The Yellow Patient. Dr Chiradeep Raychaudhuri, Consultant Hepatologist, Hull University Teaching Hospitals NHS Trust
|
|
|
- Loraine George
- 5 years ago
- Views:
Transcription


1 The Yellow Patient Dr Chiradeep Raychaudhuri, Consultant Hepatologist, Hull University Teaching Hospitals NHS Trust
2 there s a yellow patient in bed 40. It s one of yours.
3 Liver Cirrhosis Why.When.What.etc. Compensated and Decompensated. Clinical states Acute on Chronic Liver Failure. Management of Common Complications.
4 Definition Liver cirrhosis is anatomically defined as a diffuse process with fibrosis and nodule formation. It is the end result of the fibrogenesis that occurs with chronic liver injury Although causes are many, the end result of fibrogenesis is the same Can be compensated or decompensated Cirrhosis and End-stage liver disease ARE NOT THE SAME THING!!
5 Causes Alcohol Non-alcoholic fatty liver disease Viral Hepatitis: B/C/D Haemochromatosis Autoimmune: AIH, PBC, PSC Drugs: Methotrexate, Amiodarone Alpha 1 Antitrypsin deficiency
6 Scores Child-Pugh MELD and MELD-Na UKELD CLIF-OF and CLIF-ACLF
7 Cirrhosis is typically classified as compensated or decompensated, based on the absence or presence (or previous history) of Variceal bleeding Ascites Jaundice Hepatic encephalopathy Compensated patients have Significantly longer survivals Usually asymptomatic Much better quality of life The transition from compensated asymptomatic cirrhosis to decompensated cirrhosis occurs at a rate of about 5-7% per year Once decompensation occurs, cirrhosis becomes a systemic disease Decompensation represents a prognostic watershed wherein median survival drops from 12 years to about 2 years
8 Where and how does things go wrong Cirrhosis Portal Hypertension Bacterial translocation Peripheral arterial vasodilatation End-organ damage Hyperdynamic circulation Splanchnic vasodilatation Cardiovascular dysfunction Release of proinflammatory molecules
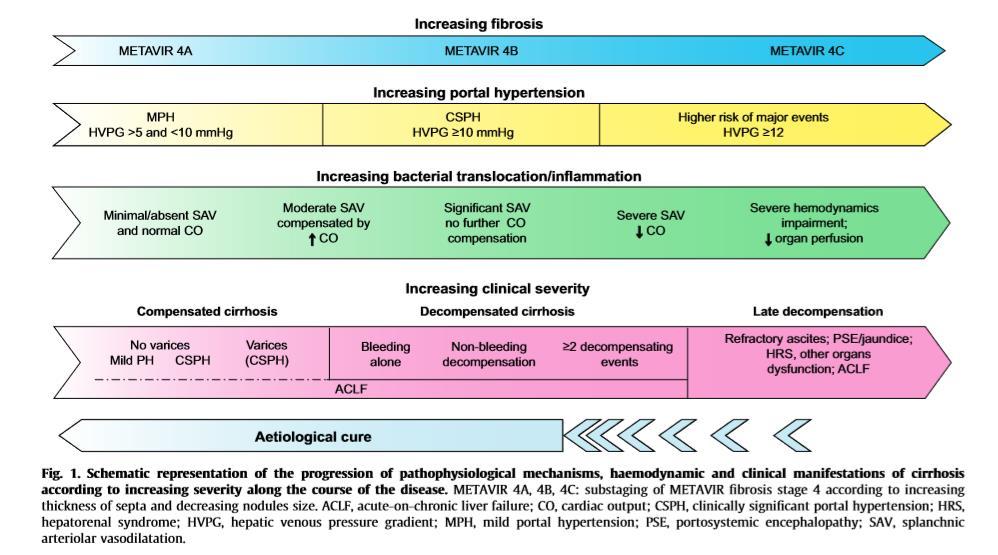
9 Clinically significant portal hypertension (CSPH) This is defined by a Hepatic venous pressure gradient (HVPG) 10mmHg Development of gastro-oesophageal varices and decompensation usually doesn t happen below CSPH Histological stages of cirrhosis run parallel to the progression of portal hypertension and clinical states of disease
10 Clinical states of Cirrhosis Stage 0: Compensated cirrhosis without CSPH Stage 1: Compensated cirrhosis with CSPH but without varices Stage 2: Compensated cirrhosis with varices Stage 3: Variceal bleed (only) Stage 4: First non-bleed decompensation Stage 5: Further decompensation Stage 6: Late advanced decompensation (End Stage Liver Disease) refractory ascites, infections, persistent encephalopathy, jaundice, renal/circulatory/respiratory dysfunction
11 Stage of Cirrhosis 0/1 Low 5 year Risks 2 Death before decompensation 10% Variceal bleeding 8% Single non-bleed decompensation 20% 3 Death before other complications 18-20% Re-bleed before other decompensation 19% Further decompensation 45-54% 4 Death before further decompensation 25% 5 5 year mortality up to 88% 6 1 Year Mortality 60-80%
12
 Precipitating events vary between populations and may include: Bacterial infections (30 57% of cases) Active alcohol intake or")
13 Acute on Chronic Liver Failure (ACLF) ACLF is characterised by acute decompensation, organ failure(s) and high short term mortality It may occur in previously compensated or decompensated cirrhosis Major cause of death in patients with cirrhosis (50% mortality rate) Precipitating events vary between populations and may include: Bacterial infections (30 57% of cases) Active alcohol intake or alcohol binge Reactivation of HBV Superimposed HAV and HEV infection
14 Chronic liver failure organ failure score system 1 Organ/system 1 point 2 points 3 points Liver (bilirubin, mg/dl) <6 6 < Kidney (creatinine, mg/dl) < < or renal replacement Brain/HE (West Haven Criteria) Grade 0 Grades 1 2 Grades 3 4 Coagulation (INR, PLT count) < < Circulation (MAP, mmhg and vasopressors) 70 <70 Use of vasopressors Lungs PaO 2 /FiO 2, or > > SpO 2 /FiO 2 >357 > Grades of ACLF NO ACLF ACLF 1a ACLF 1b ACLF II ACLF III Clinical characteristics No organ failure, or single non-kidney organ failure, creatinine <1.5 mg/dl, no HE Single renal failure Single non-kidney organ failure, creatinine mg/dl and/or HE grade 1 2 Two organ failures Three or more organ failures


15 App Hull Audit: 30-day mortality was significantly greater in those with ACLF than without (71% vs 12% :p <0.001)
16 Management of ACLF Management of precipitants where possible Organ support and management of complications ITU involvement Involve Gastroenterology/Hepatology early
17 Common Complications
18 Ascites Most common complication Impacts quality of life, both work and social Frequently leads to hospitalisation Development of ascites in patients with cirrhosis is associated with a poor prognosis 1-year mortality: 40% 2-year mortality: 50% Ascites is uncomplicated when not infected, refractory or associated with impairment of renal function Can lead to other complications such as SBP and renal failure There are other causes of ascites.
