Pain, Opioids, & Substance Use Disorders
|
|
|
- Hilary O’Brien’
- 6 years ago
- Views:
Transcription
1 Pain, Opioids, & Substance Use Disorders Kenny Jackson, PharmD, CPE Professor & Senior Associate Dean for Academic Affairs College of Pharmacy Larkin University Miami, Florida Editor-in-Chief Journal of Pain & Palliative Care Pharmacotherapy
2 Disclosure Statement Employee of Depomed, Inc. from February 2016 February No other disclosures.
3 Learning Objectives Define the following terms: physical dependence, tolerance, addiction, and substance use disorder. List tools that assist providers in determining pain levels in patients who are recovering from addiction and explain how the information from these tools can be utilized when selecting an appropriate analgesic regimen. Discuss strategies that can be implemented by providers to ensure effective pain management for patients in addiction recovery, including opioid treatment agreements and opioid regimen selection. Describe methods to treat opioid use disorder while concurrently treating pain.
4 Pain is a Problem! Condition Incidence Source Chronic Pain Diabetes Coronary Heart Disease (heart attack & chest pain) Stroke 100 million Americans 25.8 million Americans (diagnosed & estimated undiagnosed) 16.3 million Americans 7.0 million Americans Institute of Medicine of The National Academies American Diabetes Association American Heart Association Cancer 11.9 million Americans American Cancer Society
5 Chronic Pain 22% of primary care visits focus on pain Chronic pain patients visit primary care providers up to 5 times more often than patients with other chronic conditions Cost to United States (US) healthcare is $ billion/year Lost productivity estimated $ billion/year Opioids accounted for 20% of overall drug cost $3.57 billion/year between Rasu RS, et al. J Manag Care Pharm
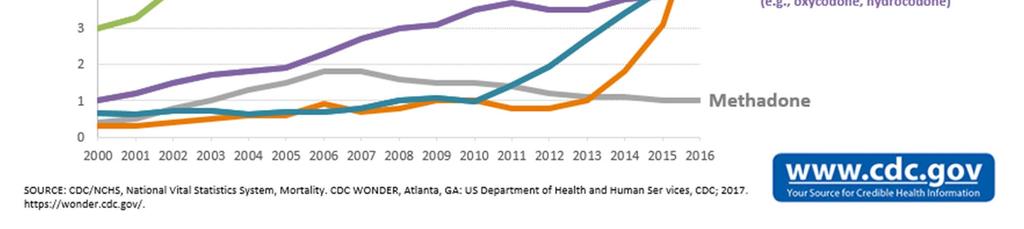
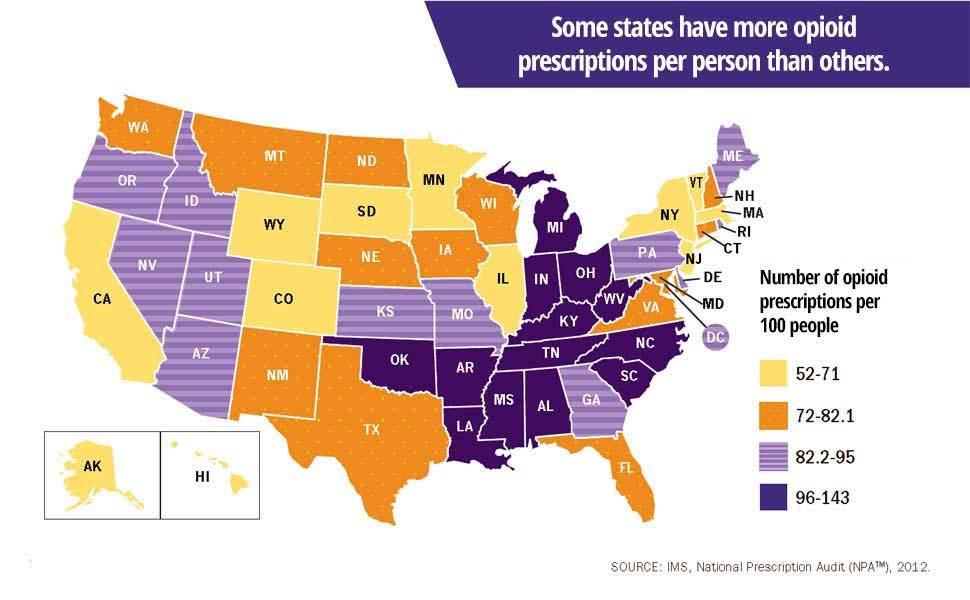
6 US Opioid Consumption 2011 Drug mg/capita ME mg/capita Fentanyl Hydromorphone Methadone Morphine Oxycodone Meperidine Total Morphine Equivalence states america
7
8
9
10
11 How do we reconcile these problems?

12 Terminology Associated with Opioids Addiction Pseudo addiction Physical Dependence Tolerance Pseudo tolerance Substance Use Disorder

13 What is opioiphobia? Question
14 Answer Opioiphobia the irrational fear by clinicians and/or patients related to appropriate opioid use for analgesic purposes. This phenomenon appears to be due in part to misunderstanding such terms as addiction, dependence & tolerance.



15 Narcotic Narcotic a term many clinicians still inappropriately use when they refer to opioid analgesics. This archaic term was used to describe opium & its derivatives in prior generations. Today the word narcotic is a legal term that includes a wide range of sedating & potentially abused substances, & is no longer limited to opioid analgesics.
16 What is this? HG is a 39 yr old caucasian female with intermittent back pain. Never diagnosed, never prescribed opioids. She is routinely chewing controlled release oxycodone that is prescribed for her mother, although her mother is unaware of this. HG is always calling the physician & pharmacy to pick up the Rx early for her mother.

17 Addiction Compulsive use of a substance resulting in physical psychological, or social harm to the user and Continued use despite of that harm Rinaldi R et al. JAMA 1988;259:555-7.
18 Addiction Short Definition Addiction is a primary, chronic disease of brain reward, motivation, memory & related circuitry. Dysfunction in these circuits leads to characteristic biological, psychological, social & spiritual manifestations. This is reflected in an individual pathologically pursuing reward and/or relief by substance use & other behaviors. Addiction is characterized by inability to consistently abstain, impairment in behavioral control, craving, diminished recognition of significant problems with one s behaviors & interpersonal relationships, & a dysfunctional emotional response. Like other chronic diseases, addiction often involves cycles of relapse & remission. Without treatment or engagement in recovery activities, addiction is progressive & can result in disability or premature death. American Society of Addiction Medicine Public Policy Statement April 2011
19 Substance Use Disorder: DSM 5 Criteria Mild: 2 3 criteria; Moderate: 4 5 criteria; Severe: > 6 criteria 1. Taking the substance in larger amounts & for longer than intended 2. Wanting to cut down or quit substance use but not being able to do it 3. Spending a lot of time obtaining the substance 4. Craving or a strong desire to use substance 5. Repeatedly unable to carry out major obligations at work, school, or home due to substance use 6. Continued use despite persistent or recurring social or interpersonal problems caused or made worse by substance use
20 Substance Use Disorder: DSM 5 Criteria 7. Stopping or reducing important social, occupational, or recreational activities due to substance use 8. Recurrent use of substance in physically hazardous situations 9. Consistent use of substance despite acknowledgment of persistent or recurrent physical or psychological difficulties from use 10. Tolerance defined by either a need for markedly increased amounts to achieve intoxication or desired effect or markedly diminished effect with continued use of the same amount (Does not apply for diminished effect when used appropriately under medical supervision) 11. Withdrawal manifesting as either characteristic syndrome or the substance is used to avoid withdrawal (Does not apply when used appropriately under medical supervision)
21 What is this? DP is a 52 yr old Hispanic female with chronic headaches. She has been prescribed hydrocodone/apap 5/500 mg & has been using 4 6 tablets daily for the past 3 months & is now out of her prescription for the past 24 hours. She presents to the clinic with tremors, severe nausea & is sweating profusely. She states she really needs her drugs!!!
22 Physical Dependence A physiological phenomenon characterized by: abstinence syndrome upon abrupt discontinuation substantial dose reduction administration of an antagonist Occurs with steroids & many other drugs nearly universal with regularly scheduled opioids Rinaldi R et al. JAMA 1988;259:555-7.
23 Opioids & Dependence Abstinence syndrome can be induced By administration of an antagonist By marked dose reduction Time to onset variable May occur as soon as after a few days of consistent dosing Marked inter patient variability Not clinically significant if abstinence syndrome avoided Does not independently cause or indicate addiction


24 Tolerance Is tolerance a good thing, a bad thing or just a thing?
25 Opioid Tolerance Tolerance Diminished drug effect from drug exposure Varied types: associative vs pharmacologic Tolerance to side effects is desirable Tolerance to analgesia is seldom a problem in the clinical setting Tolerance rarely drives dose escalation Tolerance does not cause addiction

26 Types of Opioid Tolerance Tolerance to Analgesia may occur in first days to weeks of therapy; Rare after pain relief achieved with consistent Dosing without increasing or new pathology. Tolerance to Respiratory Depression & Sedation occurs predictably after 5 7 days of consistent opioid administration. Tolerance to Constipation does not occur; scheduled stimulating laxatives are indicated with regularly scheduled opioids. Jackson KC, Lipman AG. Opioid Analgesics. In Tollison, et al. editors. Practical Pain Management., 3 rd Edition, Lippincott, Williams, & Wilkins, 2001.
27 What is this? VB is a 25 yr old African American male with diabetic peripheral neuropathy. He has been prescribed methadone 5 mg PO BID + Morphine Sulfate IR 10 mg PO Q4H prn pain. (Rx for 60 tabs monthly) VB has called early each month (x4 months) for morphine & states the methadone doesn t work. Really wants to see if can get more morphine (2 3 tabs/dose effective) or if can switch to oxycodone.
28 Pseudo addiction Appropriate drug seeking behavior Presents as aberrant drug related behaviors Driven by poor pain control Patients demand dose increases/refills before scheduled Viscous cycle of anger, isolation, & avoidance leading to complete distrust Can be relieved by improved analgesia Weissman DE, Haddox DJ. Pain 1989;36:363-6.

