O. Giouleme Assistant Professor of Gastroenterology Ippokration General Hospital of Thessaloniki
|
|
|
- Marvin Nichols
- 5 years ago
- Views:
Transcription

1 O. Giouleme Assistant Professor of Gastroenterology Ippokration General Hospital of Thessaloniki
2 Disclosures Advisory Board: Abbvie Pharmaceuticals Speaker: Gilead Sciences, Bristol-Myers Squibb Research grants: Gilead Sciences, Abbvie Pharmaceuticals Clinical Trials: Merck&Dohme The presentations may contain new scientific data, as these have been presented in international congresses or scientific journals that may contain data beyond the approved summary of Product Characteristics (SmPC) (EOF Circular 49392/ ). For full prescription information please refer to the SmPC before prescribing.
3 SVR* (%) -2011: Have We Reached Glass Ceiling for SVR with Standard of Care? All Gt Gt 1 Gt 2/ Duration (Wk) IFN Monotherapy Peg-IFN IFN + RBV Peg-IFN + RBV *Range of values reported; lower bar represents lower value. RBV, ribavirin. Poynard T et al. Lancet. 1998;352: ; McHutchison JG et al. N Engl J Med. 1998;339: ; Reichard O et al. Lancet. 1998;351:83-7; Fried MW et al. N Engl J Med. 2002;347:975-82; Manns MP et al. Lancet. 2001;358:
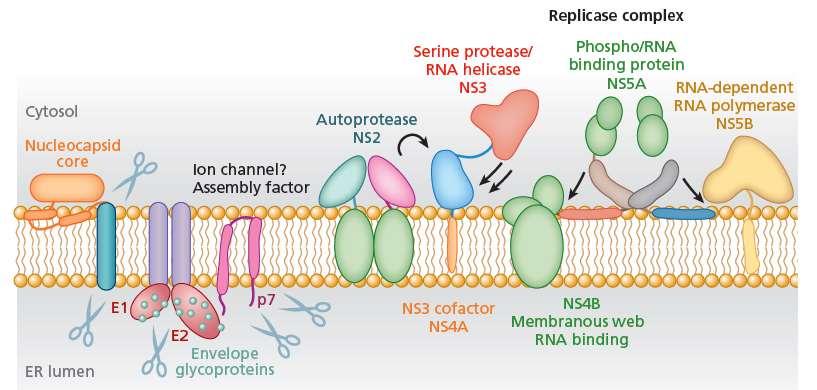
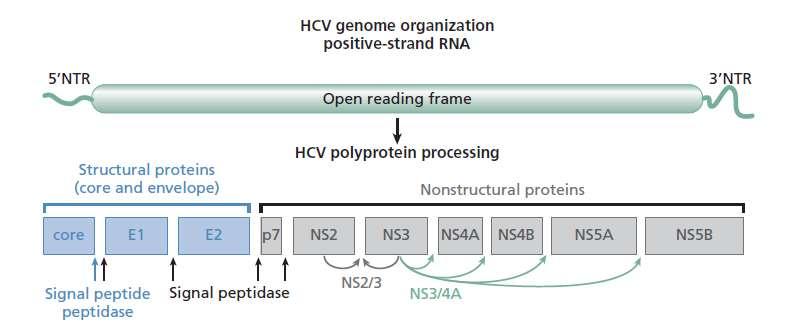
4 HCV
5 p7 Multiple Classes of Direct-Acting Antiviral Agents 5 UTR Core E1 E2 NS2 NS3 NS4B NS5A NS5B 3 UTR Protease Polymerase Ribavirin NS3 Protease Inhibitors NS5A Replication Complex Inhibitors NS5B NUC Inhibitors NS5B Non-NUC Inhibitors Telaprevir Boceprevir Simeprevir Asunaprevir ABT-450 MK-5172 Faldaprevir Sovaprevir ACH-2684 Daclatasvir Ledipasvir Ombitasvir MK-8742 GS-5885 GS-5816 ACH-3102 PPI-668 GSK Samatasvir Sofosbuvir VX-135 IDX21437 ACH-3422 Dasabuvir BMS PPI-383 GS-9669 TMC *Representative list; may not be fully inclusive.
6 First generation DAAs NS3/NS3-4A protease inhibitors (boceprevir, telaprevir) Approved 2011 Became SOC for HCV-1 patients in combination with PEG- IFN/RBV SVR ~ 70% Many limitations low genetic barrier many side effects complex medication regimen poor SVR rates in prior non-responders, cirrhosis only genotype 1
7 SVR rate (%) Evolution of HCV genotype 1 treatment: the future? % % % IFN % IFN + RBV % Peg-IFN + RBV 2 4 First wave DAA + Peg- IFN + RBV 5,6 Second wave DAA Future? McHutchison JG, et al. N Engl J Med 1998;339: ; 2. Fried M, et al. N Engl J Med 2002;347: Manns MP, et al. Lancet 2001;358:958 65; 4. Hadziyannis SJ, et al. Ann Intern Med 2004;140: Telaprevir EU SmPC; 6. Boceprevir EU SmPC
8 Sofosbuvir Nucleotide analog- inhibitor of the NS5B polymerase Acts as a chain terminator-inhibition of RNA synthesis Prodrug is converted intrahepatically to its active metabolite Advantages NS5B active site is well-conserved across HCV genotypes pangenotypic efficacy Mutations in the active site of NS5B result in the detrimental condition of the virus resistance was not observed
9 Sofosbuvir December 2013: FDA(Food & Drug Administration) approval January 2014: EMA(European Medicine Agency) approval for <pangenotyping HCV treatment either in combination with PEG-IFN/RBV, or in IFN free combination with RBV or other DAAs> Is of special interest due to: 1.pangenotypic efficacy 2.high potency 3.low side effects 4.high barrier to resistance 5.easy oral administration 6.all oral regimens
10 Sofosbuvir Phase 3 Study Designs IFN- LIMITING ALL ORAL THERAPY No response-guided therapy Week Treatment-Naïve: NEUTRINO GT 1,4,5,6 SOF + PegIFN + RBV, n=327 SVR12 SVR24 GT 2,3 GT 2,3 GT 2,3 GT 2,3 TN GT 1 TN GT 2,3 TE Treatment-Naïve and Treatment-Experienced: VALENCE GT 2 GT 3 Historical Control: TVR or BOC + PegIFN + RBV SOF + RBV, n=73 SOF + RBV, n=250 Treatment-Naïve: FISSION SOF + RBV, n=256 PegIFN + RBV, n=243 PegIFN-Unable: POSITRON SOF + RBV, n=207 PBO, n=71 Treatment-Experienced: FUSION SOF 400 mg/d; PegIFN 180 μg/wk; RBV mg/d for SOF+RBV arms and 800 mg/d for PegIFN+RBV arm SVR12 SVR12 SOF + RBV, n=103 PBO SVR12 SOF + RBV, n=98 Treatment-Naïve and Treatment-Experienced HCV/HIV: PHOTON-1 SOF + RBV, n=68 SOF + RBV, GT 1 n=114, GT 2,3 n=41 SVR12 SVR12 SVR12 SVR12 SVR12 SVR12
11 Patients with HCV RNA <LLOQ (%) > 90% SVR 12 Across Treatment-Naïve Genotypes 1, 2, 3, 4, 5, % 97% 93% 100% GT 1, 4 NEUTRINO GT 2 FISSION & VALENCE GT 3 VALENCE GT 5/6 NEUTRINO Lawitz E, et al. N Engl J Med May 16 Lawitz E, et al. APASL Singapore. Oral #LB-02 Zeuzem S, et al. AASLD Washington, DC. #1085

12 Effect of Negative Predictors on SVR Rates Across SOF Studies Predictors of Relapse Multivariate Regression Analysis (Combined Dataset) Factor Odds Ratio p-value HCV RNA 800,000 IU/mL 4.7 <0.001 Cirrhosis IL28B non-cc 3.4 <0.001 Weight 75 kg Treatment experienced Male Sofosbuvir-based regimens were highly effective, even in patients with a combination of multiple negative factors SVR12 rates were comparatively lower in patients with 5 or 6 of the negative predictors Foster G, EASL, 2014, O66
13 SVR12 (%) Effect of Negative Predictors on SVR Rates Across SOF Studies SVR Rates of SOF-Based Regimens Across Genotypes and Among Patients with Multiple Negative Predictive Factors Retrospective multivariate analysis of Phase 2 and 3 SOF data identified 6 negative predictors associated with relapse: Prior treatment failure, cirrhosis, IL28B non-cc, HCV RNA 800,000 IU/mL, body weight 75kg, male gender GT1 subgenotype (GT1a vs GT1b) was not a significant predictor in the univariate analysis. (OR:1.8; P=0.14) 89% of patients in the Phase 3 program had up to 4 negative predictors SVR12 Rates by Number of Negative Predictors and Genotype GT 1 GT 2 GT 3 GT 1 n=339 GT 2 n=285 SOF + PegIFN + RBV 12 weeks ATOMIC, NEUTRINO SOF + RBV 12 weeks FISSION, POSITRON, FUSION, VALENCE GT 3 n=247 SOF + RBV 24 weeks VALENCE Foster G, EASL, 2014, O / 4 5/ 5 26/ 26 22/ 22 22/ 22 69/ 69 69/ 70 43/ / / Number of Negative Predictors 55/ 59 89/ / 69 57/ 66 11/ 18 26/ 33 23/ 37 N/A 4/ 6 8/ 15
14 Integrated Safety Analysis of SOF Phase 3 Studies Adverse Events Summary GT 2, 3 GT 1, 4-6 All-oral IFN-based Patients, % Placebo 12 wk n=71 SOF+RBV* 12 wk n=650 SOF+RBV 16 wk n=98 SOF+RBV 24 wk n=250 PegIFN+ 800mg RBV* 24 wk n=243 SOF + PegIFN+ WB RBV* 12 wk n=327 Any AE Grade 3 AE AE leading to DC < Serious AE % discontinuations due to AEs in the SOF-containing arms No individual AE led to treatment discontinuation in more than 1 patient receiving SOF + RBV HCC, pyrexia, and cellulitis were the only SAEs occurring in >1 patient in any treatment arm Anemia was the only AE leading to treatment D/C in >1 patient receiving SOF+PegIFN+RBV (2/327) Both patients subsequently achieved SVR12 *RBV dose was mg/day with SOF-containing regimens and 800 mg/day with PegIFN+RBV regimen. DC, discontinuation. Gordon S, EASL, 2014, P1171

15 1. sofosbuvir plus ledipasvir 2. sofosbuvir plus daclatasvir 3. sofosbuvir plus simeprevir
16
17 Ledipasvir/Sofosbuvir: A Single Tablet Regimen (STR) Ledipasvir Picomolar potency against HCV GT 1a and 1b 1 Effective against NS5B RAV S282T 2 Once-daily, oral, 90 mg LDV NS5A inhibitor Sofosbuvir Potent antiviral activity against HCV GT 1 6 Effective against NS5A RAVs 3 High barrier to resistance Once-daily, oral, 400-mg tablet SOF - NS5B nucleotide polymerase inhibitor Ledipasvir/Sofosbuvir STR Once-daily, oral fixed-dose (90/400 mg) combination tablet, RBV-free Minimal DDIs, no food effect >2000 patients treated LDV NS5A inhibitor SOF - NS5B nucleotide polymerase inhibitor EMA Granted LDV/SOF Accelerated Assessment (27 March, 2014) FDA Granted Priority Review and Breakthrough Status (PDUFA: 10 Oct, 2014) 1. Lawitz E, et al. EASL 2011, poster 1219; 2. Cheng G, et al. EASL 2012, poster 1172; 3. SOVALDI [PI]. Gilead Sciences, Inc. Foster City, CA December 2013



18 LDV/SOF Clinical Development Program 1022 Cirrhotic Subjects Enrolled ELECTRON LONESTAR ELECTRON- 2 ION-2 ION-4 HCV/HIV Co-infection ERADICATE HCV/HIV Co-infection French ANRS HCV/HIV Co-infection Egypt GT 4 French GT 4,5 Russia GT 1,3 Korea/ Taiwan/ China GT 1 Australia TAP IVDU Japan GT 1 Nosocomial HCV SOLAR-1 SOLAR-2 ION-3 LONESTAR-3 SYNERGY Bleeding Disorders ION-1 SIRIUS Retreatment GT 1 GT 1, incl. PI failures GT 4 GT 1/4 GT 1/2/3/6 Immediate Post-liver Transplant GT 1/3 GT 4/5 Special populations Enrolling cirrhotics Post-renal Transplant Brain Imaging Study Sickle Cell Anaemia
19 LDV/SOF Phase 3 Program LDV/SOF Phase 3 Program (ION-1, ION-2, ION-3) Wk 0 Wk 8 Wk 12 Wk 24 LDV/SOF + RBV ION-1 ION-2 LDV/SOF LDV/SOF + RBV LDV/SOF ION-3 LDV/SOF + RBV LDV/SOF ION-1: treatment naïve,16% cirrhotic; N = 865 ION-2: treatment experienced, 20% cirrhotic; N = 440 ION-3: treatment naïve, non-cirrhotic; N = 647 N = 1952 total patients (11% cirrhotic [n=224]) Afdhal N, et al. N Engl J Med 2014; 370: ; Afdhal N, et al. N Engl J Med 2014; 370: ; Kowdley K, et al. N Engl J Med 2014; 370:
