Fall 2014 Meeting October 3-4, 2014 Overview of Pediatric Sleep Medicine
|
|
|
- Amberlynn Webb
- 5 years ago
- Views:
Transcription
1 Fall 2014 Meeting October 3-4, 2014 Overview of Pediatric Sleep Medicine Jason Coles MD Spectrum Medical Group Helen DeVos Children s Hospital
2 Conflict of Interest Disclosures for Speakers X 1. I do not have any relationships with any entities producing, marketing, re-selling, or distributing health care goods or services consumed by, or used on, patients, OR 2. I have the following relationships with entities producing, marketing, re-selling, or distributing health care goods or services consumed by, or used on, patients: Type of Potential Conflict Details of Potential Conflict Grant/Research Support Consultant Speakers Bureaus Financial support Other The material presented in this lecture has no relationship with any of these potential conflicts, OR 4. This talk presents material that is related to one or more of these potential conflicts, and the following objective references are provided as support for this lecture:
3 Objectives At the conclusion of this course, attendees should be able to Understand normal sleep development and patterns in childhood Understand common pediatric sleep disorders Understand important differences between children and adults regarding conducting, scoring and interpreting sleep studies Understand strategies to make a sleep study experience child-friendly, and to optimize study quality
4 Development of Sleep Sleep and wake can first be determined in fetus around 28 weeks gestation weeks gestation Active (REM) and Quiet (non-rem) sleep can be distinguished Quite Sleep (non-rem) characterized first by trace alternant EEG pattern Pattern persists until about 4 weeks after birth Develops into High Voltage Slow (HVS) activity more mature pattern of Quiet Sleep in infants
5 Trace alternant EEG pattern Alternating 3-8 second patterns of high amplitude slow waves and low amplitude mixed frequency activity Sleep in the child: normal and abnormal. AACP board review presentation, Lee Brooks MD
6 Infant Sleep Stages Sleep scored as Active (REM), Quite (NREM) or Indeterminate Scored based on multiple variables Active (REM) Quite (NREM) Behavior Smiles, grimaces, limb movements Rare movement EEG Low voltage, mixed frequency Trace alternant; high voltage slow waves EMG tone Low High Respirations Irregular Regular Eye Movements Present, rapid Absent Grigg-Damberger M, Gozal D, Marcus CL, et al. The visual scoring of sleep and arousal in infants and children. J Clin Sleep Med 2007; 3:201-40
7 Infant Sleep Spindles develop 2-3 months K-complexes and Slow Wave activity 4-6 months N1, N2, N3, REM can be scored once these EEG patterns distinguished Pediatric study rather than infant Nearly 50% of sleep is REM at birth Gradually decreases until age 3-4 when it stabilizes at 25% (same as adults) N3 sleep gradually decreases throughout lifetime
8 Changes to sleep architecture Higher density of N3 and fewer awakenings likely account for increased parasomnias in children Sleep Cycles min at birth 75 min at 2 years 90 min at 6 years Mindell and Owens. A Clinical Guide to Pediatric Sleep 2010
9 Normal Patterns Newborns (0-2 months) Average hours sleep, with wide variability No established Circadian pattern Sleep periods separated by 1-2 hours of wake Breast fed babies sleep for shorter periods Infants (2-12 months) Circadian patterns start to form 9-10 hours at night plus 3-4 hours of naps = hours overall By 1 year, number of naps decrease to 1-2/day
10 Normal Patterns Toddlers (1-3 years) Average hours at night plus 2-3 hours in naps = hours overall By 18 months down to 1 nap per day Nearly half stop napping by age 3 Preschool (3-5 years) 9-10 hours of sleep at night Only 15% of 5 year olds still take a nap
11 Normal Patterns School age (6-12 years) Average 9-10 hours of sleep Adolescents (12-18 years) hours recommended But, average is only hours at night 2-hour sleep debt accumulates per night across the school week Most parents think their teens are getting enough sleep
12 Common Pediatric Sleep Disorders Insomnia Problems going to bed Night wakings Delayed sleep phase Obstructive sleep apnea Restless legs syndrome (Willis-Ekbom Disease) and Periodic limb movement disorder Parasomnias
13 Insomnia
14 Behavioral Pediatric Insomnia: Night wakings Sleep onset association disorder How we fall asleep is learned Physical parental presence can become part of the ritual Normal awakenings occur multiple times a night Child doesn t know how to fall back asleep without his parents, so seeks them out by any means necessary Multiple awakenings per night, waking parents each time
15 Sleep Onset Association Disorder Treatment Behavioral interventions Educate parents Replace physical parental presence with new sleep onset associations that will be present when child wakes at night Parents leave room before child falls asleep If child cries, frequent checks and reassurance, but with increasing intervals If child comes out of room, take right back and tuck back in without unnecessary conversation, arguing, etc Child not allowed to sleep with parents
16 Behavioral Insomnia: Problems going to bed Limit Setting Sleep Disorder Child is physiologically able to fall asleep, but doesn t stay in bed long enough Refusals Stalling Repeated demands Create any reason (and many reasons) to stay up Parents intermittently or eventually give in, reinforcing behavior Child gains attention and special time from parents (even if arguing)
17 Limit Setting Sleep Disorder Comes out of room repeatedly because child can t fall asleep because Thirsty Hungry Afraid of dark, monsters, being alone Stomach hurts Not tired, etc Treatment: Behavioral Interventions Set clear, 100% predictable, 100% consistent limits Bed time is strictly enforced, following an enforced wind down period beginning predictably 1-2 hours before bed Do not give in to protests or requests after bed time Decide who is going to win
18 Delayed Sleep Phase Syndrome Sleep physiology is completely normal, but timing of sleep cycle is misaligned with school/daytime responsibilities Not ready or able to fall asleep early at night Body not ready to wake up for school most sleepy during first part of the day Total sleep becomes inadequate, causing cumulative sleep deprivation; trying to catch up on weekends If allowed to get enough total sleep, feels normal Runs in families Develops in adolescence most adolescents will have at least a mild shift in circadian rhythm
19 Delayed Sleep Phase Syndrome Treatment Education Properly timed melatonin in the evenings Bright light exposure in the mornings Consistent schedule 7 days a week
20 Obstructive Sleep Apnea
21 Obstructive Sleep Apnea Epidemiology 8% children snore frequently, according to parents Always snoring 1.5-6% 1-4% school age children have OSA based on PSG Peak age 2-8 years Corresponds to the peak of lymphoid hyperplasia, and adenotonsillar hypertrophy Boys and girls equal until adolescence, when boys outnumber girls (similar to adult patterns) More frequent in African-American and Asian children
22 OSA Risk Factors Enlarged tonsils and/or adenoids Allergies Facial abnormalities Small chin Narrow hard palate Cleft palate repair Down syndrome Obesity Neuro-Muscular disorders
23 OSA Night Symptoms Snoring most common complaint With or without snorting, choking, gasping, or witnessed pauses in breathing Restless sleep (tossing and turning) Sleeping in strange positions (extending neck to open airway) Sweats Bed wetting
24 OSA Daytime Symptoms Daytime sleepiness not present in most kids (less than 10%) Behavioral problems Inattention Hyperactivity Irritability Decreased school performance Morning headaches
25 OSA Medical Consequences Hypertension Pulmonary hypertension Failure to thrive (slow growth) Heart failure
26 Diagnosis of OSA Clinical history cannot predict presence or absence of childhood OSA Severe OSA can be present even with soft snoring and minimal symptoms Physical examination is often normal Degree of tonsillar hypertrophy does not correlate with presence of OSA Parental perception varies widely Sleep study is needed
27 OSA Treatments Adenotonsillectomy Recommended 1 st line treatment by American Academy of Pediatrics Large study* in 2010 demonstrated complete resolution of OSA in only 27% of kids, though most were improved High AHI, older age, obesity and asthma predict failure Rapid maxillary expansion (orthodontic) Medical management of allergies and GERD CPAP/BiPAP Craniofacial surgery Tracheostomy *Bhattacharjee et al. Adenotonsillectomy Outcomes in Treatment of Obstructive Sleep Apnea in Children. Am J Crit Care Med 2010; 182:
28 Central Sleep Apnea Usually periodic breathing Can be a sign of structural brain abnormalities Arnold Chiari malformation If significant, MRI brain is recommended Treatment protocols for central apnea are not defined Treat OSA if present (start with T&A) Neurosurgical consultation for Chiari malformation Oxygen CPAP BiPAP ASV/APAPs

29 12 year old with brain stem tumor

30 Trial of BiPAP with backup rate 12

31 Trial of BiPAP ASV
32 Restless Legs and PLMs
33 Restless Legs and Periodic Limb Movements Restless legs syndrome Clinical diagnosis Uncomfortable sensations in the legs accompanied by urge to move them Often described as growing pains Worse at night or when inactive (car rides) Periodic Limb Movement Disorder Identified PLMs on polysomnography Brief ( seconds) repetitive limb movements, not in association with OSA For children, >5 per hour required AND associated with sleep or daytime symptoms

34 Periodic Limb Movements
35 RLS and PLMD 70-90% of adults with RLS also have PLMs (not studied in kids) Share underlying abnormalities in the brain s dopamine system Thought to be under-recognized generally
36 Pediatric RLS Present in 1-6% of kids Equal rates in boys and girls (unlike adults) Possibly life long and severe Risk factors Family history Sleep deprivation or poor sleep hygiene Caffeine Antihistamines Antidepressants Iron deficiency (ferritin < 50 ng/ml) Present in 75% of kids with RLS
37 Pediatric PLMs Same link with iron deficiency and antidepressants 50% of kids with PLMs also have OSA on sleep study Treatment of OSA resolves the PLMs in 50% of these kids
38 Treatments for RLS/PLMD Replace iron if ferritin is low Stop or reduce antidepressants Avoid caffeine Good sleep hygiene Treat OSA if present Exercise, stretching, massage Medications only approved for adults
39 Parasomnias
40 Parasomnias Episodic disorders in sleep Not resulting in complaint of excessive sleepiness or insomnia Arousal disorders REM related disorders Sleep-wake transition disorders
41 Arousal Disorders Partial arousal from deep non-rem sleep Occurs typically first third of the night Difficult to wake up No recall of event Worsened by Sleep deprivation Sleep fragmentation (sleep apnea, caffeine) Psychological factors Anxiety, stress, change
42 Arousal Disorders Somnambulism 40% of kids at least once 5% frequently Outgrown usually by age 15 Dangerous Sleep Terrors Abrupt onset Blood curdling scream or cry Confusion, agitation, tachycardia Not associated with dream Confusional arousals
43 Arousal Disorders Treatment Reassurance Insure safety!! Locks, door alarms, gates Good sleep hygiene Minimize triggers (sleep apnea) Medications (benzodiazepines)
44 REM Associated Disorders Nightmares Last 3 rd of night Remembers dream, able to fully awaken REM Behavioral Disorder Sleep paralysis
45 Sleep-Wake Transition Disorders Rhythmic Movement Disorders Head banging, Body rocking as way to self-sooth and transition to sleep 2/3 of normal children Usually ends by age 4 Hypnic Jerks Occurs with transition to N % or normal people Somniloquy very common
46 Pediatric Polysomnography Must be child oriented. Ergonomically pediatric. Techs must be experienced, motivated to work with children, and very patient! Can be performed on any child of any age Most children tolerate it well Parent must accompany child for entire evening Interpretation and scoring different from adult criteria Children have shorter and fewer events, and higher proportion of partial obstructions: scoring requires great care
47 Getting better studies Parents are the experts for their child; use them Try to adapt to family routines Explain everything to parents to keep them involved Environment should resemble a child s room Quiet, appropriate room temperature Age appropriate toys, pictures, books Parental accommodations should be comfortable Room child-proofed Quality of study directly dependent on the skill of the technologist Preferably experienced and enjoys working with kids Set up should be fun Distraction Adequate staffing liberal use of 1:1 especially for set up Document everything!