29 Pseudo addiction How aberrant can behavior be before it is inconsistent with pseudo addiction? Can addiction & pseudo addiction coexist?
30 What is this? RY is a 29 yr old male Vietnamese American with postherpetic neuralgia. He has been receiving morphine sulfate immediate release 10 mg every 4 hours prn pain for the past couple weeks & uses an average of 3 doses daily with good pain relief. He recently has been discharged & states he is now needing 5 6 doses daily for pain relief.
31 Progressive disease New pathology Excessive activity Noncompliance Medication changes Drug interaction Drug diversion Addiction Pappagallo M. J Pharm Care Pain Sympt Control 1998; 6(2):95-98.

32
33 CDC Opioid Guidelines Recommendation Highlights Determining When to Initiate or Continue Opioids for Chronic Pain Recommendation 2: (category: A; evidence type: 4) Before starting opioid therapy for chronic pain, clinicians establish treatment goals, including realistic goals for pain & function, & consider how opioid therapy will be discontinued if benefits do not outweigh risks. Clinicians should continue opioid therapy only if there is clinically meaningful improvement in pain & function that outweighs risks to patient safety. Clinicians may use validated instruments such as the 3 item Pain average, interference with Enjoyment of life, & interference with General activity (PEG) Assessment Scale 103 to track patient outcomes. Clinically meaningful improvement has been defined as a 30% improvement in scores for both pain & function. Because depression, anxiety, & other psychological comorbidities often coexist with & can interfere with resolution of pain, clinicians should use validated instruments to assess for these conditions & ensure that treatment for these conditions is optimized.
34 CDC Opioid Guidelines Recommendation Highlights Determining When to Initiate or Continue Opioids for Chronic Pain Recommendation 3: (category: A; evidence type: 3) Before starting & periodically during opioid therapy, clinicians should discuss with patients known risks & realistic benefits of opioid therapy & patient & clinician responsibilities for managing therapy.
35 CDC Opioid Guidelines Recommendation Highlights Opioid Selection, Dosage, Duration, Follow up, & Discontinuation Recommendation 7: (Recommendation category: A; evidence type: 4) Clinicians should evaluate benefits & harms with patients within 1 to 4 weeks of starting opioid therapy for chronic pain or of dose escalation. Clinicians should evaluate benefits & harms of continued therapy with patients every 3 months or more frequently. If benefits do not outweigh harms of continued opioid therapy, clinicians should optimize other therapies & work with patients to taper opioids to lower dosages or to taper & discontinue opioids.
36 Why taper? Lack of efficacy No improvement in function/failed trial Inadequate analgesia Failure to reach treatment goals Therapy not needed any longer Pain resolving(ed) Surgical setting Unacceptable risk Adverse effects Opioid induced hyperalgesia & glial cell activation Employer prohibits drugs that may affect motor coordination
37 Case RD is a 44 yr old woman who does factory work. She has nonspecific low back pain & has been using nabumetone & tramadol 100mg q6hr for > 2 years. Her dose was reduced to 100mg q8hr (or 6 tabs/day). She reports that since the dose reduction she has not been able to go to work for the past 2 weeks due to pain. She requests that her dose be returned to 100mg q6hr.
38 Case Continued RD has been consistent with refills & per state PMP she has not been receiving controlled substances from any other provider. Per clinic policy she was identified for random UDT which was unremarkable except for (+) cocaine, confirmed
39 Why taper? Behavioral concerns Abnormal UDT Noncompliance Over or under utilization Misuse/abuse of medication Including diversion Use for reasons other than pain eg. Anxiety, sleep
40 Taper or just stop? Patients considered opioid tolerant are those receiving any of the following for 1 week or longer: 60 mg morphine/day 25 mcg transdermal fentanyl/hr 30 mg oral oxycodone/day 8 mg oral hydromorphone/day 25 mg oral oxymorphone/day
41 Opioid Taper Guidelines American Pain Society & American Academy of Pain Medicine 2009 Veterans Affairs Department of Defense 2010 Canadian National Opioid Use Guideline Group 2010 Agency Medical Directors Group 2010 American Society of Interventional Pain Physicians 2012
42 APS AAPM 2009 Guideline Slow 10% weekly reduction Rapid Anecdotal evidence for > 200 mg oral Morphine Equivalents 25 50% every few days Slow taper once oral Morphine Equivalents reach mg daily
43 VA DoD 2010 Guideline Variable 20 50% weekly taper Slower tapering may be warranted Rapid 20 50% Daily until Morphine Oral 45 mg daily; then by 15 mg every 2 5 days until DC Methadone Oral 30 mg daily; Then reduce by 5 mg daily every 3 5 days until 10 mg daily; Then reduce by 2.5 mg every 3 5 days until DC
44 Canadian National Opioid Use Group 2010 Guideline Slow 10% total daily dose every 1 2 weeks Rapid 10% total daily dose every day Caveats Once 1/3 of original daily dose is reached, reduce taper rate by at least 50% Consider converting hydromorphone & oxycodone patients to morphine to begin taper Use 50% of calculated equianalgesic dose.
45 Agency Medical Directors Group 2010 & American Society of Interventional Pain Physicians 2012 Decrease dose by 10% of original dose Some patients may be weaned more rapidly over 6 8 weeks
46 Adjusting tapers Patients with anxiety & fear about tapering May not be emotionally ready Recurrence or worsening of pain Re evaluate reasons for taper & minimum effective dose Withdrawal symptoms Tends to occur at about 30 45mg/day MEDD Taper is too fast, slow by 50% OR hold current dose & treat symptoms
47 CDC Opioid Guidelines Recommendation Highlights Assessing Risk & Addressing Harms of Opioid Use Recommendation 8: (Recommendation category: A; evidence type: 4) Before starting & periodically during continuation of opioid therapy, clinicians should evaluate risk factors for opioid related harms. Clinicians should incorporate into the management plan strategies to mitigate risk, including considering offering naloxone when factors that increase risk for opioid overdose such as: history of overdose; history SUD; higher opioid dosages; concurrent benzodiazepine use Certain risk factors can increase susceptibility to opioid associated harms. Patients with moderate or sever sleep disordered breathing; Pregnancy; Patients with impaired hepatic or renal function; Age > 65 years; Presence of depression or mental health conditions
48 CDC Opioid Guidelines Recommendation Highlights Assessing Risk & Addressing Harms of Opioid Use Recommendation 8 continued : (Recommendation category: A; evidence type: 4) If clinicians consider opioid therapy for patients with drug or alcohol use disorders or for patients with prior nonfatal overdose, they should discuss increased risks for opioid use disorder & overdose with patients, carefully consider whether benefits of opioids outweigh increased risks, & increase frequency of monitoring opioid therapy. Clinicians should consider offering naloxone when prescribing opioids to patients at increased risk of overdose, including patients with a history of overdose, patients with a history of substance use disorder, patients taking benzodiazepines with opioids, patients at risk of returning to a high dose to which they are no longer tolerant (eg, patients recently released from prison), & patients taking higher dosages of opioids. Practices should provide education on overdose prevention & naloxone use to patients receiving naloxone prescriptions & to members of their households.
49 CDC Opioid Guidelines Recommendation Highlights Assessing Risk & Addressing Harms of Opioid Use Recommendation 9: (Recommendation category: A; evidence type: 4) Review history of controlled substance prescriptions using state prescription drug monitoring program (PDMP) data to determine whether the patient is receiving opioid dosages or dangerous combinations (e.g. benzos) that put patient at high risk for overdose. Review PDMP data when starting opioid therapy for chronic pain & periodically during therapy for chronic pain, ranging from every prescription to every 3 months. Clinicians should discuss safety concerns, including increased risk for respiratory depression & overdose, with patients found to be receiving opioids from more than 1 prescriber or receiving medications that increase risk when combined with opioids (eg, benzodiazepines). Clinicians should avoid prescribing opioids & benzodiazepines concurrently whenever possible. Clinicians should consider the possibility of a substance use disorder & discuss concerns with their patient.
50 CDC Opioid Guidelines Recommendation Highlights Assessing Risk & Addressing Harms of Opioid Use Recommendation 10: (Recommendation category: B; evidence type: 4) When prescribing opioids for chronic pain, clinicians should use urine drug testing (UDT) before starting opioid therapy & consider UDT urine at least annually to assess for prescribed medications as well as other controlled prescription drugs & illicit drugs. Assess for prescribed opioids as well as other controlled substances & illicit drugs that increase risk for overdose when combined with opioids, including nonprescribed opioids, benzodiazepines, & heroin. Clinicians should be familiar with the drugs included in UDT panels used in their practice & should understand how to interpret results for these drugs. Clinicians should not dismiss patients from care based on UDT result. This could have adverse consequences for patient safety, including missed opportunities to facilitate treatment for substance use disorder.

