MANAGING END STAGE LIVER DISEASE IN RESOURCE LIMITED SETTINGS
|
|
|
- Harry Fields
- 5 years ago
- Views:
Transcription





1 MANAGING END STAGE LIVER DISEASE IN RESOURCE LIMITED SETTINGS Mark W. Sonderup Division of Hepatology and Liver Laboratory Department of Medicine University of Cape Town & Groote Schuur Hospital
2 Cirrhosis.. End stage of any chronic liver disease Characterized histologically by regenerative nodules surrounded by fibrous tissue - is technically a histological diagnosis However, in patients with chronic liver disease the presence of various clinical features suggest cirrhosis Non-invasive assessment can reliably replace biopsy Clinically there are two distinct phases of cirrhosis: -> Compensated -> Decompensated

 Stigma of chronic liver")

3 Diagnostic Algorithm Yes Patient with chronic liver disease and any of the following: Variceal hemorrhage Ascites Hepatic encephalopathy No Physical findings: Laboratory findings: Non-invasive tests Enlarged left hepatic lobe Thrombocytopenia APRI, FIB-4 Splenomegaly Impaired synthetic liver function VCTE (Fibroscan) Stigma of chronic liver disease Yes No Yes Liver biopsy not necessary for the diagnosis of cirrhosis Radiological findings: Small nodular/irregular liver Intra-abdominal collaterals Ascites Splenomegaly No Liver biopsy
4 Natural History of Chronic Liver Disease Chronic liver disease Compensated cirrhosis Decompensated cirrhosis Death e.g. hep B/C; iron, alcohol etc
5


6
7 Management of Compensated Cirrhosis Chronic liver disease Compensated cirrhosis Diagnosis: Liver biopsy Clinical/Radiology/Bloods/Non-invasive Decompensated cirrhosis Death Screen for varices (OGD): Orthotopic liver transplant (OLT) Screen for HCC: α-fp; Ultrasound every 6 months? treatment of underlying problem Measures to stop alcohol Hep A and B vaccination
8 LT-Free Survival (%) HBV Therapy Reduces Risk of Disease Progression Prospective cohort study in pts with HBV and first-onset complications of decompensated cirrhosis (N = 707) treated predominantly with lamivudine (n = 203) or entecavir (n = 198) Bonferroni-adjusted P < Months Treated, responder (n = 245) Treated, nonresponder* (n = 178) Untreated (n = 284) Antiviral therapy improved transplant-free survival over mean follow-up of 49 mos * (P =.0098 vs untreated) Nonresponders included pts with HBV rebound or genotypic resistance, primary nonresponse, NE due to early event (death, LT, LTFU). Jang JW, et al. Hepatology. 2015;61:
 Progression to cirrhosis of non-cirrhotics : 3/252")
9 ETV, n=57, median FU 280 weeks TDF, n=348 Cirrhosis regression: 71/96 (74%) Progression to cirrhosis of non-cirrhotics : 3/252 (1,2%)
10
11 Percent HCV Treatment Improves Health Advanced fibrosis Multicenter study [1] 5 hospitals (Europe, Canada) 530 pts with HCV IFN regimens Advanced fibrosis or cirrhosis Median follow-up: 8.4 yrs Early-stage disease Extra-hepatic manifestations [2] Health-related quality of life [3] All cause mortality Liver-related mortality or transplant 5.1 HCC 10-Yr Cumulative Incidence [1] 21.8 SVR No SVR 1. van der Meer AJ, et al. JAMA. 2012;308: van der Meer AJ. Expert Rev Gastroenterol Hepatol. 2015;9: Younossi Z, et al. Clin Gastroenterol Hepatol. 2014;12:
12 Survival HCC-Free Survival SVR With DAA Therapy: Mortality and HCC Risk Patients with HCV infection, FIB-4 > 3.25 in VA HCV Clinical Case Registry (N = 15,059) SVR with DAA therapy significantly lowered all-cause mortality and incident HCC 1 All-Cause Mortality SVR 1 Incident HCC SVR 0,9 0,8 0,7 79% reduction with SVR P <.001 No SVR 0,9 0,8 0,7 84% reduction with SVR P <.001 No SVR 0,6 0,6 0,5 0, Time Since DAA EOT (Years) Time Since DAA EOT (Years) Backus LI, et al. Hepatology. 2017
13

14

15 Pathophysiology of bacterial translocation and bacteremias in cirrhosis


16 PAMP s: pathogen associated molecular patterns e.g.

17 Pathophysiology of Ascites Formation : splanchnic and systemic vasodilation

18

19
20 Prophylactic Antibiotics Improve Outcomes in Cirrhotic Patients with GI Hemorrhage Control Antibiotic Absolute (n=270) (n=264) difference (95% CI) Infection 45% 14% -32% (-42 to 23) SBP / Bacteremia 27% 8% -18% (-26 to 11) Death 24% 15% -9% (-15 to 3) Bernard et al., Hepatology 1999; 29:1655

21

22
23 Bacterial infections in cirrhosis Incidence of infection and severity in cirrhosis is greater than general population Infection with multi-resistant organisms is greater in cirrhosis and associated with higher mortality rates Infections provoke Acute on Chronic Liver Failure Diagnostic and treatment delays enhances mortality Jalan et al. J Hep Jun 60(6). 1310
24 Cirrhosis and portal HPT Vascular resistance to portal blood flow Portal pressure Splanchnic arteriolar resistance Portal blood inflow Varices



25 Varices Increase in Diameter Progressively No varices Small varices Large varices 7-8%/year 7-8%/year Merli et al. J Hepatol 2003;38:266
26 Large Varices Are More Likely To Rupture No Varices Small Varices p<0.01 * % Patients without bleeding 50 Large Varices * * 25 Six-week mortality of VB is 15-20% year probability of first bleed: Small varices: 7% Large varices: 30% Time (months) One year recurrence rate is 60% * Merli et al., Hepatol 2003; 38:266, ** Conn et al., Hepatology 1991; 13:902
27 Mortality from 1 st variceal bleed has improved McCormick. Gut Nov;49(5):682-5.

28 B-blockers still recommended as 1 st line however local factors determine approach Khuroo et al. APT

29
30 Does everyone need to be scoped of OV surveillance? Can we risk stratify patients who need screening? If so, how? Can Transient Elastography (Fibroscan R ) help us select patients?

31 Stiffness (kpa) Liver Stiffness y = ,037 r 2 = 0,61 p < 0,0001 PH scarcely related to Fibrosis: CIRRHOSIS BECOMES A SYSTEMIC DISEASE PH related to Fibrosis HVPG (mmhg) Vizzutti F et al., Hepatology 2007; 45:
32 Diagnostic performance of transient elastography for the detection of clinically significant portal hypertension (HVPG 10 mm Hg) Authors Patients (n) Etiologies Study design Prevalence of Cinically Significant Portal hypertension Cut-offs HVPG 10 mm Hg (kpa) AUC Se (%) Sp (%) PPV (%) NPV (%) +LR -LR Carrion et al. (35) Vizzutti et al. (36) HCV-LT HCV Prospective monocentric Prospective monocentric 21% 77% 8.7* ** Sanchez-Condé et al. (39) Lemoine et al. (38) Bureau et al. (37) HIV-HCV HCV Alcohol CLD Prospective monocentric Retrospective monocentric Prospective monocentric 74% 77% 83% 51% ** * Hepatic Venous Pressure Gradient (HVPG) 6 mm Hg; ** severe portal hypertension HVPG 12 mm Hg AUC: area under ROC curve; Se sensitivity; Sp specificity; +LR positive likelihood ratio; -LR negative likelihood ratio; HCV chronic hepatitis C; HCV-LT Liver transplant for hepatitis C; CLD chronic liver diseases; Castera L, Pinzani M, Bosch J, J Hepatology 2012
 at risk of developing clinically significant portal hypertension (CSPH) (1b;A).")
33 BAVENO VI Screening and surveillance: Invasive and non-invasive The introduction of transient elastography (TE) in clinical practice has allowed the early identification of patients with chronic liver disease (CLD) at risk of developing clinically significant portal hypertension (CSPH) (1b;A). Identification of patients with cacld who can safely avoid screening endoscopy (new) Patients with a liver stiffness <20 kpa and with a platelet count >150,000 have a very low risk (<5%) of having varices requiring treatment, and can avoid screening endoscopy (1b;A). AASLD guidance 2016




34 The Spleen in the Assessment of Advanced Chronic Liver Disease INCREASE IN SPLEEN STIFFNESS?? Congestion Hypertrophy and Hyperplasia Fibrosis


35 Measurement of Spleen Stiffness by Fibroscan 1. Sufficient intercostal space width 2. - Splenic parenchymal thickness > 4 cm (by US) 3. Success rate > 60% and IQR < 30% of median value 4. Intra-observer reproducibility 96%, inter-observer reproducibility 94% 5. Probe upper limit 75 kpa

:646-54 35 35 30")

