6/5/2017. Mellar P Davis MD FCCP FAAHPM Geisinger Medical Center Danville, PA
|
|
|
- Jade Freeman
- 5 years ago
- Views:
Transcription
 and obstructive sleep apnea (OSA) Clinically opioids worsen pre-existing sleep disordered breathing (SDB) Recent studies have shown increased morbidity and mortality in")
1 Mellar P Davis MD FCCP FAAHPM Geisinger Medical Center Danville, PA Opioids adversely influence respiration in five distinct ways Opioids cause complex sleep disordered breathing consisting of central sleep apnea (CSA) and obstructive sleep apnea (OSA) Clinically opioids worsen pre-existing sleep disordered breathing (SDB) Recent studies have shown increased morbidity and mortality in patients receiving opioids for chronic non-cancer pain and chronic obstructive pulmonary disease (COPD)which appear to be related to cardiovascular events, not overdose Recommendations regarding management of SDB on opioids are not well developed and there is little trials data to give evidence to management 1
2 Breathlessness or dyspnea is a subjective experience of breathing discomfort with qualitatively distinct sensations that vary in intensity and from patient to patient The relief from breathlessness at the end of life is a critically important qualitative measure. Refractory breathlessness which is breathlessness that persists despite aggressive pulmonary rehabilitation, optimal bronchial dilatation and meticulous treatment of concurrent morbidities is palliated by morphine. Morphine modestly reduces the subjective severity of breathlessness. Unfortunately, opioids have not been shown to improve activities of daily living or function limited by breathless Two recent systematic reviews of randomized trials have gauged the benefits of opioids in reducing breathlessness in patients with COPD and advanced cardiopulmonary disease. Patients (n=797) had reduced dyspnea with a NNT of

3 The design of the opioid trials was centered on efficacy and not safety. Both showed improvements in dyspnea but not function. None of the studies involved assessment of patients for SDB. Almost all were less than 4 weeks in duration and a significant number were single dose studies. Safety was not well described Apnea is defined as the absence of air flow for at least 10 seconds while hypopnea is 50% or greater reduction in air flow for 10 seconds with a 4% reduction in oxygen saturation or a 3% desaturation with subsequent arousal. Obstructive sleep apnea is separated from central sleep apnea by the presence of respiratory effort during the period of reduced airflow. Obstructive sleep apnea is caused by recurrent upper airway collapse during inspiration SDB is clinically and diagnostically defined as an AHI >5. Mild SDB is an AHI ( episodes per hour) of 5-15, moderate and severe >30 Complex sleep disordered breathing consists of both CSA and OSA 3
4 Patient with a pre-existing cardiovascular disease and SDB have higher healthcare costs and a greater risk for adverse cardiovascular events with an odds ratio (OR) of 4.1 (95%CI ) compared with matched controls without SDB The number of obstructive events and the degree of hypoxemia during sleep strongly predicts for occurrence of an arrhythmia Those with SBD and comorbid COPD (overlap syndrome) or those with cardiovascular disease are at greater risk of for arrhythmias at night. The overlap syndrome compounds the risk of nocturnal arrhythmias relative to COPD or SDB alone. Those with the overlap syndrome have a 2.5- fold greater risk of tachyarrhythmias relative to those with OSA alone The prevalence of SDB is higher in patients who have chronic pain than in the normal population. The prevalence of OSA in patients with chronic spinal pain is 13.8%. Sleep disordered breathing occurs more frequently in individuals with temporomandibular joint disease or who have chronic headaches of all types (tension, migraine and cluster) 4

5 One mechanisms behind the arrhythmias at night relates to the dispersion of the QTc interval (differences between maximum and minimum QTc intervals over time). QTc intervals were found to lengthen with OSA and hypoxia. QTc dispersions were positively associated with the severity of the AHI (r=0.913, p<0.001 and were a direct marker of arrhythmia risk. Most sudden cardiac deaths from arrhythmias in individuals without SDB occur during the day with a nadir between midnight and 6AM. However, 50% of sudden deaths in those with SDB occur between midnight and 6am, a reversal of the common timing of sudden cardiac death Sleep disordered breathing has been associated with risk factors for cardiovascular disease. OSA is associated with increased risks of uncontrolled hypertension leading to a greater prevalence for myocardial infarction and strokes as well as deep venous thrombosis, all of which may cause sudden death. Hypertension, myocardial infarctions, strokes and deep venous thrombosis are related to increased sympathetic tone caused by SDB and hypoxia which is reduced by positive airway pressure 5
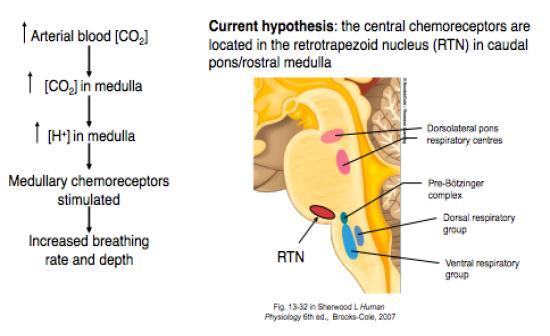
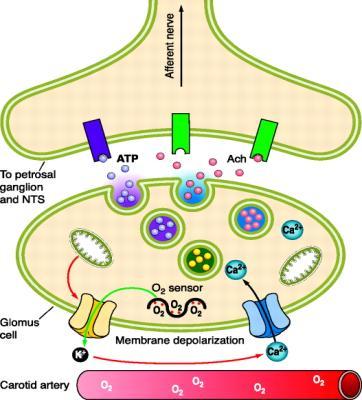
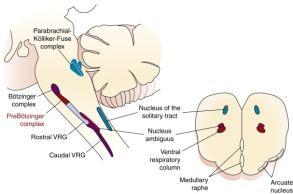
6 Opioids delay inspiration through hyperpolarization of pre-botzinger complex neurons thereby slowing respiratory rate by delaying inspiration Tidal volume compensatorially increases when doses are low thereby maintaining minute ventilation which is lost with higher opioid doses An inspiratory cycle is missed (called quantal breathing or integer multiples of the control period of breathing in the absence of the opioid Opioids are not associated with Cheyne -Stokes respiration Hypoxic drive is depressed to a greater extent than hypercapnic drive and suppression is longer lasting Opioids blunt responses to hypoxia by binding to mu receptors within the Nucleus Tractus Solitarius thus blocking neurotransmission from Glomus cells to the medulla Breath to breath tidal volume variability and delayed hyperventilation response to rising pco2 levels suggests both a central and peripheral opioid effect Blunted respiratory response to context cues ( breath holding) 6
7 7
 by the medial pontine reticular group of neurons In both REM sleep and NREM sleep ventilatory responses to CO2 are blunted, responses to hypoxia are better maintained.")
8 Respiratory drive is maintained by cortical activity while awake but during non-rapid eye movement sleep (NREM sleep), respiratory drive is maintained by metabolic drive (O2 and CO2) During rapid eye movement sleep (REM) by the medial pontine reticular group of neurons In both REM sleep and NREM sleep ventilatory responses to CO2 are blunted, responses to hypoxia are better maintained. During REM sleep, breathing becomes more variable (less rhythmic) and intercostal muscles become atonic Intermittent and sometimes severe hypoxemia can occur during REM sleep particularly if there is diaphragmatic impairment. Hypoxia becomes quite severe if the diaphragm is compromised by obesity, rib cage, deformity or COPD During REM sleep, there is a greater dependence on the chemoreceptor centers within and around the retrotrapezoid neuron complex (RTN) to maintain respiration 8

9 The respiratory rate is normally reduced during REM sleep but further reduced with opioid therapy due to opioid receptors on the NTS. REM sleep is a vulnerable time for opioidrelated impaired breathing; some Individuals with SDB depend on arousal at night to reinstate wakeful- related cerebral cortex respiratory drive to compensate for hypoxemia. Opioids blunt this compensatory arousal which reduces waking after sleep onset (WASO) episodes. This may improve sleep subjectively but will worsen or prolong hypoxemia during sleep, potentially leading to arrhythmias Opioid receptors on the mechanosensory neurons in upper airways activate laryngeal adductor and pharyngeal constrictors and depress laryngeal abductor muscles resulting in a decreased the upper airway caliber causing increased airway resistance. Upper airway dilator muscles become less active during REM sleep, when OSA most often occurs. The addition of benzodiazepines to opioids aggravates induced airway obstruction 9

.")