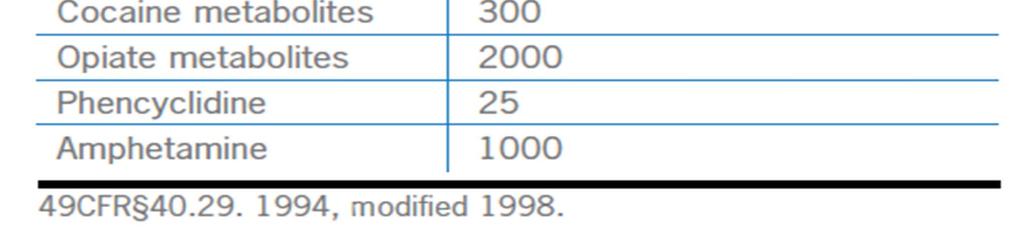
51 The Federal 5


52 Example of Point of Care UDT
53 Opiate Screens & UDT? Opiates are naturally occurring opioids Codeine & morphine Rarely sensitive for semi synthetic agents (e.g. oxycodone) To determine methadone (a synthetic opioid) a specific assay is required
54 Question A patient has a UDT & is prescribed methadone. He is actually taking the methadone but the UDT is not specific for methadone. Is this a false negative? Why?

55 UDT
56 Pitfalls of UDT for Compliance Not actually using the medication Relationship of timing of last dose of medication to the UDT Rapid excreter or metabolizer of the substance ph of urine UDT not sensitive enough Clerical errors caused to a positive UDT to be reported as negative.
57 CDC Opioid Guidelines Recommendation Highlights Assessing Risk & Addressing Harms of Opioid Use Recommendation 12: (Recommendation category: A; evidence type: 2) Clinicians should offer or arrange evidence based treatment (usually medicationassisted treatment with buprenorphine or methadone in combination with behavioral therapies) for patients with opioid use disorder. If clinicians suspect opioid use disorder based on patient concerns or behaviors or on findings in PDMP data or from urine drug testing, they should discuss their concerns with their patient & provide an opportunity for the patient to disclose related concerns or problems. Clinicians should assess for opioid use disorder using DSM 5 criteria. Physicians prescribing opioids in communities without sufficient treatment capacity for opioid use disorder should strongly consider obtaining a waiver from SAMHSA that allows them to prescribe buprenorphine to treat patients with opioid use disorder. Clinicians unable to provide treatment themselves should arrange for patients with opioid use disorder to receive care from a substance use disorder treatment specialist, such as an office based clinician who prescribes buprenorphine or naltrexone treatment, or from an opioid treatment program certified by SAMHSA to provide supervised medication assisted treatment for patients with opioid use disorder.
58 Critical outcomes Pain relief Function physical psychosocial Side effects Drug related behaviors The 4 A's of Pain" Analgesia Activities of daily living Adverse effects Aberrant drug taking behaviors Passik SD, Weinreb HJ. Adv Ther. 2000;17:70-83.
59 Aberrant Drug taking Behaviors Major Selling prescription drugs Prescription forgery Stealing or borrowing another patient s drugs Injecting oral formulation Obtaining prescription drugs from nonmedical sources Concurrent abuse of related illicit drugs Multiple unsanctioned dose escalations Recurrent prescription losses Minor Aggressive complaining about need for higher doses Drug hoarding during periods of reduced symptoms Requesting specific drugs Acquisition of similar drugs from other medical sources Unsanctioned dose escalation 1 2 times Unapproved use of the drug to treat another symptom Reporting psychic effects not intended by the clinician 23 Passik SD et al. Oncology. 1998;12(4): ,524. Passik SD et al. Oncology. 1998;12(5): ,736.
60 Screening Tools for Opioids & Substance Misuse ORT: Opioid Risk Tool Simple 5 Question Tool SOAPP: Screener Assessment for Patients with Pain Proprietary Multiple versions (8, 14, & 24 Question Versions) CAGE AID: CAGE Adapted to Include Drugs Simple 4 Question Tool COMM: Current Opioid Misuse Measure Proprietary 17 Questions
61

62

63 Opioid Therapy & Substance Abuse Differential Diagnoses of Aberrant Drug Related Behavior Addiction vs. Pseudo addiction vs. Pseudo tolerance Pychiatric disorders e.g. borderline personality disorder Cognitive disorders E.g. mild encephalopathy Family issues Criminal intent

64 Monitoring Aberrant Drug Related Behaviors: 2 Step Approach Step 1: Are there aberrant drug related behaviors? Step 2: If yes, are these behaviors best explained by the existence of a substance use disorder?
 Medication agreements")
65 Aberrant Behaviors: Strategies Frequent visits & small quantities 1 Prescriber & 1 Pharmacy NO replacements or early scripts Long acting drugs with no rescue doses No access to meds for breakthrough pain Use of random UDTs Coordination with sponsor, program, psychotherapist, others Consultation with addiction medicine specialist Prescription Drug Monitoring Programs (PDMP) Medication agreements

66 Patient Care Agreements Widely used but not evidence based Reminder: opioids one modality in multifaceted approach to achieving goals of therapy Detailed outline of procedures & expectations Prohibited behaviors, & grounds for taper or DC Limitations on prescriptions Emergency issues Refill & dose adjustment procedures Exit strategy May contain elements of Informed Consent 11

