Emergency ENT Anaesthesia. Richard Semenov
|
|
|
- Annice Hodges
- 5 years ago
- Views:
Transcription
1 Emergency ENT Anaesthesia Richard Semenov
 FANZCA Dept of Anaesthesia Royal Adelaide")
2 Emergency ENT Anaesthesia Dr Richard Semenov MBBS (Adel) FRCA (UK) FANZCA Dept of Anaesthesia Royal Adelaide Hospital
3 My Experience in Emergency ENT Anaesthesia Dr Richard Semenov MBBS (Adel) FRCA (UK) FANZCA Dept of Anaesthesia Royal Adelaide Hospital

4

5

6 and we ll throw in a Free set of Steak Knives!

7
8

9

10

11

12
13
14

15 Emergency ENT Anaesthesia Dr Richard Semenov Royal National Throat Nose & Ear Hospital
16 Techniques for difficult intubation in ENT Emergencies
17 Techniques for difficult intubation in ENT Emergencies 1. Alternative laryngoscope blades 2. Awake intubation 3. Blind intubation (oral or nasal) 4. Fiberoptic intubation 5. Intubating stylet/tube changer 6. Laryngeal mask airway as an intubating conduit 7. Light wand 8. Retrograde intubation 9. Invasive airway access
18 Techniques for difficult ventilation in ENT Emergencies
19 Techniques for difficult ventilation in ENT Emergencies 1. Two-person mask ventilation 2. Oral and nasopharyngeal airways 3. Laryngeal mask airway 4. Esophageal-tracheal combitube 5. Intratracheal jet stylet 6. Rigid ventilating bronchoscope 7. Invasive airway access 8. Transtracheal jet ventilation
20 Overview Unsuspected difficult airway Acute Epiglottitis Stridor Obstructed Airway Tracheostomy Stridor in recovery Post thyroidectomy bleed Tracheostomy fire Base of tongue tumour Foreign body Bleeding Tonsil Children Neck trauma Mandibular abscess
21 Techniques for difficult intubation & ventilation in ENT Emergencies 1. Two-person mask ventilation 2. Oral and nasopharyngeal airways 3. Laryngeal mask airway 4. Esophageal-tracheal combitube 5. Intratracheal jet stylet 6. Rigid ventilating bronchoscope 7. Invasive airway access 8. Transtracheal jet ventilation 1. Alternative laryngoscope blades 2. Awake intubation 3. Blind intubation (oral or nasal) 4. Fiberoptic intubation 5. Intubating stylet/tube changer 6. Laryngeal mask airway as an intubating c 7. Light wand 8. Retrograde intubation 9. Invasive airway access 10. Videolaryngoscopy

22
23 ENT Emergencies Take a breath Go back to basics
24 RAH ENT Report 1 July June 2012
25 RAH ENT Report 1 July June 2012 Total Number of Cases 1051 Emergency Cases 153
26 RAH ENT Report 1 July June Abscess Drainage Ear Infection Grommet Examination of Postnasal space Exploration of Neck wound Extubation in theatre FESS 22
27 RAH ENT Report 1 July June FESS 22 CSF Leak 01 Sinus Infection 04 Epistaxis/ SPA Ligation 12 Epistaxis/ Diathermy Vessels 05
28 RAH ENT Report 1 July June Foreign Body removal Oesophagoscopy Foreign Body removal Bronchoscopy Emergency Intubation Post-op Bleed Tonsillectomy Panendoscopy Tracheostomy 44
29 RAH ENT Report 1 July June Tracheostomy 44 Tube change 09 Awake Trach for tumour 14 Awake Trach for trauma 01 Prolonged Intubation in ICU 14 Failed or inapprop to extubate in Theatre 06
30 No perfect solution ENT Anaesthesia

31 Emergency ENT Anaesthesia No perfect solution
32 ENT Anaesthesia No perfect solution
33 ENT Anaesthesia No perfect solution 1. Inhalational
34 ENT Anaesthesia No perfect solution 1. Inhalational 2. Awake FOB 3. 4.
35 ENT Anaesthesia No perfect solution 1. Inhalational 2. Awake FOB 3. Rapid Sequence 4.
36 ENT Anaesthesia No perfect solution 1. Inhalational 2. Awake FOB 3. Rapid Sequence 4. Trache under Local
37 ENT Anaesthesia No perfect solution 1. Inhalational 2. Awake FOB 3. Rapid Sequence 4. Trache under Local Child
38 ENT Anaesthesia No perfect solution 1. Inhalational Child Rapid Sequence 4.

39 ENT Anaesthesia No perfect solution 1. Inhalational Rapid Sequence 4.
40 ENT Anaesthesia No perfect solution 1. Inhalational 2. Awake FOB 3. Rapid Sequence 4. Trache under Local
41 ENT Anaesthesia No perfect solution Trauma 1. Inhalational 2. Awake FOB 3. Rapid Sequence 4. Trache under Local
42 ENT Anaesthesia No perfect solution 1. Trauma Rapid Sequence 4. Trache LA

43 ENT Anaesthesia No perfect solution Rapid Sequence 4. Trache LA

44 ENT Anaesthesia No perfect solution Rapid Sequence 4. Trache LA
45 Emergency ENT Anaesthesia 1 Plan each case 2 Keep to known basics
46 Bleeding Tonsil
47 Bleeding Tonsil Issues Frightened child & anxious parents Hypovolaemia Full stomach Residual effects of anaesthetic Difficult intubation
48 Post Tonsillectomy haemorrhage 3.3% in a series of Krishna et al, % in a series of Bhattacharyya, % in a series of Collison et al, % in a series of Ranjit et al, 1999
49 Post Tonsillectomy haemorrhage Risk factors proposed : Patient profile - age, medical conditions Time of the year of surgery Use of local vasoconstrictors and dissection method Immediate post operative state
50 Bleeding Tonsil Prevention Resuscitation Procedure in theatre
51 ENT Anaesthesia Bleeding Tonsil 1. Inhalational 2. Awake FOB 3. Rapid Sequence 4. Trache under Local
52 ENT Anaesthesia Bleeding Tonsil 1. Inhalational Rapid Sequence 4.

53 Bleeding Tonsil Inhalational Lateral Position

54 Bleeding Tonsil Supine Rapid Sequence Previous laryngoscopy LMA
55 Another Call to A & E
56 Another Call to A & E 4 year old girl with inspiratory stridor
57 Another Call to A & E 4 year old girl with inspiratory stridor Unwell for the last 6 hours
58 Another Call to A & E 4 year old girl with inspiratory stridor Unwell for the last 6 hours With a temp of 39 and is now drooling.

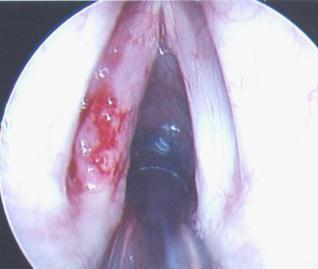
59 Acute Epiglottitis Infection Haemophilus Influenza type b Children 2-5 year olds Typical clinical features
60 Acute Epiglottitis Febrile Tachypnoea Sitting forward Drooling

61 Acute Epiglottitis Calm environment No intervention Inhalational Induction

62 Prepared for difficult intubation Tube 1 size smaller than normal Urgent tracheostomy?change to nasal Acute Epiglottitis

63 Prepared for difficult intubation Tube 1 size smaller than normal Urgent tracheostomy?change to nasal Acute Epiglottitis

64
65

66
67 Acute Epiglottitis Sevoflurane vs Halothane Myocardial dysrhythmias Apnoea in deep planes Airway obstruction
68 Acute Epiglottitis Changing incidence Hib vaccine Introduced Oct , 3 & 4 months