10 Higher potency opioids such as the phenylpiperdine class (fentanyl) more profoundly reduce upper airway discharges control upper airway patency. This results in inspiratory glottic closure and increased airway resistance during inspiration. 30% of individuals on methadone maintenance therapy have CSA which only weakly correlated with dose, age and BMI 35% of patients on methadone maintenance therapy, have OSA which correlated with BMI and longer duration of maintenance therapy 46% of patients on opioids for chronic pain had severe SDB (AHI>30). 46% had mild day time increases in Paco2 which became more prevalent with increasing doses 75% of patients on a mean morphine equivalent dose of 266 mg, a median dose 187 mg per day, had a AHI > 5, 39% has OSA, 24% CSA and 8% both CSA and OSA. Severe SDB (AHI>30) was occurred in approximately 40%. The AHI worsened with the addition of muscle relaxants to opioid therapy. Combinations of methadone and benzodiazepines was highly associated with CSA 10
11 A comparison of patients on opioid therapy for chronic pain and a similar cohort of patients with chronic pain not on opioids found a AHI of 41 in those on opioids and 22 in those not on opioids (p=0.018). In a subset who underwent opioid taper, the AHI decreased to (p<0.01). Central sleep apnea resolved off opioids. Hypoxia during REM sleep which had occurred in 27% of individuals before opioid taper also improved significantly (p<0.01) Author (Reference) Numbers Benefits / Risks NNT Comments Elkstrom M N=271 Dyspnea relief 7-9 All but I study< 30 days in duration Barnes H Systematic review Dyspnea relief 9-10 All but I study< 30 of 26 studies with N=526 days in duration Vozoris NT N=130,979 Risks HR/NNH Opioid Matched-cohort study Hospitalizations HR1.5 / NNH 66 Short-acting opioids COPD/pneumonia related mortality All-cause mortality HR 4.79 /NNH 77 Short-acting opioids HR 3.38 / NNH 28 Mortality related to cardiac events Vozoris NT N=22,912 Hospitalizations HR 1.73 /NNH 71 Morphine dose<30mg/day Matched-cohort study COPD/pneumonia related mortality All-cause mortality HR 7.55 / NNH 71 Morphine dose<30mg/day HR 5.19 / NNH 17 Morphine dose<30mg/day There is a narrow therapeutic index between benefits and mortality when opioids are used to treat breathlessness or pain in patients with COPD. This influences our choices of analgesics and should be used to inform our patients about benefits and risks. We cannot assume that there is a safe dose of opioid until longer randomized trials are completed. 11

12 It should not be assumed that the morbidity and mortality risk of opioids in COPD is the same as that which occurs in the addiction maintenance population or in the chronic noncancer pain population. Methadone maintenance reduces mortality from addiction by reducing the use of street drugs Individuals with the overlap syndrome and a subset with SDB alone have daytime fatigue, daytime sleepiness, reduced cognitive function and frequently complain of insomnia Patients may also complain of WASO as a compensatory mechanism. Therefore, if one only treats the complaint, it would seem reasonable to prescribe a sedative at night and an opioid for breathlessness which would reduce breathlessness and WASO but deepen nocturnal hypoxia, worsen SDB and increase the risk for nocturnal arrhythmias 12


13 The STOP BANG questionnaire, although originally validated to screen for sleep apnea in perioperative setting, has been used in numerous studies to screen for OSA outside of the perioperative setting with high sensitively for moderate to severe sleep apnea. This screening tool may be useful in screening patients for the presence of sleep apnea Do Not Start an Opioid in a Patient with COPD Without a Clear Indication This may appear self-evident but most patients with COPD in the Ontario study were given an opioid not for dyspnea but for chronic noncancer musculoskeletal pain, an indication which has recently been questioned When Opioids Are Necessary for Advanced Cancer Pain and Survival Expectations Are Months to a Year or More, Monitor the Patient with COPD for a Sleep Disordered Breathing and Nocturnal Hypoxemia. It is not known if it is the degree of hypoxemia at night or the severity of the SDB as measured by the AHI that predisposes patients to respiratory and cardiovascular adverse events. It may be that the obstructive episodes at night predispose patients to pneumonia and COPD exacerbations while hypoxia causes arrhythmia. 13
14 Use an Opioid -Sparing Strategy for Pain Management and Avoid Benzodiazepines The level of evidence for opioid-sparing strategies is derived largely from nonrandomized trials and should be validated in randomized prospective studies. The evidence is also mixed with some negative studies Regional blocks, radiation and palliative surgery reduce pain and opioid requirements If a 24- hour sustained release opioid is used, one study suggested that it be given in the morning to avoid peaked plasma levels at night Consider Positive Airway Pressure for Those with COPD Overlap Syndrome and SDB on Opioids The level of evidence is derived from nonrandomized prospective and retrospective studies and so should be validated in randomized trials Efforts to manage CSA on opioids by continuous positive airway pressure (CPAP) have largely been unsuccessful whereas OSA responds relatively well The American Academy of Sleep Medicine guidelines do not make recommendations as to which positive airway pressure method should be used for CSA CPAP is generally less expensive than bi-level positive airway pressure (BiPAP) and adaptive servoventilation (ASV). Therefore, CPAP should be tried first and BiPAP and ASV used for individuals not responding to CPAP 14
15 A recent review six studies which explored the use of ASV for opioid induced SDB found in five of the six studies a reduction in both the AHI and central apnea index. The sixth demonstrated long-term benefits beyond 3 month. However, ASV should not be used for patients with congestive heart failure and an ejection fraction of <40; ASV increases mortality in these patients. Increased overdose deaths may be related to prescriptions of opioids given to patients with undiagnosed SDB- are these overdoses or are these individuals who follow a physician s order with unsuspected SDB? There are large gaps in evidence particularly regarding the benefits of positive pressure support and clinical outcomes- Does positive pressure support are night reduce opioid mortality? Who would benefit? 15
Opioids, Dyspnea and Risks
 Opioids, Dyspnea and Risks Opioids and Respira1on Opioids delay inspira.on through hyperpolariza.on of pre-botzinger complex neurons thereby slowing respiratory rate by delaying inspira.on Tidal volume
Opioids, Dyspnea and Risks Opioids and Respira1on Opioids delay inspira.on through hyperpolariza.on of pre-botzinger complex neurons thereby slowing respiratory rate by delaying inspira.on Tidal volume
Mario Kinsella MD FAASM 10/5/2016
 Mario Kinsella MD FAASM 10/5/2016 Repetitive episodes of apnea or reduced airflow Due to upper airway obstruction during sleep Patients often obese Often have hypertension or DM 1 Obstructive apneas, hypopneas,
Mario Kinsella MD FAASM 10/5/2016 Repetitive episodes of apnea or reduced airflow Due to upper airway obstruction during sleep Patients often obese Often have hypertension or DM 1 Obstructive apneas, hypopneas,
Circadian Variations Influential in Circulatory & Vascular Phenomena
 SLEEP & STROKE 1 Circadian Variations Influential in Circulatory & Vascular Phenomena Endocrine secretions Thermo regulations Renal Functions Respiratory control Heart Rhythm Hematologic parameters Immune
SLEEP & STROKE 1 Circadian Variations Influential in Circulatory & Vascular Phenomena Endocrine secretions Thermo regulations Renal Functions Respiratory control Heart Rhythm Hematologic parameters Immune
Sleep Disordered Breathing: Beware Snoring! Dr T A McDonagh Consultant Cardiologist Royal Brompton Hospital London. UK
 Sleep Disordered Breathing: Beware Snoring! Dr T A McDonagh Consultant Cardiologist Royal Brompton Hospital London. UK Sleep Disordered Breathing in CHF Erratic breathing during sleep known for years e.g.
Sleep Disordered Breathing: Beware Snoring! Dr T A McDonagh Consultant Cardiologist Royal Brompton Hospital London. UK Sleep Disordered Breathing in CHF Erratic breathing during sleep known for years e.g.