67 Physical Back exercises Aerobic exercise Behavioral Stress management Mental Health Pharmacotherapy
Opiate Use Disorder and Opiate Overdose
 Opiate Use Disorder and Opiate Overdose Irene Ortiz, MD Medical Director Molina Healthcare of New Mexico and South Carolina Clinical Professor University of New Mexico School of Medicine Objectives DSM-5
Opiate Use Disorder and Opiate Overdose Irene Ortiz, MD Medical Director Molina Healthcare of New Mexico and South Carolina Clinical Professor University of New Mexico School of Medicine Objectives DSM-5
CDC Guideline for Prescribing Opioids for Chronic Pain. Centers for Disease Control and Prevention National Center for Injury Prevention and Control
 CDC Guideline for Prescribing Opioids for Chronic Pain Centers for Disease Control and Prevention National Center for Injury Prevention and Control THE EPIDEMIC Chronic Pain and Prescription Opioids 11%
CDC Guideline for Prescribing Opioids for Chronic Pain Centers for Disease Control and Prevention National Center for Injury Prevention and Control THE EPIDEMIC Chronic Pain and Prescription Opioids 11%
HOPE. Considerations. Considerations ISING. Safe Opioid Prescribing Guidelines for ACUTE Non-Malignant Pain
 Due to the high level of prescription drug use and abuse in Lake County, these guidelines have been developed to standardize prescribing habits and limit risk of unintended harm when prescribing opioid
Due to the high level of prescription drug use and abuse in Lake County, these guidelines have been developed to standardize prescribing habits and limit risk of unintended harm when prescribing opioid
New Guidelines for Prescribing Opioids for Chronic Pain
 New Guidelines for Prescribing Opioids for Chronic Pain Andrew Lowe, Pharm.D. CAPA Meeting October 6, 2016 THE EPIDEMIC Chronic Pain and Prescription Opioids 11% of Americans experience daily (chronic)
New Guidelines for Prescribing Opioids for Chronic Pain Andrew Lowe, Pharm.D. CAPA Meeting October 6, 2016 THE EPIDEMIC Chronic Pain and Prescription Opioids 11% of Americans experience daily (chronic)
SAFE PRESCRIBING: RULES AND REGULATIONS. Michelle Y. Owens, MD MS State Board of Medical Licensure June 30, 2017
 SAFE PRESCRIBING: RULES AND REGULATIONS Michelle Y. Owens, MD MS State Board of Medical Licensure June 30, 2017 DISCLOSURES I have no financial disclosures. OBJECTIVES Discuss the significance of the opiate
SAFE PRESCRIBING: RULES AND REGULATIONS Michelle Y. Owens, MD MS State Board of Medical Licensure June 30, 2017 DISCLOSURES I have no financial disclosures. OBJECTIVES Discuss the significance of the opiate
Opioid Review and MAT Clinic CDC Guidelines
 1 Opioid Review and MAT Clinic CDC Guidelines January 10, 2018 Housekeeping Use chat feature to inform everyone who s at your clinic Click chat on Zoom option bar Chat Everyone the names of those who are
1 Opioid Review and MAT Clinic CDC Guidelines January 10, 2018 Housekeeping Use chat feature to inform everyone who s at your clinic Click chat on Zoom option bar Chat Everyone the names of those who are
Summary of Recommendations...3. PEG: A Three-Item Scale Assessing Pain (Appendix A) Chronic Pain Flow Sheet Acute Pain Flow Sheet...
 Chronic Pain Flow Sheet Acute Pain Flow Sheet...") Table of Contents Summary of Recommendations....3 PEG: A Three-Item Scale Assessing Pain (Appendix A)...12 Chronic Pain Flow Sheet...13 Acute Pain Flow Sheet...14 Pocket Guide: Tapering Opioids for Chronic
Table of Contents Summary of Recommendations....3 PEG: A Three-Item Scale Assessing Pain (Appendix A)...12 Chronic Pain Flow Sheet...13 Acute Pain Flow Sheet...14 Pocket Guide: Tapering Opioids for Chronic
Knock Out Opioid Abuse in New Jersey:
 Knock Out Opioid Abuse in New Jersey: A Resource for Safer Prescribing GUIDELINE FOR PRESCRIBING OPIOIDS FOR CHRONIC PAIN IMPROVING PRACTICE THROUGH RECOMMENDATIONS CDC s Guideline for Prescribing Opioids
Knock Out Opioid Abuse in New Jersey: A Resource for Safer Prescribing GUIDELINE FOR PRESCRIBING OPIOIDS FOR CHRONIC PAIN IMPROVING PRACTICE THROUGH RECOMMENDATIONS CDC s Guideline for Prescribing Opioids
Addressing the Opioid Epidemic: Prescribing Opioids for Non-Cancer Pain
 Addressing the Opioid Epidemic: Prescribing Opioids for Non-Cancer Pain Ajay D. Wasan, MD, MSc Professor of Anesthesiology and Psychiatry Vice Chair for Pain Medicine, Department of Anesthesiology University
Addressing the Opioid Epidemic: Prescribing Opioids for Non-Cancer Pain Ajay D. Wasan, MD, MSc Professor of Anesthesiology and Psychiatry Vice Chair for Pain Medicine, Department of Anesthesiology University
Risk Reduction Strategies in Pain Management
 Risk Reduction Strategies in Pain Management Melissa J. Durham, PharmD, MACM, BCACP, DAAPM Assistant Professor of Clinical Pharmacy USC School of Pharmacy Clinical Pharmacist, The USC Pain Center Learning
Risk Reduction Strategies in Pain Management Melissa J. Durham, PharmD, MACM, BCACP, DAAPM Assistant Professor of Clinical Pharmacy USC School of Pharmacy Clinical Pharmacist, The USC Pain Center Learning
Appendix F Federation of State Medical Boards
 Appendix F Federation of State Medical Boards Model Policy Guidelines for Opioid Addiction Treatment in the Medical Office SECTION I: PREAMBLE The (name of board) recognizes that the prevalence of addiction
Appendix F Federation of State Medical Boards Model Policy Guidelines for Opioid Addiction Treatment in the Medical Office SECTION I: PREAMBLE The (name of board) recognizes that the prevalence of addiction
Interdisciplinary Management of Opioid Use Disorder in Rural Primary Care Settings
 Interdisciplinary Management of Opioid Use Disorder in Rural Primary Care Settings BRIAN GARVEY, MD, MPH REBECCA CANTONE, MD OREGON HEALTH & SCIENCE UNIVERSITY SCAPPOOSE RURAL HEALTH CENTER Disclosures
Interdisciplinary Management of Opioid Use Disorder in Rural Primary Care Settings BRIAN GARVEY, MD, MPH REBECCA CANTONE, MD OREGON HEALTH & SCIENCE UNIVERSITY SCAPPOOSE RURAL HEALTH CENTER Disclosures
New Guidelines for Opioid Prescribing
 New Guidelines for Opioid Prescribing What They Mean for Elders with Chronic Pain Manu Thakral, PhD, ARNP Kaiser Permanente Washington Health Research Institute Kaiser Permanente Washington Health Research
New Guidelines for Opioid Prescribing What They Mean for Elders with Chronic Pain Manu Thakral, PhD, ARNP Kaiser Permanente Washington Health Research Institute Kaiser Permanente Washington Health Research
Prescribing drugs of dependence in general practice, Part C
 HO O Prescribing drugs of dependence in general practice, Part C Key recommendations and practice points for management of pain with opioid therapy H H HO N CH3 Acute pain Acute pain is an unpleasant sensory
HO O Prescribing drugs of dependence in general practice, Part C Key recommendations and practice points for management of pain with opioid therapy H H HO N CH3 Acute pain Acute pain is an unpleasant sensory
Recommendations in Opioid Prescribing Guidelines for Chronic Pain
 Recommendations in Opioid Prescribing Guidelines for Chronic Pain The use of opioids for treating chronic pain has been increasing. 1 In 2010, an estimated 20% of patients presenting to physician offices
Recommendations in Opioid Prescribing Guidelines for Chronic Pain The use of opioids for treating chronic pain has been increasing. 1 In 2010, an estimated 20% of patients presenting to physician offices
Safe Prescribing of Drugs with Potential for Misuse/Diversion
 College of Physicians and Surgeons of British Columbia Safe Prescribing of Drugs with Potential for Misuse/Diversion Preamble This document establishes both professional standards as well as guidelines
College of Physicians and Surgeons of British Columbia Safe Prescribing of Drugs with Potential for Misuse/Diversion Preamble This document establishes both professional standards as well as guidelines
Best Practices in Prescribing Opioids for Chronic Non-cancer Pain
 Best Practices in Prescribing Opioids for Chronic Non-cancer Pain Disclosures S C O T T S T E I G E R, M D, F A C P, D A B A M A S S I S T A N T C L I N I C A L P R O F E S S O R D I V I S I O N O F G
Best Practices in Prescribing Opioids for Chronic Non-cancer Pain Disclosures S C O T T S T E I G E R, M D, F A C P, D A B A M A S S I S T A N T C L I N I C A L P R O F E S S O R D I V I S I O N O F G
Opioid Analgesics: Responsible Prescribing in the Midst of an Epidemic
 Opioid Analgesics: Responsible Prescribing in the Midst of an Epidemic Lucas Buffaloe, MD Associate Professor of Clinical Family and Community Medicine University of Missouri Health Care Goals for today
Opioid Analgesics: Responsible Prescribing in the Midst of an Epidemic Lucas Buffaloe, MD Associate Professor of Clinical Family and Community Medicine University of Missouri Health Care Goals for today
Clinical Guidelines for the Use of Buprenorphine in the Treatment of Opioid Addiction
 Clinical Guidelines for the Use of Buprenorphine in the Treatment of Opioid Addiction Multiple Choice Identify the choice that best completes the statement or answers the question. 1. Executive Summary
Clinical Guidelines for the Use of Buprenorphine in the Treatment of Opioid Addiction Multiple Choice Identify the choice that best completes the statement or answers the question. 1. Executive Summary
Proposed Revision to Med (i)
") Proposed Revision to Med 501.02 (i) I. Purpose This rule has been adopted to enable the Board to best protect public health and safety while providing a framework for licensees to effectively treat and
Proposed Revision to Med 501.02 (i) I. Purpose This rule has been adopted to enable the Board to best protect public health and safety while providing a framework for licensees to effectively treat and
