Treatment of hepatitis C today and tomorrow Antonio Craxì GI & Liver Unit, Di.Bi.M.I.S., University of Palermo, Italy
|
|
|
- Dinah Fleming
- 6 years ago
- Views:
Transcription


1 Treatment of hepatitis C today and tomorrow Antonio Craxì GI & Liver Unit, Di.Bi.M.I.S., University of Palermo, Italy antonio.craxi@unipa.it
2 Ad Board and grants: Abbvie, Achillion, BristolMyers Squibb, Gilead, Janssen, Merck, Novartis, Roche Speaker: Abbvie, Bristol-Myers Squibb, Gilead, Janssen, Merck, Novartis, Roche

3 Flaviviridae could be as ancient as the differentiation of primate species (35 million years) - HCV has coevolved with human populations migrating out of Africa within the past,000 to 150,000 years - Current HCV genotypes appeared over the last 2,000 years - Genotypes 6 and 4 originated 700 years and 350 years ago - Subtypes 1a and 1b arose less than years ago Pybus et al Science 2001

4 HCV infects >185 million people worldwide HAJARIZADEH et al. Nat Rev Gastroenterol Hepatol 2013;10: NEGRO and ALBERTI. Liver Int 2011;31 Suppl 2:1-3 HANAFIAH et al. Hepatology 2013;57:


5 Treated/cured patients represent only a small proportion of those diagnosed Eligibility Reliability Tolerability Sensitivity North CS, et al. Gen Hosp Psych 2013;35:122 8.
6 DAAs currently approved 2013 Sofosbuvir Simeprevir Daclatasvir Nucleotide polymerase inh.all Gts (±3) NS5A inh. Protease inh.(8-12 wks), Short therapy 1, 3, 4, 5, 6 Gt 1, 4may needgt cirrhotics 24 wks - >90% SVR - Few pills, no IFN 2014 Dasabuvir - No RBV, but not for all pts Non-Nuc - Not all regimens suitable for Gt 1, 3, 4 Polymerase Gt 1-(4) Inh. decompensated pts Paritaprevir/R Ombitasvir Protease inh./ Ritonavir NS5A inh. Fixed dose combination of three DAAs ± ribavirin Sofosbuvir Triple therapy with PEG IFN and ribavirin SOF and ribavirin, no IFN Off-label combination of two DAAs ± ribavirin Ledipasvir NS5A inh Nucleotide polymerase inh. Fixed dose combination of two DAAs ± ribavirin.
7 Large body of evidence shows IFN-free therapy new combinations are highly effective in GT 1 Summary of 8 N Engl J Med studies on IFN-free therapy in GT 1 published in 2014 Regimen ION-1 LDV/SOF ± RBV ION-2 LDV/SOF ± RBV ION-3 LDV/SOF ± RBV SAPPHIRE-I PAR/r/OMB + DAS + RBV SAPPHIRE-II PAR/r/OMB + DAS + RBV PEARL-III PAR/r/OMB + DAS ± RBV PEARL-IV PAR/r/OMB + DAS ± RBV TURQUOISE-II J. Feld PAR/r/OMB + DAS + RBV PERFECTOVIR? SVR (%) Trial / Short, well-tolerated treatment regimens 8 24 weeks NB: Summary of 8 heterogeneous Phase 3 studies Included treatment-naïve and -experienced patients and cirrhotics LDV, PAR/r, OMB and DAS are investigational agents and not approved for use in HCV by the EMA/FDA Liang J, Ghany MG. N Engl J Med 2014;370: DAS: dasabuvir; LDV: ledipasvir; OMB: ombitasvir; PAR: paritaprevir; r: ritonavir
8 2014: HCV guidelines, recommendations & anti HCV drugs approval by International agencies EMA APPROVAL Olysio Olysio Sovaldi Sovaldi EASL guideline s Jan WHO guideline s Feb AASLD RECOM MENDA TIONS 1 FDA APPROVAL Sovaldi Sovaldi & & Olysio Olysio Mar Apr Daklinza Daklinza Viekirak Viekirak Exviera Harvoni Harvoni Exviera EACS guideline s May Jun Jul Aug Sept Oct Nov Dec AASLD RECOM MENDA TIONS 2 EASL RECOM MENDA TIONS Harvoni Harvoni Viekira Viekira Pack Pack
9 WHOM TO TREAT: EASL AND AASLD-IDSA RECOMMENDATIONS Indications to All treatment-naïve treatment and -experienced patients with compensated disease due to HCV should be considered for therapy (A1) Treatment is recommended for patients with chronic HCV infection (IA)
10 Clinical setting Compensated Cirrhosis Strongly recommended (A1) Highest priority (IA) Decompensate d cirrhosis not on the transplant list On clinical trial or expanded access program or within experienced centres (B1) treated by physicians with experience in treating HCV in conjunction with a liver transplantation center
11 WHOM TO TREAT: EASL AND AASLD-IDSA RECOMMENDATIONS Clinical setting F3 Strongly recommende d (A1) Highest priority (IA) F2 Justified (A2) High priority (IB) F0-F1 Indication for and timing of therapy can be Individualized (B1) Individual decision (IB)
 Highest priority (IIaB) Solid Organ Transplant Recipients No specific priority (A2) considered for individual decision Highest priority (IB) Haemodialysis Should be considered (B1)")
12 RECOMMENDATIONS HCV related extrahepatic diseases & comorbidities Clinical setting Cryoglobulinemia with vasculitis HCV related immune complex Nephropathy Highest priority (IB) Treatment should be prioritized (A1) Highest priority (IIaB) Solid Organ Transplant Recipients No specific priority (A2) considered for individual decision Highest priority (IB) Haemodialysis Should be considered (B1) Consider treatment prioritization In order to yield transmission reduction benefits (IIaC) HIV No specific priority (A1) considered for individual decision High priority based on available resources(ib)
13 DAA combos reaching the clinic by Fixed dose combination of two or three DAAs Pangenotipic (± Gt3) Elbasvir Grazoprevir 2nd generation 2nd generation NS5A inh protease inh. MK 3682 (IDX 21437) Polymerase Inh. Pangenotipi c Sofosbuvir Nucleotide polymerase inh. Pangenotipi c Beclabuvir Polymerase Inh. Asunaprevir Daclatasvir Protease inh. NS5A inh. Ultra-short therapy (4-8 wks) >95% SVR for all pts. Pangenotypic One-pill regimen, no RBV ACH-3422 Suitable for all disease stages Polymerase GS nd generation NS5A inh. Pangenotipic (?) Sovaprevir (ACH-1625 Protease inh. Inh. ACH-3102 NS5A inh.
14
15 SVR rates with 12 and 8-wk regimens in Gt 1, 2, 3 Part A: 12-Wk Duration Part B: 8-Wk Duration SOF + GS mg SOF + GS-5816 mg SOF + GS mg + RBV SOF + GS-5816 mg + RBV / 27 28/ 28 10/ 11 10/ /2 7 25/ 27 26/ 30 25/ 30 26/ / 31 20/ / 25 23/ 26 23/ 26 SVR12 (%) GT 1 GT 2 GT 3 Tran TT, et al. AASLD Abstract 80. GT1 GT2
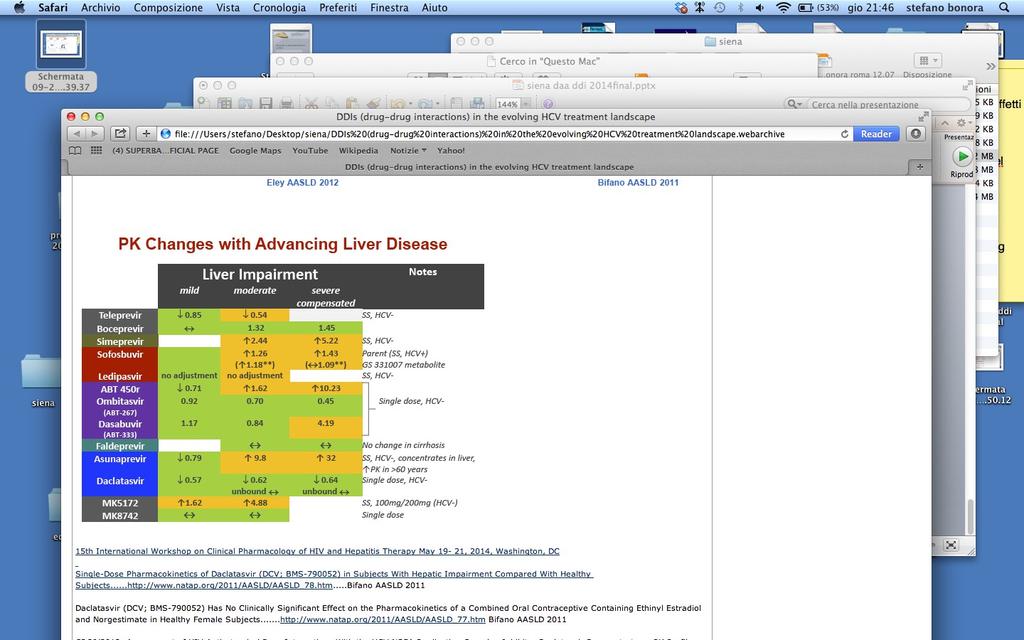