19 Grading of Ascites Grade 1 Mild ascites: only detectable by ultrasound examination Grade 2 Moderate ascites: manifest by moderate symmetrical distension of abdomen Grade 3 Large or gross ascites: provokes marked abdominal distension
20 Management of ascites Diagnostic tap (deranged clotting/low platelets not a contra-indication) Moderate sodium restriction (no added salts/avoid prepared meals) Grade 1 value of pharmacotherapy unknown Grade 2 Hospitalisation not required First episode of uncomplicated Grade 2 ascites, start spironolactone 100mg OD aiming for weight loss of 0.5kg per day (no oedema) to 1kg/day (oedema+) Monitor U&Es post diuretic Review in 72 hours Grade 3 - LVP
21 Variceal Bleed 2 nd most common decompensating event Resuscitate A B C Do not over-transfuse Hb 7-8 Terlipressin + Antibiotics Early scope
22 Spontaneous Bacterial Peritonitis Fluid neutrophil >250 May or may not have clinical signs and symptoms Early diagnosis and treatment has reduced mortality form 90% when first described to 20% now Antibiotics as per local protocol, if high clinical suspicion then don t wait for results (particularly out of hours) Albumin significantly decreases the incidence of type-1 hepatorenal syndrome and reduces mortality The administration of albumin recommended in patients with SBP 1.5 g/kg at diagnosis and 1 g/kg on Day 3

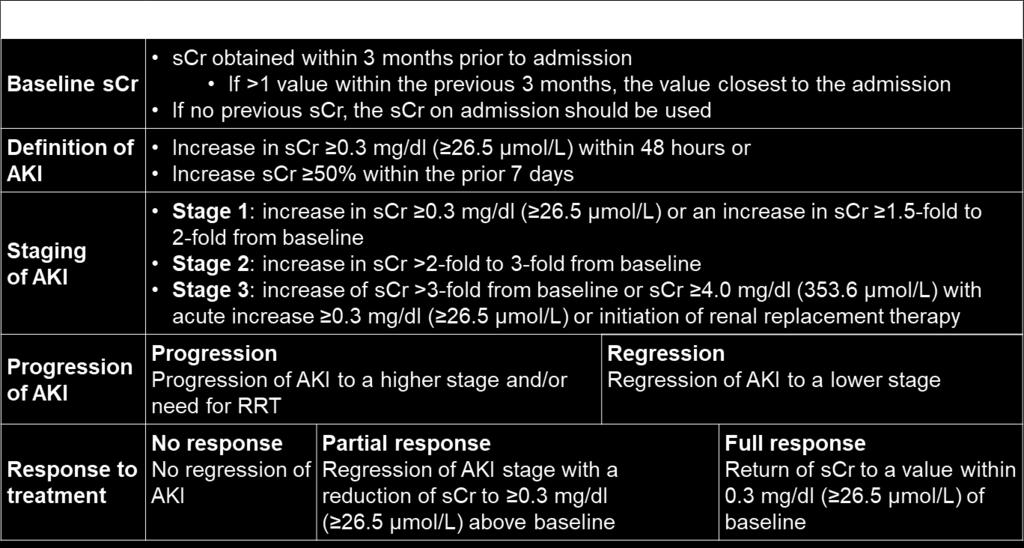
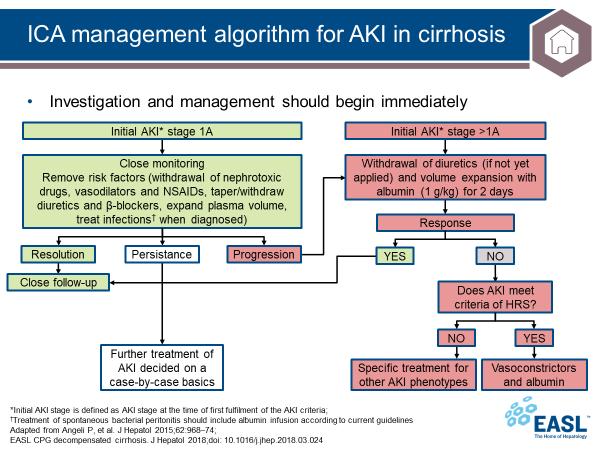
23 Renal Failure
24
25 ICA diagnostic criteria for HRS-AKI Cirrhosis and ascites Diagnosis of AKI according to ICA-AKI criteria No response after 2 consecutive days of diuretic withdrawal and plasma volume expansion with albumin 1 g per kg of body weight Absence of shock No current or recent use of nephrotoxic drugs (NSAIDs, aminoglycosides, iodinated contrast media, etc.) No macroscopic signs of structural kidney injury,* defined as: Absence of proteinuria (>500 mg/day) Absence of microhaematuria (>50 RBCs per high power field) Normal findings on renal ultrasonography
26 Management of Type 1 HRS Terlipressin 1mg iv QDS, to be reviewed after 48 hours and can be increased to 2mg QDS Albumin 20-40g per day Monitor renal function daily
27 Hyponatraemia Sodium <130 Associated with increased mortality and morbidity Review drugs Volume status assessment and management Hepatic encephalopathy Look for precipitating factors Review drugs Avoid/stop opiates/benzodiazepines Lactulose first line 20-30mls TDS aiming for 3 soft/loose stools per day (NG if too drowsy for oral intake) Phosphate enema Rifaximin
28 Take home messages Proper assessment Don t miss ACLF Look for infection Correct volume status Review drugs Urgent USS Check AFP, particularly in patients who suddenly decompensate for no apparent reason NUTRITION
29

30
CONTROLLED DOCUMENT. Cirrhosis Care Bundle CATEGORY: Clinical Guidelines. CLASSIFICATION: Clinical. Controlled Document CG201 Number:
 Cirrhosis Care Bundle CONTROLLED DOCUMENT CATEGORY: Clinical Guidelines CLASSIFICATION: Clinical Controlled Document CG201 Number: Version Number: 1 Controlled Document Clinical Guidelines Group Sponsor:
Cirrhosis Care Bundle CONTROLLED DOCUMENT CATEGORY: Clinical Guidelines CLASSIFICATION: Clinical Controlled Document CG201 Number: Version Number: 1 Controlled Document Clinical Guidelines Group Sponsor:
Complications of Cirrhosis
 Complications of Cirrhosis Causes of Cirrhosis Alcohol Chronic Viral Hepatitis (B/C) Haemochromatosis Autoimmune Hepatitis NAFLD/NASH Primary Biliary Cirrhosis Primary Sclerosing Cholangitis 1-AT deficiency
Complications of Cirrhosis Causes of Cirrhosis Alcohol Chronic Viral Hepatitis (B/C) Haemochromatosis Autoimmune Hepatitis NAFLD/NASH Primary Biliary Cirrhosis Primary Sclerosing Cholangitis 1-AT deficiency
Management of Ascites and Hepatorenal Syndrome. Florence Wong University of Toronto. June 4, /16/ Gore & Associates: Consultancy
 Management of Ascites and Hepatorenal Syndrome Florence Wong University of Toronto June 4, 2016 6/16/2016 1 Disclosures Gore & Associates: Consultancy Sequana Medical: Research Funding Mallinckrodt Pharmaceutical:
Management of Ascites and Hepatorenal Syndrome Florence Wong University of Toronto June 4, 2016 6/16/2016 1 Disclosures Gore & Associates: Consultancy Sequana Medical: Research Funding Mallinckrodt Pharmaceutical:
Hepatorenal Syndrome
 Necker Seminars in Nephrology Institut Pasteur Paris, April 22, 2013 Hepatorenal Syndrome Dr. Richard Moreau 1 INSERM U773, Centre de Recherche Biomédicale Bichat-Beaujon CRB3, 2 Université Paris Diderot
Necker Seminars in Nephrology Institut Pasteur Paris, April 22, 2013 Hepatorenal Syndrome Dr. Richard Moreau 1 INSERM U773, Centre de Recherche Biomédicale Bichat-Beaujon CRB3, 2 Université Paris Diderot
HEPATOrenal Syndrome Type I: Correct Diagnosis = Correct Management
 HEPATOrenal Syndrome Type I: Correct Diagnosis = Correct Management Stephen G. M. Wong BSc, BSc(Med), MD, MHSc, FRCPC Associate Professor of Medicine Director, Hepatology Education Section of Hepatology
HEPATOrenal Syndrome Type I: Correct Diagnosis = Correct Management Stephen G. M. Wong BSc, BSc(Med), MD, MHSc, FRCPC Associate Professor of Medicine Director, Hepatology Education Section of Hepatology
Decompensated chronic liver disease
 Decompensated chronic liver disease Definition of decompensated chronic liver disease Patients with chronic liver disease can present with acute decompensation due to various causes. The decompensation
Decompensated chronic liver disease Definition of decompensated chronic liver disease Patients with chronic liver disease can present with acute decompensation due to various causes. The decompensation
GI bleeding in chronic liver disease
 GI bleeding in chronic liver disease Stuart McPherson Consultant Hepatologist Liver Unit, Freeman Hospital, Newcastle upon Tyne and Institute of Cellular Medicine, Newcastle University. Case 54 year old