69 Acute Epiglottitis Changing incidence Hib vaccine Introduced Oct , 3 & 4 months

70 Changing Incidence Acute Epiglottitis Incidence in Sheffield Midwinter et al, 1999


71 Acute Epiglottitis Garpenholt et al 1999 Vaccination program in Sweden
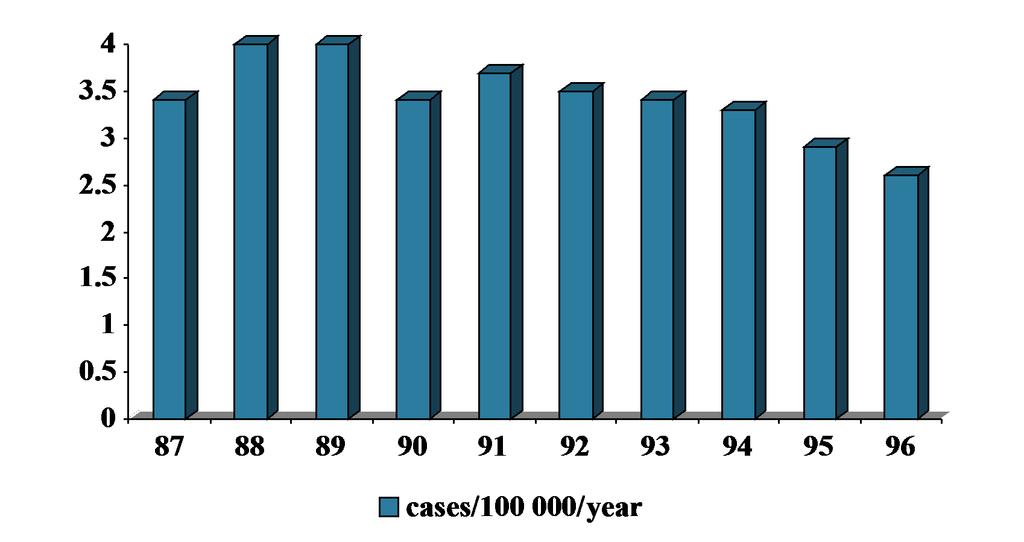

72 Acute Epiglottitis >15 year olds
73 Acute Epiglottitis In adults incidence has remained stable Missed vaccination Homeopathy Increased awareness
74 Emergency Bell Rings!
75 Emergency Bell Rings! Patient left in recovery after a long procedure last night. Neck is swelling
76 Postop Thyroid Bleeding
77 Head & Neck Bleed Plan A Prevention Plan B Prevention Plan C Prevention
78 ENT Anaesthesia 1.Inhalational 2.Awake FOB 3.Rapid Sequence 4.Trache under Local
79 ENT Anaesthesia 1.Inhalational 2. 3.Rapid Sequence 4.Trache under Local
80 ENT Anaesthesia PHONE A FRIEND 1.Inhalational 2. 3.Rapid Sequence 4.Trache under Local
81 Head & Neck Bleed Plan A Prevention Plan B Prevention Plan C Prevention Plan Y Remove clips, inhalational induction, remove clot Plan Z Surgical airway

82
83
84 Trache under Local

85 **Emergency Tracheostomy**

86

87

88

89

90
91 Mr Krishnan s ENT list tomorrow, the first patient is a 76 year old man for Panedoscopy and Biopsy.
92 Stridor Obstructed Airway The worst fear of most Anaesthetists
93 Stridor Obstructed Airway - issues
94 Stridor Obstructed Airway - issues 1. Elderly cachetic patient 2. Shared airway & poor access 3. Abn anatomy difficult intubation 4. Smoking CVS & Resp disease 5. Large intraop blood loss 6. Carotid sinus stimulation 7. Air embolus or pneumothorax
95 CEPOD recommendations Discussion with Surgeons Adequate preop evaluation SpR s receive training Fibreoptic Intubation Tracheostomy under LA
96





97 Mild Moderate Severe

98 Nasendoscope Assess airway OPD Do not touch cords Supraglottic CT scan

99 Nasendoscope Assess airway OPD Do not touch cords Supraglottic CT scan
100
101 Supraglottic - Moderate stridor
102 Supraglottic - Moderate stridor Plan A
103 Supraglottic - Moderate stridor Plan A Inhalation induction in theatre Maintain spontaneous ventilation
104 Supraglottic - Moderate stridor Plan A Inhalation induction in theatre Maintain spontaneous ventilation Anaesthesia 1999, 54, The obstructed airway in head and neck surgery. Mason, Fielder.
105 Supraglottic - Moderate stridor Plan A Inhalation induction in theatre Maintain spontaneous ventilation or Take over ventilation & give relaxant
106 Supraglottic - Moderate stridor Take over ventilation & give relaxant Reach end point quicker PEEP to splint airway Achieve ideal intubating conditions
107 Supraglottic - Moderate stridor Plan A Inhalation induction in theatre Maintain spontaneous ventilation or Take over ventilation & give relaxant Plan B LMA & trache asleep
108 Supraglottic - Moderate stridor Plan A Inhalation induction in theatre Maintain spontaneous ventilation or Take over ventilation & give relaxant Plan B LMA Plan C Wake up
109 Supraglottic - Moderate stridor Plan A Inhalation induction in theatre Maintain spontaneous ventilation or Take over ventilation & give relaxant Plan B LMA Plan C Wake up Plan D Surgical Airway

110

111
112 Which Tubes Moderate Stridor
113 Tubes Laser tube Jet ventilate MLT Cricothyroid needle Moderate stridor
114 Where issues arise! Extubation

115
116
117 Extubation 1 Leave tube in and send to ICU

118 Extubation 1 Leave tube in and send to ICU
119
120 Extubation 1 Leave tube in and send to ICU 2 Extubate Awake

121 Extubation 1 Leave tube in and send to ICU 2 Extubate Awake
122 Extubation 1 Leave tube in and send to ICU 2 Extubate Awake 3 Extubate Deep
123 Extubation 1 Leave tube in and send to ICU 2 Extubate Awake 3 Extubate Deep Who would do this?

124 Extubation 1 Leave tube in and send to ICU 2 Extubate Awake 3 Extubate Deep

125

126
127 Extubation Deep 1 Smooth slow emergence 2 No risk of coughing on the tube 3 Less risk of laryngospasm
128 Extubation Deep 1 Smooth slow emergence 2 No risk of coughing on the tube 3 Less risk of laryngospasm Change to an LMA
129 Ext Guidelines Advanced Technique 1. Was the patient Easy to Intubate 2. Replace Pillow 3. Suction under direct vision 4. Check for Coroner s clot 5. Leave Sevoflurane ON!
130 Supraglottic lesions Severe Stridor Implications of stridor Late presentation Misdiagnosis

131 Supraglottic Severe stridor Arrive as emergency or deteriorated after radiotherapy Avoid sedation Helium Oxygen mixture Nebulised Adrenaline

132

133
134 ENT Anaesthesia No perfect solution 1. Inhalational 2. Awake FOB 3. Rapid Sequence 4. Trache under Local
135 Supraglottic Severe stridor Surgical airway under LA Tracheostomy Cricothyroidotomy cannulae below the lesion

