Disclosures. Target Audience. A Focus on Local, Regional and Global Tools for Caring for Clients with Opioid Addictions
|
|
|
- Lesley Wade
- 6 years ago
- Views:
Transcription
1 Disclosures A Focus on Local, Regional and Global Tools for Caring for Clients with Opioid Addictions Dana Murphy-Parker, MS, CRNP, PMHNP-BC, CARN-AP Carmel Clancy, PhD, RN, BSc (Hons), FPH The International Nurses Society on Addictions Dana Murphy-Parker, MS, CRNP, PMHNP-BC, CARN AP No Disclosures Carmel Clancy No Disclosures September 28, Target Audience PCSS-O is a collaborative effort led by American Academy of Addiction Psychiatry (AAAP) in partnership with: Addiction Technology Transfer Center (ATTC), American Academy of Neurology (AAN), American Academy of Pain Medicine (AAPM), American Academy of Pediatrics (AAP), American College of Physicians (ACP), American Dental Association (ADA), American Medical Association (AMA), American Osteopathic Academy of Addiction Medicine (AOAAM), American Psychiatric Association (APA), American Society for Pain Management Nursing (ASPMN), International Nurses Society on Addictions (IntNSA), and Southeast Consortium for Substance Abuse Training (SECSAT). The overarching goal of PCSS-O is to offer evidence-based trainings on the safe and effective prescribing of opioid medications in the treatment of pain and/or opioid addiction. Our focus is to reach providers and/or providers-in-training from diverse healthcare professions including physicians, nurses, dentists, physician assistants, pharmacists, and program administrators. For more information visit: For questions pcss-o@aaap.org Funding for this initiative was made possible (in part) by Providers Clinical Support System for Opioid Therapies (grant no. 1H79TI025595) from SAMHSA. The views expressed in written conference materials or publications and by speakers and moderators do not necessarily reflect the official policies of the Department 3 of Health and Human Services; nor does mention of trade names, commercial practices, or organizations imply endorsement by the U.S. Government.
2 PCSS-O Colleague Support Program Educational Objectives PCSS-O Colleague Support Program is designed to offer general information to health professionals seeking guidance in their clinical practice in prescribing opioid medications. PCSS-O Mentors comprise a national network of trained providers with expertise in addiction medicine/psychiatry and pain management. Our mentoring approach allows every mentor/mentee relationship to be unique and catered to the specific needs of both parties. The mentoring program is available at no cost to providers. For more information on requesting or becoming a mentor visit: Listserv: A resource that provides an Expert of the Month who will answer questions about educational content that has been presented through PCSS-O project. To join pcss-o@aaap.org. 5 At the conclusion of this activity participants should be able to: Incorporate updates of ASAM s Press Conference and Stakeholder Summit held in Washington, D.C. on September 2, Discuss ASAM s National Practice Guideline for the Use of Medications, pocket guide, mobile phone application, slide deck and future educational opportunities. Increase knowledge of online networking tools, specifically wikis and their role in building international co-operation from diverse cultural communities in the area of addiction Share initial lessons from GAaP s first 6 months of operation: planning and set up Explore with participants the challenges and possibilities particularly focusing on the impact of such methodology on achieving wider engagement on a global public health issue and enhancing interprofessional learning. 6 Definitions: No doubt, this is a Medical Disorder: A Neurobiological Disorder What is this about? ASAM defines addiction as a primary, chronic disease of brain reward, motivation, memory, and related circuitry, with a dysfunction in these circuits being reflected in an individual pathologically pursuing reward and/or relief by substance use and other behaviors. The Diagnostic and Statistical Manual of Mental Disorders, 5th Edition (DSM-5) states Substance Use Disorder is a cluster of cognitive, behavioral, and physiological symptoms indicating that the individual continues using the substance despite significant substance-related problems. Opioid use disorder (OUD) include. Opioid Use Disorder Opioid Intoxication Opioid Withdrawal Other Opioid-Induced Disorders Unspecified Opioid-Related Disorders 7 The ASAM National Practice Guideline for the Use of Medications in the Treatment of Addiction Involving Opioid Use The ASAM National Practice Guideline is the 1st to include all FDA-approved medications in single document 8








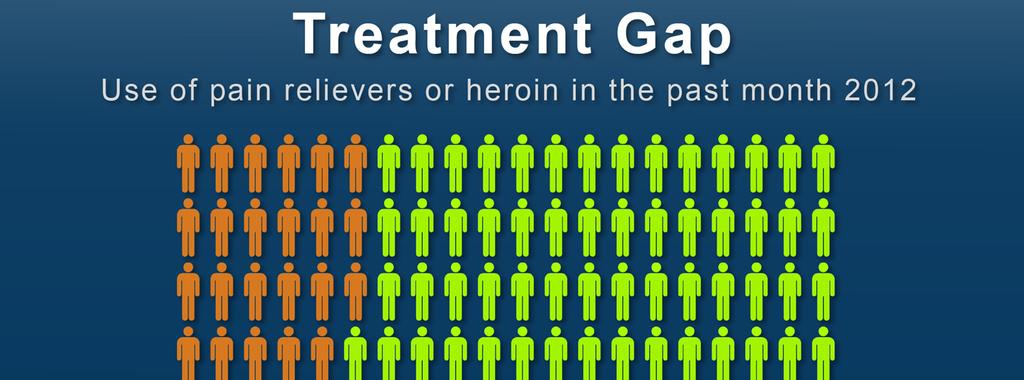
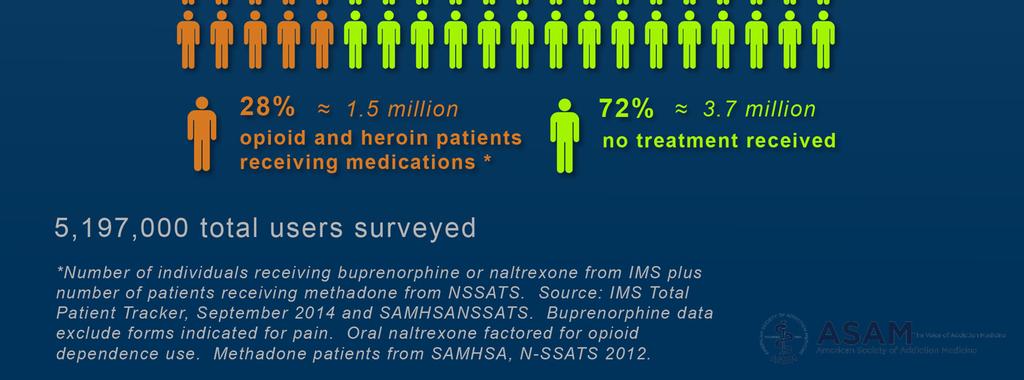
3 Why is this so important? 9 12
4 Journal of Addictions Medicine (2015) Psychosocial Treatment in Conjunction With Medications for the Treatment of Opioid Use Disorder Just published: Kampman, K. & Jarvis, M. (2015). American Society of Addiction Medicine (ASAM) National Practice Guidelines for the Use of Medications in the Treatment of Addiction Involving Opioid Use. Journal of Addiction Medicine, 9 (5). September/October A review of the literature on the efficacy of psychosocial treatment to be used in conjunction with Medication Assisted Treatment (MAT) of opioid use disorder was conducted. The review was partially funded by National Institute of Drug Abuse (NIDA). Methodology of this review can be found with the ASAM journal article previously mentioned. A full article on the literature review will be published in a subsequent Journal of Addiction Medicine edition. 1 Categories covered in the National Practice Guidelines Assessment Diagnosis Treatment 15 ASSESSMENT The first clinical priority should be given to identifying and making appropriate referral for any urgent or emergent medical or psychiatric problem(s), including drug-related impairment or overdose. Completion of the patient s medical history should include screening for concomitant medical conditions, including infectious diseases (hepatitis, HIV, and TB), acute trauma, and pregnancy. (The leading causes of death in people using opioids for nonmedical purposes are overdose and trauma). A physical examination should be completed as a component of the comprehensive assessment process. The prescriber (the clinician authorizing the use of a medication for the treatment of OUD) may conduct this physical examination him/herself, or, in accordance with the ASAM Standards1, ensure that a current physical examination is contained within the patient medical record before a patient is started on a new medication for the treatment of his/her addiction. Initial laboratory testing should include a complete blood count, liver function tests, and tests for hepatitis A, B, C and HIV. Testing for TB and sexually transmitted infections should also be considered. Hepatitis A and B vaccination should be offered, for those who are pregnant and the general population. 16
5 Diagnosis Symptoms of Opioid Intoxication Other clinicians may diagnose OUD, but confirmation of the diagnosis by the provider with prescribing authority, and who recommends medication use, must be obtained before pharmacotherapy for OUD commences. OUD is primarily diagnosed on the basis of the history provided by the patient and a comprehensive assessment that includes a physical examination. Validated clinical scales that measure withdrawal symptoms may be used to assist in the evaluation of patients with OUD: Examples include; The Objective Opioid Withdrawal Scale (OOWS)a The Subjective Opioid Withdrawal Scale (SOWS)a The Clinical Opioid Withdrawal Scale (COWS)a Visit www. GuidelineCentral.com/OUD for calculators Drooping eyelids Constricted pupils Reduced respiratory rate Scratching (due to histamine release) Head nodding Urine drug testing during the comprehensive assessment process, and frequently during treatment, is recommended Withdrawal Signs Treatment Setting Yawning Rhinorrhea OOWS SOWS COWS Piloerection (observe arm) Perspiration Lacrimation Tremor (hands) Mydriasis Hot and cold flushes Restlessness Vomiting Muscle twitches Abdominal cramps Anxiety I feel anxious. I feel like yawning. I m perspiring. My eyes are tearing. My nose is running. I have goose flesh. I am shaking. I have hot flashes. I have cold flashes. My bones and muscles ache. I feel restless. I feel nauseous. I feel like vomiting. Pulse Sweating Restlessness Pupil size Bone or joint aches Rhinorrhea Tearing GI upset Tremor of outstretched hands Yawning Anxiety or irritability Gooseflesh skin 19 Clinicians should consider the patient s preferences, past treatment history, and treatment setting when deciding between the use of methadone, buprenorphine, and naltrexone in the treatment of addiction involving opioid use. The treatment setting described as Level 1 treatment in the ASAM Criteria may be a general outpatient location such as a clinician s practice site. The setting as described as Level 2 in the ASAM Criteria may be an intensive outpatient treatment or partial hospitalization program housed in a specialty addiction treatment facility, a community mental health center, or another setting. The ASAM Criteria describes Level 3 or Level treatment respectively as a residential addiction treatment facility or hospital. The venue in which treatment is provided is as important as the specific medication selected. 20