48 PSG Interpretation Adult criteria do not apply to children 80% of kids with clinically significant OSA would be missed Cutoffs continue to be debated, but abnormal if AHI>1 (HDVCH uses AHI 1.5 or OAI of 1.0) EtCO2 > 45 mmhg for >60% of TST (some researchers suggest this cutoff should be as low as 10%) Pediatric respiratory scoring rules may be used until age 18 Adult respiratory scoring rules may be used starting at age 13
49 Pediatric PSG Scoring Sleep Stages Wakefulness defined by dominant posterior rhythm gradually increasing in frequency with age until full alpha rhythm of 8 Hz first seen at ages 1-3 Stages N1, N2, N3, and REM similar rules as adults, can be scored as soon as K-complexes and Spindles seen (2-6 months) N (NREM), REM, and Indeterminate scored if <6 months, and no N2 Cardiac Events Heart rates 2 Standard Deviations from the mean, based on age normative values
50 Respiratory Monitoring Apneas detected by thermal sensor Alternate (if not reliable) nasal pressure transducer Hypopneas detected by nasal pressure transducer Alternate oronasal thermal sensor Alveolar hypoventilation detected by either transcutaneous (Tc) or end-tidal (ET) PCO2 Crucial to obtain a plateau in the EtCO2 waveform for the signal to be considered valid Transcutaneous PCO2 not always reliable Et PCO2 will yield inaccurately low values if Nasal obstruction Nasal secretions Obligate mouth breathers Receiving supplemental oxygen
51 Scoring Respiratory Events Obstructive Apnea Central Apnea Adults 10 seconds with respiratory effort 10 seconds with no respiratory effort Children 2 missed breaths with respiratory effort 20 seconds or 2 missed breaths with arousal or 3% desaturation Hypopnea Hypoventilation Periodic Breathing 10 seconds 30% drop in nasal pressure with arousal or 3% desat PCO2 > 55 mmhg for 10 minutes Cheyne-Stokes breathing pattern 2 breaths 30% drop in nasal pressure with arousal or 3% desat PCO2 > 50 mmhg for > 25% TST 3 episodes of CA lasting >3 seconds, separated by 20 seconds or normal breathing AASM Manual for the Scoring of Sleep and Associated Events Version
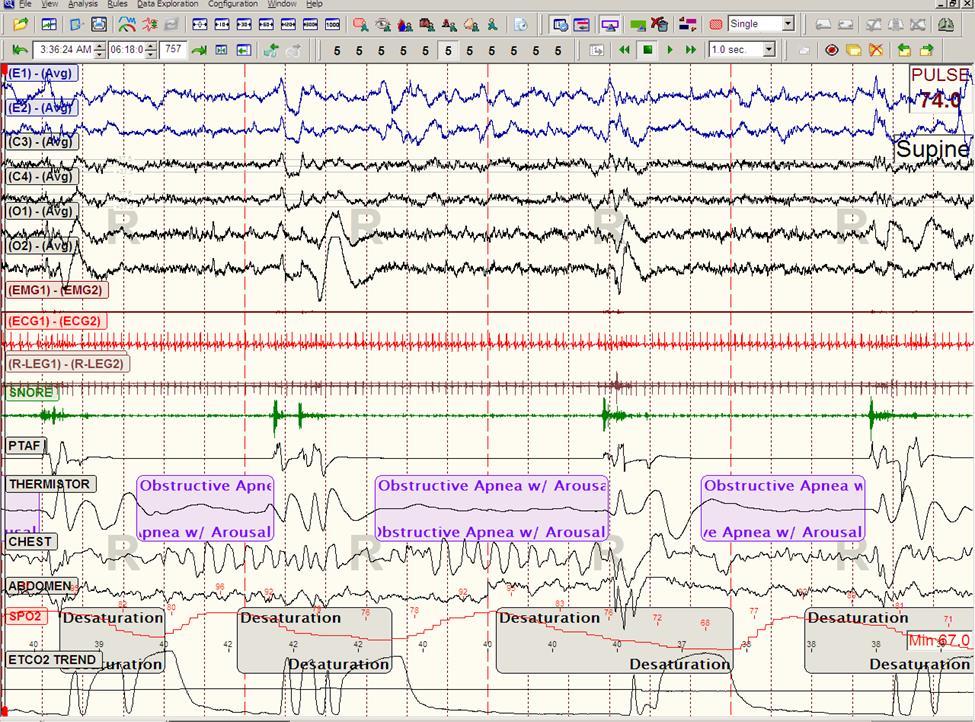
52 Obstructive Apneas
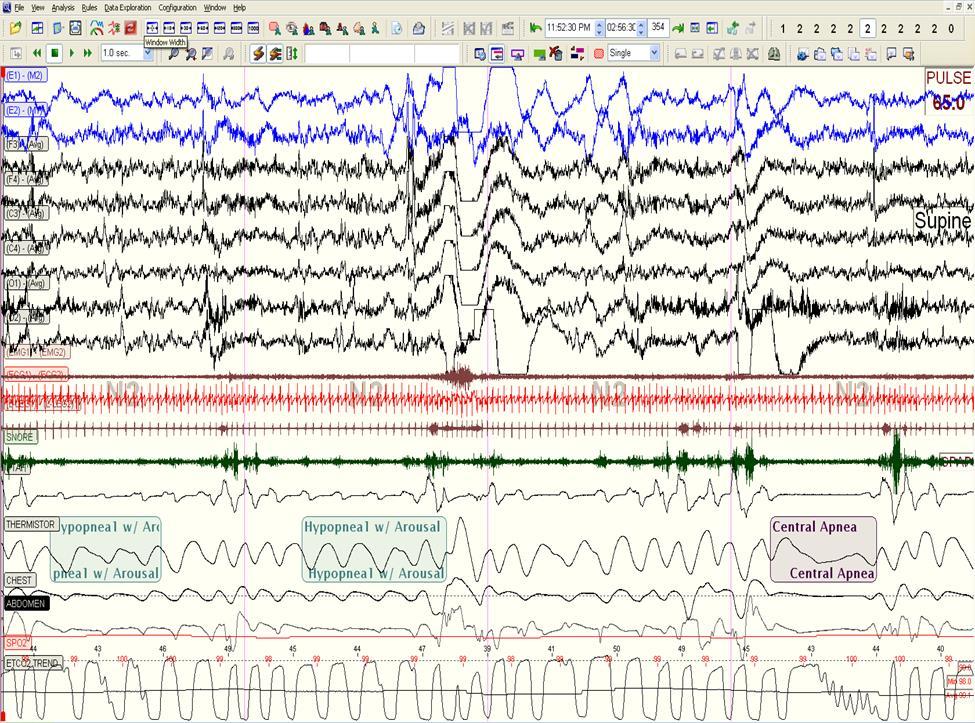
53 Hypopneas
54 Obstructive Hypoventilation

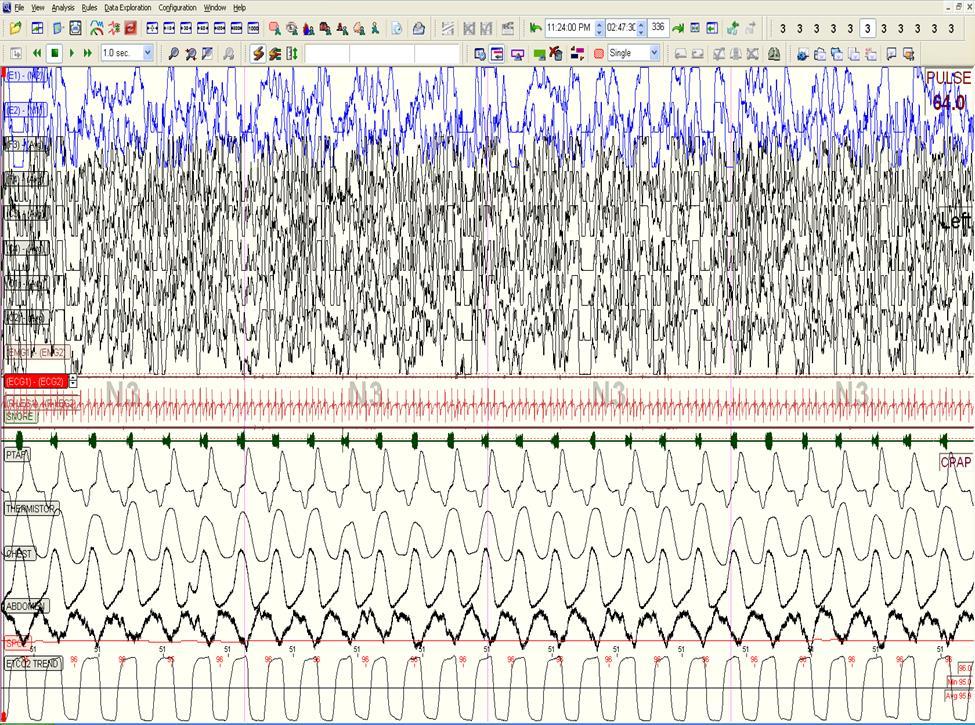
55 Periodic Breathing
56 Summary Pediatric sleep and sleep disorders can appear very different from adult patients Pediatric sleep studies present special challenges to perform and interpret Treatment of pediatric sleep disorders can sometimes require more trial and error, and an appreciation for the child as a member of a family
57 References Berry RB, Brooks R, Gamaldo CE, Harding SM, Lloyd RM, Marcus CL and Vaughn BV for the American Academy of Sleep Medicine. The AASM Manual for the Scoring of Sleep and Associated Events: Rules, Terminology and Technical Specifications, Version Darien, Illinois: American Academy of Sleep Medicine, 2013 Mindell J, Owens J. Clinical Guide to Pediatric Sleep: Diagnosis and Management of Sleep Problems Sheldon S, Ferber R, Kryger M. Principles and Practice of Pediatric Sleep Medicine, 2005
WAKE UP SLEEPYHEAD: NORMAL SLEEP IN CHILDREN AND COMMON PROBLEMS
 WAKE UP SLEEPYHEAD: NORMAL SLEEP IN CHILDREN AND COMMON PROBLEMS Faculty Disclosure No Financial interests to disclose Zoran Danov, MD Associate Professor University of Kentucky Division of Pediatric Pulmonology
WAKE UP SLEEPYHEAD: NORMAL SLEEP IN CHILDREN AND COMMON PROBLEMS Faculty Disclosure No Financial interests to disclose Zoran Danov, MD Associate Professor University of Kentucky Division of Pediatric Pulmonology
Pediatric Considerations in the Sleep Lab
 AAST Technologist Fundamentals Date: May 7, 2017 Focus Conference Location: Orlando, Florida Workshop Pediatric Considerations in the Sleep Lab By Joel Porquez, BS, RST/RPSGT, CCSH X X X X X X Conflict
AAST Technologist Fundamentals Date: May 7, 2017 Focus Conference Location: Orlando, Florida Workshop Pediatric Considerations in the Sleep Lab By Joel Porquez, BS, RST/RPSGT, CCSH X X X X X X Conflict
Polysomnography (PSG) (Sleep Studies), Sleep Center
 (Sleep Studies), Sleep Center") Policy Number: 1036 Policy History Approve Date: 07/09/2015 Effective Date: 07/09/2015 Preauthorization All Plans Benefit plans vary in coverage and some plans may not provide coverage for certain service(s)