20 SVR12 (%) ION Phase 3 Program (ION-1, ION-2, ION-3) Efficacy Summary LDV/SOF LDV/SOF+RBV / / / / / / Weeks 24 Weeks 8 Weeks 12 Weeks 12 Weeks 24 Weeks ION-1 GT 1 treatment-naïve including cirrhotics ION-3 GT 1 treatment-naïve non-cirrhotic ION-2 GT 1 treatment-experienced including cirrhotics and PI failures 208/ / / / / % (1888/1952) overall SVR rate 3% (64/1952) did not achieve SVR 1.3% (26) LTFU 0.1% (2) virologic breakthrough (both due to non-adherence) 1.8% (36) relapsed Error bars represent 95% confidence intervals. Afdhal N, et al. N Engl J Med 2014; 370: ; Afdhal N, et al. N Engl J Med 2014; 370: ; Kowdley K, et al. N Engl J Med 2014; 370:
21 SVR12 (%) ION-2 (LDV/SOF±RBV x 12 or 24 weeks) SVR12: Absence of Cirrhosis vs. Cirrhosis Absence of Cirrhosis Cirrhosis /87 19/22 89/89 18/22 86/87 22/22 88/89 22/22 LDV/SOF LDV/SOF + RBV LDV/SOF LDV/SOF + RBV Error bars represent 95% confidence intervals Afdhal N, EASL, 2014, O109 Afdhal N, et al. N Engl J Med 2014; 370: Weeks 24 Weeks
22 ION Phase 3 Program (ION-1, ION-2, ION-3) Pooled Safety n (%) LDV/SOF (N=1080) LDV/SOF+RBV (N=872) Total (N=1952) Adverse Event 800 ( 74%) 745 ( 85%) 1545 ( 79%) Treatment Related AEs 484 ( 45%) 617 ( 71%) 1101 ( 56%) Grade 3 AE 46 ( 4%) 45 ( 5%) 91 ( 5%) SAE 34 ( 3%) 17 ( 2%) 51 ( 3%) Treatment-Related SAE 4 ( <1%) 1 ( <1%) 5 ( <1%) AEs Leading to Study Drug Modification/Interruption 6 ( 1%) 118 ( 14%) 124 ( 6%) Treatment DC due to AE 6 ( 1%) 7 ( 1%) 13 ( 1%) Death Data on File, Gilead Sciences, Inc.
23 LDV/SOF ± RBV: Compensated Cirrhosis An Integrated Safety and Efficacy Analysis of >500 Subjects with Compensated Cirrhosis Treated with LDV/SOF±RBV Wk 0 Wk 12 Wk 24 Wk 36 n=118 LDV/SOF SVR12 n=204 LDV/SOF + RBV SVR12 n=133 LDV/SOF SVR12 n=58 LDV/SOF + RBV SVR subjects with HCV GT 1, compensated cirrhosis Pooled data from Phase 2 and 3 LDV/SOF ± RBV studies LONESTAR, ELECTRON, ELECTRON-2, Japanese Phase 3 study, ION-1, ION-2, SIRIUS Primary efficacy endpoint: SVR12 Bourliere, AASLD, 2014, Oral #82
24 LDV/SOF ± RBV: Compensated Cirrhosis Demographics Treatment Naïve n=161 Treatment Experienced n=352 Total N=513 Mean age, y (range) 58 (35 77) 57 (23 77) 58 (23 77) Male, n (%) 101 (63) 241 (68) 342 (67) Black, n (%) 13 (8) 13 (4) 26 (5) Asian, n (%) 27 (17) 52 (15) 79 (15) Mean BMI, kg/m 2 (range) 27 (18 44) 28 (17 50) 28 (17 50) IL28B non-cc, n (%) 104 (65) 300 (85) 404 (79) GT 1a, n (%) 86 (53) 220 (63) 306 (60) Mean HCV RNA, log 10 IU/mL (range) 6.4 ( ) 6.5 ( ) 6.4 ( ) Prior PI failure N/A 240 (68) 240 (47) Cirrhosis determination method, n (%) Liver biopsy 72 (45) 169 (48) 241 (47) FibroScan >12.5 kpa 65 (40) 160 (45) 225 (44) FibroTest > APRI >2 24 (15) 23 (7) 47 (9) Bourliere, AASLD, 2014, Oral #82
25 SVR12 (%) LDV/SOF ± RBV: Compensated Cirrhosis Results: SVR12 by Treatment Duration LDV/SOF ± RBV, N= / / Weeks 24 Weeks SVR rates were similar with 12 or 24 weeks of LDV/SOF ± RBV Error bars represent 95% confidence intervals. Bourliere, AASLD, 2014, Oral #82
26 LDV/SOF ± RBV: Compensated Cirrhosis Results: SVR12 by Treatment Regimen Overall SVR wk wk Duration 24 wk Treatment Naïve 98% 97% 99% Treatment Experienced 95% 94% 98% Regimen LDV/SOF LDV/SOF + RBV 96% 99% 95% 96% LDV/SOF 12 wk 96% 90% Duration/± RBV LDV/SOF + RBV 12 wk LDV/SOF 24 wk 98% 97% 96% 98% LDV/SOF + RBV 24 wk 100% 100% Among TE cirrhotic subjects, 12 weeks of LDV/SOF + RBV resulted in similar SVR rates to 24 weeks of LDV/SOF alone Bourliere, AASLD, 2014, Oral # The combination of SOF/LDV with RBV is not approved for the treatment of HCV patients with compensated cirrhosis
27 LDV/SOF ± RBV: Compensated Cirrhosis Results: Safety Summary Subjects, n (%) LDV/SOF 12 and 24 Wk n=251 LDV/SOF + RBV 12 and 24 Wk n=262 TOTAL N=513 AEs 190 (76) 225 (86) 415 (81) Treatment-related AE 118 (47) 196 (75) 314 (61) Grade 3 AE 19 (8) 20 (8) 39 (8) Serious AE 15 (6) 9 (3) 24 (5) Treatment-related serious AE 1 (<1) 4 (2) 5 (1) AE leading to study drug modification/interruption 3 (1) 38 (15) 41 (8) Treatment D/C due to AE 0 1 (<1) 1 (<1) Death 0 1 (<1) 1 (<1) Grade 3 4 lab abnormality 39 (16) 35 (13) 74 (14) Hemoglobin < 10 g/dl 1 (<1) 26 (10) 27 (5) Hemoglobin < 8.5 g/dl 0 3 (1) 3 (<1) Bourliere, AASLD, 2014, Oral #82
28 Bourliere, AASLD, 2014, Oral #82 The combination of SOF/LDV with RBV is not approved for the treatment of HCV patients with compensated cirrhosis LDV/SOF ± RBV: Compensated Cirrhosis Conclusion 96% of this group of 513 subjects with compensated cirrhosis achieved an SVR High rates of SVR were observed in all subgroups Among treatment-experienced subjects, 12 weeks of LDV/SOF resulted in a 90% SVR rate Adding RBV or extending treatment duration increased this rate to 96% LDV/SOF was well tolerated in subjects with cirrhosis Use of RBV resulted in more frequent AEs and Hb declines
29 SVR Rate (%) High SVR Rates with LDV/SOF in HCV Genotype 1 Treatment-Naïve Patients * IFN 6 mo IFN 12 mo IFN+RBV 6 mo IFN+RBV 12 mo *Year of data presentation at EASL 2014 and publication in NEJM PEG 12 mo PEG+RBV 12 mo PI+PEG +RBV 6-12 mo SMV+PEG +RBV 6-12 mo SOF+PEG +RBV 3 mo Adapted from Strader DB, et al. Hepatology 2004;39: INCIVEK [PI]. Cambridge, MA: Vertex Pharmaceuticals; VICTRELIS [PI]. Whitehouse Station, NJ: Merck & Co; Jacobson I, et al. EASL Amsterdam. The Netherlands. Poster #1425. Manns M, et al. EASL Amsterdam. The Netherlands. Oral #1413. Lawitz E, et al. APASL Singapore. Oral #LB-02; Afdhal N, et al. N Engl J Med 2014; 370: ; Kowdley K, et al. N Engl J Med 2014; 370: LDV/SOF 2-3 mo
30 SVR Rate (%) High SVR Rates with LDV/SOF in HCV GT 1 TN or TE Patients with Bridging Fibrosis-Cirrhosis * 2014 * IFN 6 mo IFN 12 mo IFN+RBV 6 mo IFN+RBV 12 mo PEG 12 mo PEG+RBV 12 mo BOC+ PEG+RBV 6-12 mo TVR+ PEG+RBV 6-12 mo SMV+ PEG+RBV 6-12 mo FDV+ PEG+RBV 6-12 mo SOF+ PEG+RBV 3 mo LDV/SOF 3 mo *Year of presentation/publication of SMV-, FDV-, and SOF-based regimens in HCV GT 1-3 patients with bridging fibrosis-cirrhosis Adapted from Strader DB, et al. Hepatology 2004;39: INCIVEK [PI]. Cambridge, MA: Vertex Pharmaceuticals; VICTRELIS [PI]. Whitehouse Station, NJ: Merck & Co; McHutchison J, et al. NEJM 1998; 339: ; Poynard T, et al. Lancet 1998: 352: ; Manns M, et al. Lancet 2001; 358: ; Fried M, et al. NEJM 2002; 347: ; Hadziyannis S, et al. Ann Intern Med 2004; 140: ; McHutchison J, et al. NEJM 2009; 361: PEGASYS [PI]. Hoffmann-La Roche Inc; PEGINTRON [PI]. Whitehouse Station, NJ: Merck & Co; Jacobson I, et al. EASL 2013; Manns M, et al. EASL 2013; Ferenci P, et al. EASL 2013; Fontaine H, et al. EASL Amsterdam, The Netherlands. #60; Lawitz E, et al. EASL Amsterdam, The Netherlands. Oral #1411; Lawitz E, et al. N Engl J Med May 16; ; Afdhal N, et al. N Engl J Med 2014; 370: ; Afdhal N, et al. N Engl J Med 2014; 370: ; Kowdley K, et al. N Engl J Med 2014; 370:
31 SVR12, % Cross-Study Comparison: VALENCE, LONESTAR-2, PROTON/ELECTRON, and ELECTRON-2 SOF-Based Regimens for HCV GT SOF+RBV x 24 weeks (VALENCE) LDV/SOF+RBV x 12 weeks (ELECTRON-2) SOF+PegIFN+RBV x 12 weeks (TN: PROTON/ELECTRON; TE: LONESTAR-2) Treatment Naïve Treatment Experienced Non-Cirrhotic Treatment Experienced Cirrhotic SOF-based regimens resulted in similar SVR12 rates in TN and TE HCV GT 3 Zeuzem S, et al. NEJM Gane, EASL, 2014, Oral #6 Gane E et al. NEJM 2013;368: Lawitz E et al. Lancet Infect Dis 2013;13: Gane, AASLD, 2014, Poster #LB-11 99/105 26/26 38/39 85/98 25/28 10/12 29/47 16/22 10/12 The approved treatment duration of the combination of SOF/LDV with RBV for GT3 is 24 weeks
32 SVR12, % NIAID SYNERGY All-Oral Treatment for GT 4 with LDV/SOF Interim results from a single center, open-label, Phase 2a trial of LDV/SOF in HCV GT 4 Wk 0 Wk 12 Wk 24 N=21 LDV/SOF SVR12 Demographics Age 55 ± 10 Male, n (%) 14 (67) Black, n (%) 9 (43) Country of Origin Egypt, n (%) 6 (29) United States, n (%) 5 (24) Ethiopia, n (%) 4 (19) Cameroon, n (%) 3 (14) HCV RNA > 800,000 IU/mL, n (%) 13 (62) Treatment Experienced, n (%) 8 (38) Cirrhotic, n (%) 7 (33) /20 * *One subject has not reached SVR12 timepoint yet Kapoor, AASLD, 2014, Oral #240 95% SVR12 with LDV/SOF for GT 4 HCV No subject discontinued due to an AE
33 SVR12, % ELECTRON-2: LDV/SOF in GT 6 LDV/SOF for 12 Weeks for HCV GT 6 Two-center, open label study of LDV/SOF for 12 weeks in TN/TE subjects with HCV GT 6 Wk 0 Wk 12 Wk 24 N=25 LDV/SOF SVR12 Demographics Mean age, y (range) 51 (26 76) Male, n (%) 16 (64) White, n (%) 4 (16) Asian, n (%) 22 (88) Mean BMI, kg/m 2 (range) 23.6 ( ) IL28B non-cc, n (%) 5 (20) Cirrhosis, n (%) 2 (8) Mean HCV RNA, log 10 IU/mL (range) 6.7 ( ) TN, n (%) 23 (92) /25 No subjects discontinued due to an AE Gane, AASLD, 2014, Poster #LB-11 HCV genotype 6 is not included in the approved indications of SOF/LDV.
