is irrigated (one ear at a time) with approximately 50 cc of ice water. Movement of the eyes should be absent during 1 minute of observation. Both sides are tested, with an interval of at least five minutes. Absence of corneal reflex. o Absent corneal reflex is demonstrated by touching the cornea with a piece of tissue paper, a cotton swab, or squirts of water. No eyelid movement should be seen.
25 Practical Guidance for Determining Brain Death, cont. Absence of facial muscle movement to a noxious stimulus. o Deep pressure on the condyles at the level of the temporomandibular joints and deep pressure at the supraorbital ridge should produce no grimacing or facial muscle movement. Absence of the pharyngeal and tracheal reflexes. o The pharyngeal or gag reflex is tested after stimulation of the posterior pharynx with a tongue blade or suction device. The tracheal reflex is most reliably tested by examining the cough response to tracheal suctioning. The catheter should be inserted into the trachea and advanced to the level of the carina followed by one or two suctioning passes.
26 Practical Guidance for Determining Brain Death, cont. Apnea. Absence of a breathing drive. o Absence of a breathing drive is tested with a CO 2 challenge. Documentation of an increase in (partial pressure of carbon dioxide [PaCO 2 ] above normal levels is typical practice. It requires preparation before the test. Prerequisites. o Normotension o Normothermia o Euvolemia o Eucapnia (PaCO mm Hg) o Absence of hypoxia o No prior evidence of CO 2 retention (i.e., chronic obstructive pulmonary disease, severe obesity)
27 Practical Guidance for Determining Brain Death, cont. Procedure. o Adjust vasopressors to a systolic blood pressure 100 mm Hg or have them available. o Preoxygenate for at least 10 minutes with 100% oxygen to a PaO 2 >200 mm Hg. o Reduce ventilation frequency to 10 breaths per minute to eucapnia. o Reduce positive end-expiratory pressure (PEEP) to 5 cm H 2 O (oxygen desaturation with decreasing PEEP may suggest difficulty with apnea testing). o If pulse oximetry oxygen saturation remains >95%, obtain a baseline blood gas (partial pressure of oxygen [PaO 2 ], PaCO 2, ph, bicarbonate, base excess). o Disconnect the patient from the ventilator. o Preserve oxygenation (e.g., place an insufflation catheter through the endotracheal tube and close to the level of the carina and deliver 100% O 2 at 6 L/min). o Look closely for respiratory movements for 8 10 minutes. Respiration is defined as abdominal or chest excursions and may include a brief gasp.
28 Practical Guidance for Determining Brain Death, cont. o Abort if systolic blood pressure decreases to <90 mm Hg. o Abort if oxygen saturation measured by pulse oximetry is <85% for >30 seconds. Retry procedure with T-piece, continuous positive airway pressure (CPAP) 10 cm H 2 O, and 100% O 2 12 L/minute. o If no respiratory drive is observed, repeat blood gas (PaO 2, PaCO 2, ph, bicarbonate, base excess) after approximately 8 minutes. o If respiratory movements are absent and arterial PCO 2 is 60 mm Hg (or 20 mm Hg increase in arterial PCO 2 over a baseline normal arterial PCO 2 ), the apnea test result is positive (i.e., supports the clinical diagnosis of brain death). o If the test is inconclusive but the patient is hemodynamically stable during the procedure, it may be repeated for a longer period of time (10 15 minutes) after the patient is again adequately preoxygenated.
29 All Criteria Met Patient should be declared DEAD (By Brain Death Criteria) Activity found: ---- ABORT testing. Meets Criteria ---- Cant complete Apnea Testing Next Step: Confirmatory Testing.
30 Practical Guidance for Determining Brain Death, cont. Ancillary tests. EEG, cerebral angiography Nuclear scan Transcranial Doppler (TCD), CT angiography (CTA), and MRI/magnetic resonance angiography (MRA) Ancillary tests can be used when uncertainty exists about the reliability of parts of the neurologic examination or when the apnea test cannot be performed.
31 Practical Guidance for Determining Brain Death, cont. Expertise is required. In adults, ancillary tests are not needed for the clinical diagnosis of brain death and cannot replace a neurologic examination. Physicians ordering ancillary tests should appreciate the disparities between tests and the potential for false positives (i.e., the test suggests brain death, but the patient does not meet clinical criteria). Rather than ordering ancillary tests, physicians may decide not to proceed with the declaration of brain death if clinical findings are unreliable.
32 Practical Guidance for Determining Brain Death, cont. Documentation. The time of brain death is documented in the medical records. Time of death is the time the arterial PCO 2 reached the target value. In patients with an aborted apnea test, the time of death is when the ancillary test has been officially interpreted. A checklist is filled out, signed, and dated Federal and state law requires the physician to contact an organ procurement organization following determination of brain death. 4,5
33 Patient Selection Potential Bias Examination Test Selection Communication Post Discussion What After that Where Can it go Wrong: Pitfalls
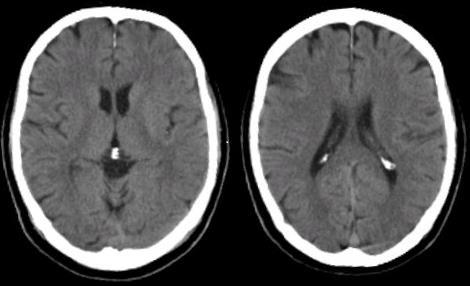
34 Question What is the next step in Brain Death Examination? A 55 year old female was with her children on Thanksgiving day and is brought to hospital unresponsive. CT head was normal at presentation and usual lab studies are normal. Two days later patient is still not waking up, and a neurology consultation is called for brain death examination.

35 Question: CT head
36 Question: So What should we do next Does not meet the Brain Death Criteria (by US criteria). She may do so after sometime But not now. So make sure all the pre brain Death Criteria are met. Coma Irreversible, catastrophic whole brain injury is evident. Brain Stem reflexes are absent. Other reasons for the coma have been ruled out (even in case of above). Before you proceed to a Neurologic Exam/Apnea Test/Confirmatory testing). Talk to your Attendings before activating Organ donation Agency.
37 Perception of Conflict Organ Donation Agency team and Treatment Team should avoid all contact and perception of collaboration. Federal and state law requires the physician to contact an organ procurement organization following determination of brain death. 4,5 Trust in the system is fundamental to the integrity of the system. Any perception of collusion undermines the whole system.
38 Perception of Conflict. Most places allow staff to call organ donation to evaluate patient for organ donation. Problems: Organ Donation Engages with family. Organ Donation Engages with staff. Organ Donation Engages with Physician care team. Ok to inform: Should not engage with FAMILY/TREATMENT TEAM.
39 Examination What will be the next step in your examination? A 19 year old male from Lake Wobegon is brought to ER after his ATV submerged a frozen lake. Patient was in pulse less electrical rhythm (heart beating according to electrocardiogram but no discernable pulse or blood pressure). Patient was cooled. Neurology consult called as he is in coma. Neurology resident examines patient, and reports that he meets criteria for brain death.
40 Examination
41 Examination Avoid Rush Establish Coma Rule out other possible causes of coma: Sedating drugs, paralytics, medical conditions. Meet all prerequisites. Assess Brain Stem and Reversibility. Examination is relevant only after all of above has been done. Apnea testing --- regimented. Second examination. Confirm if needed. No compromise: You got to get this right.
42 Ancillary Tests Cerebral Circulation Brain Edema high ICP --- Higher than MAP thus arresting flow. Cerebral Angiography (CTA) Cerebral scintigraphy Technetium Tc 99m Transcranial Doppler EEG
43 Communicating Brain Death A healthcare worker talking to a family states, We will take your son off of life support now that he has been declared brain dead. If you want to say your goodbyes, please do so now. What is wrong with the statement. Avoid Using Brain Death altogether ---- Use Dead in your conversations. Wait for the actual declaration before discussing anything with the family/friends Remember patient is alive until pronounced dead.