136

137

138

139

140

141

142

143

144
145

146

147

148

149

150

151 Postop?

152

153

154

155

156
157 Tracheostomy Induction

158

159

160

161

162

163

164

165
166 No perfect solution ENT Anaesthesia
167 ENT Anaesthesia No perfect solution 1. Inhalational 2. Awake FOB 3. Rapid Sequence 4. Trache under Local
168 Emergency ENT Anaesthesia Thank you
DIFFICULT AIRWAY MANAGMENT. Dr.N.SANTHOSH KUMAR MD ANESTHESIA (2 nd Yr)
") DIFFICULT AIRWAY MANAGMENT Dr.N.SANTHOSH KUMAR MD ANESTHESIA (2 nd Yr) AIRWAY MANAGEMENT AND MAINTAINING OXYGENATION ARE THE FUNDAMENTAL RESPONSIBILITIES OF ANY BASIC DOCTOR. TO MANAGE A DIFFICULT AIRWAY,
DIFFICULT AIRWAY MANAGMENT Dr.N.SANTHOSH KUMAR MD ANESTHESIA (2 nd Yr) AIRWAY MANAGEMENT AND MAINTAINING OXYGENATION ARE THE FUNDAMENTAL RESPONSIBILITIES OF ANY BASIC DOCTOR. TO MANAGE A DIFFICULT AIRWAY,
Emergency Airway Management. Richard P. Dutton, M.D., M.B.A. Chief Quality Officer US Anesthesia Partners
 Emergency Airway Management Richard P. Dutton, M.D., M.B.A. Chief Quality Officer US Anesthesia Partners Disclosures I have studied a lot of airway gizmos over the years. I have no financial interest in
Emergency Airway Management Richard P. Dutton, M.D., M.B.A. Chief Quality Officer US Anesthesia Partners Disclosures I have studied a lot of airway gizmos over the years. I have no financial interest in
Preface... Acknowledgements... Contributors... 1 The Difficult Airway: Definitions and Algorithms The Expected Difficult Airway...
 Contents Preface... Acknowledgements... Contributors... vii ix xvii 1 The Difficult Airway: Definitions and Algorithms... 1 Zdravka Zafirova and Avery Tung Introduction 1 Definitions 2 Incidence 3 Algorithms
Contents Preface... Acknowledgements... Contributors... vii ix xvii 1 The Difficult Airway: Definitions and Algorithms... 1 Zdravka Zafirova and Avery Tung Introduction 1 Definitions 2 Incidence 3 Algorithms
Difficult Airway. Victor M. Gomez, M.D. Pulmonary Critical Care Medicine Medical City Dallas Hospital
 Difficult Airway Victor M. Gomez, M.D. Pulmonary Critical Care Medicine Medical City Dallas Hospital Difficult Airway Definition Predicting a difficult airway Preparing for a difficult airway Extubation
Difficult Airway Victor M. Gomez, M.D. Pulmonary Critical Care Medicine Medical City Dallas Hospital Difficult Airway Definition Predicting a difficult airway Preparing for a difficult airway Extubation
Angkana Lurngnateetape,, MD. Department of Anesthesiology Siriraj Hospital
 AIRWAY MANAGEMENT Angkana Lurngnateetape,, MD. Department of Anesthesiology Siriraj Hospital Perhaps the most important responsibility of the anesthesiologist is management of the patient s airway Miller
AIRWAY MANAGEMENT Angkana Lurngnateetape,, MD. Department of Anesthesiology Siriraj Hospital Perhaps the most important responsibility of the anesthesiologist is management of the patient s airway Miller
Diagnosis & Management of the Difficult Airway
 Diagnosis & Management of the Difficult Airway Dr. E. Rawlings Plymouth Anaesthetic Department Complications of Airway Management Medicolegal Serious morbidity Mortality Complications of Airway Management
Diagnosis & Management of the Difficult Airway Dr. E. Rawlings Plymouth Anaesthetic Department Complications of Airway Management Medicolegal Serious morbidity Mortality Complications of Airway Management
(ix) Difficult & Failed Intubation Queen Charlotte s Hospital
 Difficult & Failed Intubation Queen Charlotte s Hospital") (ix) Difficult & Failed Intubation Queen Charlotte s Hospital Pre-operative Assessment Clinical assessment of airway and risk of difficult intubation: (can be performed in a matter of seconds): 1. Mouth
(ix) Difficult & Failed Intubation Queen Charlotte s Hospital Pre-operative Assessment Clinical assessment of airway and risk of difficult intubation: (can be performed in a matter of seconds): 1. Mouth
Other methods for maintaining the airway (not definitive airway as still unprotected):
:") Page 56 Where anaesthetic skills and drugs are available, endotracheal intubation is the preferred method of securing a definitive airway. This technique comprises: rapid sequence induction of anaesthesia
Page 56 Where anaesthetic skills and drugs are available, endotracheal intubation is the preferred method of securing a definitive airway. This technique comprises: rapid sequence induction of anaesthesia
Final FRCA Written PAEDIATRICS Past Paper Questions November March 2014
 Final FRCA Written PAEDIATRICS Past Paper Questions November 1996- March 2014 March 2014 A 5-year-old patient presents for a myringotomy and grommet insertion as a day case. During your pre-operative assessment
Final FRCA Written PAEDIATRICS Past Paper Questions November 1996- March 2014 March 2014 A 5-year-old patient presents for a myringotomy and grommet insertion as a day case. During your pre-operative assessment
Airway Anaesthesia for Final FRCA
 Airway Anaesthesia for Final FRCA Final FRCA Teaching July 2018 Dr Kate Henderson Learning Outcomes Popular exam topics Anatomy Case based discussions Exam questions Potential Topics Recent publications
Airway Anaesthesia for Final FRCA Final FRCA Teaching July 2018 Dr Kate Henderson Learning Outcomes Popular exam topics Anatomy Case based discussions Exam questions Potential Topics Recent publications
Airway management problem during anaesthesia. Airway management problem in ICU / HDU. Airway management problem occurring in the Emergency Department
 4th National Audit Project of the Royal College of Anaesthetists: Major Complications of Airway Management in the UK Please select one form from the list below Airway management problem during anaesthesia
4th National Audit Project of the Royal College of Anaesthetists: Major Complications of Airway Management in the UK Please select one form from the list below Airway management problem during anaesthesia
Failed tracheal intubation in obstetrics why do we need a guideline?
 Failed tracheal intubation in obstetrics why do we need a guideline? Chris Elton Leicester Royal Infirmary OAA Cases & Clinical Challenges in Obstetric Anaesthesia Churchhouse Westminster 2/3/16 Declarations
Failed tracheal intubation in obstetrics why do we need a guideline? Chris Elton Leicester Royal Infirmary OAA Cases & Clinical Challenges in Obstetric Anaesthesia Churchhouse Westminster 2/3/16 Declarations
ANAESTHESIA FOR BLEEDING TONSIL
 ANAESTHESIA FOR BLEEDING TONSIL BY Dr.S.C.Ganeshprabu, MD., D.A., Professor of Anaesthesiology, Madurai Medical College & Govt. Rajaji Hospital, Madurai -652 020. A 5-year-old child who had tonsillectomy
ANAESTHESIA FOR BLEEDING TONSIL BY Dr.S.C.Ganeshprabu, MD., D.A., Professor of Anaesthesiology, Madurai Medical College & Govt. Rajaji Hospital, Madurai -652 020. A 5-year-old child who had tonsillectomy
If you suspect airway problems, get a second opinion before you anaesthetise, not after!
 Assessing the airway It is more important to be aware of the various methods of dealing with difficult laryngoscopy than to expect to be able to accurately identify the rare difficult patients without
Assessing the airway It is more important to be aware of the various methods of dealing with difficult laryngoscopy than to expect to be able to accurately identify the rare difficult patients without
GENERAL ANAESTHESIA AND FAILED INTUBATION
 GENERAL ANAESTHESIA AND FAILED INTUBATION INTRODUCTION The majority of caesarean sections in the UK are performed under regional anaesthesia. However, there are situations where general anaesthesia (GA)
GENERAL ANAESTHESIA AND FAILED INTUBATION INTRODUCTION The majority of caesarean sections in the UK are performed under regional anaesthesia. However, there are situations where general anaesthesia (GA)
Airway Management. Teeradej Kuptanon, MD
 Airway Management Teeradej Kuptanon, MD Outline Anatomy Detect difficult airway Rapid sequence intubation Difficult ventilation Difficult intubation Surgical airway access ICU setting Intubation Difficult
Airway Management Teeradej Kuptanon, MD Outline Anatomy Detect difficult airway Rapid sequence intubation Difficult ventilation Difficult intubation Surgical airway access ICU setting Intubation Difficult
