Pediatric Difficult Airway Management. R2 Nichakan Rewurai R2 Pattiya Suttidate Supervisor: Assist. Prof. Sahatsa Mandee
|
|
|
- Shannon Hood
- 5 years ago
- Views:
Transcription
1 Pediatric Difficult Airway Management R2 Nichakan Rewurai R2 Pattiya Suttidate Supervisor: Assist. Prof. Sahatsa Mandee
: i3 i5 (2016)")
2 The pediatric difficult airway is associated with a high risk for complications during airway management N. Jagannathan,British Journal of Anaesthesia 117 (S1): i3 i5 (2016)

3 Pediatric difficult airway management: What every anesthetist should know! The pediatric difficult airway is associated with a high risk for complications A multicenter study of 1018 children with difficult airways in 13 pediatric center more than 2 direct laryngoscopy attempts is associated with high failure rates increased incidence of severe complications. Cardiac arrest was most common severe complication (2%). Hypoxemia (SpO2<85%) was the most common complication. N. Jagannathan,British Journal of Anaesthesia 117 (S1): i3 i5 (2016)
4 Definition and Incidence
5 Definition of Difficult Airway the clinical situation in which a conventionally trained anesthesiologist experiences difficulty with facemask ventilation of the upper airway, difficulty with tracheal intubation, or both. ASA Practice Guidelines Management of the Difficult Airway 2013
 Predictors: 1. Younger age 2. ENT surgery 3.")
6 Incidence of Pediatric Difficult Airway Difficult Ventilation -484 children scheduled for elective surgery between 2007 and the ages of 0-8 years -unexpected difficult BMV was 6.6% (In adult 2.5%) Predictors: 1. Younger age 2. ENT surgery 3. Neuromuscular blockade Valois-Gomez, Peds Anesth 2013;23
 Predictors: 1. Age < 1 year 2. ASA III & IV 3. MP III & IV 4.")
7 Incidence of Pediatric Difficult Airway Difficult Laryngoscopy -From a 5-year time period ( ) -11,219 general anesthesia procedures -Neonate to adolescent -Incidence DL was 1.35% (In adult 4.4%) Predictors: 1. Age < 1 year 2. ASA III & IV 3. MP III & IV 4. Low BMI Heinrich, Peds Anesth 2012;22
8 Differences between pediatric and adult airways

9 Anatomic differences between pediatric and adult airways Large occiput Narrow nares Large tongue Larynx more cephalad Narrow cricoid Difficult ventilate and laryngoscopy
10 Diseases and Syndromes Associated with the Difficult Pediatric Airway



11 Nasopharynx Choanal atresia, stenosis, Cleft lip cleft palate Adenoidal hypertrophy Tongue Hemangioma, Down syndrome Beckwith-Wiedemann syndrome Mandible maxilla Pierre Robin syndrome, Treacher Collins syndrome, Goldenhar syndrome, Apert syndrome Neck burn with contracture, Juvenile rheumatoid arthritis Pharynx/larynx Laryngomalacia, Freeman-Sheldon syndrome Epiglottitis, peritonsillar abscess Trachea Vascular ring, tracheal stenosis, tracheomalacia, Mediastinal tumors


12 Diseases and Syndromes Associated with the Difficult Pediatric Airway Head & Nasopharynx Congenital hydrocephalus Cleft lip cleft palate


13 Diseases and Syndromes Associated with the Difficult Pediatric Airway Tongue Down syndrome Hemagioma



14 Diseases and Syndromes Associated with the Difficult Pediatric Airway Mandible & Maxilla Pierre Robin syndrome Treacher Collins syndrome



15 Diseases and Syndromes Associated with the Difficult Pediatric Airway Mandible & Maxilla Goldenhar syndrome Apert syndrome


16 Diseases and Syndromes Associated with the Difficult Pediatric Airway Mandible & Maxilla Burn with contracture Juvenile rheumatoid arthritis


17 Diseases and Syndromes Associated with the Difficult Pediatric Airway Pharynx/larynx Peritonsillar abscess Acute epiglottitis


18 Diseases and Syndromes Associated with the Difficult Pediatric Airway Trachea Tracheal stenosis Tracheomalacia
19 Respiratory physiologic differences between children and adults High oxygen consumption: 7-9 ml O2/kg/min vs 3 ml O2/kg/min in adult Reduced FRC Elevated closing volume Rapid desaturation when apnea
20 Pediatric difficult airway management different from adult Awake approaches to intubation used in adult difficult airways are more problematic for pediatric patients For pediatric patients, anesthetized intubation remains most common
21 Complication
 -tracheal tube-related events accounting")
22 Complication of difficult airway -229 critical incidents were reported from 49,373 anesthetic procedures. -between January 2008 and August The most frequently reported incidents were associated with the respiratory system (55%) -tracheal tube-related events accounting for 40.9% of respiratory incidents Ji-Hyun Lee, Peds Anesth 2016
23 Complication of difficult airway arrests (49%) were related to anesthesia. - 27% of cardiac arrest due to respiratory causes 8% due to difficult ventilation and intubation Bhananker SM, Anesth Analg 2007, Aug;105(2):344-50
 of cases -30 (3%) of these were")

24 Complication of difficult airway -Tracheal intubation failed in 19 (2%) of cases -30 (3%) of these were severe complication : cardiac arrest, death, aspiration, pneumothorax John Edem Fiadjoe, Lancet Respir Med,2016.
25 Guideline for management of the unanticipated difficult airway in pediatric practice
 346")
26 Guideline for the management of the unanticipated difficult airway in pediatric practice Pediatric Anesthesia 25 (2015)
27 Method The Working Group established a panel of 27 consultant pediatric anesthetists, the Delphi Group Delphi Group included anesthetists from 25 different hospitals in the UK and Ireland Delphi Group reviewed research into airway management in children and graded papers for the level of evidence according to agreed criteria. A Delphi panel considered the steps of the acute airway management guidelines to reach consensus on the best interventions to use them.
28 3 Guidelines for pediatric airway management Difficult mask ventilation Unanticipated difficult tracheal intubation Cannot intubate and cannot ventilate (CICV)
29
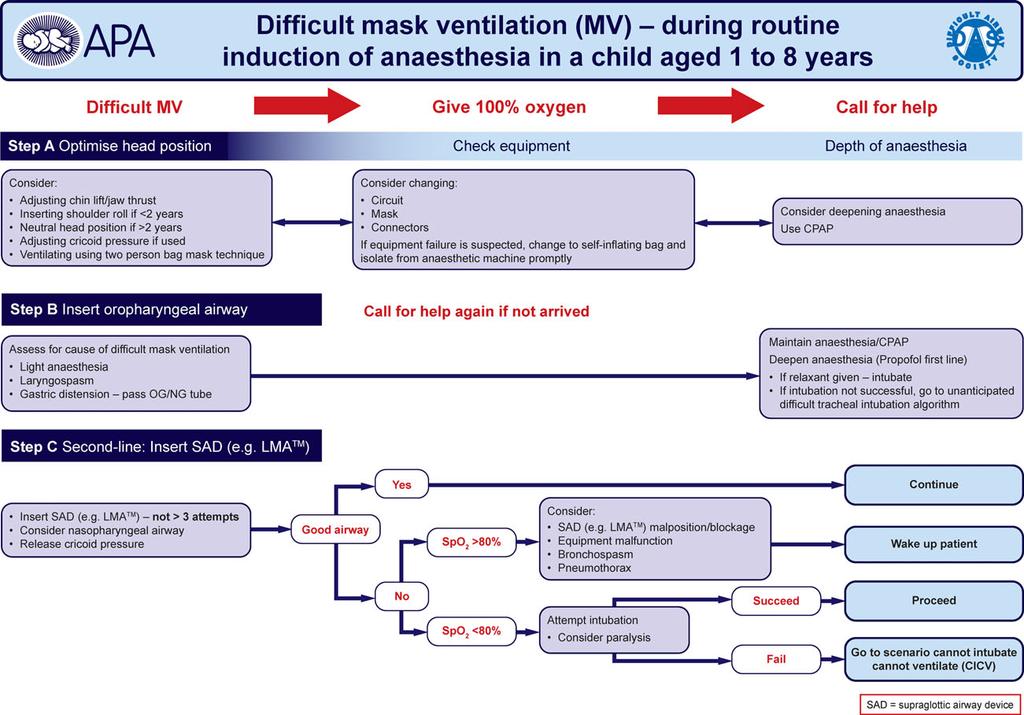
30 Difficult mask ventilation Step A : Optimizing head position Adjusting chin lift with or without jaw thrust in all aged Lateral position can improve obstructive airway Inserting shoulder roll if < 2 years Neutral head position if > 2 years Using a 2 hands technique for ventilation

31 Insert shoulder roll and chin lift

32 Neutral head position

33 Adjusting jaw thrust and ventilating using two person bag mask technique
34 Difficult mask ventilation Check equipment Check : circuit Mask connector If equipment failure is suspect, change to self inflating bag and isolate from anesthetic machine
35 Difficult mask ventilation Depth of anesthesia Propofol is a first-line drug for deepen anesthesia or increase volatile agent concentration if not has IV asscess.
36 Difficult mask ventilation Maintain anesthesia with 100% oxygen Apply CPAP Insert oropharygeal airway
37 Difficult mask ventilation Assess for cause of difficult mask ventilation - Light of anesthesia - Laryngospasm - Gastric distension Pass OG/NG If relaxant given Intubation If intubation not successful Go to Unanticipated difficult tracheal intubation
38 Difficult mask ventilation Step C Use of a supraglottic airway device Consider - SAD malposition/blockage - Equipment malfunction - Bronchospasm - Pneumothorax