44 Communication Cont. Save a life ---- Make a difference. Do not create False Hope We as medical professionals get nervous around death and uncertainty. Clearly define death Help Family Grieve Alleviate pain of family Understand For us another day at work for us. For the family it is 1: experience that they are not prepared for and nothing we can do can prepare them for this.
45 Communication Cont. We are here to help family. Culture Mistrust Getting defensive Extend yourself. Bring your professional integrity along
46 Communication Cont. Never use Brain Death Unless that is the case Be very crisp and clear when describing states of consciousness Coma is coma and not brain death. Your Specificity has to be 110%, when in doubt, patient is not dead! YOU CAN NEVER BE WRONG. Be empathetic ---- be human. State what you can stand behind 100%. Bring yourself down to layman s terminology Do not quote data and studies.
47 Brain Death In Adults Compared to Children Interval between two evaluations Term to 2 mo old, 48 hr >2 mo to 1 yr old, 24 hr >1 yr to <18 yr old, 12 hr >18 yr old, interval optional Confirmatory tests Term to 2 mo old, 2 confirmatory tests >2 mo to 1 yr old, 1 confirmatory test >1 yr to <18 yr old, optional >18 yr old, optional
48 Final Thoughts 1. Patient in coma 2. Evidence of Injury: Irreversible, Catastrophic whole brain injury on imaging 3. No obvious metabolic cause, medication or intoxicant to explain this. 4. Neurological Exam No Brain stem or cerebral function 5. Apnea testing 6. If steps 1, 2, 3, 4 are met and we can not pursue apnea testing, confirmatory test can be used. 7. Communicating with family.
49 Clinical Context, cont. To determine cessation of all functions of the entire brain, including the brain stem, physicians must: determine the presence of unresponsive coma determine the absence of brainstem reflexes determine the absence of respiratory drive after a CO 2 challenge To ensure that the cessation of brain function is irreversible, physicians must: determine the cause of coma exclude mimicking medical conditions observe the patient for a period of time to exclude the possibility of recovery
50 References 1. Practice parameters for determining brain death in adults (summary statement). The Quality Standards Subcommittee of the American Academy of Neurology. Neurology 1995;45: Guidelines for the determination of death. Report of the medical consultants on the diagnosis of death to the President s commission for the study of ethical problems in medicine and biochemical and behavioral research. JAMA 1981;246: Uniform Determination of Death Act, 12 uniform laws annotated 589 (West 1993 and West sup 1997). 4. Title 42 CFR (Condition of participation: Organ, tissue, and eye procurement). 5. Title 42 USC 1320b-8 (Hospital protocols for organ procurement and standards for organ procurement agencies). 6. Plum and Posner s Diagnosis of Stupor and Coma "by Posner, Saper, Schiff, and Plum. 4 th Ed, Coma and Impaired Consciousness by Young, Ropper, and Bolton, Brain Death AAN guidelines 1995,
Determination of Death
 Policy Legal Standard UTMB physicians will determine death in accordance with this policy which is based on Texas law and the practice parameters recommended by the American Academy of Neurology for adults
Policy Legal Standard UTMB physicians will determine death in accordance with this policy which is based on Texas law and the practice parameters recommended by the American Academy of Neurology for adults
PROPOSED REVISIONS OF ISMA BRAIN DEATH GUIDELINES
 RESOLUTION 17-04 Introduced by: Action: PROPOSED REVISIONS OF ISMA BRAIN DEATH GUIDELINES Emil Weber, MD Adopted as Amended RESOLVED, that ISMA adopt updated brain death guidelines for adults and children,
RESOLUTION 17-04 Introduced by: Action: PROPOSED REVISIONS OF ISMA BRAIN DEATH GUIDELINES Emil Weber, MD Adopted as Amended RESOLVED, that ISMA adopt updated brain death guidelines for adults and children,
Brain Death Determination: Outline. Definition. Brain Death Determination. Brain Death Determination. No conflict of interest
 No conflict of interest : Outline Definition Definition Confounding factors Clinical examination Apnea test Confirmatory testing Communicating the diagnosis Ethical issues Brain death remains the preferred
No conflict of interest : Outline Definition Definition Confounding factors Clinical examination Apnea test Confirmatory testing Communicating the diagnosis Ethical issues Brain death remains the preferred
Hospital of the University of Pennsylvania POLICY MANUAL
 Page 1 of 8 KEY WORDS: Brain Death Coma # 1-6-11 Procedures Following Patient Death # 1-6-13 Organ Donation and Anatomical Donation and Pennsylvania s Anatomical Gift Act #1-6-17 Withholding and Withdrawing
Page 1 of 8 KEY WORDS: Brain Death Coma # 1-6-11 Procedures Following Patient Death # 1-6-13 Organ Donation and Anatomical Donation and Pennsylvania s Anatomical Gift Act #1-6-17 Withholding and Withdrawing
GUIDELINES: The following guidelines for determining brain death in adults are accepted practice parameters of the American Academy of Neurology 1
 Page 1 of 5 PURPOSE: The purpose of this policy is to provide licensed staff and medical personnel with a guideline to determine when a patient on a ventilator demonstrates clinical brain death. POLICY
Page 1 of 5 PURPOSE: The purpose of this policy is to provide licensed staff and medical personnel with a guideline to determine when a patient on a ventilator demonstrates clinical brain death. POLICY
Name Signature Date IRB & Ethics Committee Dr. Ejaz A. Khan Chairman IRB & EC Dr. Shoukat Matabddin
 Prepared by Reviewed By Name Signature Date IRB & Ethics Committee Dr. Ejaz A. Khan Chairman IRB & EC Dr. Shoukat Matabddin Dr. M. Salim Khan Medical Director Approved by Dr. Manzoor H Qazi Chief Executive
Prepared by Reviewed By Name Signature Date IRB & Ethics Committee Dr. Ejaz A. Khan Chairman IRB & EC Dr. Shoukat Matabddin Dr. M. Salim Khan Medical Director Approved by Dr. Manzoor H Qazi Chief Executive
YALE-NEW HAVEN HOSPITAL CLINICAL ADMINISTRATIVE POLICY & PROCEDURE MANUAL
 YALE-NEW HAVEN HOSPITAL CLINICAL ADMINISTRATIVE POLICY & PROCEDURE MANUAL Administrative Policy Title: Brain Death, Guidelines Determination of Death by Neurological Criteria in the Pediatric Patient Manual
YALE-NEW HAVEN HOSPITAL CLINICAL ADMINISTRATIVE POLICY & PROCEDURE MANUAL Administrative Policy Title: Brain Death, Guidelines Determination of Death by Neurological Criteria in the Pediatric Patient Manual
DETERMINATION OF NEUROLOGIC DEATH IN ADULTS AND CHILDREN April 2010
 Chicago, Illinois PAGE: 1 of 7 DETERMINATION OF NEUROLOGIC DEATH IN ADULTS AND CHILDREN April 2010 Key Content Expert: Medical Center Ethics Committee in consultation with Chiefs of Service for Neurology
Chicago, Illinois PAGE: 1 of 7 DETERMINATION OF NEUROLOGIC DEATH IN ADULTS AND CHILDREN April 2010 Key Content Expert: Medical Center Ethics Committee in consultation with Chiefs of Service for Neurology
Declaring Brain Death. Ali Salim, MD Professor of Surgery Chief, Division of Trauma, Burns, Surgical Critical Care, and Emergency General Surgery
 Declaring Brain Death Ali Salim, MD Professor of Surgery Chief, Division of Trauma, Burns, Surgical Critical Care, and Emergency General Surgery Disclosures I have nothing to disclose Why should we know
Declaring Brain Death Ali Salim, MD Professor of Surgery Chief, Division of Trauma, Burns, Surgical Critical Care, and Emergency General Surgery Disclosures I have nothing to disclose Why should we know
The Determination of Brain Death. James Zisfein, M.D. Chief, Division of Neurology Lincoln Medical Center, Bronx, NY
 The Determination of Brain Death James Zisfein, M.D. Chief, Division of Neurology Lincoln Medical Center, Bronx, NY James.Zisfein@nychhc.org The early history of brain death Until recently, death was determined
The Determination of Brain Death James Zisfein, M.D. Chief, Division of Neurology Lincoln Medical Center, Bronx, NY James.Zisfein@nychhc.org The early history of brain death Until recently, death was determined