Opioid Management of Chronic (Non- Cancer) Pain
 Pain") Optima Health Opioid Management of Chronic (Non- Cancer) Pain Guideline History Original Approve Date 5/08 Review/Revise Dates 11/09, 9/11, 9/13, 09/15, 9/17 Next Review Date 9/19 These Guidelines are
Optima Health Opioid Management of Chronic (Non- Cancer) Pain Guideline History Original Approve Date 5/08 Review/Revise Dates 11/09, 9/11, 9/13, 09/15, 9/17 Next Review Date 9/19 These Guidelines are
An overview of Medication Assisted Treatment (MAT) and acute pain management on MAT
 and acute pain management on MAT") An overview of Medication Assisted Treatment (MAT) and acute pain management on MAT Goals of Discussion Recognize opioid use disorder (OUD) Discuss the pharmacology of medication assisted treatments (MAT)
An overview of Medication Assisted Treatment (MAT) and acute pain management on MAT Goals of Discussion Recognize opioid use disorder (OUD) Discuss the pharmacology of medication assisted treatments (MAT)
NBPDP Drug Utilization Review Process Update
 Bulletin # 802 December 1, 2010 NBPDP Drug Utilization Review Process Update The New Brunswick Prescription Drug Program (NBPDP) employs a Drug Utilization Review (DUR) process which identifies, investigates
Bulletin # 802 December 1, 2010 NBPDP Drug Utilization Review Process Update The New Brunswick Prescription Drug Program (NBPDP) employs a Drug Utilization Review (DUR) process which identifies, investigates
Rule Governing the Prescribing of Opioids for Pain
 Rule Governing the Prescribing of Opioids for Pain 1.0 Authority This rule is adopted pursuant to Sections 14(e) and 11(e) of Act 75 (2013) and Sections 2(e) and 2a of Act 173 (2016). 2.0 Purpose This
Rule Governing the Prescribing of Opioids for Pain 1.0 Authority This rule is adopted pursuant to Sections 14(e) and 11(e) of Act 75 (2013) and Sections 2(e) and 2a of Act 173 (2016). 2.0 Purpose This
Kurt Haspert, MS, CRNP University of Maryland Baltimore Washington Medical Center
 Kurt Haspert, MS, CRNP University of Maryland Baltimore Washington Medical Center Data from the National Vital Statistics System Mortality The age-adjusted rate of drug overdose deaths in the United States
Kurt Haspert, MS, CRNP University of Maryland Baltimore Washington Medical Center Data from the National Vital Statistics System Mortality The age-adjusted rate of drug overdose deaths in the United States
Disclosures. Ms. Walsh has nothing to disclose Ms. Broglio is on the speaker s bureau for Genentech and Meda Pharmaceuticals
 Anne F. Walsh, MSN, ANP BC, ACHPN, CWOCN Kathleen Broglio, MN, ANP BC, ACHPN, CPE Disclosures Ms. Walsh has nothing to disclose Ms. Broglio is on the speaker s bureau for Genentech and Meda Pharmaceuticals
Anne F. Walsh, MSN, ANP BC, ACHPN, CWOCN Kathleen Broglio, MN, ANP BC, ACHPN, CPE Disclosures Ms. Walsh has nothing to disclose Ms. Broglio is on the speaker s bureau for Genentech and Meda Pharmaceuticals
Opioids: Use and Misuse/Steven Feinberg, MD; Scott Levy, MD, MPH, FACOEM
 Western Occupational Health Conference September 14, 2012 Opioid - Use & Misuse Scott Levy, MD MPH FACOEM Steven Feinberg, MD, MPH Disclosure Information Western Occupational Health Conference 2012 Steven
Western Occupational Health Conference September 14, 2012 Opioid - Use & Misuse Scott Levy, MD MPH FACOEM Steven Feinberg, MD, MPH Disclosure Information Western Occupational Health Conference 2012 Steven
Tapering Opioids Best Practices*
 Tapering Opioids Best Practices* Chuck Hofmann, MD, MACP 5 th Annual EOCCO Office Staff and Provider Summit September 28, 2017 Disclosure No Conflicts of Interest to report Learning Objectives Understand
Tapering Opioids Best Practices* Chuck Hofmann, MD, MACP 5 th Annual EOCCO Office Staff and Provider Summit September 28, 2017 Disclosure No Conflicts of Interest to report Learning Objectives Understand
Controlled Substances Evidence-based Tips for Improved Workflow: Diagnosis, Screening & Drug Testing
 Controlled Substances Evidence-based Tips for Improved Workflow: Diagnosis, Screening & Drug Testing Mississippi Primary Health Care Association Pearl, MS March 7, 2018 Scott Hambleton, MD, DFASAM Medical
Controlled Substances Evidence-based Tips for Improved Workflow: Diagnosis, Screening & Drug Testing Mississippi Primary Health Care Association Pearl, MS March 7, 2018 Scott Hambleton, MD, DFASAM Medical
Practical Tools to Successfully Taper Prescription Opioids. Melissa Weimer, DO, MCR
 Practical Tools to Successfully Taper Prescription Opioids Melissa Weimer, DO, MCR Objectives Understand how to calculate morphine equivalents per day Understand the steps necessary to plan a successful
Practical Tools to Successfully Taper Prescription Opioids Melissa Weimer, DO, MCR Objectives Understand how to calculate morphine equivalents per day Understand the steps necessary to plan a successful
INFORMED CONSENT FOR OPIOID TREATMENT FOR NON-CANCER/CANCER PAIN Texas Pain and Regenerative Medicine
 INFORMED CONSENT FOR OPIOID TREATMENT FOR NON-CANCER/CANCER PAIN Texas Pain and Regenerative Medicine The purpose of this agreement is to give you information about the medications you will be taking for
INFORMED CONSENT FOR OPIOID TREATMENT FOR NON-CANCER/CANCER PAIN Texas Pain and Regenerative Medicine The purpose of this agreement is to give you information about the medications you will be taking for
MANAGING PAIN IN PATIENTS WITH SUBSTANCE USE DISORDER Melissa B. Weimer, DO, MCR Chief of Behavioral Health & Addiction Medicine St.
 MANAGING PAIN IN PATIENTS WITH SUBSTANCE USE DISORDER Melissa B. Weimer, DO, MCR Chief of Behavioral Health & Addiction Medicine St. Peter s Health Partners, Albany, NY Assistant Professor of Medicine,
MANAGING PAIN IN PATIENTS WITH SUBSTANCE USE DISORDER Melissa B. Weimer, DO, MCR Chief of Behavioral Health & Addiction Medicine St. Peter s Health Partners, Albany, NY Assistant Professor of Medicine,
OCCUPATIONAL AND PROFESSIONAL LICENSING MEDICINE AND SURGERY PRACTITIONERS MANAGEMENT OF PAIN AND OTHER CONDITIONS WITH CONTROLLED SUBSTANCES
 TITLE 16 CHAPTER 10 PART 14 OCCUPATIONAL AND PROFESSIONAL LICENSING MEDICINE AND SURGERY PRACTITIONERS MANAGEMENT OF PAIN AND OTHER CONDITIONS WITH CONTROLLED SUBSTANCES 16.10.14.1 ISSUING AGENCY: New
TITLE 16 CHAPTER 10 PART 14 OCCUPATIONAL AND PROFESSIONAL LICENSING MEDICINE AND SURGERY PRACTITIONERS MANAGEMENT OF PAIN AND OTHER CONDITIONS WITH CONTROLLED SUBSTANCES 16.10.14.1 ISSUING AGENCY: New
Fighting the Good Fight: How to Convert Opioids Just Right!
 Fighting the Good Fight: How to Convert Opioids Just Right! Tanya J. Uritsky, PharmD, BCPS, CPE Clinical Pharmacy Specialist - Pain Medication Stewardship Hospital of the University of Pennsylvania - Philadelphia,
Fighting the Good Fight: How to Convert Opioids Just Right! Tanya J. Uritsky, PharmD, BCPS, CPE Clinical Pharmacy Specialist - Pain Medication Stewardship Hospital of the University of Pennsylvania - Philadelphia,
THE PROS & CONS OF THE CDC GUIDELINES FOR SAFE OPIOID PRESCRIBING
 THE PROS & CONS OF THE CDC GUIDELINES FOR SAFE OPIOID PRESCRIBING Ernest J Dole, PharmD, PhC, FASHP, BCPS Clinical Pharmacist University of New Mexico Hospitals And Clinical Associate Professor University
THE PROS & CONS OF THE CDC GUIDELINES FOR SAFE OPIOID PRESCRIBING Ernest J Dole, PharmD, PhC, FASHP, BCPS Clinical Pharmacist University of New Mexico Hospitals And Clinical Associate Professor University
Brief History of Methadone Maintenance Treatment
 METHADONE Brief History of Methadone Maintenance Treatment Methadone maintenance treatment was on the cusp of the social revolution in the sixties. Doctors and public health workers had concluded what
METHADONE Brief History of Methadone Maintenance Treatment Methadone maintenance treatment was on the cusp of the social revolution in the sixties. Doctors and public health workers had concluded what
Pain and Addiction. Edward Jouney, DO Department of Psychiatry
 Pain and Addiction Edward Jouney, DO Department of Psychiatry Case 43 year-old female with a history chronic lower back pain presents to your clinic ongoing care. She has experienced pain difficulties
Pain and Addiction Edward Jouney, DO Department of Psychiatry Case 43 year-old female with a history chronic lower back pain presents to your clinic ongoing care. She has experienced pain difficulties
Chronic Pain, Opioids, & Addiction: Assessing and Managing Risk
 Chronic Pain, Opioids, & Addiction: Assessing and Managing Risk Randy Brown MD, PhD, FASAM Associate Professor, Dept of Family Medicine Director, Center for Addictive Disorders, UWHC Director, UW Addiction
Chronic Pain, Opioids, & Addiction: Assessing and Managing Risk Randy Brown MD, PhD, FASAM Associate Professor, Dept of Family Medicine Director, Center for Addictive Disorders, UWHC Director, UW Addiction
Approved Procedures for Prescribing and Monitoring Controlled Substances in South Carolina
 Approved Procedures for Prescribing and Monitoring Controlled Substances in South Carolina Robert B. Hanlin, M.D., FAAFP Vice Chair, Medical Staff Affairs Greenville Health System Greenville, SC Disclosures
Approved Procedures for Prescribing and Monitoring Controlled Substances in South Carolina Robert B. Hanlin, M.D., FAAFP Vice Chair, Medical Staff Affairs Greenville Health System Greenville, SC Disclosures
Substitution Therapy for Opioid Use Disorder The Role of Suboxone
 Substitution Therapy for Opioid Use Disorder The Role of Suboxone Methadone/Buprenorphine 101 Workshop, December 10, 2016 Leslie Lappalainen, MD, CCFP, dip ABAM Prepared by Mandy Manak, MD, ABAM, CCSAM
Substitution Therapy for Opioid Use Disorder The Role of Suboxone Methadone/Buprenorphine 101 Workshop, December 10, 2016 Leslie Lappalainen, MD, CCFP, dip ABAM Prepared by Mandy Manak, MD, ABAM, CCSAM