39 Difficult mask ventilation Step C Use of a supraglottic airway device Attempt intubation

40 Unanticipated difficult tracheal intubation
41

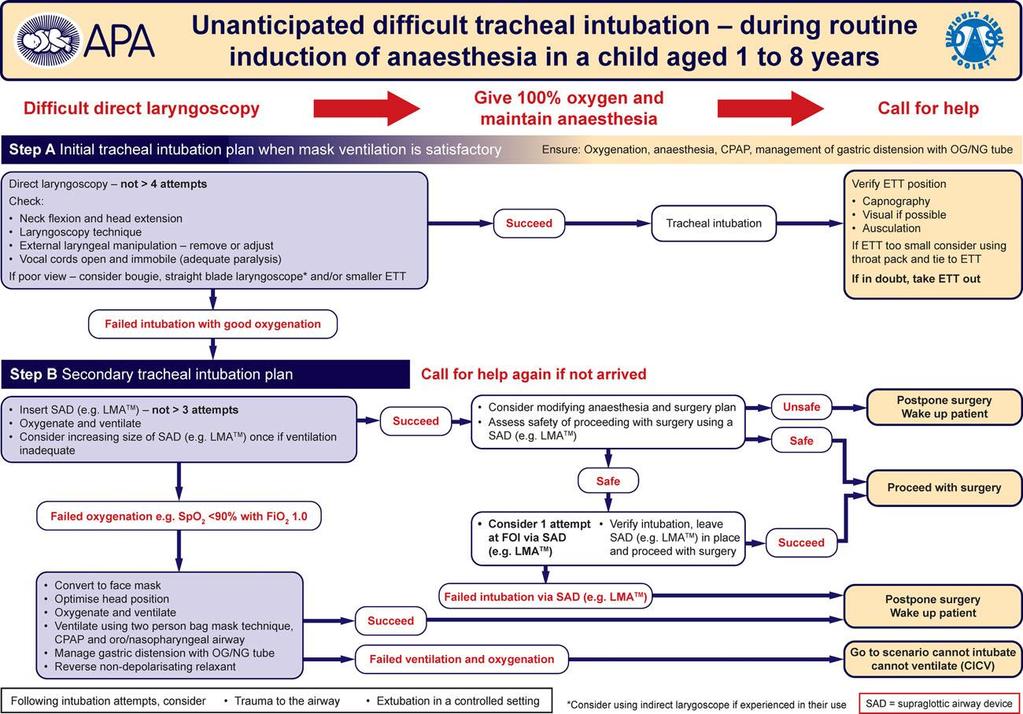
42 Unanticipated difficult tracheal intubation Step A : Initial tracheal intubation plan when mask ventilation is satisfactory
43 Unanticipated difficult tracheal intubation Step A : Initial tracheal intubation plan when mask ventilation is satisfactory After failed intubation attempt Adjustment head and neck extension With or without pillow and shoulders rolls Succeed tracheal intubation -Capnography (Gold standard) -Ausculation External laryngeal manipulation: remove or adjust Laryngoscope and adjuvants to intubation - Straight blade DL in 1-3 years, Glidescope, Airtraq Consider smaller ETT size IF ETT too small consider using throat pack Failed intubation with good oxygenation go to Step B

44 Unanticipated difficult tracheal intubation Step B : Secondary tracheal intubation plan
45 Unanticipated difficult tracheal intubation Step B : Secondary tracheal intubation plan Insert SAD (eg. LMA) with good oxygenation - Assess safety of proceeding surgery with LMA Safe Unsafe Proceed with surgery Postpone surgery and wake up patient
46 Unanticipated difficult tracheal intubation Step B : Secondary tracheal intubation plan Placement of the SAD and inadequate oxygenation ( SpO2<90, FiO2 1.0) Convert to face mask ventilation Ventilate using two person bag mask technique Manage gastric distension with OG/NG tube Reverse non-depolarizing relaxant Succeed Failed ventilation and oxygenation Postpone surgery and wake up patient Go to scenario CICV

47 Cannot intubate and cannot ventilate
48

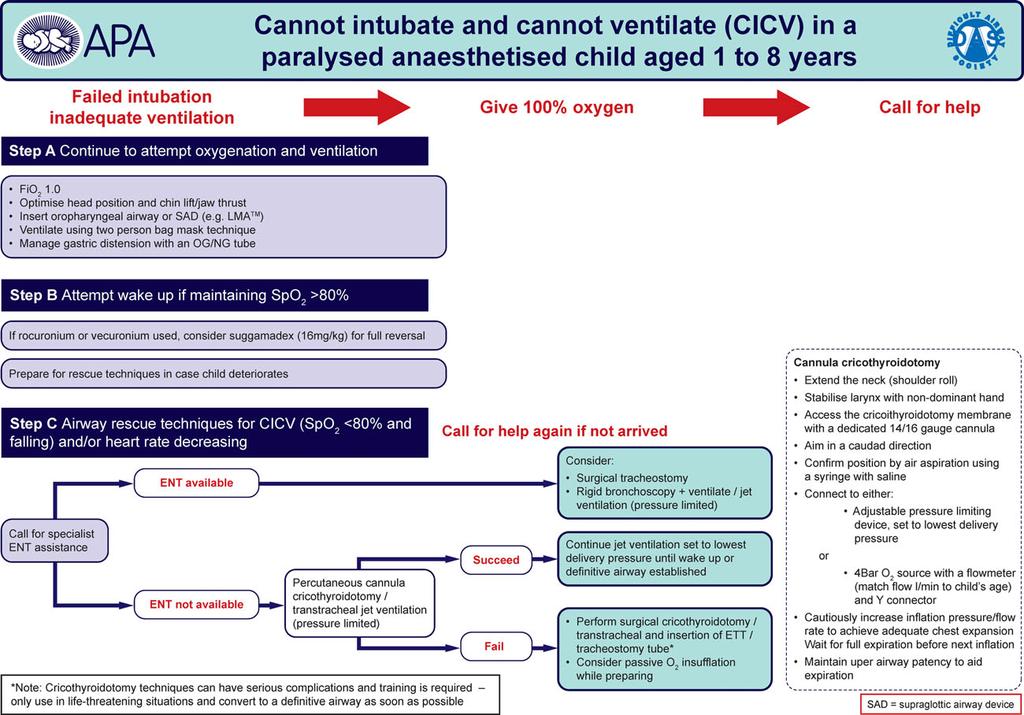
49 Cannot intubate and cannot ventilate Step A: Continue to attempt oxygenation and ventilation

50 Cannot intubate and cannot ventilate Step B: Attempt wake up if SpO2 > 80% - Continue efforts to oxygenation and ventilation. - Prepare for rescue techniques in case child deteriorate. (Desaturation, hemodynamic unstable ) - If rocuronium or vecuronium used consider suggamadex 16 mg/kg for full reversal
 and/or heart rate")
51 Cannot intubate and cannot ventilate Step C : Airway rescue techniques for CICV ( SpO2 < 80% and falling) and/or heart rate decreasing
52 Cannot intubate and cannot ventilate Step C : Airway rescue techniques for CICV ( SpO2 < 80% and falling) and/or heart rate decreasing Call for specialist ENT ENT available ENT not available Consider: Surgical tracheostomy Rigid bronchoscopy + ventilation/jet ventilation
53 Cannot intubate and cannot ventilate Step C : Airway rescue techniques for CICV ( SpO2 < 80% and falling) and/or heart rate decreasing ENT not available Percutaneous cannula cricothyroidotomy /Tracheal jet ventilation Succeed Continue jet ventilation (Lowest pressure until wake up or definite airway established Fail Surgical cricothyroidotomy or transtracheal and insertion of ETT or tracheostomy tube
54 Practice Guidelines for Management of the Difficult Airway in pediatric and adult There are awake intubation guideline for adult but not have in pediatric practice. ASA,2013
55 Case scenario

56 Large mass in oral cavity 5 years old boy with big size (6 4 cm) sublingual dermoid cyst was pushing the anterior part of the tongue and displacing the tongue superiorly and posteriorly Patient has normal mouth opening, can protrude tongue. Plan excision of sublingual dermoid cyst. What technique and equipment you consider using for intubation in this patient??
57 CASE REPORT GlideScope A rescuer in difficult pediatric airway The pharynx was anaesthetized topically using 4% viscous lidocaine and 10% Lidocaine spray. the child was awakened and spontaneous breathing with 100% oxygen. Then direct laryngoscopy was attempted and could see only the posterior commissure. And could not intubated. succeeded intubation with GlideScope >> visualising and intubating the trachea with 5.5 mm uncuffed endotracheal Nidhi Garg, An International Journal of Anesthesiology, Pain Management, Intensive Care & Resuscitation; 2014


58 GlideScope Limitation Some mouth opening is required Learning curve Difficulty passing tube despite excellent view

59 GlideScope Glidescope cobalt sizes Size (GVL) Age Weight(kg) 0 Preterm <1.5 1 Full term Toddler Child Adult 11-adult
60 Case report: Airway management in Pierre Robin Syndrome A 2 years old girl Plan for repair of cleft palate She was a known case of Pierre Robin Syndrome had short receding jaw mouth opening limited to 1.5 cm, tongue was large and retracted posteriorly. The breathing was noisy due to obstruction of the airways by large tongue and her resting SpO 2 was 90% on room air. What technique and equipment you consider using for intubation in this patient??