Policy No: Title: Determination of Death by Brain Criteria Department: PATIENT CARE. Originated: May 1992
 Title: Determination of Death by Brain Criteria Department: PATIENT CARE Policy No: Page 1 of 6 Revised: April 2009 Previous revisions: 9/96, 7/99, 7/07 Reviewed: August 2010 Originated: May 1992 I. POLICY:
Title: Determination of Death by Brain Criteria Department: PATIENT CARE Policy No: Page 1 of 6 Revised: April 2009 Previous revisions: 9/96, 7/99, 7/07 Reviewed: August 2010 Originated: May 1992 I. POLICY:
Neurological Determination of Death Adult
 Approved by: Vice President and Chief Medical Officer Neurological Determination of Death Adult Corporate Policy & Procedures Manual Number: VII-B-400 Date Approved June 9, 2015 Next Review (3 years from
Approved by: Vice President and Chief Medical Officer Neurological Determination of Death Adult Corporate Policy & Procedures Manual Number: VII-B-400 Date Approved June 9, 2015 Next Review (3 years from
Brain Death Its History (and Some Controversies ) Eelco F.M. Wijdicks, MD, PhD Division of Critical Care Neurology Mayo College of Medicine
 Eelco F.M. Wijdicks, MD, PhD Division of Critical Care Neurology Mayo College of Medicine") Brain Death Its History (and Some Controversies ) Eelco F.M. Wijdicks, MD, PhD Division of Critical Care Neurology Mayo College of Medicine 2016 MFMER 3583421-1 Brain Death or 2016 MFMER 3583421-2 Where
Brain Death Its History (and Some Controversies ) Eelco F.M. Wijdicks, MD, PhD Division of Critical Care Neurology Mayo College of Medicine 2016 MFMER 3583421-1 Brain Death or 2016 MFMER 3583421-2 Where
Sample Guidelines for the Determination of Death: Including Death by Neurologic Criteria
 Sample Guidelines for the Determination of Death: Including Death by Neurologic Criteria A. SUBJECT: Guidelines for the Determination of Death: Including Death by Neurologic Criteria B. POLICY: The Medical
Sample Guidelines for the Determination of Death: Including Death by Neurologic Criteria A. SUBJECT: Guidelines for the Determination of Death: Including Death by Neurologic Criteria B. POLICY: The Medical
Ethical Challenges With Documenting Brain Death
 Ethical Challenges With Documenting Brain Death William Reitsma, BSN, CPTC Consultant AOPO Accreditation Surveyor 2015 Doug Miller Symposium Wisconsin Dells, Wisconsin When are You Dead? History of Brain
Ethical Challenges With Documenting Brain Death William Reitsma, BSN, CPTC Consultant AOPO Accreditation Surveyor 2015 Doug Miller Symposium Wisconsin Dells, Wisconsin When are You Dead? History of Brain
Clinical Report Guidelines for the Determination of Brain Death in Infants and Children: An Update of the 1987 Task Force Recommendations
 Guidance for the Clinician in Rendering Pediatric Care Clinical Report Guidelines for the Determination of Brain Death in Infants and Children: An Update of the 1987 Task Force Recommendations abstract
Guidance for the Clinician in Rendering Pediatric Care Clinical Report Guidelines for the Determination of Brain Death in Infants and Children: An Update of the 1987 Task Force Recommendations abstract
Determination of Death by Brain Death Criteria in Adults Page 1 of 10. All attending physicians certified to determine brain death.
 Page 1 of 10 Scope: All attending physicians certified to determine brain death. Statutory Background Uniform Determination of Death Act (Adopted in various forms in most states including Connecticut)
Page 1 of 10 Scope: All attending physicians certified to determine brain death. Statutory Background Uniform Determination of Death Act (Adopted in various forms in most states including Connecticut)
Experiences as a Donation Support Physician. Dead or not Dead? Are the following statements consistent with neurological
 Experiences as a Donation Support Physician Dead or not Dead? Are the following statements consistent with neurological determination of death (dead)? or not (not dead)? With thanks to Drs. Alex Manara,
Experiences as a Donation Support Physician Dead or not Dead? Are the following statements consistent with neurological determination of death (dead)? or not (not dead)? With thanks to Drs. Alex Manara,
GUIDELINE for the diagnosis and confirmation of death within Adult Critical Care
 Guideline for the diagnosis and confirmation of death within adult critical care 1. Introduction Death occurs when there is permanent loss of capacity for consciousness and loss of all brainstem functions.
Guideline for the diagnosis and confirmation of death within adult critical care 1. Introduction Death occurs when there is permanent loss of capacity for consciousness and loss of all brainstem functions.
Take A Breath: Pulmonary Management of the Organ Donor. Whitni Noyes, RN, CPTC Midwest Transplant Network
 Take A Breath: Pulmonary Management of the Organ Donor Whitni Noyes, RN, CPTC Midwest Transplant Network Objectives Recognize MTN referral criteria. Be familiar with the apnea test for brain death pronouncement.
Take A Breath: Pulmonary Management of the Organ Donor Whitni Noyes, RN, CPTC Midwest Transplant Network Objectives Recognize MTN referral criteria. Be familiar with the apnea test for brain death pronouncement.
NEW YORK CITY HEALTH AND HOSPITALS CORPORATION CORPORATE BRAIN DEATH POLICY
 NEW YORK CITY HEALTH AND HOSPITALS CORPORATION CORPORATE BRAIN DEATH POLICY PURPOSE: To describe the guidelines, procedure, and documentation requirements for: Initiation of a brain death evaluation, Determination
NEW YORK CITY HEALTH AND HOSPITALS CORPORATION CORPORATE BRAIN DEATH POLICY PURPOSE: To describe the guidelines, procedure, and documentation requirements for: Initiation of a brain death evaluation, Determination
BRAIN DEATH. Frequently Asked Questions 04for the General Public
 BRAIN DEATH Frequently Asked Questions 04for the General Public Neurocritical Care Society BRAIN DEATH FAQ s FOR THE GENERAL PUBLIC NEUROCRITICAL CARE SOCIETY 1. Q: Why was this FAQ created? A: Several
BRAIN DEATH Frequently Asked Questions 04for the General Public Neurocritical Care Society BRAIN DEATH FAQ s FOR THE GENERAL PUBLIC NEUROCRITICAL CARE SOCIETY 1. Q: Why was this FAQ created? A: Several
Committee on Organ Donor Intervention Research
 National Academics of Science, Engineering, Medicine Committee on Organ Donor Intervention Research Galen V. Henderson, MD Director, Neurocritical Care Brigham and Women s Hospital Harvard Medical School
National Academics of Science, Engineering, Medicine Committee on Organ Donor Intervention Research Galen V. Henderson, MD Director, Neurocritical Care Brigham and Women s Hospital Harvard Medical School
First Person Consent Uniform Anatomical Gift Act of 1968
 Andrew Wilson, Medicolegal Death Investigator Not-for-profit Organ Procurement Organization (OPO) & Tissue Recovery Agency Regulated by Centers for Medicaid and Medicare Services (CMS) and FDA Offices
Andrew Wilson, Medicolegal Death Investigator Not-for-profit Organ Procurement Organization (OPO) & Tissue Recovery Agency Regulated by Centers for Medicaid and Medicare Services (CMS) and FDA Offices
Brain Death and Disorders of Consciousness. John Banja, PhD Center for Ethics Emory University
 Brain Death and Disorders of Consciousness John Banja, PhD Center for Ethics Emory University jbanja@emory.edu Five kinds of catastrophic neurological injury Minimal Responsiveness Persistent Vegetative
Brain Death and Disorders of Consciousness John Banja, PhD Center for Ethics Emory University jbanja@emory.edu Five kinds of catastrophic neurological injury Minimal Responsiveness Persistent Vegetative
Med 536 Communicating About Prognosis Workshop. Case 2
 Med 536 Communicating About Prognosis Workshop Case 2 ID / CC: 33 year-old man with intracranial hemorrhage History of the Presenting Illness 33 year-old man with a prior history of melanoma of the neck
Med 536 Communicating About Prognosis Workshop Case 2 ID / CC: 33 year-old man with intracranial hemorrhage History of the Presenting Illness 33 year-old man with a prior history of melanoma of the neck