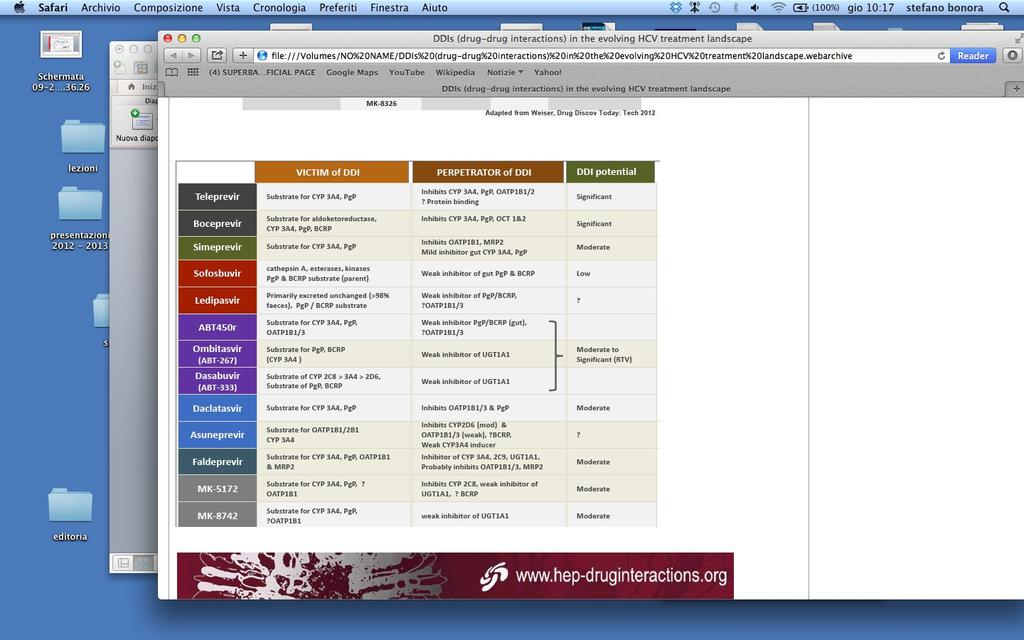
16 Factors impacting response to HCV treatment: before 2015 Viral Viral factors factors Baseline viral load HCV genotype HIV/HCV co-infection DAA baseline resistance HBV/HCV co-infection Host Host factors factors Age Prior response to treatment Gender Race Genetics (IL28B, IP10, etc) Cirrhosis Transplant Obesity Diabetes/insulin resistance Hepatic decompensation Pharmacokinetics and DDIs
17 Factors impacting response to HCV treatment: after 2015 Viral Viral factors factors HCV genotype Posttreatment DAA RAVs Host Host factors factors
18 Can baseline HCV RNA inform decision to treat with LDV/SOF for 8 or 12 weeks? Similar SVR rates for 8 and 12 weeks of therapy in ION-3 If baseline HCV RNA 6 million IU/mL, treatment for 12 weeks can reduce chance of relapse LDV/SOF 8 weeks LDV/SOF 12 weeks SVR rate similar with 8 or 12 weeks 94% (202/215) 96% (208/216) Relapse rate according to baseline HCV RNA HCV RNA <6 million IU/mL 2% (2/121) 2% (2/128) HCV RNA 6 million IU/mL 10% (9/92) 1% (1/83) HCV-TARGET: 78% (253/323) of GT 1, non-cirrhotic, treatment-naïve had a baseline HCV RNA <6 million IU/mL Gilead Sciences Europe Ltd. HARVONI (ledipasvir/sofosbuvir) Summary of Product Characteristics. November 2014; Jensen D, et al. AASLD 2014; Oral #45.
 change Log10 HCV RNA (IU/mL) Week 1 Week 2 Week 3 Week")
19 COSMOS Cohort 2: On-treatment HCV RNA over time Ba se lin e Da y Da 2 y Da 3 y4 Mean (+/- SD) change Log10 HCV RNA (IU/mL) Week 1 Week 2 Week 3 Week 4

20 Time to Viral Suppression is not related to Achievement of SVR12 in GT1 treated with ABT-450/r/Ombitasvir+Dasabuvir +/- RBV Pooled analysis of 6 phase III Trials Aim: To evaluate the predictive value of time of first occurrence of HCVRNA TND and SVR12 Longer time to suppression associated with higher baseline HCVRNA, older age, GT1a and cirrhosis Sulkowsky M. Abst 1950 AASLD 2014
21 Is the Q80K mutation relevant for patients on SOF + SMV? Limited data but little apparent effect of Q80K for SMV in combination with SOF COSMOS: SVR12 in cohorts 1 and 2 by HCV subgenotype and baseline Q80K Cohort 2 (F3 F4 naïves/nulls)* Cohort 1 (F0 F2 nulls)* GT 1b GT 1a without Q80K 89 GT 1a with Q80K SVR12 (%) / 4 7/ 7 8/ 9 3/ 3 7/ 7 3/ 3 6/ 12/ 8/ / 4 4/ 4 5/ 6 17/ 30/ 24/ / 11/ 11/ / 7/ 4 7 4/ 4 5/ 13/ 7/ / 3 7/ 3/ / 38/ 25/ SOF + SMV SOF + SMV SOF + SMV SOF + SMV SOF + SMV SOF + SOF + SMV SOF + SMV SOF + SMV SOF + SMV + RBV + RBV ± RBV SMV + RBV + RBV ± RBV 24 weeks 12 weeks Overall Lawitz E, et al. Lancet 2014;384: weeks 12 weeks Overall *Excluding patients who discontinued for non-virological reasons
 Svarovskaia ES et al.")
22 L159F and V321A emergence in 408 virological failures from 8 SOF and 5 LDV/SOF trials Ultra deep sequencing of NS5B (1% assay cut-off) Svarovskaia ES et al., AASLD 2014

23 Svarovskaia ES et al., AASLD

24 Krishnan, Abst 1936
25 Is Gt 1 subtype still relevant? LDV/SOF 8 weeks LDV/SOF 12 weeks 94% (202/215) 95% (206/216) GT 1a 93% (159/171) 95% (163/172) GT 1b 98% (42/43) 98% (43/44) SVR rate overall SVR according to subtype Kowdley KV, et al. N Engl J Med 2014;370:
26 Is Gt 1 subtype still relevant? RBV-free PEARL-IV1 90 * + RBV PEARL-III1 99,5 80 SVR12 (%) SVR12 (%) / / GT 1a Treatment-naïve Ferenci P, et al. N Engl J Med 2014;370: / / 210 GT 1b Treatment-naïve *RBV-free arm did not meet non-inferiority vs RBV-containing arm; Ombitasvir, paritaprevir, RTV + dasabuvir are not approved for use in HCV by the EMA; EMA: European Medicines Agency; RTV: ritonavir
27 HCV Gt 3: still a difficult genotype SOF + RBV x 24 weeks (VALENCE) LDV/SOF + RBV x 12 weeks (ELECTRON-2) SOF + DCV x 12 weeks (ALLY-3) SVR12, % /92 21/21 73/75 38/39 12/13 5/5 11/19 0 SOF + PEG-IFN + RBV x 12 weeks (TN: PROTON/ELECTRON 85/98 25/28 32/34 10/12 29/47 16/22 9/13 10/12 Treatment-experienced Non-cirrhotic LDV/SOF + RBV for 12 weeks and SOF + DCV for 12 weeks are not EMA-recommended treatment regimens for GT 3 Zeuzem S, et al. N Engl J Med 2014;370: ; Gane E, et al. EASL 2014; Oral #6; Gane E et al. NEJM 2013;368:34 44; Lawitz E et al. Lancet Infect Dis 2013;13: ; Gane E et al. AASLD 2014, Poster #LB-11; Lawitz E et al. AASLD 2013, Oral #LB-4; Nelson M et al. AASLD 2014, Oral #LB-3.
28 Factors impacting response to HCV treatment: after 2015 Viral Viral factors factors HCV genotype Posttreatment DAA RAVs Host Host factors factors Cirrhosis Post OLT status Pharmacokinetics and DDIs
29 Efficacy of SOF + SMV ± RBV in real-world settings HCV-TARGET: Prospective Observational Cohort Study: Adjusted SVR4 in GT1 HCV Pts[1] SOF + SMV TRIO: Prospective Observational Cohort Study: SVR12 in Tx-Naive GT1 HCV Pts[2] GT1 GT1a SOF + SMV + RBV SVR12 (%) n= SVR4 (%) 83 GT1b All Pts Tx-Naive Pts Tx-Exp d Pts SMV + SOF ± RBV 1. Jensen DM, et al. AASLD Abstract Dieterich D, et al. AASLD Abstract
30 LDV/SOF efficacy in compensated Gt1 cirrhosis 24 wks of LDV/SOF 24 wks of LDV/SOF + RBV 12 wks of LDV/SOF 12 wks of LDV/SOF + RBV SVR12 (%) n= Total Bourlière M, et al. AASLD Abstract Treatment Naive Treatment Experienced 22
31 SVR12 rates with LDV/SOF ± RBV by stage of cirrhosis Total Overall SVR12 Platelets (x 103/µL) FibroScan (kpa) Treatment Experienced 96% 98% 95% < 75 84% 90% 82% 75 to < 99% % 98% to < % 98% 93% % 98% 98% > 12.5 to 20 99% % 99% > 20 96% % 95% 80 Treatment Naive SVR12 (%) SVR12 rates lower among pts determined to have cirrhosis using FibroTest + APRI (89%) and among pts with a platelet count < 75,000 cells/mm3 (84%) Bourlière M, et al. AASLD Abstract 82.
32 SVR12 with PTV/RTV/OMV + DSV + RBV in Gt1 compensated cirrhosis 12 wks wks / 13/ / 59/ / 115/ / 51/ / 33/ / 102/ / 31/ CC CT TT SVR12 (%) n/n = 0 81/ 71/ Naive 28/ 23/ Relapser Partial Null Responder Responder Factor GT1a GT1b HCV Subtype IL28B Genotype P Value IL28B TT genotype.021 Previous null response to pegifn/rbv.038 GT1a HCV.046 Fried MW, et al. AASLD Abstract 81.