Policy Number: 1036 Policy History Approve Date: 07/09/2015 Effective Date: 07/09/2015 Preauthorization All Plans Benefit plans vary in coverage and some plans may not provide coverage for certain service(s)
Sleep: What s the big deal?
 Rise & Shine: The Importance of Sleep Sleep: What s the big deal? Sleep affects every aspect of a child s physical, emotional, cognitive, and social development. 1 Sleep is the Primary Activity of the
Rise & Shine: The Importance of Sleep Sleep: What s the big deal? Sleep affects every aspect of a child s physical, emotional, cognitive, and social development. 1 Sleep is the Primary Activity of the
Participant ID: If you had no responsibilities, what time would your body tell you to go to sleep and wake up?
 What does your sleep look like on a typical week? Total Sleep Time: Bedtime:, Sleep onset latency:, Number of Awakenings:, Wake time after sleep onset:, Rise time:, Out of bed:, Naps:? Notes: Is your sleep
What does your sleep look like on a typical week? Total Sleep Time: Bedtime:, Sleep onset latency:, Number of Awakenings:, Wake time after sleep onset:, Rise time:, Out of bed:, Naps:? Notes: Is your sleep
Objectives 11/11/14. Identifying and Treating Pediatric Sleep Disorders. Normal Sleep in Children. When baby ain t sleepin, ain t nobody sleepin!
 When baby ain t sleepin, ain t nobody sleepin! Identifying and Treating Pediatric Sleep Disorders Theodore Wagener, PhD OU Children s Physicians, Pediatric Behavioral Sleep Medicine Clinic Objectives Attendees
When baby ain t sleepin, ain t nobody sleepin! Identifying and Treating Pediatric Sleep Disorders Theodore Wagener, PhD OU Children s Physicians, Pediatric Behavioral Sleep Medicine Clinic Objectives Attendees
Brian Palmer, D.D.S, Kansas City, Missouri, USA. April, 2001
 Brian Palmer, D.D.S, Kansas City, Missouri, USA A1 April, 2001 Disclaimer The information in this presentation is for basic information only and is not to be construed as a diagnosis or treatment for any
Brian Palmer, D.D.S, Kansas City, Missouri, USA A1 April, 2001 Disclaimer The information in this presentation is for basic information only and is not to be construed as a diagnosis or treatment for any
Infant Sleep Problems and their effects: A Public Health Issue
 Infant Sleep Problems and their effects: A Public Health Issue Wendy Hall, RN, PhD Assessing the Physical Development and Well-Being of Children 8 th Annual Assessment Workshop Outline for Sleep Workshop
Infant Sleep Problems and their effects: A Public Health Issue Wendy Hall, RN, PhD Assessing the Physical Development and Well-Being of Children 8 th Annual Assessment Workshop Outline for Sleep Workshop
OSA in children. About this information. What is obstructive sleep apnoea (OSA)?
?") About this information This information explains all about sleep-related breathing problems in children, focusing on the condition obstructive sleep apnoea (OSA). It tells you what the risk factors are
About this information This information explains all about sleep-related breathing problems in children, focusing on the condition obstructive sleep apnoea (OSA). It tells you what the risk factors are
Index. sleep.theclinics.com. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Actigraphy, 475, 485, 496 Adolescents, sleep disorders in, 576 578 Adults, sleep disorders in, 578 580 Advanced sleep phase disorder, 482 Age,
Note: Page numbers of article titles are in boldface type. A Actigraphy, 475, 485, 496 Adolescents, sleep disorders in, 576 578 Adults, sleep disorders in, 578 580 Advanced sleep phase disorder, 482 Age,
HEALTHY LIFESTYLE, HEALTHY SLEEP. There are many different sleep disorders, and almost all of them can be improved with lifestyle changes.
 HEALTHY LIFESTYLE, HEALTHY SLEEP There are many different sleep disorders, and almost all of them can be improved with lifestyle changes. HEALTHY LIFESTYLE, HEALTHY SLEEP There are many different sleep
HEALTHY LIFESTYLE, HEALTHY SLEEP There are many different sleep disorders, and almost all of them can be improved with lifestyle changes. HEALTHY LIFESTYLE, HEALTHY SLEEP There are many different sleep
Questions: What tests are available to diagnose sleep disordered breathing? How do you calculate overall AHI vs obstructive AHI?