(To be filled by the treating physician)
") CERTIFICATE OF MEDICAL NECESSITY TO BE ISSUED TO CGHS BENEFICIAREIS BEING PRESCRIBED BILEVEL CONTINUOUS POSITIVE AIRWAY PRESSURE (BI-LEVEL CPAP) / BI-LEVEL VENTILATORY SUPPORT SYSTEM Certification Type
CERTIFICATE OF MEDICAL NECESSITY TO BE ISSUED TO CGHS BENEFICIAREIS BEING PRESCRIBED BILEVEL CONTINUOUS POSITIVE AIRWAY PRESSURE (BI-LEVEL CPAP) / BI-LEVEL VENTILATORY SUPPORT SYSTEM Certification Type
Bi-Level Therapy: Boosting Comfort & Compliance in Apnea Patients
 Bi-Level Therapy: Boosting Comfort & Compliance in Apnea Patients Objectives Describe nocturnal ventilation characteristics that may indicate underlying conditions and benefits of bilevel therapy for specific
Bi-Level Therapy: Boosting Comfort & Compliance in Apnea Patients Objectives Describe nocturnal ventilation characteristics that may indicate underlying conditions and benefits of bilevel therapy for specific
Sleep and the Heart Reversing the Effects of Sleep Apnea to Better Manage Heart Disease
 1 Sleep and the Heart Reversing the Effects of Sleep Apnea to Better Manage Heart Disease Rami Khayat, MD Professor of Internal Medicine Director, OSU Sleep Heart Program Medical Director, Department of
1 Sleep and the Heart Reversing the Effects of Sleep Apnea to Better Manage Heart Disease Rami Khayat, MD Professor of Internal Medicine Director, OSU Sleep Heart Program Medical Director, Department of
AHA Sleep Apnea and Cardiovascular Disease. Slide Set
 AHA 2008 Sleep Apnea and Cardiovascular Disease Slide Set Based on the AHA 2008 Scientific Statement Sleep Apnea and Cardiovascular Disease Virend K. Somers, MD, DPhil, FAHA, FACC Mayo Clinic and Mayo
AHA 2008 Sleep Apnea and Cardiovascular Disease Slide Set Based on the AHA 2008 Scientific Statement Sleep Apnea and Cardiovascular Disease Virend K. Somers, MD, DPhil, FAHA, FACC Mayo Clinic and Mayo
Sleep and the Heart. Sleep Stages. Sleep and the Heart: non REM 8/31/2016
 Sleep and the Heart Overview of sleep Hypertension Arrhythmias Ischemic events CHF Pulmonary Hypertension Cardiac Meds and Sleep Sleep Stages Non-REM sleep(75-80%) Stage 1(5%) Stage 2(50%) Stage 3-4*(15-20%)
Sleep and the Heart Overview of sleep Hypertension Arrhythmias Ischemic events CHF Pulmonary Hypertension Cardiac Meds and Sleep Sleep Stages Non-REM sleep(75-80%) Stage 1(5%) Stage 2(50%) Stage 3-4*(15-20%)
BiPAPS/TVAPSCPAPASV???? Lori Davis, B.Sc., R.C.P.T.(P), RPSGT
, RPSGT") BiPAPS/TVAPSCPAPASV???? Lori Davis, B.Sc., R.C.P.T.(P), RPSGT Modes Continuous Positive Airway Pressure (CPAP): One set pressure which is the same on inspiration and expiration Auto-PAP (APAP) - Provides
BiPAPS/TVAPSCPAPASV???? Lori Davis, B.Sc., R.C.P.T.(P), RPSGT Modes Continuous Positive Airway Pressure (CPAP): One set pressure which is the same on inspiration and expiration Auto-PAP (APAP) - Provides
Recognition and Management of High Loop Gain Sleep Apnea
 Recognition and Management of High Loop Gain Sleep Apnea Robert Joseph Thomas, M.D. Beth Israel Deaconess Medical Center, Boston, MA 02215 Associate Professor of Medicine, Harvard Medical School NEPS 2016
Recognition and Management of High Loop Gain Sleep Apnea Robert Joseph Thomas, M.D. Beth Israel Deaconess Medical Center, Boston, MA 02215 Associate Professor of Medicine, Harvard Medical School NEPS 2016
In-Patient Sleep Testing/Management Boaz Markewitz, MD
 In-Patient Sleep Testing/Management Boaz Markewitz, MD Objectives: Discuss inpatient sleep programs and if they provide a benefit to patients and sleep centers Identify things needed to be considered when
In-Patient Sleep Testing/Management Boaz Markewitz, MD Objectives: Discuss inpatient sleep programs and if they provide a benefit to patients and sleep centers Identify things needed to be considered when
Policy Specific Section: October 1, 2010 January 21, 2013
 Medical Policy Bi-level Positive Airway Pressure (BPAP/NPPV) Type: Medical Necessity/Not Medical Necessity Policy Specific Section: Durable Medical Equipment Original Policy Date: Effective Date: October
Medical Policy Bi-level Positive Airway Pressure (BPAP/NPPV) Type: Medical Necessity/Not Medical Necessity Policy Specific Section: Durable Medical Equipment Original Policy Date: Effective Date: October
Causes and Consequences of Respiratory Centre Depression and Hypoventilation
 Causes and Consequences of Respiratory Centre Depression and Hypoventilation Lou Irving Director Respiratory and Sleep Medicine, RMH louis.irving@mh.org.au Capacity of the Respiratory System At rest During
Causes and Consequences of Respiratory Centre Depression and Hypoventilation Lou Irving Director Respiratory and Sleep Medicine, RMH louis.irving@mh.org.au Capacity of the Respiratory System At rest During
Chronic NIV in heart failure patients: ASV, NIV and CPAP
 Chronic NIV in heart failure patients: ASV, NIV and CPAP João C. Winck, Marta Drummond, Miguel Gonçalves and Tiago Pinto Sleep disordered breathing (SDB), including OSA and central sleep apnoea (CSA),
Chronic NIV in heart failure patients: ASV, NIV and CPAP João C. Winck, Marta Drummond, Miguel Gonçalves and Tiago Pinto Sleep disordered breathing (SDB), including OSA and central sleep apnoea (CSA),
CONTROL OF BREATHING DURING WAKEFULNESS AND SLEEP. Renata Pecotić, M.D., PhD.
 CONTROL OF BREATHING DURING WAKEFULNESS AND SLEEP Renata Pecotić, M.D., PhD. Shev Gul, BSc, NLP & Hypnosis Master Pract, Life and Sports Coach, WSCA, ASCA, ASA GB FIOS(cc) Why do we have to breathe?? Breathing
CONTROL OF BREATHING DURING WAKEFULNESS AND SLEEP Renata Pecotić, M.D., PhD. Shev Gul, BSc, NLP & Hypnosis Master Pract, Life and Sports Coach, WSCA, ASCA, ASA GB FIOS(cc) Why do we have to breathe?? Breathing
National Sleep Disorders Research Plan
 Research Plan Home Foreword Preface Introduction Executive Summary Contents Contact Us National Sleep Disorders Research Plan Return to Table of Contents SECTION 5 - SLEEP DISORDERS SLEEP-DISORDERED BREATHING
Research Plan Home Foreword Preface Introduction Executive Summary Contents Contact Us National Sleep Disorders Research Plan Return to Table of Contents SECTION 5 - SLEEP DISORDERS SLEEP-DISORDERED BREATHING
Sleep Apnea and ifficulty in Extubation. Jean Louis BOURGAIN May 15, 2016
 Sleep Apnea and ifficulty in Extubation Jean Louis BOURGAIN May 15, 2016 Introduction Repetitive collapse of the upper airway > sleep fragmentation, > hypoxemia, hypercapnia, > marked variations in intrathoracic
Sleep Apnea and ifficulty in Extubation Jean Louis BOURGAIN May 15, 2016 Introduction Repetitive collapse of the upper airway > sleep fragmentation, > hypoxemia, hypercapnia, > marked variations in intrathoracic
New Government O2 Criteria and Expert Panel. Jennifer Despain, RPSGT, RST, AS
 New Government O2 Criteria and Expert Panel Jennifer Despain, RPSGT, RST, AS Lead Sleep Technologist, Central Utah Clinic Sleep Disorders Center; Provo, Utah Objectives: Review new government O2 criteria
New Government O2 Criteria and Expert Panel Jennifer Despain, RPSGT, RST, AS Lead Sleep Technologist, Central Utah Clinic Sleep Disorders Center; Provo, Utah Objectives: Review new government O2 criteria
Challenging Cases in Pediatric Polysomnography. Fauziya Hassan, MBBS, MS Assistant Professor Pediatric Pulmonary and Sleep
 Challenging Cases in Pediatric Polysomnography Fauziya Hassan, MBBS, MS Assistant Professor Pediatric Pulmonary and Sleep Conflict of Interest None pertaining to this topic Will be using some slides from
Challenging Cases in Pediatric Polysomnography Fauziya Hassan, MBBS, MS Assistant Professor Pediatric Pulmonary and Sleep Conflict of Interest None pertaining to this topic Will be using some slides from
Dr Alireza Yarahmadi and Dr Arvind Perathur Mercy Medical Center - Winter Retreat Des Moines February 2012
 Dr Alireza Yarahmadi and Dr Arvind Perathur Mercy Medical Center - Winter Retreat Des Moines February 2012 Why screen of OSA prior to surgery? What factors increase the risk? When due to anticipate problems?
Dr Alireza Yarahmadi and Dr Arvind Perathur Mercy Medical Center - Winter Retreat Des Moines February 2012 Why screen of OSA prior to surgery? What factors increase the risk? When due to anticipate problems?