61 Case report Successful intubation with intubating LMA in Pierre Robin syndrome Inhalation induction with spontaneous ventilation. McIntosh blade No. 1 was inserted but failed An attempt with Miller blade also failed. Then LMA No. 1.5 was inserted and easy ventilated After ventilation for five minutes, ETT No. 3.5 was inserted through the intubating LMA the intubating LMA was pulled out. Manual ventilation was resumed through the ETT Tariq Hayat Khan, An International Journal of Anesthesiology, Pain Management, Intensive Care & Resuscitation; 2013
62 Intubating LMA Several methods for placing the ETT through the LMA Blind Fiberoptic assisted Stylet or bougie assisted Ventilation can be provided during intubation attempts

63 Intubating LMA Limitation Smaller LMA may not allow passage of pilot balloon of cuffed tubes. LMA removal over the ETT may cause simultaneous withdrawal of the ETT.

64 Case report: Hunter syndrome with difficult airway A 5 years old boy Plan for dental examination under GA requiring nasal intubation He was a known case of Hunter syndrome Coarse facial features, macrocephaly, macroglossia Limited mouth opening Limited range of motion of the neck had a history of asthma, bicuspid aortic valve What technique and equipment you consider using for intubation in this patient??

65 Case report Successful intubation with fiberoptic in Hunter syndrome Inhalation induction with spontaneous ventilation. Easy mask ventilation was confirmed. Rocuronium was administered. Laryngoscopy with Glidescope blade size 3 and showed a very anterior larynx with enlarged epiglottis. At this point decision was made to proceed with nasal fiberoptic intubation. Flexible bronchoscope was passed and vocal cords were visualized, ETT Size 4.5 was passed over bronchoscope. Palatnik md Y,pedsanesthesia;2012

66 Fiberoptic Bronchoscope gold standard for the management of the difficult airway can use with variety of abnormal airway It is well tolerated by the awake, sedate and spontaneously breathing child
67 Fiberoptic Bronchoscope Limitations: Optical problems with fogging, blood or secretions Requires extensive experience Fragile and Expensive
68 Pediatric airway equipment in Siriraj hospital


