Sepsis. Reliability- can we achieve Dr Ron Daniels
|
|
|
- Alisha Hawkins
- 5 years ago
- Views:
Transcription




1 Sepsis. Reliability- can we achieve Dr Ron Daniels Chief Executive, Global Sepsis Alliance Fellow: NHS Improvement Faculty Chief Executive: United Kingdom Sepsis Trust & Chair, UK SSC RRAILS llandrindod Wells, 18 th July 2013
2

3 A U.K. Perspective
4 A U.K. Perspective North Stand
5 A U.K. Perspective Breast cancer
6 A U.K. Perspective Breast cancer
7 A U.K. Perspective Breast cancer
8 A U.K. Perspective
9 Sepsis is on the up.. CDC National Center of Hospital Statistics
10 Why do we need to change?
11
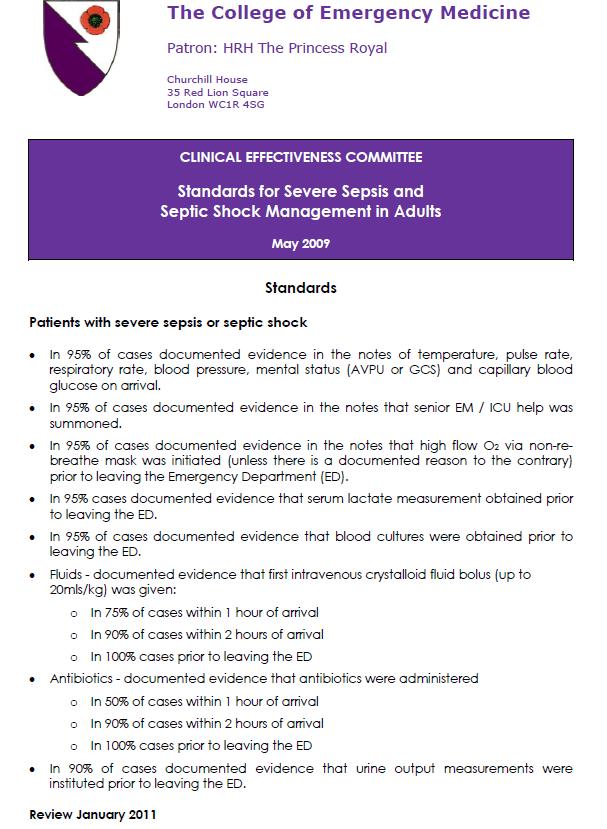
12 Severe Sepsis Bundle 2008 Serum lactate measured Blood cultures obtained prior to antibiotic administration From the time of presentation, broad-spectrum antibiotics to be given within 1 hour Control infective source In the event of hypotension and/or lactate >4mmol/L (36mg/dl): Deliver an initial minimum of 20 ml/kg of crystalloid (or colloid equivalent) Give vasopressors for hypotension not responding to initial fluid resuscitation to maintain mean arterial pressure (MAP) > 65 mm Hg. In the event of persistent arterial hypotension despite volume resuscitation (septic shock) and/or initial lactate >4 mmol/l (36 mg/dl): Achieve central venous pressure (CVP) of >8 mm Hg Achieve central venous oxygen saturation (ScvO 2 ) >70%
13
14
15 Severe Sepsis Bundle 2012 To be completed within 3 hours: 1) Measure lactate level 2) Obtain blood cultures prior to administration of antibiotics 3) Administer broad spectrum antibiotics 4) Administer 30 ml/kg crystalloid for hypotension or lactate 4mmol/L To be completed within 6 hours: 5) Apply vasopressors for hypotension that does not respond to initial fluid resuscitation to maintain a mean arterial pressure [MAP] 65 mm Hg) 6) In the event of persistent arterial hypotension despite volume resuscitation (septic shock) or initial lactate 4 mmol/l (36 mg/dl): - Measure central venous pressure (CVP)* - Measure central venous oxygen saturation (ScvO2)* 7) Remeasure lactate if initial lactate was elevated*
16 The Sepsis Six 1. Give high-flow oxygen via non-rebreathe bag 2. Take blood cultures and consider source control 3. Give IV antibiotics according to local protocol 4. Start IV fluid resuscitation Hartmann s or equivalent 5. Check lactate 6. Monitor hourly urine output consider catheterisation within one hour..plus Critical Care support to complete EGDT
17 Perspective Severe Sepsis Acute coronary syndrome No. cases per 100,000 per annum NNT basic care Sepsis Six (our data) 4 First hour antibiotics 6 Clopidogrel 48 β-blockade 42 Aspirin 26 NNT invasive care EGDT (Rivers) 6 Resusc Bundle (SSC) 18 Thrombolysis 15 PCI over thrombolysis 33
18
19

20 First hour antibiotics in 27%...
21 Early, appropriate antibiotics are the key to sepsis improvement
22 fraction of total patients Cumulative Initiation of Effective Antimicrobial Therapy and Survival in Septic Shock 1.0 survival fraction cumulative antibiotic initiation time from hypotension onset (hrs) Kumar et al. CCM. 2006:34:
23 Running average survival in septic shock based on antibiotic delay (n=2154) For each hour s delay in administering antibiotics in septic shock, mortality increases by 7.6% Funk and Kumar Critical Care Clinics 2011 (in press)
24 Begin IV antibiotics as early as possible, and always within the first hour of recognising severe sepsis (1D) and septic shock. (1B) Citation: Kumar A et al. Crit Care Med 2006: 34(6) Retrospective, 15 years, 14 sites n = 2,154 median 6 h, 50% administered in 6h Only 5% first 30 minutes- survival 87% 12% first hour- survival 84%
25 Early antibiotics are good... Author n Setting Median time (mins) Odds Ratio for death Gaieski Crit Care Med 2010; 38: Daniels Emerg Med J 2010; doi: Kumar Crit Care Med 2006; 34(6): Appelboam Critical Care 2010; 14(Suppl 1): ED, USA (Shock) 567 Whole hospital, UK 2154 ED, Canada (Shock) 375 Whole hospital, UK (first hour vs all times) (first hour vs all times) (first hour vs second hour) (first 3 hours vs delayed) Levy Crit Care Med 2010; 38 (2): Multi-centre 0.86 (first 3 hours vs delayed)
26 Running average survival in septic shock based on antibiotic delay (n=4195) Cumulative fraction of total survivors Running average survival Funk and Kumar Critical Care Clinics 2012

27 Retrospective, 22 hospitals, n= 4532 Bagshaw SM et al Intensive Care Med. 2009;35(5):871-81
28 Retrospective, 22 hospitals, n= % septic shock patients developed early AKI Bagshaw SM et al Intensive Care Med. 2009;35(5):871-81

29 64.4% septic shock patients developed early AKI Retrospective, 22 hospitals, n= 4532 Median time shock to antibiotic = 5.5 h Bagshaw SM et al Intensive Care Med. 2009;35(5):871-81

 P < 0.")
30 64.4% septic shock patients developed early AKI Median time shock to antibiotic = 5.5 h Retrospective, 22 hospitals, n= 4532 OR for AKI 1.14 ( ) P < per hour s delay Bagshaw SM et al Intensive Care Med. 2009;35(5):871-81
31 How do we know which septic patient is going to get organ failure? We often don t know the source, let alone the bug... We don t adhere to guidelines, and the guidelines aren t much good We re not very good with our timing So...