33 SVR12 with LDV/SOF + RBV in Gt1 patients with decompensated cirrhosis LDV/SOF + RBV 12 wks SVR12 (%) LDV/SOF + RBV 24 wks relapses 1 death 40 1 relapse 1 death 1 LTFU 1 relapse 2 deaths /52 42/47 26/30 Overall 24/27 19/22 CPT B Pts, n (%) 1 relapse 1 death 18/20 CPT C CPT B CPT C 12 Wks (n = 30) 24 Wks (n = 29) 12 Wks (n = 23) 24 Wks (n = 26) AE 29 (97) 27 (93) 23 () 26 () SAE 3 (10) 10 (34) 6 (26) 11 (42) Treatment-emergent, -related SAEs 2 (7) (8) Treatment discontinuation due to AE 0 1 (3) 0 2 (8) Flamm SL, et al. AASLD Abstract 239. Reproduced with permission.
34 SVR12 SVR12 with LDV/SOF + RBV in Gt1 post-olt patients wk LDV/SOF + RBV 24-wk LDV/SOF + RBV SVR12 (%) 80 1 relapse 2 deaths 1 consent withdrawn n/n = 0 2 relapses 1 death 1 death 1 consent withdrawn 53/ 55 55/ 56 F0-F3 25/ 26 24/ 25 CPT A 2 relapses 1 relapse 3 deaths 22/ 26 15/ 18 CPT B 3 / 5 2 / 3 CPT C In the 24-wk arm, 8 pts with CPT B and 1 pt with CPT C have not reached the follow-up Wk 12 visit MELD scores improved from baseline through follow-up Wk 4 in 15/48 pts with CPT A and 8/41 pts with CPT B disease Reddy RT, et al. AASLD Abstract 8.
35
36
37 IFN free DAA have expanded the pool of treatable patients IFN-free combination regimens dominate the treatment landsca SOF-based regimens are effective in real-world settings Safety demonstrated in noncirrhotic and cirrhotic patients Mild Severe HCV chronic disease spectrum Currently treated Decomp - By enrolling new patients at the extreme of the spectrum - By enforcing need for mass screening for HCV
38 Who should be treated: EASL recommendations 2014 In principle, all patients with chronic HCV infection, but in a situation of limited availability: F3-F4: Priority F2: Reasonable F0-F1: Debatable Informed deferral of treatment for patients with mild disease EASL Online Recommendations on Treatment of Hepatitis C, April 2014
39 AASLD/IDSA: Patients With F3/F4 Fibrosis Have Highest Priority for HCV Treatment When constrained resources prevent treatment of all HCV infection cases, highest priority should be given to patients with advanced fibrosis (Metavir F3) or compensated cirrhosis (Metavir F4), liver transplant recipients, and patients with severe extrahepatic hepatitis C Based on available resources, treatment should be prioritized as necessary so that patients at high risk for liver-related complications and severe extrahepatic hepatitis C complications are given high priority AASLD/IDSA HCV Management Guidance. October 2014.
40 SVR associated with reduced 5-Yr risk of death and HCC in all populations SVR on IFN-based therapy was associated with substantial benefit vs no SVR 62% to 84% reduction in all-cause mortality, 90% reduction in liver transplantation, 68% to 79% reduction in HCC 5-Yr Risk of All-Cause Death by SVR SVR Pts Dead After 5 Yrs (%) General Cirrhotic Pts 1.3 HIVCoinfected Pts Hill AM, et al. AASLD Abstract Yr Risk of HCC by SVR No SVR Pts With HCC After 5 Yrs (%) General 0.9 Cirrhotic Pts HIVCoinfected Pts
41 Survival after P/R treatment in 440 patients with HCV cirrhosis, C-P A5-6 (mean follow-up 7.7 yrs) No esophageal varices before P/R Esophageal varices before P/R Patients alive (%) SVR SVR SVR SVR NoNo SVR SVR Log rank p = Log rank p = No SVR No SVR Di Marco V, submitted

42 Deaths due to HCC or liver decompensation after P/R treatment in 440 patients with HCV cirrhosis Di Marco V, submitted
43 Cost per SVR for GT1 HCV Patients GT1, TREATMENT-NAIVE COST PER SVR GT1, TREATMENT-EXPERIENCED (PI+PR-EXPERIENCED) , GT1, TREATMENT-EXPERIENCED (PR-EXPERIENCED) COST PER SVR COST PER SVR *SOF+SMV data from Phase IIb study and 12W regimen for NC, 24W regimen for CC patients as per label Younossi, AASLD, 2014, Poster # ,
44 Evaluation of Health Outcomes from LDV/SOF Treatment of Patients with Early vs. Advanced Liver Fibrosis Initiating LDV/SOF treatment at F0-F1 and F2 rather than F3-F4 reduces lifetime costs of treatment, and has a lower cost per SVR COST PER SVR LIFETIME COSTS Initiating LDV / SOF treatment in F0-F1 or F2 as opposed to F3-F4 results in substantial savings per successfully treated patient (cost per SVR) and lifetime costs. Ahmed A, AASLD, 2014, #1751

45 Hepatologist HCV
IFN-free therapy in naïve HCV GT1 patients
 IFN-free therapy in naïve HCV GT1 patients Paris Hepatitis Conference Paris, 12th January, 2015 Pr Tarik Asselah MD, PhD; Service d Hépatologie & INSERM U773 University Paris Diderot, Hôpital Beaujon,
IFN-free therapy in naïve HCV GT1 patients Paris Hepatitis Conference Paris, 12th January, 2015 Pr Tarik Asselah MD, PhD; Service d Hépatologie & INSERM U773 University Paris Diderot, Hôpital Beaujon,
HCV In 2015: Maximizing SVR
 HCV In 2015: Maximizing SVR Alnoor Ramji Gastroenterology & Hepatology Clinical Associate Professor Division of Gastroenterology University Of British Columbia ramji_a@hotmail.com Disclosures (within Last
HCV In 2015: Maximizing SVR Alnoor Ramji Gastroenterology & Hepatology Clinical Associate Professor Division of Gastroenterology University Of British Columbia ramji_a@hotmail.com Disclosures (within Last
HCV Treatment Failure: What Next? Dr Ashley Brown, Imperial College Healthcare NHS Trust, London
 HCV Treatment Failure: What Next? Dr Ashley Brown, Imperial College Healthcare NHS Trust, London European HIV Hepatitis Co-infection Conference QEII Conference Centre 10 th December 2015 Dr Ashley Brown
HCV Treatment Failure: What Next? Dr Ashley Brown, Imperial College Healthcare NHS Trust, London European HIV Hepatitis Co-infection Conference QEII Conference Centre 10 th December 2015 Dr Ashley Brown
Why make this statement?
 HCV Council 2014 10 clinical practice statements were evaluated by the Council A review of the available literature was conducted The level of support and level of evidence for the statements were discussed
HCV Council 2014 10 clinical practice statements were evaluated by the Council A review of the available literature was conducted The level of support and level of evidence for the statements were discussed
Initial Treatment of HCV G Hugo E. Vargas, MD Professor of Medicine Medical, Director Office of Clinical Research Mayo Clinic Arizona
 Initial Treatment of HCV G1 2016 Hugo E. Vargas, MD Professor of Medicine Medical, Director Office of Clinical Research Mayo Clinic Arizona Disclosure Information Disclosure Information Dr. Vargas receives
Initial Treatment of HCV G1 2016 Hugo E. Vargas, MD Professor of Medicine Medical, Director Office of Clinical Research Mayo Clinic Arizona Disclosure Information Disclosure Information Dr. Vargas receives
Tough Cases in HIV/HCV Coinfection
 NORTHWEST AIDS EDUCATION AND TRAINING CENTER Tough Cases in HIV/HCV Coinfection John Scott, MD, MSc Assistant Professor University of Washington Presentation prepared by: J Scott Last Updated: Jun 5, 2014
NORTHWEST AIDS EDUCATION AND TRAINING CENTER Tough Cases in HIV/HCV Coinfection John Scott, MD, MSc Assistant Professor University of Washington Presentation prepared by: J Scott Last Updated: Jun 5, 2014
Future strategies with new DAAs
 Future strategies with new DAAs Ola Weiland professor New direct antiviral drugs Case no 1 male with genotype 2b Male with gt 2b chronic HCV Male with gt 2b relapse afer peg-ifn + RBV during 24 weeks
Future strategies with new DAAs Ola Weiland professor New direct antiviral drugs Case no 1 male with genotype 2b Male with gt 2b chronic HCV Male with gt 2b relapse afer peg-ifn + RBV during 24 weeks
What is the Optimized Treatment Duration? To Overtreat versus Undertreat. Nancy Reau, MD Associate Professor of Medicine University of Chicago
 What is the Optimized Treatment Duration? To Overtreat versus Undertreat Nancy Reau, MD Associate Professor of Medicine University of Chicago Learning Objectives: 1. Discuss patient populations appropriate
What is the Optimized Treatment Duration? To Overtreat versus Undertreat Nancy Reau, MD Associate Professor of Medicine University of Chicago Learning Objectives: 1. Discuss patient populations appropriate
Update on the Treatment of HCV
 Update on the Treatment of HCV K. Rajender Reddy, MD Professor of Medicine Director of Hepatology Director, Viral Hepatitis Center University of Pennsylvania Philadelphia, USA 1 K. Rajender Reddy, MD Disclosure