Revised 9/30/2016. Primary Care Provider Pain Management Toolkit
 Revised 9/30/2016 Primary Care Provider Pain Management Toolkit TABLE OF CONTENTS 1. INTRODUCTION Page 1 2. NON-OPIOID SERVICES &TREATMENTS FOR CHRONIC PAIN Page 2 2.1 Medical Services Page 2 2.2 Behavioral
Revised 9/30/2016 Primary Care Provider Pain Management Toolkit TABLE OF CONTENTS 1. INTRODUCTION Page 1 2. NON-OPIOID SERVICES &TREATMENTS FOR CHRONIC PAIN Page 2 2.1 Medical Services Page 2 2.2 Behavioral
Canadian Guideline for Opioids for Chronic Non-Cancer Pain. Speaker Disclosure. Objectives. Canadian Guideline for Opioids for Chronic Non-Cancer Pain
 Canadian Guideline for Opioids for Chronic Non-Cancer Pain John Fraser Community Hospital Program New Glasgow November 1, 2017 This speaker has been asked to disclose to the audience any involvement with
Canadian Guideline for Opioids for Chronic Non-Cancer Pain John Fraser Community Hospital Program New Glasgow November 1, 2017 This speaker has been asked to disclose to the audience any involvement with
SUBOXONE Film, SUBOXONE Tablets, and SUBUTEX Tablets. Risk Evaluation and Mitigation Strategy (REMS) Program
 Program") SUBOXONE Film, SUBOXONE Tablets, and SUBUTEX Tablets Risk Evaluation and Mitigation Strategy (REMS) Program Office-Based Buprenorphine Therapy for Opioid Dependence: Important Information for Prescribers
SUBOXONE Film, SUBOXONE Tablets, and SUBUTEX Tablets Risk Evaluation and Mitigation Strategy (REMS) Program Office-Based Buprenorphine Therapy for Opioid Dependence: Important Information for Prescribers
Use of Opioids for Chronic Non Malignant Pain (CNMP)
") I. PURPOSE Use of Opioids for Chronic Non Malignant Pain (CNMP) We the Safe Opioid Prescribing and Review Committee (SOPARC) are inspired to support a shift in opioid prescribing that improves clinical
I. PURPOSE Use of Opioids for Chronic Non Malignant Pain (CNMP) We the Safe Opioid Prescribing and Review Committee (SOPARC) are inspired to support a shift in opioid prescribing that improves clinical
What do they have in common?
 What do they have in common? Opioid use in USA Approximately 9 million people on long term opioids Approximated 5 million people reporting non-medical use of opioids 1997: 96mg/person morphine eq dispensed
What do they have in common? Opioid use in USA Approximately 9 million people on long term opioids Approximated 5 million people reporting non-medical use of opioids 1997: 96mg/person morphine eq dispensed
MAT in the Corrections Setting
 MEDICATION ASSISTED TREATMENT AND CORRECTIONS Frank Filippelli, DO, PhD September 2017 MAT in the Corrections Setting Who Does This Affect? What is MAT and What is the Evidence of Efficacy? Emphasis on
MEDICATION ASSISTED TREATMENT AND CORRECTIONS Frank Filippelli, DO, PhD September 2017 MAT in the Corrections Setting Who Does This Affect? What is MAT and What is the Evidence of Efficacy? Emphasis on
Chronic Pain Pharmacist role in the clinic
 Chronic Pain Pharmacist role in the clinic WSPA Annual Meeting 2015 Alvin Goo, PharmD Clinical Associate Professor University of Washington Schools of Pharmacy and Family Medicine Speakers Declaration
Chronic Pain Pharmacist role in the clinic WSPA Annual Meeting 2015 Alvin Goo, PharmD Clinical Associate Professor University of Washington Schools of Pharmacy and Family Medicine Speakers Declaration
CDC Guideline for Prescribing Opioids for Chronic Pain
 National Center for Injury Prevention and Control CDC Guideline for Prescribing Opioids for Chronic Pain John Halpin, MD, MPH Medical Officer Division of Unintentional Injury Prevention Prescription Drug
National Center for Injury Prevention and Control CDC Guideline for Prescribing Opioids for Chronic Pain John Halpin, MD, MPH Medical Officer Division of Unintentional Injury Prevention Prescription Drug
Standard of Practice for Prescribing Opioids (Excluding Cancer, Palliative, and End-of-Life Care)
") Standard of Practice for Prescribing Opioids (Excluding Cancer, Palliative, and End-of-Life Care) Preamble This Standard establishes the standards of practice and ethical requirements of all physicians
Standard of Practice for Prescribing Opioids (Excluding Cancer, Palliative, and End-of-Life Care) Preamble This Standard establishes the standards of practice and ethical requirements of all physicians
Department of Veterans Affairs Network Policy No.: VA Desert Pacific Healthcare Network (VISN 22) Date: September 23, 2014 Long Beach, CA
 Date: September 23, 2014 Long Beach, CA") Department of Veterans Affairs Network Policy No.: 2014-01 VA Desert Pacific Healthcare Network (VISN 22) Date: September 23, 2014 Long Beach, CA CHRONIC OPIOID USE FOR NON-MALIGNANT PAIN 1. PURPOSE: To
Department of Veterans Affairs Network Policy No.: 2014-01 VA Desert Pacific Healthcare Network (VISN 22) Date: September 23, 2014 Long Beach, CA CHRONIC OPIOID USE FOR NON-MALIGNANT PAIN 1. PURPOSE: To
Michael O Neil, Pharm.D. Professor and Vice-Chair, Department of Pharmacy Practice Drug Diversion, Substance Abuse, and Pain Management Consultant
 Michael O Neil, Pharm.D. Professor and Vice-Chair, Department of Pharmacy Practice Drug Diversion, Substance Abuse, and Pain Management Consultant South College School of Pharmacy Knoxville, TN (304) 546-7746
Michael O Neil, Pharm.D. Professor and Vice-Chair, Department of Pharmacy Practice Drug Diversion, Substance Abuse, and Pain Management Consultant South College School of Pharmacy Knoxville, TN (304) 546-7746
NORTHWEST AIDS EDUCATION AND TRAINING CENTER. Opioid Use Disorders. Joseph Merrill M.D., M.P.H. University of Washington April 10, 2014
 NORTHWEST AIDS EDUCATION AND TRAINING CENTER Opioid Use Disorders Joseph Merrill M.D., M.P.H. University of Washington April 10, 2014 Opioid Use Disorders Importance of opioid use disorders Screening and
NORTHWEST AIDS EDUCATION AND TRAINING CENTER Opioid Use Disorders Joseph Merrill M.D., M.P.H. University of Washington April 10, 2014 Opioid Use Disorders Importance of opioid use disorders Screening and
Opioid Prescribing Tips & Tricks CANDY STOCKTON, MD MAY 2018
 Opioid Prescribing Tips & Tricks CANDY STOCKTON, MD MAY 2018 Disclosures None Educational Objectives Understand CA state medical board guidelines for prescribing opioids for chronic pain Understand the
Opioid Prescribing Tips & Tricks CANDY STOCKTON, MD MAY 2018 Disclosures None Educational Objectives Understand CA state medical board guidelines for prescribing opioids for chronic pain Understand the
Taking Opioids Responsibly for Your Safety and the Safety of Others: Patient Information Guide on Long-term Opioid Therapy for Chronic Pain
 Taking Opioids Responsibly for Your Safety and the Safety of Others: Patient Information Guide on Long-term Opioid Therapy for Chronic Pain Department of Veterans Affairs (VA) and Department of Defense
Taking Opioids Responsibly for Your Safety and the Safety of Others: Patient Information Guide on Long-term Opioid Therapy for Chronic Pain Department of Veterans Affairs (VA) and Department of Defense
The Role of the PDMP: Foundational Knowledge and Best Practices
 The Role of the PDMP: Foundational Knowledge and Best Practices Brent I. Fox, PharmD, PhD Health Outcomes Research and Policy Harrison School of Pharmacy Auburn University DISCLOSURE I, Brent Fox, have
The Role of the PDMP: Foundational Knowledge and Best Practices Brent I. Fox, PharmD, PhD Health Outcomes Research and Policy Harrison School of Pharmacy Auburn University DISCLOSURE I, Brent Fox, have
MEDICATION MANAGEMENT AGREEMENT
 MEDICATION MANAGEMENT AGREEMENT The goal of this agreement is to ensure that you and your physician comply with all state and federal regulations concerning the prescribing of controlled substances. The
MEDICATION MANAGEMENT AGREEMENT The goal of this agreement is to ensure that you and your physician comply with all state and federal regulations concerning the prescribing of controlled substances. The
4/3/2018. The Role of Pharmacists in the Safe Prescribing of Opioids: Having the Tough Talks with Patients and Prescribers. Learning Objectives
 The Role of Pharmacists in the Safe Prescribing of Opioids: Having the Tough Talks with Patients and Prescribers Melissa Durham Tania Gregorian Vlada Manzur Learning Objectives Describe current issues
The Role of Pharmacists in the Safe Prescribing of Opioids: Having the Tough Talks with Patients and Prescribers Melissa Durham Tania Gregorian Vlada Manzur Learning Objectives Describe current issues
Prescription Opioid Addiction
 CSAM-SCAM Fundamentals Prescription Opioid Addiction Presentation provided by Meldon Kahan, MD Family & Community Medicine University of Toronto Conflict of interest statement I received funds from Rickett
CSAM-SCAM Fundamentals Prescription Opioid Addiction Presentation provided by Meldon Kahan, MD Family & Community Medicine University of Toronto Conflict of interest statement I received funds from Rickett
SHARED CARE GUIDELINE FOR THE MANAGEMENT OF PATIENTS ON NALTREXONE FOR OPIOID DEPENDENCE
 SHARED CARE GUIDELINE FOR THE MANAGEMENT OF PATIENTS ON NALTREXONE FOR OPIOID DEPENDENCE INDICATION Naltrexone is a pure opiate antagonist licensed as an adjunctive prophylactic therapy in the maintenance
SHARED CARE GUIDELINE FOR THE MANAGEMENT OF PATIENTS ON NALTREXONE FOR OPIOID DEPENDENCE INDICATION Naltrexone is a pure opiate antagonist licensed as an adjunctive prophylactic therapy in the maintenance
The Prescription Review Program and College Expectations. Dr. Rashmi Chadha MBChB MScCH CCFP MRCGP Dip. ABAM
 The Prescription Review Program and College Expectations Dr. Rashmi Chadha MBChB MScCH CCFP MRCGP Dip. ABAM April 28, 2017 Disclosure Relationship with commercial interests: None Professional roles: Addictions