32 Should we have, for first dose, the Sepsis Antibiotic? Pip/ taz? Meropenem? Co-amoxiclav?
33 How to achieve better sepsis outcomes?
34 2 groups with 2 sets of needs. 1. Get community-acquired sepsis patients to hospital quickly

35
36
37


38

39
40

41
42 2 groups with 2 sets of needs. 2. Recognize in-patient deterioration reliably

43 Inpatient deterioration Critical Care expenditure Critical Care length of stay Compared with ACS Cost per episode

44

45

46 Moore LJ, Jones SL, Kreiner LA, et al: Validation of a screening tool for the early identification of sepsis. J Trauma 2009; 66:
47 2 groups with 1 identical need. 3. Respond and escalate appropriately

48 Sepsis Six delivery
49 Compliance at Good Hope Hospital (%) Sepsis 6 Resusc Both Mortality Apr-09 Jun-09 Aug-09 Oct-09
50 Mortality by Sepsis Six Cohort size (%) Mortality % RRR % (NNT) Total 567 (100) Sepsis Six Sepsis Six 347 (61.2) (38.8) (4.16)
51 2 groups with 1 identical need. 4. Monitor long-term outcomes and rehab needs
52 Long-term cognitive impairment after sepsis Mild Moderate-severe Before sepsis After sepsis Iwashyna et al: Long-term cognitive impairment & functional disability among survivors of severe sepsis. JAMA, 2010.

53 Incidence of PTSD (%) Fire/ natural disasters 4.5 Assault leading to injury 11.5 ITU survivors 22 War 38.8 Rape Davydow DS, Gifford JM, Desai SV, et al.: Post traumatic stress disorder in general intensive care unit survivors: a systematic review. Gen Hosp Psychiatry 2008; 30: ,
54 2 groups with 1 identical need. 5. Get the public message right
55

56
57

58 Healthcare-associated infection Urinary tract Surgical Site Infection Pneumonia Bloodstream infection 17% 18% 43% 22%


59 Sources of sepsis Healthcareassociated 38% Communityacquired 62%

60 Sources of sepsis Pneumonia Intra-abdominal UTI SSTI 7% 10% 25% 58%
61 Infections management is about Prevention of avoidable infection 2. Antimicrobial stewardship 3. Rapid treatment of sepsis and other severe infection
62 Infections management is about...
63

64 World Sepsis Day
65
66
67 What doing sepsis right might mean for us
68 Achieving 80% reliability For each year, for every 100k in the local population.. 20 lives saved 285 fewer bed days 168 fewer CC bed days Direct costs for survivors reduced by 0.25M For Wales, that s 600 lives and 7.5 million. Every year.
69 Summary Sepsis is a medical emergency- and a big killer Awareness and recognition are the key Early antibiotics and fluids will save more lives than Critical Care We need a whole-systems approach The public message around infections management needs to be refined To give equal weight to all important aspects