34
35 AI study: objective and design Objective: Phase 2 study to evaluate DCV + sofosbuvir (SOF), ± ribavirin (RBV), in treatment-naive, genotype (GT)-1-3 infected patients, and in GT1-infected patients who failed telaprevir (TVR) or boceprevir (BOC) treatment Primary endpoint: SVR 12 following 12 or 24 weeks of treatment Week 24 SVR 12 n=15 7dLI A: 7 d Lead-in SOF, then DCV+SOF Follow-up Chronic HCV GT1a/1b naive (n = 126) n=14 C: DCV+SOF Follow-up n=15 E: DCV+SOF+RBV Follow-up n=41 G: DCV + SOF Follow-up n=41 H: DCV+SOF+RBV Follow-up Chronic HCV GT2/3 naive (n = 44) Chronic HCV GT 1, TVR or BOC failure (n = 41) n=16 n=14 n=14 n=21 n=20 Week 12 SVR 12 7dLI B: 7 d Lead-in Follow-up SOF, then DCV+SOF Follow-up D: DCV+SOF Follow-up F: DCV+SOF+RBV Follow-up Week 24 SVR 12 I: DCV+SOF Follow-up J: DCV+SOF+RBV Follow-up RBV: mg/day, weight-based (GT 1); 800 mg/day (GT 2/3). GT, genotype, DCV, daclatasvir, SOF, sofosbuvir (GS-7977), RBV, ribavirin, TVR, telaprevir, BOC, boceprevir, SVR, sustained virologic response Sulkowski et al. N Engl J Med 2014;370:
36 HCV RNA <LLOQ Patients, % HCV RNA <LLOQ Patients, % AI study: SVR 12 primary endpoint (mitt) for treatment-naive patients GT1 GT2 GT3 a 100% 100% 100% 100% 95% a 92% 89% A LI b SOF, DCV + SOF C DCV + SOF E DCV + SOF + RBV G DCV + SOF H DCV + SOF + RBV DCV + SOF ± RBV DCV + SOF ± RBV 24 weeks 12 weeks 24 weeks SVR 12 rates were 98% in GT1a and 100% in GT1b SVR 24 rates ranged from % in GT1, and % in GT2/3 c LI, lead in; LLOQ = lower limit of quantitation (25 IU/mL), mitt, modified intent to treat a One patient had missing data at post treatment week 12 but achieved SVR24, and one who was lost to follow-up after achieving SVR4 b LI (lead in) with SOF was not included in subsequent trials c 93% and 88% were the percentage for the lead in arm. Sulkowski et al. N Engl J Med 2014;370: HCV genotype 2 is not included in the approved indications of Daclatasvir in combination with sofosbuvir.
37
38 SMV + SOF ± RBV: COSMOS study design Cohort 1: Prior null responders (METAVIR F0 F2), n=80 Cohort 2: Treatment-naïve and prior null responders (METAVIR F3 F4), n=87 Arm 1 SMV + SOF + RBV Follow up Randomised 2:1:2:1 Arm 2 Arm 3 SMV + SOF + RBV SMV + SOF Follow up Follow up Arm 4 SMV + SOF Follow up Stratification Week Cohort 1: HCV geno/subtype and IL28B Cohort 2: HCV geno/subtype and population (naïve/null) SMV 150 mg QD + SOF 400 mg QD ± RBV 1000/1200 mg/day Jacobson I, et al. AASLD Abstract LB-3
39 SVR12, % COSMOS (SMV+SOF±RBV) Results SMV+SOF 12 weeks (N=14) SMV+SOF 24 weeks (N=15) SMV+SOF+RBV 12 weeks (N=27) SMV+SOF+RBV 24 weeks (N=24) / / 27 No viral breakthrough 93 14/ 15 5 non-virologic failures Overall Q80K No Q80K GT1b GT1a 4 early treatment D/C 19/ 24 1 patient achieved SVR4 but died before SVR12 5/ 6 8/ 9 3/ 3 Relapse occurred in 3 patients (all GT 1a patients with Q80K polymorphism) SMV+SOF±RBV for 12 or 24 weeks led to SVR rates 90% in Metavir F0 2 null responders with HCV GT 1 Subgroup analyses are modified ITT Sulkowski M, EASL, 2014, O7 8/ 9 4/ 4 12/ 12 7/ 7 7/ 7 4/ 4 6/ 6 3/ 3 4/ 4
40 SVR12, % COSMOS (SMV+SOF±RBV) Results SMV+SOF 12 weeks (N=14) SMV+SOF 24 weeks (N=16) SMV+SOF+RBV 12 weeks (N=27) SMV+SOF+RBV 24 weeks (N=30) / / / 16 28/ 30 3/ 3 7/ 8 4/ 4 11/ 11 Overall GT1a Q80K GT1b Metavir F4 No viral breakthrough Relapse occurred in 3 GT1a-infected patients (1 with Q80K, 2 without Q80K; all had NS3 mutations) Most common AEs: fatigue 37.9%, headache 19.5% Four serious AEs reported One patient D/C treatment due to AE 3/ 3 5/ 5 4/ 4 6/ 6 6/ 7 10/ 11 9/ 9 12/ 12 Subgroup analyses are modified ITT Lawitz E EASL, 2014, O165
41

 and")
42 HCV-TARGET Effectiveness and Safety of SOF-Containing Regimens for HCV Started Therapy HCV-TARGET 2.0 N=2063 SOF/P/R N=384 SOF/RBV N=667 SOF/SMV N=784 SOF/SMV/RBV N=228 SOF/SMV/RBV 14.9% SOF/PegIFN/RBV 23.1% SOF/RBV 8.8% SOF SM V SOF/PegIFN/RBV 0.9% SOF/PegIFN/RBV 8.5% SOF/SMV 53.1% SOF/RBV 99.1% SOF/RBV 91.5% Genotype 1 Jensen, AASLD, 2014, Oral #45 Genotype 2 Genotype 3 Real-world observational study of 2,063 patients treated with DAAs at academic (n=38) and community medical centers (n=15) in North America and Europe Post liver transplant HCV recurrence is not included in the approved indications of simeprevir and sorosbuvir
43 HCV-TARGET Demographics n (%) SOF+PegIFN +RBV n=384 SOF+RBV n=667 SOF+SMV n=784 SOF+SMV +RBV n=228 Total n=2063 Male 253 (66.2) 422 (63.6) 478 (62.0) 147 (65.3) 1300 (63.7) Mean age, y (range) 53.9 (23-79) 56.9 (21-82) 59.5 (20-83) 58.8 (29-80) 57.6 (20-83) Caucasian 270 (70.3) 539 (80.8) 584 (74.5) 177 (77.6) 1570 (76.1) Black 68 (17.8) 37 (5.6) 96 (12.5) 33 (14.7) 234 (11.5) Treatment Status Naive 211 (54.9) 371 (55.6) 318 (40.6) 82 (36.0) 982 (47.6) Experienced 172 (44.8) 296 (44.4) 465 (59.3) 144 (63.2) 1077 (52.2) PI Failure 47 (27.3) 25 (8.4) 76 (24.8) 45 (31.3) 193 (17.9) Cirrhosis 120 (31.3) 302 (45.3) 440 (56.1) 137 (60.1) 999 (48.4) Hx Decompensation 12 (11.4) 136 (49.5) 167 (44.8) 60 (50.8) 375 (43.1) MELD >10 18 (17.1) 120 (43.6) 122 (32.7) 34 (28.8) 294 (33.8) Liver Cancer 25 (6.5) 66 (9.9) 88 (11.2) 32 (14.0) 211 (10.2) Liver Transplant 27 (7.0) 57 (8.5) 111 (14.2) 32 (14.0) 227 (11.0) HIV 14 (3.6) 18 (2.7) 8 (1.0) 7 (3.1) 47 (2.3) 78% (253/323) of GT 1, non-cirrhotic, naïve had a baseline HCV RNA <6 million IU/mL Jensen, AASLD, 2014, Oral #45 Post liver transplant HCV recurrence is not included in the approved indications of simeprevir and sorosbuvir
44 SVR4, % HCV-TARGET Effectiveness and Safety of SOF-Containing Regimens Wk Regimens 85 SOF+PegIFN +RBV 89 SOF+SMV ±RBV SOF+PegIFN+ SOF+SMV SOF+SMV SOF+RBV Total RBV ±RBV n=784 n=667 n=2063 n (%) n=384 n=228 Completed treatment 332 (86.5) 189 (82.9) 663 (84.6) 429 (64.3) 1613 (78.2) Ongoing treatment 41 (10.7) 32 (14.0) 101 (12.9) 205 (30.7) 379 (18.4) D/C Prematurely* 11 (2.9) 7 (3.1) 20 (2.6) 33 (4.9) 71 (3.4) AE 6 (1.6) 5 (2.2) 16 (2.0) 17 (2.5) 44 (2.1) Death 1 (0.3) 2 (0.9) 6 (0.8) 3 (0.4) 12 (0.6) / /303 44/54 168/187 *Not all premature D/C are summarised. Full list available in final slides. GT 1 GT 2 SOF+SMV±RBV Prior PI Failures SVR4/SVR12 Concordance: % PPV 90 SOF+RBV Jensen, AASLD, 2014, Oral #45

45 HCV-TARGET Post Transplant Effectiveness and Safety of Post-Transplant Patients Treated with SOF-Containing Regimens for HCV Started Therapy N=227 SOF/P/R N=27 SOF/RBV N=57 SOF/SMV N=111 SOF/SMV/RBV N=32 SOF/SMV/RBV 17.9% SOF/Peg/RBV 13.4% SOF/RBV 7.3% SOF/Peg/RBV 5.3% SOF/SMV 61.8% SOF/RBV 100% SOF/RBV 94.7% Genotype 1 N=5 will not start treatment; N=3 Data transfer pending Brown, AASLD, 2014, Oral #LB-4 Genotype 2 Genotype 3 Real-world observational study of 2,063 patients treated with DAAs at academic (n=38) and community medical centers (n=15) in North America and Europe
46 HCV-TARGET Post Transplant Demographics Post-Transplant Patients n(%) *Total, patients who started therapy SOF+PegIFN+ RBV N=27 SOF+RBV N=57 SOF+SMV N=111 SOF+SMV+ RBV N=32 Total* N=227 MALE 21 (77.8) 42 (73.7) 77 (69.4) 27 (84.4) 167 (73.6) MEAN Age, y (range) 60 (53-67) 59 (31-78) 61 (49-78) 59 (46-71) 60 (31-78) Age (11.1) 13 (22.8) 25 (22.5) 4 (12.5) 45 (19.8) CAUCASIAN 22 (81.5) 47 (82.5) 81 (73.0) 27 (84.4) 177 (78.0) BLACK 3 (11.1) 3 (5.3) 10 (9.0) 3 (9.4) 19 (8.4) TREATMENT STATUS NAIVE 8 (29.6) 28 (49.1) 51 (45.9) 10 (31.3) 97 (42.7) EXPERIENCED 19 (70.4) 29 (50.9) 60 (54.1) 22 (68.8) 130 (57.3) PI FAILURE 4 (21) 0 (0.0) 7 (11.7) 4 (18.2) 15 (11.5) CIRRHOSIS 15 (55.6) 27 (47.4) 67 (60.4) 19 (59.4) 128 (56.4) MELD 10 6 (40.0) 14 (51.9) 14 (20.9) 6 (31.6) 40 (31.3) BASELINE IMMUNOSUPPRESSION TAC 21 (77.8) 41 (71.9) 90 (81.1) 22 (68.8) 174 (76.7) CSA 4 (14.8) 9 (15.8) 13 (11.7) 2 (6.3) 28 (12.3) EVEROLIMUS/SIROLIMUS 3 (11.1) 10 (17.5) 13 (11.7) 10 (31.3) 36 (15.9) MMF/MPA 11 (40.7) 17 (29.8) 48 (43.2) 20 (62.5) 96 (42.3) Brown, AASLD, 2014, Oral #LB-4
47 SVR24 % HCV-TARGET Post Transplant HCV RNA Outcomes for SOF+SMV±RBV: Genotype 1 100% 94% 95% 90% 90% 86% 83% 80% 70% 60% 50% 40% 30% 20% 10% 0% 61/68 29/31 32/37 30/36 18/19 Overall No Cirrhosis Cirrhosis G1a G1b Cohort of patients with known treatment start date Excludes prior PI failures Brown, AASLD, 2014, Oral #LB-4 Post liver transplant HCV recurrence is not included in the approved indications of simeprevir and sorosbuvir
48