")
36 HVPG (mm Hg) HVPG (mm Hg) Spleen Stiffness (SS), a Diagnostic Parameter in Cirrhosis Colecchia A. et al., Gastroenterology 2012 ; 143(3): P = R² = 0,70 30 P = R 2 = 0, Compensated Cirrhosis Liver Stiffness (kpa) Spleen Stiffness (kpa) Esophageal Varices: NO Esophageal Varices: YES
37 Liver and Spleen Stiffness for the Prediction of the Presence of Esophageal Varices Colecchia A. et al., Gastroenterology 2012 ; 143(3): EV: NO EV: YES EV: NO EV: YES

38
39 Using Beta Blockers: Practical Tips Monitor Resting Heart Rate, BP Long-acting agents (eg. Propranolol LA) preferred - Administer in the evening If non Long Acting BD or TDS (low doses! e.g mg per dose to start with) Start low and increment to target Target: Resting heart rate beats per minute/25% reduction in heart rate/maximal tolerated dose Ideal titrate to HVPG<12mmHg

40



41 B-blockers decrease intestinal permeability and endotoxaemia irrespective of haemodynamic response 50 patients with cirrhosis Increased intestinal permeability/bacterial translocation when Improvement with NSBBs irrespective of HVPG response HVPG Reiberger J Hepatol 2013
42 B-blockers and prevention of ascites 83 patients with HVPG > 12 mmhg, b-blockers for primary prophylaxis of VB 53 months mean-follow-up 52 decompensated, 81% with ascites Reduced probability of ascites, refractory ascites and HRS If HVPGreductionof 10%,only19%developedascites Hernandez-Gea AmJGastro 2012

43
44 Propranolol: the aspirin of hepatologists? Cheap Universal availability May affect outcomes other than bleeding e.g. Portal Gastropathy Propranolol in combination: - statin agents (Abraldes 2009) - non absorbable antibiotics (Fernandez 2007)

45
46
47

48
49 J Hepatol Mar;64(3):574-82

50 Beta blockers in cirrhosis: The window re-opens.
51 Management of Ascites
52
 Sinusoidal pressure (HVPG 10-12 mmhg) Na restriction")

53 Cirrhosis Intrahepatic resistance Arteriolar resistance (vasodilation) Sinusoidal pressure (HVPG mmhg) Na restriction Effective arterial blood volume Ascites LVP Sodium and water retention Diuretics Activation of neuro-humoral systems (renin, angiotensin, aldosterone)

54 Dietary Na + restriction
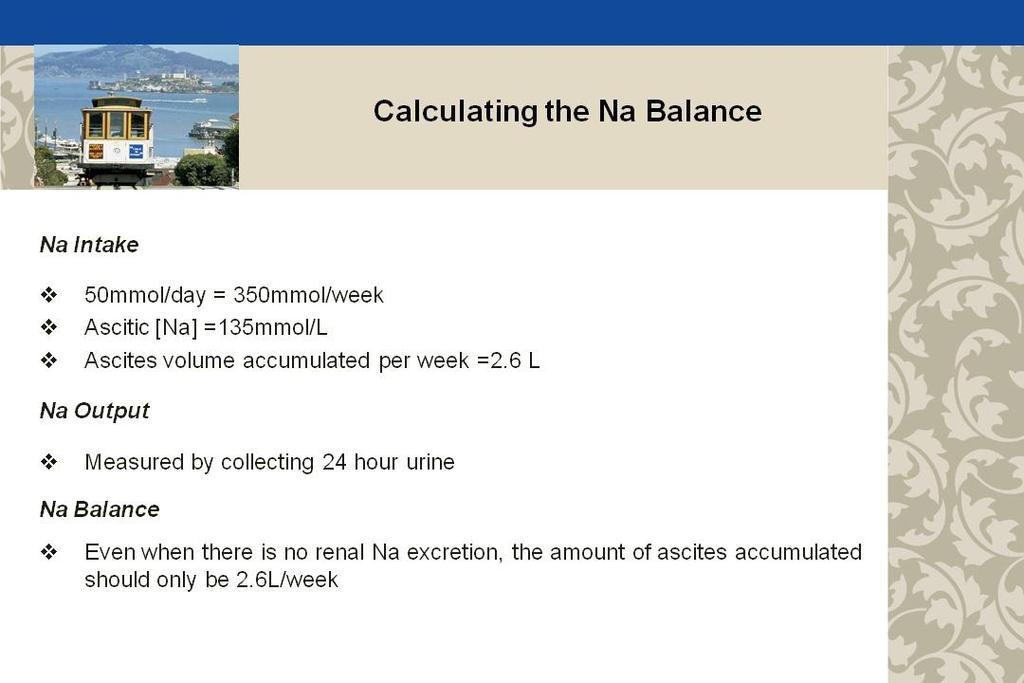
55 Calculating the Na + balance Calculating the Na + balance
56 Diuretic Therapy Diuretic Therapy Angeli et al. GUT 2010

57 Diuretic Diuretic Therapy Therapy Angeli et al. GUT 2010
58 Diuretics best to initiate with combination of spironolactone and furosemide spironolactone titrated to maximum 400mg/day furosemide titrated to maximum 160mg/day start low and monitor response (weight), renal function, K + taper doses when ascites free

59 Large Volume Paracentesis best approach for tense ascites does not address underlying issue viz. salt/h 2 O retention

60 Large Volume Paracentesis

61 Gines et al Gastroenterology 1998.
62 Post Paracentesis Circulatory Dysfunction Definition Increase in >50% PRA from pre-paracentesis level to a maximum on day of >4ng/ml/hr Incidence 27% Associated with: 20% AKI Decreased survival HRS

63 Gines et al Gastroenterology 1998.

64 Use of albumin with LVP how much?
65 Intrahepatic resistance Cirrhosis worsening liver disease Arteriolar resistance (vasodilation) Sinusoidal pressure Effective arterial blood volume Refractory Ascites Sodium and water retention Activation of neurohumoral systems
66 Refractory Ascites International Ascites Club criteria Diuretic resistant (20%) failure to lose at least 1.5kg/wk on: - 400mg spironolactone - 160mg furosemide Diuretic intractable (80%) failure to lose weight due to the inability to use effective doses of diuretics because of intolerance or SE s

67 Management of refractory ascites
68
69 Patients who benefited the most with albumin: Creatinine > 88umol/L (>1mg/dl) Bilirubin > 68umol/L (>4mg/dl)
70

71
72

73 Sarcopaenia

74

75
76 Hepatic Encephalopathy

77 Pathogenesis of Hepatic Encephalopathy Toxins Failure to metabolise NH 3 NH 3 shunting Bacterial action Protein load GABA-BDZ receptors

78 Precipitants of hepatic encephalopathy Protein excess GI Bleeds Sedative/ Hypnotic drugs TIPSS Diuretics Temperature K + Dehydration Renal failure Infections
79 Treatment of Hepatic Encephalopathy Identify and treat precipitating factor Infection GI hemorrhage Dehydration Sedatives Constipation Lactulose (adjust to 2-3 bowel movements/day) Protein restriction, short-term
80

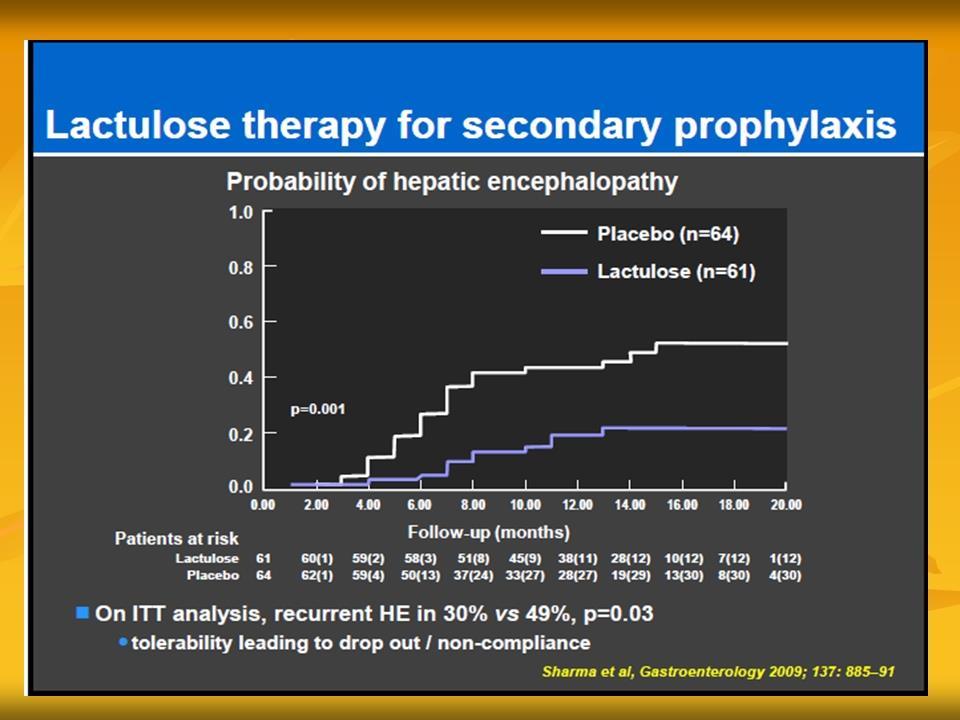
81 Lactulose as the Gold Standard for Rx of Encephalopathy Systematic review of randomised trials Bodil Als-Nielsen et al. BMJ 2004