Sleep and the Heart. Physiologic Changes in Cardiovascular Parameters during Sleep
 Sleep and the Heart Rami N. Khayat, MD Professor of Internal Medicine Medical Director, Department of Respiratory Therapy Division of Pulmonary, Critical Care and Sleep Medicine The Ohio State University
Sleep and the Heart Rami N. Khayat, MD Professor of Internal Medicine Medical Director, Department of Respiratory Therapy Division of Pulmonary, Critical Care and Sleep Medicine The Ohio State University
Sleep and the Heart. Rami N. Khayat, MD
 Sleep and the Heart Rami N. Khayat, MD Professor of Internal Medicine Medical Director, Department of Respiratory Therapy Division of Pulmonary, Critical Care and Sleep Medicine The Ohio State University
Sleep and the Heart Rami N. Khayat, MD Professor of Internal Medicine Medical Director, Department of Respiratory Therapy Division of Pulmonary, Critical Care and Sleep Medicine The Ohio State University
OSA and COPD: What happens when the two OVERLAP?
 2011 ISRC Seminar 1 COPD OSA OSA and COPD: What happens when the two OVERLAP? Overlap Syndrome 1 OSA and COPD: What happens when the two OVERLAP? ResMed 10 JAN Global leaders in sleep and respiratory medicine
2011 ISRC Seminar 1 COPD OSA OSA and COPD: What happens when the two OVERLAP? Overlap Syndrome 1 OSA and COPD: What happens when the two OVERLAP? ResMed 10 JAN Global leaders in sleep and respiratory medicine
OSA and cardiovascular disease what is the evidence? Mohan Edupuganti, MD, FACC. Baptist Health Cardiology. Disclosures: None
 OSA and cardiovascular disease what is the evidence? Mohan Edupuganti, MD, FACC. Baptist Health Cardiology. Disclosures: None 1 OSA basics Affects 20-30% of males and 10-15% of females in North America
OSA and cardiovascular disease what is the evidence? Mohan Edupuganti, MD, FACC. Baptist Health Cardiology. Disclosures: None 1 OSA basics Affects 20-30% of males and 10-15% of females in North America
Is CPAP helpful in severe Asthma?
 Is CPAP helpful in severe Asthma? P RAP UN KI TTIVORAVITKUL, M.D. PULMONARY AND CRITICAL CARE DIVISION DEPARTMENT OF MEDICINE, PHRAMONGKUTKLAO HOSPITAL Outlines o Obstructive sleep apnea syndrome (OSAS)
Is CPAP helpful in severe Asthma? P RAP UN KI TTIVORAVITKUL, M.D. PULMONARY AND CRITICAL CARE DIVISION DEPARTMENT OF MEDICINE, PHRAMONGKUTKLAO HOSPITAL Outlines o Obstructive sleep apnea syndrome (OSAS)
Update on Sleep Apnea Diagnosis and Treatment
 Update on Sleep Apnea Diagnosis and Treatment Damien Stevens MD Pulmonary/Critical Care/Sleep Medicine Medical Director KU Medical Center Sleep Laboratory Objectives Discuss physiology of sleep and obstructive
Update on Sleep Apnea Diagnosis and Treatment Damien Stevens MD Pulmonary/Critical Care/Sleep Medicine Medical Director KU Medical Center Sleep Laboratory Objectives Discuss physiology of sleep and obstructive
Sleep Disordered Breathing
 Sleep Disordered Breathing SDB SDB Is an Umbrella Term for Many Disorders characterized by a lack of drive to breathe Results n repetitive pauses in breathing with no effort Occurs for a minimum of 10
Sleep Disordered Breathing SDB SDB Is an Umbrella Term for Many Disorders characterized by a lack of drive to breathe Results n repetitive pauses in breathing with no effort Occurs for a minimum of 10
What is SDB? Obstructive sleep apnea-hypopnea syndrome (OSAHS)
") Have a Good Sleep? Estimated 70 million Americans have clinically significant sleep problems Chronic insomnias report decreased quality of life, memory and attention problems, decreased physical health
Have a Good Sleep? Estimated 70 million Americans have clinically significant sleep problems Chronic insomnias report decreased quality of life, memory and attention problems, decreased physical health
Polysomnography (PSG) (Sleep Studies), Sleep Center
 (Sleep Studies), Sleep Center") Policy Number: 1036 Policy History Approve Date: 07/09/2015 Effective Date: 07/09/2015 Preauthorization All Plans Benefit plans vary in coverage and some plans may not provide coverage for certain service(s)
Policy Number: 1036 Policy History Approve Date: 07/09/2015 Effective Date: 07/09/2015 Preauthorization All Plans Benefit plans vary in coverage and some plans may not provide coverage for certain service(s)
Novel pathophysiological concepts for the development and impact of sleep apnea in CHF.
 Olaf Oldenburg Novel pathophysiological concepts for the development and impact of sleep apnea in CHF. Sleep apnea the need to synchronize the heart, the lung and the brain. Heart Failure 2011 Gothenburg,
Olaf Oldenburg Novel pathophysiological concepts for the development and impact of sleep apnea in CHF. Sleep apnea the need to synchronize the heart, the lung and the brain. Heart Failure 2011 Gothenburg,
1/27/2017 RECOGNITION AND MANAGEMENT OF OBSTRUCTIVE SLEEP APNEA: STRATEGIES TO PREVENT POST-OPERATIVE RESPIRATORY FAILURE DEFINITION PATHOPHYSIOLOGY
 RECOGNITION AND MANAGEMENT OF OBSTRUCTIVE SLEEP APNEA: STRATEGIES TO PREVENT POST-OPERATIVE RESPIRATORY FAILURE Peggy Hollis MSN, RN, ACNS-BC March 9, 2017 DEFINITION Obstructive sleep apnea is a disorder
RECOGNITION AND MANAGEMENT OF OBSTRUCTIVE SLEEP APNEA: STRATEGIES TO PREVENT POST-OPERATIVE RESPIRATORY FAILURE Peggy Hollis MSN, RN, ACNS-BC March 9, 2017 DEFINITION Obstructive sleep apnea is a disorder
Heart Failure and Sleep Disordered Breathing (SDB) Unhappy Bedfellows
 Unhappy Bedfellows") Question Heart Failure and Sleep Disordered Breathing (SDB) Unhappy Bedfellows 1 ResMed 2012 07 2 ResMed 2012 07 Open Airway 3 ResMed 2012 07 Flow Limitation Snore 4 ResMed 2012 07 Apnoea 5 ResMed 2012
Question Heart Failure and Sleep Disordered Breathing (SDB) Unhappy Bedfellows 1 ResMed 2012 07 2 ResMed 2012 07 Open Airway 3 ResMed 2012 07 Flow Limitation Snore 4 ResMed 2012 07 Apnoea 5 ResMed 2012
COMPLEX SLEEP APNEA IS IT A DISEASE? David Claman, MD UCSF Sleep Disorders Center
 COMPLEX SLEEP APNEA IS IT A DISEASE? David Claman, MD UCSF Sleep Disorders Center CENTRAL APNEA Central Apnea Index > 5 ( >50% of apnea are central) Mayo Clinic Proc 1990; 65:1255 APNEA AT SLEEP ONSET
COMPLEX SLEEP APNEA IS IT A DISEASE? David Claman, MD UCSF Sleep Disorders Center CENTRAL APNEA Central Apnea Index > 5 ( >50% of apnea are central) Mayo Clinic Proc 1990; 65:1255 APNEA AT SLEEP ONSET
MCOEM Spring Chapter Meeting April 5, Sleep Apnea An Overview with Emphasis on Cardiovascular Correlations Jacques Conaway, MD
 MCOEM Spring Chapter Meeting April 5, 2014 Sleep Apnea An Overview with Emphasis on Cardiovascular Correlations Jacques Conaway, MD Case Presentation History of Present Illness 57 year old man with ihh/
MCOEM Spring Chapter Meeting April 5, 2014 Sleep Apnea An Overview with Emphasis on Cardiovascular Correlations Jacques Conaway, MD Case Presentation History of Present Illness 57 year old man with ihh/
Opioid adverse reactions not the usual suspects! DR ANDREW DAVIES
 Opioid adverse reactions not the usual suspects! DR ANDREW DAVIES Overview Introduction Musical hallucinations Charles Bonnet syndrome (Nightmares, vivid dreams) Sleep disordered breathing Sphincter of