49 Please refer to the Summaries of Product Characteristics of individual products for the approved indications and treatment durations AASLD/EASL RECOMMENDATIONS 2014 GENOTYPE 1 AASLD LDV/SOF 12 or 24 weeks SOF+ SIM 12 or 24 weeks EASL SOF+PEG-IFN+RBV 12 weeks SOF+RIB 24weeks SOF+SIM± RBV 12 weeks SOF+DCV± RBV 12 or 24weeks GENOTYPE 2 SOF+RBV 12 or 16 weeks SOF+RBV 12or 16 weeks SOF+RBV+PEG-IFN 12 weeks GENOTYPE 3 GENOTYPE 4 SOF+RBV 24 weeks SOF+RBV+PEG-IFN 12 weeks LDV/SOF 12 weeks SOF+RBV 24 weeks SOF+PEG-IFN+RBV 12 weeks SOF+SIM± RBV 12 weeks SOF+PEG-IFN+RBV 12 weeks SOF+RBV 24 weeks SOF+DCV± RBV 12 or 24weeks SOF+PEG-IFN+RBV 12 weeks SOF+RBV 24 weeks SOF+SIM± RBV 12 weeks SOF+DCV± RBV 12 or 24weeks GENOTYPE 5 SOF+PEG-IFN+RBV 12 weeks SOF+PEG-IFN+RBV 12 weeks SOF+RBV 24 weeks GENOTYPE 6 LDV/SOF 12 weeks SOF+PEG-IFN+RBV 12 weeks SOF+PEG-IFN+RBV 12 weeks SOF+RBV 24 weeks
50 HCV Guidelines Greece (December 2014) Genotype 1 Genotype 2 Genotype 3 Genotype 4 Genotype 5 or 6 Peg-IFNα+RBV (PR) x24 or 48 wks x12-16 or 24 wks x16 or 24 wks x24 or 48 wks x24 or 48 wks (in naïve patients with mild moderate fibrosis, (in naïve pts without severe (in naïve pts without severe (in naïve patients with mild moderate (in naïve patients with mild moderate low viraemia, IL28B CC, check for RVR) fibrosis or cirrhosis) fibrosis or cirrhosis) fibrosis, IL28B CC, check for RVR) fibrosis, IL28B CC, check for RVR) SOF+PR x12 wks x12 wks x12 wks x12 wks SMV+PR / PR* x12 / 12 or 36 wks x12 / 12 or 36 wks (alternative) DCV+PR / PR (alternative) PR / BOC+PR /PR* (only if SOF or SMV not available) TPV+PR / PR* (only if SOF or SMV not available) SOF+RBV (not in 1a with Q80K) x4 / 24 or 44 / 0 or 20 or 0 wks x12 / 12 or 36 wks x24 wks (only if IFN contraindicated and other IFN free regimen not available) x12 or 24 / 12 or 0 wks x12 wks x24 wks x24 wks x24 wks SOF+SMV* x12 wks x12 wks SOF+DCV x12 or 24 wks x12 wks (non cirrhotics) (alternative) x12 or 24 wks (alternative) SOF/LDV SOF/LDV+RBV PRV/r/OBV+DSV+RBV* x12 wks (x8 wks for treatment naïve non-cirrhotics) x12 wks (for treatment experienced cirrhotics) x12 wks for 1a or 24 wks. (cirrhotics) x12 wks x12 wks (alternative) PRV/r/OBV+DSV* PRV/r/OBV±RBV x12 wks for 1b (alternative) *Not in patients with previous BOC/TPV failure. Peg-IFNα: pegylated interferon -α, RBV: ribavirin, SOF: sofosbuvir, SMV: simeprevir, DCV: daclatasvir, ΒΟC: boceprevir, TPV: telaprevir, LDV: ledipasvir, PRV/r: paritaprevir with ritonavir, OBV: ombitasvir, DSV: dasabuvir Please refer to the Summaries of Product Characteristics of individual products for the approved indications and treatment durations x12 wks
51 Reflections-dilemmas in 2015 According to recent phase II,III studies, HCV treatment is moving to interferon-free regimens as SOC These regimens increase the possibility of cure HCV in all CHC patients Sofosbuvir represents an almost ideal backbone in HCV treatment especially in difficult to treat patients BUT High cost of new DAAs raises public health debates Their optimal and cost-effective use differ among different countries Treatment options depends on the health care and financial resources available
52
Update on chronic hepatitis C treatment: current trends, new challenges, what next?
 Update on chronic hepatitis C treatment: current trends, new challenges, what next? Matti Maimets 12.06.2015 MMaimets15 Disclosure this presentation is sponsored by Gilead Sciences MMaimets15 MMaimets15
Update on chronic hepatitis C treatment: current trends, new challenges, what next? Matti Maimets 12.06.2015 MMaimets15 Disclosure this presentation is sponsored by Gilead Sciences MMaimets15 MMaimets15
IFN-free therapy in naïve HCV GT1 patients
 IFN-free therapy in naïve HCV GT1 patients Paris Hepatitis Conference Paris, 12th January, 2015 Pr Tarik Asselah MD, PhD; Service d Hépatologie & INSERM U773 University Paris Diderot, Hôpital Beaujon,
IFN-free therapy in naïve HCV GT1 patients Paris Hepatitis Conference Paris, 12th January, 2015 Pr Tarik Asselah MD, PhD; Service d Hépatologie & INSERM U773 University Paris Diderot, Hôpital Beaujon,
Associate Professor of Medicine University of Chicago
 Nancy Reau, MD Associate Professor of Medicine University of Chicago Management of Hepatitis C: New Drugs and New Paradigms HCV is More Lethal than HIV Infection HCV superseded HIV as a cause of death
Nancy Reau, MD Associate Professor of Medicine University of Chicago Management of Hepatitis C: New Drugs and New Paradigms HCV is More Lethal than HIV Infection HCV superseded HIV as a cause of death
TREATMENT OF GENOTYPE 2
 Treatment of Genotype 2, 3,and 4 David E. Bernstein, MD, FACG Advisory Committee/Board Member: AbbVie Pharmaceuticals, Gilead, Merck, Janssen Consultant: AbbVie Pharmaceuticals, Bristol-Myers Squibb, Gilead,
Treatment of Genotype 2, 3,and 4 David E. Bernstein, MD, FACG Advisory Committee/Board Member: AbbVie Pharmaceuticals, Gilead, Merck, Janssen Consultant: AbbVie Pharmaceuticals, Bristol-Myers Squibb, Gilead,
Treatments of Genotype 2, 3,and 4: Now and in the future
 Treatments of Genotype 2, 3,and 4: Now and in the future THERAPY FOR THE TREATMENT OF GENOTYPE 2 1 GT 2 and GT 3 Treatment-Naïve: SOF+RBV vs PEG-IFN+RBV FISSION Study Design HCV GT 2 and GT 3 Treatment-naïve
Treatments of Genotype 2, 3,and 4: Now and in the future THERAPY FOR THE TREATMENT OF GENOTYPE 2 1 GT 2 and GT 3 Treatment-Naïve: SOF+RBV vs PEG-IFN+RBV FISSION Study Design HCV GT 2 and GT 3 Treatment-naïve
Rome, February nd Riunione Annuale AISF th AISF ANNUAL MEETING
 Rome, February 20-21 nd 2014 Riunione Annuale AISF 2014 14 th AISF ANNUAL MEETING Present and future treatment strategies for patients with HCV infection: chronic hepatitis and special populations IFN
Rome, February 20-21 nd 2014 Riunione Annuale AISF 2014 14 th AISF ANNUAL MEETING Present and future treatment strategies for patients with HCV infection: chronic hepatitis and special populations IFN
The HCV Pipeline Ira M. Jacobson, MD, FACP, FACG, AGAF. Slide Presentation. IFN-free DAA combinations (G1)
") Slide Presentation The HCV Pipeline Vincent Astor Distinguished Professor of Medicine Chief, Division of Gastroenterology and Hepatology Medical Director, Center for the Study of Hepatitis C Weill Cornell
Slide Presentation The HCV Pipeline Vincent Astor Distinguished Professor of Medicine Chief, Division of Gastroenterology and Hepatology Medical Director, Center for the Study of Hepatitis C Weill Cornell
Future strategies with new DAAs
 Future strategies with new DAAs Ola Weiland professor New direct antiviral drugs Case no 1 male with genotype 2b Male with gt 2b chronic HCV Male with gt 2b relapse afer peg-ifn + RBV during 24 weeks
Future strategies with new DAAs Ola Weiland professor New direct antiviral drugs Case no 1 male with genotype 2b Male with gt 2b chronic HCV Male with gt 2b relapse afer peg-ifn + RBV during 24 weeks
What is the Optimized Treatment Duration? To Overtreat versus Undertreat. Nancy Reau, MD Associate Professor of Medicine University of Chicago
 What is the Optimized Treatment Duration? To Overtreat versus Undertreat Nancy Reau, MD Associate Professor of Medicine University of Chicago Learning Objectives: 1. Discuss patient populations appropriate
What is the Optimized Treatment Duration? To Overtreat versus Undertreat Nancy Reau, MD Associate Professor of Medicine University of Chicago Learning Objectives: 1. Discuss patient populations appropriate
Hepatitis C Treatment 2014
 Hepatitis C Treatment 214 Brendan M. McGuire, MD UAB Liver Center Outline Epidemiology/National History Terminology for Treatment Treatment Considerations Current Treatment Options Genotype 1 (GT 1) Genotype
Hepatitis C Treatment 214 Brendan M. McGuire, MD UAB Liver Center Outline Epidemiology/National History Terminology for Treatment Treatment Considerations Current Treatment Options Genotype 1 (GT 1) Genotype
Azienda ULSS12 Veneziana
 Azienda ULSS12 Veneziana Risultati del trattamento dei monoinfetti con Sofosbuvir, Simeprevir nella coorte veneziana. Confronto di esito con la coorte del trattamento con Boceprevir e Telaprevir Dr.ssa
Azienda ULSS12 Veneziana Risultati del trattamento dei monoinfetti con Sofosbuvir, Simeprevir nella coorte veneziana. Confronto di esito con la coorte del trattamento con Boceprevir e Telaprevir Dr.ssa
Program Disclosure. Provider is approved by the California Board of Registered Nursing, Provider #13664, for 1.5 contact hours.