Update on the Treatment of HCV K. Rajender Reddy, MD Professor of Medicine Director of Hepatology Director, Viral Hepatitis Center University of Pennsylvania Philadelphia, USA 1 K. Rajender Reddy, MD Disclosure
Case 4: A 61-year-old man with HCV genotype 3 with cirrhosis. Ira M. Jacobson, M.D. Weill Cornell Medical College New York, New York USA
 Case 4: A 61-year-old man with HCV genotype 3 with cirrhosis Ira M. Jacobson, M.D. Weill Cornell Medical College New York, New York USA 1 Genotype 3 case 61-year-old man with HCV genotype 3 Cirrhosis on
Case 4: A 61-year-old man with HCV genotype 3 with cirrhosis Ira M. Jacobson, M.D. Weill Cornell Medical College New York, New York USA 1 Genotype 3 case 61-year-old man with HCV genotype 3 Cirrhosis on
Rome, February nd Riunione Annuale AISF th AISF ANNUAL MEETING
 Rome, February 20-21 nd 2014 Riunione Annuale AISF 2014 14 th AISF ANNUAL MEETING Present and future treatment strategies for patients with HCV infection: chronic hepatitis and special populations IFN
Rome, February 20-21 nd 2014 Riunione Annuale AISF 2014 14 th AISF ANNUAL MEETING Present and future treatment strategies for patients with HCV infection: chronic hepatitis and special populations IFN
Update in the Management of Hepatitis C: What Does the Future Hold
 Update in the Management of Hepatitis C: What Does the Future Hold Paul Y Kwo, MD, FACG Professor of Medicine Mdi Medical ldirector, Liver Transplantation tti Gastroenterology/Hepatology Division Indiana
Update in the Management of Hepatitis C: What Does the Future Hold Paul Y Kwo, MD, FACG Professor of Medicine Mdi Medical ldirector, Liver Transplantation tti Gastroenterology/Hepatology Division Indiana
4/30/2015. Interactive Case-Based Presentations and Audience Discussion. Debika Bhattacharya, MD, MSc. Learning Objectives
 4/3/215 Interactive Case-Based Presentations and Audience Discussion Debika Bhattacharya, MD, MSc Assistant Clinical Professor University of California Los Angeles Los Angeles, California Formatted:4-27-215
4/3/215 Interactive Case-Based Presentations and Audience Discussion Debika Bhattacharya, MD, MSc Assistant Clinical Professor University of California Los Angeles Los Angeles, California Formatted:4-27-215
Current Treatment Options for HCV Patients. Michael Manns Dept. of Gastroenterology, Hepatology and Endocrinology Hannover Germany
 Current Treatment Options for HCV Patients Michael Manns Dept. of Gastroenterology, Hepatology and Endocrinology Hannover Germany 7th International Congress of Internal Medicine of Central Greece, Larissa,
Current Treatment Options for HCV Patients Michael Manns Dept. of Gastroenterology, Hepatology and Endocrinology Hannover Germany 7th International Congress of Internal Medicine of Central Greece, Larissa,
Genotype 1 HCV in 2016: Clinical Decision Making in a Time of Plenty
 Genotype 1 HCV in 216: Clinical Decision Making in a Time of Plenty Ira M. Jacobson, MD Chair, Department of Medicine Mount Sinai Beth Israel Senior Faculty and Vice-Chair, Department of Medicine Icahn
Genotype 1 HCV in 216: Clinical Decision Making in a Time of Plenty Ira M. Jacobson, MD Chair, Department of Medicine Mount Sinai Beth Israel Senior Faculty and Vice-Chair, Department of Medicine Icahn
Pivotal New England Journal of Medicine papers 2014 Phase 3 Trial data
 4 th HCV Therapy Advances Meeting Paris, December 12-13, 14 Pivotal New England Journal of Medicine papers 14 Phase 3 Trial data Stefan Zeuzem, MD University of Frankfurt Germany Disclosures Consultancies:
4 th HCV Therapy Advances Meeting Paris, December 12-13, 14 Pivotal New England Journal of Medicine papers 14 Phase 3 Trial data Stefan Zeuzem, MD University of Frankfurt Germany Disclosures Consultancies:
TREATMENT OF GENOTYPE 2
 Treatment of Genotype 2, 3,and 4 David E. Bernstein, MD, FACG Advisory Committee/Board Member: AbbVie Pharmaceuticals, Gilead, Merck, Janssen Consultant: AbbVie Pharmaceuticals, Bristol-Myers Squibb, Gilead,
Treatment of Genotype 2, 3,and 4 David E. Bernstein, MD, FACG Advisory Committee/Board Member: AbbVie Pharmaceuticals, Gilead, Merck, Janssen Consultant: AbbVie Pharmaceuticals, Bristol-Myers Squibb, Gilead,
Baseline and acquired viral resistance to DAAs: how to test and manage
 Baseline and acquired viral resistance to DAAs: how to test and manage Round table discussion by Marc Bourliere, Robert Flisiak, Vasily Isakov, Mark Sulkowsky & Konstantin Zhdanov Prevalence of baseline
Baseline and acquired viral resistance to DAAs: how to test and manage Round table discussion by Marc Bourliere, Robert Flisiak, Vasily Isakov, Mark Sulkowsky & Konstantin Zhdanov Prevalence of baseline
How to optimize treatment in G3 patients? Jérôme GOURNAY, MD Hépatologie Centre Hospitalier Universitaire de Nantes France
 How to optimize treatment in G3 patients? Jérôme GOURNAY, MD Hépatologie Centre Hospitalier Universitaire de Nantes France Paris Hepatitis Conference, January 12, 2016 Disclosures I have received funding
How to optimize treatment in G3 patients? Jérôme GOURNAY, MD Hépatologie Centre Hospitalier Universitaire de Nantes France Paris Hepatitis Conference, January 12, 2016 Disclosures I have received funding
HCV Treatment of Genotype 1: Now and in the Future
 HCV Treatment of Genotype 1: Now and in the Future Bruce R. Bacon, MD, FACG James F. King, MD Endowed Chair in Gastroenterology Professor of Internal Medicine Co-Director of the Abdominal Transplant Program
HCV Treatment of Genotype 1: Now and in the Future Bruce R. Bacon, MD, FACG James F. King, MD Endowed Chair in Gastroenterology Professor of Internal Medicine Co-Director of the Abdominal Transplant Program
Hepatitis C in Special Populations
 Hepatitis C in Special Populations David E. Bernstein, MD, FACG Vice Chairman of Medicine for Clinical Trials Chief, Division of Hepatology and Sandra Atlas Bass Center for Liver Diseases Northwell Health
Hepatitis C in Special Populations David E. Bernstein, MD, FACG Vice Chairman of Medicine for Clinical Trials Chief, Division of Hepatology and Sandra Atlas Bass Center for Liver Diseases Northwell Health
Ari Bunim, M.D. Director of Hepatology New York Hospital Queens Assistant Professor of Clinical Medicine Weill Cornell Medical College
 Ari Bunim, M.D. Director of Hepatology New York Hospital Queens Assistant Professor of Clinical Medicine Weill Cornell Medical College New York State Law Goes into Effect January 1, 2014 Hepatitis C Virus
Ari Bunim, M.D. Director of Hepatology New York Hospital Queens Assistant Professor of Clinical Medicine Weill Cornell Medical College New York State Law Goes into Effect January 1, 2014 Hepatitis C Virus
Terapie attuali. Eradicazione di HCV e nuove prospettive:
 Eradicazione di HCV e nuove prospettive: Terapie attuali Luisa Pasulo U.S.C. Gastroenterologia Epatologia e Trapiantologia Ospedale Papa Giovanni XXIII - Bergamo From Infection to liver disease Infezione
Eradicazione di HCV e nuove prospettive: Terapie attuali Luisa Pasulo U.S.C. Gastroenterologia Epatologia e Trapiantologia Ospedale Papa Giovanni XXIII - Bergamo From Infection to liver disease Infezione
The HCV Pipeline Ira M. Jacobson, MD, FACP, FACG, AGAF. Slide Presentation. IFN-free DAA combinations (G1)
") Slide Presentation The HCV Pipeline Vincent Astor Distinguished Professor of Medicine Chief, Division of Gastroenterology and Hepatology Medical Director, Center for the Study of Hepatitis C Weill Cornell
Slide Presentation The HCV Pipeline Vincent Astor Distinguished Professor of Medicine Chief, Division of Gastroenterology and Hepatology Medical Director, Center for the Study of Hepatitis C Weill Cornell
Treatement Experienced patients without cirrhosis. Rafael Esteban Hospital Universitario Valle Hebron Barcelona
 Treatement Experienced patients without cirrhosis Rafael Esteban Hospital Universitario Valle Hebron Barcelona Agenda With IFN PegIFN+ Ribavirin + Simeprevir PegIFN+ Ribavirin+ Sofosbuvir Without IFN Sofosbuvir
Treatement Experienced patients without cirrhosis Rafael Esteban Hospital Universitario Valle Hebron Barcelona Agenda With IFN PegIFN+ Ribavirin + Simeprevir PegIFN+ Ribavirin+ Sofosbuvir Without IFN Sofosbuvir
IL TRAPIANTO DI FEGATO: QUALE FUTURO CON LE NUOVE TERAPIE PER LE MALATTIE EPATICHE?