69 C-MAC Miller 1 Macintosh 2

70 Glidescope <1.5 kg kg kg kg >10kg-adult
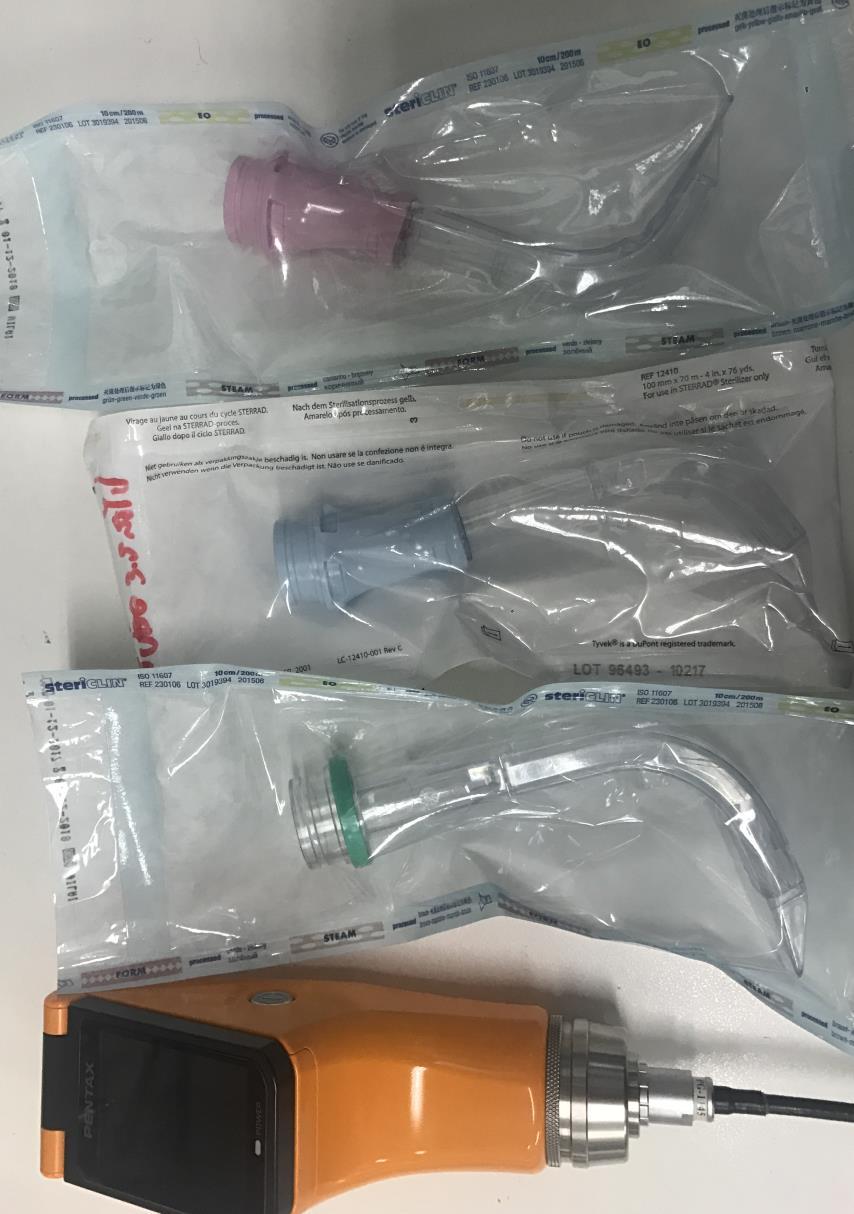
71 Pentax

72 Bonfils 2 3.5

73 LMA < 5 kg 5-10 kg kg kg kg

74 LMA i-gel
75 Fiberoptic Bronchoscope

76
77
Advanced Airway Management. University of Colorado Medical School Rural Track
 Advanced Airway Management University of Colorado Medical School Rural Track Advanced Airway Management Basic Airway Management Airway Suctioning Oxygen Delivery Methods Laryngeal Mask Airway ET Intubation
Advanced Airway Management University of Colorado Medical School Rural Track Advanced Airway Management Basic Airway Management Airway Suctioning Oxygen Delivery Methods Laryngeal Mask Airway ET Intubation
Other methods for maintaining the airway (not definitive airway as still unprotected):
:") Page 56 Where anaesthetic skills and drugs are available, endotracheal intubation is the preferred method of securing a definitive airway. This technique comprises: rapid sequence induction of anaesthesia
Page 56 Where anaesthetic skills and drugs are available, endotracheal intubation is the preferred method of securing a definitive airway. This technique comprises: rapid sequence induction of anaesthesia
DIFFICULT AIRWAY MANAGMENT. Dr.N.SANTHOSH KUMAR MD ANESTHESIA (2 nd Yr)
") DIFFICULT AIRWAY MANAGMENT Dr.N.SANTHOSH KUMAR MD ANESTHESIA (2 nd Yr) AIRWAY MANAGEMENT AND MAINTAINING OXYGENATION ARE THE FUNDAMENTAL RESPONSIBILITIES OF ANY BASIC DOCTOR. TO MANAGE A DIFFICULT AIRWAY,
DIFFICULT AIRWAY MANAGMENT Dr.N.SANTHOSH KUMAR MD ANESTHESIA (2 nd Yr) AIRWAY MANAGEMENT AND MAINTAINING OXYGENATION ARE THE FUNDAMENTAL RESPONSIBILITIES OF ANY BASIC DOCTOR. TO MANAGE A DIFFICULT AIRWAY,
Diagnosis & Management of the Difficult Airway
 Diagnosis & Management of the Difficult Airway Dr. E. Rawlings Plymouth Anaesthetic Department Complications of Airway Management Medicolegal Serious morbidity Mortality Complications of Airway Management
Diagnosis & Management of the Difficult Airway Dr. E. Rawlings Plymouth Anaesthetic Department Complications of Airway Management Medicolegal Serious morbidity Mortality Complications of Airway Management
THE DIFFICULT PEDIATRIC AIRWAY. Learning Objectives. The Pediatric Airway 6/7/18. Jason W. Gatling, MD Department of Anesthesiology June 7, 2018
 THE DIFFICULT PEDIATRIC AIRWAY Jason W. Gatling, MD Department of Anesthesiology June 7, 2018 Learning Objectives At the conclusion of this activity, the participants should be able to: 1. Describe what
THE DIFFICULT PEDIATRIC AIRWAY Jason W. Gatling, MD Department of Anesthesiology June 7, 2018 Learning Objectives At the conclusion of this activity, the participants should be able to: 1. Describe what
Anatomy and Physiology. The airways can be divided in to parts namely: The upper airway. The lower airway.
 Airway management Anatomy and Physiology The airways can be divided in to parts namely: The upper airway. The lower airway. Non-instrumental airway management Head Tilt and Chin Lift Jaw Thrust Advanced
Airway management Anatomy and Physiology The airways can be divided in to parts namely: The upper airway. The lower airway. Non-instrumental airway management Head Tilt and Chin Lift Jaw Thrust Advanced
(ix) Difficult & Failed Intubation Queen Charlotte s Hospital
 Difficult & Failed Intubation Queen Charlotte s Hospital") (ix) Difficult & Failed Intubation Queen Charlotte s Hospital Pre-operative Assessment Clinical assessment of airway and risk of difficult intubation: (can be performed in a matter of seconds): 1. Mouth
(ix) Difficult & Failed Intubation Queen Charlotte s Hospital Pre-operative Assessment Clinical assessment of airway and risk of difficult intubation: (can be performed in a matter of seconds): 1. Mouth
Angkana Lurngnateetape,, MD. Department of Anesthesiology Siriraj Hospital
 AIRWAY MANAGEMENT Angkana Lurngnateetape,, MD. Department of Anesthesiology Siriraj Hospital Perhaps the most important responsibility of the anesthesiologist is management of the patient s airway Miller
AIRWAY MANAGEMENT Angkana Lurngnateetape,, MD. Department of Anesthesiology Siriraj Hospital Perhaps the most important responsibility of the anesthesiologist is management of the patient s airway Miller
Dr.Bharghavi.M 2 nd year post graduate Dept of Anaesthesia
 DIFFICULT AIRWAY CANNOT VENTILATE, CANNOT INTUBATE. Dr.Bharghavi.M 2 nd year post graduate Dept of Anaesthesia Difficult airway According to AMERICAN SOCIETY OF ANAESTHESIOLOGISTS Difficult Airway is defined
DIFFICULT AIRWAY CANNOT VENTILATE, CANNOT INTUBATE. Dr.Bharghavi.M 2 nd year post graduate Dept of Anaesthesia Difficult airway According to AMERICAN SOCIETY OF ANAESTHESIOLOGISTS Difficult Airway is defined
Airway Management. Teeradej Kuptanon, MD
 Airway Management Teeradej Kuptanon, MD Outline Anatomy Detect difficult airway Rapid sequence intubation Difficult ventilation Difficult intubation Surgical airway access ICU setting Intubation Difficult
Airway Management Teeradej Kuptanon, MD Outline Anatomy Detect difficult airway Rapid sequence intubation Difficult ventilation Difficult intubation Surgical airway access ICU setting Intubation Difficult
Airway/Breathing. Chapter 5
 Airway/Breathing Chapter 5 Airway/Breathing Introduction Skillful, rapid assessment and management of airway and ventilation are critical to preventing morbidity and mortality. Airway compromise can occur
Airway/Breathing Chapter 5 Airway/Breathing Introduction Skillful, rapid assessment and management of airway and ventilation are critical to preventing morbidity and mortality. Airway compromise can occur
All I need is an LMA
 All I need is an LMA Narasimhan Sim Jagannathan, M.D. Associate Chairman, Academic Affairs Director, Pediatric Anesthesia Research Ann & Robert H. Lurie Children s Hospital of Chicago Associate Professor
All I need is an LMA Narasimhan Sim Jagannathan, M.D. Associate Chairman, Academic Affairs Director, Pediatric Anesthesia Research Ann & Robert H. Lurie Children s Hospital of Chicago Associate Professor
Airway management problem during anaesthesia. Airway management problem in ICU / HDU. Airway management problem occurring in the Emergency Department
 4th National Audit Project of the Royal College of Anaesthetists: Major Complications of Airway Management in the UK Please select one form from the list below Airway management problem during anaesthesia
4th National Audit Project of the Royal College of Anaesthetists: Major Complications of Airway Management in the UK Please select one form from the list below Airway management problem during anaesthesia
Airway/Breathing. Chapter 5
 Airway/Breathing Chapter 5 Airway/Breathing Introduction Rapid assessment and management of airway and ventilation are critical to preventing morbidity and mortality. Airway compromise can occur rapidly
Airway/Breathing Chapter 5 Airway/Breathing Introduction Rapid assessment and management of airway and ventilation are critical to preventing morbidity and mortality. Airway compromise can occur rapidly
Airway Anatomy. Soft palate. Hard palate. Nasopharynx. Tongue. Oropharynx. Hypopharynx. Thyroid cartilage
 Airway Anatomy Hard palate Soft palate Tongue Nasopharynx Oropharynx Hypopharynx Thyroid cartilage Airway Anatomy Hyoid bone Thyroid cartilage Cricoid cartilage Trachea Cricothyroid membrane Airway Anatomy
Airway Anatomy Hard palate Soft palate Tongue Nasopharynx Oropharynx Hypopharynx Thyroid cartilage Airway Anatomy Hyoid bone Thyroid cartilage Cricoid cartilage Trachea Cricothyroid membrane Airway Anatomy
Airway/Breathing. Chapter 5
 Airway/Breathing Chapter 5 Airway/Breathing Introduction Skillful, rapid, assessment and management of airway and ventilation are critical to preventing morbidity and mortality. Airway compromise can occur
Airway/Breathing Chapter 5 Airway/Breathing Introduction Skillful, rapid, assessment and management of airway and ventilation are critical to preventing morbidity and mortality. Airway compromise can occur
Joint Theater Trauma System Clinical Practice Guideline
 Page 1 of 7 Joint Theater Trauma System Clinical Practice Guideline TRAUMA AIRWAY MANAGEMENT Original Release/Approval 18 Dec 2004 Note: This CPG requires an annual review. Reviewed: May 2012 Approved:
Page 1 of 7 Joint Theater Trauma System Clinical Practice Guideline TRAUMA AIRWAY MANAGEMENT Original Release/Approval 18 Dec 2004 Note: This CPG requires an annual review. Reviewed: May 2012 Approved:
Airway management problem occurring in the Emergency Department
 NAP4EM Airway management problem occurring in the Emergency Department Inclusion criteria 1. Please indicate the inclusion criteria by selecting one or more from the list below: Death Brain damage Emergency
NAP4EM Airway management problem occurring in the Emergency Department Inclusion criteria 1. Please indicate the inclusion criteria by selecting one or more from the list below: Death Brain damage Emergency
Cricoid pressure: useful or dangerous?
 Cricoid pressure: useful or dangerous? Francis VEYCKEMANS Cliniques Universitaires Saint Luc Bruxelles (2009) Controversial issue - Can J Anaesth 1997 JR Brimacombe - Pediatr Anesth 2002 JG Brock-Utne
Cricoid pressure: useful or dangerous? Francis VEYCKEMANS Cliniques Universitaires Saint Luc Bruxelles (2009) Controversial issue - Can J Anaesth 1997 JR Brimacombe - Pediatr Anesth 2002 JG Brock-Utne
General Medical Procedure. Emergency Airway Techniques (General Airway Protocol)
") General Medical Procedure Appropriate airway management is often the most important intervention a prehospital care provider makes, as ensuring adequate oxygenation and ventilation is crucial to the survival