Opioid adverse reactions not the usual suspects! DR ANDREW DAVIES Overview Introduction Musical hallucinations Charles Bonnet syndrome (Nightmares, vivid dreams) Sleep disordered breathing Sphincter of
Sleep Diordered Breathing (Part 1)
") Sleep Diordered Breathing (Part 1) History (for more topics & presentations, visit ) Obstructive sleep apnea - first described by Charles Dickens in 1836 in Papers of the Pickwick Club, Dickens depicted
Sleep Diordered Breathing (Part 1) History (for more topics & presentations, visit ) Obstructive sleep apnea - first described by Charles Dickens in 1836 in Papers of the Pickwick Club, Dickens depicted
more than 50% of adults weigh more than 20% above optimum
 In the US: more than 50% of adults weigh more than 20% above optimum >30 kg m -2 obesity >40 kg m -2 morbid obesity BMI = weight(kg) / height(m 2 ) Pounds X 2.2 Inches divided by 39, squared From 2000
In the US: more than 50% of adults weigh more than 20% above optimum >30 kg m -2 obesity >40 kg m -2 morbid obesity BMI = weight(kg) / height(m 2 ) Pounds X 2.2 Inches divided by 39, squared From 2000
Σύνδρομο σπνικής άπνοιας. Ποιός o ρόλος ηοσ ζηη γένεζη και ανηιμεηώπιζη ηων αρρσθμιών;
 Σύνδρομο σπνικής άπνοιας. Ποιός o ρόλος ηοσ ζηη γένεζη και ανηιμεηώπιζη ηων αρρσθμιών; E.N. Σημανηηράκης MD, FESC Επίκ. Καθηγηηής Καρδιολογίας Πανεπιζηημιακό Νοζοκομείο Ηρακλείοσ Epidemiology 4% 2% 24%
Σύνδρομο σπνικής άπνοιας. Ποιός o ρόλος ηοσ ζηη γένεζη και ανηιμεηώπιζη ηων αρρσθμιών; E.N. Σημανηηράκης MD, FESC Επίκ. Καθηγηηής Καρδιολογίας Πανεπιζηημιακό Νοζοκομείο Ηρακλείοσ Epidemiology 4% 2% 24%
Sleep Apnea: Vascular and Metabolic Complications
 Sleep Apnea: Vascular and Metabolic Complications Vahid Mohsenin, M.D. Professor of Medicine Yale University School of Medicine Director, Yale Center for Sleep Medicine Definitions Apnea: Cessation of
Sleep Apnea: Vascular and Metabolic Complications Vahid Mohsenin, M.D. Professor of Medicine Yale University School of Medicine Director, Yale Center for Sleep Medicine Definitions Apnea: Cessation of
Auto Servo Ventilation Indications, Basics of Algorithm, and Titration
 Auto Servo Ventilation Indications, Basics of Algorithm, and Titration 1 ASV Learning Objectives Understand the indications for Auto Servo Ventilation Differentiate obstructive versus central hypopneas
Auto Servo Ventilation Indications, Basics of Algorithm, and Titration 1 ASV Learning Objectives Understand the indications for Auto Servo Ventilation Differentiate obstructive versus central hypopneas
Reasons Providers Use Bilevel
 Reasons Providers Use Bilevel More comfort, improve therapy compliance Noncompliant OSA (NCOSA) 1 Scripts from lab referrals Central/Complex Sleep Apnea 2 For ventilations needs Restrictive Thoracic Disorders/Neuromuscular
Reasons Providers Use Bilevel More comfort, improve therapy compliance Noncompliant OSA (NCOSA) 1 Scripts from lab referrals Central/Complex Sleep Apnea 2 For ventilations needs Restrictive Thoracic Disorders/Neuromuscular
Dear, Respectfully, United Sleep Centers SLEEP STUDY DATE: FEBUARY 26, 2015 AT OUR DOWNEY CENTER TIME: 10PM, PLEASE ARRIVE ON TIME
 Sleep Study Instructions SLEEP STUDY DATE: FEBUARY 26, 2015 AT OUR DOWNEY CENTER TIME: 10PM, PLEASE ARRIVE ON TIME ADDRESS: 11411 BROOKSHIRE AVE SUITE 505 DOWNEY, CA Dear, Thank you for choosing us as
Sleep Study Instructions SLEEP STUDY DATE: FEBUARY 26, 2015 AT OUR DOWNEY CENTER TIME: 10PM, PLEASE ARRIVE ON TIME ADDRESS: 11411 BROOKSHIRE AVE SUITE 505 DOWNEY, CA Dear, Thank you for choosing us as
Alaska Sleep Education Center
 Alaska Sleep Education Center The 3 Types of Sleep Apnea Explained: Obstructive, Central, & Mixed Posted by Kevin Phillips on Jan 28, 2015 6:53:00 PM Sleep apnea is a very common sleep disorder, affecting
Alaska Sleep Education Center The 3 Types of Sleep Apnea Explained: Obstructive, Central, & Mixed Posted by Kevin Phillips on Jan 28, 2015 6:53:00 PM Sleep apnea is a very common sleep disorder, affecting
Sleep Apnea: Diagnosis & Treatment
 Disclosure Sleep Apnea: Diagnosis & Treatment Lawrence J. Epstein, MD Sleep HealthCenters Harvard Medical School Chief Medical Officer for Sleep HealthCenters Sleep medicine specialty practice group Consultant
Disclosure Sleep Apnea: Diagnosis & Treatment Lawrence J. Epstein, MD Sleep HealthCenters Harvard Medical School Chief Medical Officer for Sleep HealthCenters Sleep medicine specialty practice group Consultant
SLEEP DISORDERED BREATHING The Clinical Conditions
 SLEEP DISORDERED BREATHING The Clinical Conditions Robert G. Hooper, M.D. In the previous portion of this paper, the definitions of the respiratory events that are the hallmarks of problems with breathing
SLEEP DISORDERED BREATHING The Clinical Conditions Robert G. Hooper, M.D. In the previous portion of this paper, the definitions of the respiratory events that are the hallmarks of problems with breathing
Edoardo Gronda UO cardiologia e Ricerca Dipartimento Cardiovascolare IRCCS MultiMedica
 Convegno Pneumologia 2016 Milano 16-18 giugno 2016 Centro Congressi Palazzo delle Stelline Edoardo Gronda UO cardiologia e Ricerca Dipartimento Cardiovascolare IRCCS MultiMedica Central apnea 10 second
Convegno Pneumologia 2016 Milano 16-18 giugno 2016 Centro Congressi Palazzo delle Stelline Edoardo Gronda UO cardiologia e Ricerca Dipartimento Cardiovascolare IRCCS MultiMedica Central apnea 10 second
SLEEP DISORDERED BREATHING AND CHRONIC LUNG DISEASE: UPDATE ON OVERLAP SYNDROMES
 SLEEP DISORDERED BREATHING AND CHRONIC LUNG DISEASE: UPDATE ON OVERLAP SYNDROMES ROBERT OWENS, MD ASSISTANT CLINICAL PROFESSOR OF MEDICINE UNIVERSITY OF CALIFORNIA AT SAN DIEGO LA JOLLA, CA Robert L. Owens,
SLEEP DISORDERED BREATHING AND CHRONIC LUNG DISEASE: UPDATE ON OVERLAP SYNDROMES ROBERT OWENS, MD ASSISTANT CLINICAL PROFESSOR OF MEDICINE UNIVERSITY OF CALIFORNIA AT SAN DIEGO LA JOLLA, CA Robert L. Owens,
Outline. Major variables contributing to airway patency/collapse. OSA- Definition
 Outline Alicia Gruber Kalamas, MD Associate Clinical Professor of Anesthesia & Perioperative Care University of California, San Francisco September 2011 Definition Pathophysiology Patient Risk Factors
Outline Alicia Gruber Kalamas, MD Associate Clinical Professor of Anesthesia & Perioperative Care University of California, San Francisco September 2011 Definition Pathophysiology Patient Risk Factors
Obstructive sleep apnea (OSA) is the periodic reduction
 is the periodic reduction") Obstructive Sleep Apnea and Oxygen Therapy: A Systematic Review of the Literature and Meta-Analysis 1 Department of Anesthesiology, Toronto Western Hospital, University Health Network, University of Toronto,
Obstructive Sleep Apnea and Oxygen Therapy: A Systematic Review of the Literature and Meta-Analysis 1 Department of Anesthesiology, Toronto Western Hospital, University Health Network, University of Toronto,
Respiratory/Sleep Disorder Breathing (SDB) SDB is highly prevalent, under recognized, under reported and under treated