 Program Disclosure This activity has been planned and implemented in accordance with the Essential Areas and policies of the Accreditation Council for Continuing Medical Education (ACCME) through the joint-sponsorship
Program Disclosure This activity has been planned and implemented in accordance with the Essential Areas and policies of the Accreditation Council for Continuing Medical Education (ACCME) through the joint-sponsorship
Case 4: A 61-year-old man with HCV genotype 3 with cirrhosis. Ira M. Jacobson, M.D. Weill Cornell Medical College New York, New York USA
 Case 4: A 61-year-old man with HCV genotype 3 with cirrhosis Ira M. Jacobson, M.D. Weill Cornell Medical College New York, New York USA 1 Genotype 3 case 61-year-old man with HCV genotype 3 Cirrhosis on
Case 4: A 61-year-old man with HCV genotype 3 with cirrhosis Ira M. Jacobson, M.D. Weill Cornell Medical College New York, New York USA 1 Genotype 3 case 61-year-old man with HCV genotype 3 Cirrhosis on
Evolution of Therapy in HCV
 Hepatitis C: Update on New Therapies and AASLD 13 David Bernstein, MD, FACP, AGAF, FACP Professor of Medicine Hofstra North Shore-LIJ School of Medicine Evolution of Therapy in HCV 199 1999 1 13 (%) SVR
Hepatitis C: Update on New Therapies and AASLD 13 David Bernstein, MD, FACP, AGAF, FACP Professor of Medicine Hofstra North Shore-LIJ School of Medicine Evolution of Therapy in HCV 199 1999 1 13 (%) SVR
Hepatitis C Emerging Treatment Paradigms
 Hepatitis C Emerging Treatment Paradigms David R Nelson MD Assistant Vice President for Research Professor of Medicine Director, Clinical and Translational Science Institute University of Florida Gainesville,
Hepatitis C Emerging Treatment Paradigms David R Nelson MD Assistant Vice President for Research Professor of Medicine Director, Clinical and Translational Science Institute University of Florida Gainesville,
Clinical Management: Treatment of HCV Mono-infection
 Clinical Management: Treatment of HCV Mono-infection Curtis Cooper, MD, FRCPC Associate Professor-University of Ottawa The Ottawa Hospital- Infections Diseases Viral Hepatitis Program- Director Industry
Clinical Management: Treatment of HCV Mono-infection Curtis Cooper, MD, FRCPC Associate Professor-University of Ottawa The Ottawa Hospital- Infections Diseases Viral Hepatitis Program- Director Industry
Update in the Management of Hepatitis C: What Does the Future Hold
 Update in the Management of Hepatitis C: What Does the Future Hold Paul Y Kwo, MD, FACG Professor of Medicine Mdi Medical ldirector, Liver Transplantation tti Gastroenterology/Hepatology Division Indiana
Update in the Management of Hepatitis C: What Does the Future Hold Paul Y Kwo, MD, FACG Professor of Medicine Mdi Medical ldirector, Liver Transplantation tti Gastroenterology/Hepatology Division Indiana
Initial Treatment of HCV G Hugo E. Vargas, MD Professor of Medicine Medical, Director Office of Clinical Research Mayo Clinic Arizona
 Initial Treatment of HCV G1 2016 Hugo E. Vargas, MD Professor of Medicine Medical, Director Office of Clinical Research Mayo Clinic Arizona Disclosure Information Disclosure Information Dr. Vargas receives
Initial Treatment of HCV G1 2016 Hugo E. Vargas, MD Professor of Medicine Medical, Director Office of Clinical Research Mayo Clinic Arizona Disclosure Information Disclosure Information Dr. Vargas receives
Latest Treatment Updates for GT 2 and GT 3 Patients
 Latest Treatment Updates for GT 2 and GT 3 Patients Eric Lawitz, MD, AGAF, CPI Vice President, Scientific and Research Development The Texas Liver Institute Clinical Professor of Medicine University of
Latest Treatment Updates for GT 2 and GT 3 Patients Eric Lawitz, MD, AGAF, CPI Vice President, Scientific and Research Development The Texas Liver Institute Clinical Professor of Medicine University of
Pivotal New England Journal of Medicine papers 2014 Phase 3 Trial data
 4 th HCV Therapy Advances Meeting Paris, December 12-13, 14 Pivotal New England Journal of Medicine papers 14 Phase 3 Trial data Stefan Zeuzem, MD University of Frankfurt Germany Disclosures Consultancies:
4 th HCV Therapy Advances Meeting Paris, December 12-13, 14 Pivotal New England Journal of Medicine papers 14 Phase 3 Trial data Stefan Zeuzem, MD University of Frankfurt Germany Disclosures Consultancies:
EASL 2013 Interferon Free, All Oral Regimens for Hepatitis C. Maria Buti Hospital Universitario Valle Hebron Barcelona Spain
 EASL 2013 Interferon Free, All Oral Regimens for Hepatitis C Maria Buti Hospital Universitario Valle Hebron Barcelona Spain The first Results with Oral therapy: a Protease Inhibitor and NS5A inhibitor
EASL 2013 Interferon Free, All Oral Regimens for Hepatitis C Maria Buti Hospital Universitario Valle Hebron Barcelona Spain The first Results with Oral therapy: a Protease Inhibitor and NS5A inhibitor
5/12/2016. Learning Objectives. Management of Hepatitis C Virus Genotype 2 or 3 Infected Treatment-Naive or Experienced Patients
 5/12/216 Management of Hepatitis C Virus Genotype 2 or 3 Infected Treatment-Naive or Experienced Patients Alexander Monto, MD Professor of Clinical Medicine University of California San Francisco San Francisco,
5/12/216 Management of Hepatitis C Virus Genotype 2 or 3 Infected Treatment-Naive or Experienced Patients Alexander Monto, MD Professor of Clinical Medicine University of California San Francisco San Francisco,
Update on the Treatment of HCV
 Update on the Treatment of HCV K. Rajender Reddy, MD Professor of Medicine Director of Hepatology Director, Viral Hepatitis Center University of Pennsylvania Philadelphia, USA 1 K. Rajender Reddy, MD Disclosure
Update on the Treatment of HCV K. Rajender Reddy, MD Professor of Medicine Director of Hepatology Director, Viral Hepatitis Center University of Pennsylvania Philadelphia, USA 1 K. Rajender Reddy, MD Disclosure
HCV Treatment Failure: What Next? Dr Ashley Brown, Imperial College Healthcare NHS Trust, London
 HCV Treatment Failure: What Next? Dr Ashley Brown, Imperial College Healthcare NHS Trust, London European HIV Hepatitis Co-infection Conference QEII Conference Centre 10 th December 2015 Dr Ashley Brown
HCV Treatment Failure: What Next? Dr Ashley Brown, Imperial College Healthcare NHS Trust, London European HIV Hepatitis Co-infection Conference QEII Conference Centre 10 th December 2015 Dr Ashley Brown
HCV In 2015: Maximizing SVR
 HCV In 2015: Maximizing SVR Alnoor Ramji Gastroenterology & Hepatology Clinical Associate Professor Division of Gastroenterology University Of British Columbia ramji_a@hotmail.com Disclosures (within Last
HCV In 2015: Maximizing SVR Alnoor Ramji Gastroenterology & Hepatology Clinical Associate Professor Division of Gastroenterology University Of British Columbia ramji_a@hotmail.com Disclosures (within Last
Transformation of Chronic Hepatitis C Treatment
 Transformation of Chronic Hepatitis C Treatment UVHS, Adana, 22 May 2015 Christoph Sarrazin Goethe-University Hospital Frankfurt am Main Germany Epidemiology of HCV Infection Global Global HCV Prevalence
Transformation of Chronic Hepatitis C Treatment UVHS, Adana, 22 May 2015 Christoph Sarrazin Goethe-University Hospital Frankfurt am Main Germany Epidemiology of HCV Infection Global Global HCV Prevalence
HCV Treatment of Genotype 1: Now and in the Future
 HCV Treatment of Genotype 1: Now and in the Future Bruce R. Bacon, MD, FACG James F. King, MD Endowed Chair in Gastroenterology Professor of Internal Medicine Co-Director of the Abdominal Transplant Program
HCV Treatment of Genotype 1: Now and in the Future Bruce R. Bacon, MD, FACG James F. King, MD Endowed Chair in Gastroenterology Professor of Internal Medicine Co-Director of the Abdominal Transplant Program
How to optimize treatment in G3 patients? Jérôme GOURNAY, MD Hépatologie Centre Hospitalier Universitaire de Nantes France
 How to optimize treatment in G3 patients? Jérôme GOURNAY, MD Hépatologie Centre Hospitalier Universitaire de Nantes France Paris Hepatitis Conference, January 12, 2016 Disclosures I have received funding
How to optimize treatment in G3 patients? Jérôme GOURNAY, MD Hépatologie Centre Hospitalier Universitaire de Nantes France Paris Hepatitis Conference, January 12, 2016 Disclosures I have received funding
Expert Perspectives: Best of HCV from EASL 2015
 Best of HCV from EASL 2015 Expert Perspectives: Best of HCV from EASL 2015 Saeed Hamid, MD Alex Thompson, MD, PhD This activity is supported by educational grants from AbbVie, Bristol-Myers Squibb, and
Best of HCV from EASL 2015 Expert Perspectives: Best of HCV from EASL 2015 Saeed Hamid, MD Alex Thompson, MD, PhD This activity is supported by educational grants from AbbVie, Bristol-Myers Squibb, and
Ed Gane NZ Liver Transplant Unit Auckland City Hospital
 Clinical Management of Hepatitis C Patients Treat Now or Wait Ed Gane NZ Liver Transplant Unit Auckland City Hospital SVR24 rates with PEG/RBV by HCV genotype Data from the real-world PROPHESYS cohort
Clinical Management of Hepatitis C Patients Treat Now or Wait Ed Gane NZ Liver Transplant Unit Auckland City Hospital SVR24 rates with PEG/RBV by HCV genotype Data from the real-world PROPHESYS cohort
Tough Cases in HIV/HCV Coinfection
 NORTHWEST AIDS EDUCATION AND TRAINING CENTER Tough Cases in HIV/HCV Coinfection John Scott, MD, MSc Assistant Professor University of Washington Presentation prepared by: J Scott Last Updated: Jun 5, 2014
NORTHWEST AIDS EDUCATION AND TRAINING CENTER Tough Cases in HIV/HCV Coinfection John Scott, MD, MSc Assistant Professor University of Washington Presentation prepared by: J Scott Last Updated: Jun 5, 2014
HCV-G3: Sofosbuvir with ledipasvir or daclatasvir?