GI bleeding in chronic liver disease Stuart McPherson Consultant Hepatologist Liver Unit, Freeman Hospital, Newcastle upon Tyne and Institute of Cellular Medicine, Newcastle University. Case 54 year old
Norepinephrine versus Terlipressin for the Treatment of Hepatorenal Syndrome
 Norepinephrine versus Terlipressin for the Treatment of Hepatorenal Syndrome Disclosure I have no conflicts of interest to disclose Name: Margarita Taburyanskaya Title: PharmD, PGY1 Pharmacy Practice Resident
Norepinephrine versus Terlipressin for the Treatment of Hepatorenal Syndrome Disclosure I have no conflicts of interest to disclose Name: Margarita Taburyanskaya Title: PharmD, PGY1 Pharmacy Practice Resident
Management of the Cirrhotic Patient in the ICU
 Management of the Cirrhotic Patient in the ICU Peter E. Morris, MD Professor & Chief, Pulmonary, Critical Care and Sleep Medicine University of Kentucky Conflict of Interest Funding US National Institutes
Management of the Cirrhotic Patient in the ICU Peter E. Morris, MD Professor & Chief, Pulmonary, Critical Care and Sleep Medicine University of Kentucky Conflict of Interest Funding US National Institutes
Management of Acute Decompensation of Cirrhosis JOHN O GRADY KING S COLLEGE HOSPITAL
 Management of Acute Decompensation of Cirrhosis JOHN O GRADY KING S COLLEGE HOSPITAL Terminology Acute decompensation of cirrhosis - stable patient with sudden deterioration Acute-on-chronic liver failure
Management of Acute Decompensation of Cirrhosis JOHN O GRADY KING S COLLEGE HOSPITAL Terminology Acute decompensation of cirrhosis - stable patient with sudden deterioration Acute-on-chronic liver failure
Hepatology on the AMU
 Hepatology on the AMU RCP day, 8 th February 2018 Jo Leithead Consultant in Hepatology and Liver Transplantation Addenbrookes Hospital Cambridge Is liver disease relevant to me? Williams R, Lancet 2014
Hepatology on the AMU RCP day, 8 th February 2018 Jo Leithead Consultant in Hepatology and Liver Transplantation Addenbrookes Hospital Cambridge Is liver disease relevant to me? Williams R, Lancet 2014
Sign up to receive ATOTW weekly -
 HEPATORENAL SYNDROME ANAESTHESIA TUTORIAL OF THE WEEK 240 10 TH SEPTEMBER 2011 Gerry Lynch Rotherham General Hospital Correspondence to gerry.lynch@rothgen.nhs.uk QUESTIONS Before continuing, try to answer
HEPATORENAL SYNDROME ANAESTHESIA TUTORIAL OF THE WEEK 240 10 TH SEPTEMBER 2011 Gerry Lynch Rotherham General Hospital Correspondence to gerry.lynch@rothgen.nhs.uk QUESTIONS Before continuing, try to answer
Hepatocytes produce. Proteins Clotting factors Hormones. Bile Flow
 R.J.Bailey MD Hepatocytes produce Proteins Clotting factors Hormones Bile Flow Trouble.. for the liver! Trouble for the Liver Liver Gall Bladder Common Alcohol Hep C Fatty Liver Cancer Drugs Viruses Uncommon
R.J.Bailey MD Hepatocytes produce Proteins Clotting factors Hormones Bile Flow Trouble.. for the liver! Trouble for the Liver Liver Gall Bladder Common Alcohol Hep C Fatty Liver Cancer Drugs Viruses Uncommon
Management of Cirrhosis Related Complications
 Management of Cirrhosis Related Complications Ke-Qin Hu, MD, FAASLD Professor of Clinical Medicine Director of Hepatology University of California, Irvine Disclosure I have no disclosure related to this
Management of Cirrhosis Related Complications Ke-Qin Hu, MD, FAASLD Professor of Clinical Medicine Director of Hepatology University of California, Irvine Disclosure I have no disclosure related to this
Cirrhosis and Portal Hypertension Gastroenterology Teaching Project American Gastroenterological Association
 CIRRHOSIS AND PORTAL HYPERTENSION Cirrhosis and Portal Hypertension Gastroenterology Teaching Project American Gastroenterological Association WHAT IS CIRRHOSIS? What is Cirrhosis? DEFINITION OF CIRRHOSIS
CIRRHOSIS AND PORTAL HYPERTENSION Cirrhosis and Portal Hypertension Gastroenterology Teaching Project American Gastroenterological Association WHAT IS CIRRHOSIS? What is Cirrhosis? DEFINITION OF CIRRHOSIS
King s College Hospital NHS Foundation Trust. Acute on Chronic Liver Failure: Practical management outside the tertiary centre.
 King s College Hospital NHS Foundation Trust NHS Acute on Chronic Liver Failure: Practical management outside the tertiary centre. William Bernal Professor of Liver Critical Care Liver Intensive Therapy
King s College Hospital NHS Foundation Trust NHS Acute on Chronic Liver Failure: Practical management outside the tertiary centre. William Bernal Professor of Liver Critical Care Liver Intensive Therapy
Management of Cirrhotic Complications Uncontrolled Ascites. Siwaporn Chainuvati, MD Siriraj Hospital Mahidol University
 Management of Cirrhotic Complications Uncontrolled Ascites Siwaporn Chainuvati, MD Siriraj Hospital Mahidol University Topic Definition, pathogenesis Current therapeutic options Experimental treatments
Management of Cirrhotic Complications Uncontrolled Ascites Siwaporn Chainuvati, MD Siriraj Hospital Mahidol University Topic Definition, pathogenesis Current therapeutic options Experimental treatments
Beta-blockers in cirrhosis: Cons
 Beta-blockers in cirrhosis: Cons Eric Trépo MD, PhD Dept. of Gastroenterology. Hepatopancreatology and Digestive Oncology. C.U.B. Hôpital Erasme. Université Libre de Bruxelles. Bruxelles. Belgium Laboratory
Beta-blockers in cirrhosis: Cons Eric Trépo MD, PhD Dept. of Gastroenterology. Hepatopancreatology and Digestive Oncology. C.U.B. Hôpital Erasme. Université Libre de Bruxelles. Bruxelles. Belgium Laboratory
ACUTE-ON-CHRONIC LIVER FAILURE: DEFINITION, DIAGNOSIS AND CLINICAL CHARACTERISTICS.
 ACUTE-ON-CHRONIC LIVER FAILURE: DEFINITION, DIAGNOSIS AND CLINICAL CHARACTERISTICS. Vicente Arroyo 1, 2, Rajiv Jalan 2, 3 1 Institut de Investigacions Biomèdiques August Pi I Sunyer. University of Barcelona.
ACUTE-ON-CHRONIC LIVER FAILURE: DEFINITION, DIAGNOSIS AND CLINICAL CHARACTERISTICS. Vicente Arroyo 1, 2, Rajiv Jalan 2, 3 1 Institut de Investigacions Biomèdiques August Pi I Sunyer. University of Barcelona.