82 Rifaximin in the treatment of HE

83 Rifaximin reduced the risk of breakthrough HE by 58% vs. placebo Bass et al. NEJM 2010;362:

84 Rifaximin reduced the risk of HE related hospitalization by 50% vs. placebo
85 Summary : Cirrhosis Management in Resource limited Benefits associated with survival settings Treat underlying cause of cirrhosis!!! Albumin with SBP and post LVP (if available, otherwise crystalloid) Antibiotic prophylaxis post GI bleed β-blocker value extends beyond OV prophylaxis Don t stop statins Nutrition!
Screening for Portal Hypertension in Cirrhosis
 Screening for Portal Hypertension in Cirrhosis MASSIMO PINZANI, MD, PhD, FRCP Sheila Sherlock Chair of Hepatology UCL Institute for Liver and Digestive Health Royal Free Hospital, London, UK m.pinzani@ucl.ac.uk
Screening for Portal Hypertension in Cirrhosis MASSIMO PINZANI, MD, PhD, FRCP Sheila Sherlock Chair of Hepatology UCL Institute for Liver and Digestive Health Royal Free Hospital, London, UK m.pinzani@ucl.ac.uk
Steps in Assessing Fibrosis 4/30/2015. Overview of Liver Disease Associated With HCV
 Overview of Liver Disease Associated With HCV Marion G. Peters, MD John V. Carbone, Endowed Chair Professor of Medicine Chief of Hepatology Research University of California San Francisco San Francisco,
Overview of Liver Disease Associated With HCV Marion G. Peters, MD John V. Carbone, Endowed Chair Professor of Medicine Chief of Hepatology Research University of California San Francisco San Francisco,
Diagnostic Procedures. Measurement of Hepatic venous pressure in management of cirrhosis. Clinician s opinion
 5 th AISF Post-Meeting Course Diagnostic and Therapeutic Invasive Procedures in Hepatology Rome, February 25 th Diagnostic Procedures Measurement of Hepatic venous pressure in management of cirrhosis Clinician
5 th AISF Post-Meeting Course Diagnostic and Therapeutic Invasive Procedures in Hepatology Rome, February 25 th Diagnostic Procedures Measurement of Hepatic venous pressure in management of cirrhosis Clinician
Approved regimens for cirrhotic patients
 5th Workshop on HCV THERAPY ADVANCES New antivirals in clinical practice Approved regimens for cirrhotic patients Amsterdam, 4-5 december 2015 Disease burden in Spain 400000 350000 300000 F0 Peak cirrhosis
5th Workshop on HCV THERAPY ADVANCES New antivirals in clinical practice Approved regimens for cirrhotic patients Amsterdam, 4-5 december 2015 Disease burden in Spain 400000 350000 300000 F0 Peak cirrhosis
HCV care after cure. This program is supported by educational grants from
 HCV care after cure This program is supported by educational grants from Raffaele Bruno,MD Department of Infectious Diseases, Hepatology Outpatients Unit University of Pavia Fondazione IRCCS Policlinico
HCV care after cure This program is supported by educational grants from Raffaele Bruno,MD Department of Infectious Diseases, Hepatology Outpatients Unit University of Pavia Fondazione IRCCS Policlinico
Primary Prophylaxis against Variceal Hemorrhage Pharmacotherapy vs Endoscopic Band Ligation
 Primary Prophylaxis against Variceal Hemorrhage Pharmacotherapy vs Endoscopic Band Ligation Siwaporn Chainuvati, MD Faculty of Medicine Siriraj Hospital Outline Natural history of esophageal varices Which
Primary Prophylaxis against Variceal Hemorrhage Pharmacotherapy vs Endoscopic Band Ligation Siwaporn Chainuvati, MD Faculty of Medicine Siriraj Hospital Outline Natural history of esophageal varices Which
Transient elastography the state of the art
 Transient elastography the state of the art Laurent CASTERA, MD PhD Department of Hepatology, Hôpital Beaujon, Clichy Université Paris-7, France White Nights of Hepatology, St Petersburg, Russia, june
Transient elastography the state of the art Laurent CASTERA, MD PhD Department of Hepatology, Hôpital Beaujon, Clichy Université Paris-7, France White Nights of Hepatology, St Petersburg, Russia, june
Management of Cirrhotic Complications Uncontrolled Ascites. Siwaporn Chainuvati, MD Siriraj Hospital Mahidol University
 Management of Cirrhotic Complications Uncontrolled Ascites Siwaporn Chainuvati, MD Siriraj Hospital Mahidol University Topic Definition, pathogenesis Current therapeutic options Experimental treatments
Management of Cirrhotic Complications Uncontrolled Ascites Siwaporn Chainuvati, MD Siriraj Hospital Mahidol University Topic Definition, pathogenesis Current therapeutic options Experimental treatments
Ascites Management. Atif Zaman, MD MPH Oregon Health & Science University Professor of Medicine Division of Gastroenterology and Hepatology
 Ascites Management Atif Zaman, MD MPH Oregon Health & Science University Professor of Medicine Division of Gastroenterology and Hepatology Disclosure 1. The speaker Atif Zaman, MD MPH have no relevant
Ascites Management Atif Zaman, MD MPH Oregon Health & Science University Professor of Medicine Division of Gastroenterology and Hepatology Disclosure 1. The speaker Atif Zaman, MD MPH have no relevant
Transient elastography in chronic viral liver diseases
 4 th AISF POST-MEETING COURSE Roma, 26 Febbraio 2011 Transient elastography in chronic viral liver diseases CRISTINA RIGAMONTI, M.D., Ph.D. Transient elastography (TE): a rapid, non-invasive technique
4 th AISF POST-MEETING COURSE Roma, 26 Febbraio 2011 Transient elastography in chronic viral liver diseases CRISTINA RIGAMONTI, M.D., Ph.D. Transient elastography (TE): a rapid, non-invasive technique
Management of Ascites and Hepatorenal Syndrome. Florence Wong University of Toronto. June 4, /16/ Gore & Associates: Consultancy
 Management of Ascites and Hepatorenal Syndrome Florence Wong University of Toronto June 4, 2016 6/16/2016 1 Disclosures Gore & Associates: Consultancy Sequana Medical: Research Funding Mallinckrodt Pharmaceutical:
Management of Ascites and Hepatorenal Syndrome Florence Wong University of Toronto June 4, 2016 6/16/2016 1 Disclosures Gore & Associates: Consultancy Sequana Medical: Research Funding Mallinckrodt Pharmaceutical:
Learning Objectives. After attending this presentation, participants will be able to:
 Learning Objectives After attending this presentation, participants will be able to: Describe HCV in 2015 Describe how to diagnose advanced liver disease and cirrhosis Identify the clinical presentation
Learning Objectives After attending this presentation, participants will be able to: Describe HCV in 2015 Describe how to diagnose advanced liver disease and cirrhosis Identify the clinical presentation
Invasive Evaluation of Portal Hypertension. Vincenzo La Mura, MD PhD Department of Biomedical Sciences for Health University of Milan
 Invasive Evaluation of Portal Hypertension Vincenzo La Mura, MD PhD Department of Biomedical Sciences for Health University of Milan Vincenzo La Mura, MD, PhD Dipartimento di scienze Biomediche per la
Invasive Evaluation of Portal Hypertension Vincenzo La Mura, MD PhD Department of Biomedical Sciences for Health University of Milan Vincenzo La Mura, MD, PhD Dipartimento di scienze Biomediche per la
Initial approach to ascites
 Ascites: Filling and Draining the Water Balloon Common Pathogenesis in Refractory Ascites, Hyponatremia, and Cirrhosis intrahepatic resistance sinusoidal portal hypertension Splanchnic vasodilation (effective
Ascites: Filling and Draining the Water Balloon Common Pathogenesis in Refractory Ascites, Hyponatremia, and Cirrhosis intrahepatic resistance sinusoidal portal hypertension Splanchnic vasodilation (effective
Beta-blockers in cirrhosis: Cons
 Beta-blockers in cirrhosis: Cons Eric Trépo MD, PhD Dept. of Gastroenterology. Hepatopancreatology and Digestive Oncology. C.U.B. Hôpital Erasme. Université Libre de Bruxelles. Bruxelles. Belgium Laboratory
Beta-blockers in cirrhosis: Cons Eric Trépo MD, PhD Dept. of Gastroenterology. Hepatopancreatology and Digestive Oncology. C.U.B. Hôpital Erasme. Université Libre de Bruxelles. Bruxelles. Belgium Laboratory
BETA-BLOCKERS IN CIRRHOSIS.PRO.