 HCV-G3: Sofosbuvir with ledipasvir or daclatasvir? Ioannis Goulis, MD Aristotelian University of Thessaloniki XXIII International Hepatitis B & C Meeting of Athens Hadziyannis HCV genotype 3 therapy Chronic
HCV-G3: Sofosbuvir with ledipasvir or daclatasvir? Ioannis Goulis, MD Aristotelian University of Thessaloniki XXIII International Hepatitis B & C Meeting of Athens Hadziyannis HCV genotype 3 therapy Chronic
Why make this statement?
 HCV Council 2014 10 clinical practice statements were evaluated by the Council A review of the available literature was conducted The level of support and level of evidence for the statements were discussed
HCV Council 2014 10 clinical practice statements were evaluated by the Council A review of the available literature was conducted The level of support and level of evidence for the statements were discussed
New developments in HCV research and their implications for front-line practice
 New developments in HCV research and their implications for front-line practice Dr. Curtis Cooper Associate Professor, University of Ottawa Director, Ottawa Hospital Viral Hepatitis Program June 17, 2013
New developments in HCV research and their implications for front-line practice Dr. Curtis Cooper Associate Professor, University of Ottawa Director, Ottawa Hospital Viral Hepatitis Program June 17, 2013
EASL and The Future of HCV Treatment
 EASL and The Future of HCV Treatment Douglas T. Dieterich, M.D Professor of Medicine Division of Liver Diseases, Gastroenterology and Infectious Diseases Department of Medicine Mount Sinai School of Medicine
EASL and The Future of HCV Treatment Douglas T. Dieterich, M.D Professor of Medicine Division of Liver Diseases, Gastroenterology and Infectious Diseases Department of Medicine Mount Sinai School of Medicine
Treatement Experienced patients without cirrhosis. Rafael Esteban Hospital Universitario Valle Hebron Barcelona
 Treatement Experienced patients without cirrhosis Rafael Esteban Hospital Universitario Valle Hebron Barcelona Agenda With IFN PegIFN+ Ribavirin + Simeprevir PegIFN+ Ribavirin+ Sofosbuvir Without IFN Sofosbuvir
Treatement Experienced patients without cirrhosis Rafael Esteban Hospital Universitario Valle Hebron Barcelona Agenda With IFN PegIFN+ Ribavirin + Simeprevir PegIFN+ Ribavirin+ Sofosbuvir Without IFN Sofosbuvir
Treating HCV After Liver Transplantation: What are the Treatment Options?
 4 th OPTIMIZE WORKSHOP USING DAAs IN PATIENTS WITH CIRRHOSIS AND LIVER RECIPIENTS Treating HCV After Liver Transplantation: What are the Treatment Options? Maria Carlota Londoño, MD Liver Unit, Hospital
4 th OPTIMIZE WORKSHOP USING DAAs IN PATIENTS WITH CIRRHOSIS AND LIVER RECIPIENTS Treating HCV After Liver Transplantation: What are the Treatment Options? Maria Carlota Londoño, MD Liver Unit, Hospital
Treating HCV Genotype 2 & 3
 Treating HCV Genotype 2 & 3 3rd Workshop on HCV Therapy Advances, Rome 14.12.2013 Christoph Sarrazin Klinikum der J. W. Goethe-Universität Frankfurt am Main, Germany HCV Genotypes 2 & 3 Laurel and Hardy
Treating HCV Genotype 2 & 3 3rd Workshop on HCV Therapy Advances, Rome 14.12.2013 Christoph Sarrazin Klinikum der J. W. Goethe-Universität Frankfurt am Main, Germany HCV Genotypes 2 & 3 Laurel and Hardy
Case 2: A 71-year-old man with cirrhosis
 Case 2: A 71-year-old man with cirrhosis 1 JM, 71 year old African American male with known cirrhosis Asymptomatic apart from fatigue No prior history of decompensation Past history: Diabetes for 11 years
Case 2: A 71-year-old man with cirrhosis 1 JM, 71 year old African American male with known cirrhosis Asymptomatic apart from fatigue No prior history of decompensation Past history: Diabetes for 11 years
Feeling right at home
 Feeling right at home Getting to Cure From Cure to Eradication Jordan J. Feld MD MPH Toronto Centre for Liver Disease Sandra Rotman Centre for Global Health University of Toronto SVR Dramatic Improvements
Feeling right at home Getting to Cure From Cure to Eradication Jordan J. Feld MD MPH Toronto Centre for Liver Disease Sandra Rotman Centre for Global Health University of Toronto SVR Dramatic Improvements
Can we afford to Cure all HIV-HCV Co-infected Patients of HCV?
 Can we afford to Cure all HIV-HCV Co-infected Patients of HCV? Michael S. Saag, MD Professor of Medicine University of Alabama at Birmingham Birmingham, Alabama FINAL AU EDITED: 09-17-14 Disclosure Dr
Can we afford to Cure all HIV-HCV Co-infected Patients of HCV? Michael S. Saag, MD Professor of Medicine University of Alabama at Birmingham Birmingham, Alabama FINAL AU EDITED: 09-17-14 Disclosure Dr
Hepatitis C in Special Populations
 Hepatitis C in Special Populations David E. Bernstein, MD, FACG Vice Chairman of Medicine for Clinical Trials Chief, Division of Hepatology and Sandra Atlas Bass Center for Liver Diseases Northwell Health
Hepatitis C in Special Populations David E. Bernstein, MD, FACG Vice Chairman of Medicine for Clinical Trials Chief, Division of Hepatology and Sandra Atlas Bass Center for Liver Diseases Northwell Health
47 th Annual Meeting AISF
 47 th Annual Meeting AISF Rome, 21 February 2014 Present and future treatment strategies for patients with HCV infection: chronic hepatitis and special populations (HCV/HIV coinfection, advanced cirrhosis,
47 th Annual Meeting AISF Rome, 21 February 2014 Present and future treatment strategies for patients with HCV infection: chronic hepatitis and special populations (HCV/HIV coinfection, advanced cirrhosis,
Saeed Hamid, MD Alex Thompson, MD, PhD
 Saeed Hamid, MD Alex Thompson, MD, PhD 1 We will review some top line data from EASL Majority of the time discussing how the data affects daily practice 2 Grazoprevir (GZR; MK-5172) + Elbasvir (EBR; MK-
Saeed Hamid, MD Alex Thompson, MD, PhD 1 We will review some top line data from EASL Majority of the time discussing how the data affects daily practice 2 Grazoprevir (GZR; MK-5172) + Elbasvir (EBR; MK-
Treatment of hepatitis C today and tomorrow Antonio Craxì GI & Liver Unit, Di.Bi.M.I.S., University of Palermo, Italy
 Treatment of hepatitis C today and tomorrow Antonio Craxì GI & Liver Unit, Di.Bi.M.I.S., University of Palermo, Italy antonio.craxi@unipa.it Ad Board and grants: Abbvie, Achillion, BristolMyers Squibb,
Treatment of hepatitis C today and tomorrow Antonio Craxì GI & Liver Unit, Di.Bi.M.I.S., University of Palermo, Italy antonio.craxi@unipa.it Ad Board and grants: Abbvie, Achillion, BristolMyers Squibb,
Current Treatment Options for HCV Patients. Michael Manns Dept. of Gastroenterology, Hepatology and Endocrinology Hannover Germany
 Current Treatment Options for HCV Patients Michael Manns Dept. of Gastroenterology, Hepatology and Endocrinology Hannover Germany 7th International Congress of Internal Medicine of Central Greece, Larissa,
Current Treatment Options for HCV Patients Michael Manns Dept. of Gastroenterology, Hepatology and Endocrinology Hannover Germany 7th International Congress of Internal Medicine of Central Greece, Larissa,
Failure after treatment with DAAs: What to do? Marseille France 2-3 th June 2016
 Failure after treatment with DAAs: What to do? Marc Bourliere, MD White Nights of Hepatology Hôpital Saint Joseph Saint Petersburg Marseille France 2-3 th June 16 Disclosures Board member for : Schering-Plough,
Failure after treatment with DAAs: What to do? Marc Bourliere, MD White Nights of Hepatology Hôpital Saint Joseph Saint Petersburg Marseille France 2-3 th June 16 Disclosures Board member for : Schering-Plough,
HCV Case Study. Treat Now or Wait for New Therapies
 HCV Case Study Treat Now or Wait for New Therapies This program is supported by educational grants from Kadmon and Merck Pharmaceuticals. Program Disclosure This activity has been planned and implemented
HCV Case Study Treat Now or Wait for New Therapies This program is supported by educational grants from Kadmon and Merck Pharmaceuticals. Program Disclosure This activity has been planned and implemented
Will difficult-to-treat patients remain difficultto-treat. generation of treatments?