End-Stage Liver Disease (ESLD): A Guide for HIV Physicians
: A Guide for HIV Physicians") Slide 1 of 32 End-Stage Liver Disease (ESLD): A Guide for HIV Physicians Marion G. Peters, MD John V. Carbone, MD, Endowed Chair Professor of Medicine Chief of Hepatology Research University of California
Slide 1 of 32 End-Stage Liver Disease (ESLD): A Guide for HIV Physicians Marion G. Peters, MD John V. Carbone, MD, Endowed Chair Professor of Medicine Chief of Hepatology Research University of California
Ascites Management. Atif Zaman, MD MPH Oregon Health & Science University Professor of Medicine Division of Gastroenterology and Hepatology
 Ascites Management Atif Zaman, MD MPH Oregon Health & Science University Professor of Medicine Division of Gastroenterology and Hepatology Disclosure 1. The speaker Atif Zaman, MD MPH have no relevant
Ascites Management Atif Zaman, MD MPH Oregon Health & Science University Professor of Medicine Division of Gastroenterology and Hepatology Disclosure 1. The speaker Atif Zaman, MD MPH have no relevant
CIRRHOSIS Definition
 Cirrhosis Update Robert S. Brown, Jr., MD, MPH Vice Chair, Transitions of Care Interim Chief, Division of Gastroenterology & Hepatology Weill Cornell Medical College CIRRHOSIS Definition Irreversible fibrous
Cirrhosis Update Robert S. Brown, Jr., MD, MPH Vice Chair, Transitions of Care Interim Chief, Division of Gastroenterology & Hepatology Weill Cornell Medical College CIRRHOSIS Definition Irreversible fibrous
WEEK. MPharm Programme. Liver Biochemistry. Slide 1 of 49 MPHM14 Liver Biochemistry
 MPharm Programme Liver Biochemistry Slide 1 of 49 MPHM Liver Biochemistry Learning Outcomes Assess and evaluate the signs and symptoms of illness Assess and critically appraise a patients medication regimen,
MPharm Programme Liver Biochemistry Slide 1 of 49 MPHM Liver Biochemistry Learning Outcomes Assess and evaluate the signs and symptoms of illness Assess and critically appraise a patients medication regimen,
European. Young Hepatologists Workshop. Organized by : Quantification of fibrosis and cirrhosis outcomes
 supported by from Gilea Quantification of fibrosis and cirrhosis outcomes th 5 European 5 European Young Hepatologists Workshop Young Hepatologists Workshop August, 27-29. 2015, Moulin de Vernègues Vincenza
supported by from Gilea Quantification of fibrosis and cirrhosis outcomes th 5 European 5 European Young Hepatologists Workshop Young Hepatologists Workshop August, 27-29. 2015, Moulin de Vernègues Vincenza
Optimal management of ascites
 Optimal management of ascites P. Angeli, Dept. of Medicine, Unit of Internal Medicine and epatology (), University of Padova (Italy) pangeli@unipd.it 10th Paris epatology Conference National Conference
Optimal management of ascites P. Angeli, Dept. of Medicine, Unit of Internal Medicine and epatology (), University of Padova (Italy) pangeli@unipd.it 10th Paris epatology Conference National Conference
Liver failure &portal hypertension
 Liver failure &portal hypertension Objectives: by the end of this lecture each student should be able to : Diagnose liver failure (acute or chronic) List the causes of acute liver failure Diagnose and
Liver failure &portal hypertension Objectives: by the end of this lecture each student should be able to : Diagnose liver failure (acute or chronic) List the causes of acute liver failure Diagnose and
Acute Liver Failure. Neil Shah, MD UNC School of Medicine High-Impact Hepatology Saturday, Dec 8 th, 2018
 Acute Liver Failure Neil Shah, MD UNC School of Medicine High-Impact Hepatology Saturday, Dec 8 th, 2018 Disclosures None Outline Overview of ALF Management of ALF Diagnosis of ALF Treatments and Support
Acute Liver Failure Neil Shah, MD UNC School of Medicine High-Impact Hepatology Saturday, Dec 8 th, 2018 Disclosures None Outline Overview of ALF Management of ALF Diagnosis of ALF Treatments and Support
Steps in Assessing Fibrosis 4/30/2015. Overview of Liver Disease Associated With HCV
 Overview of Liver Disease Associated With HCV Marion G. Peters, MD John V. Carbone, Endowed Chair Professor of Medicine Chief of Hepatology Research University of California San Francisco San Francisco,
Overview of Liver Disease Associated With HCV Marion G. Peters, MD John V. Carbone, Endowed Chair Professor of Medicine Chief of Hepatology Research University of California San Francisco San Francisco,
ESLD a Guide for HIV Physicians. Marion Peters University of California San Francisco June 2015
 ESLD a Guide for HIV Physicians Marion Peters University of California San Francisco June 2015 Disclosures Honararia from Johnson and Johnson Roche Merck Gilead Spouse employee of Hoffman La Roche Natural
ESLD a Guide for HIV Physicians Marion Peters University of California San Francisco June 2015 Disclosures Honararia from Johnson and Johnson Roche Merck Gilead Spouse employee of Hoffman La Roche Natural
Faculty Disclosure. Objectives. Cirrhosis Management for the Family Physician 18/11/2014
 Cirrhosis Management for the Family Physician Mang Ma, MD, FRCP Professor University of Alberta Faculty: Mang Ma Faculty Disclosure Relationships with commercial interests: Advisory Board: Merck, Gilead
Cirrhosis Management for the Family Physician Mang Ma, MD, FRCP Professor University of Alberta Faculty: Mang Ma Faculty Disclosure Relationships with commercial interests: Advisory Board: Merck, Gilead
Definition: fibrosis and nodular regeneration resulting from hepatocellular injury
 Cirrhosis Understanding the liver: Patterns of LFT Abnormalities - Hepatocellular/Transaminitis: o Ratio of AST: ALT >2:1 ETOH (keep in mind AST is also produced by red cells, heart muscle) o If Aminotransferases
Cirrhosis Understanding the liver: Patterns of LFT Abnormalities - Hepatocellular/Transaminitis: o Ratio of AST: ALT >2:1 ETOH (keep in mind AST is also produced by red cells, heart muscle) o If Aminotransferases
Chronic Hepatic Disease
 Chronic Hepatic Disease 10 th Leading Cause of Death Liver Functions Energy Metabolism Protein Synthesis Solubilization, Transport, and Storage Protects and Clears drugs, damaged cells Causes of Liver
Chronic Hepatic Disease 10 th Leading Cause of Death Liver Functions Energy Metabolism Protein Synthesis Solubilization, Transport, and Storage Protects and Clears drugs, damaged cells Causes of Liver
Patterns of abnormal LFTs and their differential diagnosis
 Patterns of abnormal LFTs and their differential diagnosis Professor Matthew Cramp South West Liver Unit and Peninsula Schools of Medicine and Dentistry, Plymouth Outline liver function tests / tests of
Patterns of abnormal LFTs and their differential diagnosis Professor Matthew Cramp South West Liver Unit and Peninsula Schools of Medicine and Dentistry, Plymouth Outline liver function tests / tests of
Approved regimens for cirrhotic patients
 5th Workshop on HCV THERAPY ADVANCES New antivirals in clinical practice Approved regimens for cirrhotic patients Amsterdam, 4-5 december 2015 Disease burden in Spain 400000 350000 300000 F0 Peak cirrhosis
5th Workshop on HCV THERAPY ADVANCES New antivirals in clinical practice Approved regimens for cirrhotic patients Amsterdam, 4-5 december 2015 Disease burden in Spain 400000 350000 300000 F0 Peak cirrhosis
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Accelerated intravascular coagulation and fibrinolysis (AICF) in liver disease, 390 391 Acid suppression in liver disease, 403 404 ACLF.
Index Note: Page numbers of article titles are in boldface type. A Accelerated intravascular coagulation and fibrinolysis (AICF) in liver disease, 390 391 Acid suppression in liver disease, 403 404 ACLF.