 BETA-BLOCKERS IN CIRRHOSIS.PRO. Angela Puente Sánchez. MD PhD Hepatology Unit. Gastroenterology department Marques de Valdecilla University Hospital. Santander INTRODUCTION. Natural history of cirrhosis
BETA-BLOCKERS IN CIRRHOSIS.PRO. Angela Puente Sánchez. MD PhD Hepatology Unit. Gastroenterology department Marques de Valdecilla University Hospital. Santander INTRODUCTION. Natural history of cirrhosis
Esophageal Varices Beta-Blockers or Band Ligation. Cesar Yaghi MD Hotel-Dieu de France University Hospital Universite Saint Joseph
 Esophageal Varices Beta-Blockers or Band Ligation Cesar Yaghi MD Hotel-Dieu de France University Hospital Universite Saint Joseph Esophageal Varices Beta-Blockers or Band Ligation? Risk of esophageal variceal
Esophageal Varices Beta-Blockers or Band Ligation Cesar Yaghi MD Hotel-Dieu de France University Hospital Universite Saint Joseph Esophageal Varices Beta-Blockers or Band Ligation? Risk of esophageal variceal
Hepatitis Alert: Management of Patients With HCV Who Have Achieved SVR
 Hepatitis Alert: Management of Patients With HCV Who Have Achieved SVR This program is supported by educational grants from AbbVie, Gilead Sciences, and Merck About These Slides Please feel free to use,
Hepatitis Alert: Management of Patients With HCV Who Have Achieved SVR This program is supported by educational grants from AbbVie, Gilead Sciences, and Merck About These Slides Please feel free to use,
B C Outlines. Child-Pugh scores
 B C 2016-12-09 Outlines Child-Pugh scores CT MRI Fibroscan / ARFI Histologic Scoring Systems for Fibrosis Fibrosis METAVIR Ishak None 0 0 Portal fibrosis (some) 1 1 Portal fibrosis (most) 1 2 Bridging
B C 2016-12-09 Outlines Child-Pugh scores CT MRI Fibroscan / ARFI Histologic Scoring Systems for Fibrosis Fibrosis METAVIR Ishak None 0 0 Portal fibrosis (some) 1 1 Portal fibrosis (most) 1 2 Bridging
End-Stage Liver Disease (ESLD): A Guide for HIV Physicians
: A Guide for HIV Physicians") Slide 1 of 32 End-Stage Liver Disease (ESLD): A Guide for HIV Physicians Marion G. Peters, MD John V. Carbone, MD, Endowed Chair Professor of Medicine Chief of Hepatology Research University of California
Slide 1 of 32 End-Stage Liver Disease (ESLD): A Guide for HIV Physicians Marion G. Peters, MD John V. Carbone, MD, Endowed Chair Professor of Medicine Chief of Hepatology Research University of California
The Impact of HBV Therapy on Fibrosis and Cirrhosis
 The Impact of HBV Therapy on Fibrosis and Cirrhosis Jordan J. Feld, MD, MPH Associate Professor of Medicine University of Toronto Hepatologist Toronto Centre for Liver Disease Sandra Rotman Centre for
The Impact of HBV Therapy on Fibrosis and Cirrhosis Jordan J. Feld, MD, MPH Associate Professor of Medicine University of Toronto Hepatologist Toronto Centre for Liver Disease Sandra Rotman Centre for
Management of Cirrhosis Related Complications
 Management of Cirrhosis Related Complications Ke-Qin Hu, MD, FAASLD Professor of Clinical Medicine Director of Hepatology University of California, Irvine Disclosure I have no disclosure related to this
Management of Cirrhosis Related Complications Ke-Qin Hu, MD, FAASLD Professor of Clinical Medicine Director of Hepatology University of California, Irvine Disclosure I have no disclosure related to this
Cirrhosis and Portal Hypertension Gastroenterology Teaching Project American Gastroenterological Association
 CIRRHOSIS AND PORTAL HYPERTENSION Cirrhosis and Portal Hypertension Gastroenterology Teaching Project American Gastroenterological Association WHAT IS CIRRHOSIS? What is Cirrhosis? DEFINITION OF CIRRHOSIS
CIRRHOSIS AND PORTAL HYPERTENSION Cirrhosis and Portal Hypertension Gastroenterology Teaching Project American Gastroenterological Association WHAT IS CIRRHOSIS? What is Cirrhosis? DEFINITION OF CIRRHOSIS
Jong Young Choi, M.D.
 The Liver Week 2014 Jong Young Choi, M.D. Dept. of Internal Medicine The Catholic University of Korea, College of Medicine The clinical study for natural history of LC is not many. Most of them was done
The Liver Week 2014 Jong Young Choi, M.D. Dept. of Internal Medicine The Catholic University of Korea, College of Medicine The clinical study for natural history of LC is not many. Most of them was done
The Liver for the Nonhepatologist
 The Liver for the Nonhepatologist Michael R. Charlton, MBBS, FRCP Hepatology Director and Medical Director of Liver Transplantation Intermountain Medical Center Salt Lake City, Utah FORMATTED: 05-14-15
The Liver for the Nonhepatologist Michael R. Charlton, MBBS, FRCP Hepatology Director and Medical Director of Liver Transplantation Intermountain Medical Center Salt Lake City, Utah FORMATTED: 05-14-15
Life After SVR for Cirrhotic HCV
 Life After SVR for Cirrhotic HCV KIM NEWNHAM MN, NP CIRRHOSIS CARE CLINIC UNIVERSITY OF ALBERTA Objectives To review the benefits of HCV clearance in cirrhotic patients To review some of the emerging data
Life After SVR for Cirrhotic HCV KIM NEWNHAM MN, NP CIRRHOSIS CARE CLINIC UNIVERSITY OF ALBERTA Objectives To review the benefits of HCV clearance in cirrhotic patients To review some of the emerging data
ESLD a Guide for HIV Physicians. Marion Peters University of California San Francisco June 2015
 ESLD a Guide for HIV Physicians Marion Peters University of California San Francisco June 2015 Disclosures Honararia from Johnson and Johnson Roche Merck Gilead Spouse employee of Hoffman La Roche Natural
ESLD a Guide for HIV Physicians Marion Peters University of California San Francisco June 2015 Disclosures Honararia from Johnson and Johnson Roche Merck Gilead Spouse employee of Hoffman La Roche Natural
CIRRHOSIS Definition
 Cirrhosis Update Robert S. Brown, Jr., MD, MPH Vice Chair, Transitions of Care Interim Chief, Division of Gastroenterology & Hepatology Weill Cornell Medical College CIRRHOSIS Definition Irreversible fibrous
Cirrhosis Update Robert S. Brown, Jr., MD, MPH Vice Chair, Transitions of Care Interim Chief, Division of Gastroenterology & Hepatology Weill Cornell Medical College CIRRHOSIS Definition Irreversible fibrous
The Yellow Patient. Dr Chiradeep Raychaudhuri, Consultant Hepatologist, Hull University Teaching Hospitals NHS Trust
 The Yellow Patient Dr Chiradeep Raychaudhuri, Consultant Hepatologist, Hull University Teaching Hospitals NHS Trust there s a yellow patient in bed 40. It s one of yours. Liver Cirrhosis Why.When.What.etc.
The Yellow Patient Dr Chiradeep Raychaudhuri, Consultant Hepatologist, Hull University Teaching Hospitals NHS Trust there s a yellow patient in bed 40. It s one of yours. Liver Cirrhosis Why.When.What.etc.
The Liver for the Nonhepatologist
 The Liver for the Nonhepatologist Michael R. Charlton, MBBS, FRCP Professor of Medicine University of Chicago Chicago, Illinois Overview Initial assessment of liver disease How do you diagnose cirrhosis?
The Liver for the Nonhepatologist Michael R. Charlton, MBBS, FRCP Professor of Medicine University of Chicago Chicago, Illinois Overview Initial assessment of liver disease How do you diagnose cirrhosis?
Faculty Disclosure. Objectives. Cirrhosis Management for the Family Physician 18/11/2014
 Cirrhosis Management for the Family Physician Mang Ma, MD, FRCP Professor University of Alberta Faculty: Mang Ma Faculty Disclosure Relationships with commercial interests: Advisory Board: Merck, Gilead
Cirrhosis Management for the Family Physician Mang Ma, MD, FRCP Professor University of Alberta Faculty: Mang Ma Faculty Disclosure Relationships with commercial interests: Advisory Board: Merck, Gilead
Case Report: Refractory variceal bleeding Christophe Hézode, Henri Mondor Hospital, Paris-Est University, Créteil, France
 Case Report: Refractory variceal bleeding Christophe Hézode, Henri Mondor Hospital, Paris-Est University, Créteil, France Thank you to Marika Rudler, Dominique Thabut, Adrian Gadano, and Jaime Bosch for
Case Report: Refractory variceal bleeding Christophe Hézode, Henri Mondor Hospital, Paris-Est University, Créteil, France Thank you to Marika Rudler, Dominique Thabut, Adrian Gadano, and Jaime Bosch for