70 @sepsisuk
MAKING SENSE OF IT ALL AUGUST 17
 MAKING SENSE OF IT ALL AUGUST 17 @SepsisUK Dr Ron Daniels B.E.M. CEO, UK Sepsis Trust CEO, Global Sepsis Alliance Special Adviser to WHO SCALE AND BURDEN @sepsisuk Dr Ron Daniels B.E.M. CEO, UK Sepsis
MAKING SENSE OF IT ALL AUGUST 17 @SepsisUK Dr Ron Daniels B.E.M. CEO, UK Sepsis Trust CEO, Global Sepsis Alliance Special Adviser to WHO SCALE AND BURDEN @sepsisuk Dr Ron Daniels B.E.M. CEO, UK Sepsis
The changing face of
 The changing face of sepsis. @SepsisUK Dr Ron Daniels B.E.M. CEO, UK Sepsis Trust CEO, Global Sepsis Alliance Special Adviser (maternal sepsis) to WHO Breast cancer Cognitive impairment Mild 3.8 7.1
The changing face of sepsis. @SepsisUK Dr Ron Daniels B.E.M. CEO, UK Sepsis Trust CEO, Global Sepsis Alliance Special Adviser (maternal sepsis) to WHO Breast cancer Cognitive impairment Mild 3.8 7.1
Sepsis in primary care. what is good care?
 Sepsis in primary care @SepsisUK what is good care? Emmanuel Nsutebu Consultant Infectious Disease Physician & Clinical lead for sepsis Tropical and Infectious Disease Unit Royal Liverpool Hospital Do
Sepsis in primary care @SepsisUK what is good care? Emmanuel Nsutebu Consultant Infectious Disease Physician & Clinical lead for sepsis Tropical and Infectious Disease Unit Royal Liverpool Hospital Do
Guidelines are the Future of Sepsis Management Pro
 Guidelines are the Future of Sepsis Management Pro R. Phillip Dellinger MD, MCCM Professor and Chair of Medicine Director Adult Health Institute Senior Critical Care Attending Camden NJ USA Objectives
Guidelines are the Future of Sepsis Management Pro R. Phillip Dellinger MD, MCCM Professor and Chair of Medicine Director Adult Health Institute Senior Critical Care Attending Camden NJ USA Objectives
The Septic Patient. Dr Arunraj Navaratnarajah. Renal SpR Imperial College NHS Healthcare Trust
 The Septic Patient Dr Arunraj Navaratnarajah Renal SpR Imperial College NHS Healthcare Trust Objectives of this session Define SIRS / sepsis / severe sepsis / septic shock Early recognition of Sepsis The
The Septic Patient Dr Arunraj Navaratnarajah Renal SpR Imperial College NHS Healthcare Trust Objectives of this session Define SIRS / sepsis / severe sepsis / septic shock Early recognition of Sepsis The
Saving Lives: Focusing on Severe Sepsis and Septic Shock
 Saving Lives: Focusing on Severe Sepsis and Septic Shock Deborah Cameron, RN, CPHQ Paul Pratt, RN Glenn Russ, RN Providence Little Company of Mary Medical Center San Pedro January 18, 2011 Objectives 1.
Saving Lives: Focusing on Severe Sepsis and Septic Shock Deborah Cameron, RN, CPHQ Paul Pratt, RN Glenn Russ, RN Providence Little Company of Mary Medical Center San Pedro January 18, 2011 Objectives 1.
Early Goal Directed Therapy in 2015: What Did the Big Trials Teach us?
 Early Goal Directed Therapy in 2015: What Did the Big Trials Teach us? Mitchell M. Levy MD, FCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care Warren Alpert Medical School
Early Goal Directed Therapy in 2015: What Did the Big Trials Teach us? Mitchell M. Levy MD, FCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care Warren Alpert Medical School
2016 Sepsis Update: Pearls, Pitfalls, and Core Measure Quicksand
 2016 Sepsis Update: Pearls, Pitfalls, and Core Measure Quicksand Jack Perkins, MD FACEP, FAAEM, FACP Assistant Professor of Emergency and Internal Medicine Virginia Tech Carilion School of Medicine Why
2016 Sepsis Update: Pearls, Pitfalls, and Core Measure Quicksand Jack Perkins, MD FACEP, FAAEM, FACP Assistant Professor of Emergency and Internal Medicine Virginia Tech Carilion School of Medicine Why
Early Goal-Directed Therapy
 Early Goal-Directed Therapy Where do we stand? Jean-Daniel Chiche, MD PhD MICU & Dept of Host-Pathogen Interaction Hôpital Cochin & Institut Cochin, Paris-F Resuscitation targets in septic shock 1 The
Early Goal-Directed Therapy Where do we stand? Jean-Daniel Chiche, MD PhD MICU & Dept of Host-Pathogen Interaction Hôpital Cochin & Institut Cochin, Paris-F Resuscitation targets in septic shock 1 The
DELIRIUM IN SEPSIS. Professor Kevin Rooney: National Clinical Lead for Sepsis Alison Hunter: Improvement Advisor, Sepsis Collaborative
 DELIRIUM IN SEPSIS Professor Kevin Rooney: National Clinical Lead for Sepsis Alison Hunter: Improvement Advisor, Sepsis Collaborative What is Sepsis? Diagnostic Criteria for Sepsis: A U.K. Perspective
DELIRIUM IN SEPSIS Professor Kevin Rooney: National Clinical Lead for Sepsis Alison Hunter: Improvement Advisor, Sepsis Collaborative What is Sepsis? Diagnostic Criteria for Sepsis: A U.K. Perspective
Staging Sepsis for the Emergency Department: Physician
 Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
Sepsis: Identification and Management in an Acute Care Setting
 Sepsis: Identification and Management in an Acute Care Setting Dr. Barbara M. Mills DNP Director Rapid Response Team/ Code Resuscitation Stony Brook University Medical Center SEPSIS LECTURE NPA 2018 OBJECTIVES
Sepsis: Identification and Management in an Acute Care Setting Dr. Barbara M. Mills DNP Director Rapid Response Team/ Code Resuscitation Stony Brook University Medical Center SEPSIS LECTURE NPA 2018 OBJECTIVES
Sepsis Management Update 2014
 Sepsis Management Update 2014 Laura J. Moore, MD, FACS Associate Professor, Department of Surgery The University of Texas Health Science Center, Houston Medical Director, Shock Trauma ICU Texas Trauma
Sepsis Management Update 2014 Laura J. Moore, MD, FACS Associate Professor, Department of Surgery The University of Texas Health Science Center, Houston Medical Director, Shock Trauma ICU Texas Trauma
Sepsis - A Year in Transition
 Sepsis - A Year in Transition Todd L. Allen, MD, FACEP Chair, Emergency Department Development Team; Assistant Quality Officer, Institute for Healthcare Leadership Russell R. Miller, III, MD, MPH, FCCM
Sepsis - A Year in Transition Todd L. Allen, MD, FACEP Chair, Emergency Department Development Team; Assistant Quality Officer, Institute for Healthcare Leadership Russell R. Miller, III, MD, MPH, FCCM
Updates On Sepsis Updates based on 2016 updates on sepsis from The International Surviving Sepsis Campaign
 Updates On Sepsis Updates based on 2016 updates on sepsis from The International Surviving Sepsis Campaign Dr. Joseph K Erbe, DO Medical Director Hospitalist Division of Medicine Objectives 1. Review the
Updates On Sepsis Updates based on 2016 updates on sepsis from The International Surviving Sepsis Campaign Dr. Joseph K Erbe, DO Medical Director Hospitalist Division of Medicine Objectives 1. Review the
Sepsis Early Recognition and Management. Therese Hughes, PhD, MPA, RN
 Sepsis Early Recognition and Management Therese Hughes, PhD, MPA, RN 1 Sepsis a Deadly Progression Affects millions around the world each year, killing one in four Contributes to approximately 50% of all
Sepsis Early Recognition and Management Therese Hughes, PhD, MPA, RN 1 Sepsis a Deadly Progression Affects millions around the world each year, killing one in four Contributes to approximately 50% of all
Sepsis! Dr Eric Van Den Bergh Consultant in Emergency Medicine 2015
 Sepsis! Dr Eric Van Den Bergh Consultant in Emergency Medicine 2015 Annual UK Mortality Sepsis Stroke Heart attack COPD Lung cancer COPD Heart attack Stroke Sepsis Lung cancer 0 10000 20000 30000 40000
Sepsis! Dr Eric Van Den Bergh Consultant in Emergency Medicine 2015 Annual UK Mortality Sepsis Stroke Heart attack COPD Lung cancer COPD Heart attack Stroke Sepsis Lung cancer 0 10000 20000 30000 40000
6/5/2014. Sepsis Management and Hemodynamics. 2004: International group of experts,