MANAGEMENT OF LIVER CIRRHOSIS: PRACTICE ESSENTIALS AND PATIENT SELF-MANAGEMENT
 MANAGEMENT OF LIVER CIRRHOSIS: PRACTICE ESSENTIALS AND PATIENT SELF-MANAGEMENT Sherona Bau, ACNP The Pfleger Liver Institute 200 UCLA Medical Plaza, Suite 214 Los Angeles, CA 90095 September 30, 2017 I
MANAGEMENT OF LIVER CIRRHOSIS: PRACTICE ESSENTIALS AND PATIENT SELF-MANAGEMENT Sherona Bau, ACNP The Pfleger Liver Institute 200 UCLA Medical Plaza, Suite 214 Los Angeles, CA 90095 September 30, 2017 I
PACT module Acute hepatic failure. Intensive Care Training Program Radboud University Medical Centre Nijmegen
 PACT module Acute hepatic failure Intensive Care Training Program Radboud University Medical Centre Nijmegen Acute Liver Failure Acute on Chronic Liver Failure Acute loss of hepatocellular function in
PACT module Acute hepatic failure Intensive Care Training Program Radboud University Medical Centre Nijmegen Acute Liver Failure Acute on Chronic Liver Failure Acute loss of hepatocellular function in
Patterns of abnormal LFTs and their differential diagnosis
 Patterns of abnormal LFTs and their differential diagnosis Professor Matthew Cramp South West Liver Unit and Peninsula Schools of Medicine and Dentistry, Plymouth Outline liver function / liver function
Patterns of abnormal LFTs and their differential diagnosis Professor Matthew Cramp South West Liver Unit and Peninsula Schools of Medicine and Dentistry, Plymouth Outline liver function / liver function
Topics to be covered
 Caring for the patient with cirrhosis Role of the hospitalist Danielle Brandman, MD, MAS Associate Professor of Clinical Medicine Associate Program Director, Transplant Hepatology Fellowship October 18,
Caring for the patient with cirrhosis Role of the hospitalist Danielle Brandman, MD, MAS Associate Professor of Clinical Medicine Associate Program Director, Transplant Hepatology Fellowship October 18,
EDUCATION PRACTICE. Management of Refractory Ascites. Clinical Scenario. The Problem
 CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2005;3:1187 1191 EDUCATION PRACTICE Management of Refractory Ascites ANDRÉS CÁRDENAS and PERE GINÈS Liver Unit, Institute of Digestive Diseases, Hospital Clínic,
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2005;3:1187 1191 EDUCATION PRACTICE Management of Refractory Ascites ANDRÉS CÁRDENAS and PERE GINÈS Liver Unit, Institute of Digestive Diseases, Hospital Clínic,
DISEASE LEVEL MEDICAL EVIDENCE PROTOCOL
 DISEASE LEVEL MEDICAL EVIDENCE PROTOCOL 1. This Protocol sets out the medical evidence that must be delivered to the Administrator for proof of Disease Level. It is subject to such further and other Protocols
DISEASE LEVEL MEDICAL EVIDENCE PROTOCOL 1. This Protocol sets out the medical evidence that must be delivered to the Administrator for proof of Disease Level. It is subject to such further and other Protocols
The Continuum of Care for Advanced Liver Disease: Partnering with the Liver Specialist. K V Speeg, MD, PhD UT Health San Antonio
 The Continuum of Care for Advanced Liver Disease: Partnering with the Liver Specialist K V Speeg, MD, PhD UT Health San Antonio Objectives Review staging of liver disease Review consequences of end-stage
The Continuum of Care for Advanced Liver Disease: Partnering with the Liver Specialist K V Speeg, MD, PhD UT Health San Antonio Objectives Review staging of liver disease Review consequences of end-stage
Contraindications. Indications. Complications. Currently TIPS is considered second or third line therapy for:
 Contraindications Absolute Relative Primary prevention variceal bleeding HCC if centrally located Active congestive heart failure Obstruction all hepatic veins Thomas D. Boyer, M.D. University of Arizona
Contraindications Absolute Relative Primary prevention variceal bleeding HCC if centrally located Active congestive heart failure Obstruction all hepatic veins Thomas D. Boyer, M.D. University of Arizona
Alcoholic Hepatitis: Routine Screening for Early Recognition and Management. Juan Guerrero, MD
 Alcoholic Hepatitis: Routine Screening for Early Recognition and Management Juan Guerrero, MD Global Problem 1% of GNP of medium/high income countries Additional societal costs Disproportionately affects
Alcoholic Hepatitis: Routine Screening for Early Recognition and Management Juan Guerrero, MD Global Problem 1% of GNP of medium/high income countries Additional societal costs Disproportionately affects
Etiology of liver cirrhosis
 Liver cirrhosis 1 Liver cirrhosis Liver cirrhosis is the progressive replacement of normal hepatic cells by fibrous scar tissue, This scarring is accompanied by the loss of viable hepatocytes, which are
Liver cirrhosis 1 Liver cirrhosis Liver cirrhosis is the progressive replacement of normal hepatic cells by fibrous scar tissue, This scarring is accompanied by the loss of viable hepatocytes, which are
CIRROSI E IPERTENSIONE PORTALE NELLA DONNA
 Cagliari, 16 settembre 2017 CIRROSI E IPERTENSIONE PORTALE NELLA DONNA Vincenza Calvaruso, MD, PhD Ricercatore di Gastroenterologia Gastroenterologia & Epatologia, Di.Bi.M.I.S. Università degli Studi di
Cagliari, 16 settembre 2017 CIRROSI E IPERTENSIONE PORTALE NELLA DONNA Vincenza Calvaruso, MD, PhD Ricercatore di Gastroenterologia Gastroenterologia & Epatologia, Di.Bi.M.I.S. Università degli Studi di
Module 1 Introduction of hepatitis
 Module 1 Introduction of hepatitis 1 Training Objectives At the end of the module, trainees will be able to ; Demonstrate improved knowledge of the global epidemiology of the viral hepatitis Understand
Module 1 Introduction of hepatitis 1 Training Objectives At the end of the module, trainees will be able to ; Demonstrate improved knowledge of the global epidemiology of the viral hepatitis Understand
JOURNAL PRESENTATION. Dr Tina Fan Tseung Kwan O Hospital 17 th Jan 2013
 JOURNAL PRESENTATION Dr Tina Fan Tseung Kwan O Hospital 17 th Jan 2013 THE COMBINATION OF OCTREOTIDE AND MIDODRINE IS NOT SUPERIOR TO ALBUMIN IN PREVENTING RECURRENCE OF ASCITES AFTER LARGE-VOLUME PARACENTESIS
JOURNAL PRESENTATION Dr Tina Fan Tseung Kwan O Hospital 17 th Jan 2013 THE COMBINATION OF OCTREOTIDE AND MIDODRINE IS NOT SUPERIOR TO ALBUMIN IN PREVENTING RECURRENCE OF ASCITES AFTER LARGE-VOLUME PARACENTESIS
CHAPTER 1. Alcoholic Liver Disease
 CHAPTER 1 Alcoholic Liver Disease Major Lesions of Alcoholic Liver Disease Alcoholic fatty liver - >90% of binge and chronic drinkers Alcoholic hepatitis precursor of cirrhosis Alcoholic cirrhosis end
CHAPTER 1 Alcoholic Liver Disease Major Lesions of Alcoholic Liver Disease Alcoholic fatty liver - >90% of binge and chronic drinkers Alcoholic hepatitis precursor of cirrhosis Alcoholic cirrhosis end
Management of Chronic Liver Failure/Cirrhosis Complications in Hospitals. By: Dr. Kevin Dolehide
 Management of Chronic Liver Failure/Cirrhosis Complications in Hospitals By: Dr. Kevin Dolehide Overview DX Cirrhosis and Prognosis Compensated Decompensated Complications Of Cirrhosis Management Of Complications
Management of Chronic Liver Failure/Cirrhosis Complications in Hospitals By: Dr. Kevin Dolehide Overview DX Cirrhosis and Prognosis Compensated Decompensated Complications Of Cirrhosis Management Of Complications
Program Disclosure. This program is supported by an educational grant from Salix Pharmaceuticals.
 Program Disclosure This activity has been planned and implemented in accordance with the Essential Areas and Policies of the Accreditation Council for Continuing Medical Education (ACCME) through the sponsorship
Program Disclosure This activity has been planned and implemented in accordance with the Essential Areas and Policies of the Accreditation Council for Continuing Medical Education (ACCME) through the sponsorship
Investigations before OLT, Immunosuppression and rejection, Follow up after OLT.
 Investigations before OLT, Immunosuppression and rejection, Follow up after OLT andrea.degottardi@insel.ch When is liver transplantation indicated? When is liver transplantation indicated? Frequent: CIRRHOSIS
Investigations before OLT, Immunosuppression and rejection, Follow up after OLT andrea.degottardi@insel.ch When is liver transplantation indicated? When is liver transplantation indicated? Frequent: CIRRHOSIS
INCIDENCE OF BACTERIAL INFECTIONS IN CIRRHOSIS
 INCIDENCE OF BACTERIAL INFECTIONS IN CIRRHOSIS Yoshida H et al (1993)* Deschenes M et al (1999)** Strauss E et al (1993) Borzio M et al (2002) PATIENTS 1140 140 170 405 INFECTIONS 15.4% 20% 47% 34% * Many
INCIDENCE OF BACTERIAL INFECTIONS IN CIRRHOSIS Yoshida H et al (1993)* Deschenes M et al (1999)** Strauss E et al (1993) Borzio M et al (2002) PATIENTS 1140 140 170 405 INFECTIONS 15.4% 20% 47% 34% * Many
CLINICAL How Should a Hospitalized Patient with Newly Diagnosed Cirrhosis Be Evaluated and Managed?