Causes of Liver Disease in US
 Learning Objectives Updates in Outpatient Cirrhosis Management Jennifer Guy, MD MAS Director, Liver Cancer Program California Pacific Medical Center guyj@sutterhealth.org Review cirrhosis epidemiology,
Learning Objectives Updates in Outpatient Cirrhosis Management Jennifer Guy, MD MAS Director, Liver Cancer Program California Pacific Medical Center guyj@sutterhealth.org Review cirrhosis epidemiology,
Diagnosi e management non invasivo dell epatite cronica da HCV
 Diagnosi e management non invasivo dell epatite cronica da HCV Giovanni Squadrito Clinical and Molecular Hepatology University of Messina gsquadrito@unime.it Outline Diagnosis of HCV Non invasive tools
Diagnosi e management non invasivo dell epatite cronica da HCV Giovanni Squadrito Clinical and Molecular Hepatology University of Messina gsquadrito@unime.it Outline Diagnosis of HCV Non invasive tools
La gestione corrente dell infezione cronica da HCV: la progressione verso la cirrosi. Simona Landonio I Div Mal inf H Sacco Milano
 La gestione corrente dell infezione cronica da HCV: la progressione verso la cirrosi Simona Landonio I Div Mal inf H Sacco Milano HCV Natural History Viganò M et al Gastroenterology 27;133:835-842 Overall
La gestione corrente dell infezione cronica da HCV: la progressione verso la cirrosi Simona Landonio I Div Mal inf H Sacco Milano HCV Natural History Viganò M et al Gastroenterology 27;133:835-842 Overall
CIRROSI E IPERTENSIONE PORTALE NELLA DONNA
 Cagliari, 16 settembre 2017 CIRROSI E IPERTENSIONE PORTALE NELLA DONNA Vincenza Calvaruso, MD, PhD Ricercatore di Gastroenterologia Gastroenterologia & Epatologia, Di.Bi.M.I.S. Università degli Studi di
Cagliari, 16 settembre 2017 CIRROSI E IPERTENSIONE PORTALE NELLA DONNA Vincenza Calvaruso, MD, PhD Ricercatore di Gastroenterologia Gastroenterologia & Epatologia, Di.Bi.M.I.S. Università degli Studi di
Evidence-Base Management of Esophageal and Gastric Varices
 Evidence-Base Management of Esophageal and Gastric Varices Rino Alvani Gani Hepatobiliary Division Department of Internal Medicine Faculty of Medicine Universitas Indonesia Cipto Mangunkusumo National
Evidence-Base Management of Esophageal and Gastric Varices Rino Alvani Gani Hepatobiliary Division Department of Internal Medicine Faculty of Medicine Universitas Indonesia Cipto Mangunkusumo National
JOURNAL PRESENTATION. Dr Tina Fan Tseung Kwan O Hospital 17 th Jan 2013
 JOURNAL PRESENTATION Dr Tina Fan Tseung Kwan O Hospital 17 th Jan 2013 THE COMBINATION OF OCTREOTIDE AND MIDODRINE IS NOT SUPERIOR TO ALBUMIN IN PREVENTING RECURRENCE OF ASCITES AFTER LARGE-VOLUME PARACENTESIS
JOURNAL PRESENTATION Dr Tina Fan Tseung Kwan O Hospital 17 th Jan 2013 THE COMBINATION OF OCTREOTIDE AND MIDODRINE IS NOT SUPERIOR TO ALBUMIN IN PREVENTING RECURRENCE OF ASCITES AFTER LARGE-VOLUME PARACENTESIS
Title: The Baveno VI criteria for predicting esophageal varices: validation in real life practice
 Title: The Baveno VI criteria for predicting esophageal varices: validation in real life practice Authors: Mafalda Sousa, Sónia Fernandes, Luísa Proença, Ana Paula Silva, Sónia Leite, Joana Silva, Ana
Title: The Baveno VI criteria for predicting esophageal varices: validation in real life practice Authors: Mafalda Sousa, Sónia Fernandes, Luísa Proença, Ana Paula Silva, Sónia Leite, Joana Silva, Ana
NON INVASIVE EVALUATION OF DISEASE PROGRESSION IN CHRONIC LIVER DISEASES
 Best of EASL -, Ethiopia 29 Sep to 01 Oct, 2016 Inaugural meeting of the Sub Saharan GI-Hepatology Working Group Incorporating Best of AGA and Best of EASL NON INVASIVE EVALUATION OF DISEASE PROGRESSION
Best of EASL -, Ethiopia 29 Sep to 01 Oct, 2016 Inaugural meeting of the Sub Saharan GI-Hepatology Working Group Incorporating Best of AGA and Best of EASL NON INVASIVE EVALUATION OF DISEASE PROGRESSION
European. Young Hepatologists Workshop. Organized by : Quantification of fibrosis and cirrhosis outcomes
 supported by from Gilea Quantification of fibrosis and cirrhosis outcomes th 5 European 5 European Young Hepatologists Workshop Young Hepatologists Workshop August, 27-29. 2015, Moulin de Vernègues Vincenza
supported by from Gilea Quantification of fibrosis and cirrhosis outcomes th 5 European 5 European Young Hepatologists Workshop Young Hepatologists Workshop August, 27-29. 2015, Moulin de Vernègues Vincenza
DISCLOSURES. This activity is jointly provided by Northwest Portland Area Indian Health Board and Cardea
 DISCLOSURES This activity is jointly provided by Northwest Portland Area Indian Health Board and Cardea Cardea Services is approved as a provider of continuing nursing education by Montana Nurses Association,
DISCLOSURES This activity is jointly provided by Northwest Portland Area Indian Health Board and Cardea Cardea Services is approved as a provider of continuing nursing education by Montana Nurses Association,
Variceal bleeding. Mainz,
 Variceal bleeding Mainz, 21.09.2008 Risk of complications 5 years 10 years Ascites 10 % 25 % HCC 10 % 25 % Bleeding < 5 % 5-10 % Enceph. < 5 % < 5 % Typical situation : Mortality 10 % to 40 % Sequence
Variceal bleeding Mainz, 21.09.2008 Risk of complications 5 years 10 years Ascites 10 % 25 % HCC 10 % 25 % Bleeding < 5 % 5-10 % Enceph. < 5 % < 5 % Typical situation : Mortality 10 % to 40 % Sequence
Worldwide Causes of HCC
 Approach to HCV Treatment in Patients with HCC Mark W. Russo, MD, MPH, FACG Carolinas HealthCare System Charlotte Worldwide Causes of HCC 60% 50% 40% 30% 20% 10% 0% 54% 31% 15% Hepatitis B Hepatitis C
Approach to HCV Treatment in Patients with HCC Mark W. Russo, MD, MPH, FACG Carolinas HealthCare System Charlotte Worldwide Causes of HCC 60% 50% 40% 30% 20% 10% 0% 54% 31% 15% Hepatitis B Hepatitis C
GI bleeding in chronic liver disease
 GI bleeding in chronic liver disease Stuart McPherson Consultant Hepatologist Liver Unit, Freeman Hospital, Newcastle upon Tyne and Institute of Cellular Medicine, Newcastle University. Case 54 year old
GI bleeding in chronic liver disease Stuart McPherson Consultant Hepatologist Liver Unit, Freeman Hospital, Newcastle upon Tyne and Institute of Cellular Medicine, Newcastle University. Case 54 year old
Prof. Mohammad Umar. MBBS, MCPS, FCPS, FACG (USA), FRCP (London), FRCP (Glasgow), FAGA
, FRCP (London), FRCP (Glasgow), FAGA") Prof. Mohammad Umar MBBS, MCPS, FCPS, FACG (USA), FRCP (London), FRCP (Glasgow), FAGA Chairman and Head Department of Medicine Rawalpindi Medical College, Rawalpindi. Consultant Gastroenterologist / Hepatologist
Prof. Mohammad Umar MBBS, MCPS, FCPS, FACG (USA), FRCP (London), FRCP (Glasgow), FAGA Chairman and Head Department of Medicine Rawalpindi Medical College, Rawalpindi. Consultant Gastroenterologist / Hepatologist
Contraindications. Indications. Complications. Currently TIPS is considered second or third line therapy for:
 Contraindications Absolute Relative Primary prevention variceal bleeding HCC if centrally located Active congestive heart failure Obstruction all hepatic veins Thomas D. Boyer, M.D. University of Arizona
Contraindications Absolute Relative Primary prevention variceal bleeding HCC if centrally located Active congestive heart failure Obstruction all hepatic veins Thomas D. Boyer, M.D. University of Arizona
MANAGEMENT OF LIVER CIRRHOSIS: PRACTICE ESSENTIALS AND PATIENT SELF-MANAGEMENT
 MANAGEMENT OF LIVER CIRRHOSIS: PRACTICE ESSENTIALS AND PATIENT SELF-MANAGEMENT Sherona Bau, ACNP The Pfleger Liver Institute 200 UCLA Medical Plaza, Suite 214 Los Angeles, CA 90095 September 30, 2017 I
MANAGEMENT OF LIVER CIRRHOSIS: PRACTICE ESSENTIALS AND PATIENT SELF-MANAGEMENT Sherona Bau, ACNP The Pfleger Liver Institute 200 UCLA Medical Plaza, Suite 214 Los Angeles, CA 90095 September 30, 2017 I
Assessment of Liver Function: Implications for HCC Treatment
 Assessment of Liver Function: Implications for HCC Treatment A/P Dan Yock Young MBBS, PhD, MRCP, MMed. FAMS Chair, University Medicine Cluster. NUHS Head, Department of Medicine, National University of