 SDB is highly prevalent, under recognized, under reported and under treated") Respiratory/Sleep Disorder Breathing (SDB) Definitions SDB is highly prevalent, under recognized, under reported and under treated Central 1. Central sleep apnea (CSA) is defined by the cessation of air
Respiratory/Sleep Disorder Breathing (SDB) Definitions SDB is highly prevalent, under recognized, under reported and under treated Central 1. Central sleep apnea (CSA) is defined by the cessation of air
High Flow Nasal Cannula in Children During Sleep. Brian McGinley M.D. Associate Professor of Pediatrics University of Utah
 High Flow Nasal Cannula in Children During Sleep Brian McGinley M.D. Associate Professor of Pediatrics University of Utah Disclosures Conflicts of Interest: None Will discuss a product that is commercially
High Flow Nasal Cannula in Children During Sleep Brian McGinley M.D. Associate Professor of Pediatrics University of Utah Disclosures Conflicts of Interest: None Will discuss a product that is commercially
Opioid use in COPD: balancing benefits and harms. St. Michael s Hospital, University of Toronto
 Opioid use in COPD: balancing benefits and harms Nicholas Vozoris MHSc, MD, FRCPC Assistant Professor St. Michael s Hospital, University of Toronto Conflicts of interest None None of my own drug safety
Opioid use in COPD: balancing benefits and harms Nicholas Vozoris MHSc, MD, FRCPC Assistant Professor St. Michael s Hospital, University of Toronto Conflicts of interest None None of my own drug safety
Apnea-Hypopnea- Index The new old biomarker for Sleep-Disordered Breathing. Alan S Maisel MD
 Apnea-Hypopnea- Index The new old biomarker for Sleep-Disordered Breathing Alan S Maisel MD Triumvirate of Health-public awareness 1.8% Sleep Physical Fitness Nutrition 91.3% 99.9% Sleep is important to
Apnea-Hypopnea- Index The new old biomarker for Sleep-Disordered Breathing Alan S Maisel MD Triumvirate of Health-public awareness 1.8% Sleep Physical Fitness Nutrition 91.3% 99.9% Sleep is important to
Opioid Review and MAT Clinic Comorbidities Associated with Opioid Overdose
 1 Opioid Review and MAT Clinic Comorbidities Associated with Opioid Overdose March 7, 2018 Learning Objectives Differentiate the medical diagnoses that increase the risk of taking opioids Identify the
1 Opioid Review and MAT Clinic Comorbidities Associated with Opioid Overdose March 7, 2018 Learning Objectives Differentiate the medical diagnoses that increase the risk of taking opioids Identify the
ROBERT C. PRITCHARD DIRECTOR MICHAEL O. FOSTER ASSISTANT DIR. SLEEP APNEA
 ROBERT C. PRITCHARD DIRECTOR MICHAEL O. FOSTER ASSISTANT DIR. SLEEP APNEA A Person is physically qualified to drive a motor vehicle if that person; -(5) has no established medical history or clinical diagnosis
ROBERT C. PRITCHARD DIRECTOR MICHAEL O. FOSTER ASSISTANT DIR. SLEEP APNEA A Person is physically qualified to drive a motor vehicle if that person; -(5) has no established medical history or clinical diagnosis
Pain patient with sleep-disordered breathing
 Pain patient with sleep-disordered breathing Clinical scenario: A 50-year old female with a history of acid reflux, fibromyalgia, spinal stenosis and degenerative disk disease s/p C3/C4 disk fusion, depression
Pain patient with sleep-disordered breathing Clinical scenario: A 50-year old female with a history of acid reflux, fibromyalgia, spinal stenosis and degenerative disk disease s/p C3/C4 disk fusion, depression
General Outline. General Outline. Pathogenesis of Metabolic Dysfunction in Sleep Apnea: The Role of Sleep Fragmentation and Intermittent Hypoxemia
 Pathogenesis of Metabolic in Sleep Apnea: The Role of Sleep Fragmentation and Intermittent Hypoxemia Naresh M. Punjabi, MD, PhD Associate Professor of Medicine and Epidemiology Johns Hopkins University,
Pathogenesis of Metabolic in Sleep Apnea: The Role of Sleep Fragmentation and Intermittent Hypoxemia Naresh M. Punjabi, MD, PhD Associate Professor of Medicine and Epidemiology Johns Hopkins University,
Medicare C/D Medical Coverage Policy. Respiratory Assist Devices for Obstructive Sleep Apnea and Breathing Related Sleep Disorders
 Medicare C/D Medical Coverage Policy Respiratory Assist Devices for Obstructive Sleep Apnea and Breathing Related Sleep Disorders Origination: June 26, 2000 Review Date: January 18, 2017 Next Review January,
Medicare C/D Medical Coverage Policy Respiratory Assist Devices for Obstructive Sleep Apnea and Breathing Related Sleep Disorders Origination: June 26, 2000 Review Date: January 18, 2017 Next Review January,
PAP Therapy Devices: Delivering the Right Therapy To The Right Patient. Ryan Schmidt, BS, RRT Clinical Specialist Philips Respironics
 PAP Therapy Devices: Delivering the Right Therapy To The Right Patient Ryan Schmidt, BS, RRT Clinical Specialist Philips Respironics Conflict of Interest Disclosure(s) I do not have any potential conflicts
PAP Therapy Devices: Delivering the Right Therapy To The Right Patient Ryan Schmidt, BS, RRT Clinical Specialist Philips Respironics Conflict of Interest Disclosure(s) I do not have any potential conflicts
Pediatric Sleep-Disordered Breathing
 Pediatric Sleep-Disordered Breathing OSA in infants and young children is generally characterized by partial, persistent obstruction of the upper airway Continuum Benign primary snoring Upper-airway resistance
Pediatric Sleep-Disordered Breathing OSA in infants and young children is generally characterized by partial, persistent obstruction of the upper airway Continuum Benign primary snoring Upper-airway resistance
CAPNOGRAPHY in the SLEEP CENTER Julie DeWitte, RCP, RPSGT, RST Assistant Department Administrator Kaiser Permanente Fontana Sleep Center
 FOCUS Fall 2018 CAPNOGRAPHY in the SLEEP CENTER Julie DeWitte, RCP, RPSGT, RST Assistant Department Administrator Kaiser Permanente Fontana Sleep Center 1 Learning Objectives The future of in laboratory
FOCUS Fall 2018 CAPNOGRAPHY in the SLEEP CENTER Julie DeWitte, RCP, RPSGT, RST Assistant Department Administrator Kaiser Permanente Fontana Sleep Center 1 Learning Objectives The future of in laboratory
Management of OSA in the Acute Care Environment. Robert S. Campbell, RRT FAARC HRC, Philips Healthcare May, 2018
 Management of OSA in the Acute Care Environment Robert S. Campbell, RRT FAARC HRC, Philips Healthcare May, 2018 1 Learning Objectives Upon completion, the participant should be able to: Understand pathology
Management of OSA in the Acute Care Environment Robert S. Campbell, RRT FAARC HRC, Philips Healthcare May, 2018 1 Learning Objectives Upon completion, the participant should be able to: Understand pathology
Anesthetic Risks of Obstructive Sleep Apnea in Children
 Anesthetic Risks of Obstructive Sleep Apnea in Children Dawn M. Sweeney, M.D. Associate Professor of Anesthesiology and Pediatrics University of Rochester Medical Center Risk Factors for OSA in Children
Anesthetic Risks of Obstructive Sleep Apnea in Children Dawn M. Sweeney, M.D. Associate Professor of Anesthesiology and Pediatrics University of Rochester Medical Center Risk Factors for OSA in Children
Sleep Apnea in Women: How Is It Different?