6 Treatment Setting, con t FDA Approved Medications for Opioid Use Disorder Opioid Treatment Programs offer daily supervised dosing of methadone, and increasingly of buprenorphine. Naltrexone can be prescribed in any setting by any clinician with the authority to prescribe any medication. In accordance with federal law (21 CFR ), Office-Based Opioid Treatment (OBOT), which provides medication on a prescribed weekly or monthly basis, is limited to buprenorphine. Clinicians should consider a patient s psychosocial situation, co-occurring disorders, and risk of diversion when determining whether Opioid Treatment Programs (OTP) or OBOT is most appropriate. OBOT may not be suitable for patients with active alcohol use disorder or sedative, hypnotic, or anxiolytic use disorder (or who are in the treatment of addiction involving the use of alcohol or other sedative drugs, including benzodiazepines or benzodiazepine receptor agonists). It may also be unsuitable for persons who are regularly using alcohol or other sedatives but do not have addiction or a specific substance use disorder related to that class of drugs. The prescribing of benzodiazepines or other sedative-hypnotics should be used with extreme caution in patients who are prescribed methadone or buprenorphine for the treatment of an OUD 21 Methadone Buprenorphine (In ASAM s pocket guide, reference to buprenorphine is for the combination buprenorphine/naloxone formulations. If the single reference is made to buprenorphine, it is referred to as buprenorphine monoproduct. Naltrexone, both the oral and the injectable (Vivitrol) Naloxone The Guideline Committee recommends the inclusion of clonidine as a practice to support opioid withdrawal. Clonidine is not FDA-approved for the treatment of opioid withdrawal but it has been extensively used off-label for this purpose. Clonidine may be used orally or transdermally at doses of mg every 6 8 hours with a maximum dose of 1.2 mg daily to assist in the management of opioid withdrawal symptoms. Its hypotensive effects often limit the amount that can be used. Clonidine can be combined with other non-narcotic medications targeting specific opioid withdrawal symptoms such as benzodiazepines for anxiety, loperamide for diarrhea, acetaminophen or nonsteroidal anti-inflammatory medications (NSAIDs) for pain, and ondansetron or other agents for nausea. 22 Venue for Treatment Setting Current Prescribers for Buprenorphine Opioid Treatment Programs offer daily supervised dosing of methadone, and increasingly of buprenorphine. Naltrexone can be prescribed in any setting by any clinician with the authority to prescribe any medication. In accordance with federal law (21 CFR ), Office-Based Opioid Treatment (OBOT), which provides medication on a prescribed weekly or monthly basis, is limited to buprenorphine. Clinicians should consider a patient s psychosocial situation, cooccurring disorders, and risk of diversion when determining whether Opioid Treatment Programs (OTP) or OBOT is most appropriate. Time Frame Past 30 days Past 60 days Past 90 days Last year Current 30 patient certified ,037 20,722 % 100 patient certified 68.% 15 60% 65.6% 67.1% 67.9% ,89 9,801 % Total 31.6% % % 1,388 32,9%,526 30, % 23 2
7 The TREAT ACT Obama Administration Makes Big Announcement Addressing Heroin Epidemic Introduced in July, 201 by Senator Edward J. Markey (D-Massachusetts) introduced the Recovery Enhancement for Addiction Treatment (TREAT ACT). This bill will increase the number of patients that qualified physicians could treat for opioid dependency and, for the first time, allow certain nurse practitioners and physician assistants to treat patients by allowing other prescribers to prescribe buprenorphine. This legislation is supported by: The American Medical Association The American Society of Addictions Medicine The American Association of Nurse Practitioners The International Nurses Society on Addictions Rundio, A (2015). Landmark legislation to expand treatment for heroin and prescription drug addiction. Journal of Addictions Nursing,26 (3), pp This past spring, Sen. Edward Markey (D-Mass.) and Sen. Rand Paul (R-Ky.) introduced legislation that would raise the first-year cap from 30 patients to 100 and offer nurse practitioners and physician assistants the ability to prescribe the medication. After one year, doctors could seek to remove the cap entirely Buprenorphine, a Partial Agonist Buprenorphine, con t Opioid-dependent patients should wait until they are experiencing mild to moderate opioid withdrawal before taking the first dose of buprenorphine to reduce the risk of precipitated withdrawal. Generally, buprenorphine initiation should occur at least 6 12 hours after the last use of heroin or other short-acting opioids, or 2 72 hours after their last use of long-acting opioids such as methadone. Induction of buprenorphine should start with a dose of 2 mg. Dosages may be increased in increments of 2 mg. Clinicians should observe patients in their offices during induction. However, home buprenorphine induction may be considered. Home-based induction is recommended only if the patient or prescribing physician is experienced with the use of buprenorphine. Buprenorphine doses after induction and titration should be, on average, 8 mg per day. However, if patients are continuing to use opioids, consideration should be given to increasing the dose by 8 mg (daily doses of mg or higher). The FDA approves dosing to a limit of 2 mg per day, and there is limited evidence regarding the relative efficacy of higher doses. In addition, the use of higher doses may increase the risk of diversion. When considering a switch from buprenorphine to naltrexone, 7 1 days should elapse between the last dose of buprenorphine and the start of naltrexone to ensure that the patient is not physically dependent on opioids prior to starting naltrexone. When considering a switch from buprenorphine to methadone, there is no required time delay since the addition of a full mu-opioid agonist to a partial agonist does not typically result in any type of adverse reaction. Patients who discontinue agonist therapy and resume opioid use should be made aware of the risks associated with an opioid overdose, and especially the increased risk of death
8 Methadone Methadone, con t Methadone is a treatment option recommended for patients who are physiologically dependent on opioids, able to give informed consent, and who have no specific contraindications for agonist treatment when it is prescribed in the context of an appropriate plan that includes psychosocial intervention. The recommended initial dose ranges for methadone are from mg with reassessment in 3 hours, and a second dose not to exceed 10 mg on the first day if withdrawal symptoms are persisting. The usual daily dosage of methadone ranges from mg. Some patients may respond to lower doses, and some patients may need higher doses. Dosage increases in 5 10 mg increments applied no more frequently than every 7 days (depending on clinical response) are necessary to avoid over-sedation, toxicity, or even iatrogenic overdose deaths. The administration of methadone should be monitored because unsupervised administration can lead to misuse and diversion. OTP regulations require monitored medication administration until the patient s clinical response and behavior demonstrates that the prescribing of non-monitored 29 doses is appropriate. Switching from methadone to another medication for the treatment of OUD may be appropriate if the patient experiences intolerable side effects or is not successful in attaining or maintaining treatment goals through the use of methadone. Patients switching from methadone to buprenorphine in the treatment of OUD should be on low doses of methadone prior to switching medications. Patients on low doses of methadone (30 0 mg per day or less) generally tolerate transition to buprenorphine with minimal discomfort, whereas patients on higher doses of methadone may experience significant discomfort in switching medications. Patients switching from methadone to oral naltrexone or extended-release injectable naltrexone must be completely withdrawn from methadone and other opioids, before they can receive naltrexone. The only exception would apply when an experienced clinician receives consent from the patient to embark on a plan of naltrexone-facilitated opioid withdrawal management. Patients who discontinue agonist therapy with methadone or buprenorphine and then resume opioid use should be made aware of the risks associated with opioid overdose, and especially the increased risk of death. 30 Naltrexone, an Opioid Antagonist Medication Naltrexone, con t Naltrexone is a recommended treatment in preventing relapse in OUD. Oral formula naltrexone may be considered for patients where adherence can be supervised or enforced. Extended-release injectable naltrexone (Vivitrol) may be more suitable for patients who have issues with adherence. Oral naltrexone should be taken daily in 50 mg doses, or 3 times weekly in two 100 mg doses followed by one 150 mg dose. Extended-release injectable naltrexone should be administered every weeks by deep intramuscular injection in the gluteal muscle at a set dosage of 380 mg per injection. There is no recommended length of treatment with oral naltrexone or extended-release injectable naltrexone. Duration depends on clinical judgment and the patient s individual circumstances. Because there is no physical dependence associated with naltrexone, it can be stopped abruptly without withdrawal symptoms. Switching from naltrexone to methadone or buprenorphine should be planned, considered, and monitored. Switching from an antagonist such as naltrexone to a full agonist (methadone) or a partial agonist (buprenorphine) is generally less complicated than switching from a full or partial agonist to an antagonist because there is no physical dependence associated with antagonist treatment and thus no possibility of precipitated withdrawal


 0. mg/0.")