General Medical Procedure Appropriate airway management is often the most important intervention a prehospital care provider makes, as ensuring adequate oxygenation and ventilation is crucial to the survival
Pre anaesthetic evaluation of difficult tracheal intubation
 Pre anaesthetic evaluation of difficult tracheal intubation Dr. AL. Meenakshi Sundaram M.D., D.A., GC Member,ISA National Professor of Anesthesiology Thanjavur Medical College Thanjavur, TamilNadu Phone:
Pre anaesthetic evaluation of difficult tracheal intubation Dr. AL. Meenakshi Sundaram M.D., D.A., GC Member,ISA National Professor of Anesthesiology Thanjavur Medical College Thanjavur, TamilNadu Phone:
Preface... Acknowledgements... Contributors... 1 The Difficult Airway: Definitions and Algorithms The Expected Difficult Airway...
 Contents Preface... Acknowledgements... Contributors... vii ix xvii 1 The Difficult Airway: Definitions and Algorithms... 1 Zdravka Zafirova and Avery Tung Introduction 1 Definitions 2 Incidence 3 Algorithms
Contents Preface... Acknowledgements... Contributors... vii ix xvii 1 The Difficult Airway: Definitions and Algorithms... 1 Zdravka Zafirova and Avery Tung Introduction 1 Definitions 2 Incidence 3 Algorithms
Emergency Airway Management. Richard P. Dutton, M.D., M.B.A. Chief Quality Officer US Anesthesia Partners
 Emergency Airway Management Richard P. Dutton, M.D., M.B.A. Chief Quality Officer US Anesthesia Partners Disclosures I have studied a lot of airway gizmos over the years. I have no financial interest in
Emergency Airway Management Richard P. Dutton, M.D., M.B.A. Chief Quality Officer US Anesthesia Partners Disclosures I have studied a lot of airway gizmos over the years. I have no financial interest in
Airway Workshop Lecture. University of Ottawa
 Airway Workshop Lecture Department of Anesthesiology University of Ottawa Overview Ventilation Airway assessment Difficult airways Airway management equipment aids Intubation/Improving Intubation Success
Airway Workshop Lecture Department of Anesthesiology University of Ottawa Overview Ventilation Airway assessment Difficult airways Airway management equipment aids Intubation/Improving Intubation Success
Question: Is this patient an infant? A patient less than 12 months old is considered an infant. Please check the box next to the appropriate choice.
 Question: Date of Intubation (Month, Day, Year): Question: Date of Data Entry This should be within 4 weeks to the day of intubation: Question: Is this patient an infant? A patient less than 12 months
Question: Date of Intubation (Month, Day, Year): Question: Date of Data Entry This should be within 4 weeks to the day of intubation: Question: Is this patient an infant? A patient less than 12 months
Pediatric upper airway and congenital anomalies
 Anesthesiology Clin N Am 20 (2002) 747 766 Pediatric upper airway and congenital anomalies Andrew Infosino, MD Department of Anesthesia and Perioperative Care, University of California at San Francisco,
Anesthesiology Clin N Am 20 (2002) 747 766 Pediatric upper airway and congenital anomalies Andrew Infosino, MD Department of Anesthesia and Perioperative Care, University of California at San Francisco,
AIRWAY MANAGEMENT AND VENTILATION
 AIRWAY MANAGEMENT AND VENTILATION D1 AIRWAY MANAGEMENT AND VENTILATION Basic airway management and ventilation The laryngeal mask airway and Combitube Advanced techniques of airway management D2 Basic
AIRWAY MANAGEMENT AND VENTILATION D1 AIRWAY MANAGEMENT AND VENTILATION Basic airway management and ventilation The laryngeal mask airway and Combitube Advanced techniques of airway management D2 Basic
Educational Session: Evaluation and Management of the Difficult Airway
 Educational Session: Evaluation and Management of the Difficult Airway Diane M. Birnbaumer, MD, FACEP 3/24/2010 7:30 AM - 8:30 AM The Difficult Airway What s Up YOUR Sleeve? Diane M. Birnbaumer, M.D.,
Educational Session: Evaluation and Management of the Difficult Airway Diane M. Birnbaumer, MD, FACEP 3/24/2010 7:30 AM - 8:30 AM The Difficult Airway What s Up YOUR Sleeve? Diane M. Birnbaumer, M.D.,
LEVITAN S FIBREOPTIC STYLET: BEYOND BARRIERS. - Our Perspective.
 ISSN: 2250-0359 Volume 3 Issue 4 2013 LEVITAN S FIBREOPTIC STYLET: BEYOND BARRIERS - Our Perspective. Justin Ebenezer Sargunaraj * Dr.Balasubramaniam Thiagarajan * *Stanley Medical College ABSTRACT: This
ISSN: 2250-0359 Volume 3 Issue 4 2013 LEVITAN S FIBREOPTIC STYLET: BEYOND BARRIERS - Our Perspective. Justin Ebenezer Sargunaraj * Dr.Balasubramaniam Thiagarajan * *Stanley Medical College ABSTRACT: This
Airway Management & Safety Concerns Experience from Bariatric Surgery
 Airway Management & Safety Concerns Experience from Bariatric Surgery Issues of the Obese Critical Care Patient - Airway Srikantha Rao MBBS MS Associate Professor Department of Anesthesia Aug 2010 Objectives
Airway Management & Safety Concerns Experience from Bariatric Surgery Issues of the Obese Critical Care Patient - Airway Srikantha Rao MBBS MS Associate Professor Department of Anesthesia Aug 2010 Objectives
This interdisciplinary clinical support document provides guidelines for the safe establishment of an artificial airway.
 PURPOSE This interdisciplinary clinical support document provides guidelines for the safe establishment of an artificial airway. POLICY STATEMENTS Endotracheal intubation will be performed by the Most
PURPOSE This interdisciplinary clinical support document provides guidelines for the safe establishment of an artificial airway. POLICY STATEMENTS Endotracheal intubation will be performed by the Most
Fiberoptic bronchoscope and C-MAC video laryngoscope assisted nasal-oral tube exchange: two case reports
 Case Report pissn 2383-9309 eissn 2383-9317 J Dent Anesth Pain Med 2017;17(3):219-223 https://doi.org/10.17245/jdapm.2017.17.3.219 Fiberoptic bronchoscope and C-MAC video laryngoscope assisted nasal-oral
Case Report pissn 2383-9309 eissn 2383-9317 J Dent Anesth Pain Med 2017;17(3):219-223 https://doi.org/10.17245/jdapm.2017.17.3.219 Fiberoptic bronchoscope and C-MAC video laryngoscope assisted nasal-oral
Emergency Department/Trauma Adult Airway Management Protocol
 Emergency Department/Trauma Adult Airway Management Protocol Purpose: A standardized protocol for management of the airway in the setting of trauma in an academic center, with the goal of maximizing successful
Emergency Department/Trauma Adult Airway Management Protocol Purpose: A standardized protocol for management of the airway in the setting of trauma in an academic center, with the goal of maximizing successful
Recent Advances in Airway Management HA Convention 2014
 Recent Advances in Airway Management HA Convention 2014 Dr. HK Cheng Chief of Service (Dept. of Anaesthesia & OT) Service Director (Ambulatory Surgery Centre) Tseung Kwan O Hospital Recent Advances in
Recent Advances in Airway Management HA Convention 2014 Dr. HK Cheng Chief of Service (Dept. of Anaesthesia & OT) Service Director (Ambulatory Surgery Centre) Tseung Kwan O Hospital Recent Advances in
Unanticipated difficult tracheal intubation - during routine induction of anaesthesia in an adult patient
 Unanticipated difficult tracheal intubation - during routine induction of anaesthesia in an adult patient Direct laryngoscopy Any problems Call for help Plan A: Initial tracheal intubation plan Direct
Unanticipated difficult tracheal intubation - during routine induction of anaesthesia in an adult patient Direct laryngoscopy Any problems Call for help Plan A: Initial tracheal intubation plan Direct
General OR Rotations GOALS & OBJECTIVES
 General OR Rotations GOALS & OBJECTIVES Goals At the end of the CA 1 year General OR rotations, the resident should competently manage uncomplicated ambulatory, orthopedic, maxillo-facial, ENT, gynecologic,
General OR Rotations GOALS & OBJECTIVES Goals At the end of the CA 1 year General OR rotations, the resident should competently manage uncomplicated ambulatory, orthopedic, maxillo-facial, ENT, gynecologic,
ISPUB.COM. The Video-Intubating Laryngoscope. M Weiss THE LARYNGOSCOPE INTRODUCTION TECHNICAL DESCRIPTION
 ISPUB.COM The Internet Journal of Anesthesiology Volume 3 Number 1 M Weiss Citation M Weiss.. The Internet Journal of Anesthesiology. 1998 Volume 3 Number 1. Abstract A Macintosh intubating laryngoscope
ISPUB.COM The Internet Journal of Anesthesiology Volume 3 Number 1 M Weiss Citation M Weiss.. The Internet Journal of Anesthesiology. 1998 Volume 3 Number 1. Abstract A Macintosh intubating laryngoscope
Airway Management. Key points. Rapid Sequence Intubation. Rapid Sequence Intubation Recognizing difficult airway Managing difficult airway
 Airway Management Prasha Ramanujam and Guy Shochat Department of Emergency Medicine UCSF Medical Center Key points Rapid Sequence Intubation Recognizing difficult airway Managing difficult airway Rapid
Airway Management Prasha Ramanujam and Guy Shochat Department of Emergency Medicine UCSF Medical Center Key points Rapid Sequence Intubation Recognizing difficult airway Managing difficult airway Rapid
If you suspect airway problems, get a second opinion before you anaesthetise, not after!
 Assessing the airway It is more important to be aware of the various methods of dealing with difficult laryngoscopy than to expect to be able to accurately identify the rare difficult patients without
Assessing the airway It is more important to be aware of the various methods of dealing with difficult laryngoscopy than to expect to be able to accurately identify the rare difficult patients without
Difficult Airway. Victor M. Gomez, M.D. Pulmonary Critical Care Medicine Medical City Dallas Hospital
 Difficult Airway Victor M. Gomez, M.D. Pulmonary Critical Care Medicine Medical City Dallas Hospital Difficult Airway Definition Predicting a difficult airway Preparing for a difficult airway Extubation