 Sepsis Management and Hemodynamics Javier Perez-Fernandez, M.D., F.C.C.P. Medical Director Critical Care Services, Baptist t Hospital of Miamii Medical Director Pulmonary Services, West Kendall Baptist
Sepsis Management and Hemodynamics Javier Perez-Fernandez, M.D., F.C.C.P. Medical Director Critical Care Services, Baptist t Hospital of Miamii Medical Director Pulmonary Services, West Kendall Baptist
Nothing to disclose 9/25/2017
 Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Nothing to disclose 1 Explain
Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Nothing to disclose 1 Explain
9/25/2017. Nothing to disclose
 Nothing to disclose Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Explain
Nothing to disclose Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Explain
Septic Shock. Rontgene M. Solante, MD, FPCP,FPSMID
 Septic Shock Rontgene M. Solante, MD, FPCP,FPSMID Learning Objectives Identify situations wherein high or low BP are hemodynamically significant Recognize complications arising from BP emergencies Manage
Septic Shock Rontgene M. Solante, MD, FPCP,FPSMID Learning Objectives Identify situations wherein high or low BP are hemodynamically significant Recognize complications arising from BP emergencies Manage
Fluid Resuscitation and Monitoring in Sepsis. Deepa Gotur, MD, FCCP Anne Rain T. Brown, PharmD, BCPS
 Fluid Resuscitation and Monitoring in Sepsis Deepa Gotur, MD, FCCP Anne Rain T. Brown, PharmD, BCPS Learning Objectives Compare and contrast fluid resuscitation strategies in septic shock Discuss available
Fluid Resuscitation and Monitoring in Sepsis Deepa Gotur, MD, FCCP Anne Rain T. Brown, PharmD, BCPS Learning Objectives Compare and contrast fluid resuscitation strategies in septic shock Discuss available
Evidence-Based. Management of Severe Sepsis. What is the BP Target?
 Evidence-Based Management of Severe Sepsis Michael A. Gropper, MD, PhD Professor and Vice Chair of Anesthesia Director, Critical Care Medicine Chair, Quality Improvment University of California San Francisco
Evidence-Based Management of Severe Sepsis Michael A. Gropper, MD, PhD Professor and Vice Chair of Anesthesia Director, Critical Care Medicine Chair, Quality Improvment University of California San Francisco
Initial Resuscitation of Sepsis & Septic Shock
 Initial Resuscitation of Sepsis & Septic Shock Dr. Fatema Ahmed MD (Critical Care Medicine) FCPS (Medicine) Associate professor Dept. of Critical Care Medicine BIRDEM General Hospital Is Sepsis a known
Initial Resuscitation of Sepsis & Septic Shock Dr. Fatema Ahmed MD (Critical Care Medicine) FCPS (Medicine) Associate professor Dept. of Critical Care Medicine BIRDEM General Hospital Is Sepsis a known
Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016
 Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016 Mitchell M. Levy MD, MCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care
Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016 Mitchell M. Levy MD, MCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care
DESIGNER RESUSCITATION: TITRATING TO TISSUE NEEDS
 DESIGNER RESUSCITATION: TITRATING TO TISSUE NEEDS R. Phillip Dellinger MD, MSc, MCCM Professor and Chair of Medicine Cooper Medical School of Rowan University Chief of Medicine Cooper University Hospital
DESIGNER RESUSCITATION: TITRATING TO TISSUE NEEDS R. Phillip Dellinger MD, MSc, MCCM Professor and Chair of Medicine Cooper Medical School of Rowan University Chief of Medicine Cooper University Hospital
Inflammatory Statements
 Inflammatory Statements Using ETCO 2 Analysis in Sepsis Syndromes George A. Ralls M.D. Orange County EMS System Sepsis Sepsis Over 750,000 cases annually Expected growth of 1.5% per year Over 215,000 deaths
Inflammatory Statements Using ETCO 2 Analysis in Sepsis Syndromes George A. Ralls M.D. Orange County EMS System Sepsis Sepsis Over 750,000 cases annually Expected growth of 1.5% per year Over 215,000 deaths
BREAK 11:10-11:
 1. Sepsis Tom Heaps 09:30-10:20 2. Oncological Emergencies Clare Pollard 10:20-11:10 ------------------------ BREAK 11:10-11:30 ------------------------ 3. Diabetic Ketoacidosis Tom Heaps 11:30-12:20 4.
1. Sepsis Tom Heaps 09:30-10:20 2. Oncological Emergencies Clare Pollard 10:20-11:10 ------------------------ BREAK 11:10-11:30 ------------------------ 3. Diabetic Ketoacidosis Tom Heaps 11:30-12:20 4.
Understand the scope of sepsis morbidity and mortality Identify risk factors that predispose a patient to development of sepsis Define and know the
 Understand the scope of sepsis morbidity and mortality Identify risk factors that predispose a patient to development of sepsis Define and know the differences between sepsis, severe sepsis and septic
Understand the scope of sepsis morbidity and mortality Identify risk factors that predispose a patient to development of sepsis Define and know the differences between sepsis, severe sepsis and septic
Sepsis Story At Intermountain Healthcare Intensive Medicine Clinical Program
 Sepsis Story At Intermountain Healthcare 2004-2012 Intensive Medicine Clinical Program The International Surviving Sepsis Campaign Was Organized In 2002 During The ESICM International Meeting In Barcelona,
Sepsis Story At Intermountain Healthcare 2004-2012 Intensive Medicine Clinical Program The International Surviving Sepsis Campaign Was Organized In 2002 During The ESICM International Meeting In Barcelona,
Core Measures SEPSIS UPDATES
 Patricia Walker, RN-BC, BSN Evidence Based Practice Manager Quality Management Services UCLA Health System, Ronald Reagan Medical Center Core Measures SEPSIS UPDATES Severe Sepsis and Septic Shock Based
Patricia Walker, RN-BC, BSN Evidence Based Practice Manager Quality Management Services UCLA Health System, Ronald Reagan Medical Center Core Measures SEPSIS UPDATES Severe Sepsis and Septic Shock Based
Sepsis Bundle Project (SEP) Kathy Wonderly RN, MSEd, CPHQ Consultant Developed: April 2015 Most recent Revision: December 2018
 Kathy Wonderly RN, MSEd, CPHQ Consultant Developed: April 2015 Most recent Revision: December 2018") Sepsis Bundle Project (SEP) Kathy Wonderly RN, MSEd, CPHQ Consultant Developed: April 2015 Most recent Revision: December 2018 Objectives 1. To identify the symptom of severe sepsis and septic shock syndrome.
Sepsis Bundle Project (SEP) Kathy Wonderly RN, MSEd, CPHQ Consultant Developed: April 2015 Most recent Revision: December 2018 Objectives 1. To identify the symptom of severe sepsis and septic shock syndrome.
Sepsis Management: Past, Present, and Future
 Sepsis Management: Past, Present, and Future Benjamin Ferrell, MD Tennessee ACP Meeting October 28, 2017 Learning Objectives Identify the most updated definition and clinical criteria for sepsis Describe
Sepsis Management: Past, Present, and Future Benjamin Ferrell, MD Tennessee ACP Meeting October 28, 2017 Learning Objectives Identify the most updated definition and clinical criteria for sepsis Describe
Sepsis 3 & Early Identification. Disclosures. Objectives 9/19/2016. David Carlbom, MD Medical Director, HMC Sepsis Program
 Sepsis 3 & Early Identification David Carlbom, MD Medical Director, HMC Sepsis Program Disclosures I have no relevant financial relationships with a commercial interest and will not discuss off-label use
Sepsis 3 & Early Identification David Carlbom, MD Medical Director, HMC Sepsis Program Disclosures I have no relevant financial relationships with a commercial interest and will not discuss off-label use
SEPSIS UPDATE WHY DO WE NEED A CORE MEASURE CHAD M. KOVALA DO, FACOEP, FACEP
 SEPSIS UPDATE WHY DO WE NEED A CORE MEASURE CHAD M. KOVALA DO, FACOEP, FACEP OBJECTIVES Arise, ProMISE, ProCESS Key points in sepsis management The CMS sepsis core measure COST OF SEPSIS CARE IN US Most