9 Naloxone, an Opioid Antagonist Medication Naloxone should be given in case of opioid overdose. Naloxone can and should be administered to pregnant women in cases of overdose in order to save the mother s life. The Guideline Committee, based on consensus opinion, recommends that patients who are being treated for OUD and their family members/significant others be given prescriptions for naloxone. Patients and family members/significant others should be trained in the use of naloxone in overdose. The Guideline Committee, based on consensus opinion, recommends that first responders such as emergency medical services personnel, police officers, and firefighters be trained in and authorized to administer naloxone. Naloxone injection Evzio (auto-injector) 0. mg/0. ml For emergency treatment of overdose Narcan, generic (various) Opioid depression, diagnosis of suspected opioid overdose, Naloxone There is not yet an FDA-approved intranasal formulation. There are only kits made available to deliver the injectable formulation intranasally WHO UK The Guidelines review the use of medicines such as methadone, buprenorphine, naltrexone and clonidine in combination with psychosocial support in the treatment of people dependent on heroin or other opioids. Based on systematic reviews of the literature and using the GRADE approach to determining evidence quality, the guidelines contain specific recommendations on the range of issues faced in organizing treatment systems, managing treatment programmes and in treating people dependent on opioids edition New guidelines coming out in early 2016 Addresses management of opi 35 36




10 Primary Care Setting - UK Australia GAaP History and Background Some of the GAaP members Although established formally in May 201 the origins and idea for GAaP have been around a long time, primary through ongoing collaboration between Dana Murphy-Parker and Carmel Clancy since 1998 GAaP has been initially supported via small grants via Middlesex University founding members of GAaP are drawn from UK, USA, Brazil and New Zealand 39 Presentation title 3 0 Presentation title
11 Drexel University GAaP USA Middlesex University GAaP UK University San Paolo GAaP Brazil Who is GAaP Nordland Hospital, GAaP Norway NCETA, GAaP Australia Potential members coming online GAaP China GAaP Israel GAaP Ireland GAaP S. Korea GAaP Japan Universiteti Planetari I Tiranes GAaP Albania Matua Raki GAaP New Zealand Structure Each country has an identified GAaP Co-ordinating Centre e.g. GAaP USA is Drexel University (contact person Dana Murphy-Parker dam355@drexel.edu) The Co-ordinating Centre has a responsibility to set up a GAaP Country Reference Group these groups must be interdisciplinary, members should have a background in addiction, and be representative of different types of facilities e.g. universities; practice; policy; research etc The GAaP co-ordinating centers meet online employing the use of a WIKI platform and Skype 1 2 Presentation title Our Vision for GAaP Explore addiction issues across countries e.g. policies; service user lived experience; treatment comparing differences and similarities Raise the profile of addiction including an aspect of activism Establish joint workforce guidelines standardization of preparation for professionals working in the field of addiction - Getting it into the Water Supply Provide a virtual room for everyone to enter to discuss the issues as outlined above Become a knowledge Hub Become a vehicle/platform to transfer best practice or 3 Middlesex explore University what good looks like To provide a platform communication tool to raise awareness and explore brief interventions; psychosocial issues; pharmacology To be a global online classroom A place to increase curiosity/increasing competencies directly in the field A community of practice and a resource tool, which can be sliced in different ways An Intersection between policy/clinical/academic communities A global knowledge network finding synergies
12 Key Strategic Areas Practice Education Research Policy Workforce Planning Methodology for staying connected & working together Wiki (online network community) Jointly delivered on-line courses Off line linking e.g. conferences; staff & student exchanges 5 6 It is not without its challenges First major project Slow burner Techno issues access issues; variation in level of members expertise The world clock I m awake, you re asleep! Finding the time Funding issues and volunteer syndrome MOOC (Massive Open Online Course) Falling Down Older People and Problematic Substance Use Course release/ teaching starts on 7 th of March until 10 April Presentation title 8
13 Broad Learning Outcomes for MOOC 1. To explore problematic substances use in relation to older people and their carers through current research, practice and service user and carers perspectives. 2. To promote awareness of current challenges when working with problematic substance use in ageing contexts for practitioners working with problematic substance use and for those working in ageing services who may not have a detailed knowledge of this issue. 3. To identify the scope of the issue within an international and national context and to identify the need for further knowledge, skills, service development and partnerships as well as future research and guidance in order to meet these challenges 9. References ASAM (2015). National Practice Guidelines and Associated Products at Press Conference and Stakeholder Summit on September 2, Retrieved at Website, Department of Health (England) and the devolved administrations (2007). Drug Misuse and Dependence: UK Guidelines on Clinical Management. London: Department of Health (England), the Scottish Government, Welsh Assembly Government and Northern Ireland Executive. Guidance for the use of substitute prescribing in the treatment of opioid dependence in primary care. Available at : Rundio, A (2015). Landmark legislation to expand treatment for heroin and Journal of Addictions Nursing,26 (3), pp prescription drug addiction. World Health Organization (WHO) (2009). Guidelines for psychosocially assisted pharmacological treatment of persons dependent on opioids. Retrieved at: 50
Clinical Guidelines for the Pharmacologic Treatment of Opioid Use Disorder
 Clinical Guidelines for the Pharmacologic Treatment of Community Behavioral Health (CBH) is committed to working with our provider partners to continuously improve the quality of behavioral healthcare
Clinical Guidelines for the Pharmacologic Treatment of Community Behavioral Health (CBH) is committed to working with our provider partners to continuously improve the quality of behavioral healthcare
Addiction Prediction: Errors from the bedside hurt patients with pain. Objectives. CDC guideline for prescribing OPIOIDS for Chronic Pain
 Addiction Prediction: Errors from the bedside hurt patients with pain Renee C.B. Manworren, PhD, APRN, BC, PCNS-BC, AP-PMN, FAAN Director of Nursing Research and Professional Practice Posy and Fred Love
Addiction Prediction: Errors from the bedside hurt patients with pain Renee C.B. Manworren, PhD, APRN, BC, PCNS-BC, AP-PMN, FAAN Director of Nursing Research and Professional Practice Posy and Fred Love
Pain Care & Prescription Drug Abuse: Current Topics, Legislation & Policy. Disclosure. Preview
 Providers Clinical Support System for Opioid Therapies (PCSS-O) Webinar March 7, 2017 Pain Care & Prescription Drug Abuse: Current Topics, Legislation & Policy Wade Delk, Government Affairs Director, ASPMN
Providers Clinical Support System for Opioid Therapies (PCSS-O) Webinar March 7, 2017 Pain Care & Prescription Drug Abuse: Current Topics, Legislation & Policy Wade Delk, Government Affairs Director, ASPMN
Managing Pain in the Patient with Opioid Use Disorder: Inpatient Management. Melissa Weimer, DO, MCR Oregon Health & Science University
 Managing Pain in the Patient with Opioid Use Disorder: Inpatient Management Melissa Weimer, DO, MCR Oregon Health & Science University 1 Educational Objectives At the conclusion of this activity participants
Managing Pain in the Patient with Opioid Use Disorder: Inpatient Management Melissa Weimer, DO, MCR Oregon Health & Science University 1 Educational Objectives At the conclusion of this activity participants
Nursing Regulatory Boards Efforts to Provide Guidance to Nurses About Mitigating Prescription Medication Abuse/Diversion
 Nursing Regulatory Boards Efforts to Provide Guidance to Nurses About Mitigating Prescription Medication Abuse/Diversion Cathy Carlson, PhD, APN, FNP-BC Aaron Gilson, MS, MSSW, PhD Authors Conflicts of
Nursing Regulatory Boards Efforts to Provide Guidance to Nurses About Mitigating Prescription Medication Abuse/Diversion Cathy Carlson, PhD, APN, FNP-BC Aaron Gilson, MS, MSSW, PhD Authors Conflicts of
Course Overview Management of Chronic Pain: A Core Curriculum for Primary Care Providers
 Course Overview Management of Chronic Pain: A Core Curriculum for Primary Care Providers Sponsored by PCSS-O American Academy of Addiction Psychiatry Roger Chou, MD 1 About PCSS-O PCSS-O is a national
Course Overview Management of Chronic Pain: A Core Curriculum for Primary Care Providers Sponsored by PCSS-O American Academy of Addiction Psychiatry Roger Chou, MD 1 About PCSS-O PCSS-O is a national
PCSS Projects. Kathryn L. Cates-Wessel Executive Director, AAAP PCSS-MAT and PCSS-O PI and Project Director
 PCSS Projects Kathryn L. Cates-Wessel Executive Director, AAAP PCSS-MAT and PCSS-O PI and Project Director 1 Educational Objectives At the conclusion of this activity participants should be able to: Describe
PCSS Projects Kathryn L. Cates-Wessel Executive Director, AAAP PCSS-MAT and PCSS-O PI and Project Director 1 Educational Objectives At the conclusion of this activity participants should be able to: Describe
Kurt Haspert, MS, CRNP University of Maryland Baltimore Washington Medical Center
 Kurt Haspert, MS, CRNP University of Maryland Baltimore Washington Medical Center Data from the National Vital Statistics System Mortality The age-adjusted rate of drug overdose deaths in the United States
Kurt Haspert, MS, CRNP University of Maryland Baltimore Washington Medical Center Data from the National Vital Statistics System Mortality The age-adjusted rate of drug overdose deaths in the United States
Financing Factors for Implementing Medication-Assisted Treatment
 Financing Factors for Implementing Medication-Assisted Treatment Jeremy Attermann, MSW, National Council for Behavioral Health Nick Szubiak, LCSW, National Council for Behavioral Health Brad DeCamp, MPA,
Financing Factors for Implementing Medication-Assisted Treatment Jeremy Attermann, MSW, National Council for Behavioral Health Nick Szubiak, LCSW, National Council for Behavioral Health Brad DeCamp, MPA,
Opioids Research to Practice
 Opioids Research to Practice CRIT Program May 2009 Daniel P. Alford, MD, MPH Associate Professor of Medicine Boston University School of Medicine Boston Medical Center 32 yo female brought in after heroin