Assessment of Liver Function: Implications for HCC Treatment A/P Dan Yock Young MBBS, PhD, MRCP, MMed. FAMS Chair, University Medicine Cluster. NUHS Head, Department of Medicine, National University of
Evaluating HIV Patient for Liver Transplantation. Marion G. Peters, MD Professor of Medicine University of California San Francisco USA
 Evaluating HIV Patient for Liver Transplantation Marion G. Peters, MD Professor of Medicine University of California San Francisco USA Slide 2 ESLD and HIV Liver disease has become a major cause of death
Evaluating HIV Patient for Liver Transplantation Marion G. Peters, MD Professor of Medicine University of California San Francisco USA Slide 2 ESLD and HIV Liver disease has become a major cause of death
Worldwide Causes of HCC
 Approach to HCV Treatment in Patients with HCC JORGE L. HERRERA, MD, MACG UNIVERSITY OF SOUTH ALABAMA COLLEGE OF MEDICINE Worldwide Causes of HCC 60% 50% 40% 54% 30% 20% 10% 31% 15% 0% Hepatitis B Hepatitis
Approach to HCV Treatment in Patients with HCC JORGE L. HERRERA, MD, MACG UNIVERSITY OF SOUTH ALABAMA COLLEGE OF MEDICINE Worldwide Causes of HCC 60% 50% 40% 54% 30% 20% 10% 31% 15% 0% Hepatitis B Hepatitis
New York State HCV Provider Webinar Series
 New York State HCV Provider Webinar Series Overview of Fibrosis-Staging, Child s Pugh, MELD Scores Paul J Gaglio, MD, FACP, AGAF, FAASLD Director: Hepatology Outreach Professor of Medicine (in Surgery)
New York State HCV Provider Webinar Series Overview of Fibrosis-Staging, Child s Pugh, MELD Scores Paul J Gaglio, MD, FACP, AGAF, FAASLD Director: Hepatology Outreach Professor of Medicine (in Surgery)
Cirrhosis is different from Fibrosis
 Riunione Monotematica AISF 2016 «The Future of Liver Disease: Beyond HCV is there a Role for Hepatologist» Milan 13 th -14 th 2016 Cirrhosis is different from Fibrosis I have not disclosures to declare
Riunione Monotematica AISF 2016 «The Future of Liver Disease: Beyond HCV is there a Role for Hepatologist» Milan 13 th -14 th 2016 Cirrhosis is different from Fibrosis I have not disclosures to declare
Complications of Cirrhosis
 Complications of Cirrhosis Causes of Cirrhosis Alcohol Chronic Viral Hepatitis (B/C) Haemochromatosis Autoimmune Hepatitis NAFLD/NASH Primary Biliary Cirrhosis Primary Sclerosing Cholangitis 1-AT deficiency
Complications of Cirrhosis Causes of Cirrhosis Alcohol Chronic Viral Hepatitis (B/C) Haemochromatosis Autoimmune Hepatitis NAFLD/NASH Primary Biliary Cirrhosis Primary Sclerosing Cholangitis 1-AT deficiency
REVIEW. Ariel W. Aday, M.D.,* Nicole E. Rich, M.D.,* Arjmand R. Mufti, M.D., and Shannan R. Tujios, M.D.
 REVIEW CON ( The Window Is Closed ): In Patients With Cirrhosis With Ascites, the Clinical Risks of Nonselective beta-blocker Outweigh the Benefits and Should NOT Be Prescribed Ariel W. Aday, M.D.,* Nicole
REVIEW CON ( The Window Is Closed ): In Patients With Cirrhosis With Ascites, the Clinical Risks of Nonselective beta-blocker Outweigh the Benefits and Should NOT Be Prescribed Ariel W. Aday, M.D.,* Nicole
Non-Invasive Testing for Liver Fibrosis
 NORTHWEST AIDS EDUCATION AND TRAINING CENTER Non-Invasive Testing for Liver Fibrosis John Scott, MD, MSc Associate Professor, University of Washington Associate Clinic Director, Hep/Liver Clinic, Harborview
NORTHWEST AIDS EDUCATION AND TRAINING CENTER Non-Invasive Testing for Liver Fibrosis John Scott, MD, MSc Associate Professor, University of Washington Associate Clinic Director, Hep/Liver Clinic, Harborview
Management of Chronic Liver Failure/Cirrhosis Complications in Hospitals. By: Dr. Kevin Dolehide
 Management of Chronic Liver Failure/Cirrhosis Complications in Hospitals By: Dr. Kevin Dolehide Overview DX Cirrhosis and Prognosis Compensated Decompensated Complications Of Cirrhosis Management Of Complications
Management of Chronic Liver Failure/Cirrhosis Complications in Hospitals By: Dr. Kevin Dolehide Overview DX Cirrhosis and Prognosis Compensated Decompensated Complications Of Cirrhosis Management Of Complications
Norepinephrine versus Terlipressin for the Treatment of Hepatorenal Syndrome
 Norepinephrine versus Terlipressin for the Treatment of Hepatorenal Syndrome Disclosure I have no conflicts of interest to disclose Name: Margarita Taburyanskaya Title: PharmD, PGY1 Pharmacy Practice Resident
Norepinephrine versus Terlipressin for the Treatment of Hepatorenal Syndrome Disclosure I have no conflicts of interest to disclose Name: Margarita Taburyanskaya Title: PharmD, PGY1 Pharmacy Practice Resident
Carvedilol or Propranolol in the Management of Portal Hypertension?
 Evidence Based Case Report Carvedilol or Propranolol in the Management of Portal Hypertension? Arranged by: dr. Saskia Aziza Nursyirwan RESIDENCY PROGRAM OF INTERNAL MEDICINE DEPARTMENT UNIVERSITY OF INDONESIA
Evidence Based Case Report Carvedilol or Propranolol in the Management of Portal Hypertension? Arranged by: dr. Saskia Aziza Nursyirwan RESIDENCY PROGRAM OF INTERNAL MEDICINE DEPARTMENT UNIVERSITY OF INDONESIA
Viral Hepatitis The Preventive Potential of Antiviral Therapy. Thomas Berg
 Viral Hepatitis The Preventive Potential of Antiviral Therapy Thomas Berg Therapeutic and preventive strategies in patients with hepatitis virus infection Treatment of acute infection Treatment of chronic
Viral Hepatitis The Preventive Potential of Antiviral Therapy Thomas Berg Therapeutic and preventive strategies in patients with hepatitis virus infection Treatment of acute infection Treatment of chronic
Conflict of interest disclosures. Complications of end stage liver disease. None. The many complications of Cirrhosis. Portal Hypertension.
 Complications of end stage liver disease Conflict of interest disclosures None Amir Qamar, MD Instructor of Medicine Brigham and Women s s Hospital Harvard Medical School Boston, MA 02115 The many complications
Complications of end stage liver disease Conflict of interest disclosures None Amir Qamar, MD Instructor of Medicine Brigham and Women s s Hospital Harvard Medical School Boston, MA 02115 The many complications
Treatment of chronic hepatitis delta Case report
 Treatment of chronic hepatitis delta Case report George Papatheodoridis Professor in Medicine & Gastroenterology Medical School of National and Kapodistrian University of Athens, Director of Academic Department
Treatment of chronic hepatitis delta Case report George Papatheodoridis Professor in Medicine & Gastroenterology Medical School of National and Kapodistrian University of Athens, Director of Academic Department
ANTIVIRAL THERAPY FOR HCV. Alfredo Alberti
 CLINICAL IMPACT OF SVR AFTER ANTIVIRAL THERAPY FOR HCV Alfredo Alberti Department of Histology,Microbiology and Medical Biotechnologies Molecular Hepatology Unit Venetian Institute of Molecular Medicine
CLINICAL IMPACT OF SVR AFTER ANTIVIRAL THERAPY FOR HCV Alfredo Alberti Department of Histology,Microbiology and Medical Biotechnologies Molecular Hepatology Unit Venetian Institute of Molecular Medicine
Hepatorenal syndrome. Jan T. Kielstein Departent of Nephrology Medical School Hannover
 Hepatorenal syndrome Jan T. Kielstein Departent of Nephrology Medical School Hannover Hepatorenal Syndrome 1) History of HRS 2) Pathophysiology of HRS 3) Definition of HRS 4) Clinical presentation of HRS
Hepatorenal syndrome Jan T. Kielstein Departent of Nephrology Medical School Hannover Hepatorenal Syndrome 1) History of HRS 2) Pathophysiology of HRS 3) Definition of HRS 4) Clinical presentation of HRS
Research Elastography: Liver
 Research Elastography: Liver Giovanna Ferraioli EFSUMB Ultrasound Learning Center Ultrasound Unit - Infectious Diseases Dept. Fondazione IRCCS Policlinico S. Matteo Medical School University of Pavia,
Research Elastography: Liver Giovanna Ferraioli EFSUMB Ultrasound Learning Center Ultrasound Unit - Infectious Diseases Dept. Fondazione IRCCS Policlinico S. Matteo Medical School University of Pavia,
Treating now vs. post transplant