SEPSIS UPDATE WHY DO WE NEED A CORE MEASURE CHAD M. KOVALA DO, FACOEP, FACEP OBJECTIVES Arise, ProMISE, ProCESS Key points in sepsis management The CMS sepsis core measure COST OF SEPSIS CARE IN US Most
No conflicts of interest to disclose
 No conflicts of interest to disclose Introduction Epidemiology Surviving sepsis guidelines 2012 Updates Resuscitation protocols Map Goals Transfusion Sepsis-3 Bundle Management Questions Sepsis is a systemic,
No conflicts of interest to disclose Introduction Epidemiology Surviving sepsis guidelines 2012 Updates Resuscitation protocols Map Goals Transfusion Sepsis-3 Bundle Management Questions Sepsis is a systemic,
Sepsis Care and the New Core Measures. Daniel S. Hagg, MD January 15, 2016
 Sepsis Care and the New Core Measures Daniel S. Hagg, MD January 15, 2016 Outline What is sepsis? A brief history of sepsis care How should we take care of septic patients now? Core measures What strategies
Sepsis Care and the New Core Measures Daniel S. Hagg, MD January 15, 2016 Outline What is sepsis? A brief history of sepsis care How should we take care of septic patients now? Core measures What strategies
Early-goal-directed therapy and protocolised treatment in septic shock
 CAT reviews Early-goal-directed therapy and protocolised treatment in septic shock Journal of the Intensive Care Society 2015, Vol. 16(2) 164 168! The Intensive Care Society 2014 Reprints and permissions:
CAT reviews Early-goal-directed therapy and protocolised treatment in septic shock Journal of the Intensive Care Society 2015, Vol. 16(2) 164 168! The Intensive Care Society 2014 Reprints and permissions:
Objectives. Management of Septic Shock. Definitions Progression of sepsis. Epidemiology of severe sepsis. Major goals of therapy
 Objectives Management of Septic Shock Review of the Evidence and Implementation of Pediatric Guidelines at Christus Santa Rosa Manish Desai, M.D. PL 5 2 nd year Pediatric Critical Care Fellow Review of
Objectives Management of Septic Shock Review of the Evidence and Implementation of Pediatric Guidelines at Christus Santa Rosa Manish Desai, M.D. PL 5 2 nd year Pediatric Critical Care Fellow Review of
SURVIVING SEPSIS: Early Management Saves Lives
 SURVIVING SEPSIS: Early Management Saves Lives Pat Posa RN, BSN, MSA System Performance Improvement Leader St. Joseph Mercy Health System Ann Arbor, MI Patricia.posa@stjoeshealth.org Objectives a. Understand
SURVIVING SEPSIS: Early Management Saves Lives Pat Posa RN, BSN, MSA System Performance Improvement Leader St. Joseph Mercy Health System Ann Arbor, MI Patricia.posa@stjoeshealth.org Objectives a. Understand
Sepsis care and the new core measures
 Sepsis care and the new core measures Daniel S. Hagg, MD January 15, 2016 Outline What is sepsis? A brief history of sepsis care How should we take care of septic patients now? Core measures What strategies
Sepsis care and the new core measures Daniel S. Hagg, MD January 15, 2016 Outline What is sepsis? A brief history of sepsis care How should we take care of septic patients now? Core measures What strategies
BC Sepsis Network Emergency Department Sepsis Guidelines
 The provincial Sepsis Clinical Expert Group developed the BC, taking into account the most up-to-date literature (references below) and expert opinion. For more information about the guidelines, and to
The provincial Sepsis Clinical Expert Group developed the BC, taking into account the most up-to-date literature (references below) and expert opinion. For more information about the guidelines, and to
SIRS, NICE, SOFAs and CQUINs: Challenges of changing definitions and guidelines. Dr Sian Coggle Consultant Acute Medicine and Infectious Diseases
 SIRS, NICE, SOFAs and CQUINs: Challenges of changing definitions and guidelines Dr Sian Coggle Consultant Acute Medicine and Infectious Diseases Objectives Context Case Changing definitions Systems for
SIRS, NICE, SOFAs and CQUINs: Challenges of changing definitions and guidelines Dr Sian Coggle Consultant Acute Medicine and Infectious Diseases Objectives Context Case Changing definitions Systems for
The Ever Changing World of Sepsis Management. Laura Evans MD MSc Medical Director of Critical Care Bellevue Hospital
 The Ever Changing World of Sepsis Management Laura Evans MD MSc Medical Director of Critical Care Bellevue Hospital COI Disclosures No financial interests to disclose Learning Objectives Review the evolution
The Ever Changing World of Sepsis Management Laura Evans MD MSc Medical Director of Critical Care Bellevue Hospital COI Disclosures No financial interests to disclose Learning Objectives Review the evolution
Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE
 Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE In critically ill patients: too little fluid Low preload,
Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE In critically ill patients: too little fluid Low preload,
Sepsis overview. Dr. Tsang Hin Hung MBBS FHKCP FRCP
 Sepsis overview Dr. Tsang Hin Hung MBBS FHKCP FRCP Epidemiology Sepsis, severe sepsis, septic shock Pathophysiology of sepsis Recent researches and advances From bench to bedside Sepsis bundle Severe sepsis
Sepsis overview Dr. Tsang Hin Hung MBBS FHKCP FRCP Epidemiology Sepsis, severe sepsis, septic shock Pathophysiology of sepsis Recent researches and advances From bench to bedside Sepsis bundle Severe sepsis
Troubleshooting Audio
 Welcome! Audio for this event is available via ReadyTalk Internet Streaming. No telephone line is required. Computer speakers or headphones are necessary to listen to streaming audio. Limited dial-in lines
Welcome! Audio for this event is available via ReadyTalk Internet Streaming. No telephone line is required. Computer speakers or headphones are necessary to listen to streaming audio. Limited dial-in lines
John Park, MD Assistant Professor of Medicine
 John Park, MD Assistant Professor of Medicine Faculty photo will be placed here park.john@mayo.edu 2015 MFMER 3543652-1 Sepsis Out with the Old, In with the New Mayo School of Continuous Professional Development
John Park, MD Assistant Professor of Medicine Faculty photo will be placed here park.john@mayo.edu 2015 MFMER 3543652-1 Sepsis Out with the Old, In with the New Mayo School of Continuous Professional Development
IV fluid administration in sepsis. Dr David Inwald Consultant in PICU St Mary s Hospital, London CATS, London
 IV fluid administration in sepsis Dr David Inwald Consultant in PICU St Mary s Hospital, London CATS, London The talk What is septic shock? What are the recommendations? What is the evidence? Do we follow
IV fluid administration in sepsis Dr David Inwald Consultant in PICU St Mary s Hospital, London CATS, London The talk What is septic shock? What are the recommendations? What is the evidence? Do we follow
Update in Critical Care Medicine
 Update in Critical Care Medicine Michael A. Gropper, MD, PhD Professor and Executive Vice Chair Department of Anesthesia and Perioperative Care Director, Critical Care Medicine UCSF Disclosure None Update
Update in Critical Care Medicine Michael A. Gropper, MD, PhD Professor and Executive Vice Chair Department of Anesthesia and Perioperative Care Director, Critical Care Medicine UCSF Disclosure None Update
Guidebook for ED and Inpatient Sepsis Order Set Initiatives 2018
 Background The leadership of the Surviving Sepsis Campaign (SSC) believes, since its inception, that both the SSC Guidelines and the SSC performance improvement indicators (1) will evolve as new evidence
Background The leadership of the Surviving Sepsis Campaign (SSC) believes, since its inception, that both the SSC Guidelines and the SSC performance improvement indicators (1) will evolve as new evidence
Sepsis and Antimcrobial Stewardship: Are they really mutually Exclusive?