Opioids Research to Practice CRIT Program May 2009 Daniel P. Alford, MD, MPH Associate Professor of Medicine Boston University School of Medicine Boston Medical Center 32 yo female brought in after heroin
Opioids for Pain Treatment in Persons with Opioid Use Disorder. Patricia Pade, MD Seddon R. Savage, MD, MS Melissa Weimer, DO, MCR
 Opioids for Pain Treatment in Persons with Opioid Use Disorder Patricia Pade, MD Seddon R. Savage, MD, MS Melissa Weimer, DO, MCR 1 Educational Objectives At the conclusion of this activity participants
Opioids for Pain Treatment in Persons with Opioid Use Disorder Patricia Pade, MD Seddon R. Savage, MD, MS Melissa Weimer, DO, MCR 1 Educational Objectives At the conclusion of this activity participants
Opioid Dependence 101 and Medication Assisted Treatment
 Opioid Dependence 101 and Medication Assisted Treatment Dr. Joji Suzuki Director of the Division of Addiction Psychiatry, Brigham & Women s Hospital Assistant Professor of Psychiatry, Harvard Medical School
Opioid Dependence 101 and Medication Assisted Treatment Dr. Joji Suzuki Director of the Division of Addiction Psychiatry, Brigham & Women s Hospital Assistant Professor of Psychiatry, Harvard Medical School
(Adapted with permission from the D-H Knowledge Map Primary Care Buprenorphine Guidelines)
") Buprenorphine Initiation and Maintenance in Pregnancy (Adapted with permission from the D-H Knowledge Map Primary Care Buprenorphine Guidelines) Assessment The diagnosis of OUD should be confirmed by DSM-5
Buprenorphine Initiation and Maintenance in Pregnancy (Adapted with permission from the D-H Knowledge Map Primary Care Buprenorphine Guidelines) Assessment The diagnosis of OUD should be confirmed by DSM-5
Opioids Research to Practice
 Opioids Research to Practice CRIT Program May 2008 Daniel P. Alford, MD, MPH Associate Professor of Medicine Boston University School of Medicine Boston Medical Center 32 yo female brought in after heroin
Opioids Research to Practice CRIT Program May 2008 Daniel P. Alford, MD, MPH Associate Professor of Medicine Boston University School of Medicine Boston Medical Center 32 yo female brought in after heroin
STOPPING OPIOIDS. William Morrone, DO MS, FACOFP DABAM DAAPM Deputy Chief Medical Examiner & AOAAM June 24, 2015 Noon ET
 STOPPING OPIOIDS William Morrone, DO MS, FACOFP DABAM DAAPM Deputy Chief Medical Examiner & AOAAM June 24, 2015 Noon ET 1 William Morrone DO, Disclosures William Morrone, DO has presented numerous programs
STOPPING OPIOIDS William Morrone, DO MS, FACOFP DABAM DAAPM Deputy Chief Medical Examiner & AOAAM June 24, 2015 Noon ET 1 William Morrone DO, Disclosures William Morrone, DO has presented numerous programs
Disclosures. Target Audience 4/28/2015. The Road Less Traveled: Using Buprenorphine-Naloxone to Treat High-Risk Chronic Pain Patients
 The Road Less Traveled: Using Buprenorphine-Naloxone to Treat High-Risk Chronic Pain Patients Patrick Marshalek, MD Jenna Martino, MSN, FNP-C Audrey Royce, MSN, FNP-C Sarah Roy, MSN, RN, CCRN West Virginia
The Road Less Traveled: Using Buprenorphine-Naloxone to Treat High-Risk Chronic Pain Patients Patrick Marshalek, MD Jenna Martino, MSN, FNP-C Audrey Royce, MSN, FNP-C Sarah Roy, MSN, RN, CCRN West Virginia
DISCLAIMER: ECHO Nevada emphasizes patient privacy and asks participants to not share ANY Protected Health Information during ECHO clinics.
 DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
Opioid dependence: Detoxification
 Opioid dependence: Detoxification What is detoxification? A. Process of removal of toxins from the body? B. Admitting a drug dependent person in a hospital and giving him nutrition? C. Stopping drug use
Opioid dependence: Detoxification What is detoxification? A. Process of removal of toxins from the body? B. Admitting a drug dependent person in a hospital and giving him nutrition? C. Stopping drug use
Rates of Opioid Misuse, Abuse, and Addiction in Chronic Pain. Kevin E. Vowles, PhD University of New Mexico
 Rates of Opioid Misuse, Abuse, and Addiction in Chronic Pain Kevin E. Vowles, PhD University of New Mexico 1 Kevin E. Vowles, Disclosures Consultant, Pfizer Independent Grants for Learning and Change,
Rates of Opioid Misuse, Abuse, and Addiction in Chronic Pain Kevin E. Vowles, PhD University of New Mexico 1 Kevin E. Vowles, Disclosures Consultant, Pfizer Independent Grants for Learning and Change,
People inject, sniff, snort, or smoke heroin. Some people mix heroin with crack cocaine, a practice called speedballing.
 What is heroin? Heroin is an opioid drug made from morphine, a natural substance taken from the seed pod of the various opium poppy plants grown in Southeast and Southwest Asia, Mexico, and Colombia. Heroin
What is heroin? Heroin is an opioid drug made from morphine, a natural substance taken from the seed pod of the various opium poppy plants grown in Southeast and Southwest Asia, Mexico, and Colombia. Heroin
SHARED CARE GUIDELINE FOR THE MANAGEMENT OF PATIENTS ON NALTREXONE FOR OPIOID DEPENDENCE
 SHARED CARE GUIDELINE FOR THE MANAGEMENT OF PATIENTS ON NALTREXONE FOR OPIOID DEPENDENCE INDICATION Naltrexone is a pure opiate antagonist licensed as an adjunctive prophylactic therapy in the maintenance
SHARED CARE GUIDELINE FOR THE MANAGEMENT OF PATIENTS ON NALTREXONE FOR OPIOID DEPENDENCE INDICATION Naltrexone is a pure opiate antagonist licensed as an adjunctive prophylactic therapy in the maintenance
Opioids Research to Practice
 Opioids Research to Practice May 2013 Daniel P. Alford, MD, MPH, FACP, FASAM Associate Professor of Medicine Assistant Dean, Continuing Medical Education Case 32 yo female brought in after heroin overdose
Opioids Research to Practice May 2013 Daniel P. Alford, MD, MPH, FACP, FASAM Associate Professor of Medicine Assistant Dean, Continuing Medical Education Case 32 yo female brought in after heroin overdose
Medications in the Treatment of Opioid Use Disorder: Methadone and Buprenorphine What Really Are They?
 Medications in the Treatment of Opioid Use Disorder: Methadone and Buprenorphine What Really Are They? Yngvild Olsen, MD, MPH Cecil County Board of Health Workgroup Meeting Elkton, MD October 8, 2013 Objectives
Medications in the Treatment of Opioid Use Disorder: Methadone and Buprenorphine What Really Are They? Yngvild Olsen, MD, MPH Cecil County Board of Health Workgroup Meeting Elkton, MD October 8, 2013 Objectives
Appendix F Federation of State Medical Boards
 Appendix F Federation of State Medical Boards Model Policy Guidelines for Opioid Addiction Treatment in the Medical Office SECTION I: PREAMBLE The (name of board) recognizes that the prevalence of addiction
Appendix F Federation of State Medical Boards Model Policy Guidelines for Opioid Addiction Treatment in the Medical Office SECTION I: PREAMBLE The (name of board) recognizes that the prevalence of addiction
Hospitals Role in Addressing the Opioid Crisis
 Hospitals Role in Addressing the Opioid Crisis Webinar 5: Buprenorphine in the Emergency Department November 14, 2017 Agenda Hospital Based Buprenorphine Initiatives Yngvild Olsen, M.D., Medical Consultant,
Hospitals Role in Addressing the Opioid Crisis Webinar 5: Buprenorphine in the Emergency Department November 14, 2017 Agenda Hospital Based Buprenorphine Initiatives Yngvild Olsen, M.D., Medical Consultant,
Opioids Research to Practice
 Opioids Research to Practice CRIT/FIT 2016 April 2016 Daniel P. Alford, MD, MPH Associate Professor of Medicine Assistant Dean, Continuing Medical Education Director, Clinical Addiction Research and Education
Opioids Research to Practice CRIT/FIT 2016 April 2016 Daniel P. Alford, MD, MPH Associate Professor of Medicine Assistant Dean, Continuing Medical Education Director, Clinical Addiction Research and Education
ROSC & MAT II: Opioid Treatment Services
 ROSC & MAT II: Opioid Treatment Services September 23, 2015 Stan DeKemper Executive Director Indiana Credentialing Association on Addiction and Drug Abuse 1 GOALS Review medication assisted recovery Identify
ROSC & MAT II: Opioid Treatment Services September 23, 2015 Stan DeKemper Executive Director Indiana Credentialing Association on Addiction and Drug Abuse 1 GOALS Review medication assisted recovery Identify
Main Results and Clinical Implications of the X:BOT Trial: XR-Naltrexone vs. Buprenorphine-Naloxone Film
 Main Results and Clinical Implications of the X:BOT Trial: XR-Naltrexone vs. Buprenorphine-Naloxone Film July 31 st, 2018 Hosted by John A. Renner, Jr., MD, DLFAPA Professor of Psychiatry Boston University
Main Results and Clinical Implications of the X:BOT Trial: XR-Naltrexone vs. Buprenorphine-Naloxone Film July 31 st, 2018 Hosted by John A. Renner, Jr., MD, DLFAPA Professor of Psychiatry Boston University
Opioids Research to Practice
 Opioids Research to Practice CRIT Program May 2010 Daniel P. Alford, MD, MPH Associate Professor of Medicine Boston University School of Medicine Boston Medical Center 32 yo female brought in after heroin
Opioids Research to Practice CRIT Program May 2010 Daniel P. Alford, MD, MPH Associate Professor of Medicine Boston University School of Medicine Boston Medical Center 32 yo female brought in after heroin
Pregnancy and Addiction
 Pregnancy and Addiction Carl Christensen, MD, PhD, D-FASAM Clinical Associate Professor, OB Gyn & Psychiatry Wayne State University School of Medicine November 16, 2016 1 Educational Objectives At the
Pregnancy and Addiction Carl Christensen, MD, PhD, D-FASAM Clinical Associate Professor, OB Gyn & Psychiatry Wayne State University School of Medicine November 16, 2016 1 Educational Objectives At the
Prepublication Requirements
 Issued Prepublication Requirements The Joint Commission has approved the following revisions for prepublication. While revised requirements are published in the semiannual updates to the print manuals
Issued Prepublication Requirements The Joint Commission has approved the following revisions for prepublication. While revised requirements are published in the semiannual updates to the print manuals
The CARA & Buprenorphine Prescribing for APNs & PAs
 The CARA & Buprenorphine Prescribing for APNs & PAs William J. Lorman, JD, PhD, MSN, PMHNP-BC, CARN-AP FIAAN Assistant Clinical Professor, Drexel University, Philadelphia, PA V. P. & Chief Clinical Officer,
The CARA & Buprenorphine Prescribing for APNs & PAs William J. Lorman, JD, PhD, MSN, PMHNP-BC, CARN-AP FIAAN Assistant Clinical Professor, Drexel University, Philadelphia, PA V. P. & Chief Clinical Officer,
Disclosures. I have no disclosures or commercial interests to report
 Colleen T. LaBelle, MSN, RN-BC,CARN Program Director, Office-Based Addiction Treatment Director, STATE OBAT Boston Medical Center Disclosures I have no disclosures or commercial interests to report Medication-Assisted
Colleen T. LaBelle, MSN, RN-BC,CARN Program Director, Office-Based Addiction Treatment Director, STATE OBAT Boston Medical Center Disclosures I have no disclosures or commercial interests to report Medication-Assisted
Medication-Assisted Treatment. What Is It and Why Do We Use It?