 CLINICAL How Should a Hospitalized Patient with Newly Diagnosed Cirrhosis Be Evaluated and Managed? The Hospitalist. 2016 August;2016(8) Author(s): Raj Sehgal, MD; Joshua Hanson, MD, MPH; Division OF The
CLINICAL How Should a Hospitalized Patient with Newly Diagnosed Cirrhosis Be Evaluated and Managed? The Hospitalist. 2016 August;2016(8) Author(s): Raj Sehgal, MD; Joshua Hanson, MD, MPH; Division OF The
Infections In Cirrhotic patients. Dr Abid Suddle Institute of Liver Studies King s College Hospital
 Infections In Cirrhotic patients Dr Abid Suddle Institute of Liver Studies King s College Hospital Infection in cirrhotic patients Leading cause morbidity/mortality Common: 30-40% of hospitalised cirrhotic
Infections In Cirrhotic patients Dr Abid Suddle Institute of Liver Studies King s College Hospital Infection in cirrhotic patients Leading cause morbidity/mortality Common: 30-40% of hospitalised cirrhotic
Conflict of interest disclosures. Complications of end stage liver disease. None. The many complications of Cirrhosis. Portal Hypertension.
 Complications of end stage liver disease Conflict of interest disclosures None Amir Qamar, MD Instructor of Medicine Brigham and Women s s Hospital Harvard Medical School Boston, MA 02115 The many complications
Complications of end stage liver disease Conflict of interest disclosures None Amir Qamar, MD Instructor of Medicine Brigham and Women s s Hospital Harvard Medical School Boston, MA 02115 The many complications
Hepatology for the Nonhepatologist
 Hepatology for the Nonhepatologist Kenneth E. Sherman, MD, PhD Gould Professor of Medicine Director, Division of Digestive Diseases University of Cincinnati College of Medicine Cincinnati, Ohio Learning
Hepatology for the Nonhepatologist Kenneth E. Sherman, MD, PhD Gould Professor of Medicine Director, Division of Digestive Diseases University of Cincinnati College of Medicine Cincinnati, Ohio Learning
LIVER CIRRHOSIS. The liver extracts nutrients from the blood and processes them for later use.
 LIVER CIRRHOSIS William Sanchez, M.D. & Jayant A. Talwalkar, M.D., M.P.H. Advanced Liver Disease Study Group Miles and Shirley Fiterman Center for Digestive Diseases Mayo College of Medicine Rochester,
LIVER CIRRHOSIS William Sanchez, M.D. & Jayant A. Talwalkar, M.D., M.P.H. Advanced Liver Disease Study Group Miles and Shirley Fiterman Center for Digestive Diseases Mayo College of Medicine Rochester,
Hepatorenal syndrome. Jan T. Kielstein Departent of Nephrology Medical School Hannover
 Hepatorenal syndrome Jan T. Kielstein Departent of Nephrology Medical School Hannover Hepatorenal Syndrome 1) History of HRS 2) Pathophysiology of HRS 3) Definition of HRS 4) Clinical presentation of HRS
Hepatorenal syndrome Jan T. Kielstein Departent of Nephrology Medical School Hannover Hepatorenal Syndrome 1) History of HRS 2) Pathophysiology of HRS 3) Definition of HRS 4) Clinical presentation of HRS
Pharmacology in Liver Disease. Sandeep Whitehead Advanced Clinical Pharmacist Hepatology and Liver Transplant
 Pharmacology in Liver Disease Sandeep Whitehead Advanced Clinical Pharmacist Hepatology and Liver Transplant Objectives Outline the drug management for patients with: Ascites Spontaneous Bacterial Peritonitis
Pharmacology in Liver Disease Sandeep Whitehead Advanced Clinical Pharmacist Hepatology and Liver Transplant Objectives Outline the drug management for patients with: Ascites Spontaneous Bacterial Peritonitis
The Liver for the Nonhepatologist
 The Liver for the Nonhepatologist Michael R. Charlton, MBBS, FRCP Professor of Medicine University of Chicago Chicago, Illinois Overview Initial assessment of liver disease How do you diagnose cirrhosis?
The Liver for the Nonhepatologist Michael R. Charlton, MBBS, FRCP Professor of Medicine University of Chicago Chicago, Illinois Overview Initial assessment of liver disease How do you diagnose cirrhosis?
VARICEAL BLEEDING. Ram Subramanian MD Hepatology & Critical Care Medical Director of Liver Transplant Emory University, Atlanta.
 VARICEAL BLEEDING Ram Subramanian MD Hepatology & Critical Care Medical Director of Liver Transplant Emory University, Atlanta Disclosures: None OUTLINE Pathophysiology of portal hypertension Splanchnic
VARICEAL BLEEDING Ram Subramanian MD Hepatology & Critical Care Medical Director of Liver Transplant Emory University, Atlanta Disclosures: None OUTLINE Pathophysiology of portal hypertension Splanchnic
Initial approach to ascites
 Ascites: Filling and Draining the Water Balloon Common Pathogenesis in Refractory Ascites, Hyponatremia, and Cirrhosis intrahepatic resistance sinusoidal portal hypertension Splanchnic vasodilation (effective
Ascites: Filling and Draining the Water Balloon Common Pathogenesis in Refractory Ascites, Hyponatremia, and Cirrhosis intrahepatic resistance sinusoidal portal hypertension Splanchnic vasodilation (effective
The Management of Ascites & Hepatorenal Syndrome. Florence Wong University of Toronto. Falk Symposium March 14, 2008
 The Management of Ascites & Hepatorenal Syndrome Florence Wong University of Toronto Falk Symposium March 14, 2008 Management of Ascites Sodium Restriction Mandatory at all stages of ascites in order to
The Management of Ascites & Hepatorenal Syndrome Florence Wong University of Toronto Falk Symposium March 14, 2008 Management of Ascites Sodium Restriction Mandatory at all stages of ascites in order to
COMPLICATIONS OF CIRRHOSIS: ASCITES & HEPATIC ENCEPHALOPATHY
 COMPLICATIONS OF CIRRHOSIS: ASCITES & HEPATIC ENCEPHALOPATHY DR. ESTER YAGUDAYEVA CLINICAL PHARMACIST HOSPICE PHARMACY SOLUTIONS OBJECTIVES Understand the prognosis of End Stage Liver Disease (ESLD) Identify
COMPLICATIONS OF CIRRHOSIS: ASCITES & HEPATIC ENCEPHALOPATHY DR. ESTER YAGUDAYEVA CLINICAL PHARMACIST HOSPICE PHARMACY SOLUTIONS OBJECTIVES Understand the prognosis of End Stage Liver Disease (ESLD) Identify
Transplant Hepatology
 Transplant Hepatology Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of the certified
Transplant Hepatology Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of the certified
Korean Multicenter Cohort Study of Acute-on- Chronic Liver Failure : Korean Acute-on-Chronic Liver Failure Study (KACLiF)
") 2015 KASL Single Topic Symposium Korean Multicenter Cohort Study of Acute-on- Chronic Liver Failure : Korean Acute-on-Chronic Liver Failure Study (KACLiF) Do Seon Song Department of Internal Medicine,
2015 KASL Single Topic Symposium Korean Multicenter Cohort Study of Acute-on- Chronic Liver Failure : Korean Acute-on-Chronic Liver Failure Study (KACLiF) Do Seon Song Department of Internal Medicine,
MANAGING END STAGE LIVER DISEASE IN RESOURCE LIMITED SETTINGS
 MANAGING END STAGE LIVER DISEASE IN RESOURCE LIMITED SETTINGS Mark W. Sonderup Division of Hepatology and Liver Laboratory Department of Medicine University of Cape Town & Groote Schuur Hospital Cirrhosis..
MANAGING END STAGE LIVER DISEASE IN RESOURCE LIMITED SETTINGS Mark W. Sonderup Division of Hepatology and Liver Laboratory Department of Medicine University of Cape Town & Groote Schuur Hospital Cirrhosis..
EASL-EORTC Guidelines
 Pamplona, junio de 2008 CLINICAL PRACTICE GUIDELINES: PARADIGMS IN MANAGEMENT OF HCC EASL-EORTC Guidelines Bruno Sangro Clínica Universidad de Navarra. CIBERehd. Pamplona, Spain Levels of Evidence according
Pamplona, junio de 2008 CLINICAL PRACTICE GUIDELINES: PARADIGMS IN MANAGEMENT OF HCC EASL-EORTC Guidelines Bruno Sangro Clínica Universidad de Navarra. CIBERehd. Pamplona, Spain Levels of Evidence according
4/3/2014. Elizabeth Thompson, PharmD April Understand the importance of the liver and basic physiology.