Difficult Airway Victor M. Gomez, M.D. Pulmonary Critical Care Medicine Medical City Dallas Hospital Difficult Airway Definition Predicting a difficult airway Preparing for a difficult airway Extubation
Procedure No: Procedure Approved for Use By: WCCSS Divisional Quality Meeting. Date: May 2017
 Standard Operating Procedure (SOP): Standard operating procedure for Neonatal Difficult Airway Kit and Intubation Pathway Procedure No: 1 Document replaced: Version 1 Version: 2.0 Procedure Written By:
Standard Operating Procedure (SOP): Standard operating procedure for Neonatal Difficult Airway Kit and Intubation Pathway Procedure No: 1 Document replaced: Version 1 Version: 2.0 Procedure Written By:
Orotracheal Intubation
 T h e n e w e ng l a nd j o u r na l o f m e dic i n e videos in clinical medicine Orotracheal Intubation Christopher Kabrhel, M.D., Todd W. Thomsen, M.D., Gary S. Setnik, M.D., and Ron M. Walls, M.D.
T h e n e w e ng l a nd j o u r na l o f m e dic i n e videos in clinical medicine Orotracheal Intubation Christopher Kabrhel, M.D., Todd W. Thomsen, M.D., Gary S. Setnik, M.D., and Ron M. Walls, M.D.
The LMA CTrach TM, a new laryngeal mask airway for endotracheal intubation under vision: evaluation in 100 patients
 British Journal of Anaesthesia 96 (3): 396 400 (2006) doi:10.1093/bja/ael001 Advance Access publication January 16, 2006 The LMA CTrach TM, a new laryngeal mask airway for endotracheal intubation under
British Journal of Anaesthesia 96 (3): 396 400 (2006) doi:10.1093/bja/ael001 Advance Access publication January 16, 2006 The LMA CTrach TM, a new laryngeal mask airway for endotracheal intubation under
Equipment: NRP algorithm, MRSOPA table, medication chart, SpO 2 table Warm
 NRP Skills Stations Performance Skills Station OR Integrated Skills Station STATION: Assisting with and insertion of endotracheal tube (ETT) Equipment: NRP algorithm, MRSOPA table, medication chart, SpO
NRP Skills Stations Performance Skills Station OR Integrated Skills Station STATION: Assisting with and insertion of endotracheal tube (ETT) Equipment: NRP algorithm, MRSOPA table, medication chart, SpO
Difficult Airway. Department of Anesthesiology University of Colorado Health Sciences Center (prepared by Brenda A. Bucklin, M.D.)
") Difficult Airway Department of Anesthesiology University of Colorado Health Sciences Center (prepared by Brenda A. Bucklin, M.D.) Objectives Definition & incidence of the difficult airway Evaluation of
Difficult Airway Department of Anesthesiology University of Colorado Health Sciences Center (prepared by Brenda A. Bucklin, M.D.) Objectives Definition & incidence of the difficult airway Evaluation of
Respiratory Anesthetic Emergencies in Oral and Maxillofacial Surgery. By: Lillian Han
 Respiratory Anesthetic Emergencies in Oral and Maxillofacial Surgery By: Lillian Han Background: Respiratory anesthetic emergencies are the most common complications during the administration of anesthesia
Respiratory Anesthetic Emergencies in Oral and Maxillofacial Surgery By: Lillian Han Background: Respiratory anesthetic emergencies are the most common complications during the administration of anesthesia
Comparison of the Berman Intubating Airway and the Williams Airway Intubator for fibreoptic orotracheal intubation in anaesthetised patients.
 Title Comparison of the Berman Intubating Airway and the Williams Airway Intubator for fibreoptic orotracheal intubation in anaesthetised patients Author(s) Greenland, KB; Ha, ID; Irwin, MG Citation Anaesthesia,
Title Comparison of the Berman Intubating Airway and the Williams Airway Intubator for fibreoptic orotracheal intubation in anaesthetised patients Author(s) Greenland, KB; Ha, ID; Irwin, MG Citation Anaesthesia,
ADVANCED AIRWAY MANAGEMENT
 The Advanced Airway Management protocol should be used on all patients requiring advanced airway management procedures. This protocol is divided into three sections the Crash Airway Algorithm, the Rapid
The Advanced Airway Management protocol should be used on all patients requiring advanced airway management procedures. This protocol is divided into three sections the Crash Airway Algorithm, the Rapid
Basic Airway Management
 Basic Airway Management Dr. Madhurita Singh, Assoc. Professor, Dept. of Critical Care, CMC Vellore. This is the first module in a series on management of airway and ventilation in critically ill patients.
Basic Airway Management Dr. Madhurita Singh, Assoc. Professor, Dept. of Critical Care, CMC Vellore. This is the first module in a series on management of airway and ventilation in critically ill patients.
student handbook BARS handbook September 2012.indd Front Cover 27/11/12 12:08 PM
 student handbook BARS handbook September 2012.indd Front Cover 27/11/12 12:08 PM All materials regarding the Basic Airway Resuscitation Strategy Course were written and developed by Dr. Richard Morris
student handbook BARS handbook September 2012.indd Front Cover 27/11/12 12:08 PM All materials regarding the Basic Airway Resuscitation Strategy Course were written and developed by Dr. Richard Morris
Intubation techniques
 Operative Techniques in Otolaryngology (2005) 16, 166-170 FEATURE ARTICLES Intubation techniques Geoffrey Lane, MB, BChir, FRCA From the Department of Anesthesiology, The University of Colorado Health
Operative Techniques in Otolaryngology (2005) 16, 166-170 FEATURE ARTICLES Intubation techniques Geoffrey Lane, MB, BChir, FRCA From the Department of Anesthesiology, The University of Colorado Health
AIRWAY MANAGEMENT SUZANNE BROWN, CRNA
 AIRWAY MANAGEMENT SUZANNE BROWN, CRNA OBJECTIVE OF LECTURE Non Anesthesia Sedation Providers Review for CRNA s Informal Questions encouraged 2 AIRWAY MANAGEMENT AWARENESS BASICS OF ANATOMY EQUIPMENT 3
AIRWAY MANAGEMENT SUZANNE BROWN, CRNA OBJECTIVE OF LECTURE Non Anesthesia Sedation Providers Review for CRNA s Informal Questions encouraged 2 AIRWAY MANAGEMENT AWARENESS BASICS OF ANATOMY EQUIPMENT 3
ENDOTRACHEAL INTUBATION POLICY
 POLICY Indications: Ineffective ventilation with mask and t-piece, or mask and bag technique Inability to maintain a patent airway Need or anticipation of need for prolonged ventilation Need for endotracheal
POLICY Indications: Ineffective ventilation with mask and t-piece, or mask and bag technique Inability to maintain a patent airway Need or anticipation of need for prolonged ventilation Need for endotracheal
All bedside percutaneously placed tracheostomies
 Page 1 of 5 Scope: All bedside percutaneously placed tracheostomies Population: All ICU personnel Outcomes: To standardize and outline the steps necessary to safely perform a percutaneous tracheostomy
Page 1 of 5 Scope: All bedside percutaneously placed tracheostomies Population: All ICU personnel Outcomes: To standardize and outline the steps necessary to safely perform a percutaneous tracheostomy
Airway Management and The Difficult Airway
 Airway Management and The Difficult Airway Gary McCalla, MD, FACEP Medical Director REACH Air Medical Services Services 1 It is not enough to do your best, unless you have prepared to be the best. -John
Airway Management and The Difficult Airway Gary McCalla, MD, FACEP Medical Director REACH Air Medical Services Services 1 It is not enough to do your best, unless you have prepared to be the best. -John
GENERAL ANAESTHESIA AND FAILED INTUBATION
 GENERAL ANAESTHESIA AND FAILED INTUBATION INTRODUCTION The majority of caesarean sections in the UK are performed under regional anaesthesia. However, there are situations where general anaesthesia (GA)
GENERAL ANAESTHESIA AND FAILED INTUBATION INTRODUCTION The majority of caesarean sections in the UK are performed under regional anaesthesia. However, there are situations where general anaesthesia (GA)
Rapid Sequence Induction
 Rapid Sequence Induction Virtual simultaneous administration, after preoxygenation, of a potent sedative agent and a rapidly acting neuromuscular blocking agent to facilitate rapid tracheal intubation
Rapid Sequence Induction Virtual simultaneous administration, after preoxygenation, of a potent sedative agent and a rapidly acting neuromuscular blocking agent to facilitate rapid tracheal intubation
Use of the Aintree Intubation Catheter with the Laryngeal Mask Airway and a Fiberoptic Bronchoscope in a Patient with an Unexpected Difficult Airway
 Case Report Use of the Aintree Intubation Catheter with the Laryngeal Mask Airway and a Fiberoptic Bronchoscope in a Patient with an Unexpected Difficult Airway Andrew Zura MD, D. John Doyle MD PhD FRCPC,
Case Report Use of the Aintree Intubation Catheter with the Laryngeal Mask Airway and a Fiberoptic Bronchoscope in a Patient with an Unexpected Difficult Airway Andrew Zura MD, D. John Doyle MD PhD FRCPC,
The reasons 13/11/ Cost 2. Availability 3. Comparison 4. Complications 5. Knowledge. Pulmonary and critical care medicine (PCCM) fellows.
 fellows.") The reasons Why shouldn t we use videolaryngoscope for routine intubation? Wariya Sukhupragarn, MD Associate Professor Department of Anesthesiology Faculty of Medicine, Chiang Mai University 1. Cost 2.
The reasons Why shouldn t we use videolaryngoscope for routine intubation? Wariya Sukhupragarn, MD Associate Professor Department of Anesthesiology Faculty of Medicine, Chiang Mai University 1. Cost 2.
REVERSE LMA INSERTION IN A NEONATE WITH KLIPPEL-FEIL SYNDROME
 REVERSE LMA INSERTION IN A NEONATE WITH KLIPPEL-FEIL SYNDROME - Case report - TARIQ AL ZAHRANI * Klippel-Feil syndrome (KFS) was first described by Maurice Klippel and Andre Feil in 1912 in a patient with
REVERSE LMA INSERTION IN A NEONATE WITH KLIPPEL-FEIL SYNDROME - Case report - TARIQ AL ZAHRANI * Klippel-Feil syndrome (KFS) was first described by Maurice Klippel and Andre Feil in 1912 in a patient with