 Resistance with treatment failure Treating now vs. post transplant Pros (for treating pre transplant) If SVR efficacy means Better quality of life Removal from waiting list No post transplant recurrence
Resistance with treatment failure Treating now vs. post transplant Pros (for treating pre transplant) If SVR efficacy means Better quality of life Removal from waiting list No post transplant recurrence
CLINICAL How Should a Hospitalized Patient with Newly Diagnosed Cirrhosis Be Evaluated and Managed?
 CLINICAL How Should a Hospitalized Patient with Newly Diagnosed Cirrhosis Be Evaluated and Managed? The Hospitalist. 2016 August;2016(8) Author(s): Raj Sehgal, MD; Joshua Hanson, MD, MPH; Division OF The
CLINICAL How Should a Hospitalized Patient with Newly Diagnosed Cirrhosis Be Evaluated and Managed? The Hospitalist. 2016 August;2016(8) Author(s): Raj Sehgal, MD; Joshua Hanson, MD, MPH; Division OF The
The place of bariatric surgery in NASH: can we extend the indications? - No
 The place of bariatric surgery in NASH: can we extend the indications? - No Nicolas Goossens Service de Gastroentérologie & Hépatologie Hôpitaux Universitaires de Genève Genève, Suisse How to extend the
The place of bariatric surgery in NASH: can we extend the indications? - No Nicolas Goossens Service de Gastroentérologie & Hépatologie Hôpitaux Universitaires de Genève Genève, Suisse How to extend the
Cases: Treatment of Hepatitis C in Patients with Cirrhosis and Advanced Liver Disease
 Slide 1 of 20 Cases: Treatment of Hepatitis C in Patients with Cirrhosis and Advanced Liver Disease Kenneth E. Sherman, MD, PhD Gould Professor of Medicine Director, Division of Digestive Diseases University
Slide 1 of 20 Cases: Treatment of Hepatitis C in Patients with Cirrhosis and Advanced Liver Disease Kenneth E. Sherman, MD, PhD Gould Professor of Medicine Director, Division of Digestive Diseases University
The Management of Ascites & Hepatorenal Syndrome. Florence Wong University of Toronto. Falk Symposium March 14, 2008
 The Management of Ascites & Hepatorenal Syndrome Florence Wong University of Toronto Falk Symposium March 14, 2008 Management of Ascites Sodium Restriction Mandatory at all stages of ascites in order to
The Management of Ascites & Hepatorenal Syndrome Florence Wong University of Toronto Falk Symposium March 14, 2008 Management of Ascites Sodium Restriction Mandatory at all stages of ascites in order to
th Annual AISF Meeting 44 th th th, 2011 Rome, February 23 rd -26
 44 th 44 th Annual AISF Meeting Rome, February 23 rd -26 th th, 2011 Update on the Baveno Consensus Conference Roberto de Franchis Department of of Clinical Sciences, University of of Milan, Head, Gastroenterology
44 th 44 th Annual AISF Meeting Rome, February 23 rd -26 th th, 2011 Update on the Baveno Consensus Conference Roberto de Franchis Department of of Clinical Sciences, University of of Milan, Head, Gastroenterology
The New World of HCV Therapy
 HCV: Assessing the Patient Prior to Treatment: Diagnostic Testing and Strategy JORGE L. HERRERA, MD, MACG UNIVERSITY OF SOUTH ALABAMA COLLEGE OF MEDICINE, MOBILE, AL The New World of HCV Therapy Interferon-free
HCV: Assessing the Patient Prior to Treatment: Diagnostic Testing and Strategy JORGE L. HERRERA, MD, MACG UNIVERSITY OF SOUTH ALABAMA COLLEGE OF MEDICINE, MOBILE, AL The New World of HCV Therapy Interferon-free
The Future is Here Now!
 HCV Treatment: Assessing the Patient Prior to Treatment. How Will This Change in the Future? JORGE L. HERRERA M.D., FACG UNIVERSITY OF SOUTH ALABAMA COLLEGE OF MEDICINE, MOBILE, AL The Future is Here Now!
HCV Treatment: Assessing the Patient Prior to Treatment. How Will This Change in the Future? JORGE L. HERRERA M.D., FACG UNIVERSITY OF SOUTH ALABAMA COLLEGE OF MEDICINE, MOBILE, AL The Future is Here Now!
Hepatorenal Syndrome
 Necker Seminars in Nephrology Institut Pasteur Paris, April 22, 2013 Hepatorenal Syndrome Dr. Richard Moreau 1 INSERM U773, Centre de Recherche Biomédicale Bichat-Beaujon CRB3, 2 Université Paris Diderot
Necker Seminars in Nephrology Institut Pasteur Paris, April 22, 2013 Hepatorenal Syndrome Dr. Richard Moreau 1 INSERM U773, Centre de Recherche Biomédicale Bichat-Beaujon CRB3, 2 Université Paris Diderot
Module 1 Introduction of hepatitis
 Module 1 Introduction of hepatitis 1 Training Objectives At the end of the module, trainees will be able to ; Demonstrate improved knowledge of the global epidemiology of the viral hepatitis Understand
Module 1 Introduction of hepatitis 1 Training Objectives At the end of the module, trainees will be able to ; Demonstrate improved knowledge of the global epidemiology of the viral hepatitis Understand
Hepatology for the Nonhepatologist
 Hepatology for the Nonhepatologist Kenneth E. Sherman, MD, PhD Gould Professor of Medicine Director, Division of Digestive Diseases University of Cincinnati College of Medicine Cincinnati, Ohio Learning
Hepatology for the Nonhepatologist Kenneth E. Sherman, MD, PhD Gould Professor of Medicine Director, Division of Digestive Diseases University of Cincinnati College of Medicine Cincinnati, Ohio Learning
A. Purpose and Scope of the Guidance PRACTICE GUIDANCE HEPATOLOGY, VOL. 65, NO. 1, 2017
 AMERICAN ASSOCIATION FOR THE STUDY OFLIVERD I S E ASES PRACTICE GUIDANCE HEPATOLOGY, VOL. 65, NO. 1, 2017 Portal Hypertensive Bleeding in Cirrhosis: Risk Stratification, Diagnosis, and Management: 2016
AMERICAN ASSOCIATION FOR THE STUDY OFLIVERD I S E ASES PRACTICE GUIDANCE HEPATOLOGY, VOL. 65, NO. 1, 2017 Portal Hypertensive Bleeding in Cirrhosis: Risk Stratification, Diagnosis, and Management: 2016
The New World of HCV Therapy
 HCV: Assessing the Patient Prior to Treatment: Diagnostic Testing and Strategy JORGE L. HERRERA M.D., MACG UNIVERSITY OF SOUTH ALABAMA COLLEGE OF MEDICINE, MOBILE, AL The New World of HCV Therapy Interferon-free
HCV: Assessing the Patient Prior to Treatment: Diagnostic Testing and Strategy JORGE L. HERRERA M.D., MACG UNIVERSITY OF SOUTH ALABAMA COLLEGE OF MEDICINE, MOBILE, AL The New World of HCV Therapy Interferon-free
3 Workshop on HCV THERAPY ADVANCES New Antivirals in Clinical Practice
 3 Workshop on HCV THERAPY ADVANCES New Antivirals in Clinical Practice Rome, 13 December 2013 Management and monitoring of HCC in the future era of DAA s Prof. Massimo Colombo Chairman Department of Liver,
3 Workshop on HCV THERAPY ADVANCES New Antivirals in Clinical Practice Rome, 13 December 2013 Management and monitoring of HCC in the future era of DAA s Prof. Massimo Colombo Chairman Department of Liver,
Hepatocytes produce. Proteins Clotting factors Hormones. Bile Flow
 R.J.Bailey MD Hepatocytes produce Proteins Clotting factors Hormones Bile Flow Trouble.. for the liver! Trouble for the Liver Liver Gall Bladder Common Alcohol Hep C Fatty Liver Cancer Drugs Viruses Uncommon
R.J.Bailey MD Hepatocytes produce Proteins Clotting factors Hormones Bile Flow Trouble.. for the liver! Trouble for the Liver Liver Gall Bladder Common Alcohol Hep C Fatty Liver Cancer Drugs Viruses Uncommon
VARICEAL BLEEDING. Ram Subramanian MD Hepatology & Critical Care Medical Director of Liver Transplant Emory University, Atlanta.
 VARICEAL BLEEDING Ram Subramanian MD Hepatology & Critical Care Medical Director of Liver Transplant Emory University, Atlanta Disclosures: None OUTLINE Pathophysiology of portal hypertension Splanchnic
VARICEAL BLEEDING Ram Subramanian MD Hepatology & Critical Care Medical Director of Liver Transplant Emory University, Atlanta Disclosures: None OUTLINE Pathophysiology of portal hypertension Splanchnic
Evaluation of liver and spleen stiffness using a ultrasound guided method: Accuracy of ARFI(R) measurements in liver disease patients
 measurements in liver disease patients") Evaluation of liver and spleen stiffness using a ultrasound guided method: Accuracy of ARFI(R) measurements in liver disease patients Poster No.: C-3242 Congress: ECR 2010 Type: Topic: Authors: Keywords:
Evaluation of liver and spleen stiffness using a ultrasound guided method: Accuracy of ARFI(R) measurements in liver disease patients Poster No.: C-3242 Congress: ECR 2010 Type: Topic: Authors: Keywords:
ACG & AASLD Joint Clinical Guideline: Prevention and Management of Gastroesophageal Varices and Variceal Hemorrhage in Cirrhosis
 ACG & AASLD Joint Clinical Guideline: Prevention and Management of Gastroesophageal Varices and Variceal Hemorrhage in Cirrhosis Guadalupe Garcia-Tsao, M.D., 1 Arun J. Sanyal, M.D., 2 Norman D. Grace,
ACG & AASLD Joint Clinical Guideline: Prevention and Management of Gastroesophageal Varices and Variceal Hemorrhage in Cirrhosis Guadalupe Garcia-Tsao, M.D., 1 Arun J. Sanyal, M.D., 2 Norman D. Grace,
Top Hepatology Findings/Papers of 2013
 Top Hepatology Findings/Papers of 2013 David Nelson, MD, FACG Assistant Vice President for Research Director, Clinical and Translational Science Institute University of Florida FGS/ACG meeting 3/28/14
Top Hepatology Findings/Papers of 2013 David Nelson, MD, FACG Assistant Vice President for Research Director, Clinical and Translational Science Institute University of Florida FGS/ACG meeting 3/28/14
INCIDENCE OF BACTERIAL INFECTIONS IN CIRRHOSIS
 INCIDENCE OF BACTERIAL INFECTIONS IN CIRRHOSIS Yoshida H et al (1993)* Deschenes M et al (1999)** Strauss E et al (1993) Borzio M et al (2002) PATIENTS 1140 140 170 405 INFECTIONS 15.4% 20% 47% 34% * Many
INCIDENCE OF BACTERIAL INFECTIONS IN CIRRHOSIS Yoshida H et al (1993)* Deschenes M et al (1999)** Strauss E et al (1993) Borzio M et al (2002) PATIENTS 1140 140 170 405 INFECTIONS 15.4% 20% 47% 34% * Many
PORTAL HYPERTENSION An Introduction to the Culprit of Many Liver Failure Complications
 PORTAL HYPERTENSION An Introduction to the Culprit of Many Liver Failure Complications Edy G. Trujillo, RN, MSN, ACNP-BC Liver Transplant RRUCLA Medical Center July 31, 2018 What Do We All Look Forward
PORTAL HYPERTENSION An Introduction to the Culprit of Many Liver Failure Complications Edy G. Trujillo, RN, MSN, ACNP-BC Liver Transplant RRUCLA Medical Center July 31, 2018 What Do We All Look Forward
Clinical Trials & Endpoints in NASH Cirrhosis
 Clinical Trials & Endpoints in NASH Cirrhosis April 25, 2018 Peter G. Traber, MD CEO & CMO, Galectin Therapeutics 2018 Galectin Therapeutics NASDAQ: GALT For more information, see galectintherapeutics.com
Clinical Trials & Endpoints in NASH Cirrhosis April 25, 2018 Peter G. Traber, MD CEO & CMO, Galectin Therapeutics 2018 Galectin Therapeutics NASDAQ: GALT For more information, see galectintherapeutics.com
Invasive. Sampling error. Interobserver variability. Nondynamic evaluation of
 How to assess liver fibrosis Serum markers or FibroScan vs. liver biopsy? Laurent CASTERA & Pierre BEDOSSA Hôpital Beaujon, AP-HP, Clichy Université Paris-VII France 4 th Paris Hepatitis Conference, Paris,
How to assess liver fibrosis Serum markers or FibroScan vs. liver biopsy? Laurent CASTERA & Pierre BEDOSSA Hôpital Beaujon, AP-HP, Clichy Université Paris-VII France 4 th Paris Hepatitis Conference, Paris,
Management of the Cirrhotic Patient in the ICU
 Management of the Cirrhotic Patient in the ICU Peter E. Morris, MD Professor & Chief, Pulmonary, Critical Care and Sleep Medicine University of Kentucky Conflict of Interest Funding US National Institutes
Management of the Cirrhotic Patient in the ICU Peter E. Morris, MD Professor & Chief, Pulmonary, Critical Care and Sleep Medicine University of Kentucky Conflict of Interest Funding US National Institutes
Filippo Schepis, MD Università degli Studi di Modena e Reggio Emilia
 Filippo Schepis, MD Università degli Studi di Modena e Reggio Emilia Il sottoscritto dichiara di non aver avuto/di aver avuto negli ultimi 12 mesi conflitto d interesse in relazione a questa presentazione
Filippo Schepis, MD Università degli Studi di Modena e Reggio Emilia Il sottoscritto dichiara di non aver avuto/di aver avuto negli ultimi 12 mesi conflitto d interesse in relazione a questa presentazione
Liver stiffness predicts liver related events and mortality in HIV/HCV coinfected patients
 Liver stiffness predicts liver related events and mortality in HIV/HCV coinfected patients José Vicente Fernández-Montero, Pablo Barreiro, Eugenia Vispo, Pablo Labarga, Francisco Blanco, Fernanda Rick,
Liver stiffness predicts liver related events and mortality in HIV/HCV coinfected patients José Vicente Fernández-Montero, Pablo Barreiro, Eugenia Vispo, Pablo Labarga, Francisco Blanco, Fernanda Rick,
Care of the Patient With Cirrhosis
 REVIEW Care of the Patient With Cirrhosis Anitha Yadav, M.D., and Hugo E. Vargas, M.D. Caring for patients with cirrhosis involves multidisciplinary and timely management of several complications while
REVIEW Care of the Patient With Cirrhosis Anitha Yadav, M.D., and Hugo E. Vargas, M.D. Caring for patients with cirrhosis involves multidisciplinary and timely management of several complications while
NON INVASIVE ASSESSMENT OF LIVER FIBROSIS : FIBROSCAN
 NON INVASIVE ASSESSMENT OF LIVER FIBROSIS : FIBROSCAN M. Beaugrand Service d Hépatologied Hopital J. Verdier BONDY 93143 et Université Paris XIII MAINZ 21.09.2008 ASSESSMENT OF FIBROSIS : WHY? Management
NON INVASIVE ASSESSMENT OF LIVER FIBROSIS : FIBROSCAN M. Beaugrand Service d Hépatologied Hopital J. Verdier BONDY 93143 et Université Paris XIII MAINZ 21.09.2008 ASSESSMENT OF FIBROSIS : WHY? Management
Protocol for daclatasvir (Daklinza ) Approved October 2015 (updated February 2018)
 Approved October 2015 (updated February 2018)") PREFERRED AGENTS: (See drug specific NOTES for exceptions.) Protocol for daclatasvir (Daklinza ) Approved October 2015 (updated February 2018) https://providers.amerigroup.com For genotype 1, Mavyret and
PREFERRED AGENTS: (See drug specific NOTES for exceptions.) Protocol for daclatasvir (Daklinza ) Approved October 2015 (updated February 2018) https://providers.amerigroup.com For genotype 1, Mavyret and
When to Treat: Staging Liver Disease David L. Thomas, MD, MPH
 When to Treat: Staging Liver Disease David L. Thomas, MD, MPH Professor of Medicine Johns Hopkins School of Medicine Disclosures Received royalties from UpToDate, Inc. Staging refers to the assessment
When to Treat: Staging Liver Disease David L. Thomas, MD, MPH Professor of Medicine Johns Hopkins School of Medicine Disclosures Received royalties from UpToDate, Inc. Staging refers to the assessment
Case 4: A 61-year-old man with HCV genotype 3 with cirrhosis. Ira M. Jacobson, M.D. Weill Cornell Medical College New York, New York USA
 Case 4: A 61-year-old man with HCV genotype 3 with cirrhosis Ira M. Jacobson, M.D. Weill Cornell Medical College New York, New York USA 1 Genotype 3 case 61-year-old man with HCV genotype 3 Cirrhosis on
Case 4: A 61-year-old man with HCV genotype 3 with cirrhosis Ira M. Jacobson, M.D. Weill Cornell Medical College New York, New York USA 1 Genotype 3 case 61-year-old man with HCV genotype 3 Cirrhosis on
Evaluation of liver and spleen stiffness using a ultrasound guided method: Accuracy of ARFI(R) measurements in liver disease patients
 measurements in liver disease patients") Evaluation of liver and spleen stiffness using a ultrasound guided method: Accuracy of ARFI(R) measurements in liver disease patients Poster No.: C-3242 Congress: ECR 2010 Type: Topic: Authors: Keywords:
Evaluation of liver and spleen stiffness using a ultrasound guided method: Accuracy of ARFI(R) measurements in liver disease patients Poster No.: C-3242 Congress: ECR 2010 Type: Topic: Authors: Keywords:
Hepatitis C: New Antivirals in the Liver Transplant Setting. Maria Carlota Londoño Liver Unit Hospital Clínic Barcelona
 Hepatitis C: New Antivirals in the Liver Transplant Setting Maria Carlota Londoño Liver Unit Hospital Clínic Barcelona Patient survival Hepatitis C and Liver Transplantation Years after transplantation
Hepatitis C: New Antivirals in the Liver Transplant Setting Maria Carlota Londoño Liver Unit Hospital Clínic Barcelona Patient survival Hepatitis C and Liver Transplantation Years after transplantation