Post-tonsillectomy bleeding - Beware (Part I) M De W Wium. (CME, Nov/Dec 2003, Vol 21, No 11.) Anaesthetic management
 M De W Wium. (CME, Nov/Dec 2003, Vol 21, No 11.) Anaesthetic management") Post-tonsillectomy bleeding - Beware (Part I) M De W Wium (CME, Nov/Dec 2003, Vol 21, No 11.) Anaesthetic management If a child is returned to theatre for a post-tonsillectomy haemorrhage it is almost
Post-tonsillectomy bleeding - Beware (Part I) M De W Wium (CME, Nov/Dec 2003, Vol 21, No 11.) Anaesthetic management If a child is returned to theatre for a post-tonsillectomy haemorrhage it is almost
Advanced Airway Management. University of Colorado Medical School Rural Track
 Advanced Airway Management University of Colorado Medical School Rural Track Advanced Airway Management Basic Airway Management Airway Suctioning Oxygen Delivery Methods Laryngeal Mask Airway ET Intubation
Advanced Airway Management University of Colorado Medical School Rural Track Advanced Airway Management Basic Airway Management Airway Suctioning Oxygen Delivery Methods Laryngeal Mask Airway ET Intubation
AIRWAY MANAGEMENT AND VENTILATION
 AIRWAY MANAGEMENT AND VENTILATION D1 AIRWAY MANAGEMENT AND VENTILATION Basic airway management and ventilation The laryngeal mask airway and Combitube Advanced techniques of airway management D2 Basic
AIRWAY MANAGEMENT AND VENTILATION D1 AIRWAY MANAGEMENT AND VENTILATION Basic airway management and ventilation The laryngeal mask airway and Combitube Advanced techniques of airway management D2 Basic
Airway/Breathing. Chapter 5
 Airway/Breathing Chapter 5 Airway/Breathing Introduction Skillful, rapid assessment and management of airway and ventilation are critical to preventing morbidity and mortality. Airway compromise can occur
Airway/Breathing Chapter 5 Airway/Breathing Introduction Skillful, rapid assessment and management of airway and ventilation are critical to preventing morbidity and mortality. Airway compromise can occur
General OR Rotations GOALS & OBJECTIVES
 General OR Rotations GOALS & OBJECTIVES Goals At the end of the CA 1 year General OR rotations, the resident should competently manage uncomplicated ambulatory, orthopedic, maxillo-facial, ENT, gynecologic,
General OR Rotations GOALS & OBJECTIVES Goals At the end of the CA 1 year General OR rotations, the resident should competently manage uncomplicated ambulatory, orthopedic, maxillo-facial, ENT, gynecologic,
Dr.Bharghavi.M 2 nd year post graduate Dept of Anaesthesia
 DIFFICULT AIRWAY CANNOT VENTILATE, CANNOT INTUBATE. Dr.Bharghavi.M 2 nd year post graduate Dept of Anaesthesia Difficult airway According to AMERICAN SOCIETY OF ANAESTHESIOLOGISTS Difficult Airway is defined
DIFFICULT AIRWAY CANNOT VENTILATE, CANNOT INTUBATE. Dr.Bharghavi.M 2 nd year post graduate Dept of Anaesthesia Difficult airway According to AMERICAN SOCIETY OF ANAESTHESIOLOGISTS Difficult Airway is defined
Risky Extubation. Andy Higgs. Warrington Hospitals Cheshire UK
 Andy Higgs Warrington Hospitals Cheshire UK Declaration COOKMEDICAL Extubation plan DAS guideline Airway Exchange Catheters # 11 CAEC post maxillo-facial surgery Used as intubation stylets Airway Exchange
Andy Higgs Warrington Hospitals Cheshire UK Declaration COOKMEDICAL Extubation plan DAS guideline Airway Exchange Catheters # 11 CAEC post maxillo-facial surgery Used as intubation stylets Airway Exchange
2/3/2015. Anterior Mediastinal Masses and Lower Airway Problems
 es and Lower Airway Problems es and Lower Airway Problems 25 y.o. Female Ant. Mediastinal Mass Cervical Mediastinoscopy + Biopsy Most Important History? A) Dysphagia B) Fever C) Orthopnea D) Chest pain
es and Lower Airway Problems es and Lower Airway Problems 25 y.o. Female Ant. Mediastinal Mass Cervical Mediastinoscopy + Biopsy Most Important History? A) Dysphagia B) Fever C) Orthopnea D) Chest pain
PREDICTION AND MANAGEMENT OF DIFFICULT TRACHEAL INTUBATION
 PREDICTION AND MANAGEMENT OF DIFFICULT TRACHEAL INTUBATION Dr I H Wilson, Department of Anaesthesia, Royal Devon and Exeter Hospital, Exeter, EX2 5DW Dr Andreas Kopf, Department of Anaesthesia, Benjamin
PREDICTION AND MANAGEMENT OF DIFFICULT TRACHEAL INTUBATION Dr I H Wilson, Department of Anaesthesia, Royal Devon and Exeter Hospital, Exeter, EX2 5DW Dr Andreas Kopf, Department of Anaesthesia, Benjamin
Management of airway in patients with laryngeal tumors
 Journal of Clinical Anesthesia (2005) 17, 604 609 Original contribution Management of airway in patients with laryngeal tumors Sreenivasa S. Moorthy MD (Professor, Chief) a,b, Sanjay Gupta MBBS (Staff)
Journal of Clinical Anesthesia (2005) 17, 604 609 Original contribution Management of airway in patients with laryngeal tumors Sreenivasa S. Moorthy MD (Professor, Chief) a,b, Sanjay Gupta MBBS (Staff)
Airway Anatomy. Soft palate. Hard palate. Nasopharynx. Tongue. Oropharynx. Hypopharynx. Thyroid cartilage
 Airway Anatomy Hard palate Soft palate Tongue Nasopharynx Oropharynx Hypopharynx Thyroid cartilage Airway Anatomy Hyoid bone Thyroid cartilage Cricoid cartilage Trachea Cricothyroid membrane Airway Anatomy
Airway Anatomy Hard palate Soft palate Tongue Nasopharynx Oropharynx Hypopharynx Thyroid cartilage Airway Anatomy Hyoid bone Thyroid cartilage Cricoid cartilage Trachea Cricothyroid membrane Airway Anatomy
Upper Airway Obstruction
 Upper Airway Obstruction Adriaan Pentz Division of Otorhinolaryngology University of Stellenbosch and Tygerberg Hospital Stridor/Stertor Auditory manifestations of disordered respiratory function ie noisy
Upper Airway Obstruction Adriaan Pentz Division of Otorhinolaryngology University of Stellenbosch and Tygerberg Hospital Stridor/Stertor Auditory manifestations of disordered respiratory function ie noisy
ANESTHESIOLOGY CASE LOG CHANGES 2015
 ANESTHESIOLOGY CASE LOG CHANGES 2015 I. Case Information FORMER: 1. Role removed. 2. Setting removed. 3. Involved Morbidity has been renamed Life-Threatening Pathology. a. All former cases that included
ANESTHESIOLOGY CASE LOG CHANGES 2015 I. Case Information FORMER: 1. Role removed. 2. Setting removed. 3. Involved Morbidity has been renamed Life-Threatening Pathology. a. All former cases that included
The 2015 DAS Guidelines
 The 2015 DAS Guidelines Housekeeping & provenance Housekeeping & provenance Preparation for intubation Algorithms New Plans A-D New features Housekeeping 2004 2009 2011 2012 2015 2004 2009 2011 2012 2015
The 2015 DAS Guidelines Housekeeping & provenance Housekeeping & provenance Preparation for intubation Algorithms New Plans A-D New features Housekeeping 2004 2009 2011 2012 2015 2004 2009 2011 2012 2015
Recognizing the Difficult Airway in Pediatric Patients. Nancy L. Glass, MD, MBA,
 Recognizing the Difficult Airway in Pediatric Patients Nancy L. Glass, MD, MBA, FAAP nglass@bcm.edu @DrNancyGlass1 None Disclosures Learning Objectives At the end of this presentation, participants will
Recognizing the Difficult Airway in Pediatric Patients Nancy L. Glass, MD, MBA, FAAP nglass@bcm.edu @DrNancyGlass1 None Disclosures Learning Objectives At the end of this presentation, participants will
Major complications of airway management in the United Kingdom
 The Royal College of Anaesthetists The Difficult Airway Society 4th National Audit Project of The Royal College of Anaesthetists and The Difficult Airway Society Major complications of airway management
The Royal College of Anaesthetists The Difficult Airway Society 4th National Audit Project of The Royal College of Anaesthetists and The Difficult Airway Society Major complications of airway management
Airway/Breathing. Chapter 5
 Airway/Breathing Chapter 5 Airway/Breathing Introduction Skillful, rapid, assessment and management of airway and ventilation are critical to preventing morbidity and mortality. Airway compromise can occur
Airway/Breathing Chapter 5 Airway/Breathing Introduction Skillful, rapid, assessment and management of airway and ventilation are critical to preventing morbidity and mortality. Airway compromise can occur
Airway Management in Trauma
 Editorial Volume 2 Number 1, January - June 2015 9 DOI: https://dx.doi.org/10.21088/ijaa.2349.8471.2115.1 Airway Management in Trauma The primary goal in the early treatment of the trauma patient is to