 Medication-Assisted Treatment What Is It and Why Do We Use It? What is addiction, really? o The four C s of addiction: Craving. Loss of Control of amount or frequency of use. Compulsion to use. Use despite
Medication-Assisted Treatment What Is It and Why Do We Use It? What is addiction, really? o The four C s of addiction: Craving. Loss of Control of amount or frequency of use. Compulsion to use. Use despite
Clinical Guidelines for the Use of Buprenorphine in the Treatment of Opioid Addiction
 Clinical Guidelines for the Use of Buprenorphine in the Treatment of Opioid Addiction Multiple Choice Identify the choice that best completes the statement or answers the question. 1. Executive Summary
Clinical Guidelines for the Use of Buprenorphine in the Treatment of Opioid Addiction Multiple Choice Identify the choice that best completes the statement or answers the question. 1. Executive Summary
SC MAT ACCESS. Medication Assisted Treatment Academic Community Capacity Expansion for Sustainable Success Kathleen Brady, MD, PhD, VPR, MUSC
 SC MAT ACCESS Medication Assisted Treatment Academic Community Capacity Expansion for Sustainable Success Kathleen Brady, MD, PhD, VPR, MUSC Overdose Death Rates from Opiates Most important sign of a
SC MAT ACCESS Medication Assisted Treatment Academic Community Capacity Expansion for Sustainable Success Kathleen Brady, MD, PhD, VPR, MUSC Overdose Death Rates from Opiates Most important sign of a
Opioid Management of Chronic (Non- Cancer) Pain
 Pain") Optima Health Opioid Management of Chronic (Non- Cancer) Pain Guideline History Original Approve Date 5/08 Review/Revise Dates 11/09, 9/11, 9/13, 09/15, 9/17 Next Review Date 9/19 These Guidelines are
Optima Health Opioid Management of Chronic (Non- Cancer) Pain Guideline History Original Approve Date 5/08 Review/Revise Dates 11/09, 9/11, 9/13, 09/15, 9/17 Next Review Date 9/19 These Guidelines are
Opioid Use Disorders &Medication Treatment
 Agency medical director comments Opioid Use Disorders &Medication Treatment Charissa Fotinos, MD, MSc Deputy Chief Medical Officer Washington State Health Care Authority Learning Objectives: 1) Review
Agency medical director comments Opioid Use Disorders &Medication Treatment Charissa Fotinos, MD, MSc Deputy Chief Medical Officer Washington State Health Care Authority Learning Objectives: 1) Review
Addressing the Opioid Crisis Workgroup: Treatment and Overdose Prevention
 The Accountable Community for Health of King County Addressing the Opioid Crisis Workgroup: Treatment and Overdose Prevention May 7, 2018 1 Opiate Treatment & Overdose Prevention Project Goal Immediate:
The Accountable Community for Health of King County Addressing the Opioid Crisis Workgroup: Treatment and Overdose Prevention May 7, 2018 1 Opiate Treatment & Overdose Prevention Project Goal Immediate:
Disclosure Statement. Learning Objectives. American Psychiatric Nurses Association. Christian J. Teter, PharmD, BCPP 1 BUPRENORPHINE UPDATE
 BUPRENORPHINE UPDATE Christian J. Teter, Pharm.D., BCPP Associate Professor, Psychopharmacology College Of Pharmacy, University Of New England Portland, ME E-Mail: cteter@une.edu Image Source: pubchem.ncbi.nlm.nih.gov
BUPRENORPHINE UPDATE Christian J. Teter, Pharm.D., BCPP Associate Professor, Psychopharmacology College Of Pharmacy, University Of New England Portland, ME E-Mail: cteter@une.edu Image Source: pubchem.ncbi.nlm.nih.gov
Expanding Access To Medication Assisted Treatment for Opioid Use Disorders to Patients in the Hospital
 Expanding Access To Medication Assisted Treatment for Opioid Use Disorders to Patients in the Hospital August 28, 2018 Hosted by John A. Renner, Jr., MD, DLFAPA Professor of Psychiatry Boston University
Expanding Access To Medication Assisted Treatment for Opioid Use Disorders to Patients in the Hospital August 28, 2018 Hosted by John A. Renner, Jr., MD, DLFAPA Professor of Psychiatry Boston University
Opioid dependence and buprenorphine treatment
 Opioid dependence and buprenorphine treatment David Roll, MD Revere Family Health, Cambridge Health Alliance Instructor in Medicine, Harvard Medical School Joji Suzuki MD Medical Director of Addictions
Opioid dependence and buprenorphine treatment David Roll, MD Revere Family Health, Cambridge Health Alliance Instructor in Medicine, Harvard Medical School Joji Suzuki MD Medical Director of Addictions
MEDICATION ASSISTED TREATMENT
 MEDICATION ASSISTED TREATMENT MODULE 14 ALLIED TRADES ASSISTANCE PROGRAM PREVENTATIVE EDUCATION: SUBSTANCE USE DISORDER Medication Assisted Treatment Types of Medication Assisted Treatment: Methadone Naltrexone
MEDICATION ASSISTED TREATMENT MODULE 14 ALLIED TRADES ASSISTANCE PROGRAM PREVENTATIVE EDUCATION: SUBSTANCE USE DISORDER Medication Assisted Treatment Types of Medication Assisted Treatment: Methadone Naltrexone
Treatment Alternatives for Substance Use Disorders
 Treatment Alternatives for Substance Use Disorders Dean Drosnes, MD, FASAM Associate Medical Director Director, Chronic Pain and SUD Program Caron Treatment Centers 1 Disclosure The speaker has no conflict
Treatment Alternatives for Substance Use Disorders Dean Drosnes, MD, FASAM Associate Medical Director Director, Chronic Pain and SUD Program Caron Treatment Centers 1 Disclosure The speaker has no conflict
Demystifying Buprenorphine Prescribing for Youth With Opioid Use Disorders. Providers Clinical Support System Opioid Therapies (PCSSO) CME 6/21/2017
 CME 6/21/2017") Demystifying Buprenorphine Prescribing for Youth With Opioid Use Disorders Geetha A. Subramaniam MD, DFAACAP, DFAPA National Institute on Drug Abuse June 21, 2017 1 Providers Clinical Support System Opioid
Demystifying Buprenorphine Prescribing for Youth With Opioid Use Disorders Geetha A. Subramaniam MD, DFAACAP, DFAPA National Institute on Drug Abuse June 21, 2017 1 Providers Clinical Support System Opioid
Methadone and Naltrexone ER
 Methadone and Naltrexone ER Laura G. Kehoe, MD, MPH, FASAM Medical Director MGH Substance Use Disorder Bridge Clinic Assistant Professor of Medicine Harvard Medical School Disclosures Neither I nor my
Methadone and Naltrexone ER Laura G. Kehoe, MD, MPH, FASAM Medical Director MGH Substance Use Disorder Bridge Clinic Assistant Professor of Medicine Harvard Medical School Disclosures Neither I nor my
MAT in the Corrections Setting
 MEDICATION ASSISTED TREATMENT AND CORRECTIONS Frank Filippelli, DO, PhD September 2017 MAT in the Corrections Setting Who Does This Affect? What is MAT and What is the Evidence of Efficacy? Emphasis on
MEDICATION ASSISTED TREATMENT AND CORRECTIONS Frank Filippelli, DO, PhD September 2017 MAT in the Corrections Setting Who Does This Affect? What is MAT and What is the Evidence of Efficacy? Emphasis on
Substance Use Disorders (SUDs) and Medication Assisted Treatment (MAT) for Opiates