VANDERBILT UNIVERSITY MEDICAL CENTER DIVISION OF ANESTHESIOLOGY CRITICAL CARE MEDICINE AIRWAY MANAGEMENT
 These guidelines are based upon medical literature review and expert opinion and are intended to provide recommendations for in the care of critically ill patients. Best Practice Guidelines Checklist for
These guidelines are based upon medical literature review and expert opinion and are intended to provide recommendations for in the care of critically ill patients. Best Practice Guidelines Checklist for
Case 1: Fast and noisy. The Ins and Outs of the Pediatric Airway. Airway: anatomic differences. Objectives 2/16/2014
 Case 1: Fast and noisy The Ins and Outs of the Pediatric Airway Judith Klein, MD, FACEP Assistant Professor of Emergency Medicine UCSF-SFGH Department of Emergency Medicine 8 month old BIB parents for
Case 1: Fast and noisy The Ins and Outs of the Pediatric Airway Judith Klein, MD, FACEP Assistant Professor of Emergency Medicine UCSF-SFGH Department of Emergency Medicine 8 month old BIB parents for
INTUBATION/RSI. PURPOSE: A. To facilitate secure, definitive control of the airway by endotracheal intubation in an expeditious and safe manner
 Manual: LifeLine Patient Care Protocols Section: Adult/Pediatrics Protocol #: AP1-009 Approval Date: 03/01/2018 Effective Date: 03/05/2018 Revision Due Date: 12/01/2018 INTUBATION/RSI PURPOSE: A. To facilitate
Manual: LifeLine Patient Care Protocols Section: Adult/Pediatrics Protocol #: AP1-009 Approval Date: 03/01/2018 Effective Date: 03/05/2018 Revision Due Date: 12/01/2018 INTUBATION/RSI PURPOSE: A. To facilitate
Upper Airway Obstruction
 Upper Airway Obstruction Adriaan Pentz Division of Otorhinolaryngology University of Stellenbosch and Tygerberg Hospital Stridor/Stertor Auditory manifestations of disordered respiratory function ie noisy
Upper Airway Obstruction Adriaan Pentz Division of Otorhinolaryngology University of Stellenbosch and Tygerberg Hospital Stridor/Stertor Auditory manifestations of disordered respiratory function ie noisy
Displacement of the epiglottis during intubation with the Pentax-AWS Airway Scope. Suzuki, Akihiro ; Katsumi, Norifumi ; Honda, Takashi ; Sasakawa,
 AMCoR Asahikawa Medical University Repository http://amcor.asahikawa-med.ac.jp/ Journal of Anesthesia (2010) 24(1): 124-127. Displacement of the epiglottis during intubation with the Pentax-AWS Airway
AMCoR Asahikawa Medical University Repository http://amcor.asahikawa-med.ac.jp/ Journal of Anesthesia (2010) 24(1): 124-127. Displacement of the epiglottis during intubation with the Pentax-AWS Airway
Nicolette Mosinski MPAS, PA-C
 Nicolette Mosinski MPAS, PA-C 1. Impaired respiratory effort 2. Airway obstruction Observe patient for detection Rate Pattern Depth Accessory muscle use Evidence of injury Noises Silent manifestations
Nicolette Mosinski MPAS, PA-C 1. Impaired respiratory effort 2. Airway obstruction Observe patient for detection Rate Pattern Depth Accessory muscle use Evidence of injury Noises Silent manifestations
Retrospective audit of the air-q intubating laryngeal airway as a conduit for tracheal intubation in pediatric patients with a difficult airway
 Pediatric Anesthesia ISSN 1155-5645 ORIGINAL ARTICLE Retrospective audit of the air-q intubating laryngeal airway as a conduit for tracheal intubation in pediatric patients with a difficult airway Narasimhan
Pediatric Anesthesia ISSN 1155-5645 ORIGINAL ARTICLE Retrospective audit of the air-q intubating laryngeal airway as a conduit for tracheal intubation in pediatric patients with a difficult airway Narasimhan
Anesthetic consideration in Clefts & Craniofacial surgery
 Anesthetic consideration in Clefts & Craniofacial surgery พญ.เด อนเพ ญ ห อร ตนาเร อง ภาคว ชาว ส ญญ ว ทยา คณะแพทย แพทยศาสตร มหาว ทยาล ยขอนแก น Preoperative evaluation Cleft lip & Cleft palate reconstruction
Anesthetic consideration in Clefts & Craniofacial surgery พญ.เด อนเพ ญ ห อร ตนาเร อง ภาคว ชาว ส ญญ ว ทยา คณะแพทย แพทยศาสตร มหาว ทยาล ยขอนแก น Preoperative evaluation Cleft lip & Cleft palate reconstruction
Effectiveness of Fiberoptic Intubation in Anticipated Difficult Airway
 Original Article Effectiveness of Fiberoptic Intubation in Anticipated Difficult Airway Khawaja Kamal Nasir, Faraz Mansoor From Department of Anesthesia, Pakistan Institute of Medical Sciences, Islamabad.
Original Article Effectiveness of Fiberoptic Intubation in Anticipated Difficult Airway Khawaja Kamal Nasir, Faraz Mansoor From Department of Anesthesia, Pakistan Institute of Medical Sciences, Islamabad.
The Pediatric Patient. Morgen Bernius, MD NCEMS Conference February 24, 2007
 The Pediatric Patient Morgen Bernius, MD NCEMS Conference February 24, 2007 Rule #1: Everyone Loves the Pediatric Patient Pediatrics in EMS Approximately 10% of all EMS treatment is for children younger
The Pediatric Patient Morgen Bernius, MD NCEMS Conference February 24, 2007 Rule #1: Everyone Loves the Pediatric Patient Pediatrics in EMS Approximately 10% of all EMS treatment is for children younger
CASE PRIMERS. Pediatric Anesthesia Fellowship Program. Laryngotracheal Reconstruction (LTR) Tufts Medical Center
 Tufts Medical Center") CASE PRIMERS Pediatric Anesthesia Fellowship Program Tufts Medical Center Department of Anesthesiology and Perioperative Medicine Division of Pediatric Anesthesia 800 Washington Street, Box 298 Boston,
CASE PRIMERS Pediatric Anesthesia Fellowship Program Tufts Medical Center Department of Anesthesiology and Perioperative Medicine Division of Pediatric Anesthesia 800 Washington Street, Box 298 Boston,
19RC1 Paediatric airway problems
 19RC1 Paediatric airway problems M. Weiss Department of Anaesthesia, University Children s Hospital, Zurich, Switzerland Saturday, June 6, 2009 13:00-13:45 Room: Yellow 3 In recent years, airway management
19RC1 Paediatric airway problems M. Weiss Department of Anaesthesia, University Children s Hospital, Zurich, Switzerland Saturday, June 6, 2009 13:00-13:45 Room: Yellow 3 In recent years, airway management
Nobuko Tachibana Yukitoshi Niiyama Michiaki Yamakage
 DOI 10.1007/s00540-014-1847-1 ORIGINAL ARTICLE Incidence of cannot intubate-cannot ventilate (CICV): results of a 3-year retrospective multicenter clinical study in a network of university hospitals Nobuko
DOI 10.1007/s00540-014-1847-1 ORIGINAL ARTICLE Incidence of cannot intubate-cannot ventilate (CICV): results of a 3-year retrospective multicenter clinical study in a network of university hospitals Nobuko
Advanced Airway Management PRESENTED BY: JOSIAH POIRIER RN, JOHN GRUBER FP-C
 Advanced Airway Management PRESENTED BY: JOSIAH POIRIER RN, JOHN GRUBER FP-C Advanced Airway Objectives Advanced airway management is a relatively low frequency, high risk intervention. The following education
Advanced Airway Management PRESENTED BY: JOSIAH POIRIER RN, JOHN GRUBER FP-C Advanced Airway Objectives Advanced airway management is a relatively low frequency, high risk intervention. The following education
Michigan General Procedures EMERGENCY AIRWAY. Date: November 15, 2012 Page 1 of 16
 Date: November 15, 2012 Page 1 of 16 Emergency Airway Effective airway management and ventilation are important lifesaving interventions that all EMS providers must be able to perform. The approach to
Date: November 15, 2012 Page 1 of 16 Emergency Airway Effective airway management and ventilation are important lifesaving interventions that all EMS providers must be able to perform. The approach to
Pediatric Airway- You Swallowed What?
 Pediatric Airway- You Swallowed What? Staci Kothbauer, CRNA, MS, APNP University of Wisconsin Hospital American Family Children s Hospital Madison, WI 1 Objectives * Understand basic pediatric airway anatomy
Pediatric Airway- You Swallowed What? Staci Kothbauer, CRNA, MS, APNP University of Wisconsin Hospital American Family Children s Hospital Madison, WI 1 Objectives * Understand basic pediatric airway anatomy
The Ins and Outs of the Pediatric Airway
 The Ins and Outs of the Pediatric Airway Judith Klein, MD, FACEP Assistant Professor of Emergency Medicine UCSF-SFGH Department of Emergency Medicine Case 1: Fast and noisy 8 month old BIB parents for
The Ins and Outs of the Pediatric Airway Judith Klein, MD, FACEP Assistant Professor of Emergency Medicine UCSF-SFGH Department of Emergency Medicine Case 1: Fast and noisy 8 month old BIB parents for
The Laryngeal Mask and Other Supraglottic Airways: Application to Clinical Airway Management
 The Laryngeal Mask and Other Supraglottic Airways: Application to Clinical Airway Management D. John Doyle MD PhD FRCPC Department of General Anesthesiology Cleveland Clinic Foundation 9500 Euclid Avenue
The Laryngeal Mask and Other Supraglottic Airways: Application to Clinical Airway Management D. John Doyle MD PhD FRCPC Department of General Anesthesiology Cleveland Clinic Foundation 9500 Euclid Avenue
Section 4.1 Paediatric Tracheostomy Introduction
 Bite- sized training from the GTC Section 4.1 Paediatric Tracheostomy Introduction This is one of a series of bite- sized chunks of educational material developed by the Global Tracheostomy Collaborative.
Bite- sized training from the GTC Section 4.1 Paediatric Tracheostomy Introduction This is one of a series of bite- sized chunks of educational material developed by the Global Tracheostomy Collaborative.
In 2011 I received an unrestricted lecture honorarium from Ambu I have been loaned equipment by Intavent Direct (Teleflex) and Aircraft Medical As an
 and Aircraft Medical As an") Alistair McNarry In 2011 I received an unrestricted lecture honorarium from Ambu I have been loaned equipment by Intavent Direct (Teleflex) and Aircraft Medical As an organiser of airway workshops I have