 Sepsis and Antimcrobial Stewardship: Are they really mutually Exclusive? DR KATE ADAMS CONSULTANT INFECTIOUS DISEASES HULL AND EAST YORKSHIRE NHS TRUST AMS Sepsis No! At least not if the sepsis programme
Sepsis and Antimcrobial Stewardship: Are they really mutually Exclusive? DR KATE ADAMS CONSULTANT INFECTIOUS DISEASES HULL AND EAST YORKSHIRE NHS TRUST AMS Sepsis No! At least not if the sepsis programme
Sepsis in primary care. Sarah Bailey, Emma Evans, Nicola Shoebridge, Fiona Wells
 Sepsis in primary care Sarah Bailey, Emma Evans, Nicola Shoebridge, Fiona Wells sepsisnurses@uhcw.nhs.uk Quiz!! OR Hands on your heads Hands on your hips Definition. The Third International Consensus Definition
Sepsis in primary care Sarah Bailey, Emma Evans, Nicola Shoebridge, Fiona Wells sepsisnurses@uhcw.nhs.uk Quiz!! OR Hands on your heads Hands on your hips Definition. The Third International Consensus Definition
Sepsis. From EMS to ER to ICU. What we need to be doing
 Sepsis From EMS to ER to ICU What we need to be doing NEHAL BHATT, MD ATHENS PULMONARY, CRITICAL CARE AND SLEEP Objectives 1. Define the changes to the definition of Sepsis 2. Describe the assessment,
Sepsis From EMS to ER to ICU What we need to be doing NEHAL BHATT, MD ATHENS PULMONARY, CRITICAL CARE AND SLEEP Objectives 1. Define the changes to the definition of Sepsis 2. Describe the assessment,
Sepsis Update: Focus on Early Recognition and Intervention. Disclosures
 Sepsis Update: Focus on Early Recognition and Intervention Jessie Roske, MD October 2017 Disclosures I have no actual or potential conflict of interest in relation to this program/presentation. I will
Sepsis Update: Focus on Early Recognition and Intervention Jessie Roske, MD October 2017 Disclosures I have no actual or potential conflict of interest in relation to this program/presentation. I will
No conflicts of interest
 Robert M. Rodriguez, MD FAAEM Clinical Professor of Medicine and Emergency Medicine, UCSF No conflicts of interest Major Points Most ICU patients start in ED Chain of critical care starting in field and
Robert M. Rodriguez, MD FAAEM Clinical Professor of Medicine and Emergency Medicine, UCSF No conflicts of interest Major Points Most ICU patients start in ED Chain of critical care starting in field and
Sepsis is an important issue. Clinician s decision-making capability. Guideline recommendations
 Surviving Sepsis Campaign: International Guidelines for Management of Severe Sepsis and Septic Shock: 2012 Clinicians decision-making capability Guideline recommendations Sepsis is an important issue 8.7%
Surviving Sepsis Campaign: International Guidelines for Management of Severe Sepsis and Septic Shock: 2012 Clinicians decision-making capability Guideline recommendations Sepsis is an important issue 8.7%
Patient Safety Safe Table Webcast: Sepsis (Part III and IV) December 17, 2014
 December 17, 2014") Patient Safety Safe Table Webcast: Sepsis (Part III and IV) December 17, 2014 Presenters Mark Blaney, RN Regional Nurse Educator CHI Franciscan Health Karen Lautermilch Director, Quality & Performance
Patient Safety Safe Table Webcast: Sepsis (Part III and IV) December 17, 2014 Presenters Mark Blaney, RN Regional Nurse Educator CHI Franciscan Health Karen Lautermilch Director, Quality & Performance
Updates in Sepsis 2017
 Mortality Cases Total U.S. Population/1,000 Updates in 2017 Joshua Solomon, M.D. Associate Professor of Medicine National Jewish Health University of Colorado Denver Background New Definition of New Trials
Mortality Cases Total U.S. Population/1,000 Updates in 2017 Joshua Solomon, M.D. Associate Professor of Medicine National Jewish Health University of Colorado Denver Background New Definition of New Trials
Managing Patients with Sepsis
 Managing Patients with Sepsis Diagnosis; Initial Resuscitation; ARRT Initiation Prof. Achim Jörres, M.D. Dept. of Nephrology and Medical Intensive Care Charité University Hospital Campus Virchow Klinikum
Managing Patients with Sepsis Diagnosis; Initial Resuscitation; ARRT Initiation Prof. Achim Jörres, M.D. Dept. of Nephrology and Medical Intensive Care Charité University Hospital Campus Virchow Klinikum
EFFECT OF EARLY VASOPRESSIN VS NOREPINEPHRINE ON KIDNEY FAILURE IN PATIENTS WITH SEPTIC SHOCK. Alexandria Rydz
 EFFECT OF EARLY VASOPRESSIN VS NOREPINEPHRINE ON KIDNEY FAILURE IN PATIENTS WITH SEPTIC SHOCK Alexandria Rydz BACKGROUND- SEPSIS Sepsis is defined as life-threatening organ dysfunction caused by a dysregulated
EFFECT OF EARLY VASOPRESSIN VS NOREPINEPHRINE ON KIDNEY FAILURE IN PATIENTS WITH SEPTIC SHOCK Alexandria Rydz BACKGROUND- SEPSIS Sepsis is defined as life-threatening organ dysfunction caused by a dysregulated
Sepsis Awareness and Education
 Sepsis Awareness and Education Meets the updated New York State Department of Health (NYSDOH) requirements for Infection Control and Barrier Precautions coursework Element VII: Sepsis Awareness and Education
Sepsis Awareness and Education Meets the updated New York State Department of Health (NYSDOH) requirements for Infection Control and Barrier Precautions coursework Element VII: Sepsis Awareness and Education
Jarisch A. Kreislauffragen, Dünser et al. Critical Care 2013, 17:326 Sunday, March 30, 14
 It was fatal for the development of our understanding of circulation that blood flow is relatively difficult while blood pressure so easy to measure: This is the reason why the sphygmomanometer has gained
It was fatal for the development of our understanding of circulation that blood flow is relatively difficult while blood pressure so easy to measure: This is the reason why the sphygmomanometer has gained
FLUID RESUSCITATION AND MONITORING IN SEPSIS PROTOCOLIZED VS USUAL CARE DEEPA BANGALORE GOTUR MD, FCCP ASSISTANT PROFESSOR, WEILL CORNELL MEDICAL
 FLUID RESUSCITATION AND MONITORING IN SEPSIS PROTOCOLIZED VS USUAL CARE DEEPA BANGALORE GOTUR MD, FCCP ASSISTANT PROFESSOR, WEILL CORNELL MEDICAL COLLEGE NOVEMBER 10 TH 2017 TEXAS SCCM SYMPOSIUM Disclosures
FLUID RESUSCITATION AND MONITORING IN SEPSIS PROTOCOLIZED VS USUAL CARE DEEPA BANGALORE GOTUR MD, FCCP ASSISTANT PROFESSOR, WEILL CORNELL MEDICAL COLLEGE NOVEMBER 10 TH 2017 TEXAS SCCM SYMPOSIUM Disclosures
Last frontier of infection in critically ill patients
 Last frontier of infection in critically ill patients Nick Beeching Tropical & Infectious Disease Unit Royal Liverpool University Hospital Liverpool School of Tropical Medicine Liverpool School of Tropical
Last frontier of infection in critically ill patients Nick Beeching Tropical & Infectious Disease Unit Royal Liverpool University Hospital Liverpool School of Tropical Medicine Liverpool School of Tropical
Andrea Blotsky MDCM FRCPC General Internal Medicine, McGill University Thursday, October 15, 2015
 The TIMES Project: (Time to Initiation of Antibiotic Therapy in Medical Patients Presenting to the Emergency Department with Sepsis) - Preliminary Findings Andrea Blotsky MDCM FRCPC General Internal Medicine,
The TIMES Project: (Time to Initiation of Antibiotic Therapy in Medical Patients Presenting to the Emergency Department with Sepsis) - Preliminary Findings Andrea Blotsky MDCM FRCPC General Internal Medicine,
Bedside assessment of fluid status
 Bedside assessment of fluid status 2nd AKI Academy October 18 th 2014 David Treacher Guy s & St Thomas NHS Trust Assessing the circulation - the 3 key questions v Is my patient adequately filled? v What
Bedside assessment of fluid status 2nd AKI Academy October 18 th 2014 David Treacher Guy s & St Thomas NHS Trust Assessing the circulation - the 3 key questions v Is my patient adequately filled? v What
R2R: Severe sepsis/septic shock. Surat Tongyoo Critical care medicine Siriraj Hospital