 Sleep Apnea in Women: How Is It Different? Grace Pien, MD, MSCE Division of Pulmonary and Critical Care Department of Medicine Johns Hopkins School of Medicine 16 February 2018 Outline Prevalence Clinical
Sleep Apnea in Women: How Is It Different? Grace Pien, MD, MSCE Division of Pulmonary and Critical Care Department of Medicine Johns Hopkins School of Medicine 16 February 2018 Outline Prevalence Clinical
PEDIATRIC OBSTRUCTIVE SLEEP APNEA (OSA)
") PEDIATRIC OBSTRUCTIVE SLEEP APNEA (OSA) DEFINITION OSA Inspiratory airflow is either partly (hypopnea) or completely (apnea) occluded during sleep. The combination of sleep-disordered breathing with daytime
PEDIATRIC OBSTRUCTIVE SLEEP APNEA (OSA) DEFINITION OSA Inspiratory airflow is either partly (hypopnea) or completely (apnea) occluded during sleep. The combination of sleep-disordered breathing with daytime
Index. sleep.theclinics.com. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Accidents. See Motor vehicle accidents. Acetazolamide, in OSA therapy, 531 Acetylcholinesterase inhibitors, in OSA therapy, 532 533 Acromegaly,
Note: Page numbers of article titles are in boldface type. A Accidents. See Motor vehicle accidents. Acetazolamide, in OSA therapy, 531 Acetylcholinesterase inhibitors, in OSA therapy, 532 533 Acromegaly,
Complex Sleep Apnea. Can we do better? David Weed D.O.,FCCP,FAASM. September 8, 2016
 Complex Sleep Apnea Can we do better? David Weed D.O.,FCCP,FAASM September 8, 2016 If you don t know where you are going, you ll end up somewhere else. Yogi Berra Objectives Discuss what syndromes comprise
Complex Sleep Apnea Can we do better? David Weed D.O.,FCCP,FAASM September 8, 2016 If you don t know where you are going, you ll end up somewhere else. Yogi Berra Objectives Discuss what syndromes comprise
Sleep and Neuromuscular Disease. Sharon De Cruz, MD Tisha Wang, MD
 Sleep and Neuromuscular Disease Sharon De Cruz, MD Tisha Wang, MD Case Presentation Part I GR is a 21-year old male with Becker muscular dystrophy who comes to your office complaining of progressively
Sleep and Neuromuscular Disease Sharon De Cruz, MD Tisha Wang, MD Case Presentation Part I GR is a 21-year old male with Becker muscular dystrophy who comes to your office complaining of progressively
The Sleep-Stroke Connection: An Under-recognized Entity. Simin Khavandgar MD UPMC Neurology Department
 The Sleep-Stroke Connection: An Under-recognized Entity Simin Khavandgar MD UPMC Neurology Department Sleep Disordered Breathing (SDB) Obstructive Sleep Apnea (OSA): -Transient cessation of airflow, duration
The Sleep-Stroke Connection: An Under-recognized Entity Simin Khavandgar MD UPMC Neurology Department Sleep Disordered Breathing (SDB) Obstructive Sleep Apnea (OSA): -Transient cessation of airflow, duration
Choosing the Appropriate Mode of PAP Therapy in the Perioperative Setting
 Choosing the Appropriate Mode of PAP Therapy in the Perioperative Setting Lisa F. Wolfe MD Northwestern University Chicago, Illinois Choosing the Appropriate Mode of PAP Therapy in the Perioperative Setting
Choosing the Appropriate Mode of PAP Therapy in the Perioperative Setting Lisa F. Wolfe MD Northwestern University Chicago, Illinois Choosing the Appropriate Mode of PAP Therapy in the Perioperative Setting
Obstructive Sleep Apnea and COPD overlap syndrome. Financial Disclosures. Outline 11/1/2016
 Obstructive Sleep Apnea and COPD overlap syndrome Chitra Lal, MD, FCCP, FAASM Associate Professor of Medicine, Pulmonary, Critical Care, and Sleep, Medical University of South Carolina Financial Disclosures
Obstructive Sleep Apnea and COPD overlap syndrome Chitra Lal, MD, FCCP, FAASM Associate Professor of Medicine, Pulmonary, Critical Care, and Sleep, Medical University of South Carolina Financial Disclosures
Index SLEEP MEDICINE CLINICS. Note: Page numbers of article titles are in boldface type.
 549 SLEEP MEDICINE CLINICS Sleep Med Clin 1 (2007) 549 553 Note: Page numbers of article titles are in boldface type. A Abdominal motion, in assessment of sleep-related breathing disorders, 452 454 Adherence,
549 SLEEP MEDICINE CLINICS Sleep Med Clin 1 (2007) 549 553 Note: Page numbers of article titles are in boldface type. A Abdominal motion, in assessment of sleep-related breathing disorders, 452 454 Adherence,
PVDOMICS. Sleep Core. Cleveland Clinic Cleveland, Ohio
 PVDOMICS Sleep Core Rawan Nawabit, Research Coordinator and Polysomnologist Joan Aylor, Research Coordinator Dr. Reena Mehra, Co-Investigator, Sleep Core Lead Cleveland Clinic Cleveland, Ohio 1 Obstructive
PVDOMICS Sleep Core Rawan Nawabit, Research Coordinator and Polysomnologist Joan Aylor, Research Coordinator Dr. Reena Mehra, Co-Investigator, Sleep Core Lead Cleveland Clinic Cleveland, Ohio 1 Obstructive
A Deadly Combination: Central Sleep Apnea & Heart Failure
 A Deadly Combination: Central Sleep Apnea & Heart Failure Sanjaya Gupta, MD FACC FHRS Ohio State University Symposium May 10 th, 2018 Disclosures Boston Scientific: fellowship support, speaking honoraria
A Deadly Combination: Central Sleep Apnea & Heart Failure Sanjaya Gupta, MD FACC FHRS Ohio State University Symposium May 10 th, 2018 Disclosures Boston Scientific: fellowship support, speaking honoraria
Obstructive sleep apnoea How to identify?
 Obstructive sleep apnoea How to identify? Walter McNicholas MD Newman Professor in Medicine, St. Vincent s University Hospital, University College Dublin, Ireland. Potential conflict of interest None Obstructive
Obstructive sleep apnoea How to identify? Walter McNicholas MD Newman Professor in Medicine, St. Vincent s University Hospital, University College Dublin, Ireland. Potential conflict of interest None Obstructive
Childhood Obstructive Sleep Apnea
 Childhood Obstructive Sleep Apnea 1 PROF. RAJESHWAR DAYAL MD, FAMS,FIAP,DNB, DCH (LONDON) NATIONAL CONVENOR,IAP SLEEP PROGRAM NATIONAL VICE PRESIDENT IAP 2011 HEAD DEPARTMENT OF PAEDIATRICS S. N. MEDICAL
Childhood Obstructive Sleep Apnea 1 PROF. RAJESHWAR DAYAL MD, FAMS,FIAP,DNB, DCH (LONDON) NATIONAL CONVENOR,IAP SLEEP PROGRAM NATIONAL VICE PRESIDENT IAP 2011 HEAD DEPARTMENT OF PAEDIATRICS S. N. MEDICAL
DECLARATION OF CONFLICT OF INTEREST
 DECLARATION OF CONFLICT OF INTEREST Obstructive sleep apnoea How to identify? Walter McNicholas MD Newman Professor in Medicine, St. Vincent s University Hospital, University College Dublin, Ireland. Potential
DECLARATION OF CONFLICT OF INTEREST Obstructive sleep apnoea How to identify? Walter McNicholas MD Newman Professor in Medicine, St. Vincent s University Hospital, University College Dublin, Ireland. Potential
Julie Zimmerman, MSN, RN, CCRN Clinical Nurse Specialist
 Julie Zimmerman, MSN, RN, CCRN Clinical Nurse Specialist Objectives Define capnography vs. end tidal CO2 (EtCO 2 ) Identify what normal vs. abnormal EtCO2 values mean and what to do Understand when to
Julie Zimmerman, MSN, RN, CCRN Clinical Nurse Specialist Objectives Define capnography vs. end tidal CO2 (EtCO 2 ) Identify what normal vs. abnormal EtCO2 values mean and what to do Understand when to
Average volume-assured pressure support
 Focused review Average volume-assured pressure support Abdurahim Aloud MD Abstract Average volume-assured pressure support (AVAPS) is a relatively new mode of noninvasive positive pressure ventilation
Focused review Average volume-assured pressure support Abdurahim Aloud MD Abstract Average volume-assured pressure support (AVAPS) is a relatively new mode of noninvasive positive pressure ventilation
The most accurate predictors of arterial hypertension in patients with Obstructive Sleep Apnea Syndrome
 The most accurate predictors of arterial hypertension in patients with Obstructive Sleep Apnea Syndrome Natsios Georgios University Hospital of Larissa, Greece Definitions Obstructive Sleep Apnea (OSA)
The most accurate predictors of arterial hypertension in patients with Obstructive Sleep Apnea Syndrome Natsios Georgios University Hospital of Larissa, Greece Definitions Obstructive Sleep Apnea (OSA)
TEAM Educational Module Page 1 of 11
 TEAM Educational Module Page 1 of 11 Control of Breathing during Wakefulness and Sleep Learning Objectives:? Describe the elements of ventilatory control (e.g. central control of rate and depth, chemo-
TEAM Educational Module Page 1 of 11 Control of Breathing during Wakefulness and Sleep Learning Objectives:? Describe the elements of ventilatory control (e.g. central control of rate and depth, chemo-