 Will difficult-to-treat patients remain difficultto-treat with the new generation of treatments? Jordan J Feld MD MPH Toronto Centre for Liver Disease Sandra Rotman Centre for Global Health University
Will difficult-to-treat patients remain difficultto-treat with the new generation of treatments? Jordan J Feld MD MPH Toronto Centre for Liver Disease Sandra Rotman Centre for Global Health University
Treatment of Unique Populations Raymond T. Chung, MD
 Treatment of Unique Populations Raymond T. Chung, MD Director of Hepatology and Liver Center Vice Chief, Gastroenterology Kevin and Polly Maroni Research Scholar Mass General Hospital Disclosures Research
Treatment of Unique Populations Raymond T. Chung, MD Director of Hepatology and Liver Center Vice Chief, Gastroenterology Kevin and Polly Maroni Research Scholar Mass General Hospital Disclosures Research
Antiviral agents in HCV
 Antiviral agents in HCV : Upcoming Therapeutic Options Su Jong Yu, M.D., Ph.D. Department of Internal Medicine, Liver Research Institute, Seoul National University College of Medicine Estimated 170 Million
Antiviral agents in HCV : Upcoming Therapeutic Options Su Jong Yu, M.D., Ph.D. Department of Internal Medicine, Liver Research Institute, Seoul National University College of Medicine Estimated 170 Million
Treatment of HCV in 2016
 5/1/16 Treatment of HCV in 16 Graham R Foster Professor of Hepatology QMUL Conflicts of Interest Speaker and consultancy fees received from AbbVie, BI, BMS, Gilead, Janssen, Roche, Merck, Novartis, Springbank,
5/1/16 Treatment of HCV in 16 Graham R Foster Professor of Hepatology QMUL Conflicts of Interest Speaker and consultancy fees received from AbbVie, BI, BMS, Gilead, Janssen, Roche, Merck, Novartis, Springbank,
Dr Janice Main Imperial College Healthcare NHS Trust, London
 BHIVA AUTUMN CONFERENCE 2014 Including CHIA Parallel Sessions Dr Janice Main Imperial College Healthcare NHS Trust, London 9-10 October 2014, Queen Elizabeth II Conference Centre, London BHIVA AUTUMN CONFERENCE
BHIVA AUTUMN CONFERENCE 2014 Including CHIA Parallel Sessions Dr Janice Main Imperial College Healthcare NHS Trust, London 9-10 October 2014, Queen Elizabeth II Conference Centre, London BHIVA AUTUMN CONFERENCE
Direct-acting Antiviral (DAA) Regimens in Late-stage Development: Which Patients Should Wait? Fred Poordad, MD
 Regimens in Late-stage Development: Which Patients Should Wait? Fred Poordad, MD") Direct-acting Antiviral (DAA) Regimens in Late-stage Development: Which Patients Should Wait? Fred Poordad, MD The HCV Lifecycle: Multiple Targets Polymerase Inhibitors Protease Inhibitors NS5A Inhibitors
Direct-acting Antiviral (DAA) Regimens in Late-stage Development: Which Patients Should Wait? Fred Poordad, MD The HCV Lifecycle: Multiple Targets Polymerase Inhibitors Protease Inhibitors NS5A Inhibitors
SVR Updates from the 2013 EASL
 Updates from the 2013 EASL By Tracy Swan, Treatment Action Group Streamlining HCV Treatment Treatment for hepatitis C virus (HCV) is becoming simpler, shorter, and more effective. All-oral combinations
Updates from the 2013 EASL By Tracy Swan, Treatment Action Group Streamlining HCV Treatment Treatment for hepatitis C virus (HCV) is becoming simpler, shorter, and more effective. All-oral combinations
I nuovi farmaci per HCV: frequenza della patologia, evidenze di efficacia e sicurezza, strategie di gestione. la pratica clinica
 I nuovi farmaci per HCV: frequenza della patologia, evidenze di efficacia e sicurezza, strategie di gestione La revisione ii delle dll evidenze e indicazioni i iper la pratica clinica Marco Marzioni Segretario
I nuovi farmaci per HCV: frequenza della patologia, evidenze di efficacia e sicurezza, strategie di gestione La revisione ii delle dll evidenze e indicazioni i iper la pratica clinica Marco Marzioni Segretario
HCV therapy : Clinical case
 HCV therapy : Clinical case PHC 2018 Paris January 14th, 2018 Tarik Asselah (MD, PhD) Professor of Medicine Hepatology, Chief INSERM UMR 1149, Hôpital Beaujon, Clichy, France. Disclosures Professor Asselah
HCV therapy : Clinical case PHC 2018 Paris January 14th, 2018 Tarik Asselah (MD, PhD) Professor of Medicine Hepatology, Chief INSERM UMR 1149, Hôpital Beaujon, Clichy, France. Disclosures Professor Asselah
Clinical Studies and Recent Real-World Data with Sofosbuvir/Ledipasvir
 Clinical Studies and Recent Real-World Data with Sofosbuvir/Ledipasvir Kalliopi Zachou Assistant Professor of Medicine University of Thessaly Disclosures Speaker s bureau and advisory: Gilead Bristol History
Clinical Studies and Recent Real-World Data with Sofosbuvir/Ledipasvir Kalliopi Zachou Assistant Professor of Medicine University of Thessaly Disclosures Speaker s bureau and advisory: Gilead Bristol History
Treatment of HCV infection in daily clinical practice. Which are the optimal options for Genotypes 2 and 3? Jiannis Vlachogiannakos
 Treatment of HCV infection in daily clinical practice. Which are the optimal options for Genotypes 2 and 3? Jiannis Vlachogiannakos Associate Professor of Gastroenterology Academic Department of Gastroenterology
Treatment of HCV infection in daily clinical practice. Which are the optimal options for Genotypes 2 and 3? Jiannis Vlachogiannakos Associate Professor of Gastroenterology Academic Department of Gastroenterology
Addressing Unmet Medical Needs in HCV Genotype 3
 Addressing Unmet Medical Needs in HCV Genotype 3 Karen Doucette, MD, MSc (Epi), FRCPC Associate Professor, Division of Infectious Diseases, Department of Medicine University of Alberta Objectives Identify
Addressing Unmet Medical Needs in HCV Genotype 3 Karen Doucette, MD, MSc (Epi), FRCPC Associate Professor, Division of Infectious Diseases, Department of Medicine University of Alberta Objectives Identify
Ledipasvir-Sofosbuvir (Harvoni)
") HEPATITIS WEB STUDY HEPATITIS C ONLINE Ledipasvir-Sofosbuvir (Harvoni) Robert G. Gish MD Professor, Consultant, Stanford University Medical Center Senior Medical Director, St Josephs Hospital and Medical
HEPATITIS WEB STUDY HEPATITIS C ONLINE Ledipasvir-Sofosbuvir (Harvoni) Robert G. Gish MD Professor, Consultant, Stanford University Medical Center Senior Medical Director, St Josephs Hospital and Medical
Protease inhibitor based triple therapy in treatment experienced patients
 Protease inhibitor based triple therapy in treatment experienced patients Universitätsklinikum Leipzig Thomas Berg Sektion Hepatologie Klinik und Poliklinik für Gastroenterologie und Rheumatologie Leber
Protease inhibitor based triple therapy in treatment experienced patients Universitätsklinikum Leipzig Thomas Berg Sektion Hepatologie Klinik und Poliklinik für Gastroenterologie und Rheumatologie Leber
NS5A inhibitors: ideal candidates for combination?
 NS5A inhibitors: ideal candidates for combination? Professor Vasily Isakov, MD, PhD, AGAF Dep.Gastroentrology & Hepatology, ION, Russian Academy of Sciences, Moscow Structure and function of NS5A Meigang
NS5A inhibitors: ideal candidates for combination? Professor Vasily Isakov, MD, PhD, AGAF Dep.Gastroentrology & Hepatology, ION, Russian Academy of Sciences, Moscow Structure and function of NS5A Meigang
Introduction. The ELECTRON Trial
 63rd AASLD November 9-13, 12 Boston, Massachusetts Faculty Douglas T. Dieterich, MD Professor of Medicine and Director of CME Department of Medicine Director of Outpatient Hepatology Division of Liver
63rd AASLD November 9-13, 12 Boston, Massachusetts Faculty Douglas T. Dieterich, MD Professor of Medicine and Director of CME Department of Medicine Director of Outpatient Hepatology Division of Liver
Ari Bunim, M.D. Director of Hepatology New York Hospital Queens Assistant Professor of Clinical Medicine Weill Cornell Medical College
 Ari Bunim, M.D. Director of Hepatology New York Hospital Queens Assistant Professor of Clinical Medicine Weill Cornell Medical College New York State Law Goes into Effect January 1, 2014 Hepatitis C Virus
Ari Bunim, M.D. Director of Hepatology New York Hospital Queens Assistant Professor of Clinical Medicine Weill Cornell Medical College New York State Law Goes into Effect January 1, 2014 Hepatitis C Virus
Clinical Сase A previously relapse to PEG IFN + RBV in HCV G3a patient. Konstantin Zhdanov
 Clinical Сase A previously relapse to PEG IFN + RBV in HCV G3a patient Konstantin Zhdanov Genotype 3 in Europe Canada Norway Germany Sweden Czech Republic Poland Approximately 1/3 of HCV-infected patients
Clinical Сase A previously relapse to PEG IFN + RBV in HCV G3a patient Konstantin Zhdanov Genotype 3 in Europe Canada Norway Germany Sweden Czech Republic Poland Approximately 1/3 of HCV-infected patients
Program Disclosure. Provider is approved by the California Board of Registered Nursing, Provider #13664, for 1.5 contact hours.
 Program Disclosure This activity has been planned and implemented in accordance with the Essential Areas and policies of the Accreditation Council for Continuing Medical Education (ACCME) through the joint-sponsorship
Program Disclosure This activity has been planned and implemented in accordance with the Essential Areas and policies of the Accreditation Council for Continuing Medical Education (ACCME) through the joint-sponsorship
Baseline and acquired viral resistance to DAAs: how to test and manage
 Baseline and acquired viral resistance to DAAs: how to test and manage Round table discussion by Marc Bourliere, Robert Flisiak, Vasily Isakov, Mark Sulkowsky & Konstantin Zhdanov Prevalence of baseline
Baseline and acquired viral resistance to DAAs: how to test and manage Round table discussion by Marc Bourliere, Robert Flisiak, Vasily Isakov, Mark Sulkowsky & Konstantin Zhdanov Prevalence of baseline
Drug Class Monograph
 Drug Class Monograph Class: Chronic Hepatitis C Drugs(s): Daclatasvir (Daklinza), Dasabuvir/ombitasivir/paritaprevir/ritonavir (Viekira Pak), Elbasvir/grazoprevir (Zepatier), Peginterferon alfa-2a (Pegasys),
Drug Class Monograph Class: Chronic Hepatitis C Drugs(s): Daclatasvir (Daklinza), Dasabuvir/ombitasivir/paritaprevir/ritonavir (Viekira Pak), Elbasvir/grazoprevir (Zepatier), Peginterferon alfa-2a (Pegasys),
Interferon-based and interferon-free new treatment options
 Interferon-based and interferon-free new treatment options White Nights of Hepatology St. Petersburg, 7. June 2013 Christoph Sarrazin Klinikum der J. W. Goethe-Universität Medizinische Klinik I Frankfurt
Interferon-based and interferon-free new treatment options White Nights of Hepatology St. Petersburg, 7. June 2013 Christoph Sarrazin Klinikum der J. W. Goethe-Universität Medizinische Klinik I Frankfurt
Chronic Hepatitis C Drug Class Prior Authorization Protocol
 Line of Business: Medi-Cal Effective Date: August 16, 2017 Revision Date: August 16, 2017 Chronic Hepatitis C Drug Class Prior Authorization Protocol This policy has been developed through review of medical
Line of Business: Medi-Cal Effective Date: August 16, 2017 Revision Date: August 16, 2017 Chronic Hepatitis C Drug Class Prior Authorization Protocol This policy has been developed through review of medical
The Changing World of Hepatitis C
 The Changing World of Hepatitis C Alnoor Ramji Gastroenterology & Hepatology Clinical Associate Professor Division of Gastroenterology University Of British Columbia St. Paul s Hospital Site Disclosures
The Changing World of Hepatitis C Alnoor Ramji Gastroenterology & Hepatology Clinical Associate Professor Division of Gastroenterology University Of British Columbia St. Paul s Hospital Site Disclosures
Genotype 1 HCV in 2016: Clinical Decision Making in a Time of Plenty
 Genotype 1 HCV in 216: Clinical Decision Making in a Time of Plenty Ira M. Jacobson, MD Chair, Department of Medicine Mount Sinai Beth Israel Senior Faculty and Vice-Chair, Department of Medicine Icahn
Genotype 1 HCV in 216: Clinical Decision Making in a Time of Plenty Ira M. Jacobson, MD Chair, Department of Medicine Mount Sinai Beth Israel Senior Faculty and Vice-Chair, Department of Medicine Icahn
Approved regimens for cirrhotic patients
 5th Workshop on HCV THERAPY ADVANCES New antivirals in clinical practice Approved regimens for cirrhotic patients Amsterdam, 4-5 december 2015 Disease burden in Spain 400000 350000 300000 F0 Peak cirrhosis
5th Workshop on HCV THERAPY ADVANCES New antivirals in clinical practice Approved regimens for cirrhotic patients Amsterdam, 4-5 december 2015 Disease burden in Spain 400000 350000 300000 F0 Peak cirrhosis
IFN-free for Genotype 1 HCV: the current landscape. Prof. Graham R Foster
 IFN-free for Genotype 1 HCV: the current landscape Prof. Graham R Foster Wonderful new drugs are coming Poordad F, et al. New Engl J Med 2014; online DOI: 10.1056/NEJMoa1402869. 2 The New Drugs Two treatment
IFN-free for Genotype 1 HCV: the current landscape Prof. Graham R Foster Wonderful new drugs are coming Poordad F, et al. New Engl J Med 2014; online DOI: 10.1056/NEJMoa1402869. 2 The New Drugs Two treatment
VII CURSO AVANCES EN INFECCIÓN VIH Y HEPATITIS VIRALES
 VII CURSO AVANCES EN INFECCIÓN VIH Y HEPATITIS VIRALES REGIMENES TERAPÊUTICOS DE LA HEPATITIS C, INTERFERÓN FREE A Coruña 2 Febrero 2013 Rui Sarmento e Castro Centro Hospitalar do Porto HJU ECS Universidade
VII CURSO AVANCES EN INFECCIÓN VIH Y HEPATITIS VIRALES REGIMENES TERAPÊUTICOS DE LA HEPATITIS C, INTERFERÓN FREE A Coruña 2 Febrero 2013 Rui Sarmento e Castro Centro Hospitalar do Porto HJU ECS Universidade
Chronic Hepatitis C Drug Class Monograph
 Chronic Hepatitis C Drug Class Monograph Line of Business: Medi-Cal Effective Date: July 10, 2017 (Interim Guidelines; Final Review and Approval by the P&T Subcommittee Pending) This policy has been developed
Chronic Hepatitis C Drug Class Monograph Line of Business: Medi-Cal Effective Date: July 10, 2017 (Interim Guidelines; Final Review and Approval by the P&T Subcommittee Pending) This policy has been developed
Management of HCV Tawesak Tanwandee
 Management of HCV 2016 Tawesak Tanwandee Topics Burden of HCV in our countries Natural history and unmet need for HCV treatment Current treatment as for 2016 Conclusion Evolution from HCV infection to
Management of HCV 2016 Tawesak Tanwandee Topics Burden of HCV in our countries Natural history and unmet need for HCV treatment Current treatment as for 2016 Conclusion Evolution from HCV infection to
Supplementary Material*
 Supplementary Material* Najafzadeh M, Andersson K, Shrank WH, Krumme AA, Matlin OS, Brennan T, et al. Cost- Effectiveness of Novel Regimens for the Treatment of Hepatitis C Virus. Ann Intern Med. doi:10.7326/m14-1152
Supplementary Material* Najafzadeh M, Andersson K, Shrank WH, Krumme AA, Matlin OS, Brennan T, et al. Cost- Effectiveness of Novel Regimens for the Treatment of Hepatitis C Virus. Ann Intern Med. doi:10.7326/m14-1152
HCV Management in Decompensated Cirrhosis: Current Therapies
 Treatment of Patients with Decompensated Cirrhosis and Liver Transplant Recipients Paul Y. Kwo, MD, FACG Professor of Medicine Gastroenterology/Hepatology Division Stanford University email pkwo@stanford.edu
Treatment of Patients with Decompensated Cirrhosis and Liver Transplant Recipients Paul Y. Kwo, MD, FACG Professor of Medicine Gastroenterology/Hepatology Division Stanford University email pkwo@stanford.edu
What do we need to know about RAVs clinically?