Editorial Volume 2 Number 1, January - June 2015 9 DOI: https://dx.doi.org/10.21088/ijaa.2349.8471.2115.1 Airway Management in Trauma The primary goal in the early treatment of the trauma patient is to
PRACTICE GUIDELINES FOR MANAGEMENT OF THE DIFFICULT AIRWAY 1 (Approved by House of Delegates on October 21, 1992, and last amended October 16, 2002)
") PRACTICE GUIDELINES FOR MANAGEMENT OF THE DIFFICULT AIRWAY 1 (Approved by House of Delegates on October 21, 1992, and last amended October 16, 2002) Practice guidelines are systematically developed recommendations
PRACTICE GUIDELINES FOR MANAGEMENT OF THE DIFFICULT AIRWAY 1 (Approved by House of Delegates on October 21, 1992, and last amended October 16, 2002) Practice guidelines are systematically developed recommendations
Difficult Airway. Summary. Setting. Time. Participants. Progressive Complexity. Potential Systems Explored. Page.
 Scenario Overview Summary ww man, arrives at the operating room (OR) holding area from the emergency room for urgent surgery due to a suspected ruptured appendix. During induction he becomes difficult
Scenario Overview Summary ww man, arrives at the operating room (OR) holding area from the emergency room for urgent surgery due to a suspected ruptured appendix. During induction he becomes difficult
Anatomy and Physiology. The airways can be divided in to parts namely: The upper airway. The lower airway.
 Airway management Anatomy and Physiology The airways can be divided in to parts namely: The upper airway. The lower airway. Non-instrumental airway management Head Tilt and Chin Lift Jaw Thrust Advanced
Airway management Anatomy and Physiology The airways can be divided in to parts namely: The upper airway. The lower airway. Non-instrumental airway management Head Tilt and Chin Lift Jaw Thrust Advanced
Effectiveness of Fiberoptic Intubation in Anticipated Difficult Airway
 Original Article Effectiveness of Fiberoptic Intubation in Anticipated Difficult Airway Khawaja Kamal Nasir, Faraz Mansoor From Department of Anesthesia, Pakistan Institute of Medical Sciences, Islamabad.
Original Article Effectiveness of Fiberoptic Intubation in Anticipated Difficult Airway Khawaja Kamal Nasir, Faraz Mansoor From Department of Anesthesia, Pakistan Institute of Medical Sciences, Islamabad.
Case Presentation Topic: Difficult to Ventilate Difficult to Intubate
 Case Presentation Topic: Difficult to Ventilate Difficult to Intubate Dr. K. Shruthi Jeevan 1 st Year Post Graduate Department of Anaesthesiology CASE SCENARIO : 1 A 65 years old female patient, resident
Case Presentation Topic: Difficult to Ventilate Difficult to Intubate Dr. K. Shruthi Jeevan 1 st Year Post Graduate Department of Anaesthesiology CASE SCENARIO : 1 A 65 years old female patient, resident
Disclosures. Learning Objectives. Coeditor/author. Associate Science Editor, American Heart Association
 Tracheotomy Challenges for airway specialists Elizabeth H. Sinz, MD Professor of Anesthesiology & Neurosurgery Associate Dean for Clinical Simulation Disclosures Coeditor/author Associate Science Editor,
Tracheotomy Challenges for airway specialists Elizabeth H. Sinz, MD Professor of Anesthesiology & Neurosurgery Associate Dean for Clinical Simulation Disclosures Coeditor/author Associate Science Editor,
When I started. 10/27/2009. Gerald Wydro, MD Clinical Associate Professor Emergency Medicine Temple University School of Medicine
 When I started. Gerald Wydro, MD Clinical Associate Professor Emergency Medicine Temple University School of Medicine When I started. When I started. When I started. When I started. How To Make A Fertile
When I started. Gerald Wydro, MD Clinical Associate Professor Emergency Medicine Temple University School of Medicine When I started. When I started. When I started. When I started. How To Make A Fertile
LEVITAN S FIBREOPTIC STYLET: BEYOND BARRIERS. - Our Perspective.
 ISSN: 2250-0359 Volume 3 Issue 4 2013 LEVITAN S FIBREOPTIC STYLET: BEYOND BARRIERS - Our Perspective. Justin Ebenezer Sargunaraj * Dr.Balasubramaniam Thiagarajan * *Stanley Medical College ABSTRACT: This
ISSN: 2250-0359 Volume 3 Issue 4 2013 LEVITAN S FIBREOPTIC STYLET: BEYOND BARRIERS - Our Perspective. Justin Ebenezer Sargunaraj * Dr.Balasubramaniam Thiagarajan * *Stanley Medical College ABSTRACT: This
1/3/2008. Karen Burke Priscilla LeMone Elaine Mohn-Brown. Medical-Surgical Nursing Care, 2e Karen Burke, Priscilla LeMone, and Elaine Mohn-Brown
 Medical-Surgical Nursing Care Second Edition Karen Burke Priscilla LeMone Elaine Mohn-Brown Chapter 23 Caring for Clients with Upper Respiratory Disorders Rhinitis Inflammation of Nasal Cavities Types
Medical-Surgical Nursing Care Second Edition Karen Burke Priscilla LeMone Elaine Mohn-Brown Chapter 23 Caring for Clients with Upper Respiratory Disorders Rhinitis Inflammation of Nasal Cavities Types
Surgical Care at the District Hospital. EMERGENCY & ESSENTIAL SURGICAL CARE
 Surgical Care at the District Hospital 1 14 Practical Anesthesia Key Points 2 14.1 General Anesthesia Have a clear plan before starting anesthesia Never use an unfamiliar anesthetic technique in an emergency
Surgical Care at the District Hospital 1 14 Practical Anesthesia Key Points 2 14.1 General Anesthesia Have a clear plan before starting anesthesia Never use an unfamiliar anesthetic technique in an emergency
Australian and New Zealand College of Anaesthetists (ANZCA)
") PS61 2017 Australian and New Zealand College of Anaesthetists (ANZCA) Guidelines for the Management of Evolving Airway Obstruction: Transition to the Can t Intubate Can t Oxygenate Airway Emergency 1.
PS61 2017 Australian and New Zealand College of Anaesthetists (ANZCA) Guidelines for the Management of Evolving Airway Obstruction: Transition to the Can t Intubate Can t Oxygenate Airway Emergency 1.
Basic Scope Care and Handling
 Basic Scope Care and Handling Basic principles behind fibre-optic instruments Light and image transfer via coherent(image transmission) and incoherent (light)bundles Fibre coating with lower refractory
Basic Scope Care and Handling Basic principles behind fibre-optic instruments Light and image transfer via coherent(image transmission) and incoherent (light)bundles Fibre coating with lower refractory
Pediatrics Grand Rounds 25 October University of Texas Health Science Center at San Antonio, Texas
 PEDIATRIC ENT & YOU A PATIENT CARE PARTNERSHIP Disclosure Timothy McEvoy, MD has no relevant relationships with commercial interests to disclose. Timothy McEvoy, MD UTHSCSA Department of Otolaryngology-
PEDIATRIC ENT & YOU A PATIENT CARE PARTNERSHIP Disclosure Timothy McEvoy, MD has no relevant relationships with commercial interests to disclose. Timothy McEvoy, MD UTHSCSA Department of Otolaryngology-
Your anaesthetic for heart surgery
 Your anaesthetic for heart surgery Information for patients and carers First Edition 2018 www.rcoa.ac.uk/patientinfo This leaflet gives you information about your anaesthetic for adult heart (cardiac)
Your anaesthetic for heart surgery Information for patients and carers First Edition 2018 www.rcoa.ac.uk/patientinfo This leaflet gives you information about your anaesthetic for adult heart (cardiac)
FAILED INTUBATION DURING RSI: PLAN A, C & D
 FAILED INTUBATION DURING RSI: PLAN A, C & D MODULE: NOVICE & AIRWAY TARGET: NOVICE INITIAL ASSESSMENT OF COMPETENCY ALL ANAESTHETISTS BACKGROUND: Management of the Can t Intubate, Can t Ventilate situation
FAILED INTUBATION DURING RSI: PLAN A, C & D MODULE: NOVICE & AIRWAY TARGET: NOVICE INITIAL ASSESSMENT OF COMPETENCY ALL ANAESTHETISTS BACKGROUND: Management of the Can t Intubate, Can t Ventilate situation
difficult airway CASE management
 difficult airway CASE management DEPT. OF ANAESTHESIA Dr. SUPRIYA PUSAPATI ANAESTHESIA PG 2 ND YR 09 04 2015 In a case of Cervical spine fracture and myelopathy CASE PRESENTATION A 60yr male presented
difficult airway CASE management DEPT. OF ANAESTHESIA Dr. SUPRIYA PUSAPATI ANAESTHESIA PG 2 ND YR 09 04 2015 In a case of Cervical spine fracture and myelopathy CASE PRESENTATION A 60yr male presented