 Liver Disease Elizabeth Thompson, PharmD thompse@sarmc.org April 2014 Objectives Understand the importance of the liver and basic physiology. Review hepatic disorders Recognize liver function scoring systems
Liver Disease Elizabeth Thompson, PharmD thompse@sarmc.org April 2014 Objectives Understand the importance of the liver and basic physiology. Review hepatic disorders Recognize liver function scoring systems
BREAK 11:10-11:
 1. Sepsis Tom Heaps 09:30-10:20 2. Oncological Emergencies Clare Pollard 10:20-11:10 ------------------------ BREAK 11:10-11:30 ------------------------ 3. Diabetic Ketoacidosis Tom Heaps 11:30-12:20 4.
1. Sepsis Tom Heaps 09:30-10:20 2. Oncological Emergencies Clare Pollard 10:20-11:10 ------------------------ BREAK 11:10-11:30 ------------------------ 3. Diabetic Ketoacidosis Tom Heaps 11:30-12:20 4.
CLIF Consortium. Protocol of the CLIF Acute-oN-ChrONic LIver Failure in Cirrhosis (CANONIC) Core Study
 Core Study") CLIF Consortium Protocol of the CLIF Acute-oN-ChrONic LIver Failure in Cirrhosis (CANONIC) Core Study Case Report Form (Final) Center: Investigator: Investigator s Signature: The highlighted information
CLIF Consortium Protocol of the CLIF Acute-oN-ChrONic LIver Failure in Cirrhosis (CANONIC) Core Study Case Report Form (Final) Center: Investigator: Investigator s Signature: The highlighted information
Liver disease in 2017: challenges and opportunities
 Liver disease in 2017: challenges and opportunities Dr Matthew Cowan Consultant Gastroenterologist and Hepatologist Surrey and Sussex Healthcare NHS Trust Faculty of Physician Associates 2 nd National
Liver disease in 2017: challenges and opportunities Dr Matthew Cowan Consultant Gastroenterologist and Hepatologist Surrey and Sussex Healthcare NHS Trust Faculty of Physician Associates 2 nd National
Causes of Liver Disease in US
 Learning Objectives Updates in Outpatient Cirrhosis Management Jennifer Guy, MD MAS Director, Liver Cancer Program California Pacific Medical Center guyj@sutterhealth.org Review cirrhosis epidemiology,
Learning Objectives Updates in Outpatient Cirrhosis Management Jennifer Guy, MD MAS Director, Liver Cancer Program California Pacific Medical Center guyj@sutterhealth.org Review cirrhosis epidemiology,
PALLIATIVE CARE IN END-STAGE LIVER DISEASE
 PALLIATIVE CARE IN END-STAGE LIVER DISEASE Ken S. Ota, DO Family Medicine Banner Good Samaritan Medical Center Learning Objectives: Describe the common bio-psycho-social issues in end-stage liver disease
PALLIATIVE CARE IN END-STAGE LIVER DISEASE Ken S. Ota, DO Family Medicine Banner Good Samaritan Medical Center Learning Objectives: Describe the common bio-psycho-social issues in end-stage liver disease
LIVER DISORDERS (PRACTICAL MANAGEMENT) Dr Pok Kern (PK) TAN Gastroenterologist Calvary hospital, ACT 1 st April 2017
 Dr Pok Kern (PK) TAN Gastroenterologist Calvary hospital, ACT 1 st April 2017") LIVER DISORDERS (PRACTICAL MANAGEMENT) Dr Pok Kern (PK) TAN Gastroenterologist Calvary hospital, ACT 1 st April 2017 TOPICS TO COVER Acute liver failure Chronic liver failure Portal hypertension : Ascites
LIVER DISORDERS (PRACTICAL MANAGEMENT) Dr Pok Kern (PK) TAN Gastroenterologist Calvary hospital, ACT 1 st April 2017 TOPICS TO COVER Acute liver failure Chronic liver failure Portal hypertension : Ascites
PORTAL HYPERTENSION An Introduction to the Culprit of Many Liver Failure Complications
 PORTAL HYPERTENSION An Introduction to the Culprit of Many Liver Failure Complications Edy G. Trujillo, RN, MSN, ACNP-BC Liver Transplant RRUCLA Medical Center July 31, 2018 What Do We All Look Forward
PORTAL HYPERTENSION An Introduction to the Culprit of Many Liver Failure Complications Edy G. Trujillo, RN, MSN, ACNP-BC Liver Transplant RRUCLA Medical Center July 31, 2018 What Do We All Look Forward
Alcoholic Liver Disease Strategies for Seamless Care or An Clinical Approach to the Jaundiced Alcoholic Patient
 Alcoholic Liver Disease Strategies for Seamless Care or An Clinical Approach to the Jaundiced Alcoholic Patient Liver Disease for the General Physician Royal College of Physicians July 2017 Dr Ewan Forrest
Alcoholic Liver Disease Strategies for Seamless Care or An Clinical Approach to the Jaundiced Alcoholic Patient Liver Disease for the General Physician Royal College of Physicians July 2017 Dr Ewan Forrest
The Sheila Sherlock Royal Free Hepatology Postgraduate Course Date: 15 th 17 th May 2019 Location: Royal Free Hospital, London, United Kingdom
 The Sheila Sherlock Royal Free Hepatology Postgraduate Course 2019 Date: 15 th 17 th May 2019 Location: Royal Free Hospital, London, United Kingdom *Includes histopathology within talk # Includes radiology
The Sheila Sherlock Royal Free Hepatology Postgraduate Course 2019 Date: 15 th 17 th May 2019 Location: Royal Free Hospital, London, United Kingdom *Includes histopathology within talk # Includes radiology
Title: CLIF-C ACLF score is a better mortality. patients with Acute on Chronic Liver Failure admitted to the ward
 Title: CLIF-C ACLF score is a better mortality predictor than MELD, MELD-Na and CTP in patients with Acute on Chronic Liver Failure admitted to the ward Authors: Rita Barosa, Lídia Roque Ramos, Marta Patita,
Title: CLIF-C ACLF score is a better mortality predictor than MELD, MELD-Na and CTP in patients with Acute on Chronic Liver Failure admitted to the ward Authors: Rita Barosa, Lídia Roque Ramos, Marta Patita,
Hepatitis. Dr. Mohamed. A. Mahdi 5/2/2019. Mob:
 Hepatitis Dr. Mohamed. A. Mahdi Mob: 0123002800 5/2/2019 Hepatitis Hepatitis means the inflammation of the liver. May cause by viruses or bacteria, parasites, radiation, drugs, chemical and toxins (alcohol).
Hepatitis Dr. Mohamed. A. Mahdi Mob: 0123002800 5/2/2019 Hepatitis Hepatitis means the inflammation of the liver. May cause by viruses or bacteria, parasites, radiation, drugs, chemical and toxins (alcohol).
Life After SVR for Cirrhotic HCV
 Life After SVR for Cirrhotic HCV KIM NEWNHAM MN, NP CIRRHOSIS CARE CLINIC UNIVERSITY OF ALBERTA Objectives To review the benefits of HCV clearance in cirrhotic patients To review some of the emerging data
Life After SVR for Cirrhotic HCV KIM NEWNHAM MN, NP CIRRHOSIS CARE CLINIC UNIVERSITY OF ALBERTA Objectives To review the benefits of HCV clearance in cirrhotic patients To review some of the emerging data
But. therefore, I: Liver Transplantation a non transplant centre perspective HOW AM I QUALIFIED TO DO THIS?