 and Medication Assisted Treatment (MAT) for Opiates") Substance Use Disorders (SUDs) and Medication Assisted Treatment (MAT) for Opiates What is MAT? Medication Assisted Treatment (MAT) is the use of medications, in addition to counseling, cognitive behavioral
Substance Use Disorders (SUDs) and Medication Assisted Treatment (MAT) for Opiates What is MAT? Medication Assisted Treatment (MAT) is the use of medications, in addition to counseling, cognitive behavioral
From Medicaid Transformation Approved Project Toolkit, June 2017
 From Medicaid Transformation Approved Project Toolkit, June 2017 Domain 3: Prevention and Health Promotion Transformation projects within this domain focus on prevention and health promotion to eliminate
From Medicaid Transformation Approved Project Toolkit, June 2017 Domain 3: Prevention and Health Promotion Transformation projects within this domain focus on prevention and health promotion to eliminate
SHARED CARE GUIDELINE FOR THE MANAGEMENT OF PATIENTS ON NALTREXONE FOR ALCOHOL DEPENDENCE INDICATION
 SHARED CARE GUIDELINE FOR THE MANAGEMENT OF PATIENTS ON NALTREXONE FOR ALCOHOL DEPENDENCE INDICATION Naltrexone is used as part of a comprehensive programme of treatment against alcoholism to reduce the
SHARED CARE GUIDELINE FOR THE MANAGEMENT OF PATIENTS ON NALTREXONE FOR ALCOHOL DEPENDENCE INDICATION Naltrexone is used as part of a comprehensive programme of treatment against alcoholism to reduce the
Revised 9/30/2016. Primary Care Provider Pain Management Toolkit
 Revised 9/30/2016 Primary Care Provider Pain Management Toolkit TABLE OF CONTENTS 1. INTRODUCTION Page 1 2. NON-OPIOID SERVICES &TREATMENTS FOR CHRONIC PAIN Page 2 2.1 Medical Services Page 2 2.2 Behavioral
Revised 9/30/2016 Primary Care Provider Pain Management Toolkit TABLE OF CONTENTS 1. INTRODUCTION Page 1 2. NON-OPIOID SERVICES &TREATMENTS FOR CHRONIC PAIN Page 2 2.1 Medical Services Page 2 2.2 Behavioral
Clinical Policy: Lofexidine (Lucemyra) Reference Number: ERX.NPA.88 Effective Date:
 Reference Number: ERX.NPA.88 Effective Date:") Clinical Policy: (Lucemyra) Reference Number: ERX.NPA.88 Effective Date: 07.31.18 Last Review Date: 08.18 Revision Log See Important Reminder at the end of this policy for important regulatory and legal
Clinical Policy: (Lucemyra) Reference Number: ERX.NPA.88 Effective Date: 07.31.18 Last Review Date: 08.18 Revision Log See Important Reminder at the end of this policy for important regulatory and legal
Use of Suboxone and Other Treatment Modalities: Myths, Facts & Tips for Better Outcomes
 Use of Suboxone and Other Treatment Modalities: Myths, Facts & Tips for Better Outcomes MPHP Prescribers Summit 2018 Gulfport, MS March 13, 2018 Scott Hambleton, MD, DFASAM Medical Director, MRO Mississippi
Use of Suboxone and Other Treatment Modalities: Myths, Facts & Tips for Better Outcomes MPHP Prescribers Summit 2018 Gulfport, MS March 13, 2018 Scott Hambleton, MD, DFASAM Medical Director, MRO Mississippi
Opioid Agonists. Natural derivatives of opium poppy - Opium - Morphine - Codeine
 Natural derivatives of opium poppy - Opium - Morphine - Codeine Opioid Agonists Semi synthetics: Derived from chemicals in opium -Diacetylmorphine Heroin - Hydromorphone Synthetics - Oxycodone Propoxyphene
Natural derivatives of opium poppy - Opium - Morphine - Codeine Opioid Agonists Semi synthetics: Derived from chemicals in opium -Diacetylmorphine Heroin - Hydromorphone Synthetics - Oxycodone Propoxyphene
An Alternative Payment Model Concept for Office-based Treatment of Opioid Use Disorder
 An Alternative Payment Model Concept for Office-based Treatment of Opioid Use Disorder CONTENTS I. Need for an Alternative Payment Model for Opioid Use Disorder and Addiction... 2 A. Improving Services
An Alternative Payment Model Concept for Office-based Treatment of Opioid Use Disorder CONTENTS I. Need for an Alternative Payment Model for Opioid Use Disorder and Addiction... 2 A. Improving Services
MGH Substance Use Disorder Initiative. Dawn Williamson, RN, DNP, PMHCNS-BC, CARN-AP MGH ED Christopher Shaw, RN, ANP, PMHNP-BC, CARN-AP MGH ACT
 Bridging the Gap: Bridging the Gaps to addiction treatment through comprehensive collaborative practice among Advanced Practice Nurses in a large urban Medical Center Dawn Williamson, RN, DNP, PMHCNS-BC,
Bridging the Gap: Bridging the Gaps to addiction treatment through comprehensive collaborative practice among Advanced Practice Nurses in a large urban Medical Center Dawn Williamson, RN, DNP, PMHCNS-BC,
Rule Governing the Prescribing of Opioids for Pain
 Rule Governing the Prescribing of Opioids for Pain 1.0 Authority This rule is adopted pursuant to Sections 14(e) and 11(e) of Act 75 (2013) and Sections 2(e) and 2a of Act 173 (2016). 2.0 Purpose This
Rule Governing the Prescribing of Opioids for Pain 1.0 Authority This rule is adopted pursuant to Sections 14(e) and 11(e) of Act 75 (2013) and Sections 2(e) and 2a of Act 173 (2016). 2.0 Purpose This
Medication Assisted Treatment. Karen Drexler, MD National Mental Health Program Director-Substance Use Disorders Department of Veterans Affairs
 Medication Assisted Treatment Karen Drexler, MD National Mental Health Program Director-Substance Use Disorders Department of Veterans Affairs Disclosures Employed by the Department of Veterans Affairs
Medication Assisted Treatment Karen Drexler, MD National Mental Health Program Director-Substance Use Disorders Department of Veterans Affairs Disclosures Employed by the Department of Veterans Affairs
Taking the pain out of prescribing: An opioid primer for the primary care provider
 Taking the pain out of prescribing: An opioid primer for the primary care provider Amy K. Paul, PharmD PGY1 Pharmacy Resident Pharmacy Grand Rounds April 26, 2016 2016 MFMER slide-1 Objectives Describe
Taking the pain out of prescribing: An opioid primer for the primary care provider Amy K. Paul, PharmD PGY1 Pharmacy Resident Pharmacy Grand Rounds April 26, 2016 2016 MFMER slide-1 Objectives Describe
Substitution Therapy for Opioid Use Disorder The Role of Suboxone
 Substitution Therapy for Opioid Use Disorder The Role of Suboxone Methadone/Buprenorphine 101 Workshop, December 10, 2016 Leslie Lappalainen, MD, CCFP, dip ABAM Prepared by Mandy Manak, MD, ABAM, CCSAM
Substitution Therapy for Opioid Use Disorder The Role of Suboxone Methadone/Buprenorphine 101 Workshop, December 10, 2016 Leslie Lappalainen, MD, CCFP, dip ABAM Prepared by Mandy Manak, MD, ABAM, CCSAM
Guidelines for Community Detoxification using Buprenorphine.
 Subject Title NHS Fife Community Health Partnerships Addiction Services Guidelines for Community Detoxification using Buprenorphine. Intranet Procedure No A3 Author Dr A Baldacchino Copy No 3 Reviewer
Subject Title NHS Fife Community Health Partnerships Addiction Services Guidelines for Community Detoxification using Buprenorphine. Intranet Procedure No A3 Author Dr A Baldacchino Copy No 3 Reviewer
QUARTERLY PROVIDER MEETING MARCH 9, 2017 SUZANNE BORYS, ED.D.