Pre-Operative Services Teaching Rounds 11 March 2011
 Pre-Operative Services Teaching Rounds 11 March 2011 Deborah Richman MBChB FFA(SA) Director Pre-Operative Services Department of Anesthesia Stony Brook University Medical Center, NY drichman@notes.cc.sunysb.edu
Pre-Operative Services Teaching Rounds 11 March 2011 Deborah Richman MBChB FFA(SA) Director Pre-Operative Services Department of Anesthesia Stony Brook University Medical Center, NY drichman@notes.cc.sunysb.edu
UCSD Pulmonary and Critical Care
 Sleep Apnea Phenotyping Atul Malhotra, MD amalhotra@ucsd.edu UCSD Pulmonary and Critical Care Director of Sleep Medicine NAMDRC 2014 Dr. Malhotra has declared no conflicts of interest related to the content
Sleep Apnea Phenotyping Atul Malhotra, MD amalhotra@ucsd.edu UCSD Pulmonary and Critical Care Director of Sleep Medicine NAMDRC 2014 Dr. Malhotra has declared no conflicts of interest related to the content
Dr. Karan Madan Senior Resident
 SLEEP DISORDERED BREATHING DIAGNOSIS & MANAGEMENT Dr. Karan Madan Senior Resident Department of Pulmonary medicine Sleep disordered breathing (SDB) Definition- Sleep-disordered breathing (SDB) is present
SLEEP DISORDERED BREATHING DIAGNOSIS & MANAGEMENT Dr. Karan Madan Senior Resident Department of Pulmonary medicine Sleep disordered breathing (SDB) Definition- Sleep-disordered breathing (SDB) is present
Observations on Sleep Apnoea and Cardiac disease
 Observations on Sleep Apnoea and Cardiac disease Tim Sutton, Cardiologist Middlemore Hospital What is sleep? a naturally recurring state of relatively suspended sensory and motor activity, characterized
Observations on Sleep Apnoea and Cardiac disease Tim Sutton, Cardiologist Middlemore Hospital What is sleep? a naturally recurring state of relatively suspended sensory and motor activity, characterized
Diabetes & Obstructive Sleep Apnoea risk. Jaynie Pateraki MSc RGN
 Diabetes & Obstructive Sleep Apnoea risk Jaynie Pateraki MSc RGN Non-REM - REM - Both - Unrelated - Common disorders of Sleep Sleep Walking Night terrors Periodic leg movements Sleep automatism Nightmares
Diabetes & Obstructive Sleep Apnoea risk Jaynie Pateraki MSc RGN Non-REM - REM - Both - Unrelated - Common disorders of Sleep Sleep Walking Night terrors Periodic leg movements Sleep automatism Nightmares
Sleep and Stroke. M.V. Padma Srivastava Department of Neurology All-India Institute of Medical Sciences, New Delhi ABSTRACT
 Ann Natl Acad Med Sci (India), 49(3&4): 169-176, 2013 Sleep and Stroke M.V. Padma Srivastava Department of Neurology All-India Institute of Medical Sciences, New Delhi Circadian variations in conjunction
Ann Natl Acad Med Sci (India), 49(3&4): 169-176, 2013 Sleep and Stroke M.V. Padma Srivastava Department of Neurology All-India Institute of Medical Sciences, New Delhi Circadian variations in conjunction
Medical Affairs Policy
 Medical Affairs Policy Service: Sleep Disorder Treatment: Positive Airway Pressure Devices and Oral Appliances (CPAP, BPAP, BiPAP, BiPAP ST, BiPAP with backup, BiPAP -Auto SV, VPAP, VPAP Adapt, VPAP adapt
Medical Affairs Policy Service: Sleep Disorder Treatment: Positive Airway Pressure Devices and Oral Appliances (CPAP, BPAP, BiPAP, BiPAP ST, BiPAP with backup, BiPAP -Auto SV, VPAP, VPAP Adapt, VPAP adapt
SHORT TERM EFFECTS OF NIV ON SLEEP IN END STAGE CF. Moran Lavie MD The national center for Cystic Fibrosis Sheba medical center
 SHORT TERM EFFECTS OF NIV ON SLEEP IN END STAGE CF Moran Lavie MD The national center for Cystic Fibrosis Sheba medical center Sleeping with CF (1) In CF, sleep can place a significant physiologic load
SHORT TERM EFFECTS OF NIV ON SLEEP IN END STAGE CF Moran Lavie MD The national center for Cystic Fibrosis Sheba medical center Sleeping with CF (1) In CF, sleep can place a significant physiologic load
3/10/2014. Pearls to Remember. 1) Consequences of OSA related to both arousals and hypoxia. 2) Arousals provoke increased
 Consequences of OSA related to both arousals and hypoxia. 2) Arousals provoke increased") Cardiovascular disease and Sleep Disorders Timothy L. Grant, M.D.,F.A.A.S.M. Medical Director Baptist Sleep Center at Sunset Medical Director Baptist Sleep Education Series Medical Director Sleep Division
Cardiovascular disease and Sleep Disorders Timothy L. Grant, M.D.,F.A.A.S.M. Medical Director Baptist Sleep Center at Sunset Medical Director Baptist Sleep Education Series Medical Director Sleep Division
Objectives. Health care significance of ARF 9/10/15 TREATMENT OF ACUTE RESPIRATORY FAILURE OF VARIABLE CAUSES: INVASIVE VS. NON- INVASIVE VENTILATION
 TREATMENT OF ACUTE RESPIRATORY FAILURE OF VARIABLE CAUSES: INVASIVE VS. NON- INVASIVE VENTILATION Louisa Chika Ikpeama, DNP, CCRN, ACNP-BC Objectives Identify health care significance of acute respiratory
TREATMENT OF ACUTE RESPIRATORY FAILURE OF VARIABLE CAUSES: INVASIVE VS. NON- INVASIVE VENTILATION Louisa Chika Ikpeama, DNP, CCRN, ACNP-BC Objectives Identify health care significance of acute respiratory
Anesthetic Challenges in Morbid Obesity
 Anesthetic Challenges in Morbid Obesity The Challenge Postoperative pain management of the morbid obese patient The number of patients who present for elective surgery, with a BMI of greater than 30 kgm
Anesthetic Challenges in Morbid Obesity The Challenge Postoperative pain management of the morbid obese patient The number of patients who present for elective surgery, with a BMI of greater than 30 kgm
Overlap Syndrome. José M. Marin Hospital Universitario Miguel Servet Zaragoza, Spain.
 Overlap Syndrome José M. Marin Hospital Universitario Miguel Servet Zaragoza, Spain. I have nothing to disclose. Agenda Effects of sleep on breathing Sleep in COPD The Overlap Syndrome Treatment of the
Overlap Syndrome José M. Marin Hospital Universitario Miguel Servet Zaragoza, Spain. I have nothing to disclose. Agenda Effects of sleep on breathing Sleep in COPD The Overlap Syndrome Treatment of the
Sleep Disorders and the Metabolic Syndrome
 Sleep Disorders and the Metabolic Syndrome Tom V. Cloward, M.D. Intermountain Sleep Disorders Center LDS Hospital Objectives Describe how sleep disorders impact your daily medical practice Don Don t do
Sleep Disorders and the Metabolic Syndrome Tom V. Cloward, M.D. Intermountain Sleep Disorders Center LDS Hospital Objectives Describe how sleep disorders impact your daily medical practice Don Don t do
BTS sleep Course. Module 10 Therapies I: Mechanical Intervention Devices (Prepared by Debby Nicoll and Debbie Smith)
") BTS sleep Course Module 10 Therapies I: Mechanical Intervention Devices (Prepared by Debby Nicoll and Debbie Smith) S1: Overview of OSA Definition History Prevalence Pathophysiology Causes Consequences
BTS sleep Course Module 10 Therapies I: Mechanical Intervention Devices (Prepared by Debby Nicoll and Debbie Smith) S1: Overview of OSA Definition History Prevalence Pathophysiology Causes Consequences
Identification and Treatment of the Patient with Sleep Related Hypoventilation
 Identification and Treatment of the Patient with Sleep Related Hypoventilation Hillary Loomis-King, MD Pulmonary and Critical Care of NW MI Munson Sleep Disorders Center X Conflict of Interest Disclosures
Identification and Treatment of the Patient with Sleep Related Hypoventilation Hillary Loomis-King, MD Pulmonary and Critical Care of NW MI Munson Sleep Disorders Center X Conflict of Interest Disclosures
Are We Sure That Obstructive Sleep Apnea Is Not a Risk factor for Atrial Fibrillation in the Elderly Population?
 ISPUB.COM The Internet Journal of Geriatrics and Gerontology Volume 6 Number 1 Are We Sure That Obstructive Sleep Apnea Is Not a Risk factor for Atrial Fibrillation in the Elderly H Ganga, Y Thangaraj,
ISPUB.COM The Internet Journal of Geriatrics and Gerontology Volume 6 Number 1 Are We Sure That Obstructive Sleep Apnea Is Not a Risk factor for Atrial Fibrillation in the Elderly H Ganga, Y Thangaraj,
Ron Hosp, MS-HSA, RRT Regional Respiratory Specialist. This program has been approved for 1 hour of continuing education credit.
 Ron Hosp, MS-HSA, RRT Regional Respiratory Specialist This program has been approved for 1 hour of continuing education credit. Course Objectives Identify at least four goals of home NIV Identify candidates
Ron Hosp, MS-HSA, RRT Regional Respiratory Specialist This program has been approved for 1 hour of continuing education credit. Course Objectives Identify at least four goals of home NIV Identify candidates