 Pediatric Obstructive Sleep Apnea Case Study : Margaret-Ann Carno PhD, CPNP, D,ABSM for the Sleep Education for Pulmonary Fellows and Practitioners, SRN ATS Committee April 2014. Facilitator s guide Part
Pediatric Obstructive Sleep Apnea Case Study : Margaret-Ann Carno PhD, CPNP, D,ABSM for the Sleep Education for Pulmonary Fellows and Practitioners, SRN ATS Committee April 2014. Facilitator s guide Part
Sleep problems 4/10/2014. Normal sleep (lots of variability at all ages) 2 phases of sleep. Quantity. Quality REM. Non-REM.
 2 phases of sleep. Quantity. Quality REM. Non-REM.") Sleep problems Normal sleep (lots of variability at all ages) Quantity Newborns: 16-20 hrs/day 1-yr olds: 12 hrs/day 6-12 yr olds: 10-11 hrs/day Quality Newborns: distributed between day and night 3-months:
Sleep problems Normal sleep (lots of variability at all ages) Quantity Newborns: 16-20 hrs/day 1-yr olds: 12 hrs/day 6-12 yr olds: 10-11 hrs/day Quality Newborns: distributed between day and night 3-months:
Diagnosis and treatment of sleep disorders
 Diagnosis and treatment of sleep disorders Normal human sleep Sleep cycle occurs about every 90 minutes, approximately 4-6 cycles occur per major sleep episode NREM (70-80%) slow wave sleep heart rate,
Diagnosis and treatment of sleep disorders Normal human sleep Sleep cycle occurs about every 90 minutes, approximately 4-6 cycles occur per major sleep episode NREM (70-80%) slow wave sleep heart rate,
PEDIATRIC OBSTRUCTIVE SLEEP APNEA (OSA)
") PEDIATRIC OBSTRUCTIVE SLEEP APNEA (OSA) DEFINITION OSA Inspiratory airflow is either partly (hypopnea) or completely (apnea) occluded during sleep. The combination of sleep-disordered breathing with daytime
PEDIATRIC OBSTRUCTIVE SLEEP APNEA (OSA) DEFINITION OSA Inspiratory airflow is either partly (hypopnea) or completely (apnea) occluded during sleep. The combination of sleep-disordered breathing with daytime
Sleep - Definition. Slide 1 Sleep & Developmental Disabilities: Lessons for All Children. Slide 2 Importance of Sleep. Slide 3. Lawrence W.
 1 Sleep & Developmental Disabilities: Lessons for All Children March 28, 2012 Lawrence W. Brown, MD Pediatric Neuropsychiatry Program Sleep Disorders Center The Children s Hospital of Philadelphia 2 Importance
1 Sleep & Developmental Disabilities: Lessons for All Children March 28, 2012 Lawrence W. Brown, MD Pediatric Neuropsychiatry Program Sleep Disorders Center The Children s Hospital of Philadelphia 2 Importance
Pediatric Sleep Disorders
 Pediatric Sleep Disorders S. SHAHZEIDI, MD, FAAP, FCCP, FAASM GRAND HEALTH INSTITUTE Objectives Discuss the importance of screening for snoring Explain the signs and symptoms of parasomnias and sleep apnea
Pediatric Sleep Disorders S. SHAHZEIDI, MD, FAAP, FCCP, FAASM GRAND HEALTH INSTITUTE Objectives Discuss the importance of screening for snoring Explain the signs and symptoms of parasomnias and sleep apnea
No Rest For the Weary: Some Common Sleep Disorders
 No Rest For the Weary: Some Common Sleep Disorders Student Activity 3G Activity Introduction: It seems Mom does know best ; sleep has been proven to be essential to our health and well-being. In order
No Rest For the Weary: Some Common Sleep Disorders Student Activity 3G Activity Introduction: It seems Mom does know best ; sleep has been proven to be essential to our health and well-being. In order
TOP 10 LIST OF SLEEP QUESTIONS. Kenneth C. Sassower, MD Sleep Disorders Unit Massachusetts General Hospital for Children
 TOP 10 LIST OF SLEEP QUESTIONS Kenneth C. Sassower, MD Sleep Disorders Unit Massachusetts General Hospital for Children QUESTION #1: ARE SLEEP ISSUES IN CHILDREN THE SAME AS IN ADULTS? Distinctive Features
TOP 10 LIST OF SLEEP QUESTIONS Kenneth C. Sassower, MD Sleep Disorders Unit Massachusetts General Hospital for Children QUESTION #1: ARE SLEEP ISSUES IN CHILDREN THE SAME AS IN ADULTS? Distinctive Features
SLEEP DISORDERS. Kenneth C. Sassower, MD Division of Sleep Medicine; Department of Neurology Massachusetts General Hospital for Children
 SLEEP DISORDERS Kenneth C. Sassower, MD Division of Sleep Medicine; Department of Neurology Massachusetts General Hospital for Children Distinctive Features of Pediatric Sleep Daytime sleepiness uncommon
SLEEP DISORDERS Kenneth C. Sassower, MD Division of Sleep Medicine; Department of Neurology Massachusetts General Hospital for Children Distinctive Features of Pediatric Sleep Daytime sleepiness uncommon
Facts about Sleep. Circadian rhythms are important in determining human sleep patterns/ sleep-waking cycle
 Sleep Sleep is described as a state of unconsciousness or partial consciousness from which a person can be roused by stimulation Period of rest and recovery People spend about a third of their lives sleeping
Sleep Sleep is described as a state of unconsciousness or partial consciousness from which a person can be roused by stimulation Period of rest and recovery People spend about a third of their lives sleeping
Article printed from
 What Are Sleep Disorders? Sleep disorders are conditions that affect how much and how well you sleep. The causes range from poor habits that keep you awake to medical problems that disrupt your sleep cycle.
What Are Sleep Disorders? Sleep disorders are conditions that affect how much and how well you sleep. The causes range from poor habits that keep you awake to medical problems that disrupt your sleep cycle.
WHY CAN T I SLEEP? Deepti Chandran, MD
 WHY CAN T I SLEEP? Deepti Chandran, MD Sleep and Aging How does sleep change as we age? Do we need less sleep as we get older? Can a person expect to experience more sleep problems or have a sleep disorder
WHY CAN T I SLEEP? Deepti Chandran, MD Sleep and Aging How does sleep change as we age? Do we need less sleep as we get older? Can a person expect to experience more sleep problems or have a sleep disorder
The AASM Manual for the Scoring of Sleep and Associated Events
 The AASM Manual for the Scoring of Sleep and Associated Events The 2007 AASM Scoring Manual vs. the AASM Scoring Manual v2.0 October 2012 The American Academy of Sleep Medicine (AASM) is committed to ensuring
The AASM Manual for the Scoring of Sleep and Associated Events The 2007 AASM Scoring Manual vs. the AASM Scoring Manual v2.0 October 2012 The American Academy of Sleep Medicine (AASM) is committed to ensuring
Obstructive Sleep Apnea
 Obstructive Sleep Apnea Introduction Obstructive sleep apnea is an interruption in breathing during sleep. It is caused by throat and tongue muscles collapsing and relaxing. This blocks, or obstructs,
Obstructive Sleep Apnea Introduction Obstructive sleep apnea is an interruption in breathing during sleep. It is caused by throat and tongue muscles collapsing and relaxing. This blocks, or obstructs,
Sleep: A Forgotten Component of Overall Health Demarcus Sneed Health and Human Sciences Educator Madison County October 5, 2016
 Sleep: A Forgotten Component of Overall Health Demarcus Sneed Health and Human Sciences Educator Madison County October 5, 2016 Lesson Objectives Understand the importance of having consistent, quality
Sleep: A Forgotten Component of Overall Health Demarcus Sneed Health and Human Sciences Educator Madison County October 5, 2016 Lesson Objectives Understand the importance of having consistent, quality
Healthy Sleep Tips Along the Way!
 Women and Sleep What You Will Learn The Benefits and Importance of Sleep States and Stages of the Sleep Cycle Unique Physiology of Women s Sleep Common Disorders in Women that Affect Sleep Women s Role
Women and Sleep What You Will Learn The Benefits and Importance of Sleep States and Stages of the Sleep Cycle Unique Physiology of Women s Sleep Common Disorders in Women that Affect Sleep Women s Role
Stage REM. Stage 3/4. Stage 2. Sleep 101. NREM vs. REM. Circadian Rhythms. Sleep Is Needed To: 9/24/2013
 The Power of Sleep: Supporting Healthy Sleep in Children with Autism Spectrum Disorders REM Stage 1 TERRY KATZ, PHD UNIVERSITY OF COLORADO SCHOOL OF MEDICINE JFK PARTNERS CHILD DEVELOPMENT UNIT, CHILDREN
The Power of Sleep: Supporting Healthy Sleep in Children with Autism Spectrum Disorders REM Stage 1 TERRY KATZ, PHD UNIVERSITY OF COLORADO SCHOOL OF MEDICINE JFK PARTNERS CHILD DEVELOPMENT UNIT, CHILDREN
Are you skimping on sleep, or could you have a sleep disorder?