 2017 State Targeted Response to the Opioid Crisis Grants QUARTERLY PROVIDER MEETING MARCH 9, 2017 SUZANNE BORYS, ED.D. H.R.6-21st Century Cures Act The 21st Century Cures Act is a United States law enacted
2017 State Targeted Response to the Opioid Crisis Grants QUARTERLY PROVIDER MEETING MARCH 9, 2017 SUZANNE BORYS, ED.D. H.R.6-21st Century Cures Act The 21st Century Cures Act is a United States law enacted
Understanding Medication in Addiction Treatment for Drug Court Participants
 Understanding Medication in Addiction Treatment for Drug Court Participants Introduction This pocket guide is for drug court participants who may be prescribed or considering medication as a part of addiction
Understanding Medication in Addiction Treatment for Drug Court Participants Introduction This pocket guide is for drug court participants who may be prescribed or considering medication as a part of addiction
Clinical Guidelines and Coverage Limitations for Medication Assisted Treatment (MAT)
") Clinical Guidelines and Coverage Limitations for Medication Assisted Treatment (MAT) What has changed? Effective January 16, 2018, Coordinated Care will change the requirement for form HCA 13-333 Medication
Clinical Guidelines and Coverage Limitations for Medication Assisted Treatment (MAT) What has changed? Effective January 16, 2018, Coordinated Care will change the requirement for form HCA 13-333 Medication
Medication Treatment and Opioid Use Disorder
 Medication Treatment and Opioid Use Disorder Colleen T. LaBelle, MSN, RN-BC,CARN Program Director, Office-Based Addiction Treatment Director, STATE OBOT-B Boston Medical Center Disclosures I have no disclosures
Medication Treatment and Opioid Use Disorder Colleen T. LaBelle, MSN, RN-BC,CARN Program Director, Office-Based Addiction Treatment Director, STATE OBOT-B Boston Medical Center Disclosures I have no disclosures
Colleen T. LaBelle, MSN, RN-BC,CARN Program Director, Office-Based Addiction Treatment Director, STATE OBAT Boston Medical Center
 Colleen T. LaBelle, MSN, RN-BC,CARN Program Director, Office-Based Addiction Treatment Director, STATE OBAT Boston Medical Center Disclosures I have no disclosures or commercial interests to report Addiction
Colleen T. LaBelle, MSN, RN-BC,CARN Program Director, Office-Based Addiction Treatment Director, STATE OBAT Boston Medical Center Disclosures I have no disclosures or commercial interests to report Addiction
Medication Assisted Treatment. MAT Opioid dependence/addiction Opioid treatment programs OTP Regulation of OTP Office Based Treatment
 Medication Assisted Treatment MAT Opioid dependence/addiction Opioid treatment programs OTP Regulation of OTP Office Based Treatment Opioid Drugs Opium Morphine Heroin Codeine Oxycodone Roxycodone Oxycontin
Medication Assisted Treatment MAT Opioid dependence/addiction Opioid treatment programs OTP Regulation of OTP Office Based Treatment Opioid Drugs Opium Morphine Heroin Codeine Oxycodone Roxycodone Oxycontin
2016 American Academy of Neurology
 2016 American Academy of Neurology PCSS-O is a collaborative effort led by American Academy of Addiction Psychiatry (AAAP) in partnership with: Addiction Technology Transfer Center (ATTC), American Academy
2016 American Academy of Neurology PCSS-O is a collaborative effort led by American Academy of Addiction Psychiatry (AAAP) in partnership with: Addiction Technology Transfer Center (ATTC), American Academy
Building capacity for a CHC response to Ontario's Opioid Crisis
 Building capacity for a CHC response to Ontario's Opioid Crisis Rob Boyd Oasis Program Director Luc Cormier, RN, MScN Community Health Nurse Sandy Hill Community Health Centre #AOHC2016 @rboyd6 @SandyHillCHC
Building capacity for a CHC response to Ontario's Opioid Crisis Rob Boyd Oasis Program Director Luc Cormier, RN, MScN Community Health Nurse Sandy Hill Community Health Centre #AOHC2016 @rboyd6 @SandyHillCHC
Opioid Use in Youth. Amy Yule M.D. March 2,
 Opioid Use in Youth Amy Yule M.D. March 2, 2018 An opioid is a substance that acts on opioid receptors Beta-endorphin Endogenous opioids Dynorphin Opiates Natural products of the poppy plant Morphine Heroin
Opioid Use in Youth Amy Yule M.D. March 2, 2018 An opioid is a substance that acts on opioid receptors Beta-endorphin Endogenous opioids Dynorphin Opiates Natural products of the poppy plant Morphine Heroin
Disclosures. Objectives 2/5/2018. Women and opioid use disorder: Optimizing care during pregnancy and beyond
 Women and opioid use disorder: Optimizing care during pregnancy and beyond Susanne Astrab Fogger, DNP, PMHNP-BC, CARN-AP, FAANP Ashley L. Hodges, PhD, CRNP, WHNP-BC Disclosures Dr. Fogger has nothing to
Women and opioid use disorder: Optimizing care during pregnancy and beyond Susanne Astrab Fogger, DNP, PMHNP-BC, CARN-AP, FAANP Ashley L. Hodges, PhD, CRNP, WHNP-BC Disclosures Dr. Fogger has nothing to
SUBOXONE Film, SUBOXONE Tablets, and SUBUTEX Tablets. Risk Evaluation and Mitigation Strategy (REMS) Program
 Program") SUBOXONE Film, SUBOXONE Tablets, and SUBUTEX Tablets Risk Evaluation and Mitigation Strategy (REMS) Program Office-Based Buprenorphine Therapy for Opioid Dependence: Important Information for Prescribers
SUBOXONE Film, SUBOXONE Tablets, and SUBUTEX Tablets Risk Evaluation and Mitigation Strategy (REMS) Program Office-Based Buprenorphine Therapy for Opioid Dependence: Important Information for Prescribers
Protocol For: Personally Furnishing Naloxone. Update Log
 Protocol For: Personally Furnishing Naloxone Update Log Updated By: Reason for Update: Date: Approved By: K. Benick RN Original draft 6/7/16 Pam Butler Protocol: Personally Furnishing Naloxone_Morrow County
Protocol For: Personally Furnishing Naloxone Update Log Updated By: Reason for Update: Date: Approved By: K. Benick RN Original draft 6/7/16 Pam Butler Protocol: Personally Furnishing Naloxone_Morrow County
201 KAR 9:270. Professional standards for prescribing or dispensing Buprenorphine-Mono-Product or Buprenorphine-Combined-with-Naloxone.
 201 KAR 9:270. Professional standards for prescribing or dispensing Buprenorphine-Mono-Product or Buprenorphine-Combined-with-Naloxone. RELATES TO: KRS 311.530-311.620, 311.990 STATUTORY AUTHORITY: KRS
201 KAR 9:270. Professional standards for prescribing or dispensing Buprenorphine-Mono-Product or Buprenorphine-Combined-with-Naloxone. RELATES TO: KRS 311.530-311.620, 311.990 STATUTORY AUTHORITY: KRS
Clinical Guidelines and Procedures for the Use of Naltrexone in the Management of Opioid Dependence Abbreviated Version
 Clinical Guidelines and Procedures for the Use of Naltrexone in the Management of Opioid Dependence Abbreviated Version Clinical Guidelines and Procedures for the Use of Naltrexone in the Management of
Clinical Guidelines and Procedures for the Use of Naltrexone in the Management of Opioid Dependence Abbreviated Version Clinical Guidelines and Procedures for the Use of Naltrexone in the Management of
Stress, Relaxation, and Mindful Breathing: A Primer. Kevin E. Vowles, Ph.D. University of New Mexico
 Stress, Relaxation, and Mindful Breathing: A Primer Kevin E. Vowles, Ph.D. University of New Mexico 1 Educational Objectives At the conclusion of this activity participants should be able to: State the
Stress, Relaxation, and Mindful Breathing: A Primer Kevin E. Vowles, Ph.D. University of New Mexico 1 Educational Objectives At the conclusion of this activity participants should be able to: State the
Clinical Guidelines and Coverage Limitations for Medication Assisted Treatment (MAT)
") Clinical Guidelines and Coverage Limitations for Medication Assisted Treatment (MAT) For Apple Health clients served Fee-for-Service and through contracted Medicaid Managed Care Organizations Updated January
Clinical Guidelines and Coverage Limitations for Medication Assisted Treatment (MAT) For Apple Health clients served Fee-for-Service and through contracted Medicaid Managed Care Organizations Updated January
CDC Guideline for Prescribing Opioids for Chronic Pain. Centers for Disease Control and Prevention National Center for Injury Prevention and Control
 CDC Guideline for Prescribing Opioids for Chronic Pain Centers for Disease Control and Prevention National Center for Injury Prevention and Control THE EPIDEMIC Chronic Pain and Prescription Opioids 11%
CDC Guideline for Prescribing Opioids for Chronic Pain Centers for Disease Control and Prevention National Center for Injury Prevention and Control THE EPIDEMIC Chronic Pain and Prescription Opioids 11%
Module II Opioids 101 Opiate Opioid
 BUPRENORPHINE TREATMENT: A TRAINING FOR MULTIDISCIPLINARY ADDICTION PROFESSIONALS Module II Opioids 101 Module II Goals of the Module This module reviews the following:! Opioid addiction and the brain!
BUPRENORPHINE TREATMENT: A TRAINING FOR MULTIDISCIPLINARY ADDICTION PROFESSIONALS Module II Opioids 101 Module II Goals of the Module This module reviews the following:! Opioid addiction and the brain!
A Drug Court Team Member s Guide to Medication in Addiction Treatment
 A Drug Court Team Member s Guide to Medication in Addiction Treatment Introduction This pocket guide is intended for non-clinical drug court team members (e.g., court coordinators, judges, defense attorneys,
A Drug Court Team Member s Guide to Medication in Addiction Treatment Introduction This pocket guide is intended for non-clinical drug court team members (e.g., court coordinators, judges, defense attorneys,
Medical Assisted Treatment. Dr. Michael Baldinger Medical Director Haymarket Center Harborview Recovery Center
 Medical Assisted Treatment Dr. Michael Baldinger Medical Director Haymarket Center Harborview Recovery Center Current Trends Prescription Drug Abuse/Addiction Non-medical use of prescription pain killers
Medical Assisted Treatment Dr. Michael Baldinger Medical Director Haymarket Center Harborview Recovery Center Current Trends Prescription Drug Abuse/Addiction Non-medical use of prescription pain killers
Buprenorphine as a Treatment Option for Opioid Use Disorder
 Buprenorphine as a Treatment Option for Opioid Use Disorder Joji Suzuki, MD Assistant Professor of Psychiatry Harvard Medical School Director, Division of Addiction Psychiatry Brigham and Women s Hospital
Buprenorphine as a Treatment Option for Opioid Use Disorder Joji Suzuki, MD Assistant Professor of Psychiatry Harvard Medical School Director, Division of Addiction Psychiatry Brigham and Women s Hospital
Summary of Recommendations...3. PEG: A Three-Item Scale Assessing Pain (Appendix A) Chronic Pain Flow Sheet Acute Pain Flow Sheet...