The Prescription Review Program and College Expectations Dr. Rashmi Chadha MBChB MScCH CCFP MRCGP Dip. ABAM April 28, 2017 Disclosure Relationship with commercial interests: None Professional roles: Addictions
Equianalgesic Dosing: Making Opioid Interchange Easier. Joseph Bubalo PharmD, BCPS, BCOP Oncology Clinical Pharmacist Assistant Professor Of Medicine
 Equianalgesic Dosing: Making Opioid Interchange Easier Joseph Bubalo PharmD, BCPS, BCOP Oncology Clinical Pharmacist Assistant Professor Of Medicine 1 Why Change Opioids? Side Effects Insufficient Pain
Equianalgesic Dosing: Making Opioid Interchange Easier Joseph Bubalo PharmD, BCPS, BCOP Oncology Clinical Pharmacist Assistant Professor Of Medicine 1 Why Change Opioids? Side Effects Insufficient Pain
Scope of the Opiate Problem 6/5/18. Chronic Pain Management and the Use of Opioid Medications: The CDC Guideline and Beyond. Overview.
 Chronic Pain Management and the Use of Opioid Medications: The CDC Guideline and Beyond David Anisman, MD Medical Director, Farmington Health Center (Primary Care) Associate Medical Director, Community
Chronic Pain Management and the Use of Opioid Medications: The CDC Guideline and Beyond David Anisman, MD Medical Director, Farmington Health Center (Primary Care) Associate Medical Director, Community
UnitedHealthcare Pharmacy Clinical Pharmacy Programs
 UnitedHealthcare Pharmacy Clinical Pharmacy Programs Program Number 2018 P 4000-3 Program Opioid Overutilization Cumulative Drug Utilization Review Criteria Medication Includes all salt forms, single and
UnitedHealthcare Pharmacy Clinical Pharmacy Programs Program Number 2018 P 4000-3 Program Opioid Overutilization Cumulative Drug Utilization Review Criteria Medication Includes all salt forms, single and
KANSAS Kansas State Board of Healing Arts. Source: Kansas State Board of Healing Arts. Approved: October 17, 1998
 KANSAS Kansas State Board of Healing Arts Source: Kansas State Board of Healing Arts Approved: October 17, 1998 GUIDELINES FOR THE USE OF CONTROLLED SUBSTANCES FOR THE TREATMENT OF PAIN Section 1: Preamble
KANSAS Kansas State Board of Healing Arts Source: Kansas State Board of Healing Arts Approved: October 17, 1998 GUIDELINES FOR THE USE OF CONTROLLED SUBSTANCES FOR THE TREATMENT OF PAIN Section 1: Preamble
2. Is this request for a preferred medication? Y N
 Pharmacy Prior Authorization AETA BETTER HEALTH EW JERSE (MEDICAID) Opioids Long-Acting and Short-Acting (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review
Pharmacy Prior Authorization AETA BETTER HEALTH EW JERSE (MEDICAID) Opioids Long-Acting and Short-Acting (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review
Subject: Pain Management (Page 1 of 7)
") Subject: Pain Management (Page 1 of 7) Objectives: Managing pain and restoring function are basic goals in helping a patient with chronic non-cancer pain. Federal and state guidelines require that all
Subject: Pain Management (Page 1 of 7) Objectives: Managing pain and restoring function are basic goals in helping a patient with chronic non-cancer pain. Federal and state guidelines require that all
2/21/2018. What are Opioids?
 Opioid Crisis: South Carolina Responds Carolyn Bogdon, MSN, FNP-BC Coordinator for Emergency Department Medication Assisted Treatment Program Medical University of South Carolina Opioid Crisis: A Mounting
Opioid Crisis: South Carolina Responds Carolyn Bogdon, MSN, FNP-BC Coordinator for Emergency Department Medication Assisted Treatment Program Medical University of South Carolina Opioid Crisis: A Mounting
Management of Pain - A Comparison of Current Guidelines
 Management of Pain - A Comparison of Current Guidelines The Centers for Disease Control and Prevention (CDC) released a guideline in 2016 regarding the prescribing of opioids for chronic non-cancer pain
Management of Pain - A Comparison of Current Guidelines The Centers for Disease Control and Prevention (CDC) released a guideline in 2016 regarding the prescribing of opioids for chronic non-cancer pain
ten questions you might have about tapering (and room for your own) an informational booklet for opioid pain treatment
 an informational booklet for opioid pain treatment") ten questions you might have about tapering (and room for your own) an informational booklet for opioid pain treatment This booklet was created to help you learn about tapering. You probably have lots
ten questions you might have about tapering (and room for your own) an informational booklet for opioid pain treatment This booklet was created to help you learn about tapering. You probably have lots
The Population is Abusing Drugs, but are Drugs Abusing Insurance?
 Image licensed from Shutterstock The Population is Abusing Drugs, but are Drugs Abusing Insurance? 01/30/2018 Gina C. Guzman, MD, DBIM, FALU, FLMI, VP and Chief Medical Director Tim Morant, FSA, MAAA,
Image licensed from Shutterstock The Population is Abusing Drugs, but are Drugs Abusing Insurance? 01/30/2018 Gina C. Guzman, MD, DBIM, FALU, FLMI, VP and Chief Medical Director Tim Morant, FSA, MAAA,
Managed Care Pushes for Safer Opioid Oversight
 Page 1 of 6 Clinical AUGUST 11, 2017 Managed Care Pushes for Safer Opioid Oversight High-risk pain Rx eyed Denver Health systems haven t escaped the nation s ongoing opioid crisis, as evidenced by surging
Page 1 of 6 Clinical AUGUST 11, 2017 Managed Care Pushes for Safer Opioid Oversight High-risk pain Rx eyed Denver Health systems haven t escaped the nation s ongoing opioid crisis, as evidenced by surging
Medication Use & Chronic Pain Control: Managing Tolerance, Dependence, Addiction & Aberrant Medication Taking Behavior
 Medication Use & Chronic Pain Control: Managing Tolerance, Dependence, Addiction & Aberrant Medication Taking Behavior Ernest J Dole, PharmD, PhC, FASHP, BCPS, CDE Pharmaceutical Care Coordinator ABQ Health
Medication Use & Chronic Pain Control: Managing Tolerance, Dependence, Addiction & Aberrant Medication Taking Behavior Ernest J Dole, PharmD, PhC, FASHP, BCPS, CDE Pharmaceutical Care Coordinator ABQ Health
PROVIDER BULLETIN. Published by Wyoming Workers Compensation Medical Case Management Unit October 21, 2015
 Matthew H. Mead Governor State of Wyoming Department of Workforce Services DIVISION OF WORKERS COMPENSATION 1510 East Pershing Boulevard, South Wing Cheyenne, Wyoming 82002 http://www.wyomingworkforce.org
Matthew H. Mead Governor State of Wyoming Department of Workforce Services DIVISION OF WORKERS COMPENSATION 1510 East Pershing Boulevard, South Wing Cheyenne, Wyoming 82002 http://www.wyomingworkforce.org
Wasted AN INTRODUCTION TO SUBSTANCE ABUSE
 Wasted AN INTRODUCTION TO SUBSTANCE ABUSE Dr. Brian L. Bethel Child and Family Therapist Independent Trainer and Consultant LPCC-S, LCDC III, RPT-S www.brianlbethel.com INTERPLAY COUNSELING & CONSULTING
Wasted AN INTRODUCTION TO SUBSTANCE ABUSE Dr. Brian L. Bethel Child and Family Therapist Independent Trainer and Consultant LPCC-S, LCDC III, RPT-S www.brianlbethel.com INTERPLAY COUNSELING & CONSULTING
Opiate Use among Ohio Medicaid Recipients
 Opiate Use among Ohio Medicaid Recipients July 12, 2012 Ohio Colleges of Medicine Government Resource Center The Ohio State University College of Public Health Sponsored by The Ohio Department of Alcohol
Opiate Use among Ohio Medicaid Recipients July 12, 2012 Ohio Colleges of Medicine Government Resource Center The Ohio State University College of Public Health Sponsored by The Ohio Department of Alcohol
Education Program for Prescribers and Pharmacists
 Transmucosal Immediate Release Fentanyl (TIRF) Products Risk Evaluation and Mitigation Strategy (REMS) Education Program for Prescribers and Pharmacists Products Covered Under this Program Abstral (fentanyl)
Transmucosal Immediate Release Fentanyl (TIRF) Products Risk Evaluation and Mitigation Strategy (REMS) Education Program for Prescribers and Pharmacists Products Covered Under this Program Abstral (fentanyl)
Medication-Assisted Treatment. What Is It and Why Do We Use It?
 Medication-Assisted Treatment What Is It and Why Do We Use It? What is addiction, really? o The four C s of addiction: Craving. Loss of Control of amount or frequency of use. Compulsion to use. Use despite
Medication-Assisted Treatment What Is It and Why Do We Use It? What is addiction, really? o The four C s of addiction: Craving. Loss of Control of amount or frequency of use. Compulsion to use. Use despite
Chapter 7. Screening and Assessment
 Chapter 7 Screening and Assessment Screening And Assessment Starting the dialogue and begin relationship Each are sizing each other up Information gathering Listening to their story Asking the questions
Chapter 7 Screening and Assessment Screening And Assessment Starting the dialogue and begin relationship Each are sizing each other up Information gathering Listening to their story Asking the questions
15mg oxycodone is equivalent to how much morphine
 15mg oxycodone is equivalent to how much morphine The Borg System is 100 % 15mg oxycodone is equivalent to how much morphine nursing home activity director cover letter 15 mg oxycodone equal to how much
15mg oxycodone is equivalent to how much morphine The Borg System is 100 % 15mg oxycodone is equivalent to how much morphine nursing home activity director cover letter 15 mg oxycodone equal to how much
Utah. Prescribing and Dispensing Profile. Research current through November 2015.
 Prescribing and Dispensing Profile Utah Research current through November 2015. This project was supported by Grant No. G1599ONDCP03A, awarded by the Office of National Drug Control Policy. Points of view
Prescribing and Dispensing Profile Utah Research current through November 2015. This project was supported by Grant No. G1599ONDCP03A, awarded by the Office of National Drug Control Policy. Points of view