 IL TRAPIANTO DI FEGATO: QUALE FUTURO CON LE NUOVE TERAPIE PER LE MALATTIE EPATICHE? Francesco Paolo Russo Department of Surgery, Oncology and Gastroenterology Multivisceral/ Gastroenterology Section University
IL TRAPIANTO DI FEGATO: QUALE FUTURO CON LE NUOVE TERAPIE PER LE MALATTIE EPATICHE? Francesco Paolo Russo Department of Surgery, Oncology and Gastroenterology Multivisceral/ Gastroenterology Section University
6/2/2015. Interactive Case-Based Presentations and Audience Discussion
 6/2/215 Interactive Case-Based Presentations and Audience Discussion Andrew Aronsohn, MD Assistant Professor of Medicine University of Chicago Medical Center Chicago, Illinois Formatted:5-6-215 Washington,
6/2/215 Interactive Case-Based Presentations and Audience Discussion Andrew Aronsohn, MD Assistant Professor of Medicine University of Chicago Medical Center Chicago, Illinois Formatted:5-6-215 Washington,
Associate Professor of Medicine University of Chicago
 Nancy Reau, MD Associate Professor of Medicine University of Chicago Management of Hepatitis C: New Drugs and New Paradigms HCV is More Lethal than HIV Infection HCV superseded HIV as a cause of death
Nancy Reau, MD Associate Professor of Medicine University of Chicago Management of Hepatitis C: New Drugs and New Paradigms HCV is More Lethal than HIV Infection HCV superseded HIV as a cause of death
5/12/2016. Learning Objectives. Management of Hepatitis C Virus Genotype 2 or 3 Infected Treatment-Naive or Experienced Patients
 5/12/216 Management of Hepatitis C Virus Genotype 2 or 3 Infected Treatment-Naive or Experienced Patients Alexander Monto, MD Professor of Clinical Medicine University of California San Francisco San Francisco,
5/12/216 Management of Hepatitis C Virus Genotype 2 or 3 Infected Treatment-Naive or Experienced Patients Alexander Monto, MD Professor of Clinical Medicine University of California San Francisco San Francisco,
HCV Management in Decompensated Cirrhosis: Current Therapies
 Treatment of Patients with Decompensated Cirrhosis and Liver Transplant Recipients Paul Y. Kwo, MD, FACG Professor of Medicine Gastroenterology/Hepatology Division Stanford University email pkwo@stanford.edu
Treatment of Patients with Decompensated Cirrhosis and Liver Transplant Recipients Paul Y. Kwo, MD, FACG Professor of Medicine Gastroenterology/Hepatology Division Stanford University email pkwo@stanford.edu
HCV therapy : Clinical case
 HCV therapy : Clinical case PHC 2018 Paris January 14th, 2018 Tarik Asselah (MD, PhD) Professor of Medicine Hepatology, Chief INSERM UMR 1149, Hôpital Beaujon, Clichy, France. Disclosures Professor Asselah
HCV therapy : Clinical case PHC 2018 Paris January 14th, 2018 Tarik Asselah (MD, PhD) Professor of Medicine Hepatology, Chief INSERM UMR 1149, Hôpital Beaujon, Clichy, France. Disclosures Professor Asselah
Antiviral treatment in HCV cirrhotic patients on waiting list
 Antiviral treatment in HCV cirrhotic patients on waiting list Krzysztof Tomasiewicz Department of Hepatology and Infectious Diseases Medical University of Lublin, Poland Disclosures Consultancy/Advisory
Antiviral treatment in HCV cirrhotic patients on waiting list Krzysztof Tomasiewicz Department of Hepatology and Infectious Diseases Medical University of Lublin, Poland Disclosures Consultancy/Advisory
Treatment of HCV in 2016
 5/1/16 Treatment of HCV in 16 Graham R Foster Professor of Hepatology QMUL Conflicts of Interest Speaker and consultancy fees received from AbbVie, BI, BMS, Gilead, Janssen, Roche, Merck, Novartis, Springbank,
5/1/16 Treatment of HCV in 16 Graham R Foster Professor of Hepatology QMUL Conflicts of Interest Speaker and consultancy fees received from AbbVie, BI, BMS, Gilead, Janssen, Roche, Merck, Novartis, Springbank,
Management of HCV Tawesak Tanwandee
 Management of HCV 2016 Tawesak Tanwandee Topics Burden of HCV in our countries Natural history and unmet need for HCV treatment Current treatment as for 2016 Conclusion Evolution from HCV infection to
Management of HCV 2016 Tawesak Tanwandee Topics Burden of HCV in our countries Natural history and unmet need for HCV treatment Current treatment as for 2016 Conclusion Evolution from HCV infection to
Can we afford to Cure all HIV-HCV Co-infected Patients of HCV?
 Can we afford to Cure all HIV-HCV Co-infected Patients of HCV? Michael S. Saag, MD Professor of Medicine University of Alabama at Birmingham Birmingham, Alabama FINAL AU EDITED: 09-17-14 Disclosure Dr
Can we afford to Cure all HIV-HCV Co-infected Patients of HCV? Michael S. Saag, MD Professor of Medicine University of Alabama at Birmingham Birmingham, Alabama FINAL AU EDITED: 09-17-14 Disclosure Dr
Selecting HCV Treatment
 Selecting HCV Treatment Caveats Focus on treatment selection for genotypes 1, 2, and 3. Majority of US population infected with GT 1, 2, or 3 GT 4 treatment closely reflects GT 1 treatment GT 5 and 6 are
Selecting HCV Treatment Caveats Focus on treatment selection for genotypes 1, 2, and 3. Majority of US population infected with GT 1, 2, or 3 GT 4 treatment closely reflects GT 1 treatment GT 5 and 6 are
A treatment revolution: current management for chronic HCV
 A treatment revolution: current management for chronic HCV Ray Chung, M.D. Director of Hepatology and Liver Center Kevin and Polly Maroni Research Scholar Massachusetts General Hospital Disclosures Research
A treatment revolution: current management for chronic HCV Ray Chung, M.D. Director of Hepatology and Liver Center Kevin and Polly Maroni Research Scholar Massachusetts General Hospital Disclosures Research
Drug Class Monograph
 Drug Class Monograph Class: Chronic Hepatitis C Drugs(s): Daclatasvir (Daklinza), Dasabuvir/ombitasivir/paritaprevir/ritonavir (Viekira Pak), Elbasvir/grazoprevir (Zepatier), Peginterferon alfa-2a (Pegasys),
Drug Class Monograph Class: Chronic Hepatitis C Drugs(s): Daclatasvir (Daklinza), Dasabuvir/ombitasivir/paritaprevir/ritonavir (Viekira Pak), Elbasvir/grazoprevir (Zepatier), Peginterferon alfa-2a (Pegasys),
The Dawn of a New Era: Hepatitis C
 The Dawn of a New Era: Hepatitis C Naudia L. Jonassaint Assistant Professor of Medicine and Surgery University Pittsburgh School of Medicine December 1, 2015 Objectives After presentation the learner should
The Dawn of a New Era: Hepatitis C Naudia L. Jonassaint Assistant Professor of Medicine and Surgery University Pittsburgh School of Medicine December 1, 2015 Objectives After presentation the learner should
Latest Treatment Updates for GT 2 and GT 3 Patients
 Latest Treatment Updates for GT 2 and GT 3 Patients Eric Lawitz, MD, AGAF, CPI Vice President, Scientific and Research Development The Texas Liver Institute Clinical Professor of Medicine University of
Latest Treatment Updates for GT 2 and GT 3 Patients Eric Lawitz, MD, AGAF, CPI Vice President, Scientific and Research Development The Texas Liver Institute Clinical Professor of Medicine University of
Treatments of Genotype 2, 3,and 4: Now and in the future
 Treatments of Genotype 2, 3,and 4: Now and in the future THERAPY FOR THE TREATMENT OF GENOTYPE 2 1 GT 2 and GT 3 Treatment-Naïve: SOF+RBV vs PEG-IFN+RBV FISSION Study Design HCV GT 2 and GT 3 Treatment-naïve
Treatments of Genotype 2, 3,and 4: Now and in the future THERAPY FOR THE TREATMENT OF GENOTYPE 2 1 GT 2 and GT 3 Treatment-Naïve: SOF+RBV vs PEG-IFN+RBV FISSION Study Design HCV GT 2 and GT 3 Treatment-naïve
Chronic Hepatitis C Drug Class Prior Authorization Protocol
 Line of Business: Medi-Cal Effective Date: August 16, 2017 Revision Date: August 16, 2017 Chronic Hepatitis C Drug Class Prior Authorization Protocol This policy has been developed through review of medical
Line of Business: Medi-Cal Effective Date: August 16, 2017 Revision Date: August 16, 2017 Chronic Hepatitis C Drug Class Prior Authorization Protocol This policy has been developed through review of medical
Drug Class Prior Authorization Criteria Hepatitis C
 Drug Class Prior Authorization Criteria Hepatitis C Line of Business: Medicaid P & T Approval Date: Interim Criteria Pending P&T Approval Effective Date: August 16, 2018 This drug class prior authorization
Drug Class Prior Authorization Criteria Hepatitis C Line of Business: Medicaid P & T Approval Date: Interim Criteria Pending P&T Approval Effective Date: August 16, 2018 This drug class prior authorization
2017 Bruce Lucas Hepatology and Liver Transplant Symposium October 13th 2017 Management of Hepatitis C in Pre- and Post-Transplant Patients
 2017 Bruce Lucas Hepatology and Liver Transplant Symposium October 13th 2017 Management of Hepatitis C in Pre- and Post-Transplant Patients Jens Rosenau, MD Associate Professor of Medicine Acting Director
2017 Bruce Lucas Hepatology and Liver Transplant Symposium October 13th 2017 Management of Hepatitis C in Pre- and Post-Transplant Patients Jens Rosenau, MD Associate Professor of Medicine Acting Director
HARVARD PILGRIM HEALTH CARE RECOMMENDED MEDICATION REQUEST GUIDELINES
 HARVARD PILGRIM HEALTH CARE Generic Brand HICL GCN Exception/Other DACLATASVIR DAKLINZA 41377 ELBASVIR/GRAZOPREVIR ZEPATIER 43030 GLECAPREVIR/PIBRENTASVIR MAVYRET 44453 OMBITASVIR/PARITAPREVIR/ RITONAVIR
HARVARD PILGRIM HEALTH CARE Generic Brand HICL GCN Exception/Other DACLATASVIR DAKLINZA 41377 ELBASVIR/GRAZOPREVIR ZEPATIER 43030 GLECAPREVIR/PIBRENTASVIR MAVYRET 44453 OMBITASVIR/PARITAPREVIR/ RITONAVIR
Will difficult-to-treat patients remain difficultto-treat. generation of treatments?