 Chronic Pain Flow Sheet Acute Pain Flow Sheet...") Table of Contents Summary of Recommendations....3 PEG: A Three-Item Scale Assessing Pain (Appendix A)...12 Chronic Pain Flow Sheet...13 Acute Pain Flow Sheet...14 Pocket Guide: Tapering Opioids for Chronic
Table of Contents Summary of Recommendations....3 PEG: A Three-Item Scale Assessing Pain (Appendix A)...12 Chronic Pain Flow Sheet...13 Acute Pain Flow Sheet...14 Pocket Guide: Tapering Opioids for Chronic
Medication-Assisted Treatment (MAT) Overview
 Overview") Medication-Assisted Treatment (MAT) Overview 2014 Opiate Conference: Don t Get Me Started Hyatt Regency, Columbus, Ohio June 30-July 1, 2014 Christina M. Delos Reyes, MD Medical Consultant, Center for
Medication-Assisted Treatment (MAT) Overview 2014 Opiate Conference: Don t Get Me Started Hyatt Regency, Columbus, Ohio June 30-July 1, 2014 Christina M. Delos Reyes, MD Medical Consultant, Center for
The Role of Primary Care Teams and the Medical Neighborhood in Addressing the Opioid Crisis in Maine. March 10, 2016
 The Role of Primary Care Teams and the Medical Neighborhood in Addressing the Opioid Crisis in Maine March 10, 2016 Objectives Review current state of opioid crisis in Maine Briefly review physiology of
The Role of Primary Care Teams and the Medical Neighborhood in Addressing the Opioid Crisis in Maine March 10, 2016 Objectives Review current state of opioid crisis in Maine Briefly review physiology of
FY17 SCOPE OF WORK TEMPLATE. Name of Program/Services: Medication-Assisted Treatment: Buprenorphine
 FY17 SCOPE OF WORK TEMPLATE Name of Program/Services: Medication-Assisted Treatment: Buprenorphine Procedure Code: Modification of 99212, 99213 and 99214: 99212 22 99213 22 99214 22 Definitions: Buprenorphine
FY17 SCOPE OF WORK TEMPLATE Name of Program/Services: Medication-Assisted Treatment: Buprenorphine Procedure Code: Modification of 99212, 99213 and 99214: 99212 22 99213 22 99214 22 Definitions: Buprenorphine
Medication for the Treatment of Alcohol Use Disorder. Pocket Guide
 Medication for the Treatment of Alcohol Use Disorder Pocket Guide Medications are underused in the treatment of alcohol use disorder. According to the National Survey on Drug Use and Health, of the estimated
Medication for the Treatment of Alcohol Use Disorder Pocket Guide Medications are underused in the treatment of alcohol use disorder. According to the National Survey on Drug Use and Health, of the estimated
Policy on Pharmacological Therapies Practice Guidance Note Reducing Dosing Errors with Opioid Medicines V04
 Policy on Pharmacological Therapies Practice Guidance Note Reducing Dosing Errors with Opioid Medicines V04 Date issued Issue 1 Nov 2018 Planned review Nov 2021 PPT-PGN 18 part of NTW(C)38 Pharmaceutical
Policy on Pharmacological Therapies Practice Guidance Note Reducing Dosing Errors with Opioid Medicines V04 Date issued Issue 1 Nov 2018 Planned review Nov 2021 PPT-PGN 18 part of NTW(C)38 Pharmaceutical
POWER TO HELP REVERSE AN OPIOID OVERDOSE
 POWER TO HELP REVERSE AN OPIOID OVERDOSE FDA APPROVED Concentrated 4 mg dose Needle-free; no assembly required Designed for ease-of-use in the community setting Requires no specialized training* Not a
POWER TO HELP REVERSE AN OPIOID OVERDOSE FDA APPROVED Concentrated 4 mg dose Needle-free; no assembly required Designed for ease-of-use in the community setting Requires no specialized training* Not a
Buprenorphine Order Set and Rapid Access Referral. Copyright 2017, CAMH
 2 Buprenorphine Order Set and Rapid Access Referral 1 Agenda Problem Identification / Identification Importance / Importance Baseline Workflow Baseline Workflow Baseline Data Baseline Data Objectives Solution
2 Buprenorphine Order Set and Rapid Access Referral 1 Agenda Problem Identification / Identification Importance / Importance Baseline Workflow Baseline Workflow Baseline Data Baseline Data Objectives Solution
Prescribing Framework for Naltrexone in Relapse Prevention (Opioid Dependence)
") Hull & East Riding Prescribing Committee Prescribing Framework for Naltrexone in Relapse Prevention (Opioid Dependence) Patients Name: Unit Number: Patients Address:.. G.P s Name:.. Communication We agree
Hull & East Riding Prescribing Committee Prescribing Framework for Naltrexone in Relapse Prevention (Opioid Dependence) Patients Name: Unit Number: Patients Address:.. G.P s Name:.. Communication We agree
Opioid Use Disorders as a Brain Disease Why MAT is so important. Ron Jackson, M.S.W., L.I.C.S.W.
 Opioid Use Disorders as a Brain Disease Why MAT is so important Ron Jackson, M.S.W., L.I.C.S.W. Affiliate Professor School of Social Work University of Washington Organization Name: CareOregon Course Title:
Opioid Use Disorders as a Brain Disease Why MAT is so important Ron Jackson, M.S.W., L.I.C.S.W. Affiliate Professor School of Social Work University of Washington Organization Name: CareOregon Course Title:
Medication and Behavioral Treatment of Substance Use Disorders
 Medication and Behavioral Treatment of Substance Use Disorders Brian Fuehrlein, MD, PhD Director, Psychiatric Emergency Room, VA Connecticut and Assistant Professor of Psychiatry, Yale University 1 Brian
Medication and Behavioral Treatment of Substance Use Disorders Brian Fuehrlein, MD, PhD Director, Psychiatric Emergency Room, VA Connecticut and Assistant Professor of Psychiatry, Yale University 1 Brian
Initiation of Medication in Treating Opioid Use Disorder.
 Initiation of Medication in Treating Opioid Use Disorder. Colleen T. LaBelle MSN RN-BC CARN Program Director STATE OBAT B Nurse Manager Boston Medical Center OBAT Executive Director MA IntNSA *Images used
Initiation of Medication in Treating Opioid Use Disorder. Colleen T. LaBelle MSN RN-BC CARN Program Director STATE OBAT B Nurse Manager Boston Medical Center OBAT Executive Director MA IntNSA *Images used
Acute General Medical and Surgical Admission:
 Acute General Medical and Surgical Admission: Managing Substance Use Disorders in Patients Who are Severely Ill Scott Grantham, MD Executive Director, Behavioral Health Saint Francis Health System By the
Acute General Medical and Surgical Admission: Managing Substance Use Disorders in Patients Who are Severely Ill Scott Grantham, MD Executive Director, Behavioral Health Saint Francis Health System By the
See Important Reminder at the end of this policy for important regulatory and legal information.
 Clinical Policy: (Lucemyra) Reference Number: CP.PMN.152 Effective Date: 07.31.18 Last Review Date: 08.18 Line of Business: Commercial, HIM, Medicaid Revision Log See Important Reminder at the end of this
Clinical Policy: (Lucemyra) Reference Number: CP.PMN.152 Effective Date: 07.31.18 Last Review Date: 08.18 Line of Business: Commercial, HIM, Medicaid Revision Log See Important Reminder at the end of this
State Opioid Response (SOR) Grant
 Grant") State Opioid Response (SOR) Grant Adam Bucon, LSW DMHAS Provider Meeting September 20, 2018 Philip D. Murphy Governor Shereef M. Elnahal Commissioner Sheila Y. Oliver Lt. Governor NJ Opioid Statistics
State Opioid Response (SOR) Grant Adam Bucon, LSW DMHAS Provider Meeting September 20, 2018 Philip D. Murphy Governor Shereef M. Elnahal Commissioner Sheila Y. Oliver Lt. Governor NJ Opioid Statistics
Guidance for naltrexone prescribing
 Document level: Drug Alcohol (Trustwide) Code: DA7 Issue number: 2 Guidance for naltrexone prescribing Lead executive Authors details Type of document Target audience Document purpose Lead Clinical Director
Document level: Drug Alcohol (Trustwide) Code: DA7 Issue number: 2 Guidance for naltrexone prescribing Lead executive Authors details Type of document Target audience Document purpose Lead Clinical Director
Opioid Dependence and Buprenorphine Management
 Opioid Dependence and Buprenorphine Management Kevin Kapila, MD Fenway Health Medical Director of Behavioral Health Instructor in Medicine Harvard Medical School Learning Objectives Understand the rationale
Opioid Dependence and Buprenorphine Management Kevin Kapila, MD Fenway Health Medical Director of Behavioral Health Instructor in Medicine Harvard Medical School Learning Objectives Understand the rationale
Drug Misuse and Dependence Guidelines on Clinical Management
 Department of Health Scottish Office Department of Health Welsh Office Department of Health and Social Services, Northern Ireland Drug Misuse and Dependence Guidelines on Clinical Management An Executive
Department of Health Scottish Office Department of Health Welsh Office Department of Health and Social Services, Northern Ireland Drug Misuse and Dependence Guidelines on Clinical Management An Executive