 Are you skimping on sleep, or could you have a sleep disorder? Look around you: the guy nodding off on the bus, the co-worker snoozing during a dull presentation, the people with heavy eyelids lined up
Are you skimping on sleep, or could you have a sleep disorder? Look around you: the guy nodding off on the bus, the co-worker snoozing during a dull presentation, the people with heavy eyelids lined up
Better Bedtime Routines. Michelle Mogenson, D.O. Children s Physicians Spring Valley
 Better Bedtime Routines Michelle Mogenson, D.O. Children s Physicians Spring Valley Outline Sleep expectations Guidance on how to improve sleep Infant sleep methods What you want: Why are you here? Why
Better Bedtime Routines Michelle Mogenson, D.O. Children s Physicians Spring Valley Outline Sleep expectations Guidance on how to improve sleep Infant sleep methods What you want: Why are you here? Why
Sweet Dreams: The Relationship between Sleep Health and Your Weight
 Sweet Dreams: The Relationship between Sleep Health and Your Weight Jason C. Ong, PhD Associate Professor Department of Neurology Center for Circadian and Sleep Medicine Northwestern University Feinberg
Sweet Dreams: The Relationship between Sleep Health and Your Weight Jason C. Ong, PhD Associate Professor Department of Neurology Center for Circadian and Sleep Medicine Northwestern University Feinberg
Sleep Disorders. Sleep. Circadian Rhythms
 Sleep Disorders Sleep The Sleep Wakefulness Cycle: Circadian Rhythms Internally generated patterns of bodily functions that vary over a ~24-hour period Function even in the absence of normal cues 2 Circadian
Sleep Disorders Sleep The Sleep Wakefulness Cycle: Circadian Rhythms Internally generated patterns of bodily functions that vary over a ~24-hour period Function even in the absence of normal cues 2 Circadian
Sleep is Critical to a Child s Development, Health and Quality of Life
 Sleep is Critical to a Child s Development, Health and Quality of Life Childhood is an Opportune Time for Parents to Help Their Children Establish Good Sleep Habits This is important for: Prevention of
Sleep is Critical to a Child s Development, Health and Quality of Life Childhood is an Opportune Time for Parents to Help Their Children Establish Good Sleep Habits This is important for: Prevention of
Sleep Disordered Breathing
 Sleep Disordered Breathing SDB SDB Is an Umbrella Term for Many Disorders characterized by a lack of drive to breathe Results n repetitive pauses in breathing with no effort Occurs for a minimum of 10
Sleep Disordered Breathing SDB SDB Is an Umbrella Term for Many Disorders characterized by a lack of drive to breathe Results n repetitive pauses in breathing with no effort Occurs for a minimum of 10
Summary of the SDIS Development & Psychometric Qualities Content Validation
 Summary of the SDIS Development & Psychometric Qualities This was a national study undertaken over a four year time period at some of the most highly respected sleep clinics in the USA and some of the
Summary of the SDIS Development & Psychometric Qualities This was a national study undertaken over a four year time period at some of the most highly respected sleep clinics in the USA and some of the
The AASM Manual for the Scoring of Sleep and Associated Events
 The AASM Manual for the Scoring of Sleep and Associated Events Summary of Updates in Version 2.1 July 1, 2014 The American Academy of Sleep Medicine (AASM) is committed to ensuring that The AASM Manual
The AASM Manual for the Scoring of Sleep and Associated Events Summary of Updates in Version 2.1 July 1, 2014 The American Academy of Sleep Medicine (AASM) is committed to ensuring that The AASM Manual
Sleep disorders. Norbert Kozak
 Sleep disorders Norbert Kozak About the sleep Each of us will spend about 1/3 of our lifetime sleeping....and 1/3 part of the population has sleep complain Sleep is an essential biological function, but
Sleep disorders Norbert Kozak About the sleep Each of us will spend about 1/3 of our lifetime sleeping....and 1/3 part of the population has sleep complain Sleep is an essential biological function, but
Sleep Medicine. Maintenance of Certification Examination Blueprint. Purpose of the exam
 Sleep Medicine Maintenance of Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of the
Sleep Medicine Maintenance of Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of the
Challenging Cases in Pediatric Polysomnography. Fauziya Hassan, MBBS, MS Assistant Professor Pediatric Pulmonary and Sleep
 Challenging Cases in Pediatric Polysomnography Fauziya Hassan, MBBS, MS Assistant Professor Pediatric Pulmonary and Sleep Conflict of Interest None pertaining to this topic Will be using some slides from
Challenging Cases in Pediatric Polysomnography Fauziya Hassan, MBBS, MS Assistant Professor Pediatric Pulmonary and Sleep Conflict of Interest None pertaining to this topic Will be using some slides from
Individual Planning: A Treatment Plan Overview for Individuals Sleep Disorder Problems.
 COURSES ARTICLE - THERAPYTOOLS.US Individual Planning: A Treatment Plan Overview for Individuals Sleep Disorder Problems. Individual Planning: A Treatment Plan Overview for Individuals Sleep Disorder Problems.
COURSES ARTICLE - THERAPYTOOLS.US Individual Planning: A Treatment Plan Overview for Individuals Sleep Disorder Problems. Individual Planning: A Treatment Plan Overview for Individuals Sleep Disorder Problems.
Assessment of Sleep Disorders DR HUGH SELSICK
 Assessment of Sleep Disorders DR HUGH SELSICK Goals Understand the importance of history taking Be able to take a basic sleep history Be aware the technology used to assess sleep disorders. Understand
Assessment of Sleep Disorders DR HUGH SELSICK Goals Understand the importance of history taking Be able to take a basic sleep history Be aware the technology used to assess sleep disorders. Understand
PEDIATRIC SLEEP GUIDELINES Version 1.0; Effective
 MedSolutions, Inc. Clinical Decision Support Tool Diagnostic Strategies This tool addresses common symptoms and symptom complexes. Requests for patients with atypical symptoms or clinical presentations
MedSolutions, Inc. Clinical Decision Support Tool Diagnostic Strategies This tool addresses common symptoms and symptom complexes. Requests for patients with atypical symptoms or clinical presentations
SLEEP STUDIES IN THE VERY, VERY YOUNG
 SLEEP STUDIES IN THE VERY, VERY YOUNG Julie DeWitte, RCP, RPSGT, RST Assistant Department Administrator Kaiser Permanente Fontana Sleep Center AAST Director-at-Large Board Member NEONATES THROUGH INFANCY
SLEEP STUDIES IN THE VERY, VERY YOUNG Julie DeWitte, RCP, RPSGT, RST Assistant Department Administrator Kaiser Permanente Fontana Sleep Center AAST Director-at-Large Board Member NEONATES THROUGH INFANCY
The International Franco - Palestinian Congress in Sleep Medicine
 The International Franco - Palestinian Congress in Sleep Medicine Temporomandibular Disorders and Sleep Apnea 26 and 27 October, 2017 Notre Dame Hotel, Jerusalem Polysomnography Reports Interpreting the
The International Franco - Palestinian Congress in Sleep Medicine Temporomandibular Disorders and Sleep Apnea 26 and 27 October, 2017 Notre Dame Hotel, Jerusalem Polysomnography Reports Interpreting the
ADHD and Sleep. Dr. Jessica Agnew-Blais MRC Postdoctoral Fellow SDGP Centre Institute of Psychiatry, Psychology & Neuroscience
 ADHD and Sleep Dr. Jessica Agnew-Blais MRC Postdoctoral Fellow SDGP Centre Institute of Psychiatry, Psychology & Neuroscience Who am I? Who I am: ADHD researcher Parent Who I am not: Clinician Sleep expert
ADHD and Sleep Dr. Jessica Agnew-Blais MRC Postdoctoral Fellow SDGP Centre Institute of Psychiatry, Psychology & Neuroscience Who am I? Who I am: ADHD researcher Parent Who I am not: Clinician Sleep expert
A TECH S TOOLKIT FOR THE PEDIATRIC SLEEP LAB
 A TECH S TOOLKIT FOR THE PEDIATRIC SLEEP LAB Craig Canapari, MD craig.canapari@gmail.com drcraigcanapari.com: Updated syllabus will be here along with link to visual presentation. Twitter: DrCanapari INTRODUCTION
A TECH S TOOLKIT FOR THE PEDIATRIC SLEEP LAB Craig Canapari, MD craig.canapari@gmail.com drcraigcanapari.com: Updated syllabus will be here along with link to visual presentation. Twitter: DrCanapari INTRODUCTION
Diagnosis and Management of Childhood Obstructive Sleep Apnea Syndrome
 Diagnosis and Management of Childhood Obstructive Sleep Apnea Syndrome Director, Sleep Laboratory Center for Pediatric Sleep Disorders Boston Children s Hospital Copyright 2014 Boston Children s Hospital
Diagnosis and Management of Childhood Obstructive Sleep Apnea Syndrome Director, Sleep Laboratory Center for Pediatric Sleep Disorders Boston Children s Hospital Copyright 2014 Boston Children s Hospital
PULMONARY & CRITICAL CARE CONSULTANTS OF AUSTIN 1305 West 34 th Street, Suite 400, Austin, TX Phone: Fax:
 Name: Sex: Age: Date: Date of Birth Height Weight Neck size Referring Physician: Primary Care MD: Main Sleep Complaint(s) trouble falling asleep trouble remaining asleep excessive sleepiness during the
Name: Sex: Age: Date: Date of Birth Height Weight Neck size Referring Physician: Primary Care MD: Main Sleep Complaint(s) trouble falling asleep trouble remaining asleep excessive sleepiness during the
PedsCases Podcast Scripts
 PedsCases Podcast Scripts This is a text version of a podcast from Pedscases.com on Obstructive Sleep Apnea These podcasts are designed to give medical students an overview of key topics in pediatrics.