 R2R: Severe sepsis/septic shock Surat Tongyoo Critical care medicine Siriraj Hospital Diagnostic criteria ACCP/SCCM consensus conference 1991 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference
R2R: Severe sepsis/septic shock Surat Tongyoo Critical care medicine Siriraj Hospital Diagnostic criteria ACCP/SCCM consensus conference 1991 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference
towards early goal directed therapy
 Paediatric Septic Shock- towards early goal directed therapy Elliot Long Paediatric Acute Care 2011 Conference Outline Emergency Department Rivers Protocol (EGDT) ACCM Sepsis Protocol Evidence Barriers
Paediatric Septic Shock- towards early goal directed therapy Elliot Long Paediatric Acute Care 2011 Conference Outline Emergency Department Rivers Protocol (EGDT) ACCM Sepsis Protocol Evidence Barriers
Shock and hemodynamic monitorization. Nilüfer Yalındağ Öztürk Marmara University Pendik Research and Training Hospital
 Shock and hemodynamic monitorization Nilüfer Yalındağ Öztürk Marmara University Pendik Research and Training Hospital Shock Leading cause of morbidity and mortality Worldwide: dehydration and hypovolemic
Shock and hemodynamic monitorization Nilüfer Yalındağ Öztürk Marmara University Pendik Research and Training Hospital Shock Leading cause of morbidity and mortality Worldwide: dehydration and hypovolemic
HAP/VAP care bundle interventions - a UK approach. Dr R G Masterton NHS Ayrshire & Arran
 HAP/VAP care bundle interventions - a UK approach Dr R G Masterton NHS Ayrshire & Arran How Hazardous Is Health Care? (Leape and Amalberti) Total lives lost per year 100,000 10,000 1,000 100 10 1 HAZARDOUS
HAP/VAP care bundle interventions - a UK approach Dr R G Masterton NHS Ayrshire & Arran How Hazardous Is Health Care? (Leape and Amalberti) Total lives lost per year 100,000 10,000 1,000 100 10 1 HAZARDOUS
INTENSIVE CARE MEDICINE CPD EVENING. Dr Alastair Morgan Wednesday 13 th September 2017
 INTENSIVE CARE MEDICINE CPD EVENING Dr Alastair Morgan Wednesday 13 th September 2017 WHAT IS NEW IN ICU? (RELEVANT TO ANAESTHETISTS) Not much! SURVIVING SEPSIS How many deaths in England were thought
INTENSIVE CARE MEDICINE CPD EVENING Dr Alastair Morgan Wednesday 13 th September 2017 WHAT IS NEW IN ICU? (RELEVANT TO ANAESTHETISTS) Not much! SURVIVING SEPSIS How many deaths in England were thought
The Sepsis Timebomb. James Wigfull Critical Care and Anaesthesia Sheffield Teaching Hospitals
 The Sepsis Timebomb James Wigfull Critical Care and Anaesthesia Sheffield Teaching Hospitals Relationship of SIRS, Sepsis and Infection BACTEREMIA PANCREATITIS INFECTION FUNGEMIA PARASITEMIA VIREMIA SEPSIS
The Sepsis Timebomb James Wigfull Critical Care and Anaesthesia Sheffield Teaching Hospitals Relationship of SIRS, Sepsis and Infection BACTEREMIA PANCREATITIS INFECTION FUNGEMIA PARASITEMIA VIREMIA SEPSIS
EARLY GOAL DIRECTED THERAPY : seminaires iris. Etat des lieux en Daniel De Backer
 EARLY GOAL DIRECTED THERAPY : Etat des lieux en 2017 Daniel De Backer Head Dept Intensive Care, CHIREC hospitals, Belgium Professor of Intensive Care, Université Libre de Bruxelles Past-President European
EARLY GOAL DIRECTED THERAPY : Etat des lieux en 2017 Daniel De Backer Head Dept Intensive Care, CHIREC hospitals, Belgium Professor of Intensive Care, Université Libre de Bruxelles Past-President European
Surviving Sepsis Campaign Guidelines 2012 & Update for David E. Tannehill, DO Critical Care Medicine Mercy Hospital St.
 Surviving Sepsis Campaign Guidelines 2012 & Update for 2015 David E. Tannehill, DO Critical Care Medicine Mercy Hospital St. Louis Be appropriately aggressive the longer one delays aggressive metabolic
Surviving Sepsis Campaign Guidelines 2012 & Update for 2015 David E. Tannehill, DO Critical Care Medicine Mercy Hospital St. Louis Be appropriately aggressive the longer one delays aggressive metabolic
Sepsis: A Medical Emergency
 Sepsis: A Medical Emergency April 24, 2017 Jim O Brien, MD, MS System Vice President, Quality and Patient Safety OhioHealth Disclosures: 2010 February 2017 Non-industry grant monies: NIH Clinical Research
Sepsis: A Medical Emergency April 24, 2017 Jim O Brien, MD, MS System Vice President, Quality and Patient Safety OhioHealth Disclosures: 2010 February 2017 Non-industry grant monies: NIH Clinical Research
Updates in Emergency Department Management of Sepsis
 Resident Journal Review Updates in Emergency Department Management of Sepsis Authors: Eli Brown, MD; Allison Regan, MD; Kaycie Corburn, MD; Jacqueline Shibata, MD Edited by: Jay Khadpe, MD FAAEM; Michael
Resident Journal Review Updates in Emergency Department Management of Sepsis Authors: Eli Brown, MD; Allison Regan, MD; Kaycie Corburn, MD; Jacqueline Shibata, MD Edited by: Jay Khadpe, MD FAAEM; Michael
Actualités de la prise en charge hémodynamique initiale Daniel De Backer
 Actualités de la prise en charge hémodynamique initiale Daniel De Backer Head Dept Intensive Care, CHIREC hospitals, Belgium Professor of Intensive Care, Université Libre de Bruxelles Past- President European
Actualités de la prise en charge hémodynamique initiale Daniel De Backer Head Dept Intensive Care, CHIREC hospitals, Belgium Professor of Intensive Care, Université Libre de Bruxelles Past- President European
Vasopressors in septic shock
 Vasopressors in septic shock Prof. Jean-Louis TEBOUL Medical ICU Bicetre hospital University Paris-South France Questions 1- Why do we use vasopressors in septic shock? 2- Which first-line agent? 3- When
Vasopressors in septic shock Prof. Jean-Louis TEBOUL Medical ICU Bicetre hospital University Paris-South France Questions 1- Why do we use vasopressors in septic shock? 2- Which first-line agent? 3- When
SEPSIS: Seeing Through the. W. Graham Carlos MD, MSCR, ATSF, FACP
 SEPSIS: Seeing Through the W. Graham Carlos MD, MSCR, ATSF, FACP Objectives Forget everything you have known about sepsis Learn new things Objectives Define sepsis Explain why Early Goal Directed Therapy
SEPSIS: Seeing Through the W. Graham Carlos MD, MSCR, ATSF, FACP Objectives Forget everything you have known about sepsis Learn new things Objectives Define sepsis Explain why Early Goal Directed Therapy
What is sepsis? RECOGNITION. Sepsis I Know It When I See It 9/21/2017
 Sepsis I Know It When I See It September 15, 2017 Matthew Exline, MD MPH Medical Director, Medical ICU What is sepsis? I shall not today attempt further to define the kinds of material [b]ut I know it
Sepsis I Know It When I See It September 15, 2017 Matthew Exline, MD MPH Medical Director, Medical ICU What is sepsis? I shall not today attempt further to define the kinds of material [b]ut I know it
Sepsis Wave II Webinar Series. Sepsis Reassessment
 Sepsis Wave II Webinar Series Sepsis Reassessment Presenters Nova Panebianco, MD Todd Slesinger, MD Fluid Reassessment in Sepsis Todd L. Slesinger, MD, FACEP, FCCM, FCCP, FAAEM Residency Program Director
Sepsis Wave II Webinar Series Sepsis Reassessment Presenters Nova Panebianco, MD Todd Slesinger, MD Fluid Reassessment in Sepsis Todd L. Slesinger, MD, FACEP, FCCM, FCCP, FAAEM Residency Program Director
3/14/2017. Pediatric Sepsis: From Goal Directed Therapy to Protocolized Care. Objectives. Developmental Response to Sepsis
 Pediatric Sepsis: From Goal Directed Therapy to Protocolized Care March 20, 2017 Reid WD Farris, MS MD Objectives Review the evolution & current state of the pediatric septic shock treatment guidelines
Pediatric Sepsis: From Goal Directed Therapy to Protocolized Care March 20, 2017 Reid WD Farris, MS MD Objectives Review the evolution & current state of the pediatric septic shock treatment guidelines