 Will difficult-to-treat patients remain difficultto-treat with the new generation of treatments? Jordan J Feld MD MPH Toronto Centre for Liver Disease Sandra Rotman Centre for Global Health University
Will difficult-to-treat patients remain difficultto-treat with the new generation of treatments? Jordan J Feld MD MPH Toronto Centre for Liver Disease Sandra Rotman Centre for Global Health University
Evolution of Therapy in HCV
 Hepatitis C: Update on New Therapies and AASLD 13 David Bernstein, MD, FACP, AGAF, FACP Professor of Medicine Hofstra North Shore-LIJ School of Medicine Evolution of Therapy in HCV 199 1999 1 13 (%) SVR
Hepatitis C: Update on New Therapies and AASLD 13 David Bernstein, MD, FACP, AGAF, FACP Professor of Medicine Hofstra North Shore-LIJ School of Medicine Evolution of Therapy in HCV 199 1999 1 13 (%) SVR
THE LIVER MEETING 2014:
 THE LIVER MEETING 2014: Summary of presentations from the 65 th Annual Liver Meeting of the American Association for the of Liver Diseases (AASLD), held in Boston, Massachusetts, USA, on 7 th -11 th November
THE LIVER MEETING 2014: Summary of presentations from the 65 th Annual Liver Meeting of the American Association for the of Liver Diseases (AASLD), held in Boston, Massachusetts, USA, on 7 th -11 th November
Hepatitis C Emerging Treatment Paradigms
 Hepatitis C Emerging Treatment Paradigms David R Nelson MD Assistant Vice President for Research Professor of Medicine Director, Clinical and Translational Science Institute University of Florida Gainesville,
Hepatitis C Emerging Treatment Paradigms David R Nelson MD Assistant Vice President for Research Professor of Medicine Director, Clinical and Translational Science Institute University of Florida Gainesville,
I nuovi farmaci per HCV: frequenza della patologia, evidenze di efficacia e sicurezza, strategie di gestione. la pratica clinica
 I nuovi farmaci per HCV: frequenza della patologia, evidenze di efficacia e sicurezza, strategie di gestione La revisione ii delle dll evidenze e indicazioni i iper la pratica clinica Marco Marzioni Segretario
I nuovi farmaci per HCV: frequenza della patologia, evidenze di efficacia e sicurezza, strategie di gestione La revisione ii delle dll evidenze e indicazioni i iper la pratica clinica Marco Marzioni Segretario
Transformation of Chronic Hepatitis C Treatment
 Transformation of Chronic Hepatitis C Treatment UVHS, Adana, 22 May 2015 Christoph Sarrazin Goethe-University Hospital Frankfurt am Main Germany Epidemiology of HCV Infection Global Global HCV Prevalence
Transformation of Chronic Hepatitis C Treatment UVHS, Adana, 22 May 2015 Christoph Sarrazin Goethe-University Hospital Frankfurt am Main Germany Epidemiology of HCV Infection Global Global HCV Prevalence
VII CURSO AVANCES EN INFECCIÓN VIH Y HEPATITIS VIRALES
 VII CURSO AVANCES EN INFECCIÓN VIH Y HEPATITIS VIRALES REGIMENES TERAPÊUTICOS DE LA HEPATITIS C, INTERFERÓN FREE A Coruña 2 Febrero 2013 Rui Sarmento e Castro Centro Hospitalar do Porto HJU ECS Universidade
VII CURSO AVANCES EN INFECCIÓN VIH Y HEPATITIS VIRALES REGIMENES TERAPÊUTICOS DE LA HEPATITIS C, INTERFERÓN FREE A Coruña 2 Febrero 2013 Rui Sarmento e Castro Centro Hospitalar do Porto HJU ECS Universidade
Drug Class Prior Authorization Criteria Hepatitis C
 Drug Class Prior Authorization Criteria Hepatitis C Line of Business: Medicaid P & T Approval Date: Interim (pending P&T approval) Effective Date: July 1, 2018 This policy has been developed through review
Drug Class Prior Authorization Criteria Hepatitis C Line of Business: Medicaid P & T Approval Date: Interim (pending P&T approval) Effective Date: July 1, 2018 This policy has been developed through review
STATE OF THE ART Update: Treatment Options 2016 Mark Sulkowski, MD
 Housekeeping Please turn off or silence cell phones. Restrooms are located on this floor. Make a left out of the ballroom foyer and the men s room is on your left. The ladies room is across from the elevators
Housekeeping Please turn off or silence cell phones. Restrooms are located on this floor. Make a left out of the ballroom foyer and the men s room is on your left. The ladies room is across from the elevators
Feeling right at home
 Feeling right at home Getting to Cure From Cure to Eradication Jordan J. Feld MD MPH Toronto Centre for Liver Disease Sandra Rotman Centre for Global Health University of Toronto SVR Dramatic Improvements
Feeling right at home Getting to Cure From Cure to Eradication Jordan J. Feld MD MPH Toronto Centre for Liver Disease Sandra Rotman Centre for Global Health University of Toronto SVR Dramatic Improvements
A One-day Scientific Conference: Updates on Hepatitis C Treatments along with Consensus on Management of Hepatitis C in Iran
 A One-day Scientific Conference: Updates on Hepatitis C Treatments along with Consensus on Management of Hepatitis C in Iran Teheran, 22 July 2016 Massimo Colombo Treatment of HCV genotype 1 & 4 with DAAs
A One-day Scientific Conference: Updates on Hepatitis C Treatments along with Consensus on Management of Hepatitis C in Iran Teheran, 22 July 2016 Massimo Colombo Treatment of HCV genotype 1 & 4 with DAAs
EASL 2013 Interferon Free, All Oral Regimens for Hepatitis C. Maria Buti Hospital Universitario Valle Hebron Barcelona Spain
 EASL 2013 Interferon Free, All Oral Regimens for Hepatitis C Maria Buti Hospital Universitario Valle Hebron Barcelona Spain The first Results with Oral therapy: a Protease Inhibitor and NS5A inhibitor
EASL 2013 Interferon Free, All Oral Regimens for Hepatitis C Maria Buti Hospital Universitario Valle Hebron Barcelona Spain The first Results with Oral therapy: a Protease Inhibitor and NS5A inhibitor
Failure after treatment with DAAs: What to do? Marseille France 2-3 th June 2016
 Failure after treatment with DAAs: What to do? Marc Bourliere, MD White Nights of Hepatology Hôpital Saint Joseph Saint Petersburg Marseille France 2-3 th June 16 Disclosures Board member for : Schering-Plough,
Failure after treatment with DAAs: What to do? Marc Bourliere, MD White Nights of Hepatology Hôpital Saint Joseph Saint Petersburg Marseille France 2-3 th June 16 Disclosures Board member for : Schering-Plough,
O. Giouleme Assistant Professor of Gastroenterology Ippokration General Hospital of Thessaloniki
 O. Giouleme Assistant Professor of Gastroenterology Ippokration General Hospital of Thessaloniki Disclosures Advisory Board: Abbvie Pharmaceuticals Speaker: Gilead Sciences, Bristol-Myers Squibb Research
O. Giouleme Assistant Professor of Gastroenterology Ippokration General Hospital of Thessaloniki Disclosures Advisory Board: Abbvie Pharmaceuticals Speaker: Gilead Sciences, Bristol-Myers Squibb Research
HEPATITIS C: UPDATE AND MANAGEMENT
 HEPATITIS C: UPDATE AND MANAGEMENT José Franco, MD Professor of Medicine Associate Dean for Educational Improvement Associate Director, Kern Institute STAR Center Director José Franco, MD Disclosures I
HEPATITIS C: UPDATE AND MANAGEMENT José Franco, MD Professor of Medicine Associate Dean for Educational Improvement Associate Director, Kern Institute STAR Center Director José Franco, MD Disclosures I
Hepatitis C Prior Authorization Policy
 Hepatitis C Prior Authorization Policy Line of Business: Medi-Cal P&T Approval Date: November 15, 2017 Effective Date: January 1, 2018 This policy has been developed through review of medical literature,
Hepatitis C Prior Authorization Policy Line of Business: Medi-Cal P&T Approval Date: November 15, 2017 Effective Date: January 1, 2018 This policy has been developed through review of medical literature,
10/21/2016. Susanna Naggie, MD, MHS Associate Professor of Medicine Duke University Durham, North Carolina. Learning Objectives
 A Crash Course on the AASLD/IDSA Hepatitis C Virus Infection Treatment Guidelines: What s New Susanna Naggie, MD, MHS Associate Professor of Medicine Duke University Durham, North Carolina FORMATTED: 1/3/16
A Crash Course on the AASLD/IDSA Hepatitis C Virus Infection Treatment Guidelines: What s New Susanna Naggie, MD, MHS Associate Professor of Medicine Duke University Durham, North Carolina FORMATTED: 1/3/16
CCO Official Conference Coverage: Clinical Impact of New Data From AASLD 2015
 CCO Official Conference Coverage: Clinical Impact of New Data From AASLD 2015 CCO Official Conference Coverage of the 2015 Annual Meeting of the American Association for the Study of Liver Diseases, November
CCO Official Conference Coverage: Clinical Impact of New Data From AASLD 2015 CCO Official Conference Coverage of the 2015 Annual Meeting of the American Association for the Study of Liver Diseases, November
Treatment of Unique Populations Raymond T. Chung, MD
 Treatment of Unique Populations Raymond T. Chung, MD Director of Hepatology and Liver Center Vice Chief, Gastroenterology Kevin and Polly Maroni Research Scholar Mass General Hospital Disclosures Research
Treatment of Unique Populations Raymond T. Chung, MD Director of Hepatology and Liver Center Vice Chief, Gastroenterology Kevin and Polly Maroni Research Scholar Mass General Hospital Disclosures Research
NS5A inhibitors: ideal candidates for combination?