Non Opioid Approaches to Pain and Musculoskeletal Disorders KEVIN ODONNELL, DO FLAGSTAFF BONE AND JOINT
 Non Opioid Approaches to Pain and Musculoskeletal Disorders KEVIN ODONNELL, DO FLAGSTAFF BONE AND JOINT Learning Objectives Review Opioid Crisis CDC Guidelines for opioid prescribing Discuss Alternatives
Non Opioid Approaches to Pain and Musculoskeletal Disorders KEVIN ODONNELL, DO FLAGSTAFF BONE AND JOINT Learning Objectives Review Opioid Crisis CDC Guidelines for opioid prescribing Discuss Alternatives
Pain Management and Addiction: Clinical Challenges
 Pain Management and Addiction: Clinical Challenges MMS Pain Management Forum March 12, 2010 Associate Professor of Medicine Boston University School of Medicine Boston Medical Center Conflicts of Interest
Pain Management and Addiction: Clinical Challenges MMS Pain Management Forum March 12, 2010 Associate Professor of Medicine Boston University School of Medicine Boston Medical Center Conflicts of Interest
Substance Abuse Level of Care Criteria
 Substance Abuse Level of Care Criteria Table of Contents SUBSTANCE ABUSE OUTPATIENT: Adolescent... 3 SUBSTANCE ABUSE PREVENTION: Adult... 7 OPIOID MAINTENANCE THERAPY: Adult... 8 SUBSTANCE ABUSE INTERVENTION:
Substance Abuse Level of Care Criteria Table of Contents SUBSTANCE ABUSE OUTPATIENT: Adolescent... 3 SUBSTANCE ABUSE PREVENTION: Adult... 7 OPIOID MAINTENANCE THERAPY: Adult... 8 SUBSTANCE ABUSE INTERVENTION:
SHARED CARE GUIDELINE FOR THE MANAGEMENT OF PATIENTS ON NALTREXONE FOR ALCOHOL DEPENDENCE INDICATION
 SHARED CARE GUIDELINE FOR THE MANAGEMENT OF PATIENTS ON NALTREXONE FOR ALCOHOL DEPENDENCE INDICATION Naltrexone is used as part of a comprehensive programme of treatment against alcoholism to reduce the
SHARED CARE GUIDELINE FOR THE MANAGEMENT OF PATIENTS ON NALTREXONE FOR ALCOHOL DEPENDENCE INDICATION Naltrexone is used as part of a comprehensive programme of treatment against alcoholism to reduce the
(Adapted with permission from the D-H Knowledge Map Primary Care Buprenorphine Guidelines)
") Buprenorphine Initiation and Maintenance in Pregnancy (Adapted with permission from the D-H Knowledge Map Primary Care Buprenorphine Guidelines) Assessment The diagnosis of OUD should be confirmed by DSM-5
Buprenorphine Initiation and Maintenance in Pregnancy (Adapted with permission from the D-H Knowledge Map Primary Care Buprenorphine Guidelines) Assessment The diagnosis of OUD should be confirmed by DSM-5
Managing Pain in Individuals with Serious Illness and Comorbid Substance Use Disorder
 Managing Pain in Individuals with Serious Illness and Comorbid Substance Use Disorder Presented by: Kathleen Broglio, DNP, ANP-BC, ACHPN, CPE, FPCN on December 1, 2016 Webcast Questions and Answers (Answers
Managing Pain in Individuals with Serious Illness and Comorbid Substance Use Disorder Presented by: Kathleen Broglio, DNP, ANP-BC, ACHPN, CPE, FPCN on December 1, 2016 Webcast Questions and Answers (Answers
Bree Collaborative AMDG Opioid Prescribing Guidelines Workgroup. Opioid Prescribing Metrics - DRAFT
 Bree Collaborative AMDG Opioid Prescribing Guidelines Workgroup Opioid Prescribing Metrics - DRAFT Definitions: Days Supply: The total of all opioid prescriptions dispensed during the calendar quarter
Bree Collaborative AMDG Opioid Prescribing Guidelines Workgroup Opioid Prescribing Metrics - DRAFT Definitions: Days Supply: The total of all opioid prescriptions dispensed during the calendar quarter
Treating Opioid Addiction
 Treating Opioid Addiction Some people who start taking opioid pain medications eventually have serious problems with them and become addicted. Every day, 68 people die in the US from opioid overdose. More
Treating Opioid Addiction Some people who start taking opioid pain medications eventually have serious problems with them and become addicted. Every day, 68 people die in the US from opioid overdose. More
Pain Management Wrap-Up Chronic Care. David Tauben, MD Medicine Anesthesia & Pain Medicine
 Pain Management Wrap-Up Chronic Care David Tauben, MD Medicine Anesthesia & Pain Medicine Objectives Understand that Pain is Complex Know how to select Rx based on Pain type Be aware that Rx only reduces
Pain Management Wrap-Up Chronic Care David Tauben, MD Medicine Anesthesia & Pain Medicine Objectives Understand that Pain is Complex Know how to select Rx based on Pain type Be aware that Rx only reduces
Pharmacist s Role In Pain Management. Katrina Lynn, Pharm D PSHP Annual Assembly: October 12, 2017
 Pharmacist s Role In Pain Management Katrina Lynn, Pharm D PSHP Annual Assembly: October 12, 2017 1 Presentation Objectives Briefly discuss Geisinger Health System and the use of Pain Management Pharmacists
Pharmacist s Role In Pain Management Katrina Lynn, Pharm D PSHP Annual Assembly: October 12, 2017 1 Presentation Objectives Briefly discuss Geisinger Health System and the use of Pain Management Pharmacists
Policy on Pharmacological Therapies Practice Guidance Note Reducing Dosing Errors with Opioid Medicines V04
 Policy on Pharmacological Therapies Practice Guidance Note Reducing Dosing Errors with Opioid Medicines V04 Date issued Issue 1 Nov 2018 Planned review Nov 2021 PPT-PGN 18 part of NTW(C)38 Pharmaceutical
Policy on Pharmacological Therapies Practice Guidance Note Reducing Dosing Errors with Opioid Medicines V04 Date issued Issue 1 Nov 2018 Planned review Nov 2021 PPT-PGN 18 part of NTW(C)38 Pharmaceutical
HARM REDUCTION & TREATMENT. Devin Reaves MSW
 HARM REDUCTION & TREATMENT Devin Reaves MSW The mission of PAHRC is to promote the health, dignity, and human rights of individuals who use drugs and communities impacted by drug use. Recognizing that
HARM REDUCTION & TREATMENT Devin Reaves MSW The mission of PAHRC is to promote the health, dignity, and human rights of individuals who use drugs and communities impacted by drug use. Recognizing that
Universal Precautions and Opioid Risk. Assessment. Questions: How often do you screen your patients for risk of misuse when prescribing opioids?
 Learning objectives 1. Identify the contribution of psychosocial and spiritual factors to pain 2. Incorporate strategies for identifying and mitigating opioid misuse 3. Incorporate non-pharmaceutical modalities
Learning objectives 1. Identify the contribution of psychosocial and spiritual factors to pain 2. Incorporate strategies for identifying and mitigating opioid misuse 3. Incorporate non-pharmaceutical modalities
3. Has the patient had a sustained improvement in Pain or Function (e.g. PEG scale with a 30 percent response from baseline)?
?") Pharmacy Prior Authorization AETA BETTER HEALTH KETUCK Opioids Long-Acting and Short-Acting (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review
Pharmacy Prior Authorization AETA BETTER HEALTH KETUCK Opioids Long-Acting and Short-Acting (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review
Morphine er to oxycontin conversion
 Morphine er to oxycontin conversion The Borg System is 100 % Morphine er to oxycontin conversion 17-4-2011 Conversion dose from Oxycontin 40mg 3x a day to morphine sulfate 15 mg?. Oxycontin vs morphine
Morphine er to oxycontin conversion The Borg System is 100 % Morphine er to oxycontin conversion 17-4-2011 Conversion dose from Oxycontin 40mg 3x a day to morphine sulfate 15 mg?. Oxycontin vs morphine
ADVANCED BEHAVIORAL HEALTH, INC. Clinical Level of Care Guidelines
 The Clinical Level of Care Guidelines contained on the following pages have been developed as a guide to assist care managers, physicians and providers in making medical necessity decisions about the least
The Clinical Level of Care Guidelines contained on the following pages have been developed as a guide to assist care managers, physicians and providers in making medical necessity decisions about the least
MANAGING PAIN IN PATIENTS WITH SUBSTANCE USE DISORDER
 MANAGING PAIN IN PATIENTS WITH SUBSTANCE USE DISORDER Melissa B. Weimer, DO, MCR Chief of Behavioral Health & Addiction Medicine St. Peter s Health Partners Grand Rounds October 11, 2017 Disclosures One
MANAGING PAIN IN PATIENTS WITH SUBSTANCE USE DISORDER Melissa B. Weimer, DO, MCR Chief of Behavioral Health & Addiction Medicine St. Peter s Health Partners Grand Rounds October 11, 2017 Disclosures One
Trainwreck: Addressing Complex Pharmacotherapy With the Inherited Pain Patient
 Trainwreck: Addressing Complex Pharmacotherapy With the Inherited Pain Patient Douglas Gourlay MD, MSc, FRCPC, FASAM Disclosures Nothing to disclose 2 1 Learning Objectives Assess the prescription drug
Trainwreck: Addressing Complex Pharmacotherapy With the Inherited Pain Patient Douglas Gourlay MD, MSc, FRCPC, FASAM Disclosures Nothing to disclose 2 1 Learning Objectives Assess the prescription drug
The Difficult Patient: Risk Mitigation Strategies
 The Difficult Patient: Risk Mitigation Strategies C. Scott Anthony, D.O. Pain Management of Tulsa 1 Opioid Backlash National emergency Opioids not indicated for chronic pain Forces pushing for reduction
The Difficult Patient: Risk Mitigation Strategies C. Scott Anthony, D.O. Pain Management of Tulsa 1 Opioid Backlash National emergency Opioids not indicated for chronic pain Forces pushing for reduction
Mark Edlund, MD, PhD RTI International. Photo courtesy of The Herb Museum, Vancouver, BC
 Opioid Use Disorders and Their Treatment Mark Edlund, MD, PhD RTI International Photo courtesy of The Herb Museum, Vancouver, BC Acknowledgements Funded by NIDA R01 DA022560-01 NIDA R01 DA034627 NIDA R01
Opioid Use Disorders and Their Treatment Mark Edlund, MD, PhD RTI International Photo courtesy of The Herb Museum, Vancouver, BC Acknowledgements Funded by NIDA R01 DA022560-01 NIDA R01 DA034627 NIDA R01