Airway management problem during anaesthesia. Airway management problem occurring in the Emergency Department
 4th National Audit Project of the Royal College of Anaesthetists: Major Complications of Airway Management in the UK Please select one form from the list below Airway management problem during anaesthesia
4th National Audit Project of the Royal College of Anaesthetists: Major Complications of Airway Management in the UK Please select one form from the list below Airway management problem during anaesthesia
Tracheostomy. Intensive Care Unit Patient Information Leaflet
 Tracheostomy Intensive Care Unit Patient Information Leaflet Introduction This leaflet is for patients having a tracheostomy and their relatives. It gives information on the procedure, and its benefits
Tracheostomy Intensive Care Unit Patient Information Leaflet Introduction This leaflet is for patients having a tracheostomy and their relatives. It gives information on the procedure, and its benefits
Department of Pediatric Otolarygnology. ENT Specialty Programs
 Department of Pediatric Otolarygnology ENT Specialty Programs Staffed by fellowship-trained otolaryngologists, assisted by pediatric nurse practitioners, ENT (Otolaryngology) at Nationwide Children s Hospital
Department of Pediatric Otolarygnology ENT Specialty Programs Staffed by fellowship-trained otolaryngologists, assisted by pediatric nurse practitioners, ENT (Otolaryngology) at Nationwide Children s Hospital
ASPIRATION DURING ANAESTHESIA
 ASPIRATION DURING ANAESTHESIA MODULE: CRITICAL INCIDENTS TARGET: ALL ANAESTHETISTS BACKGROUND: Passive regurgitation or vomiting can occur during the pre-, peri- or post- operative period risking aspiration
ASPIRATION DURING ANAESTHESIA MODULE: CRITICAL INCIDENTS TARGET: ALL ANAESTHETISTS BACKGROUND: Passive regurgitation or vomiting can occur during the pre-, peri- or post- operative period risking aspiration
student handbook BARS handbook September 2012.indd Front Cover 27/11/12 12:08 PM
 student handbook BARS handbook September 2012.indd Front Cover 27/11/12 12:08 PM All materials regarding the Basic Airway Resuscitation Strategy Course were written and developed by Dr. Richard Morris
student handbook BARS handbook September 2012.indd Front Cover 27/11/12 12:08 PM All materials regarding the Basic Airway Resuscitation Strategy Course were written and developed by Dr. Richard Morris
Management of pediatric cannot intubate, cannot oxygenate
 Acute Medicine & Surgery 2017; 4: 462 466 doi: 10.1002/ams2.305 Case Report Management of pediatric cannot intubate, cannot oxygenate Yohei Okada, 1 Wataru Ishii, 1 Norio Sato, 2 Hirokazu Kotani, 3 and
Acute Medicine & Surgery 2017; 4: 462 466 doi: 10.1002/ams2.305 Case Report Management of pediatric cannot intubate, cannot oxygenate Yohei Okada, 1 Wataru Ishii, 1 Norio Sato, 2 Hirokazu Kotani, 3 and
APPROACH TO THE EMERGENCY AIRWAY. Scott B. Davidson MD, FACS Trauma Surgery Service Bronson Methodist Hospital
 APPROACH TO THE EMERGENCY AIRWAY Scott B. Davidson MD, FACS Trauma Surgery Service Bronson Methodist Hospital Objectives History Initial recognition Get your act together Surgical options Complications
APPROACH TO THE EMERGENCY AIRWAY Scott B. Davidson MD, FACS Trauma Surgery Service Bronson Methodist Hospital Objectives History Initial recognition Get your act together Surgical options Complications
Pediatric Difficult Airway Management. R2 Nichakan Rewurai R2 Pattiya Suttidate Supervisor: Assist. Prof. Sahatsa Mandee
 Pediatric Difficult Airway Management R2 Nichakan Rewurai R2 Pattiya Suttidate Supervisor: Assist. Prof. Sahatsa Mandee The pediatric difficult airway is associated with a high risk for complications during
Pediatric Difficult Airway Management R2 Nichakan Rewurai R2 Pattiya Suttidate Supervisor: Assist. Prof. Sahatsa Mandee The pediatric difficult airway is associated with a high risk for complications during
Microdebrider. Microdebrider. Mohamed Hesham,MD. The Management of Different Laryngeal Lesions. Dr. Ahmad Yassin 4/11/2013
 Microdebrider In The Management of Different Laryngeal Lesions Mohamed Hesham,MD Dr. Ahmad Yassin Otolaryngology Head&Neck Surgery Alexandria Faculty of Medicine Microdebrider The microdebrider is a powered
Microdebrider In The Management of Different Laryngeal Lesions Mohamed Hesham,MD Dr. Ahmad Yassin Otolaryngology Head&Neck Surgery Alexandria Faculty of Medicine Microdebrider The microdebrider is a powered
FAILED ELECTIVE INTUBATION: PLAN A- C
 FAILED ELECTIVE INTUBATION: PLAN A- C MODULE: AIRWAY TARGET: NOVICE, BASIC LEVEL TRAINEES & ALL ANAESTHETISTS BACKGROUND: Management of the unexpectedly difficult airway is a core skill for all anaesthetists.
FAILED ELECTIVE INTUBATION: PLAN A- C MODULE: AIRWAY TARGET: NOVICE, BASIC LEVEL TRAINEES & ALL ANAESTHETISTS BACKGROUND: Management of the unexpectedly difficult airway is a core skill for all anaesthetists.
Management of the Obstructed Airway
 G E N E R A L Tutorial 336 Management of the Obstructed Airway Dr Helen Bryant Anaesthetic Registrar, Queen Alexandra Hospital, Portsmouth, UK Dr Bisanth Batuwitage Consultant Anaesthetist, Queen Alexandra
G E N E R A L Tutorial 336 Management of the Obstructed Airway Dr Helen Bryant Anaesthetic Registrar, Queen Alexandra Hospital, Portsmouth, UK Dr Bisanth Batuwitage Consultant Anaesthetist, Queen Alexandra
CAN T INTUBATE, CAN T VENTILATE: PLAN A- D
 CAN T INTUBATE, CAN T VENTILATE: PLAN A- D MODULE: AIRWAY TARGET: BASIC LEVEL TRAINEES & ALL ANAESTHETISTS BACKGROUND: Management of the Can t Intubate, Can t Ventilate situation is a core skill for all
CAN T INTUBATE, CAN T VENTILATE: PLAN A- D MODULE: AIRWAY TARGET: BASIC LEVEL TRAINEES & ALL ANAESTHETISTS BACKGROUND: Management of the Can t Intubate, Can t Ventilate situation is a core skill for all
Translaryngeal Tracheostomy - TLT Fantoni Method
 Translaryngeal Tracheostomy - TLT Fantoni Method Fantoni A., Ripamonti D., Lesmo A. About the Authors Fantoni Antonio Chief Emeritus of Department of Anaesthesia and Intensive Care - San Carlo Borromeo
Translaryngeal Tracheostomy - TLT Fantoni Method Fantoni A., Ripamonti D., Lesmo A. About the Authors Fantoni Antonio Chief Emeritus of Department of Anaesthesia and Intensive Care - San Carlo Borromeo
Translaryngeal tracheostomy
 Translaryngeal tracheostomy Issued: August 2013 NICE interventional procedure guidance 462 guidance.nice.org.uk/ipg462 NICE has accredited the process used by the NICE Interventional Procedures Programme
Translaryngeal tracheostomy Issued: August 2013 NICE interventional procedure guidance 462 guidance.nice.org.uk/ipg462 NICE has accredited the process used by the NICE Interventional Procedures Programme
THE DIFFICULT PEDIATRIC AIRWAY. Learning Objectives. The Pediatric Airway 6/7/18. Jason W. Gatling, MD Department of Anesthesiology June 7, 2018
 THE DIFFICULT PEDIATRIC AIRWAY Jason W. Gatling, MD Department of Anesthesiology June 7, 2018 Learning Objectives At the conclusion of this activity, the participants should be able to: 1. Describe what
THE DIFFICULT PEDIATRIC AIRWAY Jason W. Gatling, MD Department of Anesthesiology June 7, 2018 Learning Objectives At the conclusion of this activity, the participants should be able to: 1. Describe what
All bedside percutaneously placed tracheostomies
 Page 1 of 5 Scope: All bedside percutaneously placed tracheostomies Population: All ICU personnel Outcomes: To standardize and outline the steps necessary to safely perform a percutaneous tracheostomy
Page 1 of 5 Scope: All bedside percutaneously placed tracheostomies Population: All ICU personnel Outcomes: To standardize and outline the steps necessary to safely perform a percutaneous tracheostomy
Pediatric upper airway and congenital anomalies
 Anesthesiology Clin N Am 20 (2002) 747 766 Pediatric upper airway and congenital anomalies Andrew Infosino, MD Department of Anesthesia and Perioperative Care, University of California at San Francisco,
Anesthesiology Clin N Am 20 (2002) 747 766 Pediatric upper airway and congenital anomalies Andrew Infosino, MD Department of Anesthesia and Perioperative Care, University of California at San Francisco,