A Critical Review of Early Goal Directed Therapy and Government Endorsement
 A Critical Review of Early Goal Directed Therapy and Government Endorsement Charles Natanson M.D. Critical Care Medicine Department Clinical Center National Institutes of Health Clinical Center None Conflicts
A Critical Review of Early Goal Directed Therapy and Government Endorsement Charles Natanson M.D. Critical Care Medicine Department Clinical Center National Institutes of Health Clinical Center None Conflicts
Early Recognition and Timely Management of Sepsis Amid Changes in Definitions
 Early Recognition and Timely Management of Sepsis Amid Changes in Definitions Tze Shien Lo, MD, FACP Chief, Infectious Disease Service Fargo VA Medical Center Professor of Medicine UND School of Medicine
Early Recognition and Timely Management of Sepsis Amid Changes in Definitions Tze Shien Lo, MD, FACP Chief, Infectious Disease Service Fargo VA Medical Center Professor of Medicine UND School of Medicine
Sepsis Learning Collaborative: Sepsis New Definitions
 Sepsis Learning Collaborative: Sepsis New Definitions Sepsis 3, a New Definition Todd L. Slesinger, MD, FACEP, FCCM, FCCP, FAAEM Program Director and Academic Chair Department of Emergency Medicine Disclosures
Sepsis Learning Collaborative: Sepsis New Definitions Sepsis 3, a New Definition Todd L. Slesinger, MD, FACEP, FCCM, FCCP, FAAEM Program Director and Academic Chair Department of Emergency Medicine Disclosures
Pediatric Sepsis Treatment:
 Disclosures Pediatric Sepsis Treatment: (treat) Early & (reevaluate) Often None June 11, 2018 Leslie Dervan, MD MS Pacific Northwest Sepsis Conference 1 Agenda Sepsis: pathophysiology at-a-glance Pediatric
Disclosures Pediatric Sepsis Treatment: (treat) Early & (reevaluate) Often None June 11, 2018 Leslie Dervan, MD MS Pacific Northwest Sepsis Conference 1 Agenda Sepsis: pathophysiology at-a-glance Pediatric
Fluid balance and clinically relevant outcomes
 Fluid balance and clinically relevant outcomes Rui Moreno, MD, PhD, Professor UCINC, Hospital de São José Centro Hospitalar de Lisboa Central, E.P.E. INSULT PRIMARY MODS SIRS SECONDARY MODS OUTCOME RECOVERY
Fluid balance and clinically relevant outcomes Rui Moreno, MD, PhD, Professor UCINC, Hospital de São José Centro Hospitalar de Lisboa Central, E.P.E. INSULT PRIMARY MODS SIRS SECONDARY MODS OUTCOME RECOVERY
Sepsis 2015: You say you wanted a revolution
 Thomas Jefferson University Jefferson Digital Commons Pulmonary and Critical Care Medicine, Presentations and Grand Rounds Division of Pulmonary and Critical Care Medicine 6-10-2015 Sepsis 2015: You say
Thomas Jefferson University Jefferson Digital Commons Pulmonary and Critical Care Medicine, Presentations and Grand Rounds Division of Pulmonary and Critical Care Medicine 6-10-2015 Sepsis 2015: You say
Diagnosis and Management of Sepsis and Septic Shock. Martin D. Black MD Concord Pulmonary Medicine Concord, New Hampshire
 Diagnosis and Management of Sepsis and Septic Shock Martin D. Black MD Concord Pulmonary Medicine Concord, New Hampshire Financial: none Disclosures Objectives: Identify physiologic principles of septic
Diagnosis and Management of Sepsis and Septic Shock Martin D. Black MD Concord Pulmonary Medicine Concord, New Hampshire Financial: none Disclosures Objectives: Identify physiologic principles of septic
OHSU. Update in Sepsis
 Update in Sepsis Jonathan Pak, MD June 1, 2017 Structure of Talk 1. Sepsis-3: The latest definition 2. Clinical Management - Is EGDT dead? - Surviving Sepsis Campaign Guidelines 3. A novel therapy: Vitamin
Update in Sepsis Jonathan Pak, MD June 1, 2017 Structure of Talk 1. Sepsis-3: The latest definition 2. Clinical Management - Is EGDT dead? - Surviving Sepsis Campaign Guidelines 3. A novel therapy: Vitamin
AMI Talking Points. Provide appropriate treatment to Acute MI patients with these core measures:
 AMI Provide appropriate treatment to Acute MI patients with these core measures: Aspirin received within 24 hours of arrival or contraindication documented Primary PCI Received Within 90 Minutes of Hospital
AMI Provide appropriate treatment to Acute MI patients with these core measures: Aspirin received within 24 hours of arrival or contraindication documented Primary PCI Received Within 90 Minutes of Hospital
Dr. F Javier Belda Dept. Anesthesiology and Critical Care Hospital Clinico Universitario Valencia (Spain) Pulsion MAB
 Pulsion MAB") State of the Art Hemodynamic Monitoring III CO, preload, lung water and ScvO2 The winning combination! Dr. F Javier Belda Dept. Anesthesiology and Critical Care Hospital Clinico Universitario Valencia
State of the Art Hemodynamic Monitoring III CO, preload, lung water and ScvO2 The winning combination! Dr. F Javier Belda Dept. Anesthesiology and Critical Care Hospital Clinico Universitario Valencia
Introduction of the concept of value in sepsis care
 Introduction of the concept of value in sepsis care January 11, 2017 Jim O Brien, MD, MS System Vice President, Quality and Patient Safety OhioHealth Disclosures: 2010 January 2017 Non-industry grant monies:
Introduction of the concept of value in sepsis care January 11, 2017 Jim O Brien, MD, MS System Vice President, Quality and Patient Safety OhioHealth Disclosures: 2010 January 2017 Non-industry grant monies:
Tailored Volume Resuscitation in the Critically Ill is Achievable. Objectives. Clinical Case 2/16/2018
 Tailored Volume Resuscitation in the Critically Ill is Achievable Heath E Latham, MD Associate Professor Fellowship Program Director Pulmonary and Critical Care Objectives Describe the goal of resuscitation
Tailored Volume Resuscitation in the Critically Ill is Achievable Heath E Latham, MD Associate Professor Fellowship Program Director Pulmonary and Critical Care Objectives Describe the goal of resuscitation
Sepsis or Severe Sepsis? Is there a right thing, and how do we do it?
 Sepsis or Severe Sepsis? Is there a right thing, and how do we do it? Steven Q Simpson, MD, FCCP, FACP Professor of Medicine Division of Pulmonary and Critical Care University of Kansas Disclosures No
Sepsis or Severe Sepsis? Is there a right thing, and how do we do it? Steven Q Simpson, MD, FCCP, FACP Professor of Medicine Division of Pulmonary and Critical Care University of Kansas Disclosures No
Appendix. Supplementary figures and tables
 This appendix was part of the submitted manuscript and has been peer reviewed. It is posted as supplied by the authors. Appendix. Supplementary figures and tables Figure A1. Flowchart describing patient
This appendix was part of the submitted manuscript and has been peer reviewed. It is posted as supplied by the authors. Appendix. Supplementary figures and tables Figure A1. Flowchart describing patient
Reducing the Door to Needle Time for Antibiotics in Suspected Neutropenic Sepsis using a Dedicated Clinical Pathway
 Reducing the Door to Needle Time for Antibiotics in Suspected Neutropenic Sepsis using a Dedicated Clinical Pathway Dr Alex Williams, Oncology Specialty Doctor. Cheltenham General Hospital Oncology Centre
Reducing the Door to Needle Time for Antibiotics in Suspected Neutropenic Sepsis using a Dedicated Clinical Pathway Dr Alex Williams, Oncology Specialty Doctor. Cheltenham General Hospital Oncology Centre
Full Disclosure. The case for why it matters. Goal-directed Fluid Resuscitation
 Goal-directed Fluid Resuscitation Christopher G. Choukalas, MD, MS Department of Anesthesia and Perioperative Care University of California, San Francisco I own no stocks Full Disclosure The case for why
Goal-directed Fluid Resuscitation Christopher G. Choukalas, MD, MS Department of Anesthesia and Perioperative Care University of California, San Francisco I own no stocks Full Disclosure The case for why