 14 th European HIV & Hepatitis Workshop Rome, 25-27 May, 2016 What do we need to know about RAVs clinically? Stefan Zeuzem, MD University of Frankfurt Germany Background Resistance associated variants
14 th European HIV & Hepatitis Workshop Rome, 25-27 May, 2016 What do we need to know about RAVs clinically? Stefan Zeuzem, MD University of Frankfurt Germany Background Resistance associated variants
10/21/2016. Susanna Naggie, MD, MHS Associate Professor of Medicine Duke University Durham, North Carolina. Learning Objectives
 A Crash Course on the AASLD/IDSA Hepatitis C Virus Infection Treatment Guidelines: What s New Susanna Naggie, MD, MHS Associate Professor of Medicine Duke University Durham, North Carolina FORMATTED: 1/3/16
A Crash Course on the AASLD/IDSA Hepatitis C Virus Infection Treatment Guidelines: What s New Susanna Naggie, MD, MHS Associate Professor of Medicine Duke University Durham, North Carolina FORMATTED: 1/3/16
Drug Class Monograph
 Drug Class Monograph Class: Chronic Hepatitis C Drugs(s): Daclatasvir (Daklinza), Dasabuvir/ombitasivir/paritaprevir/ritonavir (Viekira XR), Elbasvir/grazoprevir (Zepatier), Peginterferon alfa-2a (Pegasys),
Drug Class Monograph Class: Chronic Hepatitis C Drugs(s): Daclatasvir (Daklinza), Dasabuvir/ombitasivir/paritaprevir/ritonavir (Viekira XR), Elbasvir/grazoprevir (Zepatier), Peginterferon alfa-2a (Pegasys),
8/5/2014. A new era of HCV clinical management. Direct-Acting Antivirals for Hepatitis C. Goal of HCV treatment is viral cure HIV HBV HCV
 NS5B NS5B 8/5/214 A new era of HCV clinical management Mark Sulkowski, MD Professor of Medicine Medical Director, Viral Hepatitis Center Divisions of Infectious Disease and Gastroenterology/Hepatology
NS5B NS5B 8/5/214 A new era of HCV clinical management Mark Sulkowski, MD Professor of Medicine Medical Director, Viral Hepatitis Center Divisions of Infectious Disease and Gastroenterology/Hepatology
Hepatitis C Resistance Associated Variants (RAVs)
") Hepatitis C Resistance Associated Variants (RAVs) Atif Zaman, MD MPH Oregon Health & Science University Professor of Medicine Division of Gastroenterology and Hepatology Nothing to disclose Disclosure
Hepatitis C Resistance Associated Variants (RAVs) Atif Zaman, MD MPH Oregon Health & Science University Professor of Medicine Division of Gastroenterology and Hepatology Nothing to disclose Disclosure
Drug Class Prior Authorization Criteria Hepatitis C
 Drug Class Prior Authorization Criteria Hepatitis C Line of Business: Medicaid P & T Approval Date: Interim Criteria Pending P&T Approval Effective Date: August 16, 2018 This drug class prior authorization
Drug Class Prior Authorization Criteria Hepatitis C Line of Business: Medicaid P & T Approval Date: Interim Criteria Pending P&T Approval Effective Date: August 16, 2018 This drug class prior authorization
2017 Bruce Lucas Hepatology and Liver Transplant Symposium October 13th 2017 Management of Hepatitis C in Pre- and Post-Transplant Patients
 2017 Bruce Lucas Hepatology and Liver Transplant Symposium October 13th 2017 Management of Hepatitis C in Pre- and Post-Transplant Patients Jens Rosenau, MD Associate Professor of Medicine Acting Director
2017 Bruce Lucas Hepatology and Liver Transplant Symposium October 13th 2017 Management of Hepatitis C in Pre- and Post-Transplant Patients Jens Rosenau, MD Associate Professor of Medicine Acting Director
Eliminating Hepatitis C from New Zealand
 Eliminating Hepatitis C from New Zealand Catherine Stedman Associate Professor of Medicine, University of Otago, Christchurch Gastroenterology Department, Christchurch Hospital Disclosures I have the following
Eliminating Hepatitis C from New Zealand Catherine Stedman Associate Professor of Medicine, University of Otago, Christchurch Gastroenterology Department, Christchurch Hospital Disclosures I have the following
HCV Resistance Clinical Aspects. Sanjay Bhagani Royal Free Hospital/UCL London
 HCV Resistance Clinical Aspects Sanjay Bhagani Royal Free Hospital/UCL London DAAs in 2018, and beyond % patients % patients Changing characteristics of patients treated with DAA over time Prospective,
HCV Resistance Clinical Aspects Sanjay Bhagani Royal Free Hospital/UCL London DAAs in 2018, and beyond % patients % patients Changing characteristics of patients treated with DAA over time Prospective,
Viva La Revolución: Options to Combat Hepatitis C
 Viva La Revolución: Options to Combat Hepatitis C David L. Wyles, MD Professor of Medicine University of Colorado Chief, Division of Infectious Disease Denver Health Learning Objectives After attending
Viva La Revolución: Options to Combat Hepatitis C David L. Wyles, MD Professor of Medicine University of Colorado Chief, Division of Infectious Disease Denver Health Learning Objectives After attending
The Pipeline of New HCV Therapies: What to Expect in the Next 5 Years. Nancy Reau, MD Associate Professor University of Chicago
 The Pipeline of New HCV Therapies: What to Expect in the Next 5 Years Nancy Reau, MD Associate Professor University of Chicago Learning Objectives Upon completion of this presentation, learners should
The Pipeline of New HCV Therapies: What to Expect in the Next 5 Years Nancy Reau, MD Associate Professor University of Chicago Learning Objectives Upon completion of this presentation, learners should
A One-day Scientific Conference: Updates on Hepatitis C Treatments along with Consensus on Management of Hepatitis C in Iran
 A One-day Scientific Conference: Updates on Hepatitis C Treatments along with Consensus on Management of Hepatitis C in Iran Teheran, 22 July 2016 Massimo Colombo Treatment of HCV genotype 1 & 4 with DAAs
A One-day Scientific Conference: Updates on Hepatitis C Treatments along with Consensus on Management of Hepatitis C in Iran Teheran, 22 July 2016 Massimo Colombo Treatment of HCV genotype 1 & 4 with DAAs
Can a One-Size-Fits-All Approach Be Applied to All Treatment-Naïve GT1 HCV Patients?
 Can a One-Size-Fits-All Approach Be Applied to All Treatment-Naïve GT1 HCV Patients? Ira M. Jacobson, MD Vincent Astor Distinguished Professor of Medicine Chief, Division of Gastroenterology and Hepatology
Can a One-Size-Fits-All Approach Be Applied to All Treatment-Naïve GT1 HCV Patients? Ira M. Jacobson, MD Vincent Astor Distinguished Professor of Medicine Chief, Division of Gastroenterology and Hepatology
A treatment revolution: current management for chronic HCV
 A treatment revolution: current management for chronic HCV Ray Chung, M.D. Director of Hepatology and Liver Center Kevin and Polly Maroni Research Scholar Massachusetts General Hospital Disclosures Research
A treatment revolution: current management for chronic HCV Ray Chung, M.D. Director of Hepatology and Liver Center Kevin and Polly Maroni Research Scholar Massachusetts General Hospital Disclosures Research
Hepatitis C Prior Authorization Policy
 Hepatitis C Prior Authorization Policy Line of Business: Medi-Cal P&T Approval Date: November 15, 2017 Effective Date: January 1, 2018 This policy has been developed through review of medical literature,
Hepatitis C Prior Authorization Policy Line of Business: Medi-Cal P&T Approval Date: November 15, 2017 Effective Date: January 1, 2018 This policy has been developed through review of medical literature,
Drug Class Prior Authorization Criteria Hepatitis C
 Drug Class Prior Authorization Criteria Hepatitis C Line of Business: Medicaid P & T Approval Date: Interim (pending P&T approval) Effective Date: July 1, 2018 This policy has been developed through review
Drug Class Prior Authorization Criteria Hepatitis C Line of Business: Medicaid P & T Approval Date: Interim (pending P&T approval) Effective Date: July 1, 2018 This policy has been developed through review
Management of CHC G1 patients who are relapsers or non-responders to Peg IFN and RBV therapy: Wait or Triple Therapy?
 Management of CHC G1 patients who are relapsers or non-responders to Peg IFN and RBV therapy: Wait or Triple Therapy? Prof. Teerha Piratvisuth NKC Institute of Gastroenterology and Hepatology Prince of
Management of CHC G1 patients who are relapsers or non-responders to Peg IFN and RBV therapy: Wait or Triple Therapy? Prof. Teerha Piratvisuth NKC Institute of Gastroenterology and Hepatology Prince of
ICVH 2016 Oral Presentation: 28
 Ledipasvir/Sofosbuvir Is Safe and Effective for the Treatment of Patients with Genotype 1 Chronic HCV Infection in Both HCV Mono- and HIV/HCV Coinfected Patients A Luetkemeyer 1, C Cooper 2, P Kwo 3, K
Ledipasvir/Sofosbuvir Is Safe and Effective for the Treatment of Patients with Genotype 1 Chronic HCV Infection in Both HCV Mono- and HIV/HCV Coinfected Patients A Luetkemeyer 1, C Cooper 2, P Kwo 3, K
Genotype 4, finally cured? Imam Waked Professor of Medicine National Liver Institute
 Genotype 4, finally cured? Imam Waked Professor of Medicine National Liver Institute Paris, January 12, 215 Disclosures Investigator, speaker, and advisory board member for: Roche, MSD, BMS, Gilead, Janssen,
Genotype 4, finally cured? Imam Waked Professor of Medicine National Liver Institute Paris, January 12, 215 Disclosures Investigator, speaker, and advisory board member for: Roche, MSD, BMS, Gilead, Janssen,
Emerging Therapies for HCV: Highlights from AASLD 2012 (Part 2)
") Emerging Therapies for HCV: Highlights from AASLD 2012 (Part 2) PegIFN and RBV remain vital components of HCV therapy-- selected presentations from: Program Disclosure This activity has been planned and
Emerging Therapies for HCV: Highlights from AASLD 2012 (Part 2) PegIFN and RBV remain vital components of HCV therapy-- selected presentations from: Program Disclosure This activity has been planned and