The use of metallic expandable tracheal stents in the management of inoperable malignant tracheal obstruction
 The use of metallic expandable tracheal stents in the management of inoperable malignant tracheal obstruction Alaa Gaafar-MD, Ahmed Youssef-MD, Mohamed Elhadidi-MD A l e x a n d r i a F a c u l t y o f
The use of metallic expandable tracheal stents in the management of inoperable malignant tracheal obstruction Alaa Gaafar-MD, Ahmed Youssef-MD, Mohamed Elhadidi-MD A l e x a n d r i a F a c u l t y o f
Airway complications on the general medical unit after prolonged ICU admission
 Airway complications on the general medical unit after prolonged ICU admission Palash Kar Discipline of Acute Care Medicine, University of Adelaide Intensive Care Unit, Royal Adelaide Hospital, Adelaide,
Airway complications on the general medical unit after prolonged ICU admission Palash Kar Discipline of Acute Care Medicine, University of Adelaide Intensive Care Unit, Royal Adelaide Hospital, Adelaide,
How to Predict and Avoid Airway Disasters. Muhammad Umer Ihsan
 How to Predict and Avoid Airway Disasters Muhammad Umer Ihsan Four Key Aspect of Assessing a Difficult Airway Difficult Bag Mask Ventilation Difficult Direct Laryngoscopy Difficult Extra-glottic devices
How to Predict and Avoid Airway Disasters Muhammad Umer Ihsan Four Key Aspect of Assessing a Difficult Airway Difficult Bag Mask Ventilation Difficult Direct Laryngoscopy Difficult Extra-glottic devices
Sedation explained. Information for patients. First Edition
 Sedation explained Information for patients First Edition 2018 www.rcoa.ac.uk/patientinfo This leaflet explains what sedation is, how it works and when you may need it. It also explains the benefits and
Sedation explained Information for patients First Edition 2018 www.rcoa.ac.uk/patientinfo This leaflet explains what sedation is, how it works and when you may need it. It also explains the benefits and
Care of the Deteriorating Patient in Recovery NADIA TICEHURST : CLINICAL NURSE EDUCATOR PERI ANAESTHETICS BENDIGO HEALTH
 Care of the Deteriorating Patient in Recovery NADIA TICEHURST : CLINICAL NURSE EDUCATOR PERI ANAESTHETICS BENDIGO HEALTH Intended learning outcomes Describe the components of a comprehensive clinician
Care of the Deteriorating Patient in Recovery NADIA TICEHURST : CLINICAL NURSE EDUCATOR PERI ANAESTHETICS BENDIGO HEALTH Intended learning outcomes Describe the components of a comprehensive clinician
L.J. Hoeve and R.H.M. van Poppelen * (Received 12 July 1989) (Accepted 10 August 1989)
 (Accepted 10 August 1989)") International Journal of Pediatric Otorhinolaryngolo~. 18 (1990) 241-245 Elsevier 241 PEDOT 00617 Fiberoptic laryngoscopy under in neonates general anesthesia L.J. Hoeve and R.H.M. van Poppelen * Lkpar?ments
International Journal of Pediatric Otorhinolaryngolo~. 18 (1990) 241-245 Elsevier 241 PEDOT 00617 Fiberoptic laryngoscopy under in neonates general anesthesia L.J. Hoeve and R.H.M. van Poppelen * Lkpar?ments
-Discussed in the Ebers Papyrus and the Rig Veda BC
 Tracheotomy History -Discussed in the Ebers Papyrus and the Rig Veda -1500 BC History -Treatment obstructive diseases (Antyllus, 2 nd century AD) -Discussed in the writings of Braassarolo (1546) -Considered
Tracheotomy History -Discussed in the Ebers Papyrus and the Rig Veda -1500 BC History -Treatment obstructive diseases (Antyllus, 2 nd century AD) -Discussed in the writings of Braassarolo (1546) -Considered
Case Report Laryngeal Radiation Fibrosis: A Case of Failed Awake Flexible Fibreoptic Intubation
 Case Reports in Anesthesiology Volume 2011, Article ID 878910, 4 pages doi:10.1155/2011/878910 Case Report Laryngeal Radiation Fibrosis: A Case of Failed Awake Flexible Fibreoptic Intubation Johannes M.
Case Reports in Anesthesiology Volume 2011, Article ID 878910, 4 pages doi:10.1155/2011/878910 Case Report Laryngeal Radiation Fibrosis: A Case of Failed Awake Flexible Fibreoptic Intubation Johannes M.
1.0 Abstract. Title. Keywords. Sevoflurane. Anaesthesia. Difficult to intubate (DTI) Rationale and Background
 Rationale and Background") 1.0 Abstract Title A prospective, open-label, multicenter, post marketing, observational study to investigate the effectiveness of Sevoflurane anaesthesia in difficult-to-intubate Egyptian patients. Keywords
1.0 Abstract Title A prospective, open-label, multicenter, post marketing, observational study to investigate the effectiveness of Sevoflurane anaesthesia in difficult-to-intubate Egyptian patients. Keywords
Postoperative management of the difficult airway
 BJA Education, 17 (7): 235 241 (2017) doi: 10.1093/bjaed/mkw077 Advance Access Publication Date: 15 February 2017 Matrix reference 1C01, 2A01, 3A01 Postoperative management of the difficult airway B Batuwitage
BJA Education, 17 (7): 235 241 (2017) doi: 10.1093/bjaed/mkw077 Advance Access Publication Date: 15 February 2017 Matrix reference 1C01, 2A01, 3A01 Postoperative management of the difficult airway B Batuwitage
Airway Workshop Lecture. University of Ottawa
 Airway Workshop Lecture Department of Anesthesiology University of Ottawa Overview Ventilation Airway assessment Difficult airways Airway management equipment aids Intubation/Improving Intubation Success
Airway Workshop Lecture Department of Anesthesiology University of Ottawa Overview Ventilation Airway assessment Difficult airways Airway management equipment aids Intubation/Improving Intubation Success
Perioperative Care in OSA Surgery
 Perioperative Care in OSA Surgery Overview Estimate of Major Peri-Op Complications Risk Factors for Airway Complications Peri-Operative Planning Avoidance of Complications Andrew N. Goldberg, MD, MSCE
Perioperative Care in OSA Surgery Overview Estimate of Major Peri-Op Complications Risk Factors for Airway Complications Peri-Operative Planning Avoidance of Complications Andrew N. Goldberg, MD, MSCE
Can't Intubate, Can't oxygenate (CICO) The new terminology What is the Military Experience What is the Civilian Experience What is your role.
 The new terminology What is the Military Experience What is the Civilian Experience What is your role.") Disclaimer The views in the presentation are the author's, and do not reflect the views of the Department of Defence I am a full time Australian Defence Force Procedural Specialist (Anaesthetist) Can't
Disclaimer The views in the presentation are the author's, and do not reflect the views of the Department of Defence I am a full time Australian Defence Force Procedural Specialist (Anaesthetist) Can't
Question: Is this patient an infant? A patient less than 12 months old is considered an infant. Please check the box next to the appropriate choice.
 Question: Date of Intubation (Month, Day, Year): Question: Date of Data Entry This should be within 4 weeks to the day of intubation: Question: Is this patient an infant? A patient less than 12 months
Question: Date of Intubation (Month, Day, Year): Question: Date of Data Entry This should be within 4 weeks to the day of intubation: Question: Is this patient an infant? A patient less than 12 months
Airway management problem occurring in the Emergency Department
 NAP4EM Airway management problem occurring in the Emergency Department Inclusion criteria 1. Please indicate the inclusion criteria by selecting one or more from the list below: Death Brain damage Emergency
NAP4EM Airway management problem occurring in the Emergency Department Inclusion criteria 1. Please indicate the inclusion criteria by selecting one or more from the list below: Death Brain damage Emergency
TRACHEOSTOMY. Tracheostomy means creation an artificial opening in the trachea with tracheostomy tube insertion
 TRACHEOSTOMY Definition Tracheostomy means creation an artificial opening in the trachea with tracheostomy tube insertion Indications for tracheostomy 1-upper airway obstruction with stridor, air hunger,
TRACHEOSTOMY Definition Tracheostomy means creation an artificial opening in the trachea with tracheostomy tube insertion Indications for tracheostomy 1-upper airway obstruction with stridor, air hunger,
OPEN ACCESS ATLAS OF OTOLARYNGOLOGY, HEAD & NECK OPERATIVE SURGERY