PedsCases Podcast Scripts This is a text version of a podcast from Pedscases.com on Obstructive Sleep Apnea These podcasts are designed to give medical students an overview of key topics in pediatrics.
Baptist Health Floyd 1850 State Street New Albany, IN Sleep Disorders Center Lung & Sleep Specialists. Date of Birth: Age:
 Page 1 of 7 GENERAL INFORMATION Name: Date of Birth: Age: Social Security #: Sex: Height: Weight: Address: City: State: Zip: Home Phone: Cell Phone: Work Phone: Employer s Name: Marital Status: Married
Page 1 of 7 GENERAL INFORMATION Name: Date of Birth: Age: Social Security #: Sex: Height: Weight: Address: City: State: Zip: Home Phone: Cell Phone: Work Phone: Employer s Name: Marital Status: Married
Help I Have Problems with My Sleep!
 Help I Have Problems with My Sleep! Over An 85 Year Lifespan Sleep 31% Work 21% Exercise 1% Food and Drink 11% Sleep Is Important! You can survive without food for up to 2 months Without water 3-5 days
Help I Have Problems with My Sleep! Over An 85 Year Lifespan Sleep 31% Work 21% Exercise 1% Food and Drink 11% Sleep Is Important! You can survive without food for up to 2 months Without water 3-5 days
Complications of Sleep-Disordered Breathing
 Complications of Sleep-Disordered Breathing Similarities between Pediatrics and Adults CATHERINE KIER, MD Professor of Clinical Pediatrics Division Chief, Pediatric Pulmonary, and Cystic Fibrosis Center
Complications of Sleep-Disordered Breathing Similarities between Pediatrics and Adults CATHERINE KIER, MD Professor of Clinical Pediatrics Division Chief, Pediatric Pulmonary, and Cystic Fibrosis Center
Managing Sleep Disorders in Primary Care. Objectives. Disclosures. Nancy Nadolski, FNP, MSN, M.Ed Insomnia Medicine of Idaho Boise Counseling Center
 Managing Sleep Disorders in Primary Care Nancy Nadolski, FNP, MSN, M.Ed Insomnia Medicine of Idaho Boise Counseling Center www.sleeplessinidaho.com 1 Objectives 1) Identify stages and behaviors for normal
Managing Sleep Disorders in Primary Care Nancy Nadolski, FNP, MSN, M.Ed Insomnia Medicine of Idaho Boise Counseling Center www.sleeplessinidaho.com 1 Objectives 1) Identify stages and behaviors for normal
Sleep Center. Have you had a previous sleep study? Yes No If so, when and where? Name of facility Address
 Patient Label For office use only Appt date: Clinician: Sleep Center Main Campus Highlands Ranch Location 1400 Jackson Street 8671 S. Quebec St., Ste 120 Denver, CO 80206 Highlands Ranch, CO 80130 Leading
Patient Label For office use only Appt date: Clinician: Sleep Center Main Campus Highlands Ranch Location 1400 Jackson Street 8671 S. Quebec St., Ste 120 Denver, CO 80206 Highlands Ranch, CO 80130 Leading
RETT SYNDROME AND SLEEP
 2015 A good night s sleep promotes learning, improved mood, general good health, and a better quality of life for both your child and the whole family. This article written for Rettsyndrome.org by Dr Daniel
2015 A good night s sleep promotes learning, improved mood, general good health, and a better quality of life for both your child and the whole family. This article written for Rettsyndrome.org by Dr Daniel
Patricia Carter, PhD, RN, CNS UT Austin School of
 Patricia Carter, PhD, RN, CNS UT Austin School of Nursing pcarter@mail.nur.utexas.edu @carter3236 Overview Normal sleep & Why we sleep Sleep architecture changes with aging Sleep disruptors Evidence based
Patricia Carter, PhD, RN, CNS UT Austin School of Nursing pcarter@mail.nur.utexas.edu @carter3236 Overview Normal sleep & Why we sleep Sleep architecture changes with aging Sleep disruptors Evidence based
Diana Corzine, MD ABMS Sleep Chief MT VA Sleep Medicine Common Sleep Disorders
 Diana Corzine, MD ABMS Sleep Chief MT VA Sleep Medicine 2018 Common Sleep Disorders Objectives: Understand Understand how Sleep Disorders affects health. Describe Describe some Common Sleep Disorders.
Diana Corzine, MD ABMS Sleep Chief MT VA Sleep Medicine 2018 Common Sleep Disorders Objectives: Understand Understand how Sleep Disorders affects health. Describe Describe some Common Sleep Disorders.
Pediatric Sleep-Disordered Breathing
 Pediatric Sleep-Disordered Breathing OSA in infants and young children is generally characterized by partial, persistent obstruction of the upper airway Continuum Benign primary snoring Upper-airway resistance
Pediatric Sleep-Disordered Breathing OSA in infants and young children is generally characterized by partial, persistent obstruction of the upper airway Continuum Benign primary snoring Upper-airway resistance
Emergency Contact Information Name: Phone: Address: Employer Information Employer Name: Address/Street: City: Zip: Phone: Fax:
 SUNSET SLEEP LABS PATIENT INFORMATION FORM Patient Information Name: Sex: M F Date of Birth: Address/Street: City: Zip: Phone: Alt Phone: Parent/Guardian: Phone: Social Security Number: Drivers License:
SUNSET SLEEP LABS PATIENT INFORMATION FORM Patient Information Name: Sex: M F Date of Birth: Address/Street: City: Zip: Phone: Alt Phone: Parent/Guardian: Phone: Social Security Number: Drivers License:
RESTLESS LEGS SYNDROME IN CHILDREN AND ADOLESCENTS
 RESTLESS LEGS SYNDROME IN CHILDREN AND ADOLESCENTS Tracy Carbone, MD Medical Director of Sleep Medicine Lee Health Golisano Children s Hospital of Southwest Florida Fort Myers, FL OVERVIEW Although the
RESTLESS LEGS SYNDROME IN CHILDREN AND ADOLESCENTS Tracy Carbone, MD Medical Director of Sleep Medicine Lee Health Golisano Children s Hospital of Southwest Florida Fort Myers, FL OVERVIEW Although the
SLEEP DISORDERED BREATHING The Clinical Conditions
 SLEEP DISORDERED BREATHING The Clinical Conditions Robert G. Hooper, M.D. In the previous portion of this paper, the definitions of the respiratory events that are the hallmarks of problems with breathing
SLEEP DISORDERED BREATHING The Clinical Conditions Robert G. Hooper, M.D. In the previous portion of this paper, the definitions of the respiratory events that are the hallmarks of problems with breathing
Asleep at the Wheel Understanding and Preventing Drowsy Driving
 LIFESAVERS April 23, 2018 San Antonio, TX 2:15 3:45 PM Room 214 D Sleepiness and Accidents: A Crash Course EVOLVING SAFETY PRIORITIES AND SOLUTIONS Asleep at the Wheel Understanding and Preventing Drowsy
LIFESAVERS April 23, 2018 San Antonio, TX 2:15 3:45 PM Room 214 D Sleepiness and Accidents: A Crash Course EVOLVING SAFETY PRIORITIES AND SOLUTIONS Asleep at the Wheel Understanding and Preventing Drowsy
SLEEP THEORIES. Sleep Protects: Sleeping in the darkness when predators loomed
 SLEEP THEORIES Sleep Protects: Sleeping in the darkness when predators loomed about kept our ancestors out of harm s way. Sleep Recuperates: Sleep helps restore and repair brain tissue. Sleep Helps Remembering:
SLEEP THEORIES Sleep Protects: Sleeping in the darkness when predators loomed about kept our ancestors out of harm s way. Sleep Recuperates: Sleep helps restore and repair brain tissue. Sleep Helps Remembering:
SLEEP STUDY. Nighttime. 1. How many hours of sleep are you now getting in a typical night?