UNIVERSITY OF TENNESSEE HOSPITAL 1924 Alcoa Highway * Knoxville, TN (865) LABEL
 LABEL") 1003 UNIVERSITY OF TENNESSEE HOSPITAL 1924 Alcoa Highway * Knoxville, TN 37920 (865) 544-9000 LABEL Knoxville Neurology Clinic Orders and Progress tes : NAME: MED REC#: PHYSICIAN: DATE: DATE PHYSICIAN'S
1003 UNIVERSITY OF TENNESSEE HOSPITAL 1924 Alcoa Highway * Knoxville, TN 37920 (865) 544-9000 LABEL Knoxville Neurology Clinic Orders and Progress tes : NAME: MED REC#: PHYSICIAN: DATE: DATE PHYSICIAN'S
Understanding Neurological Death
 Understanding Neurological Death Special thanks to Trillium Gift Of Life Network s Donor Family Advisory Council, whose dedication and commitment never fail to profoundly move us all. Understanding Neurological
Understanding Neurological Death Special thanks to Trillium Gift Of Life Network s Donor Family Advisory Council, whose dedication and commitment never fail to profoundly move us all. Understanding Neurological
Form for the Diagnosis of Death using Neurological Criteria in Children >2 months to <18 years {full guidance version}
 This form is consistent with and should be used in conjunction with, the AoMRC (2008) A Code of Practice for the Diagnosis and Confirmation of Death 1 and has been endorsed for use by the following institutions:
This form is consistent with and should be used in conjunction with, the AoMRC (2008) A Code of Practice for the Diagnosis and Confirmation of Death 1 and has been endorsed for use by the following institutions:
Babak Tamizi Far MD. Assistant professor of internal medicine Al-zahra hospital, Isfahan university of medical sciences
 Babak Tamizi Far MD. Assistant professor of internal medicine Al-zahra hospital, Isfahan university of medical sciences ٢ Level of consciousness is depressed Stuporous patients respond only to repeated
Babak Tamizi Far MD. Assistant professor of internal medicine Al-zahra hospital, Isfahan university of medical sciences ٢ Level of consciousness is depressed Stuporous patients respond only to repeated
HeartCode PALS. PALS Actions Overview > Legend. Contents
 HeartCode PALS PALS Actions Overview > Legend Action buttons (round buttons) Clicking a round button initiates an action. Clicking this button, for example, checks the child s carotid pulse. Menu buttons
HeartCode PALS PALS Actions Overview > Legend Action buttons (round buttons) Clicking a round button initiates an action. Clicking this button, for example, checks the child s carotid pulse. Menu buttons
Last printed 9/15/2016 9:51 AM. Departmental/Patient Care Page 1 of 6. Origination Date: 6/18/2014. Grady Memorial Hospital Brain Death Policy
 Last printed 9/15/2016 9:51 AM Departmental/Patient Care Page 1 of 6 Grady Memorial Hospital Brain Death Policy Origination Date: 6/18/2014 Revision Date: 2/2/2015 I. POLICY STATEMENT: Mission statement:
Last printed 9/15/2016 9:51 AM Departmental/Patient Care Page 1 of 6 Grady Memorial Hospital Brain Death Policy Origination Date: 6/18/2014 Revision Date: 2/2/2015 I. POLICY STATEMENT: Mission statement:
Neurologic Determination of Death. Ian Ball FRCPC Regional Medical Lead for Organ Donation October 26, 2015
 Neurologic Determination of Death Ian Ball FRCPC Regional Medical Lead for Organ Donation October 26, 2015 Format Definition of Brain Death Historical Perspectives International consistency / inconsistency
Neurologic Determination of Death Ian Ball FRCPC Regional Medical Lead for Organ Donation October 26, 2015 Format Definition of Brain Death Historical Perspectives International consistency / inconsistency
Pronouncing brain death Contemporary practice and safety of the apnea test
 Pronouncing brain death Contemporary practice and safety of the apnea test Eelco F.M. Wijdicks, MD, PhD Alejandro A. Rabinstein, MD Edward M. Manno, MD John D. Atkinson, MD Address correspondence and reprint
Pronouncing brain death Contemporary practice and safety of the apnea test Eelco F.M. Wijdicks, MD, PhD Alejandro A. Rabinstein, MD Edward M. Manno, MD John D. Atkinson, MD Address correspondence and reprint
Legal Determination of Brain Death
 Research and Reviews Legal Determination of Brain Death JMAJ 54(6): 363 367, 2011 Yoshihiro NATORI* 1 Abstract Revisions to the Organ Transplant Act have made it possible for the organs of a brain-dead
Research and Reviews Legal Determination of Brain Death JMAJ 54(6): 363 367, 2011 Yoshihiro NATORI* 1 Abstract Revisions to the Organ Transplant Act have made it possible for the organs of a brain-dead
Simulation-Based Training In Brain Death Determination
 Yale University EliScholar A Digital Platform for Scholarly Publishing at Yale Yale Medicine Thesis Digital Library School of Medicine January 2015 Simulation-Based Training In Brain Death Determination
Yale University EliScholar A Digital Platform for Scholarly Publishing at Yale Yale Medicine Thesis Digital Library School of Medicine January 2015 Simulation-Based Training In Brain Death Determination
Alex Manara Regional Clinical Lead in Organ Donation South West Region Frenchay Hospital, Bristol
 Alex Manara Regional Clinical Lead in Organ Donation South West Region Frenchay Hospital, Bristol Diagnosis of Death Masterclass 2. Increased diagnosis of brain stem death 3. Increased donation after cardiac
Alex Manara Regional Clinical Lead in Organ Donation South West Region Frenchay Hospital, Bristol Diagnosis of Death Masterclass 2. Increased diagnosis of brain stem death 3. Increased donation after cardiac
Practice variability in brain death determination A call to action
 Practice variability in brain death determination A call to action Claire N. Shappell, BA Jeffrey I. Frank, MD Khalil Husari, MD Matthew Sanchez, BS Fernando Goldenberg, MD Agnieszka Ardelt, MD, PhD Correspondence
Practice variability in brain death determination A call to action Claire N. Shappell, BA Jeffrey I. Frank, MD Khalil Husari, MD Matthew Sanchez, BS Fernando Goldenberg, MD Agnieszka Ardelt, MD, PhD Correspondence
Ethical Dilemmas Brain Death and Overdose. Disclosures
 Ethical Dilemmas Brain Death and Overdose Ross W. Sullivan MD Director Toxicology Consultation Service Medical Toxicology Fellowship Director Assistant Professor Emergency Medicine SUNY Upstate Hospital,
Ethical Dilemmas Brain Death and Overdose Ross W. Sullivan MD Director Toxicology Consultation Service Medical Toxicology Fellowship Director Assistant Professor Emergency Medicine SUNY Upstate Hospital,
PRACTICE GUIDELINE. DEFINITIONS: Mild head injury: Glasgow Coma Scale* (GCS) score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8
 score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8") PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
Post-Cardiac Arrest Syndrome. MICU Lecture Series
 Post-Cardiac Arrest Syndrome MICU Lecture Series Case 58 y/o female collapses at home, family attempts CPR, EMS arrives and notes VF, defibrillation x 3 with return of spontaneous circulation, brought
Post-Cardiac Arrest Syndrome MICU Lecture Series Case 58 y/o female collapses at home, family attempts CPR, EMS arrives and notes VF, defibrillation x 3 with return of spontaneous circulation, brought
Post-Arrest Care: Beyond Hypothermia
 Post-Arrest Care: Beyond Hypothermia Damon Scales MD PhD Department of Critical Care Medicine Sunnybrook Health Sciences Centre University of Toronto Disclosures CIHR Physicians Services Incorporated Main
Post-Arrest Care: Beyond Hypothermia Damon Scales MD PhD Department of Critical Care Medicine Sunnybrook Health Sciences Centre University of Toronto Disclosures CIHR Physicians Services Incorporated Main
Pulse normal; brain dead
 Page 1 of 5 w w w. h a a r e t z. c o m Last update - 03:03 25/09/2007 Pulse normal; brain dead By Avinoam Reches There is no more difficult moment in medicine than when a doctor is required to inform
Page 1 of 5 w w w. h a a r e t z. c o m Last update - 03:03 25/09/2007 Pulse normal; brain dead By Avinoam Reches There is no more difficult moment in medicine than when a doctor is required to inform