 NS5A inhibitors: ideal candidates for combination? Professor Vasily Isakov, MD, PhD, AGAF Dep.Gastroentrology & Hepatology, ION, Russian Academy of Sciences, Moscow Structure and function of NS5A Meigang
NS5A inhibitors: ideal candidates for combination? Professor Vasily Isakov, MD, PhD, AGAF Dep.Gastroentrology & Hepatology, ION, Russian Academy of Sciences, Moscow Structure and function of NS5A Meigang
Program Disclosure. Provider is approved by the California Board of Registered Nursing, Provider #13664, for 1.5 contact hours.
 Program Disclosure This activity has been planned and implemented in accordance with the Essential Areas and policies of the Accreditation Council for Continuing Medical Education (ACCME) through the joint-sponsorship
Program Disclosure This activity has been planned and implemented in accordance with the Essential Areas and policies of the Accreditation Council for Continuing Medical Education (ACCME) through the joint-sponsorship
Current trends in CHC 1st genotype treatment
 Current trends in CHC 1st genotype treatment Tarik Asselah MD, PhD Professor of Medicine Hepatology, Chief INSERM UMR 1149, Hôpital Beaujon, Clichy, France Disclosures Employee of Paris Public University
Current trends in CHC 1st genotype treatment Tarik Asselah MD, PhD Professor of Medicine Hepatology, Chief INSERM UMR 1149, Hôpital Beaujon, Clichy, France Disclosures Employee of Paris Public University
Treating HCV After Liver Transplantation: What are the Treatment Options?
 4 th OPTIMIZE WORKSHOP USING DAAs IN PATIENTS WITH CIRRHOSIS AND LIVER RECIPIENTS Treating HCV After Liver Transplantation: What are the Treatment Options? Maria Carlota Londoño, MD Liver Unit, Hospital
4 th OPTIMIZE WORKSHOP USING DAAs IN PATIENTS WITH CIRRHOSIS AND LIVER RECIPIENTS Treating HCV After Liver Transplantation: What are the Treatment Options? Maria Carlota Londoño, MD Liver Unit, Hospital
Update on chronic hepatitis C treatment: current trends, new challenges, what next?
 Update on chronic hepatitis C treatment: current trends, new challenges, what next? Matti Maimets 12.06.2015 MMaimets15 Disclosure this presentation is sponsored by Gilead Sciences MMaimets15 MMaimets15
Update on chronic hepatitis C treatment: current trends, new challenges, what next? Matti Maimets 12.06.2015 MMaimets15 Disclosure this presentation is sponsored by Gilead Sciences MMaimets15 MMaimets15
Chronic Hepatitis C Drug Class Monograph
 Chronic Hepatitis C Drug Class Monograph Line of Business: Medi-Cal Effective Date: July 10, 2017 (Interim Guidelines; Final Review and Approval by the P&T Subcommittee Pending) This policy has been developed
Chronic Hepatitis C Drug Class Monograph Line of Business: Medi-Cal Effective Date: July 10, 2017 (Interim Guidelines; Final Review and Approval by the P&T Subcommittee Pending) This policy has been developed
Ledipasvir-Sofosbuvir (Harvoni)
") HEPATITIS WEB STUDY HEPATITIS C ONLINE Ledipasvir-Sofosbuvir (Harvoni) Robert G. Gish MD Professor, Consultant, Stanford University Medical Center Senior Medical Director, St Josephs Hospital and Medical
HEPATITIS WEB STUDY HEPATITIS C ONLINE Ledipasvir-Sofosbuvir (Harvoni) Robert G. Gish MD Professor, Consultant, Stanford University Medical Center Senior Medical Director, St Josephs Hospital and Medical
Direct-acting Antiviral (DAA) Regimens in Late-stage Development: Which Patients Should Wait? Fred Poordad, MD
 Regimens in Late-stage Development: Which Patients Should Wait? Fred Poordad, MD") Direct-acting Antiviral (DAA) Regimens in Late-stage Development: Which Patients Should Wait? Fred Poordad, MD The HCV Lifecycle: Multiple Targets Polymerase Inhibitors Protease Inhibitors NS5A Inhibitors
Direct-acting Antiviral (DAA) Regimens in Late-stage Development: Which Patients Should Wait? Fred Poordad, MD The HCV Lifecycle: Multiple Targets Polymerase Inhibitors Protease Inhibitors NS5A Inhibitors
Wonder pills, breakthroughs and continuing challenges HIV and Hepatitis C antiviral treatments revisited
 Wonder pills, breakthroughs and continuing challenges HIV and Hepatitis C antiviral treatments revisited Harald Hofer Department of Internal Medicine III Division of Gastroenterology and Hepatology Medical
Wonder pills, breakthroughs and continuing challenges HIV and Hepatitis C antiviral treatments revisited Harald Hofer Department of Internal Medicine III Division of Gastroenterology and Hepatology Medical
Drug Class Monograph
 Drug Class Monograph Class: Chronic Hepatitis C Drugs(s): Daclatasvir (Daklinza), Dasabuvir/ombitasivir/paritaprevir/ritonavir (Viekira XR), Elbasvir/grazoprevir (Zepatier), Peginterferon alfa-2a (Pegasys),
Drug Class Monograph Class: Chronic Hepatitis C Drugs(s): Daclatasvir (Daklinza), Dasabuvir/ombitasivir/paritaprevir/ritonavir (Viekira XR), Elbasvir/grazoprevir (Zepatier), Peginterferon alfa-2a (Pegasys),
Individual Optmizaton of therapy. Graham R Foster Professor of Hepatology QMUL
 Individual Optmizaton of therapy Graham R Foster Professor of Hepatology QMUL Conflicts of Interest Speaker and consultancy fees received from AbbVie, BI, BMS, Gilead, Janssen, Roche, Merck, Novarts, Springbank,
Individual Optmizaton of therapy Graham R Foster Professor of Hepatology QMUL Conflicts of Interest Speaker and consultancy fees received from AbbVie, BI, BMS, Gilead, Janssen, Roche, Merck, Novarts, Springbank,
Dr Janice Main Imperial College Healthcare NHS Trust, London
 BHIVA AUTUMN CONFERENCE 2014 Including CHIA Parallel Sessions Dr Janice Main Imperial College Healthcare NHS Trust, London 9-10 October 2014, Queen Elizabeth II Conference Centre, London BHIVA AUTUMN CONFERENCE
BHIVA AUTUMN CONFERENCE 2014 Including CHIA Parallel Sessions Dr Janice Main Imperial College Healthcare NHS Trust, London 9-10 October 2014, Queen Elizabeth II Conference Centre, London BHIVA AUTUMN CONFERENCE
Need to Assess HCV Resistance to DAAs: Is it Useful and When?