 SLEEP STUDY Patient Name: Date of Birth: Date of Study: This questionnaire involves a broad range of sleep and sleep-related behaviors. Your answers enable us to develop a clearer picture of your sleep/wake
SLEEP STUDY Patient Name: Date of Birth: Date of Study: This questionnaire involves a broad range of sleep and sleep-related behaviors. Your answers enable us to develop a clearer picture of your sleep/wake
An update on childhood sleep-disordered breathing
 An update on childhood sleep-disordered breathing แพทย หญ งวนพร อน นตเสร ภาคว ชาก มารเวชศาสตร คณะแพทยศาสตร มหาว ทยาล ยสงขลานคร นทร Sleep-disordered breathing Primary snoring Upper airway resistance syndrome
An update on childhood sleep-disordered breathing แพทย หญ งวนพร อน นตเสร ภาคว ชาก มารเวชศาสตร คณะแพทยศาสตร มหาว ทยาล ยสงขลานคร นทร Sleep-disordered breathing Primary snoring Upper airway resistance syndrome
Sleep Challenges and Strategies for Change. Parent Presentation July 11, 2013 By Maggie Teske, OTS
 Sleep Challenges and Strategies for Change Parent Presentation July 11, 2013 By Maggie Teske, OTS What is Sleep? Two main phases of sleep rapid eye movement (REM) and non-rapid eye movement (Non-REM) REM
Sleep Challenges and Strategies for Change Parent Presentation July 11, 2013 By Maggie Teske, OTS What is Sleep? Two main phases of sleep rapid eye movement (REM) and non-rapid eye movement (Non-REM) REM
The Medical Center Sleep Center
 The Medical Center Sleep Center Date: / / Name: Age: (First) (M.I.) (Last) Address: (Street / P.O. Box) (City) (State) (Zip) (County) Phone: Home ( ) Work ( ) Date of Birth: / / Education: Marital Status:
The Medical Center Sleep Center Date: / / Name: Age: (First) (M.I.) (Last) Address: (Street / P.O. Box) (City) (State) (Zip) (County) Phone: Home ( ) Work ( ) Date of Birth: / / Education: Marital Status:
Teenagers: Sleep Patterns and School Performance
 The National Healthy Sleep Awareness Project involves a partnership between the American Academy of Sleep Medicine, Center for Disease Control and Sleep Research Society. The long term goal of the project
The National Healthy Sleep Awareness Project involves a partnership between the American Academy of Sleep Medicine, Center for Disease Control and Sleep Research Society. The long term goal of the project
Sleep Disorders Diagnostic Center 9733 Healthway Drive, Berlin, MD , ext. 5118
 Sleep Questionnaire *Please complete the following as accurate as possible. Please bring your completed questionnaire, insurance card, photo ID, Pre-Authorization and/or Insurance referral form, and all
Sleep Questionnaire *Please complete the following as accurate as possible. Please bring your completed questionnaire, insurance card, photo ID, Pre-Authorization and/or Insurance referral form, and all
Medications that are not FDA approved for children will be discussed. NAPNAP National Conference 2018
 Medications that are not FDA approved for children will be discussed NAPNAP National Conference 2018 (Honaker & Meltzer, 2016; Keyes, Maslowsky, Hamilton & Schulenberg, 2015) Chronically disrupted sleep
Medications that are not FDA approved for children will be discussed NAPNAP National Conference 2018 (Honaker & Meltzer, 2016; Keyes, Maslowsky, Hamilton & Schulenberg, 2015) Chronically disrupted sleep
Presented By Dr. Ramesh. Adverse Health Effects of Sleep Deprivation
 Presented By Dr. Ramesh Adverse Health Effects of Sleep Deprivation Definition of Sleep (medical dictionary) A period of rest for the body and mind during which volition and consciousness are in partial
Presented By Dr. Ramesh Adverse Health Effects of Sleep Deprivation Definition of Sleep (medical dictionary) A period of rest for the body and mind during which volition and consciousness are in partial
SLEEP HISTORY QUESTIONNAIRE
 Date of birth: Today s date: Dear Patient: SLEEP HISTORY QUESTIONNAIRE Thank you for taking the time to fill out a sleep history questionnaire. This will help our healthcare team to provide the best possible
Date of birth: Today s date: Dear Patient: SLEEP HISTORY QUESTIONNAIRE Thank you for taking the time to fill out a sleep history questionnaire. This will help our healthcare team to provide the best possible
Sleep Studies: Attended Polysomnography and Portable Polysomnography Tests, Multiple Sleep Latency Testing and Maintenance of Wakefulness Testing
 Portable Polysomnography Tests, Multiple Sleep Latency Testing and Maintenance of Wakefulness Testing MP9132 Covered Service: Yes when meets criteria below Prior Authorization Required: Yes as indicated
Portable Polysomnography Tests, Multiple Sleep Latency Testing and Maintenance of Wakefulness Testing MP9132 Covered Service: Yes when meets criteria below Prior Authorization Required: Yes as indicated
Diagnosis and Management of Common Sleep Problems in Children Sumit Bhargava. DOI: /pir
 Diagnosis and Management of Common Sleep Problems in Children Sumit Bhargava Pediatr. Rev. 2011;32;91-99 DOI: 10.1542/pir.32-3-91 The online version of this article, along with updated information and
Diagnosis and Management of Common Sleep Problems in Children Sumit Bhargava Pediatr. Rev. 2011;32;91-99 DOI: 10.1542/pir.32-3-91 The online version of this article, along with updated information and
Sleep Diordered Breathing (Part 1)
") Sleep Diordered Breathing (Part 1) History (for more topics & presentations, visit ) Obstructive sleep apnea - first described by Charles Dickens in 1836 in Papers of the Pickwick Club, Dickens depicted
Sleep Diordered Breathing (Part 1) History (for more topics & presentations, visit ) Obstructive sleep apnea - first described by Charles Dickens in 1836 in Papers of the Pickwick Club, Dickens depicted
Polysomnography Course Session: Sept 2017
 Polysomnography Course Session: Sept 2017 General Information Polysomnography course will be held at SLEEP AND ALERTNESS CLINIC Med-West Medical centre 750 Dundas St. W., Suite 2-259 (Conference Room)
Polysomnography Course Session: Sept 2017 General Information Polysomnography course will be held at SLEEP AND ALERTNESS CLINIC Med-West Medical centre 750 Dundas St. W., Suite 2-259 (Conference Room)
Childhood Obstructive Sleep Apnea
 Childhood Obstructive Sleep Apnea 1 PROF. RAJESHWAR DAYAL MD, FAMS,FIAP,DNB, DCH (LONDON) NATIONAL CONVENOR,IAP SLEEP PROGRAM NATIONAL VICE PRESIDENT IAP 2011 HEAD DEPARTMENT OF PAEDIATRICS S. N. MEDICAL
Childhood Obstructive Sleep Apnea 1 PROF. RAJESHWAR DAYAL MD, FAMS,FIAP,DNB, DCH (LONDON) NATIONAL CONVENOR,IAP SLEEP PROGRAM NATIONAL VICE PRESIDENT IAP 2011 HEAD DEPARTMENT OF PAEDIATRICS S. N. MEDICAL
Consciousness, Stages of Sleep, & Dreams. Defined:
 Consciousness, Stages of Sleep, & Dreams I. Consciousness Conscious is: Waking Consciousness Defined: Altered State of Consciousness Defined: Most of waking life Fuzzy, organized, bizarre thoughts Examples:
Consciousness, Stages of Sleep, & Dreams I. Consciousness Conscious is: Waking Consciousness Defined: Altered State of Consciousness Defined: Most of waking life Fuzzy, organized, bizarre thoughts Examples:
Basics of Polysomnography. Chitra Lal, MD, FCCP, FAASM Assistant professor of Medicine, Pulmonary, Critical Care and Sleep, MUSC, Charleston, SC
 Basics of Polysomnography Chitra Lal, MD, FCCP, FAASM Assistant professor of Medicine, Pulmonary, Critical Care and Sleep, MUSC, Charleston, SC Basics of Polysomnography Continuous and simultaneous recording
Basics of Polysomnography Chitra Lal, MD, FCCP, FAASM Assistant professor of Medicine, Pulmonary, Critical Care and Sleep, MUSC, Charleston, SC Basics of Polysomnography Continuous and simultaneous recording
I. What Is Consciousness? Definition Awareness of things inside you and outside you. 3 Meanings of Consciousness
 I. What Is? Definition Awareness of things inside you and outside you I. What Is? is a construct What is a construct? Something that we can t directly see or measure Examples: self-esteem intelligence
I. What Is? Definition Awareness of things inside you and outside you I. What Is? is a construct What is a construct? Something that we can t directly see or measure Examples: self-esteem intelligence
Patient History & Sleep Questionnaire
 Patient History & Sleep Questionnaire Patient Full Name: Nick Name: Birth date: Age: Sex: Height: Current Weight: Weight Five Years Ago: Peak Lifetime Weight: Marital Status: Single Married Divorced Widowed
Patient History & Sleep Questionnaire Patient Full Name: Nick Name: Birth date: Age: Sex: Height: Current Weight: Weight Five Years Ago: Peak Lifetime Weight: Marital Status: Single Married Divorced Widowed
New Patient Sleep Intake
 New Patient Sleep Intake Name: Date of Birth: Primary Care Physician: Date of Visit: Referring Physician and/or Other Physicians: Retail Pharmacy: Mail Order Pharmacy: Address: Mail Order Phone #: Phone
New Patient Sleep Intake Name: Date of Birth: Primary Care Physician: Date of Visit: Referring Physician and/or Other Physicians: Retail Pharmacy: Mail Order Pharmacy: Address: Mail Order Phone #: Phone
Associated Neurological Specialties and Sleep Disorder Center
 Sleep Center Questionnaire Name: Sex: Age: Date: Date of Birth: Height: Weight: Neck Size: Primary Care Physician: Referring Physician: Main Sleep Issues/Complaints Trouble falling asleep Trouble staying
Sleep Center Questionnaire Name: Sex: Age: Date: Date of Birth: Height: Weight: Neck Size: Primary Care Physician: Referring Physician: Main Sleep Issues/Complaints Trouble falling asleep Trouble staying
Littleton, CO Welcome Packet 8151 Southpark Lane, Suite 200 Littleton, CO 80120
 Littleton, CO Welcome Packet For any after-hours questions, please call (303) 956-5145 Dear Mountain Sleep Patient, You have been scheduled for a sleep study at 8151 Southpark Lane, Suite 200, Littleton,
Littleton, CO Welcome Packet For any after-hours questions, please call (303) 956-5145 Dear Mountain Sleep Patient, You have been scheduled for a sleep study at 8151 Southpark Lane, Suite 200, Littleton,
SLEEP APNEA IN THE ELDERLY SLEEP THAT KNITS UP THE RAVELED SLEEVE OF CARE
 SLEEP APNEA IN THE ELDERLY SLEEP THAT KNITS UP THE RAVELED SLEEVE OF CARE OBJECTIVES 1. TO DESCRIBE THE NORMAL AGE RELATED CHANGES TO SLEEP 2. TO DESCRIBE THE SPECTRUM OF SLEEP-DISORDERED BREATHING. 3.