Defining Death. Defining Death. Defining Death. Death at 50 & Organ Donation ORGAN TRANSPLANTATION. Dying (obvious) Death (not so obvious)
 Death (not so obvious)") Page 2 Page 4 Page 2 Page 4 Page 3 Page 5 Page 3 Page 5 Death at 50 & Organ Donation Dr. Mark Twite MA MB BChir FRCP Director of Congenital Cardiac Anesthesiology Associate Professor Department of Anesthesiology
Page 2 Page 4 Page 2 Page 4 Page 3 Page 5 Page 3 Page 5 Death at 50 & Organ Donation Dr. Mark Twite MA MB BChir FRCP Director of Congenital Cardiac Anesthesiology Associate Professor Department of Anesthesiology
Respiratory Care and Organ Donation
 Respiratory Care and Organ Donation Whitni Noyes, RN, OPTC Midwest Transplant Network Midwest Transplant Network CMS requires every accredited hospital to have an agreement with an OPO. MTN is the first
Respiratory Care and Organ Donation Whitni Noyes, RN, OPTC Midwest Transplant Network Midwest Transplant Network CMS requires every accredited hospital to have an agreement with an OPO. MTN is the first
Acute Respiratory Failure
 Acute Respiratory Failure For family, friends and caregivers of a patient with acute respiratory failure in the Medical Surgical Intensive Care Unit (MSICU) This brochure will give you more information
Acute Respiratory Failure For family, friends and caregivers of a patient with acute respiratory failure in the Medical Surgical Intensive Care Unit (MSICU) This brochure will give you more information
Prepared by : Bayan Kaddourah RN,MHM. GICU Clinical Instructor
 Mechanical Ventilation Prepared by : Bayan Kaddourah RN,MHM. GICU Clinical Instructor 1 Definition Is a supportive therapy to facilitate gas exchange. Most ventilatory support requires an artificial airway.
Mechanical Ventilation Prepared by : Bayan Kaddourah RN,MHM. GICU Clinical Instructor 1 Definition Is a supportive therapy to facilitate gas exchange. Most ventilatory support requires an artificial airway.
The updated guidelines for the determination of brain
 Developing a Standard Method for Apnea Testing in the Determination of Brain Death for Patients on Venoarterial Extracorporeal Membrane Oxygenation: A Pediatric Case Series Rima J. Jarrah, MD 1 ; Samuel
Developing a Standard Method for Apnea Testing in the Determination of Brain Death for Patients on Venoarterial Extracorporeal Membrane Oxygenation: A Pediatric Case Series Rima J. Jarrah, MD 1 ; Samuel
Foundation in Critical Care Nursing. Airway / Respiratory / Workbook
 Foundation in Critical Care Nursing Airway / Respiratory / Workbook Airway Anatomy: Please label the following: Tongue Larynx Epiglottis Pharynx Trachea Vertebrae Oesophagus Where is the ET (endotracheal)
Foundation in Critical Care Nursing Airway / Respiratory / Workbook Airway Anatomy: Please label the following: Tongue Larynx Epiglottis Pharynx Trachea Vertebrae Oesophagus Where is the ET (endotracheal)
Retraction Retracted: Clinical Brain Death with False Positive Radionuclide Cerebral Perfusion Scans
 Hindawi Publishing Corporation Volume 2016, Article ID 2057806, 1 page http://dx.doi.org/10.1155/2016/2057806 Retraction Retracted: Clinical Brain Death with False Positive Radionuclide Cerebral Perfusion
Hindawi Publishing Corporation Volume 2016, Article ID 2057806, 1 page http://dx.doi.org/10.1155/2016/2057806 Retraction Retracted: Clinical Brain Death with False Positive Radionuclide Cerebral Perfusion
Waiting for a Kidney. Objectives
 Waiting for a Kidney Department of Urologic Sciences Grand Rounds William Gourlay Christopher Nguan April 25, 2007 Objectives 1. review the waiting times for deceased-donor kidney transplants in BC and
Waiting for a Kidney Department of Urologic Sciences Grand Rounds William Gourlay Christopher Nguan April 25, 2007 Objectives 1. review the waiting times for deceased-donor kidney transplants in BC and
Diagnosis and Declaration of Death: A Dilemma
 Review Article Print ISSN: 2321-6379 Online ISSN: 2321-595X DOI: 10.17354/ijss/2016/392 Diagnosis and Declaration of Death: A Dilemma Niranjan Kumar Verma 1, Ashutosh Ranjan 2, Alok Kumar Singh 3 1 Professor
Review Article Print ISSN: 2321-6379 Online ISSN: 2321-595X DOI: 10.17354/ijss/2016/392 Diagnosis and Declaration of Death: A Dilemma Niranjan Kumar Verma 1, Ashutosh Ranjan 2, Alok Kumar Singh 3 1 Professor
Competency Title: Continuous Positive Airway Pressure
 Competency Title: Continuous Positive Airway Pressure Trainee Name: ------------------------------------------------------------- Title: ---------------------------------------------------------------
Competency Title: Continuous Positive Airway Pressure Trainee Name: ------------------------------------------------------------- Title: ---------------------------------------------------------------
Neurocritical Care Basics. Tapan Kavi, MD Christina Fox, RN
 Neurocritical Care Basics Tapan Kavi, MD Christina Fox, RN GOAL 1: DON T LET THE PATIENT DIE Not unique ACLS, ATLS, ENLS, other strategies common to all emergency medical care ABCs MORE not less important
Neurocritical Care Basics Tapan Kavi, MD Christina Fox, RN GOAL 1: DON T LET THE PATIENT DIE Not unique ACLS, ATLS, ENLS, other strategies common to all emergency medical care ABCs MORE not less important
Lecture Notes. Chapter 2: Introduction to Respiratory Failure
 Lecture Notes Chapter 2: Introduction to Respiratory Failure Objectives Define respiratory failure, ventilatory failure, and oxygenation failure List the causes of respiratory failure Describe the effects
Lecture Notes Chapter 2: Introduction to Respiratory Failure Objectives Define respiratory failure, ventilatory failure, and oxygenation failure List the causes of respiratory failure Describe the effects
Donation after Circulatory Determination of Death: Ethical Tensions
 Donation after Circulatory Determination of Death: Ethical Tensions Robert D. Truog, MD Frances Glessner Lee Professor of Medical Ethics, Anaesthesia, & Pediatrics, Harvard Medical School Director, Center
Donation after Circulatory Determination of Death: Ethical Tensions Robert D. Truog, MD Frances Glessner Lee Professor of Medical Ethics, Anaesthesia, & Pediatrics, Harvard Medical School Director, Center
ITLS Pediatric Provider Course Basic Pre-Test
 ITLS Pediatric Provider Course Basic Pre-Test 1. You arrive at the scene of a motor vehicle collision and are directed to evaluate a child who was in one of the vehicles. The patient appears to be a child
ITLS Pediatric Provider Course Basic Pre-Test 1. You arrive at the scene of a motor vehicle collision and are directed to evaluate a child who was in one of the vehicles. The patient appears to be a child
Variability of brain death determination guidelines in leading US neurologic institutions
 Variability of brain death determination guidelines in leading US neurologic institutions David M. Greer, MD, MA Panayiotis N. Varelas, MD, PhD Shamael Haque, DO, MPH Eelco F.M. Wijdicks, MD, PhD Address
Variability of brain death determination guidelines in leading US neurologic institutions David M. Greer, MD, MA Panayiotis N. Varelas, MD, PhD Shamael Haque, DO, MPH Eelco F.M. Wijdicks, MD, PhD Address
2/20/2018. Organ Donation after Cardiac Death. STA Introduction. Disclosure. The Need
 STA Introduction Organ Donation after Cardiac Death Geoffrey Funk, MD, FACS Associate Medical Director Southwest Transplant Alliance Disclosure Canadian by birth Three degrees from Texas A&M Trauma and
STA Introduction Organ Donation after Cardiac Death Geoffrey Funk, MD, FACS Associate Medical Director Southwest Transplant Alliance Disclosure Canadian by birth Three degrees from Texas A&M Trauma and
Deceased donor. Solid organ transplantation
 Deceased donor Solid organ transplantation Deceased donor donation process 1. Potential donor detection 2. Brain death diagnosis 3. Donor management 4. Organ allocation 5. Organ retrieval Brain death Irreversible
Deceased donor Solid organ transplantation Deceased donor donation process 1. Potential donor detection 2. Brain death diagnosis 3. Donor management 4. Organ allocation 5. Organ retrieval Brain death Irreversible
Legal Issues at the End of Life: Who Decides?