Alistair McNarry In 2011 I received an unrestricted lecture honorarium from Ambu I have been loaned equipment by Intavent Direct (Teleflex) and Aircraft Medical As an organiser of airway workshops I have
Emergency ENT Anaesthesia. Richard Semenov
 Emergency ENT Anaesthesia Richard Semenov Emergency ENT Anaesthesia Dr Richard Semenov MBBS (Adel) FRCA (UK) FANZCA Dept of Anaesthesia Royal Adelaide Hospital My Experience in Emergency ENT Anaesthesia
Emergency ENT Anaesthesia Richard Semenov Emergency ENT Anaesthesia Dr Richard Semenov MBBS (Adel) FRCA (UK) FANZCA Dept of Anaesthesia Royal Adelaide Hospital My Experience in Emergency ENT Anaesthesia
L.J. Hoeve and R.H.M. van Poppelen * (Received 12 July 1989) (Accepted 10 August 1989)
 (Accepted 10 August 1989)") International Journal of Pediatric Otorhinolaryngolo~. 18 (1990) 241-245 Elsevier 241 PEDOT 00617 Fiberoptic laryngoscopy under in neonates general anesthesia L.J. Hoeve and R.H.M. van Poppelen * Lkpar?ments
International Journal of Pediatric Otorhinolaryngolo~. 18 (1990) 241-245 Elsevier 241 PEDOT 00617 Fiberoptic laryngoscopy under in neonates general anesthesia L.J. Hoeve and R.H.M. van Poppelen * Lkpar?ments
Management of pediatric cannot intubate, cannot oxygenate
 Acute Medicine & Surgery 2017; 4: 462 466 doi: 10.1002/ams2.305 Case Report Management of pediatric cannot intubate, cannot oxygenate Yohei Okada, 1 Wataru Ishii, 1 Norio Sato, 2 Hirokazu Kotani, 3 and
Acute Medicine & Surgery 2017; 4: 462 466 doi: 10.1002/ams2.305 Case Report Management of pediatric cannot intubate, cannot oxygenate Yohei Okada, 1 Wataru Ishii, 1 Norio Sato, 2 Hirokazu Kotani, 3 and
THE DIFFICULT PAEDIATRIC AIRWAY
 THE DIFFICULT PAEDIATRIC AIRWAY INTRODUCTION A difficult airway in anaesthesia is defined as the clinical situation in which a conventionally trained anaesthetist experiences difficulties with facemask
THE DIFFICULT PAEDIATRIC AIRWAY INTRODUCTION A difficult airway in anaesthesia is defined as the clinical situation in which a conventionally trained anaesthetist experiences difficulties with facemask
How to Predict and Avoid Airway Disasters. Muhammad Umer Ihsan
 How to Predict and Avoid Airway Disasters Muhammad Umer Ihsan Four Key Aspect of Assessing a Difficult Airway Difficult Bag Mask Ventilation Difficult Direct Laryngoscopy Difficult Extra-glottic devices
How to Predict and Avoid Airway Disasters Muhammad Umer Ihsan Four Key Aspect of Assessing a Difficult Airway Difficult Bag Mask Ventilation Difficult Direct Laryngoscopy Difficult Extra-glottic devices
Haemodynamic response to orotracheal intubation: direct laryngoscopy versus fiberoptic bronchoscopy
 Haemodynamic response to orotracheal intubation: direct laryngoscopy versus fiberoptic bronchoscopy Amir Murad Khudad* Hoshyar Najeeb Karem** ABSTRACT Background and Objectives: The cardiovascular response
Haemodynamic response to orotracheal intubation: direct laryngoscopy versus fiberoptic bronchoscopy Amir Murad Khudad* Hoshyar Najeeb Karem** ABSTRACT Background and Objectives: The cardiovascular response
Airway management problem during anaesthesia. Airway management problem occurring in the Emergency Department
 4th National Audit Project of the Royal College of Anaesthetists: Major Complications of Airway Management in the UK Please select one form from the list below Airway management problem during anaesthesia
4th National Audit Project of the Royal College of Anaesthetists: Major Complications of Airway Management in the UK Please select one form from the list below Airway management problem during anaesthesia
Anesthesia Final Exam
 Anesthesia Final Exam 1) For a patient who is chronically taking the following medications, which two should be withheld on the day of surgery? a) Lasix b) Metoprolol c) Glucophage d) Theodur 2) A 51 year
Anesthesia Final Exam 1) For a patient who is chronically taking the following medications, which two should be withheld on the day of surgery? a) Lasix b) Metoprolol c) Glucophage d) Theodur 2) A 51 year
Introducing the Fastrach-LMA. Prepared by Jim Medeiros, NREMT-P Regional Field Coordinator Lord Fairfax EMS Council
 Introducing the Fastrach-LMA Prepared by Jim Medeiros, NREMT-P Regional Field Coordinator Lord Fairfax EMS Council Objectives Review Anatomy of the Upper Airway Review LFEMSC LMA Protocol Discuss Indications
Introducing the Fastrach-LMA Prepared by Jim Medeiros, NREMT-P Regional Field Coordinator Lord Fairfax EMS Council Objectives Review Anatomy of the Upper Airway Review LFEMSC LMA Protocol Discuss Indications
Disclosures. Learning Objectives. Coeditor/author. Associate Science Editor, American Heart Association
 Tracheotomy Challenges for airway specialists Elizabeth H. Sinz, MD Professor of Anesthesiology & Neurosurgery Associate Dean for Clinical Simulation Disclosures Coeditor/author Associate Science Editor,
Tracheotomy Challenges for airway specialists Elizabeth H. Sinz, MD Professor of Anesthesiology & Neurosurgery Associate Dean for Clinical Simulation Disclosures Coeditor/author Associate Science Editor,
APPROACH TO THE EMERGENCY AIRWAY. Scott B. Davidson MD, FACS Trauma Surgery Service Bronson Methodist Hospital
 APPROACH TO THE EMERGENCY AIRWAY Scott B. Davidson MD, FACS Trauma Surgery Service Bronson Methodist Hospital Objectives History Initial recognition Get your act together Surgical options Complications
APPROACH TO THE EMERGENCY AIRWAY Scott B. Davidson MD, FACS Trauma Surgery Service Bronson Methodist Hospital Objectives History Initial recognition Get your act together Surgical options Complications
Airway Management Adult
 Airway Management Adult Goals: Provide effective oxygenation and ventilation; recognize and alleviate respiratory distress or failure; provide necessary interventions quickly and safely to patients who
Airway Management Adult Goals: Provide effective oxygenation and ventilation; recognize and alleviate respiratory distress or failure; provide necessary interventions quickly and safely to patients who
Advanced Airway Management
 CHAPTER 37 Advanced Airway Management Airway Anatomy and Physiology Review Respiratory System: The Airway Respiratory System (Supine) Physiology: Factors of Adequate Breathing Functioning brainstem Open
CHAPTER 37 Advanced Airway Management Airway Anatomy and Physiology Review Respiratory System: The Airway Respiratory System (Supine) Physiology: Factors of Adequate Breathing Functioning brainstem Open
Recognizing the Difficult Airway in Pediatric Patients. Nancy L. Glass, MD, MBA,
 Recognizing the Difficult Airway in Pediatric Patients Nancy L. Glass, MD, MBA, FAAP nglass@bcm.edu @DrNancyGlass1 None Disclosures Learning Objectives At the end of this presentation, participants will
Recognizing the Difficult Airway in Pediatric Patients Nancy L. Glass, MD, MBA, FAAP nglass@bcm.edu @DrNancyGlass1 None Disclosures Learning Objectives At the end of this presentation, participants will
How do you use a bougie as an airway adjunct for endotracheal intubation?
 Ruth Bird, MBBCh -Specialist Registrar: Anaesthesia & Paediatric Trauma Fellow Daniel Nevin, MBBCh -Consultant in Anaesthesia & Pre-Hospital Care The Royal London Hospital London s Air Ambulance (HEMS)
Ruth Bird, MBBCh -Specialist Registrar: Anaesthesia & Paediatric Trauma Fellow Daniel Nevin, MBBCh -Consultant in Anaesthesia & Pre-Hospital Care The Royal London Hospital London s Air Ambulance (HEMS)
Airway Management in a Patient with Klippel-Feil Syndrome Using Extracorporeal Membrane Oxygenator
 Airway Management in a Patient with Klippel-Feil Syndrome Using Extracorporeal Membrane Oxygenator Beckerman Z*, Cohen O, Adler Z, Segal D, Mishali D and Bolotin G Department of Cardiac Surgery, Rambam
Airway Management in a Patient with Klippel-Feil Syndrome Using Extracorporeal Membrane Oxygenator Beckerman Z*, Cohen O, Adler Z, Segal D, Mishali D and Bolotin G Department of Cardiac Surgery, Rambam
Management of the Airway
 Management of the Airway Kristen Bridges, M.D. Kings County Hospital Center November 12 th 2015 Case Presentation 64F PMHx CHF EF 5-10%, NYHF III-IV, atrial fibrillation/la thrombus, CVA x2, DM, HTN Home
Management of the Airway Kristen Bridges, M.D. Kings County Hospital Center November 12 th 2015 Case Presentation 64F PMHx CHF EF 5-10%, NYHF III-IV, atrial fibrillation/la thrombus, CVA x2, DM, HTN Home
Anesthetic challenges when elective case becomes emergent
 Anesthetic challenges when elective case becomes emergent Shridevi Pandya Shah MD Asst Professor Dept of Anesthesiology Rutgers-NJMS Rutgers, The State University of New Jersey Conflicts of interest: none
Anesthetic challenges when elective case becomes emergent Shridevi Pandya Shah MD Asst Professor Dept of Anesthesiology Rutgers-NJMS Rutgers, The State University of New Jersey Conflicts of interest: none
Joint Trauma System. Airway Trauma Injury Management
 Joint Trauma System Airway Trauma Injury Management 1 Agenda Contributors Purpose Summary Key Principles of CPG Performance Improvement (PI) Monitoring References List of Appendices in CPG 2 Contributors
Joint Trauma System Airway Trauma Injury Management 1 Agenda Contributors Purpose Summary Key Principles of CPG Performance Improvement (PI) Monitoring References List of Appendices in CPG 2 Contributors
Basic Scope Care and Handling
 Basic Scope Care and Handling Basic principles behind fibre-optic instruments Light and image transfer via coherent(image transmission) and incoherent (light)bundles Fibre coating with lower refractory
Basic Scope Care and Handling Basic principles behind fibre-optic instruments Light and image transfer via coherent(image transmission) and incoherent (light)bundles Fibre coating with lower refractory