SLEEP APNEA IN THE ELDERLY SLEEP THAT KNITS UP THE RAVELED SLEEVE OF CARE OBJECTIVES 1. TO DESCRIBE THE NORMAL AGE RELATED CHANGES TO SLEEP 2. TO DESCRIBE THE SPECTRUM OF SLEEP-DISORDERED BREATHING. 3.
Sleep Apnea. Herbert A Berger, MD Pulmonary Division Department of Internal Medicine University of Iowa
 Sleep Apnea Herbert A Berger, MD Pulmonary Division Department of Internal Medicine University of Iowa Disclosures No Relevant Financial Interests to Report Objectives Learn the history and physical examination
Sleep Apnea Herbert A Berger, MD Pulmonary Division Department of Internal Medicine University of Iowa Disclosures No Relevant Financial Interests to Report Objectives Learn the history and physical examination
Pediatric Obstructive Sleep apnea An update What else is there to know?
 Pediatric Obstructive Sleep apnea An update What else is there to know? Garani S. Nadaraja, MD, FAAP Medical Director BCH-Oakland Clinical Assistant Professor Division of Pediatric Otolaryngology UCSF
Pediatric Obstructive Sleep apnea An update What else is there to know? Garani S. Nadaraja, MD, FAAP Medical Director BCH-Oakland Clinical Assistant Professor Division of Pediatric Otolaryngology UCSF
11/20/2015. Eighth Bi-Annual Pediatric Sleep Medicine Conference. November 12-15, 2015 Omni Amelia Island Plantation Resort Amelia Island, Florida
 Eighth Bi-Annual Pediatric Sleep Medicine Conference November 12-15, 2015 Omni Amelia Island Plantation Resort Amelia Island, Florida Carol L. Rosen, MD Case Western Reserve University School of Medicine
Eighth Bi-Annual Pediatric Sleep Medicine Conference November 12-15, 2015 Omni Amelia Island Plantation Resort Amelia Island, Florida Carol L. Rosen, MD Case Western Reserve University School of Medicine
PORTABLE OR HOME SLEEP STUDIES FOR ADULT PATIENTS:
 Sleep Studies: Attended Polysomnography and Portable Polysomnography Tests, Multiple Sleep Latency Testing and Maintenance of Wakefulness Testing MP9132 Covered Service: Prior Authorization Required: Additional
Sleep Studies: Attended Polysomnography and Portable Polysomnography Tests, Multiple Sleep Latency Testing and Maintenance of Wakefulness Testing MP9132 Covered Service: Prior Authorization Required: Additional
PEDIATRIC HISTORY FORM
 Lehigh Valley Health Network Pediatric Sleep Center PEDIATRIC HISTORY FORM Please answer the following questions frankly and accurately by filling in the blank or checking/circling the appropriate answer.
Lehigh Valley Health Network Pediatric Sleep Center PEDIATRIC HISTORY FORM Please answer the following questions frankly and accurately by filling in the blank or checking/circling the appropriate answer.
in China Shanghai Office Beijing Office (+86) (+86)
 (+86)") SLEEP Apnea in China Guide 2018-2019 Shanghai Office (+86) 21 2426 6400 Beijing Office (+86) 010 6464 0611 www.pacificprime.cn Follow us on WeChat t A comprehensive overview of sleep apnea Perhaps you
SLEEP Apnea in China Guide 2018-2019 Shanghai Office (+86) 21 2426 6400 Beijing Office (+86) 010 6464 0611 www.pacificprime.cn Follow us on WeChat t A comprehensive overview of sleep apnea Perhaps you
THE SLEEP DISORDERS CLINIC Medical Director: Dr Raymond Gottschalk PATIENT QUESTIONNAIRE
 THE SLEEP DISORDERS CLINIC Medical Director: Dr Raymond Gottschalk 55 Frid Street, Unit 7, Hamilton, Ontario L8P 4M3 Phone:905-529-2259 Fax: 905-529-2262 282 Linwell Road, Suite 118, St. Catharines, Ontario
THE SLEEP DISORDERS CLINIC Medical Director: Dr Raymond Gottschalk 55 Frid Street, Unit 7, Hamilton, Ontario L8P 4M3 Phone:905-529-2259 Fax: 905-529-2262 282 Linwell Road, Suite 118, St. Catharines, Ontario
Pediatric Sleep History
 Fax 423-431-2983 Pediatric Sleep History Patient/ Child s Name: Date of Birth: Parent Name: Last 4 of Social Security No: Gender: Male Female Height: Weight: Age: Race: Street Address: City: State: Zip:
Fax 423-431-2983 Pediatric Sleep History Patient/ Child s Name: Date of Birth: Parent Name: Last 4 of Social Security No: Gender: Male Female Height: Weight: Age: Race: Street Address: City: State: Zip:
SLEEP UPDATE 2008 SLEEP HYPNOGRAM. David Claman, MD UCSF Sleep Disorders Center
 SLEEP UPDATE 2008 SLEEP HYPNOGRAM David Claman, MD UCSF Sleep Disorders Center Insomnia Case A 40 year old man c/o insomnia at sleep onset. He worries about sleep at night, and takes 2-3 hrs to fall asleep.
SLEEP UPDATE 2008 SLEEP HYPNOGRAM David Claman, MD UCSF Sleep Disorders Center Insomnia Case A 40 year old man c/o insomnia at sleep onset. He worries about sleep at night, and takes 2-3 hrs to fall asleep.
Sleep History Questionnaire
 Sleep History Questionnaire Name: DOB: Phone: Date of Consultation: Consultation is requested by: Primary care provider: _ Preferred pharmacy: Chief complaint: Please tell us why you are here: How long
Sleep History Questionnaire Name: DOB: Phone: Date of Consultation: Consultation is requested by: Primary care provider: _ Preferred pharmacy: Chief complaint: Please tell us why you are here: How long
Sleep stages. Awake Stage 1 Stage 2 Stage 3 Stage 4 Rapid eye movement sleep (REM) Slow wave sleep (NREM)
 Slow wave sleep (NREM)") Sleep stages Awake Stage 1 Stage 2 Stage 3 Stage 4 Rapid eye movement sleep (REM) Slow wave sleep (NREM) EEG waves EEG Electrode Placement Classifying EEG brain waves Frequency: the number of oscillations/waves
Sleep stages Awake Stage 1 Stage 2 Stage 3 Stage 4 Rapid eye movement sleep (REM) Slow wave sleep (NREM) EEG waves EEG Electrode Placement Classifying EEG brain waves Frequency: the number of oscillations/waves
Home Sleep Testing Questionnaire
 Home Sleep Testing Questionnaire Patient Name: DOB: / / Gender: Male Female Study Date: / / Marital Status: Married Cohabitate Single Divorced Widow/Widower Email: Phone: Height: Weight: Neck Size: What
Home Sleep Testing Questionnaire Patient Name: DOB: / / Gender: Male Female Study Date: / / Marital Status: Married Cohabitate Single Divorced Widow/Widower Email: Phone: Height: Weight: Neck Size: What
Sleep Apnea. What is sleep apnea? How does it occur? What are the symptoms?
 What is sleep apnea? Sleep Apnea Sleep apnea is a serious sleep problem. If you have it, you stop breathing for more than 10 seconds at a time many times while you sleep. Another term for this problem
What is sleep apnea? Sleep Apnea Sleep apnea is a serious sleep problem. If you have it, you stop breathing for more than 10 seconds at a time many times while you sleep. Another term for this problem
Sleep and Ageing. Siobhan Banks PhD. Body and Brain at Work, Centre for Sleep Research University of South Australia
 Sleep and Ageing Siobhan Banks PhD Body and Brain at Work, Centre for Sleep Research University of South Australia Health and Active Ageing, 22 nd September 2015 Sleep and Aging How does sleep change as
Sleep and Ageing Siobhan Banks PhD Body and Brain at Work, Centre for Sleep Research University of South Australia Health and Active Ageing, 22 nd September 2015 Sleep and Aging How does sleep change as
Denver, CO Welcome Packet
 Fax: (303) 957-5414 or 720-542-8699 For any after-hours questions, please call (303) 956-5145 Dear Mountain Sleep Patient, You have been scheduled for a sleep study at 1210 S Parker Road, Suite 101, Denver,
Fax: (303) 957-5414 or 720-542-8699 For any after-hours questions, please call (303) 956-5145 Dear Mountain Sleep Patient, You have been scheduled for a sleep study at 1210 S Parker Road, Suite 101, Denver,