 OPEN ACCESS ATLAS OF OTOLARYNGOLOGY, HEAD & NECK OPERATIVE SURGERY LARYNGOMALACIA Laryngomalacia is characterised by collapse of the supraglottic tissues on inspiration, and is the most common cause of
OPEN ACCESS ATLAS OF OTOLARYNGOLOGY, HEAD & NECK OPERATIVE SURGERY LARYNGOMALACIA Laryngomalacia is characterised by collapse of the supraglottic tissues on inspiration, and is the most common cause of
Airway/Breathing. Chapter 5
 Airway/Breathing Chapter 5 Airway/Breathing Introduction Rapid assessment and management of airway and ventilation are critical to preventing morbidity and mortality. Airway compromise can occur rapidly
Airway/Breathing Chapter 5 Airway/Breathing Introduction Rapid assessment and management of airway and ventilation are critical to preventing morbidity and mortality. Airway compromise can occur rapidly
Tracheostomy. Information for patients and relatives
 Tracheostomy Information for patients and relatives page 2 What is a tracheostomy? A tracheostomy is a small hole (stoma) made at the front of the neck, which goes into the trachea (windpipe). A tube called
Tracheostomy Information for patients and relatives page 2 What is a tracheostomy? A tracheostomy is a small hole (stoma) made at the front of the neck, which goes into the trachea (windpipe). A tube called
CASE PRIMERS. Pediatric Anesthesia Fellowship Program. Laryngotracheal Reconstruction (LTR) Tufts Medical Center
 Tufts Medical Center") CASE PRIMERS Pediatric Anesthesia Fellowship Program Tufts Medical Center Department of Anesthesiology and Perioperative Medicine Division of Pediatric Anesthesia 800 Washington Street, Box 298 Boston,
CASE PRIMERS Pediatric Anesthesia Fellowship Program Tufts Medical Center Department of Anesthesiology and Perioperative Medicine Division of Pediatric Anesthesia 800 Washington Street, Box 298 Boston,
RAPID SEQUENCE INTUBATION FOR THE RURAL DOC
 Society of Rural Physicians of Canada 26TH ANNUAL RURAL AND REMOTE MEDICINE COURSE ST. JOHN'S NEWFOUNDLAND AND LABRADOR APRIL 12-14, 2018 Dr. Braam de Klerk VICTORIA BC 240 RAPID SEQUENCE INTUBATION FOR
Society of Rural Physicians of Canada 26TH ANNUAL RURAL AND REMOTE MEDICINE COURSE ST. JOHN'S NEWFOUNDLAND AND LABRADOR APRIL 12-14, 2018 Dr. Braam de Klerk VICTORIA BC 240 RAPID SEQUENCE INTUBATION FOR
Enhanced Sedation for GI Endoscopy
 Enhanced Sedation for GI Endoscopy Department of Anaesthesia and The Digestive Diseases Centre Please read this booklet carefully, as it contains important instructions for you to follow before you come
Enhanced Sedation for GI Endoscopy Department of Anaesthesia and The Digestive Diseases Centre Please read this booklet carefully, as it contains important instructions for you to follow before you come
Procedure No: Procedure Approved for Use By: WCCSS Divisional Quality Meeting. Date: May 2017
 Standard Operating Procedure (SOP): Standard operating procedure for Neonatal Difficult Airway Kit and Intubation Pathway Procedure No: 1 Document replaced: Version 1 Version: 2.0 Procedure Written By:
Standard Operating Procedure (SOP): Standard operating procedure for Neonatal Difficult Airway Kit and Intubation Pathway Procedure No: 1 Document replaced: Version 1 Version: 2.0 Procedure Written By:
Management of Pediatric Tracheostomy
 Management of Pediatric Tracheostomy Deepak Mehta Associate Professor Of Otolaryngology Director Pediatric Aerodigestive Center Definitions Tracheotomy: The making of an incision in the trachea The name
Management of Pediatric Tracheostomy Deepak Mehta Associate Professor Of Otolaryngology Director Pediatric Aerodigestive Center Definitions Tracheotomy: The making of an incision in the trachea The name
Society of Rural Physicians of Canada 26TH ANNUAL RURAL AND REMOTE MEDICINE COURSE ST. JOHN'S NEWFOUNDLAND AND LABRADOR APRIL 12-14, 2018
 Society of Rural Physicians of Canada 26TH ANNUAL RURAL AND REMOTE MEDICINE COURSE ST. JOHN'S NEWFOUNDLAND AND LABRADOR APRIL 12-14, 2018 Dr. Andrea Losier OTTAWA ON 332 PEDS ER CASES Pediatric ED Cases
Society of Rural Physicians of Canada 26TH ANNUAL RURAL AND REMOTE MEDICINE COURSE ST. JOHN'S NEWFOUNDLAND AND LABRADOR APRIL 12-14, 2018 Dr. Andrea Losier OTTAWA ON 332 PEDS ER CASES Pediatric ED Cases
AIRWAY MANAGEMENT SUZANNE BROWN, CRNA
 AIRWAY MANAGEMENT SUZANNE BROWN, CRNA OBJECTIVE OF LECTURE Non Anesthesia Sedation Providers Review for CRNA s Informal Questions encouraged 2 AIRWAY MANAGEMENT AWARENESS BASICS OF ANATOMY EQUIPMENT 3
AIRWAY MANAGEMENT SUZANNE BROWN, CRNA OBJECTIVE OF LECTURE Non Anesthesia Sedation Providers Review for CRNA s Informal Questions encouraged 2 AIRWAY MANAGEMENT AWARENESS BASICS OF ANATOMY EQUIPMENT 3
TRACHEOSTOMY EMERGENCIES
 TRACHEOSTOMY EMERGENCIES MODULE: AIRWAY TARGET: ALL ANAESTHETISTS, INTENSIVISTS, ED & ACUTE PHYSICIANS, FOUNDATION DOCTORS BACKGROUND: Around 16% of ICU patients may have a tracheostomy. Life- threatening
TRACHEOSTOMY EMERGENCIES MODULE: AIRWAY TARGET: ALL ANAESTHETISTS, INTENSIVISTS, ED & ACUTE PHYSICIANS, FOUNDATION DOCTORS BACKGROUND: Around 16% of ICU patients may have a tracheostomy. Life- threatening
Patient information. You and Your Anaesthetic Information to help you prepare for anaesthetic. Anaesthesia Directorate PIF 344/ V5
 Patient information You and Your Anaesthetic Information to help you prepare for anaesthetic Anaesthesia Directorate PIF 344/ V5 Types of anaesthesia Anaesthesia stops you feeling pain and other sensations.
Patient information You and Your Anaesthetic Information to help you prepare for anaesthetic Anaesthesia Directorate PIF 344/ V5 Types of anaesthesia Anaesthesia stops you feeling pain and other sensations.
Advanced Airway Management PRESENTED BY: JOSIAH POIRIER RN, JOHN GRUBER FP-C
 Advanced Airway Management PRESENTED BY: JOSIAH POIRIER RN, JOHN GRUBER FP-C Advanced Airway Objectives Advanced airway management is a relatively low frequency, high risk intervention. The following education
Advanced Airway Management PRESENTED BY: JOSIAH POIRIER RN, JOHN GRUBER FP-C Advanced Airway Objectives Advanced airway management is a relatively low frequency, high risk intervention. The following education
Airway Management and Ventilation. Eric V. Ernest, M.D., EMT-P Department of Emergency Medicine University of Nebraska Medical Center
 Airway Management and Ventilation Eric V. Ernest, M.D., EMT-P Department of Emergency Medicine University of Nebraska Medical Center Airway/Ventilation Overview Respiratory Assessment Supplemental Oxygen
Airway Management and Ventilation Eric V. Ernest, M.D., EMT-P Department of Emergency Medicine University of Nebraska Medical Center Airway/Ventilation Overview Respiratory Assessment Supplemental Oxygen
Difficult Airway. Department of Anesthesiology University of Colorado Health Sciences Center (prepared by Brenda A. Bucklin, M.D.)
") Difficult Airway Department of Anesthesiology University of Colorado Health Sciences Center (prepared by Brenda A. Bucklin, M.D.) Objectives Definition & incidence of the difficult airway Evaluation of
Difficult Airway Department of Anesthesiology University of Colorado Health Sciences Center (prepared by Brenda A. Bucklin, M.D.) Objectives Definition & incidence of the difficult airway Evaluation of
The Dif fi cult Airway
 The Difficult Airway David B. Glick, MD, MBA Richard M. Cooper, B.Sc, M.Sc, MD, FRCPC Andranik Ovassapian, MD Editors The Difficult Airway An Atlas of Tools and Techniques for Clinical Management Editors
The Difficult Airway David B. Glick, MD, MBA Richard M. Cooper, B.Sc, M.Sc, MD, FRCPC Andranik Ovassapian, MD Editors The Difficult Airway An Atlas of Tools and Techniques for Clinical Management Editors
Comparison of the Berman Intubating Airway and the Williams Airway Intubator for fibreoptic orotracheal intubation in anaesthetised patients.
 Title Comparison of the Berman Intubating Airway and the Williams Airway Intubator for fibreoptic orotracheal intubation in anaesthetised patients Author(s) Greenland, KB; Ha, ID; Irwin, MG Citation Anaesthesia,
Title Comparison of the Berman Intubating Airway and the Williams Airway Intubator for fibreoptic orotracheal intubation in anaesthetised patients Author(s) Greenland, KB; Ha, ID; Irwin, MG Citation Anaesthesia,