 Legal Issues at the End of Life: Who Decides? Dan Larriviere, MD, JD University of Virginia Schools of Law and Medicine Chair, American Academy of Neurology Ethics, Law and Humanities Committee My Perspective
Legal Issues at the End of Life: Who Decides? Dan Larriviere, MD, JD University of Virginia Schools of Law and Medicine Chair, American Academy of Neurology Ethics, Law and Humanities Committee My Perspective
DOI: /WNL.0b013e3181e242a8. This information is current as of June 8, 2010
 Evidence-based guideline update: Determining brain death in adults: Report of the Quality Standards Subcommittee of the American Academy of Neurology Eelco F.M. Wijdicks, Panayiotis N. Varelas, Gary S.
Evidence-based guideline update: Determining brain death in adults: Report of the Quality Standards Subcommittee of the American Academy of Neurology Eelco F.M. Wijdicks, Panayiotis N. Varelas, Gary S.
Airway Management and The Difficult Airway
 Airway Management and The Difficult Airway Gary McCalla, MD, FACEP Medical Director REACH Air Medical Services Services 1 It is not enough to do your best, unless you have prepared to be the best. -John
Airway Management and The Difficult Airway Gary McCalla, MD, FACEP Medical Director REACH Air Medical Services Services 1 It is not enough to do your best, unless you have prepared to be the best. -John
Test Bank Pilbeam's Mechanical Ventilation Physiological and Clinical Applications 6th Edition Cairo
 Instant dowload and all chapters Test Bank Pilbeam's Mechanical Ventilation Physiological and Clinical Applications 6th Edition Cairo https://testbanklab.com/download/test-bank-pilbeams-mechanical-ventilation-physiologicalclinical-applications-6th-edition-cairo/
Instant dowload and all chapters Test Bank Pilbeam's Mechanical Ventilation Physiological and Clinical Applications 6th Edition Cairo https://testbanklab.com/download/test-bank-pilbeams-mechanical-ventilation-physiologicalclinical-applications-6th-edition-cairo/
Session 15. Brain Death, Permanent Vegetative State, and Medical Futility
 American Academy of Pediatrics Bioethics Resident Curriculum: Case-Based Teaching Guides Session 15. Brain Death, Permanent Vegetative State, and Medical Futility Ásdís Finnsdóttir Wagner, DO; Julio Quezada,
American Academy of Pediatrics Bioethics Resident Curriculum: Case-Based Teaching Guides Session 15. Brain Death, Permanent Vegetative State, and Medical Futility Ásdís Finnsdóttir Wagner, DO; Julio Quezada,
Capnography: The Most Vital of Vital Signs. Tom Ahrens, PhD, RN, FAAN Research Scientist, Barnes-Jewish Hospital, St. Louis, MO May, 2017
 Capnography: The Most Vital of Vital Signs Tom Ahrens, PhD, RN, FAAN Research Scientist, Barnes-Jewish Hospital, St. Louis, MO May, 2017 Assessing Ventilation and Blood Flow with Capnography Capnography
Capnography: The Most Vital of Vital Signs Tom Ahrens, PhD, RN, FAAN Research Scientist, Barnes-Jewish Hospital, St. Louis, MO May, 2017 Assessing Ventilation and Blood Flow with Capnography Capnography
Ancillary Testing in Death
 Ancillary Testing in Death MICHAËL CHASSÉ, MD, PHD, FRCPC ASSISTANT PROFESSOR, DEPARTMENT OF ANESTHESIOLOGY AND CRITICAL CARE, UNIVERSITÉ LAVAL INTENSIVIST, DEPARTMENT OF ANESTHESIOLOGY, DIVISION OF CRITICAL
Ancillary Testing in Death MICHAËL CHASSÉ, MD, PHD, FRCPC ASSISTANT PROFESSOR, DEPARTMENT OF ANESTHESIOLOGY AND CRITICAL CARE, UNIVERSITÉ LAVAL INTENSIVIST, DEPARTMENT OF ANESTHESIOLOGY, DIVISION OF CRITICAL
Waitin In The Wings. Esophageal/Tracheal Double Lumen Airway (Combitube ) Indications and Use for the Pre-Hospital Provider
 Indications and Use for the Pre-Hospital Provider") Waitin In The Wings Esophageal/Tracheal Double Lumen Airway (Combitube ) Indications and Use for the Pre-Hospital Provider 1 CombiTube Kit General Description The CombiTube is A double-lumen tube with
Waitin In The Wings Esophageal/Tracheal Double Lumen Airway (Combitube ) Indications and Use for the Pre-Hospital Provider 1 CombiTube Kit General Description The CombiTube is A double-lumen tube with
Capnography for Pediatric Procedural Sedation Learning Module Last revised: February 18, 2014
 Capnography for Pediatric Procedural Sedation Learning Module Last revised: February 18, 2014 Capnography 40 Non-invasive device that continually monitors EtCO 2 While pulse oximetry measures oxygen saturation,
Capnography for Pediatric Procedural Sedation Learning Module Last revised: February 18, 2014 Capnography 40 Non-invasive device that continually monitors EtCO 2 While pulse oximetry measures oxygen saturation,
Brain Death: An Investigation of Current Controversies
 The University of Akron IdeaExchange@UAkron Honors Research Projects The Dr. Gary B. and Pamela S. Williams Honors College Spring 2018 Brain Death: An Investigation of Current Controversies Meile Moore
The University of Akron IdeaExchange@UAkron Honors Research Projects The Dr. Gary B. and Pamela S. Williams Honors College Spring 2018 Brain Death: An Investigation of Current Controversies Meile Moore
Introduction to Emergency Medical Care 1
 Introduction to Emergency Medical Care 1 OBJECTIVES 8.1 Define key terms introduced in this chapter. Slides 12 15, 21, 24, 31-34, 39, 40, 54 8.2 Describe the anatomy and physiology of the upper and lower
Introduction to Emergency Medical Care 1 OBJECTIVES 8.1 Define key terms introduced in this chapter. Slides 12 15, 21, 24, 31-34, 39, 40, 54 8.2 Describe the anatomy and physiology of the upper and lower
University of Wisconsin - Madison Cardiovascular Medicine Fellowship Program UW CICU Rotation Goals and Objectives
 Background: The field of critical care cardiology has evolved considerably over the past 2 decades. Contemporary critical care cardiology is increasingly focused on the management of patients with advanced
Background: The field of critical care cardiology has evolved considerably over the past 2 decades. Contemporary critical care cardiology is increasingly focused on the management of patients with advanced
Pediatric Advanced Life Support
 Pediatric Advanced Life Support Pediatric Chain of Survival Berg M D et al. Circulation 2010;122:S862-S875 Prevention Early cardiopulmonary resuscitation (CPR) Prompt access to the emergency response system
Pediatric Advanced Life Support Pediatric Chain of Survival Berg M D et al. Circulation 2010;122:S862-S875 Prevention Early cardiopulmonary resuscitation (CPR) Prompt access to the emergency response system
Handling Common Problems & Pitfalls During. Oxygen desaturation in patients receiving mechanical ventilation ACUTE SEVERE RESPIRATORY FAILURE
 Handling Common Problems & Pitfalls During ACUTE SEVERE RESPIRATORY FAILURE Pravit Jetanachai, MD QSNICH Oxygen desaturation in patients receiving mechanical ventilation Causes of oxygen desaturation 1.