 Need to Assess HCV Resistance to DAAs: Is it Useful and When? Stéphane Chevaliez French National Reference Center for Viral Hepatitis B, C and delta Department of Virology & INSERM U955 Henri Mondor Hospital
Need to Assess HCV Resistance to DAAs: Is it Useful and When? Stéphane Chevaliez French National Reference Center for Viral Hepatitis B, C and delta Department of Virology & INSERM U955 Henri Mondor Hospital
The Changing World of Hepatitis C
 The Changing World of Hepatitis C Alnoor Ramji Gastroenterology & Hepatology Clinical Associate Professor Division of Gastroenterology University Of British Columbia St. Paul s Hospital Site Disclosures
The Changing World of Hepatitis C Alnoor Ramji Gastroenterology & Hepatology Clinical Associate Professor Division of Gastroenterology University Of British Columbia St. Paul s Hospital Site Disclosures
Hepatitis C: Difficult-to-treat Patients 11th Paris Hepatology Conference 16th January 2018 Stefan Zeuzem, MD University Hospital, Frankfurt, Germany
 Hepatitis C: Difficult-to-treat Patients 11th Paris Hepatology Conference 16th January 2018 Stefan Zeuzem, MD University Hospital, Frankfurt, Germany PHC 2018 - www.aphc.info Disclosures Advisory boards:
Hepatitis C: Difficult-to-treat Patients 11th Paris Hepatology Conference 16th January 2018 Stefan Zeuzem, MD University Hospital, Frankfurt, Germany PHC 2018 - www.aphc.info Disclosures Advisory boards:
8/5/2014. A new era of HCV clinical management. Direct-Acting Antivirals for Hepatitis C. Goal of HCV treatment is viral cure HIV HBV HCV
 NS5B NS5B 8/5/214 A new era of HCV clinical management Mark Sulkowski, MD Professor of Medicine Medical Director, Viral Hepatitis Center Divisions of Infectious Disease and Gastroenterology/Hepatology
NS5B NS5B 8/5/214 A new era of HCV clinical management Mark Sulkowski, MD Professor of Medicine Medical Director, Viral Hepatitis Center Divisions of Infectious Disease and Gastroenterology/Hepatology
Clinical Management: Treatment of HCV Mono-infection
 Clinical Management: Treatment of HCV Mono-infection Curtis Cooper, MD, FRCPC Associate Professor-University of Ottawa The Ottawa Hospital- Infections Diseases Viral Hepatitis Program- Director Industry
Clinical Management: Treatment of HCV Mono-infection Curtis Cooper, MD, FRCPC Associate Professor-University of Ottawa The Ottawa Hospital- Infections Diseases Viral Hepatitis Program- Director Industry
HEPATITIS WEB STUDY. Treatment of Hepatitis C following Liver Transplantation
 HEPATITIS WEB STUDY Treatment of Hepatitis C following Liver Transplantation Terry D. Box, MD Associate Professor of Medicine Division of Gastroenterology/Hepatology University of Utah Health Sciences
HEPATITIS WEB STUDY Treatment of Hepatitis C following Liver Transplantation Terry D. Box, MD Associate Professor of Medicine Division of Gastroenterology/Hepatology University of Utah Health Sciences
IFN-free for Genotype 1 HCV: the current landscape. Prof. Graham R Foster
 IFN-free for Genotype 1 HCV: the current landscape Prof. Graham R Foster Wonderful new drugs are coming Poordad F, et al. New Engl J Med 2014; online DOI: 10.1056/NEJMoa1402869. 2 The New Drugs Two treatment
IFN-free for Genotype 1 HCV: the current landscape Prof. Graham R Foster Wonderful new drugs are coming Poordad F, et al. New Engl J Med 2014; online DOI: 10.1056/NEJMoa1402869. 2 The New Drugs Two treatment
Case 2: A 71-year-old man with cirrhosis
 Case 2: A 71-year-old man with cirrhosis 1 JM, 71 year old African American male with known cirrhosis Asymptomatic apart from fatigue No prior history of decompensation Past history: Diabetes for 11 years
Case 2: A 71-year-old man with cirrhosis 1 JM, 71 year old African American male with known cirrhosis Asymptomatic apart from fatigue No prior history of decompensation Past history: Diabetes for 11 years
Hepatitis C Treatment 2014
 Hepatitis C Treatment 214 Brendan M. McGuire, MD UAB Liver Center Outline Epidemiology/National History Terminology for Treatment Treatment Considerations Current Treatment Options Genotype 1 (GT 1) Genotype
Hepatitis C Treatment 214 Brendan M. McGuire, MD UAB Liver Center Outline Epidemiology/National History Terminology for Treatment Treatment Considerations Current Treatment Options Genotype 1 (GT 1) Genotype
New developments in HCV research and their implications for front-line practice
 New developments in HCV research and their implications for front-line practice Dr. Curtis Cooper Associate Professor, University of Ottawa Director, Ottawa Hospital Viral Hepatitis Program June 17, 2013
New developments in HCV research and their implications for front-line practice Dr. Curtis Cooper Associate Professor, University of Ottawa Director, Ottawa Hospital Viral Hepatitis Program June 17, 2013
VIRAL LIVER DISEASE. OAG Post DDW Course Westin Prince, Toronto, June 13-14, 2015
 VIRAL LIVER DISEASE OAG Post DDW Course Westin Prince, Toronto, June 13-14, 2015 Financial Interest Disclosure (over the past 24 months) Dr. Paul Marotta Relationships related to this presentation! Research
VIRAL LIVER DISEASE OAG Post DDW Course Westin Prince, Toronto, June 13-14, 2015 Financial Interest Disclosure (over the past 24 months) Dr. Paul Marotta Relationships related to this presentation! Research
Eliminating Hepatitis C from New Zealand
 Eliminating Hepatitis C from New Zealand Catherine Stedman Associate Professor of Medicine, University of Otago, Christchurch Gastroenterology Department, Christchurch Hospital Disclosures I have the following
Eliminating Hepatitis C from New Zealand Catherine Stedman Associate Professor of Medicine, University of Otago, Christchurch Gastroenterology Department, Christchurch Hospital Disclosures I have the following
Case. 63 year old woman now with:
 Case 63 year old woman now with: HCV GT 1b, HCV RNA 6.2 x 10 6 IU/mL Asymptomatic except for fatigue Normal exam ALT 72 IU/mL, Bili 0.9 mg/dl, INR 1.1, Albumin 3.9 g/dl, Creatinine 0.7 mg/dl Normal EGD
Case 63 year old woman now with: HCV GT 1b, HCV RNA 6.2 x 10 6 IU/mL Asymptomatic except for fatigue Normal exam ALT 72 IU/mL, Bili 0.9 mg/dl, INR 1.1, Albumin 3.9 g/dl, Creatinine 0.7 mg/dl Normal EGD
HCV-G3: Sofosbuvir with ledipasvir or daclatasvir?
 HCV-G3: Sofosbuvir with ledipasvir or daclatasvir? Ioannis Goulis, MD Aristotelian University of Thessaloniki XXIII International Hepatitis B & C Meeting of Athens Hadziyannis HCV genotype 3 therapy Chronic
HCV-G3: Sofosbuvir with ledipasvir or daclatasvir? Ioannis Goulis, MD Aristotelian University of Thessaloniki XXIII International Hepatitis B & C Meeting of Athens Hadziyannis HCV genotype 3 therapy Chronic
Approved regimens for cirrhotic patients
 5th Workshop on HCV THERAPY ADVANCES New antivirals in clinical practice Approved regimens for cirrhotic patients Amsterdam, 4-5 december 2015 Disease burden in Spain 400000 350000 300000 F0 Peak cirrhosis
5th Workshop on HCV THERAPY ADVANCES New antivirals in clinical practice Approved regimens for cirrhotic patients Amsterdam, 4-5 december 2015 Disease burden in Spain 400000 350000 300000 F0 Peak cirrhosis
HCV Infection: EASL Clinical Practice Guidelines Francesco Negro University Hospital Geneva Switzerland
 HCV Infection: EASL Clinical Practice Guidelines 2016 Francesco Negro University Hospital Geneva Switzerland Panel Codinat: Jean-Michel Pawlotsky Panel: Alessio Aghemo David Back Geoffrey Dusheiko Xavier
HCV Infection: EASL Clinical Practice Guidelines 2016 Francesco Negro University Hospital Geneva Switzerland Panel Codinat: Jean-Michel Pawlotsky Panel: Alessio Aghemo David Back Geoffrey Dusheiko Xavier
HCV Treatment in 2016
 HCV Treatment in 2016 Hugo E. Vargas, MD Professor of Medicine Mayo College of Medicine Medical Director, Clinical Trials Office Vice Chair, Department of Research Educational Goals Caveats: Cannot cover
HCV Treatment in 2016 Hugo E. Vargas, MD Professor of Medicine Mayo College of Medicine Medical Director, Clinical Trials Office Vice Chair, Department of Research Educational Goals Caveats: Cannot cover
HCV disease: treatment or deferral? Antonio Craxì Gastroenterologia & Epatologia, Di.Bi.M.I.S., Università di Palermo
 HCV disease: treatment or deferral? Antonio Craxì Gastroenterologia & Epatologia, Di.Bi.M.I.S., Università di Palermo antonio.craxi@unipa.it Key factors in deciding to treat or wait Patient factors Urgency
HCV disease: treatment or deferral? Antonio Craxì Gastroenterologia & Epatologia, Di.Bi.M.I.S., Università di Palermo antonio.craxi@unipa.it Key factors in deciding to treat or wait Patient factors Urgency
HIV/HCV Coinfection: Why It Matters and What To Do About It. Cody A. Chastain, MD 10/26/16
 HIV/HCV Coinfection: Why It Matters and What To Do About It Cody A. Chastain, MD 10/26/16 Disclosures I have no relevant financial disclosures. Objectives At the end of this lecture, the learner will be
HIV/HCV Coinfection: Why It Matters and What To Do About It Cody A. Chastain, MD 10/26/16 Disclosures I have no relevant financial disclosures. Objectives At the end of this lecture, the learner will be
HIV and Hepatitis C Have we finally slayed the beast?
 HIV and Hepatitis C Have we finally slayed the beast? Mark W. Sonderup Division of Hepatology Department of Medicine University of Cape Town & Groote Schuur Hospital Accelerated Fibrosis in HIV-HCV co-infected
HIV and Hepatitis C Have we finally slayed the beast? Mark W. Sonderup Division of Hepatology Department of Medicine University of Cape Town & Groote Schuur Hospital Accelerated Fibrosis in HIV-HCV co-infected
Hepatitis C Resistance Associated Variants (RAVs)
") Hepatitis C Resistance Associated Variants (RAVs) Atif Zaman, MD MPH Oregon Health & Science University Professor of Medicine Division of Gastroenterology and Hepatology Nothing to disclose Disclosure
Hepatitis C Resistance Associated Variants (RAVs) Atif Zaman, MD MPH Oregon Health & Science University Professor of Medicine Division of Gastroenterology and Hepatology Nothing to disclose Disclosure
Special developments in the management of Hepatitis C. Disclosures
 Special developments in the management of Hepatitis C Sandeep Mukherjee,MD Division of Gastroenterology CHI Health and Creighton University Medical Center Omaha, NE 68154 Sandeep.Mukherjee@alegent.org
Special developments in the management of Hepatitis C Sandeep Mukherjee,MD Division of Gastroenterology CHI Health and Creighton University Medical Center Omaha, NE 68154 Sandeep.Mukherjee@alegent.org
Viva La Revolución: Options to Combat Hepatitis C
 Viva La Revolución: Options to Combat Hepatitis C David L. Wyles, MD Professor of Medicine University of Colorado Chief, Division of Infectious Disease Denver Health Learning Objectives After attending
Viva La Revolución: Options to Combat Hepatitis C David L. Wyles, MD Professor of Medicine University of Colorado Chief, Division of Infectious Disease Denver Health Learning Objectives After attending
PHARMACY PRIOR AUTHORIZATION Hepatitis C Clinical Guideline
 PHARMACY PRIOR AUTHORIZATION Hepatitis C Clinical Guideline Preferred Regimen Based on Diagnosis: Mavyret (glecaprevir/pibrentasvir ) Non-Preferred: Daklinza (daclatasvir) Epclusa (sofosbuvir/velpatasvir)
PHARMACY PRIOR AUTHORIZATION Hepatitis C Clinical Guideline Preferred Regimen Based on Diagnosis: Mavyret (glecaprevir/pibrentasvir ) Non-Preferred: Daklinza (daclatasvir) Epclusa (sofosbuvir/velpatasvir)