 Liver Transplantation a non transplant centre perspective Dermot Gleeson Consultant Hepatologist Gastroententerology SpR 29th September 2012 Clinical Update HOW AM I QUALIFIED TO DO THIS? Don t work in
Liver Transplantation a non transplant centre perspective Dermot Gleeson Consultant Hepatologist Gastroententerology SpR 29th September 2012 Clinical Update HOW AM I QUALIFIED TO DO THIS? Don t work in
SERUM CYSTATIN C CONCENTRATION IS A POWERFUL PROGNOSTIC INDICATOR IN PATIENTS WITH CIRRHOTIC ASCITES
 SERUM CYSTATIN C CONCENTRATION IS A POWERFUL PROGNOSTIC INDICATOR IN PATIENTS WITH CIRRHOTIC ASCITES YEON SEOK SEO, 1 SOO YOUNG PARK, 2 MOON YOUNG KIM, 3 SANG GYUNE KIM, 4 JUN YONG PARK, 5 HYUNG JOON YIM,
SERUM CYSTATIN C CONCENTRATION IS A POWERFUL PROGNOSTIC INDICATOR IN PATIENTS WITH CIRRHOTIC ASCITES YEON SEOK SEO, 1 SOO YOUNG PARK, 2 MOON YOUNG KIM, 3 SANG GYUNE KIM, 4 JUN YONG PARK, 5 HYUNG JOON YIM,
The Liver for the Nonhepatologist
 The Liver for the Nonhepatologist Michael R. Charlton, MBBS, FRCP Hepatology Director and Medical Director of Liver Transplantation Intermountain Medical Center Salt Lake City, Utah FORMATTED: 05-14-15
The Liver for the Nonhepatologist Michael R. Charlton, MBBS, FRCP Hepatology Director and Medical Director of Liver Transplantation Intermountain Medical Center Salt Lake City, Utah FORMATTED: 05-14-15
Treating patients with end-stage liver disease: Are we ready? Dr. Mino R. Mitri, M.D., C.M., M.Ed., FRCPC
 Treating patients with end-stage liver disease: Are we ready? Dr. Mino R. Mitri, M.D., C.M., M.Ed., FRCPC mino.mitri@ubc.ca No Conflict of Interest 157 patients 157 patients 6 transplanted Criteria Liver
Treating patients with end-stage liver disease: Are we ready? Dr. Mino R. Mitri, M.D., C.M., M.Ed., FRCPC mino.mitri@ubc.ca No Conflict of Interest 157 patients 157 patients 6 transplanted Criteria Liver
Esophageal Varices Beta-Blockers or Band Ligation. Cesar Yaghi MD Hotel-Dieu de France University Hospital Universite Saint Joseph
 Esophageal Varices Beta-Blockers or Band Ligation Cesar Yaghi MD Hotel-Dieu de France University Hospital Universite Saint Joseph Esophageal Varices Beta-Blockers or Band Ligation? Risk of esophageal variceal
Esophageal Varices Beta-Blockers or Band Ligation Cesar Yaghi MD Hotel-Dieu de France University Hospital Universite Saint Joseph Esophageal Varices Beta-Blockers or Band Ligation? Risk of esophageal variceal
Alpha-1 Antitrypsin Deficiency: Liver Disease
 Alpha-1 Antitrypsin Deficiency: Liver Disease Who is at risk to develop Alpha-1 liver disease? Alpha-1 liver disease may affect children and adults who have abnormal Alpha-1 antitrypsin genes. Keys to
Alpha-1 Antitrypsin Deficiency: Liver Disease Who is at risk to develop Alpha-1 liver disease? Alpha-1 liver disease may affect children and adults who have abnormal Alpha-1 antitrypsin genes. Keys to
Update in abdominal Surgery in cirrhotic patients
 Update in abdominal Surgery in cirrhotic patients Safi Dokmak HBP department and liver transplantation Beaujon Hospital, Clichy, France Cairo, 5 April 2016 Cirrhosis Prevalence in France (1%)* Patients
Update in abdominal Surgery in cirrhotic patients Safi Dokmak HBP department and liver transplantation Beaujon Hospital, Clichy, France Cairo, 5 April 2016 Cirrhosis Prevalence in France (1%)* Patients
PACT module Acute hepatic failure. Intensive Care Training Program Radboud University Medical Centre Nijmegen
 PACT module Acute hepatic failure Intensive Care Training Program Radboud University Medical Centre Nijmegen Acute Liver Failure Acute on Chronic Liver Failure Acute loss of hepatocellular function in
PACT module Acute hepatic failure Intensive Care Training Program Radboud University Medical Centre Nijmegen Acute Liver Failure Acute on Chronic Liver Failure Acute loss of hepatocellular function in
The Use of Albumin for the Prevention of Hepatorenal Syndrome in Patients with Spontaneous Bacterial Peritonitis and Cirrhosis
 The Use of Albumin for the Prevention of Hepatorenal Syndrome in Patients with Spontaneous Bacterial Peritonitis and Cirrhosis http://www.funnyjunk.com/funny_pictures/1743659/enlarged/ Daniel Giddings,
The Use of Albumin for the Prevention of Hepatorenal Syndrome in Patients with Spontaneous Bacterial Peritonitis and Cirrhosis http://www.funnyjunk.com/funny_pictures/1743659/enlarged/ Daniel Giddings,
Management in Cirrhosis
 Management in Cirrhosis Outline Introduction Cause of cirrhosis and management General management in cirrhosis Management complication and surveillance Clue of Chronic Liver Disease and Cirrhosis Risk
Management in Cirrhosis Outline Introduction Cause of cirrhosis and management General management in cirrhosis Management complication and surveillance Clue of Chronic Liver Disease and Cirrhosis Risk
RENAL DISEASE IN END STAGE LIVER DISEASE
 RENAL DISEASE IN END STAGE LIVER DISEASE Mitchell L Shiffman, MD Director Health System Richmond and Newport News, VA Medical Group Good Help to Those in Need Mitchell L Shiffman, MD POTENTIAL CONFLICTS
RENAL DISEASE IN END STAGE LIVER DISEASE Mitchell L Shiffman, MD Director Health System Richmond and Newport News, VA Medical Group Good Help to Those in Need Mitchell L Shiffman, MD POTENTIAL CONFLICTS
Evaluating HIV Patient for Liver Transplantation. Marion G. Peters, MD Professor of Medicine University of California San Francisco USA
 Evaluating HIV Patient for Liver Transplantation Marion G. Peters, MD Professor of Medicine University of California San Francisco USA Slide 2 ESLD and HIV Liver disease has become a major cause of death
Evaluating HIV Patient for Liver Transplantation Marion G. Peters, MD Professor of Medicine University of California San Francisco USA Slide 2 ESLD and HIV Liver disease has become a major cause of death
Management of autoimmune hepatitis. Pierre-Emmanuel RAUTOU Inserm U970, Paris Service d hépatologie, Hôpital Beaujon, Clichy, France
 Management of autoimmune hepatitis Pierre-Emmanuel RAUTOU Inserm U970, PARCC@HEGP, Paris Service d hépatologie, Hôpital Beaujon, Clichy, France 41 year-old woman, coming to emergency department for fatigue
Management of autoimmune hepatitis Pierre-Emmanuel RAUTOU Inserm U970, PARCC@HEGP, Paris Service d hépatologie, Hôpital Beaujon, Clichy, France 41 year-old woman, coming to emergency department for fatigue
Management of critically-ill cirrhotic patients
 Management of critically-ill cirrhotic patients Pere Ginès 1,2, *, Javier Fernández 1,François Durand 2, Faouzi Saliba 3 1 Liver Unit, IMDiM, Hospital Clinic Barcelona, University of Barcelona and IDIBAPS
Management of critically-ill cirrhotic patients Pere Ginès 1,2, *, Javier Fernández 1,François Durand 2, Faouzi Saliba 3 1 Liver Unit, IMDiM, Hospital Clinic Barcelona, University of Barcelona and IDIBAPS
Diseases of liver. Dr. Mohamed. A. Mahdi 4/2/2019. Mob:
 Diseases of liver Dr. Mohamed. A. Mahdi Mob: 0123002800 4/2/2019 Cirrhosis Cirrhosis is a complication of many liver disease. Permanent scarring of the liver. A late-stage liver disease. The inflammation
Diseases of liver Dr. Mohamed. A. Mahdi Mob: 0123002800 4/2/2019 Cirrhosis Cirrhosis is a complication of many liver disease. Permanent scarring of the liver. A late-stage liver disease. The inflammation
King s College Hospital NHS Foundation Trust. Acute Liver Disease: what you really need to know.
 King s College Hospital NHS Foundation Trust Acute Liver Disease: what you really need to know. William Bernal Professor of Liver Critical Care Liver Intensive Therapy Unit Institute of Liver Studies Kings
King s College Hospital NHS Foundation Trust Acute Liver Disease: what you really need to know. William Bernal Professor of Liver Critical Care Liver Intensive Therapy Unit Institute of Liver Studies Kings