Handling Common Problems & Pitfalls During ACUTE SEVERE RESPIRATORY FAILURE Pravit Jetanachai, MD QSNICH Oxygen desaturation in patients receiving mechanical ventilation Causes of oxygen desaturation 1.
Pediatric emergencies (SHOCK & COMA) Dr Mubarak Abdelrahman Assistant Professor Jazan University
 Dr Mubarak Abdelrahman Assistant Professor Jazan University") Pediatric emergencies (SHOCK & COMA) Dr Mubarak Abdelrahman Assistant Professor Jazan University SHOCK Definition: Shock is a syndrome = inability to provide sufficient oxygenated blood to tissues. Oxygen
Pediatric emergencies (SHOCK & COMA) Dr Mubarak Abdelrahman Assistant Professor Jazan University SHOCK Definition: Shock is a syndrome = inability to provide sufficient oxygenated blood to tissues. Oxygen
Michigan Pediatric Cardiac Protocols. Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS
 Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS Pediatric Asystole Section 4-1 Pediatric Bradycardia Section 4-2 Pediatric Cardiac Arrest General Section 4-3 Pediatric Narrow Complex Tachycardia
Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS Pediatric Asystole Section 4-1 Pediatric Bradycardia Section 4-2 Pediatric Cardiac Arrest General Section 4-3 Pediatric Narrow Complex Tachycardia
Approximately five minutes after a terrible car accident
 Report on Progress 2015 Disorders of Consciousness: Brain Death, Coma, and the Vegetative and Minimally Conscious States Thomas I. Cochrane M.D., MBA, Neurology, Brigham & Women s Hospital Michael A. Williams,
Report on Progress 2015 Disorders of Consciousness: Brain Death, Coma, and the Vegetative and Minimally Conscious States Thomas I. Cochrane M.D., MBA, Neurology, Brigham & Women s Hospital Michael A. Williams,
Standardize comprehensive care of the patient with severe traumatic brain injury
 Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Management of Patients with Severe Traumatic Brain Injury (GCS < 9) ADULT Practice Management Guideline Contact: Trauma
Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Management of Patients with Severe Traumatic Brain Injury (GCS < 9) ADULT Practice Management Guideline Contact: Trauma
ITLS Pediatric Provider Course Advanced Pre-Test
 ITLS Pediatric Provider Course Advanced Pre-Test 1. You arrive at the scene of a motor vehicle crash and are directed to evaluate a child who was in one of the vehicles. The patient appears to be a child
ITLS Pediatric Provider Course Advanced Pre-Test 1. You arrive at the scene of a motor vehicle crash and are directed to evaluate a child who was in one of the vehicles. The patient appears to be a child
UNIT VI: ACID BASE IMBALANCE
 UNIT VI: ACID BASE IMBALANCE 1 Objectives: Review the physiological mechanism responsible to regulate acid base balance in the body i.e.: Buffers (phosphate, hemoglobin, carbonate) Renal mechanism Respiratory
UNIT VI: ACID BASE IMBALANCE 1 Objectives: Review the physiological mechanism responsible to regulate acid base balance in the body i.e.: Buffers (phosphate, hemoglobin, carbonate) Renal mechanism Respiratory
Guslihan Dasa Tjipta Division of Perinatology Department of Child Health Medical School University of Sumatera Utara
 Guslihan Dasa Tjipta Division of Perinatology Department of Child Health Medical School University of Sumatera Utara 1 Definition Perinatal asphyxia is a fetus/newborn, due to: is an insult to the Lack
Guslihan Dasa Tjipta Division of Perinatology Department of Child Health Medical School University of Sumatera Utara 1 Definition Perinatal asphyxia is a fetus/newborn, due to: is an insult to the Lack
Chapter 8. Bellringer. Write as many words or phrases that describe the circulatory system as you can. Lesson 5 The Circulatory System
 Lesson 5 The Circulatory System Bellringer Write as many words or phrases that describe the circulatory system as you can. Lesson 5 The Circulatory System Objectives Trace the path of blood through the
Lesson 5 The Circulatory System Bellringer Write as many words or phrases that describe the circulatory system as you can. Lesson 5 The Circulatory System Objectives Trace the path of blood through the
Examination Approach. Examination Approach. Case 1: Mental Status. The Neurological Exam In the ICU: High Yield Techniques 5/8/2015
 The Neurological Exam In the ICU: High Yield Techniques Examination Approach Two types of neurologic examinations 1. Screening Examination 2. Testing Hypotheses Select high-yield tests and techniques S.
The Neurological Exam In the ICU: High Yield Techniques Examination Approach Two types of neurologic examinations 1. Screening Examination 2. Testing Hypotheses Select high-yield tests and techniques S.
Bilaga 4 till rapport 1 (17)
") Bilaga 4 Tabeller, beskrivning av studier Bilaga 4 till rapport 1 (17) Bilddiagnostik vid misstanke om total hjärninfarkt en systematisk litteraturöversikt, rapport 282 (2018) SBU Statens beredning för
Bilaga 4 Tabeller, beskrivning av studier Bilaga 4 till rapport 1 (17) Bilddiagnostik vid misstanke om total hjärninfarkt en systematisk litteraturöversikt, rapport 282 (2018) SBU Statens beredning för
INTRODUCTION The effect of CPAP works on lung mechanics to improve oxygenation (PaO 2
 2 Effects of CPAP INTRODUCTION The effect of CPAP works on lung mechanics to improve oxygenation (PaO 2 ). The effect on CO 2 is only secondary to the primary process of improvement in lung volume and
2 Effects of CPAP INTRODUCTION The effect of CPAP works on lung mechanics to improve oxygenation (PaO 2 ). The effect on CO 2 is only secondary to the primary process of improvement in lung volume and
Pediatric Shock. Hypovolemia. Sepsis. Most common cause of pediatric shock Small blood volumes (80cc/kg)
") Critical Concepts: Shock Inadequate peripheral perfusion where oxygen delivery does not meet metabolic demand Adult vs Pediatric Shock - Same causes/different frequencies Pediatric Shock Hypovolemia Most
Critical Concepts: Shock Inadequate peripheral perfusion where oxygen delivery does not meet metabolic demand Adult vs Pediatric Shock - Same causes/different frequencies Pediatric Shock Hypovolemia Most
Causes and Consequences of Respiratory Centre Depression and Hypoventilation
 Causes and Consequences of Respiratory Centre Depression and Hypoventilation Lou Irving Director Respiratory and Sleep Medicine, RMH louis.irving@mh.org.au Capacity of the Respiratory System At rest During
Causes and Consequences of Respiratory Centre Depression and Hypoventilation Lou Irving Director Respiratory and Sleep Medicine, RMH louis.irving@mh.org.au Capacity of the Respiratory System At rest During
Neonatal Life Support Provider (NLSP) Certification Preparatory Materials
 Certification Preparatory Materials") Neonatal Life Support Provider (NLSP) Certification Preparatory Materials NEONATAL LIFE SUPPORT PROVIDER (NRP) CERTIFICATION TABLE OF CONTENTS NEONATAL FLOW ALGORITHM.2 INTRODUCTION 3 ANTICIPATION OF RESUSCITATION
Neonatal Life Support Provider (NLSP) Certification Preparatory Materials NEONATAL LIFE SUPPORT PROVIDER (NRP) CERTIFICATION TABLE OF CONTENTS NEONATAL FLOW ALGORITHM.2 INTRODUCTION 3 ANTICIPATION OF RESUSCITATION
뇌사의진단과진단을위한보조적검사 서울아산병원신경과. The Diagnosis and Ancillary Tests of Brain Death. Kim, Cheon-Sik
 대한임상검사학회지 : 36 권제 1 호, 64-68, 2004 뇌사의진단과진단을위한보조적검사 김천식 The Diagnosis and Ancillary Tests of Brain Death Kim, Cheon-Sik Department of Clinical Neurosciences, Asan Medical Center Brain death is defined
대한임상검사학회지 : 36 권제 1 호, 64-68, 2004 뇌사의진단과진단을위한보조적검사 김천식 The Diagnosis and Ancillary Tests of Brain Death Kim, Cheon-Sik Department of Clinical Neurosciences, Asan Medical Center Brain death is defined
How to Diagnose Brainstem Death. Akhmad Imron Dept./SMF Bedah Saraf FK.Unpad/RSHS
 How to Diagnose Brainstem Death Akhmad Imron Dept./SMF Bedah Saraf FK.Unpad/RSHS RSUP Dr. Hasan Sadikin Bandung Jalan Pasteur No. 38 Bandung telephone.62-022-2034953/57 Fax.62-022-2032216 Diagnosis of
How to Diagnose Brainstem Death Akhmad Imron Dept./SMF Bedah Saraf FK.Unpad/RSHS RSUP Dr. Hasan Sadikin Bandung Jalan Pasteur No. 38 Bandung telephone.62-022-2034953/57 Fax.62-022-2032216 Diagnosis of
Donation after Brain-Stem Death DBD
 Donation after Brain-Stem Death DBD Dr Peter Hall Dr Dale Gardiner Dr Gerlinde Mandersloot 22 nd May 2013 1 YORKSHIRE Regional Data Dr Peter Hall CLOD Calderdale and Huddersfield NHS Trust 2 Session Objectives
Donation after Brain-Stem Death DBD Dr Peter Hall Dr Dale Gardiner Dr Gerlinde Mandersloot 22 nd May 2013 1 YORKSHIRE Regional Data Dr Peter Hall CLOD Calderdale and Huddersfield NHS Trust 2 Session Objectives
Anesthesia Monitoring
 Anesthesia Monitoring Horatiu V. Vinerean, DVM, DACLAM Anesthesia Monitoring Anesthesia can be divided into four progressive phases. The signs relating to a certain phase are based upon the presence or
Anesthesia Monitoring Horatiu V. Vinerean, DVM, DACLAM Anesthesia Monitoring Anesthesia can be divided into four progressive phases. The signs relating to a certain phase are based upon the presence or
Hypothermia in Neonates with HIE TARA JENDZIO, DNP(C), RN, RNC-NIC
, RN, RNC-NIC") Hypothermia in Neonates with HIE TARA JENDZIO, DNP(C), RN, RNC-NIC Objectives 1. Define Hypoxic-Ischemic Encephalopathy (HIE) 2. Identify the criteria used to determine if an infant qualifies for therapeutic
Hypothermia in Neonates with HIE TARA JENDZIO, DNP(C), RN, RNC-NIC Objectives 1. Define Hypoxic-Ischemic Encephalopathy (HIE) 2. Identify the criteria used to determine if an infant qualifies for therapeutic
NEONATAL HYPOXIC-ISCHAEMIC ENCEPHALOPATHY (HIE) & COOLING THERAPY
 & COOLING THERAPY") Background NEONATAL HYPOXIC-ISCHAEMIC ENCEPHALOPATHY (HIE) & COOLING THERAPY A perinatal hypoxic-ischaemic insult may present with varying degrees of neonatal encephalopathy, neurological disorder and
Background NEONATAL HYPOXIC-ISCHAEMIC ENCEPHALOPATHY (HIE) & COOLING THERAPY A perinatal hypoxic-ischaemic insult may present with varying degrees of neonatal encephalopathy, neurological disorder and
Hospital Resource and Clinical Management Guidelines for Hospital Healthcare Providers When Routine Critical Care Resources Are Not Available
 Hospital Resource and Clinical Management Guidelines for Hospital Healthcare Providers When Routine Critical Care Resources Are Not Available Medical College of Wisconsin Center for Medical Incident Management
Hospital Resource and Clinical Management Guidelines for Hospital Healthcare Providers When Routine Critical Care Resources Are Not Available Medical College of Wisconsin Center for Medical Incident Management
Nursing the critical care patient part 1: triage
 Nursing the critical care patient part 1: triage EJCAP 26(3) Autumn 2016 P 51 Commissioned paper* Nursing the critical care patient part 1: triage Katherine Howie 1 SUMMARY Good nursing of the emergency
Nursing the critical care patient part 1: triage EJCAP 26(3) Autumn 2016 P 51 Commissioned paper* Nursing the critical care patient part 1: triage Katherine Howie 1 SUMMARY Good nursing of the emergency
Case 1. Case 5/30/2013. Traumatic Brain Injury : Review, Update, and Controversies
 Case 1 Traumatic Brain Injury : Review, Update, and Controversies Shirley I. Stiver MD, PhD 32 year old male s/p high speed MVA Difficult extrication Intubated at scene Case BP 75 systolic / palp GCS 3
Case 1 Traumatic Brain Injury : Review, Update, and Controversies Shirley I. Stiver MD, PhD 32 year old male s/p high speed MVA Difficult extrication Intubated at scene Case BP 75 systolic / palp GCS 3
Facilitating EndotracheaL Intubation by Laryngoscopy technique and Apneic Oxygenation Within the Intensive Care Unit (FELLOW)
") Facilitating EndotracheaL Intubation by Laryngoscopy technique and Apneic Oxygenation Within the Intensive Data Analysis Plan: Apneic Oxygenation vs. No Apneic Oxygenation Background Critically ill patients
Facilitating EndotracheaL Intubation by Laryngoscopy technique and Apneic Oxygenation Within the Intensive Data Analysis Plan: Apneic Oxygenation vs. No Apneic Oxygenation Background Critically ill patients
Stayin Alive: Pediatric Advanced Life Support (PALS) Updated Guidelines
 Updated Guidelines") Stayin Alive: Pediatric Advanced Life Support (PALS) Updated Guidelines Margaret Oates, PharmD, BCPPS Pediatric Critical Care Specialist GSHP Summer Meeting July 16, 2016 Disclosures I have nothing to
Stayin Alive: Pediatric Advanced Life Support (PALS) Updated Guidelines Margaret Oates, PharmD, BCPPS Pediatric Critical Care Specialist GSHP Summer Meeting July 16, 2016 Disclosures I have nothing to
WHEN IT S A MATTER OF LIFE AND DEATH THE QUESTIONS YOU SHOULD ASK EDUCATION FUND
 WHEN IT S A MATTER OF LIFE AND DEATH THE QUESTIONS YOU SHOULD ASK EDUCATION FUND WHAT QUESTIONS SHOULD YOU ASK YOUR DOCTOR IN LIFE-OR-DEATH SITUATIONS? Your mother has a stroke and is rushed to the hospital.
WHEN IT S A MATTER OF LIFE AND DEATH THE QUESTIONS YOU SHOULD ASK EDUCATION FUND WHAT QUESTIONS SHOULD YOU ASK YOUR DOCTOR IN LIFE-OR-DEATH SITUATIONS? Your mother has a stroke and is rushed to the hospital.